Calcinosis cutis involves deposition of calcium salts in skin and subcutaneous tissue. It is commonly associated with autoimmune connective tissue diseases and can be a source of pain and disability1. It can occur in damaged or devitalized tissues in the presence of abnormal or even normal calcium/phosphorus metabolism. These calcifications can lead to contractures, muscle atrophy, skin ulceration and infections2. There are four types of calcinosis cutis: idiopathic, dystrophic, metastatic, and iatrogenic. Determining the type of calcinosis is very important for accurate management3.Calcinosis cutis is a condition seen in the middle to elderly aged population and has rarely been described in neonates in the medical literature. We discuss a neonate in the succeeding text who presented to our Emergency department with a leg swelling.
Case Report
A 20 days old full term neonate was brought to our Emergency department with right leg swelling for the past ten days. He was feeding well and was afebrile. On examination there was swelling of right lower leg including the right foot with minimal redness of overlying skin. We did x-rays of the right foot and right leg, which showed a sheath of cutaneous calcification in right foot (Image A and Image B) and anterior-lateral of right leg (Image C and Image D).
Image A
Image B
Image C
Image D
There was no evidence of any bony destruction. White cell count and other inflammatory markers were normal. Upon reviewing the previous records we found that soon after the birth the neonate was admitted with pneumonia and during the hospital admission there was extravasation of calcium gluconate infusion at the dorsum of the right foot which explains the whitish sheath seen in the imaging. Musculoskeletal ultrasound did not reveal any signs of fluid collection or periosteal swelling. The patient was treated conservatively and regular follow up was insignificant and showed complete regression of the swelling three months later.
Discussion
Calcinosis cutis is an uncommon disorder caused by an abnormal deposit of calcium phosphate in the skin in various parts of the body. It is often noted in the subcutaneous tissues of connective tissues diseases primarily systemic lupus erythematosus, scleroderma and juvenile dermatomyositis4,7. Four main types of calcinosis cutis have been recognized according to etiology: associated with localized or widespread tissue changes or damage (dystrophic calcification), that associated with an abnormal calcium and phosphorus metabolism (metastatic calcification), not associated with any tissue damage or demonstrable metabolic disorder (idiopathic calcification), and Iatrogenic2-3,6-7.
It is recommended that patients be evaluated for abnormalities of calcium and phosphorus metabolism and that they be assessed for associated systemic conditions, such as collagen vascular diseases, renal insufficiency, and vitamin D poisoning. Determining the exact type of calcinosis cutis is very important for selecting accurate management3. Many agents have been used for treatment of calcinosis but none has been accepted as a standard therapy. Case studies have shown that aggressive treatment of the underling inflammatory condition with intravenous immunoglobulin, anti TNF agents, thalidomide and haematopoietic stem cell transplantation has also led to improvement of the calcinosis1,3. Moreover, agents such as warfarin, bisphosphonates and diltiazem have been aimed at treating the process of calcinosis with varying success3.Some experts have advocated surgical excision in severe resistant cases4.Calcinosis cutis has been rarely reported in neonates. It almost exclusively occurs due to iatrogenic causes8. Calcium gluconate has been widely used in the treatment of neonatal hypocalcemia which is a common problem confronted in this age group. When extravasation of calcium gluconate occurs; swelling, erythema, signs of soft tissue necrosis or infection may be seen. Rarely local calcification appears, called calcinosis cutis9-10.
Plain radiography is gold standard for diagnosis but are initially negative because calcium solutions used therapeutically are radiolucent. X-ray findings usually appear within 1-3 weeks9.This is consistent with our case. The pathogenesis of calcinosis cutis caused by extravasation of IV calcium is degeneration and soft tissue necrosis11. If extravasation of calcium gluconate is suspected; the IV line must be removed immediately. Cold packs should be applied for 15 minutes four times a day to treat edema at extravasation sites and limb elevation for 48 hours is suggested12. Supportive care remains the main element of the treatment and only in case of skin necrosis and secondary infection, debridement and antibiotics should be used8.
Calcinosis cutis in neonate can be easily misdiagnosed ascellulitis, arthritis, pyogenic abscess, osteomyelitis and thrombophelibitis8.In the present case also initially we were suspecting an infectious etiology. Initial x-rays can be misleadingly normal as it take about ten days to precipitate. The clinical and radiological findings usually disappear over a span of 2-6 months which is compatible with our case too13.
Dengue made its debut as early as 1780, when Benjamin Rush described the condition as “break bone fever”. This hitherto unfamiliar infection has now grown to demand the attention of all public health care providers. It is a mosquito borne, fast emerging, viral infection manifesting in four serotypes (1). Approximately 2.5 billion people, living mainly in urban areas of tropical and subtropical regions, are estimated to be at risk of acquiring dengue infection (2). While dengue is endemic in more than 100 countries, most cases are reported from Southeast Asia and the western Pacific regions. Around 50 million cases and 24,000 deaths are estimated to occur in these 100 endemic countries. This includes hospitalisation of nearly half a million cases of dengue haemorrhagic fever (DHF), of which 90% are children. Treated (DHF)/dengue shock syndrome (DSS) is associated with a 1% mortality rate while mortality rate among untreated cases escalates to 20%(3,4).
India is one of the seven identified countries in the Southeast Asia region regularly reporting incidence of DF/DHF outbreaks. The first confirmed report of dengue infection in India dates back to 1940s, and since then more and more new states have been reporting the disease which mostly strikes in epidemic proportions often inflicting heavy morbidity and mortality, in both urban and rural environments.(5)
The various manifestations of dengue may not have a distinct line of demarcation: apart from the classic features, reports of rare presentations have recently become more frequent (6,7). During recent outbreaks in India, the clinical manifestations which were shown by the patients were slightly different from those in previous years(8).. There have been many reports of difficulties in the use of the previous classification, which were summarised in a systematic literature review (9). Difficulties in applying the criteria for dengue haemorrhagic fever in the clinical situation, together with the increase in clinically severe dengue cases which did not fulfil the strict criteria, led to the request for the classification to be reconsidered .Hence, WHO revised the dengue case classification into dengue (with or without warning signs), and severe dengue (10).The present study was done to analyse the clinical features, complications, cost incurred and outcome of cases admitted to a tertiary care teaching hospital in Bangalore.
Methodology:
A record based descriptive study was conducted in paediatric patients admitted with signs and symptoms suggestive of dengue fever to KIMS hospital Bangalore, during the period between January 2012 to December 2012. SD BioLine kit was used for testing with NS1 antigen\ IgM\ IgG. The medical records were perused for collecting data about these cases using a pre-designed proforma. Data was analysed for the clinical presentations, outcome and direct cost incurred in respect to hospital charges and laboratory investigations.
Results:
Out of 1230 cases admitted with clinical signs and symptoms suggestive of dengue syndrome 757 (61.5%) cases were found to be NS1 antigen\ IgM\ IgG positive for dengue. Among the 757 positive cases, males were 499 (65.9%) and females 258 (34.1%). The majority of the cases were in the school going age group and this consisted of 310 cases (41%) and adolescent children which accounted for 249 cases (33%), the median age being 8 years of age. The least number of cases were seen in infants which accounted for 45 cases (6%).
