Psychiatry is an unattractive profession. A bold statement to be made by medical students who have committed four years to this vocation, with an additional lifetime to follow. However, if facts and figures are to be believed medical students are turning their backs on this once valued and highly sought after profession and are chasing the glamour of emergency room medicine, serialised by popular television programmes. Within the UK approximately 4% of newly-qualified doctors specify Psychiatry as their first preference1, a remarkable low number, considering vast numbers qualify every August.
Maybe approaches like The Student Psychotherapy Scheme (SPS), implemented some 43years ago at University College London is needed. Whereby, medical students were given the opportunity to experience the doctor-patient relationship in a psychiatric setting. This led to a higher proportion of students choosing Psychiatry as a speciality, compared to a control group that were not given the opportunity.
The influence of a student psychotherapy scheme – a10-year retrospective study (2004)2
163 medical students undertook the SPS scheme, of which 77 replied to the questionnaire. Of these, 11, (14.3%), had become Psychiatrists, who had not thought about doing Psychiatry before entering the scheme. In the control group of 152, of which 128 responded, only two, (1.6%), had become Psychiatrists, who had not thought about this speciality at the same stage.
So why did the SPS have such an impact improving recruitment rates amongst medical students? From my point of view, it seems to be simply due to exposure. Exposure to the unknown and familiarisation of a speciality that is not regularly given the time and efforts during our medical training at University.
Our time in Psychiatry was punctuated by apprehension and a sense of intrigue. The hesitancy was rooted in preconceived notions that we were being sent to a sanatorium, whereby we would be battling to shake off patients that had latched on to my trouser legs in a bittersweet attempt to escape everyday - thankfully that never came into fruition. However, what did occur was far more surprising. We could see ourself pursuing a career in this speciality in the not so distant future. With acute medical emergencies, there seems to be an emphasis placed on ‘patching’ patients up and sending them home in an attempt to meet targets and tick all the boxes. With Psychiatry you play the ‘waiting game’, it requires patience, the efficacy of treatments rely on regular and lasting compliance, and the majority of benefits are seen in the long-term rather in an acute setting. Maybe the high rate of morbidity in psychiatric illnesses we see in our ageing population is dissuading potential Psychiatrists. Whatever the reason, there is a risk that this speciality will be understaffed in the future, creating a vacuum of care for those that really need it, especially when they do not have the mental faculties to be aware of their own needs.
The problem with Medicine as opposed to other careers is the wide range of specialities and sub-specialities that are available to students once they have finished the formal University training. There are the baseline individual specialities, such as Surgery, Medicine or General Practice – all of which have sub-specialities, intensifying their focus on particular area of clinical care available to patients. Perhaps that is why, in most cases, students allow their path to be dictated by their interests rather then the greater good of Medicine as a whole. As stated, there is a current crisis in Psychiatry, with only a 4% recruitment of newly qualified doctors. The 5-year undergraduate medical degree only allows a small window of exposure to Psychiatry and this is not enough to be able to explore the speciality and come to a conclusion, which would affect the students for the rest of their lives. Perhaps the short period of exposure continues to exacerbate the problem that most medical students view Psychiatry as a separate entity to Medicine, completely devoid of concrete management, unable to implement true and tested methods that would guarantee a cure.
There are 12 different sub-specialities in psychiatry3, of which we were exposed to General Adult and Old Age Psychiatry, from our time there we were able to experience the full spectrum of presentation, from the difficulties of dealing with mentally unstable patients, to the satisfaction of seeing slowed and gradual progress in someone’s mental wellbeing. What Psychiatry offers, that some fields tend to lack is rapport, created by extended patient contact and treating them as a whole rather then a specified issue. It dawned on me that even general practitioners do not have the luxury of getting to know their patients as well as Psychiatrists and that appealed to me a great deal, as I believe in the holistic approach to management. However, Psychiatry is still viewed as being disconnected from the rest of Medicine, perhaps due to the different history taking techniques, the lack of focus on the practical skills of medicine, the ‘trial and error’ method of therapy, whereby if one drug does not work another is given. Instead the focus lies on communication skills and other psychosocial aspects and this I find dissuades many of my colleagues, as there is nothing tangible for them to get to grips with and apply their knowledge to. In hindsight, Psychiatrists are not wholly responsible for just the mental health of a patient, but it does fall within their remit to identify, and manage co-morbidities they may have as well. A sound knowledge of all aspects of Medicine is required, and maybe the fact that ‘mind and body’ needs treating discourages future Psychiatrists.
Overall, there have been many times when we have been surprised at our own interest in Psychiatry. It is comforting to know that it is a welcoming speciality, unlike many other competitive specialities where there is intense pressure and any sense of enjoyment or achievement may be diminished. There are also immense opportunities open for research, even at this level as a medical student. Undoubtedly compared to other fields, Psychiatry offers a balance between work and personal life. Our only regret is that we did not have the opportunity to experience everything that Psychiatry has to offer, and make a more informative and well balanced decision on where my future lies within Medicine. Perhaps we will take the initiative to explore this field in my own time. One thing is for certain, Psychiatry is a dynamic field with many opportunities, and should not be disregarded for the flashing blue lights of emergency medicine.
COMPETEING INTERESTS
None Declared
AUTHOR DETAILS
MASHUD SOUROYER, 4th Year Medical Student, Bart’s and London School of Medicine and Dentistry, United Kingdom
MATHAVI UTHAYANAN, 4th Year Medical Student, Bart’s and London School of Medicine and Dentistry, United Kingdom
[1] The Royal College of Psychiatrists: Tackling the recruitment crisis in psychiatry Student Psychotherapy Scheme encourages medical students to choose psychiatry as a career [online]. 2004. Available URL: http://www.rcpsych.ac.uk/pressparliament/pressreleasearchive/pr550.aspx [Accessed 02/12/2008]
[4] Michael Gelder, Richard Mayou and John Geddes. Psychiatry: Third edition. Oxford University Press, 2005.
[5] Psychiatric Bulletin: What impact do undergraduate experiences have upon recruitment into psychiatry? [online]. 2007. Available URL:http://pb.rcpsych.org/cgi/content/full/31/2/70 [Accessed 02/12/2008]
We report a case of the rare coronal unicondylar fracture of the distal femur called Hoffa fracture. Hoffa fracture is a rare injury consisting of unicondylar tangential posterior fracture of the distal femur. These fractures are due to high energy trauma and sometime not easy to visualise on routine imaging, and therefore could represent a diagnostic challenge to the accident department and to the orthopaedics surgeon. Clinically however, our patient had obvious knee swelling, localised tenderness and was unable to weight bear. Plain radiograph and CT scan confirmed the fracture and was treated surgically with cancellous screws.
Case Presentation
A thirty-four year old male injured his left knee whilst turning on a motocross bike. He put his left leg on to the ground with his knee in 20 degrees of flexion to stabilise himself whilst turning a left hand corner at about 30 mph. He did not crash, but was unable to weight bear afterwards.
The initial AP and lateral radiographs showed a coronal fracture of lateral condyle of the distal femur.
[FIG 1: AP radiograph right knee / Lateral radiograph right knee].
This fracture could have been easily missed on the plain radiograph. Further imaging with the CT scan confirmed the fracture and its pattern.
[FIG2: Axial CT of distal femur / Saggital CT of distal femur].
He had an open reduction and internal fixation via a lateral approach, vastus lateralis was reflected off the lateral intermuscular septum and the knee joint opened. Maintaining the knee flexed during the surgery relaxes the posterior capsule, gastrocnemius and protects the neurovascular structures. Soft tissue attachments of the fractured fragment constitute the sole source of blood supply and must be preserved. The joint was carefully inspected for associated injuries. After reduction the fragments were temporarily fixed with Kirschner wires. Partially threaded cancellous screws were used in the lag mode to secure compression across the fracture.
FIG3: Image Intensifier of ORIF with cancellous screw]
Discussion
This fracture pattern was initially described by Hoffa in 1904 1 hence the name for this fracture. The Hoffa fracture is an intra-articular fracture of the knee analogous to the capitellum fracture of the elbow 2. This injury is the result of violent force and generally occurs in young adults. There is usually a combination of forces: direct trauma, possibly with an element of abduction, the ground reaction is transmitted through the tibial plateau and the axial compression on a flexed knee concentrates the force in the posterior half of the femoral condyles1. In flexion the lateral condyle is the leading part of the knee to receive the impact1. Although the Hoffa fracture may be of either condyle4 the preponderance of lateral condylar fractures suggests an anatomic-biomechanical vulnerability due to the physiological valgus.
Few cases have been reported in literature with associated femoral shaft fracture 6, ligament entrapment with irreducible knee dislocation5, open and bicondylar fractures7. Our case is unique as it is a closed injury, uniconylar fracture with no associated ligamentous or meniscal disruptions. Open reduction has been shown to be mandatory for good long-term function 2, 3. High index of suspicion, further imaging with CT scan / 3D reconstruction, open reduction and internal fixation is necessary for good outcome following these types of fractures.
Post-operative urinary retention affects up to 38% of the 200,000 patients undergoing elective TKRs or THRs in the UK every year, according to literature.
Objectives:
This study aims to identify both patient and anaesthetic factors that predispose to urinary retention, and in doing so develop a protocol of pre-operative urinary catheterisations that will minimize its incidence and subsequent complications, as well as hasten patient recovery and discharge.
Methods:
Analysis of prospectively collected data of 54 patients over a three-month period at a British district general hospital.
Results:
10% of patients in the study developed urinary retention, and 60% of these developed renal failure complicating recovery and lengthening stay. All were male, and a history of renal disease and a current elevated serum creatinine were identified as common factors in these patients.
Conclusions:
A protocol of pre-operatively catheterizing males with either a history of renal disease or a current elevated creatinine is suggested – this would potentially reduce incidence rates of urinary retention by 80% whilst only increasing the rate of unnecessary catheterizations by 2%.
Introduction:
Every year, approximately 200,000 people undergo elective total hip and knee replacement surgery in the UK 1. There is limited available literature on the incidence of post-operative urinary retention and even less regarding the onset of subsequent renal failure which, besides posing immediate medical problems, necessitates treatment and can significantly prolong recovery – all of which have personal and financial implications for both patient and healthcare trust.
Summary of Current Literature:
Surprisingly little research is available which offers data on the association on the incidence of, risk factors for, and associations with urinary retention for patients undergoing elective total hip or knee replacement surgery. The following table summarises seven studies conducted between 1980 and 2007:
Study
Year
n
Males
Females
Retention
Sepsis
TKR
THR
Overall
Wroblewski & Del Sel 2
1980
195
195
6.20%
Waterhouse et al. 3
1987
103
103
0
10.70%
O' Riordan et al. 4
2000
116
47
69
18.10%
Kumar et al. 5
2004
19%
22%
0.93%
Cronin et al. 6
2005
118
118
0
38.10%
Kumar et al. 7
2006
142
19.70%
2.10%
Lingaraj et al. 8
2007
119
10
109
10%
Analysing the available literature, the following conclusions can be made.
Males are more likely than females to develop urinary retention.
Risk factors include a history of urinary retention, the use of epidural analgesia and patient-controlled analgesia (PCA).
Retention rates varied between 10% and 38.1% (mean 19.6%).
Deep sepsis rates varied between 0.93% and 2.1% in the total post-operative group, rising to 6.2% in those developing urinary retention.
Objectives:
This study aims to develop a policy of pre-operative catheterisation, anaesthetic technique and post-operative analgesia in patients undergoing elective total hip and knee replacement surgery that will:
Minimize the incidence of urinary retention.
Minimize the incidence of subsequent complications.
Hasten patient recovery and discharge.
Methods:
A prospective study was conducted between February and April 2008 in the operating theatres and on the Orthopaedic wards at Bedford Hospital, a district general hospital in Bedfordshire, UK. Data was collected that would enable the following questions to be addressed:
Are these patients catheterised pre-operatively?
Of those who are not, how many develop urinary retention?
Is any particular anaesthetic technique associated with an increased incidence of retention?
Is antibiotic prophylaxis administered for catheterisation?
How frequently does renal failure arise in those patients who develop urinary retention?
Can a protocol be created which might reduce the incidence of retention?
How effective and efficient would this be?
54 patients undergoing elective total hip and knee replacements were recruited into the study. Of these, 4 were catheterised pre-operatively and hence were excluded (n = 50).
Data Collection:
The primary source of data collection was from patients’ notes and anaesthetic charts, assessed pre- and post-operatively. Data was gathered in the following areas:
Demographics – Name, Age, Sex
ASA Classification – 1 to 4
History of Renal disease
History of Urological disease
Pre-operative Creatinine
Nature & Date of Operation
Type of Anaesthetic Technique employed
Onset of post-operative Urinary Retention necessitating catheterization
Duration of Epidural Analgesia (if applicable)
Administration of Antibiotic Prophylaxis for catheterization
Progress from urinary retention to Renal Failure
Results:
As mentioned, 4 of the original 54 patients were excluded from the study as they had already been catheterised pre-operatively. All were female, 75% of whom were over the age of 80; it appears that the main indication for pre-operatively catheterisation was existing urinary incontinence.
There was a female preponderance amongst the sample population, with females outnumbering males by a ratio of 3 to 2. In terms of the sample population’s co-morbidities and anaesthetic risk, the majority of patients were classified as ASA 2 (60%) by the assessing anaesthetist, with ASA 3 patients (26%) outnumbering ASA 1 patients (14%) by a ratio of approximately 2 to 1 in the remainder. Over the period covered, knee replacements (70%) outnumbered hip replacements (30%) by a ratio of 7 to 3.
A range of anaesthetic techniques were employed, including:
Combined Spinal Epidural (CSE)
Spinal Anaesthetic (Spinal)
General Anaesthetic + Epidural (GA + Epidural)
General + Spinal Anaesthetic (GA + Spinal)
General Anaesthetic + Lumbar Plexus Block (GA + LPB)
General Anaesthetic + Femoral Nerve Block (GA + FNB)
General Anaesthetic +/- Patient Controlled Analgesia (GA + PCA)
Spinal anaesthetics appeared to be most commonly employed, either alone or in conjunction with a general anaesthetic. GAs in combination with a nerve block was also often used, followed by CSEs.
In total, there were a total of 5 cases of post-operative urinary retention, all of which necessitated catheterisation. This results in an incidence rate of 10% across elective total hip and knee replacements. Of these anaesthetic techniques, spinal anaesthesia was associated with the highest risk of post-operative urinary retention (22.2%), followed by GAs (20%), CSEs (14.3%) and GA + FNBs (14.3%). No cases were reported for patients who underwent GA + Spinals (n = 13), GA + LPBs (n = 8) or GA + Epidurals (n = 1).
Of those patients who had undergone epidural anaesthesia, whether in combination either with a GA or a spinal, no documentation was found regarding the duration for which they had been active in 25% of cases. In the remainder, the epidural had been functional for less than 24 hours in 50% of cases.
All five patients who developed post-operative urinary retention were male; three of whom were below the age of 80. Only three of these patients received the recommended antibiotic prophylaxis on catheterisation (60%), and on following up their subsequent inpatient progress and serum creatinine, it appeared the same number progressed to renal failure (60%).
Analysis:
Two factors were identified in this study which may have predisposed these five patients into developing post-operative urinary retention. The first is a history of renal disease – 4% of the total sample had such a history (n = 2) and both went on to develop retention. The second is a currently elevated serum creatinine – 6% of the total sample had this at the time of surgery (n = 3), and of these, two went on the develop retention. The remaining patient who developed retention had neither of these risk factors.
The table below compares the results found in this study with those described in existing literature, namely the aforementioned publications. As can be seen, the post-operative urinary retention rate was on the lower extreme of that noted in the literature; only the studies by Waterhouse et al.3 and Lingaraj et al.7 demonstrated similar rates.
Factor
Study
Literature
Pre-op Cath Rate
7.4%
Unknown
Post-op Retention Rate
10%
10 - 38.1%
Hx of Renal Disease
Increased
Unknown
Elevated Creatinine
Increased
Unknown
Male Incidence
Increased
Increased
Epidural Incidence
Average
Increased
This study concurred with the existing opinion that males have a higher incidence of retention, but the study population was insufficient to draw any specific conclusions regarding the influence of epidural anaesthesia on post-operative urinary retention. It was noted however, that in half of the cases for which data was available, the epidural was functional for less than 24 hours – one might argue that the risk/benefit ratio of epidural anaesthesia would cause it to be a relative contraindication if only employed for relatively short durations, particularly if the patient is admitted to a ward on which nursing staff are unfamiliar with its care.
