The United Kingdom kicked off its leading mass coronavirus disease-2019 (COVID-19) vaccination programme by vaccinating the first person, Margaret Keenan on 8th December 20201 which was followed by many other countries.2 COVID-19 vaccines were developed in less than 12 months after the pandemic began3, 4 and have offered hope of bringing normalcy back to many around the globe, but it is not without its challenges.5, 6 The infrastructure of coordinating frontline response and the development of confidence among various communities to accept vaccination posed significant challenges. This required input from governments, healthcare professionals, the media, and importantly the public who play a vital role in not only accepting the vaccines and busting the myths but also actively volunteering for this great cause.
After watching my father, a frontline COVID-19 healthcare worker, receive the vaccine and at the same time sensing the reluctance of some family and friends to take the vaccine, despite the pandemic hitting Black, Asian and minority ethnic (BAME) communities disproportionately, I felt energised to play my role. When I saw an exciting opportunity for volunteering for this noble cause coordinated by my school, Bolton School, I promptly put an application forward in February 2021. The whole process was streamlined, and soon afterwards I embarked on volunteering at the Bolton Wanderers Football Club vaccination centre.7 There was some initial anxiety about contracting COVID-19, but I discussed it with my mentor and was reassured about the safety standards of the vaccination centres.
I was pleasantly surprised to see a range of roles for a non-clinician volunteer including being the face of the vaccination programme by greeting patients, explaining the vaccination process and allying anxieties, handing out written information, managing patient flow, ensuring maintenance of social distancing, checking temperatures, and liaising with clinical staff. There was also an element of an administrative role and keeping the registers. However, what I found most fulfilling was to talk to some of the patients who said that they had been socially isolating for several months and were excited to talk to someone face to face. One could see a sense of liberation the vaccination was bringing to them. It was a truly humbling experience to go out of my way to support some of the BAME patients, and speaking to them in their native language to make the whole process a memorable experience. I remembered one elderly lady who seemed distressed as she could only communicate in Hindi and I was fortunate that she allowed me to take her through the whole process and later assist with arranging transport.
I am going to continue with my volunteering on weekly basis and I found that it revitalised me for the rest of the week to engage in my full-time academic studies at school. This being my first work experience, I must admit the shifts were well-paced, lasting 4-5 hours and not too demanding. I was made to feel safe, and the senior members of the team would regularly communicate and offer me guidance and support.
Working closely with clinicians helped me gain new insights into the importance of true multidisciplinary teamwork in healthcare. I appraised it as the epitome of how colleagues with a unique set of skills, and driven by a shared desire to bring about a real difference to people’s lives, strived together selflessly as a team. Furthermore, it was inspiring to observe the leadership of the senior volunteers acting as role models with their professionalism, unflinching dedication to their job and willingness to proactively offer support to others. However, the watershed moment that shaped my thinking to take on medicine as a career was the reward I got from the empathic interaction with patients and gratitude in their eyes. It was pleasing to see in practice the Good Medical Practice8 attributes of working collaboratively with colleagues, professionalism, communicating effectively, and treating patients with dignity.
I have been feeling proud to be at the frontline working shoulder to shoulder with my clinical colleagues in this battle to end the pandemic. I would highly recommend vaccination volunteering to others as it is truly a once in a lifetime opportunity to make a real difference in the lives of so many.
It is widely acknowledged that medicine can be a high-stress profession. The reasons behind this observation have been the focus of research over recent years, because concerns over the welfare of doctors have grown due to its relevance to burnout of individuals and safeguard of healthcare systems. However, a recent survey of hospital doctors still showed that 80% experienced workplace stress, and the junior doctors surveyed suffered significantly higher burnout rates than their consultants.1 Separate research has specifically found that junior doctors have a poor work-life balance, a composite measure of individual factors affecting wellbeing.2 There seem to be differences in the wellbeing of doctors in different specialities studied – a study in 2016 showed higher levels of leisure time enjoyed by general practitioners compared to doctors working in other specialities.3 Another survey showed that psychiatrists experienced lower levels of burnout than surgeons did.4 Furthermore, different burnout rates have been observed between consultants and junior doctors working in Psychaitry.5
We sought to build on existing research by studying the work-life balance of junior doctors and how some factors might affect that. We also decided to explore what factors might contribute to the differences in wellbeing between medical specialties and professional grades.
Method
Junior doctors working across an English county in general practice, medical and surgical specialities (the “non-psychiatric setting”), and in psychiatric specialities (the “psychiatric setting”), were recruited into a cross-sectional study between September and December 2019. To enable appropriate comparison between groups, junior doctors must have worked between the level of Foundation Year 2 (FY2) and consultant in their relevant speciality. This was necessary because the on-call responsibility of Foundation Year 1 (FY1) doctors in this locality varies significantly from that of more senior doctors.
All doctors were required to complete the SWING (Survey Work-home Interaction-NijmeGen), questionnaire6; a validated instrument measuring four aspects of work-home interaction. This questionnaire is split into negative (questions 1-12) and positive (questions 13-22) subscales, where lower and higher scores are better respectively. For each question four responses ranging from never to always could be returned. Demographic information was also collected to assess participant group similarity and identify any effect of these variables. These included age, gender, and whether they have children under the age of 18. No identifying information was requested to allow for staff anonymity, and no incentive was offered for participating.
Ethical approval for the study was granted by the local Medical Education Departments. Data from completed questionnaires was recorded in an Excel spreadsheet, which was used for collation and analysis. Significance of the between-group differences was calculated using the Chi-Squared test, with the threshold for statistical significance set at p<0.05. In order to allow comparison between the answers given for each questionnaire item, 1, 2, and 3 points were respectively allocated to each “sometimes”, “often”, or “always” response. The sum of these points for each question gave the “overall question score”, with lower and higher scores reflecting better work-life-balance on negative and positive subscales respectively. Overall question scores were also calculated as percentages of the maximum possible score for each question or subscale (i.e. if every respondent had answered “always”).
Results
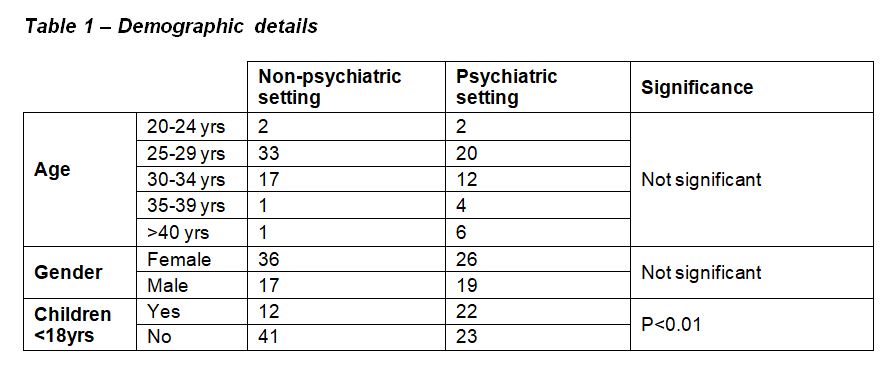
Questionnaires were returned by 99 junior doctors (54 working in the non-psychiatric setting, and 45 working in the psychiatric setting). Demographic details are shown in Table 1. Not all respondents returned demographic details. There were no significant differences in the ages and genders of respondents between the two settings, but there were significantly more doctors with children <18 years in the psychiatric setting.
Table 1
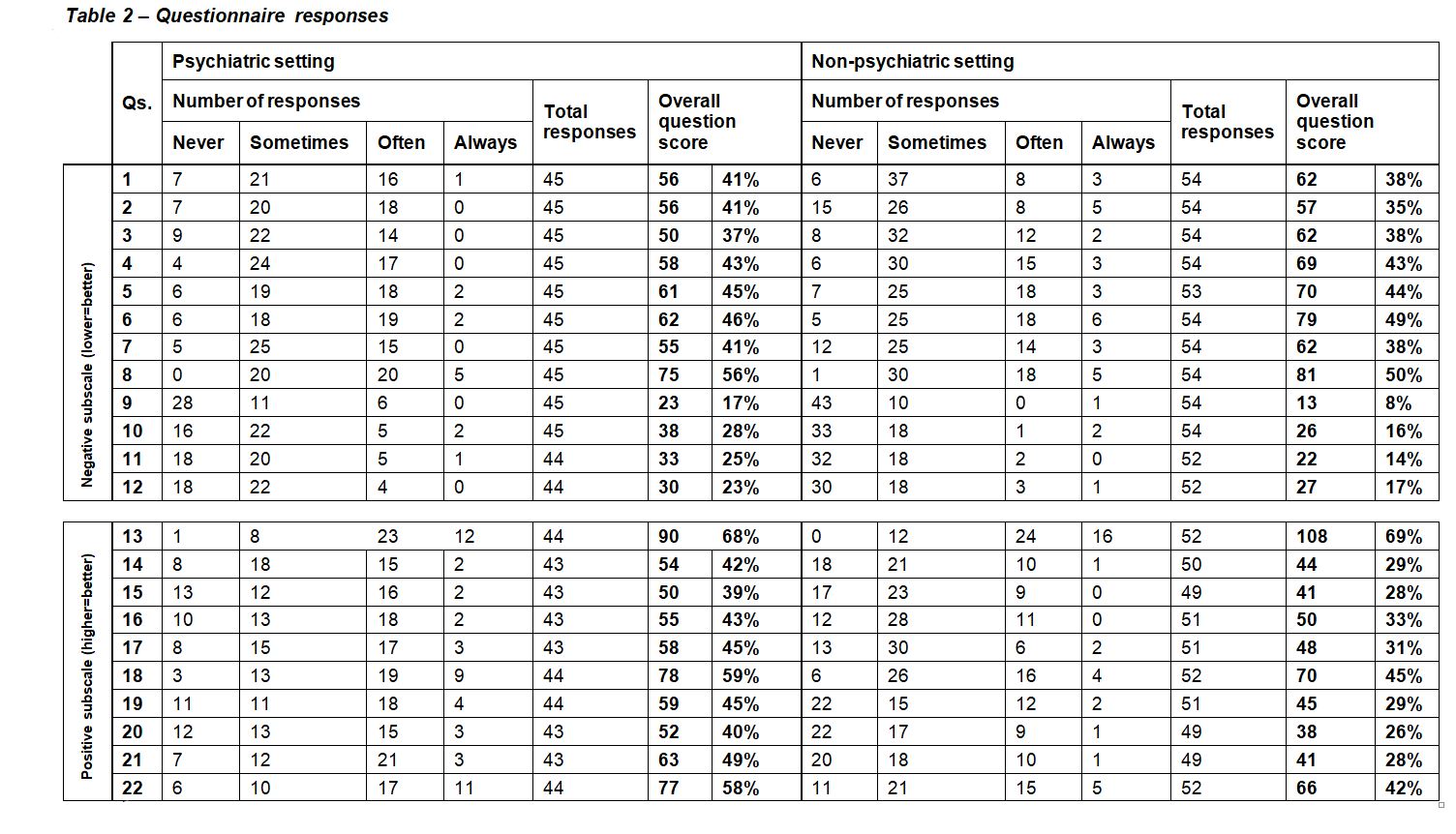
Table 2
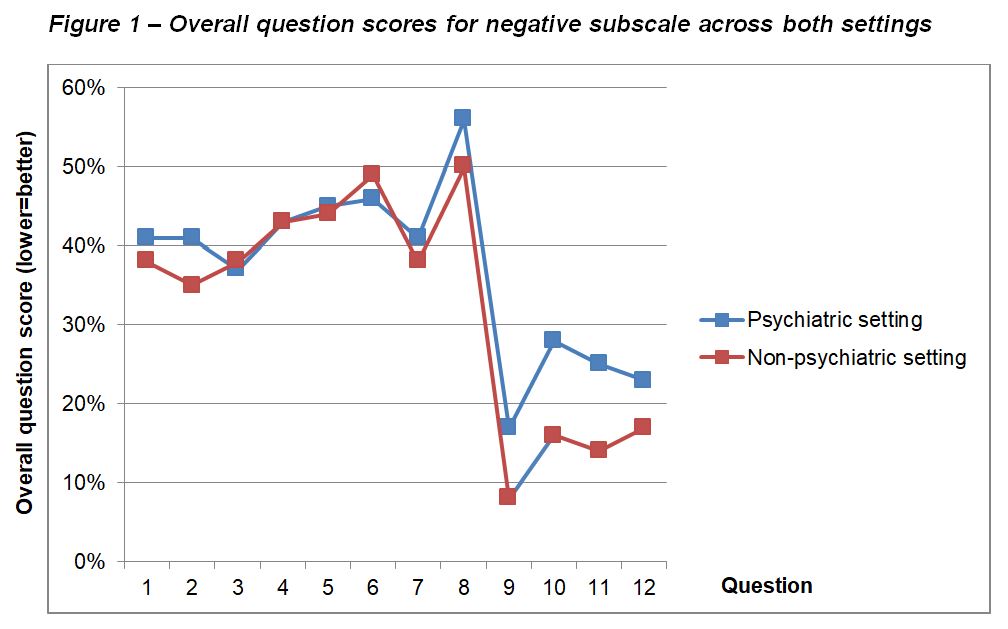
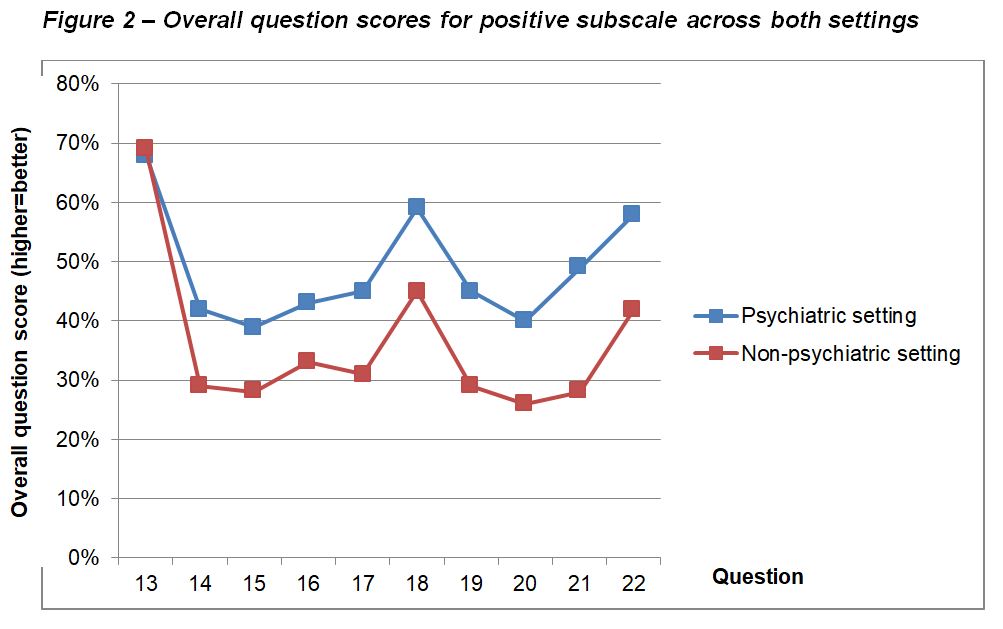
Questionnaire responses are shown in Table 2, along with calculated overall question scores and overall subscale scores for each subscale in both settings. Differences in overall question scores between settings are shown in Figure 1 and Figure 2.
Figure1
Figure 2
Overall question scores across the negative subscale were generally high, indicating a high incidence of negative work-home interaction among all respondents. Scores for questions 1-8, which ask about negative impact of work on home life, showed little/no difference between the two settings. Questions 9-12, which ask about negative impact of home life on work, recorded much lower scores in both settings, but there was separation between the settings, with scores in the psychiatric setting being higher than those in the non-psychiatric setting.
In the positive subscale, questions 13-17 ask about positive impact of work on home life, and questions 18-22 ask about positive impact of home life on work. Overall, there was a much more clear separation in scores between the two settings than that seen in the negative subscale. Aside from question 13, scores in the psychiatric setting being consistently higher than those in the non-psychiatric setting.
Main findings of this study can therefore be summarised as:
High negative impact of work on home life in both settings
Lower levels of negative impact of home life on work, but higher in the psychiatric setting
Higher positive impact of home life on work, and work on home life, in the psychiatric setting than in the non-psychiatric setting
Discussion
There has been a great interest in the wellbeing of junior doctors in recent years, resulting in a number of changes in working patterns, such as the move away from the old “firm” structure to medical training, and the introduction of the European Working Time Directive.7 However, the perceived wellbeing of junior doctors in the UK seems to still be poor, and has resulted in a so-called “Drexit” of junior doctors to other countries, such as Australia, providing a better quality of life or away from medicine altogether.7 One survey shockingly revealed that almost half of UK junior doctors have considered leaving the National Health Service, citing concerns over wellbeing.7 It is, therefore, unsurprising that in 2018, only 38% of FY2 doctors continued into speciality training.8
Various aspects of junior doctor wellbeing and contributory factors have been researched. For example, a large survey of Australian junior doctors published in 2020 showed that those working only a few more hours than the average were more than twice as likely to report common mental disorders.9 Many interacting themes have been qualitatively identified, such as those found in a recent Australian qualitative survey.10 These ranged from institutional issues such as discouragement to claim overtime, to cultural issues such as not wanting to ask for assistance, to personal issues such as time for personal care. Another study found multiple factors to be correlated with higher rates of burnout in hospital doctors, including male sex, younger age, and lower years of practice.1
It seems that wellbeing in junior doctors is a highly complex, multifactorial issue with many interacting contributory factors. In addition to considering the individual factors at work, it is also necessary to consider how these factors interact on a larger scale. One way which researchers have done this, and which we have replicated, is to consider the concept of “work-life balance”, which explores the interaction between work and home life, and vice-versa. Existing research in junior doctors has found work-life balance to be particularly poor in those with children and in women, who frequently cited that this had resulted in a change in career direction.2
Unsurprisingly, we have found high levels of work negatively impacting on home life in both psychiatric and non-psychiatric settings. Since work-life balance involves many interacting components, we speculated that it may differ between junior doctors working in different medical specialities. Indeed, we detected such differences, with the reported negative impact of home life on work being higher among those trainees in the psychiatric setting than those in the non-psychiatric setting. In a cross-sectional study like ours, it is not possible to comment on causality but we noted that there were significantly more trainees in the psychiatric setting who had children. This correlates with previous findings,2 and raises the possibility of a causative relationship between having children under 18 and negative impact on work. A study of stress in psychiatrists which gathered responses from 449 participants found that sickness of children and arranging childcare were among the top five stressors identified.11
Trainees in the psychiatric setting have consistently reported higher levels of positive impact of work on home life and vice-versa. One possible explanation is that the nature of psychiatry is inherently different to other areas of medicine, with a focus on promoting the quality of patient interaction, and training time dedicated to exploring this in detail. Supervision of patient contact is also conducted more thoroughly than in other specialities, which may lead to a greater sense of being supported in clinical decision making when trainees work in psychiatry.
Strengths and limitations
Regarding strengths of this study, we used an innovative method in seeking to compare trainees across two different settings. The questionnaire used was validated and holistic in examining bidirectional interaction between work and home life. Groups were well-matched in terms of the selection of trainees with broadly similar working rotas, and in their age and sex, which have been shown to be important variables which can affect work-life balance. We also used an innovative method in analysing the questionnaire responses which enabled us to compare directly between the two settings.
There are several limitations with this methodology which identify possible interesting and important areas for future research. For example, we did not investigate for differences in work-life balance between staff working in inpatient and community settings. Additionally, it was not possible to make conclusions about causality with this cross-sectional methodology, and the use of a longitudinal method with a more detailed exploration of demographic factors may provide interesting insights in the future. Due to local factors in the way psychiatric and general healthcare services are set up in our area, it was not practical to measure participant engagement with the study, and this would have presented a barrier making this study impossible. There were however 99 responses included in this study, with similar representation in both healthcare settings, which relative to the local population of doctors in the settings studied represents a good sample.
There will inherently be local differences in working patterns, and therefore the results of this study are not directly generalizable to a national or international population. The non-psychiatric setting is broad in its scope and includes trainees undertaking varied forms of medical and surgical training, and therefore there are likely to be more subtle variations which were missed in this approach.
Conclusion
This study adds to the literature on work-life balance in junior doctors, which is an important area of research in order to promote the wellbeing of the current and future medical workforce. It also explores how factors affecting wellbeing might interact on a higher level than when studied in isolation, and how these interactions may differ depending on the medical speciality in which the respective doctors work.
Because of the local variations in working patterns, we would suggest a replication of this research in other areas in the UK and abroad. We would also suggest that an interesting area for future research may be the exploration of differences in work-life balance between narrower groups of trainees, which may aid developmental policy generation in supporting doctors to maintain a healthy work-life balance across different specialities. The group we feel would benefit from further research in particular is the trainees with young children, as we found a possible negative association between this and impact of home life on work.
Sceptical attitudes towards Covid 19 vaccines effectiveness and/ or safety are currently a major risk to global health. However, not every person declining Covid 19 vaccination is an irrational conspiracy theorist (1). Patients suffering from specific conditions may have justified concerns that in the absence of safety data for their specific health problems, they may find it difficult to appraise the risks associated with the vaccination in their condition.
Patients suffering from long term complications of Covid 19 have coined the term long covid to describe their debilitating illness (2). Many clinicians feel that long covid complexity may reflect different pathological processes (3) with respiratory symptoms being primarily secondary to tissue damage whilst fatigue and its associated post exertional symptoms such as physical pain or brain fog resulting from a dysregulated immune response (4).
Two mRNA vaccines developed by Pfizer Biontech and Moderna have demonstrated impressive levels of immunity against SARS CoV-2 virus in randomised controlled trials (5,6). This relatively new technology had several advantages that made it one of the earliest vaccines to be developed, tested, scaled up and subsequently approved for use all over the world. The potency of the immune response is another significant advantage of mRNA vaccine as suggested by previous in vitro and animal experiments (7).
This potency is naturally a positive characteristic especially when mRNA vaccine technology is used against an easily transmissible and potentially lethal disease. However, for patients suffering from long covid, such a strong immune response could be a cause for concern.
As vaccination programmes against SARS CoV. 2 Virus are rolled out around the world, long covid patients face a difficult decision as no data is available about the impact of the mRNA vaccines on their condition. In the UK, long covid is not considered to be a contraindication for vaccination (8); however, in the absence of any safety data for this group of patients, it is very difficult to provide an informed opinion about the risk.
Methods
In the summer of 2020, Wrightington, Wigan and Leigh NHS Trust Hospitals established a dedicated service for staff suffering from long covid. As Health Care Workers (HCW) in the UK were prioritised for vaccination, Pfizer Biontech Vaccine was offered to all Hospital employees with the first dose provided between end of December 2020 and end of January 2021.
A survey questionnaire was sent to all long covid staff members 2 weeks following the conclusion of the first dose roll out. The e-mail addresses were obtained from the long covid clinic data base. This short questionnaire evaluated the rate of acceptance of the vaccine, reasons for declining, immediate side effects and any persistent change of the long covidsymptoms following the vaccination. The survey was approved by the information governance department.
