Schizophrenia (SCZ) is a chronic relapsing and remitting disorder with a lifetime prevalence of 4 per 1000 persons.1Positive symptoms include delusions and hallucinations. Negative symptoms are characterised by deficits in normal behaviour, which are categorised into five domains: blunted affect, alogia, social withdrawal, anhedonia, and avolition. In clinical practice, when monotherapy fails multiple augmentation strategies – such as another antipsychotic, mood-stabilisers, benzodiazepines, lithium, electroconvulsive therapy, and repetitive trans-cranial magnetic stimulation – have been used to improve the clinical state of these patients, but evidence relating to the use of these interventions is lacking.2None of the regulatory bodies has openly endorsed polytherapy with antipsychotics.
The introduction of chlorpromazine in the 1950s revolutionised psychiatry, and the coming of slow-release, slow-acting forms (depot medication) contributed to the closure of asylums and paved the way to community psychiatry. Second-generation antipsychotics ameliorated the situation for a number of psychotic patients, but some remained resistant to all forms of psychopharmacology. In 1958, clozapine was formulated and marketed commercially in 1972. 3 The arrival of clozapine facilitated the rescue of some schizophrenia sufferers for a short time, but the drug disappeared from the scene because of initial untoward incidents. 4,5 The observation that clozapine has the potential to control the motor symptoms of tardive dyskinesia and to treat the psychotic symptoms of patients already diagnosed with tardive dyskinesia, led to its reintroduction, but with restrictions. 6,7,8 Clozapine is recommended for use only after a trial of two other antipsychotics. Combining depot antipsychotics with oral drugs of a different class has been the practice ever since the introduction of depot medications, and this practice has come to have general clinical acceptance.
Treatment resistance
Historically, it was observed that a specific group of chlorpromazine users remained symptomatic. They were considered to be refractory to phenothiazines. The availability of clozapine led to a better definition of treatment resistance. ‘Response to treatment’ means a reduction in the severity of symptoms, while ‘remission’ implies an absence of symptoms for a considerable period. ‘Recovery’ signifies absence of the disease for a long period.9‘Treatment resistant schizophrenia’ (TRS) is the term used for persistence of psychotic symptoms despite a certain number of adequate treatments. Since the introduction of first-generation antipsychotics, clinicians have been cognizant of TRS and operational definitions have been used such as those developed by Kane et al. 10 Sometimes, treatment has been based on algorithms such as the Texas Medication Algorithm Project (TMAP).
According to the most common definition of TRS, if patients present with persistent, moderate to severe, positive disorganization or negative symptoms together with poor social and work function over a prolonged period of time after at least 2 adequate trials of neuroleptic drugs, they may meet the criteria of having TRS. 11 A common agreement is that adequate drug treatment requires a duration of 4 to 10 weeks, a dosage equivalent to 1000 mg/d of chlorpromazine, and trials of 2 to 3 different classes of antipsychotic drugs. 12 The current treatment guidelines recommend 2 or more treatment trials of atypical antipsychotics at adequate dosages. Adequate response to treatment has been defined as at least a 20% reduction in symptoms as measured by rating scales. Typical antipsychotics can also be used for 4 to 6 weeks to screen for TRS.
Resistance to treatment and poor outcome are different from genuine TRS. Resistance to treatment may be defined as a state in which the patient has access to medication, but the effectiveness of the treatment is suboptimal. TRS may be conceptualised as a state in which medication has reached target receptors but does not seem to be effective. Chronicity has often been misconstrued with treatment-resistance. Schizophrenia is a chronic disorder that progresses to various levels of clinical deterioration without sustained remission or full recovery. Poor-outcome SCZ applies to 50% of patients, and TRS comprises a subset of such patients. In these, cognitive impairment, negative symptoms and mood symptoms are independent of positive symptoms, resulting in poor-outcome SCZ.
It is generally accepted that 30% of SCZ sufferers have TRS. Many people with SCZ do not achieve a satisfactory treatment response to their initial antipsychotic drug treatment. They may manifest a poor response to therapy because of intolerance to medication, poor adherence and inappropriate dosing, as well as true resistance of their illness to antipsychotic drug therapy. Assessing treatment resistance is a priority in the management of TRS. 13 TRS has to be closely evaluated before a comprehensive management plan is developed (Table 1). From a multidimensional point of view, TRS is dependent on manifold factors, such as longer duration, several episodes, gender, early onset, poor pre-morbid personality, family history, substance misuse, presence of soft neurological signs and a long untreated period.14 Genes are thought to be involved in the development of TRS; reliable genetic prediction of which patients will be TRS would have serious clinical implications. Structural neuroimaging techniques have revealed that TRS patients do not differ importantly than those responsive SCZ in terms of brain abnormalities.15
When clozapine fails or rejected
Clozapine may be the preferred drug for TRS – effectively the gold standard – but its side effects put off many patients to the extent that some of them refuse clozapine therapy. It is a unique atypical antipsychotic and there is robust evidence supporting its use in people with TRS. Though clozapine often represents the best hope for recovery, it is associated with severe and enduring adverse reactions that may delay its prescription and increase morbidity and mortality. The major side effects are a) agranulocytosis; b) metabolic side effects; c) myocarditis; d) seizures; e) severe constipation with gastrointestinal complications such as intestinal obstruction, bowel perforation, paralytics ileus and toxic megacolon; and f) sialorrhea. These side effects hinder the popular use of clozapine in TRS. It is a life-saving drug, but without extra care it may itself shorten the life span. Side effects are more common with higher doses. It has been estimated that between 10 and 60% of patients resistant or intolerant with other antipsychotic drugs respond to clozapine.
The side effects mentioned above are inevitably an impediment to its common use. When standard doses (300mg to 5oomg) do not produce the desired effects or patients develop unwanted effects, combining clozapine with other antipsychotics is a common practice for TRS. To mention a few antipsychotics, amisulpride and aripiprazole are atypical antipsychotics ordinarily used in combination with clozapine. The anti-salivatory effect of amisulpride and the alerting effect of aripiprazole are added advantages of such a combination, and these drugs are fairly weight neutral – in contrast to clozapine. Clozapine, representing a second generation of so-called atypical antipsychotic drugs, has shown positive effects in desperate cases of TRS. Furthermore, two epidemiological studies have shown that clozapine has the lowest mortality rate among antipsychotics.
Nevertheless, even supported by the literature as the best-known antipsychotic in terms of efficacy and rates of response, a sizeable number of patients remain resistant to clozapine therapy and continue as symptomatic and dysfunctional. It has been estimated that 40–70% of patients on clozapine may not respond satisfactorily to it.16 When patients do not respond to clozapine, they are categorised as super-refractory, but the very concept of super-refractory state is debatable. They do not differ from the refractory cases in terms of demographical factors but have high score of positive symptoms. It may be simply explainable that the aetiological mechanism of the illness of such patients may be different from the clozapine responders and that makes them unresponsive to clozapine. There are no operational definitions for super-refractory schizophrenia. According to the schizophrenia algorithm of the International Psychopharmacology Algorithm Project (www.jpap.org), persistence of psychotic symptoms after a trial with adequate doses of clozapine(300-900mg/day) for at least six months is designated as super-refractory cases. 17
Many predictors of clozapine response have been suggested without any firm ground. These include severe clinical symptoms, higher levels of functioning before the onset of schizophrenia, low levels of homovanillic acid and 5-hydroxyindoleacetic acid in cerebrospinal fluid, reduced metabolism in the prefrontal cortex, reduced volume of the caudate, and the improvement of P50 gating at the 500-ms prepulse interval. 18 However, none of these factors is consistent or specific as a predictor of clozapine response. More genetic and brain imaging studies are warranted with such patients. In these cases, augmenting strategies are necessary, and some have been in use: typical and atypical antipsychotics, mood stabilizers, antidepressants and electroconvulsive therapy. Some studies have favoured ECT, but no definitive conclusion has been drawn. So also, half of clozapine patients discontinue taking the medication on their own accord. In a retrospectively studied sample of patients who discontinued clozapine, the majority terminated the treatment as a result of their own decision or because of non-compliance with medical procedures such as blood sampling.19
There are currently no evidence-based pharmacotherapies for the TRS patients who do not respond to clozapine 20,21 or those who terminate clozapine therapy due to adversative reactions. 22 In the nutshell, clinicians should be prepared to try different alternative treatment options for TRS and super-refractory cases. Thus, combination therapy may become a choice as pre-clozapine therapy or post-clozapine therapy. Clozapine is not a drug that could normally be imposed on patients, but it has to be earned by the patient.
Combination therapy
The range of antipsychotic medications available is wide, with variable effectiveness, and there are also differing profiles for typical and atypical agents, adding to a confusing array of terminologies and dilemmas regarding what the best drug for service users is.23 Combination therapy involves the addition of a second antipsychotic to the therapy regimen. It is different from adjunctive therapy, in which a second agent is employed to reverse an emergent side effect or to obtain a complementary clinical effect. Augmentation involves the use of a non-antipsychotic along with the antipsychotic already in use. Combination therapy and augmentation therapy are sometimes used interchangeably. In general, ‘combination’ refers to the use of more than one type of disease-specific treatment to treat a particular illness.
A change from one antipsychotic to another in same class seldom produces any additional benefit, whereas switching to an antipsychotic with a different mechanism of action has proved to produce a more impressive response rate. Combination becomes desirable when the drug already in use produces some favourable effect, but that is not sufficient to control the symptoms. It is imperative to distinguish between partial response and no response when considering a change in medication. Past antipsychotic drug response, adverse effect profile differences, concomitant medical disorders and concurrent drug therapy are factors to be considered when choosing between switching and combination or augmentation approaches. A switch is indicated when there is no response to the drug and combination therapy; augmentation is recommended for partial response. Another antipsychotic combination may become necessary as an option for TRS patients who cannot be treated with clozapine for various reasons. It is common practice in such situations to add a second antipsychotic, in combination with the original one.
Clinical team do not have to be disheartened or disillusioned when clozapine therapy fails due to non-response or clozapine intolerance, and also when augmentation and combination therapies do not bring about the desired outcome. Switching back to atypical drugs once again may turn out to be effective in some cases and clozapine is not to be considered as the last resort. A multicentre open label 18-week trial evaluated a switch to olanzapine in 48 clozapine resistant or intolerant patients. 24 Switching to olanzapine 5-25 mg per day resulted in a mean drop in total scores on the Positive and Negative Syndrome Scale (PANNS) and Brief Psychiatric Rating Scale (BPRS) of 17.7 (14.2%) and 9.8 points (20.2%) respectively.
Cautions
Monotherapy is the most desirable form of treatment for SCZ. There is no good objective evidence to support dual antipsychotic therapy except in combination with clozapine. The evidence base supporting such combinations consists mostly of small open-label studies and case series.25 Combination therapy should be considered only when several attempts at monotherapy, including one atypical antipsychotic, fail. It is assumed that two different treatments together may have a different mechanism of action and therapeutic response from that of either drug alone. Studies have been conducted to determine whether treatment with antipsychotic combinations is effective for SCZ and whether such treatment is safe for the same illness. The results of trial studies are based on very low or low-quality results, and research that provides high-quality evidence is needed before firm conclusions may be drawn. The results so far show that there may be some clinical benefit in combination therapy in that more people receiving a combination of antipsychotics showed an improvement in symptoms. For other important outcomes – such as relapse, hospitalisation, adverse events and discontinuing treatment – no clear differences between the two treatment options were observed. Currently, most evidence regarding the use of antipsychotic combinations comes from short-term trials; the assessment of long-term efficacy and safety is limited. There is some very low-quality evidence that a combination of antipsychotics may improve the clinical response.
There are published case reports of serious side effects, such as a higher prevalence of extrapyramidal symptoms (EPS), metabolic side effects, paralytic ileus, grand mal seizures and prolonged QTc in association with a combination of antipsychotics.26Combining three antipsychotics may be extremely dangerous; studies have revealed that such a procedure substantially increases mortality.27A negative case control study exists.28 It should be usual practice to document the rationale for combined antipsychotic use in individual cases in clinical records, along with a clear account of benefits and disadvantages, including side effects.
Newer combinations and augmentation strategies are supported only by case reports and open trial data. Along with advantages, a number of potential concerns regarding antipsychotic combinations have been identified (Table 2) and specific clinical cautions have to be implemented in combination therapy (Table 3). Yet, fixed combinations of drugs are common in medicine and at one time were common in psychiatry. An example is small doses of an antipsychotic in combination with an antidepressant for treating major depression; this lost popularity because of side effects. Also, SNRI-NaSSA combination therapy (e.g. California Rocket Fuel) is prevalently used for treatment-resistant depression.
Olanzapine–amisulpride combination
In spite of the objections put forward against combination therapy, there are isolated case studies favouring the olanzapine–amisulpride combination. Zink et al. (2004) performed a retrospective study, aiming at the systematic evaluation of patients on combined olanzapine and amisulpride. The open study designed as a retrospective chart review of Zink et al. concludes that the olanzapine–amisulpride combination for TRS is encouraging, but requires further evaluation in prospective and randomised studies.29They point out that a reduction of the daily dose of both drugs helped to minimise the side effects of these drugs – such as weight gain and EPS – resulting in better compliance. They did not notice any additional side effects or undesirable drug interactions.
Within the heterogeneous group of atypical antipsychotics, the thienobenzodiazepine derivative olanzapine has a receptor profile that is quite similar to that of clozapine, indicated by having a greater affinity for serotonergic 5-HT2A receptors than for dopaminergic D2 receptors. The positive and negative symptoms of schizophrenic psychoses usually respond well to this drug. In contrast to clozapine, olanzapine does not induce major agranulocytosis but may, in a significant number of cases, lead to troublesome side effects including significant weight gain, type ii diabetes, sedation, anticholinergic effects and transient increases in liver enzymes. Assertive weight management from the start of treatment is recommended. Weight should be monitored and also waist circumference measurements made. In addition, blood lipids should be assessed routinely. A suggested schedule for these investigations would be at 3, 6, and 12-month intervals, and biannually thereafter.30The pharmacology of antipsychotics is not the only factor that determines their effect on weight. Olanzapine has also been shown to elevate prolactin significantly in some patients.31 As indicated earlier, Olanzapine can succeed in some cases even where clozapine fails.24
Amisulpride is an atypical antipsychotic of the benzamide class. It blocks D2 and D3 receptors (presynaptic in low doses, postsynaptic in higher). Unlike other atypical or typical antipsychotics, it has low affinity for serotonin, α-adrenergic, histaminergic, muscarinic and sigma receptors including D1, D4 and D5 receptors. It can lead to dose-related EPS that are significantly less than those of typical antipsychotics such as haloperidol and comparable to risperidone.32It is recognised that amisulpride is only sparingly metabolised by liver enzymes, and thus it is not known to participate in many drug interactions.33 Amisulpride may elevate prolactin, which may cause sexual dysfunction, osteoporosis, amenorrhoea, gynaecomastia or galactorrhoea. It is a weight-neutral compound and may ameliorate negative symptoms.34 Both olanzapine and amisulpiride are not associated with QTc prolongation.
One advantage of the combination of these drugs is that when olanzapine and amisulpride are combined, they may be given at a lower dose, which will spare the patients from the main unwanted side effects of the individual drugs: the over-sedation and weight gain of olanzapine; and the hyperprolactinemia of amisulpride, resulting in sexual side effects of a particularly undesirable extent. Our limited studies have found that this combination was well tolerated by TRS patients and its efficaciousness was similar to that of clozapine, but without any major side effects. Patients have been fully compliant. The combination of these drugs is managed by slowly introducing them one at a time and has been transformative in many cases. More studies of the olanzapine–amisulpride combination are needed in order to report on such outcomes as relapse, remission, social functioning, service utilisation, cost-effectiveness, satisfaction with care, and quality of life.
Table 1. Assessing Treatment Resistance
Re-evaluate current antipsychotic treatment Has an adequate trial been given? Suboptimal dose and non-adherence can lead to pseudo-resistance-poor adherence is unwaveringly associated with adverse effects, poor insight, and a poor therapeutic alliance. Consider exceeding BNF limits-recommended only in specialist centres Review the differential diagnosis eg schizo-affective disorder or bipolar affective disorder-Bipolar Disorder can present with first rank symptoms in the initial stages, it could take up to 10 years to establish a diagnosis of BD. Asses for psychotic symptoms Re-evaluate personal history and psychological pressures Investigate co-morbid psychiatric symptoms eg substance misuse or alcohol dependency, depression, obsessive compulsive disorder and panic attacks Investigate organic factors-temporal lobe epilepsy, endocrinopathies Check blood levels if facilities available Longer duration Multiple episodes Male gender Onset of illness at an earlier age Poor pre-morbid functioning Length of untreated psychosis Family history of schizophrenia Soft neurological signs-lateral and third ventricular enlargement and low catecholamine level in CSF Suicidal tendencies Aggression Asses adverse effects of psychiatric and other medications that may mimic worsening of positive and negative symptoms Complete physical and neurological examination and specialist consultation, as appropriate Rule out the desire to to be ill
Table 2. Advantages and disadvantages
Advantages: Discontinuation symptoms due to the withdrawal of the first antipsychotic could be avoided Patients unresponsive to the initial antipsychotic may achieve clinical response when the second agent is introduced Patient does not have to cope with another waiting period for the substituted drug to produce full results The benefits of the first drug are preserved in addition to the favourable effects of the added drug Switching involves tapering off the initial drug, wash out period and delay in the onset of the second drug Switching of antipsychotic drug requires additional supervision and care in the transitional period and could be delayed due to discontinuation symptoms; the addition of a second antipsychotic drug solves these problems Disadvantages: The possibility of unnecessarily high doses An increased acute and/or chronic side-effect burden Adverse pharmacodynamic and pharmacokinetic interactions Difficulties in determining cause and effect of multiple treatments Potential increased mortality, Higher costs Poorly documented risks and benefits of this practice Reduced compliance
Table 3 Physical cautions with combination
History of cardiac disorder (eg, MI, arrythmias, abnormal ECG) Hepatic impairment Renal impairment Obesity (high BMI) Heavy smoking High alcohol intake Substance misuse Hyperlipidaemia Above age 70 ECG, Haematological investigations. Side effect rating scales Physical effects Record justification for combination
Summary
Combination therapies are the second choice when monotherapy fails. Clozapine is the first choice in severe cases of TRS, but there are super-refractory cases of TRS where clozapine fails. At least in isolated cases, the combination of olanzapine and amisulpride (Ami-olan combination) is worth considering for TRS patients who are reluctant to go on to clozapine therapy or in instances when clozapine failed, or patents dropped out. Combination therapies are normally avoided, but clinicians’ helplessness and patients’ despair justifies such measures in hard-to-treat cases of TRS. Only time will tell whether this combination will become an important part of clinical practice in future or will be ruled out as just another dual antipsychotic therapy.
The aetiology of SCZ remains obscure. The symptoms of different psychotic disorders are not clearly demarcated and there are no physiological parameters on which to make a firm diagnosis. In such a situation, the treatment of TRS has to be tailored on an individual basis. Even though it is normally well calculated, it may be somewhat hit and miss. Finding the right combination of antipsychotics or augmenting agents when the clinician is stranded and torn between monotherapy and polypharmacy is a gargantuan task. Clinical judgement along with patient preference must take over when treatment algorithms fall short. Given the data on polytherapy with antipsychotics that is available, it is hard to make any firm recommendation regarding its efficacy and safety of its use. Clinicians should be reminded that they should try monotherapy in adequate dosages before considering combinations.
For the management of TRS, comprehensive treatment strategies that integrate pharmacological, psychological, and psychosocial approaches are highly relevant and for that to happen, TRS should be clearly recognised. NICE offers very little guidance on clozapine resistant cases of SCZ. Combination of antipsychotics is not a panacea or a permanent solution for TRS. More investigation of schizophrenic illness is the only way forward. In comparison with other medical conditions (eg,HIV), research into it is making little progress. As it stands now, deconstructing clozapine’s unique pharmacology may offer ‘light at the end of the tunnel’ for patients who are clozapine intolerant or non-responders.
In the absence of systemic inflammation, procalcitonin synthesis is mainly restricted to the neuroendocrine cells of the thyroid.1 This is not released into the blood until cleaved/mature form (i.e. calcitonin). Therefore, procalcitonin levels remain undetectable.2 Almost all body tissues can produce procalcitonin. The main triggers for its synthesis are bacterial toxins (endotoxins) and cytokines released in response to bacterial infections (TNF alpha, IL-1-beta and IL-6). See Table 1. Cytokines released due to viral infections (e.g. interferon-gamma) inhibit TNF-alpha production.1, 3 During an inflammatory response, procalcitonin levels start rising within 2-4 hours and peak in 24-48 hours. Peak levels correlate to the severity of the bacterial infection. When inflammation resolves, procalcitonin levels fall quickly, falling by 50% every 24-36 hours. If the inflammation is ongoing, procalcitonin levels plateau (due to ongoing production of procalcitonin).4
Table 1: Points to remember: 5-11 1. Most bacterial infections will cause a rise in procalcitonin levels (levels >0.25ng/ml). 2. The following bacterial infections will not cause a rise in procalcitonin levels: a. Mycoplasma pneumoniae. b. Chlamydia pneumoniae. 3. Parapneumonic effusions, empyema and lung abscesses may not cause a rise in procalcitonin levels. 4. Mycobacterium tuberculosis, can and can’t cause a rise in the procalcitonin levels 5. Viral infections will not cause a rise in procalcitonin levels (levels <0.25ng/ml). 6. Amongst fungal organisms, candida infections can cause a rise in procalcitonin levels (levels >0.25ng/ml). 7. Malaria can cause a rise in procalcitonin levels (levels >0.25ng/ml). 8. Clostridium difficile colonization will not cause a rise in procalcitonin levels (levels <0.25ng/ml). 9. Lung cancers (especially neuroendocrine) and medullary thyroid cancers can cause a rise in procalcitonin levels (levels >0.25ng/ml). 10. Renal insufficiency (which hinders the clearance) can cause a rise in the baseline procalcitonin levels. 11. Physiological stress can cause a rise in procalcitonin levels (levels >0.25ng/ml). This includes trauma, surgery, burns, bowel ischemia, cerebrovascular accident (infarct and haemorrhage), pancreatitis and any kind of shock-like situation.
Community Acquired Pneumonia (CAP) and Procalcitonin
As we know, it can take 24-48 hours for the procalcitonin to reach its peak levels, hence in an acute clinical setting (where CAP is the diagnosis, or suspected), the decision to start antibiotics can’t depend on the initial procalcitonin levels (because of high morbidities associated with CAP). Nevertheless, serial levels will help in guiding antibiotic therapy. a. If procalcitonin levels are persistently <0.25ng/ml in a CAP patient with suspected viral aetiology (based on history and investigations), antibiotics can be stopped. We should keep in mind that procalcitonin levels do not normally rise in the case of mycoplasma and chlamydia pneumonia. b. Suspected or known CAP patients should receive empiric antibiotics as per local protocol in an acute setting. c. Antibiotics can be stopped in patients with suspected or known bacterial CAP who have received antibiotics for at least five days and shown clinical improvement with procalcitonin levels dropping <0.25ng/ml. d. CAP patients who are not clinically improving, and procalcitonin levels are rising or not decreasing, will need a review of antibiotics. e. Optimal threshold for discontinuing antibiotic therapy has not been established.12 f. Procalcitonin levels have prognostic value. Again, there is no optimal threshold. Serial levels have more prognostic value than a single level.