Table 1. Sex distribution
Age group
Male
Female
Total
Infant
31
14
45
Toddler
114
39
153
School going
208
102
310
Adolescent
146
103
249
TOTAL
499 (65.9%)
258(34.1%)
757
The majority, 88.5% of cases presented as dengue fever without warning signs, 6.34% with dengue fever with warning signs and 5.15% with severe dengue. Of the cases with warning signs 92.3% of cases had fever, 42.5% cases had vomiting and 38.2% cases had abdominal pain. Haemorrhagic manifestations were seen in about 4.5% of cases of which majority (87%) presented with petechiae followed by haematemesis (9%) and epistaxis (4%). Rashes were seen in 4% and arthralgia in 13% of cases. Pleural effusion was seen in 21% of cases and ascites was seen in 16% of cases. Complications in the form of acute respiratory distress syndrome (ARDS) was seen in 12.06% cases, 6% cases showed neurological manifestations in the form of encephalopathy and 1.3% cases had renal failure.
Table 2. Severity of dengue
SEVERITY
PERCENTAGE
DF without warning signs
88.5
DF with warning signs
6.3
Severe dengue
5.15
Table 3. Presenting complaints
Presenting Complaints
Number (%)
Fever
699(92.3)
Myalgia
148(19.5)
Haemorrhagic manifestations
34(4.5)
Vomiting
321(42.5)
Abdominal pain
289(38.1)
Headache
201(26.5)
Arthralgia
99(13)
Diarrhoea
80(10.5)
Others
121(16)
Fig 1 presenting complaints.
Haemoglobin level of > 12gm% was found in 73.4% cases, 9-12gm% in 23.4%, 6-9gm% in 2.1% and <6 gm% in 1.1% of cases. Platelet count of < 20,000 was found in 21.5% of cases, 20-50 thousand in 39.5% , 50,000 to 1.5 lakh in 36% of cases and >1.5 lakh was found in 3% of cases. Majority (65.5%) of cases were NS1 Ag positive alone or with IgM/ IgG/ or both positive.
Remaining were positive for either of the antibodies.13.7% cases werepositive for all the three i.e. Ag, IgM,& IgG. The mortality rate was found to be 8.6%
Figure 2: outcome
Cost incurred which includes direct cost (transporting patient to the hospital, diagnostic testing and laboratory investigations, medications, hospitalisation, food) was found to been average of Rs.12,611=00. The indirect cost loss of wages of patient &attendants) was found to be an average of Rs.3, 109=00. The hidden cost (out of pocket expenses) was found to be an average of Rs.50=00. The cost of treatment of other co-morbid conditions was found to be an average of Rs.2, 275=00. The total cost of treating dengue syndrome was 18,045=00
Discussion:
In the present study it was found that males were commonly affected and the most common age group was between 5 to 15 yrs of age. Similar results were reported in a study by Faridi et al, 76% of all cases of DHF /DSS were aged 6 years or more[11].
In the present study, the most common presenting symptoms was fever followed by vomiting and abdominal pain which is similar to study done by Kumar A et al showed fever in 99.2% followed by myalgia (64.6%), vomiting (47.6%), headache (47.6%) and abdominal pain (37.5%) (12).
In the present study, the most common bleeding manifestation was haematemesis and epistaxis. In a study by Ratageri et al, common bleeding manifestations were gastrointestinal bleeding (22%) and petechiae (18%) [13]. The gastrointestinal tract was reported as the commonest site of bleeding (61%) in a study by Ahmed et al [14].
In the present study majority of cases had platelet count between 20,000 to 50,000/mm3.In a study by Kamath et al, platelet counts less than 50,000/mm were noted in 62.3% [15]. In our study complicated cases showed ARDS and neurological manifestations in the form of encephalopathy. Almost all the cases which expired were found to have ARDS. Dengue associated ARDS is associated with a high mortality [16]. Dengue infection is found to cause neurological manifestation ranging from non-specific symptoms to encephalitis and rarely Guillain-Barre Syndrome [17]. In our study the mortality rate was found to be 8.6% , in the study by Anju et al overall mortality seen was 6% [18], compared to 3% by Ahmed et al [14].
Conclusion:
The seropositivity for dengue was 61.5% with NS1 antigen\ IgM\ IgG. Males were commonly affected and most vulnerable age group was found to be 5-15 year olds. The median age was 8 years. 88.5% of cases presented as dengue fever without warning signs, the remaining being dengue with warning signs and severe dengue. Fever was the most common symptom seen followed by vomiting and abdominal pain. Haemorrhagic manifestations were seen in about 4.5% of cases of which majority presented with petechiae followed by haematemesis. The mortality rate was 8.6%. Acute Respiratory Distress Syndrom (ARDS) and multiple organ dysfunction syndrome (MODS) was found to be the most dreadful complications with high rates of mortality .
In this study it was found that cost incurred which includes direct cost (transporting patient to the hospital, diagnostic testing and lab investigations, medications, hospitalisation, food) was found to bean average of Rs. 12,611=00. Thus dengue syndrome also causes significant economic burden on the patients.
In the recent few years, the world has seen varied clinical presentation of the dengue fever in different epidemics, even in the same regions and even with the period of time. Where some known features are still manifesting, few atypical features are noted from several parts of the world. A continuous seroepidemiological surveillance and timely interventions are needed to indentify the cases, so that its complications, outbreak and mortality can be minimised.
Moreover community awareness, early diagnosis and management and vector control measures need to be strengthened, especially during peri-monsoon period, in order to curb the increasing number of dengue cases.
Polyarteritis nodosa (PAN) is a rare vasculitis in childhood. Since first described by Kussmaul and Maier in 1866 1, there have been approximately 140 pediatric case reports in the literature. Traditionally, children were classified as having one of three forms: infantile, cutaneous, and systemic. Infantile PAN is now recognized as a severe form of Kawasaki disease. Criteria for a diagnosis of systemic PAN in childhood have been proposed but not validated2.
Cutaneous PAN (cPAN) is recognized as a separate entity but there are no diagnostic criteria for cPAN2. cPAN is characterized by disease affecting the skin with no major organ system involvement. The cutaneous symptoms are similar to systemic PAN and mild fever, muscle, joint, and peripheral nervous system involvement may also occur. Fever, rash, and musculoskeletal symptoms are common in children and cPAN needs to be differentiated from other diagnostic entities. Definitive diagnosis is by histopathologic evidence of necrotizing inflammation of the medium and small-sized arteries. There is a paucity of knowledge of the spectrum of clinical presentation and management of children with cPAN. Here we describe a case of cPAN and summarize the clinical manifestations, laboratory data and treatment regimens of our patient.