Results
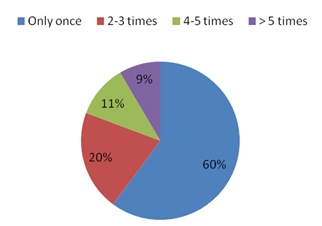
The questionnaire was sent to 117 HCW. Out of 83 responses, 77 subjects were offered the vaccine (age range:18 - 65 with only 7 male respondents).
10 HCW declined having the vaccine (13 %) with 5 of them citing concerns about worsening symptoms as the main reason. Out of 67 HCW receiving the vaccine 48 (72%) had immediate but self-limiting side effects.
Fatigue, shortness of breath and anxiety were the most common symptoms of long covid our cohort originally had (75%, 53% and 18% respectively). Several weeks following vaccination, 45 subjects reported no change (67%) in symptoms. Fourteen (21%) subjects reported improvement of one or more of their symptoms (8 of them experienced improving respiratory symptoms, 4 improving fatigue, 5 improving anxiety and 2 mentioned improving other symptoms). Eight subjects (12%) reported worsening symptoms including fatigue (3 subjects), respiratory (1 subject), anxiety (2 subjects). Two subjects experienced worsening of other symptoms.
Discussion
When offered vaccination, our long covidpatients showed higher rates of compliance (86%) compared to the general population (9). However, five patients declined the vaccine because of their concerns about worsening symptoms.
Despite having a small number of subjects, limitations to the survey methodology and the relatively short period following vaccination, our report is the first to comment on the response of a cohort of long covid patients to mRNA vaccination. Most of our HCWs didn’t report any change in their symptoms with encouragingly 21% experiencing subjective improvement of symptoms with 10% of all participants reporting respiratory symptoms improvement. The 8 subjects reporting worsening of symptoms experienced more diverse problems with worsening fatigue the most common.
Our results were consisted with unpublished data reporting the feedback of 473 long covid social media users (10). 32% of this self-selecting population reported improvement of symptoms whilst 17% reported worsening of symptoms.
We would like to suggest two potential explanations for our findings. Comprehensive investigations for the respiratory system could be normal in some long covid patients complaining of shortness of breath (11). Dysfunctional breathing might contribute to the severity of shortness of breath (12). The confidence given to the patients from taking the vaccine may act in a positive way to reduce their anxiety and subsequently such perception of the respiratory effort.
Another potential explanation is the complex way mRNA vaccines manipulate the immune system potentially improving or worsening the already dysregulated immunity in long covid patients (4). It is encouraging to see that long covid patients are about twice as likely to experience improvement of symptoms compared to patients experiencing worsening of symptoms. We hope that our findings may be an early source of reassurance that mRNA Covid 19 vaccines are not commonly associated with adverse effects in long covid patients.
We feel that longitudinal studies appraising long covid symptoms and immunological markers correlating the pre and post mRNA vaccines may have the potential not only to improve understanding of the main long covid pathologies but may also unlock the secrets of Chronic Fatigue Syndrome / Myalgic Encephalomyelitis (ME/CFS) as a common condition possibly sharing many of long covid characteristics.
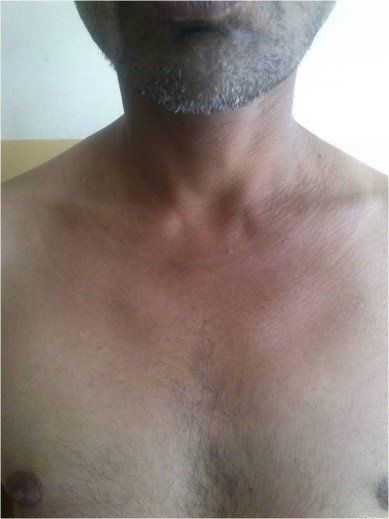
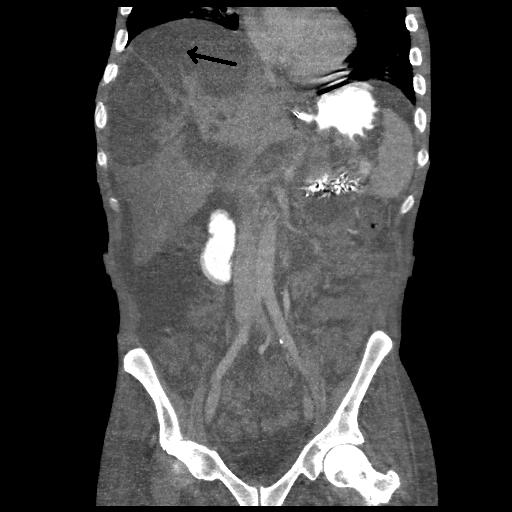
A 40 years old non-alcoholic and non-diabetic agricultural laborer presented with skin lesions around his neck, forearms and feet (sun exposed areas) along with glossitis. Pellagra was suspected because of Casal's necklace (i.e., erythematous, hyperpigmented, scaly lesions around his neck- arrow mark in figure 1). However he did not have diarrhea or neurological manifestations. Pellagra is due to Niacin (Vitamin B3) deficiency. Typical cases of pellagra are associated with 3 Ds - Dermatitis, Diarrhea, Dementia, (and if not treated, the 4th D- Death).1,2 Not many will have all the three Ds. Most commonly involved is skin – dermatitis (Pelle-skin; agra -rough). The patient belonged to poor socioeconomic status.2 His vital parameters and basic investigations were all within normal limits and HIV-ELISA was negative.
The diagnosis of a pellagra-like dermatitis was entertained.3 He was treated with multivitamin capsules which included Niacinamide.2
The skin lesions had disappeared dramatically at the time of follow-up after one month (figure 2).
Since 2005, there has been an increase of 10% in hospital admissions with acquired brain injury (ABI), with 348,453 United Kingdom (UK) admissions in 2016-17.1 With improvements to both medical and surgical management, a higher proportion of patients survive to hospital discharge, resulting in more people with complex physical and cognitive disabilities reaching the community.2,3
Prolonged disorders of consciousness (PDOC) can occur following ABI. This can vary from coma, to vegetative state (VS), and minimally conscious state (MCS). Following acute stabilisation, the treating team must provide the correct diagnosis, prognosis, and management. Ethical and legal issues, such as best interests decision-making (considering patient wishes, advanced decisions, and best possible quality of life), deciding when appropriate to provide end-of-life care, and understanding the legal framework around these issues can further complicate the process.
Whilst there is currently no national registry for patients with PDOC, information taken from patients in nursing homes in the UK give an estimated 4000 – 16000 patients in VS, and up to three times this many in MCS.4
Early and ongoing assessment of the patient is vital, as is good communication with those close to the patient, and an understanding of the legal requirements of the treating clinician. These are likely to present even more of a challenge to General Practitioners (GP) in the community who are managing these patients as part of their larger responsibilities.
This review article summarises guidance from the Royal College of Physicians (RCP) and British Medical Association (BMA), in conjunction with our own clinical experience, to improve understanding surrounding the assessment, long term management, and the ethical and legal issues in patients with PDOC, aiming to improve the confidence of clinicians managing these patients.5,6
Identifying Patients
Consciousness requires a combination of wakefulness and awareness (self and environment). Patients with significant deficits in either of these can be said to have a disorder of consciousness. Various brain injuries can result in disorders of consciousness (see Table 1).
Table 1: Aetiology of acquired brain injury.5
Cause
Examples
Vascular
Stroke, subarachnoid haemorrhage
Hypoxic
Cardiac arrest, hypovolaemia
Infection / inflammatory
Encephalitis, vasculitis
Trauma
Primary brain trauma, diffuse axonal injury
Metabolic / Endocrine
Hypoglycaemia, drug overdose, alcohol
Degenerative
Primary neurodegenerative conditions such as dementia
This article focuses on acute causes of PDOC rather than those with primary neurodegenerative conditions, as they present separate clinical entities with different issues affecting prognosis and management choices.
Disorders of consciousness, like a sliding scale, vary from coma, to VS, and MCS:
Coma - unrousable unresponsiveness. Patients cannot be roused, lack a sleep-wake cycle, exhibit no purposeful movement, and do not respond to stimuli.
VS - wakefulness but not awareness. Patients have a sleep-wake cycle and open their eyes spontaneously, but lack awareness of self or their environment. These patients can exhibit spontaneous and reflexive movements, and external stimuli can produce arousal responses.
MCS - wakefulness but reduced or inconsistent awareness. Patients have a sleep-wake cycle and demonstrate reproducible but inconsistent awareness of self, and ability to interact with others and their environment.
Diagnosis
As per RCP guidance 2020, patients with impaired consciousness for over 4 weeks are deemed to have PDOC.5 It is first important to differentiate possible VS / MCS from other conditions:5
Abnormalities on electroencephalography (EEG) can aid diagnosis of coma. These patients tend to progress to VS or death within weeks, so assessments of consciousness are not appropriate during this period.
Patients with locked-in syndrome have wakefulness and awareness, but paralysis of the limbs and majority of facial musculature, preventing communication by these means. EEG in locked-in syndrome is usually normal, and patients may be able to communicate using eye movements.
Patients with brainstem death have loss of all brainstem reflexes and respiratory effort, and organ survival is only temporarily achieved with life support machines.
Once ‘mimic’ conditions are ruled out, making a diagnosis of VS or MCS in patients with a suspected disorder of consciousness follows a 3-step process with input of clinicians trained in the management of PDOC:
1. Establishing a cause
This can be straightforward in some cases, such as those with direct trauma to the brain, or acquired brain infections or inflammation causing structural damage to the brain. In other cases this can be more difficult, and it may not possible to reach an exact diagnosis. The treating clinician must establish that the patient’s current condition is due to a brain injury, and take reasonable steps to determine the cause.
2. Reversible causes should be excluded
This includes reviewing medications to stop sedative medications whenever possible, blood tests to look for infection or metabolic / electrolyte abnormalities, up-to-date imaging to rule out new onset hydrocephalus, or performing an EEG to rule out subclinical seizures needing antiepileptic medication. This step also includes establishing that neurological pathways are intact, so that any assessment of consciousness provides an accurate reflection of the patient’s condition. Briefly, this involves examination and investigations to confirm that sensory, visual, auditory, and motor pathways are intact.
3. Structured assessment
There are several tools available which can confirm the diagnosis of VS or MCS. All of these require a trained assessor and an appropriate environment. These tools provide a structured method of assessing the patient to:
Observe spontaneous behaviours.
Observe the patient’s reaction to stimuli from different sensory modalities.
Document the findings of family / friends / members of the healthcare team following their interactions with the patient.
Tools available include the Wessex Head Injury Matrix (WHIM), the JFK Coma Recovery Scale-Revised (CRS-R), and the Sensory Modality Assessment and Rehabilitation Technique (SMART), amongst others. As per RCP guidance, the CRS-R should be the primary assessment tool, and WHIM or SMART can be used to provide additional information. Furthermore, assessments need to be performed on at least 10 occasions, at several different times of the day, and over the course of a 2-3 week period.5,7-9
The 2020 RCP guidance also addresses how to manage patients that do not present through the acute hospital pathway.5 In these ‘late assessment’ cases, formal assessment is still required to establish their level of consciousness and guide management. These patients should be referred to an experienced PDOC assessor to establish the cause of PDOC, rule out reversible causes, and arrange formal evaluation. This should ideally be achieved by outreach assessments, but if this is not possible, structured interviews should be held with family and care staff to complete the CRS-R. If these measures do not provide a definite diagnosis, admission to a PDOC centre can be considered.5,8
Vegetative State & Minimally Conscious State
Patients in VS are unable to interact with their surroundings or those around them (no voluntary behaviours / communication / purposeful movements), and show no evidence of awareness of self. The patient may demonstrate reflexive behaviour (such as increased heart rate or startle response to noise), or spontaneous, purposeless movements (such as eye movements, teeth grinding, or limb movements). These behaviours can be misleading, which is why an objective and structured assessment method is vital.
Patients in MCS have some evidence of awareness of self or their environment, on a reproducible but inconsistent basis. Patients demonstrate behaviours such as: following simple commands, verbalisation, and purposeful behaviour MCS which is further classified based on the level of responsiveness:
MCS-minus - less complex behaviours such as orientation to noxious stimuli, or purposeful eye movements.
MCS-plus - more complex behaviours such as following instructions or interacting with objects.
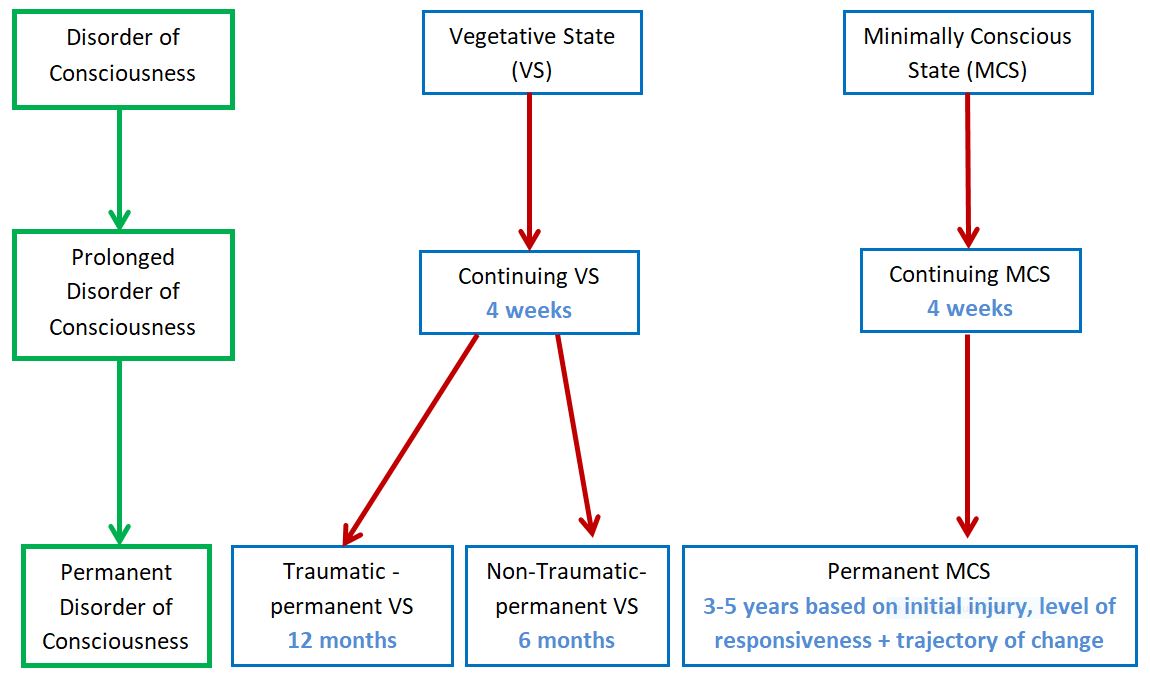
Prognosis depends on cause, time since brain injury, and the trajectory of improvement (better prognosis for those who quickly progressed from VS to MCS). Those with traumatic brain injury are more likely to regain awareness and have a longer window for potential recovery. The majority of VS patients that regain consciousness tend do so within 12 months in traumatic cases, and 3 months in non-traumatic cases. The majority of MCS patients that regain consciousness do so within 2 years post injury, although others can emerge at up to 4 years. Whilst these are the expected outcomes, there are, however, rare case reports of patients emerging later than this.
VS / MCS-minus are classed as ‘continuing’ at >4 weeks post brain injury, and ‘chronic’ at >3 months for non-traumatic cases, or >12 months in traumatic cases. MCS-plus is classed as ‘continuing’ at >4 weeks post brain injury, and ‘chronic’ at >9 months for non-traumatic cases, or >18 months in traumatic cases. Chronic VS / MCS can be classed as ‘permanent’ when there has been no further change in trajectory of serial CRS-R for 6 months. In permanent PDOC it is predicted that consciousness is highly improbable to recover. It is important to remember these time frames, and their implications during discussions with family, when making best interests decisions and planning further assessments of consciousness.5,10,11
With the longer time period for potential emergence, and improved survival rate compared to VS, GPs are more likely to come across these patients in the community. Figure 1 outlines the key time points for assessment of VS and MCS.12
Figure 1: Timeline for assessment of VS & MCS.5
Emergence
A patient is considered to have ‘emerged’ from PDOC if they are able to consistently demonstrate awareness of self and surroundings. The RCP advise that patients who have emerged are able to do at least one of the following:5
Functional interactive communication (accurate yes/no responses to 6/6 basic questions on 2 consecutive evaluations).
Functional use of objects (intelligent use of ≥2 objects on 2 consecutive evaluations).
Consistent discriminatory choice-making (correct identification between 2 pictures, 6/6 times, on 2 consecutive evaluations).
Specialist Involvement
Early specialist input from a neurological rehabilitation team is recommended. The Royal College of Physicians Guideline Development Group advise that those with an ongoing disorder of consciousness at 4 days (Glasgow Coma Scale ≤10/15) should be referred for assessment, and advice regarding neurological disability and prevention of complications.5,13 At 2 weeks the patient should be referred for specialist neurological evaluation to identify the cause of the disorder of consciousness, assess the primary neurological pathways, and advise on further investigations.
Patients with ongoing disorder of consciousness at 4 weeks should have regular input from a specialist neurological rehabilitation team, led by a consultant in Rehabilitation Medicine. Once stable the patient should ideally be transferred to a specialist neurorehabilitation unit for multidisciplinary care, objective assessment of level of consciousness, formal best interests decision-making, and discharge planning.
Following this initial period, the patient should be placed in a unit away from the acute setting, where they can be monitored until it is evident that they are likely to remain in VS / MCS. These ‘slow-stream’ rehabilitation units, are designed to deliver care to patients with complex neurological disability, and provide appropriate maintenance therapy to manage physical disability. Medical input is usually provided by the GP surgery covering the area, although units should also have access to rehabilitation medicine physicians with experience in managing PDOC.
If it is agreed that a patient has permanent VS / MCS, then longer-term of care can be provided in a nursing home or, if appropriate, in the patient’s own home. A skilled assessor should review the patient yearly, with formal assessment of consciousness until either the patient emerges or dies.
Medicolegal & Ethical Issues
Capacity Assessments
By definition a person in PDOC lacks capacity to make decisions about medical treatment. The Mental Capacity Act 2005 requires this to be formally documented in the medical notes. A Deprivation of Liberty Safeguard should be put in place during hospital admission or nursing / residential home stay, providing that restraint and restrictions are in the patient’s best interests.14
Identifying Advance Decisions
The team providing care need to identify as early as possible whether the patient has a valid and relevant Advance Decision, Health and Welfare Lasting Power of Attorney, or Court-appointed Welfare Deputy. If one of these is in place, the team need to request to see the relevant documentation to understand what exactly it entails.
Best Interests Meetings
All medical treatment provided must be in the patient’s best interests. In the UK, the treating clinician must by law identify those people close to the patient that can provide insight into the patient’s beliefs / previous expressed wishes / likely wishes, and take part in best interests meetings. If there is nobody to fulfil this role then an Independent Mental Capacity Advocate must be appointed. An initial best interests meeting should be held to discuss the diagnosis, likely prognosis, and to plan treatment. Further meetings should be held at planned regular intervals, for major medical decisions, and following repeat assessments to decide future management, discharge planning, and ceilings of care.
Ceiling of Care Discussions:
Many relatives may not feel comfortable bringing up these topics themselves, so it is advisable to make the discussion part of a routine review as standard for PDOC patients.
In patients with PDOC, cardiopulmonary resuscitation (CPR) has a very low success rate, and will likely result in further brain injury due to hypoxia. For the majority of patients where emergence is not expected, or if it is felt that the patient would not accept their level of quality of life, CPR could be considered to be futile. This is because CPR would not provide a perceivable benefit to the patient, but would carry significant risks of harm (worsening brain injury, injury related to the CPR itself, undignified end of life). Decisions regarding ceiling of care or appropriateness of resuscitation should either follow the instructions set out in existing advanced directives, or be discussed together with the treating multidisciplinary team (MDT). It is highly advisable to involve close family / friends in discussions, but ultimately it is a medical decision.
For similar reasons, it should be considered whether hospital admission for treatment of acute deterioration is in the patient’s best interests. For example in a patient with permanent VS, treating an acute chest infection may improve their lungs, but will not improve the patient as a whole in a way that can be perceived and appreciated by that patient, so may be considered futile. Additionally, it may be considered appropriate to stop medications not aimed at providing comfort, or stop performing observations and investigations. As with all major medical decisions, this should be discussed within the MDT and with those close to the patient. Although patients with PDOC have absent / reduced awareness, care should be taken to maximise patient comfort, and if appropriate consider input from the palliative care team.
Decisions relating to withdrawing clinically assisted nutrition and hydration (CANH) have previously been managed differently than withdrawal of life-sustaining treatment. Until recently, the decision to withdraw CANH could not be made without referring to the Court of Protection (COP). More recent guidance published by the BMA advises that in PDOC this is not always necessary. The treating team should first establish whether there are any valid and relevant advance directives / health and welfare attorney with relevant power, and then follow a best interests decision-making process. If all parties are agreed that withdrawal of CANH is in the patient’s best interests, then a second opinion should be obtained (from an independent, expert PDOC physician); if they also agree, then CANH can be withdrawn. If there is any doubt or disagreement about the decision, then an application to the COP is required. Now in the UK, it is essential to have best interests meetings to decide whether provision or continuation of CANH is of benefit to the patient, rather than deciding whether to withdraw it. If CANH is determined to not be of overall benefit to the patient, then it should not be continued. Prior to the withdrawal of CANH, an appropriate end-of-life care plan should be agreed and be ready to put in place.6
Conclusion
Disorders of consciousness can occur following brain injury, and vary from coma to MCS. If the disorder of consciousness continues for 4 weeks, it is described as a PDOC. Diagnosis requires structured assessment by trained clinicians, once the patient is medically optimised and reversible causes are excluded. Ongoing assessment is crucial to monitor recovery, guide prognosis, and establish when the disorder is permanent.
There are many ethical and medicolegal issues involved in managing patients with PDOC, which are mainly centred on the patient’s loss of mental capacity to make decisions. The cost implications of providing care as outlined in these guidelines can be quite significant. This article reflects our experience working within the National Health Service (NHS) within the UK, which provides free healthcare to all at the point of delivery. Therefore the costing is less relevant to the patients, although this does need to be considered when commissioning services. In other private healthcare settings, costs may vary widely based on hospital and wider multidisciplinary team costs, and this may need to be taken into account when commissioning services. Also, we appreciate that in other countries there are likely to be different laws surrounding PDOC, and varying views regarding the ethical decisions discussed.
Currently, these guidelines are based on expert opinion from the Royal College of Physicians Guideline Development Group. In future, management of patients with PDOC could be improved with the establishment of a national registry, further studies into PDOC, and better integration with community services. Furthermore, an improved education about PDOC and the issues surrounding it, as we have aimed to outline in this article, will help physicians understand their responsibilities and provide the best possible patient care.
