



ISSN 1757-8515
A comparison of different methods of assessing cosmetic outcome following breast-conserving surgery and factors influencing cosmetic outcome
Charfare H, MacLatchie E, Cordier C , Bradley M, Eadie C, Byrtus A, Burnet K, Chapman D, Wishart GC and Purushotham AD
Cite this article as: BJMP 2010;3(1):310
|
|
Abstract Methods to assess cosmesis following breast-conserving surgery are varied and assumed to yield similar results. The aim of this study was to compare three different methods of cosmetic assessment following breast-conserving surgery and to assess the impact of certain factors on cosmetic outcome. One hundred and fifteen patients undergoing breast-conserving surgery had 3 view digital photographs taken for assessment of cosmesis at one year post-surgery. Subjective cosmetic assessment was performed by a 5 member panel and objective assessment by Breast Retraction Assessment (BRA) and Nipple Deviation (ND). Factors including tumour size, percentage breast volume excised, location of tumour and number of breast operations performed was correlated with final cosmetic outcome. The majority of patients undergoing breast-conserving surgery demonstrated satisfactory cosmetic results. Inter-observer variation assessed using a kappa statistic for panel assessment gave a value of 0.42 with a 95% confidence interval (CI) of 0.37 to 0.47, indicating moderate agreement between observers. The kappa statistic for agreement between the three methods used for assessing cosmesis was -0.23 with 95% CI of -0.35, -0.11 indicating poor concordance between the three methods used. These methods however, may be complementary to each other and therefore these observations merit further investigation. Tumour location, tumour size and the number of operations performed did not influence cosmetic outcome. However, cosmetic outcome was related to percentage breast volume excised. Keywords: breast-conserving surgery, cosmetic assessment |
Introduction:
Cosmetic outcome following breast-conserving surgery depends on various factors including location of the tumour, weight of the specimen excised, number of surgical procedures, volume of breast, length of scar and postoperative adjuvant treatment1. The best method of cosmetic assessment following breast-conserving surgery is still unclear. However various objective and subjective methods in combination are known to give a good assessment of cosmesis2, 3, 4. It has been shown that photographic assessment is as effective as live assessment in the post-surgical setting5. Methods to assess cosmesis following breast-conserving surgery are varied and more recently computer software are being used to assess cosmesis following breast-conserving surgery.
The aim of this study was to compare three different methods of cosmetic assessment following breast-conserving surgery and to assess the influence of various factors on final cosmetic outcome.
Methods:
One hundred and fifteen patients underwent breast-conserving surgery for carcinoma of breast by wide local excision and level 2 axillary clearance. Following wide local excision, cavity shavings were taken to ensure adequate local excision. Breast drainage was not used but suction drains were used routinely following axillary clearance. All patients received adjuvant breast radiotherapy (46 Gy, 23 fractions with a cavity boost of 12 Gy in 4 fractions) administered over a period of 6 weeks.
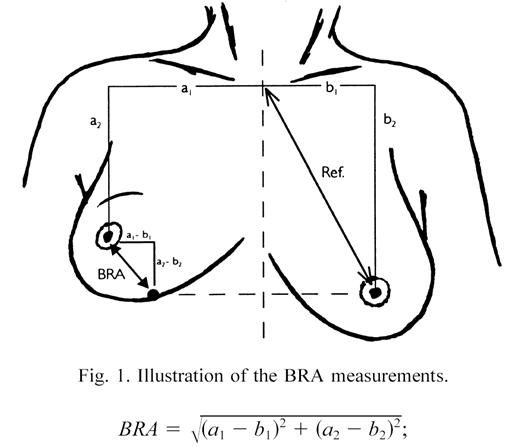
Figure-1: Measurement of Breast Retraction Assessment6 (reprinted with permission from Elsevier, ref 6 (page 670), copyright 1999)
Digital photographs were taken at one year in three views; frontal with arm by the side, frontal and oblique with arm abducted to 90 degrees. The photographs were used for subjective and objective assessment of cosmesis. The objective assessment of cosmesis was carried out using Breast Retraction Assessment (BRA) and Nipple Deviation (ND). BRA was calculated as indicated in figure 16. ND was calculated as a percentage difference from suprasternal notch to nipple on normal side compared with the operated side. BRA and ND were then categorised into three groups; BRA: (excellent to good <3.1 cm, fair 3.1-6.5, poor >6.5), ND: (difference of <5% - excellent to good, 5-10% fair and >10% poor). Subjective assessment was carried out using a panel consisting of a Consultant Breast Surgeon, Research Fellow, Secretary, Breast Care Nurse and Nurse Practitioner with each scoring independently. The method described by Harris et al7 with a score of 9-10 for excellent (no visible difference between two breasts), good (slight difference; score 7-8), fair (obvious difference but no major distortion; score 4-6) and poor (major distortion; score <4) was used to categorise patients.