Conclusions:
Existing literature fails to comment upon the impact of the aforementioned risk factors for retention highlighted in this study, namely a history of renal disease and a current elevated serum creatinine. However, these two factors in conjunction with the increased incidence in males allows for the creation of a system by which patients who are at high risk of developing post-operative urinary retention may be successfully identified and catheterised pre-operatively, hence preventing the problem from arising.
If a protocol had been established in which males with either of these two factors were catheterised pre-operatively, 5 patients from the sample population of 50 would have qualified; this includes 4 of the 5 patients who developed urinary retention post-operatively. In addition, only 1 patient who did not develop urinary retention post-operatively would have met these criteria and been unnecessarily catheterised pre-operatively. These figures are demonstrated in the graph below.
On the basis of these findings, one can deduce that a protocol indicating pre-operative catheterisation in males with either a history of renal disease and a current elevated serum creatinine undergoing total hip and knee replacement surgery would have a profound impact on the incidence of post-operative urinary retention, essentially reducing it by 80%. Unnecessary catheterisations as a result of this protocol would be minimal, affecting only 2% of patients.
Although this study has obvious limitations in terms of its size and its single-centred nature, findings were comparable to existing literature and are likely to be representative of incidence rates on a national, if not international basis. Further research, ideally with a larger population spread across multiple centres would allow for more accurate data to be collected, which in turn would allow for a more effective and efficient protocol to be developed.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
SUMIT DUTTA, MBBS, Speciality Trainee Registrar in Emergency Medicine, Bedford Hospital, United Kingdom
CORRESPONDENCE: Sumit Dutta, Specialty Trainee Registrar in Emergency Medicine, Bedford Hospital, Kempston Road, Bedford, MK429DJ, United Kingdom.
Waterhouse N, Beaumont AR, Murray K, Staniforth P, Stone MH. Urinary Retention after Total Hip Replacement. A Prospective Study. Journal of Bone and Joint Surgery, British Volume. 1987 Jan; 69 (1): 64-6
O’Riordan JA, Hopkins PM, Ravenscroft A, Stevens JD. Patient controlled analgesia and urinary retention following lower limb joint replacement: prospective audit and logistic regression analysis. European Journal of Anaesthesiology. 2000 Jul; 17 (7): 431-5
Kumar P, Mannan K, Chowdhury AM, Kong KC, Pati J. Urinary retention following arthroplasty. Urology, 2005 Sep; 66(3); Supp I: 22
Cronin JJ, Shannon FJ, Bale E, Quinlan W. Prediction of post-operative urinary retention following hip and knee arthroplasty in a male population. European Journal of Orthopaedic Surgery and Traumatology. 2007 Jan; (17): 47-50
Kumar P, Mannan K, Chowdhury AM, Kong KC, Pati J. Urinary retention and the role of indwelling catheterization following total knee arthroplasty. International Brazilian Journal of Urology 2006 Jan-Feb; (32): 1
Lingaraj K, Ruben M, Chan YH, De Das S. Identification of risk factors for urinary retention following total knee arthroplasty: a Singapore hospital experience. Singapore Medical Journal. 2007 Mar; 48 (3): 213-6
Psychotherapy, psychological treatment and psychological techniques are the motherhood and apple pie of psychiatry. No one can be found to say a bad word against them although the word psychotherapy is often preceded with some qualifier such as “sensible” to indicate that the farther shores of the discipline may not have much place in psychiatry. Sadly though psychotherapy and its congeners, unlike motherhood or even apple pie are is far from widespread in the practice of many psychiatrists and training in the topic is woefully patchy across the country. In this occasional series I hope to introduce the reader to some key concepts in the field not so much from a scholarly perspective in an academic paper decorated with references (although there will be reading for those with sufficient interest and leisure) but from the perspective of practice. I hope to show how each of these psychotherapeutic concepts can be applied both to the practice of formal therapies and to more general aspects of psychiatric practice.
Topic 1 - Alliance
The term alliance refers to the maintenance of a certain kind of positive relationship between the patient and their therapist or doctor. We know that the quality of the alliance in psychotherapy is quite predictive of the likely outcome of treatment so that, while a good alliance does not guarantee a good outcome a bad alliance often ensures a poor outcome. Alliance is something of a portmanteau term since it covers aspects both of trust and liking but also of faith in the skill of the doctor or therapist and a willingness to make positive efforts towards furthering the aims of treatment on the part of the patient. Sometimes this last aspect of alliance – the willingness of the patient to put their best foot forward is referred to by the more descriptive term “working alliance”. Treatments differ in the extent to which they require anything resembling a working alliance. For example many surgical procedures require only that the patient consents and submits to treatment. Other treatments in medicine require that the patient complies with treatment by which is meant carrying out medical instructions accurately. As treatments become more complex and conditions more chronic the degree to which the patient must be an active agent in the administration of their own treatment increases with diabetes being a classic example.
In psychiatry some treatments such as submitting to depot neuroleptic administration require minimal levels of compliance and little in the way of alliance. However other treatments and particularly those which involve making substantial changes in lifestyle require that the patient be almost entirely responsible for the carrying through of their treatment. As such they resemble fitness training or education far more than they resemble “treatments”. In these situations the alliance made between the patient and their doctor is a critical factor in determining the success or failure of treatment.
The making of alliances in ordinary life is not a special skill but something which we all possess however psychotherapists and psychiatrists need to make alliances with people that others shun or who are hostile, ambivalent, distracted or cognitively impaired. The will and the skill to form an alliance with such individuals take training and crucially practice. It can be thought of as comprising three essential parts.
First – preparation.
Second – the interaction (s)
Third – follow up.
Let’s see how these stages play out in a clinical situation. In which a man’s helpers struggle to maintain a fragile alliance.
Rodger was a large and heavily tattooed man. He walked with a rolling gait and with his arms held out from his side as though he was always ready for a fight. He had suffered several head injuries as a younger man and could be both impulsive somewhat unpredictable and volatile. He used drugs and, at bad times would self harm by slashing himself with tin can lids. Staff in the day hospital had managed to engage him to an extent some months ago but he had become enraged when another patient had started winding him up calling him a stupid fathead. He blundered around the unit like an angry bull threw a chair and made threats to kill the other patient. As a result he was excluded from the unit. Rodger simply could not understand why this had happened and asked to see his key worker to make a complaint.
It would certainly be fair to say that the working alliance with Rodger has all but evaporated. The key worker was faced with the task of explaining Rodger’s new situation to him, rebuilding the alliance and possibly defusing an aggressive encounter. She prepared herself in two ways. First she took care with her own safety and the safety of others in the setting. She warned other people she was seeing Rodger and carried a personal alarm. Her objective was to free her mind from too many anxious thoughts about being assaulted as well as to ensure her physical safety. She also prepared herself by reflecting on Rodger’s world imagining it as to him always potentially threatening either physically or psychologically where he felt under threat of being belittled or disrespected in ways he secretly worried but could not afford to admit to himself were true. Last she prepared Rodger by writing to him and telephoning him before the meeting to tell him what was going to happen and why. She made a point of speaking to him in quite formal and respectful terms as “Mr X” and, knowing that he would be very anxious when he arrived she made a point of starting the appointment on time.
The key worker began by asking Rodger what he felt about the meeting and what was on his mind. Starting with the patient’s perspective and seeking to understand things from their point of view is a critical element of forming an alliance. It communicates to the patient that alliance is a two way affair. Rodger began angrily about the whole business and started to wind himself up about the person who had been rude to him and also about the unfairness of being excluded. The key worker agreed that it must feel very unfair to him. Rodger went on crossly that he was always given the “prick tease” invited into places and then chucked out. The key worker agreed that Rodger was often chucked out of things and asked him why he thought that had happened. Rodger said people were down on him and they all picked on him.
In terms of the alliance Rodger and his key worker are already doing better than before. Rodger is able to speak about what is on his mind and the key worker is able to hear it without becoming defensive or frightened. However this is not yet working alliances because the Key worker has not done much other than agree with Rodger’s perspective in as far as it seems correct.
So now the key worker said that he wondered if Rodger had ever thought patients and staff were frightened of him. Rodger bridled and said angrily “there you go you are all the same I don’t care about them what about me. No one asks how I feel.” The key worker had moved too quickly and the alliance, already fragile has collapsed again. So the key worker said. “I have done the same thing as other people do to you, you always feel you get told off and no one ever listens to your point.” Rodger agreed and again warmed to his theme describing the way in which he was always being put down and treated unfairly. As he became more vehement he stood up and began to pace around the room gesticulating. At times he would refer to “them” putting him down but on other occasions he would say “you”. The key worker said, “When you walk around and raise your voice I get frightened of what you might do and it is hard for me to listen to you properly when I feel scared.” Rodger looked startled and sat down abruptly saying rather defensively “I am not going to do anything”
The key worker’s response which was neither threatened nor defensive but tried to state plainly the effect that Rodger’s behaviour was having explicitly referred to the way in which some behaviour can threaten the alliance. The key worker then went on to explain that although Rodger did not feel that his behaviour was threatening other people interpreted it that way. This allowed the key worker to mention the incident in the day hospital again and to say that people had been frightened of Rodger. At this point the Key worker felt Rodger had taken the point and so he suggested they meet again to talk about it some more next week. Notice that the key worker did not try to “close the deal either clinically by, for example making a contract for good behaviour with Rodger or managerially by seeing if Rodger was satisfied by how his complaint had been heard. This was because the key worker judged that these moves might threaten the alliance again and a further outburst could wipe out Rodger’s memory of his new understanding of himself as potentially frightening others and his new understanding of others as frightened.
The key worker followed up on the meeting with Rodger in a number of ways. First by feeding back to the staff at the day hospital, By doing this the key worker was helping them to repair, even in Rodger’s absence, their sense of an alliance with him and maybe preparing the ground for Rodger’s return. The key worker also telephoned Rodger later in the week to find out how he was timing the phone call to a time when Rodger would normally have been in the day hospital. The Key worker began the call by saying “I was thinking about how you might feel today”. By doing this the key worker conveyed to Rodger that Rodger was in his mind even when Rodger himself was not in the room and that Rodger is an object of concern to him. Giving patients the sense of being “held in mind” is crucial to fostering the alliance. When medical staff gives a sense that they do not have the patient in mind there is almost always a severe rupture in the alliance as for example when the doctor starts reading the patient’s notes while they are in the room.
Conclusion
The story of Rodger and his key worker may seem to some over simple. In such natural seeming interactions the skill is cleverly disguised. Although the Key worker appeared spontaneous and appeared not to be considering his words he was in fact weighing them very carefully. He chose language that was appropriate to Rodger’s intellectual level. His statements were brief and contained only a single point. Thus the key worker matched Rodger’s cognitive level. The Key worker also managed the feeling tone in the room very carefully intervening to calm but not truncate potentially explosive feelings and ultimately promoting a little nugget of increased knowledge about the relationships between Rodger and other people. By maintaining an alliance and by carefully moving it into being (even if briefly) a working alliance the key worker managed a little step of progress with Rodger.
COMPETEING INTERESTS
None Declared
AUTHOR DETAILS
CHESS DENMAN, Consultant Psychiatrist in Psychotherapy, Complex Cases Service, Springbank Ward, Cambridge And Peterborough Mental Health Foundation Trust, Fulbourn Hospital, Cambridge, CB15EF
Email: Chess.Denman@cpft.nhs.uk
Follow up Reading:
For those who want a basic text: Oxford Textbook of Psychotherapy, Glen O Gabbard Judith S. Beck & Jeremy Holmes, Oxford University Press 2005
For those who would like more: Cognitive Behaviour Therapy for challenging Problems. Judith Beck, Guildford press New York 2005, Chapters 4,5,6
For the very keen: Safran J. D. & Muran, J. C. (2006). Has the concept of the alliance outlived its usefulness? Psychotherapy, 43, 286-291.
Septic shock still remains one of the leading causes of death in hospital patients. Greater awareness, understanding of the condition .and the knowledge of most effective treatment measures available can decrease the rate of mortality. Making an early, accurate diagnosis of septic shock is the key to increasing survival rates. Excessive inflammation, excessive coagulation and suppression of fibrinolysis are the hallmarks of Sepsis. Infection control, haemodynamic stabilization, and modulation of the septic response are the cornerstones of treatment. The management is influenced more by appropriate treatment with antibiotics and fluids than by specific intensive care. Septic response can be modulated by the use of Steroids and Activated Protein C and with tight glucose control. Low Tidal Volume ventilation and high volume Haemofilteration are other beneficial strategies in Sepsis. As septic shock worsens and fails to respond to all therapy, one must be prepared to limit and withdraw treatment.
Septic shock still remains the one of the leading causes of death in hospital patients. Barely more than 50% of the patients with severe sepsis survive their hospital admission. This unacceptable high mortality can only be reduced if there is greater awareness and understanding of the condition .and the knowledge of most effective treatment measures available. Unplanned admissions to the Intensive Care Unit (ICU) and potentially preventable deaths on wards are associated with a failure to institute early preventive conditions. Greater than 40% of the intensive Care Unit admissions are potentially preventable with improved ward care.
Survival of patients with Septic shock appears to be better if shock develops while the patient is in Intensive Care Unit rather than on general ward despite greater severity of illness in the intensive care group [1].This suggests that the closer observation and earlier treatment can influence the outcome of sepsis.
INCIDENCE:
Septic shock is an increasingly common problem. The incidence of sepsis is increasing year by year. The reasons for this increase are that the people are living longer and this aged population are the most vulnerable to sepsis. We are using advanced technology to sustain life and there has been a rise in the number of immunocompromised patients due to aggressive cancer therapy and the increased prevalence of HIV. The widespread use of broad spectrum antibiotics has increased the rate of both antibiotic resistance and nosocomial infections.
A prospective, multicentre, observational study, recently conducted to evaluate the epidemiology of Sepsis and other characteristics of Intensive Care Unit patients in European countries (called the SOAP study) was endorsed by the European Society of Intensive Care Medicine [2]. This observational study showed a marked difference in the frequency of sepsis between countries, and higher frequencies of sepsis were mirrored by higher mortality rates. (Fig.1)
Fig 1: Incidence of Sepsis in European Countries
There was a direct relationship between the number of organs failing and the Intensive Care Unit mortality. Patients with no organ dysfunction on admission had mortality rates of 6% whereas those with four or more organ failures had mortality rates of 65 %. [2] (Fig. 2)
Fig 2: The SOAP study
As compared to the incidence of other pathologies in Europe the incidence of severe sepsis is higher (32%) [2] (Fig 3)
Fig 3: Incidence of different pathologies in Europe
In septic patients, older age, positive fluid balance, co morbid diseases on admission; cancer and cirrhosis are the most important variables of mortality.
DEFINITIONS
Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response Syndrome (SIRS). This is characterised by body temperature outside 36oC - 38oC, HR >90 beats/min, respiratory rate >20/min, WBC count >12,000/mm3 or < 4,000/mm3. (Fig 4)
Fig 4: Definitions
There are three recognised stages in the hierarchy of the inflammatory response, with progressively increased risk of organ failure and death. Patients with infections plus two or more elements of the SIRS meet the criteria for sepsis. Those who have end organ failure are considered as having severe sepsis; and those who have refractory hypotension along with the above said criteria are consider to be in septic shock (Fig. 5)
Fig 5: Definitions
PATHOPHYSIOLOGY:
Sepsis is a complex condition starting from an infective stimulus and resulting in an exaggerated immune response. The inflammatory response that was initiated to fight the infection ultimately leads to damage of various organs thorough out the body.