Epidural anaesthesia is one of the favored and effective treatment options for labour pain. It is usually safe and only a handful situations lead to absolute contraindications to this technique such as patient’s refusal, lack of expertise and equipment, severe coagulopathy and infection at the site of puncture (1). However, as with any other technique and procedure, epidural anaesthesia is not flawless. The side effects and complications include hypotension, pruritus, inadequate analgesia, post puncture headache, nerve damage, infection, and epidural haematoma (1,2). Headache is common in one third of the patients after lumbar puncture however, the frequency is less in epidural anaesthesia as the fluid is injected in and not removed in the latter (3). Accidental dural damage and subsequent headache following epidural anaesthesia is uncommon and is an important cause of morbidity which can limit patient severely. Further, in rarest of rare cases Pneumocephalus can develop after epidural anaesthesia which has rarely been reported. We report a patient who developed Pneumocephalus after receiving epidural anaesthesia for labour pain.
Case Report:
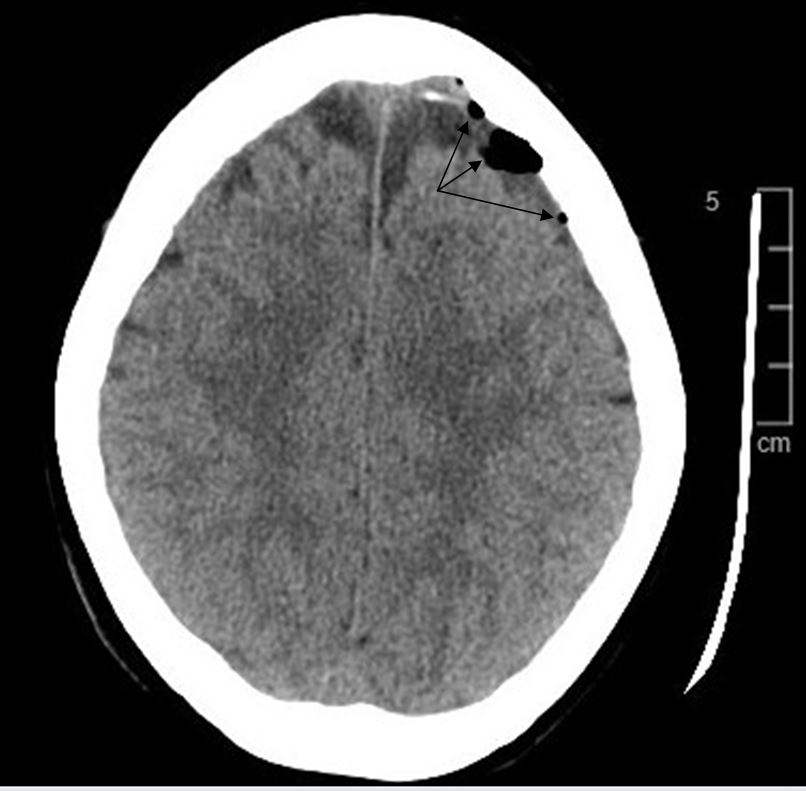
A 39 year old female presented to our Emergency Department with severe headache not responsive to analgesics. The headache started developing 10 to 12 hours after she was given an epidural which was attempted three times for labour pain which was four days prior at a nearby medical center . The severity of the headache did not change with lying or the upright position. She had no symptoms of vomiting, no fever and no confusion. Neurological examination and vital signs were unremarkable. The site of the spinal anaesthesia did not reveal any swelling or any signs of infection. An urgent head CT scan was performed which revealed Pneumocephalus denoted by numerous left fronto-parietal extra axial air locules (Figure 1 and Figure 2). MRI spine revealed mild subcutaneous oedema at the site of the needle insertion without any haemorrhage or collection. The patient was admitted and treated conservatively for six days and follow up serial head CT scans showed complete resorption of the Pneumocephalus and the patient’s symptoms resolved completely. The patient was discharged and the follow up was uneventful.
Figure 1: Pneumocephalus seen as locules of air (black color) in the left fronto-parietal region denoted by arrows (Axial section)
Figure 2: Multiple pockets of air seen in the Saggital section marked by arrows demonstrate the Pneumocephalus.
Discussion:
Pneumocephalus is the presence of air in the intracranial cavity. It can be acute ( less than72 hours ) or delayed (more than 72 hours). The most common site is the frontal region (4). Plain skull x-rays can detect Pneumocephalus of about 2 ml, whereas it requires only 0.5 ml of air to be detected by a CT scan (5). Pneumocephalus is most commonly a result of traumatic brain injury, surgical intervention of the brain or infection (5). Trauma accounts for up to 75% percent of the total cases. Chronic infections of ENT especially otitis media also amounts to a number of significant cases. Surgical procedures of brain, spine and ENT like sinus surgery, nasal polypectomy and nasal septum resection accounts for the causes. The incidence after supratentorial craniotomy has been reported to be 100% (6, 7). However, it is very unusual for pneumocephalus to develop post epidural anaeasthesia possibly due to ball valve mechanism in which the air enters the space through the CSF leakage which allows input but not output. Headache post lumbar puncture and epidural anaesthesia is relatively not uncommon but certain situations may demand a more thoughtful approach (3).
In our patient we suspect there was a puncture of the dura during epidural anaesthesia which led to air being trapped and siphoned upwards in an inverted soda bottle fashion. This is supported by the meta-analysis done by Choi et al. which states the incidence of accidental dural puncture in epidural insertion to be 1.5% and among those 52 % will have post puncture headaches (8). In another extensive study performed over ten years, the overall incidence of accidental dural puncture and postdural puncture headache were 0.32% and 0.38%, respectively (9). The authors further stressed that if more than one attempt was required to identify the epidural space, the accidental dural puncture rate increased to 0.91%. In our patient we witnessed the same wherein three attempts were made to identify the epidural space which increased the risk of dural injury and subsequent leaking. Pneumocephalus usually gets absorbed without any clinical manifestations. The conservative treatment involves placing the patient at rest, avoiding Valsalva manoeuver, administering analgesics. With these measures, reabsorption was observed in 85% of cases after 2–3 weeks (5). Use of oxygen mask, nasal catheter, hyperbaric oxygen sessions and good hydration have also been reported. If conservative measures fail to provide the desired results then specific treatment like a epidural blood patch or even surgical closure of the dural gap is indicated (3, 10).
Ventilator-associated pneumonia (VAP) is a type of nosocomial pneumonia that occurs in patients who receive mechanical ventilation and is usually acquired in the hospital setting approximately 48–72 hours after mechanical ventilation.1 VAP is one of the most frequent hospital-acquired infections occurring in mechanically ventilated patients and is associated with increased mortality, morbidity, and health-related costs. Several risk factors have been reported to be associated with VAP, including the duration of mechanical ventilation, and the presence of chronic pulmonary disease, sepsis, acute respiratory distress syndrome (ARDS), neurological disease, trauma, prior use of antibiotics, and red cell transfusions.2 VAP occurrence is closely related to intubation and the presence of the endotracheal tube (ETT) itself.
Since there are inadequate objective tools that are utilized to make an assessment of bacterial-induced lung injury in a heterogeneous group of hosts, the diagnosis of VAP is challenging. Around 90% of ICU-acquired pneumonias occur during mechanical ventilation, and 50 % of these ventilator-associated pneumonias begin in the first 4 days after intubation.3 VAP has a cumulative incidence of 10-25% and accounts for approximately 25% of all ICU infections and 50% of its antibiotic prescription, making it the primary focus for risk-reduction strategies.1,4 For all these reasons, early diagnosis and prevention of VAP has held a prominent position on the research agenda of intensive care medicine in the past 25 years, with an ultimate goal of improving patient outcome, preferably by reducing mortality.
The keywords, ‘ventilator-associated pneumonia,’ in PUBMED revealed a total of 3612 titles and 625 review articles within the search limit of 10 years, between 2005 and 2014. Only articles in English were chosen.
PATHOGENESIS
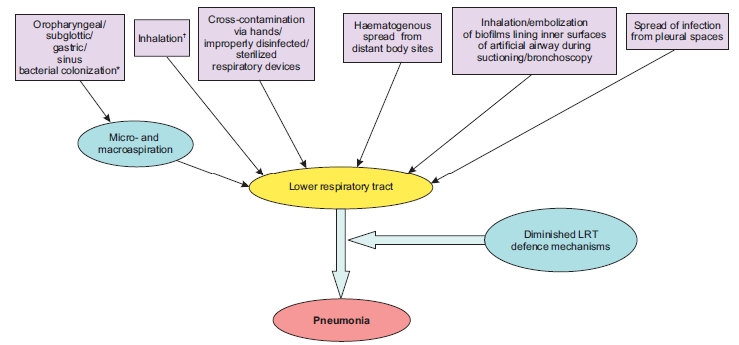
Understanding the pathogenesis of VAP is the first step in the formulation of its appropriate preventive and therapeutic strategies. The initial step in the pathogenesis of VAP is bacterial colonization of the oropharynx and gastric mucosa, followed by translocation of the pathogens to lower respiratory tract. The most common means of acquiring pneumonia is via aspiration which is promoted by supine position and upper airway and nasogastric tube placement.2,5 In a mechanically ventilated patients, aspiration occurs around the outside of the endotracheal tube rather than through the lumen. Secondly, aerobic Gram-negative bacteria presumably reach the lower airway via aspiration of gastric contents or of upper airway secretions. Other means by which VAP can be acquired include aspiration from the stomach or nose and paranasal sinuses. Figure 1 depicts the essential elements favoring colonization of lower respiratory tract with the bacterial pathogens with subsequent development of pneumonia.2,5,6
Figure 1: Pathogenesis of Ventilator-associated pneumonia5 *Gastric alkalinization; prior antimicrobials; ICU stay; intubation; supine position; circuit/airway manipulation and mishandling; device cross-contamination; sedation; diminished cough reflex; and malnutrition predispose to colonization and aspiration. As the duration of ICU stay increases, colonization with MDR Gram-negative pathogens like Pseudomonas and Acinetobacter increases. †Via contaminated nebulizers/aerosols Reproduced with permission from the publisher.
COMMON CAUSES
The specific microbial causes of VAP vary widely depending in epidemiological and clinical factors. Common pathogens include aerobic gram negative bacteria such as Pseudomonas aeruginosa and members of family Enterobacteriaceae, staphylococci, streptococci, and Haemophilus species. Microorganisms like Pseudomonas spp., Acinetobacter spp. and Methicillin-Resistant Staphylococcus aureus occur commonly after prior antibiotic treatment, prolonged hospitalization, mechanical ventilation or when other risk factors are present.6,7
Moreover, deliberated ill patients may have defect in phagocytosis and behave as functionally immunosuppressed even prior to emergence of nosocomial infection as seen by many recent studies.8,9
DIAGNOSIS
Clinical Diagnosis
No gold standard of diagnosis for identifying VAP is there inspite of variety of proposed definitions. VAP has traditionally been diagnosed by clinical criteria of Johanson and colleagues (appearance of new or progressive pulmonary infiltrates, fever, leucocytosis and purulent tracheobronchial secretions), which are non-specific. When findings on histologic analysis and cultures of lung samples obtained immediately after death were used as references, a new and persistent (>48-h) infiltrate on chest radiograph plus two or more of the three criteria (i) fever of >38.3°C, (ii) leukocytosis of >12 × 109/ml, and/or (iii) purulent tracheobronchial secretions had a sensitivity of 69% and a specificity of 75% for establishing the diagnosis of VAP.10
Because of the poor specificity of the clinical diagnosis of VAP and of qualitative evaluation of ETAs, Pugin et al. developed a composite clinical score, called the clinical pulmonary infection score (CPIS), based on six variables: temperature, blood leukocyte count, volume and purulence of tracheal secretions, oxygenation, pulmonary radiography, and semi-quantitative culture of tracheal aspirate. The score varied from 0 to 12. A CPIS of >6 had a sensitivity of 93% and a specificity of 100%.11 Accuracy of CPIS in diagnosis of VAP is debated, despite of its clinical popularity. In one meta-analysis study evaluating the accuracy of CPIS in diagnosing VAP reported pooled estimates for sensitivity and specificity for CPIS as 65 % (95 % CI 61-69 %) and 64 % (95 % CI 60-67 %), respectively.12 The poor accuracy of clinical criteria for diagnosing VAP is due to purulent tracheobronchial secretions in patients receiving prolonged mechanical ventilation which are rarely caused by pneumonia. Moreover, in pneumonia systemic signs such as fever, tachycardia, and leukocytosis are nonspecific; they can be caused by any state that releases the cytokines interleukin-1, interleukin-6, interleukin-8, tumor necrosis factor alpha (TNFα), and gamma interferon.13,14 The weak point of CPIS is probably the inter-individual variability (kappa= 0.16), since a subjective evaluation is required when we are judging the quality of tracheal secretion (purulent/not purulent) and the presence of infiltrate at chest ray.15
Radiologic Diagnosis
Radiographical evidence of pneumonia in ventilated patients is also notoriously inaccurate. In a study of autopsy proven VAP, of the total population, only air bronchograms correlated with pneumonia and no specific roentgenographic sign correlated with pneumonia in patients with adult respiratory distress syndrome. The differential diagnoses of VAP based on radiographical appearance, include adult respiratory distress syndrome, congestive heart failure, atelectasis, pulmonary embolism and neoplastic infiltration.16
Microbiologic Diagnosis
The type of specimen that should be obtained for microbiologic processing as soon as VAP is suspected is another area of importance. The use of quantitative cultures is one of the main issues for any diagnostic laboratory because there is oropharyngeal bacterial contamination of all respiratory secretion samples, despite this is not always undertaken in many hospitals today.16,17
Blood cultures
Blood cultures have limited value because organisms isolated from blood in suspected VAP cases are often from extrapulmonary sites of origin.18 Blood cultures in patients with VAP are clearly useful if there is suspicion of another probable infectious condition, but the isolation of a microorganism in the blood does not confirm that microorganism as the pathogen causing VAP.
Quantitative cultures of airway specimens
Simple qualitative culture of endotracheal aspirates has high percentage of false-positive results due to bacterial colonization of the proximal airways observed in most patients in the ICU.20 Quantitative culture techniques suggest that endotracheal aspirate cultures (QEA) may have an acceptable overall diagnostic accuracy, similar to that with several other, more invasive techniques including BAL, protected BAL (pBAL) ,protected specimen brush (PSB) or tracheobronchial aspirate(TBA).7,19,20 Threshold values often employed for diagnosing pneumonia by quantitative cultures are ≥105 to 106, ≥104, and ≥103 CFU/ml for QEA, bronchoscopic BAL, and PSB, respectively, with ≥105 CFU/ml being the most widely accepted value for QEA.21,22,23 Also, blind aspiration sampling can lead to errors but bronchoscope also carries risks, such as inducing cardiac arrhythmia, hypoxemia, bleeding, pneumothorax, along with greater costs both in terms of time and resources. It is accepted that before administering the first dose of antibiotic or before any change in treatment patient specimens for culture should be taken, so that the results interpreted are valid.24 Lalwani et al., in their study, observed that culture results of a properly collected tracheal aspirate should be taken into consideration along with Centre for Disease Control and Prevention (CDC's) diagnostic criteria to maximize the diagnosis of VAP.25
The recent guidelines of Society for Healthcare Epidemiology of America/ Infectious Diseases Society of America (SHEA/IDSA) recommend Gram staining of endotracheal aspirates. However, the sensitivity (57-95%) and specificity (48-87%) of this technique are highly variable. The role of procalcitonin and other biomarkers for the diagnosis of VAP is yet unsubstantiated.5,26
Since VAP diagnosis founded on radiographic findings of pneumonia, which have intrinsic variability in technique, interpretation, and reporting, and on clinical signs and symptoms- that are subjective- in 2011 a Working Group of the CDC proposed a new approach to surveillance for Ventilator-Associated Events (VAE). Table 1 According to the new CDC definition algorithm, VAP is an Infection-related Ventilator-Associated Complication (IVAC) occurring after 3 days of mechanical ventilation and 2 days before or after the onset of worsening oxygenation, if purulent respiratory secretions with positive cultures or objective signs of respiratory infection have been found.27
Table 1: CDC Algorithm for VAP diagnosis30
1= Purulent respiratory secretions AND one of the following:
2= One of the following (without requirement for purulent respiratory secretions):
Positive culture of endotracheal aspirate, ≥ 105 CFU/ml *
Positive pleural fluid culture
Positive culture of bronchoalveolar lavage, ≥ 104 CFU/ml*
Positive lung histopathology
Positive culture of lung tissue, ≥ 104 CFU/ml*
Positive diagnostic test for Legionella spp.
Positive culture of protected specimen brush, ≥ 103 CFU/ml*
Positive diagnostic test on respiratory secretions for influenza virus, respiratory syncytial virus, adenovirus, parainfluenza virus
On or after calendar day 3 of mechanical ventilation and within 2 calendar days before or after the onset of worsening oxygenation, criteria 1 or 2 is met (*or equivalent semi-quantitative result).
Table 2: Practices for which insufficient evidence or no consensus exists about Efficacy8,57
Rotational or turning therapy
Routine use of turning or rotational therapy, either by ‘kinetic’ therapy or by continuous lateral rotational therapy
Systemic antimicrobial agent prophylaxis
Routine administration of systemic antimicrobial agent(s) to prevent pneumonia in those receiving mechanically-assisted ventilation. Changes in the antimicrobial agents class used for empiric therapy
Oral chlorhexidine
rinse for oropharyngeal colonization
Routine use of an oral chlorhexidine rinse for the prevention of healthcare-associated pneumonia in all postoperative or critically ill patients and/or other patients at high risk for pneumonia.
Ventilator breathing circuits with HMEs
No recommendation can be made for the preferential use of HMEs to prevent pneumonia in patients receiving mechanically assisted ventilation No recommendation can be made for placing a filter or trap at the distal end of the expiratory-phase tubing of the breathing circuit to collect condensate
Suctioning of respiratory tract secretions
No recommendation can be made for the preferential use of either the multiuse closed-system suction catheter or the single-use open-system suction catheter
Prevention of aspiration associated with enteral feeding
Small-bore tubes for enteral feeding Enteral feedings continuously or intermittently should be given
Patient care with tracheostomy
Daily application of topical antimicrobial agent at the tracheostoma
Gloving
Wearing sterile rather than clean gloves when performing endotracheal suctioning
STRATEGIES FOR VAP PREVENTION
There are multiple recommended measures for prevention of VAP. Practices for which insufficient evidence or no consensus exists about efficacy are summarized in Table2. Preventive VAP strategies can be grouped into two classes: non-pharmacologic strategies, which are focused on preventing aspiration, and pharmacologic strategies, which are aimed at preventing colonization.
Non-Pharmacologic Strategies
Staff Education in the Intensive Care Unit
Various barriers to adhering to VAP prevention recommendations include disagreement with the reported results of source studies, resource paucity, elevated costs, inconvenience for nurses, fear of potential adverse effects and patient discomfort. There is considerable variability in practice between countries regarding humidification systems, intubation route, endotracheal suction system, kinetic therapy beds, subglottic secretion drainage and body position. For efficient patient care staffing must be sufficient while ensuring that staff is able to comply with essential infection control practices and other prevention strategies.17,28
Hand Hygiene
Microorganisms can be spread easily from patient to patient on the hands of healthcare workers. Moreover, wrist watches, rings, bangles and other jewelry commonly act as reservoirs for organisms, and impede effective hand cleaning. Moreover, healthcare workers compliance to hand hygiene is low, and high workload decreases their compliance.29
Impact of patient position
Patients positioned semi-recumbently 45 degrees have significantly lower incidence of clinically diagnosed VAP compared to patients positioned supinely.30 Moreover, the incidence of clinically diagnosed VAP among patients positioned prone, does not differ significantly from the incidence of clinically diagnosed VAP among patients positioned supine.31,32
Kinetic Beds
Critical patients often for a long time remain immobile in the supine position so the functional residual capacity is decreased because of alveolar closure in dependent lung zones and impaired mucociliary clearance. This leads to the accumulation of mucus, atelectasis onset and ensuing infection.33 Rotational therapy uses a special bed designed to turn continuously, or nearly continuously, the patient from side to side; specific designs include kinetic therapy and continuous lateral rotation therapy (CLRT).34,35
Artificial Airway Management
Oral vs Nasal Intubation: Both nasogastric and nasotracheal tubes can cause oropharyngeal colonization and nosocomial sinusitis. Thus, use of the oral route for both endotracheal and gastric intubation should be considered to decrease the risk of VAP.36
Endotracheal tube cuff pressure: The secretions that pool above inflated endotracheal tube cuffs may be a source of aspirated material and ensuing VAP. The pressure of the endotracheal tube cuff should be optimized in order to prevent the leakage of colonized subglottic secretions into the lower airways. Persistent pressures into the tube cuff below 20 cm H2O have been associated with the development of VAP.37
Silver-Coated Endotracheal Tubes: Silver-coated endotracheal tubes appear to be safe, reduces bacterial biofilm formation, has bactericidal activity, reduces bacterial burden and can delay airway colonization. However, further studies are needed to for determing its efficacy.38,39
Mechanical Ventilation Management
Ventilator Circuit Change: The CDCs recommendation was ‘do not change routinely, on basis of duration of use, the breathing circuit that is in use on an individual patient. Change the circuit when it is visibly soiled or mechanically malfunctioning.40
Humidification With Heat and Moisture Exchangers: The effect of HME in preventing VAP is still controversial and recent studies have failed to show a significant difference in rates of infection.41
Subglottic secretion drainage: Intermittent subglottic secretions drainage using inspiratory pause during mechanical ventilation results in a significant reduction in VAP.42 SSD reduces VAP in patients ventilated for >72 hours and should be considered with other recommended strategies such as semi-recumbent positioning.43
Pharmacologic Strategies
Modulation of Oropharyngeal Colonization
Policies encouraging routine tropical oral decontamination with chlorhexidine for patients merit reevaluation. It is a cheap measure, but whether is it a safe one − it does not select resistant microorganisms − remains to be investigated.8,44
Selective Decontamination of the Digestive Tract
Selective decontamination of the digestive tract (SDD) is the decontamination ofpotentially pathogenic microorganisms living in the mouth and stomach, whilst preserving the indigenous anaerobic flora. SDD is an effective and safe preventive measure in ICUs where incidence rates of MRSA and VRE are low, but in ICUs with high rates of multi-resistant microorganisms it is a measure that is effective but not safe.45,46
Stress Ulcer Prophylaxis
Patients at risk from important gastrointestinal bleeding (shock, respiratory failure requiring mechanical ventilation or coagulopathy) should receive H2 antagonists such as ranitidine rather than sucralfate.47
Ventilator sedation protocol
In patients receiving mechanical ventilation and requiring sedative infusions with midazolam or propofol, the use of a nurse-implemented sedation protocol decreases the rate of VAP and the duration of mechanical ventilation.48 An objective assessment-based Analgesia-Delirium-Sedation (ADS) protocol without daily interruption of medication infusion decreases ventilator days and hospital length of stay in critically ill trauma patients.49
Antibiotic Policy and Infection Control
Rational antibiotic policy is a key issue for better patient care and preventing antimicrobial resistance.50,51 Infection control programs like using a scheduled switch of antibiotic class have demonstrated efficacy in reducing nosocomial infection rates and restraining multidrug resistant (MDR) microorganism emergence.52
VAP prevention in low resource/developing countries
Though the incidence of VAP has declined in the developed countries, it continues to be unacceptably high in the developing world. Its incidence in these countries is 20 times that in the developed nations with significant morbidity, mortality, and increase in ICU length of stay, which may represent an additional burden on the scarce resources in developing countries.53 Insufficient preventive strategies and probably inappropriate antibiotics administration may have lead to this scenario. Since microbiology and resistance pattern in India is different from other countries, there is need for data from our country to choose appropriate antimicrobials for management.54 Simple and effective preventive measures can be instituted easily and at minimal costs. Such measures might include hand hygiene, diligent respiratory care, elevation of head, oral and not nasal cannulation, minimization of sedation, institution of weaning protocols, judicious antibiotics use, de-escalation, and leveraging PK/PD characteristics for antibiotics administered. More costly interventions should be reserved for appropriate situations. Strategies to prevent VAP, probably by emphasis on practical, low-cost, low technology, easily implemented measures is need of the hour.