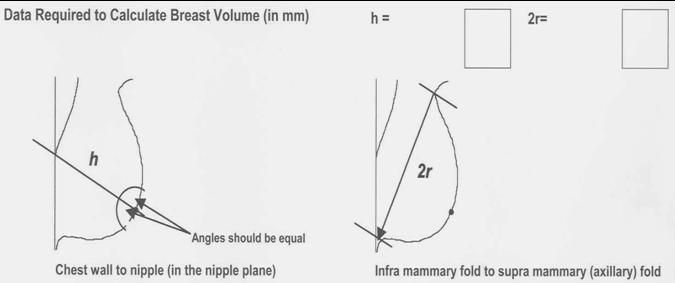
Figure- 2: Measurement of breast volume (Sloane method) Formula for calculation of breast volume: 1/3 π r2h (reprinted with kind permission from Sloane project)
The volume of breast tissue excised was estimated with the length (L), width (W) and height (H) of the excised tissue specimen and the cavity shave measured by the pathologist and using the formulas for a prolate ellipse (V= 0.52* L* W* H); this was added on to the volume of cavity shave calculated using the formula 0.79* L* W* H. The total breast volume was estimated using the mammogram and applying the formula (1/3 πr2h) as shown in figure-2. Based on these measurements the percentage breast volume excised was calculated and compared with cosmetic outcome.
Statistics:
Multirater kappa statistics8 were used to assess inter-observer agreement between five different members of the panel and also to test agreement between the three different methods for assessing cosmesis. The average value given by the panel was used and categories good and excellent were combined in order to compare the three methods of cosmetic assessment. A kappa statistic of less than or equal to 0.20 was considered to demonstrate poor agreement, 0.21 to 0.40 fair agreement, 0.41 to 0.60 moderate agreement, 0.61 to 0.80 good agreement and 0.81-1.00 very good agreement9.
The effect of the percentage volume of the breast tissue excised and the tumour size on the three methods of cosmetic assessment was examined using where appropriate a Jonckhneere-Terpstra test for trend, a Kruskal Wallis test or a Mann-Whitney U test. The effect of the number of breast operations performed and the location of the tumour were assessed using Chi-square test or Fisher’s exact test when appropriate.
Results:
Of the 115 patients assessed using panel assessment 64 (56%) scored good to excellent, 39 (34%) scored fair and 12 (10%) scored poor. ND scored 50(43%) as good to excellent, 32 (28%) as fair and 33 (29%) as poor. Using BRA, the scores were 76 (66%), 38 (33%) and 1(1%) respectively. These results are shown graphically in figure-3.
Figure- 3: Number of patients classified into each of the three categories poor, fair and good/excellent for the three methods bra, nipple deviation and panel assessment. BRA= breast retraction assessment; Panel= assessment by different panel members; ND= nipple deviation
Taking the mean scores for these three methods of assessment and dichotomising the results into two categories of good to excellent and poor to fair, 52% of patients in this study had good to excellent cosmetic result and 48% were categorised as fair to poor cosmetic result. The Kappa statistic was calculated on 115 patients for the three methods of assessment and it was found to have a value of –0.23 (95% CI (–0.35, – 0.11) which falls within the poor agreement category.
Figure- 4: Comparison of panel assessment by different panel members. Pa, Ph, Pg, Pk and Pd= Codes for the different panel members
Examining the panel assessment using the kappa statistics for the 115 patients assessed there was moderate agreement between the panel members (Kappa statistic of 0.42; 95% confidence interval of (0.37, 0.47). This suggests there is moderate chance that the panel members will categorise each patient the same way. If one plots the panel assessment graphically one can see that excellent is used least by all and fair most frequently (figure 4).
