Hepatitis B (HB) is a major disease and is a serious global public health problem. About 2 billion people (latest figures so far by WHO) are infected with the hepatitis B virus (HBV) all over the world. Interestingly, rates of new infection and acute disease are highest among adults, but chronic infection is more likely to occur in persons infected as infants or young children, which leads to cirrhosis and hepatocellular carcinoma in later life. More than 350 million persons are reported to have chronic infection globally at present1,2. These chronically infected people are at high risk of death from cirrhosis and liver cancer. This virus kills about 1 million persons each year. For a newborn infant whose mother is positive for both HB surface antigen (HBsAg) and HB e antigen (HBeAg), the risk of chronic HB Virus (HBV) infection is 70% - 90% by the age of 6 months in the absence of post-exposure immunoprophylaxis3.
HB vaccination is the only effective measure to prevent HBV infection and its consequences. Since its introduction in 1982, recommendations for HB vaccination have evolved into a comprehensive strategy to eliminate HBV transmission globally4. In the United States during 1990–2004, the overall incidence of reported acute HB declined by 75%, from 8.5 to 2.1 per 100,000 population. The most dramatic decline occurred in children and adolescents. Incidence among children aged <12 years and adolescents aged 12-19 years declined by 94% from 1.1 to 0.36 and 6.1 to 2.8 per 100,000 population, respectively2,5.
Population of countries with intermediate and high endemicity rates are at high risk of acquiring HB infection. Pakistan lies in an intermediate endemic region with a prevalence of 3-4% in the general population6. WHO has included the HB vaccine in the Expanded Programme on Immunisation (EPI) globally since 1997. Pakistan included the HB vaccination in the EPI in 2004. Primary vaccination consists of 3 intramuscular doses of the HB vaccine. Studies show seroprotection rates of 95% with standard immunisation schedule at 0, 1 and 6 months using a single antigen HB vaccine among infants and children7,8. Almost similar results have been reported with immunisation schedules giving HB injections (either single antigen or in combination vaccines) at 6, 10 and 14 weeks along with other vaccines in the EPI schedule. But various factors like age, gender, genetic and socioenvironmetal influences, are likely to affect seroprotection rates9.So there is need to know actual seroprotection rates in our population where different vaccines, EPI procured and privately procured incorporated in different schedules are used. This study has been conducted to know the real status of seroprotection against HB in our children. Results will help in future policy-making, highlighting our shortcomings, comparing our programme with international standards and moreover augment future confidence in vaccination programmes.
Materials And Methods
This study was conducted at vaccinations centres and paediatrics OPDs (Outpatient Departments) of CMH and MH, Rawalpindi, Pakistan. Children reporting for measles vaccination at vaccination centres at 9 months of age were included. Their vaccination cards were examined and ensured that they had received 3 doses of HB vaccine according to the EPI schedule, duly endorsed in their cards. They included mainly children of soldiers but some civilians also who were invited for EPI vaccination at the MH vaccination centre. Children of officers were similarly included from the CMH vaccination centre and vaccination record was ensured by examining their vaccination cards. Some civilians who received private HB vaccination were included from paediatric OPDs . Some children beyond 9 months and less than 2 years of age who reported for non-febrile minor illnesses in the paediatric OPD at CMH and MH, were also included and their vaccination status was confirmed by examining their vaccination cards.
Inclusion Criteria
1) Male and female children >9 months and <2 years of age.
2) Children who had received 3 doses of HBV according to the EPI schedule at 6,10 and 14 weeks.
3) Children who had a complete record of vaccination- duly endorsed in vaccination cards.
4) Childen who did not have history of any chronic illness.
Exclusion Criteria
1) Children who did not have proper vaccination records endorsed in their vaccination cards.
2) Interval between last dose of HBV and sampling was <1 month.
3) Children suffering from acute illness at time of sampling.
4) Children suffering from chronic illness or on immunosuppressive drugs.
Informed consent for blood sample collection was obtained from the parents or guardians. The study and the informed consent form was approved by the institutional ethical review board. Participants were informed about results of HBs antibody screening. After proper antiseptic measures, blood samples (3.5 ml) were obtained by venepuncture. Autodisabled syringes were used. Collected blood samples were taken in vaccutainers and labelled by identification number and name of child. Samples were immediately transported to the Biochemistery Department of Army Medical College. Samples were kept upright for half an hour and then centrifuged for 10 minutes. Supernatant serum was separated and stored at -20 0C in 1.5 ml eppendorf tubes till the test was performed. Samples were tested using ELISA (DiaSorin S.p.A Italy kit) for detection of anti-HBs antibodies according to manufacturers’ instructions. The diagnostic specificity of this kit is 98.21% (95% confidence interval 97.07-99.00%) and diagnostic sensitivity is 99.11% (95% confidence interval 98.18-99.64%) as claimed by the manufacturer. Anti-HBs antibody enumeration was done after all 3 doses of vaccination (at least 1 month after the last dose was received).
As per WHO standards, anti-HBs antibody titres of >10 IU/L is taken as protective and samples showing antibody titres <10 IU/L were considered as non-protected. Samples having antibody titres >10 IU/L were taken as seroprotected against HB infection. All relevant information was entered in a predesigned data sheet and used accordingly at the time of analysis. Items entered included age, gender, place of vaccination, type of vaccination (private or government procured), number of doses and entitlement status (dependent of military personnel or civilian). The study was conducted from 1st January 2010 to 31st Dec 2010.
Statistical Analysis
Data was analysed using SPSS version 15. Descriptive statistics were used to describe the data, i.e. mean and standard deviation (SD) for quantitative variables, while frequency and percentages were used for qualitative. Quantitative variables were compared through independent samples’ t-test and qualitative variables were compared through the chi-square test between both the groups. A P-value <0.05 was considered as significant.
The mean age of the children was 13.7 months. The overall frequency of children with titres <10 IU/L was 61 (31.4%) while frequency of children with titres >10 IU/L was 133 (68.6%).
Geometric mean titres (GMT) were 85.81 for the seroprotected (>10 IU/L) category.
Results
One hundred and ninety-four children, who had received HB vaccination according to EPI schedule, were tested for anti-HBs titres. Out of them 61 (31.4%) had anti-HBs titres less than 10 IU/L (non-protective level) while 133 (68.6%) had anti-HBs titres above 10 IU/L (protective level) as shown in Figure 1. The GMT of anti-HBs among the individuals having protective levels (> 10 IU/L) was found to be 85.81 IU/L.
Figure 1
Figure 2
Figure 2 shows that anti-HBs titres between 10–100 IU/L was found in 75 (50.4%) children. Twenty-six (19.5%) individuals had titres between 100–200 IU/L. Twenty (14%) children had titres between 20–500 IU/L, 10 (7%) children had titres between 500–1000 IU/L and only 2 (1.5%) children had anti-HBs titres > 1000 IU/L.
One hundred and eighty-four children received vaccination supplied by government sources (Quinevaxem by Novartis) out of which 61 (33.1%) children had anti-HBs titres <10 IU/L (non- protective) and 123 (66.9%) had anti-HBs titres >10 IU/L (protective level). Only 10 children had received vaccination obtained from a private source (Infanrix Hexa by GSK), out of which all 10 (100%) had anti-HBs titres >10 IU/L (protective level). Comparison between the two groups revealed the difference to be significant (P value= 0.028).
One hundred and thirty-two children received vaccination from army health facilities (CMH and MH) out of which 36 (27.3%) had anti-HBs titres < 10 IU/L while 96 (72.7%) had anti-HBs titres >10 IU/L. Sixty-two children were vaccinated at civilian health facilities (health centres or vaccination teams visiting homes). Out of them 25 (40.3%) had anti-HBs titres <10 IU/L while 37 (59.7%) had anti- HBs titres >10 IU/L. The difference was insignificant (P value= 0.068). Gender analysis revealed that in the study group 129 (68.5%) were male children. Out of them 34 (26.4%) had anti-HBs titres <10 IU/L and 95 (73.6%) had anti-HBs titres >10 IU/L. Sixty-five (31.5%) were female children and out of them 27 (41.5%) had anti-HBs titres <10 IU/L while 38 (58.5%) had anti-HBs titres > 10 IU/L. Statistical analysis revealed the difference between males and females was significant (P value= 0.032).
One hundred and twenty-two (62.9%) children were less than 1 year of age. Out of them 37 (30.3%) had anti-HBs titres <10 IU/L and 85 (69.7%) had anti- HBs titres >10 IU/L. Seventy-two (37.1%) children ranged between 1 to 2 years of age. Out of them 24 (33.3%) had anti-HBs titres <10 IU/L while 48 (66.7%) had anti-HBs titres >10 IU/L. On comparison the difference between the two groups was insignificant (P value= 0.663), as shown in Table 1.
Patient characteristics
Anti-HBs titres (< 10 IU/L) (n = 61)
Anti-HBs titres (> 10 IU/L) (n = 133)
P – values
Age groups
0.63 NS
< 1year (n = 122)
37 (30.0%)
85 (69.7%)
> 1year (n = 72)
24 (33.3%)
48 (66.7%)
Gender
0.032
Male (n = 129)
34 (26.4%)
95 (73.6%)
Female (n = 65)
27 (41.5%)
38 (58.5%)
Hospital
0.068 NS
Army (n = 132)
36 (27.3%)
96 (72.7%)
Civilian (n = 62)
25 (40.3%)
37 (59.7%)
Vaccine Type
0.028
Government (n = 184)
61 (33.2%)
123 (66.8%)
Private ( n = 10)
0 (0%)
10 (100%)
Table 1 (NS = Insignificant; * = Significant )
Discussion
HB is a global health problem with variable prevalence in different parts of the world1. Various studies carried out in different parts of Pakistan in different groups of population have shown diverse figures regarding prevalence of HB. However, a figure of 3-4% is accepted as general consensus by and large, thus making Pakistan an area of intermediate endemicity for HB6. Yet when we extrapolate these figures to our population, it is estimated that Pakistan hosts about seven million carriers of HB which is about 5% of the worldwide 350 million carriers of HB10,11.
Age at the time of infection plays the most important role in acquisition of acute or chronic HBV disease. HBV infection acquired in infancy is responsible for a very high risk of chronic liver disease due to HBV in later life12. HB is a preventable disease and fortunately vaccination at birth and during infancy can eradicate the disease globally, if vaccination strategy is effectively implemented13. This can be claimed as the first anti-cancer vaccine which prevents hepatocellular carcinoma in later life.
In Pakistan, the HB vaccine was included in the EPI in 2004, given along with DPT (Diphtheria, Pertussis, Tetanus) at 6, 10 and 14 weeks of age. The vaccine is provided through government health infrastructure to health facilities. Private HB vaccines supplied as a single antigen or in combination vaccines are also available in the market. The efficacy of these recombinant vaccines is claimed to be more than 95% among children and 90% among normal healthy adults14. The immunity of the HB vaccination is directly measured by development of anti-HBs antibodies more than 10 IU/L, which is considered as a protective level15. However, it is estimated that 5–15 % of vaccine recipients may not develop this protective level and remain non-responders due to undermentioned reasons.16 Published studies regarding antibody development in relation to various factors in terms of immunogenicity and seroprotection, show highly varied results. Multiple factors like dose, dosing schedules, sex, storage, site and route of administration, obesity, genetic factors, diabetes mellitus and immunosupression, affect HB antibodies development response17.
Although the HB vaccine was included in the EPI in 2004 in Pakistan, until now no published data showing seroconversion and seroprotection among vaccine recipients of this programme is available on a national level to our knowledge. Our study has revealed that out of 194 children, only 133 (68.6%) had anti-HBs titres in the protective range (>10 IU/L) while 61 (31.4%) did not develop seroprotection. These results are low as compared to other international studies. A study from Bangladesh among EPI vaccinated children shows a seroprotection rate of 92.2%13 while studies from Brazil18 and South Africa19 have separately reported seroprotection rates of 90.0% and 86.6%, respectively. Studies from Pakistan carried out in adults also show seroprotection rates (anti-HBe titres >10 IU/L) of more than 95% in Karachi University students14 and 86% in health care workers of Agha Khan University Hospital20, respectively. However, in these studies the dosing schedule was 0, 1 and 6 months, and participants were adults. These results are consistent with international reports.
The gravity of low seroprotection after HB vaccination is further aggravated when we extrapolate these figures to our overall low vaccination coverage rates of 37.6% to 45% as shown in studies at Peshawar and Karachi respectively21,22. One can imagine a significantly high percentage of individuals vulnerable to HBV infection even after receiving HB vaccine in an extensive national EPI programme. Therefore, a large population still remains exposed to risk of HBV infection, and national and global eradication of HBV infection will remain a dream. Failure of seroprotection after receiving the HBV vaccination in the EPI will also be responsible for projecting a sense of false protection among vaccine recipients.
Dosing schedule is an important factor in the development of an antibody response and titre levels. According to the Advisory Committee on Immunization Practices (ACIP) of America, there should be a minimum gap of 8 weeks between the second and third doses and at least 16 weeks between the first and third doses of the HB vaccination23. To minimize frequent visits and improve compliance, the dosing schedule has been negotiated in the EPI to 6, 10 and 14 weeks24. Although some studies have shown this schedule to be effective, the GMT of anti-HBs antibodies achieved was lower than that achieved by the standard WHO schedule25. This may be one explanation of lower rates of seroprotection in our study. The GMT achieved in our study among the children having protective levels of antibodies is 85.81 IU/L which is lower than most other studies. This supports the observation that GMT achieved in this schedule is lower than that produced by the standard WHO schedule. This may result in breakthrough infection of HB in vaccinated individuals in later life due to waning immunity. However, the immune memory hypothesis supports protection of vaccinated individuals in later life in spite of low anti-HBs antibody titres26. Yet further studies are required to dispel this risk.
Another shortcoming of this schedule is to miss the dose at birth (‘0 dose’). It has been reported that the 0 dose of the HB vaccine alone is 70% - 95% effective as post-exposure prophylaxis in preventing perinatal HBV transmission without giving HB immunoglobulins27. This may also be a factor contributing to lower rates of seroprotection in our study as we have not done HBsAg and other relevant tests to rule out HBV infection in these children. Moreover pregnant ladies by and large are not screened for HBV infection in Pakistan routinely in the public sector except in a few big cities like Islamabad, Lahore or Krachi. Therefore, we do not know the HB status of pregnant mothers and the risk of transmission to babies remains high. Different studies have reported much varied figures of HB status in pregnant ladies. A study from Karachi reports 1.57% pregnant ladies are positive for HBsAg while a study from Rahim Yar Khan reports this figure to be up to 20%28,29. A study by Waheed et al regarding the transmission of HBV infection from mother to infants reports the risk to be up to 90%30. All of these studies support the importance of the birth dose of the HB vaccination and augment the fact that control and eradication of HB with the present EPI schedule is not possible. Jain from India has reported a study using an alternative schedule of 0, 6 weeks and 9 months. He has reported it to be comparable to the standard WHO schedule of 0, 1, 6 months in regards to seroprotection and GMT levels achieved31. This schedule can be synchronised with the EPI schedule, avoiding extra visits and incorporating the birth dose. A similar schedule can also be incorporated in our national EPI.
In our study, seroprotection rates were found to be low in the female gender and the difference was significant. This finding differs with other studies which report lower seroprotection rates in males32. Although the number of female children was less, there is no plausible explanation for this observation. The site of inoculation of the HB vaccine is also very important for an adequate immune response. Vaccines given in the buttocks or intradermally produce lower antibody titres than intramuscular injections given in the outer aspect of the thigh in children, due to poor distribution and absorption of the vaccine within the host body. The practice of giving vaccinations in the buttocks by vaccinators is a common observation which they feel convenient for intramuscular injection in children. This may also be one reason for low seroprotection rates in our study, as we picked the children at random who had received vaccination at public health facilities except a small number of private cases.
The effectiveness of the vaccine also depends on the source of procurement and proper maintenance of the cold chain. In this study 100% seroprotection was observed in children who received the HB vaccine procured from a private source. Although the number of private cases was less, this factor of source and the cold chain also needs attention. To address this issue proper training of EPI teams regarding maintenance of temperature, injection techniques, motivation and monitoring can improve outcomes substantially.
The findings of this study are different from published literature because this is a cross-sectional observational study. This reports the actual seroprotection rates after receiving the HB vaccination in the EPI schedule. While most other studies show the results after ensuring control of influencing factors such as type of vaccine, dose, schedule, route of administration, training and monitoring of local EPI teams and health status of vaccine recipients, etc. Therefore, this is an effort to look at a practical scenario and evaluate outcomes which can help in framing future guidelines to achieve the goal of control and eradication of HB infection. Further studies are required at a large scale to determine the effect of HB vaccination at a national level.
Conclusion
The HB vaccination programme has decreased the global burden of HBV infection, but evidence of decreased burden is not uniform amongst world population.Of course figures witness marked decrease in developed world while in developing world statistics show little change. Unfortunately, implementation of this programme is not uniformly effective in all countries, thus resvoirs of infection and the source of continued HBV transmission persists. HBV infection is moderately endemic in Pakistan. The HB vaccine has been included in the national EPI since 2004. The present study shows seroprotection rates of only 68.6% in vaccine recipients, which is low when compared with other studies; 31.4% of vaccine recipients remain unprotected even after vaccination. Moreover GMT achieved in seroprotected vaccine recipients is also low (85.81 IU/L). There can be multiple reasons for these results, such as type of vaccine used, maintenance of the cold chain, route and site of administration, training and monitoring of EPI teams and dosing schedule. In present practice, the very important birth dose is also missing. These observations warrant review of the situation and appropriate measures to be taken to rectify the above mentioned factors, so that desired seroprotection rates after HB vaccination in the EPI can be achieved among vaccine recipients.
An 86-year-old lady was admitted from her residential home with acute on chronic confusion, new symptoms of expressive and receptive dysphasia, dysphagia, vacant episodes and urinary incontinence. She had a previous significant history of haemorrhagic stroke with residual right sided weakness, atrial fibrillation, hypertension, and moderate dementia. Following a CT head, this lady was started on acyclovir for encephalitis. She failed to respond to treatment, and developed constipation. With careful consideration of her poor prognosis and quality of life, this lady was placed on the End of Life Pathway. She was catheterised for comfort. Nine days after initial insertion of the urinary catheter, purple urine was noted in the catheter bag with yellow urine in the tubing leading to the bag. Urine dipstick showed Blood ++, Protein ++, Leuc +, Nit –ve, Glu -ve, Ketone +, pH 8.0. Urine microscopy showed: WCC 454, RBC 279, epithelial cells 52, no casts. Urine culture revealed heavy mixed growth with multiple organisms.
Question: What is the diagnosis?
Answers:
Porphyria
Propofol infusion syndrome
Purple urine bag syndrome
Blue diaper syndrome
Differential diagnoses: Discoloration of urine can be caused by trauma if blood stained, urinary tract infections, ingestion of dye (methylene blue), medications (amitriptyline, indomethacin, triamterene, flutamide, and phenol).
Explanation:
Porphyria usually presents with severe pain with neuropsychological symptoms or photosensitivity, and urine discoloration is likely to occur from initial onset of disease.
Propofol is an anaesthetic agent, excreted in the urine as phenol derivatives which can cause a green urine discolouration1. This medication is unlicensed for End of Life Pathway. Propofol infusion syndrome is associated with prolonged high dose infusion, but is not always accompanied by urine discoloration.
Blue diaper syndrome is an inherited metabolic disorder of tryptophan with presentation at infancy2-3.
Correct answer
Purple urine bag syndrome (PUBS)
Purple urine bag syndrome (PUBS)
PUBS is an uncommon condition with purple discoloration of the urine catheter system. This phenomenon is due to the presence of indigo and indirubin in the collected urine. PUBS was first published in 19784. Some academics would argue that PUBS was reported even earlier historically as an observation in Sir Henry Halford's bulletin in 18115-6. Two recent literature reviews suggested the prevalence of PUBS is as high as 9.8% in institutionalized patients with long-term urinary catheterisation8-9, 12.
A triad of key factors are suggested as cause of PUBS:
high level of tryptophan in the gut due to diet intake or bowel stasis
long term catheterisation8
urinary tract infection (UTI) with bacteria possessing indoxyl phosphatase and sulphatase enzymes, commonly Providencia stuarttiand rettgeri, Pseudomonas auruginosa, Proteus mirabilis, Escherichia coli,Klebsiella pneumoniae, Morganella, Citrobacter species, Group BStreptococci and Enterococci8, 13.
It is understood that bowel stasis causes accumulation of tryptophan, which leads to an increase in urinary indoxyl sulphate (UIS). In the presence of indoxyl phosphatase and sulphatase enzyme activities, whilst collected in the catheter system, UIS is degraded to form a mixture of indigo and dissolved indirubin in the plastic11, coating the catheter system with a purple appearance. Intensity of discoloration is deeper the longer the urine is in contact with the catheter plastic7, 10-12. The urine does not appear purple prior to entering the catheter.
Recent literature7-8 also suggested female gender, alkaline urine, bed bound debilitated patient population, PVC material7 and institutionalization are further predisposing factors of PUBS.
Management of PUBS requires catheter change and treatment of underlying UTI.
Good catheter hygiene and shorter duration of catheterisation can reduce PUBS1.
A colonic diverticulum is defined as a sac-like protrusion of mucosa through the muscular component of the colonic wall1. The terms “diverticulosis” and “diverticular disease” are used to express the presence of diverticula without associated inflammation. While the term “diverticulitis” indicates there is inflammation of a diverticulum or diverticula, which is commonly accompanied by either microscopic or macroscopic perforation2.
In the developed world, diverticular disease of the colon is widespread and in those aged over 65 years of age it is present in greater than 65%3. The incidence increases dramatically with time and while only 5% of the western population are affected in the fifth decade this rises steeply to over 50% by the eight decade and 60% in the ninth 4.
Although diverticulosis is extremely common, complications requiring surgery only occur in 1% of patients overall 5 and 10% of those admitted to hospital as an emergency for treatment6. Despite this, there is a substantial healthcare burden inflicted by diverticular disease and within the United States alone it accounts for 312,000 hospital admissions, 1.5 million days of inpatient treatment and a total estimated cost of 2.6 billion dollars per annum 7.
The aetiology of the diverticulosis is poorly understood but it is probably a multi-factorial process involving dietary habits (specifically low fibre intake) as well as changes in colonic pressure, motility and wall structure that are associated with ageing8. The pathogenesis of diverticulitis is also uncertain, however stasis or obstruction in a narrow necked diverticulum leading to overgrowth of pathogens and local tissue ischemia is thought likely 2.
This review will discuss the common presentations, investigations and current treatment strategies utilised in the management of acute diverticulitis and its complications as well as providing an up to date synopsis of existing recommendations for follow up and prevention.
Symptoms and Signs
In Western nations, diverticula are most commonly situated in the left colon9 and 99% of patients will have some element of sigmoid involvement10. Therefore patients commonly present with sigmoid diverticulitis that typically displays features of left iliac fossa pain and fever with raised inflammatory markers (see below). Physical exam will disclose left lower quadrant peritonism for simple disease, but in complicated cases physical examination findings may reveal a palpable abdominal mass, evidence of fistulas or obstruction, or widespread peritonitis11.
In cases of complicated diverticulosis, a stricture may lead to obstructive symptoms with complaints of nausea, vomiting and distension being present. If a fistula has developed, a history of recurrent urinary tract infection, pneumaturia and faecaluria may also be elicited12. In a female with a previous history of hysterectomy suspicion will be further raised as colovesical and colovaginal fistulas are rare in females with their uterus in place. If a patient reports passing stools per vagina, insertion of a vaginal speculum and inspection may confirm this latter diagnosis12.
Differential diagnosis
The differential diagnosis for diverticulitis and its complications is extensive and includes irritable bowel syndrome, inflammatory bowel disease, ischaemic or infective colitis, pelvic inflammatory disease and malignancy. It is obviously most imperative to exclude the latter differential 4, particularly in the case of a stricture that is impassable on colonoscopy, as many of these specimens following resection (32% in one series13) will transpire to be adenocarcinoma4. It should also be noted that sigmoid diverticulitis may also masquerade as acute appendicitis if the colon is long and redundant or otherwise situated within the abdomen or pelvis such that the inflamed segment lies in the suprapubic region, right iliac fossa or McBurney’s point2.
Complications
Although diverticulosis is present in nearly two thirds of the elderly population, the vast majority of patients will remain entirely asymptomatic. Even so, an estimated 20% of those affected will manifest symptomatology, mainly as diverticulitis, but potentially with further complications of perforation, abscesses, fistulas, and obstruction, as well as bleeding per rectum6.
The European Association for Endoscopic Surgeons (EAES) developed a classification scheme based upon the severity of diverticulitis, which broadly classifies patients into either simple symptomatic or complicated disease (Table 1)14. Where an abscess or perforation develops the Hinchey classification is used as a staging tool and can provide prognostic information on the likely outcome (Table 2)15.
Table 1 - European Association for Endoscopic Surgeons classification system for diverticulitis 14
Grade of disease
Clinical explanation of grade
Clinical state of the patient
I
Symptomatic uncomplicated disease
Pyrexia, abdominal pain, CT findings consistent with diverticulitis
II
Recurrent symptomatic disease
Recurrence of Grade I
III
Complicated disease
Bleeding, abscess formation, phlegmon, colonic perforation, purulent and faecal peritonitis, stricturing, fistula and obstruction
Table 2 – Hinchey classification of perforated diverticulitis15
Hinchey stage
Features of disease
Risk of death71
Stage I*
Diverticulitis with a pericolic abscess
5%
Stage II**
Diverticulitis with a distant abscess (this may be retroperitoneal or pelvic)
5%
Stage III
Purulent peritonitis
13%
Stage IV
Faecal peritonitis
43%
* Stage I has been divided into Ia Phlegmon and Ib confined pericolic abscess in later modifications38 72 ** Stage II has been divided into IIa abscesses amenable to percutaneous drainage and IIb complex abscess with or without fistula in later modifications14 73
Perforation is probably the most feared complication and the annual prevalence of perforated diverticulitis within a northern European population is currently thought to stand at 3.8 per 100,000 of the population, which is a figure that is increasing16. Despite this only 1-2% of patients who attend for urgent assessment and treatment will have a gross perforation2 but for 80% this will be their first presentation so a high index of suspicion is still required17.
Blood investigations
In clinical practice, inflammatory markers, commonly the White Blood Cell (WBC) count and C-Reactive Protein (CRP) level, are frequently employed to assist in diagnosing diverticulitis and its complications. In a recent retrospective study, a White Blood Cell (WBC) count >10,000/μL was present in 62% of patients with Computed Tomography (CT) confirmed diverticulitis and the presence of leukocytosis was significantly more common in patients with diverticulitis and associated perforation than without (86% v 65%, p=0.01)18.
