BJMP 2009: 2(3) 57-58
A case of accidental carotid artery cannulation in a patient for Hemofilter: complication and management
Sanil Nair , Harshal Wagh , Kavita Mordani and Salim Bhuiyan
In the 'Author Details' block of the left column on page 58, the correct details of SALIM BHUIYAN should be
A 75 year old woman with a history of prosthetic mitral valve replacement, atrial fibrillation & TIA on warfarin was scheduled for TURBT to be done under spinal anaesthetic. Warfarin was stopped one day prior to admission and heparin infusion commenced on admission, with target APTT 2.5 times the normal. Heparin was stopped 4 hours prior to the spinal anaesthetic, which was difficult due to ankylosing spondylitis and needed four attempts. However, after an atraumatic tap and good sensory motor block, surgery was commenced without incident. Post-operatively, the patient developed a lower respiratory tract infection for which co-amoxyclav was commenced. On the fourth day post-op, the patient developed sudden onset, right leg weakness and paraesthesia, with right lower limb power 3/5, decreased tone and absent reflexes, leading to the diagnosis of a spinal haematoma post spinal anaesthesia. However on further examination, she was also noted to be anaemic with a drop in haemoglobin to 6g/dl, with an INR of 3.4 and an acute renal impairment with a serum creatinine of 120. In addition, bruising in the right flank, abdominal pain and a right iliac fossa mass were also noted. An urgent MRI was booked, but as the patient was haemodynamically unstable, a CT scan was deemed more appropriate, which showed a retroperitoneal bleed into the right illio-psoas. This was confirmed with a spinal MRI done subsequently, which also ruled out any spinal haematoma. The patient was treated conservatively with 5units PCV and 3units FFP. Her clotting profile gradually normalised as did her renal function and her right sensory-motor deficit continues to improve.
Discussion:Retroperitoneal bleed The predilection for bleeding into the retroperitoneal space has not been fully explained but a unique weakness of the vascular and connective tissue has been suggested.2 It is also most commonly seen in association with patients on anticoagulation therapy or haemodialysis, or with bleeding abnormalities,3 and may represent one of the most serious and potentially lethal complications of anticoagulation therapy. The incidence of retroperitoneal haematoma has been reported at 0.6-6.6% of patients undergoing therapeutic anticoagulation.4, 5, 6 Warfarin, unfractionated and low-molecular weight heparin have all been implicated.7 The risk of bleeding during unfractionated heparin therapy has been estimated to be two- to five fold greater than that with warfarin.8 However, it is nonetheless important to note that the therapeutic index of warfarin is narrow 9 and anticoagulant control is easily deranged by drugs (such as antibiotics) and co-morbid factors such as renal or hepatic dysfunction. Frequent INR measurement is the best way to avoid haemorrhagic complications. Patients report lower abdominal or hip pain radiating to the groin or anterior thigh. Bleeding into the psoas muscle causes spasm and hip flexion and, as it extends, flank or thigh bruising may appear. Femoral nerve compression reduces quadriceps power and causes loss of knee jerk and paraesthesia in the area of cutaneous supply. CT scan is the investigation of choice10 but ultrasound is also sensitive and is more rapidly available. Delay in diagnosis is potentially fatal because severe haemorrhage can supervene. Locally the haematoma may cause ureteric obstruction and acute renal failure, or femoral nerve compression.11 (Both of which were seen in the case reported). Treatment options are surgery 12 and conservative management consisting of treating the anaemia associated with the bleed and correcting the coagulopathy.13 Options to treat the coagulopathy would mainly depend on how quickly correction is required, to what range and how long normal clotting indices would be safe in a patient on therapeutic or treatment anticoagulation. Fresh frozen plasma (FFP at a dose 15ml/kg) is given for rapid but short-lived correction with the usual risks of transfusion of blood products. Vitamin K (>2.5mg) is given for a slower but more prolonged correction (leaving patients with artificial valves at risk of thromboembolic events and valve failure). Over-anticoagulation due to warfarin can be reversed completely and immediately by infusion of a complex concentrate of factors 2, 7, 9 and 10.14Spinal haematoma The true incidence of spinal haematoma is unknown and due to its rarity it is very difficultto evaluate risk factors prospectively and any properly poweredstudy would require many thousands of patients to investigatethis. Therefore, data on the incidence of spinal haematoma followingneuraxial blockade are mainly based on audit studies and casereports. Tryba15 reported that the incidence of spinal haematoma afterepidural and spinal anaesthesia is 1 in 150,000 and 1 in 220,000, respectively. The insertion and removal of an epidural catheter appeared to be of far greater importance in the genesis of a spinal hematoma.16, 17 The incidence of spontaneous spinal haematomais rarer still and is estimated at 1 patient per 1,000,000 patientsper year. 18 Central neuraxial blockade has a low incidence of major complications, many of which resolve within 6 months. 19 The symptoms of an acute spinal hematoma include a sharp irradiating back pain of radicular character, and sensory and motor deficits which outlast the expected duration of the anaesthetic. Not all of these symptoms have to be present at the same time. The clinical suspicion can only be confirmed by means of an emergency CT-scan (with myelography) or magnetic resonance imaging.20 The only treatment of a compressing spinal hematoma is an emergency decompressive laminectomy with evacuation of the hematoma. Final neurologic outcome depends on21, 22 the speed with which the hematoma develops; the severity of the preoperative neurologic deficit; the size of the hematoma; and most importantly, the time span between hematoma formation and surgical decompression. Complete recovery of neurologic function is possible if surgery is performed within 8 hours of the onset of the paraplegia. Conclusion The aim of this report is in no way to undermine the importance of Alderman’s advice to suspect the spine as an area of bleeding in patients on anticoagulant therapy. The above case is a reminder to consider retroperitoneal bleeding as one of the differential diagnoses of spinal haematoma in an anticoagulated patient who develops sudden onset spinal pain, with or without neurological deficit post spinal anaesthetic. The presenting symptoms are similar and early management is equally important in terms of associated morbidity when management is delayed.
Malnutrition is defined as state of nutrition in which there is a deficiency or excess of energy, protein and other nutrients causing measurable adverse effects on tissue/body form, function and clinical outcome. (1) It is recognised that 30% of in-hospital patients are malnourished (undernourished) on admission and the majority of these will lose further weight while in hospital. (2) In this review article the term undernutrition will be used instead of the generalised term malnutrition. Undernutrition develops due to increased losses (vomiting, diarrhoea, malabsorption), decreased intake (anorexia, vomiting, nausea, dysphagia), increased requirements (catabolic state) or a combination of all these processes.
Is undernutrition important?
Consequences of undernutrition include reduced muscle mass, impaired immune function, poor tissue viability, poor clinical outcome and psychosocial effects. (3) Reduced muscle mass decreases cardio-pulmonary function, lean muscle mass and muscle weakness. Impaired immune function increases infection and sepsis risk. Poor tissue viability can cause pressure sores and poor wound healing. Undernutrition can amplify the length of hospital stay. Psychosocial effects include altered mood and poor quality of life. (4) It is therefore essential that undernutrition is properly treated to diminish patient morbidity and mortality.
How to recognise undernutrition:
1. Malnutrition screening tools
Screening tools should be performed easily with low-level staff training. Hospital patients at risk of undernutrition are identified by screening methods such as MUST (Malnutrition Universal Screening Tool) (5), SGA (Subjective Global Assessment) (6) or MNA (Mini Nutritional Assessment – validated for > 65 years) (7). These screening methods usually consider current body mass index (BMI), recent weight loss and possible future weight loss. MUST is currently well advertised as a nutritional screening tool within UK hospitals. The British Association of Parenteral and Enteral Nutrition have endorsed this 5 step-screening tool. The MUST score (low, moderate, high risk) has been shown to correlate with mortality (low risk group 8% vs. high risk group 32%, p 0.01) and length of hospital stay (low risk group 15 days vs. high risk group 28 days, p 0.02) (8). See Table 1.
Table 1
MUST Screening tool (5)
Step 1: BMI (can use alternatives such as ulna length for height or mid-upper arm circumference (MUAC) as approximation for BMI: MUAC <23 cm = BMI 20kg/m2, MUAC >32cm = BMI >30 kg/m2)
Step 2: Percentage weight loss
Step 3: Establish Acute Disease Effect and score
Step 4: Add scores step 1,2,3 together to obtain overall risk of malnutrition
Step 5: Develop care plan
2. Assessment of nutritional status:
If a patient is found to be at risk of undernutrition, following screening, then a formal nutritional assessment ensues. This assessment involves anthropometrics, biochemical testing, clinical methods and dietary history.
a) Anthropometrical data: appropriately trained staff can perform weight, height, waist circumference, mid-upper arm circumference and skinfold thickness measurements. Indices can subsequently be calculated. These include percentage weight loss, BMI and waist-hip ratio.
b) Biochemical data: information acquired from blood testing includes renal function as a marker of hydration. Also sepsis markers including CRP, ESR and WBC’s are valuable surrogate markers for stress response. Albumin is a poor marker of nutritional status. (9)
c) Clinical: medical history including past and present is valuable. It is essential to obtain plans regarding fasting for investigations. Knowledge of current treatment that may cause decreased intake or increased losses is essential.
d) Dietary History: there are assorted techniques of obtaining dietary history. Mostly recall, record diary and food frequency questionnaires methods are utilised.
The overall nutritional assessment entails considering all the information obtained from these different methods. Subsequently a clinical decision is reached regarding the overall nutritional status.
How to assess nutritional requirements:
In-patient energy requirements are calculated using a combination of:
a) basal metabolic rate equations such as Schofield, Harris Benedict and Ireton Jones
b) stress factors or weight gain/loss
c) combined factor for activity level and diet induced thermogenesis.
The basal metabolic rate is typically calculated using the Schofield equation (10). Schofield estimates basal metabolic rate of a healthy individual. An adjustment is then made for stress or weight gain/loss. Stress factors have been published for various clinical conditions including brain injury, infection, pancreatitis and surgery. Finally a combined factor (activity and diet-induced thermogenesis) is added to calculate total energy requirements. This combined factor is adjusted depending on patient mobility. Community patient’s energy requirements are calculated using a separate method. Occupational and non-occupational activity is estimated to determine a physical activity level which is multiplied by basal metabolic rate to achieve overall energy requirements.
Nitrogen/protein requirements are estimated using current patient clinical state i.e. hypermetabolic, depleted or normal state. Normal state nitrogen requirements are 0.14-0.20 g/kg/day. Depleted state patients nitrogen requirements are 0.20-0.40 g/kg/day. (1g nitrogen = 6.25g protein)
Methods of treating undernutrition
Following identification of undernutrition a patient’s treatment can be instituted. Undernutrition is typically treated using a graded stepwise approach and subsequently monitoring response. If however it appears clinically obvious that the first steps would not be advantageous then treatment can be commenced at a more aggressive phase. Improving energy intake using the following methods can treat undernutrition:
Step 1. Increase frequency and quantity of food intake. Consider nutrient dense foods. Encourage foods that are energy and nutrient dense such as meat, fish, cheese, eggs, dairy produce and snack foods.
Step 2. Increase nourishing drinks including milk based drinks, soups, fruit juices and sugary drinks. Nourishing drinks are simple to make and can provide high calories in a small quantity.
Step 3. Food fortification. This essentially increases the energy density of foods by adding high-energy components such as addition of cheese, milk powder, cream, jam and butter to other foods.
Step 4. Supplements. These can be milk, yoghurt or juice based. They contain varying calories (1-2kcal/ml) and protein (4-6g protein/100ml). Supplements are very useful at boosting energy intake. Most are nutritionally complete but others contain calories only. Examples include Ensure Plus, Fortisip, Calogen and Calshake.
Step 5. Enteral feeding. Enteral feeding is used to provide either supplementary or complete nutrition to patients that are unable to maintain adequate nutrition by oral route. It is only likely to benefit malnourished patients or those at risk of malnutrition. This includes patients that have had a failed trial of diet modification or supplementary feeds or patients at pulmonary aspiration risk from oral nutrition.
Step 6. Parenteral nutrition. The development of parenteral nutrition in the 1960’s meant that feeding was possible even in patients that did not have a functioning gastrointestinal tract. Although it is mentioned in this article as a final step in nutritional support it may also be appropriate to use early depending on clinical scenario.
Enteral versus Parenteral feeding
Enteral feeding produces gastro-intestinal luminal contents that can decrease the possibility of gut atrophy. Maintaining a normal intestinal mucosa reduces the hazard of bacteria and toxins crossing the gastro-intestinal wall and therefore can decrease proinflammatory mediator levels. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. (11) Hernandez et al have shown that enteral feeds decrease gut mucosal atrophy in critically ill patients. (12) A meta-analysis has shown that in acute pancreatitis use of EN was associated with a significant reduction in infectious morbidity, hospital length of stay, and a trend toward reduced organ failure when compared with use of parenteral nutrition. (13) However it is important to note that many of the studies involving parenteral nutrition had full dose daily calorie intake whereas enteral feeding studies were less likely to reach estimated energy requirements. This is significant since ill stressed patients should not be given full calorie energy requirements in the first 24-48 hours of commencing feeding. Therefore the parenteral feeding groups were disadvantaged in that the patients were overfed initially and received excess energy calorie intake. National Institute of Clinical Excellence states that parenteral nutrition is only to be used in patients with “inadequate or unsafe oral and/or enteral nutritional intake and a non-functional, inaccessible or perforated (leaking) gastrointestinal tract.” (14) Enteral nutrition can be provided by a number of methods including nasogastic tubes, nasojejunal tubes, gastrostomy tunes (including PEG tubes) and jejunostomy tubes (including PEG-J and D-PEJ). Parenteral nutrition can be given peripherally for approximately 14 days but central access should be used if greater than 14 days. Refeeding syndrome
Refeeding syndrome is a potentially lethal condition with severe electrolyte and fluid shifts with resulting metabolic disturbances in malnourished patients. (15) It is caused by refeeding in malnourished patients with resulting insulin release and intracellular movement of potassium, phosphate and magnesium and increased thiamine uptake. It is essential that patients are correctly identified (See Table 2) and electrolytes corrected and intravenous Vitamin B and C is given. Feeding should be initiated slowly. Fluid balance and electrolytes should be monitored closely.
Table 2
NICE guidelines: Risk of refeeding syndrome (14)
>1 of
BMI <16.5 kg/m2
Weight loss >15%
No food intake 10 days
Decreased magnesium/phosphate/potassium
>2 of
BMI <18.5 kg/m2
Weight loss <10%
No food intake 5 days
Alcohol abuse, Insulin, Chemotherapy
Cardiovascular disease and nutrition
Research has confirmed link between cardiovascular disease and serum cholesterol. The NHANES II data has shown that patients who died form myocardial infarction had increased cholesterol. (16) Hooper et al confirmed that dietary fat is linked to cardiovascular risk. (17) This group demonstrated that decreasing total dietary fat over 6 month period reduced cardiac events by 16%. The Seven Countries Study illustrated that cardiovascular mortality was linked to saturated fat intake. (18)
There has been recent interest in the role of the Mediterranean diet in the prevention of cardiovascular disease. (See Table 3)
Table 3
Mediterranean Diet Studies
Population Studies CARDIO2000. Panagiotakos et al 2002. (28) Greece. 2000-2002. CVD group versus control group. Intake of Mediterranean diet type foods significantly decreased risk of developing CVD. The daily use of olive oil and consumption of vegetables, legumes, cereals and fish was associated with 23% risk of developing acute coronary syndromes. Trichopoulou. 2005. (29) Studies relationship between Mediterranean diet and survival in 1302 Greek patients with CVD. Patients with higher compliance with Mediterranean diet had lower cardiac mortality. Martinez-Gonzalez. 2002. (30) Case-control study. Examined the relationship between a Mediterranean diet and risk of first MI. Better compliance with Mediterranean diet lowered risk of MI.
Intervention Studies Medi-RIVAGE. Dietary intervention Study. (31) 3 month diet. Compared Mediterranean diet and low fat diet. There was greater reduction in cardiovascular risk in Mediterranean diet group compared to low fat group (15% vs 9%). GISSI-Prevenzione. Barzi et al. (32) Supplement of Vit-E and omega-3 FA’s given to survivors of recent MI. Also informed to increase intake of Mediterranean diet foods. Outcomes showed that lower chance of premature death if higher intake of Mediterranean foods. Lyon Diet Heart Study. (33) Key study in relation to Mediterranean diet and CVD. Secondary prevention trial. Examined the effects of a Mediterranean diet in survivors of first MI. Experimental group supplied with margarine with high levels of alpha-linolenic acid (n-3 FA). Mediterranean diet group had lower total mortality (70%).
Patients were previously educated regarding low fat diet benefits but Mediterranean diet appears to have enhanced beneficial effects. There is however some complexity with definition of a Mediterranean diet. The diet is based on dietary patterns of Greece, Crete and Southern Italy in 1960’s. This diet was abundant in plant foods, fresh fruit, olive oil as principal fat source (monounsaturated fatty acid), low red meat intake, fish (polyunsaturated fatty acid) and red wine in low to moderate amounts. In respect to dietary fats the Mediterranean diet is low in saturated fat but high in monounsaturated fatty acid and polyunsaturated fatty acid.
Diabetes and nutrition
The diabetic diet is essentially a healthy diet. The total fat intake should be less than 35% with saturated fat less than 10%. Total monounsaturated fatty acid 10-20% and polyunsaturated fatty acid less than 10% which corresponds to oily fish 1-2 per week. Interestingly polyunsaturated fatty acid supplements should be avoided in this group as they have been shown to increase LDL-cholesterol. Diabetic patients should also be encouraged to eat regular starchy carbohydrate, avoid sugar, increase fibre, eat regular meals and snacks and avoid diabetic foods.
Cancer and nutrition
Is there a link between diet and cancer?
The World Cancer Research Fund states that 30% of all cancers could be prevented by a change in diet, increased physical activity and healthy weight. Animal studies and metabolic studies have been performed that reveal evidence linking diet and cancer. An ecological study linking diet and cancer compared risk of cancer against intakes of fat, cereals and vegetables in 39 countries (19). The ATBC was a clinical trial that related Vitamin A and E to increased lung cancer rates. (20) 2 large cohort studies have been performed in relation to colorectal cancer and dietary fibre. (21, 22). EPIC showed a significant benefit of dietary fibre against colorectal cancer. The EPIC data showed a 40% difference in colorectal cancer rates between the lowest and highest quintile dietary fibre groups. NIH-AARP however showed no benefit when adjusted for multivariate analysis. The American Gastroenterology Association suggest that available evidence form animal, epidemiological and interventional studies does not unequivocally support protective role of fibre against development of CRC. However the whole body of evidence is analysed overall the overall conclusion is that there is an inverse relationship between dietary fibre and CRC.
Cancer cachexia
Cancer cachexia is defined as anorexia, weight loss and muscle wasting, fatigue and weakness in a cancer patient. Cancer instigates an inflammatory response and production of tumour products. This triggers metabolic abnormalities that produce lipolysis, protein loss and anorexia. As with all disease processes the dietary management of cancer cachexia is initiated by a nutritional assessment. Any symptoms including vomiting and nausea should be treated. There has also been some research regarding fish oils and cancer cachexia. One available product contains docosahexaenoic acid, eicosapentaenoic acid and antioxidants. However a Cochrane review has shown no benefit in relation to beneficial effects of fish oils and cancer cachexia. (23)
Critical care
Injury and sepsis cause major disturbance to clinical state. There is rapid weight loss, increased metabolic rate, protein losses and sodium retention. There are also changes in hormone levels including increased insulin, catecholamines, growth hormone, glucagons and cortisol. The energy requirements in critical care can vary greatly. The Ireton-Jones equation is often used to calculate energy requirements in the critical care setting (See Table 4).
Table 4
Immunonutrition: ESPEN guidelines (34)
Surgical patients
Perioperatively for
Major Cancer Neck Surgery
Major Cancer Abdominal Surgery
Critical Care Patients
Elective Upper GIT surgery
Mild Sepsis
Trauma
ARDS (n-3 FA’s and antioxidants)
Glutamine (burns and trauma)
The specific immune modulating aspects of nutrients have been widely researched in the critical care setting. This field of immunonutrition has shown disparaging results.
Arginine has been investigated as an immune modulating nutrient. Arginine levels can increase or decrease in relation to clinical state. It produces nitric oxide that can lower blood pressure and has been revealed to have detrimental effects in critically ill patients. (24) Glutamine is another possible immune modulating nutrient. It has lots of metabolic functions. It enhances heat shock protein that protect against sepsis. It is thought to be useful in septic shock. Omega-3 fatty acids (alpha-linolenic acid, docosahexaenoic acid, eicosapentaenoic acid) have also been investigated as an immune modulating nutrient. Omega-3 fatty acids produce less proinflammatory eicosanoids than omega-6 fatty acids. There is some evidence that omega-3 fatty acids decrease duration of hospital stay (25) Antioxidants have also been researched as an immunomodulator. Antioxidant levels are lower in critically ill patients. Vitamins A,C,E and Selenium have been studied. A recent meta-analysis has suggested overall mortality benefit but no septic complications benefit in anti-oxidant trials. (26)
Gastrointestinal disease and nutrition
Liver disease
The energy requirements in chronic liver disease are dependent on clinical state i.e. compensated or decompensated. Nutritional requirements for compensated liver disease are 25-35 kcal per kg (dry body weight) day and protein 1.2g per day. Nutritional requirements for decompensated liver disease are energy 35-45 kcal per kg (dry body weight) day and protein 1.5grams per day.
Porto-systemic encephalopathy
This disease process is multifactorial and comprises increased ammonia levels, increased aromatic amino acids, decreased branched chain amino acids and alterations of brain neurotransmitters. There is a widely held belief among doctors that protein intake should be restricted but this is mistaken. Protein requirements are approximately 1g/kg/day and should be divided throughout day.
Ascites
Low salt intake (<6g per day) is an essential component of ascites treatment. Advice should include no salt in cooking, no added salt, avoid processed foods, and avoid foods rich in salt.