Case report
This 10 year old female adolescent presented with pain in both the elbow joints followed by pain in the left knee joint and both the ankle joints in a course of 8 days and fever for the past 2 days .On admission her vitals were stable, both the elbow joints were tender and the knee and ankle joints were swollen and tender .She had multiple subcutaneous nodules over extensor aspect of both her forearms, both her tibial shins and few on her thighs. Systemic examination showed presence of a soft PSM of grade 2 intensity over left sternal edge. Blood investigations showed leucocytosis, elevated CRP, elevated ASLO titres and 2Decho revealed a mild tricuspid regurgitation. An initial diagnosis of acute rheumatic fever was made and child was started on penicillin and Aspirin. But child continued to have excruciating arthralgia and hence a rheumatologist opinion was taken. Child was advised a skin biopsy from the nodular lesions which showed small and medium vessel vasculitis suggestive of cutaneous polyarteritis nodosa. Hence she was stopped with aspirin therapy , given pulse therapy with methyl prednisolone and continued with penicillin therapy .Her arthralgia subsided within a day of pulse therapy and the subcutaneous nodules gradually disappeared .On discharge child was put on oral steroid therapy and penicillin prophylaxis and advised regular follow up.
Fig1 showing segmental fibrinoid necrosis with inflammatory infiltrates of small artery.
Fig2 showing leukocystoclastic vasculitis with fragmentation of neutrophils in and around blood vessels.
DISCUSSION:
cPAN is not common in the pediatric population with approximately 140 cases reported in the literature. Disease is limited to skin, joints, and muscles in the majority with a minority having nerve involvement. Constitutional symptoms are common. Most children have a chronic and relapsing benign course.
The precise etiology of cPAN remains to be unknown. However, an immune mediated mechanism has been postulated. Several infectious and noninfectious conditions have been associated both to initiation and relapse of the disease3,4,5. Among them, streptococcal infection has been commonly implicated6,7. Although some evidence of streptococcal infection as an initiating factor for cPAN is present, caution must be exercised when interpreting elevations in the serologic markers of streptococcal infection in the absence of an appropriate clinical presentation.
Cutaneous and systemic PAN share the same histopathologic features of necrotizing arteritis of small and medium sized vessels. Kussmaul and Meier described the first case of systemic PAN in 1866 1. Early reports 8,9 confirm that cPAN is a separate entity to systemic PAN. We have limited our definition of cPAN to disease affecting the skin, muscle, joints, and peripheral nervous system, with corresponding biopsy confirmation. Any evidence of visceral involvement, either clinically (central nervous system, pulmonary, cardiac, gastrointestinal, or renal), radiographically (abnormal angiography), or by histology (visceral biopsy) were classified as systemic PAN. Nakamura et al 10 proposed further restriction of the definition of cutaneous PAN in that any extracutaneous involvement such as peripheral neuropathy and myalgias must be limited to the same area as skin lesions. Systemic PAN and cPAN appear to be fairly distinct entities on a clinical continuum. There are only 5 reported cases of cPAN evolving into systemic PAN 11,12.
On review of treatment regimens reported in the literature, most children respond to corticosteroids. Penicillin should be considered in children with increased ASO titres 13,14. Recent case series report success with low-dose methotrexate, cyclophosphamide, intravenous immunoglobulin, and biologic therapies 15,16.
In summary, cPAN can be challenging to diagnose and manage. A diagnosis of cPAN should be considered in a child with fever, tender subcutaneous nodules, livido reticularis, and arthralgias/arthritis. Most children respond to corticosteroids and have a benign course, but some children may be corticosteroid dependent or corticosteroid resistant, necessitating other immunosuppressive agents including DMARDs and biologic therapy. Multicentre pediatric vasculitis disease registries are necessary to inform development and standardization of best clinical practice for childhood cPAN.
A 34 week preterm, small for gestational age, third born male neonate to a non consanguinous married couple with father having short extremities was admitted in our NICU prematurely with respiratory distress.
On examination the baby was tachypneic with grunt and lower chest indrawing. The baby was also found to have a narrow thorax, short fingers with postaxial polydactyly in both upper limbs and right lower limb, with syndactyly in right upper and lower limb (figures 1,2,3). The cardiovascular, respiratory, abdominal and neurological examination were unremarkable with no facial dysmorphism. The fundus examination was inconclusive.
The antenatal scan showed all long bones short in configuration. The liver function tests were normal except for mild elevation of alkaline phosphatase. The Ultrasound abdomen showed hepatomegaly and no evidence of any other mass lesions. The urine examination was negative for proteinuria and haematuria. The chest x ray showed short ribs, high position of clavicle and features of hyaline membrane disease (Figure 4).
The baby was put on continuous positive airway pressure and given surfactant through an endotracheal tube twice for two consecutive days, but as the condition deteriorated, with hypercarbia and hypoxia as evident on arterial blood gases, the baby was electively ventilated with minimal settings. The baby improved and hence was extubated. After a few hours of being extubation the baby gradually developed respiratory distress and started to deteriorate. Hence the baby was reintubated. The condition of baby was explained to attenders and as the attenders were not willing to continue the treatment, the baby was discharged from hospital against medical advice and later we were informed that the baby expired within few hours after discharge from the hospital.
Fig 1 : showing long narrow thorax and short upper extremities
Fig 2 : showing postaxial polydactyly with syndactyly in upper extremity
Fig 3 : showing polydactyly with syndactyly in lower extremity
Fig 4 : chest xray showing long narrow thorax and short and horizontally oriented ribs with irregular costochondral junctions and bulbous and irregular anterior ends
Discussion
Jeune syndrome or asphyxiating thoracic dystrophy is a rare autosomal recessive skeletal dysplasia characterised by a small chest and short ribs which restrict the growth and expansion of the lungs1. The inheritance is autosomal recessive and a locus has been identified on chromosome 15q13 2. Other symptoms may include shortened bones in the arms and legs, unusually shaped pelvic bones, and extra fingers and/or toes (polydactyly)3 . It is estimated to occur in 1 per 1,00,000 -1,30,000 (again is this 130,000?) live births4.. The diagnosis is based on clinical and radiological findings. Our patient fulfills the diagnostic criteria for Jeune syndrome. The most consistent and characteristic findings were the abnormalities of the thoraxand limbs. Jeune syndrome was first described in 1955 by Jeune in two siblings with severely narrow thorax5. It is known to be genetically heterogeneous.
Several complications of asphyxiating thoracic dystrophy have been described in the literature. The respiratory problems are the main concern. A large percentage of the children with asphyxiating thoracic dystrophy die as a result of these problems. Percentages up to 80% have been mentioned in literature6,7. In our case the baby experienced respiratory distress on day one of life needing ventilator support. The thoracic malformation tends to become less pronounced with age8. A possible explanation could be the improved mechanical properties of the chest wall with growth.
Clinically, Jeune syndrome is characterized by a small, narrow chest and variable limb shortness. Associated congenital abnormalities can be postaxial polydactyly of both hands and/or feet (20%). Typical radiographic findings include a narrow, bell-shaped thorax with short, horizontally oriented ribs and irregular costochondral junctions, elevated clavicles, short iliac bones with a typical trident appearance of the acetabula, relatively short and wide long bones of the extremities, and hypoplastic phalanges of both hands and feet with cone-shaped epiphyses9. The reported case has long narrow chest, short and horizontally oriented ribs with irregular costochondral junctions and bulbous and irregular anterior ends with post axial polydactyly in both upper extremities and right lower limb with left lower limb being normal.