Ventilator Associated Pneumonia (VAP) and Procalcitonin
Patients with VAP are usually very unwell. Antibiotics should be started as soon as VAP is suspected. Procalcitonin can be used to stop antibiotics in VAP patients. As per ProVAP trial, stopping antibiotics when procalcitonin level drops <0.5ng/ml, or >80% from its peak value, did not result in an adverse outcome.
Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) and Procalcitonin
Use of procalcitonin to guide antibiotic therapy in patients with AECOPD has not been established yet. Some experts use the levels to help in making decisions about stopping antibiotics (in a similar way as mentioned in the above section of CAP). Infections in AECOPD are less invasive and pathogens differ from CAP; procalcitonin levels may not correlate well with the severity of the episode. In one trial, antibiotic use was found to be of no benefit in patients with AECOPD with levels <0.1ng/ml.13
Acute Bronchitis and Procalcitonin
Mostly acute bronchitis is caused by viral infections and do not need antibiotics. In patients where the need for antibiotics is unclear, serum procalcitonin levels can help in making this decision.
Summary
Table 2: Procalcitonin levels in lower respiratory tract infections:
Level (ng/ml)
Likelihood of bacterial infection
<0.10
Very unlikely
0.10 – 0.25
Unlikely
0.25 – 0.50
Likely
>0.50
Very likely
(This should aid clinical decision making i.e. decision should not be solely based on these levels).
In an acute clinical setting, where pneumonia is suspected or is the cause for sepsis, empirical antibiotics should be started according to a local protocol without considering the serum procalcitonin levels. If serial serum procalcitonin levels remain below 0.10 ng/ml on day 3, antibiotics can be stopped, aided by clinical judgment. The above-mentioned points should be kept in mind with the fact that certain bacterial infections do not cause a rise in serum procalcitonin levels. The levels also have prognostic value in case of CAP and VAP. Usually, acute bronchitis is a viral illness; if symptoms are not improving or bacterial infection is suspected, raised serum procalcitonin levels can aid the clinical judgment in starting antibiotics. In the case of infective AECOPD, the levels are not very helpful in making a decision about starting antibiotic therapy. In respiratory tract infections, where the patient has received adequate duration of antibiotic therapy, and procalcitonin levels fall <0.10 ng/ml, treatment can be stopped safely (if clinical judgment allows). See Table 2.
Psychiatric trainees in Iraq face many challenges that limit their immediate access to improved training opportunities. These include limited access to classroom teaching, regular clinical supervision meetings and fewer opportunities to attend international conferences and placements. These challenges are more acute in those specialities with the greatest shortage of consultants (for example, forensic and child and adolescent psychiatry).
Furthermore, the fragile security situation in the capital and larger cities and the post-conflict disruption to educational institutions consequent to these difficulties makes it difficult for those in the UK and elsewhere to visit the country and support educators and training on the ground.
Against this background and as a medical educational team in the UK (Oxford University Medical Education Fellows, OUMEF) with an interest in developing training opportunities for peers and colleagues in Iraq, we set up the Oxford Psychiatry in Iraq (OxPIQ) Project, beginning with a project development team that included Medicine Africa, an experienced online distance learning platform.
So what is the role of TEL in the delivery of online distance learning targeted at medical professionals in these circumstances?
Meeting the Challenge – the role of TEL
The concept of Technology-enhanced Learning (TEL), or Web-based learning (WBL), defined as the use of information and communication technologies in teaching and learning 1, is a relatively new phenomenon. Nevertheless, there is a considerable body of evidence supporting the use of TEL in various clinical and non-clinical settings.
Mccutcheon et al. 2 systematically reviewed thirteen studies and found that ten of these studies concluded that online learning is as effective as traditional or classroom teaching, despite the limitations of some of these studies.
In a large meta-analysis, Means and colleagues 3 concluded that students using online teaching performed modestly better compared to students learning similar material using face-to-face teaching. Combining face-to-face and online teaching resulted in larger benefit compared to the use of face to face methods only.
TEL can address the learning limitations in classroom settings due to expanding curriculum coverage and limits on contact time between students and lecturers/trainers alike. It can contribute to better use of such face-to-face classroom contact through the facilitation of the flipped classroom approach. 4 In this approach (also called inverted instruction and upside-down teaching), students acquire the basic information of the lesson outside the class (usually using online materials) and then develop their knowledge further in the class by sharing their learning, interacting with other classmates and teacher, and discussing various aspects of the study topic.These advantages have enabled TEL to revolutionise distance learning at many levels – enabling greater access to education by overcoming geographical and time-zone boundaries.
An allied concept within distance TEL is the concept of virtual teams 5 where health professionals come together to teach and learn from each other independent of location. Of itself, this offers some advantages. These include the possibility of addressing speciality-specific training gaps through the incorporation of the relevant expertise within the team - and to the creation of what is termed “connectivism”. This term refers to the use of internet technologies to enhance learning through online peer networks 6 and the development of communities of practice. 7 The latter allows for workplace-based learning with trainees learning from more experienced practitioners and moving towards the same through greater competency acquisition.
In a similar vein, creating networks of professionals may help to establish more longer-lasting relationships of mutual benefit between the UK and Iraqi professionals (e.g. through collaboration on training programmes, conferences, etc.). Also, cross-cultural online learning has been shown to be very useful in improving language skills and cultural awareness of learners and educators. 8 With language translation technology, any language difficulties can also be overcome, especially if the educator can observe the learners’ responses to the translated text and offered the opportunity to give further explanations and clarifications when necessary. 9 Finally, as well as sharing knowledge and experience within groups, TEL enables opportunities for mentoring and coaching individuals. 10
For our purposes, these findings and opinions support the use of online learning as a suitable distance learning “add-on” to existing training opportunities in Iraq.
TEL and Learning Theories
Learning theorists suggest that experiential and constructive learning theories are most appropriate to learning in the clinical context. Both are possible with TEL (as well as being facilitative of behaviourist and cognitivist approaches).
For example, the virtual classroom environment can enhance the learning experience of the participants by improving their analytical skills by thinking through case formulation and management plans. 11 Participants in online learning could be assessed and receive the feedback immediately. Ideas can be shared, and there is no passive acquisition or transfer of knowledge as is the case with traditional lectures. These aspects have implications for the design of the educational sessions and are discussed below in the learning methods section.
Challenges of Online Distance Learning
There are many challenges associated with online distance learning. Firstly, there is the potential lack of the required technologies (internet access, laptops or desktop computers), the expenses of subscribing to these online learning templates, the need to have technical support, and similar technical and logistic issues. 12 These technical problems may impair access to and functioning of the virtual team. The choice of an experienced online platform must, therefore, be considered carefully.
Secondly, there may be ethical issues about the protection of patients’ confidentiality in these sessions, especially when there are different laws of privacy that are applied in the UK and Iraq. This will require knowledge of the relevant professional requirements by the tutor team for example.
Furthermore, the student-teacher relationship has traditionally been underpinned by direct face-to-face contact and being present at the same time and place. 11 Therefore, learners and educators might be less satisfied with online learning. For these reasons, the concept of blended learning (careful integration of online learning with face to face learning experience) has been developed to overcome the limitations of a standalone online or face to face learning and has been found effective and applicable in various settings. 13
Thirdly, any distance online learning programme must understand and support existing “local” training provision and arrangements, in the classroom and the workplace. This requires liaison and cooperation with the training providers and institutions on the ground.
For clinical training to be relevant, it needs to reflect the learning needs of trainees in the workplace – in keeping with adult learning principles and cognitive apprenticeship models of learning. 14 The latter includes the importance of clinical decision-making underscored by the higher levels of Bloom’s (1956) cognitive domain. 15 To this end, then appropriate learning and assessment methods are needed to enable effecting learning.
In other words, while necessary, TEL may be insufficient in enhancing learning outcomes if allied learning methods are not chosen appropriately. Also, in our view, TEL is not a substitute for bedside teaching.
Table 1 summarises this appraisal of online distance learning (using the online platform provided by MedicineAfrica).
Table 1 Strengths and limitation of using MedicineAfrica (web-based virtual classroom environment)
Strengths
Limitations
Better use of the participants time and resources
Limited or lack of internet access
Overcome geographical barriers between two countries
Technical and logistic issues
Improve critical thinking and communication skills
Subscription expenses Appropriate choice of learning methods
Form long-standing professional networks
Ethical and legal issues (e.g., confidentiality)
Interactivity
Lack of direct face to face contact
OxPIQ & Project Development Team
OxPIQ is a partnership between Medicine Africa and psychiatrist members of the Oxford University Medical Education Fellows, with experience of working in Iraq. The Oxford University Medical Education Fellows (http://OUMEF.org) is a group of trainees from across medical and surgical specialities with interest in medical education and training.
Medicine Africa (http://medicineafrica.com) is an innovative clinically targeted online platform developed in collaboration with King’s College London’s Centre for Global Health, within the King’s Somaliland Partnership. Built at low bandwidth, it enables collaboration between medical professionals in the UK and those in remote or fragile states to enhance education in various clinical specialities using online sessions (live courses and mentoring sessions). Please see Appendix 3 for a screenshot of one of the active sessions of OxPIQ.
The next step was to invite representation and support from the Iraqi Board of Psychiatry and the Medical Education Unit in Baghdad. These developments led to the formal launch of OxPIQ Partnership in March 2016. Later on, the many UK and Iraqi doctors joined the Partnership as tutors and learners.
The Virtual Learning Team: Trainees, Specialty Consultants & Tutors
Iraqi psychiatry trainees were then recruited, and their more pressing learning needs to be appraised based on their views and those of the Iraqi Board of Psychiatry supervisors. Learning needs to emerge included the management of older patients with dementia and functional disorders, assessment and management of children and adolescents (with autism and ADHD for example), forensic patients and those with drug and alcohol addiction. The team thus formed was composed of up to ten psychiatry trainees from Iraq and five senior psychiatrists/tutors each, from Iraq and the UK respectively. A schedule of fortnightly seminars was agreed and published on the learning platform. Case-based discussions were used as the main educational activity during these seminars.
Learning Methods and Processes
As noted earlier, the importance of experiential and constructivist learning methods are key to clinical education. Our literature appraisal revealed that they are essential elements of successful TEL in this context too. 16, 17 To these must be added learner engagement. 18
Virtual or online (anonymised) case-based discussions (CBDs) are valid and reliable learning tools. 16 They are interactive and centred around the students and their learning needs while a facilitator guides the process of learning. Learners are engaged through discussion of actual clinical cases, so preparing learners for real-life experience. 19 Also, expert facilitation and peer feedback to trainees promotes clinical knowledge and skills’ development. 20, 21
Effective small group teaching is characterised by four main strengths: flexibility, interaction, reflexivity and engagement. 22 Flexibility is when the teacher responds to the needs and learning of the students dynamically and helps them to explore wider pedagogic spaces. A higher degree of interactivity is usually seen in small group teaching compared to a larger group. Teachers are better able to continually engage in self-reflection and listen sensitively to students in a small group and observe the dynamics between the members of the group, leading therefore to better reflexivity. Engagement refers to encouraging the students to develop their academic identity and engage in lively debate about the various aspects of the topic discussed.
We aimed to replicate these characteristics. For example, a small group discussion allowed better interaction with each participant (interactivity); the presence of chat windows enables the facilitator to self-reflect on the process, monitor engagement and respond reflexively using questions and answers to stimulate interest and respond flexibly to individual trainee knowledge gaps. Tutors are encouraged to identify trainees’ learning needs and facilitate interactivity, and timely feedback as these are highly valued by the participants and help to keep them motivated and engaged. 18
For further reading in this area, we recommend Brindly and colleagues’ 23 ten strategies to increase students’ motivation towards and engagement with online learning (see table 2).
Table 2- Strategies to increase engagement in online teaching (modified from Brindly and colleagues, 2009) 23
1. Transparency of expectations: Making the learning objectives very clear and relevant to the participants learning needs. The teachers must be open to the learners’ suggestions and must be willing to discuss the process and purpose of the educational activities.
2. Clear instructions: The educational activity, its timing, duration, and the technical aspects are described in detail to the participants. They should not be left to ‘try out things’ and must be guided explicitly.
3. Appropriateness of task for group work: For the online activity to succeed, individual versus group tasks should be differentiated. In our example, this may be done by asking the participants to do a particular task before the session (e.g., read about severe and enduring mental illness), and then to work together on producing a formulation for the case discussed. This will increase their motivation to be involved in various tasks.
4. Meaning-making/relevance: The case-based discussions (and any online activity) should have relevance for the participants and aim to enrich their experience in their clinical work.
5. The motivation for participation embedded in course design: It is essential that participants in the online activity understand that the success of the group and the course depend on the individual effort of each participant.
6. The readiness of learners for group work: This aspect describes the development of a sense of community through a professional relationship which leads to better collaborative work.
7. The timing of group formation: Before the participants join in the educational activity, it is preferable to have some discussions before the tutorial on their learning needs to allow a time for rapport to develop to enable better group activities.
8. Respect for the autonomy of learners: Joining and leaving the educational activity (and the whole online course) should be voluntary. No penalties should be attached to leaving the course. Learners should have the freedom to choose what aspects of the online course is relevant to them.
9. Monitoring and feedback: The tutor should monitor the progress of the participants, and timely feedback is given respectfully to enhance the engagement and motivation of the participants. Please see Appendix 1 (lesson plan) for more details on feedback and evaluation.
10. Sufficient time for the task: Participants should be given time to be actively involved in the session. This is particularly important in a distant learning session when issues related to sound quality or speed of internet connection may prevent some participants from engagement.
The focus of the Lesson Plan Design
To these ends, the focus on the lesson design was on using problem-based learning methods (e.g. CBDs) within a small group setting (between 4-12 members) and a format that promoted learner engagement. A sample lesson plan is provided in Appendix 1.
In practical terms, tutorials were held fortnightly in term-time. All participants received an email notification to inform them of the session topic, and the tutor uploaded the slides from the session to the website beforehand. Participants logged-in to the site (http://medicineafrica.com) and interact with the tutor by voice (requiring only simple microphone equipment) and by writing in a chat window.
Evaluation and feedback gathering
The evaluation of the effectiveness of these sessions was reliant originally on trainees’ immediate reaction (table 3, level 1 evaluation, Kirkpatrick 24) using formal feedback tools provided online by MedicineAfrica. This feedback was shared with tutors and the Project Team. Please see Appendix 2 for the template used in collecting feedback after each session.
Subsequently, members of the project team approached trainee representatives, tutors and Iraqi Psychiatry Board leads separately for further feedback and appraisal of learning needs. Furthermore, some months after a tutorial we have asked trainees for evidence of learning across the higher levels of Kirkpatrick’s evaluation model.
Regular feedback from the Iraqi and UK participants has been positive. The sessions have been associated with improved clinical knowledge and skills of the Iraqi Psychiatry Trainees. Requests for certificates of tutorial participation have been agreed upon and provided by the project team addition, so supporting learners’ (and tutors) portfolio development.
Table 3 Kirkpatrick’s (1996) Levels of Training Assessment
Level
How to assess
Level 1: Reaction (the participants feeling about the training
Feedback during and after the tutorial using the feedback questionnaire
Level 2: Learning (improving the participants’ knowledge)
Post-tutorial questionnaire and interviews
Level 3: Behaviour-also called Transfer (improving the participant's performance)
Direct or indirect observation and assessment of the skills and competencies of the trainees
Level 4: Results (cost-effectiveness, engagement, sustainability, adherence to evidence-based practices)
regular meetings between the participants, tutors, and stakeholders.
Further cooperation
A surprising (and very welcome) outcome of the project was, through the facilitation and support of the Iraqi Board of Psychiatry, the introduction of educational workshops in Baghdad. These workshops were held in Medical City, Baghdad, in May 2017 and April 2018 and were facilitated by tutors (YH & H Al-T) from the OxPIQ Partnership. They covered targeted topics such as old age psychiatry, addiction, organic and forensic psychiatry. Trainees and senior psychiatrists from Iraq attended; their feedback showed how they valued the interactive nature of the teaching and use of CBDs as learning methods, resulting in high levels of engagement.
Conclusions
This paper describes the process of designing, delivering, and the early evaluation of an online distance TEL programme for mental health professionals based in the UK and Iraq.
TEL has had an important role in overcoming the geographical barriers and other challenges to developing training opportunities in Iraq and other developing countries. We are of the view that it could be used more often to connect professionals working in similar circumstances and with other disadvantaged groups, including refugee and asylum seekers. It is a flexible way of providing training to professionals working with those groups in relatively remote and resource-deprived environments.
Greenhalgh 25 suggests that three factors are needed for the success of online educational activity: ease of access, perceived usefulness of the activity to the learning requirements of the students, and the interactivity of the session. In our experience, these are important. Also, we believe that additional consideration should be given to (i) working with an experienced online platform provider; (ii) working with local educational institutions, trainers and learners to identify unmet learning needs and support existing learning opportunities/programmes; and (iii) adopting an iterative approach to feedback and evaluation.
Appendix 1: Example of a Lesson Plan
Session title
Case-based discussion on management of severe and enduring mental illness.
Duration of session
60 minutes
Tutor
A UK-based Psychiatrist
Learner group
Psychiatry Board Trainees and Senior Psychiatrists in Iraq and UK
Step 1– Learning outcomes
a) Describe the various stages in the management of the cases discussed during the session.
b) Enhance the participants learning using case-based discussion with peers and seniors in the UK and Iraq.
c) Improve the presentation and discussion skills of the participants and their communication skills.
d) Explore ethical, cultural, and social issues related to the management of mental disorders and improve cultural competency and awareness.
Step 2 – Learning Plan
Introduction to the online tutorial -10 minutes
a) Highlight the learning objectives of the tutorial
b) Stimulate the thinking of the participants by asking about their current knowledge of the subject, whether they managed similar cases in their clinical work, and what are their learning needs.
c) Outline the tutorial structure and further engage the participants by informing them about other details (e.g., if they can ask the question during or after the case presentation)
2. The tutorial in a case with severe and enduring mental disorder – 30 minutes
a) Participants are encouraged to interact with the tutor who should be invited to keep the tutorial interactive.
b) The case presented will provide an overview of the patient’s journey from the initial presentation, followed by the investigation, then treatment plans. Discussions of the differential diagnosis are important.
c) The tutor will assess the knowledge of the participants by asking questions on the various aspects of the case presentation (e.g., what is your differential diagnosis for a patient presenting with auditory and visual hallucination? What investigations would you request?).
3. Recap and Q&A time- 20 minutes
a) Tutor to give a summary of the main learning points from the tutorial and linking these to the learning outcomes presented at the beginning.
b) Participants are given enough time to ask questions and to participate actively in the session.
Step 3 – Assessment
Before Lesson
Before the tutorial, the tutor should know the current educational curriculum of the participants and their learning outcomes in that subject. UK and Iraqi Psychiatry curriculum are different, and therefore knowing what is relevant is important.
Stating the learning outcomes at the beginning of the tutorial will also help in the baseline assessment of the knowledge and skills of the participants.
Pre-session questionnaires could be used as well (for example, asking questions on the prognosis of various mental disorders and comparing the participant’s knowledge before and after the session).
After the lesson
· Ongoing assessment during the tutorial using questions on various aspects related to the case presented.
· Questions in the recap section at the end of the tutorial.
· Post tutorial feedback forms will allow the participants to give their views about their learning needs and if they feel the tutorial was relevant to their learning outcomes.
It is important to provide personalised feedback to the participants about their performance on these assessment tools as this will help them to identify gaps in their knowledge and improve their learning. 26
Step 4 – Resources required
MedicineAfrica is free to join and designed to work well even with low bandwidth. Hence it won’t be affected by slow internet connections which are likely to be the case in developing countries.
Trainees and Tutors will need a computer (desktop or laptop) with an internet connection. No other resources are needed. Recommended readings could be disseminated by email to the trainees after the session.
Step 5 – Evaluation
Student evaluation
Gathering feedback is an essential step to influence the learning outcomes favourable and continue to improve the structure and content of the tutorials (After the tutorial, the participants will be asked to fill an electronic feedback form (please see Appendix 2).
The form contains various questions with rating (from 1-5, ranging from strongly disagree to strongly agree) on various aspects of the tutorial. These include structure, organisation, the range of aids used and meeting of the learning outcomes.
Also, direct feedback from the trainees, tutors, facilitators, and the stakeholders responsible for running the online learning platform is gathered to assess the effectiveness of these tutorials.
Teacher evaluation
Professionals invest a significant amount of time and efforts in these lessons, and it is imperative to assess how the tutorials could be improved to meet the needs of the trainees and keep them and the tutors motivated and interested. Tutors in these tutorials meet regularly using Skype to reflect on their teaching sessions and discuss ways of improving the delivery and quality of the tutorials.
Mutual learning is another aspect that needs to be assessed (is the tutor also benefitting from these lessons, for example, by improving their cultural competencies or their teaching skills).
Appendix 2: Feedback form to be completed by the participants after the session
Session title
Case-based discussion on management of severe and enduring mental illness.
Speaker
Date
Content
The session was relevant to my training needs
Strongly disagree 1 2 3 4 5 Strongly agree
Organisation
Sufficient time was allowed for the session
Strongly disagree 1 2 3 4 5 Strongly agree
Presentation
The session was well presented
Strongly disagree 1 2 3 4 5 Strongly agree
The session was delivered at the right pace
Strongly disagree 1 2 3 4 5 Strongly agree
The session was interactive and encouraged discussion/questions
Strongly disagree 1 2 3 4 5 Strongly agree
Structure
The session was well organised and structured
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were clear
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were met
Strongly disagree 1 2 3 4 5 Strongly agree
Overall evaluation
Overall, I would rate this session as
Extremely poor 1 2 3 4 5 Extremely good
Appendix 3: MedicineAfrica screenshot during an active session
The recent increase in the number of patients presenting with a borderline personality disorder (BPD) in general adult psychiatry and primary care is creating pressure within the National Health Service (NHS)1.Currently, BPD is perceived to be like an ‘epidemic’ entity, particularly in areas with a high incidence of socioeconomic deprivation. Similarly, there is a parallel increase in the human and medical resources needed to manage this disorder efficiently. In fact, the authors have found that BPD tends to be comorbid with factitious disorders and depression (Tripolar syndrome) with a tendency to overuse hospital and medical facilities, inclusive of Accident and Emergency (A&E) departments, family doctors and General Practitioner (GP) surgeries2.
Consequently, patients with BPD require a constant and unlimited allocation of medical and psychiatric resources, together with targeted care plans. In fact, they might be prone to frequent self-referrals to A&E, seek hospital admissions and augment all their psychotropic medications in order to deal with their on-going crises not solvable in their homes. Also, the skills needed by healthcare personnel to reduce chronic self-harming and suicidal ideation in this vulnerable population are complex and need to be updated on an on-going basis also due to the tendency of these patients to raise allegations towards their healthcarers3. Nonetheless, the provision of treatment is often hindered by various healthcare system limitations, such as the lack of beds on medical and psychiatric units, forced reduction in the length of stay in a hospital and insufficient human resources. This scenario has mostly affected female patients with BPD who seek admission to psychiatric hospitals often for respite from chronic suicidal ideation4.Moments of amplified suicidal ideas become evident when internal voices, perceived as auditory hallucinations commanding to self-harm or to commit suicide, become more intense5.