Inflammatory Bowel Disease
Inflammatory bowel disease patients are often undernourished due to meagre intake (anorexia, vomiting), amplified losses (diarrhoea and malabsorption) and increased demands (catabolic state). Protein requirements are also increased due to nitrogen losses and catabolic state. It is therefore important that nutritional measures are instituted to improve calorie and protein intake. Interestingly nutrition has been investigated as a treatment for active Crohn’s Disease. Elemental diet is used in active paediatric Crohn’s Disease more than adult Crohn’s Disease to achieve remission. (27). Often this has to be given via naso-gastric tube due to unpalatability. After 4-6 weeks if the patient is in remission foods are introduced slowly over a 3-week period.
Coeliac Disease
Coeliac disease is genetically determined chronic inflammatory disease secondary to gluten (glaidin is the alcohol-soluble fraction) that is a component of wheat. In addition the allergy involves similar proteins found in barley, rye and possibly oats. Coeliac patients consequently exclude these dietary sources. Oats can be reintroduced later depending on response. Dietary sources can be obvious or hidden as gluten can be found in numerous manufactured foods. Coeliac patients can however eat natural gluten-free foods or gluten-free proprietary foods (e.g. Schar, Juvela, Dietary Specials, Glutafin).
Irritable Bowel Syndrome
Simple healthy eating advice is suggested. Diet is tailored to either constipation or diarrhoea symptoms. Typically increasing dietary fibre gradually ameliorates constipation symptoms. Soluble fibre appears to offer benefit more than non-soluble fibre. Decreasing dietary fibre intake treats diarrhoea symptoms. There is not enough evidence regarding exclusion diets although some centres do offer exclusion diets.
Renal disease
Acute renal failure and nutrition is divided into non-catabolic and catabolic patients. Non-catabolic patients do not usually have increased energy requirements. Catabolic patients have high protein requirements but no benefit of >0.2 g nitrogen per kg per day. Their energy requirements should be no greater than >20% above resting energy expenditure.
Chronic kidney disease patients have estimated energy requirements of 35 kcal/kg/IBW/day. (IBW = Ideal Body Weight which in the UK this approximates to BMI 23kg/m2). There has been much research regarding protein restriction and possibility of slowing progression of chronic kidney disease. The Northern Italian Co-op study (protein <0.6grams/day) did show possible slower progression of CKD. However it is known that low protein diets have poor compliance and can increase risk of malnutrition. The Renal Association Standards suggest protein intake 0.75g/kg/IBW/day.
Discussing the dietary management of end-stage renal disease, nephrotic syndrome and renal stones is beyond the scope of this article.
Conclusion
This review article has highlighted the importance of undernutrition in patients under our care. There are numerous methods of screening and assessing patients for undernutrition. There is also a stepwise approach to improving calorie intake: improving oral intake by various methods to enteral and parenteral nutrition. Nutrition is an important aspect of treatment of different disease processes that include cardiovascular disease, diabetes, gastrointestinal disease, renal disease, critical care and cancer. This review article will hopefully provide the medical practitioner with improved knowledge that can be translated into improved awareness and treatment of undernutrition.
Leo Kanner, a Boston physician, first used the word ‘Autism’ in 1943 when he reported on a group of children with deficits in social communication1. Independently, in 1944, Hans Asperger, an Austrian physician, identified similar difficulties in a group of young boys2. Today the term Autism is used to describe a behaviourally defined disorder that is characterised by impairments in social communication, social interaction, and problems with repetitive behaviours and narrow interests.
To receive a diagnosis of autism, a child must have shown delayed language development alongside the characteristic behavioural deficits described in Table One below. Asperger’s Syndrome is used to describe children who had no such delay in acquiring spoken language, and who also have IQ’s above 70. Given that early language development is the key in differentiating between these two disorders, it is not possible for a child to change their diagnosis from Autism to Asperger’s regardless of their later language development and progress.
Debate exists as to whether the two conditions are distinct and it is now generally accepted that they are both part of a spectrum of disorders, hence the term Autistic Spectrum Disorders (ASD). In both the Diagnostic Statistical Manual (DSM IV)3 and International Classification of Diseases (ICD 10)4 Autism and Asperger’s Syndrome come under the category of Pervasive Developmental Disorders. Table One shows the main characteristics of the Pervasive Developmental Disorder.
Table One: Key characteristics of the Pervasive Developmental Disorders
Autism
Deficits in sociability and empathy
Deficits in communicative language
Deficit in cognitive flexibility
Delay with speech development
Detectable before the age of 3
Asperger’s Syndrome
Poor social skills, lack of insight
Behavioural inflexibility, narrow range of interests
IQ over 70
No delay with speech
Motor clumsiness
PDD not otherwise specified
Applies to less severely affected children who do not meet the criteria for either Autism or Asperger’s Syndrome
CLINICAL PRESENTATION
The main characteristics of ASD’s are:
Qualitative impairment in social interaction
Qualitative impairment in communication
Restrictive, repetitive and stereotyped patterns of behaviour, interests and activities
These are known as the ‘triad of impairment’5 and deficits in all three areas must be present for a diagnosis of autism. Each part of the triad will be described, but it is important to remember that not all children with autism will present with all of the difficulties suggested below. Qualitative impairment in social interaction: This includes poor eye contact, poor use of gestures and facial expressions, not sharing, lack of interest in forming social relationships with peers, not joining in with group activities and an inability to recognise the effect of their behaviour on others.
Qualitative impairment in communication: This includes delay in speech, misinterpreting others use of speech such as idioms, sarcasm, jokes and taking things literally. Poor use of speech and also poor understanding of non-verbal gestures such as others’ facial expressions. Limited non-verbal gestures such as pointing.
Restrictive, repetitive and stereotyped patterns of behaviour, interests and activities: Overwhelming interest in a specific topic to such an extent that the child talks about the topic excessively, becomes anxious if unable to perform a ritual or dislikes any interruption to routine and every day life. The child may also have unusual interests such as a fascination with traffic lights, telegraph poles or number plates.
About 70% of children with classic autism have IQ below 708 and approximately one third will have epileptic seizures which continue into adulthood9. PREVALENCE
Recent studies have found a prevalence rate of 20-40 per 10,0006. However if the broader phenotype is used, the prevalence may be as high as 100 per 10,000, or 1% 7. The ratio of males to females is four to one for autism and ten to one for Asperger’s Syndrome. In the last few years, epidemiological studies have suggested that the prevalence of ASD have been increasing. Possible explanations include the fact that the diagnostic criteria has broadened, as well as generally improved case recognition.
ASSOCIATED CONDITIONS
Often in children with autism there are signs and symptoms which are not readily explained by a diagnosis of autism alone. Other medical and psychiatric conditions may co-exist with autism including;
Learning difficulties
Epilepsy
Speech and Language problems
Attention Deficit / Hyperactivity Disorder (ADHD)
Developmental Co-ordination Disorder (DCD)
Tourette’s Syndrome and Tics
Feeding and Eating problems
This is not an exhaustive list8, but we will briefly consider some of the most common conditions and difficulties that a child with autism may also be diagnosed with.
Learning Difficulties: As noted above, approximately 70% of children with classic autism also have an IQ below 70 and are therefore recognised to have mild, moderate or severe learning difficulties9.
Epilepsy: As with learning difficulties, epilepsy is more common among children diagnosed with classic autism, with around 30% being affected into adulthood10. Epilepsy is less common among children with Asperger’s Syndrome, but may be more prevalent than in typically developing children11.
Speech and Language Problems: Most children with an ASD have slower language development than their peers. It is not only expressive language that may show problems, receptive language may also appear delayed in young children, and children may appear to be less responsive to their own name. Some children with autism also appear to lose words that they had previously learnt. This regression is described in approximately 25% of children with classic autism, and is usually a gradual process where a child fails to learn new words, and may stop using previously learnt words altogether12.
ADHD: ADHD is the most common psychiatric disorder to occur alongside an ASD and there are clinical benefits from receiving a dual diagnosis13. Children are likely to benefit from receiving treatment aimed specifically at their ADHD symptoms, as well as having both impairments recognized by parents and teachers.
DCD: Developmental Co-ordination Disorder (or Dyspraxia) describes the motor co-ordination problems and clumsiness typical in AS. Such difficulties may benefit from intervention from an Occupational Therapist or Physiotherapist.
Tics and Tourette’s syndrome: Several reports have documented the co-occurrence of tics in Asperger’s Syndrome. Tourette’s syndrome has also been observed in children with autism. Tics may be verbal or motor. Feeding and Eating Problems: Problems with food including food refusal, selective eating, hoarding, pica and overeating have all been observed among children with an ASD14. Some children have difficulties coping with mixed textures, may eat their food in a certain order and may even ask for their food on different plates.
ASSESSMENT
A general assessment should cover the following areas:
The child’s developmental history.
Observations of the child in structured and semi-structured situations15.
Nursery/School report.
Assessment of cognitive level.
Assessment of problem behaviours.
Speech and language assessment.
Audiology and visual tests if indicated. Chromosomal screen is needed if there are dysmorphic (abnormal) features.
Physical investigations may be specifically indicated in some cases including the need for an EEG, or screening for Fragile X and other chromosomal abnormalities. It is still debatable as to whether these investigations are worth performing routinely as the yield of positive results is relatively low.
Diagnostic Interviews: A number of interviews exist that help clarify the diagnosis and are also used in research. These include the Autism Diagnostic Interview16, the Diagnostic Interview for Social and Communication Disorders17, the Childhood Autism Rating Scale18 and a new computerised interview, the Developmental, Dimensional and Diagnostic Interview (3Di)19. DIFFERENTIAL DIAGNOSES
Information from the above assessments can be used to determine the degree to which a child meets the criteria for an ASD and can also be used to exclude alternative diagnoses. The following conditions should be considered in the differential diagnosis of autism20
- Learning Difficulties
- Hearing Problems
- Speech and Language Disorders
- Rett’s Syndrome
- Childhood Disintegrative Disorder (Heller’s Syndrome)
- Landau-Kleffner Syndrome
- Reactive Attachment Disorder
Learning Difficulties: Children with learning difficulties without an autistic spectrum disorder do not show deficits in their reciprocal social behaviour and their language development is typically in line with their overall intellectual abilities. Hearing Problems: Fluctuating hearing loss, such as glue ear may cause children to show problems in their reciprocal communication, for example, not hearing their name being called. Some may rely on lip-reading during these times of hearing loss, and may appear to make less eye contact. However, these children are capable of making eye contact and may also use sign-based means of social interaction. Speech and Language Disorders: Children with developmental language disorders are unlikely to show the non-verbal communication difficulties typical of children with autism. These children are also less likely to have restricted interests and repetitive behaviours. Rett’s Syndrome: Rett’s Syndrome is a disorder found only in girls. Its typical onset occurs between 5 and 30 months, and is accompanied by a deceleration of head growth. It is characterised by abnormalities in language and social development, as well as a decrease in purposeful hand movements and an increase in stereotyped ‘hand-washing’ movements. Severe or profound intellectual difficulties are also common and epilepsy occurs in the majority of children. Childhood Disintegrative Disorder (Heller’s Syndrome): CDD is characterised by a marked loss of skills following a period of normal development for at least two years. There may also be an increased chance of epilepsy. There is no known consistent cause of CDD. Landau-Kleffner Syndrome: Similarly to CDD, a child with Landau-Kleffner Syndrome would show typical language and cognitive development with a loss of expressive and receptive language skills and seizures consistent with a diagnosis of epilepsy. Landau-Kleffner typically occurs between three and seven years of age and two-thirds of children result in having irreversible receptive and expressive language disorder. Reactive Attachment Disorder: RAD as a result of severe psychosocial deprivation may appear similar to autism in a number of ways. For example, children may have delayed language skills, and may show unusual social interaction and stereotyped behaviours. Early diagnosis may be difficult but once placed in an appropriate social environment, children with RAD tend to gradually develop more typical social behaviours.
AETIOLOGY AND MMR Biological Theories: Genetics play a big role with monozygotic twins of an affected individual having autistic features in 69% of cases compared with zero percent concordance rate for dizygotic twins21. The genetic model is likely to be polygenic in nature with at least 3 to 5 genes responsible. No specific gene has been identified but studies have indicated susceptibility located on chromosomes 2,7, 16 and 17 22.
Imaging techniques have implicated brain regions that play a part in the development of autism including those regions that are responsible for emotional and social functions, regions involving face recognition and social-cognitive systems involved in understanding the intentions of others. A recent fMRI study by DiMartino et al 23 has shown hypoperfusion in the pregenual anterior cingulate cortex in adults with autism. This region is linked to an individual’s capacity to reason about the thoughts and beliefs of others, known as the theory of mind.
The neurotransmitter Serotonin (5-HT) is thought to be involved in autism24. 5-HT is thought to be involved in neurodevelopment and in particular it is abundant in brain limbic areas critical for emotional expression and social behaviour.
MMR: Some parents and families of children with autism believe that the Measles/Mumps/ Rubella (MMR) vaccine caused their children’s autism. These parents’ beliefs and observations were reinforced by a small study of bowel disease and autism, published by Wakefield and his colleagues in 1998 25. The authors suggested that there was a link between the MMR vaccine and autism. However this study was seriously flawed since there was ascertainment bias, unreliable reporting of early symptoms and a lack of a clear pathogenic model.
To date there is no definite, scientific proof that any vaccine or combination of vaccines can cause autism 26. The British Association of Paediatricians recommends that children receive two doses of the MMR vaccine, as long as they have no known health problems that prevent the vaccine from being effective. The immunization schedules recommend that the first dose be given at age 12-to-15 months, while the second dose should be given at either four-to-six years of age or 11-to-12 years of age.
Psychological Theories: Psychological theories have failed to identify one primary deficit that could account for all the features associated with the autistic phenotype.
An interesting theory is the ‘Theory of Mind’ abnormality27. Autistic children lack a ‘theory of mind’and thus are unable to understand that another person can have thoughts, feelings and intentions. MANAGEMENT AND INTERVENTIONS
There is no cure for autism and there is no one specific treatment that is more effective than others (For a review of psychological and educational interventions see Howlin, 199828 and Francis, 200529). However, interventions can be focussed on helping children with autism develop their skills to compensate for their communicative, cognitive and behavioural differences. Interventions need also to be targeted at parents and families to empower them to cope with their children in the most effective way.
Psychoeducation: Receiving a diagnosis of autism is a stressful event for families. The first logical step in providing intervention must be to give parents the opportunity to understand the disorder. Autism is a chronic, life-long neurodevelopmental condition and parents must learn to cope with and manage their child’s behaviours, which may sometimes be distressing and confusing. Children with autism have a lack of empathy, and may not show as much warmth towards their parents as other children. They are also likely to prefer routines, and become frustrated and aggressive if their preferred routine or activity is interfered with. Some children with autism also self-harm. Parental support groups, both national and local, can also offer a much needed source of support and reassurance.
Educational Placement: Improving the child’s educational situation remains one of the most important interventions. While the policy about educational inclusion is somewhat controversial, there is currently no data available about which approach is the most effective, and so choices must be based on pragmatic considerations for the individual. It is sometimes difficult to arrange sufficient support within a mainstream environment, even with a Statement of Special Educational Needs, and so specialist placements may need to be sought. Regardless of the educational placement, structured teaching will help make the school world more comprehensible to a child with autism. The TEACHH programme30, 31 acknowledges the deficits associated with autism and works on structuring learning activities to capitalise on the child’s strengths. For example, children with autism often have good visual processing skills, and so tasks can be structured so that the child can visualise what is expected of them. Special interests can also be used to capture and maintain interest.
Behavioural Treatment: Behavioural analysis of the child’s skills is used to set specific treatment goals and to identify behavioural methods for achieving those goals. Parents as well as other professionals, including teachers and specialist tutors are trained in the implementation of programmes such as ABA (Applied Behavioural Analysis) and Lovaas32. Materials should be matched to the child’s developmental level, and large tasks should be broken down into more manageable tasks to make success more likely. Modelling and reinforcement are key tools in training, helping to increase and maintain desired behaviours.
Some local services and support groups run social skills groups, which can be helpful. If there is a specific behavioural problem then it is helpful talking to a psychologist who can help the parent look more closely at possible precipitants and contributing factors.
Diet: It has been suggested that foods containing gluten and casein may play a role in the difficulties associated with autism33. However, research in this area is scarce so far, and in a recent systematic review34, only one study is considered to be adequate for inclusion35. Based on urine samples, it was suggested that a diet excluding gluten and casein may result in a decrease in autistic traits such as echolalia and rigidity. While this small-scale study and anecdotal evidence may support a diet excluding gluten and casein, such diets are not without their added financial cost and inconvenience, as well as limiting food choices for the affected individual. Further good quality studies are awaited in this area.
Medication: There have been encouraging trials on the use of Risperidone for reducing aggressive and self-injurious behaviour36.
PROGNOSIS
Outcome generally depends on IQ and language development. There may be improvement in language after the pre-school years. However, most individuals continue to show impairments in social skills and communication. Asperger’s Syndrome is associated with a better prognosis due to a relatively greater IQ.
Behaviours and symptoms may vary over time and it is a myth that symptoms remain fixed. Many individuals will require support such help with living independently and obtaining employment. Teenagers may be particularly vulnerable to developing depression and occasionally self-injurious behaviour, particularly if bullying and teasing become a problem.
The genus pseudomonas are Gram-negative, aerobic, rod-shaped bacterium with unipolar motility,[1]contains more than 140 species, most of which are saprophytic. More than 25 species of pseudomonas are associated with humans [2]. Most pseudomonads known to cause disease in humans are associated with opportunistic infections. These include Ps. aeruginosa,Ps. fluorescens, Ps. putida, Ps. cepacia, Ps. stutzeri, Ps. maltophilia, and Ps. putrefaciens. Only two species, Ps. mallei and Ps. pseudomallei, produce specific human diseases: glanders and melioidosis. Ps. aeruginosa and Ps. maltophilia account for approximately 80 percent of pseudomonads recovered from clinical specimens [1,4].
Because of the frequency with which it is involved in human disease, Pseudomonas. aeruginosa has received the most attention. It is a ubiquitous free-living bacterium and is found in most moist environments. Although it seldom causes disease in healthy individuals, it is a major threat to hospitalised and immunocompromised patients, particularly those with serious underlying diseases such as cancer and burns [5]. The high mortality associated with these infections is due to a combination of weakened host defenses, bacterial resistance to antibiotics, and the production of extracellular bacterial enzymes and toxins [6].
Pseudomonas aeruginosa is a leading gram negative pathogen that causes nosocomial infections, accounting for 20% of pneumonia and 16% of urinary tract infections according to recent data from national nosocomial infection surveillance system [7]. According to the CDC, the overall incidence of Pseudomonas aeruginosa infections in U.S. hospitals averages about 0.4 percent (4 per 1000 discharges), and the bacterium is the fourth most commonly isolated nosocomial pathogen accounting for 10.1 percent of all hospital-acquired infections[9].
Resistance of this notorious bacterium to commonly used antimicrobial agents is becoming an increasing clinical problem and a recognised public health threat because there are limited number of antimicrobial agents including the antipseudomonal penicillins, cephalosporins, carbapenems, aminoglycosides and fluoroquinolones with reliable activity against it [11]. It has intrinsic resistance to many antimicrobial agents and only a few antimicrobial agents show potent antibacterial activity against this bacterium. The emergence of multidrug resistance (MDR) Pseudomonas aeruginosa has became a serious problem [12]. There are several mechanisms which may contribute to the antimicrobial resistance among Pseudomonas aeruginosa including the production of chromosomally encoded Amy C B-lactamases [13]. Hypermutable strains of Pseudomonas aeruginosa with defects in themethyl directed mismatch repair (MMR) system are also being frequently isolated from the lungs of cystic fibrosis (CF) patients [13].
MATERIALS AND METHODS:
Samples collection: For this study, a total of 1008 clinical isolates of Pseudomonas aeruginosa, were isolated from 2800 different clinical specimens including; urine (n= 905), ear swabs (n= 496), eye swabs (n=26), fluids (n= 31), pus swabs (n= 342), HVS (n= 157), and sputum (n= 843) received at the microbiology section of Burgor Anklesaria Hospital’s pathological laboratory between January 2008 and September 2008.
Primary isolation of test strains: For the primary isolation of test culture specimens were inoculated on routine culture media including CLED agar (Merck, Germany), EMB agar (Merck, Germany), MacConkey’s agar (Oxoid, UK), and Chocolate agar (Merck, Germany). Pigment production was interpreted on the basis of growth on Nutrient agar (Merck, Germany).
Control stain: ATCC Control strain of Pseudomonas aeruginosa(27853).
Spot tests: Selected colonies were further confirmed by spot tests including; Gram’s stain (Merck, Germany), Oxidase test (Oxoid, UK), Citrate utilisation test (Merck, Germany), and Urease tests (Merck, Germany) [1,4].
Sugar fermentation & IMVIC: Selected colonies were also subjected to Oxidative fermentation and IMVIC i.e. Indole, Methyl reductase test, Vogus prosekure test for confirmation of specie [1,4].
Antibacterial susceptibility testing: Antibacterial susceptibility testing of selected Pseudomonas aeruginosa species was done on Mueller Hinton agar (MHA) (Merck, Germany). To make bacterial suspensions, four to five colonies of pure growth from overnight cultures of test strains were transferred into a tube containing four to five millilitres of nutrient broth (Merck, Germany), and incubated at 37 °C to match the turbidity with McFarland’s index of 0.5 (usually 2-6 hours). Lawns of each bacterial suspension were made on MHA using sterile cotton swabs. Commercially available standard antibiotic discs of standardised concentrations (Oxoid, UK) (Amikacin, Ceftriaxone, Cefotaxime, Sulzone (Cefapeozone+Sulbactum), Meropenam, Ciprofloxacin, and Fosfomycin) were positioned at appropriate distances on the bacterial lawns and incubated at 37 °C for 24 hours. The growth inhibition zones were carefully measured with calipers and recorded according to the standard Kirby-Bauer disc diffusion method[2] and CLSI/NCCLS guidelines 2003 & 2007[8,9,13].