Jeune syndrome is sometimes compatible with life, although respiratory failure and infections are often fatal during infancy. The severity of thoracic constriction widely varies. For those patients who survive infancy, the thorax tends to revert to normal with improving respiratory function. This suggests that the lungs have a normal growth potential and the respiratory problems are secondary to restricted rib cage deformity 10.
Gastro-oesophageal reflux (GOR) is the passage of gastric contents into the oesophagus. In most infants with GOR the outcome is benign & self-limiting. (1)
Incidence/Prevalence
Peak incidence of GOR is around 4 months of age, and it resolves spontaneously by 1-2 years of age in most patients. (2)
Regurgitation (possetting or spitting up) is the most common presentation in infants with GOR. Regurgitation of at least one episode a day is seen in:
50% of infants 0-3 months
67% of infants at 4 months
5% at 10 to 12 months of age (3)
It is important to note that in infants (younger than 1 year of age) who are otherwise well and symptomatic, regurgitation may be considered entirely normal. (4)
Causes/Risks
GOR occurs due to the transient, inappropriate relaxation of the lower oesophageal sphincter, which allows the stomach contents to pass into the oesophagus.
GOR can be physiological or pathological:
Physiological GOR – when the infant has normal weight gain and experiences no complications and is generally well.
Pathological GOR – also known as gastro-oesophageal reflux disease (GORD) is when reflux is associated with other symptoms like failure to thrive or weight loss, feeding or sleeping problems, chronic respiratory disorders, oesophagitis, haematemesis etc (3)
Several anatomical and physiological conditions make infants (younger than 1 year of age) more prone to GORD than older children and adults:
Short, narrow oesophagus
Delayed gastric emptying
Shorter, lower oesophageal sphincter that is slightly above, rather than below, the diaphragm
Liquid diet and high calorie requirements, putting a strain on gastric capacity
Larger ratio of gastric volume to oesophageal volume(4)
Most children have no specific risk factors for GORD. Children with the following conditions are at increased risk for developing GORD and for progressing to severe GORD:
Severe neurological impairment
Prematurity
Cystic fibrosis
Gastro-oesophageal abnormalities (even after surgical repair), e.g. Oesophageal atresia, diaphragmatic hernia, pyloric stenosis
Bronchopulmonary dysplasia (preterm infants with lung disease)
Hiatus hernia
Oesophageal sphincter disorders
Raised intra-abdominal pressure(5)
Symptoms
GORD in infants and children can present with a variety of symptoms many of which can be relatively non-specific. Equally, other pathologies may lead to the development of reflux. Those in the early years tend to be based on observations by parents, while older, more vocal children express symptoms more akin to adult presentations.
As such, the history/symptoms will be broadly divided into those expected for infants (<1yr), young children (1-5yrs) and older children (>5yrs).
Infants(6-10)
Excessive possetting/regurgitation
Possetting is a normal phenomenon in infants
Frequent episodes, together with vomiting may indicate underlying GORD
Projectile vomiting may indicate an obstructive pathology
Difficult/rapid cessation of feeds
There may be difficulty initiating feeds and latching
Early cessation may be precipitated with the onset of reflux
Failure to thrive
No weight loss can be expected
Weight loss crossing centiles on the growth chart must be addressed urgently
Sleep disturbance
Particularly after an evening feed
This is often associated with irritability and inconsolable crying
Irritability and inconsolable crying
One of the commonest presentations to the GP
This may occur during feeds or shortly afterwards
Apnoeic episodes
A witnessed pausing in respiratory effort
Occurring at night, it can mimic obstructive sleep apnoea
This may indicate a more serious underlying pathology and requires urgent assessment
It is likely to be more prevalent in this age group
Young Children(6-10)
Regurgitation/vomiting
Beating/rubbing the chest may be an early sign of this pathology
Reflux symptoms can be typical of those in adults
Failure to thrive
Refusing food
Similar to the infant, however, the younger child can be more vocal in their refusal
Abdominal/chest pain
With increasing age, children may demonstrate gastric irritation with abdominal pain
Acid reflux producing oesophagitis may present as chest discomfort
Both are similar to symptoms adults experience
Irritability
Persistent/nocturnal cough/wheezing
There may be a dry, non productive cough
Secondary to pharyngeal irritation
There may be no co-morbidities or underlying pathologies
Symptoms can be mistaken for asthma by parents
Older Children (9)
Dyspepsia/vomiting
These symptoms in older children are thought to have a similar reliability in diagnosis as in adults
Dysphagia/odynophagia
As children become more articulate they may be able to describe these symptoms in relation to meals
Particularly with chronic GORD and the development of a Barrett’s Oesophagus
Abdominal/chest pains
Persistent/nocturnal coughing/wheezing
Other Symptoms
Symptoms which can be identified but which maybe considered less life-threatening include:
Dental erosions
Hiccups
Halitosis
Those deserving urgent investigation and intervention include:
Forceful/Bilious vomiting
Suggesting a possible obstructive pathology
This requires urgent surgical referral
Force of vomiting may not always indicate the severity of the problem
Upper gastrointestinal bleeding/hematemesis
This may be a consequence of increased pressure from vomiting
Similar to a Mallory-Weiss pathology
An urgent review by local Paediatric Gastroenterologists is warranted
Profuse diarrhoea or constipation
Failure to thrive/weight loss
Lethargy
Apnoeic episodes
Physical Signs
As with the previous section, physical signs will be considered for each age range as above: infants (<1yr), young children (1-5yrs) and older children (>5yrs).
Infants(9)
Irritability when lying flat
Particularly following feeds
Especially when supine
Weight loss
Regular monitoring with repeat measurements
A single weight cannot imply loss
This is usually a late sign
Arching of the back
Secondary to oesophageal irritation
Can be associated with increased tone and crying
Dehydration
Loss of fluid through vomiting
Look for
Dry mouth
Sunken fontanelle
Prolonged capillary refill time
Reduced skin turgor
Reduced urine output
Crying without tears
Apnoeas
Periods of reduced respiratory effort
Noted by parents as pauses in breathing
Young Children(9)
Weight loss
Dehydration
Anaemia
Associated with chronic symptoms and gradual loss of iron
Look for Pallor/pale conjunctivae, Glossitis, Angular stomatits, Pica
Dysphagia/choking with food
Particularly with prolonged GOR and development of stricturing
Difficulty in breathing/wheezing/lower respiratory tract infection (LRTI)
Similar to asthma on examination
Signs of LRTI on auscultation
Possibly stridor
Older Children(9)
Weight loss
Dehydration
Anaemia
Dysphagia/Choking with food
Difficulty in breathing/Wheezing/LRTI
Persistent sinusitis
Signs requiring urgent intervention include(9):
Hematochezia
Unaltered blood in stool
Stools take on a red appearance
Onset of vomiting after 6 months of life
Fever
Uncommon with GOR
Indicating an infective pathology
Hepatosplenomegaly
An underlying condition other than GOR is likely
Important pathologies must not be missed
Bulging fontanelle
Indicating increased intracranial pressure and an alternative pathology underlying the reflux
Macro/microcephaly
Suggestive of hydrocephalus or a congenital malformation
Seizures
Related to a number of other problems
Metabolic pathologies should figure highly in any differential diagnosis
Abdominal distension with reduced bowel sounds
Tinkling bowel sounds and an pain may suggest bowel obstruction
Differential diagnoses
Common differential diagnoses have been noted in Table 1, however, this is by no means a definitive list of conditions or presentations. It should be taken as an indication to the diverse presentations that can mimic or precipitate GOR (adapted from (9) and (10)).