CRP has also been shown to be of considerable benefit in the diagnosis of acute left sided colonic diverticulitis 19. A recently established diagnostic nomogram with a reported accuracy of 86% that was developed to improve the clinical diagnosis of diverticulitis includes an elevated CRP >50mg/l as well other variables including age, previous episodes, aggravation of pain on movement, absence of vomiting and localization of symptoms and tenderness in the left iliac fossa19.
In addition, it has been demonstrated that in acute sigmoid diverticulitis a CRP below 50mg/l is unlikely to correlate with an associated perforation (negative predictive value 79%) while a CRP above 200mg/l is an indicator that the patient may have a perforation (positive predictive value 69%)20. In this latter study, CRP also had the highest diagnostic accuracy in diagnosing perforation in acute sigmoid diverticulitis across a range of parameters assessed that included WBC count as well as less commonly used tests like bilirubin and alkaline phosphatase20.
Imaging investigations
In the acute phase of diverticulitis the extent of the extramural component of inflammation is more important than the degree of the intramural inflammation and as such CT associated with the use of intravenous and oral contrast and, in ideal conditions, rectal contrast is the gold standard means of investigation21.
CT can accurately identify extra-luminal complications such as an abscess, phlegmon, adjacent organ involvement, or fistula, as well as recognising other alternative diagnoses such as appendicitis, pelvic inflammatory disease, tubo-ovarian abscess or inflammatory bowel disease22.
The two most frequent signs of diverticulitis on CT are bowel wall thickening (96%) and fat stranding (95%) (Figure 1) with less common but highly specific signs including fascial thickening (50%), free fluid (45%), and the presence of inflamed diverticula (43%) 23. Specifically, abscess formation (Figure 2a and b) and extracolonic air or contrast (Figure 3a and b) are findings that are known to predict severity as summarised in the CT classification system developed by Ambrosetti et al24.
Figure 1 - Sigmoid diverticulitis: sigmoid colon with multiple diverticula, significant mural thickening (arrow) and pericolic fat stranding (circles)
Figure 2b - Sigmoid diverticulitis with abscess formation: sigmoid colon displaying mural thickening, diverticulosis and pericolic fat stranding (arrow). Adjacent low attenuation, septated collection (circle) representing abscess formation, with adhesion noted to adjacent small bowel loops.
Figure 3a - Perforated sigmoid diverticulitis: sigmoid colon displaying diverticulosis and mural thickening (arrow) with adjacent collection of intra-abdominal free air and adjacent inflammatory fat stranding (circle), representing active diverticulitis with perforation.
Figure 3b - Perforated sigmoid diverticulitis: sigmoid colon displaying diverticulosis, mural thickening and pericolic inflammatory fat stranding (arrow) with adjacent collection of intra-abdominal free air and adjacent inflammatory fat stranding (circle), again representative of active diverticulitis with perforation.
However despite CT having a reported sensitivity of 97%, specificity of 98%, and global accuracy of 98%25, a misdiagnosis of diverticulitis in cancer patients is relatively common and occurs in 5% of cases21. Therefore investigation of the colonic lumen by endoscopic means or barium enema after the acute attack is mandatory4 but avoided in the initial stages for fear of perforation and exacerbation of the disease2.
In expert hands ultrasound is the next best alternative investigation with a reported sensitivity of 94%26. It has been supported by a recent systematic review27 as well as current practice guidance4 and in critically ill patients it avoids the use of intravenous and intra-luminal contrast21. However it is rarely used in practice as it is operator dependent21 and for it to be accurately utilised it requires a highly skilled/trained individual to be available at all times28.
The other practical alternative to CT is a hydro-soluble contrast enema, however this investigation is significantly inferior both in terms of sensitivity (98 v 92%, p<0.01) and evaluation of the severity of inflammation (26 v 9%, p<0.02)29. While Magnetic resonance imaging (MRI) has a good sensitivity of 94% and a specificity of 87%30, in the acute setting it may be impractical both in terms of examination time and patient co-operation21. Finally, laparoscopy can also be helpful for diagnostic purposes but again in practical terms, with the increasing availability of cross-sectional imaging, it is rarely required for this purpose4.
Outpatient treatment
Evidence for successful and economical outpatient treatment of uncomplicated diverticulitis is beginning to emerge. In a prospective study of 70 patients classified on the basis of an ultrasound examination as having mild-to-moderate acute colonic diverticulitis (as defined by either limited inflammation within a diverticulum extending up to an abscess < 2 cm in diameter), 68 patients were successfully treated with oral antibiotics with an initial liquid diet and this led to a cost saving on inpatient treatment of 80%31.
In a further retrospective analysis, among a cohort of patients who were referred for outpatient treatment it was found that such treatment was effective for 94% of patients, with women and those with free fluid on CT scan appearing to be at higher risk for treatment failure32.
In reality the prospect of outpatient treatment in uncomplicated cases of acute diverticulitis is determined largely by access to the necessary investigative tools for accurate diagnosis and staging of disease, the general fitness of the patient, their ability to maintain adequate oral intake, the possibility of further outpatient review, patient compliance with medications, satisfactory social support and ability to plan for endoscopic follow up21.
In broad terms, if symptoms are not severe and the patient has no significant co-morbidities and is compliant with medical treatment, then a course of broad spectrum antibiotics can be administered orally on an outpatient basis and the patient followed up at subsequent outpatient clinics. However if the patient is systemically unwell, elderly, has significant co-morbidities or there are any other concerns it is safer to arrange for a hospital admission and treatment with intravenous antibiotics12.
Conservative inpatient treatment
Simple diverticulitis requiring hospital admission is usually treated by rehydration, symptomatic relief and intravenous antibiotics. Most patients with uncomplicated disease respond well to medical treatment and generally experience significant improvement in their abdominal pain, temperature and inflammatory markers within two days of initiation of antibiotic treatment33. If this is not the case or there is clinical concern a repeat CT is advocated and operative intervention or percutaneous drainage considered (see below)2.
It should be noted at this stage while the use of broad spectrum antibiotics in acute uncomplicated diverticulitis is supported by guidelines34 there is no actual evidence mandating the routine use of antibiotics in mild uncomplicated diverticulitis35 and in some European countries it is not routine36.
High-quality evidence regarding the most effective type of antibiotic is also lacking35. However anaerobic bacteria (usually bacteroides, clostridium, fusobacterium and peptostreptococcus) are the most commonly cultured organisms with gram-negative aerobes, especially Escherichiacoli, and facultative gram-positives, such as streptococci, often grown as well37. Therefore coverage against both Gram-negative and anaerobic bacteria is widely advocated2 21 38.
If combination antibiotics are selected, Metronidazole provides excellent anaerobic cover with less risk of clostridium difficle infection than alternatives4. However use of single agent may be more cost effective39. Local protocols are likely to influence selection but the patient may be safely switched from intravenous to oral therapy when they can tolerate a diet and oral medicines22 as intravenous antibiotics are not felt to be vastly superior40. Seven to ten days of antibiotic therapy is an acceptable treatment period22 however evidence is emerging to support shorter courses41.
Elective surgery
In a recent position statement from the Association of Coloproctology of Great Britain and Ireland (ASCPGBI) it was concluded that the majority of patients, whether young or old, presenting with acute diverticulitis could be managed with a conservative, medical approach in the longer term. Previous blanket recommendations for elective resection e.g. following two acute episodes of diverticulitis14 were challenged in this statement and it was proposed that the decision on elective resection should be made on an individual basis4. The traditional practice of waiting for a period of 4-6 weeks after a diverticulitis attack before performing an elective operation was not disputed12.
Surgery in the elective setting can be by either an open or laparoscopic technique with a recent randomised trial identifying a 27% reduction in major morbidity42 along with less pain, improved quality of life and shorter hospitalization at the cost of a longer operating time with the laparoscopic approach43. In expert centres conversion rates as low as 2.8% and median hospitals stays of 4 days can be achieved44 and individual case reports of resections using single laparoscopic port access have also emerged45. However if a laparoscopic resection is considered, it is currently recommended that patients should be treated after full recovery from the acute episode of inflammation as there is evidence to suggest lower complication and conversion rates can be achieved4.
The principles for both approaches are the same. A colorectal anastomosis is a predictor of lower recurrence rates after elective sigmoid resection for uncomplicated diverticulitis46. Therefore it is recommended that the distal resection margin is taken onto the rectum as opposed to the distal sigmoid and the splenic flexure is fully mobilised to facilitate this4, however in the case of a long redundant left colon this may not be necessary12. The proximal resection margin is less clear but should be made onto soft compliant bowel4 34. Often it is possible to identify the ureters intra-operatively however, there may be cases of complicated diverticulitis in which the extent and degree of inflammatory changes warrant the use of pre-operatively placed ureteric stents to help aid their identification and avoid injury12.
Emergency surgery for complicated diverticulitis
The indications for emergency operative intervention in acute diverticulitis include the presence of generalised peritonitis, uncontained visceral perforation, gross uncontrollable sepsis, a large undrainable or inaccessible abscess, bowel obstruction and lack of improvement or clinical deterioration with initial medical management 2.
Historically, perforated diverticulitis was treated with a three-stage procedure consisting of faecal diversion with a stoma, resection of the diseased segment of bowel, followed by takedown of the stoma and restoration of intestinal continuity. This then shifted to performing a Hartmann’s procedure which includes a primary resection of the diseased segment and end colostomy followed by subsequent colostomy reversal at a second operation11. In this case reconstruction generally involves a second laparotomy because although laparoscopic reconstruction is effective, it is infrequently performed47-48. As a result reversal is often permanently deferred.
In selected cases the ideal therapeutic option in colonic perforation is a one-stage procedure with resection followed by primary anastomosis, which adds the benefits of being a definitive treatment with the avoidance of the morbidity and mortality associated with a stoma and its reversal49. A protective ileostomy after resection and primary anastomosis is viewed as a valid additional step in patients at high risk of an anastomotic leak (immunosuppression, American Society of Anaesthesiologists (ASA) grade IV, faecal peritonitis)21 but a Hartmann’s procedure may also be selected.
Particularly in cases where there is a stricture causing obstruction and significant faecal loading, a resection in conjunction with on-table colonic lavage and primary anastomosis may be used. This technique has also been described as facilitating a primary anastomosis in the case of a perforation50. However in certain patients with obstruction depending on the viability of the proximal colon a subtotal colectomy with ileorectal anastomosis may be required12 and because small-bowel obstruction may also occur, especially in the presence of a large diverticular abscess, this may also warrant further treatment2.
The use of endoscopic colonic stenting as a treatment of acute obstruction of the large bowel secondary to colonic cancer has been well documented in the literature either as a definitive procedure or as a bridge to surgery and can effectively decompresses the obstructed colon in 90% of cases51. However the use of stents in benign disease is less well documented , with it used mainly as a bridge to surgery52 and because is associated with a higher incidence of complications in acute diverticular disease53 it cannot as yet be recommended.
Laparoscopic surgery in the emergency setting
There have been a number of recent reports of laparoscopic lavage with or without the placement of an intra-abdominal drain for patients with acute diverticulitis and perforation, with the reported advantages including the avoidance of an acute resection and the possibility of a stoma 4. The evidence that has been produced thus far to support its case is highly promising.
A recent systematic review of laparoscopic lavage for perforated colonic diverticulitis identified two prospective cohort studies, nine retrospective case series and two case reports with 231patients and the vast majority of patients (77%) had Hinchey grade III purulent peritonitis. Laparoscopic peritoneal lavage successfully controlled abdominal and systemic sepsis in 95.7% of patients, mortality was 1.7%, morbidity 10.4% and only four (1.7%) patients received a colostomy54.
In the largest series in the literature to date, Myers et al reported 100 patients with perforated diverticulitis and generalised peritonitis. Eight patients with Hinchey IV disease required conversion to an open procedure, with the overall mortality being 4% and recurrence rates only 2% over a median time period of 36 months55.
Percutaneous therapy
The appropriate management of diverticular abscesses is a matter of some debate. However according to the American Society of Colon and Rectal Surgeons (ASCRS) radiologically guided percutaneous drainage is usually the most appropriate treatment for patients with a large diverticular abscess as it avoids the need for emergency surgery and possibility of a colostomy34.
When the abscess diameter is over 5 cm, percutaneous CT guided drainage, in combination with antibiotics, is the standard treatment and offers rapid improvement in symptoms in over 90% of cases, albeit with a high recurrence rate in more severe cases38 and higher likelihood of surgery being needed in those involving the pelvis56.
In practical terms diverticular abscesses less than 3 cm in diameter usually cannot be successfully drained, as the diameter of the pigtail of most drainage catheters will be a similar dimension28. Also for smaller abscesses21, especially those less than 2cm resolution usually occurs with the use intravenous antibiotics alone34. However if a drain is sited it is advisable that before it is removed, resolution of the abscess should be confirmed and a potential bowel fistula excluded by a further contrast study28.
Finally, diverticular disease of the colon is also a relatively common cause of acute lower gastrointestinal bleeding and is in fact the diagnosis in 23% of cases57. This usually settles with conservative management but if the bleeding is profuse angiography and endovascular intervention may be helpful, with surgery very rarely required for this indication4.
Follow up
Following successful medical management of an acute episode of diverticulitis, colonoscopy, flexible sigmoidoscopy or barium enema should be performed several weeks after the resolution of symptoms to confirm the diagnosis and rule out other colonic pathology such as malignancy, inflammatory bowel disease, or ischemia22.
Following surgery there is reported to be a high incidence of the order of 25% for recurrent symptoms, which is put down to the diagnostic overlap that exists with irritable bowel syndrome58. However any suspicion of recurrent diverticulitis following surgical resection should be confirmed by CT scan after which antibiotic treatment should be initiated, as for a case of primary uncomplicated disease12. If this is excluded the high incidence (17.6%) of symptomatic anastomotic stenosis after elective laparoscopic sigmoidectomy should be borne in mind with the possibility of endoscopic dilatation considered if applicable59.
Summary points
CT scan is the gold standard means of investigation for acute diverticulitis and helps classify the stage of disease.
Evidence to support outpatient treatment of uncomplicated diverticulitis is beginning to appear, however hospital admission and treatment with broad spectrum intravenous antibiotics is often required and is highly effective.
The decision to proceed with elective surgery is judged on an individual basis and there is evidence gathering to advocate a laparoscopic approach.
In Hinchey stage III or IV disease, emergency laparotomy followed by either a Hartmann’s procedure or ideally in selected patients a resection followed by primary anastomosis may be required.
In certain cases percutaneous radiologically guided drainage of abscesses is an established alternative to open surgery with laparoscopic lavage another less invasive and highly promising option.
Lifestyle modifications and prevention
Following treatment weight loss, rationalisation of certain medications and exercise are recommended as obesity is significantly associated with an increased incidence of both diverticular bleeding and diverticulitis60, as are non-steroidal anti-inflammatory drugs and paracetamol61, with physical activity significantly associated with a reduction in the risk of complications62.
Whilst dietary fibre, particularly cellulose63, is recommended22 the evidence that supports these recommendations is not particularly strong64. However foodstuffs such as nuts, seeds, popcorn and corn that are usually discouraged have no evidence to support the theory that they may lead to increased complications65.
Small studies without control groups suggest that probiotics may have a positive effect on the recurrence of symptomatic diverticular disease66-67. Long term administration of the non-absorbable antibiotic Rifaxamin has also been used with reported success68 as has the anti-inflammatory mesalazine69. However none of these medications have a strong evidence base and as a result are not in routine use70.
The use of dietary supplements has grown rapidly over the past several decades, and are now used by more than half of the adult population in the United States (US).1 In 1994, the Dietary Supplements Health and Education Act (DSHEA) significantly changed the Food and Drug Administration’s (FDA) role in regulating supplement labelling. According to the DSHEA dietary supplements may contain products taken by mouth including vitamins, minerals, herbs or other botanicals, amino acids, other dietary substances, or combinations or extracts of any of these ‘dietary ingredients.’ The DSHEA reaffirmed that dietary supplements are to be regulated as foods and not as drugs. Annual sales of supplements to Americans are now reported at about $23 billion, a substantial share of which is spent on vitamins and minerals.
The purpose of this review is to present the discussion from available research to internists and other clinicians to help guide their decisions behind the efficacy and safety of dietary supplement use in primary prevention of chronic disease in the general non-pregnant adult population.
Profile of a dietary supplement user
In general dietary supplements are used by individuals who practise healthier lifestyles. Its use is higher among women and the children of women who use supplements; in elderly persons; among people with more education, higher income, healthier diets, and lower body mass indices; and among residents of the western US.2 Individuals with chronic illnesses, or those who are seeking to prevent recurrence of a serious disease (for example, cancer) also tend to be more frequent supplement users.3 Many dietary supplement users perceive their health as better.
Why use dietary supplements?
The growth in supplement use has accelerated rapidly with marketing spurred by claims that chronic conditions could be prevented or treated by supplement use. The commonly used over-the-counter multivitamin and mineral supplements contain at least 10 vitamins and 10 minerals. On a daily basis consumers receive advertising and promotional material of unproven claims made about dietary supplements or other products and the medical wonders they can achieve. Some of the promotional material makes a consumer feel guilty if he or she is not using one. Many users feel so strongly about the potential health benefits of some of these products that they reported that they would continue to take them even if they were shown to be ineffective in scientifically conducted clinical studies.4 More than half of American adults take dietary supplements in the belief that they will make them feel better, give them greater energy, improve their health, and prevent and treat disease.
Is there clinical evidence for use of dietary supplements?
Most studies do not provide strong evidence for beneficial health-related effects of supplements taken singly, in pairs, or in combinations of 3 or more.5 In some studies, or subgroups of the study populations, there is encouraging evidence of health benefits such as increased bone mineral density and decreased fractures in postmenopausal women who use calcium and vitamin D supplements.
Huang et al 5 performed a systematic review to synthesize the published literature on the efficacy of multivitamin and mineral supplements and certain commonly used single vitamin or mineral supplements in the primary prevention of cancer and chronic disease in the general adult population. The authors concluded that the strength of evidence for the efficacy of multivitamin/mineral supplementation in the general adult US population was very low for primary prevention of cancer, cardiovascular disease, and hypertension; and low for cataract and age-related macular degeneration.
The National Institutes of Health (NIH) consensus panel statement2 on ‘multivitamin/mineral supplements and chronic disease prevention’ did not find any strong evidence for beneficial health-related effects of supplements taken singly, in pairs, or in combinations of 3 or more. The panel concluded that the present evidence is insufficient to recommend either for or against the use of dietary supplements by the American public to prevent chronic disease. It also concluded that the current level of public assurance of the safety and quality of dietary supplements is inadequate, given the fact that manufacturers of these products are not required to report adverse events and the FDA has no regulatory authority to require labeling changes or to help inform the public of these issues and concerns.
A recent study published in Archives of Internal Medicine6 raised some disturbing concerns. In this large prospective study, 38,772 older women in the Iowa Women's Health Study were followed up for a mean time of 19.0 years. The authors found that most of the supplements studied were not associated with a reduced total mortality rate in older women. In contrast, they found that several commonly used dietary vitamin and mineral supplements, including multivitamins, vitamins B6, and folic acid, as well as the minerals iron, magnesium, zinc, and copper, were associated with a higher risk of total mortality. Of particular concern, supplemental iron was strongly and dose dependently associated with increased total mortality risk. The association was consistent across shorter intervals, strengthened with multiple use reports and with increasing age at reported use. Supplemental calcium was consistently inversely related to total mortality rate; however, no clear dose-response relationship was observed. The strengths of this study include the large sample size and longitudinal design. In addition, the use of dietary supplements was queried three times: at baseline in 1986, in 1997, and in 2004. The use of repeated measures enabled evaluation of the consistency of the findings and decreased the risk that the exposure was misclassified.
Summary
The use of dietary supplements has grown rapidly over the past several decades even though clinical deficiency of vitamins or minerals, other than iron, is now uncommon in the US.2 Fortification of foods has led to the remediation of vitamin and mineral deficits. The cumulative effects of supplementation and fortification have also raised safety concerns about exceeding upper levels besides interactions of dietary supplements with the prescriptions drugs taken by a consumer. There is no evidence-based data about what the optimal compositions and dose of a multivitamin and mineral supplement should be. Though dietary supplements are perceived to be safe, that should not be sufficient reason for using them without a valid medical need. Providers should take into consideration their efficacy and cost-effectiveness. There are also no outcomes data or data about quality adjusted life years gained by using dietary supplements taken singly, in pairs, or in combinations. The current data available on the efficacy and safety of dietary supplements is conflicting. Clinicians considering the use of dietary supplements should be aware of their risks, consider the likelihood of the adverse effects, interaction with prescription medications, safety, efficacy, costs, and possibility of unintended effectsof dietary supplements.
Conclusion
The conclusion from the available data (new and old) is that consumption of dietary supplements for prolonged periods appears not to be safe and is not cost-effective in primary prevention of chronic disease in the general non-pregnant adult US population. Practitioners should evaluate each case individually and take a decision based on available evidence-based data when considering dietary supplements in this population. Given the potential for widespread use of dietary supplements, there is a need for robust study methods in the future.
In anticipation of new recommendations from the Institute of Medicine and others, it behooves physicians and healthcare providers to review their knowledge base concerning adequate vitamin D intake for fall and fracture prevention in the elderly. There is enough new data for the Institute of Medicine to consider a new Dietary Reference Intake, or DRI, for vitamin D.1 A recent review by Bischoff-Ferrari et al, of numerous randomized controlled trials of vitamin D supplementation in older persons, concluded that both falls and fractures could be prevented. In addition, a dose-response relationship suggested that the optimal supplementation dose is 700 IU to 1000 IU per day.2 Epidemiologic associations between low vitamin D status and various cancers has led some to recommend balancing risk and benefit of moderate ultraviolet light (UV) exposure against complete UV protection for prevention of skin cancer.3 Others have reviewed the epidemiologic evidence for vitamin D supplementation in treatment of hypertension and prevention of cardiovascular disease.4 These epidemiologic studies are tantalizing, yet the evidence is not sufficient to support a causal relationship in making decisions about vitamin D supplementation for the prevention of cancer and cardiovascular disease. I will limit my editorial comments to preventing falls and fractures.
I would suggest looking at potential short- and long-term risks as well as the benefits of any intervention. What evidence do we have for the risks of vitamin D use for prevention? One recent study using a single dose of 500,000 IU of vitamin D daily showed an increased relative risk of fractures,5 but the dose of vitamin D in that study was far higher than other randomized controlled trials. Bischoff-Ferrari et al reviewed documented cases of hypercalcaemia in the randomized controlled trials;2 those authors add that only one trial reported nephrolithiasis, the Women’s Health Initiative.6 It is noteworthy that only the self-reported vitamin D and calcium dose was determined in that study, not the vitamin D status of the subjects. My opinion is that hypercalcaemia is uncommon and its complications are rare.
Many interventions that are routinely recommended for the older person probably have higher risks than the 700 IU to 1000 IU of vitamin D per day suggested by the evidence. Medications for hyperlipidaemia are one case in point; antihypertensives are another. Both are considered relatively safe and effective in primary and secondary prevention of cardiovascular disease. The long-term risks of the supplementation of 700 IU to 1000 IU of vitamin D are not well known compared to those long-term risks associated with lipid-lowering drugs or antihypertensives. On the other hand, some older persons at increased fall risk have more immediate threats to their health from a fall or fracture than any long-term risks of vitamin D supplementation. Given the detrimental consequences of falls and fractures in the elderly, the risks of vitamin D supplementation may be worth it.
Vertigo is the hallucination of movement of the environment around the patient, or of the patient with respect to the environment 1. It is not a fear of heights.
Vertigo is not necessarily the same as dizziness
Dizziness is a non-specific term which can be categorised into four different subtypes according to symptoms described by the patients:
Vertigo
Presyncope: the sense of impending faint, caused by a reduced total cerebral perfusion
Light-headedness: often described as giddiness or wooziness 2
Disequilibrium: a feeling of unsteadiness or imbalance when standing 2
Classification Vertigo may be classified as:
Central - due to a brainstem or cerebellar disorder
Peripheral - due to disorders of the inner ear or the Vestibulocochlear (VIIIth) cranial nerve
Incidence/Prevalence: Most patients who complain about dizziness do not have true vertigo:
5 community based studies into dizziness indicated that around 30% of patients were found to have vertigo, rising to 56.4% in an older population 3
A postal questionnaire study which examined 2064 patients, aged 18-65, 7% described true vertigo in the previous year 3
A full time GP can therefore expect between 10-20 patients with vertigo in one year 3
93% of primary care patients with vertigo have either benign paroxysmal positional vertigo (BPPV), acute vestibular neuronitis, or Ménière's disease 4. These conditions are highlighted in Table 2
Causes A wide range of conditions can cause vertigo, and identifying whether deafness or CNS signs are present, can help narrow the differential diagnosis, as shown in Table 1.
Brain tumour:- e.g. ependymoma or metastasis in the fourth ventricle
Acute cochleo-vestibular dysfunction
Cervical spondylosis
Migraine
Syphilis (rare)
Following flexion-extension injury
Multiple sclerosis
Aura of epileptic attack – especially temporal lobe epilepsy
Drugs – e.g. phenytoin, barbiturates
Syringobulbia
Symptoms
Vertigo may be due to central lesions or peripheral lesions. Vertigo may also be psychogenic or occur in conditions which limit neck movement, such as vertigo caused by cervical spondylosis, or following a “whiplash” flexion-extension injury.
It is essential to determine whether the patient has a peripheral or central cause of vertigo 1.
Information obtained from the history that can be used to make this distinction includes 1:
The timing and duration of the vertigo
Provoking or exacerbating factors
Associated symptoms such as
Pain
Nausea
Neurological symptoms
Hearing loss
Central vertigo:
The vertigo usually develops gradually
Except in: an acute central vertigo is probably vascular in origin, e.g. CVA
Central lesions usually cause neurological signs in addition to the vertigo
Auditory features tend to be uncommon.
Causes severe imbalance
Nystagmus is purely vertical, horizontal, or torsional and is not inhibited by fixation of eyes onto an object
The duration of vertigo episodes and associated auditory symptoms will help to narrow the differential diagnosis 5. This is illustrated for various pathologies that cause vertigo, in Table 2
Table 2 Timing of symptoms
Pathology
Duration Of Episode
Associated Auditory Symptoms
Peripheral or Central Origin
Benign Paroxysmal Positional Vertigo
Seconds
No
Peripheral
Vestibular Neuronitis
Days
No
Peripheral
Ménière's Disease
Hours
Yes
Peripheral
Perilymphatic Fistula
Seconds
Yes
Peripheral
Transient Ischemic Attack
Seconds / Hours
No
Central
Vertiginous Migraine
Hours
No
Central
Labyrinthitis
Days
Yes
Peripheral
Stroke
Days
No
Central
Acoustic Neuroma
Months
Yes
Peripheral
Cerebellar Tumour
Months
No
Central
Multiple Sclerosis
Months
No
Central
It is important to differentiate vertigo from non-rotatory dizziness (presyncope, disequilibrium, light-headedness). Patients can be asked whether they “felt light headed or felt as if the world was spinning around” during a dizzy spell 3.