RESULTS:
This study was conducted on 2800 multiple type of clinical specimens received at Burgor Anklesaria Hospital’s pathological laboratory during January 2008 to September 2008. Out of these a total of 1008 clinical isolates were identified as Pseudomonas aeruginosa on the basis of gram’s stain and spot test reactions. Morphologically all of these isolates were gram negative, non sporing, capsulated, and motile short rods, produced typical grapes like odor of amino acetophenone and blue water soluble non fluorescent pigment pyocyanin.They were also positive for oxidase and citratase with variable ability to utilize urea agar. Of these1008 Ps. aeruginosa, 532 isolates were from male patients (504 adults and 28 children), and 476 isolates were from female patients (442 adults and 34 children) (Table 1).
Antibacterial susceptibility of seven selected antibiotics was determined against 1008 test strains of
Pseudomonas aeruginosa, using Kirby and Bauer disc diffusion method[2], against commercially available standardised antibiotic filter discs (Oxoid, UK). These strains were isolated from seven different categories of specimens including ear swabs, wound pus, urine, sputum, eye swab, fluids and high vaginal swab (HVS) (Table 2 & 3).
Another interesting observation was that a maximum number of test strains were isolated from urine i.e. 403 (40%). While, only 6 (0.6%) were isolated from eye swabs (Table 2). When susceptibility results were compared according to the age and sex, not a significant difference was observed (Table 3).
Out of a total of 504 isolates from male adults, 45 (9%) were resistant to Amikacin, 140 (28%) were resistant Ciprofloxacin, 185 (37%) were resistant to Cefotaxime, 174 (34%) were resistant to Ceftriaxone, 34 (7%) were resistant to Sulzone, 140 (28%) were resistant to Fosfornycin and 25 (6%) were resistant to Meropenam. Among 28 male children, the maximum resistance was observed to Ciprofloxacin (Table 3) out of 442 isolates from female adults 39 (9%) were resistant to Amikacin 84 (19%) were resistant to Ciprofloxacin, 78 (18%) were resistant to Cefotaxime, 151 (34%) were resistant to Ceftriaxone, 28 (6%) were resistant S ulzone (Cefapeozone+Sulbactum), 145 (33%) were resistant to Fosformycin and 11 (2%) were resistant to Meropenam. On the whole, the maximum resistance was observed from the male adults isolates against Cefotaxime (n=185, 37%) and in the case of isolates from the female adults to Ceftriaxone (n=151, 34%) .
Collectively, we can say that maximum resistance was observed when target cells were subjected to antimicrobial susceptibility testing against third generation Cephalosporins i.e. Ceftriaxone and Cefotaxime. The most effective antibiotic in the isolates from the male patients was Sulzone (Cefapeozone+Sulbactum) i.e. 465 (92%), while in the case of isolates from female patients it was Meropenam i.e. 414 (94%) (Table 3).
Table 1: Age and Gender wise distribution of clinical isolates of Pseudomonas aeruginosa
Total No. of samples N
2800 n (%)
Positive for Ps. aeruginosa
1008 (36%)
Male adult(>12 years)
504 (50%)
Male children (0-12 years)
28 (3 %)
Female adult (>12 years)
442 (44%)
Female children (0-12 years)
34 (3%)
Table 2: Resistance of Pseudomonas aeruginosa from different clinical specimens toantibiotics determined by Kirby-Bauer disc diffusion method
%=Percentage,n= Individual type of sample,N=Total number of sample,AK= Amikacin (R =>22 mm),CRO= Ceftriaxone (R=>21 mm),CTX=Cefotaxime (R=>22 mm),SCF= Sulzone (R= > 20 mm) (Cefapeozone+Sulbactum), MEM=Meropenam (R= >18 mm), CIP=Ciprofloxacin (R= > 21mm),FOS=Fosfomycin (R= > 18mm ),µgms= micro grams, S= sensitive
Table 3: Age and Gender wise sensitivity of Pseudomonas aeruginosa from different clinical specimens to antibiotics determined by Kirby-Bauer disc diffusion method
% =Percentage,n= Individual type of sample,N=Total number of sample,AK= Amikacin (R =>22 mm),CRO= Ceftriaxone (R=>21 mm),CTX=Cefotaxime (R=>22 mm),SCF= Sulzone (R= > 20 mm) (Cefapeozone+Sulbactum), MEM=Meropenam (R= >18 mm), CIP=Ciprofloxacin (R= > 21mm),FOS=Fosfomycin (R= > 18mm ),µgms= micro grams, S= sensitive
DISCUSSION:
Pseudomonasaeruginosa is a leading Gram-negative pathogen thatcauses nosocomial infections, accounting for 20% of pneumoniaand 16% of urinary tract infections according to recent datafrom the National Nosocomial Infections Surveillance System [1].
Optimisation of therapy against Pseudomonas aeruginosa starts with the initial empirical antibiotic choice. Surveillance data and hospital or unit antibiograms may inform this decision, although individualisation of the initial regimen on the basis of prior antibiotic use and prior isolation of resistant pathogens may be more important. Combinations of antibiotics are often required empirically, and "combination antibiograms" may need to be developed for this purpose. Preliminary data suggest that extending the time over which a dose of antipseudomonal beta-lactam antibiotics is infused may improve clinical outcomes; however, this idea remains to be confirmed in randomised trials. For example Moody et al in 1972 showed that some of the Pseudomonas speciesother than Pseudomonas. aeruginosa were resistant to a number of antibiotics.Among these were antibiotics that are in general use for P.aeruginosa infections. Such differences in antibiotic susceptibilities emphasise the necessity for careful speciation of this groupof microorganisms to assure proper epidemiological documentationof colonisation and infection, as well as to ensure therapywith an antimicrobial agent to which the organism is susceptiblein vitro. The role of direct susceptibility testing in aiding more rapid initiation of appropriate antibiotic therapy is also being studied. When identification and susceptibility testing is complete, the antibiotic regimen for infections due to Gram-negative pathogens can be "fine tuned." On some occasions, this fine tuning necessitates the introduction of "salvage" antibiotics, such as Colistin or Tigecycline; on others, it necessitates de-escalation and early termination of therapy. The lack of new antibiotic options against gram-negative pathogens underscores the need for optimisation of current therapies and prevention of the spread of these organisms.
In 2008 Javiya etal reported the highest number of Pseudomonas infections was found in urine, followed by pus and sputum. Pseudomonas species demonstrated marked resistance against monotherapy of penicillins, cephalosporins, fluoroquinolones, tetracyclines and macrolides. Only combination drugs like Ticarcillin + Clavulanic acid, Piperacillin + Tazobactum, Cefoperazone + Sulbactum, Cefotaxime + Sulbactum, Ceftriaxome + Sulbactum and monotherapy of Amikacin showed higher sensitivity to Pseudomonas infections; however, the maximum sensitivity was shown by the Carbapenems.
Our study was therefore carried out, using Kirby-Bauer method [2], to determine the antibiotic susceptibility patterns of Pseudomonas aeruginosa isolates from in-patients and out-patients attending the microbiology section of Burgor Anklesaria Hospital’s pathological laboratory between January 2008 and September 2008. The isolation rate of Pseudomonas aeruginosa in clinical specimens was found to be 36%, with the highest occurrence of 403 (40%) in urine samples followed by 258 (26%) occurrence in ear swabs. The susceptibility pattern showed that 85% were sensitive to Meropenam and 84% to Sulzone (Cefapeozone+Sulbactum). The isolates from the male patients showed almost equal resistance to all the antibiotics tested, as in case of isolates from the female patients, most especially Ceftriaxone and Cefotaxime. However, no consistent antibiotic susceptibility pattern could be established for this pathogenic bacterium based on sources.
Treatment of Pseudomonas aeruginosa is a challenge because resistance limits dramatically therapeutic options. In this review, we discuss data of in vitro susceptibility for the management of infections caused by Pseudomonas aeruginosa. Currently, published data from Pakistan are limited, and there are no such randomised clinical trials involving the treatment of infections caused by multidrug resistant Gram-negative rods. At present newer antimicrobial agents active against multidrug resistant bacteria like Pseudomonas aeruginosa are not available or under investigation.
CONCLUSION:
Antibiotic resistant organisms appear to be biologicallyfit and are capable of causing serious, life-threatening infectionsthat are difficult to manage because treatment options are limited.This increase in the prevalence of drug resistant pathogensis occurring at a time when the discovery and development ofnew anti-infective agents is slowing down dramatically.
The Pseudomonas aeruginosa species isolated from patients in the Microbiology section of Burgor Anklesaria Hospital’s pathological laboratory, Karachi, Pakistan were tested in vitro for antibacterial susceptibility of currently available and commonly prescribed drugs. Meropenam and Sulzone were the two antibiotics found to be the most susceptible against this pathogen. The emergence of multidrug resistant (MDR) Pseudomonas aeruginosa is a challenging clinical problem. This study investigated the pattern of antibiotic resistance to test antibiotics and helps us in determining the role of combination therapy in its management. The results of this study suggest that use of triple antimicrobial therapy (Meropenam, Sulzone and Amikacin) can be a useful alternative treatment for multidrug resistant (MDR) Pseudomonas aeruginosa infection in certain circumstances.
Kenneth Brummel-Smith, MD is the Charlotte Edwards Maguire Professor of Geriatrics and the chair of the Department of Geriatrics at the FSU College of Medicine. He is editor of five textbooks, Geriatric Rehabilitation, Practical Ambulatory Geriatrics, Interviewing and Patient Care, Geriatric Assessment, and Reichel’s Care of the Elderly. His research has addressed the effect of a support group on caregivers of patients with Alzheimer’s disease, methods of assessing pain in persons with Alzheimer’s disease, and advance care planning. He serves on the National Advisory Council on Aging for the National Institute on Aging.
How long have you been working in your speciality?
I started in geriatrics in 1983. I completed a residency in family medicine, then a fellowship in faculty development. While teaching in a family medicine residency 3 years after that, I was sent to a Society of Teachers in Family Medicine conference on integrating geriatrics into family practice teaching. I feel in love with the concept of the “functional approach” and dedicated myself to learning more geriatrics. After taking a 1-year certificate course in geriatrics at UCLA I was offered the position of Co-Chief of the Clinical Gerontology service at Rancho Los Amigos Hospital, the largest rehabilitation hospital in the US. And that was the start of it all!
Which aspect of your work do you find most satisfying?
Although my work now is primarily academic, I still get the most satisfaction is working closely with a elder in guiding them through difficult medical decision-making situations. I never cease to be amazed how well people can think through difficult medical decisions, if they are fully engaged in the process and educated about their options. We rarely give patients enough credit to do this.
What achievements are you most proud of in your medical career?
Being selected by the American Geriatrics Society for the Dennis W Jahnigen Memorial Award for outstanding contributions to geriatric education in 2006, and by the students of the Florida State University College of Medicine (FSUCOM) for the Hippocratic Award in 2008 for best representing professionalism, compassionate care, and inspirational teaching.
Which part of your job do you enjoy the least?
Dealing with personnel issues in my department
What are your views about the current status of medical training in your country and what do you think needs to change?
I think we need to make some fundamental changes. The future of medicine is in managing chronic conditions in a team environment. Much of the ways we teach medicine today is just like we did 30 years ago when I was in school. First, I would rethink the role of basic science teaching. Not every student needs the same thing. I see the best value of basic science is to teach critical thinking, but most of it today focuses on memorizing and regurgitating minute details. Second, I would provide most clinical teaching in teams of providers – especially medicine, social work, nursing and pharmacy. Third, I would equip students with real skills for helping patients to manage chronic conditions – patient-centered compassionate care, using motivational interviewing. Finally, I would adopt what most other advanced countries do – require a service commitment after graduation in rural and underserved areas, in exchange for more subsidies of educational costs.
How would you encourage more medical students into entering your speciality?
Start with positive role models – we use a senior mentor program where each student is assigned a mentor in the community in the 1st year of med school. The senior mentors are relatively healthy, very active and engaged in their communities and a real hoot to be around! We train every student in geriatric issues as a normal part of clinical care, not something special or different. And we have required integration of geriatrics into all other classes and a required 4th year rotation. Perhaps that’s why we have the highest rating by our graduates of their geriatric skills in the country.
What qualities do you think a good trainee should possess?
Compassion for others, an inquisitive mind, the recognition that authority is often wrong, and a commitment to evidence.
What is the most important advice you could offer to a new trainee?
Relax and remember you (and all of us) are not that important in the large scheme of things
What qualities do you think a good trainer should possess?
Relax and remember you (and all of us) are not that important in the large scheme of things
Do you think doctors are over-regulated compared with other professions?
No – we under-regulated. Nobody should let us do all the things we get away with. What other business can kill tens of thousands clients a year and get away with it? If you doubt this, you have not read the Institute of Medicine’s report “To Err is Human.” But you should!
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what should be done to counter this trend?
Yes. Calling patients “consumers.” Allowing doctors to advertise – especially plastic surgeons. And the growing influence of money on medicine – unnecessary surgeries and diagnostic tests, and unthinking acceptance of pharmaceutical companies information.
Which scientific paper/publication has influenced you the most?
Donald Berwick, “What patient-centered should mean: Confessions of an extremist,” Health Affairs 28, no. 4 (2009): w555–w565 (published online 19 May 2009; 10.1377/hlthaff.28.4.w555)
What single area of medical research in your speciality should be given priority?
Non-pharmaceutical management of behavioral disturbance in dementia
What is the most challenging area in your speciality that needs further development?
Developing a reasonable reimbursement system that recognizes the role of cognitive work and support of families in the patient’s care
Which changes would substantially improve the quality of healthcare in your country?
A single-payer national health insurance program, dissolution of the fee-for-service model of reimbursement, cost-effectiveness research, regulation of pharmaceutical costs
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Absolutely – if they put the patient first in all considerations.
How has the political environment affected your work?
Mostly through frustration. Washington seems to be in the lobbyist’s pocket and while I had great hopes of health care reform, I think we will be worse off if the present plans go through.
Chronic infections appear to be common features of various diseases, including neurodegenerative, psychiatric and neurobehavioral diseases, autoimmune diseases, fatiguing illnesses and other conditions.1-4 Neurodegenerative diseases, chronic degenerative diseases of the central nervous system (CNS) that cause dementia, are mainly diseases of the elderly. In contrast, neurobehavioral diseases are found mainly in younger patients and include autism spectrum disorders (ASD), such as autism, attention deficit disorder, Asperger’s syndrome and other disorders.5 For the most part, the causes of these neurological diseases remain largely unknown.2 Neurodegenerative diseases are characterized by molecular and genetic changes in nerve cells that result in nerve cell degeneration and ultimately nerve cell dysfunction and death, resulting in neurological signs and symptoms and dementia.2,3 On the other hand, neurobehavioral diseases are related to fetal brain development but are less well characterized at the cellular level and involve both genetic and environmental factors.6, 7 Even less well characterized at the cellular and genetic level are the psychiatric disorders, such as schizophrenia, paranoia, bipolar disorders, depression and obsessive-compulsive disorders.
Genetic linkages have been found in neurodegenerative and neurobehavioral diseases, but the genetic changes that occur and the changes in gene expression that have been found are complex and usually not directly related to simple genetic alterations.2, 6-8 In addition, it is thought that nutritional deficiencies, environmental toxins, heavy metals, chronic bacterial and viral infections, autoimmune immunological responses, vascular diseases, head trauma and accumulation of fluid in the brain, changes in neurotransmitter concentrations, among others, are involved in the pathogenesis of various neurodegenerative and neurobehavioral diseases.2, 3, 5-16 One of the biochemical changes found in essentially all neurological, neurodegenerative and neurobehavioral diseases is the over-expression of oxidative free radical compounds (oxidative stress) that cause lipid, protein and genetic structural changes.9-11 Such oxidative stress can be caused by a variety of environmental toxic insults, and when combined with genetic factors could result in pathogenic changes.14
Neurodegenerative diseases
Infectious agents are important factors in neurodegenerative and neurobehavioral diseases and may enter the brain within infected migratory macrophages. They may also gain access by transcytosis across the blood-brain-barrier or enter by intraneuronal transfer from peripheral nerves.15 Cell wall-deficient bacteria, such as species of Mycoplasma, Chlamydia (Chlamydophila), Borrelia and Brucella, among others, and various viruses are candidate brain infectious agents that may play important roles in neurodegenerative and neurobehavioral diseases.16-19 Such infections are systemic and can affect the immune system and essentially any organ system, resulting in a variety of systemic signs and symptoms.4, 15, 16, 19, 20
Amyotrophic lateral sclerosis
Amyotrophic lateral sclerosis (ALS) is an adult-onset, idiopathic, progressive neurodegenerative disease that affects both central and peripheral motor neurons.21 Patients show gradual progressive weakness and paralysis of muscles due to destruction of upper motor neurons in the motor cortex and lower motor neurons in the brain stem and spinal cord. This ultimately results in death, usually by respiratory failure.21, 22 The overall clinical picture of ALS can vary, depending on the location and progression of pathological changes.23
The role of chronic infections has attracted attention with the finding of enterovirus sequences in a majority of ALS spinal cord samples by polymerase chain reaction (PCR).24 However, others have failed to detect enterovirus sequences in spinal cord samples from patients with or without ALS.25-26 In spite of the mixed findings on enterovirus, infectious agents that penetrate the CNS could play a role in the aetiology of ALS. Evidence for transmission of an infectious agent or transfer of an ALS-like disease from man-to-man or man-to-animals has not been found.27
Using PCR methods systemic mycoplasmal infections have been found in a high percentage of ALS patients.28, 29 We found that 100% of Gulf War veterans from three nations diagnosed with ALS had systemic mycoplasmal infections.28 All but one patient had M. fermentans, and one veteran from Australia had a systemic M. genitalium infection. In nonmilitary ALS patients systemic mycoplasmal infections of various species were found in approximately 80% of cases.28 Of the mycoplasma-positive civilian patients who were further tested for various species of Mycoplasma, most were positive for M. fermentans (59%), but other Mycoplasma species, such as M. hominis (31%) and M. pneumoniae infections (9%) were also present. Some of the ALS patients had multiple infections; however, multiple mycoplasmal infections were not found in the military patients with ALS.28 In another study 50% of ALS patients showed evidence of systemic Mycoplasma species by PCR analysis.29
ALS patients who live in certain areas often have infections of Borrelia burgdorferi, the principal aetiological agent in Lyme disease. For example, ALS patients who live in a Lyme-prevalent area were examined for B. burgdorferi infections, and over one-half were found to be seropositive for Borrelia compared to 10% of matched controls.30 In addition, some patients diagnosed with ALS were subsequently diagnosed with neuroborreliosis.31 Spirochetal forms have been observed in the brain tissue of ALS patients and in patients with other neurodegenerative diseases.32 In general, however, the incidence of Lyme infections in ALS patients is probably much lower. In one recent study on 414 ALS patients only about 6% showed serological evidence of Borrelia infections.33 Some Lyme Disease patients may progress to ALS, but this is probably only possible in patients who have the genetic susceptibility genes for ALS as well as other environmental toxic exposures.34, 35
Additional chronic infections have been found in ALS patients, including human herpes virus-6 (HHV-6), Chlamydia pneumoniae andother infections.36, 37 There is also a suggestion that retroviruses might be involved in ALS and other motorneuron diseases.38 McCormick et al.39 looked for reverse transcriptase activity in serum and cerebrospinal fluid of ALS and non-ALS patients and found reverse transcriptase activity in one-half of ALS serum samples tested but in only 7% of controls. Interestingly, only 4% of ALS cerebrospinal fluid samples contained reverse transcriptase activity.39
Although the exact cause of ALS remains to be determined, there are several hypotheses on its pathogenesis: (1) accumulation of glutamate causing excitotoxicity; (2) autoimmune reactions against motor neurons; (3) deficiency of nerve growth factor; (4) dysfunction of superoxide dismutase due to mutations; and (5) chronic infection(s).24, 27-40 None of these hypotheses have been ruled out or are exclusive, and ALS may have a complex pathogenesis involving multiple factors. 28, 36
It is tempting to propose that infections play an important role in the pathogenesis or progression of ALS.28, 40 Infections could be cofactors in ALS pathogenesis, or they could simply be opportunistic, causing morbidity in ALS patients. For example, infections could cause the respiratory and rheumatic symptoms and other problems that are often found in ALS patients. Since the patients with multiple infections were usually those with more rapidly progressive disease,28 infections likely promote disease progression. Indeed, when Corcia et al.41 examined the cause of death in 100 ALS patients, the main causes were broncho-pneumonia and pneumonia. Finally, there are a number of patients who have ALS-like signs and symptoms but fall short of diagnostic criteria. Although a careful study has not been attempted on these patients, there is an indication that they have the same infections as those found in patients with a full diagnosis of ALS (personal communication). Thus ALS-like diseases may represent a less progressive state, in that they may lack additional changes or exposures necessary for full ALS.
Multiple sclerosis
Multiple sclerosis (MS) is the most common demyelinating neurological disease. It can occur in young or older people and is a cyclic (relapsing-remitting) or progressive disease that continues progressing without remitting.42 Inflammation and the presence of autoimmune antibodies against myelin and other nerve cell antigens are thought to cause the myelin sheath to break down, resulting in decrease or loss of electrical impulses along the nerve fibers.42, 43 In the progressive subset of MS neurological damage occurs additionally by the deposition of plaques on the nerve cells to the point where nerve cell death occurs. In addition, breakdown of the blood-brain barrier in MS is associated with local inflammation caused by glial cells.42, 43 The clinical manifestations of demyelinization, plaque damage and blood-brain barrier disruptions cause variable symptoms, but they usually include impaired vision, alterations in motor, sensory and coordination systems and cognitive dysfunction.43
There is strong evidence for a genetic component in MS.44, 45 Although it has been established that there is a genetic susceptibility component to MS, epidemiological and twin studies suggest that MS is an acquired, rather than an inherited, disease.46
MS has been linked to chronic infection(s).46, 47 For example, patients show immunological and cytokine elevations consistent with chronic infections.48-50 An infectious cause for MS has been under examination for some time, and patients have been tested for various viral and bacterial infections. 44, 45,47, 48, 51 One of the most common findings in MS patients is the presence of C. pneumoniae antibodies and DNAin their cerebrospinal fluid.51-53 By examining relapsing-remitting and progressive MS patients for the presence of C. pneumoniae in cerebrospinal fluid by culture, PCR and immunoglobulin reactivity Sriram et al.52 were able to identify C. pneumoniae in 64% of MS cerebrospinal fluid versus 11% of patients with other neurological diseases. They also found high rates (97% positive) of PCR-positive MOMP gene in MS- patients versus 18% in other neurological diseases, and this correlated with 86% of MS patients being serology-positive patients by ELISA and Western blot analysis.52 Examination of MS patients for oligoclonal antibodies against C. pneumoniae revealed that 82% of MS patients were positive, whereas none of the control non-MS neurological patients had antibodies that were absorbed by C. pneumoniae elemental body antigens.53 Similarly, Contini et al.54 found that the DNA and RNA transcript levels in mononuclear cells and cerebrospinal fluid of 64.2% of MS patients but in only 3 controls.