Condition
History/Symptoms
Signs
Pyloric Stenosis
Sudden onset vomiting Constantly hungry baby Usually males First 4-6 weeks of life
Non-bilious projectile vomiting Visible peristalsis Positive test feed
Malrotation
Sudden onset pain in volvulus Reduced bowel movement Vomiting
Bilious vomiting Abdominal distension Pulling up legs with pain onset
Cow's Milk Allergy
Vomiting and Diarrhoea Eczema Relationship to feeds Failure to thrive
Urticaria Watery stool Weight loss crossing centiles
Constipation
Infrequent stools Straining Blood in nappy
Palpable stool on examination Irritable baby
Urinary Tract Infections
Vomiting Fever (can be without focus) Poor feeding
Lethargy Reduced urinary output Abdominal pain
Viral Gastroenteritis
Vomiting Diarrhoea Fever Lethargy
Dehydration Viral Rash
Hypocalcemia
Poor feeding Lethargy Tetany Seizures
Seizures Apnoeas Tremor Abdominal distension
Hydrocephalus
Vomiting Lethargy Confusion Visual changes
Increased head size Gait change Altered consciousness
Meningitis
Fever Lethargy Vomiting Confusion
Neck stiffness Photophobia Rash (late onset)
Drugs/Toxins
Vomiting Lethargy Ingestion history
Dependant upon drug ingested
Table 1
Investigations and management of infants (<1 yr old)
Complicated cases of GORD (not gaining weight/faltering growth or non-GI symptoms e.g. cough), should be referred to a Paediatrician while investigating for causes and instituting simple management.
Simple investigations to do in primary care:
Abdominal examination for hernias/pyloric stenosis (test feed)
Urine dip to rule out UTI
Blood tests for electrolyte abnormalities, coeliac screen (if weaned)
Referral to a Paediatrician will result in imaging investigations such as Abdominal x-ray and upper GI contrast study to rule out malrotation/hiatus hernia/achalasia in older children, sometimes GORD can be seen on contrast studies. The Paediatrician may go on to arrange a pH/impedance study, upper GI endoscopy or allergy testing.
Management
Calculate feed requirements, parents may be over feeding, e.g. approximate fluid requirement 100-120ml/kg/day every 3-6hrs (depending on age and whether weaned on to solids)
In thriving infants there is no evidence that pharmacological therapy will make a significant difference to symptoms.
Therefore the mainstay of management is reassurance. Simple pharmacological intervention can be tried with feed thickener (in formula fed babies) or Alginates e.g. Gaviscon (can be mixed with water for breast fed babies)
If there are continued concerns refer to Paediatrician for on going investigations and management.
Recent evidence shows that some infants may have cow’s milk protein intolerance (9). Therefore for breast fed babies the mother could try cutting out dairy from her diet (important to have supervision from dietician re: nutritional requirements while breast feeding). Formula fed babies can have a 2 week trial of hydrolysed/amino acid based formula e.g. Progestimil, Nutramigen, Neocate.
Reviews from ESPGHAN (9) and DTB (11) recommend H2RA (H2 receptor antagonists eg. Ranitidine) may help, though there is little evidence – these could be commenced while waiting for an appointment with the Paediatrician.
(Currently there is no role for Domperidone. The next medication a Paediatrician may try is Omeprazole ± omission of cow’s milk protein) (11)
Investigation and management of older children (>18mths)
As before, complicated cases of GORD (not gaining weight/faltering growth or non-GI symptoms e.g. cough), should be referred to a Paediatrician while investigating for causes and instituting simple management.
Investigations
Urine dip, if there are symptoms of vomiting
Stool H. Pyloti antigen test
Bloods tests inc. inflammatory markers, H. Pylori antigen, celiac screen
Management
If main symptom heartburn with no evidence of H. Pylori:
Reassurance and lifestyle changes (weight loss, dietary changes, timing of meals), up to 4 week trial of PPI (Proton pump inhibitor e.g. lansoprazole, omeprazole).
If symptoms improve then continue PPI for up to 6 months, then wean off over 4 weeks (evidence that if stopped suddenly patients may get rebound symptoms) (10).
If PPI doesn’t help or symptoms recur after stopping the PPI, then refer to a Paediatrician.
The Paediatrician may investigate with more blood tests e.g. Autoimmune screen, allergy testing, imaging, pH/impedance study, endoscopy.
Bronchogenic cysts are lesions of congenital origin derived from the primitive foregut. They form due to ectopic budding of the foregut during the first trimester. Epithelial cells of the developing trachea and lung are pinched off and grow separately from the airways. Bronchogenic cysts are most commonly mediastinal, unilocular and contain clear fluid. Clinically, most cysts are symptomatic and occur in infancy or early childhood. Respiratory distress is the most common presentation in paediatric patients, manifested by recurring episodes of cough, stridor, and wheezing. Patient Description: A 13-year-old female presented with a two month history of right-sided back pain and five days of intermittent fever. The pain was worse on inspiration and made sleeping difficult. She denied wheezing, chest pain, or cough. She continued daily participation in competitive sports. Previous trials of antibiotics and an inhaled bronchodilator for presumed exercise-induced asthma were unsuccessful. Chest x-ray (CXR) showed a large cyst (10x10x8 cm3) in the posterior right lung. (Image 1). Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2) Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4) Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid. Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung. Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
Bronchogenic cyst should be included in the differential diagnosis of a child with cough, dyspnoea, and fever. Although rare, we stress the importance of keeping mycobacterial infection in mind in cases of an infected cyst. Acid-fast culture should be done on sputum and cyst contents. Due to the frequency of negative cultures, stains should also be performed on resected cyst specimens. Antibiotic therapy should be considered and administered based on the extent of infection. All symptomatic or enlarging cysts warrant surgical excision. Prophylactic removal of asymptomatic cysts is recommended due to higher rates of perioperative complications once cysts become symptomatic.10 We raise the question of whether earlier CXR is indicated to rule out bronchogenic cyst, particularly when patients do not improve after trials of watchful waiting, antibiotics, and bronchodilators for other possible respiratory diagnoses.
To identify risk factors predicting readmission of neonates within 7 days of birth and to implement guidelines to reduce this.
METHOD
All babies less than 1 week old either admitted to, or assessed at paediatric unit at Crosshouse hospital, Kilmarnock between July 2006 and December 2006 were included. Data was analysed on birth weight, gestation, age at discharge from maternity unit, age at admission to Crosshouse hospital, source of referral, problems necessitating referral, feeding, interventions, and length of stay.
RESULTS
We managed to obtain case notes for 50 babies out of the 55 who were admitted during this time. 44 babies (88%) were discharged from maternity unit within 48 hrs of birth and 23 babies (46%) were discharged from maternity unit within the first 24 hrs. Poor feeding/weight loss and physiological jaundice accounted for majority of admissions. Further poor feeding and weight loss were more common in first borns, in early discharges and in breast-fed babies.