As observed by the authors of the current editorial, increased suicidal ideation in persons with BPD also occurs during minor crises in life, when experiencing intensified flashbacks about past abuses, during minor losses, after significant conflicts with others and after the separation from influential people in their social network. Besides, admissions in psychiatric wards, very commonly, occur when there is an intensification of internal voices commanding BPD patients to take overdoses of the prescribed medication or to jump in front of a train, a car or off a pier to commit suicide. Police is often involved to stop these dramatic plans. At the same time, healthcare professionals are discouraged by the complex management of patients with BPD, which, in combination with their tendency to challenge or make unwarranted allegations against their health carers, results in feelings of sadness, rejection and alarm in the latter. Kanin reported that the reason to produce a false allegation is to create a defence or to get compassion6. Nonetheless, it is also likely that some healthcare professionals might have some preconceived ideas about people with Borderline Personality Disorder, which might reduce the depth of health carers’ empathy towards these patients and lead to burnout after prolonged treatment of BPD in hospital or community. Attempts to treat and to reduce suicidal ideation and self-harm in this group of patients are often thwarted as they challenge medical decisions and endeavour to sabotage the proposed care plans. The strain on the doctor-patient relationship is determined by the underlying ‘Mistrust/Abuse’ scheme of patients with BPD who expect from others, and are thus sensitive to, signals of relational wound, treachery and abuse7.
Consequently, a chronic feeling of inadequacy in patients with BPD translates itself in enduring dissatisfaction with any therapy and healthcare professionals. Hence, in the authors’ experience, any attempt to establish a long-term therapeutic relationship with BPD patients might have limited outcomes. Frustration in healthcare professionals aiming to create an enduring therapeutic alliance with patients with BPD happens as these patients tend to interpersonal biases and to ascribe undesirable experiences to people (hence to healthcare professionals) as opposed to circumstances8. Therefore, social interactions with primary carers result in dissatisfaction of people with BPD about any medical or psychiatric plan is set up for them. Consequently, community teams, general practitioners and hospital staff feel hopeless due to recurrent readmissions of people with BPD and the lack of definitive treatment for such pathology. Stress caused by difficulties encountered in ensuring that BPD patients comply with the therapy regularly places doctors and nurses at crisis point.
Once in the hospital, discharging patients with BPD can be difficult as they are frequently reluctant to return to the community, leading to recurrent readmissions within a short period. In fact, the period before discharge from a psychiatric hospital is complicated by mounting anxiety and distress in patients with BPD. The authors observed a regular escalation of self-harming behaviours and increased suicidal ideation in these patients just before discharge, possibly indicating their underlying anxiety in going back to the home environment. Many BPD patients suggest that they would rather stay in the hospital instead of returning to the community that is considered by them as unsafe or unstructured. Furthermore, as these patients have an intense vulnerability to social rejection, they rarely feel adequate during social interactions thus developing an enduring sense of solitude9. Therefore, any hospital discharge or a visit to the GP will be interpreted by them as disappointing and will lead patients with BPD to confirm their sense of rejection. As a reaction, the authors observed that BPD patients demand endless and unconditional attention from their primary carers. Attempts by patients with BPD to self-harm or commit suicide intensify over weekends or public holidays as their sense of solitude increases during these periods, especially when there is also a shortage of healthcare professionals available for immediate support.
The authors of the current editorial propose possible strategies of intervention both on the psychopharmacological and managerial side. The challenge is that patients with BPD often use overdoses of oral medication in a suicide attempt10. Hence, the authors recommend the use of long-lasting depot antipsychotic injections (e.g., Zuclopenthixol Decanoate) to stabilise their mood and reduce impulsivity, the risk of overdoses, pseudo-psychotic symptoms and command hallucinations leading to deliberate self-harm. The use of oral lithium to treat mood swings poses an ethical dilemma for doctors as it could be lethal when used as an overdose. Healthcare management is another way of intervention. One point of difficulty is the tendency of patients with BPD to split their teams and to create niches of protectors and opposers within staff with possible conflicts within the team that is treating them. In this case, inter-professional coordination, integrated care and constant information sharing are required11. Furthermore, several healthcare services treating patients with BPD are trying to find an integrated approach for their hospital and community treatment. The authors speculate that the increased number of admissions of patients with BPD is reducing the total capabilities of physical and mental wards to treat patients with other pathologies. Besides, the dramatic presentation of patients with BPD who tend to overuse the healthcare services poses ethical dilemmas in their management. This scenario has created discrepancies in health care policies about treatments and hospital (re)admissions of patients with BPD reaching an epidemic magnitude in many healthcare trusts. Hence, a new culture is required for the management and treatment of patients with BPD in the community.
Culture is defined as the character of an institution that affects employee gratification and organisational accomplishments12.What is needed is a frank and constructive dialogue between healthcare managers, leaders and medical staff in the hospital and in the community. Furthermore, clear and regional guidelines should exist to improve the efficacy of care which is offered to BPD patients at home and to reduce the constant risks which patients pose to themselves, their sense of solitude and their tendency to seek hospital admission in order to solve chronic existential difficulties. A model of integrated care comes from Max Weber who differentiated between ‘formal rationality’, the endorsement by healthcare managers of the most efficient ways of achieving organisational goals (e.g., ensuring more hospital beds by quick discharges of ‘bed blockers’), and ‘substantive rationality’, the expectation by healthcare professionals that values and morals should instead be based on tradition, compassion and dedication13;pertinent to the care of BPD patients in our case. The collaboration of all those involved parties is also important to reduce the risk of ‘silo management’ where confined and regional policies do not embrace a wider perspective for the management of specific problems while responding only within the confines of the own guidelines and procedures14.In these cases, integrated care in communities can halt self-harming and suicidal attempts of patients with BPD. The organigram sees inter-professional actions, targeted psychopharmacological policies and psychiatric crisis teams in A&E that can reduce the need to hospitalise patients with BPD at any ensuing crisis.
Physicians pursue the interest that during the hospital stay the best patient care needs to be provided; and achieving that in a short time - as a result the patient is expected to recover from illness and return to normal life.
The ability to prevent possible complications that the patients are exposed to, has always generated ambiguity in the current medical practice, since it is assumed, that the relief of the patients once the treatment is established, should always be the same1. However, it is the awareness and proper care of comorbidities and the baseline condition of the patients that determine the success rate of the treatment, without requiring additional interventions beyond the ones proposed at the beginning of the treatment 2, 3.
This important factor has generated in practitioners the need to be able to monitor the clinical evolution of the patients. Laboratory tests are an important basis of medical diagnosis, and are frequently used to monitor the clinical progress of the hospitalised patient. The patient clinical state sometimes changes suddenly or continuously; requiring the surveillance of the basic variables such as vital signs. Vital signs monitoring activate a warning signal for the immediate reassessment of the patient and reorient the medical decisions at any moment during the hospitalisation, with the goal of avoiding further deterioration or adequately treating any new disease state that the patient may develop 3, 4.
From that point of view and long time ago the medical community has observed the need to generate a code that could be universal and that could be used as an early warning of the patient worsening. As a result of this situation, in different countries around the world, researchers and clinicians have developed scales, scores, algorithms and others tools to identify early patients in risks to be in critical conditions. Those tools are based on the ability of easy data collection and simple clinical interpretations allowing the clinical personnel to make objective and early assessment of the overall clinical state of the patients 4.
These scales or scores are not ideal, since there is no perfect scale, and all have statistical weaknesses either in their sensitivity or specificity. The clinical judgment and the physician experience, added to a score from any of these scales, may guide the path to follow according to the particular scenario to treat the patient illness 5.
Selecting the ideal scale to be adopted is one of the controversial topics in which a practitioners and institutions can be involved in. Occasionally other services in the hospital such as clinical laboratory and clinical imaging values play an important role in the process of diagnosis of the disease and are counted in the risk scales making easier to have good standard of care. Scientific studies assess the statistical performance of these scales yield controversial results that sometimes distort or endorse these results 5. This is why the decision of the ideal scale is based first on the target population that physicians in charge will care of and select the appropriate scale or score that will be applied, to know the implications of the most representative age group of patients that will be attended and to use scales which data acquisition be a simple and quick task to perform6.
Based on that, the Royal College of Physicians of the United Kingdom headed by Bryan Williams and collaborators, and many other researchers worldwide have analysed a significant number of scales on the basis that the scale should use systems (track and trigger warning systems protocol) divided into three types. Single parameter systems, multi-parameter systems, total weighted scoring systems and combined systems 6.
The researchers came to the conclusion that the performance of these scales was better than those that conserve the third type of system, since not only the parameters are categorized but also those who develop the scale proposed management to be carried out in an easy, orderly scheme and logical within a framework of independent work or in addition to more robust strategies that involve management schemes within a hospital institutions - the so-called (Rapid Response Systems RRS) 7.
For Williams et al, the MEWS changed its name after being accepted by the Royal College of Physicians of the United Kingdom as the NEWS scale with its variables defined as (respiratory rate, oxygen saturation, systolic blood pressure, heart rate, consciousness or new confusion and temperature). This score has been recognized and quickly adopted worldwide. The NEWS has an immediate applicability as a parameter of high sensitivity in the detection of clinical deterioration, despite its known low specificity. Thus inviting the attending physician to approach and reassess the state of the patient. The score makes changes in medical decisions according to the new conditions found during the patient’s assessment7.
This kind of scales must be endorsed internationally and be easily replicable by all practitioners who wish to adopt them. This allows other physicians to obtain results when implementing actions, reaching better clinical outcomes similar to clinical studies previously published. In the daily practice and clinical application we find different scenarios to use the scales, where the main problem of its application represent extra costs in lab test or clinical images and the time invested by the practitioners and medical personnel 7.
For this reason, the scales for clinical assessment should be easy and flexible to be implemented by any person, ideally for any member of the healthcare team to avoid barriers during the process of data acquisition. From this perspective, the scales that are based on easily collected parameters are the most appropriate, but they are often the scales that suffer the rigors of the biases when they are undervalued or overvalued, just the operability can be affected by personnel knowledge and skill.
The interesting thing about this exercise is to see that the people who have the most continuous contact with the patient, such as the nursing staff, physicians with the practice have the ability to use them in their practice and this would make the scales a valuable resource to perform clinical assessments and achieve the goal proposed.
In this new era where the reincorporation of a patient into daily life in a short time is ideal scenario, the medical and nurse staffs and also service providers seek to alleviate the patient's health breakdown. It is here from the hospital point of view where the proper care not only in the quality of care but also in the prevention of complications plays an important role in the applicability of these early detection scales. This is an invitation to success from its inception and to tend to patients being hospitalized for the minimum time required.
A dermatoscope is a hand-held device for examining the appearance of the skin. Dermoscopy has become an increasingly used and valued tool in the assessment of various skin lesions, and more recently, inflammatory rashes. It is quick, cheap and when used correctly, dermoscopy is an essential tool in helping clinicians detect early stage skin cancer. Various national and international guidelines recommend routine use of dermoscopy in the assessment of pigmented lesions1,2 because it enhances melanoma detection rates3,4 and can help confirm the diagnosis of benign lesions such as haemangiomas and seborrhoeic keratoses. As with any skill, competency takes time to develop and a combination of various learning and assessment methods is best. The dermatology specialist training curriculum in the United Kingdom (UK) states that trainees should be competent in using a dermatoscope and interpreting findings, while recognizing the limitations of this tool5. Assessment of these clinical skill and behavioural competencies using direct observation of procedural skills (DOPS), case-based discussion (CBD), mini clinical examination (mini-CEX), and/or multisource feedback (MSF) is suggested. There is no specific guidance on what resources a trainee should use to achieve these competencies, nor on what is the minimum expected dermoscopy skillset at completion of specialist training.
The aim of this survey was to explore dermoscopy use amongst dermatology specialist trainee registrars in the UK including frequency of use, how it is being taught and whether trainees feel their dermoscopy training has been adequate.
An online survey was designed and distributed to dermatology trainees in the United Kingdom using an email link and hard copies were distributed at a national dermoscopy course. Respondents who did not identify themselves as dermatology trainees were removed from the analysis. Responses were collected anonymously, then collated and analysed using SurveyMonkey® computer software.
Twenty-five percent (59/238) of dermatology trainees completed the survey. On average, 92% (54/59) use dermoscopy more than once daily. Eighty-five percent (50/59) always use dermoscopy when assessing pigmented lesions while 34% (20/59) always and 59% (35/59) sometimes use it to assess non-pigmented lesions. When asked about specific tools used to learn dermoscopy, 41% (24/59) have been on a previous course, 42% (25/59) reported attendance at a lecture or seminar, 46% (27/59) have used a dermoscopy text book, 14% (8/59) have attended a conference, 19% (11/59) have used online resources. Seventeen percent (10/59) have never used any of the above learning methods. (Figure 1a). Amongst those who have attended a formal dermoscopy course (n=24), 92% (22/24) of these were ≤1 day in duration. When questioned about informal teaching in clinical practice, 12% (7/59) frequently, 56% (33/59) sometimes, 31% (18/59) rarely and 2% (1/59) never receive teaching from their supervising dermatology consultant. (Figure 1b). Fifty-four percent (32/59) feel they have received adequate training in dermoscopy while the remaining 46% (27/59) feel their dermoscopy training is inadequate for their training stage (Figure 1c). Seventy-three percent (43/59) have access to dermoscopic photography within their local dermatology department.
Fig 1a - Have you undertaken any formal study in dermoscopy? 49% of trainees have attended a lecture, 2% a seminar, 14% a conference, 41% a course, 19% have used an online resource, 46% have used a book, 17% have not used any resource.
Fig 1b- Do you receive dermoscopy training from your supervisor in clinic? 56% of trainees sometimes, 31% rarely, 12% frequently, and 2% have never received training from their seniors in clinic.
Fig 1c- Do you believe that you have received adequate training in the use of a dermoscopy for your training grade?
These results of this survey highlight the need for dermoscopy training to be reviewed within the UK national training curriculum for dermatology. Despite daily use by the vast majority, dermoscopy training is largely self-directed and highly variable amongst individual trainees. Of concern, a significant proportion of those who responded feel their dermoscopy skills are inadequate for their training stage. Of note, the 25% response rate means that the results of this survey may not be representative of dermatology trainees in the United Kingdom as a whole.
This is the first time that dermoscopy use has been explored through a national survey of dermatology trainees in the UK, to the best of our knowledge. A survey on dermoscopy use was carried out by The British Association of Dermatologists (BAD) in 20126 but the majority of responses were from dermatology consultants. This confirmed that 98.5% of respondents regularly used dermoscopy, while 81% had received any training. The most frequent source of training was UK based courses, which 62% of respondents reported attending. Of note, 39% of all respondents lacked confidence when making a diagnosis based on their interpretation of dermoscopy findings. It is not clear how many of those lacking in confidence were consultants, trainees or specialty doctors. Although the situation may have improved since 2012, these results do suggest that dermoscopy training needs have not been met for a proportion of doctors across the dermatology community.
Dermoscopy training is an important issue to address for several reasons. The volume of cutaneous lesions being referred to dermatology is increasing, and skin cancer referrals and treatment now account for 50% of a UK dermatologists’ workload7. For every melanoma diagnosed, a dermatologist may expect to see 20–40 benign lesions referred from general practitioners (GPs)7. These facts highlight the importance of maximising diagnostic skills which frequently include using dermoscopy as part of clinial assessment. Lack of adequate training is a common self-reported reason for dermatologists not using dermoscopy8. Both trainees and their supervising bodies have a responsibility to maximize training opportunities and embed the use of dermoscopy in routine practice.
In conclusion, we feel UK dermatology trainees and indeed any clinician who utilizes this tool, would benefit from a more standardized and integrated approach to dermoscopy teaching to ensure safe practice of this skill and deliver high quality evidence-based patient care.
SSRIs (Selective Serotonin Uptake Inhibitors) are very commonly used in Depression and Anxiety. Though considered as safest antidepressants, they have some common side effects which include gastrointestinal side effects, headache and at times sexual dysfunction. Yawning is one of the rare side effects of SSRIs. SSRIs were found to be the commonest cause of not so common drug induced yawning in a meta-analysis1. Isolated cases of intractable yawning have been reported with citalopram2 fluoxetine, citalopram and sertraline3 in the literature .Excessive yawning can cause injury to Temporo-Mandibular Joint (TMJ) 4. Paroxetine has also been shown to cause intractable yawning5. Yawning possibly helps in thermoregulation and is an unconscious effort by the body to cool the brain 6, 7. It is known that yawning can be contagious. Reading, talking, seeing someone yawn or even thinking about yawning can induce yawning in the subjects8. Susceptibility to contagious yawning is different for different individuals depending upon their ability to process information about self9.
Case
A 60 year old postman presented with his first episode of depression. He attended the GP who started him on sertraline (an SSRI). He developed serious headaches and did not notice any therapeutic benefit. He was then referred to the psychiatric services for further management. He was assessed, Sertraline was stopped and Cipramil 20mg was introduced. He was reviewed after 2 months and the dose was increased to 40 mg to which he responded partially but relapsed within 4 months. There were no changes in his psycho- social circumstances. Cipramil was stopped and he was started on fluoxetine 20 mg. Once again the response was partial and was overshadowed by midnight insomnia and increased sleepiness in the daytime. Fluoxetine was increased to 40 mg and he was reviewed after 4 months when he reported clear and significant improvement in his depression but complained of “excessive yawning spells” causing him problems at his work place. The psychiatrist was surprised at the number of times he yawned at the Out Patient Clinic review. On further discussion it became clear that this side effect had become highly troublesome. He complained that his jaw was in severe pain. He was unable to do his delivery rounds and was having clear episodes of attention lapses leading to letters being put to wrong addresses. He was transferred to “sorting” the post at sorting counters and was taken off delivery rounds. Even here the intractable yawning continued and he was committing sorting errors. By now it was affecting his colleagues too and they also started yawning (it is known to be contagious).It was affecting his self-confidence and was extremely embarrassing in all social situations to an extent that he started avoiding social interactions. He was drowsy all the time. He was clearly suffering more due to excessive yawning than due to depression. He was unable to perform his employment duties and was signed off sick. At that point the dose of fluoxetine was reduced to 20 mg .After a couple of weeks his yawning reduced significantly but was still disruptive to his routines. He was advised to slowly taper off fluoxetine over next 4 weeks. Unfortunately his depression relapsed and his GP restarted him on Fluoxetine 20 mg. He was reviewed by the psychiatrist after a couple of weeks. Once again he reported return of intractable yawning.
Fluoxetine was stopped once again and he was started on Mirtazapine 15 mg. There was very little response. The dose was increased to 30 mg after around two weeks. This led to him to experience nausea and vomiting. Unfortunately Mirtazapine too had to be stopped. He was then tried on amitriptyline 50 mg which improved his sleep and symptoms of Depression. He was reviewed in the outpatient clinic after a couple of months .He did not develop any side effects and responded quite well. He then started his job starting from part time to full time within 6 weeks. After 6 months on the same dose of amitriptyline, did not have any symptoms of depression and was finally discharged from the mental health services.
Discussion
SSRI is the first line antidepressants used in the treatment of depression and Anxiety disorders. They are known to have least side effects and safest when it comes to overdosing. Intractable Yawning is quite an unusual and uncommon side effect. One has to be conscious of the fact that it may cause yawning that can be pathological and can cause severe disruption of patient’s life. It can contribute to poor compliance. It is quite easy to overlook and ignore this side effect as yawning usually seems to represent sleep problems which is also a significant feature of the associated depression itself.
Excessive yawning can cause Jaw/facial pain. It can even cause dislocation of temporo-mandibular-joint. It can cause severe problems with one’s work and self-esteem. The sufferer might be misunderstood for being inattentive, indolent and sluggish. It might affect relationships with spouse/friend/relatives and especially at place of work. It can be misunderstood by doctors and lead to unnecessary tests and investigations. One has to be aware when prescribing SSRIs in patients who are driving or are involved in handling heavy machinery, athletes, airline pilots, surgeons, life guards, air traffic controllers and many other professionals. Due to its contagious nature, it’s not only the patient who is affected but also others around him. Excessive yawning can adversely affect the level of arousal, the level of concentration and work efficiency leading to poor performances in tasks requiring undiverted attention.
Hence excessive or intractable yawning has to be kept in mind while prescribing the so called most safe anti-depressant class of medication, the SSRIs, in this case fluoxetine.
The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure has long reported chronic hypertension as affecting over one billion individuals worldwide1. While the role of primary care providers in the long term management of this ubiquitous condition cannot be overstated, the hypertensive patient can also present challenges to an acute physician when the control of arterial blood pressure reaches crisis level.
The What
The clinical entity extravagantly referred to as a hypertensive crisis describes an elevated systolic blood pressure of >180mmHg with diastolic pressure of >120mmHg. Within this category of acute presentations, two subcategories are defined – the hypertensive urgency and the hypertensive emergency. Flamboyant terminology aside, what distinguishes the latter ‘emergency’ from the former ‘urgency’ is evidence of acute end-organ damage. Emergencies therefore include various incipient pathologies of the cardiovascular, renal and central nervous systems. Fortunately these are less common encounters for receiving physicians, with a recent large multicentre study identifying acute pulmonary oedema (30.9%), myocardial infarction (17%), acute aortic dissection (7.9%), acute kidney injury (5.9%), cerebrovascular accident (22%) and hypertensive encephalopathy (4.9%) as features of hypertensive emergencies in 25.3% of hypertensive crises, with the remainder of the presenting population demonstrating a hypertensive urgency with inherent lack of evidence of end organ damage2.
The Why
The pathophysiology of acute hypertension remains yet to be fully elucidated, however authors in the field of hypertensive crisis3,4 appear to converge on the point of two common proposed pathophysiological events. A sharp elevation in systemic vascular resistance is thought to be one precipitating factor, with an aberrance of cerebral autoregulation of blood flow being another.
For the purposes of an acute clinician faced with a bleeping blood pressure monitor, what is perhaps more applicable to everyday clinical practice is the potential role of non-adherence to regular antihypertensive medications5,6as discussed below.
The Who
A longitudinal study carried out in Switzerland and led by Saguner7identifies several potential risk factors for manifestation of a hypertensive crisis. Female gender, obesity and concurrent somatoform disorder accompany hypertensive and coronary artery related cardiac disease as potential red flags. Perhaps unsurprisingly, a history of multiple antihypertensive therapies was also associated with greater likelihood of presentation with hypertensive crises, as was non-adherence to the same therapeutic regimen. The latter compliance related issue was identified as the most significant by the study’s authors.
Elderly patients and also those of African American ethnicity have been shown to demonstrate higher rates of hypertensive crises in general8, while Caucasian patients are reported to have higher rates of emergencies as opposed to the more benign urgency equivalent9.
The When
The findings of a comparatively small Italian hospital-based study10utilising 360 patients were recently supported by a larger United States-based analysis11of over 400,000 patients, with a seasonal variation in presentation of hypertensive crises noted. A winter peak and summer trough was reported by both groups of authors, suggesting transcontinental extrapolation of a potential seasonal phenomenon.