Using immunohistochemistry Sriram et al.55 later examined formalin-fixed brain tissue from MS and non-MS neurological disease controls and found that in a subset of MS patients (35%) chlamydial antigens were localized to ependymal surfaces and periventricular regions. Staining was not found in brain tissue samples from other neurological diseases. Frozen tissues were available in some of these MS cases, and PCR amplification of C. pneumoniae genes was accomplished in 63% of brain tissue samples from MS patients but none in frozen brain tissues from other neurological diseases. In addition, using immuno-gold-labeled staining and electron microscopy they examined cerebrospinal fluid sediment for chlamydial antigens and found that the electron dense bodies resembling bacterial structures correlated with PCR-positive results in 91% of MS cases.55 They also used different nested PCR methods to examine additional C. pneumoniae gene sequences in the cerebrospinal fluid of 72 MS patients and linked these results to MS-associated lesions seen by MRI.56
MRI was used by Grimaldi et al.57 to link the presence of C. pneumoniae infection with abnormal MRI results and found linkage in 21% of MS patients. These turned out to be MS patients with more progressive disease.58 In addition, higher rates of C. pneumoniae transcription were found by Dong-Si et al.58 in the cerebrospinal fluid of 84 MS patients. The data above and other studies strongly support the presence of C. pneumoniae in the brains of MS patients,59-61 at least in the more progressed subset of MS patients.
Other research groups have also found evidence for C. pneumoniae in MS patients but at lower incidence. Fainardi et al.62 used ELISA techniques and found that high-affinity antibodies against C. pneumoniae were present in the cerebrospinal fluid of 17% of MS cases compared to 2% of patients with non-inflammatory neurological disorders. They found that the majority of the progressive forms of MS were positive compared to patients with remitting-relapsing MS. The presence of C. pneumoniae antibodies was also found in other inflammatory neurological disorders; thus it was not found to be specific for MS.62
In contrast to the studies above, other researchers have not found the presence of C. pneumoniaeor other bacteriain the brains of MS patients.63-65 For example, Hammerschlag et al.66 used nested PCR and culture to examine frozen brain samples from MS patients but could not find any evidence for C. pneumoniae. However, in one study C. pneumoniae was found at similar incidence in MS and other neurological diseases, but only MS patients had C. pneumoniae in their cerebrospinal fluid.64 Swanborg et al.67 reviewed the evidence linking C. pneumoniae infection with MS and concluded that it is equivocal, and they also speculated that specific genetic changes may be necessary to fulfill the role of such infections in the aetiology of MS.
Another possible reason for the equivocal evidence linking MS with infections, such as C. pneumoniae, is that multiple co-infections could be involved rather than one specific infection. In addition to C. pneumoniae found in most studies, MS patients could also have Mycoplasma species, B. burgdorferi and other bacterial infections as well as viral infections.68 When multiple infections are considered, it is likely that >90% of MS patients have obligate intracellular bacterial infections caused by Chlamydia (Chlamydophila), Mycoplasma, Borrelia or other intracellular bacterial infections. These infections were found only singly and at very low incidence in age-matched subjects.68 In spite of these findings, others did not find evidence of Mycoplasma species in MS brain tissue, cerebrospinal fluid or peripheral blood.69
Viruses have also been found in MS. For example, HHV-6 has been found at higher frequencies in MS patients, but this virus has also been found at lower incidence in control samples.70 Using PCR Sanders et al.70 examined postmortem brain tissue and controls for the presence of various neurotrophic viruses. They found that 57% of MS cases and 43% of non-MS neurological disease controls were positive for HHV-6, whereas 37% and 28%, respectively, were positive for herpes simplex virus (HSV-1 and -2) and 43% and 32%, respectively, were positive for varicella zoster virus. However, these differences did not achieve statistical significance, and the authors concluded “an etiologic association to the MS disease process [is] uncertain.” They also found that 32% of the MS active plaques and 17% of the inactive plaque areas were positive for HHV-6.70 Using sequence difference analysis and PCR Challoner et al.71 searched for pathogens in MS brain specimens. They found that >70% of the MS specimens were positive for infection-associated sequences. They also used immunocytochemistry and found staining around MS plaques more frequently than around white matter. Nuclear staining of oligodendrocytes was also seen in MS samples but not in controls.71 Using immunofluorescent and PCR methods HHV-6 DNA has also been found in peripheral leukocytes in the systemic circulation of MS patients.72, 73 However, using PCR methods, others did not found herpes viruses in the peripheral blood or CSF of MS patients.74, 75 Evidence that prior infection with EBV could be related to the development of MS was proposed; however, EBV infects more than 90% of humans without evidence of health problems and 99% of MS patients.76 The difference in MS patients could be the presence of multiple infections, including EBV. Recently Willis et al.77 used multiple molecular techniques to examine MS tissue but failed to find EBV in any MS tissues but could find EBV in CNS lymphomas.
Current reviews and the information above points to an infectious process in MS.47, 48, 75, 76, 78-80 Although a few studies did not come to this conclusion,74, 75 most studies have found infections in MS patients. It is interesting that it is the progressive rather than relapsing-remitting forms of MS which have been associated with chronic infections; therefore, infections might be more important in MS progression than in its inception. Various infections may also nonspecifically stimulate the immune system.47, 48 Infections may also invade immune cells and alter immune cell function in a way that promotes inflammation and autoimmune activity.78 If infections like C. pneumoniae and Mycoplasma species are important in MS, then antibiotics effective against these infections should improve clinical status. Although preliminary, that is in fact what has been seen, but not in all patients.81 As in other neurodegenerative diseases, multiple factors appear to be involved in the pathogenesis of MS.
Alzheimer’s disease
Alzheimer’s Disease (AD) is a family of brain disorders usually found in elderly patients and is the most common cause of dementia. AD is characterized by slow, progressive loss of brain function, notable lapses in memory, disorientation, confusion, mood swings, changes in personality, language problems, such as difficulty in finding the right words for everyday objects, loss of behavioral inhibitions and motivation and paranoia. The course of AD varies widely, and the duration of illness can range from a few years to over 20 years. During this period the parts of the brain that control memory and thinking are among the first affected, followed by other brain changes that ultimately result in brain cell death.82
AD is characterized by distinct neuropathological changes in brain tissues and cells. Among the most notable are the appearance of plaques and tangles of neurofibrils within brain nerve cells that affect synapses and nerve-nerve cell communication. These structural alterations involve the deposition of altered amyloid proteins.83, 84 Although the cause of AD is not known, the formation of the amyloid plaques and neurofibrillary tangles may be due to genetic defects and resulting changes in the structure of beta amyloid proteins. This in turn may be caused by chemicals or other toxic events, inflammatory responses, excess oxidative stress and increases in reactive oxygen species, loss of nerve trophic factors and reductions in nerve cell transmission.83-87
Recently AD brain infections have become important.88-90 For example, one pathogen that has attracted considerable attention is C. pneumoniae.91, 92 As mentioned above, this intracellular bacterium has a tropism for neural tissue, and it has been found at high incidence in the brains of AD patients by PCR and immunohistochemistry.92C. pneumoniae has also been found in nerve cells in close proximity to neurofibrillary tangles.92, 93 Similarly to Mycoplasma species, C. pneumoniae can invade endothelial cells and promote the transmigration of monocytes through human brain endothelial cells into the brain parenchyma.94C. pneumoniae has been found in the brains of most AD patients,91 and it has been cultured from AD brain tissue.95 Injection of C. pneumoniae into mice stimulates beta amyloid plaque formation.96 Although the data are compelling, some investigators have not found C. pneumoniae infections in AD.97, 98
AD patients also have other bacterial infections, such as B. burgdorferi.99 Using serology, culture, Western blot and immunofluorenscence methods this Lyme Disease infection has been examined in AD.100, 101 Not all researchers, however, have found evidence of B. burgdorferi in AD patients.102, 103 The presence of intracellular infections like B. burgdorferi in AD patients has been proposed to be a primary event in the formation of AD beta amyloid plaques. This is thought to occur by the formation of “congophilic cores” that attract beta amyloid materials.104 Multiple reports indicate that AD nerve cells are often positive for B. burgdorferi, indicating that this intracellular bacteria could be important in the pathogenesis of AD.99, 100, 104, 105
The hypothesis in AD that intracellular microorganisms could provide “cores” for the attraction of beta amyloid materials is appealing, but other factors, including the induction of reactive oxygen species, lipid peroxidation and the breakdown of the lysosomal membranes releasing lysosomal hydrolases, are also thought to be important in beta amyloid deposition.105 That infections may be important in AD pathogenesis is attractive; however, some negative reports have not confirmed the presence of infections like B. burgdorferi in AD patients.99-101 This suggests that the infection theory, although compelling, remains controversial.102, 105
Herpes virus infections have also been found in AD,especially HSV-1.106, 107 Previously it was determined that HSV-1 but not a related neurotrophic virus (varicella zoster virus) is present more often in AD brains, and this could be linked to AD patients who have the risk factor ApoE e4 allele.108, 109 HSV-1 is thought to be involved in the abnormal aggregation of beta amyloid fragments within the AD brain by reducing the amount of full-length beta amyloid precursor protein and increasing the amounts of their fragments.110 HSV-1 infection of glial and neuronal cells results in a dramatic increase in the intracellular levels of beta amyloid forms, whereas the levels of native beta amyloid precursor protein are decreased.111 This is similar to what has been found in mice infected with HSV-1, indicating that HSV-1 is probably involved directly in the development of senile-associated plaques. Another herpes virus, HHV-6, has also been found in AD patients, but it is thought that this virus is not directly involved in AD pathogenesis. HHV-6 may exacerbate the effects of HSV-1 in AD ApoE e4 carriers.112
Other infections have been found in AD patients, for example, C. pneumoniae, Helicobacter pylori amongst others.113 It has been proposed that such infections may act as a trigger or co-factor in AD.114 Although experimental evidence that pathogens can elicit the neuropathological changes and cognitive deficits that characterize AD is lacking, this approach may yield interesting and important results. These authors also stressed that systemic infections must be considered as potential contributors to the pathogenesis of AD.114
Parkinson’s disease
Parkinson’s disease (PD) is characterized by akinesia, muscular rigidity and resting tremor.103 In addition, autonomic dysfunction, olfactory disturbances, depression, sensory and sleep disturbances and frequently dementia characterize this disease.115 The pathology of PD indicates a progressive loss of the dopamine neurons of the substantia nigra together with the presence of Lewy bodies and alpha-synuclein. More extensive brain degeneration also occurs, from the medulla oblongata to the cerebral cortex.116, 117
Age-related inclusion bodies and protein aggregations or defects in their degradation characteristically occur in PD, but their role in PD pathogenesis remains unclear.117, 118 Some evidence suggests a relationship between PD and specific genetic changes, such as changes in the genes affecting mitochondria, protein degradation, organelle trafficking and vesicular fusion, and in proteins involved in oxidative stress or antioxidant function.102 Inflammation has also been associated with PD pathology.119
The pathogenesis of PD has been proposed to be due to multiple genetic and neurotoxic events that produce oxidative damage and cell death. In the case of PD the relevant targets of toxic events are neuromelanin-containing dopaminergic neurons of the substantia nigra.118, 120 A case-control study indicated that multiple environmental factors and genetic background were statistically related risk factors for PD.121 Prominent among these were long-term toxic exposures and trauma early in life.122 For example,early life exposure to brain injury, chemicals and/or infections may initiate a cyclic inflammatory process involving oxidative damage, excitotoxicity, mitochondrial dysfunction and altered proteolysis that later in life results in substantia nigra neuron death.123, 124
A role for chronic infections in PD pathogenesis has been proposed.123, 124 One infection found in PD that has aroused considerable interest is the presence of chronic gastrointestinal Helicobacter pylori.125 Indeed, treatment of this infection offers relief to late stage cachexia in PD patients receiving L-dopa.126Helicobacter pylori-infected PD patients showed reduced L-dopa absorption and increased clinical disability,127 whereas treatment of this infection increased L-dopa absorption and decreased clinical disability.128H.pylori may not be directly involved in the pathogenesis of PD, but its systemic presence could affect the progression and treatment of PD, probably by stimulating inflammation and autoimmunity.128
Chronic infections in PD have been linked to inflammation and autoimmune responses.129-131 Experimental models of PD have been developed using neurological viral or bacterial infections to initiate the pathogenic process.132, 133 Spirochetes have also been found in Lewy bodies of PD patients.30 Other infections, such as viral encephalitis,134 AIDS-associated opportunistic infections of the basal ganglia,135 coronavirus,136 among other infections,68, 137, 138 have been found in PD and could be important in stimulating inflammation and autoimmune responses. It has been stressed that additional research will be necessary to establish whether a causal link exists between PD and chronic infections.139
Neurobehavioral diseases
Autism spectrum disorders
ASD, such as autism, Asperger’s syndrome, etc., are neurobehavioral diseases of primarily the young where patients generally suffer from an inability to communicate properly, form relationships with others and respond appropriately to their environment. Such patients do not all share the same signs and symptoms but tend to share certain social, communication, motor and sensory problems that affect their behavior in predictable ways. These patients often display repetitive actions and develop troublesome fixations with specific objects, and they are often painfully sensitive to certain sounds, tastes and smells.140, 141
ASD cases are likely to be caused by multiple factors, including genetic defects, heavy metal, chemical and biological exposures, among other important events, which are probably different in each patient. ASD patients appear to have similarities in genetic defects and environmental exposures that are important in patient morbidity or in illness progression.5-8, 140-142
Chronic infections appear to be an important element in the development of ASD.6, 16, 143, 144 In ASD patients more than 50 different bacterial, viral and fungal infections have been found,6 some apparently more important than others in causing symptoms. It has been known for some time that ASD patients have a number of nonspecific chronic signs and symptoms, such as fatigue, headaches, gastrointestinal, vision problems, occasional intermittent low-grade fevers and other signs and symptoms that are generally excluded in the diagnosis of ASD but are consistent with the presence of infections.143 Indeed, increased titres to various viruses as well as bacterial and fungal infections have been commonly seen in ASD patients.6, 16, 19, 143-145 Not withstanding these reports, epidemiological evidence for an association of childhood infections in the first two years of life and ASD has been mixed.146
Environmental exposures to chemicals and heavy metals also appear to be important in the development of ASD.140, 141, 147, 148 The relationship between ASD and heavy metals may involve the role of multiple vaccines in ASD pathogenesis.130, 141 ASD patients often show their first signs and symptoms after multiple childhood immunizations, and the sharp increase in Autism rates occurred only after the multiple MMR vaccine came into widespread use.141 In some states in the U.S. children receive as many as 33 vaccines before they can enroll in school.140 Such vaccines can contain mercury and other toxic preservatives, and some may also contain contaminating bacteria, as found in veterinary vaccines.149
There are very few studies that have followed the transmission of infections and subsequent autism. Previously we found that veterans of the Gulf War with chronic fatiguing illnesses (Gulf War illnesses, GWI) exhibited multiple nonspecific signs and symptoms similar to chronic fatigue syndrome/myalgic encephalomyopathy (CFS/ME).150, 151 After returning to the home with GWI, their children subsequently became symptomatic, and these children were often diagnosed with ASD.152, 153 Symptomatic children (mostly diagnosed with ASD) were infected with the same Mycoplasma species, M. fermentans, that was found in the veterans and their symptomatic family members, and this was not seen in aged-matched control subjects or in military families without GWI. In the GWI families some non-symptomatic family members did have mycoplasmal infections (~10%), but this was not significantly different from the incidence of mycoplasmal infections in healthy control subjects.152, 153
Subsequently ASD patients who were not in military families were examined for systemic mycoplasmal infections.153 The majority (~54%) were positive for mycoplasmal infections. However, in contrast to the children of GWI patients who for the most part had only M. fermentans, the civilian children tested positive for a variety of Mycoplasma species. We also tested a few siblings without apparent signs and symptoms, and for the most part few had these infections.153 In another study we examined the blood of ASD patients from Central and Southern California and found that a large subset (>58%) of patients showed evidence of Mycoplasma infections compared to age-matched control subjects (Odds Ratio=13.8, p<0.001).19 ASD patients were also examined for C. pneumoniae (8.3% positive, Odds Ratio=5.6, p<0.01) and HHV-6 (29.2% positive, Odds Ratio=4.5, p<0.01). The results indicated that a large subset of ASD patients display evidence of bacterial and/or viral infections (Odds Ratio=16.5, p<0.001).19
ASD patients have been examined for B. burgdorferi infections.154 Various studies revealed that 22-30% of ASD patients (N=76) have Borrelia infections.6, 154 The incidence of Borrelia infections in ASD patients may be related to Lyme disease distribution, with some Lyme-intense areas having high prevalence, and other areas having a low prevalence. Other infections, such as Lyme-associated Bartonella, Babesia, Ehrlichia and non-Lyme-associated CMV, Plasmodium species, Toxoplasma species and Treponema species may also be associated with ASD.6
Final comments to part 1
When neurological symptoms are present, infections of the CNS must be considered. Brain infections can stimulate glial responses, and the presence of viral and bacterial infections in nerve cells, can stimulate autoimmune responses against nerve cell antigens as well as the infections within them.155 For example, in MS some 20 different bacterial and viral infections have been found, but the link between these infections and the pathogenesis of MS is still being debated.16,47, 75 One or even a few types of infections cannot be causally linked to MS, and the reason for this is that there may be too many possibilities. No one infection or a group of infections needs to be the trigger in MS to be important in the pathogenesis of MS. In time combinations of certain infections may eventually be identified at least in a subset of MS patients, and this will allow the development of new therapeutic approaches for many MS patients that are not recognized today.
One problem that is rarely discussed is the apparent disparity between the laboratory results from different laboratories. Often different laboratories cannot agree on types of infections found in various chronic diseases.47 There are a number of reasons for this, including differences in the source of materials, qualities of reagents and techniques used.16 Some procedures, such as PCR, have specific challenges that must be overcome in the handling of specimens, their stability, presence of interfering substances, contamination, sensitivity and specificity of the tests and interpretation of the results. Variability in results from different laboratories will remain a problem unless research groups work closely together to solve these problems. One example of how this has been overcome is a multi-centre research study on the presence of C. pneumoniae in the cerebrospinal fluid of clinically defined, mono-symptomatic MS patients.156Sriram et al.156 conducted this diagnostic trial with good concordance of results between different laboratories. Cooperative studies such as this should eventually alleviate discrepancies in the types of infections found by different research groups.
This review continues in Part 2 with psychiatric diseases, autoimmune diseases, fatiguing illnesses, and other infectious diseases with neurological aspects and an overall discussion of the topic. 157
The herniation of a gravid uterus through an incisional hernia site is a rare occurrence. Incisional hernia is a frequent complication of abdominal wall closure and the management of pregnancy with a large incisional hernia with gravid uterus in its sac is challenging. The following is a case report of gravid uterus through an incisional hernia of a midline incision. Case Report Mrs LB, 35 years, Parity 2, period of amenorrhea of 34 weeks 3 days, married for 12 years was admitted to the hospital from the outpatient department due to the ulceration of abdominal skin as a result of herniation of gravid uterus through the midline longitudinal incision of a previous caesarean section . She was a booked case of our hospital and had been receivingantenatal care since 20 weeks of gestation. At 20 weeks there was no herniation of the uterus through the incision line. In her subsequent visits she came with the uterus protruding through the incisional hernia. She was referred to the General Surgeon who recommended elective Caesarean section with repair of hernia. Her past obstetric history revealed that she had her first emergency caesarean section eight years before because of a breech presentation and a second caesarean section, due to thepremature rupture of membranes at term. Both the babies were living & well. On both occasions she was operated on through infra umbilical midline vertical incision. There was no history of caesarean section wound infection during the post operative period in the previous two pregnancies. On examination, she was moderately built and adequately nourished. There was mild pallor. Her pulse rate was 88 beats per minute and her blood pressure was 126/86 mm Hg. Heart and chest were normal. Abdominal examination revealed distention of the abdomen in thecentral area. The uterus was felt just underneath the skin with acomplete lack of anterior abdominal wall. (Figure I) Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair.
Bronchogenic cysts are lesions of congenital origin derived from the primitive foregut. They form due to ectopic budding of the foregut during the first trimester. Epithelial cells of the developing trachea and lung are pinched off and grow separately from the airways. Bronchogenic cysts are most commonly mediastinal, unilocular and contain clear fluid. Clinically, most cysts are symptomatic and occur in infancy or early childhood. Respiratory distress is the most common presentation in paediatric patients, manifested by recurring episodes of cough, stridor, and wheezing. Patient Description: A 13-year-old female presented with a two month history of right-sided back pain and five days of intermittent fever. The pain was worse on inspiration and made sleeping difficult. She denied wheezing, chest pain, or cough. She continued daily participation in competitive sports. Previous trials of antibiotics and an inhaled bronchodilator for presumed exercise-induced asthma were unsuccessful. Chest x-ray (CXR) showed a large cyst (10x10x8 cm3) in the posterior right lung. (Image 1). Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2) Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4) Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid. Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung. Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
Bronchogenic cyst should be included in the differential diagnosis of a child with cough, dyspnoea, and fever. Although rare, we stress the importance of keeping mycobacterial infection in mind in cases of an infected cyst. Acid-fast culture should be done on sputum and cyst contents. Due to the frequency of negative cultures, stains should also be performed on resected cyst specimens. Antibiotic therapy should be considered and administered based on the extent of infection. All symptomatic or enlarging cysts warrant surgical excision. Prophylactic removal of asymptomatic cysts is recommended due to higher rates of perioperative complications once cysts become symptomatic.10 We raise the question of whether earlier CXR is indicated to rule out bronchogenic cyst, particularly when patients do not improve after trials of watchful waiting, antibiotics, and bronchodilators for other possible respiratory diagnoses.