Ventilator-associated events (VAE) surveillance: an objective patient safety opportunity
Surveillance for ventilator-associated pneumonia is challenging and contains many subjective elements, including the use of chest x-ray evidence of pneumonia. In January 2013, CDC convened a VAP Surveillance Definition Working Group which transitioned VAP surveillance to ventilator-associated event (VAE) surveillance in adult inpatient settings.55 The VAE algorithm—which is a surveillance algorithm and not intended for use in the clinical management of patients—consists of 3 tiers of definitions: Tier 1, Ventilator-Associated Conditions (VAC); Tier 2, Infection -related Ventilator-Associated Complications (IVAC); and Tier 3, Possible and Probable VAP.27 The tier 1, VAC attempts to identify sustained respiratory deterioration episodes, and capture both infectious and noninfectious conditions and complications occurring in patients receiving mechanical ventilation. The tier 2, IVAC, is intended to identify the subset of VACs that are potentially related to pulmonary and extra pulmonary infections of sufficient severity to trigger respiratory deterioration. The tier 3, possible and probable VAP, attempts to identify IVAC patient subsets with respiratory infections as manifested by objective evidence of purulent respiratory secretions (where purulence is defined by using quantitative or semi-quantitative criteria for the number of neutrophils on Gram stain) and/or positive results of microbiological tests done on respiratory specimens. Because of the wide range of the lower respiratory tract specimens, their collection procedure as well as in laboratory processing and reporting of results, the Working Group of CDC determined that it was not appropriate to include these data elements in the VAC and IVAC definitions.56
This 3 tier approach is ineffective to accurately identify VAP for surveillance purposes and focuses on more mechanical ventilation complications. This approach may also reduce the likelihood of manipulation that could artificially lower event rates. Most VAEs are caused by pneumonia, pulmonary edema, atelectasis, or acute respiratory distress syndrome. In few recent studies concordance between the VAE algorithm and VAP was found to be poor.57 Thus, more studies are needed to further validate VAE surveillance compared with conventional VAP by using strong microbiologic criteria, particularly bronchoalveolar lavage with a protected specimen brush for diagnosing VAP and to better characterize the clinical entities underlying VAE.
Bundle approach to prevention of VAP
One of the five goals of the ‘Saving 100,000 Lives’ campaign, launched by the Institute for Healthcare Improvement is to prevent VAP and deaths associated with it by implementing a set of interventions for better patient care known as the ‘ventilator bundle’. The interventions should have scientific support of effectiveness, based on randomized controlled trials. All the elements of the bundles must be executed at the same time. The bundles for VAP includes four components: (a) elevation of the head end of the bed to 30-45º, (b) daily interruption of sedation, (c) daily assessment of readiness to extubate and (d) prophylaxis for deep venous thrombosis and peptic ulcer disease. The bundle approach to prevention of VAP has been found to be highly effective in reducing the incidence, mortality and ICU stay.5,58,59 The ventilator bundle should be modified and expanded to include specific processes of care that have been definitively demonstrated to be effective in VAP reduction. A multidimensional framework with a long-lasting program can successfully increase compliance with preventive measures directly dependent on healthcare workers bedside performance.
CONCLUSION
Ventilator Associated Pneumonia is one of the most common nosocomial infections in ICU presenting with non specific symptoms and clinical signs. Quantitative culture obtained by different methods, including EA, BAL, pBAL, PSB or TBA seem to be rather equivalent in diagnosing VAP. Clinical criteria used in combination, may be useful in VAP diagnosis; however, inter-observer variability and the moderate performance are to be considered.
Preventive strategies should focus on better secretion management and on reduction in bacterial colonization. Further research on targeted interventions is needed to effectively reduce VAP incidence. For VAP an approach based on multidisciplinary group is required including setting preventive benchmarks, establishing goals and time lines and providing appropriate education and training, audits and feedback to the staff, while continually updating themselves based on relevant clinical and preventive strategies.
As syphilis is a notable clinical and pathological imitator, its diagnosis remains challenging. Physicians should be vigilant to suspect syphilis in cases of non-specific signs, such as lymphadenopathies, even in patients with no apparent risk for sexually transmitted infections or a history of primary syphilis.
Case Report
We report the case of a seventy-year old woman with a medical history of arterial hypertension. She had neither smoked cigarettes nor drunk alcohol and she had no significant medical family history. The patient presented with a history of swelling in the left axilla of one year duration. The swelling gradually increased in size and was painless. There was a history of occasional low-grade fever and weight loss, but no cough or night sweats.
On initial examination, the patient was thin with generalised lymphadenopathy: she had an axillary adenopathy that measured 4 cm in diameter in the right axilla and one measuring 3 cm in the left axilla. She also had two cervical lymph nodes that were less significant, and one enlarged right inguinal lymph node of about 3 cm in diameter. The existing lymph nodes were painless, mobile, mildly tender and smooth. Otherwise, breasts, limbs and other regions were essentially normal. No skin rash or suspect lesions were noticed. All her family members were well, with no contributory medical history, and none of them had similar symptoms.
A complete blood count revealed a white blood cell count of 5300/l (neutrophils 40%, eosinophils 19%, lymphocytes 30%, monocytes 10%), and a C-reactive protein of 14 mg/l. The remaining results of her full blood count, electrolytes, liver enzymes, lactate dehydrogenase and urine analysis were within normal limits. Calcium and phosphate levels were normal in both blood and urine analyses. Both human immunodeficiency virus screening and the serological tests for hepatitis B and C were negative. Mantoux test did not show any indurations. Smear and culture of the sputum were negative. Her chest x-ray and abdominal ultrasound were normal.
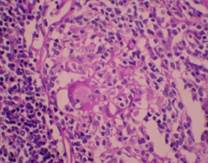
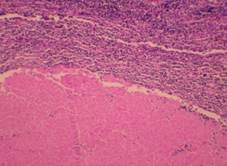
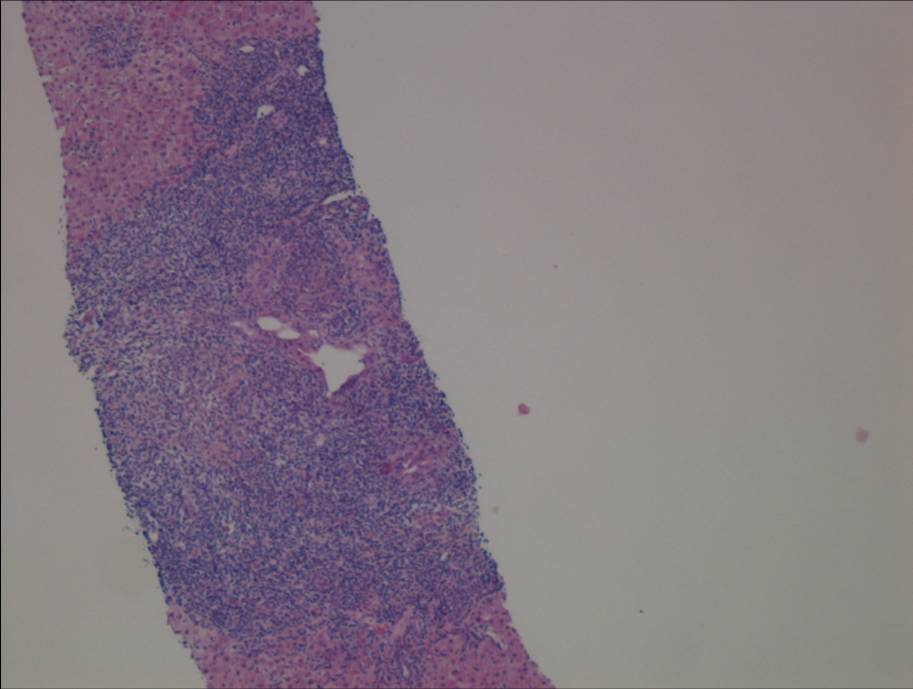
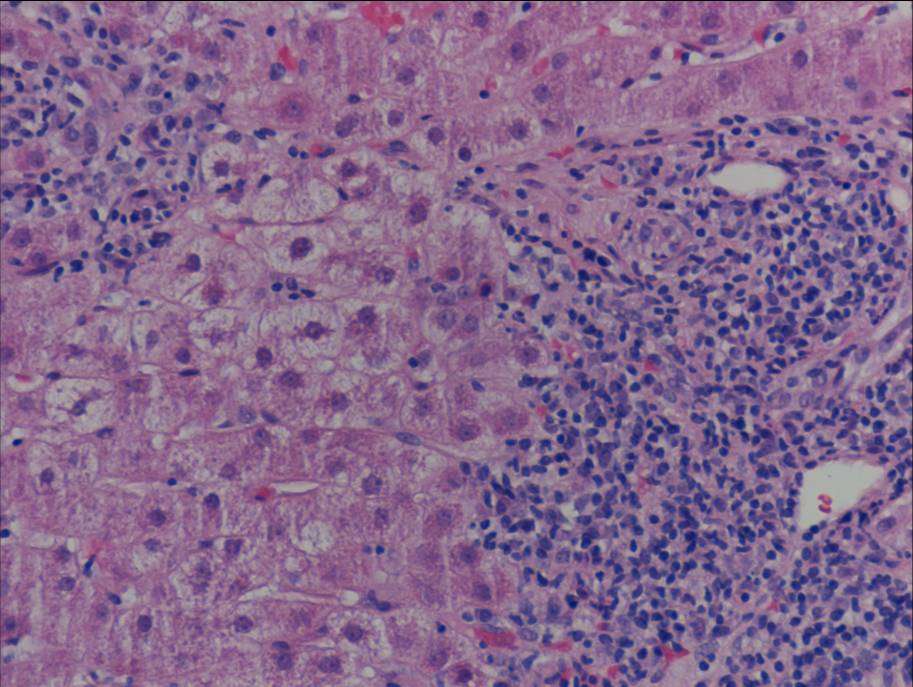
A CT scan of the patient’s neck and chest showed a marked anterior mediastinal mass of about 50 mm diameter with multiple calcifications. Several small lymph nodes were also noticed in the cervical and axillary areas. An axillary lymph node biopsy was performed. Histopathological examination of the biopsy specimen revealed a granulomatous lesion with epithelioid and multinucleated giant cells (Fig.1) associated with calcifications and central areas of caseous necrosis (Fig.2), which were highly suggestive of tuberculosis.
Fig 1: Epithelioid granuloma with giant cell
Fig 2: Eosinophilic granuloma with acellular caseous necrosis
According to these clinical and pathological findings, the most common granulomatous diseases are mycobacterial diseases such as tuberculosis, hence why the diagnosis of tuberculous lymphadenitis was highly suspected, and the patient was given anti-TB drugs. However, other differential diagnoses were considered, including bacterial infections like syphilis or actinomycosis, protozoal infections such as toxoplasmosis, and miscellaneous diseases such as sarcoidosis, Crohn's disease and Wegener's granulomatosis. To distinguish disease processes and make a definitive diagnosis, further investigations, such as special stains, culture methods and serologic tests, were indicated.
Additional histological stains, including Ziehl-Nielsen, were performed and returned negative, excluding the diagnosis of tuberculosis. In the meantime, the serological tests showed a positive venereal disease research laboratory test (VDRL: 1/8) and Treponema Pallidum haemagglutination assay (TPHA: 1/350). As a result, the diagnosis of secondary syphilis was confirmed and tuberculosis treatment was ceased.
The patient received intramuscular injections of 2.4 million units of benzathine penicillin every three weeks. Additional clinical and laboratory examinations were performed for both the patient and her family. She did not present with any manifestations of cardiovascular or neurological syphilis. Her husband’s VDRL and TPHA tests were negative. After a nine-month follow-up, the patient had no clinical or laboratory evidence of syphilis.
Discussion
Syphilis is predominantly a sexually-transmitted disease with both local and systemic manifestations. The causative organism is the spirochete Treponema Pallidum (TP) which was first demonstrated on the 17th of May 1905 1.
Syphilis has many non-specific signs and symptoms that may be overlooked by the physician, because in some cases it may simply be indistinguishable from other more common diseases. In fact, syphilis can share clinical manifestations with other treponemal and non-treponemal diseases, and it may be asymptomatic in some stages. Unfortunately, undiagnosed and untreated syphilis may lead to life-threatening complications such as hepatitis, stroke and neurological damage 2. Therefore its clinical diagnosis must be supported by laboratory tests.
Several older methods can be used to confirm syphilis diagnosis such as direct identification of TP by dark-field microscopy or direct fluorescent antibody tests, but such tests are not practical in a routine clinical setting and these methods can only be performed on lesion exudate or tissue 3.
As a consequence, the diagnosis in most patients is based on serological tests. Guidelines from the United States of America (USA) and Europe recommend a combination of two tests: the first one is a non treponemal (cardiolipin, reaginic) test, essentially Venereal Disease Research Laboratory (VDRL) or rapid plasma reagin (RPR); and the second is a treponemal test, essentially TP haemagglutination assay (TPHA), TP particle agglutination, or the fluorescent treponemal antibody absorption (FTA-abs) test 3,4.
In our patient, the most significant clinical finding was lymphadenopathy. This case presented diagnostic difficulties because of its clinical and histopathological resemblance to other pathological conditions. In fact, the presence of generalised lymphadenopathy and the finding of granulomatous lesions with epithelioid cells in the biopsy were highly suggestive of tuberculosis. As a matter of fact, tuberculosis tops the list of aetiological causes of granulomatous infections5. Worldwide it is considered the leading cause of contagious disease leading to approximately 1.4 million deaths per year 6. Its prevalence is still extremely high in certain populations especially in low-and middle-income countries such as Tunisia where the disease is endemic.
Tuberculosis is caused by Mycobacterium tuberculosis (M. tuberculosis) and M. bovis, an acid and alcohol fast organism 7,8. Histopathology is characterized by the presence of epitheloid granuloma with Langerhans giant cells and central caseous necrosis 7.
Lymphadenitis is the most common extra-pulmonary manifestation of tuberculosis but its diagnosis is difficult, often requiring biopsy. In such granulomatous disease, and in cases of persisting doubts, it is necessary to identify the specific etiological agent by further investigations such as special stains, culture methods and molecular techniques like polymerase chain reaction (PCR) and serological tests, as in the case of syphilis.
In the case of tuberculosis infection, demonstration of the mycobacteria can be done with Ziehl-Neelsen staining or by immunofluorescence using auramine-rhodamine. Mycobacterial culture and detection of mycobacterial DNA using PCR are also used 7,9. Since the growth of mycobacterium in culture requires a long time, additional histological stain with Ziehl-Nielsen was performed, but returned negative in the case of our patient. As a consequence, the diagnosis of tuberculosis was excluded and syphilis was considered as a definitive diagnosis.
Conclusion
Granulomatous lesions can be seen in numerous diseases. A definitive diagnosis cannot be made on the basis of the history and physical examination alone, confirmatory testing should be performed in order to identify the specific etiologic agent correctly. Diagnosis of the disease in the initial stages would be beneficial not only to allow the patients to receive early treatment, but also to prevent the spread of the disease to others.
Poetry is a way of expressing the subjective experiences that spill over the rational mind and it permits spontaneous overflow of subjective feelings. The ability to express oneself through poetry, and share that experience, is one of the unique human experiences that distinguish us from lower biological forms. The strife and struggle of modern men have made them miserable wretches on the face of this beautiful cosmos, and the technological revolution has taken the poetic sense from them; a time old coping mechanism. Those not capable of expressing their own sorrows and joys of everyday life in poetic words could find a surrogate writer in The Gushing Fountain.
In his collection of poetry, Dr Latoo (who is currently working as a Consultant Psychiatrist in United Kingdom) has catered poems for every mood and occasion: love, parting and sorrow, inspiration, rapture, memory, nature, solitude, and contemplation. Some of them are deeply personal and the author is trying to unearth a time capsule he had left in his native country of Kashmir. Dr Latoo appears to be searching for inner truths and making a self exploratory pilgrimage in his collection of poetry. Poetry has the power to describe and dramatize one’s own life, and Dr Latoo has done it well. The themes generally move from childhood to old age, love to grief, sorrow to joyfulness, aggressive nationalism to corrupted politicians, and depression to psychosis. There are pearls of mystical wisdom embedded in the poetry:
“Be choreographed by a great master for our sustenance Rather than just be a part of random unplanned accident?”
There are wise statements in “Divine Justice”:
“Anything like fatalism shall be a contradiction Of the Divine justice, free will and Lord’s will.”
All poetries have some hidden messages, and the book as a whole stands for immense moral values. “Woman” stands for women’s rights and dignity. The thoughts about the forgotten orphans are heart touching. “Behold a Man - Judging others” points towards the fallacy of judging other people without correcting oneself. Mental health professionals are particularly prone to this error because they are often professionally bound to assess their clients; we are only supposed to assess others and not judge others. We should not even judge ourselves, but only do self-assessment - God is the only Judge. The author writes about very ordinary humble human beings like the barber, Rupa, Ayesha, Ahmed, Puja etc. “Marriage” highlights the sanctity of wedlock. These poetries reflect the world view of the author. “Hold fast to thy dreams” may be inspired by Langston Hughes (1902 - 1967) and reminded me of my father who liked the verses of Hughes on dreams. “A raven who wants to be a dove” refers to people who pretend to be what they are not - wearing borrowed garments.
There are also poems about the author’s travelling experiences. A century ago, if a poet wrote about airport, he would have been frowned upon by the peer group, but in the 21st century it is appropriate to write such poetry. “Noisy airport and my mind” illustrates the hustle and bustle of contemporary life and gives the book a modern flavour. “By the Dal Lake” is nostalgic and the author is trying to recapture and share his lost Kashmiri literary Empire with the readers. Born in Kashmir, there is no surprise that the author renders beautiful nature in his poems. One wonders, if William Wordsworth were born in Kashmir, what would have been the content of his writings. Dr Latoo’s dual identity is evident when he writes about Kashmir and London.
In these days of global union through mere technology, poetry may have a serious role in the “international soul-union.” The days of regional poetry are over. Poets like Dr Latoo may be able to contribute to the formation of a healthier global village; poetry penetrates beyond the psychic realm into the spiritual dimension. There is a mission of peace and love in the Gushing Fountain, and the author is not enforcing any strong convictions on the readers. There is a poet-philosopher in the author of the Gushing Fountain.
The author has used rhyming and free verse styles of poetry. Metaphors and similes are appropriately embedded in various situations:
“A smile on our face blooms the gardens of her innocent soul A tear in our eyes arises from the blood of her bruised heart.” (From the poem, “Mother”)
Lyrical poetries are ravishingly harmonious and there are no repetitions. The thoughts are clear and there is an exotic element in all the poetry. On the whole, all the poems are cerebral and riveting. The works are relevant to the present century and can be appreciated by scholar and casual readers alike. Every poem is an experience to be savoured and memorised. Let these pieces of poetry echo and reverberate not only in the conflict-ridden valleys of Kashmir, but all around the world until they find rest in the minds of the waiting millions.
Psychiatry is going through an identity crisis because the newer medications are not as effective as expected to be and clinicians are turning to different forms of psychotherapy. Poetry/lyric therapy could be another form of psychotherapy that needs attention in the field of soft psychiatry. Dr Latoo’s book could be an inspiration and encouragement in this line of treatment. Hypnotherapists readily recognize that words are like loaded bullets and are highly potent. To an extent, poetry therapy involves the principles of both hetero- and self- hypnotherapy. Primitive and modern religions take advantage of the potentials of different forms of poetry in religious rituals for healing and promoting health.
A study of the mechanism of poetry writing is helpful in developing better conceptual models of creativity and deeper understanding of mental process. Sudden flashes of creative insight and other intuitive leaps, which arise from states of mind through intermediate steps that remain hidden beneath consciousness, and such ultrafast processing involving a concealed intermediate step, is consistent with quantum computations. A poet who enjoys superior mental health is capable of swinging from the unconscious quantum logic to the classical logic of consensus consciousness with an ultrafast speed. In psychotic states, “the quantum gates” do not shut swiftly as in normal mental states and the sufferers get trapped in the quantum logic. The usefulness of poetry therapy in psychotic patients, who get stuck in the quantum logic of the unconscious mind back to the classical logic of ordinary consciousness, needs further analytical studies. The primary aetiology of psychotic disorders may be biological, but secondary symptoms are quantum-linked and the new generation of psychotherapists have to learn the quantum meta-languages to communicate with psychotic and depressed patients. Poetry is such a source of quantum meta-language.
Poetry therapy promotes abstract thinking and develops imaginative powers. It is also a means of relieving and revealing innermost sentiments; it helps to ventilate overpowering emotions and hidden tensions. It is a form of self-expression and aids to build greater self-esteem; useful in strengthening interpersonal skills and communication skills. It would be valuable in repairing the assault of psychosis on the personalities of the sufferers. Quoting from my own memory lane, I became interested in poetry therapy when I comprehended the core problem of a patient who wrote:
“Moon, you shine at the centre of the sky, Catching attention from all over the world, Don’t you know that I am lonely?”
Poetry is of the heart and imagination whereas science is about reason and logic and may be grounded on contradictory principles. If science is about objectivity, poetry is essentially about subjectivity and to blend those human experiences harmoniously is a hard task; Dr Latoo has successfully achieved this goal. A man of science, when he writes poetry, has to liberate himself from the shackles of rationalism so that he can be a wholly free human: to be a poet one has to be a natural human being. To quote from Jean-Jacques Rousseau: “Man is born free and everywhere he is in chains.” Let us hope that the Gushing Fountain will have a part two and even more!
A 19 year old male presented with a history of recurrent respiratory tract infections and progressive diminution of vision. Fundoscopy was performed and showed the changes in image below.
What is the finding suggestive of?
1. Retinitis pigmentosa
2. Drug toxicity
3. Congenital rubella
4. Syphilis
Answer: Retinitis Pigmentosa
Retinitis pigmentosa (RP) is a bilateral inherited progressive retinal degeneration presenting in the first to second decades of life.1 The inheritance can be autosomal dominant, autosomal recessive or X-linked recessive. Hallmark symptoms of RP are nightblindness and visual field constriction. Fundus changes in retinitis pigmentosa include waxy pallor of optic disc (black arrow), arteriolar attenuation (white arrow head) and bony spicule pigmentation (white arrow) in the mid-peripheral fundus, which is predominantly populated by rods. Vessel attenuation is the earliest feature seen clinically. Although intraretinal pigmentary migration is relatively easy to observe, it requires years to develop, so early RP may only exhibit vessel attenuation without pigmentation (previously known as RP sine pigmento). Prognosis is variable and tends to be associated with the mode of inheritance.