During the onset of sepsis, the inflammatory system becomes hyperactive, involving both cellular and humoral defence mechanisms Endothelial and epithelial cells, as well as neutrophils, macrophages and lymphocytes, produce powerful pro-inflammatory mediators, especially tumour necrosis factor- (TNF-), interleukin (IL)-6, IL-1 and IL-8. Simultaneously, robust production of acute-phase proteins, such as C-reactive protein, occurs and humoral defence mechanisms such as the complement system are activated, resulting in production of pro-inflammatory mediators, including C5a, the complement split product. C5a ultimately enhances cytokine and chemokine production. Furthermore, the coagulation system becomes activated through various mechanisms, often resulting in disseminated intravascular coagulopathy.
The hallmarks of the sepsis are excessive inflammation, excessive coagulation and suppression of fibrinolysis. In addition endogenous Activated Protein C which modulates coagulation, controls inflammation and supports fibrinolysis is also decreased. There is considerable variability in response which is almost certainly to a large degree genetically determined. Those with a tendency to produce excessive cytokines and TNF will have a greater inflammatory response. Simultaneously, the initial vascular damage results in neutrophil activation, neutrophil-endothelial cell adhesion, and further elaboration of inflammatory cytokines. In tissues already prone to dysfunctional oxygen uptake and metabolism, this vascular injury promotes further tissue hypoxia through regional hypo perfusion. This uncontrolled cascade of inflammation and coagulation fuels the progression of sepsis, resulting in tissue hypoxia and ischemia with resultant organ dysfunction and death.
DIAGNOSIS:
Diagnosis of sepsis is not easy. Making an early, accurate diagnosis of septic shock is a key to increasing survival rates. The signs and symptoms of severe sepsis may be subtle. Although the components of SIRS are non specific, the combination of suspected infection and the presence of SIRS may help alert the clinician to a possible diagnosis of sepsis. Although hypotension is another clinical sign that may signal the onset of septic shock, patient may present with sever sepsis and clinically significant global tissue hypoxia in its absence. Metabolic marker such as serum lactate, arterial base deficit may help to identify the severe cases. A single lactate measurement of 4mmol/l or more at initial presentation is associated with an increased rate of mortality [3]. There may well be signs of altered mentation and abnormalities of renal and liver function test, as well as coagulation abnormalities. At least two blood cultures and cultures of other sites as indicated before commencement of antibiotic therapy. Diagnostic studies such as Ultra sound and CT scan should be performed promptly.
D dimmers are grossly elevated in sepsis. Levels of Protein C are lowered which has therapeutic implications. The potential role of biomarkers for diagnosis of infection in patients presenting with severe sepsis remains undefined. Perhaps the most common considerations as diagnostic biomarkers for sepsis have been C-reactive protein and procalcitonin. Despite initial enthusiasm for their potential diagnostic strengths,[4] they have more recently been related to the growing heap of biomarkers that have failed to accurately differentiate sepsis from similar critical illnesses.
The most exciting development in the last 2 years is the recognition of "soluble triggering receptor expressed on myeloid cells-1" (sTREM-1) as a potential biomarker for sepsis. [5] For this marker, a level greater than 60 ng/mL was more accurate than any other clinical and laboratory findings indicating infection
TREATMENT:
The development of new treatment modalities has resulted in a spate of treatment algorithms, often promulgated by medical societies and healthcare improvement organizations. As these modalities have rolled out, increasing levels of evidence have emerged to support or refute their utility in treating patients with sepsis. One of the greatest endeavours to date is the Surviving Sepsis Campaign (SSC) [6] that was originally launched in 2002 with the stated goal to reduce mortality by 25%. The primary method to achieve this goal was the development of evidence-based sepsis care guidelines that were published in 2004. [6] and recently revised in 2008.
The Institute for Healthcare Improvement (IHI) has highlighted sepsis as an area of focus and has identified several deficiencies that may cause suboptimal care of patients with severe sepsis. These deficiencies include inconsistency in the early diagnosis of severe sepsis and septic shock, frequent inadequate volume resuscitation without defined endpoints, late or inadequate use of antibiotics, frequent failure to support the cardiac output when depressed, frequent failure to control hyperglycemias adequately, frequent failure to use low tidal volumes and pressures in acute lung injury, and frequent failure to treat adrenal inadequacy in refractory shock.
The management of patient with sepsis is influenced more by appropriate treatment with antibiotics and fluids than by specific intensive care. Therefore early intervention should never be delayed pending admission to the intensive care unit. The early and aggressive treatment of septic shock has been well documented in the survival sepsis campaign which is based on the best current practice.
The cornerstones of treatment are infection control, haemodynamic stabilization, and modulation of the septic response.
1. Infection Control:
Infection control is vital if the patient is to have any chance of survival. Appropriate broad-spectrum antibiotics must be given within the first hour of recognition of sepsis after obtaining various cultures. Evidence clearly shows that delay or inadequate antibiotic treatment results in poorer outcome. For every hour lost mortality climbs by 9%. [7]
Initial empirical anti-infective therapy should include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal) and that penetrate in adequate concentrations into the presumed source of sepsis[8] antimicrobial regimen be reassessed daily to optimize activity, to prevent the development of resistance, to reduce toxicity, and to reduce costs
A focus of infection must be sought for and if discovered dealt with immediately. The patient should be evaluated for a focused infection amenable to source control measures including abscess drainage or tissue debridement. One must weigh up the benefits and risks of the particular procedure chosen. If intravascular devices are a potential source, they must be promptly removed after establishing other vascular access. When source control is required, the effective intervention associated with the least physiologic insult be employed (e.g., percutaneous rather than surgical drainage of an abscess)
2. Haemodynamic Stabilization:
In septic shock there is extensive cardiovascular derangement. Hypotension is caused by myocardial depression, pathological vasodilatation and extravasation of circulating volume due to widespread capillary leak. The initial resuscitative effort is to attempt to correct the absolute and relative hypovolemia by refilling the vascular tree. There is no evidence to support one type of fluid crystalloid or colloid is superior to the other. There is good evidence that early gold directed aggressive volume resuscitation improves outcome of sepsis[9] During the first 6 hours of resuscitation the goals of initial resuscitation are a Central venous pressure of 8-12 mm Hg, Mean arterial pressure (MAP) ≥ 65 mmHg, Urine output ≥ 0.5 mL • kg-1 • hr and a central venous (superior vena cava) or mixed venous oxygen saturation ≥ 70% or ≥ 65%, respectively The Rivers study clearly shows a reduction in hospital mortality, 28 day mortality as well as 60 day mortality attributed to the Early Goal Directed Therapy (EGDT) [10]. Early goal-directed resuscitation has been shown to improve survival for emergency department patients presenting with septic shock in a randomized, controlled, single-centre study.[11] Resuscitation directed toward the previously mentioned goals for the initial 6-hr period of the resuscitation was able to reduce in hospital, 28-days as well as 60 days mortality rate (Fig. 6).
Fig 6: Results of Early Goal Directed Therapy (EGDT)
If Scvo2 or SVo2 of 70% or 65%, respectively, is not achieved with fluid resuscitation to the central venous pressure target, then transfusion of packed red blood cells to achieve a hematocrit of ≥ 30% and/or administration of a dobutamine infusion (up to a maximum of 20 µg • kg-1 • min-1) be used to achieve this goal.
It is important to remember that vasopressors should be utilized not only when fluids fail to reverse hypotension, but also during resuscitation to maintain minimally adequate blood pressure. Traditionally, the use of noradrenalin in patients with shock has been restricted by the fear of excessive vasoconstriction that may result in end-organ hypo perfusion. In the past it was usually given only when other vasopressin agents failed, and thus such patients would be predicted to have a poor outcome. Recent studies indicate that the fear of deleterious effect was unwarranted and that noradrenalin may have a role as a first-line vasopressor agent in patients with septic shock.
Vasopressin should be considered in refractory shock despite high dose conventional vasopressors. Vasopressin is an endogenously produced hormone that is deficient in many patients with septic shock. Exogenously administered vasopressin in physiologic replacement doses may act synergistically with other vasopressor agents, and has been associated with early withdrawal of catecholamine. Most studies have evaluated short-term infusions of vasopressin at 0.08 U/minute or less as add-on therapy in patients requiring adrenergic agents. The results show that starting vasopressin in patients with septic shock increases systemic vascular resistance and arterial blood pressure, thus reducing the dosage requirements of adrenergic agents [12]. These effects are rapid and sustained. Substantial enhancement of urine production, likely due to increased glomerular filtration rate, was shown in several studies. A few studies demonstrated clinically significant reduced cardiac output or cardiac index after vasopressin was begun, necessitating cautious use in patients with cardiac dysfunction.
3. Modulation of Septic Response:
There are a number of ways to modulate the septic response. These includes use of steroids, tight glucose control and the use of Activated Protein C. Septic shock causes adrenal suppression and this can be confirmed by measuring cortisol levels or by using the synacthan test. Compare to placebo, the administration of low dose of hydrocortisone (200-300 mg/day in divided doses) to patients with septic shock decrease there requirements for vasopressors [13] and lowered their mortality rate [14]. Low dose hydrocortisone should only be given to non responders of the synacthan test but in practice all patient receive this treatment until the result of the test are received. Following the Corticosteroid Therapy of Septic Shock (CORTICUS) study there is now an increasing trend towards restricting the use of low dose hydrocortisone only to patients with refractory hypotension who are already on high doses on vasopressors [15]. The trial did show a faster resolution of septic shock in patients who received steroids but failed to show a mortality benefit with steroids therapy. Close control of blood glucose has been shown to increase survival in critically ill septic patient. When conservative (10 – 11.1 mol/L) glycemic control was compared with tight control (4.4-6.1mmol/L) in a multi centre, randomized controlled trial, tight control lead to a significant reduction in mortality (8% versus 4-6%), p < 0-04 and improved morbidity at 12 months [16].
Activated Protein C
Human activated Protein C (APC) is an endogenous regulator of coagulation. In order for protein C in the plasma to become activated, it must combine with thrombin and thrombomodulin along with the endothelial protein C receptor. With endothelial damage this activation does not take place resulting in its deficiency. Therefore APC supplementation is a rational therapeutic option. APC has an important role in the management of severe sepsis. It protects against the disruption of the endothelial cell membrane, improves micro circulatory perfusion, and has anti inflammatory, procoagulant, fibrinolytic and anti apoptotic activity. APC must ideally be started with in the first 24 hours of the onset of septic shock. The Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) trial found activated protein C to reduce the risk of death among all severe sepsis patients by 20% [17] This study has also recognized the risk of complications specially haemorrhages.
Subsequent studies have shown similar results. “Administration of Drotrecogin Alfa (Activated) in Early Stage Severe Sepsis” (ADDRESS trial) also provides the evidence concerning use of rhAPC in adults [18]. Additional safety information comes from an open-label observational study, “Extended Evaluation of Recombinant Activated Protein C” (ENHANCE trail). [19] The ENHANCE trial also suggested that early administration of rhAPC was associated with better outcomes.
Other beneficial Strategies in Sepsis
Low Tidal Volume Ventilation: using normal or high tidal volume (10-12mls/Kg) ventilation will cause over expansion of the normal lung segments. This will in turn result in inflammatory mediators being released in the lung tissue. The consequences of this are the development of Acute Lung Injury (ALI) or Acute Respiratory Distress Syndrome (ARDS). Therefore it is crucial to use low tidal volume Ventilation (6ml/kg) to keep plateau airway pressure less than 30 cm of water [20, 21]
High volume Haemofilteration: In the past five years, many studies have been conducted to evaluate and demonstrate benefits of increasing the volume of ultra filtration and replacement fluid during Continuous Renal replacement therapy [22, 23] particularly in complex and very severe syndromes such as Severe Sepsis and Septic Shock, associated with or without acute renal failure.
In general, the high-volume approach provides higher clearances for middle/high molecular weight solutes than a simple diffusive transport, Continuous veno venous haemodialysis (CVVHD) or a convection-based transport at lower volumes, Continuous veno venous haemofiltration (CVVH). These solutes seem to be primarily involved in the Systemic Inflammatory Response Syndrome, which characterizes the Sepsis syndrome, and their efficient removal may thus be beneficial. [24]
Alternative approaches have been based on more efficient removal of inflammatory mediators by high cut-off hemofilters, which are characterized by an increased effective pore size. Most commercially available hemofilters do not permit a substantial elimination of cytokines because of the low cut-off point of their membranes. The use of high cut-off hemofilters is a new and effective approach to cytokine removal, but it has potentially harmful side effects, such as the loss of essential proteins like albumin [25].
Because the reversibility of this disease and the resultant mortality may be greatest during the earliest stages of presentation, proper sepsis management should not be confined within the walls of an Intensive Care Unit. Specific emphasis on appropriate triage to ensure prompt diagnosis of the high-risk patient is vital to the launch of a coordinated and cooperative effort by the primary treating clinician and the intensivist
Ethical Dilemmas in Septic Shock
Patient with septic shock have a high mortality and as yet there is no predictive scoring system which gives accurate predictions of outcome for individual patient. Survival from an episode and septic shock is dependent on patient’s age, number of failed organs, previous health and the time delay before the onset of medial intervention, as well as the appropriateness and quality of medical care. The resources available to us are not limitless and so difficult decisions have to be made deciding between the potential benefits for one critically ill patient and need for several less critically ill patients. As an intensivist one must set realistic expectations which must be clearly communicated to the families concerned. As septic shock worsens and fails to respond to all therapy, one must be prepared to limit and withdraw treatment.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
KHADIJA E QURESHI, BSC, MBBS, DA, FCPS, ST2- Anaesthetics, Hemel Hempstead General Hospital, United Kingdom
ABID RAJAH, MB ChB, FRCA, FFARCSI, Lead Clinician & Consultant in Intensive Care, Hemel Hempstead General Hospital, United kingdom
CORRESPONDENCE: Dr Abid Rajah, Lead Clinician & Consultant in Intensive Care, Hemel Hempstead General Hospital, Hill field Road, Hemel Hempstead, HP2 4AD
Email: ARajah@aol.com
REFERENCES
Lundberg J, Perl TM. Septic shock: an analysis of outcomes for patients with onset on hospital wards vs. Intensive care units. Crit care Med 1998; 26: 1020-24
Vincent JL, Sakr Y, and Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006; 34:344-353.
Shapiro NI, Homel MD, Talmor D, Nathanson LA, Lisbon A, Wolfe RE, et al. Serum lactates as a predictor of mortality in emergency department patient with infection. Ann Emerg Med. 2005; 45: 524-8.
Harbarth S, Garbino J, Pugin J, et al. Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med. 2003; 115:529-535.
Gibot S, Kolopp-Sarda MN, Bene MC, et al. Plasma level of a triggering receptor expressed on myeloid cells-1: its diagnostic accuracy in patients with suspected sepsis. Ann Intern Med. 2004; 141:9-15.
Surviving Sepsis Campaign. Available at: http:// www.surviving sepsis.org/ Accessed March 6, 2007.
Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis C guidelines for management of severe sepsis and septic shock. Crit Care med. 2004;32: 858-873
Battleman DS, Callahan M, Thaler HT. Rapid antibiotic delivery and appropriate antibiotic selection reduce length of hospital stay of patients with community acquired pneumonia: link between quality of care and resource utilization. Arch Intern Medicine 2002; 162(6):682-8.
Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003; 31:1250-1256.
Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377
Emanuel Rivers. The outcome of patients presenting to the emergency department with severe sepsis or septic shock. Crit Care. 2006; 10(4): 154.
Obritsch MD; Bestul DJ; Jung R; Fish DN; MacLaren R. The role of vasopressin in vasodilatory septic shock. Pharmacotherapy. 2004; 24(8):1050-63 (ISSN: 0277-0008)
Briegel J, Frost H, Haller M, Shelling G, Kilger E, Kuprat G et. Stress doses of hydrocortisone reverse hyper dynamic septic shock: a prospective randomised double blind single centre study. Crit care Med 1999; 27:723-32.
Annane D, Sebille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002; 288:862-871.
Sprung CL. Update on clinical trials in severe sepsis. CORTICUS trial. Program and abstracts of the Society of Critical Care department patient with infection. Ann Emerg Med 2005: 45 (524-8).
Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354:449-461
Bernard GR, Vincent JL, Laterre PF, et al. Recombinant human protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study group. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001; 344:699-709.
Abraham E, Laterre PF, Garg R, et al: Drotrecogin alfa (activated) for adults with severe sepsis and a low risk of death. N Engl J Med 2005; 353:1332-1341.