RECOMMENDATIONS
Mothers deciding to breast-feed babies need proper support. It may be a good idea to delay discharge check until 24 hours after birth. First time mothers are especially naive when it comes to breast-feeding and it is important that they get properly supervised.
It may be a good idea to request mothers to fill in a questionnaire prior to discharge regarding how confident they feel about feeding their child, any feeding concerns, any other concerns etc.
ABBREVIATIONS
AMU: Ayrshire Maternity unit
CMW: Community mid wife
INTRODUCTION
The length of post partum stay in hospital has been steadily declining over the past 50 years.1,2 Reducing the number of days in the hospital after birth has several advantages like helping mother and infant recover in a familiar home environment; decreasing the risk of iatrogenic infections and cutting down on hospital costs. However, concerns have also been expressed about potential disadvantages of early discharge: For example breastfeeding is not established until the third or later postpartum day; a number of conditions do not manifest themselves until two or more days after the delivery.3 In a large study on neonatal mortality done in Washington (retrospective study looking at 47879 births between 1989 and 1990), it was found that neonates discharged before 30 hrs of age had a significantly higher mortality in the first month and first year of life than those neonates who were discharged later.4 In the United States, this has prompted the introduction of legislation making minimum 48 hour postpartum hospital stay mandatory. Through our audit, we aimed to identify risk factors predicting readmission and to implement local guidelines to reduce readmission rates.
METHOD
All babies less than 1 week old either admitted to, or assessed at paediatric unit at Crosshouse hospital, Kilmarnock between July 2006 and December 2006 were included. It was a retrospective study. List of patients was available from Medical records and paediatric case notes were obtained from medical records. The neonatal case notes were obtained from neonatal secretaries at AMU.
55 babies were admitted during this time out of which we managed to obtain paediatric and neonatal case notes for 50 babies. Data was analysed on birth weight, gestation, age at discharge from AMU, age at admission to Crosshouse hospital, source of referral, problems necessitating referral, feeding, interventions, and length of stay.
RESULTS
Most of the referrals were generated from community midwives who are often the first point of contact for neonates discharged from maternity unit (Table 1)
Source of referral (Table 1)
Source of referral
Number of babies
CMW
39
GP
5
A&E
4
Self
2
Total
50
We looked at the problems necessitating admission (Table 2). Please note that babies had more than one problem. Hence the higher numbers!
It is obvious looking at the numbers that most of the admissions are secondary to poor feeding and weight loss, majority of which could have been prevented.
Problems necessitating admission (Table 2)
Problems
Number of babies
No of babies in whom this problem was noted in AMU
Poor feeding
20
7
Wt loss >10%
18
0
Physiological jaundice Requiring phototherapy
14
1 (SBR was below treatment line)
Physiological jaundice Not requiring phototherapy
8
1
Choking episode
5
1
ABO incompatibility Requiring phototherapy
1
0 (No DCT done)
Pseudo menstruation
2
0
? Reflux (Blue episode)
1
1 (Not reported to staff)
Central posterior cleft palate
1
0 (Discharge check at 2 hrs)
? abnormal breathing (Normal baby on examination)
1
0
Mucous retention cyst under tongue
1
0
Not opened bowels for 48 hrs
1
0
Unable to abduct hip
1
0
Traumatic fat necrosis R side of face
1
0
CMW error in recording weight
1
NA
Fever? Viral illness
1
0
We also reviewed the age at readmission (Table 3). It is obvious that most readmissions were after the 3rd day of life. Most readmissions were related to poor feeding, weight loss > 10%, physiological jaundice and it is to be expected that most of the times; these problems would not become very obvious until around 3-4 days after birth.
Age at readmission (Table 3)
Age at admission
Number of babies
< 24 hrs
1
24-48 hrs
3
48-72 hrs
7
72-96 hrs
16
>96 hrs
23
Total
50
We also analysed the age when discharge check was done at the maternity unit
(Table 4). 44 babies (88%) were discharged from maternity unit within 48 hrs of birth and 23 babies (46%) were discharged from maternity unit within the first 24 hrs. Age at discharge check was important as there was an association found between early discharge from AMU and subsequent readmission with feeding difficulties especially among breast fed babies (Table 4). Also studies have shown that mothers with 1 day hospital stays post delivery are less satisfied with their length of stay.1
Age at which discharge check was done at AMU and subsequent admissions with poor feeding (Table 4)
Age at discharge check
Number of babies
Subsequent admissions with poor feeding
Breast fed
<12 hrs
11
3
2
12-24 hrs
12
8
7
24-36 hrs
15
3
3
36-48
6
3
2
48-60
6
2
2
>60 hrs
0
1
1
Total
50
20
17
Also an important association was noted between poor feeding and first time mums. Out of the 20 babies with poor feeding, 16 were born to first time mothers.
Also looking at the table below (Table 5), it is clear that feeding problems and wt loss were much more common in breast fed babies. The association between readmission and first born children, breast feeding has been shown in studies.5
Table 5
Mode of feeding
No of babies admitted with poor feeding and/or wt loss
Breast feeding
26
Bottle feeding
3 (One of whom had a cleft palate)
We also looked at relationship between birth weight and risk of readmission (Table 6) and also gestational age and risk of readmission (Table 7). There was no clear association between birth weight and readmission or between birth weight and feeding problems. Also there was no association noted between gestational age and risk of readmission in the first week of life. A likely explanation for these findings would be that infants with low birth weight or gestational age less than 37 weeks were probably less likely to be discharged early from the maternity unit.6
Birth weight and readmission (Table 6)
Birth weight as centile
Number of readmissions
Number with feeding problems
<3rd
0
0
3-10
12
5
10-50
12
5
50-90
16
8
90-97
8
2
>97th
2
0
Total
50
20
Gestational age and readmission (Table 7)
Gestational age
Readmission
<37 weeks
5
37-40 weeks
29
>40 weeks
16
Total
50
We also analysed data on length of admission in paediatric ward. 32 out of 50 admitted babies (64%) stayed less than 24 hrs (Table 8). 10 out of 50 admissions needed reassurance only (20%) but the remaining needed some form of intervention (Table 9)
Length of stay (Table 8)
Total length of stay
Number of babies
<12 hrs
13
12-24 hrs
19
24-36 hrs
7
36-48 hrs
7
48-60 hrs
4
Total
50
Interventions needed on readmission (Table 9)
Intervention
Number of babies
Help with feeding/ Change of feeding
22
Blood tests
35
Phototherapy
15
Reassurance only
10
Referral to other specialties
2
IV fluids
5
IV antibiotics
2
Folic acid supplements
1
ECG
3
Babies needing follow up and readmission (Table 10)
Readmission
2
Follow up in day unit
8
Follow up in clinic
4
Total
14
CONCLUSIONS:
Poor feeding and weight loss accounted for majority of the admissions. (Table 2)
The above problems occurred more commonly in breast fed babies. 90% of babies admitted with poor feeding and/or weight loss were breast-fed babies (Table 5).
Out of the 20 babies with poor feeding, 16 were born to first time mothers.