Evaluation
Comprehensive disposition notwithstanding, acute physicians are urged to adopt a targeted approach when considering a presentation with alarming blood pressure readings.
Present…
By nature of definition, the presentation of a hypertensive crisis encompasses a wide variety of symptomatology depending on whether a hypertensive urgency or incipient emergency is manifested.
The symptomatology of a patient demonstrating hypertensive urgency can be fairly non-specific to acute blood pressure elevation. A 2014 study into clinical presentation of hypertensive crises reported headache as the most prevalent symptom (74.11% of patients), followed by chest discomfort and dyspnoea (62.35%), vertiginous dizziness (49.41%), nausea and emesis (41.47%)12 as demonstrated in Figure 1.
Figure 1. Symptomatology in hypertensive crises (adapted from Salkic S, Batic-Mujanovic O, Ljuca F, et al12)
While all of these common presenting complaints can bring a patient to a physician’s attention, what often alerts the attending physician to the particular possibility of an acute hypertensive condition is the blood pressure reading obtained on initial assessment of the patient (for instance for triage purposes) even in the absence of overt symptomatology as reported above. Indeed, patients with minimal symptomatology may be prompted to present themselves for acute medical care by no more than the sounding of an ominous alarm on a home blood pressure reader or the disconcerted look of a perturbed primary care physician, sphygmomanometer in hand!
…and Past
The history taking process of an acute physician faced with a hypertensive crisis should target several key areas which may prove essential in differentiating a case of urgency from an evolving emergency. With the potential for end organ heart, kidney and brain-related complications in mind, a physician should probe the possibility of chest discomfort, dyspnoea and signs of congestive cardiac failure (as indicators for incipient cardiovascular complications), headache, visual changes, dizziness and altered consciousness (potential harbingers of neurological complications) as well as recent history of oliguria as a marker of possible related renal insult.
Having conducted an interrogation for worrisome symptomatology, evaluation should proceed to a ‘hypertension history’. Prior diagnosis of hypertension and hypertensive crises in particular should be elaborated on, with this including a history of any prescribed regular antihypertensive therapy and both the adherence to and effect of the latter. Relevant to the notorious polypharmacy patients, any history of concurrent medication use must be clarified so as to give an indication of potential interactions.
Of historical note is the potential for hypertensive crisis following interaction of tyramine with mono-amine oxidase inhibitors (the so-called cheese effect), while a provoked hypertensive crisis more relevant to modern medicine is the potential effect of illicit substances including cocaine and amphetamine-based products13.
Examination
As with the evaluation of the hypertensive crisis patient’s history, examination should place particular emphasis on distinguishing urgency from emergency.
Parameters
Assessment of vital signs can provide valuable indicators. Whilst initial systolic pressure is not necessarily a predictor of the ability to achieve a prespecified target range pressure within thirty minutes14, the presence of tachycardia has been shown to be an ominous sign more prevalent in emergency than urgency, with a strong statistical association demonstrated with hypertension-related left ventricular failure15.
Physical
Cardiovascular examination should assess for the presence of signs of cardiac failure (including an elevated jugular venous pressure, added S3 heart sound or pulmonary rales) as well as the feared asymmetric pulses or new mid-diastolic murmur associated with aortic dissection. Auscultation for renal bruits should be performed, and a neurological assessment for possible stroke indicators undertaken.
Whilst chronic hypertension patients will often have subtle fundoscopic abnormalities, ophthalmological review for evidence of acute changes including new retinal haemorrhages or exudates together with papilloedema should be carried out.
Investigation
The unique circumstances of individual presentations aside, the prompt acute medical investigation of a hypertensive crisis should include a minimum number of bedside, laboratory and imaging investigations16as suggested in Figure 2. Comparison of each of these to pre-existing baseline investigations may be invaluable in giving an indication of level of acute pathology and therefore care required.
Figure 2. Investigations in hypertensive crises
Bedside
Electrocardiography affords rapid exclusion of major acute ischaemic cardiac events, as well as providing an indication of chronic hypertrophic changes and a quantitative indicator of heart rate elevation. Simple dipstick urine testing can assist in exclusion of significant proteinuria pending formal urinalysis studies16.
Laboratory
Full blood count analysis will give an indication of haemoglobin level where dissection is suspected, while serum markers of renal profile including creatinine level in particular may suggest varying degrees of acute kidney injury where present. Cardiac biomarkers may complement electrocardiography in exclusion of acute events.
As ever, a metabolic panel and blood gas analysis represent valuable tools in the acute physician’s arsenal where acute and evolving physiological disturbances are suspected.16
Imaging
Presence of pulmonary congestion in keeping with left ventricular failure as well as the mediastinal widening of an aortic dissection may be assessed via simple chest radiography. More complex imaging such as computerised tomographic (CT) scanning may be indicated as dictated by clinical presentation, as in the event of neurological manifestations16.
Treatment
Established guidelines1 suggest definitive management of a hypertensive emergency should involve lowering of blood pressure by 25% in the first hour and then to 160/100-110mmHg thereafter if stable, as indicated in Figure 3. Meticulous and continuous monitoring in an intensive care setting for parenteral administration of antihypertensive agents including labetalol17, clevidipine18–20 and fenoldopam21 is beyond the scope of most practising acute physicians.
Figure 3. Broad management of a hypertensive emergency (adapted from Chobanian A V, Bakris GL, Black HR, et al1 and Börgel J, Springer S, Ghafoor J, et al26
Hypertensive urgency, however, need not require such invasive interventions, with oral therapy utilising labetalol, captopril or clonidine followed by a period of vigilant observation usually proving sufficient1,17. A once popular practice of oral nifedipine is advised against, owing to the precipitous drop in pressure with inherent risk of tissue ischaemia observed on administration of this agent1. Emergent pharmaceutical options including novel felodipine formulations22 may also be considered.
A pitfall of physicians, perhaps, panicked by the jargon ‘hypertensive urgency’ has been observed, with inappropriate management in such cases reported in multiple independent studies in recent years23–25, with a 42.6% appropriate treatment rate in one study25. A chief consideration when faced with hypertensive crises therefore, may be to avoid rash intervention.
Worthy of mention is the potential for common co-prevalent secondary causes of hypertension including sleep apnoea, renal artery stenosis or a state of hyperaldosteronism; present in 15% of cases in one series26, recommendations have been made for consideration of these prior to therapeutic intervention26.
Outcome
There…
Indicators of greater likelihood of admission in patients presenting with severe hypertension may include presence of age >75 years, dyspnoea, altered mental status or creatinine elevation27.
…And Back Again
Following discharge after an admission for acute severe hypertension, a 90-day readmission rate of up to 35% has been reported28; this includes a multiple readmission rate of 41% with similar re-presentation accounting for 29% of this data. Curiously, dyspnoeic initial presentation is emphasised by the same data source as a risk factor for readmission, with additional risk factors including ictal phenomena at initial presentation and history of both drug abuse and prior severe hypertensive admission.
Key Points
Definition
A hypertensive crisisinvolves pressures of >180mmHg systolic and >120mmHg diastolic
Ahypertensive urgency does not include end organ damage
A hypertensive emergency implies end organ damage
Symptomatology
The commonest symptoms are headache (74.11%), chest discomfort & dyspnoea (62.35%), vertiginous dizziness (49.41%) and nausea & emesis (41.47%)
Investigations
Bedside should include urinalysis and echocardiography
Laboratory should include creatinine level
Imaging should include plain chest radiography
Management
Blood pressure should be lowered by 25% over the first hour
In hypertensive urgency, oral therapy is often sufficient
Dermatomyositis (DM) is a rare autoimmune process with not yet fully understood aetiology. It is characterised by a combination of striated muscle inflammation and cutaneous changes. The pathogenesis of the cutaneous manifestations of DM is not well understood either. DM occurs in all age groups. Therefore, two clinical subgroups of DM are described: adult and juvenile. The adult form is predominant among female patients with a clinical presentation which includes a Heliotrope rash (Fig. 1), Gottron’s papules (Fig. 2), nail fold telangiectasia and other various cutaneous manifestations in association with inflammatory myopathy.1 In addition to the previous mentioned symptoms, juvenile patients also commonly suffer from ulcerative skin and recurrent abdominal pain due to vasculitis. An increased occurrence of oncological processes in combination with adult DM has been observed with a slight predominance for the female gender.2 These patients carry a higher risk for comorbid cancers. The most common ones include malignant processes of the ovary, lung, pancreas, stomach, urinary bladder and haematopoietic system.3 The significance of these observations is that the development of DM should raise suspicion with regard to a possible parallel oncological process.
Figure 1
Figure 2
Materials and Methods
A retrospective consecutive case series was performed on a group of 12 patients that were hospitalised at the Department of Dermatology, Venereology and Allergology at the Medical University of Gdansk between 1996 and 2013. The diagnostic criteria for DM included: hallmark cutaneous lesions of DM, clinically significant muscle weakness evaluated by electromyography (EMG), indicative laboratory findings - muscle enzymes, muscle biopsy, autoantibodies. All 12 cases had muscle biopsy, serum studies and EMG performed. The retrospective study analysed the age and sex of the patients, course of the disease, accompanying diseases, clinical picture and treatment. The patients with malignancies were analysed by the primary organs of origin, and the period between the diagnosis of DM and that of malignancy (Table 1).
Table 1. Patient characteristics
No.
Sex
Previous medical history
Age of onset of DM
Clinical picture
Diagnostics
Treatment
Malignancy and age at diagnosis
1
F
Chronic eosinophilic leukaemia
54
Muscle weakness of shoulder and hip area, facial oedema and erythema, palmar erythema
CK 2550, ANA Hep-2 1:640, LDH 901, AST 69, ALT 143, X-ray = N, USG = N, EMG = N
Azathioprine, Prednisone
Stage IIA ovarian cancer at 55
2
F
Peptic ulcer disease
66
Facial erythema, Gottron’s papules on the hands, muscular weakness creating difficulty in movement, weight loss, decreased appetite
ANA Hep-2 1:1280, CT = N, EMG = N
Glucocortico- steroids
Small cell carcinoma at 66
3
F
None
23
Muscular weakness of shoulder and hip area; difficulty in standing up and walking up stairs, Gottron’s papules, Heliotrope rash, upper chest erythema
ANA Hep-2 1: 2580, CPK 12022; AST 595, ALT 210, CK-MB 534; Jo 1 = N, Mi = N
Azathioprine, Prednisone Methotrexate
None
4
F
Chronic obstructive pulmonary disease
42
Muscular weakness of shoulder and hip area, facial oedema and erythema
Cyclo- phosphamide, Methyl- prednisolone
Stomach tumour at 43
5
F
None
22
Muscle weakness, painful extremities, facial oedema and erythema
ANA Hep-2 = N, CT = N
Cyclo- phosphamide, Prednisone
None
6
F
None
42
Muscle weakness, paraesthesia of hands, facial oedema and erythema
ANA Hep-2 1:640
Cyclo- phosphamide, Prednisone
None
7
F
Hypertension, diabetes type II, osteopenia, leiomyoma.
65
Muscle weakness of shoulder and hip area, facial oedema and erythema
ANA Hep-2 1:1280, LDH 650
Cyclo- phosphamide, Prednisone
None
8
F
Hyper-thyroiditis
46
Muscle weakness; difficulty in moving, facial oedema and erythema
ANA Hep-2 1:160
Cyclosporine A, Prednisone
None
9
F
Autoimmune hepatic disease, leiomyoma.
45
Muscular weakness of shoulder and hip area, facial oedema and erythema
ANA Hep-2 1:2560, CK 3700, Mi-2 = P
Azathioprine, Methyl-prednisolone
None
10
F
Hypertension, diabetes type 2, hypo-thyroidism, ovarian cysts
57
Muscle weakness of shoulder and hip area, facial oedema and erythema, upper chest erythema, Gottron’s papules, Gottron’s papules, fatigue, dysphagia
ANA Hep-2 1: 640, CK 747, LDH 363, AST 78, Ro52 = P, Mi 2 = N, Jo 1 = N, PM/Scl = N, CT= two pulmonary lesions that were biopsied and diagnosed as pneumoconiosis
Prednisone, Methotrexate
Cervical Carcinoma at 51, Breast Cancer at 57, Pulmonary Metastasis at 58
No. = number (patient), DM = dermatomyositis, F = female, M = male, CK = creatine phosphokinase, ANA = antinuclear antibodies, LDH = lactate dehydrogenase, AST = aspartate transaminase, ALT = alanine transaminase, N = negative, P = positive, USG = ultrasonography, EMG = electromyography, CT = computerised tomography
Limitations
The small sample size is a significant limitation in this retrospective analysis. DM is a rare disease with a prevalence of 1:1000. Increasing sample size, by combining cases from multiple institutions, and implementing control would further strengthen the presented material.
Results
The average age of onset of the disease was 48 years. All 12 subjects were female. Previous medical history included chronic eosinophilic leukaemia, diabetes mellitus type II, hypertension, leiomyomas, hypo- and hyper- thyroid disease, chronic obstructive pulmonary disease, peptic ulcer disease, autoimmune hepatitis and osteopenia. The two most common are diabetes mellitus type II and hypertension. The clinical picture of each case was similar in that all of the patients presented with some form of muscle weakness. In addition, typical features of DM with Gottron’s papules, periorbital oedema, facial oedema and erythema were noted in five patients. Antinuclear Antibodies (ANA) Hep-2 of values >1:160 were identified in nine patients. Additional laboratory markers such as creatine kinase (CK), lactate dehydrogenase (LDH), aspartate transaminase (AST) and alanine transaminase (ALT) were elevated in five patients. Two patients had muscle biopsies performed. The immunohistopathology picture consisted of Immunglobulin G (IgG), fibrinogen, C1q, and C3 deposition around the perimysium and granular deposits of Immunoglobulin M (IgM) in the dermal epidermal junction. Of the 12 patients, four had neoplasms in addition to the diagnosed DM. The primary cancers were originating from the cervix, breast, stomach and ovary. Of these four patients, all had the diagnosis of DM prior to the diagnosis of a malignancy.
Discussion
The diagnosis of DM is made by combining the clinical picture with the results of various laboratory findings: skin and muscle biopsies, EMG, serum enzymes and ANAs.
The clinical picture varies. The typical dermatological presentation consists of a erythematous and oedematous periorbital rash - the Heliotrope rash (Fig. 1). Symmetrical redness and flaking can be observed on the elbows and dorsal sides of the phalanges, especially over the distal metacarpal joints - Gottron’s papules (Fig. 2). Erythematous lesions can also be found on other locations such as the face, upper chest and knees.4 The dermatitis heals with atrophy, leaving behind areas that resemble radiation-damaged skin. The striated muscle inflammation most often involves the shoulder and hip area, leading to muscle weakness and atrophy. The intercostal muscles and the diaphragm may be involved causing alarm with regards to respiratory compromise. Dysphagia can be present due to inflammation of the smooth and skeletal muscles of the oesophagus. These inflammatory processes often lead to muscle calcification.5 The sum of all these changes clinically is seen most often as weakness, weight loss and subfebrile temperatures. All patients in our study had co-existing muscle and cutaneous symptoms, with variation in severity and localisation. Five patients had the classical picture of shoulder and hip area weakness. The rest of the patients had a more general muscle weakness. Two patients had atypical complaints of hand paraesthesia and extremity pain respectively.
Subtypes of DM exist for the purpose of epidemiological research and sometimes prognosis. They are categorised by the clinical presentation and presence or absence of specific laboratory findings. These subtypes are as follows: Classic DM, Amyopathic DM, Hypo-amyopathic DM and Clinically Amyopathic DM. These subtypes have little impact on routine diagnosis. Common laboratory findings in DM are enzymatic elevation of CK, AST, ALT and LDH; these mainly reflect the muscle involvement. Amyopathic DM lacks both abnormal muscle enzymes and weakness.6 Enzymatic elevation may sometimes precede the clinical symptoms of muscle involvement. Hence, an enzymatic raise in a patient with a history of DM, should raise suspicion of recurrence. Positive ANA findings are frequent in DM but not necessary for diagnosis. More myositis-specific antibodies include anti-Mi 2 and anti-Jo 1. A typical histopathological examination shows: myofiber necrosis, perifascicular atrophy, patchy endomysial infiltrate of lymphocytes and occasionally the capillaries may contain membrane attack complexes.7
Cutaneous changes and muscular complaints can correspond to: 1. Systemic scleroderma which often has a positive ANA; 2. Trichinosis, in which periorbital swelling and myositis occurs, but there is a prominent eosinophilia and a history of consuming undercooked swine or bear meat; 3. Psoriasis with joint involvement which may give a clinically similar picture to DM. However, the skin changes in psoriasis have a more flaking pattern. In doubtful cases, a skin and muscle biopsy together with an electromyography will set the diagnoses apart. A facial rash may also be observed in systemic lupus erythematosus together with nail fold telangiectasia. They are usually distinguished by a clinical picture with more organ system involvement in systemic lupus and by serological studies. A drug-induced picture of DM exists and is particularly associated with statins and hydroxyurea.8
It is estimated that around 25% of DM cases are associated with a neoplastic process that can occur prior, during or after the episode of DM. The risk of developing a malignancy is highest in the first year of DM and remains elevated for years after diagnosis. 9, 10, 11 This was the case with patient number 1, 2 and 4 in our study, where the malignant process appeared in the first year following onset of DM. Risk factors seen in DM patients include male gender, advanced age and symptoms of dysphagia.12 The age range of the four patients in our study with malignancy was between 43 and 66. Symptoms that clinically raised suspicion of a malignant process included weight loss, lack of appetite and dysphagia. All neoplasms were discovered within one year after the diagnosis of DM was made. One patient had a previous history of cervical cancer, six years prior to the onset of DM.
The most common neoplasms seen in patients with DM vary in the world. In Europe the malignancies are located mainly in the ovaries, lungs, and stomach. The cancer types associated with the DM correlate with common cancers seen in the same area. For instance, in Asia, nasopharyngeal carcinoma (which is a rare malignancy in Europe) is a frequent occurrence in DM.1, 3 The location of neoplasms seen in our study varied from gastric, breast, ovary and pulmonary. The screening in regards to malignancies in patients with DM is individualised and should be based on risk factors such as previous malignancies, alarming symptoms such as weight loss or dysphagia, or abnormal findings on physical exam. This was the case with patient number 10 in our study who had a previous history of cancer, and patient number 2 who had symptoms of weight loss and decreased appetite. Initial screening was negative for patient number 1 and 2, where the malignancy developed first after the onset of DM. Age-appropriate screening with mammography, faecal-occult blood test and Papanicolaou smear should be considered. Additional investigations with chest films, computerised tomography (CT) scanning of chest, abdomen or pelvis; colonoscopy, cancer antigens; and gynaecological ultrasonography should be done when indicated.
The main objective of treatment in DM is to improve muscle strength and obtain remission, or at least clinical stabilisation. No specific protocol exists with regard to treatment of DM. Treatment is individualised and adapted to the specific condition of the patient. High-dose corticosteroids are the basis of treatment. However, randomised placebo clinical trials failed to show their efficacy. Clinical efficacy of corticosteroid therapy demonstrates itself and hence is the initial treatment of choice. Doses start at around 1 mg/kg/day depending on the corticosteroid of preference. This dosing is maintained for approximately two months until clinical regression is achieved, followed by approximately 10 mg decrease in dose for the coming three months. A maintenance dose of approximately 5-10 mg should be achieved. The exact parameters are patient-specific. In the case of a severe flare of dermatomyositis, 1 g per day for three days of methylprednisolone intravenous pulses can be administered. The systemic effects of long term therapy with corticosteroids have to be kept in mind. Hence, yearly dual-energy X-ray absorptiometry bone scans can be administered to monitor the development of osteopenia.
Further treatment options are offered in situations where the initial disease presentation is severe, involves internal organs, if relapse occurs during steroid dose reduction, and steroid side-effects. It has been proposed that combination therapy is a better method of approach due to lower reported relapse rates and lower need to use high-dose corticosteroids. Methotrexate is second-line therapy when steroids fail alone. Methotrexate is used with a maximum dose of 25 mg per week plus folate supplementation. The limitations of Methotrexate are immunosuppression and pulmonary fibrosis. Methotrexate is considered preferable to Azathioprine because the latter has a longer onset of efficacy. Azathioprine is administered at doses ranging from 1.5 - 3 mg/kg/day and has a side-effect profile is similar to that of other immunosuppressants. Cyclosporin A is a T-cell cytokine moderator that has a similar efficacy profile to Methotrexate. Side-effects include renal impairment, gingival hyperplasia, and hypertrichosis. Dosing of Cyclosporin A ranges from 2 - 3 mg/kg/day.
An expensive but effective and rather low side-effect alternative is intravenous immunoglobulins. The dosage of this medication has not been officially established in the treatment of DM, but options are: 2 g/kg given either in 1 g/kg/day for two days every four weeks; or 0.4 mg/kg/day for five days initially, and then for three days monthly for three to six months. Other alternatives include Mycophenolate Mofetil, Cyclophosphamide, Chlorambucil, Fludarabine, Eculizumab, Rituximab.9 Further options might be treatment targeted toward malignancy when associated with DM. This was observed in our patient number 10, where full remission of DM was obtained first after lobectomy and chemotherapy for the mammary carcinoma.
Conclusion
DM mainly affects women and all 12 cases presented in our study were female. One third of our cases had malignancies associated with their course of DM. We conclude that it is reasonable to screen these patients, especially in those with already established cancer risk factor. Age-appropriate screening and beyond is indicated by high risk factors or clinical presentation. High suspicion should be raised in patients with a previous history of oncological treatment since DM can be the first clinical sign of cancer recurrence.
An audit and re-audit on the monitoring of the physical health of patients on antipsychotic medication in the Early Intervention in Psychosis Service of the 5 Boroughs Partnership NHS Foundation Trust
Introduction
A growing number of studies suggest a causal relationship between antipsychotic treatment and metabolic disturbances. The most frequent problems linked to antipsychotic drugs have been abnormalities of glucose metabolism such as insulin resistance, hyperglycaemia or new onset diabetes mellitus and dyslipidemia, including increased levels of total cholesterol, LDL-cholesterol and triglycerides.1
Developing effective models of identifying and managing physical ill health among mental health service users has increasingly become a concern for psychiatric service providers. Individuals with Serious Mental Illness (SMI) defined as any Diagnostic and Statistical Manual (DSM) mental disorder leading to substantial functional impairment, have higher than expected risks of physical morbidity and mortality in comparison with members of the general population.2 People with mental health problems such as Schizophrenia or Bipolar Disorder have been shown to die on average 16 to 25 years sooner than the general population.3 One set of explanations for these vulnerabilities points to the lifestyles of people with serious mental illnesses, which are often associated with poor dietary habits, obesity, high rates of smoking, and the use of alcohol and street drugs.4 Illness related factors have also been cited. It has been suggested that individuals with serious mental illness are less likely to spontaneously report physical symptoms.5 Poor physical activity has also been shown to be a common occurrence in people with serious mental illness.6, 7
A greater inherent predisposition to develop metabolic abnormalities coupled with metabolic adverse effects of antipsychotic drug treatments may negatively influence physical health.8 Many of these problems can be avoided if close attention is paid to the physical health of patients on antipsychotic treatment. A longstanding debate persists concerning who is responsible for the physical care of patients with serious mental illness. Psychiatrists and physicians are advised to play an active role in ensuring that patients with mental illness are not disadvantaged.9
The Warrington and Halton Early Intervention in Psychosis Team is based in the 5 Boroughs Partnership (5BP) NHS Foundation Trust in the North West region of the United Kingdom, and in collaboration with Advancing Quality Alliance (AQuA), they embarked on a joint audit between November 2012 and May 2013 with the aim of reviewing the practice regarding the routine monitoring of physical health of service users on antipsychotic treatment. The study set out to reduce the cardio-metabolic effect of antipsychotic medication in service users. The study was also aimed at contributing to a reduction in the mortality rates in people with severe mental illness as well as testing out approaches to improve the physical health of people with serious mental illness who are receiving care from the Early Intervention in Psychosis Teams. The promotion of a more integrated approach to the physical health care of people with a SMI was also targeted.