Drug toxicity with chloroquine can result in visual disturbances. History of drug usage prior to vision disturbance can be present. Fundus examination shows a subtle bulls eye macular lesion characterized by a central foveolar island of pigment surrounded by a depigmented zone of RPE atrophy, which is itself encircled by a hyperpigmented ring.2 In congenital rubella, a history of maternal infection will be present. Fundus findings include salt and pepper pigmentary disturbance involving the periphery and posterior pole with normal vessels, RPE mottling and no intraretinal pigmentary migration. Syphilitic retinopathy may have sectorial or generalised pigmentation.3 The onset can be from adulthood to old age. History of genital ulcer may be present.
Sertraline is selective serotonin reuptake inhibitor (SSRI). It is a commonly prescribed antidepressant. The common side effects of SSRI’s are nausea, vomiting, diarrhoea, dyspepsia, anorexia and weight loss.
To our knowledge this is the only second reported case of sertraline-induced hyperpigmentation. It is interesting to note that in some cases sertraline has been used as replacement medication following antidepressant induced hyperpigmentation. So it is important that both clinicians and patients are aware of this potential rare side effect of sertraline.
Case Report:
In this case report we present a 27 years old Caucasian lady that developed hyper pigmentation, after starting sertraline.
The patient, a 27 years old lady was diagnosed with Bipolar Affective Disorder (ICD-10)2 years ago. She was prescribed sertraline 50mg for low mood. Her current medications also include semi sodium valproate 1000 mg orally daily, quetiapine modified release 400 mg orally daily, tramadol 50mg orally twice a day and co-codomol orally on an as required basis for back pain. She was not prescribed any depot medications. To our knowledge she was compliant with her medication.
She responded well but reported that she had developed hyperpigmentation after four weeks. This persisted after suffering a recurrence of low mood and being seen in clinic 5 months later.
There is no significant past medical or family history. She has been on various psychotropic medications in the past including fluoxetine, venlafaxine, olanzapine and procyclidine.
Physical examination revealed focal hyperpigmentation limited to the upper lip. It was dark brown in color with sharply defined outline and was not associated with itching, redness, rash or excoriation. It was gradually getting darker in color and she had to wear a lot of make up to conceal it. The patient was referred to a consultant dermatologist for an opinion but unfortunately she did not attend her appointment. This has been acknowledged as a limitation of our case report. Routine blood tests were within the normal range. She also reported some weight gain with sertraline.
She did not report any previous history of dermatological disorders or any endocrine conditions and Addison's disease was excluded. She did not begin any new medication or vaccines prior to onset of the hyperpigmentation and denied ever having chlorpromazine, tricyclics, tetracyclines, amiodarone, hormone replacement therapy, aspirin, chemotherapy or minocycline. However three years ago, she had taken anti malarial medication before going to the Dominican Republic. She also denied any intake of herbal medication, non-prescribed medication or illicit drugs.
She also denied excessive exposure to sunlight during the time of development of hyperpigmentation and she was not pregnant. There is no history of heavy metal exposure.
The probability of adverse drug reaction assessed by using Naranjo Scale indicated a probable association between the use of sertraline and hyperpigmentation. Subsequently her sertraline was stopped and replaced by duloxetine 30mg daily. Unfortunately the hyperpigmentation persisted after three off sertraline but is no longer worsening.
Discussion:
Bipolar Affective Disorder also known as bipolar disorder, manic-depressive disorder, or manic depression is characterised by two or more episodes in which patients mood and functionality is significantly disturbed, this disturbance on some occasions includes episodes of mania or hypomania with elevated mood and increased energy levels and on others episodes of depression with low mood, tiredness and diminished pleasure in activities. Recovery is usually complete between these episodes. 1
The pharmacological treatment of bipolar affective disorder depends on nature and degree of presenting episode and includes mood stabilisers like lithium, valproate, carbamazepine and lamotrigine, anti psychotics like olanzapine, quetiapine, aripiprazole and risperidone and antidepressants like sertraline, citalopram and venlafaxine.
Sertraline, citalopram, escitalopram, fluoxetine, fluvoxamine and paroxetine selectively inhibits reuptake of serotonin, hence named selective serotonin reuptake inhibitor (SSRI).
In our case the patient was on semi sodium valproate and modified release quetiapine and was later prescribed sertraline to help with low mood.
A literature review of English language using PubMed database was done on 15th June 2013. The terms searched were “sertraline”, “serotonin reuptake inhibitor”, “SSRI”, “anti depressants”, “hyperpigmentation”, “pigmentation”, and it found case reports of antidepressant associated hyperpigmentation with citalopram2, mirtazapine3 and imipramine.4, 5,6,7 It is interesting to note that in some of the case reports the antidepressants were replaced by sertraline after development of hyperpigmentation, but there was no record as to whether the lesion resolved.2, 3,4
Only one previous case of sertraline-induced hyperpigmentation was found8,which also unfortunately persisted after discontinuation of the antidepressant.
As hyperpigmentation has also been reported with other SSRIs, clinicians should be more aware that hyperpigmentation might be related to the class effect, rather than the individual drugs.
Though the exact biological mechanism for the development of hyperpigmentation is not clear and further research is needed, the secretion of melanocyte stimulating hormone (a-MSH) is closely associated with skin pigmentation, and serotonin and dopamine transmitters appear to be involved which may point to a possible mechanism for the hyperpigmentation.
Insomnia is chronic inability to obtain the amount of sleep needed for optimal functioning and well-being. Insomnia has received much attention in last few decades, since it has become a growing and complex problem in our society.1 Insomnia is defined as the chronic complaint of difficulty initiating or maintaining sleep, early awakening, and interrupting or non-restorative sleep. Furthermore, it must be accompanied by clinically significant impairment in day time function, for which there is no identifiable cause such as another sleep, psychiatric or medical disorder.1
General Criteria for Insomnia:2
A complaint of difficulty initiating sleep, difficulty maintaining sleep, or waking up too early or sleep that is non-restorative or poor in quality. In children, the sleep difficulty is often reported by the caretaker and may consist of observed bedtime resistance or inability to sleep inadequately.
The above sleep difficulty occurs despite adequate opportunity and circumstances for sleep.
At least one of the following forms of daytime impairment related to the night-time sleep difficulty is reported by the patient:
Fatigue or malaise
Attention, concentration or memory impairment
Social or vocational dysfunction or poor school performance
Mood disturbance or irritability
Daytime sleepiness
Motivation, energy or initiative reduction
Proneness for errors, or accidents at work or while driving
Tension, headaches or GI symptoms in response to sleep loss
Concerns or worries about sleep
Insomnia is prevalent condition in both the general population and in clinical practice, and it is associated with significant morbidity and mortality. It may present as the primary complaint or in association with physical or mental health problem.
Classification:
Insomnia can be classified into two main etiologic groups:
Primary Insomnia: When identifiable etiologies for insomnia have been ruled out, a diagnosis of primary insomnia can be made.
Secondary Insomnia: Related to other medical disorders, mental disorders or related to known organic factors.
Insomnia can be divided in to three types based on duration:
Less than one month called Acute or Transient insomnia.
One to six months called Sub-acute or Short-term insomnia.
More than six months called Chronic insomnia.
Following types of Insomnia recognized in The International Classification of Sleep Disorders (ICSD) second edition, Diagnostic and Coding manual:2
Adjustment Insomnia (Acute Insomnia)
Psycho-physiological Insomnia
Paradoxical Insomnia
Idiopathic Insomnia
Insomnia Due to Mental Disorder
Inadequate Sleep Hygiene
Behavioural Insomnia of Childhood
Insomnia Due to Drug or Substance
Insomnia Due to Medical Condition
Insomnia Not Due to Substance or Known Physiological Condition, Unspecified (Nonorganic Insomnia, NOS)
Physiological (Organic) Insomnia, Unspecified
Prevalence:
One third of adult population reports insomnia, 9 to 12% experience day time consequences and approximately 6% meet formal criteria for an insomnia diagnosis.3 Insomnia is more common among women, middle-aged and increases with age, shift workers and with medical or psychiatric disorders.
Consequences:
Persistent insomnia can produce an important burden for individual and society, as evidenced by reduced quality of life, impaired daytime functioning and increased absenteeism at work, and higher health-care cost. Persistent insomnia is also associated with increased risks of depression and chronic use of hypnotics.
Diagnosis of insomnia is based on subjective complaint of difficulties falling or staying asleep or non-restorative sleep that is associated with marked distress or significant daytime impairments. Several indicators such as intensity, frequency and duration, needs to be evaluated to assess severity of insomnia.
Evaluation:
Insomnia is an important public-health problem that requires accurate diagnosis and effective treatment (Standard).4 Insomnia is a symptom of an underlying disorder or condition. The insomnia may be a problem directly related to the sleep-wake regulatory system and/or it might be associated with a comorbid psychiatric, behavioural, medical, or neurological condition.4 Insomnia is primarily diagnosed by clinical evaluation through a careful, detailed medical, psychiatric, and thorough sleep history (which includes assessment of sleep patterns and waking processes) (Standard).4
Treatment options:
Pharmacotherapy is currently the most common treatment modality for insomnia,5 but long-term use of hypnotics in chronic insomnia can become complicated by drug tolerance, dependence or rebound insomnia. Since insomnia is a chronic condition, long-term and safe treatments are warranted. Non-pharmacological options provide longer lasting benefits.
If a cause of insomnia is identified, initial treatment should be directed at the specific factor. If insomnia persists, non-pharmacologic and/or pharmacologic interventions should be instituted. Hypnotic agents are the treatment of choice for the management of acute or transient insomnia. The expected goal is to normalize the sleep pattern within a few days to weeks. Behavioural interventions are important aspect of the treatment of chronic primary insomnia.
Classification of evidence (Table 1) is used to determine different level of recommendations (Table 2), which is available for behavioural therapies in management of insomnia.
Table 1: AASM (American Academy of Sleep Medicine) Classification of Evidence (Based on Sackett system,6 the criteria for grading evidence level of each study)
Randomized well-designed trials with low alpha and beta error (Grade I) Randomized trials with high alpha and beta error (Grade II) Non-randomized concurrently controlled studies (Grade III) Non-randomized historically controlled studies (Grade IV) Case series (Grade V)
(Alpha (Type I error) refers to the probability that the null hypothesis is rejected when in fact it is true (generally acceptable at 5% or less, or p<0.05). Beta (Type II error) refers to the probability that the null hypothesis is mistakenly accepted when in fact it is false (generally trials accept a beta error of 0.20). The estimation of Type II error is generally the result of a power analysis. The power analysis takes into account the variability and the effect size to determine if sample size is adequate to find a difference in means when it is present (Power generally acceptable at 80-90%).
Table 2: AASM Levels of Recommendations (The following are recommendations of the SPC (Standards of Practice Committee) approved by the Board of Directors of the AASM).7
Term
Definition
Standard
This is a generally accepted patient-care strategy, which reflects a high degree of clinical certainty. The term standard enerally implies the use of Level I evidence, which directly addresses the clinical issue, or overwhelming Level II evidence.
Guideline
This is a patient-care strategy, which reflects a moderate degree of clinical certainty. The term guideline implies the use of Level II evidence or a consensus of Level III evidence.
Option
This is patient-care strategy, which reflects uncertain clinical use. The term option implies either inconclusive or conflicting evidence or conflicting expert opinion.
Recommendations according to type of Insomnia:10, 11, 12
For both, chronic primary insomnia and secondary insomnia, the standard psychological and behavioural interventions are effective and recommended.
Recommendations for specific therapies:
1. Stimulus control therapy
Effective and recommended therapy in treatment of chronic insomnia (Standard)
Objective is to train the insomnia patient by a set of instructions designed to re-associate the bed and bedroom with sleep and to re-establish a consistent sleep-wake schedule:
Go to bed only when sleepy;
Get out of bed when unable to sleep;
Use the bed/bedroom for sleep only (no reading, watching TV etc.);
Arise at the same time every morning;
No napping.
2. Relaxation training
Effective and recommended therapy in treatment of chronic insomnia (Standard)
Aimed at reducing somatic tension (e.g. progressive muscle relaxation, autogenic training) or intrusive thoughts at bed time (e.g. imagery training, meditation) that interfere with sleep.
3. Cognitive Behavioural Therapy (CBT) with or without relaxation therapy
Effective and recommended therapy in treatment of chronic insomnia (Standard)
CBT includes various combinations of both cognitive as well as behavioural interventions. The cognitive component is aimed at changing patient's beliefs and attitudes about insomnia. The behavioural component may include therapies such as stimulus control therapy, sleep restriction or relaxation training. Sleep hygiene education is often also included.
4. Sleep Restriction
Effective and recommended therapy in chronic insomnia (Guideline)
It involves curtailing the amount of time in bed to actual amount of time spent asleep. For example, if a patient reports sleeping an average of 6 hours per night, out of 8 hours spend in bed, the initial recommended sleep window (from lights out to final arising time) would restrict to 6 hours. Periodic adjustments to this sleep window are made contingent upon sleep efficiency, until optimal sleep duration is reached. Therapy creating mild sleep deprivation, and then lengthening sleep time as sleep efficiency improves.
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
Combining stimulus control therapy, relaxation training, sleep hygiene education
Combining stimulus control therapy, sleep restriction therapy, sleep hygiene education
Combining sleep restriction therapy, stimulus control therapy
6. Paradoxical intention
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
It involves instructing the patient to remain passively awake and avoid any effort (i.e. intention) to fall asleep. The goal is to eliminate performance anxiety, as it may inhibit sleep onset. This parameter is limited to sleep initiation insomnia.
7. Biofeedback
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
It provides visual or auditory feedback to patients to help them control some physiological parameters (e.g. muscle tension) in order to seek reduction in somatic arousal.
EEG Neurofeedback training: It is a self-regulation method that makes use of learning theory, more specifically, the paradigm of operant conditioning.8 While the EEG is measured; the patient receives instant feedback (visual and/or auditory) on the cortical activity of the brain. The goal of this treatment modality is to normalize the functioning of the brain by inhibiting and/or reinforcing specific frequency bands.
Recommendations relevant to specific patient groups:
Psychological and behavioural interventions are effective and recommended in treatment of insomnia in older adults (Standard) and among chronic hypnotic users (Standard)
Insufficient evidence is available for sleep hygiene education, imagery therapy, and cognitive therapy to be an option as a single therapy. (No recommendation level)
Sleep Hygiene Education: Please see table 3
Table 3: Sleep Hygiene Education:
1. Attempt to maintain a regular sleep-wake cycle 2. Obtain morning light exposure 3. Use the bedroom only for sleep and intimacy 4. Create a comfortable, quiet, dark and temperature-controlled bedroom environment 5. Develop a relaxing routine within an hour before bedtime 6. Exercise regularly, but not within a few hours of bed time 7. Avoid use of alcohol and other addicting substances 8. Avoid caffeine or nicotine, especially within a few hours of bedtime 9. Avoid empty stomach or heavy meals before bed time, a light snack may be of value 10. Avoid daytime napping, or if napping, be aware of the impact that napping has on nighttime sleep 11. Avoid disturbances at bedtime (e.g. disruptive noises, pets, family) 12. Avoid work, computers and emotional stress in the bedroom 13. Avoid keeping a clock close to the bed to prevent “clock watching” 14. Avoid excessive wakeful time in bed (>20 minutes)
Imagery therapy: It involves a visualization technique to focus on some pleasant or neutral images to block out unwanted thoughts before sleep.
Cognitive therapy: Psychological methods aimed at challenging and changing misconceptions about sleep and faulty beliefs and attitudes about insomnia and its perceived daytime consequences.
Limitations of non-pharmacological management:
Gains in sleep onset or total sleep time are not immediately attained.
Patient motivation and encouragement are required for success of management.
Non-pharmacological interventions are more expensive and time-consuming.
They require the availability of a skilled therapist.
Results:
Psychological and behavioural therapies produce reliable changes in several sleep parameters of individuals with either primary insomnia or insomnia associated with medical and psychiatric disorders.10 A Meta-analysis indicates that in patients with primary insomnia, behavioural interventions produce improvements in sleep parameters (sleep onset latency, time awake after sleep onset (WASO), number of awakenings and total sleep time) in about 70 to 80% of patients.9 Behavioural interventions are more expensive, time-consuming and require the availability of a skilled therapist, but the benefits are long lasting.13
Clinical Pearl:
Pharmacotherapy is currently the most common treatment modality for insomnia,5 but long-term use of hypnotics in chronic insomnia can become complicated by drug tolerance, dependence or rebound insomnia.
Psychological and behavioural therapies produce reliable changes in several sleep parameters of individuals with either primary insomnia or insomnia associated with medical and psychiatric disorders.
Behavioural interventions are important aspect of the treatment of chronic primary insomnia; they should be used in every patient of Insomnia.
Sleep is a fundamental part of our lives and about one-third of it is spent sleeping. Sleep deprivation has been linked with such high profile public disasters, as Chernobyl, the Challenger shuttle disaster and the nuclear meltdown at Three Mile Island. According to the US Highway Traffic Safety Administration, approx. 100,000 motor vehicle accidents are the result of driver’s drowsiness and fatigue1. There is an association of sleep disorders with anxiety and depression which may be bidirectional. Patients with insomnia for 2 weeks or longer, without current depression are at increased risk of developing major depression. Both insomnia and hypersomnia are considered independent predictors of depression and anxiety2.
Key Milestones in the Development of American Sleep Medicine:
The history of treatment of sleep disorders dates back to at least the use of opium as a hypnotic reported in ancient Egyptian text. Sleep medicine, however did not emerge as a distinct discipline until the 1970’s. Drs. Kleitman and Dement were significant early contributors to this field in the United States. In 1957 they first described Non Rapid Eye Movement (NREM) sleep and Rapid Eye Movement (REM) sleep and proposed the 4 stages of NREM sleep. In 1972 Dr. Dement, a Professor of Psychiatry and Behavioural Sciences at Stanford University School of Medicine, contributed to the establishment of the first sleep disorder centre in Stanford. After Stanford, other centres in New York, Texas, Ohio and Pennsylvania started providing sleep evaluations for which patients stayed in the centre overnight. The Association of Sleep Disorders Centre (ASDC) was established in 1975 and Dr. Dement served as its first president for12 years. In 1999 ASDC was renamed American Academy of Sleep Medicine (AASM). The first textbook of sleep medicine “Principles and Practice of Sleep Medicine” was published in 80’s. The journal SLEEP started in 1978. In 1998 the AASM commissioned the fellowship training committee to develop guidelines for sleep medicine fellowship training. The first two programmes to be granted formal accreditation were Stanford University in California and the Centre for Sleep and Wake in Montefiore Medical Centre, New York. The American Medical Association recognized sleep medicine as a specialty in 1996. In 2004 the Accreditation Council on Graduate Medical Education (ACGME) took over the fellowship accreditation process and approved a one year training programme 1,3,4,5.
Sleep Medicine training in Europe:
Unlike United States, there are no formal sleep medicine training programmes or qualification in the United Kingdom or Europe. Sleep medicine is restricted to a small group of respiratory physicians with a special interest in sleep medicine. Psychiatry trainees are exposed to very little formal teaching in sleep medicine. However in the last 3 years the neuropsychiatry section of the Royal College of Psychiatrists of the United Kingdom has formed the “sleep working group” under the leadership of Dr. Hugh Selsick, this group is responsible for increasing awareness of sleep medicine among British psychiatrists, by emphasizing the importance of sleep medicine in psychiatric practice and encouraging psychiatrists to contribute to the field of sleep medicine. This group has developed a competency based curriculum that incorporates the training of sleep medicine into the psychiatry curriculum, to organize sleep medicine symposia at annual conferences of the Royal College and to develop professional training (CPD) modules for psychiatrists. British Sleep Society is another forum that brings together physicians from various backgrounds interested in sleep medicine. Royal Society of Medicine also has a sleep medicine section which organizes various conferences. There are two, week long courses on sleep medicine, the Edinburgh and Cambridge courses. Recently the University of Glasgow started a Master’s of Science (MSc) in behavioural sleep medicine program for healthcare providers working in Scotland, the rest of the United Kingdom and Europe 6, 7, 8, 9. There is a trans-European move to start a formal sleep medicine certification similar to what we have in the United States. European Sleep Research Society (ESRC), a professional body of sleep scientists in Europe responsible for promoting sleep research and sleep medicine is starting its “first ESRS certification examination” in sleep medicine; this examination is scheduled to take place on September 4th, 2012 at the 21st Congress of the European Sleep Research Society in Paris. Since there are no formal training programmes this will be for those without formal training 10.
Psychiatry and Sleep:
Asking about the patient’s sleep is an integral part of a psychiatric consultation. Almost all the medication that psychiatrists prescribe has an effect on sleep architecture. Some psychiatric medications are used to treat sleep disorders and others can cause sleep disorders like Restless Legs Syndrome and PMLD. Understanding sleep can help us understand the mechanism of psychiatric illness. Many psychiatric disorders have comorbid sleep disorders and several behavioural therapies have been used successfully for the treatment of sleep disorders. There is bidirectional association between sleep disorders and psychiatric disorders. With the growing population of military soldiers returning from Iraq and Afghanistan with post-traumatic stress disorder, sleep problems and depression, there is an increased need for psychiatrists who possess knowledge in both sleep disorders and comorbid psychiatric illness. Psychiatrists have a distinct advantage dealing with sleep disorders and can bring those skills to sleep medicine.
Are psychiatrists attracted towards sleep medicine? The answer is yes. In the recent years we have seen an increased interest among psychiatry trainees for a sleep fellowship in United States. In recognition of behavioural consequences of sleep problems and multidisciplinary approach in sleep disorders, fellowship programmes are increasingly taking applicants from various backgrounds and not just pulmonology and neurology. Many psychiatry trainees are choosing a sleep medicine elective earlier in residency. Currently there are more than 710 accredited sleep centres in the United States. Many major university medical centres have a one year fellowship programme accepting applications from physicians from various backgrounds including Psychiatry, Neurology, Internal Medicine, Pulmonology, Paediatrics, ENT and Anaesthesia 1. There are more than 24 AGME approved sleep medicine fellowship programmes in the United States 11. New fellowship programmes are being opened at the University of Kansas Medical Centre and the University of Texas Health Sciences Centre, San Antonio.
Conclusion:
Sleep medicine is a new and exciting field of medicine with potential to grow in future. It’s a multidisciplinary field. American sleep medicine has evolved greatly over the last 30 years and there appears to be much to learn from the American model. There is a need for the psychiatry training programs both in the United States and the Europe to encourage and prepare their trainees to consider training in sleep medicine. Psychiatry trainees in the United States interested in sleep medicine should speak with their programme directors early in their residency training to register their interest and residents should also contact the local sleep centre for more advice. Each year American Academy of Sleep Medicine (AASM) accepts 10 international physicians for its 4 week mini-fellowship programme. Three weeks of the fellowship are spent at an AASM-accredited U.S sleep centre with their last week of the fellowship spent at the annual SLEEP conference. A certificate of training is issued at the end of the mini fellowship 12.
Non adherence to medication is a significant problem for client group in Psychiatry. Between a third and half of medicines that are prescribed for long term conditions are not used as recommended2, 3. In the case of Schizophrenia, studies reveal that almost 76% of the sufferers become non-compliant to the medication within the first 18 months of treatment 4.