Important points in the history:
Onset - specific provoking events such as flying or trauma
Associated auditory symptoms - rare in primary CNS lesion
Other associated symptoms
Nausea and vomiting in a vestibular cause
Neurological symptoms such as visual disturbance, dysarthria in a central lesion
Physical/signs
Examination of ear drums (Otoscopy/ Pneumatic otoscopy) for:
Vesicles (Ramsay Hunt syndrome)
Cholesteatoma
Tuning fork tests for hearing loss – Rinne/Weber tests
Cranial nerve examination. Cranial nerves should be examined for signs of :
Nerve palsies
Sensorineural hearing loss
Nystagmus 3
Hennebert's sign 1
Vertigo or nystagmus caused by pushing on the tragus and external auditory meatus of the affected side
Indicates the presence of a perilymphatic fistula.
Gait tests:
Romberg's sign (not particularly useful in the diagnosis of vertigo 1)
Heel-to- toe walking test
Unterberger's stepping test 1 (The patient is asked to walk on the spot with their eyes closed – if the patient rotates to one side they have labyrinth lesion on that side
Dix-Hallpike manoeuvre 1
The most helpful test to perform on patients with vertigo1
If rotational nystagmus occurs then the test is considered positive for BPPV. During a positive test, the fast phase of the rotatory nystagmus is toward the affected ear, which is the ear closest to the ground.
Head impulse test/head thrust test
Useful in recognizing acute vestibulopathy 6
Caloric tests
Cold or warm water or air is irrigated into the external auditory canal
Not commonly used
Investigations/Testing to consider:
Special auditory tests
Audiometry helps establish the diagnosis of Ménière's disease
The history is most important and may give a quite good indication of the cause of vertigo. General medical causes such as anaemia, hypotension and hypoglycaemia may present with dizziness, and therefore should be investigated.
If features of CNS causes is suspected from the history or examination:
CT/MRI Brain imaging as appropriate
Treatment
Treatment should ideally aim at the cause of the vertigo 7:
Medical management – as described below.
Vestibular rehabilitation exercises – e.g. Cawthorne-Cooksey exercises 5.
These exercises aim to help the patient return to normal activity more quickly.
Moving the eyes from side to side and up and down while in bed or sitting down - then moving the head, first with your eyes open and then closed
Other forms use gaze and gait stabilising exercises. Most exercises involve head movement
For most patients the main priority is effective control of the symptoms.
For acute attacks, treatments include 5,8: -
Betahistine hydrochloride 8-16mg upto TDS
Cinnarizine, 15-30 mg TDS or
Prochlorperazine should be reserved for rapid relieve of acute symptoms only 8,12 - tablets 5-10 mg or buccal 3mg TDS or injection 12.5 mg IM or 25mg PR suppository - if vomiting
Preventive measures for recurrent attacks include:
Restrict salt and fluid intake - stop smoking and restrict excess coffee or alcohol 9,10
Betahistine hydrochloride 16mg regularly TDS seems most effective in Ménière's
Cinnarizine 15-30 mg TDS
Points to consider
Warn patients when drugs may sedate 10.
Prochlorperazine is less sedating than some other recommended antihistamines, but may cause a dystonic reaction (particularly in children and young women) 11.
Benzodiazepines are not recommended 9.
Recurrent vertigo
The most important first step in the management of recurrent vertigo is to distinguish vertigo from 'dizziness'.
In attacks of vertigo there is a sense of mobile disequilibrium ("the room spinning") which, if severe, results in uncontrolled staggering in one direction which may be only prevented by grabbing a solid object 10.
Epley's manoeuvre
a. Aims to remove debris from the semicircular canals and deposit it in the utricle where hair cells are not stimulated 11 b. Contraindications include 10: i. Severe carotid stenosis ii. Unstable heart disease iii. Severe neck disease (cervical spondylosis with myelopathy) iv. Advanced rheumatoid arthritisConsultation and referral:
Refer to secondary care if 10 :
Recurrent separate episodes
Neurological symptoms e.g. dysphasia, paraesthesiae or weakness
Associated sensorineural deafness
If there is an inadequate visualisation of the entire tympanic membrane or an abnormality (e.g. cholesteatoma)
Atypical nystagmus e.g. non-horizontal, persisting for weeks, changing in direction or differing in each eye
Positive fistula sign: pressure on the tragus reproducing symptoms (suggests endolymphatic fistula
If the patient has hearing problems in addition to vertigo then referral should be made to an ENT specialist. Other cases should be referred to a neurologist 10.
While awaiting referral:
Consider symptomatic drug treatment for no longer than 1 week because prolonged use may delay vestibular compensation
It is important that the person stops symptomatic treatment 48 hours before seeing a specialist, as it will interfere with diagnostic tests such as the Dix-Hallpike manoeuvre.
If the person's symptoms deteriorate, seek specialist advice.
When to consider hospitalization
Admit the patient to hospital if they have severe nausea and vomiting, and are unable to tolerate oral fluids 9.
Admit or urgently refer the person to a neurologist if they have:
Very sudden onset of vertigo (within seconds) that persists.
Acute vertigo associated with neurological symptoms or signs (e.g. new type of headache - especially occipital, gait disturbance, truncal ataxia, numbness, dysarthria, weakness) which may suggest CVA, TIA, or multiple sclerosis 9.
Admit or refer the person as an emergency to an ENT specialist if they have acute deafness without other typical features of Ménière’s disease (tinnitus and a sensation of fullness in the ear). Sudden onset unilateral deafness would suggest acute ischaemia of the labyrinth or brainstem, but can also occur with infection or inflammation.
Emergency treatment may restore hearing. The person should be seen within 12 hours of the onset of symptoms 9
The urgency of referral depends on the severity of symptoms (e.g. requirement for intravenous fluids because of excessive vomiting) and the suspected diagnosis 9.
Patient InformationThe Ménière's Society www.menieres.org.ukwww.patient.co.uk/doctor/Vertigo.htm
A lifetime of happiness! No man alive could bear it: it would be hell on earth
George Bernard Shaw (1856-1950)
Guess what? Antidepressants do not work for mild or moderate depression! This amazing ‘revelation’ seems to surface periodically as a popular item in the media and platform for the experts in living, especially since talking therapies are now considered the panacea for all ills. Despite methodological flaws in the research (as with all studies)1 and noticeably, with less scrutiny of talking therapy research, this ‘fact’ is preferentially brought to our attention. That antidepressants have unpleasant side effects and are not always effective we have known all along. When one thinks about it, all drugs have adverse effects. Strange how antidepressants work - they seem to cause unpleasant adverse effects but not beneficial ones! No one doubts that neurotransmitters are involved in pain transmission or are responsible for muscle movement, yet biological pathways are dismissed when ‘emotional’ or ‘psychological factors’ are promoted as causing distress. By contrast, talking therapies cure the problem and are considered safe, it seems.
Am I alone in not being surprised? I have never understood how mild depression (whatever that is) becomes moderate, or how normal becomes mild, even with the International Classification of Diseases (ICD 10) and Diagnostic and Statistical Manual of Mental Disorders (DSM IV) to hand. And who has decided there be a minimum duration of two weeks for mild depression? Does it not count if one is suicidal for a week? The corollary of this is seen in another nugget of perceived wisdom masquerading as ‘research’ which informs us that 14 units and 21 units of alcohol per week are considered the upper limits of safe drinking for women and men, respectively. What if intake exceeds these magical figures? A rigid adherence to the dictum would castigate a woman or man as alcohol-dependent imbibing 15 and 22 units per week. This type of anecdotal research has no scientific meaning because one cannot equate units with a way of life, one’s metabolism, stature, weight, and so forth. In the laboratory I can detect mild anaemia from severe anaemia because haemoglobin can be measured, and when to treat is usually quite clear-cut. In mental health studies, as with the alcohol example quoted, the theory is also vague. The usual response from ‘researchers’ in this field is that rating scales are capable of detecting differences in mood, say, which then determines the ‘therapy’ one receives. This is a fallacy. For example, in medicine, small variations in haemoglobin do not make the slightest difference to how a patient feels, though such fluctuations are important.
How do you measure tiredness? One can feel tired and have a normal haemoglobin level. In the elderly, for example, abnormal blood indices are often present despite an outwardly well appearance. The anaemia still needs to be treated. Laboratory tests are therefore used to confirm the severity of an illness and are objective, regardless of outward appearances. Treatment is given and the haemoglobin (in this example) returns to normal, without the patient even being aware in many cases. The difference between the above example and a mental health ‘condition’ is that there is no realistic cut-off point between feeling well and being unwell. Therefore, when to intervene is arbitrary. Am I tired because I’m depressed, or is it the other way round? Do two or more weeks of mild happiness mean I am ill? ‘Is there such a thing as moderate happiness?’ ‘Should we be using mood stabilizing medication or talking therapies if we are mildly or moderately happy?’ Absurd. No one speaks of another individual as being mildly or moderately happy. So why should it make sense to talk of someone as mildly or moderately depressed? What next – mildly or moderately normal? Severe conditions require treatment; mild upsets can be managed by simple alterations in lifestyle, and one does not need a medical doctor or an expert in living to tell you so. There is little point in expecting a favourable drug treatment outcome for say, hypertension, if the patient continues to smoke or is grossly overweight. Take the metabolic syndrome of dyslipidaemia, central obesity, hypertension, and insulin resistance: treatment involves removing the causative factors, not prescribing drugs to reduce weight.
I am a kind of paranoiac in reverse. I suspect people of plotting to make me happy.
J.D. Salinger (1919-2010)
The norm for most people is to get on with matters in hand and tolerate life’s daily grind. Some good days, some bad. A lot depends on your financial status too. Nothing new there. It does not make sense to assume antidepressants will make the slightest difference to an individual’s ‘ups and downs,’ as there is no clinical syndrome to address. Living is not a genetic condition, though alterations in genes affect living. There is the risk of medicalising every difficulty one faces. Behaviour is often personality-driven and not a symptom of illness, and though personalities vary, one does not speak of a personality illness or personality condition. Even the term personality ‘disorder’ has come in for much criticism because of the difficulty in defining what is meant by personality.2 One individual may be overtly aggressive, another too passive, and to embrace all eventualities, there is the term passive-aggressive. No point in being perfectionist because nowadays you may fit the obsessive character description. On reflection though, I would rather the cardiologist, surgeon, airline pilot, concert musician and so forth, err on the side of perfectionism! It does not require much imagination to realize that the real test of a ‘condition’ is when an individual begins to feel he/she is not functioning at a healthy level because of a pervasive sense of inertia, lassitude, lack of motivation, persistent gloominess and despair, for reasons apparent or not. Most people feel despondent at times, say after bereavement, or losing one’s job, and likewise many individuals are more motivated, innovative, and ambitious than others. Some conditions, which seem to have a genetic basis, have stood the test of time, such as bipolar disorder, eating disorders, schizophrenia, borderline personality disorder and obsessive compulsive disorder; all other ‘disorders’ less so.
That antidepressants often fail to work is nothing new, even for severe depression because there are often too many factors at work. Patients who suffer from severe depression and suicidal ideation would be unlikely to be entering a clinical trial in any event. Furthermore, the theory of a chemical neurotransmitter imbalance is outmoded. It could be that an alteration in receptor sensitivity, either at the presynaptic or postsynaptic site, is the critical factor. Furthermore, it is conceivable that more neurotransmitters are involved than the handful we know of at present. What does the physician do then? Tell patients there is only a 70% chance of getting better with antidepressants and let them get on with it! Anyway, why should antidepressants be any different to other drugs used throughout the entire field of medicine? No drug has a 100% cure rate (save perhaps antibiotics or vaccines for specific infections). When one is well it is easy to be critical, cynical and dismissive. When a patient develops Hodgkin’s Lymphoma or any other serious nonsurgical illness and is told there is a 70% chance of survival with medication it is highly likely he/she would optimistically choose the latter. Why should severe depression be any different?
Rating scales cannot be robustly be relied on, at least in psychiatry, as most information is descriptive and there are few instances when a scale can be regarded as having proven validity.3 The Hamilton Rating Scale, a commonly used measure of depression, contains a large number of items relating to sleep and anxiety, and hence sedative antidepressants may seem to be appropriate. It could therefore be argued that the patient is benefiting from a good night’s sleep rather than any inherent antidepressant effect of the drug in question. Thus the side effect of the drug now has a therapeutic effect! This is akin to saying antihistamines work only through their sedative effect! Many scale items are poor contributors to the measurement of depression severity and others have poor interrater and retest reliability. Besides, mental and emotional diagnoses are so often ephemeral, and therefore defy ‘rateability’. Another example is the Beck Depression Inventory (BDI), often used as a screening tool: because it is a self-report questionnaire, it poses problems in that the person completing it may distort responses. The question therefore is: how does one prove that antidepressants are effective on the basis of flawed clinical trials even when the evidence in clinical practice is obvious?
Meta-analysis is often used as ‘proof’ that research shows or does not show evidence to support a particular theory. However, meta-analysis itself is not foolproof. The methodology is complex and fraught with difficulty.4 The sheer volume of material can impress the naïve and the search for negative outcomes, if it suits the preconceived, intended purpose, will be celebrated in the media as ‘scientists discover’ and so forth. A diligent search of the literature will uncover the sort of results one is looking for, because remember, there are lots of bad trials, no trials are identical, and there is heterogeneity among trial results.
It is clearly very difficult to devise a perfect rating scale, particularly in psychiatry where one is dealing in ‘mind matters’ and the pathoplasticity of mental disorders. Besides, leaving ‘research’ aside, the terminology in psychiatry as a whole is vague and interchanges between lay descriptions and ‘psychiatric’. Does ‘mad’ mean psychotic? What is madness anyway? Is neurotic the same as being a worrier or chronically anxious? Can one be neurotic about one thing and not another? Is a teenager worried about exams (assuming he/she is fully prepared of course) normal, anxious, neurotic or unduly concerned? In medicine, matters are clearer by and large: blood pressure is high, low or normal. We are not comparing like with like, is the usual retort.
To be stupid, selfish, and have good health are three requirements for happiness, though if stupidity is lacking, all is lost.
Gustave Flaubert (1821 - 1880)
Although it is easy to accept that antidepressants are ineffective for mild or moderate depression, one has to consider that in even in major depression the effects of spontaneous remission (75% in 12 weeks in some instances)5, 6 and natural fluctuations need to be taken into account. Even patients with chronic symptoms, who normally seek help when their symptoms are at their worst, sometimes improve anyway. Take a simple known fact: the prevalence of pain in patients with depression is high, around 65%, and the average prevalence of depression in pain clinics is nearly of a similar order. Pain symptoms in depression are not adequately treated by Selective Serotonin Reuptake Inhibitors (SSRIs) or indeed by amitriptyline (commonly used for pain relief) and hence depression is prolonged.7 On reflection it should not be too difficult to comprehend why drugs do not always work given that some three billion base pairs of deoxyribonucleic acid (DNA) make up the human genome. To add to the complexity, copy number variation refers to differences in the number of copies of a particular region in the genome, which is associated with susceptibility or resistance to disease.
Patients who are depressed and helped by medication are now being told by irresponsible ‘counsellors’ and sometimes by their own family doctors, that they are really only taking sugar pills, because of selective information taken from flawed antidepressant drug trials. By the same token should patients also give up their counselling sessions and take a sugar pill? It should not be forgotten that a true placebo control is impossible in psychotherapy unlike physical methods of treatment (though still difficult), whatever the flaws inherent in the latter. It seems odd that psychological data in ‘therapy studies’ carried out by non-clinicians and clinicians gets to be called ‘science’ whereas drug research carried out by scientists becomes ‘flawed science?’ Even so, countless dubious articles of ‘human interest’ manage to appear in prestigious medical journals under the apparent authorship of ‘leading figures in the field’ (being a pop celebrity physician or psychologist helps) where the psychobabble is fed to the reading classes who in turn regurgitate it to their naïve, well-intentioned adherents, and to the media. I don’t blame the latter: all the media want is a good story; ‘human interest’ items will sell newspapers regardless of their quality or accurateness. People who run the media have little understanding of science and wear their ignorance as a badge of honour.8 Therefore it comes as no surprise when it is discovered that antidepressants do not work for mild or moderate depression that the slogan becomes ‘antidepressants do not work at all,’ which is what the critical psychiatry faction wanted in the first place.
If you can’t explain it simply you don’t understand it well enough.
(Albert Einstein 1879-1955)
Ironically, as in neuropharmacology, it is through progress in molecular biology that advances in psychotherapy research will be made as molecular genetic findings unfold over the next few years; it is likely that biological vulnerability will become increasingly detectable; although single genes and polymorphisms will probably never account for a large proportion of variability, combinations of genes may increasingly identify specific types of environmental vulnerability.9, 10 No mental health condition is ‘all genetic or environmental.’ However, it is through neuropharmacological research that the mechanisms of action of various drugs used in neurology and psychiatry have been identified and helped to develop an understanding of biological substrates underlying the aetiology of psychiatric disorders. Genetic studies help us understand why some individuals are more prone to becoming ill given the same environmental stress factors.
The overriding clinical impression by doctors in clinical practice and in hospital settings is that patients tolerate minor side effects in the hope that benefits will accrue in the long term, as they do with the very unpleasant adverse effects from other drugs used in medicine (chemotherapy, for example). It is incumbent for doctors to stress that antidepressants do work for severe depression (though not in all cases) and mood stabilizers are helpful in bipolar disorder, and advise about untoward effects.11 Doctors should also emphasize that the therapeutic effect is not that of a placebo, much in the same way that methylphenidate helps many children with Attention Deficit Hyperactivity Disorder (ADHD) when it is properly diagnosed and not attributed to poor parenting skills. The beneficial effects of antidepressants when they do occur are noticed objectively, usually within four to eight weeks of taking the medication, sometimes sooner. Patients are not coerced into feeling better by the charismatic charm of the physician, who may be sceptical to begin with, in any event. Besides, ‘charisma’ wears a bit thin when one continues to feel miserable and unresponsive to treatment of whatever sort. Cognitive therapy is effective for those who are motivated and not too disabled with lethargic indifference to engage. Behavioural methods do work, because specific techniques are employed which allow accurate objective evidence (cessation of smoking, desensitisation for phobias, amelioration of obsessive rituals) to be gathered.
There is a vast grey area between what constitutes ‘normal’ and ‘mild or moderate’ depression. In most cases, even if one concedes that a patient is ‘mildly or moderately’ depressed there is usually no need to interfere, because everyday issues are usually the triggering factors. Most ‘psychiatric’ conditions are not psychiatric, and life’s ills and worries are best left to the General Practitioner (GP) to offer advice, perhaps a close friend, or even a next-door neighbour. Best to throw away all the psychobabble bibles and ‘treatment packages’ by the experts in living who earn a good income exploiting patients’ weaknesses. Instead, patients should be taught to rely more on their natural intuition and cultivate inner strengths and talents. When depression, mood swings, phobias, obsessive rituals, and inner turmoil (for example, derogatory hallucinations, tormenting thoughts) become overwhelming, that is the time to seek medical advice. Most people (unless delusional) know which category they fit into, and should be able to receive help or intervention to deal with mental anguish before it becomes too disabling.
Many patients get better with or without talking therapies or medication, through sheer determination. At least with pharmacotherapy the medication can be thrown out after a reasonable period of adequate dosage. Either the drug works or it does not. Psychotherapy theoretically, particularly psychoanalysis, has no end, and can prove very costly. The top-up sessions are not free either! Even the National Health Service (NHS) will only offer a certain number of sessions and then you are on your own. Of course, there is the homework and perhaps a few more top-up sessions, if you make enough fuss! By all means investigate the alleged fraudulent business practices of Big Pharma and eliminate the biased positive results of drug trials. Author bias should also be scrutinized to eliminate personal prejudice. There is no need for patients to be duped by the empty rhetoric perpetuated by the experts in living if we are simultaneously led to believe that life‘s ills will be resolved through the use of a sugar pill.
To be conscious that you are ignorant is a great step to knowledge.
Benjamin Disraeli (1804 - 1881)
Within the field of psychiatry (and psychology) there are those who do not believe in drug treatments, ADHD, eating disorders, to mention a few. Everything is environmentally induced or caused by bad parenting, we are told by some self-appointed ‘life experts‘. And there are those who thrive on being deliberately controversial in an effort to raise their media profile and income. What a pity. Cardiology does not compete with cardiothoracic surgery nor does gynaecology compete with obstetrics, for example. Debate - yes. Antagonism - no. It is time for psychiatry to re-examine and distance itself from the popular psychobabble of the agony aunts and uncles before it completely loses its sense of professionalism. Because there are so many overlapping clinical scenarios within psychiatry and neurology, the former needs to align itself with the latter specialty and by doing so will gain respectability. The ever-widening chasm between psychiatry and other medical disciplines has been gathering momentum over the years, leaving psychiatry more alienated than ever. Perhaps there is also a case for subsuming some psychiatry specialties back into general psychiatry, for example, a Consultant General Psychiatrist with a ‘special interest’ in the conditions a Child Psychiatrist might be expected to deal with, such as Tourette’s syndrome, ADHD, and psychoses. Fewer graduates are now interested in pursuing psychiatry because they do not want to study medicine for years only to end up being marginalized as an on-looker in some multidisciplinary setting, devoid of any responsibility or decision-making. It is not that Cinderella will not be going to the Ball; there will be no Ball to go to.
Prof Griffiths is a Professor of Medicine (Intensive Care), Dept of Musculoskeletal Biology, Institute of Ageing & Chronic Disease, Faculty of Health & Life Sciences University of Liverpool, and Honorary Consultant Physician in Intensive Care Medicine, Whiston Hospital, UK.
He obtained a BSc in Physiology during undergraduate training in medicine (MBBS) at University College London during the ‘70s. During the early ‘80s in London obtained a research MD studying muscle energetics in the early days of human Magnetic Resonance Spectroscopy. Became a consultant in adult Intensive Care Medicine in 1985 following a move to Liverpool in 1984 and continued research interests in muscle and expanded these into nutrition (glutamine) and the critically ill. Since then has been a pioneer of the rehabilitation of the post-ICU patient. He extensively involved over the last two decades in undergraduate curriculum reform and as the Director of the Final Year has pioneered a fully portfolio based professional learning programme.
How long have you been working in your speciality?
I have been a consultant intensive care physician for more than 25 years.
Which aspect of your work do you find most satisfying?
To be able to improve patient care through clinical research and the training of medical students.
What achievements are you most proud of in your medical career?
Raising the awareness of the physical, psychological and cognitive challenges ICU patients and relatives face during recovery and contributing to the evidence base guiding rehabilitation.Clinical nutrition research on glutamine and identifying the need to use six month mortality outcomes in the critically ill. Creating a final year of undergraduate medical training that fosters professionalism and critical self awareness based upon a clinical portfolio and appraisal process that produces graduates fit for practice.
Which part of your job do you enjoy the least?
Very little, but perhaps the ever increasing bureaucracy of regulation in practice and research.
What are your views about the current status of medical training in your country and what do you think needs to change?
In the UK most medical schools have radically reformed their curriculum to meet the needs of modern medicine and life- long learning. In Liverpool our students are recognized to be well prepared with the skills to ensure patient safety and start foundation training following a course commended by clinicians, hospitals, examiners and GMC alike. Post-graduate changes have paralleled these developments and while the training structures and closer observations are to be commended the restrictions on working time remains a concern for the acquisition of real “shop floor” experience. Our trainees simply don’t get enough “flying hours” as in the past.
How would you encourage more medical students into entering your speciality?
Intensive care medicine is popular. The problem for students is to understand how to get there. The new Faculty of Intensive Care medicine, that has just starte, brings an independent speciality out from under the umbrella of its various parent specialities and hopefully will provide the focus to make the career pathway clearer in the future.
What qualities do you think a good trainee should possess?
All those attributes that the GMC expect of a practitioner! In particular I like to see enthusiasm, self awareness and measured confidence, an enquiring and questioning mind and a degree of professional flexibility mixed with the ability to ask for help and advice. I need to trust them just as their patients need to as well.
What is the most important advice you could offer to a new trainee?
Stay calm, be professional and follow the basic principles of good medical practice doing the simple things well, and don’t be afraid to ask for help.
What qualities do you think a good trainer should possess?
Maintain professionalism and be a role model at all times with the ability to listen, support and recognize the strengths as well as being firm with those things that need developing.
Do you think doctors are over-regulated compared with other professions?
No, while regulation does not itself prevent bad medicine it does prevent it being ignored.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what should be done to counter this trend?
De-professionalising only occurs when doctors avoid taking leadership roles. I think this was a fear in the recent past but in the last 10 years in the UK there has been a strong drive to redefine professionalism and the role of the doctor for the 21st century and it is central now to modern undergraduate and post graduate training with the importance of Consultants and GPs taking leadership roles in planning health care delivery.
Which scientific paper/publication has influenced you the most?
Huxley AF 1957 A theory of muscular contraction” Prog. In Biophys. And Biophys. Chem; 7:255.
Professor Sir Andrew Huxley was awarded the Nobel prize in medicine in 1963 with AL Hodgkin for nerve conduction but my personal memory is in muscle physiology (as one of my tutors) for his work on the theory of muscle contraction and the role of cross bridges. His clarity of thought was demonstrated in his ability to always ask the question everyone else wished they had asked! He was a kind and gentle teacher that gave time even for a simple medical student.
What single area of medical research in your speciality should be given priority?
The brain is the forgotten organ in multiple organ failure. We now recognize that acute brain dysfunction is a serious problem but we know little about its pathology, how to prevent it or recover from it.
What is the most challenging area in your speciality that needs further development?
There has been a rush towards ill conceived large scale pragmatic clinical effectiveness studies of various therapies few of which have shown much to change practice. Rather there is a need for more detailed scientific research to better define efficacy of therapies by exploring the pathological processes and the genetic and environmental influences of common disorders that result in multiple organ failure.
Which changes would substantially improve the quality of healthcare in your country?
Addressing the challenge of an ageing population and in particular the community medical and non-medical support of the aged infirm so that modern medicine does not grind to a halt.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
By showing leadership and making the changes happen and not leaving it to others perhaps less informed to direct change.
How has the political environment affected your work?
I have tried to ignore it as much as possible. Politics is a business best left to politicians while the rest of the world gets on with life.
What are your interests outside of work?
I treasure my family, a marriage of 28 years, with two undergraduates in medicine and one in architecture and doing all the jobs they ask of a father. When not escaping to the south of France or walking I become a generalist handyman so it can be a gardener, electrician, plumber, decorator, carpenter, car mechanic………and the Sunday Roast!
If you were not a doctor, what would you do?
With the exception of playing a musical instrument anything that combines academia, teaching and its practical application, but with preference in the natural world.