Method
In November 2012, the Warrington and Halton Early Intervention in Psychosis service (EIP) conducted the initial audit, designed by AQuA as a baseline measure of the current standard of physical health screening amongst the Early Intervention patients in the two boroughs. The recommendations from the National Institute for Health and Care Excellence (NICE) and Maudsley prescribing guidelines were the frameworks for the AQuA design. The Research and Audit Governance Group in the 5 Boroughs Partnership NHS Foundation Trust approved the audit.
A retrospective review of the clinical records of all patients opens to the EIP, who were prescribed antipsychotics, was undertaken. Six physical health parameters were examined and these include; serum lipid profile and blood glucose levels. Others measures were body weight, height, Body Mass Index (BMI) and blood pressure. These parameters were entered into the survey monkey audit tool developed by AQuA.
Other items audited were the frequency of screening, the number of physical health parameters evaluated at each period of recording and the smoking status of the service users. Clinical records were checked for documented history of physical illness in all patients. The number of service users receiving physical health interventions as a result of the screening and the number of service users who were offered physical health interventions at the screening but either refused treatment or did not respond to the referral was also recorded. The results were presented at a Trust-wide forum and recommendations were made, and disseminated shortly afterwards. A re-audit was done in May 2013.
Results
Table 1, summarises the demographic details of patients at baseline and re-audit. 55 patients were involved in the baseline audit and 52 patients were involved in the re-audit. No significant differences were observed in both audits in terms of gender distribution and age. Majority of the patients involved in both audits were of white British ethnicity.
Table 1: Demographic details of patients at baseline audit and re-audit
Nov 2012
May 2013
Total number of patients
Male : female
35:20
22:30
Age
14-36
15-36
White British Ethnicity
52
48
Baseline audit: November 2012
Screening and monitoring
The table below indicates the number of service users receiving a screening for weight, height, BMI, glucose blood levels, lipid blood levels and blood pressure at the 4 week, 3 month, 12 month and 24 month assessments.
Table 2: Physical health screening of service users at baseline
4 weeks recorded screening
3 months recorded screening
12 months recorded screening
24 months recorded screening
1 type of screening
5 (9.1%)
12 (21.8%)
18 (32.7%)
18 (32.7%)
2 types of screening
14 (25.5%)
17 (30.9%)
5 (9.1%)
5 (9.1%)
3 types of screening
4 (7.3%)
4 (7.3%)
3 (5.5%)
6 (10.9%)
4 types of screening
5 (9.1%)
3 (5.5%)
5 (9.1%)
3 (5.5%)
5 types of screening
4 (7.3%)
0
1 (1.8%)
4 (7.3%)
6 types of screening
4 (7.3%)
3 (5.5%)
4 (7.3%)
2 (3.6)
There was no screening recorded for 19 (34.5%) patients at 4 weeks, 16 (29%) patients at 3 months, 19 (34.5%) patients at 12 months and 17 (30.9%) patients at 24 months.
Smoking status of service users
Based on the analysis of those referred to the smoking cessation service, it was concluded that around 35% of service users within the EIP Service smoke. The findings from this data also indicate high refusal rates to smoking cessation programmes (at over 80% of those service users who confirmed that they smoke).
Documented history of physical illness
The presence or absence of physical illness was documented in the records of 35 patients. Where physical health problems were identified, patients were offered a number of interventions. These include referral to the dietician/exercise programmes, smoking cessation and referral to primary care services for illnesses such as, hypertension, diabetes and hyperlipidemia.
Table 3, summarises the types of interventions available for patients when physical health issues were identified. A number of patients (N/A) required no interventions, as physical problems were not identified.
Number of service users receiving physical health interventions
Table 3: Physical health interventions
Yes
No
N/A
Referral to dietician/exercise programme
15 (28.8%)
26 (50%)
14 (25.5%)
Treatment for Diabetes
0
22 (45.8%)
33 (60%)
Treatment for
Hyperlipidemia
2 (4.2%)
23 (47.9%)
30 (54.5%)
Treatment for
Hypertension
0
22 (45.8%)
33 (60%)
Help with smoking
cessation
12 (24.5%)
19 (38.8%)
24 (43.6%)
Re-audit: May 2013
Screening and monitoring
The table below indicates the number of service users receiving a screening for weight, height, BMI, glucose blood levels, lipid blood levels and blood pressure at the 4 week, 3 month, 12 month and 24 month assessments. The table shows that 29 patients had their screening recorded at 4 weeks, 19 (66%) of which had 6 types of screening. At 24 months, out of the 16 patients who had their screening recorded, 15 (95%) had 6 types of screening. Patients with no screening parameters were omitted.
Table 4: Physical health screening of service users at re-audit
4 weeks recorded
screening
3 months recorded screening
12 months recorded screening
24 months recorded screening
1 type of screening
2 (7%)
0
0
0
2 types of screening
2 (7%)
2 (8%)
1 (4%)
1 (5%)
3 types of screening
1 (3%)
1 (4%)
3 (11%)
0
4 types of screening
3 (10%)
3 (12%)
1 (4%)
0
5 types of screening
2 (7%)
1 (4%)
1 (4%)
0
6 types of screening
19 (66%)
18 (72%)
21 (77%)
15 (95%)
Smoking status of service users
The overall data confirms that 25 patients, who were identified as smokers, were offered smoking cessation, 19 of which refused, thus giving an overall refusal rate of 76%
The table below compares the results of both audits with respect to “6 types of screening” done at 4 weeks, 3 months, 12 months and 24 months. The result shows an overall improvement over the audit period.
Comparing results of both audits with respect to “6 types of screening”
Table 5: Comparison of screening results
November 2012
May 2013
4 weeks
4 (7.4%)
19 (66%)
3 months
3 (5.5%)
18 (72%)
12 months
4 (7.4%)
21 (77%)
24 months
2 (3.7%)
15 (95%)
Discussion
The first audit revealed a suboptimal screening of the 6 targeted parameters at 4 weeks, 3 months, 12 months and 24 months in the service users audited when compared to the recommendations of the Maudsley guidelines (See Table 3). Some of the issues identified are summarised in the table below;
Table 6: Issues identified following the first audit
Sporadic health and wellbeing sessions
Ad-hoc physical health checks prior to commencing antipsychotics
Physical health screening was not perceived as priority
Physical screening were unsystematic and erratic
Poor referral links with local health promotion programmes
Poor attendance to physical health screening appointments
Poor recording of screening tests
Inadequate links with primary care services
Psychiatric clinics poorly equipped with instruments for basic health screening
No clarity about who takes responsibility for screening: Psychiatrists or GP?
Patients’ lack of interest and motivation in the screening process
SMI register not up-to-date
Recommendations made following the initial audit are outlined in the table below;
Table 7: Recommendations following the first audit
Need to finda comprehensive screening tool
Development of a documentation system
Building an alert system to remind when physical health checks are due
Improvement of links with primary care services
A more robust approach to ensure patient’s attendance at screening clinics
Improvement of links within secondary care agencies
Identification of further skills needed within the team e.g. venipuncture, ECG
A Plan, Do, Study, Act (PDSA) model was used which was useful in clarifying issues and actions needed.10 It helped us to identify issues and actions needed including:
1. Establishing physical health as a priority within the EIP
2. Involvement of primary care and health promotion
3. Establishing a database for physical health monitoring
4. Making physical health monitoring part of care planning
To tackle the identified issues a local project group was constituted. This group was made up of a consultant psychiatrist, business manager, nurse consultant, team manager, an occupational therapist (OT), a support worker (STR), a pharmacist, social services, public health leads, wellbeing nurses, a service user representative, and a locally based General Practitioner. The group had monthly meetings.
Patients in the Warrington and Halton Early Intervention in Psychosis Service were screened using the 5 Boroughs Partnership (5BP) Comprehensive Physical Health Assessment tool. This tool covered the 6 parameters targeted in the audit and other relevant health information such as, smoking, diet, exercise, sexual health, sleep, dental and optical health, ECGs, and other routine bloods checks. An in-house database in which results could be recorded was devised and implemented. A notification list which alerted on computer when a screening is due was developed; a GP DVD and information leaflet for the GP website and the Clinical Commissioning Group (CCG) Newsletter were produced. Wellbeing Nurse-led clinics were held in Halton and a STR-led physical health clinic was initiated in Warrington. Access into the path labs for both localities was established to help facilitate prompt access to blood results. Regular AQuA meetings took place in Salford, Manchester, and links were established with the Medical Director and the Clinical Commissioning Group, who were regularly, provided progress reports.
The re-audit in May 2013 showed an increase in the number of service users being screened and monitoring for the six identified parameters (see Table 8).A robust and comprehensive recording system has been developed, resulting in more service users receiving appropriate screening and physical health monitoring. Better links and working relationships have been established with primary care services and there is increased awareness of the need for physical health monitoring in professionals and service users. Regular and well-equipped physical health clinics with well-trained staff have been established across both localities. Other secondary care agencies within the Trust are now more aware of the requirements for physical health screenings.
Why should we be doing regular physical health monitoring? The benefits of monitoring the physical health of individuals with serious mental illness cannot be overemphasised; it allows early identification and subsequent management of cardiovascular and other risk factors in a timely manner.11 The Maudsley Guidelines recommend monitoring of blood lipids at baseline, at 3 months and yearly. Similar recommendations are made for the weight, which includes BMI and waist size when possible. Plasma glucose measurements are recommended at baseline, at 4 to 6 months and yearly. Blood pressure measurements are recommended at baseline and frequently during dose titration. Full blood count and electrolyte measurements are recommended at baseline and yearly.12 In the last few years, agencies worldwide have also developed clinical guidelines. In the United States, the American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologist and the North American Association for the Study of Obesity have released joint guidelines.13
Even though the side effects of antipsychotics are well established, many mental health services today have yet to adopt a practice of regular blood monitoring as recommended by international guidelines.14 The issue of responsibility for monitoring metabolic abnormalities remains a much debated topic today.9 The primary responsibility for managing the physical health of individuals with severe mental illness has been said to lie with primary care.7 Another side of the debate, however, exists, and two consensus conferences have called on mental health care providers to take responsibility for the physical health of their patients.8 It is widely recognized that mental health teams have a role to play in the monitoring of the physical health of their service users; however, many psychiatrists still consider psychiatric symptom control as their primary responsibility.14 15 Studies have also shown that Individuals with Serious Mental Illness do not readily access primary care.16 Despite the availability of Clinical Guidelines, screening for and monitoring of metabolic problems in patients with serious mental illness remains suboptimal.11
The usual practice in most centers for monitoring physical health parameters and guidelines used vary and are rarely regulated. Local resource availability is likely to play a significant role in guideline selection. Physical equipment, staffing levels and other resource issues may need to be taken into consideration prior to devising a local guideline. Development of a specialised phlebotomy service, for example, to the outpatient clinics will be a welcome addition, introduction of a key worker system as seen in the Warrington and Halton Early Intervention in Psychosis Team and consideration of the physical health needs of patients as part of the key worker’s duties, a simple one-page monitoring prompt attached to the patient’s medical file, educational intervention and oversight by the senior clinicians may all increase the adherence to routine blood testing guidelines. Regular liaison with General Practitioners regarding a joint approach to physical health monitoring would also help improve adherence to the guidelines.
What is medical pain? One answer would be a poorly defined concept which suffers the ignominy of poor management.
A quick internet search for the term brings up several hits to clinics offering the services of medical practitioners with pain specialty training. Definitions of ‘medical pain’ however, as opposed to those of its more easily construed post-surgical cousin, are both sparse and elusive in the learned literature. One potential candidate is provided by the International Association for the Study of Pain (IASP), whose professional presence on the web offers both a respectable description of pain syndromes of medical aetiologies as well as a taxonomical guide thereto1.
With a struggle to even define the concept, is it any wonder that medical patients with pain complaints continue to score reprehensible figures on studies into pain incidence and effective relief? This is far from a new phenomenon, with the British Journal of Anaesthesia (BJA) reporting a staggering 52% of medical inpatients in one study (N=1594) of a UK district general hospital to be in pain on the medical ward, with 20% and 12% of those in pain rating this complaint as severe and unbearable respectively2. What is particularly distressing about these statistics is the fact that data collection in the same study occurred over five days; more than ample time for complaints to be reported or recognised and appropriate relief strategies implemented. Barriers clearly exist to the provision of adequate medical pain relief, with practice shown to fall below standards recommended by the Royal College of Anaesthetists.3 A sketchy definition is perhaps one such barrier, but what other challenges exist to management of medical pain?
Predictability & On-Call Skills
In contrast to the anticipated pain following an elective surgical procedure, medical pain is less predictable in onset and consequently more the realm of an on-call physician than a specialist pain management team. One unambiguous fact when equating specialist pain rounds and the on-call services of a more junior recruit is that the former clearly benefit from greater levels of experience, even allowing for acquisition of specialist training. The latter inevitably rely more heavily on the knowledge base afforded them by theoretical education, which sadly tends to be rather scant in undergraduate medical programmes.
The lack of early teaching of junior staff on the subject represents one barrier to pain management in general, with formal teaching on the subject of medical pain management a particular shortcoming in several international medical curricula. This fact is supported by the findings of a cross-sectional study in one Sydney hospital utilising a multinational population of medical interns and residents4, indicating some 56.2% of responders felt education on pain management to be inadequate. Up to 68.8% of responders were willing to receive additional lectures on opiate use to increase their knowledge base in this regard, suggesting a definite dearth of dedicated teaching.
In recognition of similar sentiments, a dedicated junior doctor-targeted postgraduate pain curriculum was suggested in 2011 by the Faculty of Pain Medicine (FPM) of the Australia & New Zealand College of Anaesthetists (ANZCA)5. This not only recognises the need for effective pain management skills at an early career stage, but also proposes a core set of competencies and assessments thereof for application to early postgraduate physicians’ skill sets.
A Surgical Predilection?
Skills of junior on-call medics aside, the provision of committed specialist pain services undoubtedly represents one of the major advancements in acute pain patient care. And yet, the needs of medical patients have often been overlooked in favour of acute surgical pain relief, and presumably continue to be so in the face of a lack of convincing evidence to the contrary. One study published in 2008 reporting data from over 220 United Kingdom National Health Service (NHS) hospitals revealed a paltry 16% incidence of routine acute pain service in medical wards6. The same study revealed that 82.2% of clinical leads in acute pain services actually recognise this problem of inadequate pain control on medical wards. With this stark admission from front line algologists in mind, why do elderly and general medical patients consistently appear to produce disconcertingly poor results in pain studies?
Perhaps the lack of adequate medical pain services in the light of a frank admission to a predilection for surgical patients reflects inadequate training, staffing or application of resources as a barrier to effective management of medical pain.
Community Confounders
Limitations of secondary care pain services aside, the primary care setting also exhibits a confounding factor for professional provision of medical pain management – the propensity for patients to easily self-medicate their complaints with non-prescription remedies. The immemorial complaint of headache in the community provides a convenient example of the potential for patients to self-manage their pain symptom. In doing so however, they simultaneously skirt the legion of adverse drug reactions, drug interactions and other implications including paradoxical rebound pain which may complicate management later on in the professional setting. Data published following a recent review of literature sources7 indicate codeine-based compound analgesics to be the most popular over-the-counter medications dispensed across several international populations. This telling fact may be suggestive of a trend in non-professional pain management which impedes effective management according to professional standards. Assuming a relative deficit of surgical to medical pain patients in the community, this may represent a unique challenge to providers of medical pain services.
Chronicity
One further important consideration to be made in medical pain is its potential for chronicity, with prevalence of leading pain disorders including lower back pain and chronic migraine indicated at 10.2%8 and 1-3%9 respectively in recent studies. The former in particular has exhibited an explosive trend in prevalence over recent years, with a more than 2.5-fold increase since 1992 in relative prevalence observed in one 2006 American study of households state-wide (N=5357)8.
Implicit in the chronicity of pain complaints exist a number of secondary disorders which can prove troublesome for effective engagement of pain management services. The European Journal of Pain quotes a large transnational study of chronic pain patients (N=46,394)10 as finding 21% of patients to have been diagnosed with depression because of their pain. Interestingly while almost half of subjects were self-administering over-the-counter analgesics and only 2% were being seen by a pain specialist, an astonishing 40% reported inadequate pain relief –an almost anticipated outcome of the ‘do it yourself’ approach to pain management in chronic, refractory cases? This may be less relevant in surgical pain experiences which intuitively represent a more acute event in a more controlled environment, and therefore may be more amenable to effective management than a drawn out pain experience over several years!
Fear of Pain
Chronicity of pain in turn evokes a largely self-explanatory phenomenon known as fear of pain, which can present a potentially sizeable obstacle to management of patients. High levels of fear of pain and also movement as a provocative agent thereof have been described in 38.6% of fibromyalgia syndrome patients (N=233)11, with this heightened fear of a painful experience linked to increased disability, depressed mood and most importantly pain severity. This latter component alludes to one of the more insurmountable barriers to management of chronic medical pain – the impasse resulting from a vicious circle of pain, fear and infinite vice versas.
The fear of pain may in turn be compounded by a fear of narcotic analgesic therapy on both the part of the patient and the prescribing physician, with this being an issue in non-cancer pain as well as malignant disease. The fear of commencing and continuing long term opiates is traditionally said to be particularly prevalent in the primary care setting12. Fear can arise in view of a number of reasons, including the potential for addiction and major side effects as well as the notion that opiate drugs represent a terminal stage in a disease process. Mention of opiates has been linked to accusations of ‘hidden diagnoses’ on the part of the physician, where patients suspect malignant pathology has been concealed from them by their care provider out of a deep-rooted belief that opiate analgesia is merited solely by cancerous conditions13. Whether this signifies an already fragile patient-doctor relationship or a contribution to the deterioration thereof, the connotation for effective management of medical pain remains a significant one. Repeated careful review of patients on long term opiate therapy for chronic non-cancer pain must be emphasised however, with up to 19% of chronic pain patients found to have some form of addictive disorder in a 2001 paper on the subject14 courtesy of the BJA.
Conclusion
In summary, patients requiring relief of medical pain issues are clearly disadvantaged by the presence of numerous hurdles to effective management of their complaints. The literature base in this regard is conspicuous by its absence, with practices in medical pain management being poorly evidence-based as a result. This represents a major potential target for investigative studies and research into potential trends and best practices. Exploration of effective methods for implementation of improved education for newer staff and also resource allocation for more experienced practitioners would also be of benefit to the standard of care in medical pain.
Blue discolouration of the skin can have a multitude of causes, including Mongolian spots, blue naevi, the naevi of Ito and Ota and metallic discolouration1 or the use of drugs such as minocycline. Here we report the case of a 61 year old gentleman who developed blue macular skin lesions that were not attributable to any obvious cause and may be the result of an unidentified occupational exposure.
A 61 year old Caucasian gentleman developed blue macular skin lesions over a 14 year period. The very first lesion appeared in the middle phalanx of the right middle finger (figure 1). It was light blue and pinpoint, eventually darkening and increasing in size to approximately 1mm x 1mm, at which point becoming permanent and non-evolving. The lesion had no notable associated features and the patient was in otherwise good health.
Figure 1: The first blue macular lesion on the middle phalanx of the right middle finger.
Figure 2: A blue macular lesion on the terminal phalanx of the left middle finger.
Figure 3: A lesion on the anterior abdomen from which a punch biopsy was taken.
Figure 4: Haematoxylin and Eosin stained slide at 10x magnification. Abdominal skin biopsy showing dermal interstitial and perivascular distribution of black coloured pigment deposits
At present, he has approximately thirteen blue macular lesions in total, all of which have developed in the same manner. They are distributed predominantly on his hands with one on his left forearm and one on the right abdominal flank. New spots still continue to arise on his hands (figure 2).
A punch biopsy of the abdominal lesion (figure 3) was carried out. The histological findings were those of skin with normal intact epidermis and the presence of black coloured pigment granular deposits, located largely within the papillary dermis and occasional smaller deposits in the superficial reticular dermis (figure 4). The deep reticular dermis and subcutaneous fat were normal. The pigment had a perivascular distribution and in dendritic histiocytic cells, with close association to fibroblasts. Histiocytic cells form part of the mononuclear phagocyte system and these cells are abducted mainly for phagocytosis removal or storing material2. Apart from the pigment, the remaining skin was normal. The use of light microscopy alone does not identify all substances on examination of a Haematoxylin and Eosin (H&E) stained section of tissue. Applying polarisation light microscopy enables the identification of numerous structures, for example crystals, pigments, bone and amyloid3. However, the black coloured material here was non polarisable (no refractile foreign material could be identified). These appearances as seen on light microscopy alone are most frequently seen where there is a history of tattoo artistry, but tattoo pigment is typically identified as showing reflective properties using polarisation4. Interestingly, the patient had no clinical history of deliberate tattooing and other causes were considered.
Discussion
The discovery of black coloured deposits in the dermis excludes the diagnoses of Mongolian spots or blue naevi and the naevi of Ito and Ota, all of which are disorders of dermal melanocytes. Another important differential is malignant melanoma, but it is not the diagnosis as the histopathological findings did not find any evidence of dysplasia or malignancy.
In a disorder known as anthracosis, similar findings of black coloured deposits can be seen in other organs such as within the lung and draining lymph nodes. It is often found in smokers and urban populations and reflects the deposition of carbon which is the most commonly identified exogenous mineral substance within tissue sections. The skin is not a site where such carbon pigment is typically seen and therefore, this is not a credible diagnosis in this case.
Agyria is a condition that occurs as a result of silver particle impregnation of skin leading to blue-grey skin discolouration. Silver exposure may be due to occupational or surgical exposure (by use of silver sutures) or medication with silver salts. On interview, the patient denied any occupational exposure to silver and the use of silver salts. Although the patient had had previous shoulder surgery, silver sutures are no longer used in modern day surgical practice and therefore this cannot be the cause of his skin discolouration.
Unfortunately, histological examination of paraffin embedded tissue sections can only confirm the presence and distribution of an exogenous substance and it is not possible to precisely differentiate the exact type of material which is present. The use of an electron probe micro analyser may have been useful in identifying the substance, however, such equipment is not currently available and was not used in this case.
Interestingly, in tattoo artistry, carbon black may be used to give blue tattoos their colour5 and this is also a component of tyres and industrial rubber products6. This provided us with a link to occupational exposure, given that this gentleman is a tyre worker and has been involved in both the manufacture and assembly of tyres for 34 years. Carbon can cause discoloration of the skin, depending on the extent of deposition.