Non-adherence has consequences for both clients and the Health Care System. If the issues of non-adherence are better identified and addressed actively, it has the potential of improving the mental health of our clients which will reduce the burden of cost to mental health resources. It is estimated that unused or unwanted medications cost the NHS about £300 million every year. This does not include indirect costs which result from the increased likelihood of hospitalization and complications associated with non-adherence5.
The WHO identified non-adherence as “a worldwide problem of striking magnitude”. This problem is not only just linked with our psychiatric client groups, but also is prevalent with most chronic physical conditions. It has been reported that adherence to medications significantly drop after six months of treatment6.
In broad term compliance is defined as the extent to which the patient is following the medical advice. Adherence on the other hand is defined as the behavior of the clients towards medical advice and their concordance with the treatment plan. Adherence appears to be a more active process in which patients accept and understand the need of their treatment through their own free will and portray their understanding with either a positive or negative attitude towards their medications7
Unfortunately there is no agreed consensual standard to define non adherence. Trials suggest a rate of >50% compliance as adequate adherence while other researchers believe it should be at least >95%. As per White Paper of DOH (2010), it has been recommended that clinicians have the responsibility to identify such issues and improve collaborative relationships among multidisciplinary teams to deliver a better clinical and cost effective service8.
Methods:
Sampling:
Our cohort included a prospective consecutive sample of 179 patients. The study was conducted in North Essex Partnership NHS Trust which provides general adult services for a catchment area of approximately 147,000 in Tendring area. All these clients were seen at the out patient’s clinic at Clacton & District Hospital. Informed consent was taken as per recommendation of local clinical governance team. The study was conducted during a 2 month period from October to November in 2010. No patient was excluded from the study. Sample consists of clients who were aged 16years and above.
Tools Used:
All the clients were asked questions using a standard questionnaire and MARS (Medication Adherence Rating Scale). MARS was developed by Thompson et al in 1999 as a quick self-reported measure of adherence mainly around psychiatric clients. It was mainly devised from a 30 item Drug Attitude Inventory (DAI) and a 4 item Morisky Medication Adherence Questionnaire (MAQ). The validity and reliability of MARS has been established by Thompson et al and then Fialko et al in 2008 in a large study and has been reported to be adequate9,10.
The patient questionnaire directly asked clients about their current medications and dosage regimens. It also enquired about various factors leading to non-compliance. It included factors like whether the medication makes them feeling suicidal, causes weight gain, makes them aggressive, causes sleep disturbances, causes sexual side effects, the form and size of tablets, stigma and family pressure, their personal belief about medication or do they feel that they become non adherent because as a direct effect and consequence of the illness.
Medication Adherence Rating Scale focuses both on adherence as well as the patient’s attitudes towards medications. It includes questions about how frequently they forget to take medications or are they careless about taking their medications. It also asks them if they stop taking their medication do they feel well or more unwell. Other aspects include whether they only take medicines when they are sick and do they believe that it is un-natural for their thoughts to be controlled by medications. It also asks about the effect of medication on them, such as; are they able to think clearly, or do they feel like a zombie on them?, or are they tired all the time?. It also checks their belief that if they remain compliant to medication, will it prevent them from getting sick again.
Results:
In total 179 clients were seen in the outpatient clinic during the period of two months. Out of those (54%, n=97) were females whereas nearly half (46%, n=82) were males. Age of the clients ranged from 18 years to 93 years. The mean age of the client group was 55; mode 41 and median was 69.5.
The diagnosis profile was quite varied. As far as the primary diagnosis is concerned, the majority (n=144) of service users were given a primary diagnosis using the ICD 10 criteria. Mood disorders were the most common primary diagnosis whereas personality disorder and anxiety were the most common secondary diagnosis. Table 1 show the number and percentage of the service users who presented with the most common diagnosed conditions:
Table 1: List of primary and Secondary diagnosis
Diagnosis
Primary
Secondary
Mood Disorders
72 (50%)
07 (26.92%)
Psychotic illness
25 (17.36%)
01 (3.85%)
Anxiety and PD
13 (9%)
13 (50%)
Dementia
24 (16.7%)
02 (7.69%)
Neurological disorder
07 (4.86%)
01 (3.85%)
Drugs related illness
02 (1.39%)
02 (7.69%)
Eating disorder
01 (0.69%)
00 (0.0%)
Subjectively 160 (89%) patients reported that they were compliant with medications whereas 19(11%) patients admitted that they have not been adherent to medications. Out of those who said that they were non-adherent, 8 were suffering from Mood disorders, 2 had schizoaffective disorder, 3 had psychotic illness, 3 had organic brain disorder, 2 clients had personality disorder, whereas 1 client had anxiety and 1 had neurological illness.
Prescription rate varied between different types of psychotropic medications. Antipsychotics were the most prescribed medication in our cohort. Table 2 shows data of each individual category.
Table 2: Number and percentage of individual medication category prescribed
Medication category
N=number of prescribed meds
% of total prescriptions
Antipsychotics
100
44%
Antidepressants
72
31%
Mood Stabilisers
21
09%
Anxiolytics
21
09%
ACH Inhibitors
12
05%
Hypnotics
04
02%
Less than half (39%, n=69) of service users had only one type of psychotropic medication whereas the majority (58%, n=104) of patients were on more than one psychotropic medication. A very small number of clients (3%, n=6) were not using any medications at all. When explored further it was revealed that almost two third of the antidepressant prescriptions comprised of SSRI’s (67%, n=55), about one fourth of SNRI (24%, n=21), a small proportion (6%, n=5) of NARI’s and very few (3%, n=3) were given tricyclic antidepressants. Similarly in antipsychotics, 75% of patients were on atypical and 25% were prescribed typical antipsychotics.
Factors leading to non-adherence:
Below is the graphical representation of what clients perceived as the major factors leading to the non adherence to the medication. Weight gain, illness effect, stigma and personal belief appear to be the major factors as displayed in Chart 1.
Chart 1: Number of responses for each individual factor leading to non-adherence:
Attitude towards Medications:
The overall Service users’ attitude towards medication did not appear to be particularly good. They mainly complained of getting tired and forgetting to take medication. Below in Chart 2 is the graphical representation of what overall attitude they had expressed towards psychotropic medications.
Chart 2: Number of responses for each factor indicating attitude towards medication
As far as overall MARS score is concerned, the majority of patients (63%, n=110) scored >6 and about one third of patients (37%, n=63) scored <6. A score of less than 6 is generally considered as a poor level of adherence which means that almost one third of our client group does not comply with medications.
Discussion:
The aim of our study was to highlight the importance of the factors which often lead to non-adherence to medications and to explore patients’ attitudes towards medications. Results are indicating that the problem of non-adherence is much wider and deeper in our clients group. There is a significant gap in between subjective and objective rate of adherence. However we should be mindful that adherence appears to be more of a continuum rather than a fixed entity e.g. some patients can be more adherent than others but still have inadequate adherence and hence arises the concept of partial adherence. It is evident from the results that patients’ attitudes were not encouragingly positive towards psychotropic medications.
Human beings are born potentially non-compliant. It is our tendency to crave and indulge in things which we know might not be good for our health e.g. eating non healthy food, alcohol and substance misuse. We have better compliance to issues which give us the immediate reward like pain relief or euphoria from illicit drugs where as because of lack of this immediate reward, our compliance gradually becomes erratic. Compliance and adherence appears to be a learnt phenomenon which needs to be nurtured throughout our life.
Manifestations of non-adherence:
The consequences of non-adherence are mainly manifested and expressed through clinical and economic indicators. Clinically it means an increase in the rate of relapse and re-hospitalisation. As per one study non-adherent patients have about a 3.7 times high risk of relapse within 6 months to 2 years as compared to patients who are adherent11. In US it was estimated that at least 23% of admissions to nursing homes were happening due to non adherence which meant a cost of $31.3 billion/380,000 admissions per year12. Similarly 10% of admissions happened for the same reason costing the economy an amount of $15.2 billion/3.5 million patients13,14. Figures in UK are also not much different where the cost of prescriptions issued in 2007-08 was estimated to be £8.1 billion and it was highlighted that £4.0 billion out of that amount was not used properly15. Similarly in terms of hospitalization, about 4% admissions happen every year happen because of non-adherenceThe total cost of hospitalization in 2007 was estimated to be £16.4 billion and it was suggested that non-adherence had a burden of costs in the region of £36-196 million17.
From a clinical aspect it has been suggested that non-adherence causes about 125,000 deaths just in the US every yearMet analysis has suggested significant statistical association between non-adherence and causing depression in certain chronic physical conditions e.g. Diabetes19.
Dimensional Phenomenon?
We need to be aware that adherence is a multidimensional and a multifaceted phenomenon and is better understood in dimensional rather than categorical terms. It has been widely accepted that if concordance is the process, then adherence will be the ultimate outcome. This was highlighted by WHO guidelines using following diagram:
Chart 3: WHO diagram of the five dimension of adherence:
Therefore any strategy developed to address the issue of non-adherence should be able to consider all these five dimensions; otherwise it will be less likely to have any chance of success.
Measures to improve Compliance:
All the known as clinical and economic indicators suggest that non-adherence issue needs significant attention and special measures which ought to be taken in order to avoid complications. There are already some running campaigns in other countries in order to improve adherence and we need to learn from their experiences such as the National Medication Adherence Campaign in US (March 2011). The campaign is basically a research-based public education effort targeting patients with chronic conditions, their family caregivers, and health care professionals20.
Levine (1998) demonstrated that the following steps may help in increasing adherence:
To appropriately asses the patient’s knowledge and understanding about the disease process and the need for treatment and to address those issues if there is some dysfunctional belief.
To link the taking of medication with other daily routines of the life
To use aids to assist medication adherence e.g. MEMS, ePills, Calendar or Dossette box
To simplify the dosage regimen
Flexible Health care team who is willing to support
Addressing current Psychosocial and environmental issues which might hinder the adherence21.
It is extremely important for the clinician to take time to discuss in detail with their patients all the possible side effects and indications of the prescribed medications. Unfortunately clinicians may not be able to predict the possibility of having side effects but can certainly educate patients about their psychopathology, indication and rationale for the medication and make them realise how important it is for them to remain adherent to medication. Health education is considered equally effective as compared to any sophisticated adherence therapy and should be used routinely22.Clinicians also have very important role to play in simplifying the dosage regimen and emphasise to the patients that “Medications don’t work in patients who don’t take them”23.
Various studies have tried to estimate the efficacy of a single factor and the multi factor approaches to improve adherence 24. Studies have showed proven efficacy for education in self management25,26, pharmacy management programmes27,28, nursing, pharmacy and other non medical health professional intervention protocols29,30, counselling31,32, behavioural interventions33,34 and follow up35,36. However multi factor approaches have been found to be more effective than single factor approaches,38Therefore it has been suggested that we need to address all the five dimensions of adherence (Chart 3) with multiple interventions to improve the adherence in our patients.
One factor potentially of concern leading to non-adherence is the possibility of the current overt or covert misuse of alcohol, illicit substances and over the counter available medications. This issue understandably can lead to partial or complete non adherence as well as worsening of existing psychiatric conditions. Therefore it needs to be explored further in future research projects.
Fibromyalgia (FM) is a challenging set of chronic, overlapping and debilitating syndromes with widespread pain, abnormal pain processing, sleep disturbance, fatigue and psychological distress.1 The American College of Rheumatology (ACR) 1990 diagnostic guidelines were based primarily on tender point examination findings at 11 of 18 potential tender points;2 however, lack of consistent application of these guidelines in clinical settings led the ACR in 2010 to develop new diagnostic criteria based on a Widespread Pain Index (WPI) and symptom severity (SS) scale with no requirement of a tender point examination. Symptoms must have been present for at least three months with the absence of any other disorder that would otherwise explain the pain and other signs and symptoms.3
Type of pain and other symptoms vary widely in FM, complicating diagnosis and treatment. A cross-sectional survey of 3,035 patients in Germany utilized cluster analysis to evaluate daily records of symptoms noted by patients on handheld computers. Five subgroups were described: four with pain evoked by thermal stimuli, spontaneous burning pain, pressure pain, and pressure pain combined with spontaneous pain; the fifth subgroup had moderate sensory disturbances, but greater sleep disturbances and the highest depression scores.4
Estimates of the prevalence of FM have varied based on case definitions and survey methods. Using 1990 ACR guidelines, it was estimated to affect between 0.1 to 3.3% of populations in western countries and 2.0% in the United States. Greater prevalence occurs among females, with estimates ranging from 1.0 to 4.9%.1, 5 Reasons for the gender difference have not been determined.6-9
Fibromyalgia Risk Factors
Identification of risk factors for FM has been complicated by the array of seemingly unrelated signs and symptoms. The United States Centers for Disease Control (CDC) notes loose association with genetic predisposition,10 bacterial and viral infections, toxins, allergies, autoimmunity, obesity and both physical and emotional trauma.1, 11
Chronic fatigue syndrome and infection
Although chronic fatigue syndrome (CFS) has been defined as a separate syndrome, up to 70% of patients with FM are also diagnosed with CFS and 35-70% of patients with CFS have also been diagnosed with FM.12 Thus studies of patients with CFS may have clinical relevance to FM. Several case controlled studies of CFS and one of CFS/FM have been associated with chronic bacterial infections due to Chlamydia (Chlamydophila p.), Mycoplasma, Brucella, and Borrelia.12-18 The most prevalent chronic infection found has been that of the various Mycoplasmaspecies.15-23
Mycoplasmas are commonly found in the mucosa of the oral cavity, intestinal and urogenital tracts, but risk of systemic illness occurs with invasion into the blood vascular system and subsequent colonization of organs and other tissues.15-23Mycoplasmal infections have been identified in 52 – 70% of CFS patients compared with 5 to 10% of healthy subjects in North America15-17, 19-22 and Europe (Belgium)23. For example, the odds ratio (OR) of finding Mycoplasma species in CFS was 13.8 (95% CL 5.8-32.9, p< 0.001) in North America.17A review by Endresen12 concluded that mycoplasmal blood infection could be detected in about 50% of patients with CFS and/or FM. A CDC case-control study attempted to replicate these findings based on the hypothesis that intracellular bacteria would leave some evidence of cellular debris in cell-free plasma samples. Results were that the healthy subjects actually had evidence of more bacteria although the difference was not significant. The authors noted the complexity and limitations of this type of analysis and also postulated that since the CFS patients were years past the onset of illness, they might have previously cleared the triggering agent.24 However, most studies found Mycoplasma DNA in intracellular but not extracellular compartments in CFS patients, and this could explain the discrepancy.15-23 Other studies have found that 10.8% of CFS patients were positive for Brucella species (OR=8.2, 95% CL 1-66, p<0.01)16 and 8% werepositive for Chlamydia pn. (OR= 8.6; 95% CL 1-71.1,p< 0.01)17.
The presence of multiple co-infections may be an especially critical factor associated with either initiation or progression of CFS. Multiple infections have been found in about one-half of Mycoplasma-positive CFS patients (OR = 18.0, 95% CL 8.5-37.9, p< 0.001), compared with single infections in the few control subjects with any evidence of infection.17 A North American study identified chronic infections in 142 of 200 patients (71%) with 22% of all patients having multiple mycoplasmal infections while just 12 of the 100 control subjects (12%) had infections (p<0.01) and none had multiple infections.15 Similarly, a European study reported chronic mycoplasmal infections in 68.6% of CFS and 5.6% of controls. Multiple infections were found in 17.2% of the CFS patients compared with none in the controls (p<0.001).23 Multiple co-infections were also associated with significantly increased severity of symptoms (p<0.01).15, 23
Viral infections associated with CFS have included Epstein Barr virus, human herpes virus-6, cytomegalovirus, enteroviruses and several other viruses.15, 25, 26
Despite indications of single or multiple bacterial and/or viral infections in most patients with CFS, antibiotic or antiviral treatments have yielded inconsistent results.27 Slow growing intracellular bacteria are relatively insensitive to most antibiotics and have inactive phases when they would be completely insensitive to any antibiotics.2823 Some treatments may actually have resolved the infections, but not the immune pathways that may remain in an activated state capable of producing symptoms.
Fibromyalgia and infection
Bacterial infections associated with FM as a separate syndrome have included small intestinal bacterial overgrowth (SIBO)29, 30 and helicobacter pylori (HP)31. Utilizing the lactulose hydrogen breath test (LHBT), investigators found SIBO in 100% of 42 patients with FM. They noted that 30-75% of patients with FM have also been found to have irritable bowel syndrome (IBS).29, 30 A confounding factor is that medications prescribed for FM often have gastrointestinal side effects.29 HP diagnosed by positive immunoglobulin gamma (IgG) serum antibody was significantly higher in women with FM (44/65 or 67.7%) compared with controls (18/41 or 43.9%) (p=0.025) in Turkey31.
Viral infections associated with FM have included hepatitis C, in which two studies found an association,32-34 and two studies found no association.35, 36 Associations with FM have also been found with hepatitis B, 37 human immunodeficiency virus (HIV)38, 39 and human T cell lymphotropic virus type I (HTLV-1).40
Fibromyalgia and non-infectious associations
Non-infectious triggers associated with FM have included toxins, allergens, and physical or emotional trauma. These triggers may not have been strictly “non-infectious” as allergens and toxins may also be produced by infections, and physical or emotional trauma may lead to the reactivation of previously controlled infections. Respondents to an internet survey of people with FM (n=2,596) also identified triggers as chronic stress (41.9%), emotional trauma (31.3%), acute illness (26.7%) and accidents (motor vehicle 16.1%, non-motor vehicle 17.1%).41 Physical trauma associated with FM has included cervical spine injuries as well as motor vehicle and other accidents.42-44
Fibromyalgia and autoimmunity
Three studies have found thyroid autoantibodies to be in greater percentages in subjects with FM compared with controls, in spite of normal thyroid hormone levels. One study reported autoantibodies in 41% of FM patients versus 15% of controls.45 The second study reported 16% in FM versus 7.3% in controls, p<0.01.46 The third study reported 34.4% in FM versus 18.8% in controls (p=0.025)47 and OR =3.87, 95% CL 1.54-10.13.48 This could also have been the result of thyroiditis, because infections like Mycoplasma are often found in thyroiditis patients.15
Autoantibodies to serotonin were identified in 74% of 50 patients with FM compared with 6% of 32 healthy (blood donor) controls. Notably, serotonin levels were normal in 90% of the FM patients indicating serotonin receptor involvement.49
Fibromyalgia and Metabolic Syndrome
Metabolic Syndrome consisting of abdominal obesity, high triglycerides, high blood pressure, elevated fasting glucose and decreased high-density lipids, was associated with FM in a U.S. study in which cases were 5.6 times as likely to have Metabolic Syndrome as controls (C2MH = 3.84, p = .047, 95% CL 1.25 – 24.74).50
Fibromyalgia and emotional trauma
Although emotional trauma has been acknowledged as a contributing factor, most studies of CFS/FM have used recognized tests such as Beck’s Depression Index, Beck’s Anxiety Index and Minnesota Multi Personality Index (MMPI) to exclude potential subjects with actual psychiatric illnesses.51, 52
Psychological and physiological subsets of fibromyalgia
A Wisconsin cross sectional survey of 107 women with confirmed diagnoses of FM used validated psychological and physiological measures followed by cluster analysis. Four distinct subsets were identified: (I) history of childhood maltreatment and hypocortisolism with the most pain and disability; (II) “physiological dysregulation” described as “distinctive on nearly every biological index measured” with high levels of pain, fatigue and disability; (III) normal biomarkers with intermediate pain severity and higher global functioning; and (IV) psychological well-being with less disability and pain.53
The “physiological dysregulation” of FM subset II consisted of the highest antinuclear antibody (ANA) titers (t=4.06, p=0.001), highest total cholesterol levels (t=3.96, p<0.001), larger body mass index (BMI) values t=2.21, p<0.04), lowest Natural Killer (NK) cell numbers (t=3.95, p<0.001), lowest growth hormone (t=3.20, p<0.002), and lowest testosterone levels (t=3.80, p<0.001). Trends were also indicated toward the highest erythrocyte sedimentation rate (ESR) (t=2.02, p=0.056), lowest creatinine clearance (t=1.85, p=0.067) and lowest cortisol (t=2.78, p<0.007).53
Proposed Model of Fibromyalgia
The authors’ proposed model of FM develops a rationale for the “physiological dysregulation” indicated in subset II of the Wisconsin study. In this model, various triggers are followed by prolonged immune activation with subsequent multiple hormonal repression, disrupted collagen physiology and neuropathic pain.
Activation of immune response pathways
Innate immune responses begin with anatomical barriers, such as the epithelium and mucosal layers of the gastrointestinal, urogenital and respiratory tracts, and physiological barriers, such as the low pH of stomach acid and hydrolytic enzymes in bodily secretions. 54 Breeching of these barriers activates cell-mediated immunity launched by leucocytes with pattern recognition receptors: neutrophils, macrophages and dendritic cells (DCs).54 Insufficient or damaged anatomical or physiological barriers would necessarily keep this cell mediated level of innate defense in a constant state of alert and activity.
In contrast to the innate immune response, adaptive immunity has highly specific recognition and response activities resulting in lasting changes produced by leukocytes known as lymphocytes. B lymphocytes (B cells) secrete plasma cells producing antibodies to specific pathogens. T lymphocytes (T cells), the other major cells of adaptive immunity, can be either cytotoxic (Tc) or helper cells (Th). Tc cells produce progeny that are toxic to non-self peptides and Th lymphocytes secrete small proteins (cytokines) that mediate signaling between leukocytes and other cell types. All types of lymphocytes retain memory so that subsequent invasions provoke faster and more rapid differentiation into effector cells. 54, 55 SomeTh cells respond to intracellular pathogens (Th1) and some to extracellular pathogens (Th2). A third type (Th17) appears to respond to certain bacterial and fungal infections, tumor cells and are also involved in autoimmune diseases.56
In the presence of environmental stressors, cells may release stress proteins to alert the organism to potentially damaging conditions. These proteins can bind to peptides and other proteins to facilitate surveillance of both the intracellular and extracellular protein environment. One form of stress proteins, heat shock proteins (HSP), can mimic the effects of inflammation and can be microbicidal.52, 57
One of the earliest responses to intracellular viral or bacterial infections involves production of three types of interferon (IFNa, IFNb and IFNg). Any of these can initiate a series of metabolic events in uninfected host cells that produce an antiviral or anti-bacterial state.58, 59 When IFN-γ targets genes in uninfected cells, the targeted genes become microbicidal by encoding enzymes generating oxygen (O2) and nitric oxide (NO) radicals.58 Activation of O2 or NO radicals triggers another cascade involving IL-6, IL-1b, the cytokine Tumor Necrosis Factor-a (TNF-a) and the transcription nuclear factor kB (IKKb-NF-kB). NF-kB can be activated by a variety of inflammatory stimuli, such as cytokines, growth factors, hormones, oncogenes, viruses and their products, bacteria and fungi and their products, eukaryotic parasites, oxidative and chemical stresses, therapeutic and recreational drugs, additional chemical agents, natural products, and physical and psychological stresses.60 Activation of NF-kB releases its subunits; the p50 subunit has been associated with autoimmunity and the RelA/p65 unit with transcriptional activity involving cell adhesion molecules, cytokines, hematopoietic growth factors, acute phase proteins, transcription factors and viral genes.61 The authors propose that chronic infection or other stress would be a sustaining trigger of an immune cascade that includes NF-kB and resultant cell signaling processes that drive many of the symptoms of fibromyalgia.
