



ISSN 1757-8515
Prevention and management of accidental carotid artery cannulation; Novel use of a double male Luer lock connector
Asif Mahmood, Dumisani Ncomanzi, Asquad Sultan & Sandeep Sharma
Cite this article as: BJMP 2018;11(1):a1108
|
|
Abstract Internal jugular central line insertion is a common procedure performed in anaesthesia and intensive care. Often performed by junior staff. We performed a survey in our anaesthetic and intensive care department to review the methods used to confirm central venous cannulation before dilatation and also how they would manage accidental carotid artery cannulation including follow up. Our survey highlighted a lack of venous transduction before dilatation despite accepted benefits of doing so. This survey also revealed the management of accidental carotid artery cannulation was mostly unknown or unsafe. This survey highlighted the need educate departments regarding the management of accidental carotid artery cannulation. We also describe a method of central venous transduction before dilation via the arterial line transducer without the need to ‘break’ the arterial line transducer. Keywords: Central venous pressure wave forms; Ultrasonography; Carotid cannulation, Central lineAbbreviations: CT - computed tomography; CVP - central venous pressure |
We would like to draw the attention of your readers to the outcome of a survey undertaken in Kettering General Hospital. We wanted to determine what methods clinicians use to confirm central line cannula/needle position before dilatation and what their removal plan would be for an accidental insertion of a central line (>7 Fr) into the carotid artery.
We performed a paper survey of 52 doctors in anaesthesia/intensive care at Kettering General Hospital. We achieved a 100% return rate. We asked the doctors to answer questions based on their practise over the previous year period. The majority of people surveyed were consultants (47%). The results of the survey revealed doctors mostly utilised ultrasound confirmation of guidewire before dilatation (89%) but only 19% utilised pressure transduction. A large proportion of doctors surveyed either did not know how to manage carotid artery cannulation with a >7 Fr central line (35%) or would ‘pull and press’ (40%). Only 5% of the doctors who would ‘pull and press’ would arrange computed tomography (CT) angiogram follow up.
We highlighted a lack of clarity, which may be widespread. It is advisable to seek a vascular surgeon or interventional radiology input to facilitate line removal due to the excessive complications related to the ‘pull and press’ technique (47% complication rate).1 Complications include pseudoaneurysm formation, airway compromising haematomas, arteriovenous fistula, stroke and death.1 If such lines are removed by the ‘pull and press’ technique it is recommended to arrange CT angiogram even if the patient is asymptomatic due to the possibility of pseudoaneurysm or arteriovenous fistula formation.1