It is notable that in his 34 years of working with tyres, this gentleman did not routinely use gloves or protective uniform until only 10 years ago. This was as workplace safety precautions were not as strongly enforced in previous times. He admitted to have been in direct contact with the materials involved in tyre building and also suffered accidental superficial cuts on his hands whilst working, which may be a route by which carbon may have been introduced into the dermis. This is supported by the observation that the majority of the blue macular lesions were on the hands. Adding credibility to this theory is the identification of a colleague of this gentleman’s (who did not wish to be identified), whose job also involved the manufacture and assembly of tyres, who also has a similar single blue macular lesion on his hand.
In addition to this we have identified a forum on the internet7 that reports other similar cases of blue pin-point macular lesions appearing on the skin of tyre factory workers – some of whom worked for the same tyre company that this gentleman did. This may suggest that there is an association between exposure to a chemical, possibly carbon black, involved in the manufacture of tyres, and the appearance of these blue macular lesions.
In this case report, the identity of the material deposited and the route by which it accumulated in the dermis is unclear, but may have been related to an occupational exposure – this was in keeping with the general consensus upon presentation of this case at the West Midlands Dermatology Conference at New Cross Hospital Wolverhampton. We welcome any new case reports or literature that may be able to shed further light on this subject.
Dilated cardiomyopathy (DCM) is a cardiac muscle disease, characterized by dilatation and impaired contraction of the left ventricle or both ventricles, and leads to progressive heart failure and sudden or heart failure-related death [1]. The life expectancy is limited and varies according to the underlying etiology with a median survival time of about 5 years after diagnosis [2]. Although the pathogenesis of this disease has been extensively studied for decades, it remains ambiguous. Currently, myocarditis, immunological abnormalities, toxic myocardial damage, and persistent cardio-tropic viral infection are all assumed to be causes of DCM [3]. Dilated cardiomyopathy occurring in families, or the familial dilated cardiomyopathy (FDC) may occur in 25% to 35% of DCM cases, implicating a genetic contribution to the etiology [4-7]. More than 30 susceptibility genes have been shown to be associated with an increased risk of developing a DCM. Here we report three strange cases of FDC accompanied by hearing loss and rapid progressive course in brothers from Sichuan Province of China. The presentation of the family was really rare and it is anticipated that more susceptibility genes may be discovered.
Case report
The patient was a boy from Sichuan Province, and had lost his hearing when he was five years old. At the age of eight, the boy presented with cough and acute onset breathlessness. On examination, he had blood pressure (BP) of 90/60mmHg, heart rate (HR) 105/min, raised jugular venous pressure (JVP), crackles over the lung bases and a pansystolic murmur at the apex. A huge cardiomegaly was seen on chest X-ray (CXR), and the cardiothoracic ratio (CT ratio) was 0.721. ECG revealed primary atrioventricular block and left ventricular hypertrophy (LVH). Echocardiography (Echo) showed enlargement of both ventricles of the heart, a decreased left ventricular ejection fraction (LVEF), and severe mitral regurgitation (MR). The patient was treated in line with congestive cardiac failure (CCF). However, he died three months after the acute onset of breathlessness.
Surprisingly, the progression was nearly the same as two of his older brothers. Both of them also lost hearings at the age of five. Then presented with acute onset breathlessness and they were diagnosed with DCM aged seven to eight years. They also died three months later after the acute onset of breathlessness. Because of the terrible experience of his older brothers, the boys’ parents took him to hospital every year to be examined. ECG and Echo images were normal 6 months before the onset of breathlessness. Moreover, the boy had no symptoms 1 month before his presentation.
Discussion
The definition of FDC is clinically based on manifestation with at least two affected members from the same family [5]. The most common mode of inheritance is the autosomal dominant type, while X-linked, autosomal recessive and mitochondrial forms are less common [8, 9]. Although most people affected die in early adulthood, the age of onset, rate of progression, disease complications, as well as overall prognosis and outcome vary within families [5, 10]. Nevertheless, the age of onsets in this family were similar and with a rapid progressive course. All of the sons in the family suffered from DCM as well as hearing loss. The manifestation of the brothers haven’t been reported before. We traced back three generations of this family finding no other affected members. As all the patients were male, we speculated that the possible mode of inheritance in this family is X-linked. Regrettably, the parents had no daughters and we were not able to investigate the possible association between gender and FDC of this kind. Because of the rapid progressive course, we hypothesize that autoimmune abnormalities might be the pathogenic factors for this disease, but we do not have any solid evidence yet. Fortunately, we were able to get the blood samples from the patient and the relatives. Further studies are needed to explore new susceptibility genes as well as the molecular mechanisms that are involved in the disease.
Dengue made its debut as early as 1780, when Benjamin Rush described the condition as “break bone fever”. This hitherto unfamiliar infection has now grown to demand the attention of all public health care providers. It is a mosquito borne, fast emerging, viral infection manifesting in four serotypes (1). Approximately 2.5 billion people, living mainly in urban areas of tropical and subtropical regions, are estimated to be at risk of acquiring dengue infection (2). While dengue is endemic in more than 100 countries, most cases are reported from Southeast Asia and the western Pacific regions. Around 50 million cases and 24,000 deaths are estimated to occur in these 100 endemic countries. This includes hospitalisation of nearly half a million cases of dengue haemorrhagic fever (DHF), of which 90% are children. Treated (DHF)/dengue shock syndrome (DSS) is associated with a 1% mortality rate while mortality rate among untreated cases escalates to 20%(3,4).
India is one of the seven identified countries in the Southeast Asia region regularly reporting incidence of DF/DHF outbreaks. The first confirmed report of dengue infection in India dates back to 1940s, and since then more and more new states have been reporting the disease which mostly strikes in epidemic proportions often inflicting heavy morbidity and mortality, in both urban and rural environments.(5)
The various manifestations of dengue may not have a distinct line of demarcation: apart from the classic features, reports of rare presentations have recently become more frequent (6,7). During recent outbreaks in India, the clinical manifestations which were shown by the patients were slightly different from those in previous years(8).. There have been many reports of difficulties in the use of the previous classification, which were summarised in a systematic literature review (9). Difficulties in applying the criteria for dengue haemorrhagic fever in the clinical situation, together with the increase in clinically severe dengue cases which did not fulfil the strict criteria, led to the request for the classification to be reconsidered .Hence, WHO revised the dengue case classification into dengue (with or without warning signs), and severe dengue (10).The present study was done to analyse the clinical features, complications, cost incurred and outcome of cases admitted to a tertiary care teaching hospital in Bangalore.
Methodology:
A record based descriptive study was conducted in paediatric patients admitted with signs and symptoms suggestive of dengue fever to KIMS hospital Bangalore, during the period between January 2012 to December 2012. SD BioLine kit was used for testing with NS1 antigen\ IgM\ IgG. The medical records were perused for collecting data about these cases using a pre-designed proforma. Data was analysed for the clinical presentations, outcome and direct cost incurred in respect to hospital charges and laboratory investigations.
Results:
Out of 1230 cases admitted with clinical signs and symptoms suggestive of dengue syndrome 757 (61.5%) cases were found to be NS1 antigen\ IgM\ IgG positive for dengue. Among the 757 positive cases, males were 499 (65.9%) and females 258 (34.1%). The majority of the cases were in the school going age group and this consisted of 310 cases (41%) and adolescent children which accounted for 249 cases (33%), the median age being 8 years of age. The least number of cases were seen in infants which accounted for 45 cases (6%).
Table 1. Sex distribution
Age group
Male
Female
Total
Infant
31
14
45
Toddler
114
39
153
School going
208
102
310
Adolescent
146
103
249
TOTAL
499 (65.9%)
258(34.1%)
757
The majority, 88.5% of cases presented as dengue fever without warning signs, 6.34% with dengue fever with warning signs and 5.15% with severe dengue. Of the cases with warning signs 92.3% of cases had fever, 42.5% cases had vomiting and 38.2% cases had abdominal pain. Haemorrhagic manifestations were seen in about 4.5% of cases of which majority (87%) presented with petechiae followed by haematemesis (9%) and epistaxis (4%). Rashes were seen in 4% and arthralgia in 13% of cases. Pleural effusion was seen in 21% of cases and ascites was seen in 16% of cases. Complications in the form of acute respiratory distress syndrome (ARDS) was seen in 12.06% cases, 6% cases showed neurological manifestations in the form of encephalopathy and 1.3% cases had renal failure.
Table 2. Severity of dengue
SEVERITY
PERCENTAGE
DF without warning signs
88.5
DF with warning signs
6.3
Severe dengue
5.15
Table 3. Presenting complaints
Presenting Complaints
Number (%)
Fever
699(92.3)
Myalgia
148(19.5)
Haemorrhagic manifestations
34(4.5)
Vomiting
321(42.5)
Abdominal pain
289(38.1)
Headache
201(26.5)
Arthralgia
99(13)
Diarrhoea
80(10.5)
Others
121(16)
Fig 1 presenting complaints.
Haemoglobin level of > 12gm% was found in 73.4% cases, 9-12gm% in 23.4%, 6-9gm% in 2.1% and <6 gm% in 1.1% of cases. Platelet count of < 20,000 was found in 21.5% of cases, 20-50 thousand in 39.5% , 50,000 to 1.5 lakh in 36% of cases and >1.5 lakh was found in 3% of cases. Majority (65.5%) of cases were NS1 Ag positive alone or with IgM/ IgG/ or both positive.
Remaining were positive for either of the antibodies.13.7% cases werepositive for all the three i.e. Ag, IgM,& IgG. The mortality rate was found to be 8.6%
Figure 2: outcome
Cost incurred which includes direct cost (transporting patient to the hospital, diagnostic testing and laboratory investigations, medications, hospitalisation, food) was found to been average of Rs.12,611=00. The indirect cost loss of wages of patient &attendants) was found to be an average of Rs.3, 109=00. The hidden cost (out of pocket expenses) was found to be an average of Rs.50=00. The cost of treatment of other co-morbid conditions was found to be an average of Rs.2, 275=00. The total cost of treating dengue syndrome was 18,045=00
Discussion:
In the present study it was found that males were commonly affected and the most common age group was between 5 to 15 yrs of age. Similar results were reported in a study by Faridi et al, 76% of all cases of DHF /DSS were aged 6 years or more[11].
In the present study, the most common presenting symptoms was fever followed by vomiting and abdominal pain which is similar to study done by Kumar A et al showed fever in 99.2% followed by myalgia (64.6%), vomiting (47.6%), headache (47.6%) and abdominal pain (37.5%) (12).
In the present study, the most common bleeding manifestation was haematemesis and epistaxis. In a study by Ratageri et al, common bleeding manifestations were gastrointestinal bleeding (22%) and petechiae (18%) [13]. The gastrointestinal tract was reported as the commonest site of bleeding (61%) in a study by Ahmed et al [14].
In the present study majority of cases had platelet count between 20,000 to 50,000/mm3.In a study by Kamath et al, platelet counts less than 50,000/mm were noted in 62.3% [15]. In our study complicated cases showed ARDS and neurological manifestations in the form of encephalopathy. Almost all the cases which expired were found to have ARDS. Dengue associated ARDS is associated with a high mortality [16]. Dengue infection is found to cause neurological manifestation ranging from non-specific symptoms to encephalitis and rarely Guillain-Barre Syndrome [17]. In our study the mortality rate was found to be 8.6% , in the study by Anju et al overall mortality seen was 6% [18], compared to 3% by Ahmed et al [14].
Conclusion:
The seropositivity for dengue was 61.5% with NS1 antigen\ IgM\ IgG. Males were commonly affected and most vulnerable age group was found to be 5-15 year olds. The median age was 8 years. 88.5% of cases presented as dengue fever without warning signs, the remaining being dengue with warning signs and severe dengue. Fever was the most common symptom seen followed by vomiting and abdominal pain. Haemorrhagic manifestations were seen in about 4.5% of cases of which majority presented with petechiae followed by haematemesis. The mortality rate was 8.6%. Acute Respiratory Distress Syndrom (ARDS) and multiple organ dysfunction syndrome (MODS) was found to be the most dreadful complications with high rates of mortality .
In this study it was found that cost incurred which includes direct cost (transporting patient to the hospital, diagnostic testing and lab investigations, medications, hospitalisation, food) was found to bean average of Rs. 12,611=00. Thus dengue syndrome also causes significant economic burden on the patients.
In the recent few years, the world has seen varied clinical presentation of the dengue fever in different epidemics, even in the same regions and even with the period of time. Where some known features are still manifesting, few atypical features are noted from several parts of the world. A continuous seroepidemiological surveillance and timely interventions are needed to indentify the cases, so that its complications, outbreak and mortality can be minimised.
Moreover community awareness, early diagnosis and management and vector control measures need to be strengthened, especially during peri-monsoon period, in order to curb the increasing number of dengue cases.
Community acquired urinary tract infection (UTI) due to Escherichia coli is one of the most common form of bacterial infections, affecting people of all ages. Originally ESBL (extended spectrum β-lactamases) producing E. coli was isolated from hospital setting but lately this organism has begun to disseminate in the community.1
In India community presence of ESBL producing organisms has been well documented. However, various epidemiological factors associated with ESBL producing strains need to be documented. This will allow clinicians to separate patients with community UTI with these factors so that appropriate and timely treatment can be given.2 A community UTI when complicated may be a potentially life-threatening condition. In addition, for deciding the empirical treatment for patients with a UTI a thorough knowledge of local epidemiology is required. Therefore, the primary objective of this study was to determine the epidemiological factors associated with ESBL positive community acquired uropathogenic E. coli isolates and to determine their susceptibility to newer oral drugs. Mecillinam is a novel β-lactam antibiotic that is active against many members of family Enterobacteriaceae. It binds to penicillin binding protein (PBP 2), an enzyme critical for the establishment and maintenance of bacillary cell shape. It is given as a prodrug that is hydrolyzed into active agent. It is well tolerated orally in the treatment of acute cystitis.3
Material and Methods
This prospective study was conducted, from Jan 2012- July 2012, in our tertiary care hospital, which caters to medical needs of the community in North India.
Study Group:
The study group included patients diagnosed as having a UTI in outpatient clinic, or the emergency room or patients diagnosed within 48 hrs after of hospitalization. These patients and were labeled as patients having a community UTI. A diagnosis of symptomatic UTI was made when patient had at least one of the following signs or symptoms with no other recognized cause: fever ≥ 38.8˚C, urgency, frequency, dysuria or suprapubic tenderness and a positive urine culture (i.e. ≥105 microorganisms/ml of urine).4 Various epidemiological factors for each patient were recorded on individual forms. This included age, presence of diabetes mellitus, renal calculi, pregnancy, history of urinary instrumentation, recurrent UTI (more than 3 UTI episodes in the preceding year) and antibiotics intake (use of β-lactam in the preceding 3 months).2
Patients with a history of previous or recent hospitalization were excluded from study.
Antibiotic susceptibility testing was carried out following Clinical Laboratory Standards Institute (CLSI) guidelines using the Kirby-Bauer disc diffusion method.5 The antibiotics, which were tested included Amoxyclav (30/10µg), Norfloxacin (10µg), Ciprofloxacin (5µg), Tetracycline (30µg), Nitrofurantoin (300µg), Trimethoprim-sulfamethoxazole (23.75/1.25µg), Cephalexin (30µg), Cefaclor (30µg), Cefuroxime (30µg), Mecillinam (10µg) (Hi-Media, Mumbai, India).
Detection of ESBL
ESBL detection was done for all isolates according to latest CLSI criteria.5
Screening test - According to latest CLSI guidelines, zone diameter of E. coli strain for Ceftazidime <22mm and for Cefotaxime < 21mm is presumptively taken to indicate ESBL production.
Confirmatory test - As per CLSI guidelines, ESBLs were confirmed by placing a disc of Cefotaxime and Ceftazidime at a distance of 20mm from a disc of Cefotaxime /Clavulanic acid (30/10µg) and Ceftazidime/Clavulanic acid (30/10µg) respectively on a lawn culture of test strain (0.5 McFarland inoculum size) on Mueller-Hinton agar. After overnight incubation at 37° C, ESBL production was confirmed if there was a ≥5mm increase in zone diameter for either antimicrobial agent tested in combination with Clavulanic acid versus its zone when tested alone
Control strain - Standard strain of Klebsiella pneumonia ATCC 700603 was used as ESBL positive controland Escherichia coli ATCC 25922 was used as ESBL negative control.
Results
Out of total of 140 strains of E. coli, which were screened for ESBL production, 30 (21.4 %) isolates were found to be positive. High-level resistance was seen for many antimicrobial agents like Cephalexin (92.8%), Cefaclor (90%), Amoxy-clavulanate (88.57%), Cefuroxime (75.7%), Sulfamethoxazole-trimethoprim (72.8%), Norfloxacin (75.71%) and Ciprofloxacin (70%). Sensitivity to Nitrofurantoin was found to be 90%. Only 4.5% of uropathogenic E. coli were resistant to Mecillinam.
Various epidemiological factors seen in ESBL producers include female patients (n =24, 80%), history of antimicrobial intake (n = 17,57 %), elderly age >60 years (n =16 53%), renal calculi (n =15, 50%), history of recurrent UTI (n =11, 37 %), pregnancy (n = 11,37%), diabetes mellitus (n = 7, 23%) and history of urogenital instrumentation (n = 7, 23%).
Discussion
The epidemiology of ESBL positive uropathogenic E. coli is becoming more multifaceted, with increasingly indistinct boundaries between the community and hospital.6 In addition, infection with an ESBL producing organisms causing community UTI is associated with treatment failure, delayed clinical response, higher morbidity and mortality. These organisms are multi-resistant to other antimicrobials like Aminoglycosides, Quinolones and Co-trimoxazole. Therefore, empirical therapy with Cephalosporins and Fluoroquinolones often fail in patients with community UTI.7
The rate of ESBL producers in our study is lower than that described by other authors. In a similar study Mahesh E et al. reported higher rate (56.2%) of ESBL positivity from E. coli, which were causing UTIs from a community setting.8 Additionally Taneja N et al. described a higher rate (36.5%) of ESBL positivity in uropathogens. 9,10
A high rate of resistance was seen to almost all antimicrobial agents. This is in agreement with other authors like Mahesh et al. and Mandal J et al.8,11 Mecillinam showed very good results with only 4.5% resistance. Wootton M et al. reported similar high activity of Mecillinam against E. coli(93.5%).3 Auer S et al. reported that Mecillinam can be a good oral treatment options in patients with infections due to ESBL organisms.7
A limitation of our study was that being a developing country with limited resources, molecular typing and determination of antimicrobial resistance profiles of the isolates was not done. In our study female patients, elderly, patients with a history of antimicrobial intake, renal calculi and history of recurrent UTI were important factors for infection due to ESBL producers. These findings are similar to risk factors studied by other authors.2 In conclusion; this study confirms that ESBL-producing E. coli strains are a notable cause of community onset infections especially in predisposed patients. The widespread and rapid dissemination of ESBL-producing E. coli seems to be an emerging issue worldwide. Further clinical studies are needed to guide clinicians in the management of community onset infections caused by E. coli.
Hospital acquired infections (HAI) are one of the most common complications involving hospital care and are the leading cause of death in U.S. Central line associated Blood stream Infection (CLABSI), Ventilator Associated Pneumonia (VAP), Surgical site infection (SSI) and Catheter associated urinary tract infection (CAUTI) represent 75% of all HAI1 . HAI prevention is one of the 20 ‘priority areas’ identified in the Institute of Medicine (IOM) 2003 report ‘transforming health care quality’2. Certain HAI are preventable, but as the prevention efforts become more defined, there remains a lack of evidence of a strong return of investment for hospitals and health care payers in preventing these infections. This lack of evidence presents potential obstacles in advancing efforts to prevent infections.
Central Line Associated Blood Stream Infection (CLABSI)
CLABSI is a primary blood stream infection that develops in a patient with a central line in place within the 48 hour period before the onset of blood stream infection, which is not related to infection at another site. Central line associated blood stream infection occurs up to 80,000 times per year resulting in 28,000 deaths among patients in the Intensive Care unit (ICU). Average cost of CLABSI is approximately $ 45,000 per incidence3. CLABSI reduction is also one of the success story of how inexpensive interventions, grouped as a checklist could reduce the rate of nosocomial infections to a median rate of zero. Although quality control interventions in many areas of ICU have been studied, the idea of integrating quality indicators with group of interventions known as bundles has been validated in the ICU most successfully in CLABSI. The landmark study on reduction of CLABSI was the ‘Keystone ICU’ project funded by the Agency for Health care Research and Quality (AHRQ) 4. One hundred and three ICUs in Michigan participated in this state wide safety initiative. The study intervention recommended five evidence based procedures that were identified as having the greatest effect on the rate of catheter related BSI and the lowest barriers to implementation. The interventions were remarkably successful, nearly eliminating CLABSI entirely in most ICUs over an 18 month follow up period.
Although in short term intensive training and monitoring can lead to improved outcomes, in long term the biggest impact on decreasing HAI, is of the safety climate of the unit. Studies have linked safety climate to clinical and patient outcomes in addition to showing that the safety climate is responsive to interventions. A large study targeting the culture of safety was a follow up of the Michigan Keystone study. The study was a prospective cohort study to improve quality of care and safety culture by implementing and evaluating patient safety interventions in participating ICUs and showed large scale improvements in safety climate among diverse organizations5. As part of the national effort to reduce the HAI, the Department of Health and Human Services (HHS) launched the HHS action plan to reduce the health care associated infections in 2009. The project was titled ‘On the cusp: Stop BSI’, designed to apply the principles of comprehensive unit based safety program (CUSP) to improve the culture of patient safety and implement evidence based best practices to reduce the risk of infection. The initiative ultimately reduced mean rates of CLABSI in participating units by an average of 40%, preventing more than 2000 CLABSI, saving more than 500 lives and avoiding more than $34 million in excess health care costs6.
Ventilator Associated Pneumonia
Optimizing the care of mechanically ventilated patients is an important goal of health care providers and hospital administrators. An easily acquired and reliable marker for medical quality has been elusive for this patient population. VAP has historically been used as a marker of the quality of care associated with mechanically ventilated patient and is associated with worse outcomes7. However the diagnosis of VAP is non-specific, the clinical diagnosis by the widely used American College of Chest Physicians (ACCP) criteria includes a new progressive consolidation on chest radiography plus at least two of the following clinical criteria: fever > 38, leucocytosis or leucopenia and purulent secretions. Unfortunately, all these findings alone or in combination can occur in other non-infectious conditions, making the diagnosis of VAP subjective and prone to bias. In fact, for the last many years, the surveillance rates of VAP are decreasing, whereas the clinical diagnosis of VAP and tracheobronchitis as well as antibiotic prescribing remains prevalent. External reporting pressures may be encouraging stricter interpretation of the subjective signs that can cause artifactual lowering of the VAP rates. The result is that, it is almost impossible to detangle the relative contribution of quality improvement efforts in the ICU versus surveillance efforts as explanation for the currently observed lower rates of VAP8.