Vincent JL, Bernard GR, Beale R, et al: Drotrecogin alfa (activated) treatment in severe sepsis from the global open-label trial ENHANCE: Further evidence for survival and safety and implications for early treatment. Crit Care Med 2005; 33:2266-2277.
ARDS Network Investigators. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000; 342:1301-1308.
National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wiedemann HP, Wheeler AP, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006; 354:2564-2575.
Piccinni P, Dan M, Barbacini S, Carraro R, Lieta E, Marafon S, Zamperetti N, Brendolan A, D'Intini V, Tetta C, et al.: Early iso-volaemic haemofiltration in oliguric patients with septic shock. Intensive Care Med 2006, 32:80-86.
Reiter K, D'Intini V, Bordoni V, Baldwin I, Bellomo R, Tetta C, Brendolan A, Ronco C: High-volume hemofiltration in sepsis. Nephron 2002, 92:251-258.
Ronco C, Tetta C, Mariano F, Wratten ML, Bonello M, Bordoni V, Cardona X, Inguaggiato P, Pilotto L, d'Intini V, Bellomo R: Interpreting the mechanisms of continuous renal replacement therapy in sepsis: the peak concentration hypothesis. Artif Organs 2003, 27:792-801.
Abbreviations BSCCP British Society of Colposcopy and Cervical Pathology
CIN Cervical intraepithelial neoplasia
CGIN Cervical glandular intraepithelial neolpasia
DNA Deoxyribonucleic acid
HPV Human papillomavirus
HSIL High-grade squamous intraepithelial lesion
LBC Liquid-based cytology
LLETZ Large loop excision of transformation zone
LSIL Low-grade squamous intraepithelial lesion
NHSCSP National Health Service Cervical Screening Programme
Introduction
Papanicolaou’s publication in 1940s, which showed that exfoliated cervical cells could be reliably harvested and spread, fixed and stained on a glass slide, laid the foundations of cervical screening.
In the last two decades, there has been immense progress in the understanding of cervical carcinogenesis and the currently accepted view is that HPV is an essential factor in the causation of the disease. If HPV is persistent, integration into the cellular genome may occur, which results in the inactivation of tumour suppresser genes, suppression of apotosis, genetic instability and development of precancerous change. Additional genotoxic agents, such as smoking, contribute further to the progression of cervical cancer.
The death rate from cervical cancer was essentially unchanged until the national programme was instituted in 1988. The White Paper The Health of the Nation set a national target to reduce the mortality from cervical cancer by at least 20% by the year 2000 (from 15 per 100,000 populations in 1986 to no more than 12 per 100,000, directly standardize against the European population). The NHS Cervical Screening Programme (NHSCSP) exceeded the target by the year 1997, when the rate fell to 8.9 per 100,000. It continues to fall.
Cervical screening programme1
The programme originally involved every woman between the ages of 20 and 64 years (20-60 years in Scotland) being called and recalled every 3-5 years for a cervical smear test. The evidence has indicated that a more effective screening programme can be offered to women by changing the frequency of screening according to a woman’s age. In 2004, the NHSCSP has issued guideline number 20 which covers all of the major aspects of screening, diagnosis, treatment and follow up.
Age group (years)
Frequency of screening
25
First invitation
25 – 49
Three yearly
50 – 64
Five yearly
65+
Only screen those who have not been screened since age 50 or those who have had recent abnormal tests
Age at starting screening
The incidence of cervical cancer under the age of 25 years is low, and the prevalence of transient HPV infection is high. Much of this prevalent disease would resolve spontaneously. Hence, screening women under the age of 25 years may do more harm than good (unnecessary attendance to colposcopy clinic, increased anxiety and possible over treatment).
Screening interval
A 2003 publication indicated that, to be effective in younger women, screening needs to be more frequent. Therefore, the new screening intervals are to be 3 yearly until the age of 50 years when 5 yearly screening until the age of 64 years, because the most incidences of CIN will have been prevented by prior screening2.
Age at finishing screening
The prevalence of CIN3 and invasive cancer in women over the age of 50 is low. Although it is possible that it may be safe to withdraw well screened women with a negative smear history from screening programme at age 50 years, there is no robust evidence to withdraw this level of healthcare.
Population coverage
A major success in the cervical screening programme has been to increase population coverage. There remain certain women who do not participate, including some ethnic minorities and some women who choose not to. A significant proportion of women who develop cancer have not been regularly screened. Additional effort is required to convince some women that screening can be life saving.
LBC
Liquid base cytology provides almost total elimination of inadequate smear. The UK pilot studies concluded that inadequate cytology would be cut by 87 %, from 9.1% with Pap slides to an average of 1.6 % with LBC.
It has been established from systematic reviews that routine primary cervical screening carries a 50 – 70 % sensitivity to detect CIN3. LBC increases overall sensitivity, gives rise to less equivocation in low grade smear and leads to less referral for colposcopy. There is no difference between the specificity of LBC and Pap smear3.
Smear reports
Acceptable range4
Negative smear
Number of abnormal smear
8.1 – 8.3%
Inadequate smears
5.8 – 12.9%
Borderline nuclear abnormality Mild Dyskaryosis
4.1 – 9.5%
Moderate & Severe dyskaryosis
1 – 2 %
Referral guideline for colposcopy
Women with the following smear results should have the colposcopy assessment.
3 consecutive inadequate smears
3 borderline changes in squamous cells
3 abnormal smears at any grade in a 10 year period
1 borderline change in endocervical cells
1 or 2 mild dyskaryosis (1 mild change – acceptable to repeat a smear)
1 moderate dyskaryosis
1 severe dyskaryosis
1 abnormal glandular smear
Time interval: referral – colposcopy
Abnormal smear
within 8 weeks
Moderate or severe dyskaryosis
within 4 weeks
Glandular abnormality or possible invasion
within 2 weeks
Treatment
Recent evidence suggests that possibly all major-grade (CIN 2, CIN 3, HSIL) lesions should be treated, whereas minor-grade (CIN 1, LSIL) lesions should be managed more conservatively.
Over the last decade the trend has been directed toward more conservative methods of managing CIN. This has coincided with the introduction of the large loop diathermy excision technique. A large multicenter study covering over 13000 treatments has recorded the continuing small risk of patients treated with conservative modalities to develop invasive cancer many years after initial treatment. The risk was still present up to 14 years following treatment.
Method of treatment
Local destructive techniques
It is imperative that any such method destroys the CIN contained within the cervical glands or, more correctly the crypts. Therefore, to be totally effective, these methods must destroy the tissue to the depth of at least 6-7 cm. These methods are the treatment of choice for selected cases in which the entire abnormality is visible on the ectocervix, and in which there is no suggestion of invasion. The principal disadvantage of this method is that a histologic examination of the entire lesion is not possible and early invasive cancer may remain undetected. There are four local destructive techniques:
Cryotherapy, or freezing the area by the application of probes; anaesthesia is not usually required.
Cold coagulation, usually without, or with some local anaesthesia.
Electrodiathermy, under either local or general anaesthesia.
Carbon dioxide (CO2) laser evaporation, usually with local analgesia.
Excisional techniques
Cold knife biopsy
Laser cone biopsy
Large loop diathermy
Hysterectomy: abdominal or vaginal
The optimal method of CIN treatment
There is no obviously superior conservative surgical technique for the treatment of CIN. Excisional treatments permit histological assessment of biopsy and can determine risk factors for residual disease.
The studies have led many authors to advocate the use of excision rather than local destruction techniques as the loops have discovered early invasive lesion in excised specimens. But it can be argued that many of the early micro-invasive lesions now found by the use of excision techniques would have been quite effectively destroyed by the use of local destructive techniques. Now at the moment, it must be left to the individual clinician to choose which technique gives the best results.
Complication
Immediate
The morbidity for excisional method is 2-4 % with immediate discomfort and bleeding.
Long term
Cervical stenosis and constriction: This problem tends to occur most frequently in postmenopausal and post partum women, and result in the development of pyometra. In the younger woman, the stenosis may lead to pelvic endometriosis following on haematometra. The patient often presents with symptoms of painful and prolonged menstruation. The simple management is to perform a dilatation of cervix under general anaesthesia. Even use of a narrow endocervical brush may relieve the symptom.
Excessive eversion of the columnar epithelium : It is not uncommon for the cervix to appear with a large area of exposed columnar epithelium, especially after cone biopsy. Such a situation may result in complaints of postcoital and intermenstrual bleeding or discharge. Nevertheless, it is possible for this exposed transformation zone to become infected yet again with mutagenic agent that resulted in the development of CIN.
It may be necessary to stimulate metaplasia of this area by applying cryosurgery, cautery, or even laser vaporization to columnar epithelium. However, for most patients active treatment is not necessary.
Subsequent pregnancy: There is always concern about subsequent fertility and pregnancy outcome following treatment for CIN. The morbidity associated with the excision of a small fully visible TZ will be different from that associated with a large zone which extends 2 cm up the endocervical canal.
The evidence found no effect on subsequent fertility and pregnancy outcome following loop diathermy treatment. However, it is found to have a higher incidence of low birth-weight babies when compared with controls. More recently, other authors have shown that using the CO2 laser, a cone biopsy greater than 10 mm in depth acts as an independent risk factor for the occurrence of preterm labour5.
Success rate
Modern conservative therapies for the treatment of CIN are extremely successful, with the clearance rate in the order of 95 % or better, except cryosurgery which has a lower clearance rate than other conservative method (85%).
Recurrence
The rate of dyskaryosis in 12 months following both LLETZ and laser ablation was 4.4 %. A cumulative rate of recurrence at 4 years was 10.1 per 100 women.
Follow up
Follow up after conservative treatment
Women aged 50 years or more with positive excision margin are particularly at risk of persistent and recurrent disease. Cytology alone is recommended for follow up and should start at six month following treatment.
Women treated for high grade disease (CIN2, CIN3, CGIN) require 6 and 12 month follow up cytology and annual cytology for subsequent nine years before returning to screening at routine interval.
Women treated for low grade disease require 6, 12 and 24 month follow up cytology. If all results are negative, then women may return to screening at routine interval.
Women treated for CGIN are at higher risk of developing recurrent disease than those with high grade CIN. Ideally, six-monthly samples would be taken for five years followed by annual samples for a further five years.
Follow-up after hysterectomy
Women who have had a hysterectomy with CIN present are potentially at risk of developing vaginal intraepithelial neoplasia (incidence 1%) and invasive vaginal disease.
For women on routine recall for at least 10 years prior to hysterectomy and no CIN in the sample at hysterectomy, no vault cytology is required.
For women with less than 10 years’ routine recall and no CIN at hysterectomy, a sample should be taken from the vault six months after surgery and there should be no further cytology follow-up if it is negative.
For women with completely excised CIN at hysterectomy, a sample should be taken from the vault at 6 and 18 months after surgery and there should be no further cytology follow-up if both are negative.
For women with incomplete or uncertain excision of CIN, follow-up should be conducted as if the cervix is still in situ.
Summary of follow up
Histology/ Pre-treatment smear history
Follow up
After conservative treatment
Low grade CIN
6, 12 and 24 months and then routine screening
After conservative treatment
High grade lesion (CIN2, CIN3, CGIN)
6, 12 and annual cytology for 9 years and then routine screening
After hysterectomy
Routine recall in last10 years, No CIN
No vault smear
After hysterectomy
Less than 10 years, Routine recall, No CIN
Vault smear 6 months after hysterectomy
After hysterectomy for CIN
Complete excision of CIN
Vault smear 6 and 8 months after hysterectomy
After hysterectomy for CIN
Incomplete or uncertain excision of CIN
Follow up as if the cervix is still in situ
The potential role of HPV testing
The type II hybrid capture is a new method for the detection of HPV DNA in cervical mucosa. The following list of clinical uses of hybrid capture is suggested:
As a screening method, together with cytology:
For patients with abnormal cytology, to select patients who will be referred to a colposcopic clinic.
To evaluate the low-grade lesions forecast.
The use of hybrid capture as a screening method is based on the principle that the cytology has a sensitivity of approximately 56%, and the sensitivity of virus typification is 77%; but using both at the same time, the diagnostic sensitivity amount to 93%. Whether hybrid capture should be used as a screening method is still being debate6. A recent RCT7 reported that adjunctive HPV testing did not add significantly to the effectiveness or cost effectiveness of LBC to the detection of CIN 3.
Vaccination against cervical cancer8
Without further preventive measures, death from cervical cancer are predicted to jump four-fold to over a million a year by 2050 as a result of the explosion in HPV infection rates across the world. Vaccination as a primary prevention has obvious advantages in countries where screening programmes are not established but may also offer advantages in countries like the UK, where secondary prevention by screening and treating premalignant lesions is not only expensive but sometimes imprecise, resulting in unnecessary anxiety and intervention for some women, while at the same time failing to detect lesions in others.
Rationale
Women previously infected with a particular HPV type are unlikely to become reinfected by the same type, because of immunity largely provided by antibodies targeted against the major papillomavirus capsid protein L1. When made in the laboratory, L1 protein self-assembles into virus-like particles (VLPs) that are morphologically identical to HPV and highly immunogenic but not in themselves infectious because of lack of viral genome.
Gardasil (Merk) is a quadrivalent vaccine offering protection against HPV types 6, 11, 16 and 18. The longevity of this immune response varied, with only 76% of vaccines showing detectable antibody response to 36 months after immunisation. There is preliminary evidence of cross protection against infection with related HPV 31 and 45. Gardasil and Cervarix has an excellent safety record with only transient injection site reaction and no evidence of adverse effects on chronic disorders.
In the UK, the HPV vaccination programme targets the girls from 12 to 13 year old and additional programme for the girls from 13 to 18 years old, starting in September 2008 and finishing in 2011. HPV-specific antibodies generated by vaccination may wane with time, although current data indicate that immune responses persist through 5 years. The need for booster immunisations to maintain protection against infection will become apparent after prolonged periods of follow up.
The abnormal smear in pregnancy
Ten to fifteen in 1000 pregnant women have their smear abnormal. Recommendations for referral colposcopy are the same in pregnancy as in non-pregnant women. Much more reassurance is required, with emphasis on the fact that the colposcopy will not harm the fetus or cause miscarriage. The treatment for preinvasive lesions may be postponed until after delivery. The essential role of biopsy is to rule out an invasive disease.
The cervical smear in menopausal women
Oestrogen deficiency causes atrophy of tissue and a retraction of squamocolumnar junction. The epithelium becomes thinner and more easily traumatized. There is a greater incidence of unsatisfactory smear reports and unsatisfactory colposcopy. It is generally preferable to repeat smear after oral, transdermal or vaginal estradiol for a period of 7 to 10 days.
Conclusion
The cervical smear is a simple and effective screening which has a number of deficiencies. False-negative smears are principally due to imperfect sampling, errors of cytological interpretation, and in rare cases to rapid progression of lesions in sites which are difficult to access. New technologies can improve the sensitivity of screening. The emphasis is on developing systems that will screen for preinvasive stage of cervical cancer and thereby allow assessment and appropriate management.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
TINT TINT WAI, ST3, Obstetrics and Gynaecology Department, Bedford Hospital, United Kingdom
DILIP PATIL, Consultant Obstetrician and Gynaecologist, Bedford Hospital, United Kingdom
CORRESPONDENCE: D Patil, Consultant Obstetrician and Gynaecologist, Bedford Hospital, United Kingdom,
Email: patild@yahoo.com
References
Colposcopy and Programme Management. NHS Cervical Screening Programme publication 20. April 2004
Progress in cervical screening. Scientific Advisory Committee. RCOG Opinion paper 7. June 2006
Guidance on the use of LBC for cervical screening. NICE, Technology appraisal 69. October 2003
David M Luesley, Mohamood I. Shafi and Joseph A. Jordan. Handbook of Colposcopy; Second edition 2002
Albert Singer & John M Monaghan. Lower Genital Tract Precancer. Second edition 2000
W Prendiville, J Ritter, S Tatti, L Twiggs. Colposcopy management options. First edition 2003
Henry Kitchener, et al. ARTISTIC: A randomised trial of HPV testing in primary cervical screening: Final results; BSCCP Annual Scientific Meeting, book of abstracts, 2008
Vaccination against cervical cancer, Scientific Advisory Committee, Opinion paper 9, RCOG; February 2007
Introduction: Since Longo first described it in 1998, Stapled Haemorrhoidectomy (SH) has been emerging as the procedure of choice for symptomatic haemorrhoids (1). Several studies have shown it to be a safe, effective and relative complication free procedure (2). The aim of this study was to determine the suitability of SH as a day case procedure at a District General Hospital.