44 out of 50 babies who were readmitted had been discharged from maternity unit within 48 hrs of birth. There was a clear association between early discharge from maternity unit and subsequent readmission with feeding problems especially in breast fed babies. (Table 4). 11 out of 20 babies admitted with feeding problems (55%) were passed fit for discharge from AMU within 24 hours of birth. Again 12 of them were babies whom their mothers wanted to breast-feed. This raises the question of whether breast-feeding mothers are receiving sufficient support and whether the babies were being discharged too early. Also when these babies were subsequently admitted, many mothers decided to bottle feed despite being offered help with breast feeding. A bottle fed baby in whom a cleft palate was missed had a discharge check done when she was 2 hrs old!! Clearly not sufficient time to establish that she was feeding well!
7 out of 20 babies who were admitted with poor feeding were noted to have feeding difficulty while in AMU (Table 2). When these babies were passed fit for discharge, this would have probably given a false sense of reassurance to mothers especially the first time mums. These mums were less likely to report feeding problems to CMW leading to delayed referrals (Table 3) by which time the babies would have lost a lot of weight necessitating interventions like blood tests, IV fluids etc.
There was no association found between birth weight or gestational age and risk of subsequent readmission (Tables 6 and 7).
Physiological jaundice was the third most common problem necessitating admission (Table 2). Only 2 of the babies in this group were noted to be jaundiced in AMU.
Surprisingly parental pressure for early discharge from AMU was documented in only one neonatal notes suggesting that this might not have been an important factor causing early discharge.
For 10 of the admissions, reassurance was all that was needed but the remaining 40 needed some form of intervention (Table 9).
RECOMMENDATIONS:
Delay discharge check until 24 hours after birth: Mothers deciding to breast feed babies need proper support. It may be a good idea to delay discharge check until 24 hours after birth. This will not only give sufficient time for the mothers to familiarise with breast feeding but also provide staff the opportunity to detect any potential feeding problems.
First time mothers to be properly supervised: First time mothers are especially naive when it comes to breast-feeding and it is important that they get properly supervised.
Request mothers to fill in a questionnaire: It may be a good idea to request mothers to fill in a questionnaire prior to discharge regarding how confident they feel about feeding their child, any feeding concerns, any other concerns etc. The physical, psychological and social well being of mother and newborn must be assessed when discharge planning takes place.7