To eliminate the subjectivity and inaccuracy and to create an objective , streamlined and potentially automatable criteria, Center of Disease Control (CDC) now recommends surveillance of ventilator associated events (VAE) as a more general marker and defines it as sustained increase in patient’s ventilator settings after a period of stable or decreasing support . There are three definition tiers within the VAE algorithm; 1) Ventilator Associated Condition (VAC); 2) Infection Related Ventilator Associated Complication (IVAC); and 3) Possible and probable VAP. The screening for VAC captures a similar set of complications to traditional VAP surveillance, but it is faster, more objective and potentially a superior predictor of clinical outcomes9. In a CDC funded study of 597 mechanically ventilated patients on use of VAC as an outcome predictor, it was noted that 9.3% of the study population had a VAP, whereas 23% had VAC. VAC was associated with increased mortality (odds ratio of 2.0) but VAP was not. VAC assessment was also faster (mean 1.8 minutes vs 3.9 minute per patient) 10.
Similar to the CLABSI bundles, prevention of VAP by utilization of evidence-based bundles of care has proved to be a very successful. Heimes and colleagues recently conducted a study examining 696 consecutive ventilated patients in a level 1 trauma center to evaluate a VAP prevention bundle with 7 elements. They found a VAP rate of 5.2/1000 days of ventilator support in the pre intervention phase, while a 2.4 /1000 and 1.2/1000 days (p= 0.085) in the implementation and enforcement periods respectively11.
Health care associated UTI account for up to 40% of infections in hospitals and 23% of the infections in the ICU. The vast majority of UTIs are related to indwelling urinary catheters. CAUTI result in as much as $ 131million excess direct medical costs nationwide annually12. Since October 2008, Center of Medicare Services (CMS) no longer reimburses hospitals for the extra costs of managing a patient with hospital acquired CAUTI.
There are certain factors like Diabetes mellitus, old age or severe underlying illness that places patients at a greater risk of CAUTI, but there also are modifiable factors like non adherence to aseptic catheter care recommendations and duration of catheterization that can be targeted by quality improvement efforts, to decrease the risk13. The key strategies for prevention of CAUTI include avoiding insertion if possible, early removal by implementation of checklists, nurse based interventions or daily electronic reminders, utilization of proper techniques for insertion and maintenance and considering alternatives to indwelling catheters like intermittent catheterization, condom catheters and portable bladder ultrasound scanner. Most of these strategies have been utilized in quality improvement efforts to decrease CAUTI. Assessment of the need is essential as Munasinghe et al have found urinary catheter placed in 21 to 50% of patients for inappropriate reasons14. A nurse based reminder to physician to remove unnecessary urinary catheters in a Taiwanese hospital resulted in reduction of CAUTI from 11.5 to 8.3 /1000 catheter days15. Similarly utilization of electronic urinary catheter reminders system and stop orders have been shown to reduce the mean duration of catheters by 37% and CAUTI by 2%16. Utilization of condom catheter has also been shown to be effective in reducing bacteriuria, symptomatic UT and mortality as compared to indwelling catheter17.
Final word
Health care is often compared with airline industry with six sigma efficiency. This would translate to 0.002 defective parts or errors/million, obviously we are not close to that and may not be realistic. However this also cannot be an excuse to rationalize poor practice culture. As in any industry, in health care to establish change it is essential to regulate interpersonal interactions. With behaviors change leading to changes in processes of care, change is not only possible, it is sustainable.
We report the case of 36 year old white Caucasian female who used to work as a driving instructor and living with her parents.
She has a diagnosis of congenital adrenal hyperplasia (21 hydroxylase deficiency) and is on long term corticosteroid replacement (prednisolone 4 mg once daily and fludrocortisone
100 mcg once daily) and she is under the care of an endocrinologist.
She was referred for psychiatric evaluation with “anxiety and depressive symptoms” and failure to respond to antidepressant treatment which was prescribed by her General Practitioner.
During the psychiatric assessment, she reported long history of recurrent episodes of elevated mood and depression dating back to her late teens with clear description of distinct periods of mood elevations lasting for few weeks and longer periods of persistent low mood. There was no history of psychotic symptoms and no family history of mental illness.
She was diagnosed with bipolar affective disorder and failed to achieve remission of symptoms on two different antipsychotic medications (quetiapine and olanzapine) and anticonvulsant medication (sodium valproate) before starting lithium carbonate.
The introduction of lithium and gradual titration resulted in significant improvement in her symptoms and mood stability. However, few months later, she reported relapse in her symptoms (mainly reporting features of bipolar depression) despite adequate lithium levels.
She agreed on the introduction of lamotrigine as an adjunctive medication to lithium. The initial dose of lamotrigine was 25 mg daily for two weeks in line with dose recommendation from manufacturer and drug guides.
On the same day of lamotrigine introduction, the patient started to experience visual hallucinations that she never had before (please see patient’s perspective for detailed description of her hallucinations).
With the dose of lamotrigine increased to 50 mg daily after the initial two weeks, she started to report worsening of these abnormal perceptions which developed into more complex visual and auditory hallucinations.
More importantly, there was no evidence of accompanying manic symptoms or severe depressive symptoms to explain these symptoms and also no alcohol or drug use.
Following a psychiatric review, the dose of lamotrigine was reduced to 25 mg which resulted in immediate reduction in the intensity of the abnormal perceptions. When the lamotrigine was eventually stopped after one week, there was complete cessation of abnormal perceptions.
Lamotrigine was never re-started again and she was maintained on a combination of lithium and quetiapine with good effect.
Investigation:
We used the Naranjo Adverse Drug Reaction Probability Scale (1) to determine the likelihood of whether an adverse drug reaction is related to this specific drug or may be related to other factors. This tool examine factors such as the temporal association of drug administration and event occurrence, alternative causes for the event, drug levels, dose – response relationships and previous patient experience with the medication.
The probability of the adverse drug reaction is concluded from the total score (Definite if the overall score is 9 or greater, Probable for a score of 5-8, Possible for 1-4 and Doubtful if the score is 0).
Questionnaire
1. Are there previous conclusive reports on this reaction? Yes (+1)
2. Did the adverse events appear after the suspected drug was given? Yes (+2)
3. Did the adverse reaction improve when the drug was discontinued or a specific antagonist was given?
Yes (+1)
4. Did the adverse reaction appear when the drug was re-administered? Do not know or not done (0)
5. Are there alternative causes that could have caused the reaction? No (+2)
6. Did the reaction reappear when a placebo was given? Do not know or not done (0)
7. Was the drug detected in any body fluid in toxic concentrations?
No (0)
8. Was the reaction more severe when the dose was increased or less severe when the dose was decreased?
Yes (+1)
9. Did the patient have a similar reaction to the same or similar drugs in any previous exposure?
No (0)
10. Was the adverse event confirmed by any objective evidence? Do not know or not done (0)
Scoring 7 (Probable Adverse drug reaction)
Discussion:
Lamotrigine is a phenyltriazine derivative used as an anticonvulsant drug with established mood stabilising properties. In the United Kingdom, it is recommended for use in bipolar affective disorder according to the guidelines from the National Institute of Health and Care Excellence (2) and the British Association for Psychopharmacology (3).
We performed a literature search to find similar case reports. We searched the following databases using the keywords (lamotrigine AND hallucinations): Complementary Medicine (AMED), British Nursing Index BNI), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta Medica Database (EMBASE), Health Business Elite (HMIC), Medline, PsycINFO and Health Management Information Consortium (HMIC).
The search returned 57 results. Only 8 articles discussed hallucinations and other psychiatric symptoms as side effects associated with lamotrigine and therefore were included in this review.
Psychotic symptoms have been reported with the use of lamotrigine (both as an anticonvulsant or mood stabiliser) but this reaction is mainly seen in patients with history of epilepsy. One study reported 4.8% incidence of psychiatric and behavioural side effects with lamotrigine in 546 patients with epilepsy. (4)
Another study on paediatric patients showed that reversible visual and auditory hallucinations were reported in one patient among 9 patients with epilepsy who received lamotrigine treatment (mean age 5 years). (5)
Villari et al published a literature review on psychiatric symptoms related to lamotrigine and included case reports documenting full acute psychotic episodes hallucinations and affective switching in patients with and without history of epilepsy.(6)
They found one case report on hallucination with lamotrigine in bipolar patient without epilepsy. In patients with epilepsy, they reported two cases reports and one case series (total number of patients 9) developing psychotic symptoms following lamotrigine and one randomised controlled trial in which four out of 216 patients stopped lamotrigine due to psychotic symptoms (including hallucinations and delusions).
The authors concluded that majority of the case reports concluded that these symptoms were lamotrigine-induced due to the temporal association with lamotrigine treatment and favourable outcome following drug withdrawal. It also appeared that more case reports were from patients with epilepsy, suggesting lower incidence in patients without this condition.
Chistyakova and Amos (7) reported a case of delirium associated with lamotrigine use. The dose of lamotrigine was increased from 200 to 400 mg over two weeks prior to her admission. The patient reported visual and auditory hallucination with confusion. She took an accidental overdose of her medication (200 mg of fluoxetine and 2800 mg of lamotrigine) due to her confusion and medications were stopped.
The authors concluded that delirium may result from lamotrigine toxicity or drug interaction with fluoxetine.
Uher and Jones in 2006 (8) reported a case of a 42-year-old woman with bipolar affective disorder with comorbid alcohol abuse and no history of neurological illness.
The patient tolerated an initial dose of lamotrigine 50 mg/day but following a dose increase to 100 mg/day, she reported vivid dream-like experiences and subsequently she reported visual hallucinations. These symptoms subsided over a few days when the dose was decreased to 50 mg/day.
The authors suggested a causal association through this dose dependent effect but also pointed out that the concurrent alcohol abuse may have been a contributing factor.
They also highlighted the paucity of case reports documenting this rare adverse reaction and identified two similar case reports in their references (which we were unable to get their full text) and a third paper reporting hallucination in 2 out of 108 patients with epilepsy on a combination of lamotrigine and sodium valproate (9)
Hallucination with lamotrigine when combined with valproic acid was also reported in a case report by Roberts et al (10) in 14 year old girl with epilepsy when it was added to valproic acid and it was suggested that this adverse effect may be due to an interaction between the two medications causing lamotrigine half-life to triple with valproic acid.
Learning points:
Lamotrigine is an anticonvulsant with an established role in management of bipolar affective disorder, particularly for the treatment and prevention of depressive episodes.
However, it appears to be associated with variable incidence of psychiatric symptoms which should be known to the prescriber and patient.
These adverse effects are mainly seen in patients with history of epilepsy but can occur in patients with mental health problem without epilepsy.
Different mechanisms for inducing these psychiatric symptoms have been suggested, including idiosyncratic reaction, lamotrigine toxicity as a result of concomitant use of another drug that affect lamotrigine metabolism (e.g., valproic acid) and delirium.
Examples of these psychiatric symptoms including affective switches in depressed patients with bipolar disorder, hallucinations in depressed patients, delirium and psychotic symptoms (mainly hallucinations and delusions) in patients with or without epilepsy.
Reversible and severe psychiatric disturbances associated with lamotrigine therapy are rarely reported in literature and more research is needed to identify population at risk.
Patient education about these rare but frightening side effects is essential to improve medication adherence and better outcome of the management of the mental disorder.
Patient perspective:
“The first hallucination I had was one hour roughly after taking lithium and lamotrigine. It was the Pope which appeared as bright light on my wall. He was wearing a white gown and he had gold jewellery. The picture was so clear and very detailed. I’m not religious and this image would not be something I would think of.
Every day on lamotrigine I had black spots moving quickly around the walls. They were in size of about an inch, 20-30 moving around at one time. Like spiders but without legs. I was really scared at first because I hate spiders. It was very unsettling and I changed my whole bed, away from my wall, and had trouble sleeping.
There was another night when I had similar to the black dots, where instead I had smaller black dots like bees moving into the corner of my room. They were all slightly moving as if they were getting their places. There were hundreds of them.
The scariest incident that happened was hearing voices downstairs. I was so sure that people had broken into the house; I went downstairs armed with razors. I was going to cut DNA from the burglars to give to the police as evidence. When I checked the house, there was no one there.
When I was taking lamotrigine with the lithium, it made me very unsettled, more anxious and mentally unstable. I was so tiered for not sleeping and my decisions irrational. It wasn’t a pleasant place to be for me personally.”
Injuries in children are common.1 In the UK, incidence is found to be 20.2 fractures per 1000 per year. The peak age of incidence is on average of 9.7 years .2 Up to 42 per cent of boys and 27 per cent of girls will sustain at least one fracture during the paediatric age. 3
A study conducted in Northern Sweden in the age group of 0 - 19 years showed that there is a rise in injury related visits to emergency department over the years. Fractures and dislocations accounted for 21.4 per cent of the cases.1Consequently, this will put a pressure on fracture clinics as new cases take a considerable in fracture clinic.
The purpose of this audit was to assess the pattern of new cases referred to fracture clinic at a large paediatric university teaching hospital
Materials and Methods
This prospective audit was carried out over a four-week period in May and June of 2010 and it was approved by the institutional clinical audit department. There were a total of 18 working days. A total of 864 patients were seen in the fracture clinic during this period, which included 310 new cases and 554 follow up cases. Data was collected from the fracture clinic patient list for the respective days and the new patient list was extracted from this. Using the picture archiving and communication system (PACS), the radiographs and reports were analysed to collect the data regarding the fracture sustained.
Results
Total number of cases seen during the 4 week period were 864, which included 310 new cases and 554 follow up cases. Two hundred and ninety two cases out of 310 were analysed, as 18 cases did not have radiographs available.
There were 170 males and 140 females. The average age was 9 years (range 1 month to 16 years).
One hundred and seventy seven (61%) showed fractures. One hundred and one (34%) cases did not have any fractures and 14 (5%) were suspected fractures.
The following figure 1 shows the pattern of cases on each working day. Those, which are left blank, are non working days or cancelled clinics. The average number of cases seen per day were 48 and of these, the average of new cases seen were 17.2 and the average number of follow up cases seen were 30.7.
As shown in figure 2, fractures of the distal radius and ulna were the predominant cases (23%) followed by hand fractures (15%). Other fractures included: lower limb excluding foot [23 (8%)], elbow and humerus [14 (5%)], clavicle [11 (4%)], foot [12 (4%)] and others [5 (2%)].
Further analysis of the fractures sustained showed that forearm injuries were the predominant cases and majority of them were buckle or greenstick fractures. The detailed distribution is shown in the figure 3 below.
Figure 1 showing the daily pattern of cases
Figure 2 showing the area involved
Figure 3 showing the pattern of fracture
Discussion
Fracture clinics are a part of any trauma and orthopaedic department. One must consider the benefits of providing such a service and routine audits are necessary to improve the efficiency, accuracy and above all, best possible patient care.
Although there is evidence that simple fracture like buckle fractures of the distal radius do not need orthopaedic input and can be safely treated in emergency department using a splint, and can be discharged without follow up 4, concerns have been raised against the possibility of a misdiagnosis and providing patient information 5.
Radiographic interpretation is often done by junior doctors in the emergency department. Guly6 demonstrated that there is significant issue in misreading radiographs and missing the injuries. The second problem was noted to be not requesting a radiograph. It has been suggested that better training in interpreting radiographs and rapid reporting by radiologist could solve this problem.
Others have adapted local departmental audits and guidelines and have shown to reduce the risk.7
Another possibility is a rapid review of radiographs by orthopaedic consultants on the same day as suggested by Beiri et al.8 But if the hospital is covering a large population area including peripheral walk in centres, this becomes difficult due to accessibility and logistic reasons.
Toeh and collegues9 investigating attitudes of parents towards paediatric fracture clinic found that mothers were the one who predominantly accompanied their children and most children had to take time off school to attend the clinic. It was also interesting to note that parents perception of severity of injury prompted attendance at follow up clinics.
In another study, ninety nine per cent of the parents thought attendance at the fracture clinic was important. However, when evaluating the socio economic costs, they found that this led to loss of 0.25 working days of parents, 0.18 daily wages and 0.54 schooling days per visit.1
A combination of factors may lead to fracture clinic appointments especially in paediatric population. Departmental protocols and guidelines may help in reducing the fracture clinic visits, however careful consideration must be given while drawing up these for a successful outcome.
Inappropriate referrals lead to usage of time and resources, which can lead to delay of service meant for those in need of specialist opinion. In our audit, 34% of the cases seen did not have any fractures and 5% were suspected fractures.
One of the drawbacks of this audit includes lack of case note review of those cases where fractures were not present. It would have been ideal to investigate the nature of cases seen, and whether this was treated as soft tissue injuries, or seen just for reassurance or used as a safety net.
The following recommendations could be used as possible solutions to decrease inappropriate referrals to fracture clinic.
If the patient is seen in Accident and Emergency (A&E), where appropriate and when diagnosis is in doubt, there should be an opportunity for the patient to be seen or discussed with a more senior doctor in A&E.
With regards to Peripheral Walk In Centres, there should be an opportunity to discuss it with the on call Orthopaedic team with the integration of PACS, so that images are readily available for viewing, and to consider rapid reporting of images.
The use of Specialist Physiotherapists for soft tissue injuries in A&E with follow up in physiotherapy clinics were shown to have high patient satisfaction rates and reduce fracture clinic follow up. Similar strategy could be considered.11, 12
Conclusion
This study has shown that although the majority of patients needed treatment, a significant number (34%) did not have fractures. Considerable amounts of time can be saved, especially in a busy fracture clinic if unnecessary appointments could be avoided. It would also benefit patients by avoiding unnecessary visits to the fracture clinic. A repeat study following the consideration of recommendations would reveal any benefit of such a strategy.
There are approximately over 1.6 billion overweight people with a body mass index (BMI) greater than 25 kg/mAnnually, around 2.8 million deaths are attributed to overweight and obesity worldwide(1). Many overweight individuals underestimate their weight and despite acknowledging their overweightness, many are not motivated to losing weight(2).Accurate measurement is important as it identifies patients with diagnoses which subsequently impact on their management. Self-reported weight is often used as a means of surveillance but has been shown to bias towards under reporting of body weight and BMI as well as over reporting on height(3). Several estimation techniques has been devised to quantify anthropomorphic measurements when actual measurement cannot take place(4),(5),(6), however, these methods are associated with significant errors for hospitalised patients(7). There is no published study that questions the validity of visual estimation of obesity in daily clinical setting despite its relevance to the daily practice. We aim to investigate the accuracy of visual estimation compared to actual clinical measurements in the diagnosis of overweight and obesity.
Methods:
This is a case control study. Patients for this study were attending the endocrinology, cardiology and chest pain out-patient clinic in Cork University Hospital, Cork, Ireland. The questionnaire session was carried out at every endocrinology, cardiology and chest pain clinic for 5 consecutive weeks. A total of 100 patients were recruited allowing for a 10% margin of error at 95% confidence level in a sample population of 150 000. Ten doctors of varying grades were chosen randomly to visually score the subjects. Exclusion criteria included patients who were pregnant and who are wheelchair bound. Consent was obtained from patients prior to filling questionnaires. Ethical approval was received from the Clinical Research Ethics Committee of the Cork Teaching Hospitals.
In the waiting room, patients were asked to self- report their weight, height and waist circumference to the best of their estimate. Demographics and cardiovascular risk were obtained from medical charts and presented in Table 1. The questionnaires have a section that specifically tests patients’ awareness of abdominal obesity and patients were asked to choose between obesity and abdominal obesity, relying on their own knowledge of markers of cardiovascular risks. Clinical measurements were taken in the nurses’ assessment room. Weight was measured by using portable SECA scales (Seca 755 Mechanical Column Scale) and was measured to the nearest 0.1kilogram. All patients were measured on the same weighing scale to minimize instrumental bias. Patients were asked to remove their heavy outer garments and shoes and empty their pockets and to stand in the centre of the platform, so that weight is distributed evenly to both feet.
Height was measured by using a height rule attached to a fixed measuring rod (Seca 220 Telescopic Measuring Rod). Patients were asked to remove their shoes and are asked to stand with their back to the height rule. It was ensured that the back of the head, back, buttocks, calves and heels are touching the wall. Patients were asked to remain upright with their feet together. The top of the external auditory meatus is leveled with the inferior margin of the bony orbit. The patients were asked to look straight. Height is recorded to the resolution of the height rule (i.e. nearest millimeter).
Waist circumferences were measured using a myotape. Patients were asked to remove their outer garments and stand with their feet close together. The tape is placed horizontally at a level midway between the lower rib margin and iliac crest around the body. They were then asked to breathe normally and the reading of the measurement was taken at the end of gentle exhaling. This prevents patients from holding their breath. The measuring tape is held firmly, ensuring its horizontal position and loose enough that it allows placement of one finger between the tape and the subject's body. A single operator who has been trained to measure waist circumference as per the WHO guidelines is used repeatedly in order to reduce measurement bias(8).
The doctors were asked to visually estimate the patients' weight, height, waist circumference and BMI. The estimation is recorded on a separate sheet. All doctors were blinded to the actual clinical measurements. The questionnaires were then collected at the end of the clinic and matched to individual patients. Data entry was performed in Microsoft Excel and exported for statistical analysis on SPSS version 16.
Findings
The study enrolled 100 patients. Demographic and cardiovascular risk details are shown in Table 1. Among these, 42 were obese, 35 were overweight and 23 patients had a normal BMI. The sample has a mean BMI of 29.9kg/m2 (95% CI 28.7-31.1) with a mean waist circumference (WC) of 103.2cm (95% CI 100.7-107.2). The average male waist circumference is 105.8 cm while the average female waist circumference is 101.6cm. The mean measured weight was 84.6kg (95% CI 81.0-88.2) and the mean height measurement was 1.68m (95% CI 1.66-1.70).
Table 1: Cardiovascular risk factors
Sex
Male(n=55)
Female(n=45)
Mean age
53.6(19-84)
56.7(23-84)
Diabetes
17
14
Hypertension
16
20
Hypercholesterolaemia
24
19
Active smoker
10
5
Ex- smoker (>10years)
8
3
Previous stroke or heart attack
6
6
Previous PCI
6
3
Patient’s perception and doctor’s estimation of anthropomorphic measurements were compared to actual measurements and is displayed in Table 2.
Table 2. Deviation from actual measurement values in both groups
Patient’s Estimation
Mean estimated
Mean deviation (estimated – actual measurements)
95% Confidence interval of Mean Deviation
Weight
81.16
-3.71
-5.10 to -2.32
Height
1.6782
0.0039
-0.0112 to 0.0033
Waist
90.85
-13.09
-15.48 to -10.70
BMI
28.68
-1.24
-1.87 to -0.61
Doctor’s visual estimation
Weight
80.85
-3.78
-5.54 to -2.02
Height
1.6710
-0.0113
-0.224 to 0.002
Waist
92.10
-11.84
-13.87 to -9.81
BMI
29.08
-8.47
-1.54 to -0.15
In terms of patients own estimation of height, weight and waist circumference, 49% of patients under estimated their weight by up to 1.5kg, 35% reported accurately to 1.5 kg and 16% over reported weight. 67% of patients estimated height accurately, 18% of patients under-estimated, and 15% over-estimated. When asked to estimate their waist circumference, 68% of patients under estimated by up to 5cm, 30% over estimated and 2 patients estimated accurately to 5cm (Figure 1). We found that 70% of patients regarded obesity as the higher threat to health compared to abdominal obesity. There were no differences in patient’s self reported weight and doctor’s weight estimation (p= 0.236).