A 45- year -old man hit by a speeding vehicle presented with chest and abdominal pains, along with dyspnea and vomiting. On examination, vitals signs were pulse rate of 122 per minute, blood pressure of 100/60 mm of Hg and respiratory rate of 28 per minute. Chest examination showed tenderness on the lower ribs. The patient had ecchymotic patches and abrasions on his lower chest and abdomen. Abdominal examination showed diffuse tenderness in all quadrants. The patient also had an open fracture of right femur. Arterial blood gas analysis showed hypoxia. Liver enzymes were normal. Chest X-ray and FAST (Focused Assessment with Sonography for Trauma) did not reveal any obvious pathology. CT scan of the chest showed small contused areas of lungs on both sides. Contrast CT abdomen showed the following picture.
Medicine in pictures
CECT (Contrast Enhanced Computed Tomography) of Abdomen.
Question: What is this radiological finding?
Answers:
1. Pneumobilia
2. Liver Laceration
3. Portal vein air embolism
4. Oriental cholangiohepatitis.
Correct answer and description – at the end of the article
Differential diagnosis:
Air in the portal vein has many causes including Necrotizing entero-colitis, Inflammatory bowel disease, Pneumatosis intestinalis, Mesenteric ischemia, Perforated peptic ulcer, Trauma etc.
Explanation:
Pneumobilia means air in the biliary tree. This condition refers to central location of the air which does not extend to within 2 cm of the liver capsule. It is most commonly seen in patients following surgery in which a biliary-enteric anastomosis has been created or a sphincterotomy (sphincter of Oddi) has been performed.
Liver laceration is seen as a non-enhancing region, linear or branching, hypo-dense wedge lesion extending to liver surface.
The CT findings in oriental cholangiohepatitis can present as intra- or extra hepatic duct stones, dilatation of the extra hepatic duct with relatively mild or no dilatation of the intrahepatic ducts or as localized dilatation of the lobar or segmental bile ducts.
Discussion:
Gas in the portal vein is a rare and usually fatal condition, and its presence in trauma is a rare occurrence. Various terms are used to describe the condition like hepatic portal vein gas (HPVG), pneumoportogram, gas embolism of the portal vein etc. It has to be differentiated from air in the biliary radicals. Portal venous gas manifests on CT as small, tubular air densities in the peripheral regions of the liver, predominantly in the left hepatic lobe in the left portal vein as it is more anterior. Due to the centrifugal flow of blood in the portal venous system, air bubbles appear to extend within 2 cm of the liver capsule 1, 2 . Susman and Senturia state that air in the biliary radicals is more centrally placed and extends up to the hilum and into the common hepatic duct due to the centripetal flow of bile 3 . In the pediatric age group the commonest cause attributable is necrotizing entero-colitis, and along with pneumatosis intestinalis it is in fact pathognomic of the condition4 . The pathophysiology behind air entering portal vein is intestinal mucosal damage leading to air entering the venules that connect into the portal vein. This was demonstrated in an experiment where hydrogen enema was given to a dog and subsequent mesenteric venous gas was noted5. Outcomes are poor in non-trauma cases. In the absence of CT findings associated with bowel ischemia, portal venous gas due to trauma or iatrogenic causes may be treated conservatively 6 . However, blunt trauma can be varying in severity and intensity, and the likelihood of polytrauma should be considered by the treating physician.
Correct answer is option 3 - Portal vein air embolism. Portal Vein Air embolization also called HPVG ( hepatic portal vein Gas).Long arrow showing air in the left portal vein and the arrow head showing the contrast filled right portal vein.
Loss of a limb for any a reason is a major event with profound implications on the psychological health of an individual involved. It has been seen that 20-60% of the amputees attending surgical or rehabilitation clinics are assessed as being clinically depressed1-3. Individuals suffering traumatic limb loss at any age are likely to suffer subsequent difficulties with their body image, but these relationships are more striking in the younger age groups who have experienced traumatic injuries. The psychological reactions to amputation are clearly diverse and range from severe disability at one extreme; determined and effective resumption of a full and active life at other end. Indeed, among adults the age at which an individual receives the amputation is also an important factor. The investigation of psycho-social adaptation to amputation has generated a plethora of clinical and empirical studies 4-7. An amputation is typically equated with loss of once perception of wholeness 8, loss of spouse 9, symbolic castration and even death 10, 11. The individual’s response to a traumatic event is influenced by personality traits, psychiatric premorbid state, gender, peri-traumatic dissociation, prolonged disability of traumatic events, lack of social support and inadequate coping strategies 12-15. Even though the previous research on consequences of amputation has focused primarily on relationships among demographic variables, coping mechanisms, and outcome measures; there is lack of literature on prevalence of various specific psychiatric disorders post-amputation 16, 17. Most of the literature and research on prevalence of specific psychiatric morbidity has largely focused on symptoms of depression18.
To the best of our knowledge there has been very little published about the psychiatric co-morbidity in the victims of amputation. In view of paucity of studies in this field, especially due to prevailing sociopolitical disturbances in Kashmir valley (Indian administered), study of amputation and its co morbid psychiatric conditions seems crucial for planning care management of these patients. Such a study seems justified for more than one reason, as the present state of affairs is in sharp contrast to the traditional circumstances that people of valley used to live in. The aim of our current study is:
To study various socio-demographic variables of amputees.
To find prevalence of psychiatric disorders in amputees from the out-patient population of the bones and joint surgery hospital, Srinagar which also has an artificial limb rehabilitation centre attached with it.
Materials and methods:
The study was conducted in the Post Graduate Department of Orthopaedics, Govt. Medical College, Srinagar. This 200 bedded hospital is the sole orthopaedic hospital in the Kashmir valley and Ladakh and caters to the needs of all districts of the valley and Ladakh region and some areas of Jammu province. It is affiliated to Govt. Medical College, Srinagar as the teaching hospital, for both under and post graduate studies. A total of 100 patients were studied. The sample comprised of 100 consecutive cases of amputation. Patients who had an amputation were identified and diagnosed according to DSM-IV 19 lead criteria for psychiatric co morbidity. After patient consent, a detailed history was taken, and a general physical examination was performed to identify any medical problems. A detailed semi structured interview with all relevant items from MINI 20 (mini international neuro psychiatric interview) was administered to all the cases included in the study. The cases were selected on the basis of inclusion and exclusion criterion.
Inclusion criteria:
Informed consent from the patients under study
Amputation of more than one year duration
Age more than 14 years and less than 60 years
Patients were included in the study irrespective of their sex
Exclusion criteria:
Those who do not give consent
Those persons who have history of any DSM-IV axis I or axis II disorder before the development of amputation.
Presence of disabling medical or neurological conditions like motor neuron disease, Parkinson disease, etc.
Age less than 14 years
Age more than 60 years
Observations and results:
The data was categorised according to age, sex, residential address, education etc. Data obtained from the interview of the subjects was analysed and simple percentages were obtained. Besides socio-demographic profile, prevalence of psychiatric co-morbidities and reason for amputations were calculated. Results are shown in tables 1-3.
Table-1: Socio-demographic characteristics of the amputees
Characteristic
Number (n)
Percentage
Age 15-30
45
45
31-45
30
30
46-60
25
25
Sex Male
79
79
Female
21
21
Education Illiterate
61
61
Literate
39
39
Marriage Married
55
55
Un-married
45
45
Residence Rural
81
81
Urban
19
19
Occupation Domestic workers
42
42
Unskilled laborers
19
19
Students
17
17
Businessmen
16
16
Govt. employees
06
06
Religion Islam
95
95
Sikhism
03
03
Hinduism
02
02
Table-2: Indication/cause of amputation
Indication/cause
Number (n)
Percentage
Motor vehicle accident
53
53
Blast
11
11
Land mine
06
06
Fire arm injury
04
04
Others*
26
26
*The others include fall from tree, electrocution, machinery mishap, fall from hillock.
Table-3: Prevalence of psychiatric co-morbidities in amputees
Co morbidity
Number(n)
Percentage
Major depressive disorder
63
63
Post traumatic stress disorder
20
20
Impulse control disorder
19
19
Phantom limb phenomenon
14
14
Generalized anxiety disorder
10
10
Panic disorder
06
06
Sub syndromal PTSD
04
04
None
16
16
Discussion
Socio-demographic profile: In our study we found that males out-numbered females by approximately 4:1 ratio (79% males, 21% females). The majority (45%) of the amputees were males in the age group of 15-30 years, followed by 30% in the age group of 31-45 years and 25% in the age group of 46-60 years. The most likely explanation for this observation is that younger people are known to have higher exposure to the violence as compared to older people. In addition younger patient readily seek help for their psychological problems in comparison to older people. The results are consistent with the study conducted by Ebrahimzadeh et al 21 and Shukla 1 et al. Male predominance could be derived from the reason that ours is a patriarchal type of society where the men are the bread earners of the family and the women usually prefer to stay at home. Another reason could be that men report for rehabilitation and also seek help for their psychological problems more readily. Similar findings have also been reported by Cavanagh et al where they reported 75% of patients were male 22. 55% of our patients were married which could be due to the reason that majority of our sample were of adults in the marriageable age group. The findings of our study are consistent with the earlier reported studies by Margoob et al 23. We also observed that majority (81%) of our cases were from rural areas with low literacy rates. Most likely explanation for this observation is that the majority (74.9%) of the population in our state is from rural back ground. Low literacy rates is explained on the basis that most of the people who visit government hospitals of our valley are from poor background where it is very difficult for people to achieve and afford formal education. The other reason could be that Jammu & Kashmir is one of the states of India where literacy rates are low (54.46%) than average in India (65.38%) 24. Shukla et al in their study of amputees reported that majority of their patients were uneducated 1. In our study majority of the patients (95%) were Muslim. This is explained by the demographic profiles of the valley of Kashmir-Muslims are the majority community and other communities like Hinduism, Sikhism form part of minority. The greater percentage of Muslims is also substantiated because of mass exodus of minority community in early nineties with start of armed conflict in Kashmir whereby non Muslims migrated amass to different parts of the country.
Reason for amputation: In our study motor vehicle accident account for majority (53%) of the amputations. Most plausible explanations include overwhelming increase of traffic with road being in dilapidated conditions, narrow lanes, lack of driving skills by the motorists, lack of road signs and poor judgment while crossing the road by the pedestrians across the valley 25. The lawlessness and violence in valley also contribute to reckless driving and negligence of law enforcement agencies. The other collective percentage of 21% which includes 11% for blast injuries, 6% for land mine explosions and 4% for fire arm injury is significant by all means because of the ongoing sociopolitical disturbance in Kashmir since 1990s. The above findings are in accordance with high prevalence of traumatic events in Kashmir as observed by Margoob et al 23. The study revealed that 59.51% of adult men and 57.39% of women have lifetime prevalence of exposure to traumatic events.
Prevalence of psychiatric co-morbidities:The most common co morbid psychiatric condition in our study was major depressive disorder. 63% of patients were suffering from it. Our results are in accordance with the study conducted by Shukla et al (70.2%). Similar findings have also been reported by Rendal et al 3 and Kashif et al 26.In our study 40% of patients were suffering from anxiety disorders which included 20% as PTSD (Post Traumatic Stress Disorder), 4% as ssPTSD (sub syndromal PTSD), 10% as GAD (Generalized Anxiety Disorder), and 6% as panic disorder. The higher prevalence of PTSD in our study sample is because of higher rate of PTSD in this part of the world as reported in a series of studies by Margoob et al 23. The results of our study are also in agreement with those reported by Fukunishi 26 (33.9%), and Grieger et al 27. 19 % of patients in our study reported impulse control disorder in the form of crying spells and outbursts of anger. The lower prevalence of phantom phenomenon (14%) in our sample could be attributed to the fact that the time duration since amputation was variable and usually of longer duration. This is in agreement with the study by Ebrahimzadeh et al 21 where it is reported that 40% of the patients had phantom sensation and 32% were suffering from phantom pain. In another study by Lacorix et al 29, 90% had phantom sensation and 29% had phantom pain. Our observation is further substantiated by Melzack 30, Sherman et al 31, and Pezzin Et al 32 who in their respective studies reported that phantom limb sensation and pain gradually decreases with time. In our study 16% of the patients reported to have no psychiatric co morbidity. This could be due to various coping strategies adopted by the patients with primarily religious and spiritual involvement and obedience to local clergy, Imams (person who leads daily worship services at mosques) and spiritual healers 33. This observation is in agreement with the study by Margoob et al 34. In another study Huda et al 33 and Margoob et al 36 found that resorting to religious practices happens to be most often used coping method for dealing with problems and intense emotions of trauma in Kashmiri society. Similar observations have been made by studies in internally displaced people of Chechnya by Jong Kde et al 35.
In light of the above observations of our study, spreading awareness about the co-morbid psychiatric disorders in amputees can be very helpful in diagnosing and proper treatment of such cases and further to prevent chronic debilitating course associated with amputation. More intensive physical and psychiatric rehabilitation with the attention to the provision of prosthesis, retraining, and financial support packages may improve the quality of life of these patients.
Limitations of our study include a small sample size (100). Also results can’t be generalised for rest of India or Asia because of socio-political and religious practice differences.
Conclusion:
Psychiatric co-morbidities are very common in amputees in our study. Most of the patients were married males of younger age group from rural areas. The majority of the sample population comprised of unemployed people and those less educated. Major depressive disorder is the most common co-morbidity followed by anxiety disorders in which PTSD subjects were predominant followed by impulse control disorder and phantom phenomenon respectively. A significant number reported no symptoms of mental health illness.
Troponin T is a protein component of cardiac muscle. When death or damage of the myocardium occurs, it is released in to the circulation and can be detected by immunoassays 1. Troponin T is a sensitive and specific marker of myocardial damage when taken at least 12 hours after a suspected cardiac event and can be detected up to 7-10 days after myocardial damage 1,2. When used in conjunction with clinical history, electrocardiograms (ECGs) and cardiac imaging it is effective in excluding acute coronary syndrome (ACS) and myocardial infarction (MI). The cost of a Troponin T assay is £3.75 per sample inclusive of staff time.
Troponin concentrations have been incorporated in up to date definitions of acute MI. One of the criteria for diagnosis of acute MI is the detection of rise and/or fall of cardiac biomarkers (Troponin) with at least one value above the 99th percentile of the upper reference limit (URL) together with evidence of myocardial ischaemia with at least one of the following: ischaemic symptoms, new ischaemic ECG changes, pathological Q waves on ECG, or imaging suggesting loss of viable myocardium or new regional wall abnormality 3. Other criteria include unexpected cardiac death involving cardiac arrest, Troponin concentrations associated with percutaneous coronary intervention (PCI) and coronary bypass grafting (CABG) and pathological findings of acute MI 3. Troponin T is an important component of the risk stratification of patients with acute myocardial ischaemia and can be used to predict 30-day mortality 4,5.
Detection of a rise and/or fall in Troponin T concentration is important when diagnosing acute MI 3,6. It is the rise and fall that differentiates individuals who have sustained myocardial damage from other causes such as chronic kidney disease (CKD) 3, 7. In these other conditions the elevated Troponin T concentrations are sustained. To establish the diagnosis of MI, one elevated value above the decision level is required. The demonstration of a rise and/or fall in Troponin T levels assists clinicians in distinguishing elevated background Troponin T concentrations from elevations in the same patients suggestive of MI. Detection of rise and/or fall also identifies those patients with re-infarction within a short time period after an acute MI 8.
It is important to remember however that if the patient presents 24 hours after the onset of symptoms this rise and fall of Troponin T concentration is not necessary to make the diagnosis of MI. Troponin T levels must be interpreted in the light of the clinical presentation. An elevated concentration of Troponin T in the absence of clinical evidence of ischaemia should prompt a search for other aetiologies, such as CKD, congestive heart failure, myocarditis, aortic dissection, or pulmonary embolism 3, 6.
Risk stratification also includes the measurement of lipid profile in those presenting with suspected ACS or MI. To ensure that a cholesterol level representative of the patient’s normal baseline the blood sample must be organised within 24 hours of the event. In those with delayed presentation or where cholesterol is omitted on admission clinicians should wait until 3 months after the event to obtain a reliable cholesterol level, although most would be expected to have started lipid-lowering medications 9,10,11.
Method
We studied Troponin T requests made between 4pm and 7pm for a four-month period. Request cards were retrieved and the Troponin T result for each request was obtained. Any other Troponin T results obtained at any time relating to that event were noted as well as any rise and fall of the Troponin T concentrations. Review of the hospital notes for each patient established the working diagnosis, whether any other appropriate investigations had been carried out during admission, co-morbidities that were present and current relevant medications.
The final patient outcome was noted. The number of patients discharged on the same day, who would have otherwise been admitted overnight, based on Troponin T concentration was determined. Those patients with a Troponin T concentration above the 99th percentile of the upper reference limit (URL) used in the local laboratory (Troponin T <0.03ug/L) who were not discharged on the day of Troponin T measurement were identified and the reason for admission determined. The fiscal impact of the extended laboratory service was calculated.
Results
Of 162 Troponin T requests received during the four-month period, 140 (86%) were included in the study; 22 (14%) were excluded (12 haemolysed, 1 unlabelled, 2 not on computer system, 7 clinical notes unavailable).
The study population comprised of 74 (53%) male and 66 (47%) female patients. The age range was 21 – 101 years; mean (±SD) 67.6 (±16.8).
Half of Troponin T requests were received from the Acute Assessment Unit (AAU), 20% from the Emergency Department, 14% from inpatients, 8% from the Critical Care Complex (CCC) and 8% from the Coronary Care Unit (CCU).
Clinical notes indicated that 97 (69%) of Troponin T requests were taken appropriately at least 12 hours after the onset of the event, 19 (14%) were taken less than 12 hours after the event, in the remaining 24 (17%) the time of sample in relation to the event was not known. Interestingly only 30% of request cards had documented that sample was taken at least 12 hours after the event.
The indication documented on each request card is detailed in Figure 1. Indications detailed under other included: trauma, sepsis, collapse, cold & clammy, oesophageal cancer with hypercalcaemia, poor complex tachycardia, post-operative after abdominal aortic aneurysm repair, respiratory infection, sweating, palpitations, fall and repeat bleed because of previously unsuitable sample.
Figure 1: Indication noted on request card for Troponin T. ACS: acute coronary syndrome, MI: myocardial infarction, SOB: shortness of breath, LVF: left ventricular failure, CCF: congestive cardiac failure.
One hundred and two (73%) patients had a non-elevated Troponin T concentration of <0.030ug/L and 38 (27%) had an elevated Troponin T concentration >0.03ug/L. Only 5 (4%) patients had the rise and fall of Troponin T documented.
Eighty-three (59%) patients had no lipid profile measured during the attendance/admission. Of the remaining 57 patients, 31 (54%) had cholesterol assayed within 24 hours of the event, in 16 (28%) the cholesterol was taken between 2 and 17 days after the event and in 10 (18%) patients the time of cholesterol assay in relation to the event was not known. Overall only 1 in 5 patients had a lipid profile obtained within 24 hours of the event.
Interestingly of the 38 patients with raised Troponin T concentration of >0.03ug/L only 13 (34%) had a lipid profile organised. Only 7 of the 13 (54%) were obtained within 24 hours of the event, 4 were taken between 2 and 10 days after the event and in 2 patients it was not known when the lipid profile was obtained in relation to the event.
Overall no correlation was noted between cholesterol and Troponin T concentrations in all patients who had an elevated Troponin T concentration and cholesterol measured. Interestingly in those where cholesterol was measured within 24 hours of the suspected cardiac event there was some correlation, but the numbers involved were small.
The working diagnosis as stated in hospital notes is documented in Table 1.
Table 2: Reason why those patients with non-elevated Troponin T concentration of <0.03 (ug/L) were not discharged on the same day by the clinician.
Reason for admission
Number of patients
Trop T assayed <12hrs
5 (8%)
Ongoing chest pain
10 (15%)
ECG changes
3 (5%)
High CAD risk patient
2 (3%)
Monitoring and cardiology review
2 (3%)
Already inpatient
7 (10%)
Repeat attendance in 24hrs
1 (1%)
Other medical (non-cardiac) problem
28 (42%)
No reason documented
6 (9%)
Outcome not available
1 (1%)
Self discharge
2 (3%)
Total
67 (100%)
All of the 36 (26%) patients except one who were discharged on the day of Troponin T assay had a negative Troponin T concentration of <0.030ug/L. This patient had CABG one month previously and presented with chest pain and associated cough, although his Troponin T was 0.14ug/L, this was deemed not significant in view of a previous Troponin T concentration of 0.16ug/L assayed two days earlier.
Sixty three (45%) patients remained in the AAU or were admitted to a medical ward, 15 (11%) were admitted to CCU, 4 (3%) to CCC and 18 (13%) were already inpatients. Of the remaining 3 patients, 2 self-discharged and in 1 the final destination was not available.
Of those patients with a raised Troponin T concentration of >0.03ug/L 5 died during this attendance.
The majority (60/102) of patients in whom Troponin T was not raised (<0.030ug/L) still required hospital admission (Table 2). Another 6 patients with a non-elevated Troponin T concentration had no obvious reason for admission documented.
Based on an overnight stay cost of £657 we conclude that the laboratory’s extension of Troponin T service of 3 hours would save the hospital £70,956 annually. No additional manpower was required to provide the extended laboratory service as Biomedical Scientists are already providing urgent out of hour on-call service for other biochemical analysis. No additional laboratory costs were incurred, as the same number of samples would have been analysed during working hours the following day.
Discussion
There was sufficient demand for Troponin T assay to justify extension of the laboratory service for 3 hours each day. As expected most requests for Troponin T came from the AAU and the Emergency Department where the majority of patients with chest pain of potential cardiac origin would initially present. In those patients presenting with suspected myocardial damage 3 out of 4 had chest pain of non-cardiac origin.
In those patients where the time of event was known the majority had an appropriate Troponin T assay taken at least 12 hours after the event suggesting that most of the medical and nursing staff were well informed. In contrast it appears that only few of the medical profession were aware of the need to measure lipid profile soon after admission as only 1 in 5 patients had their lipid profile organised within 24 hours of the event.
The majority of requests had appropriate clinical details to justify Troponin T request. However one in four requests were deemed inappropriate (Fig. 1). Since Troponin T may be raised in other conditions the assay should be reserved for those patients where myocardial damage is suspected. Inappropriate testing is potentially hazardous and may expose patients to further unnecessary invasive investigations e.g. cardiac catheterisation with associated morbidity and mortality.
In patients presenting with chest pain, Troponin T assayed appropriately >12 hours after onset of the event can be used effectively to exclude myocardial damage and discharge can be made on the basis of this result without the need for admission. A small proportion (6%) of patients with non-elevated Troponin T concentrations who had no obvious reason for admission, were deemed unnecessary.
Dyslipidaemia plays an important role in the risk stratification of patients with suspected ACS or MI, yet only one in five patients with myocardial damage had a lipid profile organised within 24 hours of the event. Cholesterol measurements organised between 2 and 17 days after the event would not have been representative of the true concentration and were deemed inappropriate. Too few lipid profiles were assayed within 24 hours of the event in patients with an elevated Troponin T concentration to determine whether there is any correlation between cholesterol and Troponin T concentrations.
Similarly only a small number of patients had the rise and fall of Troponin T documented. The lack of serial measurements of Troponin T concentrations may have resulted in failure to recognise some patients with other conditions, which may cause elevated Troponin T concentrations and potentially subject them to unnecessary further invasive investigations.
The provision of the extended laboratory service had a positive impact; it enabled earlier discharge of patients with chest pain of non-cardiac origin, resulted in fewer unnecessary overnight hospital admissions and reduced the demand on hospital beds. Extending the service did not result in extra work for junior doctors, on the contrary by improving the efficiency of the process has not only speeded the patient journey but has improved junior doctors’ time-management.
We have shown that extending the provision of Troponin T assay for 3 hours daily has both fiscal and management benefits and reduces the number of unnecessary hospital admissions. Further extension to incorporate a 24-hour laboratory service for this assay would potentially reduce hospital admissions further with more potential savings.
Conclusion
Extending the provision of Troponin T assay for 3 hours daily has fiscal and management benefits and reduces the number of unnecessary hospital admissions of patients presenting with chest pain of non-cardiac origin.
Learning Points • Extending Troponin T service has a fiscal benefit. • Rise and fall of Troponin T values should be documented. • Lipid profile should be organised within 24 hours in all patients presenting with chest pain of potentially cardiac origin. • Measuring Troponin T where myocardial damage is not clinically suspected is potentially hazardous and may expose patients to further inappropriate and invasive investigations with associated morbidity and mortality. • In the current climate of litigation detailed documentation is necessary.
Currently, peripheral vascular disease (PVD), causing an inadequate oxygen supply to the limbs, globally affects no less than 3–10% of the population1. Peripheral vascular disease, including diabetic foot, arteriosclerosis obliterans, and thromboangitis obliterans, commonly affect the arteries supplying the leg. Based on the severity of the symptoms, usually two clinical presentations are distinguished: intermittent claudication (IC) is characterised by pain upon walking while critical limb ischaemia (CLI) is a more severe form in which pain occurs at rest and which is accompanied by necrosis and ulceration.
Peripheral arterial occlusive disease (PAOD) is estimated to develop in 500 to 1000 individuals per million persons per year2, 3. The prevalence of all stages of PAOD in the general population is estimated to be 4.2% to 35%. Within this group, 4.3% to 9.6% will experience progression of the disease towards CLI, eventually resulting in amputation of the affected limb4. Diabetic PAOD patients are at the highest risk within this patient group: they are about 10 times more likely to come to amputation, and the prevalence of gangrene is 20 to 30 times higher2. CLI has important functional implications and a major impact on the quality of life. Quality of life indices of patients with CLI have been reported to be similar to those of terminal cancer patients5. In addition, CLI is associated with surgery and hospitalisation6. CLI is also associated with increased mortality (the 1-year mortality is approximately 25% and may be as high as 45% after amputation)7 , and even asymptomatic PAOD by itself is a significant predictor of cardiovascular morbidity and death8. While obstructive atherosclerotic disease is the most common cause of PVD, some forms of vasculitis, such as thromboangiitis obliterans or Buerger’s disease, also result in peripheral ischaemia (in feet and/or hands), often progressing to tissue loss and major amputations9,10.
Unfortunately, a significant proportion of patients (including both IC and CLI cases) are not eligible for or do not beneficially respond to these revascularisation procedures due to the widespread nature or the distal location of the obstructions or due to the presence of co-morbidities putting them at higher risk for peri-procedural death.
For these ‘no-option’ patients, non-invasive revascularisation strategies have been introduced, which fall into two categories: single gene/protein-based or cell-based strategies. Angiogenic growth factor (e.g., vascular endothelial growth factor (VEGF), fibroblast growth factors (FGFs), and hepatocyte growth factor) therapy has been tested clinically since more than 5 years. But the overall benefit for PVD patients has been disappointing11.
Consequently, exploring new strategies for revascularisation of ischaemic limbs is of major importance.
What are stem cells?
Stem cells are defined as a cell population capable of self-renewal, proliferation and differentiation. They serve as a repair system for the body.