Introduction:The aim of the NHS Modernisation Agency’s Hospital at night project is to “Redefine how medical cover is provided in hospitals during the out of hours period.”(1) The project “requires a move from cover requirements defined by professional demarcation and grade, to cover defined by competency in order to release significant amounts of medical staff time and support the compliance with WTD (Working Time Directive) while enhancing clinical practice and training.”(1) Chairman of the BMA’s Junior Doctors Committee and also medical advisor to the Hospital at Night Project undertook a survey of junior doctors’ activity in the evening, night, and weekends. They noted that the evenings were very busy and the nights quieter, that general physicians work harder at night than those in other specialties or orthopaedic surgeons. In summary their survey showed that a huge amount of doctors’ time was wasted on tasks which did not require their level of skills. Such tasks included phlebotomy, searching for notes, and x-rays.(1) An evaluation report into the implementation and impact of the hospital at night pilot project, August 2005, identified key elements to minimize medical workload at night. These included working within a multidisciplinary, competency-based team, with extended skills ward staff to minimize reliance on the night team, reduce duplication, take away inappropriate tasks, bleep-filtering and better use of new technologies such as digital imaging and e-prescribing (2). Our aim was to assess the experience of a typical junior orthopaedic doctor’s experience during his on-call to assess their perspective of the implementation of hospital at nightand to establish whether the recommendations of the evaluation report were being implemented. Methods: A prospective review was conducted of the night duties of all junior doctors working or cross-covering trauma and orthopaedics across Frenchay and Southmead hospital sites of the North Bristol NHS Trust between December 2007 and January 2008.A questionnaire included nature of activity and level of experience, closed questions relating to the hand-over experience. Details of calls received and the nature of tasks undertaken during on-call period with times. Data were then stored and analysed using excel-office 2002. Results:Total of 51 questionnaires were completed by the junior orthopaedic doctors during their respective on-call duties. A total of 109 calls were received or tasks requested. The average time spent during hand-over was 14.1 minutes (range 5-20 minutes). Discussion: Our data indicates busiest times occurred between 21:00 – 23:00 (Fig 1) Figure 1, illustrates a distribution of the peak work-load period which occurred between 9pm-11pm and 1am-3am. This finding contradicts previous surveys done prior to the implementation of the hospital at night where it was noted that the nights were quieter and sub-specialist such as orthopaedic surgeons were not working as hard as general medics (1). Figure 2, shows the overall experience of the hand-over as judged by the orthopaedic juniors. There was an eighty-five percent (43/51) attendance by the on-call orthopaedic juniors of which seventy-two percent (32/44) thought that it was a useful experience Figure 3 illustrates a distribution of the calls received. As illustrated, 37/109 calls were viewed as inappropriate The majority of the orthopaedic juniors surveyed framed hospital-at-night hand-over was useful but thirty-four percent (37/109) of the calls they received were viewed as inappropriate (Fig 2,3). The most frequent of the inappropriate ward calls were ‘requests to rewrite drug-charts’ (Fig 4,5). Figure 4 describes the frequencies of these calls. As illustrated the most frequently inappropriate ward-call was to ‘rewrite drug-charts’. There were twenty-three (23/37) inappropriate ward-calls Figure 5 shows the reasons given by the on-call doctors for the inappropriate tasks. The most frequently given reason was that ‘the request should have been done during the day’. The second most frequently given reason for inappropriate calls was the fact that ‘it was a duplicated request’ Our survey also highlighted that the most frequently given reason for inappropriate tasks was firstly that the request should have been done during the day and secondly that it was a duplicated request. These findings seem to defeat the key purpose of the hospital-at-night project for an orthopaedic SHO on-call. Conclusion: Hospital at night cannot function in isolation. There are fewer doctors available then normally and the system has to use their time effectively. 30% of inappropriate calls to wards were to rewrite drug charts and to prescribe warfarin. This should have been identified and performed by the day staff. 10% of calls were to review X-rays. Much of the inappropriate activity could be pre-empted if both day and night staff attended the handover and the tasks outstanding from the day identified. The doctor on the night could then perform an hourly ward round completing these tasks without interrupting at the beginning of the night.
Introduction Dysmenorrhoea and other premenstrual symptoms are common among women of reproductive age and lead to suffering and impact on home, school, and work performance. Earlier studies have focused on the prevalence and risk factors of dysmenorrhoea 1, 2, 3. Surveys in Pakistan have found the prevalence of premenstrual symptoms varying from 53% to 67% in college girls 4, 5, 6. About 57% of students in one study reported that dysmenorrhoea affected their work5. Although these surveys document the prevalence and severity of symptoms they do not correlate it with the impact of specific symptoms on daily activities or with healthcare seeking behaviour. A population-based survey of 2262 women from Goa, India, revealed a linear association between pain severity and treatment seeking and time off from work 3. However the impact of specific symptoms of premenstrual syndrome on treatment seeking and rest was not reported. Aims Primary objective: The authors carried out a cross-sectional study to explore the impact of dysmenorrhoea and other premenstrual symptoms among women of reproductive age.Secondary objective: The authors intended to find out the predictors of healthcare-seeking behaviour including self-treatment for premenstrual symptoms. Methodology A cross-sectional survey study design was chosen. A 13-item questionnaire was administered to women, aged 16 to 50, who were not pregnant and had no known gynaecological, medical, musculoskeletal or neurological diagnosis. Participants were recruited from multiple sites using convenience sampling within urban areas of Islamabad and Rawalpindi in Pakistan. Trained interviewers (physicians, medical students, nursing staff, and high school students) filled out questionnaires interviewing female students at a medical college, a nursing college, and at city schools; as well as housekeeping staff and patients’ attendants at a tertiary care teaching hospital in Islamabad. A proportion of women completed the questionnaire themselves. Ethical approval was obtained from the Shifa International Hospital Ethics committee. No personally identifiable data such as the respondents’ names were recorded. ResultsStudy population characteristics A total of 1236 women from multiple locations within Islamabad and Rawalpindi, Pakistan, participated in the survey. Most of the women were in the younger age groups: 402 women (33%) were 16–20 years old and 622 (50%) were 21–35 years old. Fewer women were in the older age groups: 147 women (12%) were 36–45 years old and 63 (5%) were more than 45 years old. About 55% were unmarried and 61% had no children. The distribution of educational achievement was weighted towards the more educated: 16% were able to read a religious book (basic literacy); 49% had some school education (up to 12th grade); and 34% had professional level education. About 27% of the respondents were homemakers (among women with professional level education, 10% reported staying at home). Age at menarche was less than 12 years old for 16%; between 12 and 14 years for 62%; and more than 14 years old for 23% of the respondents. Severity of dysmenorrhoea and its correlation with premenstrual symptoms On the 10-point visual pain scale, 465 women (38%, 95% CI 35–41) reported mild dysmenorrhoea severity from 0 to 3; 517 women (42%, 95% CI 39–45) reported moderate severity from 4 to 7; and 248 women (20%, 95% CI 18–23) reported severe pain rated from 8 to 10. The linear regression coefficient between dysmenorrhoea severity score and the number of days unable to work in a month was 0.59 (standard error: 0.031). Table 1: Prevalence of premenstrual symptoms and their contribution to pain severity and days lost from work
Women reporting symptoms, n (%, 95% CI) a
Contribution to pain score b
Contribution to days out of work c
Low back pain
879 (72, 69–74)
0.39 *
0.05
Depressed mood
484 (40, 37–43)
0.17 *
-0.05
Headache
268 (22, 20–24)
0.25 *
0.22 *
Swelling
218 (18, 16–20)
0.03
0.12
Nausea
218 (18, 16–20)
0.17 *
0.01
* Statistically significant values (P < 0.005)a Respondents were allowed to select more than one option. Total respondents: 1236.b Linear regression coefficients for a 10-point visual pain score categorized into three levels.c Linear regression coefficients for self-reported days unable to work in a month. Table 1 shows the prevalence of primary symptoms of preceding menstruation and their contribution to a 10-point visual pain scale and to self-reported days unable to work in a month. Low back pain and headache contributed most to the pain score while headache and swelling correlated with days out of work. Impact of dysmenorrhoea Among the working women (366 professionals and housekeeping staff) 49% (95% CI 44–54) reported one or more days out of work in a month due to pain. Similarly, among the 452 students surveyed, 53% (95% CI 48–58) reported dysmenorrhoea affecting school performance (Table 2).
Table 2: Impact of premenstrual symptoms and dysmenorrhoea on household, school and work performance
All respondents, n (%)
Students, n (%)
Maids and housekeeping staff, n (%)
Self-employed, n (%)
Professionals, n (%)
Affected domain
Household chores
441 (37)
124 (28)
59 (40)
31 (52)
75 (35)
Household income
129 (11)
24 (5.3)
33 (22)
12 (20)
18 (8.5)
Performance in school
313 (25)
239 (53)
N/A
N/A
N/A
Social obligations
395 (33)
130 (29)
58 (39)
31 (52)
85 (40)
Unable to work for one or more days in a month
643 (53)
282 (63)
75 (51)
38 (63)
103 (50)
Percentages do not add up to 100% as respondents were allowed to select more than one affected domain.Values for 50% or more respondents acknowledging an impact in a domain are given in bold.
Treatment taken for dysmenorrhoea relief
Table 3 outlines the remedies sought for the relief of dysmenorrhoea symptoms and the reported effectiveness of each type of remedy. All treatments except homeopathic were felt to be effective. Logistic regression analysis showed that the use of any treatment type was related to low back pain (odds ratio 2.2, 95% confidence interval 1.6–2.9), pain severity (OR 2.0, 95% CI 1.6–2.5), headache (OR 1.7, 95% CI 1.2–2.4), depressed mood (OR 1.7, 95% CI 1.3–2.2), increasing education (OR 1.1, 95% CI 1.0–1.2) and not being unmarried (OR 0.52, 95% CI 0.34–0.79).
Table 3: Remedies sought for dysmenorrhoea relief and their patient-reported effectiveness
Women reporting use of treatment, n (%, 95% CI)a
Odds ratio for self-reported effectiveness, (95% CI)b
Conventional medicine
496 (56, 53–59)
13 (8.7 to 21)
Household remedies
285 (32, 29–35)
6.5 (4.1 to 11)
Herbal
90 (10, 8–12)
4.1 (2.2 to 7.7)
Homeopathic
125 (14, 12–17)
1.5 (0.89 to 2.6)
a Respondents were allowed to select more than one option. Total respondents: 1236. b Unconditional logistic regression (converged, 6 iterations, 878 cases included, using Epi Info 3.4.3). All odds ratios with P < 0.005, except homeopathic, P = 0.12.[CI, confidence interval]
Conventional medicine was sought by women with higher pain scores (OR 2.2, 95% CI 1.8–2.8) and greater years of education (OR 1.2, 95% CI 1.1–1.3); other factors such as age and specific symptoms were not statistically related. Women with a greater number of days unable to work were more likely to use herbal treatment (OR 1.4, 95% CI 1.1–1.9) while household remedies like hot water bottles and warm drinks were more commonly taken by women with headache (OR 1.66, 95% CI 1.2–2.4), depressed mood (OR 1.6, 95% CI 1.2–2.3) and lesser years of education (OR 0.88, 95% CI 0.78–0.99). Discussion This paper is the first, to the best of our knowledge, to show an association between specific premenstrual symptoms and dysmenorrhoea severity and healthcare-seeking behaviour. We found that certain symptoms, namely low back pain and headache, contributed more to the perceived severity than other complaints. This finding may be of importance to clinicians treating women with menstrual complaints especially when the treatment is symptom-oriented. In women working outside their homes clinicians may wish to target headache and swelling as these symptoms correlated with days unable to work. Prevalence of premenstrual symptoms in the present study was higher than a Japanese survey7 that reported back pain in 6.9% of women and headache in 11% of women (compared with our results of 72% and 22% respectively). This difference may be due to cultural differences in perception and reporting of symptoms, overall better health, and being strong and hardworking. It may simply be the perception difference in underdeveloped or developed country i.e. lack of resources, poor diet, and poor health. Menstrual symptoms caused a heavy impact on social, school, and work responsibilities in women, a finding we share with previous studies. A cross-sectional survey from India found that 17% of adolescent girls reported missing school classes due to dysmenorrhoea while 60% reported disruption of their daily activities8. In an Australian study, 53% of high school girls reported that dysmenorrhoea limited daily routines and 37% stated that it affected schoolwork9. A study from New York found 46% of students missing one or more days of school due to dysmenorrhoea10. Corresponding figures from the present study were: 62% students reported missing at least one day of school and 53% reported an impact on school performance. The authors would like to reiterate the need for screening for and treating menstrual symptoms because of the impact on daily activities and the potential to reduce avoidable suffering. Women seek a variety of sources for relief of menstrual symptoms. A survey of 2411 high school girls in Malaysia showed that 11% sought medical care although the majority (80%) obtained advice from their mothers regarding premenstrual symptoms11. A study of adolescent girls in Haryana, India, found that 5.3% consulted a physician for menstrual symptoms and 22% self-treated with over-the-counter medicines12. 52% reported self-treatment and 7.7% used complementary medicines in a Japanese study13. In the present study, although conventional medicine was felt to be most effective, it was used by only half of the women. This indicates poor access or awareness of available effective treatments. Even household and herbal remedies were infrequently used possibly due to their limited effectiveness. As menstruation and its associated symptoms are often thought to be a ‘normal’ part of women’s lives these issues may remain untreated in the community. Women who were more educated tended to seek more effective treatments, as did those who had more severe symptoms. Clinicians and public health professionals need to proactively reach women from less privileged background to reduce suffering from menstrual symptoms. Educational campaigns to improve awareness of safe and effective conventional medicine, such as non-steroidal anti-inflammatory drugs, could reach women not aware of these options. These public health campaigns may be addressed toward high-school girls, homemakers, and professionally employed women through separate targeted channels. The present study was limited by non-random (convenience) sampling yielding a study sample skewed towards more educated women. This may be due to sampling in urban areas only. The questionnaire was designed using closed-ended questions, to reduce subjectivity in data recording, limiting exploration of unanticipated variables. Psychosocial issues, such as socio-economic disadvantage and mental health, play an important role in the perception and reporting of menstrual symptoms3 but these factors were not explored in this study. Further research in this area should focus on awareness, access to care, and quality of life outcomes with different treatment options. ConclusionLow back pain and headache contribute the most to severity of dysmenorrhoea while headache and body swelling (fluid retention) were predictive of days unable to work. Conventional medicine is commonly used by more educated women, as well as those with more severe symptoms, and was perceived to be effective more often than other treatment modalities. Effective treatments for the relief of menstrual symptoms remain underutilized causing avoidable suffering.
IntroductionHospital inpatient falls have remained the subject of extensive research and intervention over the past 55 years1. Despite risk factor identification, multiple prediction system developments and harm reducing technologies, the issue of falls remains. The incidence of falls varies between 2.2 and 14 per 1000 patient days 2,3 and increases with age 4. In the UK’s National Health Service, 32% of adverse incident reports are due to falls 2 . In 2007 it reported 200,000 inpatient falls to the National Patient Safety Association 5. Whilst most patients (96%) came to no harm or minor harm, they estimated that over 500 hip fractures and 26 deaths resulted from these falls.Inpatient falls lead to greater morbidity and mortality than equivalent fractures in the community, 6 and they significantly increase the length of stay in hospital7. Apart from physical harm, there are also psychological consequences for patients such as anxiety, loss of confidence, and fear of falling 4. The risk of falls leads to a conundrum in rehabilitative care. Ideally, patients’ mobility, autonomy and dignity must be encouraged and respected - yet slips, trips and falls must be pre-empted often with varying degrees of intrusion and even restraint. In order to selectively target individual patients who would benefit from closer attention, many risk stratification tools have been developed to predict potential fallers. They were developed on a background of over 400 independent risk factors identified with falls 8. The most prominent in the UK are STRATIFY (St Thomas's risk assessment tool in falling elderlyinpatients) and Downton with the recent addition of the Wandering Behaviour Assessment 8. STRATIFY 4 was designed to be used once per week and assesses 5 factors –falls history, patient agitation, visual impairment that limits daily function, frequent toileting, and a transfer or mobility score of 3 or 4 . Each factor scores 1 point and a score greater than 2 was found to have a 92% sensitivity and 68% specificity for a fall in the following week. In the Wandering Behaviour study the STRATIFY criteria results were not reproduced and were found to have only an 82% sensitivity and 34% specificity in their study population 8. Downton 9 also has 5 categories of assessment; falls history, medication subtypes, audio-visual-sensory deficits, mental state (using the Mini Mental State Score <24) and stability of gait. Each category scores 1 point and a score of greater than 3 is considered significant. In the Wandering Behaviour study, when applying the Downton criteria they only found an 82% sensitivity and 36% specificity 8. The Wandering Behaviour assessment looks for the presence of the following :checking, pottering, aimless walking, walking with inappropriate purpose, walking with appropriate purpose but inappropriate frequency, excessive activity, night-time walking, attempts to leave the hospital and being brought back to hospital. The presence of any one of these was found to have a sensitivity of 43% but specificity of 91% 8. Thus, both STRATIFY and Downton are limited by the multi-disciplinary assessments required, so that even when implemented, it is difficult to repeat them on a daily or weekly basis. The Wandering Score is easily repeatable on a daily basis, but lacks the sensitivity of STRATIFY and Downton 8. The aim of this study is to investigate whether changes in a patient’s physiology can be predictive of falls risk, and if so, can they become a useful tool for calculating risk? The reason why we have chosen to investigate this is that many of the commonly encountered risk factors can potentially be reflected in the patient’s routine observations 10. For example, fever could indicate infection and delirium. Hypotension could result from anti-hypertensives, sedatives, or dehydration. Hypertensive states could result from stroke, stress response to infection, or even be a surrogate marker of cardiovascular disease predisposing to arrhythmias. Blood pressure variation could also be predictive since dynamic orthostatic challenges such as lying and standing blood pressure measurements are known to predict falls 10. Thus, by measuring fluctuations in the observations we hypothesised that it may be possible to make an accurate short term prediction of falls riskMethodsSubjectsWe obtained consent for this retrospective study from the hospital’s ethics committee. We based this study in the Acute Medical Unit of our hospital, as it has the largest case mix of patients recently admitted and is therefore most likely to have the largest physiological instability. We aimed to detect a mean difference of 10% in the physiological variability prior to falling with 80% power, p-value < 0.05, and a common standard deviation of 5 %. Our power calculation indicated that we needed to study 12 patients. We identified all the falls in the calendar year of 2008 by examining the records of all the incident report forms submitted by the ward. A total of 33 incident reports related to falls were logged. Two reports related to staff slips and trips and were excluded, and a third incident report failed to adequately identify either the patient’s name, date of birth or hospital number and so had to be excluded. One of the 30 patients fell twice, and this was treated as its own incident as with the STRATIFY paper. The incident report forms were also used to identify the time, nature, and outcome of the fall. Of all the case notes related to the 30 falls requested from medical records, only 13 were available for detailed review. MeasurementsHeart rate (HR), Blood Pressure (BP), Temperature and Respiratory Rates were all recorded and analysed. The PAR (Patient at Risk) Score as calculated by the nursing staff was included too. PAR Scores are validated mechanisms of identifying sick patients who may go on to develop deterioration to the point of requiring Intensive Care. Scores of >3 are associated with a high risk of deteriorating health and are calculated using the routine nursing observations set. Oxygen saturations were not included in this study, as even small deviations tend to be rapidly corrected by staff with oxygen and therefore were not thought to be a useful marker. Recordings of blood pressure and heart rate were all done with ward based equipment. It is impossible to know which machines were used on individual patients as the equipment has varied, both over the course of time, and between multiple wards. However, because the subjects were their own controls, we are confident that the same machine and cuff were used for taking all the 12 hour recordings as each individual machine is allocated to a given bay. Blood pressures were obtained using semi-automatic Dynamap equipment, therefore the readings are in effect calculated from the Mean Arterial Pressure (MAP). We elected to study the systolic readings only, as this represents the maximum perfusion pressure to the brain and carotid sinus. Two of the thirteen patients were known to have undergone orthostatic challenges as part of their admission work up and these were included. Other parameters recorded included the time of the fall, number of medications on the drug chart, whether the fall was observed and any injuries sustained. ControlsWe had two sets of controls. The first set was used to compare the age and gender profile of the fallers to those of the general adult admissions. We had to do this because the official hospital statistics included obstetric and paediatric admissions and comparison would have been inaccurate. We therefore took 4 random days’ of acute adult medical admissions (i.e. over the age of 18) in order to compile an age and gender profile of patients admitted with a ratio of 4:1 (n=110). In order to compare the variability in physiological parameters between fallers and non fallers we generated a second set of controls matched for age (± 5 years) and gender in a ratio of 4 to 1 from a random week’s cohort of patients in February 2009 (for practical purposes). For each matched control, recordings were made at the equivalent length of stay and the controls were not known to have previously fallen. The patients were taken from across the hospital’s medical wards (not Intensive Care or Surgical) with their diagnosis blinded from the investigators. We were able to match 47 of the 52 controls that we were aiming for. Only BP and HR data were recorded in the controls, as we already established that temperature and respiratory rate were not sensitive markers from our faller data. StatisticsOur 13 patients allowed us to reach sufficient statistical power of 80%. Physiological parameters were tested within groups using the Students t-test (paired, two tailed) and when comparing to controls using the Students t-test (unpaired, two tailed). The null hypothesis were rejected when p<0.05. Variability in heart rate, temperature, respiratory rate and PAR (Patient At Risk Score) were calculated using the mean, range and standard deviation between maximum and minimum values. Blood pressure variability was measured by using the maximum and minimum systolic pressure and calculating the mean, range and standard deviation. We have chosen to primarily measure variability by the range as it is a simple calculation that can be done by anyone on a ward. It doesn’t require a calculator nor any detailed knowledge of mathematics. It is therefore an effective and repeatable measure which could be easily implemented as part of a scoring system. Data processing and Statistical Analyses was done in MS Excel 2002 and SPSS v.14. ResultsThe mean age of fallers was 79 years old (SD 16, n=30) and of the acute medical admission controls 67 years old (SD 20, n=110) with p=0.003. The gender distribution of males to females was 63% to 37% respectively for fallers (n=30), but 38% to 62% in general medical take controls (Fishers exact test p<0.001). 54% of fallers (n=13) were admitted from their own home with 31% from Residential Homes and 15% from Nursing Homes. 54% were known to have a preceding falls history (n=13). The timings of the falls showed that 60% of falls occurred between 08.00 and 20.00 (n=30). 77% of falls occurred within 48 hours of admission (n=13). The circumstances of the falls were consistent with the NPSA statistics with 20% falling out of bed, 17% from chair, 17% from commode / toilet, 20% when walking, 3% in the bath and 23% not documented. The significance of the falls as measured by the incident report forms (n=26, in 4 cases not recorded) was 70% under the level of 6 (i.e. low level and did not require further investigation), 13% were over the level of 6 (i.e. were serious and required further investigation) and 17% were unrecorded. Most of the injuries (n=30) were none or minor – 47%, 10% had a head injury and 43% were not recorded. 95% of the falls were not observed. 31% of the patients (n=13) were taking fewer than 4 medications, 38% were taking between 4 and 7 medications and 32% were taking over 8 medications. Comparing the demographic characteristics of our fallers to the age and gender matched controls; average age was 79 for both fallers and controls (p=0.94) and the gender distribution was 7 females : 6 males in the fallers, and 27 females: 21 males in the controls (Fisher’s Exact Test p=1.0). The overall PAR score (n=13) was not sufficiently sensitive to predict falls risk – 77% had no change in their PAR score, 8% had a 1 point change and 15% had a 2 point change ( Table 1). Temperature variation (n=13) was minimal with 69% having less than 1 degree Celsius change and 31% having change of 1 to 1.5 degrees Celsius . Recorded respiratory rate variation was also minor (n=13) with 85% having a maximum change of up to 4 breaths per minute. Table 1. Physiological Parameter Data * denotes p<0.05
Fallers N = 13Mean ± SDRange (x-x)
Controls N = 47Mean ± SDRange (x-x)
PAR Score
1.2 ± 0.6(1 – 3)
PAR Score Variability
0.4 ± 0.6(0 – 2)
Temperature (Celsius)
37.1 ± 0.5(36.4 - 38.1)
Temperature Variability (Celsius)
0.6 ± 0.5(0 – 1.3)
Respiratory Rate (Breaths/Minute)
18.5 ± 1.9(16 – 22)
Respiratory Rate Variability (Breaths/Minute)
1.1 ± 1.5(0 – 4)
Highest Heart Rate (Beats/Minute)
86 ± 13(70 - 110)
86 ± 14(60 -112)
Lowest Heart Rate(Beats/Minute)
71 ± 16(50 -101)
79 ± 14(55 – 110)
*Heart Rate Variability (Beats/Minute)
15 ± 10(0 – 39)
7 ± 7(0 – 27)
Highest Systolic BP (mmHg)
142 ± 22(102 – 180)
140 ± 24(99 – 218)
Lowest Systolic BP(mmHg)
116 ± 19(71 – 150)
129 ± 24(86 – 199)
*Systolic Variability (mmHg)
26 ± 12(2 – 40)
11 ± 7(0 – 26)
In fallers (n=13), the mean highest heart rate was 86 bpm (SD=13) and the mean lowest heart rate was 71 bpm (SD=16). The range was 15 bpm (SD=9.6) with p<0.001. In controls (n=47) the mean highest heart rate was 86 bpm (SD=14) and the mean lowest heart rate was 79 bpm (SD=14). The range was 7 bpm (SD=7) with p<0.001. The significance test when comparing the highest average heart rate between fallers and controls shows p=0.98 showing that they were well matched. The significance test for comparing the variation of the heart rate between fallers and controls is p<0.001. In fallers (n=13), the mean highest systolic BP was 142 mmHg (SD=22) and the mean lowest systolic BP was 116 mmHg (SD=19). The average variation was 26 mmHg (SD=12) with p<0.001. In controls (n=47) the mean highest systolic BP was 140 mmHg (SD=24) and the mean lowest systolic BP was129 mmHg (SD=24). The average variation was 11 mmHg (SD=6.5) with p<0.001. The significance test when comparing the highest average systolic BP between fallers and controls shows p=0.77 showing that they were well matched. The significance test for comparing the variation of the systolic BP between fallers and controls is p<0.001. Charts 1 and 2 show the spread of measurements in the cardiovascular parameters between fallers and controls.