Methods From June 2001 to May 2005, 66 patients who underwent stapled haemorrhoidectomy were included in this study. Parameters recorded included post-operative complications, analgesic requirements, cost effectiveness, duration of hospital stay and patient satisfaction. Follow-up was performed at 4 weeks with a further telephone follow-up up to 4 years after.
Results Of the 66 patients that underwent a stapled haemorrhoidectomy 43 (65%) were male and 23 (35%) were female. The mean age was 49.8 years (range 16-78 years). 11% (n=7) of patients were discharged the same day and 88% (n=58) had overnight stay. Nearly 50% had complete resolution of symptoms and returned to work within a week. The satisfaction data showed that 90% of patients were completely satisfied with the procedure at initial follow-up, which increased to 98% after 6 months-4 years follow-up.
Conclusion Our present study shows that stapled haemorrhoidectomy is a safe and very well tolerated procedure with low post-operative analgesic requirements, high patient satisfaction and early return to work. The majority of patients could avoid an overnight stay which would make this procedure suitable for day surgery.
Introduction
Since Longo first described it in 1998 (1), Stapled Haemorrhoidectomy (SH) has been emerging as the procedure of choice for symptomatic haemorrhoids. Several studies have shown it to be a safe, effective and relative complication free procedure with fewer days off work, reduced requirement for analgesia and rapid discharge (2-4). Historically symptomatic haemorrhoids have been dealt with by simple dietary modification, injection sclerotherapy, cryotherapy, band ligation and surgery (5-7).
Unfortunately there is no single optimum therapeutic option. Surgery for symptomatic haemorrhoids was popularised by the open Milligan–Morgan technique in the late 1930’s or one of its variations. Unfortunately, this has been associated with postoperative pain, the risk of severe haemorrhage, and more concerning the risk of anal stenosis (especially if skin bridges are not maintained) and sphincter injury.
Controversy exists as regards to the overall safety and acceptability of SH. On the one hand recent reports of SH have been positive especially in regards reduced postoperative pain and recovery and adverse functional sequelae. A study by Pavlitidsi et al (8) included 80 patients with second to fourth degree hemorrhoidal disease in which patients were randomly allocated to undergo either the stapled Longo procedure (group 1) or Milligan-Morgan hemorrhoidectomy (group 2) under epidural anesthesia. SH had better postoperative pain scores with lower mean epidural morphine requirement and mean hospital stay. Conversely, a recent review from New Zealand (9) suggested that SH was more expensive, and the results should be looked upon with caution.
Several studies have suggested that SH may be safely performed as a Day case procedure. Patients following SH had reduced, post operative pain, hospital stay, analgesic requirements and earlier return to work (21-23). Day Surgery procedures have been at the forefront of recent changes within the NHS in the fight to reduce waiting times and better patient care. It is not only popular with patients who are able to recover and convalesce at home in a familiar environment but also reduce the chances of a hospital acquired infection and large cost saving implications for the NHS. However, not every surgical procedure is amenable for Day surgery, and thus procedures which require only moderate amounts of analgesia, reduced post operative stay and few complications and further in 2001 the Audit Commission included Haemorrhoidectomy as one of its 25 procedures suitable for Day Surgery (24).
Therefore the present study was to look critically at the learning curve, operative complications, duration of hospital stay, analgesic requirements, cost effectiveness and patient satisfaction in at the personal series of the first 66 patients who underwent SH at Watford General Hospital, a District General Hospital in Hertfordshire, United Kingdom. The aim of the present work was to determine the suitability of SH as a routine day surgery procedure which is not routine in the UK.
Patients and Methods
From June 2001 to May 2005, 66 patients who underwent stapled haemorrhoidectomy were included in this study. It was routine practice that stapled haemorrhoidectomy was performed by one dedicated surgical team (JIL).
Informed consent was obtained in writing prior to surgery. During induction at least a single dose of prophylactic antibiotics (of either a third generation cephalosporin or co-amoxiclav) was administered.
In brief, under general anaesthesia, the patient is put in lithotomy position and a rigid sigmoidoscopy done to exclude any rectal lesions. Stay-sutures with 2-0 silk are applied at the 3, 6, 9 & 12 o’clock. The anus is dilated using with a proctoscope.
An anal ring is applied and fixed to the anal verge by the previously taken stay-sutures. The inner end of the ring must be reaching beyond the dentate line.
Purse-strung sutures are taken all around the anal mucosa on top of the haemorrhoids (beyond the dentate line) followed by a per-rectal examination to make sure that the muscle layer is not taken within the sutures so as to avoid postoperative anal stenosis. Similarly, in female patients, per-vaginal examination is done to insure that vaginal wall is not taken within the sutures. A specialized circular stapler is introduced into the anal canal and the two ends of the purse-strung sutures are passed through special holes in the stapler and tied. Stapler is tightened (the indicator reads between 3 & 4 cm depth) and fired. The stapler is kept closed in place compressing them for 30 seconds in order to encourage haemostasis. The staples line then is checked for bleeding points, for which 2/0 vicryl under-running sutures may be use for further haemostasis. Finally, the anus is packed with ‘spongistan’ as well as flagyl and voltarol suppositories.
Post-operatively both groups were discharged when comfortable. Complications where noted as they occurred during the follow-up period at 4 weeks. Furthermore, a further telephone follow-up during July 2005 was done results from the survey are shown in table II.
The data was reviewed and analysed in conjunction with our department of medical statistics. Analysis was performed using the Mann-U test. Multivariate analysis of the means was performed using the Krushal-Wallis Test.
Results
Of the 66 patients that underwent a stapled haemorrhoidectomy 43 (65%) were male and 23 (35%) were female. The mean age was 49.8 years (range 16-78 years). Only 7 patients suffered with hypertension and one with diabetes mellitus.
There presenting complaints included rectal bleeding (bright red) in 86% (n=57) and pain and discomfort 53% (n=35). Other complaints included a sensation of something coming down (n=3), change in bowel habit (n=2), constipation (n=1), and incontinence (n=1).
All patients underwent evaluation with proctoscopy and rigid sigmoidoscopy. Further evaluation with colonoscopy (14%, n=9), flexible sigmoidoscopy (9%, n=6), barium enema (9%, n=6) and anorectal MRI (1%, n=1) to rule out other associated pathologies accounting for their symptoms.
Previous to SH, 57 patients (87%) had undergone previous therapeutic manoeuvres in the form of injection sclerotherapy (76%) and banding of haemorrhoidal tissue (11%).
The operating time ranged between 15-40 minutes with an average of 24 minutes. There were no major complications although the majority of patients warranted oversewing of bleeding points around the staple line after the stapling procedure.
Post-operative hospital stay revealed that 88%, (n=58) went home after overnight stay (within 24 hours) and only 1 patient had a 48 hours stay with only moderate strength analgesics (Voltarol) (Table 1).
At routine follow-up at 1 month, we found that nine patients (14%) had had minor degrees of faecal urgency, frequency and soiling rectal bleeding, all of which subsequently resolved. Only one patient had developed a peri-anal heamatoma, which was evacuated under local anaesthesia in the Outpatient Department. Further, only two patients had significant problems. One patient complained of pain and discomfort at four-week follow-up, which we think resulted from too low application of the stapler which resolved completely over a six month period with simple analgesics and a single case of rectal stenosis resulting from too high a stapling, which was referred to a specialised centre for further management (Table 2).
Indeed, only 3 patients had recurrence of symptoms, which were treated with further sclerotherapy injection in the Out-patients department and one requiring re-stapled haemorrhoidectomy.
Follow-up was in the form of Out-patient review 4-6 weeks after the procedure and a telephone questionnaire up to 4 years after the operation the results of which are shown in Table 3-5. We can see that a third of the patients did not require or use analgesia after discharge and further 44% (n=29) needed just Voltarol. As regards to symptoms we can see that approximately two thirds of patients where off analgesics, and half had complete resolution and returned to work within a week. The satisfaction data shows that the immediately 90% of patients were completely satisfied with the procedure which increased to 98% on our follow up (6 months-4 years).
Discussion
The present study shows that stapled haemorrhoidectomy is a safe and very well tolerated procedure which is amenable for Day Case Surgery. We have shown that this approach is significantly quicker than the classical conventional haemorrhoidectomy and better tolerated with reduced post-operative pain and analgesic requirements, good patient satisfaction and early return to work. Further the vast majority of patients (65/66) were discharged after overnight stay with mild and moderate oral analgesics. We have now adopted this as our technique of choice for haemorrhoidal disease.
The optimal mode for haemorrhoidal disease has been an ongoing debate for over 20 years and can be achieved by either open conventional Milligan Morgan and associated procedures and more recently stapled haemorrhoidectomy. Open haemorrhoidectomy has been associated with pain, discomfort, anal stenosis and a poor satisfaction scores (13-14). Several randomised clinical trials have compared Open haemorrhoidectomy with SH and have suggested an advantage with SH (2,3,15,16) however due to the fact that this is a new procedure there is a paucity of long term data.
In our study we looked at the complications and patient related factors associated with SH these are shown on Tables 3-5. Minor complications included rectal bleeding, fecal urgency and perianal hematoma all of which resolved conservatively. One must note that although every effort is made to ensure that at the end of the procedure the operating site is haemostatically secure some passage of blood per rectum is considered inevitable, our data is from patient self assessments who may interpret this differently. We were unable to consistently quantify this and relied upon patient testimonies. Also Van De Stadt (12) noted a 55% rate of persistent or recurrent symptoms as well as a 20% requiring recurrent or redo surgery and Thaha et al (11) showed post-defecation syndrome rate of 4%.
Major complications associated with SH have been reported mainly in the form of case reports. In our series of 66 patients we had only two major complications. One patient had quite a lot of pain and discomfort post-operatively and upon assessment in the Out-patient department it was found that the staple line was too low (i.e. less than 3 cms) and this may be encroaching on the dentate line. Fortunately the patient was very tolerant and resolved over six months with moderate analgesics. Furthermore, our other major complication the patient developed rectal stenosis and was referred to a specialised unit where he underwent a resection. We feel that this patients staple line was too high (i.e. above 4 cms). Thus the message is that although SH is a simple procedure the critical step is the application of the purse-string so that the staple line is between 3-3.5 cms as complications can arise if you are too high or too low which was recently confirmed in a study of acute haemorrhoidal crisis (17).
Several papers have expressed concern with post-operative pain, faecal urgency after SH (18-19). This has been postulated to be due to incorporation of the muscle layers in the purse-string. However a recent paper by Kam et al (20) in a series of 33 patients found no association between amount of resected muscle and incontinence. Indeed, it is important to keep the purse-string suture superficial and not encroaching on the other bowel wall layers.
Our study shows good patient satisfaction scores and symptom control (Tables 3-5). We have shown that almost all 98% (65/66) of patients were discharged after a maximum overnight stay. This has huge cost saving consequences and although the equipment costs are high for SH this is compounded by a short duration of the operation, shorter hospital stay, reduced analgesic requirement and quicker return to work with the Health Service coming up on top overall. Of note, we can see that over 50% (n=34) of patients were back to work within a week of the operation and this is further supported by the fact that the majority of patients required simple analgesics for short durations.
This study highlights the excellent results after SH, with all the advantages such as reduced pain and hospital stay, and an earlier return to work. Importantly there does not seem to be a learning curve and once a surgeon has attended a training day or supervised there seems to be no increase in complications. The complication rates are low and as we have shown earlier only a single complication requiring intervention.
In conclusion, our study demonstrates that the SH is a safe, effective and well tolerated procedure which seems to have all the requirements for Day case surgery. We have also shown that it is quick procedure and post operatively less painful and requiring only simple analgesia for a short period. Thus we have adopted this technique as our procedure of choice and will consider it as a Day Case prodedure for symptomatic haemorrhoidal disease.
Table 1 : Duration Of Stay
Same Day
7
Overnight
58
2 Days
1
Total
66
Table 2 : Complications
Minor
Rectal Bleeding
9
Faecal Urgency
10
Perinanal Hematoma
1
Periananl Lump
1
Total
21
Major
Pain And Discomfort
1
Rectal Stenosis
1
Total
2
Table 3 : Analgesia
Nil
22
Pracetamol
8
Voltarol
29
Coproxamol
4
Paracetamol & Voltarol
3
Total
66
Table 4 : Analgesia
Duration Of Analgesics
Complete Resolution
Return To Work
Nil
22
0
20
<1 Week
20
30
14
1-2 Weeks
16
22
24
>2 Weeks
6
14
8
Table 5 : Patient Satisfaction
Immediate
4-6 Weeks
>6 Months
Satisfied
90%
95%
98%
Not Satisfied
10%
5%
2%
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
PROFESSOR AA RIAZ BSc FRCS(I) FRCS (Eng) FRCS(Gen) PhD, Watford General Hospital, United kingdom
CORRESPONDENCE: Professor AA Riaz, Department of Surgery, Watford General Hospital, Vicarage Road
Watford Hertfordshire, WG1, UK.
Tel: 01923-244366 ext 7692
Fax: 01923-217962
Email: mrariaz@hotmail.com
References
1. Longo A. Treatment of haemorrhoidal disease by reduction of mucosa and haemorrhoidal prolapse with a circular stapling device: a new procedure. 6th World Congress of Endoscopic Surgery. Mundozzi Editore: Naples, 1998;777-84.
2. Boccasanta P, Capretti PG, Venturi M, Cioffi U, De Simone M, Salamina G, Contessini-Avesani E, Peracchia A. Randomised controlled trial between stapled circumferential mucosectomy and conventional circular hemorrhoidectomy in advanced hemorrhoids with external mucosal prolapse. Am J Surg. 2001;182(1):64-8.
3. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg. 2001 Aug;88(8):1049-53.
4. Ascanelli S, Gregorio C, Tonini G, Baccarini M, Azzena G. Long stapled haemorrhoidectomy versus Milligan-Morgan procedure: short- and long-term results of a randomised, controlled, prospective trial. Chir Ital. 2005 Jul-Aug;57(4):439-47.
5. Alonso-Coello P, Guyatt G, Heels-Ansdell D, Johanson J, Lopez-Yarto M, Mills E, Zhou Q, Alonso-Coello P. Laxatives for the treatment of hemorrhoids. Cochrane Database Syst Rev. 2005 Oct 19;(4):CD004649.
6. Ramzisham AR, Sagap I, Nadeson S, Ali IM, Hasni MJ. Prospective randomized clinical trial on suction elastic band ligator versus forceps ligator in the treatment of haemorrhoids. Asian J Surg. 2005 Oct;28(4):241-5.
7. Hardy A, Chan CL, Cohen CR. The surgical management of haemorrhoids--a review. Dig Surg. 2005;22(1-2):26-33.
8.Pavlidis T, Papaziogas B, Souparis A, Patsas A, Koutelidakis I, Papaziogas T. Modern stapled Longo procedure vs. conventional Milligan-Morgan hemorrhoidectomy: randomized controlled trial. Int J Colorectal Dis.2002;17(1):50-3.
9. Hill A. Stapled haemorrhoidectomy--no pain, no gain? N Z Med J. 2004 8;117(1203):U1104.
10. Peng BC, Jayne DG, Ho YH. Randomized trial of rubber band ligation vs. stapled hemorrhoidectomy for prolapsed piles. Dis Colon Rectum. 2003;46(3):291-7; discussion 296-7.
11. Shanmugam V, Thaha MA, Rabindranath KS, Campbell KL, Steele RJ, Loudon MA.Rubber band ligation versus excisional haemorrhoidectomy for haemorrhoids. Cochrane Database Syst Rev. 2005 Jul 20;(3):CD005034. Review.