Stem cells are classified into two different types during the development of the organism: embryonic stem cells and adult stem cells (ASCs).
The use of adult stem cells in research and therapy is not as controversial as embryonic stem cells, because the production of ASC does not require the destruction of an embryo. Additionally, because in some instances ASC can be obtained from the intended recipient, (an autograft) the risk of rejection is essentially non-existent in these situations.
Where are adult stem cells found, and what do they normally do?
Adult stem cells (ASCs) have been identified in many organs and tissues, including brain, bone marrow, peripheral blood, blood vessels, skeletal muscle, skin, teeth, heart, gut, liver, ovarian epithelium, and testis. In HYPERLINK "http://en.wikipedia.org/wiki/Adult" \o "Adult"adult organisms, stem cells and HYPERLINK "http://en.wikipedia.org/wiki/Progenitor_cell" \o "Progenitor cell"progenitor cells act as a repair system for the body, replenishing specialised cells, but also maintain the normal turnover of regenerative organs, such as blood, skin or intestinal tissues. They are thought to reside in a specific area of each tissue (called a "stem cell niche"). In many tissues, current evidence suggests that some types of stem cells are pericytes, cells that compose the outermost layer of small blood vessels. Stem cells may remain quiescent (non-dividing) for long periods of time until they are activated by a normal need for more cells to maintain tissues, or by disease or tissue injury.
The concept of stem cell based revascularisation emerged in 1997, when Isner’s group described circulating cells in adults called endothelial progenitor cells (EPC) with the capacity to differentiate into endothelial cells (EC) and incorporate into new vessels in ischaemic tissue12. Since then, the number of studies reporting on stem cell related revascularisation has exponentially increased. Bone marrow (BM) derived stem cells have been identified as a potential new therapeutic target. Most adult stem cells are lineage-restricted (multipotent) and are generally referred to by their tissue origin for example: mesenchymal stem cell, adipose-derived stem cell, endothelial stem cell etc13, 14.
In the 1950s, researchers discovered that the bone marrow contains at least two kinds of stem cells. One population, called hematopoietic stem cells, forms all the different types of blood cells in the body. A second population, called bone marrow stromal stem cells (also called mesenchymal stem cells, or skeletal stem cells by some), were discovered a few years later. These non-hematopoietic stem cells make up a small proportion of the stromal cell population in the bone marrow, and can generate bone, cartilage, fat, cells that support the formation of blood, and fibrous connective tissue.
Adult stem cell treatments have been successfully used for many years to treat leukaemia and related bone/blood cancers through bone marrow transplant15.
Relationship between neoangiogenesis and cell population.
Neoangiogenesis:
Three concepts of vascular growth have been described to date—angiogenesis, vasculogenesis, and arteriogenesis (collateral artery growth)—which represent different aspects of an integrated process. Stimulation of arteriogenesis seems clinically most relevant and has most recently been attempted using autologous bone marrow transplantation with some beneficial results, although the mechanism of action is not completely understood.
Cell population:
Hematopoietic stem cells may be CD34+ AC133+ or CD34- AC133+ or CD34+ AC133-. Vascular development is regulated by growth factors and their receptors such as vascular endothelial growth factor (VEGF) and VEGF tyrosine kinase receptors such as VEGFR-1 (flt-1) or VEGFR-2 (KDR or flk-1). Other growth factors such as angiopoietin-1 that bind a tyrosine kinase receptor Tie-2 may be involved in completing the vascular architecture by assembling pericytes and smooth muscle cells around endothelial cells16.
Marrow or peripheral blood CD34+ hematopoietic stem cells express VEGFR and Tie.12 When cultured ex-vivo in fibronectin-coated flasks with VEGF, CD34+ AC133+ cells differentiate into endothelial cells by morphology, acetylated low-density lipoprotein incorporation, nitric oxide release, Von Willebrand factor expression, and lectin binding17.
The unfractionated mixture of hematopoietic mononuclear cells includes more differentiated cells that are thought to provide angiogenic cytokines as well as stem cells that become incorporated into collateral vessels by a process of neoangiogenesis. In clinical trials, Tateishi-Yuyama et al.18 injected autologous bone marrow mononuclear cells into patients with ischaemic PVD. Patients were selected for chronic ischaemic extremity pain or non-healing ischaemic ulcers or both and a resting blood pressure ankle-brachial index less than 0.6. Bone marrow cells were collected under general anaesthesia from the posterior superior iliac crest and with a 26-gauge needle injected into the gastrocnemius muscle of the ischaemic leg in multiple sites divided by a 3x3 cm grid. Significant improvement in the ABI, trans-cutaneous oxygen pressure, and pain-free walking occurred following treatment18.
Several independent clinical studies have reported beneficial effects of the administration of bone marrow mononuclear cells (BM-MNC), Granulocyte Colony Stimulating Factor (G-CSF) mobilised Peripheral Blood Mononuclear Cells (PB-MNC), G-CSF-mobilised PB-MNC after ex vivo culturing, G-CSF mobilised CD34+ cells, and G-CSF mobilised CD133+ cells in patients with CLI. However, no direct comparisons have been performed and it is still unclear which cell types or subpopulations provide the best treatment results. The progenitor cells specifically involved in vascular repair and neovascularisation were initially thought to originate from the CD34+ hematopoietic progenitor cell population, analogous to the common hemangioblast precursor in embryonic development19, 20.
Consistently, in the Therapeutic Angiogenesis using Cell Transplantation (TACT) study, legs that were injected with PB-MNC, containing approximately 500-fold less CD34+ cells than BM-MNC, showed much smaller increases in collateral perfusion as compared with BM-MNC-injected legs.18,21 Furthermore, Saigawa et al demonstrated a correlation between the number of implanted CD34+ cells and the efficacy of bone marrow implantation21.
However, several studies suggest that CD34- cell populations also play an important role in the beneficial effects of BM cell therapy. Asahara et al already showed that CD34- cells, added to CD34+ cells in culture, improved outgrowth of cells with an endothelial phenotype12. Co-culture of CD34+ cells with CD34-cells in an in-vitro 3-D matrix model using human microvascular endothelial cells significantly enhanced neovascularisation as compared with CD34+ cells alone22.Other groups described that non-hematopoietic bone marrow mesenchymal precursor cells and myeloid/monocyte lineage cells (CD14+) can also differentiate into EPC or into cells with EPC characteristics23-26. Iba et al compared the angiogenic effects of the same numbers of BM-MNC and PB-MNC (containing 2.4% and 0.02% CD34+ cells, respectively) in a rat hind limb ischaemia model and showed that although there was no incorporation of PB-MNC, the angiogenic effect of PB-MNC was approximately 72% relative to that of BM-MNC27. Moreover, Tateno et al showed that there was no significant difference in stimulation of neovascularisation after infusion of PB-MNC and BM-MNC10.
These data suggest that, apart from incorporation of EPC, EPC supply of angiogenic factors such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor, and angiopoietin-1 plays an important role. This role of the paracrine effects of EPC on vascular growth have also been demonstrated by the group of Schaper28, 29.
A recent report proposed that implanted cells stimulate muscle cells to produce angiogenic factors, thereby promoting neovascularisation10. Yang and co-workers reported a simple and effective therapeutic approach for diabetic limb ischaemia by autologous transplantation of G-CSF -mobilised peripheral blood stem cells30.
Thus, different cell populations are involved in vascular repair and neovascularisation, and these cells may act via direct incorporation into the endothelial layer and endothelial differentiation, by supply of angiogenic factors, or by a combination of both31.
The majority of studies on cell therapy for CLI have used whole MNC fractions and at this moment it is unclear whether administration of more selected cell populations or ex-vivo culture toward an endothelial phenotype would be more effective.
Although clinical studies showed promising results from both BM-MNC and G-CSF-mobilized PB-MNC, recent data suggest that functional activity of the G-CSF mobilised cells, as assessed by the migratory response to VEGF and stromal cell-derived factor1, is significantly reduced as compared with non-mobilised cells from the same patient. Also in in-vivo experiments in nude mice with hind limb ischaemia, G-CSF-mobilised EPC show a reduced capacity to augment blood flow recovery and to prevent necrosis as compared with the same EPC without G-CSF stimulation32.
It is important to note that cell isolation protocols may also have a major impact on the functional activity of BM-derived progenitor cells33.
Optimal Dosage
It is remarkable that all studies discussed above reportfavourable outcome, despite varying dosages, with an even so varying concentration of CD34+ cells. In the studies involving BM cell administration, amounts of aspiratedBM cell ranging from 80 to 1000 ml, from which theinjected dosage of progenitor cells was retrieved, were reported.In the TACT Study18 and in the study by Higashi etal.34 approximately 1.6x 109 MNC were obtained from 500ml of BM, whereas Durdu et al.9 retrieved a 50-fold of MNCfrom the same amount of BM (101x109 MNC from 653 mlof BM). Bartsch et al.35 separated a 2.5 times smaller amountof MNC from the same amount of BM (0.1x109 MNC from80 ml of BM). The fraction of CD34+ cells in the isolatedMNC population varies from 0.6% in the study by Kajiguchiet al.36 to 2.4% in the TACT study18.
Clinical Evaluation
Currently used measures for clinical evaluation, such as ankle-brachial pressure index, are subject to factors other than improvements in perfusion alone. In accordance with the Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC-II) recommendations, future trials should ideally combine multiple measures for clinical improvement and quantification of the arterial flow to evaluate treatment success, which include ankle pressure, toe pressures, TcPO2, microcirculation investigation methods like laser Doppler fluxometry, and anatomic imaging1.
In addition, questionnaires addressing pain experience, pain “magnitude” (pain intensity, emotion, cognitive-evaluative, and sensitivity) and pain at rest (on a visual analogue scale), as well as quality of life questionnaires will provide patient-based parameters for the clinical effects of therapy.
Ulcer status should be assessed by measurement of the cumulative total ulcer area, with ulcer healing defined as healing of all ulcers of the treated leg. Limb status can be assessed using the criteria of Rutherford37.
Contrast-enhanced high spatial resolution magnetic resonance angiography is a reproducible and robust modality for assessment and quantification of new vessel formation, detecting different sizes of collateral vessels, and determination of (changes in) tissue perfusion.
However, Choksy and Chan38 pointed out that a major scientific weakness in angiogenesis research lies in the assessment of vascular growth.
Avenues to explore?
How do adult stem cells evolve during development and how are they maintained in the adult? Are they "leftover" embryonic stem cells, or do they arise in some other way?
If the beneficial effect of adult stem cell transplantation is a trophic effect, what are the mechanisms?
What are the factors that control adult stem cell proliferation and differentiation?
What are the factors that stimulate stem cells to relocate to sites of injury or damage, and how can this process be enhanced for better healing in PVD?
Why do stem cells remain in an undifferentiated state when all the cells around them have differentiated? What are the characteristics of their “niche” that controls their behaviour?
How can assessment of neo-angiogenesis be improved?
Conclusion
Clearly, stem cell safety must be scrutinised and assessed throughout the entire treatment or research process. Guidelines and strategies must also be developed to ensure that every aspect of stem cell use - from identification and isolation of stem cells to stem cell transplant - is stringently coordinated.
Although several clinical studies show promising results, larger randomised, blinded, placebo-controlled trials are needed to provide definite proof of the clinical effects of adult stem cell therapy in these patients. In addition, questions regarding the cell population(s) to be used, optimal dose, and routes of administration will have to be addressed. If doctors and scientists can establish safe protocols for stem cell use, everyone can benefit from the full potential of the remarkable and possibly life-saving stem cell therapies.
‘Munchausen Syndrome by Proxy’ (MSBP) was first described by Meadow in 1977 1, as a form of child abuse in which the caregiver (generally the mother) causes or simulates illness in the child for psychological gain. Three features are required for diagnosis: 1. The history, signs and symptoms of disease are not credible; 2.The child is receiving unnecessary and harmful, or potentially harmful, medical care; 3. If so, caregivers are instrumental in instigating the evaluations and treatment 2. As has been emphasized, the motivation of the mother (her psychological needs), is important in distinguishing MSBP from other forms of Paediatric Condition Falsification (PCF) 3. Initial reports described young children with acute, life-threatening events, such as sleep apnoea, epilepsy, diarrhoea, or bowel obstruction 4,5. Sudden Infant Death Syndrome (SIDS) has an ominous association with MSBS which has survived controversy 6-9. MSBP has been reported in children in learning disability settings;10 whereas there have been few, if any, reports in general child psychiatry. Causal factors for this may be that it is perceived to be less exciting, of a multi-disciplinary nature, and, arguably, due to more humdrum circumstances which surround it. Initial descriptions, indeed, required that the child present with organic symptoms 11. Psychiatric presentations may be more difficult to detect because of the paucity of objective diagnostic tests, with the consequent greater reliance on the history provided by caregivers. Caregivers who simulate school refusal in their children have been considered not to have MSB 12, (though they do show PCF). The exclusion of psychiatric presentations is noteworthy, because such psychiatric presentations may differ in important ways from the typical, dramatic, presentations seen in very young children. Since psychiatric diagnosis in children is so dependent upon parental history, such cases may also be more difficult to detect, and therefore more common than previously thought. Three cases are described here, which, though typical of MSBP in many ways, differ in their psychiatric symptoms, in their age, and in the prominence of school refusal.
Cases
Case X
This girl was born at 37 weeks gestation by emergency caesarean section because of a slowing of the foetal heart rate. She was the eldest of 4 children. Her father was severely disabled with a chronic degenerative disease. No distress was evident at birth, but she had short stature (3rd centile for height and weight). At 9 years of age, she presented to a Child & Adolescent Mental Health service with low self-esteem and an eating problem. Her parents attributed this to bullying at school, which, the mother told doctors in a subsequent interview, took place when the child was 7, and was characterised by beatings so severe as to leave her with multiple bruises, and ‘a voice which changed following this trauma’.
The girl was found to have an IQ in the borderline range. Her mother reported that she had 'allergies to milk and eggs'. At another interview she said the allergy was to ‘shellfish and nuts’, and that it had been discovered when she developed an anaphylactic reaction in another country at 18 months of age. The mother also claimed that eczema was diagnosed at that time. Her diet was restricted, and her mother commented that she 'needed to buy special foods', and that 'asthma developed at age 7'. The child was found to be unhappy, but not depressed. There was no evidence of weight loss, but an eating disorder was diagnosed on the basis of maternal reports.
X’s brother had been diagnosed as having ADHD, and was prescribed psychostimulants. Aggression and odd behaviour had given rise to suspicion of an autism spectrum disorder. After a number of assessments, no diagnosis was made. Compliance with medication was a problem, the mother claiming that, although she personally administered tablets, he had somehow avoided swallowing them, and adduced this as a reason for their lack of efficacy. The mother later reported that 'he was doing extremely well off all treatment'.
The mother expressed dissatisfaction with the attention and care her daughter had received from one service. However, a letter, written shortly afterwards, gives an insight into her personality, and the relationship which had developed with professionals. She wrote: ‘I did not realise I was so overpowering towards you all... I only feel constant pain & hurt at what has happened to our daughter. Let me know if you do not want to see us anymore.’
It was at this point that the ability of the parents to care for their children was questioned, when it was discovered that the mother had been leaving the children unsupervised overnight, so that she could help with a scout camp (with which none of her own children were involved). School authorities were also alarmed that the children were left unsupervised for long periods before school opening, and that they arrived hungry and dishevelled. The mother opposed involvement by social services, and, in the absence of any formal complaint, they were not notified.
Unhappy with the treatment she received from her psychiatrist, the mother sought a second opinion. To this doctor, the mother reported that there had been an increase in frequency of nocturnal enuresis at 7 years. She reported that her daughter was happy at school, but that there were problems at home. She reported that her daughter was 'unable to swallow solid food'; she was 'able to take liquidised food only', and 'she became increasingly anxious about solids'. The mother said she had contacted the Anorexia Nervosa Society ‘who advised she had a phobia about food'. The mother reported that when she gradually re-introduced solids, eating recovered and that appetite returned.
At 14 years, X’s mother told a paediatrician that her problems started at age 7, when she had been bullied by several children in the class. This doctor found her to have constitutional short stature. No allergies were reported or found. The mother resisted attempts to obtain copies of previous medical records. A neurologist found 'no evidence of regression'. The mother quoted a paediatrician to another professional as having said, 'It would be disastrous for her if she had a period', and she told another paediatrician that the referring doctor had said she was being referred, 'to sort out her psychological problems immediately’. She was referred to a third child psychiatrist, who found low mood, social withdrawal, and 'recent adjustment problems'. She was then referred again to local psychiatric services for follow-up. At this stage, her mother wrote: '... it is now confirmed that her short stature has a psychological basis, and that this started at 6 years of age because of bullying'.
At her mother’s insistence, X was seen then by another psychiatrist, ‘to discover the psychological cause of her short stature’. No psychopathology was found. Mother declared that she was ‘astounded’ and demanded to know how the doctor could explain ‘the dramatic fall in IQ which had taken place at age 10’.
By the time of referral to social services, the child had been seen by 3 paediatricians, 4 psychiatrists, and numerous other mental health professionals.
Case Y
This boy was born without complication, developing normally up to middle childhood. When he was 3 years old, a younger sister was born. She died at the age of 3 months, and a coroner's verdict of SIDS was returned. His mother experienced a pathological grief reaction.
The family holidayed abroad periodically; such trips were frequently marked by attendance at the A&E department of the local hospital, where the boy presented with sundry somatic complaints. There were occasional brief hospitalisations, but no physical abnormality was ever diagnosed.
The child’s mother made several unsubstantiated allegations of bullying at school. His father disputed these, though he did not oppose them. Thorough investigation failed to substantiate any such episode. The father complained to doctors of his powerlessness in the face of his wife's over-protective, domineering approach; he recognised the harmful effect this was having on their son.
Whereas the mother complained that her son had 'loss of interest', 'poor concentration', was ‘not eating', and had suffered weight loss; the boy told doctors, 'I'm good at school'; and 'I'm always happy with my friends'.
His mother had a benign brain tumour, which had presented initially with epilepsy when she was in her teens, but was well controlled. During her mid-40’s, she presented frequently with pseudo-seizures and other odd neurological symptoms. To each doctor she met, she presented herself has having a 'terminal brain tumour'. She told her neurologist that she was 'distancing herself from her son’, as she was ‘going to die soon’, and ‘he would have to be tough enough to get on without her'.
On one occasion, when brought to hospital because of suicidal ideation, Y commented that ‘school was good’, and that he had ‘a few good friends’. He listed a few favourite subjects, and responded appropriately to wishes about the future. The conclusion was that he was euthymic. Notwithstanding his reports to doctors, he was kept at home for prolonged periods because of 'bullying'. The mother claimed that her husband 'can be abusive to the child when angry', though the impression of numerous psychiatrists was that he had a passive, dependent personality. He begged professionals for help in protecting his child, and when a referral to social services was eventually made, he was profuse in his gratitude.
Case Z
This boy's monozygotic twin brother presented to a private psychiatrist at 1 ½ years of age with 'behavioural problems', and a diagnosis of autism was made. No standard observational assessments were performed, nor neurodevelopmental history taken. He was referred to specialist autism services, who found no abnormality following a multi-disciplinary assessment. When the twins were 7 years of age, the mother brought the other twin, Z, to community child psychiatric services with vague concerns regarding 'development' and 'social skills'. By this she meant that he '[had eaten] his food off the floor when he was younger', and that he currently 'behaved in a silly, immature way'. She said that 'teachers complained of disruption', and she, in turn, complained of poor cooperation from the school. Independent contact with the school disclosed no such behavioural concerns. Her husband spent most nights away on business, and the twins slept in her bed. They 'would not settle for hours' and she 'had to sing to get them to sleep'.
His mother had been treated for depression in the past. She reported that she had given up her job in order to look after her children, whom she felt had 'special needs'.
At clinical interview she was extremely reluctant to leave her son, and her prolonged departure from the room was accompanied by exaggerated displays of affection, which clearly embarrassed her son. He, on the other hand, separated easily. On his own, he was initially reserved, but became talkative and happy when discussing his friends, school, interests, etc. There was no evidence of any autistic-type disorder, nor indeed any other psychiatric problem.
At the time of writing, she has refused to accept the assurances of two different services that there was nothing wrong with her son, and she was continuing with attempts to have him re-assessed.
Discussion
All three of these children presented with complaints from mothers, which, while perhaps credible in isolation, became more and more far-fetched when viewed together as a whole. In all cases harm resulted to the child from excessive investigation, social isolation, and absence from school. In all cases, mothers had narcissistic personality problems, and fathers had a subordinate role (one because of chronic illness, another because of a dependent personality). All children had siblings with dubious or unexplained illness. All cases involved many physicians and allied professionals, who became involved in what transpired to be, when they started to communicate with one another, a pattern of simulated illnesses and symptoms. There was a general reluctance to refer to social services, and a delay in their involvement, perhaps because of the absence of acute or marked abuse, and because the caregivers seemed the opposite of the 'typical' negligent, abusive mother. These children were somewhat older than most cases of factitious disorder by proxy, who also differ in presenting with acute, life-threatening events or surgical emergencies. Although probably less lethal, psychiatric presentations may offer more scope for abuse, due to the greater reliance on parental reports in child psychiatry. Unwitting collusion by schools, in part caused by an understandable sensitivity to bullying allegations, may have facilitated presentation to psychiatric services.
Most cases of MSBP have emerged from the U.S. The phrase ‘Psychological needs’ has been emphasised, and suggests vagueness, an impression strengthened by the initial psychodynamic terms in which these case were couched. It may be a useful term, nonetheless, in that it distinguishes motivations such as revenge, delusions, or poverty, from those in which the perpetrator behaves in this way to, for example, fool doctors or exhibit herself as an ideal parent 13. Schreier and Libow 14 suggested that a key psychological factor may be an ingratiating relationship which the mother pursues with the child's physician, who tends to be male, isolated, and idealistic. The preponderance of mothers among perpetrators may be due to a satisfaction obtained by deceiving ‘authority’ or ‘power’ figures, but this (and any other explanation) has not yet been substantiated. Such manipulation was not present in any of these three cases. This may be due to the central role which the family doctor retains in many other countries, and to the multi-disciplinary nature of health care, particularly mental health services, in other health systems, which precludes the doctor from seeming a ‘hero figure’.
‘Munchausen Syndrome by Proxy’ is clearly not a disease, and can be considered a disorder only by analogy. This, as well as the general tendency in medicine to abandon eponymous diagnostic labels, argues for use of the term ‘Paediatric Condition Falsification’, preferred by the American Professional Society on the Abuse of Children (APSAC) 15; or ‘Factitious Disorder by Proxy’, as preferred by the Diagnostic & Statistical Manual of Mental Disorders (DSM) 16. Notwithstanding these compelling reasons, the radically different profile of the ‘caring mother’, in cases like those under discussion, make it essential to distinguish the situation described in this case series from other circumstances in which mothers harm children. The mother’s motivation is crucial if the child is to be protected: specific remedies in other circumstances may offer hope of an amelioration, but the rate of recidivism in ‘Munchausen Syndrome by Proxy’ 17,18, means that these children will require vigilance and protection for as long as they are in contact with their mother.
It is important to consider how these episodes might have been detected earlier. Good history-taking would have revealed the falsehood of an allergy to dairy products in the first case. A higher index of suspicion might have led to greater communication, and better detection, among disparate professionals as in the case of Munchausen Syndrome in adults. Formal channels for reporting concerns without fear of recrimination could be established in hospitals and out-patient settings. Greater institutional support for healthcare workers with concerns, as well as broader awareness among family doctors, nurses, psychologists, and social workers, is a prerequisite. In medical presentations, a bizarre, inconsistent history, a failure to cooperate with attempts to obtain medical records, features of a maternal histrionic or narcissistic personality, and any history of abuse towards other siblings, should raise the alarm. These apply also in the case of psychiatric presentations. In medical presentations, abuse can be detected by observing ‘recovery’ of the child when removed from the parent’s reach. The chronicity and gradual nature of psychiatric symptoms make these cases appear less dramatic, and such a ‘test’ impractical, but certain other features may help. Unconvincing reports of bullying at school, despite thorough investigation, poor school attendance without an adequate explanation, and an incongruity between maternal reports and the child’s mental state, may all be helpful.
Conclusion
Reports of Psychiatric presentations of Paediatric Symptom Falsification are rare, but there are good reasons for suspecting that the true incidence may be higher. Psychiatric presentations are probably not typical of Paediatric Symptom Falsification, and may for this reason be missed. Experience shows that reporting to child protection agencies is essential, but this is difficult and tends to be avoided for various reasons. There is a need for education of mental health and allied professionals in this condition so that much suffering of children can be avoided. Paediatric Symptom Falsification involves psychological problems in the caregiver (generally the mother), which are very difficult to manage. These require understanding and compassion, but should not be a barrier to protecting the child.
The authors declare that they have no conflict of interest.
The legal high ‘Ivory Wave’, also known as ‘Ivory Coast’, ‘Purple Wave’ or ‘Vanilla Sky’, is a designer drug that has become popular among clubbers in the United Kingdom (UK) after mephedrone was banned in April 2010.1 Ivory Wave is advertised as a relaxing bath salt and has been freely available on the Internet for about £15 a packet (200mg).2 Three different versions have been on the market, namely, Ivory Wave, Ivory Wave Ultra (also known as Ivory Wave 2), and Ivory Wave 3, although their differences are unknown.3 Studies have shown that Ivory Wave contains cathinone-derived stimulants and, when snorted in high doses, bring similar effects to those of amphetamine and ecstasy.4
Recently, clusters of hospital admissions have been reported around the UK following the use of Ivory Wave. The majority of patients were described to have ‘acute paranoid psychosis’ with severe agitation, which wore off after a couple of days.5 However, some patients had more serious physical complications and had to be monitored in the coronary care units for up to 12 hours.2, 5
Following the increase in the number of Accident and Emergency (A&E) admissions relating to Ivory Wave, healthcare professionals have expressed their concerns about the harmful effects of the substance. The Department of Health has issued advice on handling the users who may present to health services for help.6 However, the literature is limited on the physical and psychological effects of the substance at present. Therefore, we report our case here to describe some of the clinical features of Ivory Wave misuse.
Case presentation
A 26-year-old Caucasian male, with a background history of obsessive-compulsive disorder (OCD) and depression, attended an Accident A&E after snorting approximately 700mg of ‘Ivory Wave Version 3’ in a day. He presented with severe agitation, persecutory delusions, and auditory and visual hallucinations. He stated that ‘people’ were trying to kill him and his mother with a knife, and he could hear their voices threatening to kill him. He also complained of mild/moderate breathing difficulty and involuntary movements of his arms and feet.
In recent years he had been ‘experimenting’ with several legal highs, including Ivory Wave, ‘Charge’ and ‘Mojo’. Five weeks prior to this admission he had visited A&E with a similar presentation, but without persecutory delusions, after sniffing an unknown amount of ‘Ivory Wave 2’. The hallucinations shortly disappeared and he was discharged home.