Chart 1. Comparison of the heart rate variation between Fallers and Controls
Chart 2. Comparison of the systolic blood pressure variation between Fallers and Controls
DiscussionThe average age of the fallers was significantly greater than the average age of those admitted to the hospital in general. This is unsurprising considering both mechanical deterioration of the musculoskeletal system with advancing age and the accumulation of disease processes. It is noteworthy that despite making up the smaller percentage of admissions to the hospital, men made up the greater proportion of fallers. Other much larger studies show considerable variability in their gender proportions 11,12, therefore this finding is unlikely to be truly significant. Apart from age and gender, polypharmacy was also a feature of our fallers. This is consistent with other studies 13,14,15. Additionally, our data was consistent with the overall NPSA statistics in terms of the significance and circumstances of the falls 5. The main and novel finding of our study was that fallers were significantly more likely to display a larger range in their cardiovascular observations than the standard hospital population. Whilst it is generally expected that subjects undergoing any routine measurement of heart rate and blood pressure will have a variation in measurements of about 10% over the course of 12 hours 16,17, we found that our fallers had a variation in their heart rate and blood pressure of approximately 20%. This is similar to the dips experienced by the normal population over the course of the night and during orthostatic challenge. This was despite the fact that the baseline measurements of highest value were virtually the same for both populations. Furthermore, almost all the values recorded were within normal limits – and would not normally require specific remedial action to be taken. This could also explain why this risk factor has not previously been identified in other studies. Our study indicates that it is the cardiovascular lability rather than the cardiovascular measurements per se, which acts as an acute predictor of falls. In fact, the sensitivity for falls prediction with either a range of HR values > 15 beats per minute or range of BP systolic values >25 mmHg was 77%. We would therefore expect that when such patients mobilize, the superadded orthostatic challenge would be too great for cardiac output to be suitably matched and so patients are at greater risk of falling. In terms of the 12 hour prospective risk of falling this could certainly explain why a patient with known risk factors will fall during a given nursing shift. Indeed it may also explain why a patient may fall during a hospital admission when patients were, for example, already parkinsonian and arthritic and yet had not previously fallen. Interestingly, neither temperature, respiratory rate, nor PAR Score showed any significant lability in the lead up to the falls. This was surprising as we would have expected them to be predictive of other well known risk factors. The lack of fluctuation in temperature and respiratory rate could provide further evidence that the key short term factor responsible for falls is cardiovascular lability. More detailed analysis showed that it was more likely that these measurements were insufficiently sensitive. Only four of the fallers were admitted with infections, and those subjects showed some temperature fluctuations. However, only 2 had temperatures above 37.5 degrees Celsius, which is consistent with the blunted fever response that is well known to occur in 50% of the elderly population 19,20 (and most fallers were elderly). The lack of value in respiratory rate recordings probably reflects the lack of due care and attention paid to this, the only manually measured parameter. It has long been recognized that respiratory rate recordings tend to be inaccurate 21 . The highly limited range of measurements recorded (16-22 breaths per minute) amongst all the fallers, despite some patients having severe pneumonia, further supports this finding. Finally, the PAR score tended to be quite static. This was a result of its constituent parameters not being sensitive (temperature, respiratory rate) and the fact that most of the heart rate and blood pressure recordings were within normal limits. LimitationsDespite the fact that this study was well powered and statistically significant, ultimately it is quite limited in numbers with just 13 patients. It was disappointing that we were not able to obtain case-notes or the appropriate file in the other 17. We are also presenting calculated data from the MAP measurements, without knowing the exact algorithms being used. For this reason, we analysed the given systolic pressures as further data manipulation would have increased inaccuracies. Our data is taken from relatively acute admissions and as such may not necessarily be applicable to long stay patients, where cardiovascular lability may not play an important role.Furthermore, controls were not matched for diagnosis or for the number of medications taken. This could lead to criticism that the comparison was poor, though the baseline measurements for the two were remarkably consistent. One of our aims was to see if variability could be used to accurately model general falls risk. We therefore thought it would be more useful to study the hospital’s general physiology, in all its varying degrees of illness. ConclusionsThis study shows the value of looking closely at patients’ observations and that even ‘normal’ values have to be interpreted in context . The data supports the finding that the risk of falling at a given point in time relates not only to predisposing factors, but also to their current cardiovascular status. We therefore suggest that a one-off falls risk assessment is no longer appropriate, but should be continuously reviewed on a shift-by-shift basis by nursing staff. This has significant ramifications for modernizing current risk stratification tools so that they are able take this into account.
Barrett’s Oesophagus (BO) describes a histological abnormality of the lower oesophagus widely accepted to be associated with gastro-oesophageal reflux disease (GORD). The nature of this disease has been a subject of debate since its description by Tileston in 1906 as peptic ulceration of the oesophagus. Barrett himself initially theorised that the abnormal oesophagus was in fact stomach that had been pulled into the chest by a congenitally short oesophagus (1). This idea was ultimately challenged as the area in question lacked a peritoneal covering, contained submucosal glands and muscularis propria characteristic of the oesophagus (2). In 1976, Paull et al described a distinctive type of intestinal metaplasia the investigators called "specialised columnar epithelium”. Specialised intestinal metaplasia is now widely accepted to be the hallmark of BO with its presence predisposing to dysplasia and cancer regardless of its location within the oesophagus (3).
Barrett’s Oesophagus, its identification and treatment continues to be an area of debate and interest. Although not sinister in itself, it is a known precursor to malignant disease and strongly associated with GORD. Barrett’s oesophagus is the most frequent predisposing risk factor for the progression to adenocarcinoma in the oesophagus. Sufferers have a 40 fold increased risk when compared to the general population (4).
The progression of GORD to BO appears to be related to exposure of oesophageal tissue to the acidic contents of the stomach. It is therefore seen in hiatus hernia, lower oesophageal dysfunction, delayed oesophageal acid clearance and duodenogastric reflux. Furthermore, it is the duration and not frequency of exposure to acidity that dictates erosive damage to the oesophagus. Levels of acidity also contribute. The damage to cells incurred leads to inflammatory infiltration and cell necrosis with replacement of oesophageal epithelium by metaplastic columnar cells.
Assessing severity of BO relies partly on endoscopic visualisation techniques and length of oesophagus involved. Long segment Barrett’s oesophagus (LSBO) indicated a >3cm segment of involvement with short segment disease involving <3cm. LSBO carries a higher risk of progression to adenocarcinoma. Its development is associated with long term symptoms, severe combined patterns of reflux (both erect and supine) on 24 hour pH monitoring and reduced lower oesophageal sphincter pressures. Patients are less sensitive to direct acid exposure than those with short segment disease. The latter group also tend to have shorter duration of symptoms, normal sphincter pressures and only upright reflux on 24 hour pH monitoring (3).
The Prague C and M criteria is a recently developed classification system utilising the circumferential and maximal extent of oesophageal columnar tissue to assess disease severity endoscopically (5). Its accuracy is yet to be assessed clinically, however, it is believed to largely improve the overall assessment of Barrett’s (6). The further classification of disease severity is based on the degree of dysplasia, with high grade dysplasia carrying a higher risk of progression to malignancy.
Barrett’s oesophagus is predominantly seen in the age group 55-65, with males being affected twice as frequently as females. The disease is more prevalent in the white population. Obesity, smoking and alcohol intake being further risk factors. H.pylori may be protective against Barrett’s oesophagus with two mechanisms postulated. Namely, the induction of atrophic gastritis, which results in decreased acid production and the production of neutralising ammonia independent of gastric atrophy (7). The duration of symptoms of GORD but not necessarily symptom severity is also associated with increased risk of progression to BO. The exact pathogenesis is not clearly understood and is believed to be a culmination of both hereditary and environmental factors. For example, some studies report a greater incidence of BO amongst first degree relatives in comparison to their unrelated counterparts (8). Other reports associate environmental factors such as a high body mass index, with an increasing risk of GORD and progression to BO (9). Underlying mechanisms include the proposition that central obesity predisposes to hiatus hernia formation (10) and subsequent gastric acid reflux. However further research is required to unlock the key processes that lead to the formation of BO; as these pathways may hold novel therapeutic targets.
Prevalence of BO is difficult to ascertain due to the lack of population based studies. Studies from the United States involving patients aged over 40 years undergoing gastroscopy reported a prevalence of 6.8% in all patients (11). A Swedish study involving 1000 volunteers is the only available true population based study and found a prevalence of 1.6% (12).
Endoscopic surveillance
The most appropriate method for both diagnosis and surveillance of Barrett’s Oesophagus is endoscopy. Its sensitivity is higher than other comparative techniques, such as barium based studies or CT/MRI. Endoscopic screening programmes can be beneficial in both highlighting patients with BO from those with chronic GORD, as well as monitoring patients with established disease who are at risk of progressing to adenocarcinoma of the oesophagus. The American College of Gastroenterologists identify older patients with chronic GORD symptoms as the most likely to benefit from endoscopic surveillance techniques. Studies have also shown that five year survival rates are generally greater for patients who have had their adenocarcinoma identified by surveillance in comparison to those who have not (13). Importance also lies in the method of surveillance, for example shorter endoscopic interval analysis for surveillance in low grade dysplasia, are associated with higher rates of detection of adeonacarcinoma (14).
Although screening for Barrett’s oesophagus relies largely on established endoscopic techniques, it remains an area of contention for several reasons. These include low prevalence and the invasiveness of endoscopy, as well as a lack of an easily identifiable demographic group. Alternative methods include the use of capsule endoscopy which offers increased acceptability of screening, is less invasive and carries an increased uptake rate in comparison (15). However a study involving 96 patients demonstrated only 67% sensitivity and 84% specificity for identifying the condition using this technique (16). A recent meta-analysis of nine studies comprising 618 patients offers the most up to date evaluation of this technique. The pooled sensitivity and specificity for diagnosing BO using this method was found to be 77% and 86% respectively. Studies using OGD as reference demonstrated sensitivity 78% and specificity 90%. With intestinal metaplasia as the reference standard, sensitivity 78% and specificity 73% was discovered although the latter figure was particularly affected by one study with very low values for this (17). Capsule endoscopy offers benefits in patient tolerance and morbidity as well as cost as the capsule can be swallowed in an office, potentially under nursing supervision. Despite this latter point, cost-benefit analysis of this technique have proved equivocal. There are also several drawbacks. Views achieved are no longer under operator control and anatomical landmarks are more difficult and potentially impossible to identify. Oesophageal transition time has been demonstrated to be as short as 1 second and biopsy is not possible regardless of this. This greatly limits the use of capsule endoscopy in BO surveillance which relies on biopsy. Ultimately, the use of capsule endoscopy in diagnosis or screening of BO is unsupported at this current time and is an area for future research.
Other methods include small calibre trans-nasal endoscopy, which involves inserting a small-calibre endoscope through the nose and oesophageal sphincter to visualise the oespophagus, stomach and duodenum. It has the advantage of not requiring any sedation only topical anesthesia, having a lower complication rate, requiring less nursing staff and being more cost effective in comparison to its more frequently performed counterpart. Capsule endoscopy, as described earlier, also has the advantage of lacking sedation, being less invasive and yielding lower complication rates. Other alternatives include narrow band imaging, which involves scanning large areas of mucosa for possible neoplasia and autoflourescence imaging in which dysplastic lesions are visualised by differences in colour. The usefulness of visualisation techniques including high-resolution magnification endoscopy and tissue staining with agents such as methylene blue or indigo carmine are still an area of debate. These techniques have been evaluated when used in combination and alone. Pit patterns identified using acetic acid chemoendoscopy were described in 2001 by Guelrud et al (18) and Sharma et al described differing mucosal patterns in BO (19). Numerous other agents and classification systems have been described. Currently the use of these techniques for diagnostic purposes has not been shown to offer superior results than the current gold standard of four quadrant biopsies. Comparison of biopsies taken with methylene blue directed biopsy versus conventional biopsy showed no significant benefit (20). The ability to identify areas of BO (particularly high-grade dysplasia) are not in question. However, low grade dysplasia may be missed and operator experience and skill must be greatly superior to utilise the benefits of these techniques. Staining techniques offer the additional complications and additional expense of carrying out the procedure. Methylene blue has been shown to induce cellular DNA damage in vitro via the generation of singlet oxygen when photoexcited by light (21) thereby potentially being carcinogenic in itself. Evidence to support non-biopsy detection of BO is currently not sufficient to replace the current gold standard but is another area of current and future research.
The low prevalence of BO in the general population makes screening, with upper GI endoscopy, less viable on both a financial and logistic level. The general consensus is those individuals who suffer from chronic GORD are most susceptible to BO and would therefore benefit the most from upper GI endoscopy (22). However the factors involved in the progression of BO to dysplasia and subsequent adenocarcinoma remain unclear, and hence the value of endoscopic surveillance remains a point of discussion.
Treatment options
The treatment options for BO must also be taken into consideration when addressing surveillance and burden of the disease. The treatment options can broadly be divided into three groups, which include conservative management with surveillance endoscopy, endoscopic therapy and surgical oesophagectomy. The pathways of treatment are governed by patient-specific factors as well as the degree of oesophageal dysplasia. Surveillance endoscopy forms an integral part of the management of BO, and this is largely due to studies which have demonstrated a greater five year survival and an earlier stage of detection of oesophageal carcinomas detected by surveillance endoscopy (13, 23). Current recommendations target individuals at high risk of BO, for example those with chronic GORD symptoms. If no dysplasia is found on biopsies from two endoscopies, surveillance intervals of 3 years are recommended. However, patients with low-grade dysplasia on biopsy should have an immediate repeat endocopy to confirm the diagnosis, and then yearly surveillance endoscopies until no dysplasia is observed. The management of patients with high-grade dysplasia is contentious and varies between centres. Recommendations include a repeat endoscopy to evaluate for cancerous progression, with some centres instituting regular three month surveillance with biopsies every 1-2cm of effected mucosa (6). Other centres, depending on the multi-focal extent of dysplasia recommend surgical intervention with oesophagectomy or endoscopic therapy; which includes mucosal resection, photodynamic therapy, argon plasma coagulation and endoscopic ablative techniques.
Surgery
Oesophagectomy is normally reserved for the management of high grade dysplasia with the potential for malignant transformation. The percentage of high grade dysplasia which progress to adenocarcinoma vary throughout the literature from 5% to 59% up to seven years from initial diagnosis (7). Although oesophagectomy provides potential for complete resolution, it also carries increased number of adverse effects which include strictures, infections and anastomotic leaks. Mortality rates may also exceed 18% in centres which perform smaller amounts of the procedure on average every year (24) in comparison to high volume centres where the mortality rates can be lower than 5% (25); making the procedure very operator-dependent. As a result less invasive therapeutic modalities are preferred in the management of lower grade oesophageal dysplasia.
Endoscopic Therapy
Endoscopic treatment of Barrett’s oesophagus is currently an area of great interest. Endoscopic resection alone, or in combination with other treatments, have been investigated thoroughly in the past; however studies including large populations based and long term standardised protocol are lacking. The interpretation of these results is therefore very difficult.
Endoscopic mucosal resection (EMR) for high grade dysplasia in BO was first reported in 2000 (26). The procedure involved initial identification of macroscopically visible or chemoendoscopically identifiable Barrett’s lesions. If the lesion showed no evidence of penetration into deeper tissue or metastasis, confirmed by ultrasound guidance, it would be open to resection (27). Ideal lesions include those easily identifiable by macroscopic techniques, limited in size and restricted to the mucosa. However, almost all reports realised the risk of incomplete treatment with recurrence of disease. Some authors advocated the use of circumferential endoscopic resection in order to minimise this risk (28). Endoscopic ultrasound has also been used, prior to treatment, to optimise therapy and has a degree of use in staging of oesophageal cancers (29). Post EMR data showed a low rate of complications with high rate of complete eradication of Barrett’s tissue in the short term. Larghi et al (30) investigated the long-term follow-up of patients undergoing EMR and complete Barrett’s eradication (CBE-EMR). This study involved 24 patients over a 3 year period. Histological eradication of Barrett’s oesophagus was achieved in 87.5% of patients. 3 patients suffered strictures which were endoscopically resolved. Other studies have shown similarly successful eradication with similar complications of bleeding and stricture formation (31, 32). Comparison with previous studies also demonstrated the need for long follow-up to identify potential disease recurrence. In order to minimise stricture formation, a maximum cirmcumference of 50% could be resected during each therapy. A median of 2 sessions was required for complete eradication. 13 patients also received argon plasma photocoagulation in order to ablate isolated islands of a few centimetres of BO. These studies highlight the use of mucosal resection either alone or in conjunction with other treatment modalities, such as argon plasma coagulation, in the treatment of BO. Other options are discussed below.