The cytokine interleukin-6 (IL-6) can either activate or repress NF-kB through a switching mechanism involving IL-1ra and Interleukin 1b(IL-1b). IL-6 first activates Interleukin 1b (IL-1b), which then activates TNF-a, leading to the subsequent activation of NF-kB. 62, 63 Specifically, the release of the RelA/p65 subunit of activated NF-kB switches on an inhibitory signaling protein gene (Smad 7) that blocks phosphorylation of Transforming Growth Factor Beta (TGF-b) resulting in the repression of multiple genes. Alternatively, IL-6 activates IL-1ra, which allows TGF-b to phosphorylate and induce the expression of activating signaling protein genes Smad2 and Smad3, resulting in the full expression of multiple genes.61
NF-kB plays a key role in the development and maintenance of intra- (Th1) and inter- (Th2) cellular immunity through the regulation of developing B and T lymphocytes. The p50 dimer of NF-kB has been shown to block B Cell Receptor (BCR) editing in macrophages, resulting in loss of recognition and tolerance of host cells (autoimmunity). T cells that are strongly auto-reactive are normally eliminated in the thymus, but weakly reactive ones are allowed to survive to be subsequently regulated by regulatory T-cells and macrophages. Acquired defects in peripheral T-regulatory cells may mean failure to recognize and eliminate weakly reactive ones.54, 64 The IL-17 cytokine associated with autoimmunity can activate NF-kB through a pathway that does not require TNF-a.56 NF-kB activity can also be activated or repressed by the conversion of adenosine triphosphate (ATP) to cyclic adenosine monophosphate (c AMP) in the early phases (3 days) of nerve injury through its main effector enzyme, protein kinase A (PKA).65, 66 PKA decreases during later stages as the enzyme protein kinase C (PKC) increases. PKC then plays important roles in several cell type specific signal transduction cascades.67 An isoform of PKC within primary afferent nociceptive nerve fibers signals through IL-1b and prostaglandins E2 (PGE2) as demonstrated in animal studies.68 This process has been called “hyperalgesic priming,” and it has been described as responsible for the switch from acute to long-lasting hypersensitivity to inflammatory cytokines.69
Figure 1 depicts key immune pathways leading to expression or repression of multiple genes proposed to be important in FM and neuropathic pain.
Fibromyalgia and immune - hormonal interactions
Reciprocity exists between the immune system and the hypothalamic-pituitary-adrenal (HPA) axis through its production of glucocorticoid signal transduction cascades. 63, 70, 71. Hormones such as cortisol (hydrocortisone) produced by the adrenal cortex, affect metabolism of glucose, fat and protein.72 The glucocorticoid receptor (GR), a member of the steroid/thyroid/retinoid super family of nuclear receptors is expressed in “virtually all cells”. When the GR in the cytoplasm binds a glucocorticoid, it migrates to the nucleus where it modulates gene transcription resulting in either expression or repression of TNF-a, IL-1bβ and the NF-kB p65/RelA subunit. However, the RelA/p65 protein can also repress the Glucocorticoid Receptor. 63, 70, 71, 73
Growth hormone (GH), an activator of NF-kB,74 is usually secreted by the anterior pituitary, but changes found in FM may be hypothalamic in origin. GH is needed for normal childhood growth and adult recovery from physical stresses.75 Although low levels of GH were found in subset II of the Wisconsin study, 53 functional deficiency may be expressed as low insulin-like growth factor 1 (IGF-1) combined with elevated GH, suggesting GH resistance.76, 77 Defective GH response to exercise has been associated with increased pain and elevated levels of IL-1b, IL-6, and IL-8.77, 78
The hormones serotonin and norepinephrine modulate the movement of pain signals within the brain. Serotonin has been found to suppress inflammatory cytokine generation by human monocytes through inhibition of the NF-kB cytokine pathway in vitro;79 however, NF-kB promotion of antibodies can repress serotonin.49 Selective serotonin and norepinephrine reuptake inhibitors (SSNRIs), such as duloxetine and milnacipran, are key treatment options for fibromyalgia and have been approved of by the U.S. Food and Drug Administration (FDA).80, 81 Although serotonin has been best measured in cerebral spinal fluid (CSF), recently improved methods of collection were utilized (using rats and in 18 women) that yielded a high degree of correlation (r=0.97) between CSF and plasma, platelet, and urine measurements.82
NF-kB activation has also been documented to interfere with thyroid hormone action through impairment of Triiodothyronine (T3) gene expression in hepatic cells. 83 However, T3 administration has induced oxidative stress and activated NF-kB in rats.84
Metabolic Syndrome, a confounding factor in Fibromyalgia
Leptin and insulin hormones interact to regulate appetite and energy metabolism. Leptin, produced by adipose cells, circulates in the blood eventually crossing the blood-brain barrier to bond with a network of receptors within the hypothalamus. Insulin, produced by beta cells in the pancreas, similarly crosses the blood brain barrier to interact with its own network of hypothalamic receptors. Leptin and its receptors share structural and functional similarities to long-chain helical cytokines, such as IL-6, and it has been suggested that leptin be classified as a cytokine.85-89
Metabolic syndrome can be a confounding factor in FM due to peripheral accumulation of fatty acids, acylglycerols and lipid intermediates in liver, bone, skeletal muscle and endothelial cells. This promotes oxidative endoplasmic reticulum (ER) stress and the activation of inflammatory pathways involving PKC and hypothalamic NF-kB, leading to central insulin and leptin repression.85-87, 89-91Hyperinsulinemia further stimulates adipose cells to secrete and attract cytokines such as TNFa and IL-6 that trigger NF-kB in a positive feedback loop, which can be complicated by chronic over nutrition that increases the generation of reactive oxygen intermediates and monocytechemoattractant protein-1 (MCP-1).87, 89 When exposed to a chronic high fat diet, hypothalamic NF-kB was activated two fold in normal mice and six times in mice with the obese (OB) gene.89
Fibromyalgia and indicators of immune-hormonal activity
Although most components of either innate or adaptive cell mediated immune responses exist for only fractions of seconds, some of their effects and products can be detected long after in the skin, muscle, blood, saliva or sweat92, 93.
One component, nitric oxide (NO), can suppress bacteria; however, endothelial damage causes dysfunction with impaired release of NO and loss of its protective properties.86 The enzyme transaldolase acts as a counterbalance by limiting NO damage to normal cells. Thus, high levels of transaldolase indicate elevated reactive oxygen species, reactive nitrogen species (ROS/RNS) and cellular stress. The “exclusive and significant over-expression of transaldolase” in the saliva samples of 22 women with FM compared with 26 healthy controls (77.3% sensitivity and 84.6% specificity, p<0.0001; 3 times greater than controls; p=0.02) was “the most relevant observation”; although there was no correlation between transaldolase expression and the severity of FM symptoms.92
High levels of NO have been associated with high levels of insulin, and insulin itself is a vasodilator that, in turn, can stimulate NO production. Beta cells of the pancreas are quite susceptible to ROS/NOS damage .86When free radical damage of beta cells reaches critical mass, insulin production plummets with an associated decline in NO levels. Thus, patients with FM who have high NO levels would likely be suffering from associated metabolic syndrome, and patients with low NO levels would likely be suffering from Type II diabetes.85, 88
Figure 2 illustrates the relationship of NF-kB to various hormone systems.
Fibromyalgia and immune-hormonal influences on connective tissue
Inflammation of muscles, tendons, and/or fascia is generally followed by proliferative and remodeling phases of healing initiated by fibroblasts which lay down an extracellular matrix (ECM) composed of collagen and elastin fibers. “Fibroblasts respond to mechanical strain by altering shape and alignment, undergoing hyperplasia and secreting inflammatory cytokines including IL-6.” The extra cellular matrix is initially laid down in a disorganized pattern that is subsequently matured and aligned. Chronic and excessive mechanical tension from postural imbalance, hormonal disruption or other factors may interfere with collagen maturation. 94 Remodeling of the extracellular matrix and collagen deposition around terminal nerve fibers may be compressive and contribute to neuropathic pain.95
Oxidative stress in muscles accelerates the generation of advanced glucose (glycation) end products (AGEs). AGE-mediated cross-linked proteins have decreased solubility and are highly resistant to proteolytic digestion. Interaction of AGEs with their receptors leads to activation of NF-kB resulting in an increased expression of cytokines, chemokines, growth factors, and adhesion molecules.9697
Two AGE products have been reported at significantly elevated levels in the serum of patients with FM: N-carboxymethyllysine (CML) (2386.56 ± 73.48 pmol/mL; CL 61.36-2611.76 versus controls 2121.97 ± 459.41 pmol/mL; CL 2020.39-2223.560; p<0.05)96 and pentosidine (mean 190 ± 120 SD and median 164 versus controls mean 128 ± 37 SD and median 124; p<0.05)97 Comparison of muscle biopsies showed “clear differences in the intensity and distribution of the immunohistochemical staining”. CML was seen primarily in the interstitial tissue between the muscle fibers where collagens were localized and in the endothelium of small vessels of patients. Activated NF-kB was seen in cells of the interstitial tissue especially around the vessels of patients, but almost no activated NF-kB was seen in the control biopsies. AGE activation of NF-kB has been shown to be significantly more prolonged than the activation of NF-kB by cytokines.9697
Fibromyalgia, the nervous system and pain
Sensory transmission in humans occurs through three primary afferentnerve fiber types: heavily myelinated mechanical afferent pathways (A Beta fibers) that transmit non-noxious tactile sensations, small-diameter myelinated fibers (A Delta fibers) that transmit sharp pain, and small diameter unmyelinated fibers (C fibers) that transmit dull aching pain. The heavily myelinated non-pain Aβ fiber type has been shown to sprout axons that terminate on pain lamina in the posterior horn of the spinal cord resulting in the conversion of mechanical stimuli to pain. Within the brain, sensitization of the N-methyl D-aspartate (NMDA) receptors can amplify pain signals between the thalamus and the sensory cortex.67, 98
Chronic damage or excitation of nociceptive afferent fibers from compressive collagen deposition may develop into spontaneous (ectopic) firing oscillating at frequencies sufficient to initiate cross (ephaptic) excitation of sympathetic and sensory fibers (myelinated A-delta and non-myelinated C fibers) within the dorsal root ganglia (DRG) of the central nervous system.98 Normally, the DRG has little sympathetic innervation, but trauma can trigger sympathetic sprouting that forms basket-like structures within the DRG. Neurotrophins, in particular nerve growth factor (NGF), play an important role in sympathetic fiber sprouting of sensory ganglia in murine models. DRG can be reservoirs for latent viral infections such as Herpes Zoster, HIV and enteroviruses. In addition, the Borrelia species has been identified in a non-human primate model of Lyme disease. NGF also facilitates expression of Substance P (SP), a peptide neurotransmitter involved in the induction of the IL-6 - NF-kB pathway 60, 99, 100 and in the transmission of neuropathic pain.101, 102 SP has been found to be elevated in the cerebrospinal fluid of patients with FM in comparison to normal values,103 and control subjects.104
Summary and Conclusions
Chronic unresolved infection, trauma, and/or emotional stresses that trigger immune pathways with subsequent chronic hormonal and nervous system responses is proposed to perpetuate chronic neuropathic pain. Figure 3 provides a summary model of immune-hormonal contributions to neuropathic pain in fibromyalgia.
The ACR criteria and severity scales have defined fibromyalgia and The Wisconsin study has identified psychological and physiological subsets that are critical steps in its characterization. This type of testing could be further strengthened through the use of specific biomarkers. Potential markers of FM status include the RelA/p65 and p50 subunits of NF-kB, which are currently the focus of several clinical trials of other chronic painful conditions. Additional potential markers include: IL-6, IL-1b, TNF-a, PKC, transaldolase, CML, pentosidine and NGF. Substance P has been previously identified as a marker of pain, but is problematic as a marker for FM, since it has only been measured in the CSF. The search for markers that are truly specific to FM may continue to be a difficult task due to their overlap with other metabolic conditions, such as CFS, metabolic syndrome, type II diabetes, and IBS. Nonetheless, these markers remain important as they can indicate oxidative stress, cytokine activation, hormonal dysregulation and neuropathic pain. These potential FM markers need to be evaluated in clinical trials where they can be measured over time and correlated with patient symptoms.
Currently, family and general medical practice physicians are uniquely positioned to establish the FM diagnosis, determine subsets of FM patients, investigate potential triggers of chronic immune activation, advise patients, prescribe medications and refer patients to appropriate specialists or pain centers. Establishment of the FM diagnosis requires use of the ACR Widespread Pain Index (WPI) and symptom severity (SS) scale, but no longer requires the tender point examination. 3
Determination of FM subsets can be accomplished using the approach used in the Wisconsin cross sectional survey.53 Investigation of potential triggers of chronic immune activation needs to include sources of underlying infection, unresolved physical or emotional trauma, toxins and food sensitivities. These investigations may be accomplished through careful interviewing and well-designed questionnaires. Advising the patient should acknowledge the reality of their pain and other symptoms and provide rational approaches to resolution of those symptoms. Prescribing of medications needs to be sensitive to current and previous patient experience with medications, in addition to following current guidelines for stabilizing FM symptoms. Referral to appropriate specialists and centers would include those with expertise in physical medicine, psychology and nutrition. Physical medicine can address pain and functional deficits; psychology can address underlying emotional issues and trauma; and nutrition can focus on resolution of chronic inflammation, oxidative stress, and intestinal dysbiosis.
Where do we go from here for additional FM treatment options? Immune modulators have been used successfully in other painful conditions, such as rheumatoid arthritis. Immune modulators acting on the IL-6 - NF-kB cascade have considerable potential for FM, but only after ruling out or successfully treating any underlying infections. Numerous pharmaceutical blockers of NF-kB exist, but most are associated with serious side effects. Natural products may provide additional options as some are able to mediate pathways leading to NF-kB without the same side effects.105Medications that elevate individual hormone levels have been included in accepted treatment protocols in the case of serotonin and norepinephrine. However, elevations of other hormones, such as cortisol and thyroid hormones, are under investigation and remain controversial. Elevation of individual hormones may be problematic because of the number of different hormones influenced by the IL-6 - NF-kB pathway.
William Osler has said that "A desire to take medicine is perhaps the great feature which distinguishes man from animals" This desire, however may play havoc when a person starts taking medicines on their own (i.e. self-medicating), forgetting that all drugs are toxic and their justifiable use in therapy is based on a calculable risk 1.
Self-medication (SM) can be defined as obtaining and consuming drugs without the advice of a physician2. There is a lot of public and professional concern about the irrational use of drugs in SM. In developing countries like India, easy availability of a wide range of drugs coupled with inadequate health services result in increased proportions of drugs used as SM compared to prescribed drugs2. Although, over-the-counter (OTC) drugs are meant for SM and are of proved efficacy and safety, their improper use due to lack of knowledge of their side effects and interactions could have serious implications, especially in extremes of ages (children and old age) and special physiological conditions like pregnancy and lactation 3, 4. There is always a risk of interaction between active ingredients of hidden preparations of OTC drugs and prescription medicines, as well as increased risk of worsening of existing disease pathology 5 . As very few studies have been published in our community regarding usage of self medication we conducted this cross-sectional study in the coastal region of Pudhucherry, South India, t assess the prevalence and pattern of SM use.
Materials and methods:
The present study was a cross-sectional survey conducted in coastal region of pudhucherry, south India. For this study we recruited 200 patients randomly from both urban and rural communities (100 each) for a period of six months during 2009. Patients who were = 18 years of age and who were able to read and write the local language (Tamil) or English were included in the study after informed consent explaining the purpose of the study. Participants with intellectual, psychiatric and emotional disturbances that could affect the reliability of their responses were excluded from the study. To collect data regarding SM usage a structured questionnaire was prepared, after an extensive literature review.. The structured questionnaire contained 25 items in the form of closed and open ended questions. Initially the tool was validated by a panel of experts in the field of public health for the appropriateness of each item and assessment of content validity (0.91) and re-test reliability coefficient (0.89). Approval to conduct the study was granted by the Institute ethics committee prior to data collection. Each participant underwent a face to face interview to collect data followed by an informal educational counseling about potential adverse effects of consuming common SM. Data collected was analyzed using SPSS for windows statistical software version 14 (SPSS Inc., Chicago, Il, USA). Data was presented using descriptive statistics (i.e. numbers, percentage) and inferential statistics (i.e. Chi-square). A probability value of < 0.05 was considered to be significant.
Results
Basic demographic details:
The majority of the participants were female (56%). Most of the participants (60%) were between 26-45 years of age. There were an equal number of participants from the rural and urban community. Among the total 200 participants 70% were literate.
Findings related to usage of SM:
Overall, out of 200 participants, 71 % of them reported that they have used SM in the past. The frequency of SM use varied among the subjects with a minimum of at least one time to maximum of 5 times and above See Figure 1. When the participants were asked about the reasons for SM use, the majority of them - 41.5% - stated lack of time to visit a doctor as the main reason followed by minor illness and quick relief. See Table 1. The major source through which the participants learned to use SM were as follows, directly from pharmacist (57.3%), prescription of previous illness (21.5%), friends (12.5%), television (5.5%) and books (3%).See Table 2. The main indications for SM use were fever (36%), headache (35%), then cough/cold/sore throat (20%). See Table 3 for detailed data.
Figure 1: Frequency of self medication Use
Table 1: Reasons for Self Medication Use
Reasons
Number (%)
Lack of time
41.5
Minor illness
10.5
Economical
14
Quick relief
10
Learning opportunity
2
Ease and convenience
10.5
Avoiding crowd in visiting doctor
6
Unavailability of doctor
5.5
Table 2: Sources of Self Medication Use
Sources for self medication use
Number (%)
Directly from pharmacy without prescription
57.3
Prescription of previous illness
21.5
Friends prescription
12.5
Television media
5.5
Book
3
Table 3: Indications for Self Medication Use
Indications for self medication use
Number (%)
Headache
35
Stomach ache
3
Vomiting
1
Eye symptoms
0.73
Diarrhoea
2
Cough, cold, sore throat
20
Fever
36
Skin symptoms
0.27
Ear symptoms
2
While calculating chi-square to find out the association between usage of SM and selected demographic variables we found an association between residence (i.e. rural or urban) and gender; urban people were more likely to use SM than rural people (urban, 60/100 vs. rural 82/100, p value = .006). In relation to gender females were more likely to use SM in comparison to males (female, 78/112 vs. 43/88, p value= .002). Other variables were not significantly associated with SM use. Finally, when the subjects were asked about the side effects of their used self medications 93.5% of them said that they are not aware of the side effects and only the remaining 6.5% of them said they are aware of the side effects.
Discussion
The current study examined the prevalence and pattern of SM use in a coastal region of South India. The study findings revealed 71% of the people reporting SM use in the past, this prevalence rate in our study is consistent with previous finding3,6,7,8,9,10,11 The figure of participants who use SM is very high, which requires immediate attention. The frequency of self medication use in our study ranged from a minimum of one time to a maximum of 5 times and above, this finding was in line with the findings of a study by Nalini (2010)12.
Participants cited multiple reasons for use of SM like lack of time , quick relief from illness and ease and convenience, a similar reasons were cited in an another Indian study13. In the current study participants reported SM use in a variety of conditions like headache, stomach ache, cough and fever, this these finding are comparable with those of Sontakke et al (2011) 14. The reason for SM use may be mufti-factorial, in our study an association was found between gender and residence, i.e. female and rural people reporting more SM use, this finding was similar to two previous studies15,16 To establish the reasons why requires further research. One potential limitation of this study is the limited sample size, which we tried to overcome by adopting a random sampling method so as to generalize findings.
Conclusion
Factors influencing SM include patient satisfaction with the healthcare provider, cost of the drugs, educational level, socioeconomic factors, age and gender 17. Interactions between prescribed drugs and the drugs taken for SM is an important risk factor of which healthcare providers must be aware of.17,2
Easy availability of wide range of drugs without a prescription is the major factor responsible for irrational use of drugs in SM as, thus resulting in impending health problems (antimicrobial resistance, increased load of mortality and morbidity) and economic loss. The need for promoting appropriate use of drugs in the health care system is not only for financial reasons, with which policy makers and manager are usually most concerned, but also for health and medical care of patients and the community. There is need for authorities to strengthen existing laws regarding OTC drugs to ensure their rational sale and use. Also, specific pharmacovigilance is needed and the patient, pharmacist and physician must be encouraged to report any adverse events. Periodic studies on the knowledge, attitude about and practice of SM may give insight into the changing pattern of drug use in societies.
An 80-year old lady was referred to a gastroenterology clinic in August 2009 with deranged liver function tests; alkaline phosphatase 180 IU/L (35-120), alanine transferase 147 IU/L (<40), gamma glutamyl transferase 384 IU/L (<45) and globulins 45 g/L (20-35). She had initially presented to her general practitioner with symptoms of lethargy and malaise four months previously. She denied any symptoms of obstructive jaundice and there were no risk factors for hepatitis; she seldom consumed alcohol.
Past medical history included osteoarthritis, migraines and recurrent urinary tract infections; these had been investigated by urology and the patient had undergone cystoscopy and urethral dilatation in September 2003; despite this she continued to experience urinary tract infections and was therefore commenced on prophylactic nitrofurantion by her General Practitioner with approval by the Urologist. This was initially commenced at 50mg at night. This regime was continued for approximately three years however during this time she had a further three treatment courses of nitrofurantoin. In October 2005 her prophylactic dose was therefore increased to 100mg at night. Other medication included lansoprazole 30mg daily, pizotifen 500 micrograms at night, metoprolol 100mg twice daily, simvastatin 10mg at night, senna 15mg at night and furosemide 40mg daily.
On examination there was evidence of palmar erythema and Dupuytren’s contractures but no other stigmata of chronic liver disease. The liver was tender and palpable 4 cm below the costal margin. A liver ultrasound was performed which was normal. Liver screen and autoimmune profile are shown in table 1; notably a positive nuclear antibody was found (1 in 1280 IgG) with Hep 2 cell staining showing a homogenous (ANA) pattern at 1:320 IgG, and a nuclear lamin pattern at 1:1280 IgG;. Due to the positive ANA and raised globulins a suspected diagnosis of nitrofurantoin-induced autoimmune hepatitis was made and a liver biopsy performed.