Otherwise, he was physically fit and well. He had a long history of severe OCD with borderline psychotic features/social anxiety where he was consistently worried about what other people may do to him. There was no personal or family history of psychosis. He was taking clomipramine (125mg) and olanzapine (12.5mg) for OCD and depression but his compliance had been erratic before the admission.
In the present admission he was very agitated and restless. He had non-goal-directed involuntary movements on both arms and feet: repetitive flexion of his elbows and dorsiflexion of his ankles. The physical examination showed that he was pyrexial with a temperature of 37.9°C and had bilaterally dilated pupils. The respiratory examination was normal with an oxygen saturation of 98% on air. The heart rate was slightly fast at 109 beats per minute (bpm) and blood pressure was 122/82 mmHg. The rest of examination was unremarkable with a normal electrocardiogram (ECG). Laboratory investigations revealed a raised white blood cell (WBC) count of 23.5 ´ 109/L and C-reactive protein (CRP) of 332 mg/L. He also had hyponatraemia (Na+ 126 mmol/L) and elevated creatinine kinase (CK = 662 iu/L). Urine drug screen was negative to amphetamine, opiates, cannabinoids and cocaine.
Initially the patient was admitted to a medical ward and commenced on normal saline with intravenous antibiotics (co-amoxiclav) because of the raised inflammatory markers. The body temperature, CRP, and WBC count fell gradually; the CK level dropped as well. The blood culture came back negative. However, the patient remained agitated, was running around the ward, and experiencing visual and auditory hallucinations. He required PRN lorazepam and regular diazepam.
On day five of admission the patient was deemed medically fit and discharged from the medical ward. However, he was still agitated and confused about what had happened. Concerns were raised regarding his mental state, given his past psychiatric history and current problems. A Mental Health Act assessment was performed and the patient was admitted to a psychiatric unit under Section 2 of Mental Health Act 1983 on the same day.
On admission to the unit the persecutory delusions and hallucinations were still present but to a mild degree. The involuntary movements appeared more like muscle twitches, which occurred less frequently. He was observed on the ward and only PRN lorazepam was prescribed together with his regular medication. He then settled on the ward and did not require any further PRN medication.
After a few days the persecutory delusions and hallucinations wore off. The involuntary movements had stopped but left patches of numbness on his right arm, mainly on his fingers. The area was poorly defined and was not localized to a specific dermatome. The numbness disappeared after a few days without any complications.
The patient remained in the psychiatric unit for two weeks before discharge to the care of the Community Mental Health Team (CMHT).
Discussion
The exact components of Ivory Wave are unclear and thought to be variable.4 , 7 Studies have shown that the main ingredients include MDPV (3,4-methylenedioxypyrovalerone); desoxypipradrol, also known as 2-diphenylmethylpiperidine (2-DPMP); and lidocaine.7, 8. 9 MDPV and desoxypipradrol are both synthetic stimulants. MDPV was first synthesized in 196910 and is found as a white or light tan powder.4 Desoxypipradrol was initially developed by a pharmaceutical company in the 1950s as a treatment for Attention Deficit Hyperactivity Disorder (ADHD) and narcolepsy, but it was replaced by other related substances.8 They both act as noradrenaline and dopamine reuptake inhibitors and their effects are thought to be similar to those of amphetamine and cocaine in high doses.9, 11, 12
Ivory Wave is known to bring on several desired effects, including increased energy and sociability, increased concentration, and sexual stimulation. There are also many physical and psychological unwanted effects reported including insomnia, severe agitation/anxiety, panic attacks, kidney pain, stomach cramps, tachycardia, hypertension, dilated pupils, headache, tinnitus, skin prickles and numbness, dizziness, and dyspnoea.4, 13 These effects appear highly dose-dependent4 and have been based on self-reports made by users on online forums.
In the UK there have been several media reports of hospital admissions related to Ivory Wave. The majority of patients were described to have acute psychotic symptoms, namely paranoid delusions, and auditory and/or visual hallucinations. A few of them had physical complications, requiring cardiac monitoring in ICU.1, 2, 5 However, no detailed description of their clinical features were available.
In this case report, we have described chronologically the clinical features of a patient, who presented to A&E after taking Ivory Wave. The patient had a similar presentation to what it was described by Paolo Deluca and his colleagues.4 The patient also experienced involuntary movements in his limbs which has not been reported before in the literature. We have also reported the blood test results: raised inflammatory markers (WCC and CRP) and CK.
The findings from this case, in combination with the limited literature, suggest that the use of ‘Ivory Wave’ can lead to serious complications including over-stimulation of the cardiovascular and nervous system, hyperthermia, and acute psychosis which can potentially result in severe illnesses or even death. The risk of these effects would be greater if the drug was combined with other recreational drugs or alcohol. In addition, the exact composition and strength of the substance may vary and users may not be completely aware of what chemicals they are consuming. This implies that users of Ivory Wave may to taking potentially dangerous substances with unknown effects.
In April 2010, MDPV was made a Class B drug in the UK together with other cathinone derivatives. In addition the UK Home Office has recently announced a ban on the import of desoxypipradrol and any products containing the chemical.15 The use and availability of Ivory Wave in the UK is being closely monitored and may result in further legislative review. Changes in legislation, more research studies, and health education on Ivory Wave could help the public to realize that, irrespective of the legal status of a drug, recreational use of substances may pose a significant risk to their health.
Irritable bowel syndrome (IBS) is a common disorder characterized by abdominal pain and altered bowel habit for at least three months.(1)
IBS is further defined depending on the predominant bowel symptom: IBS with constipation (IBS-C) or IBS with diarrhoea (IBS-D). Those not classified as either IBS-C or IBS-D are considered as mixed IBS (IBS-M). Alternating IBS (IBS-A) defines patients whose bowel habits oscillate from diarrhoea to constipation and vice versa.
IBS is a prevalent and expensive condition that is associated with a significantly impaired health-related quality of life (HRQOL) and reduced work productivity. IBS care consumes over $ 20 billion in both direct and indirect expenditures. Moreover, patients with IBS consume over 50% more health care resources than matched controls without IBS.(1)Based on strict criteria, 7 – 10 % of people have IBS worldwide. Community-based data indicate that diarrhoea-predominant IBS (IBS-D) and mixed IBS (IBS-M) subtypes are more prevalent than constipation-predominant IBS (IBS-C), and that switching among subtype groups may occur. IBS is 1.5 times more common in women than in men, is more common in lower socioeconomic groups, and is more commonly diagnosed
in patients younger than 50 years of age. Prevalence estimates of IBS range from 1 % to more than 20% in North America(7%).(1)In Asia the prevalence is about 5%.(3,4,5)Recently, a School-Based Study in chinareportedthe prevalence of IBS in adolescents and children was 13.25% and the ratio of boys to girls was 1:1.8.(6)Most patient with IBS in India are middle-aged men (mean age 39.4 years).(7)
Underlying pathophysiology:
Given the lack of definitive organic markers for IBS, the absence of aconsolidatedhypothesis regarding its underlying pathophysiology is not surprising. Nevertheless, important advances in research made during the past 50 years have brought us closer than ever to understanding the numerous existing aetiological factors involved in this multifaceted disorder, including environmental factors, genetic factors, previous infection, food intolerance, and abnormal serotonergic signaling in the GI tract.
Environmental factors:
The biopsychosocial model proposed by Engel(8)takes into account the interplay between biologic, psychological, and social factors. This model proposes that there is an underlying biologic predisposition for IBS that may be acted on by environmental factors and psychological stressors, which contribute to disease development, the patient's perception of illness, and impact on treatment outcomes. Different studies have shown that stress can result in release of stress-related hormones that affect colonic sensorimotor function (eg, corticotropin-releasing factor [CRF] and inflammatory mediators [eg, interleukin (IL)-1]), leading to inflammation and altering GI motility and sensation.
Genetics factors :
Twin studies have shown that IBS is twice as prevalent in monozygotic twins than in dizygotic twins.(9,10,11)IBS may be associated with selected gene polymorphisms, including those in IL-10, G-protein GNb3, alpha adrenoceptor, and serotonin reuptake transporter (SERT).
Post-infectious IBS (PI-IBS):
Culture positive gastroenteritis is a very strong risk factor for IBS. Different prospective studies show IBS symptoms developed in 7% to 32% of patients after they recovered from bacterial gastroenteritis.(12,13,14)Specific risk factors for the development of PI-IBS have been identified, including younger age, female sex, presence of severe infectious gastroenteritis for a prolonged period, use of antibiotics to treat this infection, and presence of concomitant psychological disorders (eg, anxiety).(12,13,15,16)
Small Intestinal bacterial overgrowth
Pimentel and colleagues(17,18)have shown that, when measured by the lactose hydrogen breath test (LHBT), small intestinal bacterial overgrowth (SIBO) has been detected in 78% to 84% of patients with IBS. Hence, a higher than usual population of bacteria in the small intestine has been proposed as a potential aetiological factor in IBS. While another study involving a review for the presence of gastrointestinal-related symptoms (including IBS) has shown that asensitivity of the LHBT for SIBO has been shown to be as low as 16.7%, and specificity approximately 70% and the test alone for small intestinal bacterial overgrowth were poor. Hence, combination with scintigraphy resulted in 100% specificity to assess the treatment responce, because double peaks in serial breath hydrogen concentrations may occur as a result of lactulose fermentation by cecal bacteria. (19,20)
Food intolerance :
Approximately 60% of IBS patients believe and different studies show that allergy to certain foods could trigger IBS symptoms. Recent research involving exclusion of foods patients had immunoglobulin (Ig) G antibodies, which are associated with a more delayed response after antigen exposure than IgE antibodies, resulted in significantly better symptom improvement than in patients in the non-exclusion group.(21)
Serotonin signaling in Gastrointestinal (GI) tract:
Normal gut physiology is predicated to be an interaction between the GI musculature and the autonomic nervous system (ANS), and central nervous system (CNS) by the neurotransmitter serotonin (5-hydroxytryptamine [5-HT]) . Impairment in this interaction affects GI motility, secretion, and visceral sensitivity leading to the symptoms associated with IBS .(22)
Preliminary steps toward making a positive diagnosis of IBS:
A careful history and physical examination are frequently helpful in establishing the diagnosis. A variety of criteria have been developed to identify a combination of symptoms to diagnose IBS. Different guidelines from different studies help in making a positive diagnosis of IBS based primarily on the pattern and nature of symptoms, without the need for excessive laboratory testing. In 1978, Manning and colleagues(23,24) proposed diagnostic criteria for IBS that were found to have a reasonable sensitivity of 78% and a specificity of 72%.(1)In 1984, Kruis and colleagues developed another diagnostic criteria with a high sensitivity of 77% and a specificity 89%. Likewise, in 1990 Rome I(25)criteria came with a sensitivity of 71% and specificity of 85%. RomeII(1999)(26)and Rome III(2006)(27)have not been evaluated yet. None of the symptom based diagnostic criteria have been evaluated and ideal reliability found.(1)
Summary of diagnostic criteria used to define IBS:(1)
In 1978, Manning defined IBS as a collection of symptoms, given below, but did not describe their duration. The number of symptoms that need to be present to diagnose IBS was also not reported in the paper, but a threshold of three positive is the most commonly used:
a) Abdominal pain relieved by defecation
b) More frequent stools with onset of pain
c) Looser stools with onset of pain
d) Mucus per rectum
e) Feeling of incomplete emptying
f) Patient-reported visible abdominal distension
Kruis in 1984, defined IBS by a logistic regression model that describes the probability of IBS. Symptoms need to be present for more than two years. Symptoms are as follows:
a) Abdominal pain, flatulence, or bowel irregularity
b) Description of character and severity of abdominal pain
c) Alternating constipation and diarrhea
Signs that exclude IBS (each determined by the physician) :
a) Abnormal physical findings and/or history pathognomonic for any diagnosis other than IBS
b) Erythrocyte sedimentation rate >20 mm/2 h
c) Leukocytosis >10,000/cc
d) Anaemia (Hemoglobin < 12 for women or < 14 for men)
e) Impression, the physician could perform a PR and see blood or the patient may report it.
Again in 1990, Rome I defined IBS as abdominal pain or discomfort relieved with defecation, or associated with a change in stool frequency or consistency, PLUS two or more of the following symptoms on at least 25% of occasions or days for three months:
a) Altered stool frequency
b) Altered stool form
c) Altered stool passage
d) Passage of mucus
e) Bloating or distension
Rome II, in 1999, redefined the criteria as abdominal discomfort or pain that has two of three features for 12 weeks (need not be consecutive) in the last one year.
a) Relieved with defecation
b) Onset associated with a change in frequency of stool
c) Onset associated with a change in form of stool
Recently , Rome III (2006) defined IBS as recurrent abdominal pain or discomfort three days per month in the last three months associated with two or more of:
a) Improvement with defecation
b) Onset associated with a change in frequency of stool
c) Onset associated with a change in form of stool
The role of routine diagnostic investigation in patients with IBS:
Routine diagnostic investigation is based on the age of the patient, family history of selected organic diseases including colorectal cancer, inflammatory bowel disease(IBD), coeliac sprue and the presence of ‘alarm’ features(table1), such as rectal bleeding, weight loss, iron deficiency anaemia and nocturnal symptoms.(1) In patient with typical IBS symptoms and no alarm features, routine diagnostic investigation (complete blood count, serum chemistry, thyroid function tests, stool for ova and parasites and abdominal imaging) is not recommended(1)because of a low likelihood of uncovering organic disease.
Table-1 Lists of alarm features:
Rectal bleeding
Weight loss
Iron deficiency anaemia
Nocturnal symptoms: abdominal pain
family history of of selected organic diseases: colorectalcancer, Inflammatory Bowel Disease(IBD), celiac sprue
Summary of diagnostic investigation in patient with IBS : (1,2)
Diagnostic Investigations:
Routine serologic screening for coeliac sprue for patients with IBS-D and IBS-M.
Lactose Breath test done in lactose maldigestion despite dietary modification.
Colonoscopic Imaging done in IBS patient (>50 yrs age) with alarm feature to rule out organic diseases and screening of colorectal cancer.
Colonoscopy with random biopsies taken in IBS-D to rule out microscopic colitis.
Management of IBS:
The goal of IBS management is to provide relief of symptoms and improve overall well-being.(28)Most studies use a combination therapy including patient education and psychological therapies, diet and fibre therapy along with different types of new emerging pharmacological therapies.
Patient education and psychological therapies:
The majority of patients with IBS have anxiety, depression and features of somatization. Psychological therapies, including cognitive behavioral therapy, dynamic psychotherapy, hypnotherapy(1)shed new light on the management of patients with IBS. The outcome of psychological therapies is improved when delivered by a trained professional (physician, occupational therapist, nurse).(29) A study by Guthrie(30)showed that psychological therapy is feasible and effective in two thirds of patients with IBS who do not respond to standard medical treatment.
Role of diet in IBS:
The concept of food intolerance and the consequent elimination of certain foods from the diet benefit symptoms of IBS. However, there is no sufficient evidence to support this.(1)
Therapeutic effectof dietary fibre, bulking agents and laxatives:The quality of evidence supporting the recommended use of dietary fibre or bulking agents to regularize bowel function is poor.(31)Ispaghula husk(Psyllium hydrophilic mucilloid ) and calcium polycarbophil are moderately effective and can be given a conditional recommendation because of the weakest type of evidence.(1) Polyethylene glycol(PEG) laxative has a role in improving stool frequency but no effect on abdominal pain. Different clinical studies and expert opinion suggest that increased fibre intake may cause bloating, abdominal distension and flatulence.(32)So gradual adjustment of dose is advised for the use of these agents.
Therapeutic effectof antispasmodic agents including peppermint oil:
Certain antispasmodics (hyoscine, cimetropium,and pinaverium and peppermint oil) may provide short-term relief of abdominal pain/discomfort in IBS.(33,34)Evidence for safety and tolerability
Agent
Mechanism of action
Targeted disorder
Clinical status
Crofelemer
CFTR
IBS-D
Phase2b complete
Linaclotide
Guanylate cyclase-c agonist
IBS-C
Phase 3
Arverapamil
Calcium channel blocker
IBS-D
Phase 3
Asimadoline
Kappa opioid agonist
IBS
Phase 2b complete
Mitemcinal
Motilin receptor agonist
IBS-C
Phase 2
Ramosetron
5-HT 3 antagonist
IBS-D
Phase 3
TD-5108
5-HT 4 agonist
IBS-C
Phase 2
DDP-773
5-HT 3 agonist
IBS-C
Phase 2
DDP-225
5-HT 3 antagonist and NE reuptake inhibition
IBS-D
Phase 2
BMS-562086
Corticotropin-releasing hormone antagonist
IBS-D
Phase 2
GW876008
Corticotropin-releasing hormone antagonist
IBS
Phase 2
GTP-010
Glucagon-like peptide
IBS pain
Phase 2
AGN-203818
Alpha receptor agonist
IBS pain
Phase 2
Solabegron
Beta-3 receptor agonist
IBS
Phase 2
Espindolol (AGI-011)
Beta receptor antagonist
IBS (all subtypes)
Phase 2
Dextofisopam
2,3 benzodiazepinereceptors
IBS-D and IBS-M
Phase 3
Table 1: Source: ACG Task Force on IBS(2009)
of these agents are very limited.The commonest adverse effects are dry mouth,dizziness and blurred vision.(34-36)
Therapeutic effectof anti-diarrhoeal medications:
The anti-diarrhoeal agent ‘Loperamide’ is effective at slowing down colonic transit and improving stool consistency for the treatment of IBS-D with no severe adverse effects.(37)But safety and tolerability datas are still lacking in many studies.
Therapeutic effect of antibiotics:
Many studies show well tolerance of a short term course of non-absorbable antibiotics (Rifaximin) is most effective for improvement of global symptoms in IBS-D and IBS patient with the predominant symptom of bloating and other associated symptoms, such as diarrhoea and abdominal pain.(38-40) While, the Unted States Food and Drug Administration (FDA or USFDA) approved Rifaximin for treatment of traveler’s diarrhoea. Other antibiotics, Neomycin(41), Clarithromycin and Metronidazole(42)have been well evaluated for the management of IBS.
Therapeutic effect of Probiotics:
Probiotics have a large number of properties that can benefit IBS. Bifidobacteria is the active agent in probiotic combination therapy.Whereas many studies show Lactobacilli to have no impact on symptoms.(43)But one Korean study concluded that thecomposite probiotics containing Bifidobacterium bifidum BGN4, Lactobacillus acidophilus AD031, and other species are safe and effective, especially in patients who excrete normal or loose stools.(44) Recently, P Moayyedi and colleague in their systematic review recommend that probiotics appear to be efficacious in IBS patients ,but the magnitude of benefit and the most effective species and strain are uncertain.(45)
Therapeutic effect of the 5HT3 receptor antagonists:
Alosetron (5-HT3 receptor antagonists), with dosage of 0.5 to 1 mg daily, is more effective and the commonest drug used for treatment of patients with IBS-D in spite of serious side effects including constipation and colon ischemia.The balance model of benefits and harms for ‘Alosetron’ is most encouraging in women who have not responded to conventional therapies.(46,47)
Therapeutic effect of 5-HT4 receptor agonists:
Tegaserod (5-HT4 receptor agonist) is more effective for the treatment of IBS-C mostly in female and IBS-M. The side effects reported among the patient receiving Tegaserod are diarrhoea (commonest), cardiovascular events i.e. myocardial infarction, unstable angina, or stroke.(48,49)Currently Tegaserod is available from FDA through an emergency investigational new drug protocol. Other 5-HT4 agonists (Cisapride,Renzapride) have not demonstrated improvement compared with placebo.(50,51)
Therapeutic effect of the selective C-2 chloride channel activators:
Lubiprostone (selective C-2 chloride channel activator) is effective for relieving symptoms of IBS-C, mostly in women, and has less frequent side-effects including nausea(8%), diarrhea(6%) and abdominal pain(5%).(52)
Therapeutic effect of antidepressants :
Patients with prominent symptom of abdominal pain in IBS that fails to respond to peripherally acting agents often are considered for treatment with antidepressants (TCAs and SSRIs), however, limited data on safety and tolerability of these agents is shown.(53)Antidepressants have the combined effect of both central and peripheral mechanism in IBS.(54)SSRIs are better tolerated than TCAs and have a prokinetic effect hence work better in IBS-C.(53,55)whereas TCAs are of greater benefit for IBS-D.
Therapeutic effect of herbal therapies and acupuncture:
Unique Chinese herbal mixtures show a benefit in IBS management.(56) Traditional Chinese herbal remedies are routinely used in China to treat the condition, but so far have not been generally accepted by conventional Western medicine.(56,57)Bensoussanand colleague in one randomized, double-blind, placebo-controlledtrial concluded that the Chinese herbal formulations appear to offerimprovement in symptoms for some patients with IBS.(57) A systematic review of different trials of acupuncture was inconclusive because of heterogenous outcomes.(58,59) Hence further work is needed before any recommendations on acupuncture or herbal mixtures therapy.
Emerging therapies :
The improved understanding of underlying mechanisms in IBS is beneficial for the development of new pharmacological treatment options.
A brief overview of emerging agents in IBS therapy summarized in Table 1(1)
Conclusion:
IBS is a true medical disorder that has significant impact on those in agony with regard to symptom severity, disability, and impaired quality of life, which exceeds that of most GI disorders. Advances in research over the past several decades have paved the way for anameliorableunderstanding of the underlying pathophysiology and standardized symptom-based approaches that can be implemented in making a positive diagnosis and development of innovative treatment options for multiple IBS symptoms. Although many unanswered questions remain, the progress is promising and it has equipped physicians better to efficiently diagnose IBS and choose from a growing armamentarium of treatment options.
There has been a concerted attempt by government to engage doctors in management and the importance of medical management in psychiatry has never been greater. This commenced with the Griffiths Report on management within the National Health Service1 (NHS) but had renewed emphasis 25 years later in Lord Darzi’s report.2 The NHS Next Stage Review Final Report ‘High Quality Care for All’ sets out a vision for an NHS with quality at its heart. It places a new emphasis on enabling NHS staff to lead and manage the organisations in which they work. It pledges to incorporate leadership and management training into postgraduate medical curriculum. The proposal that management training should be integral to the training of all doctors, including psychiatrists, is not new.3, 4
Although management as a component of training for doctors is generally accepted, new consultants are often poorly prepared to deal with the complex organisational issues involved in taking on managerial responsibility.5, 6 This is partly to do with prior training and partly because learning in this area needs to be based on experience. It is essential that they be adequately prepared to fulfil the responsibilities. Recent psychiatric literature has pointed to the need for psychiatrists to have skills to develop their management and leadership roles and has called for more than ‘on the job training.’7
Management training for trainees – why?
It is important to recognise that all doctors will have some management responsibilities and it is a requirement of all doctors to fulfil these duties effectively as part of appraisal and revalidation. Medical training has traditionally focused on the clinical skills necessary to be a safe and competent clinician. It is increasingly important that doctors are not only competent clinicians but also have the skills to enable them to function efficiently and effectively within a complex healthcare system.
The aim for the doctor in training is to develop management skills in readiness to take on the responsibilities of a consultant. The management role of consultants is becoming more widely accepted and continually increasing, e.g. this may involve responsibility for teams, people, and the resources they use.8 Furthermore, the changing role of consultant psychiatrists calls for consultants to have skills to fulfil management and leadership roles.9 However, while not always recognised, all doctors including trainees are required to achieve some managerial functions from an early stage in their careers. Acquisition and application of leadership and management skills will enable them to contribute to the effective delivery of healthcare for patients.
The fast pace of change within healthcare provision means that it is important that current trainees have the appropriate skills for effective delivery of healthcare.10 It is clearly no longer acceptable that development of management and leadership competencies is left as optional.
What are the competencies that we need to acquire?
Leadership and management are a key part of a doctor’s professional work and the development of appropriate competencies needs to be an integral part of a doctor’s training and development. The objectives of the skills of all psychiatrists in training has relied on a number of documents which include Good Medical Practice11 produced by the General Medical Council (GMC), Good Psychiatric Practice12 produced by the Royal College of Psychiatrists, and the Medical Leadership Competency Framework (MLCF).13 The Royal College of Psychiatrists recognise that psychiatrists will need to acquire a basic level of management skill, and this is reflected in the curriculum which outlines the knowledge and experience to be gained during specialty training.
The intended learning outcomes for trainees are to demonstrate the ability to work effectively with colleagues including team-working, developing appropriate leadership skills, and demonstrating the knowledge, skills and behaviours to manage time and problems effectively.14 Furthermore the MLCF describes the leadership competencies that doctors need to acquire (Box 1). The MLCF was introduced in response to the recognised need to enhance medical engagement in leadership and was jointly developed by the Academy of Medical Royal Colleges, GMC and the NHS Institute for Innovation and Improvement.15
Box 1: Leadership competencies to begained during speciality training
1. Demonstrating personal qualities
Developing self awareness
Managing yourself
Continuing personal development
Acting with integrity
2. Working with others
Developing networks
Building and maintaining relationships
Encouraging contribution
Working within teams
3. Managing services
Planning
Managing resources
Managing people
Managing performance
4. Improving services
Ensuring patient safety
Critically evaluating
Encouraging improvement and innovation
Facilitating transformation
5. Setting direction
Identifying the contexts for change
Applying knowledge and evidence
Making decisions
Evaluating impact
How to attain competencies in management and leadership - formal qualifications Versus ‘On the job training’
It is important to realise that the acquisition of management competencies is an ongoing experience which starts early in one's career. Any trainee embarking on management training should consider very carefully the alternatives, assess their needs, and determine their own aims and objectives. It is often necessary to choose and tailor an individual training package. We share our experiences of two routes that can lead the trainee to acquire the relevant skills. For the convenience of the reader we will discuss these under the headings of ‘formal qualifications’ and ‘on the job training.’
Formal qualifications (MSc in Health and Social Care Management)
There are many advanced courses on offer, leading to a management qualification, usually lasting several years. Some of these courses are MBA (Health Executive), MSc in Health and Social Care Management, MSc in Health and Public Leadership, Masters degree in Medical Leadership, and Masters in Medical Management.
We (OW and AS) are pursuing an MSc in Health and Social Care Management, through the Faculty of Health and Applied Social Sciences in Liverpool John Moores University, on a part-time basis using our dedicated special interest time (six sessions per month). This degree has been specifically designed to provide all health and social care professionals the opportunity to develop their knowledge and skills to facilitate their role as managers. The programme is structured in such a way as to facilitate the part-time student and enhance their learning experience.
The MSc is modular in structure. In the first year the student will undertake three core management modules. In the second year the student will undertake a research methods module, management module and an individual work-based project. The final year culminates in a dissertation involving a significant piece of research. The student can choose to register for CPDs and there is an option to exit after one year (60 credits) with a Postgraduate Certificate or after two years (120 credits) with a Diploma. University regulations allow students to gain credit for demonstration of relevant prior learning, whether certificated or not. The course format is shown in Box 2.