Argon Plasma Coagulation
This procedure involves the use of a high voltage current to ionise a jet of argon gas and treat the effected tissue. It is also used to treat bleeding lesions endoscopically hence the term coagulation. This procedure has been suggested to be of use in the treatment of BO (33, 34) and several studies have evaluated its efficacy (35-37). Conclusions have been mixed with some studies showing high rates of Barrett’s recurrence and others also suggesting poor rates of initial lesion ablation (37). Generally, rates of complete reversal of BO range in the region of 61-70% (38-42). Other studies have shown more successful results with complete ablation in 87-100% of patients (43-46). A later study evaluated these results as well as performing a further long-term follow-up of 66 patients with high-grade dysplasia undergoing APC with anti-reflux treatment. Histologically confirmed Barrett’s oesophagus was found in 12.1% of patients during further endoscopic surveillance. Patients were treated with anti-reflux therapy (both medical and surgical) and one repeat session of APC. No intraepithelial neoplasia or oesophageal adenocarcinoma was detected during the entire follow-up period of 51 months median (range 9-85) (35).
The available evidence in relation to APC still remains slightly difficult to interpret. Even the larger trials do not involve extensive samples of patients. Furthermore there is a variance between studies with regard to patient selection and exclusion criteria, anti-reflux strategies and the procedure itself. Other pitfalls include the difficulty in assessing the precise depth of the lesion and whether the penetration during treatment was successful enough to ablate the entire lesion. There is also no histological confirmation to help correct insufficient ablation and for this reason some studies have reported an increased risk of progression to cancer and metastasis if invasion past the muscularis occurs (47). Low rates of recurrence seem to be related to the use of higher power settings for ablation, up to 90W as demonstrated by Madisch et al (35). This group also demonstrated the potential role for high dose proton pump inhibitor therapy using a total of 120mg daily in three divided doses to suppress acid for the duration of treatment. Surgical anti-reflux procedures were also found to be associated with reduced recurrence rates. As mentioned above, this procedure may in itself provide a form of treatment for BO and further progression.
Although rare, complications of APC can be severe. Oesophageal perforation has been reported with 2 patient deaths as a consequence (40, 42). Mild oesophageal strictures amenable to endoscopic dilatation have been widely reported. Pleural effusions and bleeding ulcers have also been reported. Despite this, APC can be useful as an adjunct and also effective in the treatment of distinct groups of Barrett’s sufferers with amenable lesions.
Photodynamic therapy
Photodynamic therapy (PDT) involves the systemic administration of a photosensitising drug, followed by irradiation with a controlled light source via an endoscope. The light, in the presence of oxygen, activates the photosensitiser causing photochemically induced tissue destruction (48). Although technically this sounds a difficult procedure, in practice it is actually one of the simplest to perform. However, as with surgical oesophagectomy, it is operator dependent with complication rates increasing within the community in comparison to specialist centres.
The component parts of the photosensitisation process have also evolved with time.
Several photosensitisers have undergone trial with varying results. Trials with Hematoporphyrin derivative as the photosensitising agent showed high rates of stenosis as well as prolonged sensitivity of the skin to light (49). More recently, 5-aminolevulinic acid (5-ALA) has shown promise with good therapeutic results and reduced side-effects in the short term (50-51). 5-ALA also has a reduced period of cutaneous photosensitivity of around one week, in comparison to previous photosensitisers such as sodium porfimer, in which patients would need to take precautions for thirty to ninety days (27). Several studies have demonstrated the effectiveness of photodynamic therapy in BO. The first randomised clinical trial looked at 485 patients with BO and high grade dysplasia (HGD) (52). 208 patients were accepted into the to-treat population, and received photodynamic therapy and omeprazole (PDT+OM); whilst 202 patients formed the control group and received omeprazole alone (OM). The study demonstrated a significant difference with 77% of the PDT+OM group, compared with 39% of the OM group, receiving complete ablation of HGD. The progression from HGD to adenocarcinoma was also significantly lower in the PDT+OM group (13% vs 28%). This study highlighted the effectiveness of photodynamic therapy in conjunction with medical antacid therapy, in ablating high grade dysplasia and reducing the incidence of oesophageal adenocarinoma.
Pitfalls of PDT include the suggestion that lesions greater than 2mm in depth cannot be effectively removed (53), although the photosensitising agent used can influence this. For example, some studies have shown sodium porfimer to have an increased treatment depth of 3-4mm in comparison to other agents (54-55). However limited depth of penetration overall can compromise the ability of PDT to effectively treat high-grade dysplasia. Other common complications post PDT include stricture formation with some studies reporting rates as high as 30% overall and 50% in patients undergoing more than one procedure (56). Although high, long term complications related to this are not reported and most cases are relieved with endoscopic dilatation. Similarly other endoscopic techniques, photodynamic therapy may be inadequate at eliminating dysplastic tissue that is not visible on endoscopy. The issue of buried glands is an area of great interest due to the implication that a treated patient with macroscopically normal tissue may have dysplastic or even malignant tissue beneath. This highlights the importance of regular follow-up endoscopies with a thorough biopsy protocol. An additional complication with photodynamic therapy is the lack of histological samples post therapy, which might be used to assess the completeness of resection as in EMR.
Despite its limitations, photodynamic therapy has been proven an effective treatment for BO in numerous trials and case reports. Future directions include steps to improve photosensitiser agents, dosimetry, and light parameters which should help minimise the associated complication rate.
Radiofrequency Ablation
Radiofrequency ablation is one of the newer endoscopic treatment modalities to show promise in preventing the progression of Barrett’s oesophagus and eliminating the lesion completely. The technique utilises a balloon, 3cm long and consisting of a 60 electrode rings spaced narrowly together every 500micrometres in a bipolar fashion (HALO360 system, Barrx Co, Sunnyvale, CA, USA). A sizing balloon is used to ascertain the circumference of the area to be treated before the ablation balloon is introduced. The system then delivers radiofrequency energy to the tissue circumferentially for 300milliseconds. A dose of 12J/cm2 has been shown to be effective in achieving depth penetration accurately above the muscularis mucosae thus limiting the complications involved with damaging deeper tissues (57). The close spacing of electrodes allows uniform penetration of the entire treated circumference and thus this technique can be used circumferentially with reports of stricture formation being minimal (58). This ability to control the depth of ablative penetration means that many other adverse side effects seen with alternative endoscopic techniques are greatly reduced. These include lower rates of chest pain, odynophagia, perforation and pneumothorax in comparison with laser and thermal ablation techniques.
One recent paper reviewed the progress of 142 patients with endoscopically identifiable Barrett’s oesophagus and high-grade dysplasia managed at 16 separate academic and community centres. These patients underwent a total of 229 radiofrequency ablations and were followed up with repeat endoscopy and systematic biopsy for a median length of 12 months. The only adverse event of note was a stricture noticed on endoscopy in an asymptomatic patient. At follow-up, biopsy specimens were negative for high-grade dysplasia in 90% of patients. 80% of patients had no dysplasia on biopsy and 54% of patients were negative for intestinal metaplasia (59). These results are very encouraging, particularly as high-grade dysplasia carries the greatest risk of malignant progression.
Other benefits include minimal post-procedure discomfort with patients able to go home within hours of the procedure. Regarding the issue of buried glands, a study following 102 patients post circumferential ablation showed no evidence of buried glands in 4306 biopsy samples taken over a year follow-up (60). This once again highlights the advantages of RFA in comparison to other endoscopic techniques.
Conclusion
The surveillance and treatment of Barrett’s Oesphagus remains an area of interest and controversy. This is heightened by the inability to discriminate those patients with BO which are most likely to progress to high grade dysplasia and then to adenocarcinoma of the oesophagus. This places greater emphasis on the endoscopic surveillance programme to identify this potentially pre-malignant state at an early stage. Future advances, particularly in endoscopic techniques, will help to increase efficacy of treatment and minimise complication rates. Further developments include progress in identification of genetic biomarkers which may help elucidate those patients at greatest risk. The management of Barrrett’s Oesophagus is becoming increasingly more important, particularly with the rise in incidence of oesophageal carcinomas in the Western world. The issues to address therefore include the identification and screening of at-risk groups and the further management from diagnosis of BO. Patients with chronic GORD symptoms are most in need of screening. Currently this should include the gold-standard four quadrant biopsy technique. This may include techniques to enhance visualisation as described above. In the authors opinion, non-biopsy screening does not carry enough evidence to support its use in replacement of biopsy as of yet. Medical treatment with PPI (if necessary in high-dose) as well as surgical treatment of GORD are essential considerations in the prevention and treatment of BO. Their use in combination with endoscopic therapy has proven benefits as outlined. Of the endoscopic therapies, the lack of complications combined with excellent post-procedure rates of disease elimination seen with RFA are most encouraging. Oesophagectomy should be reserved for those patients with disease not amenable to conservative or endoscopic therapy. Continual research is required to help us gain more understanding into the pathogenesis of this condition, enabling us to effectively target and manage BO appropriately.
“The mind is its own place, and in itself can make a heaven of hell, a hell of heaven” John Milton
The word 'psychiatry' is derived from the Greek for "doctor of the soul" and was first coined in the early 19th century by the German physician and anatomist, Johann Reil (1759-1813), although the treatment of mental disturbances dates back hundreds of years prior to this. The specialty of Psychiatry is regarded as dealing with the prevention, assessment, diagnosis, treatment, and rehabilitation of ‘mind’ illnesses or mental disorders. Diseases of the brain itself, for example encephalitis, tumours, and so forth, fall within the realm of neurology, generally. There are, of course, many overlapping disorders which cause neurological symptoms (paresis, slurred speech, ataxia, to cite a few) and ‘mind’ symptoms (depression, anxiety, psychosis). Disorders which affect several organ systems, for example, the autoimmune diseases, often cause multiple, bewildering neurological and mental symptoms. The primary goal of the psychiatrist is relief of suffering associated with ‘psychiatric’ disorders which include inappropriate anxiety, clinical depression, and psychotic disorders. Attempts have also been made to categorize and ‘treat’ different types of personality disorder. The latter is a contentious issue (perhaps with the exception of antisocial and borderline types) sometimes based on value judgments rather than clear scientific evidence. Treatment for mental health problems nowadays is usually community-orientated for less severe conditions and often hospital-based for more intractable disorders. The vast majority of patients are treated on a voluntary basis, whether in hospital or the community.
Medical, biological, social or psychological?
“ I think we ought always to entertain our opinions with some measure of doubt. I shouldn’t wish people to dogmatically believe any philosophy, not even mine.” Bertrand Russell
Psychiatry is sometimes criticized for adopting a ‘too’ medical or biological approach, despite the fact that many physical conditions masquerade initially with ‘mental’ symptoms. It would seem strange, if not irresponsible, were a psychiatrist, who is after all, a qualified medical doctor, not to enquire about a patient’s physical history. What is conveniently overlooked is that in everyday practice psychiatry uses a holistic approach to the patient, taking social and cultural backgrounds into account, as well as the general medical status. Treatment may thus involve medication, various forms of psychotherapy, or both, in addition to practical measures such as help with family problems, debts, housing, residential placements and so forth. In recent years, particularly in the UK, there has been a much greater emphasis on psychological treatments and social interventions. The ‘medical’ approach has taken a definitive back seat. Psychotropic drugs are frowned upon because of their side-effects, or perceived as a form of control used by psychiatrists towards their patients. Sweeping statements are made about their lack of efficacy and selective abstraction of the research is used to support such statements. Psychiatrists are denigrated for being in the grip of Big Pharma and are further demoralized by the being perceived as ‘drug pushers’. They are perceived by mostly non-medical ‘therapists’ as not being in touch with the psychological and sociological issues which are cited as underlying and perpetuating psychiatric disorders. Electroconvulsive therapy is considered barbaric; it is banned in some states in the USA. Complementary or ‘alternative’ therapies, regardless of whether or not they stand up to scientific scrutiny, are proliferating, and prescribed drugs are being replaced by ‘natural’ herbal products, despite the inherent dangers of the latter (1). Psychiatry is in decline and is becoming obsolete, a victim of its own psychobabble and increasingly mind-numbing research, understandable to the elite few. The profession is in danger of being ‘psychologised’ in order to appear acceptable and user-friendly, advocating therapies which in themselves do not stand up to scientific scrutiny. Outcome studies are quoted as favourable, when the very tenet of their foundations is very shaky, to say the least.
Perhaps there is not much reason for surprise when one considers not very long ago psychiatry advocated behaviour therapy for the treatment of homosexuality, orgone energy accumulators for neuroses, and insulin coma for schizophrenia. In hindsight such practices were totally unsound, unacceptable, and in the case of insulin coma therapy, dangerous; fortunately, they are now obsolete. Yet the history medicine is replete with such ‘cures’: mercury was once used to treat syphilis, and in surgery trepanation was widely used in ancient times for the treatment of seizures. In retrospect these procedures could be also be considered outrageous and barbaric, though with the development of scientific knowledge it is easy now to understand, reflect, and accept, that no other effective treatments were available at the time. Not so the case for psychiatry. Psychiatrists and other mental health professionals, who by and large genuinely have empathy and sympathy for their patients and want them to get better quickly, discharge them from hospital or outpatient clinics, and reunite them with their families whenever possible, are still unjustly accused of wanting to exert social control. There is no doubt that abuse of psychiatric practice does occur in some institutions and that political regimes throughout the world have used and still use powerful neurotropic drugs to subdue and control individuals who challenge the authority of the State. It is common knowledge that psychiatry was used by some totalitarian regimes as part of a system to enforce political control, for example in Nazi Germany, the Soviet Union, and the apartheid system in South Africa. Whether such abusive practices, which no doubt still exist, will ever be abolished will depend on the will of Governments and pressure from Human Rights campaigners such as Amnesty International.
What is madness?
“ Madness is rare in individuals - but in groups, parties, nations, and ages it is the rule” Friedrich Nietzche
It is not possible to delineate the boundary between sanity and insanity. Broad definitions of mental disorder have been attempted and an individual might be said to be ‘mentally disordered’, or as formerly described, ‘of unsound mind’, when there is a more than temporary impairment of cognitive functions such as memory, orientation and comprehension, an alteration of mood leading to a delusional appraisal of one’s situation, abnormal perceptions and disordered thinking. However, this concept is criticised for being overinclusive and precise definitions of mental illness remain elusive. It is probably easier to envisage mental health problems as being on a continuum from normal to abnormal for example, from a relative sense of well-being and contentment to a state of distress and unhappiness. Further exacerbations or stressors lead to a disintegration of oneself and that sense of oneness with the environment. Loss of reality ensues with further anxiety and perplexity, disordered and confused thinking or delusions, and perceptual disturbances (usually auditory hallucinations), in some cases. The same symptoms can be caused by drugs such as cocaine or amphetamines. It is known that these drugs alter the effects of dopamine, serotonin, noradrenaline, and perhaps other transmitters, leading to the assumption that anxiety, depression and psychoses are biologically driven, the often cited chemical imbalance approach. In the case of dopamine, implicating this neurotransmitter as a sole trigger factor in psychoses is simplistic and naïve. Likewise, depression and anxiety may have other biological causes such as hormone irregularities or fluctuating glucose levels. The dopamine hypothesis alone has largely been discredited in the aetiology of psychoses. Dopamine as an causative factor is only one small part of a much wider as yet unknown picture: for example, psychosis occurs in Parkinson’s disease where dopamine is actually deficient.
The ‘psychologised’ individual
‘Common sense is not so common’ Voltaire
One major criticism of psychiatry concerns the endless diagnostic categories or disorders which set out to describe and define the whole range of normal human expression, from the histrionic to the shy. No wonder then that psychiatry and allied specialties, for example, psychology and sociology, are accused of a sweeping disregard for the extraordinary complexity and richness of human behaviour. Whole subsets of psychiatric specialties have mushroomed over the last 30 or more years, to include substance misuse, forensic issues, autistic spectrum disorders and many others(2). Many disorders have variants, for example schizoaffective or schizomanic subtypes for schizophrenia, without any real scientific basis for such assertions. The eccentric individual becomes ‘schizotypal’; the individual who is detached from others and prefers his/her own company, is labelled ‘schizoid personality disorder’. Some would question whether many psychiatric descriptions are indeed ‘disorders’. There are very few ‘mental’ conditions which really could be regarded as disorders, save for example, severe clinical depression, bipolar disorder, obsessive compulsive states, and the psychoses, the latter often drug-induced. The diagnostic categories become bewildering and meaningless when subtypes are used, for example schizoaffective, bipolar I and bipolar II, depression with or without psychotic symptoms, and so forth; all have their supporters and detractors. Objectively, the symptoms are merely variations on a theme and cannot be accurately rated scientifically, unlike the gradings of say, Hodgkins or non-Hodgkins lymphoma. The distinction between normal and abnormal is blurred and varies among cultures. This is particularly pertinent when describing or defining personality disorder. For example, when does narcissistic behaviour become an illness? Why should it be seen as a disorder? Indeed, high self-esteem is encouraged in today’s’ climate and we are told to ‘love themselves more’. The usual response to the questioning of such behaviour is that it is ‘inappropriate’ or ‘out of proportion’ to the individual’s circumstances, or that ‘the patient is suffering’. Yet the entire media business, arts and entertainment, modelling and fashion industry is engaged in a narcissistic mind set, and the public love it! In other scenarios words are used interchangeably such that a psychopath, say, is perceived as a cold-blooded killer without conscience or feeling for his victim, or considered a creative genius, or indeed admired as a successful politician. The list of descriptions in the psychiatric disorders classification is wearisome and meaningless in many respects.
Much research in psychiatric journals nowadays is organic-based with ever intensive searches for newer receptors or transmitters, with increasing emphasis on the neurological basis for psychiatric conditions. In the past, emphasis was placed on the positive outcomes of drug trials, though this, fortunately, is now changing and reputable medical journals are now prepared to publish the results of negative findings. On the other hand, other researchers attempt to prove one type of psychotherapy is more effective than drug therapy, or that both together are better than either alone. Psychiatry has become polarized, with the ‘organic camp’ advocating a neurobiological basis and reductionist paradigm for psychiatric disorders, while the ‘psychotherapy model’ emphasizes the individual’s part in his/her illness with the development of strategies to defeat and overcome irrational beliefs and counterproductive emotions. There are problems with both approaches. A great deal of criticism is now being targeted against the psychology industry with its claims of treating serious illnesses through talking cures, and using labels to categorize almost every aspect of human behaviour (3). For example, how does one account for biological symptoms which are pervasive in severe depression without considering the role of neurotransmitters and regulatory hormones? How does one measure the complexity of suffering in any one individual and translate that into a rating scale for myriads of others whose problems have different origins? Are two people with severe depression really the same if they score identical marks on a depression scale? Whole books are written on the use of rating scales for research into psychological/psychiatric disorders. Yet there are over 250 different psychotherapy treatment approaches, which inevitably leads one to question the overall value of psychotherapy (4). In Epstein’s view, the whole field of psychotherapy is ‘pseudoscientific, an elaborate mysticism only differentiated from religion by a seemingly modern orientation and the cant of science (5). Research in psychotherapy is in any event notoriously difficult because of sample sizes, control groups, placebo effects and the nature of the therapeutic intervention itself (cognitive therapy, family therapy, psychoanalytic therapy). Besides, even when some patients show a moderate improvement, nonspecific factors are always operating in the period between therapy sessions and follow-up. Patients may have had a better social adjustment because of a new job, an increase in salary, or a change in a relationship and so forth, while others may have had a general decrease in life stresses, for example, through improved physical health (recovery from surgery, better control of diabetes). Some patients will deteriorate, despite ‘cognitive restructuring’, because of redundancy from a job, or ending of a relationship and so forth.
What next?
“Just trust yourself and you’ll learn the art of living” Goethe
Although many of the psychological treatments available nowadays were initially propounded by psychiatrists, psychotherapy and behavioural management are now more often carried out by psychologists, nurse practitioners and counsellors. Psychiatrists tend to deal with more severely affected individuals, ironically, those deemed to need psychotropic medication or where ‘counselling’ has failed. It could be argued that talking to a stranger for a fixed number of sessions (ranging from 10–12 one-hour slots) actually impedes the normal process of recovery and that a patient would benefit more from using his/her own social networks including family, friends, general practitioner and others, who are better placed to view the patient’s problems in context. Research claiming that depressed people are most likely to benefit from cognitive therapy, or that the majority of people suffering from panic attacks will recover with anxiety management, is deceptive and naively optimistic. Too many nonspecific factors are at play. The notion that a psychologist/counsellor/psychiatrist could turn a patient’s life around in 10 hours or so (10 sessions) is difficult to sustain when such problems have accumulated over that person’s lifetime, no matter how long or short-lived. The human mind is too complex and the human condition too intricate to be hoodwinked into such quick-fix solutions. Perhaps the best way forward is, ironically, to revert to an holistic approach with better education and training of both psychiatrists and psychologists. The former need further training in neurology (they already receive extensive training in psychology) and time spent in GP surgeries, the latter should be required to gain more experience of patients with severe types of psychiatric disorders (many hospital-affiliated psychologists already do), and general exposure to medicine via an acute emergency department or at a GP surgery (say, one year in total), preferably both, in order to broaden their horizons. The author appreciates the inherent, perhaps, unfortunately, insurmountable difficulties in setting up such a system involving the various disciplines. All ‘therapists’ should have a grounding in philosophy and sociology. It needs to be made clear that many patients simply feel better by talking to someone, though this ‘feeling better’ is not often sustained, and that knowing the cause of one’s problems does not equate with ‘cure’. Many patients have intractable conditions which are not amenable to ‘talking therapies’, and such individuals do not fit the category of the ‘worried well’, the usual ‘clients’ of counsellors and other therapists.
Chlamydia Screening In General Practice
Sexually transmitted infections are reaching epidemic proportions in Britain and Chlamydia is the commonest sexually transmitted bacterial infections.
Prevalence
Chlamydia is thought to be prevalent in 5-10% of 20-24 years old. About 75% of women and 50% of men are asymptomatic. The National Chlamydia Screening Programme currently finds about 8% of young people tested to be positive 1 but this may represent selective testing of higher risk individual.
National Chlamydia Screening Programme (NCSP)
This was initiated in 2003.The aims & objectives were early detection and treatment of asymptomatic infection, to reduce the onward transmission and to prevent the development of sequelae by screening all sexually active under the age of 25 years annually or with each change of sexual partner.
The positive rate for this group in 2008 was 8.7% 1.