12. Van de Stadt J, D'Hoore A, Duinslaeger M, Chasse E, Penninckx F; Belgian Section of Colorectal Surgery Royal Belgian Society for Surgery. Long-term results after excision haemorrhoidectomy versus stapled haemorrhoidopexy for prolapsing haemorrhoids; a Belgian prospective randomized trial. Acta Chir Belg. 2005 Feb;105(1):44-52.
14. Arroyo A, Perez F, Miranda E, Serrano P, Candela F, Lacueva J, Hernandez H, Calpena R.Milligan-Morgan haemorrhoidectomy with ultrasonic scalpel. G Chir. 2003;24(11-12):422-7.
15. Khalil KH, O'Bichere A, Sellu D. Randomized clinical trial of sutured versus stapled closed haemorrhoidectomy. Br J Surg. 2000;87(10):1352-5
16. Hetzer FH, Demartines N, Handschin AE, Clavien PA. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg. 2002 ;137(3):337-40.
17. Kang JC, Chung MH, Chao PC, Lee CC, Hsiao CW, Jao SW.Emergency stapled haemorrhoidectomy for haemorrhoidal crisis. Br J Surg. 2005;92(8):1014-6.
19. Rowsell M, Bello M, Hemingway DM. Pain after stapled haemorrhoidectomy. Lancet. 2000 Dec 23-30;356(9248):2188; author reply 2190
20. Ravo B, Amato A, Bianco V, Boccasanta P, Bottini C, Carriero A, Milito G, Dodi G, Mascagni D, Orsini S, Pietroletti R, Ripetti V, Tagariello GB. Complications after stapled hemorrhoidectomy: can they be prevented? Tech Coloproctol. 2002;6(2):83-8.
21. Law WL, Tung HM, Chu KW, Lee FC. Ambulatory stapled haemorrhoidectomy: a safe and feasible surgical technique. Hong Kong Med J. 2003 Apr;9(2):103-7,
22. Ong CH, Chee Boon Foo E, Keng V. Ambulatory circular stapled haemorrhoidectomy under local anaesthesia versus circular stapled haemorrhoidectomy under regional anaesthesia. ANZ J Surg. 2005 Apr;75(4):184-6.
23. Ascanelli S, Gregorio C, Tonini G, Baccarini M, Azzena G. Long stapled haemorrhoidectomy versus Milligan-Morgan procedure: short- and long-term results of a randomised, controlled, prospective trial. Chir Ital. 2005 Jul-Aug;57(4):439-47
24. Royal College of Surgeons of England (1992) Guidelines of day case surgery (revised edition), London: RCS.
To identify risk factors predicting readmission of neonates within 7 days of birth and to implement guidelines to reduce this.
METHOD
All babies less than 1 week old either admitted to, or assessed at paediatric unit at Crosshouse hospital, Kilmarnock between July 2006 and December 2006 were included. Data was analysed on birth weight, gestation, age at discharge from maternity unit, age at admission to Crosshouse hospital, source of referral, problems necessitating referral, feeding, interventions, and length of stay.
RESULTS
We managed to obtain case notes for 50 babies out of the 55 who were admitted during this time. 44 babies (88%) were discharged from maternity unit within 48 hrs of birth and 23 babies (46%) were discharged from maternity unit within the first 24 hrs. Poor feeding/weight loss and physiological jaundice accounted for majority of admissions. Further poor feeding and weight loss were more common in first borns, in early discharges and in breast-fed babies.
RECOMMENDATIONS
Mothers deciding to breast-feed babies need proper support. It may be a good idea to delay discharge check until 24 hours after birth. First time mothers are especially naive when it comes to breast-feeding and it is important that they get properly supervised.
It may be a good idea to request mothers to fill in a questionnaire prior to discharge regarding how confident they feel about feeding their child, any feeding concerns, any other concerns etc.
ABBREVIATIONS
AMU: Ayrshire Maternity unit
CMW: Community mid wife
INTRODUCTION
The length of post partum stay in hospital has been steadily declining over the past 50 years.1,2 Reducing the number of days in the hospital after birth has several advantages like helping mother and infant recover in a familiar home environment; decreasing the risk of iatrogenic infections and cutting down on hospital costs. However, concerns have also been expressed about potential disadvantages of early discharge: For example breastfeeding is not established until the third or later postpartum day; a number of conditions do not manifest themselves until two or more days after the delivery.3 In a large study on neonatal mortality done in Washington (retrospective study looking at 47879 births between 1989 and 1990), it was found that neonates discharged before 30 hrs of age had a significantly higher mortality in the first month and first year of life than those neonates who were discharged later.4 In the United States, this has prompted the introduction of legislation making minimum 48 hour postpartum hospital stay mandatory. Through our audit, we aimed to identify risk factors predicting readmission and to implement local guidelines to reduce readmission rates.
METHOD
All babies less than 1 week old either admitted to, or assessed at paediatric unit at Crosshouse hospital, Kilmarnock between July 2006 and December 2006 were included. It was a retrospective study. List of patients was available from Medical records and paediatric case notes were obtained from medical records. The neonatal case notes were obtained from neonatal secretaries at AMU.
55 babies were admitted during this time out of which we managed to obtain paediatric and neonatal case notes for 50 babies. Data was analysed on birth weight, gestation, age at discharge from AMU, age at admission to Crosshouse hospital, source of referral, problems necessitating referral, feeding, interventions, and length of stay.
RESULTS
Most of the referrals were generated from community midwives who are often the first point of contact for neonates discharged from maternity unit (Table 1)
Source of referral (Table 1)
Source of referral
Number of babies
CMW
39
GP
5
A&E
4
Self
2
Total
50
We looked at the problems necessitating admission (Table 2). Please note that babies had more than one problem. Hence the higher numbers!
It is obvious looking at the numbers that most of the admissions are secondary to poor feeding and weight loss, majority of which could have been prevented.
Problems necessitating admission (Table 2)
Problems
Number of babies
No of babies in whom this problem was noted in AMU
Poor feeding
20
7
Wt loss >10%
18
0
Physiological jaundice Requiring phototherapy
14
1 (SBR was below treatment line)
Physiological jaundice Not requiring phototherapy
8
1
Choking episode
5
1
ABO incompatibility Requiring phototherapy
1
0 (No DCT done)
Pseudo menstruation
2
0
? Reflux (Blue episode)
1
1 (Not reported to staff)
Central posterior cleft palate
1
0 (Discharge check at 2 hrs)
? abnormal breathing (Normal baby on examination)
1
0
Mucous retention cyst under tongue
1
0
Not opened bowels for 48 hrs
1
0
Unable to abduct hip
1
0
Traumatic fat necrosis R side of face
1
0
CMW error in recording weight
1
NA
Fever? Viral illness
1
0
We also reviewed the age at readmission (Table 3). It is obvious that most readmissions were after the 3rd day of life. Most readmissions were related to poor feeding, weight loss > 10%, physiological jaundice and it is to be expected that most of the times; these problems would not become very obvious until around 3-4 days after birth.
Age at readmission (Table 3)
Age at admission
Number of babies
< 24 hrs
1
24-48 hrs
3
48-72 hrs
7
72-96 hrs
16
>96 hrs
23
Total
50
We also analysed the age when discharge check was done at the maternity unit
(Table 4). 44 babies (88%) were discharged from maternity unit within 48 hrs of birth and 23 babies (46%) were discharged from maternity unit within the first 24 hrs. Age at discharge check was important as there was an association found between early discharge from AMU and subsequent readmission with feeding difficulties especially among breast fed babies (Table 4). Also studies have shown that mothers with 1 day hospital stays post delivery are less satisfied with their length of stay.1
Age at which discharge check was done at AMU and subsequent admissions with poor feeding (Table 4)
Age at discharge check
Number of babies
Subsequent admissions with poor feeding
Breast fed
<12 hrs
11
3
2
12-24 hrs
12
8
7
24-36 hrs
15
3
3
36-48
6
3
2
48-60
6
2
2
>60 hrs
0
1
1
Total
50
20
17
Also an important association was noted between poor feeding and first time mums. Out of the 20 babies with poor feeding, 16 were born to first time mothers.
Also looking at the table below (Table 5), it is clear that feeding problems and wt loss were much more common in breast fed babies. The association between readmission and first born children, breast feeding has been shown in studies.5
Table 5
Mode of feeding
No of babies admitted with poor feeding and/or wt loss
Breast feeding
26
Bottle feeding
3 (One of whom had a cleft palate)
We also looked at relationship between birth weight and risk of readmission (Table 6) and also gestational age and risk of readmission (Table 7). There was no clear association between birth weight and readmission or between birth weight and feeding problems. Also there was no association noted between gestational age and risk of readmission in the first week of life. A likely explanation for these findings would be that infants with low birth weight or gestational age less than 37 weeks were probably less likely to be discharged early from the maternity unit.6
Birth weight and readmission (Table 6)
Birth weight as centile
Number of readmissions
Number with feeding problems
<3rd
0
0
3-10
12
5
10-50
12
5
50-90
16
8
90-97
8
2
>97th
2
0
Total
50
20
Gestational age and readmission (Table 7)
Gestational age
Readmission
<37 weeks
5
37-40 weeks
29
>40 weeks
16
Total
50
We also analysed data on length of admission in paediatric ward. 32 out of 50 admitted babies (64%) stayed less than 24 hrs (Table 8). 10 out of 50 admissions needed reassurance only (20%) but the remaining needed some form of intervention (Table 9)
Length of stay (Table 8)
Total length of stay
Number of babies
<12 hrs
13
12-24 hrs
19
24-36 hrs
7
36-48 hrs
7
48-60 hrs
4
Total
50
Interventions needed on readmission (Table 9)
Intervention
Number of babies
Help with feeding/ Change of feeding
22
Blood tests
35
Phototherapy
15
Reassurance only
10
Referral to other specialties
2
IV fluids
5
IV antibiotics
2
Folic acid supplements
1
ECG
3
Babies needing follow up and readmission (Table 10)
Readmission
2
Follow up in day unit
8
Follow up in clinic
4
Total
14
CONCLUSIONS:
Poor feeding and weight loss accounted for majority of the admissions. (Table 2)
The above problems occurred more commonly in breast fed babies. 90% of babies admitted with poor feeding and/or weight loss were breast-fed babies (Table 5).
Out of the 20 babies with poor feeding, 16 were born to first time mothers.
44 out of 50 babies who were readmitted had been discharged from maternity unit within 48 hrs of birth. There was a clear association between early discharge from maternity unit and subsequent readmission with feeding problems especially in breast fed babies. (Table 4). 11 out of 20 babies admitted with feeding problems (55%) were passed fit for discharge from AMU within 24 hours of birth. Again 12 of them were babies whom their mothers wanted to breast-feed. This raises the question of whether breast-feeding mothers are receiving sufficient support and whether the babies were being discharged too early. Also when these babies were subsequently admitted, many mothers decided to bottle feed despite being offered help with breast feeding. A bottle fed baby in whom a cleft palate was missed had a discharge check done when she was 2 hrs old!! Clearly not sufficient time to establish that she was feeding well!
7 out of 20 babies who were admitted with poor feeding were noted to have feeding difficulty while in AMU (Table 2). When these babies were passed fit for discharge, this would have probably given a false sense of reassurance to mothers especially the first time mums. These mums were less likely to report feeding problems to CMW leading to delayed referrals (Table 3) by which time the babies would have lost a lot of weight necessitating interventions like blood tests, IV fluids etc.
There was no association found between birth weight or gestational age and risk of subsequent readmission (Tables 6 and 7).
Physiological jaundice was the third most common problem necessitating admission (Table 2). Only 2 of the babies in this group were noted to be jaundiced in AMU.
Surprisingly parental pressure for early discharge from AMU was documented in only one neonatal notes suggesting that this might not have been an important factor causing early discharge.
For 10 of the admissions, reassurance was all that was needed but the remaining 40 needed some form of intervention (Table 9).
RECOMMENDATIONS:
Delay discharge check until 24 hours after birth: Mothers deciding to breast feed babies need proper support. It may be a good idea to delay discharge check until 24 hours after birth. This will not only give sufficient time for the mothers to familiarise with breast feeding but also provide staff the opportunity to detect any potential feeding problems.
First time mothers to be properly supervised: First time mothers are especially naive when it comes to breast-feeding and it is important that they get properly supervised.
Request mothers to fill in a questionnaire: It may be a good idea to request mothers to fill in a questionnaire prior to discharge regarding how confident they feel about feeding their child, any feeding concerns, any other concerns etc. The physical, psychological and social well being of mother and newborn must be assessed when discharge planning takes place.7
Policy to transfer babies back to AMU: For babies readmitted in whom the only problem identified on assessment in paediatric ward is poor feeding, there should be a policy to transfer babies back to AMU for breast feeding training and support. This will not only persuade mothers to persevere with breast feeding but will also have a direct impact on reducing early discharges from AMU.
Re audit: The above recommendations to be implemented after discussion with staff at AMU and the audit will be repeated to see if this has resulted in a decrease in neonatal readmissions.
COMPETTING INTERESTS
None Declared
ACKNOWLEDGEMENTS
Dr Bridget Oates, Consultant Paediatrician, Crosshouse hospital for her invaluable support and guidance throughout, Dr Sheena Kinmond, Consultant Paediatrician, Crosshouse hospital, staff at medical records and neonatal secretaries at AMU.
AUTHOR DETAILS
FAHEEM MAZI KOTWAL, MBBS, MRCGP, GP registrar, Ayrshire, United Kingdom
CORRESPONDENCE: Dr F Mazi Kotwal, GP registrar, Riverside Medical Practice, 27 Dalvennan Avenue, Patna KA6 7NA
Email: faheemkotwal@yahoo.co.uk
REFERENCES
1. Jill M. Klingner, Leif I. Solberg, Susan Knudson-Schumacher, Richard R. Carlson, Karen L. Huss. How Satisfied Are Mothers with 1-Day Hospital Stays for Routine Delivery? Effective Clinical Practice, November/December 1999.
2. CDC. Trends in length of stay for hospital deliveries -- United States, 1970-1992. MMWR 1995;44:335-7
3. Danielsen B , Castles AG, Damberg CL, et al. Newborn discharge timing and readmissions: California, 1992–1995. Pediatrics 2000;106:31–9
4. Malkin J,Garber S, Broder M S, and Keeler E,. Infant Mortality and Early Postpartum Discharge Obstet Gynecol 2000;96(2):183-8.#
5. M. B. Edmonson, J. J. Stoddard and L. M. Owens. Hospital readmission with feeding-related problems after early postpartum discharge of normal newborns. Vol. 278 No. 4, July 23, 1997 JAMA
6. Oddie et al Early discharge and readmission to hospital in the first month of life in the Northern Region of the UK during 1998: a case cohort study. Arch. Dis. Child. 2005;90:119-124.
7. Cargill Y, Martel M; Postpartum maternal and newborn discharge: J obstet Gynaecol can 2007;29(4):357-359
We are in the middle of the greatest changes in mental health law in a century. This started with the introduction of the Mental Capacity Act in October 2007, continued with amendments to the Mental Health Act (MHA) in November 2008, and will finish with a final flourish when the Deprivation of Liberty Safeguards come into effect to April 2009.
But what do these changes mean for Psychiatrists and other doctors? This article explores the changes.
The Mental Health Act 1983 (as amended by the Mental Health Act 2007)
Although the structure of the Mental Health Act remains the same – for example, compulsory admission to hospital still requires the recommendations of 2 doctors and the agreement of an Approved Mental Health Professional (the replacement of the ASW), the Act has been amended in the following ways:
Key Change 1
Introducing a Simplified Single Definition of Mental Disorder.
Key Change 2
Abolishing the ‘Treatability’ Test and introducing a new Appropriate Medical Treatment Test.
Key Change 3
Ensuring that Age Appropriate Services are available to any patients admitted to hospital who are aged under 18 (anticipated by 2010).
Key Change 4
Broadening the Professional Groups that can take particular roles.
Key Change 5
Introducing the right for patients to apply to court to displace their Nearest Relative, and including civil partners in the list of potential nearest relatives.
Key Change 6
Ensuring that patients have a right to an Advocacy Service when under compulsion (implemented in 2009).
Key Change 7
Introducing new safeguards regarding Patients and Electro-Convulsive Therapy.