The ratio of coursework, in-house teaching and self-directed learning varies between modules. Each module usually requires half to one-day attendance of in-house teaching per week. The programme uses a variety of assessment procedures that include a written assignment of 2000–5000 words, video role-play, seminar presentations and work-based projects. Completion of the assignments represents the greatest challenges to time and requires commitment and motivation.
Box 2: Format of the MSc in Healthcare Managementat the Liverpool John Moores University
·Improving service delivery through human resource management (20 credits)
·The economics of World Class commissioning (20 credits)
·Advancing leadership for quality (20 credits)
·Research methods and data analysis (30 credits)
·Strategic management and entrepreneurship (20 credits)
·Individual study or work based learning (10 credits)
·Dissertation (60 credits)
Strengths and weaknesses of an MSc in Health and Social Care Management
Whilst on the course we were able to learn a variety of concepts that were completely new to us, but the main challenge was to put them into practice. As part of the course we had to work on management related projects in our workplaces, so that we could apply the learnt concepts in real time.
We believe that the MSc course has undoubtedly improved our understanding of team working and leadership whilst working on a work-based project. The projects were specific supervised experiences linked to key developmental objectives and enhanced our problem-solving and decision-making, the ability to analyse and reflect on situations, as well as the expected understanding of resource management and change management.
We have been able to analyse personal development needs to enhance personal effectiveness and leadership skills. It helped us to critically evaluate the impact of action learning for organisational development. We have gained an insight into the concepts of commissioning and the role of economic evaluation. We were able to critically appraise the impact of government policies on the commissioning process. Our skills and knowledge of human resource management within a framework of contemporary policy context has increased. We really do feel that it has improved our insight into change management.
We hope that completing a significant research project within an academic setting will further develop our research skills. So far it has been a valuable and stimulating experience that has provided us with both skills and knowledge in management. The teaching and learning approaches for all modules draw into the experiences of the workplace. All core module assessment tasks are linked to the workplace, which is particularly useful.
However the process of developing a dissertation proposal, finding a supervisor, gaining ethical approval and proceeding with the research is time consuming and at times frustrating. The financial cost is a significant consideration but can be partially funded through the study leave budget. Furthermore, there is funding available for some modules through the Strategic Health Authority. As we were using most of our special interest sessions to pursue the degree, we had to put an extra effort to develop additional clinical interests.
‘On the job training’- what does that mean?
On the job management training may entail clinical managerial experience (e.g. organising outpatient clinics, developing systems for prioritising clinical work, managing teams, and drawing up on-call rotas), specific skills (e.g. chairing meetings, organising training days, and representation on committees), specific management experience (e.g. participation in service development) and resource management (non-clinical aspects of management such as human resources and finance).
The clinical setting provides many opportunities to gain knowledge, skills, attitudes and behaviours that are identified in the management and leadership curriculum. The diversity of daily clinical practice will enable the acquisition of appropriate skills and trainees need to take advantage of all the formal and informal learning opportunities. These range from workplace-based ‘learning sets’16 and project based learning. It is the responsibility of the trainers to ensure adequate and appropriate educational opportunities are made available to the trainee. In turn the trainee should be enthusiastic and proactive in identifying their own gaps in knowledge, skills, attitudes and behaviour.
It is important to bear in mind that such training should be supplemented by selected formal courses. Some training schemes offer no organised management training, whilst some provide training as a short and often intense course.17 A variety of courses have been developed for trainees, both at regional and national level. Trusts, Deaneries, independent organisations, universities and the Royal Colleges run such courses. These courses are normally short, lasting a week or less. The components of ‘on the job training’ in Merseycare NHS Trust and generic management courses offered by Mersey Deanery are listed in Boxes 3 and 4 respectively.
Box 3: Components of ‘on the job training’ in Merseycare NHS Trust
Appropriate involvement of trainees in clinical teams
Appropriate involvement of trainees in service development
Shadowing arrangements in placements
Undertake a management project
Senior managers in the trust as mentors to trainees
Action learning sets for trainees
Trainees developing teaching and supervisory skills with junior colleagues
Management seminars
Representation on committees (e.g. school board, local negotiating committee, local education board etc)
Two-day and three-day residential management training for higher trainees
Generic management courses runby the deanery
Personal development and management courses hosted by the College
Box 4: Generic management courses offered by Mersey Deanery
Management and leadership
Mentoring, appraisal, interview skills
Effective team-working
Managing change
Time management
Preventing and managing stress
Negotiating skills
Managing meetings
Strengths and weaknesses of ‘on the job training’
‘On the job training’ may vary from one placement to another depending on the availability of resources and mentors. Achieving ‘on the job’ management experience depends on the enthusiasm of the senior trainee. It is more personalised and individually driven. Higher training posts do provide exposure to management issues, but do not necessarily provide in-depth management experience.
It is easier to gain experience in clinical management skills but it can be difficult to achieve specific management experience including resource management. Trainers with formal management roles do not routinely engage trainees in this aspect of their work, and similar experiences have been expressed in other training schemes.18 Even if there are opportunities available to get involved in service development and other operational issues, one may struggle to commit any time.
Furthermore the loss of protected training (reduction of special interest to only two sessions for specialist trainees) to service provision has impacted on training.19 The formal courses are confined to development of skills such as leadership, teamwork and management of conflict. Residential management courses are available, providing one week or less of intensive training. The amount of management theory and techniques that can be learned on such courses is limited. The limited theoretical training in management means that trainees are unlikely to be adequately prepared for the extensive management role.
Which one is for you?
Managing services and leading organisations is not for everyone. Nevertheless, the medical role has inherent elements of leading and managing patient care and therefore doctors are often involved in service improvement and development. Perhaps the key issue is whether qualifications alone are sufficient to equip a doctor to be an effective manager, or is experience simply enough? It is important to remember that management qualifications tend to involve real-time application of concepts (which may be the same as on the job training) but at the same time gives a solid knowledge base. Furthermore, limited experience (involvement in local management) is unlikely to be sufficient and therefore experience should ideally be supplemented by selected formal courses.
However, even with the most impressive portfolio of formal training, trainees will nevertheless have to demonstrate competence in leadership and management in their work. All trainees are adult learners who ought to take responsibility for their own education. Which route the trainee wants to take depends not only on what the trainee intends to do in his future role but also on where he trains and what resources are available. Training needs will differ depending on past experience, competence, and capabilities. It is important for the trainees to recognise that the training needs will differ depending on their interests and the type of consultant post to which they aspire.
Formal qualifications would suit those with a well-developed interest in management and a desire to make this a significant part of their ongoing career. If the trainee intends to take a lead management role it may be necessary and useful to complete a Master’s degree. It will provide the trainee with both skills and knowledge in management and a well-recognised and formal degree in management. Having established that, it is worthwhile appraising the variety of courses available, as they vary significantly. It is helpful to determine the course’s content, assess its relevance, and establish how much in-house teaching and self-directed learning is expected. For those who want to acquire management skills for better day-to-day functioning in their job, it is useful to analyse their personal development needs and complete relevant modules according to these needs. This could be attained through ‘on the job training’ if resources can be identified and secured. A final point to bear in mind is the Royal Colleges’ direct contribution to developing management and leadership in trainees. For example the Royal College of Psychiatrists promotes engagement of doctors in management and has a dedicated Special Interest Group for management.
Syncope is a common condition encountered in acute medical practice. Many patients with syncope are initially labelled as having “collapse query cause”. It is defined as transient loss of consciousness (T-LOC) due to transient global cerebral hypoperfusion characterized by rapid onset, short duration, and spontaneous complete recovery1. Incidence of syncope is difficult to determine accurately as many cases remain unreported. Some studies quote an overall incidence rate of a first report of syncope to be 6.2 per 100 person-years. Clearly this is age related and the incidence increases dramatically in patients over the age of 70 years2. Syncope accounts for 1-6% of hospital admissions and 1% of emergency department (ED) visits per year3-5. Hospital episode statistics from NHS hospitals in England reported a total of 119,781 episodes of collapse/syncope for the financial year 2008-09 which is about twice the number of episodes reported in the year 1999-2000. About 80% of patients were admitted and they have an average length of stay of 3 days accounting for over 269,245 bed days during that financial year6.
Syncope is also associated with significant mortality and morbidity if left untreated. Literature reports a 6-month mortality of 10%, which can go up to 30% if cardiac syncope is untreated7. Non-cardiac syncope is associated with a survival rate comparable to people with no syncope2. Syncope is also a risk factor for fractures related to falls especially in elderly and can cause significant morbidity in this group8. In addition, there are significant health care related costs associated with management of syncope. Cost per diagnosis can vary from over £611 in the UK to €1700 in Italy. Hospitalisation alone accounted for 75% of cost in some studies9,10. Diagnosis of this condition can be difficult especially if there is a lack of structured approach. Over the last few years this topic has attracted enormous interest and several studies have been published, aiming at improving the approach to this condition. Standardised syncope pathways improve diagnostic yield and reduced hospital admissions, resource consumption and over all costs10. Recently the task force for the diagnosis and management of syncope of the European Society of Cardiology published guidelines for the diagnosis and management of syncope1. However, in spite of the available evidence very few hospitals have standardised syncope pathways for the management of this complex condition. Only 18% of EDs have specific guidelines and access to a specialist syncope clinic11. This article focuses on evidence based structured evaluation of syncope. Current practice in the management of syncope Due to the difficulty in diagnosis and mortality associated with this condition, a cautious approach may be taken by physicians resulting in hospitalisation of majority of patients presenting with syncope. We recently audited the practice of syncope in our hospital, which is a tertiary centre in the north of Scotland. 58 patients admitted with this condition over a period of a month were included in the audit. It showed an average length of stay (LOS) of 4.76 days in these patients. Due to a lack of methodical approach and standardised pathway for management of this condition many patients were subjected to several inappropriate inpatient investigations significantly prolonging the LOS and increasing the cost. Only 7 (12%) cardiac events were observed in this group and in retrospect a good methodical approach would have predicted these events. It should be noted that even in the geriatric population, reflex syncope that carries a benign prognosis is more common than cardiac syncope2. A systematic approach to the management of syncope (Figures 1 and 2). The causes of syncope can be broadly divided in to cardiac causes and non-cardiac causes (Table 1). Initial evaluation leads to a diagnosis in less than 50% patients in most instances4,12-14. If there is uncertainty about diagnosis then the patient is risk stratified. High-risk patients are hospitalised, evaluated and treated whereas early discharge could be considered in low risk patients. Aetiology of Syncope41
Neurally-mediated (Reflex) Syncope
Cerebro vascular
Vasovagal syncope
Carotid sinus syncope
Situational syncope
e.g., Micturition, post prandial, defecation, cough
Relevant blood tests (e.g. to rule out metabolic abnormality)
Pacemaker check if appropriate
History Many patients with syncope are initially labelled as having “collapse query cause”. Loss of postural tone is termed “collapse”. Indeed, the term “collapse query cause” does not give any useful information regarding the underlying condition. A clear history from the patient and the bystander or witness (if available) is the key to the diagnosis. Firstly, determine if the collapse was associated with loss of consciousness (LOC). LOC can be transient (T-LOC) or prolonged. Categorising “collapse” is important at this stage as the aetiology and approach to each category is different (Figure 1). Secondly, establish if the collapse was syncopal. The LOC should be transient (e.g. did the patient regain consciousness in the ambulance, before or on arrival to hospital?), of rapid onset and associated with a spontaneous complete recovery. Also the mechanism should be due to transient global hypoperfusion. T-LOC secondary to other mechanisms such as trauma and brief seizures should be excluded. On occasions syncope could be associated with brief jerking movements mimicking seizures15. Also note that a transient ischemic attack (TIA), commonly listed as a differential diagnosis of syncope by physicians, is not a cause of syncope as this is not associated with global cerebral hypoperfusion. The absence of a coherent history because patient had no recollection of events and there was no witness account available can make this distinction difficult. This is also particularly difficult in the elderly with cognitive impairment. Other useful information includes whether the syncope was associated with postural change. Orthostatic hypotension occurs after standing. If present it will be useful to check drug history (new vasodepressive drugs). Features suggestive of Parkinson’s disease or amyloidosis may raise the possibility of autonomic neuropathy. A strong family history of sudden cardiac death may be of relevance. Table 3 summarises the features of neurally mediated and cardiac syncope. Table 3 Features suggesting neurally mediated and cardiac syncope42
Neurally mediated
Cardiac
Preceded by prodrome
Related to particular activity - e.g., Micturition, postprandial, prolonged standing, unpleasant situations
Associated with nausea and vomiting
After exertion
Absence of prodrome, no warning
Associated with chest pain, breathlessness, palpitation
During exertion or supine
History of cardiac disease
Family history of sudden cardiac death
Physical examination The next step is a thorough physical examination. This should include an ABC approach if the patient is very ill and particular attention should be given to exclude immediate life threatening conditions such as pulmonary embolism, acute myocardial infarction, life threatening arrhythmias, acute aortic dissection, seizures etc… Recording the vital signs is important as it may give a clue to diagnosis (e.g., acute hypoxia may indicate massive pulmonary embolism). Recording postural blood pressure when lying and during active standing for 3 minutes is useful to exclude orthostatic hypotension1. Recording a deficit in blood pressure in both arms may be a useful clinical finding especially if acute aortic dissection is suspected. Thorough cardio respiratory examination may reveal an obvious condition such as cardiac failure or aortic stenosis. Patients should also be examined for potential injuries as a result of syncope. Standard ECG A 12 lead ECG should be performed in all patients admitted with syncope. The abnormalities in table 4 would suggest a cardiac aetiology. The QT interval should always be measured, as it is a commonly overlooked abnormality. Blood tests Blood tests are usually unhelpful in establishing a diagnosis but can detect metabolic abnormalities such as hypoglycaemia, electrolyte abnormalities and other causes to explain LOC especially when witness account is not available. An acute drop in haemoglobin suggests blood loss. One recent study claims the usefulness of brain natriuretic peptide (BNP) for predicting adverse outcomes in syncope but it is not externally validated yet and it is too early to recommend for routine clinical practice16. Pacemaker check It is not uncommon to see a patient with a pacemaker implanted, admitted to hospital with syncope. In these circumstances, it is essential to rule out a device malfunction although this is not a common cause of syncope. A preliminary and easy test will be interrogating the pacemaker if available. This should pick up any problems with the pacemaker in most instances. With the above information establishing a diagnosis will be possible in a significant proportion of patients. Further investigations and management should be guided by the underlying diagnosis1. However in over half of patients the diagnosis may still be uncertain12,13,17. The following section explains the management of unexplained syncope. Risk stratification in patients with unexplained syncope (Tables 4 and 5)Table 4 ECG changes in ‘high-risk’ Syncope41
ECG changes favouring bradyarrhythmias
High degree AV blocks – Mobitz type 2 second degree AV block, complete heart block, trifascicular block (first degree heart block with left bundle branch block (LBBB) or right bundle branch block (RBBB) with axis deviation)
Bifascicular block (defined as either LBBB or RBBB combined with left anterior fascicular block or left posterior fascicular block) especially if new
Other intraventricular conduction abnormalities (QRS duration >0.12 s)
Asymptomatic sinus bradycardia (<50 bpm), sinoatrial block or sinus pause >3 s in the absence of negatively chronotropic medications
ECG changes favouring tachyarrhythmias
Pre-excited QRS complexes (e.g. WPW syndrome)
Prolonged QT interval
Right bundle branch block pattern with ST-elevation in leads V1–V3(Brugada syndrome)
Negative T waves in right precordial leads, epsilon waves and ventricular late potentials suggestive of arrhythmogenic RVD
Q waves suggesting myocardial infarction
Non sustained Ventricular Tachycardias
Table 5 – Clinical features of high-risk syncope1,18-23
History of severe structural heart disease or heart failure, presence of ventricular arrhythmia
Syncope during exertion or supine
Absence of prodrome or predisposing or precipitating factors
Preceded by palpitation or accompanied by chest pain or shortness of breath
Family history of sudden cardiac death
Examination suggestive of obstructive valvular heart disease
Syncope associated with trauma
Systolic blood pressure less than 90mm Hg
Hematocrit less than 30% (acute drop in hemoglobin)
When the cause of syncope is uncertain it is essential to risk stratify patients to enable appropriate treatment and further investigation. Risk stratification tools There are several scoring systems for risk stratification of syncope. Syncope Evaluation in the Emergency Department Study (SEEDS), Osservatorio Epidemiologico sulla Sincope nel Lazio (OESIL score), Evaluation of Guidelines in SYncope Study (EGSYS score), San Francisco Syncope Rule (SFSR), The Risk stratification Of Syncope in the Emergency department (ROSE) and American College of Emergency Physicians clinical policy are the popular ones and each has its own advantages and disadvantages1,16,18-23. Discussing each scoring system is beyond the scope of this article and we shall restrict the discussion to the summary of these risk stratification tools (Table 5). It will be too early to include all the factors mentioned in the ROSE study, as it is not externally validated yet. It could be argued that taking all the risk factors described may increase admission rates but this approach may at least not miss the high-risk patient. This is a developing field and more evidence is likely to be published soon. High-risk vs. low-risk syncope: A high-risk syncope patient is the one where a cardiac cause is likely and where the short-term mortality is high due to major cardiovascular events and sudden cardiac death. High-risk syncope is said to be present if any of the features in the table 4 or 5 are present. Management of low-risk syncope Patients with a single or very infrequent syncope are usually reassured and discharged, as the short-term mortality is low1,2. Tilt table test is not usually required where a single or rare episode of neurally mediated syncope is diagnosed clinically. One exceptional circumstance where single rare episodes are investigated further with a tilt table test is when there could be an occupational implication (e.g. aircraft pilot) or if there is a potential risk of physical injury. Patients with recurrent unexplained syncope need to be further investigated (see below). Management of high-risk syncope / suspected cardiac syncope High-risk patients usually require hospitalisation and inpatient evaluation. Other high-risk patients who may be considered for admission are vulnerable patients susceptible to serious injuries, for example, elderly patient or a patient with multiple co-morbidities. Further investigations (Table 6)
Non invasive
Invasive
Echocardiography
ECG monitoring
Telemetry
Holter monitoring
External loop recorder*
Carotid sinus massage
Cognitive testing (in elderly)
Ambulatory blood pressure monitoring
Tilt table test*
Exercise stress test
Implantable loop recorder*
Coronary angiography*
Electrophysiology*
* Specialist Investigation Echocardiography Echocardiography is a relatively inexpensive and non-invasive investigation. It should be performed if there is a clinical suspicion of a significant structural abnormality of heart such as ventricular dysfunction, outflow tract obstruction, obstructive cardiac tumours or thrombus, pericardial effusion etc… The yield of this test is low in the absence of clinical suspicion of structural heart disease. However in the presence of a positive cardiac history or an abnormal ECG, one study detected LV dysfunction in 27% of patients and half of these patients had syncope secondary to an arrhythmia. In patients with suspected obstructive valvular disease 40% had significant aortic stenosis as a cause of syncope24. ECG monitoring These tests have utility in identifying arrhythmogenic syncope. If a patient has syncope correlating with a significant rhythm abnormality during the monitoring period with the device, then the cause of syncope is due to the underlying rhythm abnormality. On the other hand, if no rhythm abnormality is recorded during a syncopal attack, then an underlying rhythm problem as a cause of syncope is excluded. Therefore, these tests are meaningful only if there is a symptom-rhythm correlation, which is the working principle of these devices. In the absence of syncope, during the monitoring period, these tests may pick up other abnormalities that may be relevant. For example, rapid prolonged supra-ventricular tachycardias, ventricular tachycardias, periods of high degree AV blocks (mobitz type 2 or complete heart block) or significant sinus pauses >3seconds (except during sleep, negatively chronotropic therapy and trained athletes), which will require further investigation or treatment. Telemetry Telemetry can be used in inpatients. Although the diagnostic yield of this investigation is only 16%, given the high short-term mortality, this test is indicated in the high-risk group 1. Usually patients are monitored for 24 to 48 hours although there is no agreed standard period for monitoring25. Holter monitoring This involves connecting the patient through cutaneous patch electrodes. It records the ECG activity conventionally over 24-48 hours or at times up to 7 days. It is particularly useful only in patients who have frequent regular symptoms (≥1 per week). For this reason, the yield of this test can be as low as 1-2% in unselected population1. Long inpatient waiting lists in some hospitals can significantly prolong the length of stay and cost. Selecting patients carefully for this test based on risk stratification will reduce costs and waiting lists. Carotid sinus massage This simple bedside test is indicated in patients over the age of 40 years with syncope of unexplained origin after initial evaluation. A ventricular pause lasting >3 s and/or a fall in systolic BP of >50mmHg defines carotid sinus hypersensitivity (CSH) syndrome. It is contraindicated in patients with recent cerebrovascular accidents (past 3 months) or with carotid bruit except when a Doppler study has excluded significant stenosis1. Cognition test If an elderly patient had forgotten about the events, in the absence of an obvious cause, it may be useful to test cognition. If cognitive impairment is present, common problems associated with cognitive dysfunction should be considered e.g. falls, orthostatic hypotension. Other investigations In spite of the above tests if a cause is not determined, early specialist input is recommended for further investigation and treatment. The following non-invasive and invasive investigations may be appropriate in these circumstances. An external loop recorder This is a non-invasive form of electrocardiographic monitoring. The principle is same as that of Holter monitoring. External loop recorders have a loop memory that continuously records and deletes ECG. When activated by the patient, typically after a symptom has occurred, 5 – 15 min of pre-activation ECG is stored and can be retrieved for analysis. Studies have shown that they have increased diagnostic yield compared to Holter1. They should be considered in patients who have symptoms on a monthly basis. A Tilt table test This is indicated in cases of recurrent unexplained syncope after relevant cardiac causes of syncope are excluded and a negative Carotid sinus massage performed in the absence of contraindications. It is also indicated when it is of clinical value to demonstrate patients susceptibility to reflex syncope and thereby to initiate treatment. Other less common indications are recurrent unexplained falls, differentiate jerking movements secondary to syncope and epilepsy, diagnose psychogenic pseudo syncope and differentiate orthostatic and reflex syncope. Indication of this test in the context of a single unexplained syncope is discussed above. Ambulatory blood pressure monitoring This may be useful in patients with unexplained syncope particularly in old age to check if there is an element of autonomic failure and if a single set of orthostatic blood pressure recording is not helpful. In one study, it has been shown that 25% of the elderly patients admitted with falls or syncope had postprandial hypotension especially after breakfast26. It may be more readily available than a tilt table test in some centres. Exercise stress test This may be useful in a rare entity called exercise induced syncope. Outflow tract obstruction should be excluded by echocardiography before subjecting a patient to this test especially in the presence of relevant signs. However there is no evidence for supporting this test in investigating syncope in general population. Implantable loop recorders These are implanted subcutaneously. It needs to be activated either by the patient or a bystander after a syncopal attack. It is indicated in high-risk patients where a comprehensive evaluation did not establish an underlying diagnosis. In the absence of high risk factors, it is also indicated in patients with recurrent unexplained syncope especially if infrequent. Conventionally it is used as a last resort in patients with recurrent unexplained syncope as the initial costs are high. It has been shown in one study to be more cost effective than the conventional strategy and was more likely to provide a diagnosis in patients with recurrent unexplained syncope27. However patients with poor LV function and those at high risk of life-threatening arrhythmias were excluded from this study. Coronary angiography or CT coronary angiography This may be helpful in suspected myocardial ischemia or ischemia related arrhythmias. Electrophysiological study may be considered in certain circumstances by cardiologists. When a standardised pathway is used, diagnosis is ascertained in 21% patients on initial evaluation and further 61% patients with early investigations. Only in 18% patients the diagnosis was still uncertain12. Other studies have shown similar results28. Although these results are from a dedicated syncope unit following a standardised pathway, these could be extrapolated to any unit following these standardised pathways. Further management is dictated by the underlying diagnosis with early specialist input for appropriate treatment. Treatments Single or rare episodes of reflex syncope do not require treatment. However, recurrent troublesome reflex syncope may warrant treatment. Treatment modalities are primarily non-pharmacological such as tilt training, physical counter pressure manoeuvres (leg crossing, hand gripping) and ensuring adequate hydration29. If refractory to non-pharmacologic measures midodrine (alpha agonist) may be considered in patients with frequent hypotensive symptoms30,31. Fludrocortisone may be used in elderly but there is no trial evidence to support this. Betablockers have been presumed to lessen symptoms but are shown to be ineffective in several studies 32. They may potentially exacerbate bradycardia in carotid sinus syncope and are not recommended in treatment of reflex syncope. Treatment with cardiac pacing in reflex syncope is controversial and may be considered in patients with predominant cardio inhibitory response on carotid sinus massage (in CSH syndrome) or on tilt test (in reflex syncope). It should be noted that cardiac pacing has no effect on the often-dominant vasodepressor component of reflex syncope. In patients with orthostatic hypotension, non-pharmacologic measures like increased salt and water intake, head up tilt sleeping, physical counter pressure manoeuvres, abdominal binders and compression stockings may help reducing symptoms. Midodrine is an efficient alternative in these circumstances and fludrocortisone also can be used.33,34Syncope secondary to cardiac arrhythmias needs treatment if a causal relationship is established. Potential reversible causes such as electrolyte abnormalities and drug induced causes should be excluded. Cardiac pacing is a modality of treatment in significant bradyarrhythmias secondary to sinus node or advanced AV nodal disease such as mobitz type 2 block, complete heart block or tri-fascicular block. Catheter ablation and anti-arrhythmic drug therapy are the main modalities of treatment for tachyarrhythmias. Implantable cardioverter defibrillator may be indicated in patients susceptible to malignant ventricular tachyarrhythmias. Treatment of syncope secondary to structural cardio pulmonary abnormality will need surgical intervention if possible. Driving and Syncope Doctors are poor at addressing and documenting this issue35. Table 7 gives some useful information from the DVLA website (http://www.dft.gov.uk/dvla/medical/ataglance)36. This information is country specific and subject to change. Table 7 – Driving and Syncope in the UK36
Type of Syncope
Group 1 entitlement (car, motorcycle etc.,)
Group 2 entitlement (Large goods vehicle, passenger carrying vehicle)
Simple faint
No restrictions
No restrictions
Unexplained syncope with low risk of recurrence*
Allowed to drive 1 month after the event
Allowed to drive 3 months after the event
Unexplained syncope with high risk of recurrence** and cause identified and treated
Allowed to drive 1 month after the event
Allowed to drive 3 months after the event
Unexplained syncope with high risk of recurrence** and cause not identified
Licence is refused or revoked for 6 months
Licence is refused or revoked for 12 months
*Absent clinical evidence of structural heart disease and normal ECG** Abnormal ECG, clinical evidence of structural heart disease, syncope causing injury, recurrent syncope Syncope unitsSyncope units aim to evaluate syncope (and related conditions) in dedicated units consisting of generalists and specialists with an interest in syncope. A sufficient number of patients are required to justify such a unit. They are well equipped with facilities for recording ECG, blood pressures, tilt table, autonomic function testing, ambulatory blood pressure monitoring, and invasive and non-invasive electrocardiographic monitoring. It has been shown to be cost effective and reduces health care delivery costs by reducing admission rates, readmission rates and event rates. Examples include the Newcastle model, Manchester model and the Italian model.12,18,37,38Conclusions The incidence of syncope is increasing in the UK with an aging population. There is significant cost incurred in the delivery of health care for this condition. The approach to syncope varies widely amongst practising physicians due to lack of a methodical approach. A thorough initial evaluation yields a diagnosis in less than half of the patients. When the cause of syncope remains unexplained after initial evaluation, the patients should be risk stratified. While a patient with a single episode of low risk syncope can be reassured and discharged, those with high-risk features should be hospitalised for further management. Outpatient evaluation could be offered for low risk patients if recurrent. Early specialist input should be sought in high-risk syncope and recurrent unexplained syncope. This standardised approach or pathway will reduce cost by reducing hospitalisation, inappropriate investigations and length of stay.