We correctly utilised ultrasound confirmation of guidewire position before dilatation. However ultrasound alone has not eliminated accidental arterial dilatation. This still occurs despite ultrasound usage especially in cases involving inexperienced clinicians and the guidewire going through the vein and into the artery.2 The combined use of ultrasound and transduction may further reduce the incidence of carotid cannulation.3 This may prove invaluable in centres without vascular or interventional radiology support.
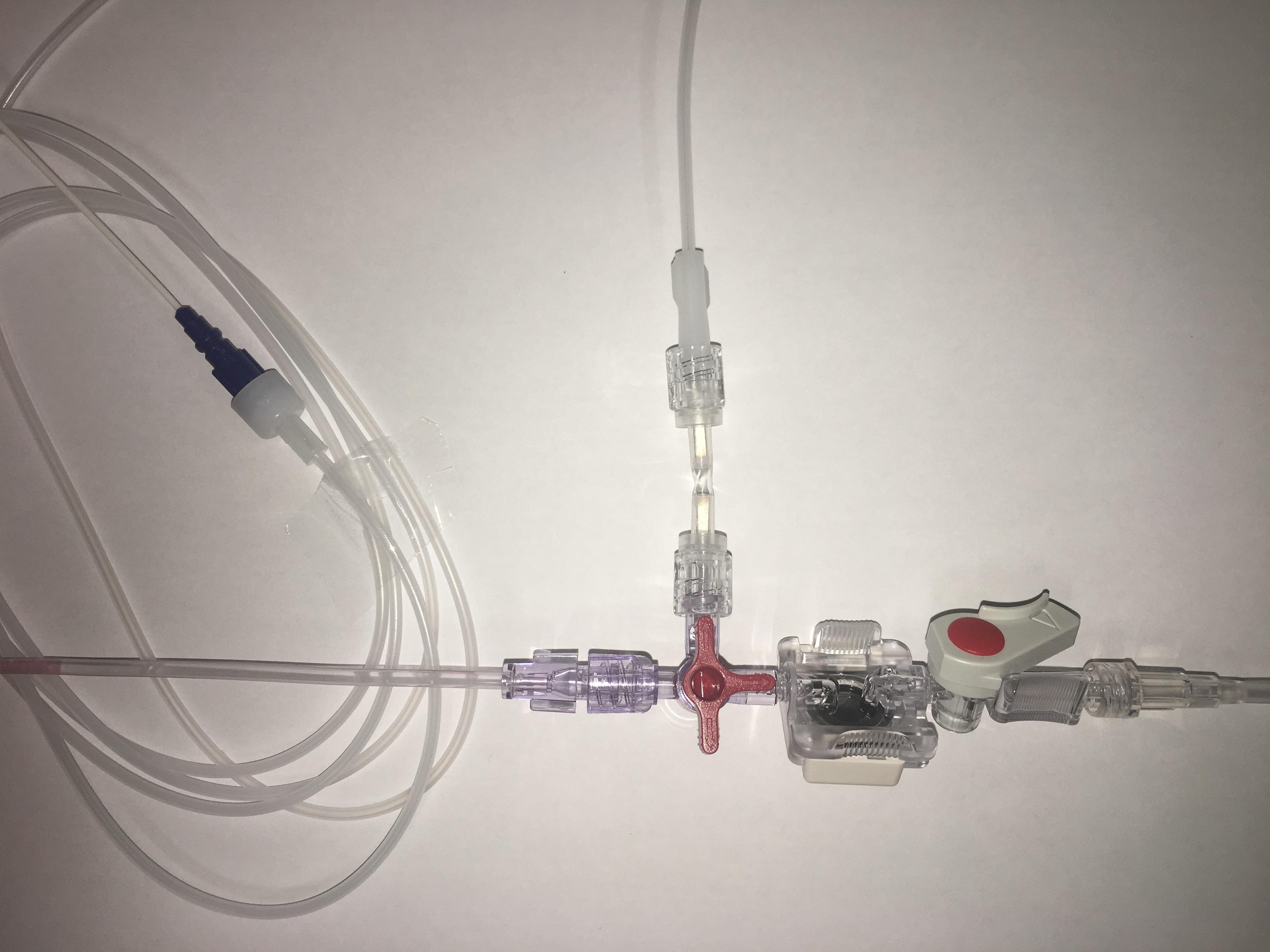
Our centre has reduced its usage of central venous pressure (CVP) monitoring. This may reflect our lack of transduction prior to dilatation for central line insertion. Hence we devised a novel use of the double male Luer lock connector. This connector allows the female connector end of an infusion line to connect to the female connector of the blood aspirating port of an arterial transducer. This will then allow transduction of a central line cannula, before dilatation, via the arterial transducer by turning the 3-way tap (Figure 1). This removes the need to set up a separate transducer and also prevents the need to disconnect connections in the arterial line to allow CVP confirmation, as this was considered an infection risk.
Figure 1: Double male Luer lock connector attached to the blood aspirating port of an arterial transducer, with a fluid line connecting this to the central venous cannula
|
Competing Interests None declared Author Details ASIF MAHMOOD MBCHB,FRCA, Kettering General Hospital, Department of Anaesthesia, Kettering, UK. DUMISANI NCOMANZI MBCHB, FRCA, Kettering General Hospital, Department of Anaesthesia, Kettering, UK. ASQUAD SULTAN MBBS, FFARCSI, DESRA, Kettering General Hospital, Department of Anaesthesia, Kettering, UK. SANDEEP SHARMA BSC, MBBS, FRCA, Kettering General Hospital, Department of Anaesthesia, Kettering, UK. CORRESPONDENCE: ASIF MAHMOOD, Kettering General Hospital, Department of Anaesthesia, Kettering, UK. Email: asifmahmood@doctors.net.uk |
References
- Guilbert MC, Elkouri S, Bracco D, et al: Arterial trauma during central venous catheter insertion: Case series, review and proposed algorithm. J Vasc Surg 2008; 48: 918-925
- Blaivas M: Video analysis of accidental arterial cannulation with dynamic ultrasound guidance for central venous access. J Ultrasound Med 2009; 28: 1239-1244
- Bowdle A. Vascular complications of central venous catheter placement: Evidence-based methods for prevention and treatment. J Cardiothorac Vasc Anesth 2014; 28: 358–68.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.