Factors affecting cosmesis:
1) Percentage breast volume excised
Figure -5: Effect of percentage breast volume excised on cosmetic outcome using Panel assessment, BRA and ND
For panel assessment it appears that removal of a larger percentage volume gives a poor cosmetic result and a smaller percentage volume an excellent/good result (figure 5) as would be expected clinically. This is supported by a Jonckhneere-Terpstra test for trend (=0.01). Using ND median percentage volumes across the groups did not appear to differ (χ2=1.05 p=0.59, Kruskal Wallis test). However, for BRA, only one patient was classified as poor and no difference was seen between those with fair and good/excellent results (U=477, p=0.34). The median volume excised for different cosmetic outcome using the three methods is shown in table 1.
Table-1: Medians volumes for the three measurements.
|
|
Panel assessment
|
BRA
|
Nipple deviation
|
|
Poor
|
157.56
|
(only 1 poor value)
|
100.61
|
|
Fair
|
88.58
|
93.11
|
55.96
|
|
Good/Excellent
|
68.33
|
76.55
|
81.33
|
BRA= breast retraction assessment
BRA= breast retraction assessment
The percentage breast volume excised was then compared with cosmetic outcome using the three methods of assessment. As shown in table 2, 45-65% of patients with <10% estimated breast volume excised had good to excellent cosmetic result compared with 35-50% good to excellent result if >10% breast volume was excised.
2) Tumour location:
Tumour location was divided into inner or outer quadrants of the breast. The distribution of tumours in the breast and the cosmetic outcome with each of the three methods of assessment is shown in table 3. The location of tumour within the breast was not significantly associated with cosmetic outcome (χ2 =1.86, p=0.39 for panel assessment), (p=0.23, Fisher’s exact test for BRA) and (χ2 =0.21, p=0.90 for ND).
Table-2: Estimated percentage breast volume excised and cosmetic outcome
|
|
< 10% breast volume excised
|
> 10% breast volume excised
|
|
Panel Assessment
|
||
|
Good to excellent (%)
|
32 (65)
|
7 (35)
|
|
Fair (%)
|
15 (31)
|
6 (30)
|
|
Poor (%)
|
2 (4)
|
7 (35)
|
|
Breast Retraction Assessment
|
||
|
Good to excellent (%)
|
32 (65)
|
10 (50)
|
|
Fair (%)
|
16 (33)
|
10 (50)
|
|
Poor (%)
|
1 (2)
|
0
|
|
Nipple Deviation
|
||
|
Good to excellent (%)
|
22 (45)
|
8 (40)
|
|
Fair (%)
|
15 (31)
|
4 (20)
|
|
Poor (%)
|
12 (24)
|
8 (40)
|
3) Number of breast operations:
The influence of number of operations (1 vs 2) was examined for each of the three methods of assessment. Using BRA and Panel assessment there was no significant difference in the cosmetic outcome for patients who underwent one or two operations ( p=0.70 for panel assessment), (p=0.99, Fisher’s exact test for BRA). For ND there does appear to be a larger proportion in the poor group for those with two operations (p =0.30 Fisher’s exact test for ND). This is illustrated in Table 3.
Table-3: Factors affecting cosmesis
Table-3: Factors affecting cosmesis
|
|
Panel
|
BRA
|
ND
|
|
Percentage volume excised
Poor (median (IQR))
Fair (median (IQR))
Good/Excellent (median (IQR))
|
13.8 (11.0,16.5)
8.4 (4.4,10.4)
5.8 (3.9,8.0)
|
-
8.0 (4.6,11.6)
6.9 (4.3,10.1)
|
8.5 (5.1,11.4)
5.8 (3.9,9.4)
7.2 (4.4,11.0)
|
|
Location
Poor (outer (n), inner (n))
Fair (outer (n), inner (n))
Good/Excellent (outer (n), inner (n))
|
8, 2
22,8
47,8
|
0,1
26,5
51,12
|
9,1
23,6
33,8
|
|
No. of Operations
Poor (One (n), Two (n))
Fair (One (n), Two (n))
Good/Excellent (One (n), Two (n))
|
9,1
24,6
48,8
|
1,0
26,5
54,10
|
20,5
27,2
34,8
|
|
Tumour size (mm)
Poor (median (IQR)
Fair (median (IQR)
Good/ Excellent (median (IQR)
|
12 (9, 15)
11 (9, 19)
12 (7, 15)
|
-
11 (8,15)
12 (7, 15)
|
12 (10, 15)
12 (8, 16)
9 (6,14)
|
Panel= panel assessment; BRA= breast retraction assessment; ND= nipple deviation; IQR= inter quartile range
Panel= panel assessment; BRA= breast retraction assessment; ND= nipple deviation; IQR= inter quartile range
4) Tumour size:
Table 3 shows the median tumour size and interquartile range for the three categories, good/ excellent, fair and poor and one can see that there is no significant difference in tumour size for these categories using panel assessment (Jonckheere-Terpstra p=0.31) or BRA (U =873, p=0.55). However, using ND there was evidence to suggest that large tumour size resulted in poor outcome (Jonckheere-Terpstra, p=0.04).