Policy to transfer babies back to AMU: For babies readmitted in whom the only problem identified on assessment in paediatric ward is poor feeding, there should be a policy to transfer babies back to AMU for breast feeding training and support. This will not only persuade mothers to persevere with breast feeding but will also have a direct impact on reducing early discharges from AMU.
Re audit: The above recommendations to be implemented after discussion with staff at AMU and the audit will be repeated to see if this has resulted in a decrease in neonatal readmissions.
COMPETTING INTERESTS
None Declared
ACKNOWLEDGEMENTS
Dr Bridget Oates, Consultant Paediatrician, Crosshouse hospital for her invaluable support and guidance throughout, Dr Sheena Kinmond, Consultant Paediatrician, Crosshouse hospital, staff at medical records and neonatal secretaries at AMU.
AUTHOR DETAILS
FAHEEM MAZI KOTWAL, MBBS, MRCGP, GP registrar, Ayrshire, United Kingdom
CORRESPONDENCE: Dr F Mazi Kotwal, GP registrar, Riverside Medical Practice, 27 Dalvennan Avenue, Patna KA6 7NA
Email: faheemkotwal@yahoo.co.uk
REFERENCES
1. Jill M. Klingner, Leif I. Solberg, Susan Knudson-Schumacher, Richard R. Carlson, Karen L. Huss. How Satisfied Are Mothers with 1-Day Hospital Stays for Routine Delivery? Effective Clinical Practice, November/December 1999.
2. CDC. Trends in length of stay for hospital deliveries -- United States, 1970-1992. MMWR 1995;44:335-7
3. Danielsen B , Castles AG, Damberg CL, et al. Newborn discharge timing and readmissions: California, 1992–1995. Pediatrics 2000;106:31–9
4. Malkin J,Garber S, Broder M S, and Keeler E,. Infant Mortality and Early Postpartum Discharge Obstet Gynecol 2000;96(2):183-8.#
5. M. B. Edmonson, J. J. Stoddard and L. M. Owens. Hospital readmission with feeding-related problems after early postpartum discharge of normal newborns. Vol. 278 No. 4, July 23, 1997 JAMA
6. Oddie et al Early discharge and readmission to hospital in the first month of life in the Northern Region of the UK during 1998: a case cohort study. Arch. Dis. Child. 2005;90:119-124.
7. Cargill Y, Martel M; Postpartum maternal and newborn discharge: J obstet Gynaecol can 2007;29(4):357-359





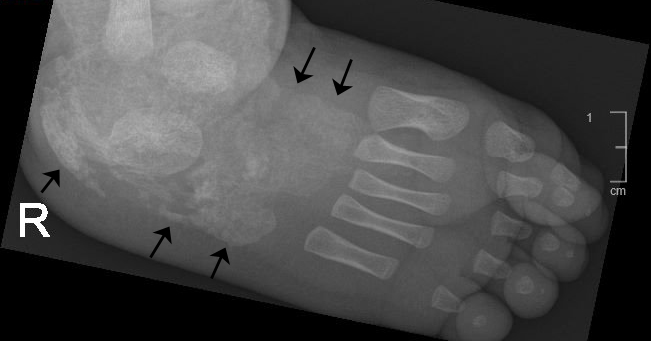
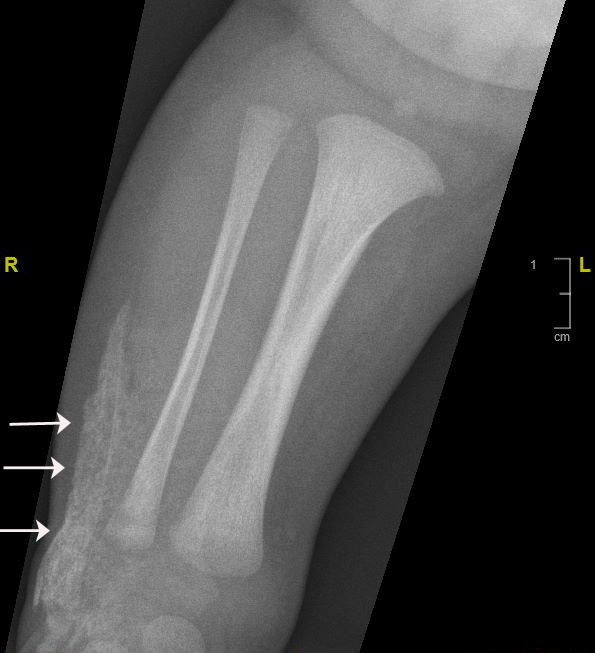
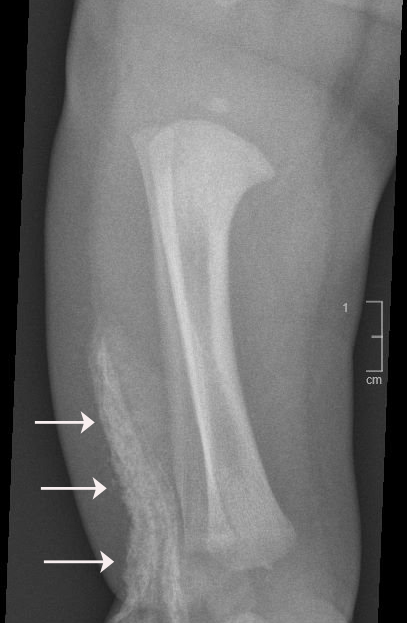
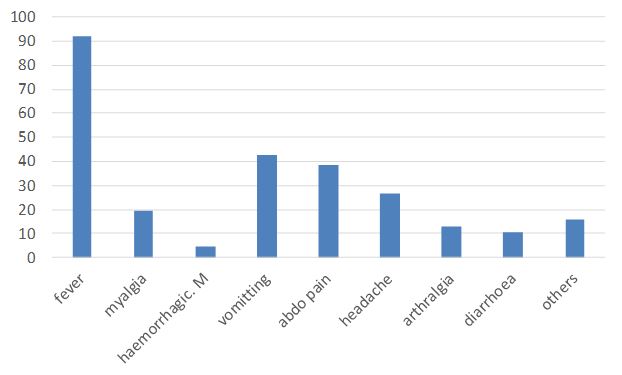
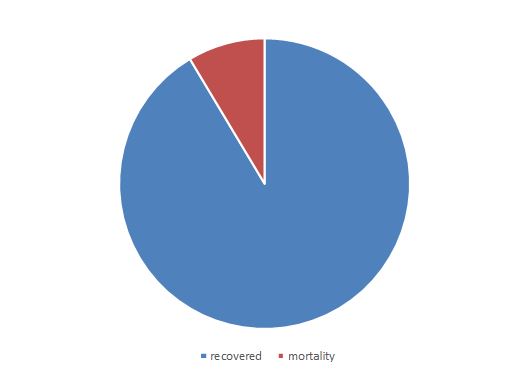
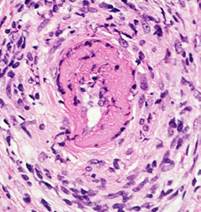
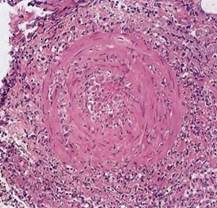



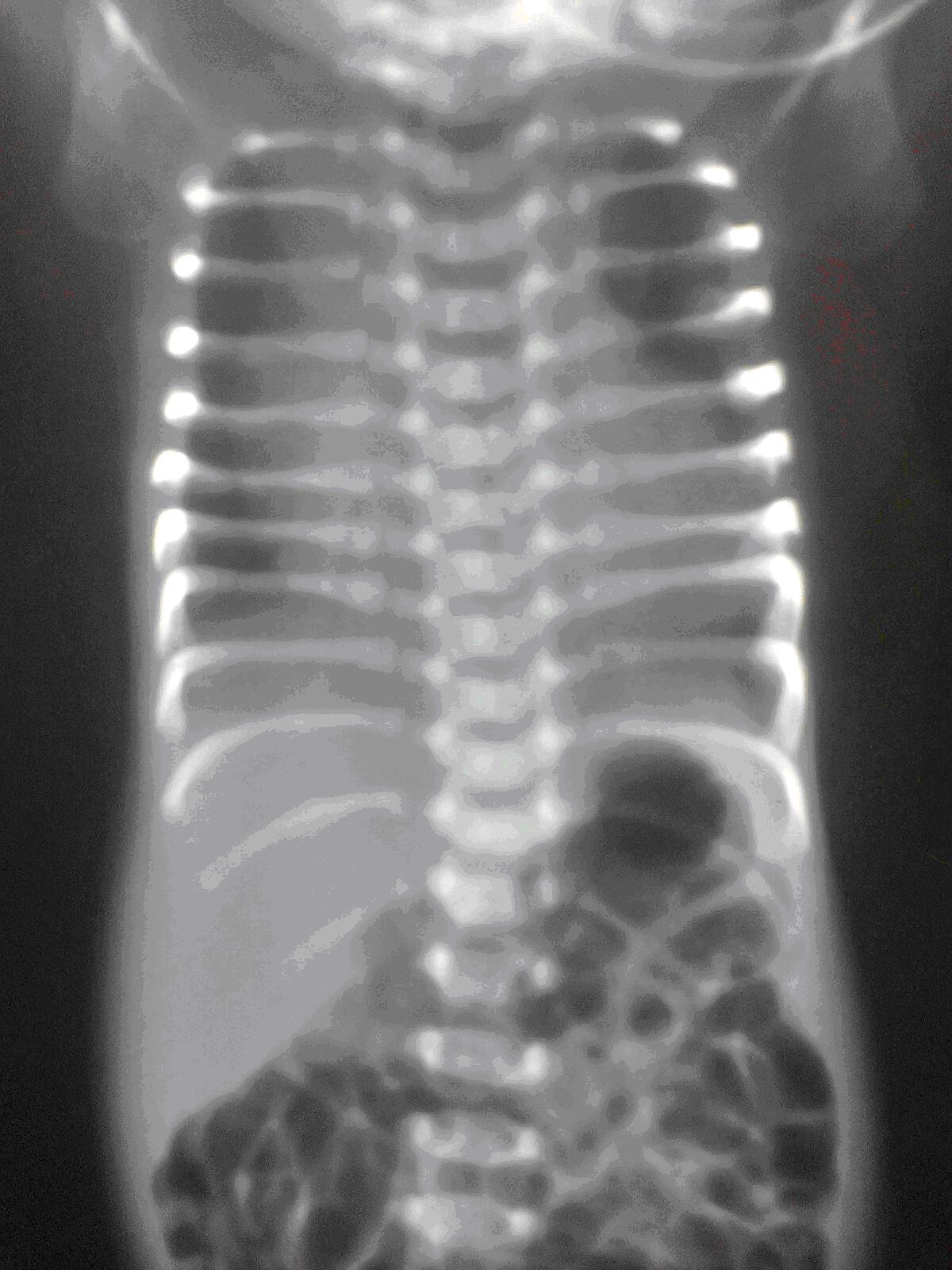
 Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2)
Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2) 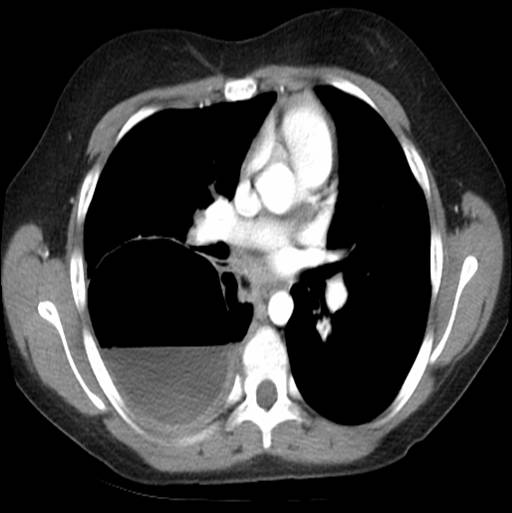 Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4)
Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4)  Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid.
Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid.  Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung.
Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung.  Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.