Liver biopsy (figure 1) indicated a moderate hepatitis which was mainly portal based with multifocal interface hepatitis; these morphological appearances were consistent with those of an autoimmune hepatitis. The patient was advised to immediately stop nitrofurantoin and was commenced on prednisolone 30mg which caused a rapid improvement in LFTs (figure 2). This improvement was maintained following a step-wise reduction in steroid dose and prednisolone was discontinued after eight months of treatment. LFTs are currently normal one month following cessation of steroids
Discussion
This case raises two points of discussion. The first is whether the long term use of nitrofurantoin as prophylaxis for urinary tract infections is appropriate and based on solid evidence. Nitrofurantoin has many side effects and is well documented to cause liver derangement1,2,3. The patient described in this case had been taking nitrofurantoin for seven years and had received a large cumulative dose, on the basis that this was effective prophylaxis. The continuous, long term use of antibiotics as prophylaxis for urinary tract infections is debatable. Madersbacher et al4 recommend the use of prophylactic antibiotics but only after or alongside additional measures including behavioural change, the use of topical oestrogens and the use of alternative therapies; this view is supported by the European Association of Urology5.A Cochrane Review6 in 2004 found that antibiotic use did decrease the number of urinary tract infections compared to placebo but only for the duration of treatment; antibiotics do not alter the natural history of the underlying condition7. There is no clear evidence for duration of treatment and any trials have only been continued for six or twelve months6. It has been noted that all antibiotics had a worse adverse event profile compared to placebo. There was no consensus as to which antibiotic should be used although nitrofurantoin has been associated with a greater withdrawal rate6. One study8 comparing nitrofurantoin and trimethoprim revealed no significant difference in recurrence rates or side effects between the two antibiotics, although this involved a lower dose of nitrofurantoin than was used in this case, and a treatment duration of just 6 months. We would argue that due to the side effect profile of nitrofurantoin and the evidence base available, it is not appropriate to continue it for a duration beyond 6 months.
The second discussion point is whether nitrofurantoin was actually the cause for liver derangement in this case. As documented in a recent review article on the diagnosis of drug-induced liver injury, establishing with any certainty whether liver injury is drug induced can be very difficult3. The key issues are whether there is a temporal relationship between the drug and the onset of liver injury, and whether other causes have been excluded. In this case the patient had negative viral serology and a normal ferritin and caeruloplasmin but her positive autoantibodies raise the possibility of autoimmune hepatitis. Guidelines from the American Association for Liver Diseases9 suggests that the diagnosis of autoimmune hepatitis should be made on the following criteria
laboratory abnormalities (serum AST or ALT, and increased serum total IgG or gamma-globulins)
positive serological markers including ANA,SMA, anti-LKM1 or anti- LC1
histological changes consistent with autoimmune hepatitis i.e. interface hepatitis
This case meets these above criteria for autoimmune hepatitis however the presence of nitrofurantoin does confound the issue. Other case reports10 have reported nitrofurantoin to have caused autoimmune hepatitis based on the relationship between the timing of the drug and the onset of biochemical abnormalities. Bjornsson et al11 performed a comparative study of patients with autoimmune hepatitis and found drugs, particularly nitrofurantoin and minocycline were causally implicated in 9% of cases. When they compared the two groups no significant differences were found in the diagnostic parameters of biochemical, serological and histological abnormalities. In fact the only difference was that no drug-induced cases relapsed on withdrawal of steroids whereas nearly two third of those with non-drug-induced hepatitis relapsed. Bjornsson et al therefore argue in favour of autoimmune immune hepatitis being induced by drugs such as nitrofurantoin; rather than particular drugs simply unmasking sporadic cases based on these management differences.
The patient in this case so far has shown no signs of relapse following steroid withdrawal. We believe that this case does represent one of nitrofurantoin-induced autoimmune hepatitis. In view of the above we would urge readers to consider their use of nitrofurantoin for recurrent urinary-tract infection prophylaxis.
Doris-Eva Bamiou is a Department of Health HEFCE funded Senior Lecturer at the UCL Ear Institute, and Consultant in Audiovestibular Medicine at the National Hospital for Neurology and Neurosurgery. She is also Honorary Consultant at the RNTNE Hospital and Great Ormond Street Hospital. She sees both adults, with vertigo, hearing problems or auditory processing disorders, and children with auditory processing disorders and complex communication needs in her clinics. She works in an academic, multidisciplinary environment.
After completing specialty training in ENT in Greece, Ms Bamiou trained in Audiological Medicine in the UK. During her training, she spent a three-month fellowship in Professor Musiek’s department in the States (on a stipendium from Professor Musiek and a grant from the TWJ foundation), where she trained in the diagnosis and management of patients with auditory processing disorders. Her PhD degree is onauditory processing in patients with structural brain lesions.
She is Director of the MSc in Audiovestibular Medicine at UCL. In addition, she has been Director and Organiser of the Current Trends in Auditory Processing Disorders instructional courses for the past several years. She is immediate past Secretaryof the British Society of Audiology (BSA), and Chair of the Auditory Processing Disorders Special Interest Group of the same Society. She is adviser in Audiology to the JLO, and in the Editorial Board of the Audiological Medicine journal.
She has a keen interest in research. Interests include the aetiology of hearing loss, auditory processing disorders in the presence of other neurological conditions as well as in the normal population, auditory neuropathy, vestibular rehabilitation and overlap between psychiatric and vestibular disorders.
How long have you been working in your speciality?
I first became interested as an ENT trainee in Greece, in 1993. At the time I was at a paediatric hospital, and we did a lot of paediatric testing (distraction and ABR). In 1994 I moved to an adult hospital, where I came across and learned to test and manage adult patients with vertigo and hearing loss.
Which aspect of your work do you find most satisfying?
Solving clinical problems, teaching postgraduate students, designing research projects and interpreting research results give me equal satisfaction – I enjoy equally the patient/doctor or student/teacher interaction and the intellectual challenges.
What achievements are you most proud of in your medical career?
I set up the first adult clinic for patients with auditory processing disorders at the National Hospital for Neurology, and the first multidisciplinary clinic in this field, again at the same hospital.
Which part of your job do you enjoy the least?
Administration and form filling exercises.
What are your views about the current status of medical training in your country and what do you think needs to change?
I wonder whether trainees get enough proper training in their very early days on and whether the length of the training is sufficient for them to be able to function independently by the end of their training.
How would you encourage more medical students into entering your speciality?
We do Audiovestibular Medicine Taster days, and we encourage them to come and “shadow” us to see what it is really like.
What qualities do you think a good trainee should possess?
He/she should be kind, hard working, highly motivated to learn and able to develop independent thinking.
What is the most important advice you could offer to a new trainee?
It may be hard work training as a Doctor, but it’s all worth it!
What qualities do you think a good trainer should possess?
Amongst many other things, empathy, and the ability to teach each trainee at their own level.
Do you think doctors are over-regulated compared with other professions?
Not more than is required.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what shouldbe done to counter this trend?
I think it is difficult to reconcile managerial activities with a doctor’s role.
Which scientific paper/publication has influenced you the most?
Several. I tend to read a lot of papers for lectures etc so this changes every few weeks!
What single area of medical research in your speciality should be given priority?
I could not separate one more than others.
What is the most challenging area in your speciality that needs further development?
Rehabilitation (auditory and vestibular) of the patient with complex needs.
Which changes would substantially improve the quality of healthcare in your country?
More funding and more rationalized use of free NHS services, depending on the patient’s income.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Yes, by working closely and by educating managers.
How has the political environment affected your work?
Not at all.
What are your interests outside of work?
I read a lot of books of every kind, I go to the theatre and to art exhibitions.
If you were not a doctor, what would you do?
This will sound very boring. I would still like to be a doctor!
Liver abscess accounts for 48% of visceral abscesses 1 and presents with significant morbidity and mortality. The overall incidence of pyogenic liver abscess is 3.6 per 100,000 populations, 2 however; elevated pancreatic enzymes within the content of a liver abscess have never been reported in the literature.
CASE REPORT:
A 36-year-old African American male with a history of chronic pancreatitis presented to the emergency department for abdominal pain in the epigastric area along with nausea, vomiting, diarrhoea, fever. His symptoms began 3-4 days before presentation. The abdominal pain was dull in nature and 6/10 in intensity, non-radiating. His past medical history was significant for HTN, diabetes mellitus and chronic diarrhoea secondary to chronic pancreatitis.
On admission the patient was alert and oriented, blood pressure was 97/44 mm Hg, heart rate 16 beats per minute, respiration 16 per minute, oxygen saturation 94% on room air and temperature 102*F. Abdominal examination revealed hyperactive bowel sounds and tenderness in the epigastrium & RUQ. Liver span was 14 cm. The rest of the examination was unremarkable.
Laboratory work revealed: Haemoglobin 9.8 g/dl, WBC 22.1 Thou/mm3 with segmented neutrophils of 81% and 9% bands, BUN 54 mg/dl, Cr 4.7 mg/dl, total protein 10.4 g/dl, albumin 1.8 g/dl, total bilirubin 1.1 mg/dl, direct bilirubin 0.3 mg/dl, AST 98 IU/L, ALT 38 IU/L, alkaline phosphatase 250 IU/L, amylase 81 units/L, lipase 10 units/L, lactate 2.3 mmol/L and INR 1.39.
The patient was started on fluids and meropenem for broad spectrum coverage. However his condition worsened and he developed acute respiratory distress syndrome secondary to sepsis necessitating intubation. Due to his abdominal pain he underwent a computer tomography (CT) scan of the abdomen, which revealed pancreatic calcifications and multiple liver abscesses; the largest measuring 7.5cm in the right lobe of the liver (Figure 1).
Figure 1
As the patient’s condition did not improve, he underwent liver abscess drainage. Fluid analysis showed ph 4.0, LDH 39 units/L, glucose 81 mg/dl, protein 1.6 g/dl, lipase of 16 units/L and amylase 68 units/L. The presence of amylase and lipase in the liver abscess without any evidence of a fistula between liver and pancreas on CT scan was unexpected, therefore it was decided to leave the catheter in situ for continuous drainage. 3 Even though his blood and fluid cultures remained negative during the hospital stay he was continued on antibiotics, which may have meant that the initial antibiotic therapy rendered the blood cultures negative. The success of management was assessed with a hepatic CT 10 days post drainage and was demonstrated by the observation of improvement in the patient’s general condition, as indicated by normal temperature, decreased draining catheter output and the resolution of deranged laboratory values. The catheter was then removed and the patient was discharged.
DISCUSSION:
Liver abscesses develop via seeding through portal circulation, directly via spread from biliary infections or from surgical or penetrating wounds and also from systemic organs via haematogenous spread. In our case the most reasonable explanation was through the involvement of portal circulation due to recurrent pancreatitis.
The morbidity and mortality rate for liver abscesses ranges from 2 – 12 % depending on the severity of underlying co-morbidities. 2 The clinical manifestations, as in our case, are characterized by abdominal pain (50-75%), 4, 5 fever (90%), nausea and vomiting. Other symptoms may include weight loss, malaise and diarrhoea. On physical exam RUQ tenderness, guarding, rebound tenderness, hepatomegaly and occasional jaundice can be appreciated. The diagnosis of a liver abscess can be made by radiographic imaging followed by aspiration and culture of the abscess material. Liver abscesses can be either polymicrobial or monomicrobial, unlike in the case with our patient, whose abscess was sterile. Depending on the microbial results additional sources of infection should be evaluated. Drainage of abscesses can be percutaneous 6 or open surgical. Percutaneous drainage with coverage of antibiotics was successful in our patient.
CONCLUSION:
In summary, we present a case of pancreato-liver abscess in a patient with a history of chronic calcified pancreatitis. It was treated with antibiotics and percutaneous drainage, with satisfactory resolution. To our knowledge this has never been reported in the literature and more work needs to be done to understand the pathophysiology of elevated pancreatic enzymes in the context of a liver abscess in a patient with a history of chronic pancreatitis.
Myocardial ischemia from coronary artery vasospasm can lead to variety of presentation including stable angina, unstable angina, myocardial infarction and sudden death 1. Although, pathognomic clinical scenario includes symptom of chest pain, transient ST-segment elevation on the electrocardiogram(ECG), and vasospasm on a coronary angiography, atypical presentations have also been reported 2. Various known physiological factors including stress, cold, hyperventilation and pharmacological agents including cocaine, ethanol, 5-Fluouracil, and triptans can precipitate a vasospastic attack. 3-7.We report a case of ST-segment elevation due to right coronary artery vasospasm, in patient with hypoxic respiratory failure, and successful treatment with calcium channel blockers.
Case description
A 56 year old man was admitted for the repair of a large ventral incisional hernia. The patient had a prior history of morbid obesity, chronic obstructive pulmonary disease (COPD), hypertension and cigarette smoking. The postoperative course was complicated by bilateral pneumonia leading to respiratory failure requiring mechanical ventilation. An electrocardiogram at the time of intubation was essentially normal. Aside from bilateral rhonchi and crackles on lung auscultation, the rest of the physical examination findings were unremarkable. Arterial blood gases at the time of intubation demonstrated PH 7.33, PO2 58 mmHg, PCO2 65 mmHg, HCO3ˉ 20 mmol/L, suggestive of hypoxia and concomitant respiratory acidosis. Baseline laboratory studies including cardiac enzymes were within normal limits. The patient was treated with intravenous vancomycin for methicillin-resistant staphylococcus pneumonia. On postoperative day 4, the patient had recurrent episodes of transient ST-elevation on a bedside monitor (Fig.1).
Figure 1
These episodes lasted for 3-5 minutes and were associated with significant bradycardia and hypotension. In view of recurrent episodes, haemodynamic instability, and underlying risk factors of coronary artery disease, cardiac catheterization was performed. Coronary angiography revealed a 90% stenosis with haziness of the mid-right coronary artery without any other significant epicardial disease. An intravascular ultrasound (IVUS) was performed and was followed by administration of 100 mcg of intracoronary nitroglycerin; the lesion was reduced to almost 20%. (Fig.2).
Figure 2
The diagnosis of prinzmetals angina was made, based on clinical course and angiographic results and prompt therapy with diltiazem (120 mg per day) was initiated. The patient had no further recurrences of similar episodes during the hospitalization and on follow up at 3 months.
Discussion
The prevalence of vasospasm has been reported to be higher in Japanese and Korean population as compared to the western population. A recent multi-institute survey in Japan documented spasm in 921 (40.9%) of the 2251 consecutive patients who underwent angiography for angina pectoris 8. In contrast to the traditional risk factors for atherosclerotic coronary artery disease, the incidence of smoking, age and dyslipdaemia has been reported higher in patients with coronary vasospasm 9. Endothelial dysfunction is now considered to the major inciting factor in the pathogenesis of the vasospasm 10. Vasospastic angina (VA) with normal coronary arteries on the angiography, impaired endothelial-dependent and endothelial-independent vasodilatation has been frequently observed in these patients. Vascular tone is normally regulated by production of vasodilator factors like nitrous oxide (NO), prostacyclin and vasoconstricting agents like endthelin-1. In the presence of dysfunctional endothelium the agents that normally cause vasodilatation lead to paradoxical vasoconstriction, due to direct muscle stimulation, like acetylcholine.
Stress, whether physical or mental stress has been shown to induce coronary vasospasm and myocardial ischemia. In a study by Kim et al, coronary spastic angina was diagnosed in 292 patients out of 672 coronary spasm provocation tests. Among 292 patients, 21 (7.2%) had myocardial infarction and 14 out of these 21 had experienced severe emotional stress before the event 11. Recently, animal studies have also shown that high circulatory level of stress hormones (cortisol) exaggerate coronary vasoconstriction through Rho-Kinase activation 12. Hypoxia has been seen in animal models to predispose to vasospasm through superoxide formation, which leads to loss of vasodilator function of NO.(13)
The ECG changes that occur during attack include ST-segment elevation, and or peaking of T wave from total or subtotal coronary occlusion 1. In some cases spasm can involve more than one artery leading to ST-segment elevation in multiple leads, which may predispose to ventricular tachycardia or fibrillation 14. Coronary spasm is diagnosed by angiography, and spasm can occur at the site of atherosclerotic plaque or in normal segment of the coronary artery. In patients with equivocal diagnosis, provocative tests including administration of acetylcholine, hyperventilation to induce spasm may be required for the diagnosis.
Current first line therapy involves used of calcium channel blockers (CCB) alone or in combination with long acting nitrates. In a study comparing the effect of long acting nitrates (Isosorbide dinitrate 40mg/day) versus calcium channel blockers (amlodipine 5mg/day or long acting nifedipine 20mg/day) on coronary endothelium and vasoconstriction between patients with normal or minimally diseased coronary artery, treatment with long acting nitrates was associated with less favourable effects on coronary endothelial functions 15. Sudden withdrawal of CCB in patients with known vasospasm can lead to rebound of symptoms and may prove dangerous. In patients with refractory symptoms alpha-blockers, nicorandil have been used. Although beta blockers are believed to enhance vasospasm, Betaxalol, a selective beta-1 blocker, has been found to be effective in the treatment of variant angina due to its vasorelaxing effects 16. In addition, elimination of or control of all other risk factors or precipitants is very important for successful treatment. In drug refractory cases the percutaneous coronary intervention or coronary artery bypass graft has been performed for the ischemia relief 17.
Our patient had multiple precipitating factors for vasospasm. Endothelial dysfunction from severe physical illness and sepsis could have precipitated the VA. Furthermore, hypoxia from respiratory failure could have also been an inciting agent and cannot be ruled out. It is worth mentioning that intensive care unit patients frequently have coexistence of both the underlying risk factors and the precipitating factors for vasospasm, yet VA as a clinical syndrome is uncommonly seen or reported.
Conclusion:
The clinician needs to be aware of coronary artery vasospasm as it can pose a serious medical threat. Early diagnosis and treatment may result in improved outcomes from vasospastic angina.
Urinary incontinence is a common and distressing condition. It is an underreported problem because of the stigma associated with the condition and many patients simply suffer in silence.
Definition
Urinary incontinence is defined as involuntary leakage of urine.
Prevelence
It has been estimated that in the United Kingdom (UK) 9.6 million women are affected by bladder problems.1, 2 An overactive bladder itself affects five million adults, nearly 1 in 5 of the over-40 population.3 Prevalence is estimated to be 15% among healthy older adults and 65% of old frail adults.4 It is twice as common in women than men. It can affect women of all ages including after childbirth. In a cross-sectional survey of adult females attending a primary care practice in the UK, nearly half had urinary incontinence but only a small minority sought help.5 Forty-two per cent of women affected wait up to 15 years before seeking treatment.6
Types
1. Stress incontinence: This is involuntary urine leakage on exertion such as coughing/laughing/sneezing or exercise. Stress incontinence is due to an incompetent urethral sphincter. It is largely caused by childbirth thus young women can develop this problem. Other causes include pelvic surgery or hysterectomy.
2.Urge incontinence:This is involuntary urinary leakage associated with urgency (a compelling desire to urinate that is difficult to defer) and is due to detrusor overactivity leading to detrusor contraction. Urge incontinence often appears later in life. Frequency or nocturia, with low volume of urine voided, are signs of an overactive bladder that can occur with or without urge incontinence.7 An overactive bladder affects both genders and its prevalence rises with age, affecting 16.7% of those aged 40 in North America and Europe.3 An overactive bladder should be managed in the same manner as urge incontinence.
3. Overflow incontinence
4. Mixed incontinence: This is both stress and urge incontinence.
Risk factors
The most important risk factor is being female. Others are:
Obesity
Pregnancy and childbirth
Obstruction - tumours in the pelvis or impacted stool
Hysterectomy 8
Neurological disease
Cognitive impairment
Burden
In 2001 the annual estimated cost of dealing with bladder problems was £353.6 million.9 This included expenditure on pads. It is expected to be much higher now. Only a small proportion of the above amount was spent on drugs,10 the remainder being spent on secondary care and surgical treatment.
Bearing this in mind, it makes sense that the general practitioner (GP) is ideally placed to screen and manage these patients in primary care. It is not necessary to refer all patients to secondary care. With the ever-increasing pressure on GPs to reduce unnecessary referrals, there is now a scope for commissioning this service. However, management of an overactive bladder is not part of the Quality and Outcome Framework - could be one reason why GPs are not keen or enthusiastic.
Primary care management
History
A good history makes the initial diagnosis. Ask the woman whether she leaks on coughing, sneezing or exertion (stress) or whether she has an urgent need to pass urine before the leakage (urge). If she gives a history of both, she probably has mixed incontinence.
A history of nocturia or frequency with low urinary volume means an overactive bladder. This should be managed in the same way as urge incontinence. Previous surgery, or an obstetric and gynaecology history, may give further clues as to the type of incontinence.
Examination
Abdominal examination - any palpable mass. This may be a palpable bladder, an ovarian cyst, or a large fibroid.
Pelvic examination - Prolapse, enlarged uterus due to fibroid. Inspection of the pelvic floor may show visible stress incontinence on straining or coughing.
Per-rectal (PR) examination if suspicion of constipation or faecal incontinence.
Investigations
Routine urine check for sugar and protein.
Mid-stream urine (MSU) to exclude urinary infection.
Bladder diary for three days. Ask the woman to complete a diary of time and fluid volume - intake and output with episodes of urinary leakage and her activity at that time. The charts are available from pharmaceutical companies (keep the booklets in your examination room).
National Institute for Health and Clinical Excellence (NICE) states that the use of cystometry, ambulatory urodynamics or video-urodynamics is not recommended before commencing non-surgical treatment.11
Treatment
Treatment depends on the type of incontinence. Pregnancy and childbirth are known risk factors and there is evidence that pelvic floor exercises during pregnancy reduce the risk. The exercises should be taught by the midwife during antenatal classes.
For stress incontinence, the first line therapy is three months of pelvic floor exercises. These should be taught by the practice nurse. An instruction leaflet on its own is not enough. There is good evidence that advising about pelvic floor exercises is an appropriate treatment for women with persistent postpartum urinary incontinence.12
For urge incontinence, bladder training is the first step. The patient should be taught to gradually increase the time between voids.
Life style advice in all with a body mass index (BMI) over 30kg/m2.11
Household modifications, mobility aids, downstairs toilets can help an elderly patient struggling to reach the toilet in time.
Regular prompting of patients, by residential or nursing home staff, to visit the toilet can make a considerable difference rather than putting a pad on.
Patients with an overactive bladder should be advised to reduce their caffeine and alcohol intake.
Encourage the patient to drink two litres of fluid a day. Many women reduce their fluid intake hoping that this would help the symptom control, but less fluid intake can lead to concentrated urine which can result in bladder irritation.
Antimuscarinic drugs such as oxybutynin can be used if bladder training is not successful. NICE recommends that immediate-release oxybutynin should be given as a first line.11 Transdermal oxybutynin can be given if oral oxybutynin is not tolerated. Compliance is often a problem because of side effects e.g. dry mouth, constipation, dry eyes, blurred vision, dizziness and cognitive impairment. Contraindications are acute angle glaucoma, myasthenia gravis, severe ulcerative colitis and gastro-intestinal obstruction.
NICE does not recommend duloxetine as a first or second line treatment for stress incontinence. It can be considered if there are persisting side effects with oxybutynin.
Desmopressin or tricyclic antidepressants can be used in women with nocturia.
The role of hormone replacement therapy (HRT) is debatable. Although oestrogens may improve atrophic vaginitis, there is no evidence that oestrogens by themselves are beneficial in incontinence.13
Pads and catheters should only be issued on prescription if all treatment options have failed and the patient is waiting to see a specialist. These are coping aids.
Referral to secondry care
GPs should refer patients to a urogynaecologist or a surgeon who has experience in this field. Extra-contractual referrals are not favoured by Primary Care Trusts (PCTs) - try convincing your PCT!
Refer if there is:
Pelvic mass
Frank haematuria
Symptomatic prolapse
Suspected neurological disease
Urogenital fistula
Previous pelvic surgery
Failure of conservative measures and anticholinergic drugs.