Thus, tumour size had a significant influence on the cosmetic outcome when ND was used as the method of assessment.
Discussion:
Cosmetic outcome following breast-conserving surgery is assessed using a combination of subjective and objective methods. The subjective method uses a panel of members from different backgrounds to assess overall cosmesis. However, Pezner et al10 showed relatively low level of agreement between observers when a four-point scale was used for assessment of overall cosmesis. The objective methods, which mainly compare the position of the nipple, are easy to reproduce but do not take into account skin changes and give poor assessment of cosmesis for lower quadrant tumours.
In this study the cosmetic outcome was assessed in 115 patients one year post-operatively. The mean cosmetic result using the three different methods of assessment was good to excellent in 55% of the patients, which compares favourably with other studies reported in the literature2, 4. Looking at inter-observer variation for the panel assessment, moderate agreement was found between different panel members. This compares favourably with an earlier study that looked at cosmetic outcome in the EORTC trial 22881/108826. However, when the three methods of cosmetic assessment were compared with each using kappa statistic there was poor concordance. Although some agreement was noted, this was likely to be due to chance as the kappa statistic was low. It is difficult to explain this finding as other authors1, 6 have reported moderate to good agreement between subjective and objective methods. One explanation for this lack of agreement is that each method assesses a different aspect of cosmesis.
The two objective methods of cosmetic assessment (BRA and ND) that are used to assess upward retraction of nipple have been found to be a very good determinant of cosmetic outcome and are easy to reproduce according to Fujishiro et al11. Furthermore, evaluation of nipple position has also been shown to be moderately representative of overall cosmetic result6. BRA is a two dimensional measurement of nipple position and some cosmetic factors such as volume, shape or skin changes cannot be accurately assessed11. This is probably the reason why BRA shows a better cosmetic outcome when compared with subjective assessment by panel members. In this study only one (1%) patient was deemed to have a poor cosmetic outcome using BRA compared with 12 (10%) using panel assessment.
A criticism of the current study is that patients’ perceptions of their own cosmetic outcome were not assessed. Previous studies have shown a significant correlation between patient satisfaction after breast-conserving surgery and their self-assessment of cosmesis12, 13. This study shows that there is need to find a reproducible method of cosmetic assessment which takes into account all the limitations of the methods currently used. More recently computer software like BCCT.core and Breast Analysing Tool have been developed and early results using these software are promising14, 15. There are various factors that are known to affect cosmesis following breast-conserving surgery. As expected larger percentage volume of excised breast tissue was associated with poorer cosmetic result. This was particularly evident from panel assessment. Such a relationship was less clear with BRA and ND. The effect of percentage volume of breast tissue excised and the outcome is consistent with a recent report that showed higher patient satisfaction if estimated percentage breast volume excised was < 10%16. Cosmetic outcome based on tumour location varies depending on the method of assessment used. BRA is adversely affected by tumour in the upper and outer quadrants of the breast, suggesting that surgery causes larger nipple deviation in this quadrant, while panel assessment gives poor scores for tumours located in inferior quadrant2, 11. In this study only 19% of patients had tumours located in the inner quadrant and the small number may explain why, no significant difference in cosmetic outcome was found. Tumour location or the number of operations performed did not appear to affect the cosmetic outcome in this study. The volume of breast tissue excised depends on tumour size. Since the majority of tumours in this study were small, the size of the tumour did not affect cosmetic outcome except when nipple deviation was used. This once again indicates that these three methods of assessment may be looking at different aspects of cosmesis.