Key Change 8
Introducing a new provision to allow Supervised Community Treatment. This allows a patient detained on a treatment order to receive their treatment in the community rather than as an in-patient.
Key Change 9
Earlier automatic referral to a Mental Health Review Tribunal (Tribunal) where patients don’t apply themselves. & new Tribunal system structure.
Key Change10
New ‘2nd Professional’ role for renewal of section 3.
All these changes need to be seen within the context of the Guiding Principles and the clarified legal status of the Code of Practice (COP).
The MHA tells us WHAT to do
The COP explains HOW to do it
The Guiding Principles help us to apply the MHA and COP in INDIVIDUAL SITUATIONS
The status of the Code of Practice
The Act makes it clear that professionals, including doctors, are expected to follow the guidance of the Code of Practice, or explain why they haven’t done so. It also makes it clear that professionals are expected to take account of a number of issues, the guiding principles, when making decisions.
The Principles:
Purpose
Decisions under the Act must be taken with a view to minimising the undesirable effects of mental disorder, by maximising the safety and well-being (mental and physical) of patients, promoting their recovery and protecting other people from harm.
Least restriction
People taking action without a patient’s consent must attempt to keep to a minimum the restrictions they impose on the patient’s liberty, having regard to the purpose for which the restrictions are imposed.
Respect
People taking decisions under the Act must recognise and respect the diverse needs, values and circumstances of each patient, including their race, religion, culture, gender, age, sexual orientation and any disability. They must consider the patient’s views, wishes and feelings (whether expressed at the time or in advance), so far as they are reasonably ascertainable, and follow those wishes wherever practicable and consistent with the purpose of the decision. There must be no unlawful discrimination.
Participation
Patients must be given the opportunity to be involved, as far as is practicable in the circumstances, in planning, developing and reviewing their own treatment and care to help ensure that it is delivered in a way that is as appropriate and effective for them as possible. The involvement of carers, family members and other people who have an interest in the patient’s welfare should be encouraged (unless there are particular reasons to the contrary) and their views taken seriously.
Effectiveness, efficiency and equity
People taking decisions under the Act must seek to use the resources available to them and to patients in the most effective, efficient and equitable way, to meet the needs of patients and achieve the purpose for which the decision was taken.
In the future, it is likely that doctors will be expected to justify decision making with reference to above principles.
Key Change 1: Definition of Mental Disorder:
The definition of disorders covered by the MHA is now “any disorder or disability of the mind”. This simplified definition now applies to all sections of the Act. The four forms of mental disorder (mental illness, mental impairment, severe mental impairment and psychopathic disorder) have disappeared. This potentially means some people previously excluded are now included. For example, there may be some people with an acquired brain injury who were not covered by the term “mental impairment or severe mental impairment” who could now benefit from the protections of the Act.
The Learning Disability Qualification has been introduced to preserve the status quo (e.g. under section 3, a person with a learning disability alone can only be detained for treatment or be made subject to Guardianship if that learning disability is associated with abnormally aggressive or seriously irresponsible conduct.) and now applies to all those sections that relate to longer-term compulsory treatment or care for a mental disorder (in particular section 3, section 7 (Guardianship), section 17A (Supervised Community Treatment) and forensic sections under Part 3 of the Act). It means that if the use of longer-terms forms of compulsion are being considered solely on the basis that a person has a learning disability, that disability must also be associated with abnormally aggressive or seriously irresponsible conduct. This does not, of course, preclude the use of compulsion for people who have another form of mental disorder (such as a mental illness) in addition to their learning disability.
Key Change 2: The Appropriate Medical Treatment Test
The MHA introduces a new “appropriate medical treatment” test that will apply to longer-term powers of compulsion concerned with treatment(for example, section 3 and Supervised Community Treatment ). As a result, it will not be possible for patients to be compulsorily detained for treatment or compulsion continued unless medical treatment which is appropriate taking into account the nature and degree of the patient’s mental disorder and all other circumstances of the case is available to that patient.
“Medical treatment” includes psychological treatment, nursing, and specialist mental health habilitation, rehabilitation and care as well as medicine. It does not have to be the “perfect” treatment, but doctors will be expected to satisfy themselves that appropriate treatment, taking into account all the circumstances of the case, is available and state in their recommendations in which hospital(s) it will be available to the patient. When making recommendations for section 3, the recommending doctors will need to confirm that there will be appropriate medical treatment available, and state on the recommendation form the hospital, hospitals or part of a hospital that the treatment will be given in.
Example:
Ellie was seen by 2 doctors in A&E after having been found by the police naked and dancing in the street. She was sexually disinhibited, and aggressive both physically and verbally. Ellie was well- known to the AOT team and was assessed by her own consultant and GP. Because they both knew her well, and knew what treatment would be of benefit to her, they felt confident in signing the form saying that appropriate medical treatment would be available, However, given her current presentation, they did not feel it would be safe to admit her to an open, mixed sex ward. Instead, her consultant rang and negotiated with the bed manager that she be admitted to a women only PICU bed. The ward name and hospital name were inserted onto the section 3 recommendation form, and the AMHP was only able to admit Ellie to that ward.
Key Change 3: Admitting young people to suitable environments
The effect of this change is that hospital managers are placed under a duty to ensure patients under 18 who are admitted to hospital for assessment or for treatment under the legislation, or who are voluntary patients are in an environment that is suitable for their age (subject to their needs). There is flexibility in the amendment to allow for patients under 18 years to be placed on adult psychiatric wards where the patient’s needs are better met this way. This is expected to come into force in 2010, by which time it is hoped new services will be available.
Section 140 of the existing Mental Health Act has also been amended to put a duty on Primary Care Trusts to let Local Social Service Authorities know where services especially suitable for admitting young people are to be found. The amendment to section140 has already come into force.
It is also now no longer possible to admit a competent and objecting 16 or 17yr old to hospital for treatment for mental disorder on the say of their parents.
Key Change 4: The Broadening of access to professional roles
This change widens the group of practitioners able to train to fulfil functions previously undertaken by Approved Social Workers (ASWs) and Responsible Medical Officers (RMOs). It does this by introducing two new roles:
Approved Mental Health Professionals (AMHPs): AMHPs are mental health professionals with specialist training in mental health assessment and legislation. The training will be opened up to include mental health and learning disability nurses, clinical psychologists and occupational therapists as well as social workers. AMHPs will assess “on behalf of” Local Authorities, who will continue to be responsible for approving AMHPs and for ensuring a 24hr AMHP service is available.
The final part of this change concerns the Approved Clinician (AC), the professional status/qualification a practitioner must obtain before they can take on the responsibilities of a Responsible Clinician (RC) for a particular person.
The RC is the old Responsible Medical Officer role which has now been opened up to include social workers, mental health and learning disability nurses, clinical psychologists and occupational therapists. The RC has overall responsibility for a patient’s case. This change allows more flexibility – for example, making it possible to transfer responsibility to professionals from different groups of staff as the patient’s needs change.
Directions make it clear that all professionals who want to be a RC need to meet particular levels of competence, undertake a short course to demonstrate their state of readiness and be approved by Strategic Health Authority as an AC.
Transitional arrangements for doctors:
Doctors with Section 12 status: for doctors with section 12 status, that status will continue unaltered for as long as had been expected to. For example, a doctor whose section 12 approval was due to expire in April 10, this will still be the case.
Doctors with section 12 status who have acted as an RMO for a patient in the 12 months prior to 3rd Nov 2008: such doctors will automatically be given Approved Clinician Status so that they can be Responsible Clinicians for people detained under the Act. If their section 12 status was due to expire during the next 12 months, it will be extended until 2rd Nov 2009.
Doctors (such as community consultants) who are section 12 approved, have been responsible for a patient’s medical treatment but have not acted as an Responsible Medical Officer (RMO) in the 12 months prior to 3rd Nov 08: such doctors will need to complete a course for Approved Clinicians before 2nd Nov 09, and as long as they do so their approval will last for a full 3 year period until 2nd Nov 2011.
In the future, a doctor (but not a professional from one of the other 4 eligible groups) who completes an Approved Clinician Course will also automatically receive section12 approval.
Accessing Approved Clinician Training:
AC training will be the responsibility of Strategic Health Authorities. Generally, people wishing to be Approved Clinicians will need to be recommended by employers – and will need to be able to demonstrate how they meet the competences for the role prior to undertaking the AC training course. The course is likely to be a few days at most, so preparatory training will be important. Each area will need to develop its own systems and policies, these are likely to be influenced by the pilot studies that have been taking place around the country in preparation for this change in the law.
Responsibilities of the Responsible Clinician (RC):
Renew detention with the agreement of another professional from a different professional background
Discharge patients from detention
Grant leave for patients.
Discharge patient on to supervised community treatment, with the agreement of an amhp
Set conditions on the community treatment order for sct with the agreement of an amhp
Extend sct with the agreement of an amhp
Recall sct patients to hospital, if necessary
Re- detain an sct patient by revoking the community treatment order, with the agreement of an amhp
Discharge patients from sct
Key Change 5: Nearest Relative Changes
Changes give patients the right to make an application to court to displace their nearest relative and introduces a new ground for displacement: that the current Nearest Relative(NR) is “otherwise unsuitable for the role”. The provisions for determining who is the NR have also been amended to include civil partners on equal terms with a husband or wife.
Key Change 6: Independent Mental Health Act Advocate (IMHA) service
Gives the right for patients who are subject to compulsion to have access to advocacy services. (that is, those on section 2, 3, section 7 Guardianship, SCT and similar forensic sections. Those on short term sections such as section 136 will not be eligible) Advocates will have the right to meet with patients in private. They will also have access to patient records, where a patient with capacity gives consent, and to meet and discuss the patient with professionals, such as doctors, involved in their care. In the case of patients lacking capacity to make such decisions, access must not conflict with decisions made by a deputy, Lasting Power of Attorney (LPA) donee or Court of Protection, and the person holding the records must agree that such access is “appropriate”. The principles of the COP should be used to decide whether it is appropriate to disclose information in a particular case.
It is planned that the new “Independent Mental Health Advocacy” services will be available from April 2009.
Key change 7: ECT and Patient Rights
Except in emergencies, detained patients may in future only be given ECT if they have capacity and agree or, (as now) if they do not have capacity, the ECT is authorised by a Second Opinion Appointed Doctor (SOAD).
In other words, this means that a detained patient can refuse to have ECT, and, except in emergencies, this can be overturned only if a SOAD agrees that the patient does not have capacity to make the decision and that giving the ECT treatment would be appropriate. In this case, the SOAD also needs to be sure that there is no valid advance decision refusing the use of ECT. If such an advance decision has been made, then ECT cannot be given, except in an emergency.
In the case of young people (aged under 18), even if the patient agrees, unless it is an emergency, they may only be given ECT with the additional agreement of a SOAD. These rules apply to young people whether or not they are detained.
In all these cases, it is only an emergency if the ECT is immediately necessary to save the patient’s life or prevent serious deterioration in their condition.
Key Change 8: Supervised Community Treatment
Introduces Supervised Community Treatment (SCT) for patients following a period of detention in hospital for treatment (mainly those on section 3 or unrestricted forensic sections such as section 37). It will allow a small number of patients who currently disengage from support once discharged from hospital to be cared for in the community, subject to the possibility of being recalled to hospital if necessary. This is to ensure they continue to get the treatment they need. There is no lower age limit.
As a statutory framework, SCT is intended to support such vulnerable patients (including some who may pose a risk to others) to:
live in the community;
help improve engagement with the care team by shifting the balance of power more in the patient’s favour;
act upon any clinical signs of relapse at an early stage;
be a mechanism to manage actual or potential relapse; and
ensure that services are aware of and responsive to any changes of circumstances which arise for the patient or their carers.
The criteria for consideration of the use of SCT include:
the person is suffering from a mental disorder and detained under s3 (or similar forensic section) for treatment;
the need for medical treatment;
the existence of a risk to the patient’s health or safety or that of others;
that appropriate treatment is available; and that the patient does not need to be in hospital to receive it but does need to be liable to recall to hospital to ensure that the risk can be managed; and
that it is necessary for the patient’s health or safety or the protection of others that the patient remains liable to recall.
Key Change 9: Changes to the Tribunal system
Changes to the MHA have introduced earlier referrals by Hospital Managers of detained patients who have not used their rights of appeal to the Tribunal.
To protect patients, everyone who is compulsorily admitted to hospital must have their detention review by the Tribunal service within the 1st 6 months, and every 3 years after that. If the patient themselves doesn’t request a tribunal referral within the above timescales, the hospital managers must do so.
For under 18s, they must be seen annually by the tribunal.
The Secretary of State has the power to reduce further these periods for referral by Hospital Managers in the future.
The MHA 2007 has also introduced the immediate referral of patients who have had their SCT revoked.
The structure of the Tribunal Service has been changed to provide a ‘1st’ and ‘2nd’ tier. The purpose of the 2nd tier is to allow appeals and clarification of legal points, without having to use the judicial review process.
In addition, new rules have been issued as guidance for professionals about what is expected to be covered in reports to tribunals.
Key Change 10: the role of the 2nd Professional in the renewal of section 3
In addition to the Responsible Clinician, the written agreement of a second professional is needed to renew section 3.
The second professional must
come from a different professional discipline compared with the RC
be involved with the care of the patient
be able to reach independent decisions
have sufficient expertise and experience to make a judgement about whether the criteria for detention continue to be met.
Even if the RC disagrees with the view of the 2nd Professional, they should not normally seek to find another professional. In such circumstances the section 3 would not be renewed. In very exceptional circumstances where a different opinion is sort, this must be brought to the attention of the hospital managers who are also required to consider and approve the renewal of the section.
ACKNOWLEDGEMENTS
This article is based on work undertaken as part of the NIMHE Implementation team for the Mental Health Act, and forms part of the National Training Materials available to all staff working within Mental Health
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
CLAIRE BARCHAM, National Coordinator, AMHP leads Network/ NIMHE National Implementation team member,United Kingdom.
CORRESPONDENCE: CLAIRE BARCHAM, ASW Training and Development Coordinator, C&I MHSCT Training and Development Team, Room 110, West Wing, St Pancras Hospital, 4 St Pancras Way, London NW1 0PE
Email: claire.barcham@candi.nhs.uk
For more information, please visit https//:mhact.csip.org.uk
The prevalence of behavioural symptoms in dementia is well known. Patients may exhibit outright psychotic features (delusions, hallucinations) and commonly experience a host of symptoms such as screaming, hitting, agitation, and wandering. The patient often appears to be upset and suffering, and whether the symptom is the cause of that distress, or a result of some inner discord, is unknown. Clearly, these behaviours are upsetting to the patient’s family, loved ones, and their caregivers. Physicians are driven to attempt to reduce the suffering of patients and support the family and other professional caregivers. Hence, medications are often the first approach to dealing with such problems. Given the similarity between these symptoms and those seen in patients with schizophrenia, antipsychotics are often the first choice. As a result, nearly 1 in 4 elderly nursing home residents in the United States are given antipsychotic drugs1.
Unfortunately, they are not very effective. Schneider, in an extensive review of the efficacy of antipsychotics found an effect size of only 18% favouring these drugs over placebo2. But much more worrisome are the potentially lethal, or permanently disabling, side-effects. A meta-analysis of 15 randomized controlled trials evaluating dementia patients with behavioural and psychological symptoms concluded that there was an overall increase in the risk of death (odds ratio 1.54, 95% CI 1.06–2.23; p = 0.02) when atypical antipsychotics were compared to placebo3. This means that for every 9 to 25 persons helped in these trials, therepossibly will be 1 death due to the treatment itself. Older “typical” antipsychotics may not be any less risky. A comedian once commented, “I don’t consider ‘death’ a side-effect, I think it’s a primary effect!” In addition, the risk of the patient acquiring the permanent though not lethal side-effect of tardive dyskinesia is higher in older patients than younger ones. Finally there are other serious potential adverse affects such as falls, confusion, and weight gain or increased risk of diabetes.