An ideal setting to provide screening is General Practice. The nationally agreed target is for 25% of 15-25 years olds-males and females to be screened by 2009/2010 and 35% by 2010/2011.
Pathogenesis
Chlamydia is an intracellular bacteria and causes disease by chronic inflammation which is exacerbated by re-infection. It infects the female & male genital tract and is primarily sexually acquired. It can be carried in the throat, thus oral sex can transmit the bacteria.
Symptoms
Over 70% of women and 50% of men are asymptomatic.
Women may experience:
• post coital or inter- menstrual bleeding
• pelvic pain
• dysuria
• increased vaginal discharge
• P.I.D with infertility (10-40% incidence)
Men may experience:
• urethral discharge
• dysuria
• epididymo- orchitis
• urinary frequency
Symptoms in both men and women:
• rectal discharge
• rectal bleed following rectal infection
• pharyngeal infection - rare.
History
Early diagnosis and treatment will reduce the risk of long term complications. A detailed history of following should be taken-
1) History of discharge-Enquire about:
• colour & consistency of the discharge
• odour
• is it aggravated by sexual intercourse
• any associated itching
• when was it first noticed
• any past history of the discharge
• was it diagnosed and treated earlier
• any association of the discharge with menstrual cycle
2) Sexual history:
• date of last sexual intercourse
• were condoms used
• and if so were they used consistently
• regular partner or not
• any other partners in the last six months
• has she or her partner had sex with some one else of the same sex
• any history of sex with a partner from a different country
• any drug abuse in either the woman or her partner
3) Contraception and cytology:
• which contraception does she use
• any recent change of contraception
• whether she is up to date with cervical cytology
• whether all previous screens have been normal
4) Menstrual history:
• date of LMP
• are periods regular or have they altered recently
• any bleeding in between periods or after intercourse
5) History of sexually transmitted infection:
• any past history of STI
• was it treated
• was the partner also treated
• did they have a test of cure
6) Others symptoms:
• ower abdominal pain
• dysparunia
• dysuria
• any soreness or warts.
7) History of treatment:
• any medication been prescribed.
• any usage of over the counter medications
Examination
Examination of the female patient is usually normal but may show some muco -purulent discharge with contact bleeding. If pelvic inflammation is present there will be tenderness on uterine and adnexal bimanual palpation. The patient may sometimes be unwell with temperature. In suspected rectal chlamydia, Proctoscopy may be normal or may show changes of bloody/muco-purulent discharge or ulceration of mucosa.In men with epididymo-orchitis there may be epididymal and testicular tenderness with or with out systemic features.
Investigations
• The older less sensitive (EIAs) Enzyme immunoassays are replaced by Nucleic acid amplification tests (NAATs) .They are based on polymerase chain reaction technology.
• In some areas a combined NATT is in use for diagnosis of both Chlamydia & gonorrhoea. NATTs are not licensed for rectal or pharyngeal sampling.
• Men should have a first void urine sample tested. In symptomatic women an endocervical swab is the sample of choice. If the patient does not require a per speculum examination a blind vulvovaginal swab could be an appropriate sample. These are almost as accurate and have become the basis for self test kits, now available widely.
• A first catch urine (FCU) sample may be taken for women (having not passed urine for at least one hour before) but this is less sensitive in women than in men2
• Sexually transmitted infection screen should include serological testing for HIV and syphilis. Current guidelines for HIV testing can be found at www.bashh.org.
Prevention
No opportunity should be lost to discuss safe sex with young people at the time of new patient check up and when prescribing contraception. It is a good practice to screen Chlamydia with informed consent when performing cervical screening in sexually active women under 25 and those over 25 with two or more partners in the last year or a change of partner in the past year.
Management
• It is appropriate to treat Chlamydia in a general practice setting. Treatment is with either macrolides or tetracyclines.
• Oral Azithromycin (Zithromax) 1gm stat should be the first choice as it avoids compliance issues. Patients must be advised to avoid sex for 7 days after the treatment. An alternative is oral Doxycycline (Vibramycin) 100 mg twice daily for 7 days or oral Erythromycin (Erymax) 500 mg twice daily for 14 days.
• Interaction with oral contraceptive pill should be discussed. In pregnant women or those at risk of pregnancy, Azithromycin is still an option.
• Retesting to verify cure is not advocated, partly because of the high cure rate and partly the test using NAA may remain positive for up to five weeks causing confusion.
• All at risk partners in the last six months for females and asymptomatic males or four weeks for symptomatic males should be informed. They should be invited and treated even if the test is negative 3.The discussion and treatment can take place by the GP if the patient is registered with the practice or by referral to local genitourinary clinic.
Locally Enhanced Service
Each primary care trust has a Chlamydia screening officer. This year the target from the Department of Health is to screen 25% of patients aged 16 to 25 years registered at the practice who are sexually active.
Fee Structure
On agreeing a service plan with the PCT the general practice can receive: ( this may vary from one PCT to another PCT)
• £4.50 per test received in the laboratory for coverage of ≤ 10% of the practice population aged 15-24 years.
• £5.00 per test received in the laboratory for coverage of 10% to ≤20% of the practice population aged 15-24 years.
• £6.50 per test received in the laboratory for coverage of 20% to ≤25% of the practice population aged 15-24 years.
• £8.00 per test received in the laboratory for coverage of over 25% of the practice population aged 15-24 years.
How To Achieve Targets
• Do a computer search of all the target patients.
• Have a practice meeting
• Involve the whole team: practice nurses, health care assistants and receptionists
• Delegate, delegate and delegate! Practice nurses or health care assistants can screen at risk groups
• “new patient health check” is an ideal opportunity to offer screening. Involve the receptionist to hand out leaflets, forms and urine pots
• Make sure the reception area is suitable for handing out these items otherwise use a side room to ensure privacy
• Decide who would be dealing with positive results, treatment and partner notification
• To earn the money for extra effort you and your staff has made, make sure you use the appropriate read codeand ask the practice manager to send the claims monthly
• Remember only patients tested with in the practice premises are included when calculating the percentage screened
• Make sure you reward your staff appropriately with the money otherwise their enthusiasm may soon vanish
Contrary to the period in 1993, when the United States (US) President Bill Clinton failed to gain any traction on his healthcare reform, the current President, Barack H Obama, has been able to embark on historic healthcare reform. This is because major stakeholders agree that US healthcare is in crisis and requires major reform. Businesses and consumer groups have joined the insurance industry, pharmaceutical industry, and physician groups in asking for this healthcare reform that would blunt the rapidly escalating costs and provide healthcare for all Americans. While the number of uninsured Americans increased from 39.8 million in 2001 to 46.3 million in 2008, the National Health Expenditure (NHE) grew from 7.2% of the gross domestic product (GDP) in 1970 to 16% in 2005 1. This growth is projected to climb further to 19.5% in 2016. To put these figures into perspective, the US is projected to spend almost $13 trillion on healthcare over the ten years from 2010 to 2019 if the current trend continues2. Add to that the number of bankruptcies filed in the US due to healthcare expenses. Himmelstein and colleagues have recently demonstrated that of all the bankruptcies filed in the US in 2007, 62.1% were due to medical reasons as opposed to 46.2% in 2001 and only 8% in 19813 .
Hence, there is no longer any debate about ‘whether there is a problem’ but rather ‘what can be done to fix this problem’. How to fix it has been, and will continue to be, a highly contentious issue that will pitch Democrats against Republicans even after the passage of the pending legislation. Some of the key elements President Obama had identified as his basic objectives in healthcare legislation, that he is expected to sign into law by the end of 2009, include:
Providing universal coverage to all Americans and requiring employers to provide health insurance to their employees.
Barring insurance companies from providing policies that would exclude patients with ‘pre-existing conditions’ thereby ensuring uniform health insurance premiums for all Americans irrespective of their health status.
Providing a one-stop marketplace for national health insurance exchange to allow consumers to compare and shop for different insurance plans.
Promoting the use of electronic medical records and the practice of evidence-based medicine.
Introducing a government-run health insurance option providing low cost, affordable health insurance that would directly compete with the private insurance industry.
This last provision, often called the ‘Public Option’, has been regarded by its opponents as an indication of how the federal government would grab political power and control the lives of all Americans. Some have gone as far as to say that the Administration is trying to introduce a ‘socialist system’ and set up ‘death panels’ to decide the fate of terminally ill Americans.
The raging debate in both Houses of Congress (House of Representatives and US Senate), since the introduction of the legislation early this year, has been highly partisan and, at times, acrimonious. The primary debate will continue to target accessibility and the ‘Public Option’ on one hand and affordability and deficit reduction on the other. Additionally, fundamental ideological issues of the rights of women to their health (read right for abortion) and accusations of ‘socialist medicine’ (read demand for free market healthcare with little or no government oversight) will continue to fuel this debate well after the legislation has been enacted into law. At the time of writing it is clear that President Obama’s deadline of this year will not be met.
On 7th November 2009, President Obama won a major battle in this war when the House of Representatives passed the ‘Affordable Healthcare for America Act’. The vote was 220-215 and essentially along party lines with the Democrats and only one Republican voting for this legislation. According to Representative John Dingle, the 83-year-old Michigan lawmaker who had introduced national health insurance in every congress since 1955, this 1990-page bill provides coverage for ‘96% of Americans and offers everyone, regardless of health or income, the peace of mind that comes from knowing that they will have access to affordable healthcare when they need it’. However, in the run-up to the final vote, conservatives from both political parties joined hands to impose tough restrictions on abortion coverage that will continue to be a divisive issue throughout the legislative process 4 .
President Obama won the second major victory on 21st November 2009 when the Democrats (with the help of two independents) in the US Senate pushed the legislation past a key hurdle, despite vocal Republican opposition, with 60-39 votes. Sixty votes are needed in the US Senate to prevent ‘filibuster’ or an indefinite discussion on any bill 5 . With this vote the bill will now be debated in the Senate. Table 1 highlights some of the important features of the two bills:
Table 1: Important features of the Senate Bill and House Bill.
Senate Bill
House Bill
Cost*
$848 billion
$1.02 trillion
Projected deficit savings*
$127 billion
$104 billion
New patients*
31 million
36 million
Protection against generic drugs**
12 years
12 years
Government sponsored program
New plan to compete with private plans; government to negotiate payment rates.
New public plan through insurance exchanges; government to negotiate payment rates.
Projected reduction in Medicare growth***
$400 billion
$400 billion
How is it paid for?
Fees on insurance companies, pharmaceutical and medical devices industries. A new payroll tax and 5% tax on elective cosmetic surgery.
$460 billion over the next decade from income tax on individuals making over $500,000 and couples making over $1 million per year.
* These are the estimates for the 10-year-period (2009-2019) from the Congressional Budget Office 6 .
** Both bills would protect biological drugs (made from living organisms rather than chemical
compounds) from competition from generic drugs.
*** The reduction in Medicare spending is non-binding and future Congress can restore these cuts.
In this national debate, two well-known medical centres in the US, the Mayo Clinic of Minnesota and the Cleveland Clinic in Ohio, have frequently been cited as examples that could perhaps be emulated to deliver quality care in an efficient and cost-effective fashion. Both centres practise a ‘medical home’ concept based on a coordinated team approach that was introduced by the American Academy of Paediatrics in 1967. This has been further refined into the ‘patient-centred medical home’ by the American College of Physicians (ACP), American Academy of Family Physicians, and the American Academy of Paediatrics in 2007. This concept is exceedingly important for the management of chronic illnesses because the cost associated with unmanaged chronic conditions is astronomically high. It is estimated that 45% of the US population has a chronic medical condition. Amongst Medicare recipients aged 65 and above, 83% have at least one chronic health problem and almost 25% have at least five co-morbidities. Whereas the current system rewards acute care, it generally does not reimburse preventative care, chronic care management or active integrated inter-specialty management 7. A medical home provides expanded primary care that is personalized, focuses on prevention, actively involves patients in making decisions about their care and helps coordinates all of their care.
One of the deficiencies of the proposed reform is the absence of any tort reform. For physicians in the US the threat of a malpractice lawsuit is real. Without legislative relief, ‘defensive medicine’ will take a significant chunk out of healthcare dollars. Estimates suggest that savings accrued from such legislation could account for 20-25% of the NHE and may be prudently used to reduce the healthcare costs. President Obama’s outright rejection to consider tort reform in his address to the American Medical Association in June is very unfortunate and runs counter to his passionate plea to help reduce medical waste. Some of the important discussions that will take place relate to the need to revamp the physician reimbursement schedules and empower the Medicare Payment Advisory Commission to enhance primary care reimbursement, establish incentives to implement health information technology (including electronic medical records), and mandate the use of evidence based medicine and established protocols to stem the tide of escalating costs with ‘pay for performance’ and other quality measurements 8.
Healthcare reform must also address the physician shortage issue. Several studies, including those from the Institute of Medicine and the American Association of Medical Colleges (AAMC), have indicated a growing physician shortage particularly in Primary Care. In order to address this rising tide of physician shortages the Balanced Budget Act of 1996, that froze the number of reimbursable training positions at the 1996 level, needs to be revisited. As a preliminary target ACP and AAMC have recommended that the availability of Medicare-funded training positions in adult primary care specialties be increased by 3000 each year for the next 15 years 9-11.
From here on I suspect a bruising legislative debate (and drama) will continue with passion and, undoubtedly, some acrimony. Since mid-term elections are coming up in 2010, both the parties are jockeying their position as best as they can. To end the ‘filibuster’ the Democrats will need, yet again, 60 votes to pass the bill in the Senate. However that is not guaranteed at this time since many Democratic senators continue to have concerns and Republicans have made it clear that they will do whatever they can to derail this initiative. Hence further deliberation, particularly in the Senate, will entail significant manoeuvring and arm-twisting, passionate appealing, horse-trading, and perhaps additional funding for select senators to achieve 60 votes. However, in the end there will be a bill from the Senate, perhaps in mid to late January 2010. Subsequently, a conference committee will hammer out the differences in the two bills that can be presented to both houses for final passage and submitted to the President for signature. I believe the President will have the bill on his desk for signature at the end of January or early February 2010.




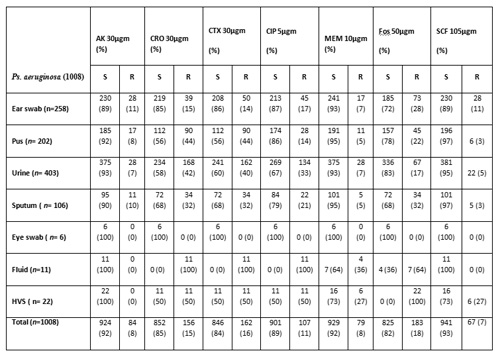

 Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair.
Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair. Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2)
Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2) 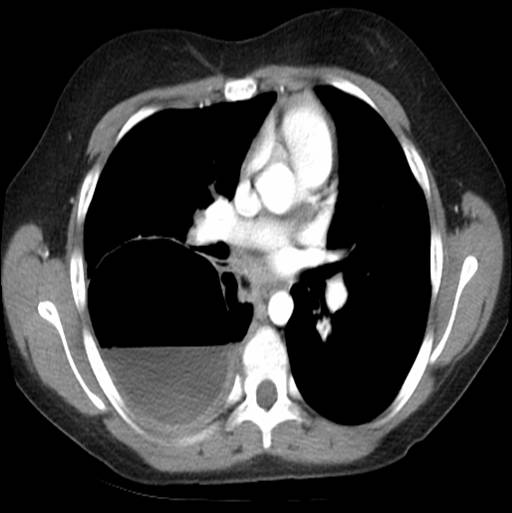 Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4)
Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4)  Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid.
Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid.  Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung.
Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung.  Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
 Figure 1, illustrates a distribution of the peak work-load period which occurred between 9pm-11pm and 1am-3am. This finding contradicts previous surveys done prior to the implementation of the hospital at night where it was noted that the nights were quieter and sub-specialist such as orthopaedic surgeons were not working as hard as general medics (1).
Figure 1, illustrates a distribution of the peak work-load period which occurred between 9pm-11pm and 1am-3am. This finding contradicts previous surveys done prior to the implementation of the hospital at night where it was noted that the nights were quieter and sub-specialist such as orthopaedic surgeons were not working as hard as general medics (1).  Figure 2, shows the overall experience of the hand-over as judged by the orthopaedic juniors. There was an eighty-five percent (43/51) attendance by the on-call orthopaedic juniors of which seventy-two percent (32/44) thought that it was a useful experience
Figure 2, shows the overall experience of the hand-over as judged by the orthopaedic juniors. There was an eighty-five percent (43/51) attendance by the on-call orthopaedic juniors of which seventy-two percent (32/44) thought that it was a useful experience 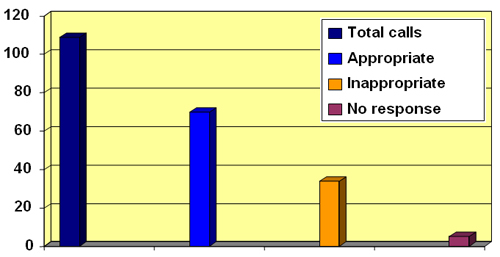 Figure 3 illustrates a distribution of the calls received. As illustrated, 37/109 calls were viewed as inappropriate The majority of the orthopaedic juniors surveyed framed hospital-at-night hand-over was useful but thirty-four percent (37/109) of the calls they received were viewed as inappropriate (Fig 2,3). The most frequent of the inappropriate ward calls were ‘requests to rewrite drug-charts’ (Fig 4,5).
Figure 3 illustrates a distribution of the calls received. As illustrated, 37/109 calls were viewed as inappropriate The majority of the orthopaedic juniors surveyed framed hospital-at-night hand-over was useful but thirty-four percent (37/109) of the calls they received were viewed as inappropriate (Fig 2,3). The most frequent of the inappropriate ward calls were ‘requests to rewrite drug-charts’ (Fig 4,5). 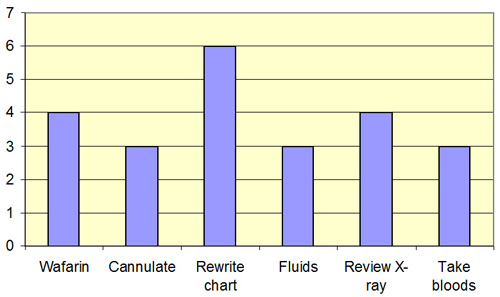 Figure 4 describes the frequencies of these calls. As illustrated the most frequently inappropriate ward-call was to ‘rewrite drug-charts’. There were twenty-three (23/37) inappropriate ward-calls
Figure 4 describes the frequencies of these calls. As illustrated the most frequently inappropriate ward-call was to ‘rewrite drug-charts’. There were twenty-three (23/37) inappropriate ward-calls 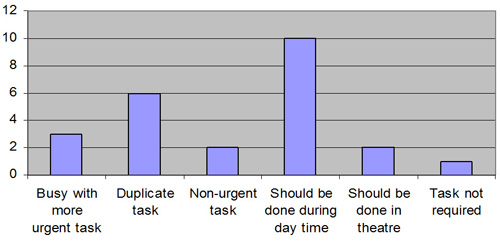 Figure 5 shows the reasons given by the on-call doctors for the inappropriate tasks. The most frequently given reason was that ‘the request should have been done during the day’. The second most frequently given reason for inappropriate calls was the fact that ‘it was a duplicated request’ Our survey also highlighted that the most frequently given reason for inappropriate tasks was firstly that the request should have been done during the day and secondly that it was a duplicated request. These findings seem to defeat the key purpose of the hospital-at-night project for an orthopaedic SHO on-call. Conclusion: Hospital at night cannot function in isolation. There are fewer doctors available then normally and the system has to use their time effectively. 30% of inappropriate calls to wards were to rewrite drug charts and to prescribe warfarin. This should have been identified and performed by the day staff. 10% of calls were to review X-rays. Much of the inappropriate activity could be pre-empted if both day and night staff attended the handover and the tasks outstanding from the day identified. The doctor on the night could then perform an hourly ward round completing these tasks without interrupting at the beginning of the night.
Figure 5 shows the reasons given by the on-call doctors for the inappropriate tasks. The most frequently given reason was that ‘the request should have been done during the day’. The second most frequently given reason for inappropriate calls was the fact that ‘it was a duplicated request’ Our survey also highlighted that the most frequently given reason for inappropriate tasks was firstly that the request should have been done during the day and secondly that it was a duplicated request. These findings seem to defeat the key purpose of the hospital-at-night project for an orthopaedic SHO on-call. Conclusion: Hospital at night cannot function in isolation. There are fewer doctors available then normally and the system has to use their time effectively. 30% of inappropriate calls to wards were to rewrite drug charts and to prescribe warfarin. This should have been identified and performed by the day staff. 10% of calls were to review X-rays. Much of the inappropriate activity could be pre-empted if both day and night staff attended the handover and the tasks outstanding from the day identified. The doctor on the night could then perform an hourly ward round completing these tasks without interrupting at the beginning of the night.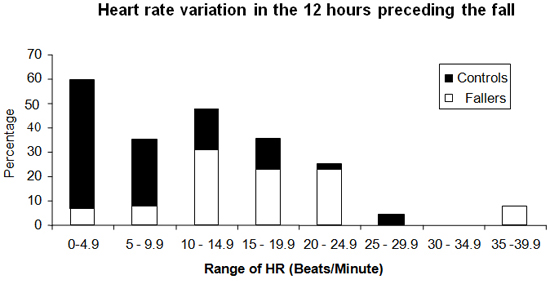
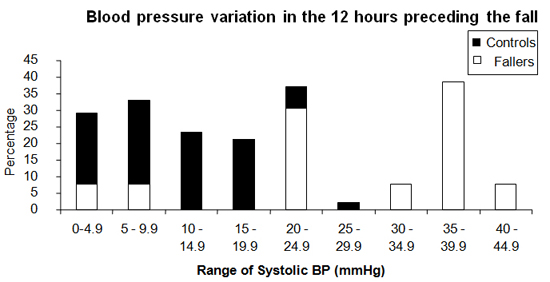
BJMP Dec 2009 Volume 2 Number 4
Welcome to this issue of the BJMP