Key Facts
Collapse associated with transient loss of consciousness is called syncope if it is due to transient global cerebral hypoperfusion and characterized by rapid onset, short duration, and spontaneous complete recovery
Standardised syncope pathways improve diagnostic yield and reduce hospital admissions, resource consumption and over all costs
A thorough initial evaluation yields a diagnosis in less than half of patients. If the cause of syncope is undetermined after initial evaluation, patients should be risk stratified
Early discharge should be considered in low risk patients while high-risk patients need urgent evaluation.
Early specialist referral is recommended in patients with high risk syncope and recurrent unexplained syncope
Future Interests Syncope had been known for several decades and still remains a complex condition, as the exact mechanisms are poorly understood especially in non-cardiac syncope. Mechanism of syncope in the elderly patients may be different from those of young patients and studies should focus in understanding the mechanics. Further research is needed in risk stratifying syncope. It may enable us to develop more robust care pathways for management of syncope. The role of BNP in investigating and risk stratifying syncope need to be further clarified. In spite of sophisticated tests the cause of syncope in a proportion of patients remain uncertain. Studies should focus on the long-term outcome and management of syncope in this group. The role of implantable loop recorder in the investigation of syncope should be better defined and more studies should focus on when it should be offered in the pathway of management of syncope. Studies are also required to develop effective pharmacotherapies for this condition.
Patients, in both the pre and post-operative periods, seek and receive advice from a number of health professionals. The advent and subsequent increasing use of day case surgery has also meant that patients have a reduced exposure to the surgical staff. This subsequently results in patients increasingly seeking post-operative advice from their general practitioner and allied health care professionals. The development of innovative surgical techniques has meant that the traditional teachings with regard to time taken for convalescence following surgery are somewhat outdated. The aim of this study was to initially determine the exact time taken for patients to return to work, driving and daily routine for a number of routine general surgical procedures. Secondly we aimed to determine the advice that GPs and surgeons would give to patients following routine surgery.
Patients and Methods
Patients aged 65 years or less, who had routine surgical procedures (open unilateral inguinal hernia repair, laparoscopic cholecystectomy, laparoscopic hernia repair and unilateral varicose vein surgery) over a six month period (January – June 2004) were identified from the theatre database. A single page questionnaire was sent to each patient (Appendix 1). Each patient was questioned with regard to the following:
Occupation
Time taken to return to normal activities following surgery
Time taken to return to driving following surgery and any advice given
Expected and actual time off from work following surgery
Distribution and length of a sick note
Expectations following surgery
Experience of day case surgery
Questionnaires were returned and data collected on a specially constructed database. Concurrent to this a further questionnaire (Appendix 2) was distributed to a number of differing groups of health professionals. These were namely:
GPs – this included the GPs of all patients who had been identified as having undergone surgery in the specified six month period as well as all doctors on the vocational training scheme.
Surgeons – this included all senior house officers on the Yorkshire School of Surgery Basic Surgical Training Scheme and all Higher Surgical Trainees (General Surgery) within the Yorkshire Deanery including non-carrier grade doctors .
Replies were anonymous and each health care professional was asked with regards to the advice they would give to an “average” patient undergoing the four procedures with regard to time it would take to return to work (office or heavy), driving and return to normal activities. They were also asked whether they felt the procedure was suitable for day case surgery. Statistical Analysis Statistical analysis was undertaken using the Analyse-it statistical package (Leeds, UK.). Non-parametric analysis using either Kruskall 1- way ANOVA or the Mann-Whitney U test was used to test for a difference between the medians of independent samples. The Wilcoxon signed-ranks test was used to test for a difference between the medians of 2 related samples. Significance was determined as a p-value < 0.05. Results Nineteen of 48 patients who underwent varicose vein surgery (39%), 44 of 72 patients who underwent a laparoscopic cholecystectomy (61%), 23 of 35 patients who underwent a laparoscopic hernia repair (65%) and 12 of 23 patients who underwent an open inguinal hernia repair (52%) over the six month period returned a completed questionnaire. Of the health care professionals, 65 primary care physicians were identified and sent questionnaire, of which fifty three GPs (81.5%) replied. From the Yorkshire deaneries database sixty five trainees were identified (Spr, SHO, HO, non-carrier grades), of which 41(63.2%) surgically trained doctors returned a completed questionnaire. Among the responders, we also include four consultant surgeons who have performed the operations on patients in our hospital. Overall one hundred and thirty participants were sent study forms, of which 94 (72.3%) health professionals responded with completed questionnaire. Varicose Vein Surgery (Table 1)
Activity
Time (IQR in Weeks)
Overall (K)
Surgeons vs. GPs (M)
Surgeons vs. Patients (M)
GPs vs. Patients (M)
Office Work
Surgeons
2 (1-2)
GPs
2 (1-2)
0.13
0.56
0.10
0.05
Patients
1 (1-2)
Heavy Work
Surgeons
3 (2-5)
GPs
4 (2-4)
<0.01
0.75
<0.01
<0.01
Patients
1 (1-1.75)
Driving
Surgeons
2 (1-2)
GPs
2 (1-2)
<0.01
0.24
<0.01
0.02
Patients
1 (1-1)
Normal Activities
Surgeons
2 (2-4)
GPs
2 (2-4)
0.05
0.57
0.04
0.02
Patients
1.5 (1-2)
Table 1: Time taken to return to work, driving and daily activities as experienced by patients and as suggested by both surgically trained doctors and GPs for unilateral varicose vein surgery. Time: Median time to return to activity (IQR - weeks) K: Kruskal Wallis ANOVA. M: Mann Whitney U test. P<0.05 deemed as significant. Of the 19/48 patients who returned a completed questionnaire, eleven (57.8%) were women with an overall median age 44 years (range 21-64 years). Seventeen of the 19 patients worked (89%), 11 of who undertook office work (57.8%). Patients tended to return to driving and normal activities quicker than that recommended by doctors. GPs and surgeons offered similar advice with regard to return to all activities following varicose vein surgery. Nine of the 19 patients were uncertain about whether they have received any advice or perhaps forgotten any information regarding when to return to driving. Five patients received no advice about when to return to work. No significant difference was observed between expected time off work and actual time off work experienced by the patients (2 weeks vs. 1 week – p=0.15 Wilcoxon Rank test). Fifteen of the 19 patients (79%) said that their recovery was what they had expected with the reasons for not meeting expectations being wound infection in 2, bruising and a larger incision in one patient each. Seventeen patients had their surgery performed as a day case (89.4%). Fifteen patients stated that they would have surgery again as a day case (88.2%). Laparoscopic Cholecystectomy (Table 2)
Activity
Time (IQR - weeks)
Overall (K)
Surgeons vs. GPs (M)
Surgeons vs. Patients (M)
GPs vs. Patients (M)
Office Work
Surgeons
2 (1-2)
GPs
2 (2-3)
<0.01
0.02
<0.01
<0.01
Patients
5 (3-7)
Heavy Work
Surgeons
4 (2-4)
GPs
4 (4-6)
<0.01
<0.01
0.26
0.04
Patients
2 (1.5-4)
Driving
Surgeons
2 (1-2)
GPs
2 (1-3)
0.19
0.19
0.10
0.43
Patients
2 (1-4)
Normal Activities
Surgeons
2 (1-4)
GPs
3 (2-4)
0.19
0.20
0.09
0.47
Patients
4 (2-6)
Table 2: Time taken to return to work, driving and daily activities as experienced by patients and as suggested by both surgically trained doctors and GPs for laparoscopic cholecystectomy. Time: Median time to return to activity (IQR - weeks) K: Kruskal Wallis ANOVA. M: Mann Whitney U test. Of the 44/72 patients who returned a completed questionnaire 39 were women (88.6%) with an overall median age 47 years (range 20-63 years). Thirty-two of the 44 patients worked (72%), 25 of who undertook office work (56%). Patients returned to office work significantly later than that recommended by both groups of doctors. Overall, patients took a significantly shorter time to return to work that involved lifting heavy objects. Surgeons also recommended shorter times to return to work when compared with GPs. Of further interest is the observation that it took a shorter time for those patients undertaking heavy work to return to work when compared with the patients undertaking office work. There was no significant difference in the time taken to return to driving and normal activities experienced by the patients when compared to the advice given by both groups of doctors. Ten of the 44 patients (22%) stated that they had received no advice regarding when to return to driving or perhaps they may have no memory about driving instructions. Seven patients stated they received no advice about when to return to work (15%). Overall, patients expected a significantly shorter time off work than was actually experienced (2.5 weeks vs. 4 weeks – p<0.01 Wilcoxon Rank test). Twenty-one of the 44 patients (48%) said that their recovery was not what they had expected (47%). Of these 21 patients, 6 said that their recovery was better than expected (28%), 5 said that their recovery was longer than expected (23%), and the rest either complained of pain or wound infection. Seventeen patients had their surgery performed as a day case (38%). Of these 17, 11 said that they would have surgery again as a day case (64%). A significantly higher proportion of GPs felt that this procedure was suitable for day case surgery compared with the proportion of patients who actually underwent the procedure as a day case (p=0.02 chi squared test). Laparoscopic Inguinal Hernia Rapair (Table 3)
Activity
Time (IQR - weeks)
Overall (K)
Surgeons vs. GPs (M)
Surgeons vs. Patients (M)
GPs vs. Patients (M)
Office Work
Surgeons
2(1-2)
GPs
2 (1-2)
0.73
0.56
0.48
0.714
Patients
2 (1-2.75)
Heavy Work
Surgeons
6 (4-6)
GPs
4 (4-6)
0.03
0.31
0.01
0.03
Patients
3 (2-4)
Driving
Surgeons
2 (1-4)
GPs
2 (1-2)
0.22
0.21
0.12
0.46
Patients
1 (1-2.25)
Normal Activities
Surgeons
2 (2-4)
GPs
3 (2-4)
0.41
0.87
0.31
0.17
Patients
2.5 (1.25-3)
Table 3: Time taken to return to work, driving and daily activities as experienced by patients and as suggested by both surgically trained doctors and GPs for laparoscopic hernia repair. Time: Median time to return to activity (IQR - weeks) K: Kruskal Wallis ANOVA. M: Mann Whitney U test. Of the 23/35 patients who returned a completed questionnaire, the majority had bilateral hernias repaired. 22 were men (95%) with an overall median age 48 years (range 35-63 years). Twenty one of the 23 patients worked (91%), 10 of who undertook office work (43%). No significant difference was found between the actual time taken to return to office work and the advice given by either group of doctors. Patients returned to heavy work significantly sooner than that recommended by both groups of doctors. There was no significant difference in the time taken to return to driving and normal activities experienced by the patients when compared to the advice given by both groups of doctors. Three (13%) patients were uncertain about receiving advice regarding when to return to driving or they might have no memory of information received. Six (26%) patients stated they cannot recall about receiving any advice regarding when to return to work. There was no significant difference seen in the time patients expected off work than was actually experienced (2 weeks vs. 2 weeks – p>0.05 Wilcoxon Rank test). Nine of the 23 patients (39%) said that their recovery was not what they had expected. Of these 9 patients, 2 (22%) said that their recovery was longer than expected, 4 (44%) said that they experienced more pain than they expected; one (11%) said that the recovery time was much shorter and one (11%) experienced some bleeding from the umbilical port. Twenty patients (86%) underwent their surgery as a day-case. Of these 20, 16 (69%) said that they would have their surgery again as a day case. Open Inguinal Hernia Repair (Table 4)
Activity
Time (IQR - weeks)
Overall (K)
Surgeons vs. GPs (M)
Surgeons vs. Patients (M)
GPs vs. Patients (M)
Office Work
Surgeons
2 (2-2)
GPs
2 (1.25-3)
0.01
0.07
<0.01
0.05
Patients
4 (3-4)
Heavy Work
Surgeons
6 (4-6)
GPs
6 (4-7.75)
0.57
0.49
0.47
0.39
Patients
5 (4.25-5.75)
Driving
Surgeons
3 (2-4)
GPs
2 (2-3)
0.03
0.06
0.02
0.15
Patients
2 (1-2)
Normal Activities
Surgeons
2 (2-2)
GPs
2 (1.25-3)
<0.01
0.07
<0.01
0.01
Patients
4 (2.5-5)
Table 4: Time taken to return to work, driving and daily activities as experienced by patients and as suggested by both surgically trained doctors and GPs for open hernia repair. Time: Median time to return to activity (IQR - weeks) K: Kruskal Wallis ANOVA. M: Mann Whitney U test. P<0.05 deemed as significant. All 12/23 patients who returned a completed questionnaire were men with an overall median age 54 years (range 42-65 years). Nine of the 12 patients worked (75%), 5 of whom undertook office work (41%). Patients took a significantly longer time to return to office work when compared to the advice given by either group of doctors. No significant difference was observed in the time taken for patients to return to manual work and the advice given by either group of doctors. Surgeons advised a longer period of abstinence from driving compared to that actually undertaken by the patients. Patients took a significantly longer time to return to normal activities when compared to the advice given by either group of doctors. Two patients (16%) replied that no information was given or may not recall in regards to when to return to driving and one patient (8.3%) stated that he cannot recall any professional advice he has received about return to work. There was no significant difference seen in the time patients expected off work than was actually experienced (3 weeks vs. 5 weeks – p>0.05 Wilcoxon Rank test). Five patients (41%) said that their recovery was not what they had expected. Of these 5 patients, 4 (80%) said that they experienced more pain than they expected and one (20%) experienced more bruising. Seven patients (58%) underwent their surgery as a day-case and of these, 5 (71%) said that they would have their surgery again as a day case. Discussion With the advent of day case surgery there is an increasing number of health professionals giving advice to patients about their post-operative course. Advocates of minimal access surgical techniquesand day case surgery claim that this is associated with a reduction in the periodof postoperative recovery1, 2. The proposed benefits,however, may never be seen if there is no concordance in the advice given by medical practitioners. The advice given to patients is still based upon personal experience rather than firm scientific evidence and indeed, there have been few studies that have analysed patients return to normal activities following surgery. Majeed et al questioned 59 general practitioners and61 surgeons with regard to the time taken for young (25 years old) and older (55 years old) patients to return to sedentary, light manual and heavy manual work following a number of common surgical procedures (including varicose vein surgery, unilateral open inguinal hernia repair and laparoscopic cholecystectomy) 3. The moststriking finding was the enormous variation in opinion betweendifferent doctors. For example, a 55 year old heavy manual workerhaving a haemorrhoidectomy could be given between one and 16 weeks off work depending on which doctor he or she consulted. Such wide variation was not observed in our study and in general, the advice given by both GPs and surgeons was similar apart from the fact that surgeons advised a shorter period off office work for patients undergoing laparoscopic cholecystectomy. The end of the twentieth century has brought an exponential growth in new surgical techniques for standard general surgical procedures. Not only there has been an increase in the use of mesh for open inguinal hernia repairs but there has also been an increasing use of laparoscopic hernia repair, with the recent guidance by the national institute for health and clinical excellence (NICE) liable to further increase the role of laparoscopic repair 4. Furthermore, there has been the widespread acceptance of laparoscopic cholecystectomy and an increased awareness of the role of general anaesthetic in increasing the number of procedures that can be undertaken as a day case. Given these continuing developments in surgical technique as well as in both pre- and post-operative care the present advice and experience of GPs could be seen to be somewhat out-dated. Two surgeons within the unit perform laparoscopic hernia repair (one the transabdominal preperitoneal repair (TAPP) and one the totally extraperitoneal (TEP) repair) with three performing solely the open technique. Although our results based on small sample size but match with evidence based recommendation by NICE (www.nice.org.uk,), suggests that laparoscopic repair does reduce the time taken for post operative recovery when compared to open repair. In fact, all patients returning to heavy work following laparoscopic hernia repair do so quicker than that advised by either GP's or surgeons although unlike the surgeons, GPs do tend to recognise the likely reduction in pain experienced following a laparoscopic repair and alter the advice given to those in heavy work accordingly. Restriction of activity on the advice of surgeons may be basedon their concern for tissue healing and strength, which may have arisen in the days when absorbablesutures such as catgut were used. The use of mesh should now change this thinking and it has indeed been shown that there is no increase in the recurrence of inguinal herniasafter early return to work 5. Office workers undergoing an open inguinal hernia repair take a longer time to return to work (4 weeks) than that advised by both groups of doctors. Furthermore, patients undergoing laparoscopic cholecystectomy take a shorter time to return to heavy work than office work. These results do require more evaluation. At face value it would appear that doctors underestimate the time taken for return to office work and in the case of the cholecystectomy overestimate the time it takes to return to heavy work. In fact the patients in office work took a significantly longer time to return to work following cholecystectomy than those in heavy work. Although only 20% of the working cohort of patients who underwent cholecystectomy were in “heavy work” this result probably represents the fact that a high proportion of people in heavy work are self-employed and time off work is money lost. Patients who are selfemployed return to work much sooner than those in salaried jobs 6. Furthermore, there may well be an element of low job satisfaction in people in office work, which has also been shown to be a major predictor of delayed return to work 7. The time taken to return to work, however, may be dependant on the patients' expectation of convalescencetime formed prior to surgery, which in many cases is based upon advice given by medical practitioners. Furthermore, the attitude of the medical profession in the post-operative period is important as they have to issue the certification necessaryto ensure financial compensation for the patient. Patients undergoing varicose vein surgery returned to heavy work, driving and normal activities significantly sooner than that suggested by either group of doctors. This may well be down to a recently concerted effort to encourage patients to walk to reduce the risk of DVT. All patients had long saphenous vein (LSV) surgery by either the standard high tie, stripping of the LSV and multiple stab avulsions or by local ligation of the LSV. Overall it would appear that a one-week period of recuperation is all that is needed following unilateral varicose vein surgery. The advent of minimally invasive treatment for varicose veins may result in a shorter post-operative recovery period 8. There are some shortcomings associated with this study. Questionnaire based studies always present methodological issues including problems with response rate. There is never an “average patient” and normal activities for one patient may be completely different from those of another patients and any advice given should be individually tailored. Furthermore, occupations were not classified as either manual or office based prior to the start of this study, but were classified on an individual basis during collation of the data. However, we hope that the data presented here will help medical practitioners advising their patients about postoperative routine life activities. Conclusion: We believe that our overall practice is not different with regards to the pre, peri and post-operative management of patients when compared to the majority of units within the UK. However, there may well be some variation with regard to healing and time taken to return to work and we would encourage other units to undertake similar studies to determine convalescence times.
Appendix 1
Sex (Male / Female)
Age at time of surgery.
Do you work
Yes / No
If yes, what job do you do?
How long did it take to you to return to your normal activities of daily living following your operation (weeks).
If you drive, how long did it take for you to start driving again (weeks).
What advice, if any, were you given about driving after your operation?
The following questions are to be completed if you do work.
Prior to your surgery, did you receive any information about how long you would be off work?
Yes / No
If YES, what information was given to you?
How long did you expect to be off work following your surgery (weeks)?
How long were you actually off work following your surgery (weeks)?
If you are in employment:
Did you get a sick-note:
· From the hospital
Yes / No
· From the GP
Yes / No
How long was the sick note for (weeks)?
Did the sick note need to be extended?
Yes / No
Was the recovery after your operation as you had expected it to be?
Yes / No
If no, why not?
Did you go home on the same day as you had your operation?
Yes / No
If YES, would you do the same if you had the operation again or would you prefer to stay overnight after your operation?
If you would prefer to stay overnight, why?
Appendix 2 Dear Doctor. We at xxxxxx Hospital are undertaking a study to determine whether the information given to patients following routine general surgical procedures is consistent and compares to the actual recovery period experienced by the patients themselves. We would be grateful if you would consider the four general surgical procedures below and give us an average length of time (in weeks) that you would advise the patient to abstain from:(a) office work(b) heavy work(c) driving(d) to return to normal activities of daily living The general surgical procedure to be considered are1) mesh repair of an inguinal hernia (unilateral)2) laparoscopic hernia repair 3) unilateral varicose vein surgery4) laparoscopic cholecystectomy




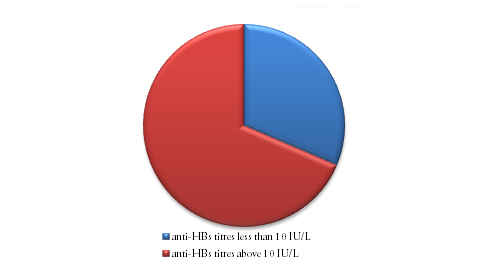
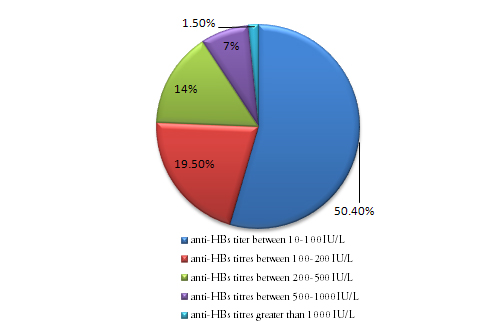


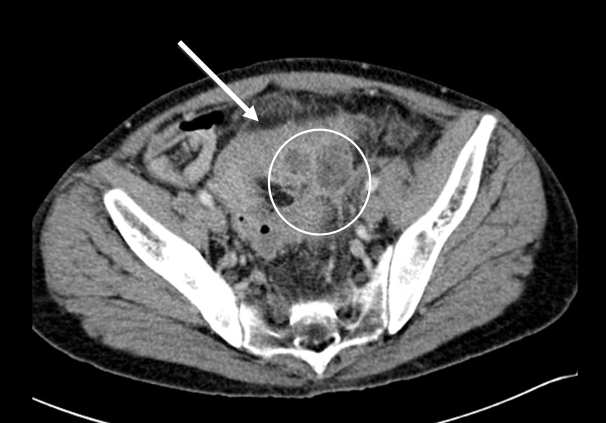





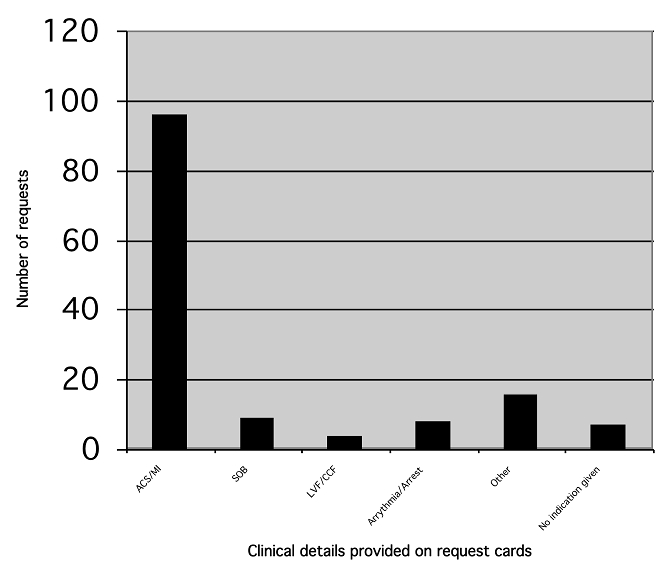

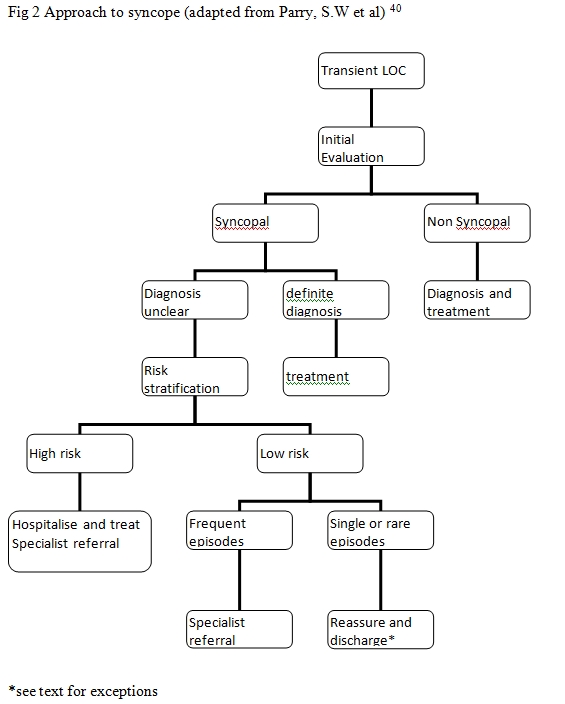 The causes of syncope can be broadly divided in to cardiac causes and non-cardiac causes (Table 1). Initial evaluation leads to a diagnosis in less than 50% patients in most instances4,12-14. If there is uncertainty about diagnosis then the patient is risk stratified. High-risk patients are hospitalised, evaluated and treated whereas early discharge could be considered in low risk patients. Aetiology of Syncope41
The causes of syncope can be broadly divided in to cardiac causes and non-cardiac causes (Table 1). Initial evaluation leads to a diagnosis in less than 50% patients in most instances4,12-14. If there is uncertainty about diagnosis then the patient is risk stratified. High-risk patients are hospitalised, evaluated and treated whereas early discharge could be considered in low risk patients. Aetiology of Syncope41
BJMP December 2011 Volume 4 Number 4
BJMP December 2011 Volume 4 Number 4
Editorial
Nasseer A Masoodi
Research Articles
Mohammad Afzal, Khaliq Naveed, Shabbir Hussain, Shaukat Mehmood Qureshi, Asifa Majeed, Zia Farooqi, Alizay Gohar and Abdul Wahab
Mohamed A. Daabiss and Mohamed Hashish
Hussain Anthony Kazi and Ashutosh Acharya
Saoud Sultan, Dirk Claassen and Stephen Stansfeld
Review Articles
Stephen O’Neill, Phillip Ross, Philip McGarry and Satheesh Yalamarthi
Seif Fadi, Gholam Pierre and Montenegro Hugo
Francis J Dunne
Medical Images
Capt Gary Chow, Katerina Achilleos and Col Hem Goshai