Some have written that using antipsychotics in dementia is “off label” prescribing, a term which is usually reserved for the use of a drug for which there has been little study but presumed efficacy based on clinical experience. However, the “Black Box Warning” on the use of antipsychotics in dementia is non-ambiguous: these drugs are “not approved for dementia-related psychosis.” Yet one company, Eli Lilly, incurred a $1.4 billion fine from the FDA for marketing Zyprexa (Olanzapine) in the use of dementia related psychosis.
Clinical guidelines by both Canadian and American interests have clearly described these risks and suggest that antipsychotics be used only as a last resort4,5. Searching for a treatable medical problem, ranging from a serious condition such as pneumonia, to a painful irritation like an ingrown toenail, is the first step. But perhaps most importantly, providing a caring, nurturing and non-stressful environment is likely to be most helpful6. The work of Tom Kitwood in defining the problematic behaviours of caregivers which may increase dementia-related agitation is refreshing7. Unfortunately, few long term care programs have provided for this type of caregiver training. Other interventions, such as music therapy, caregiver support, and caregiver stress reduction may be helpful but have not been extensively studied8. So what’s the clinician to do if an antipsychotic medication is to be used “as a last resort?”
For the patient’s protection and to reduce medical-legal risks, I believe that a formal informed consent process should be initiated. Such a process should entail adequate description of the risks of the treatment, the potential benefits, and the plan for further monitoring and adjustments to the treatment course. As in any informed discussion, it should include the alternatives available, along with the risks and benefits of each alternative. Finally, it should include a discussion of what is likely to happen if no pharmacologic treatment is provided. In most cases, these discussions will necessarily be conducted with the surrogate decision-maker (usually a family member), given the occurrence of psychotic symptoms later in the course of dementia when decision-making capacity is usually severely impaired.
The key elements of the discussion, including open and specific disclosure of the risks, should be documented in written form and entered into the patient’s medical record. An example of such documentation is in Appendix 1. Some clinicians with whom I have discussed this idea have responded that the caregivers would not be likely to approve the use of medications if these risks were so openly discussed. My response is simple – the ethical thing to do is always to inform the patient (or his or her surrogate) before initiating treatment. If that leads to a reduction in the use of these drugs, I would not be unhappy.
CORRESPONDENCE: KENNETH BRUMMEL-SMITH .M.D. Charlotte Edwards Maguire Professor and Chair, Department of Geriatrics, Florida State University College of Medicine, 1115 West Call St, Suite 3140-D, Tallahassee, FL 32306-4300, 850-644-2291
REFERENCES
Kamble P, Chen H, Sherer J, et al. Antipsychotic Drug Use Among Elderly Nursing Home Residents in the United States, Am J Geriatr Pharmacother 2008;6:187–197.
2 Schneider LS, Pollock V, Lyness S. Further analysis of meta-analysis. J Am Geriatr Soc. 1991;39:441-442.
3 Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA 2005;294:1934-43.
4 Gauthier S, Herrmann N, Diagnosis and treatment of dementia: 6. Management of severe Alzheimer disease. CMAJ 2008;179(12):1279-87
5 American Psychiatric Association (APA). Practice guideline for the treatment of patients with Alzheimer's disease and other dementias of late life. Am J Psychiatry 1997 May;154(5 Suppl):1-39.Updated Oct. 2007.
6 Verkaik R, van Weert JC, Francke AL. The effects of psychosocial methods on depressed, aggressive and apathetic behaviors of people with dementia: a systematic review. Int J Geriatr Psychiatry 2005;20:301-14.
7 Kitwood T. Dementia Reconsidered, Philadelphia, Open University Press.1997
8 Brummel-Smith K, Alzheimer’s disease and the promise of music and culture as a healing process, in The Oxford handbook of Medical Ethnomusicology, Koen BD, Lloyd J, Barz G, Brummel-Smith KL (eds), Oxford University Press, 2008, Oxford, pp.185-200.
Appendix 1
Consent for Use of Antipsychotic Medication
Indications: Antipsychotic medications are sometimes used to treat behavioral symptoms in patients with dementia. These symptoms include delusions (fixed beliefs that are not real), hallucinations (seeing or hearing things that are not real), and others. The Federal Drug Administration (FDA) has approved the use of antipsychotic medications in the treatment of schizophrenia and other mental conditions. While the FDA has not approved these medications in treatment of behavioral symptoms of dementia, physicians may use them for “off-label” purposes if it is believed they well help the patient.
These medications should be used as a last resort to help patients with dementia who are suffering behavioral symptoms. Other “treatments” include changing the person’s environment, getting them more involved in activities, making sure there are no medical problems causing the symptoms (like pain), and making sure other medications the patient is taking have not caused the symptoms. If the patient is not suffering from the symptoms (that is, they are not bothered by them) and they do not prevent the caregivers from giving good and safe care, then it is best not to give them medications for the symptoms.
These types of medications have two very serious potential side-effects, which is why it is important that you know both the risks and the benefits of using them.
Anticipated duration of use: ______________________________
Alternatives: Sometimes other medications, like sedatives, are used if the patient is anxious. But they also have side-effects and may not help the severe behavior problems and usually do not help delusions and hallucinations. Another alternative is to keep trying the non-medicine interventions described above. The final alternative is to give no treatment and just live with the symptoms. As the person’s dementia gets worse over time, the symptoms do usually go away. But that may take some time.
Expectations of Treatment: If the medication is used, we expect the person with dementia to have less suffering. The patient should be calmer and feel less distressed. The hallucinations and/or delusions may not go completely away, but they should be less bothersome to the patient. Caregiving should be more accepted by the patient. Hopefully, the patient will not experience any side effects but many patients do have some side effects so it is important to report any change that may be due to the medication.
Side effects and complications include but are not limited to:
The most serious concern is that older patients with dementia who are given these medications have an increased risk of death compared to patients given placebos (sugar-pills). That risk is about 1.7 times the risk of using the placebo. Most of the deaths were due to heart problems or pneumonia.
The second most serious concern is the development of a permanent side-effect called “tardive dyskinesia.” It is an uncontrolled movement of the face and mouth. This occurs in about 25% of patients who take the medication for a long time. Rarely, it can occur even in patients who only take a few doses of the medication.
Neuroleptic malignant syndrome – a rare but potentially fatal side effect with fever, blood pressure problems, and irregular pulse.
Contraindications: These medications should not be used if you or your loved-one has an allergy to them. A history of having bad reactions to this medication (or ones similar to this medication) is also a concern and should be discussed with the doctor.
*******************************************
I understand the above, and have had the risks, benefits, and alternatives explained to me. I have had an opportunity to ask questions about the recommended treatment. I understand that no guarantees about results have been made. I give my informed consent for the use of:
______________________________.
_______________________________
Patient Signature
_________________________
Date
_______________________________
Witness
_________________________
Surrogate Signature (if the patient does not have decision-making capacity)








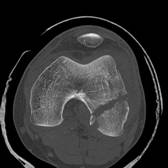

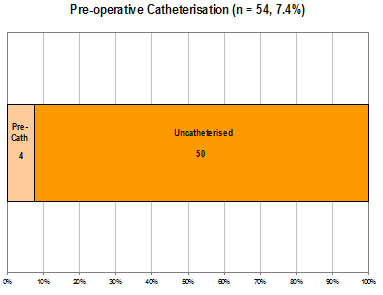
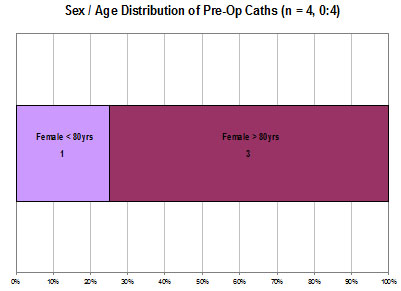
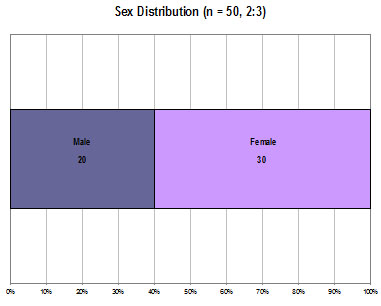
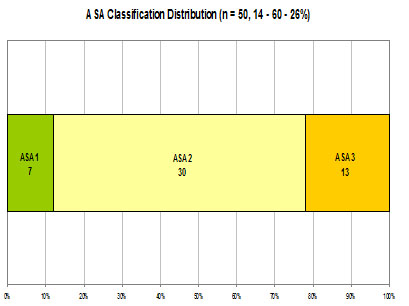
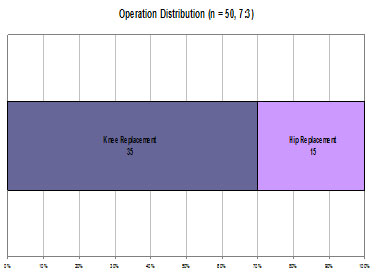
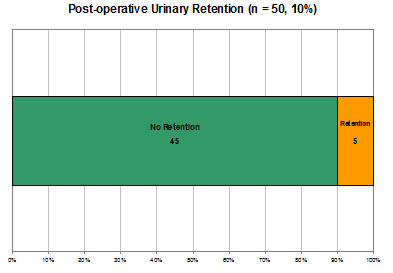
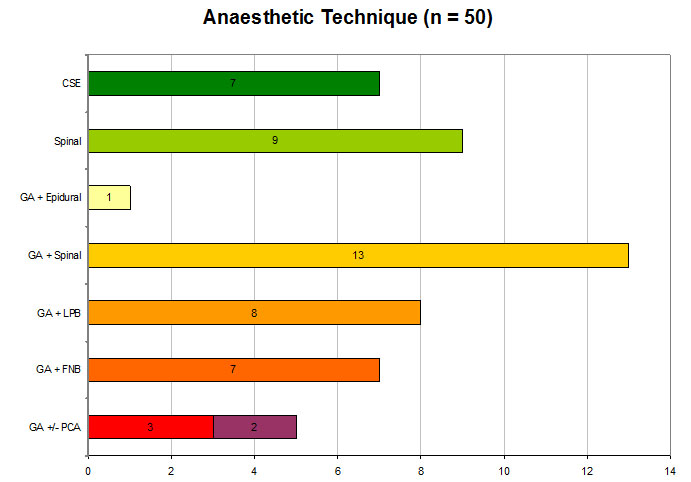
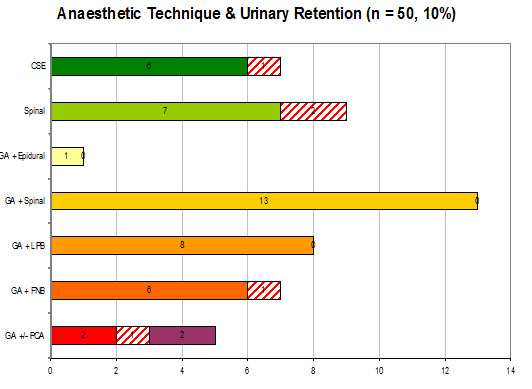
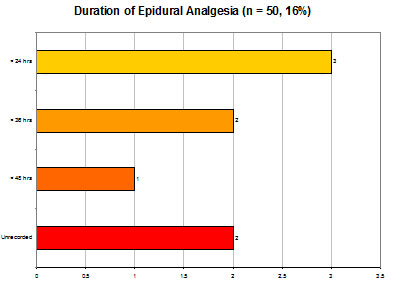
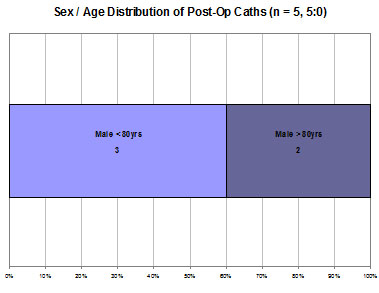
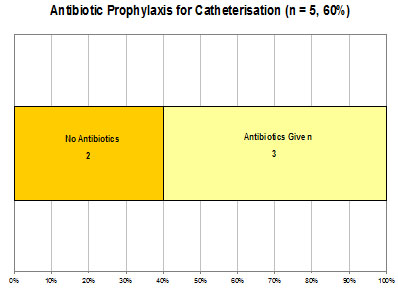
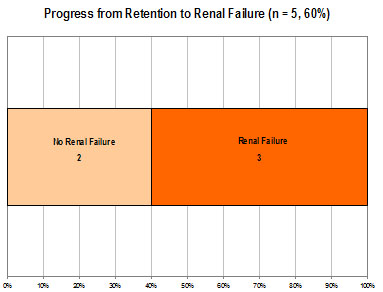
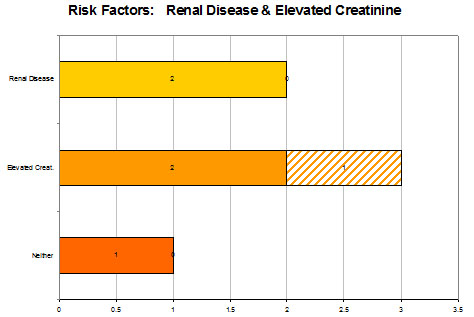
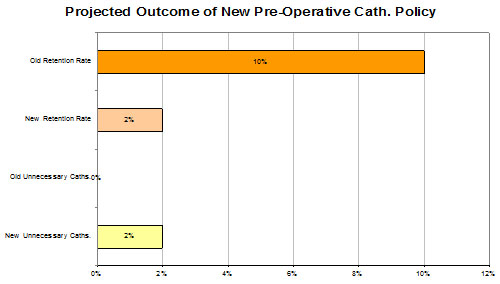
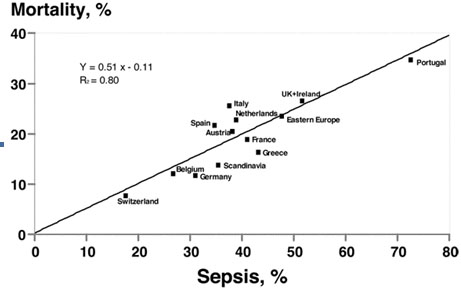
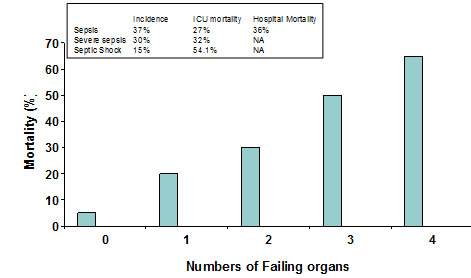
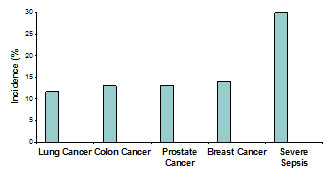
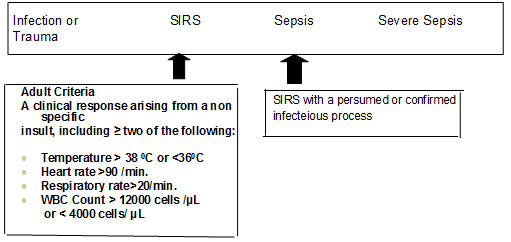
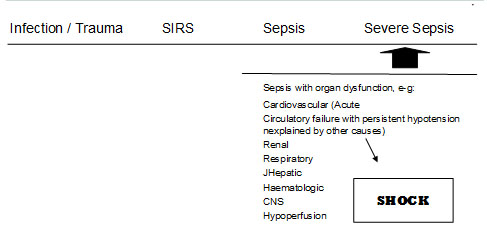
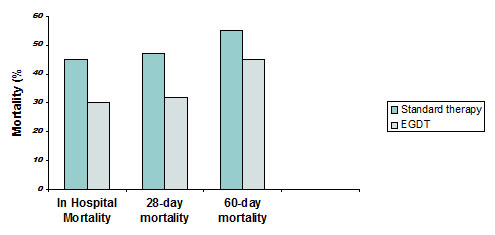
BJMP December 2008 Volume 1 Number 2
Kenneth Brummel-Smith
Khadija Qureshi and Abid Rajah
Claire Barcham
Tint Tint Wai and Dilip Patil
Riaz AA, Singh A, Patel A and Ali A, Livingstone JI.
Sumit Datta
Chess Denman
SKM Annamalai, JR Berstock, MN Shannon
F Mazi Kotwal and M S Anodiyil
Mashud Souroyer and Mathavi Uthayanan