In conclusion, cosmetic outcome following breast-conserving surgery is an important, measurable end point. However, the best method of assessment of cosmesis has not been devised17. Although, the objective methods are easier to apply and reproduce, they do not give a good assessment of global cosmetic results. Panel Assessment however, does appear to provide concordant results between different observers and may be a useful, simple measure of cosmetic assessment following breast-conserving surgery.
|
Competing Interests None declared Author Details CHARFARE H, Bedford Hospital NHS Trust, UK MACLATCHIE E, CORDIER C, EADIE C, Western Infirmary, University of Glasgow, UK BRADLEY M, Department of Public Health and Primary Care, University of Cambridge, UK BYRTUS A, PURUSHOTHAM AD, Department of Academic Oncology, King’s College London, UK BURNET K, CHAPMAN D, WISHART GC, Addenbrooke’s Hospital, Cambridge, UK CORRESPONDENCE: H CHARFARE, Bedford Hospital NHS Trust, South Wing, Kempston Road, Bedford Hospital NHS Trust, MK42 9DJ Email: habib.charfare@bedfordhospital.nhs.uk |
References
1)Al-Ghazal SK, Blamey RW, Stewart Jet al. The cosmetic outcome in early breast cancer treated with breast conservation. Eur J Surg Oncol 1999; 26 (6): 566- 570
2)Van Limbergen E, Rijnders A, van der Scheuren et al. Cosmetic evaluation of breast conserving treatment for mammary cancer. 2. A quantitative analysis of the influence of radiation dose, fractionation schedules and surgical treatment techniques on cosmetic results. Radiother and Oncol 1989; 16: 253-267
3)Christie DRH, O’Brien MY, Christie JA et al. A comparison of methods of cosmetic assessment in breast conservation treatment. The Breast 1996; 5: 358- 367
4)Ash D V, Benson E A, Sainsbury J R et al. Seven year follow-up on 334 patients treated by breast-conserving surgery and short course of radical postoperative radiotherapy: a report of the Yorkshire breast cancer group. Clin Onco (R Coll Radiol) 1995; 7 (2): 93-96
5)Eadie C, Herd A, Stallard S: An investigation into digital imaging in assessing cosmetic outcome after breast surgery. J Audiovisual Media in Medicine 2000; 23 (1): 12- 16
6)Vrieling C, Collette L, Bartelink E et al. Validation of the methods of cosmetic assessment after breast-conserving therapy in the EORTC ‘ boost versus no boost’ trial. Int J Radiat Oncol Biol Phys 1999; 45 (3): 667- 676
7)Harris JR, Levene MB, Svensson G et al: Analysis of cosmetic results following primary radiation therapy for stage I and II carcinoma of the breast.
Int J Radiat Oncol Biol Phys 1979; 5: 257- 261
8)Siegel S, Castellan Jr NJ. Nonparametric statistics for the behavioural sciences 2nd Edition, McGraw-Hill, 1988, 284- 291.
9)Altman DG. Practical statistics for medical research, Chapman & Hall, 1991, 404.
10) Pezner RD, Lipsett JA, Vora NL et al. Limited usefulness of observer-based cosmesis scales employed to evaluate patients treated conservatively for breast cancer. Int J Radiat Oncol Biol Phys 1985; 11: 1117- 1119
11) Fujishiro S, Mitsumori M, Kokubo M et al. Cosmetic results and complications after breast-conserving therapy for early breast cancer. Breast Cancer 2000; 7 (1): 57- 63
12) Al-Ghazal SK, Fallowfield L, Blamey RW. Patient evaluation of cosmetic outcome after conserving surgery for treatment of primary breast cancer. Eur J Surg Oncol 1999; 25 (4): 344- 346
13) Kaija H, Rauni S, Jorma I et al. Consistency of patient-and doctor assessed cosmetic outcome after conservative treatment of breast cancer. Breast cancer Res Treat 1997; 45 (3): 225- 228
14) Fitzal F, Krois W, Trischler H et al. The use of breast symmetry index for objective evaluation of breast cosmesis. The Breast 2007; 16: 429-435
15) Cardoso MJ, Cardoso J, Amaral N et al. Turning objective into subjective: The BCCT.core software for evaluation of cosmetic results in breast cancer conservative management. The Breast 2007; 16: 456-461
16) Cochrane RA, Valasiadou P, Wilson ARM et al. Cosmesis and satisfaction after breast-conserving surgery correlates with percentage breast volume excised. Br J Surg 2003; 90: 1505- 1509
17) A Munshi, S Kakkar, R bhutani et al. Factors influencing cosmetic outcome in breast conservation. Clin Oncol 2009; 21: 285-293

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.