Figure 1. Graphical representation of patients estimated weight, height and waist circumference
We then analysed the doctor’s estimation of height, weight, waist circumference and BMI. For the purpose of interpreting the data on BMI, the estimates that is recorded by doctors that matches the patient’s real BMI by clinical measurement is considered accurate. Therefore, for patients who have a normal BMI, 69.5% were correctly estimated as normal and the rest (30.5%) were estimated as overweight. For those patients who are obese, 81% were estimated as obese and by the doctors as a group and the rest (19%) is estimated to be overweight. In patients who are overweight, 63% were correctly estimated as being overweight by doctors, 9% were estimated as being obese and the rest (28%) were mistakenly estimated as having a normal BMI. Accurate BMI estimation by doctors was achieved in 72% patients (Figure 2).
Figure 2. Doctors estimation of BMI compared to actual clinical measurement
Doctors were noted to underestimate the patients’ weight in 53 patients, over estimated in 26, while being accurate in their estimation in 21 patients. Estimation of waist circumference to the nearest 5 cm shows marked under estimation of waist circumference in 71% of patients, over reporting in 3% of patients and 26% accurate estimation. The majority of underestimation of waist circumference happens in the region of 10 to 15cm. For patients who are obese, doctors were able to estimate waist circumference correctly in 58% of obese individuals.
Discussion:
This is the first study demonstrating the relationship of visual estimation of a cardiovascular risk factor and comparing to actual clinical measurements. As obesity and abdominal obesity becomes an increasingly common phenomenon, our perception of the 'normal' body habitus may be distorted(9).
It is observed that in the bigger hospitals out-patient departments, physicians and nurses are commonly affected by clinical workload and tend to spend a limited amount of time with patients in order to achieve a quicker turnaround time. Cleator et al looked at whether clinically significant obesity is well detected in three different outpatient department and whether they are managed appropriately once diagnosed(10). In all the outpatient departments involving the specialties of rheumatology, cardiology and orthopedics, the actual cases of clinical obesity is higher than what is being diagnosed and the management of obesity was heterogeneous and minimal in terms of intervention. With the ever increasing obese patients attending hospitals, it is understandable that healthcare providers such as physicians, nurses, dietician and physiotherapist resort to relying on visual estimation.
In terms of patient’s own estimation of height, weight and waist circumference, we gained that patients were reasonably good at estimating their own height but tend to under estimate weight. This is probably due to the fact that these patients have not had a recent measurement of weight and their weight estimation is based on previous historical measurement from months to years back, which in the majority of people, is less than their current weight. This also explains why their height estimation is more accurate, as adult heights do not undergo significant changes and are relatively constant.
When attempting to obtain patient’s own estimation of waist circumference, we found that most patients are not at all aware of the method used to measure waist circumference. Some patients even mistaken waist circumference as being their trousers’ waist size. In those who were able to give estimation, a large proportion would under estimate.
The majority of patients think that general obesity is more predictive of cardiovascular outcome compared to abdominal obesity. This lack of awareness is reflective on clinician’s effort in addressing abdominal obesity as an important cardiovascular risk factor to patients during consultations. The lack of proper awareness campaign by healthcare providers along with the evolving markers of cardiovascular risk may further confuse the general public.
Recently, waist circumference, waist to hip ratio along with many serum biomarkers have been noted to correlate to adverse outcomes in obese individuals, independent of BMI. Waist circumference measurement is a relatively new tool compared to the measurement of BMI. This would explain the discrepancy between doctors’ estimation of BMI and waist circumference. Visual estimation is further compromise as many patients would be covered in items of clothing during consultations. In order to obtain a better estimation of waist circumference, the individual have to be observed from many angles, a task that may be impossible in a busy clinic.
Although BMI is a convenient method to quantify obesity, recent studies have shown that waist circumference is a stronger predictor of cardiovascular outcomes(11),(12),(13),(14).The importance of waist circumference in predicting health risk is thought to be due to the relationship between waist circumference and intra-abdominal fat(15),(16),(17),(18),(19),(20).We now know that the presence of intra-abdominal visceral fat is associated with a poorer outcome in that patients are prone to develop metabolic syndrome and insulin resistance(21).We have yet to devise a more accurate measurement on visceral fat and at present limited to using waist circumference measurements.
Although doctors are generally good at BMI estimation, we found that in estimating overweight patients’ BMI, close to 30% were wrongly estimated as having normal BMI. Next to the obese, these groups of patients are likely to have metabolic abnormalities and increased cardiovascular risk. If actual measurement of BMI is not routinely done, we may neglect patients who would benefit from intervention. A simple, short counseling during the outpatient visit with emphasis on weight loss, the need to increase their daily activity levels and the morbidity related to being overweight may be all that is needed to improve the population health in general. Further intervention may include referrals to hospital or community dieticians and prescribed exercise programmes. These intervention tools already exist in the healthcare system and could be accessed readily.
The nature of our study design exposes it to several potential selection and measurement biases. Future studies should include patients of differing ages and socioeconomic background. Additionally, clinicians of differing appointments from various different specialties should be included to obtain a more applicable result. A measure of diagnostic efficacy should also be employed to further assess the value of clinical measurement and therapeutic intervention.
Conclusion:
The appropriateness of visual scoring of markers of obesity by doctors is flawed and limited to the obese individuals. True anthropometric measurements would avoid misdiagnosing overweight individuals as normals. We can conclude that patients’ own estimation of weight is unreliable and that they are unaware of the impact of high abdominal fat deposition on cardiovascular outcome. The latter should be addressed in consultations by both hospital physicians and general practitioners. Further emphasis and education in schools and awareness campaigns should also advocate this emerging cardiovascular risk factor.
“The more we care for the happiness of others, the greater our own sense of well being becomes.” The Medicine of Altruism: Dalai Lama
Introduction
The fundamental mission of any medical school is to select those individuals who possess the qualities and personality traits best suited to becoming a good doctor. The first part of this article takes a critical look at how United Kingdom (UK) medical schools select doctors, which can vary considerably, and asks whether it can be improved. The qualities needed to be a good doctor are discussed and asks whether work experience illustrates at least some of these personal qualities and should therefore be an essential prerequisite for applying to medical school. Such experience helps the student to make an informed career choice and exploring it at interview can reflect student motivation to study medicine. My experience in Ghana gave me the opportunity to find out at first hand if I had what it takes to become a doctor. The trip was totally inspirational. It made me realise that medicine is much more than being master of all sciences. In Ghana I saw many of the qualities one needs to be a doctor, how this contrasts with the current selection criteria in the UK, and made me wonder whether the UK system offers our society the best practice available.
Critique of UK medical school selection
Applying to medical school has become increasingly competitive. Selection into medical schools is not an exact science but one assumes that best available evidence is being used. The present system almost certainly turns away students who would make good doctors and accepts some who are mediocre or poor or even drop out of medicine altogether. The selection criteria for entry into medicine have to be accurate. However, no system is fool proof and the number of drop-outs in UK training stands at 6.8 – 12%.1,2,3 I believe that better selection criteria would reduce the drop-out rate and save personal distress among those who made an unwise choice. This makes economic sense. There is widespread agreement that we should select medical students on wider criteria than scores of academic success,4, 5 though in practice many medical schools have valued academic scores at the expense of other considerations.6, 7 A Levels alone should not be sufficient to gain a place at medical school. True communication calls for some shared life experiences and empathy with others. I believe that students who are totally absorbed in their studies to the exclusion of almost everything else are less likely to make good doctors. In one study, a ten-year follow-up after entry into medical school showed no correlation between academic score at entry and drop-out rate, but significant correlation between low interview scores and later drop-out.8 Reasons for drop-out were a variety of personal reasons including lack of motivation for study or for medicine. In a medical school that carefully evaluates applicants, empathy and motivation to be doctors were found to be particularly important in predicting both clinical and academic success.9
Another major study, looking at the dropping out from medical schools in the UK over a ten year period (1990-2000), 10 showed that drop-out rates increased during this period and concluded that the probability of dropping out of medical school is 20% lower for students with a parent who is a doctor. The authors comment that this may be the result of greater commitment or better preparation and insight before starting the course. Ethnic background of students was recorded only between 1998-2000. The study found that Indian females were around 1.9% less likely to drop out compared with white females, whereas Indian males were no different from white males. Other ethnic groups were less likely to drop-out by around 0.8%. A concerning fact in this paper was the degree to which drop-out rates varied between different medical schools. No study to date has been done to find the reasons for these differences. Surely potential applicants need to be aware of these results. The differences could be accounted for by variable selection processes among the medical schools.11 Some medical schools shortlist for interview only on predicted academic performance or the number of A* GCSEs or decide by the UK Clinical Aptitude Test (UKCAT) / BioMedical Admissions Test (BMAT) scores. Some use information presented in the candidate’s personal statement and referee’s report while others ignore this because of concern over bias. In some cases candidates fill in a supplementary questionnaire. Interviews vary in terms of length, panel composition, structure, content, and scoring methods. Some schools do not interview.
The commonest reasons cited in many papers for dropping out of medical school were because it is not for them, they found it boring, they did not like patients, the work environment was not what they want to spend their time on, or they did not like responsibility.12 Essentially they had realised too late that Medicine was not for them. They had failed to find out what they were letting themselves in for before applying and the medical school had failed to pick this up. There is a strong argument for pooling resources so that applicants get one good assessment instead of four poor ones.
A levels, used for medical selection, do not indicate any personality attributes of the candidate and are affected by socio-economic bias. The UKCAT was introduced to level the playing fields. This test doesn’t examine acquired knowledge and candidates can’t be coached to pass, so in theory it should provide a fairer assessment of aptitude than A level grades. It was also thought that the various components of the UKCAT, namely verbal reasoning, quantitative reasoning, abstract reasoning, and decision making, could help to pick the students who have the personality attributes to make good doctors. Unfortunately, a recent paper suggests that the UKCAT does not provide any more assessment of aptitude than A levels.13 However, an inherent favourable bias towards students from well-off backgrounds or from grammar and independent schools was also found. Moreover the test does not compensate for talented candidates whose education has been affected by attending a poor school. Another paper looked at the predictive validity of the UKCAT.14 This showed that UKCAT scores did not predict Year 1 performance at two medical schools. Although early prediction is not the primary aim of the UKCAT, there is some cause for concern that the test failed to show even the small-to-moderate predictive power demonstrated by similar admission tools.
There is no doubt that potential doctors must have enough intellectual capacity to do the job but they must also possess other important traits (Table 1):
Table 1: Personality traits potential doctors ought to possess
Concern for people
Committed to self-learning
Sense of responsibility
Emotionally stable
Professionalism
Good judgement and perception
Good communication skills
Good listener
Highly motivated
An enquiring mind
Honesty
Well organised
Integrity
Patience
Ability to handle pressure
Mental strength
Confident
Resilience
Determination
Respect for other people
Perseverance
Respect for confidentiality
Decisiveness
Tolerance
Conscientious
Hard working
Team player
An open mind
Leadership qualities
A rational approach to problems
Humility
Critical reasoning
Flexible and adaptable to change
Separate important points from detail
Logical thinking
Recognise limits of professional competence
What patients rate highly among the qualities of a good doctor are high levels of empathy and interpersonal skills.15 Personality traits such as conscientiousness have been positively associated with pre-clinical performance.16
The criteria being used more and more by admission tutors include the candidate’s insight into medicine including as evidenced from work experience.17Surprisingly, very little has been written on work experience and the value placed on it varies considerably between medical schools. Many would regard this experience as a prerequisite for entry into medical school. It enables a student to experience at first hand what he/she is letting him/herself in for. Some find the experience fascinating and challenging while others may find it is not for them. Work experience should not be seen as a hurdle to climb, but part of the decision-making process in determining whether medicine really is for you. I fear that another contributing factor to the increase in drop-out rates from medical schools is the increasing difficulty in obtaining work experience. Gone are the days when students could join theatre staff and watch an exciting operation or shadow doctors in Accident and Emergency (A&E). Useful work experience is so important and it is becoming harder and harder to get, but is still possible. Therefore considerable desire, commitment and motivation by the student are required to obtain it. The work does not need to be medically related, but work experience in any care setting is essential. These placements can be used to illustrate at least some of the personal qualities that are sought after in a good doctor including: appreciation of the communication skills required of a doctor; a thorough awareness of the realities of medicine and the National Health Service (NHS); an understanding of teamwork; an ability to balance commitments; and observation of the caring and compassionate nature of the doctors. Furthermore, as demonstrated in general practice,18 personal experiences can have a highly positive influence on an individual’s attitude to a particular speciality. Encouraging school students to experience general practice would therefore not only increase their awareness of the life to which they are about to commit, but could aid recruitment to general practice as a speciality.
My Ghana Experience
I decided that, as part of my work experience, I would go to Ghana with a charity organisation (Motec UK Life). The reason was not to impress medical admissions tutors, but to discover if I had what it takes to become a doctor. I realised how comfortably we live in our small bubble, with little appreciation of what goes on in the rest of the world. Ghana is a third world country, which not only has great poverty and malnutrition but also has many deadly diseases such as Acquired Immunodeficiency Syndrome (AIDS)/Human Immunodeficiency Virus (HIV), malaria, hepatitis, typhoid and sickle cell disease. My trip was demanding as I was stripped of my luxuries and removed from my comfort zone, but it helped me to understand the real values in life through helping the most needy and vulnerable people. I felt the suffering and the pain they went through, day in and day out, but knew that making even the slightest difference to their lives motivated me and enabled me to persevere through my time there.
One of the hospitals we stayedwas Nkawkaw, which was in the middle of a shantytown with houses made of metal sheets. Yet, despite the presence of great poverty and disease, I did not find a single person who was not extremely kind and welcoming and always smiling. It made me think of the contrasting situation back home in the UK where people were relatively well off, and yet so unhappy. I spoke to as many people as possible, not realising that I was developing my people- and communication-skills. I played football with the children and made them smile. I was able to visit the AIDS/HIV clinic and gained a first-hand account of how this devastating disease was controlled and dealt with in a third-world country. The pain, grief and suffering were immense and difficult to comprehend unless one was actually there witnessing it. AIDS here hurts everyone, but children are always the most vulnerable. The children were born with HIV from their mothers, or infected through breast milk, or in the past infected by unsafe medical treatments. They were often orphaned and destitute, having to build their own homes, grow their own food, and care for younger brothers and sisters. That is the cruel reality.
Equally heartbreaking was seeing so many people in the HIV clinic who could
not afford the anti-retroviral drug that would improve the quality and duration of life. This feeling of helplessness motivated me even further to pursue a career in medicine in order to help people at their most vulnerable. On this trip I was greatly impressed by the dedication, commitment and professionalism shown by the doctors in difficult situations. I saw doctors working with little supervision and little equipment, and yet they seemed confident, well organised, and adapted themselves well to the conditions. Their enthusiasm and compassion never waned despite working long hours.
I saw many types of operation being performed including joint replacements, hernia repairs and caesarean sections. On one particular day, I observed the team performing many knee and hip joint replacements. The deformities of the joints were much more severe than seen in the UK. I enjoyed and appreciated the skills of the orthopaedic surgeons in carrying out these operations, which were being done under spinal anaesthesia, and so I was able to talk to the patients and comfort them. Throughout the day, after seeing many operations, I did not flinch or feel queasy at the sight, and this further encouraged me to believe that I could handle a career in medicine. On watching the caesarean sections, the excitement of bringing new life into the world was overwhelming. Seeing another baby being born with severe hydrocephalus marred this. No treatment facilities for this condition were available for hundreds of miles and the baby was too ill to be transferred such a large distance. I witnessed the doctors conveying the heartbreaking news to the family with compassion. It became clear to me that there are negative aspects to this career. There is a great deal of emotion and stress to cope with in such circumstances but I believe that, given training, I would be mentally stronger to take control of these situations.
I was always allowed to follow the doctors on their ward rounds, and was encouraged to ask questions and make comments, so that I often felt that I was being treated as a medical student, which was strange in some ways but also very gratifying. On this trip I was involved in teaching and in helping to set up a workshop, which lasted for a whole day for doctors from all over Ghana. This involved lectures as well as demonstrating the latest surgical and theatre equipment. I was impressed by the teamwork and organisation shown by the group. The communication skills of the group had to be of the highest quality in order to get the message across. I found that teaching about the devastating effects of HIV, in a local school in Ghana, was particularly challenging as some of the students before me were sufferers and so I found it difficult to look them in the eye, knowing that although they were being taught the safety precautions, many did not have much of a future. This reinforced my feeling of helplessness but, although this situation was heartbreaking, I remained enthusiastic for the children, to keep their morale high in order to prepare them for their inevitable future.
Conclusion
My trip was totally inspirational. It made me realise that medicine is much more than being a master of all sciences. In Ghana I observed in doctors the real passion and drive needed for medicine as well as many other essential qualities I believed doctors needed. This contrasts with the current selection criteria in the UK; sadly we are missing out on too many good doctors because of our obsession with grades rather than looking for real qualities that are going to make a difference to our patients.I discovered that seeing the immense suffering, and the close bond of doctors and patients in an entirely different social and economic context, helped me to evaluate and shape my own emotions and personal values. My motivation in wanting to become a doctor has increased tremendously since this trip. My trip to Ghana also inspired me to create a medical journal in my school as a fund-raising initiative. I brought together a group of fellow students to write articles about common teenage problems (teenage drinking, anorexia, obsessive compulsive disorder (OCD), stress, smoking, sexually transmitted diseases (STDs)) as well as articles on euthanasia and assisted suicide, stem cell research and the NHS. I wrote about my personal experiences in Ghana in addition to editing and publishing the school journal. All the funds raised from the school medical journal will be going to the HIV victims in Ghana.
In 1940, Reid and Brace 1 first described the haemodynamic response to laryngoscopy and intubation due to noxious stimuli of the upper airway. Evidence from laboratory data demonstrates that epipharyngeal and laryngopharyngeal stimulation augments cervical sympathetic activity in the efferent fibres to the heart. This explains the increase in plasma levels of norepinephrine and, to a lesser extent, epinephrine, which occur during airway instrumentation 2. The rise in the pulse rate and blood pressure is usually transient occurring 30 seconds after intubation and lasting for less than 10 minutes 3. Usually these changes are well tolerated by healthy individuals. However, these changes may be fatal in patients with hypertension, coronary artery disease or intracranial hypertension 3. Numerous agents have therefore been utilised to blunt these stimulatory effects on the cardiovascular system induced by laryngoscopy and endotracheal intubation such as deepening of anaesthesia 3, pretreatment with vasodilators such as nitroglycerin 4, beta-blockers 5, and opioids 6 etc.
Lornoxicam is a nonsteroidal anti-inflammatory drug (NSAID) that belongs chemically to the oxicams and has been successfully used as a perioperative analgesic agent with a better safety profile regarding renal and hepatic function tests, in addition to better gastrointestinal tract tolerability compared to selective COX 2inhibitors 7. Riad and Moussa 8 reported that lornoxicam added to fentanyl attenuates the haemodynamic response to laryngoscopy and tracheal intubation in the elderly. Other than this, few data are available regarding the efficacy of lornoxicam in controlling the haemodynamic variations during the peri-intubation period. Therefore the present study was designed as a double-blind randomised placebo-controlled trial to investigate the effect of lornoxicam individually on the haemodynamic response and serum catecholamine levels following laryngoscopy and tracheal intubation.
Methods:
After obtaining the approval of the Hospital Research & Ethical Committee and patients' informed consent, fifty ASA I patients, aged 18-40 years, scheduled for elective surgical procedures under general anaesthesia requiring endotracheal intubation, were enrolled in this randomised, double-blinded placebo-controlled study. Those who had taken drugs that could influence haemodynamic and autonomic function, were excluded from the study. Further exclusion criteria consisted of patients with risk of pulmonary aspiration, predictably difficult airways or obesity (body mass index (BMI) > 30%) and patients with a known allergy to NSAIDs.
In a double-blind fashion and using a sealed envelope technique, patients were randomly allocated to one of two groups to receive intravenous injection (i.v.) of either Lornoxicam 16 mg diluted in 4 ml (Group L, n = 25) or placebo received saline 4 ml (Group S, n = 25) half an hour before induction of anaesthesia as the time taken by lornoxicam to reach peak plasma concentration (Tmax) was determined to be 0.5 h 9. Since lornoxicam is yellow while placebo is a clear fluid, syringes containing both solutions were prepared covered in a double blind fashion, by a collaborator not involved in data recording. The same collaborator administered drugs while a blind observer collected data.
Patients were not premedicated. In the holding area, an i.v. cannula was inserted and an i.v. infusion of Lactated Ringer’s 10 ml Kg-1 was started half an hour before induction of anaesthesia. Additionally, a 16-gauge i.v. catheter, attached to a stopcock and flushing device, was inserted into an antecubital vein of the contralateral arm to collect blood samples. Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP) and arterial oxygen saturation (SpO2) were recorded before induction (baseline value).
After 3 min of pre-oxygenation, anaesthesia was induced with propofol 2.5mg kg-1 and cisatracurium 0.15 mg kg-1 to facilitate tracheal intubation which was performed using direct laryngoscopy when neuromuscular block was achieved by train of four-Guard monitor. SBP, DBP, MAP and HR were recorded before and after administration of the i.v. anaesthetic, immediately after intubation and cuff inflation, and every minute (min) for 10 mins. after intubation. All intubations were performed by a single anaesthetist, the duration of laryngoscopy and intubation were limited to the minimum possible time and were recorded. Data from patients in whom intubationrequired longer than 20 seconds (sec) were excluded.
Blood samples were drawn before (baseline) and 1 min. after intubation and cuff inflation for measurement of serum catecholamine concentrations. The samples were collected into pre-chilled tubes containing EDTA/Na and immediately centrifuged. Plasma concentrations of epinephrine and norepinephrine were measured in duplicate by using high-pressure liquid chromatography 10.
After tracheal intubation, patients were ventilated to normocapnia with sevoflurane (2-3% end tidal) in 50% oxygen in air. Two mins. after intubation (after collecting the blood sample), all patients received fentanyl i.v. 1.5 µg kg-1 and were monitored with ECG, SBP, DBP, MAP, SpO2 and end tidal carbon dioxide (EtCO2). All measurements were completed before skin incision. At the end of surgery, muscle relaxation was reversed and patients were extubated.
Statistical analysis was performed using SPSS version 17. Numerical data are presented as mean ± SD. Statistical comparisons among the groups were performed using unpaired t-test. Haemodynamic responses to induction and intubation in a given group were analysed using a paired t-test. The number of subjects enrolled was based on a power calculation of finding a 20% difference between the two groups in MAP and HR from the baseline values at alpha error of 0.05 and beta of 0.2. Categorical data were expressed as numbers and wereanalysed by using the 2 test where appropriate. A P value <0.05was considered statistically significant.
Results:
The two groups were comparable in demographic profile, duration of laryngoscopy and intubation as well as baseline haemodynamic parameters (table 1).
Table 1: Demographic, baseline haemodynamic characteristics and duration of laryngoscopy
Group S (Saline)
Group L (Lornoxicam)
No. of patients
25
25
Sex (female/male)
10/15
12/13
Age (yrs)
31.5 ± 5.6
33.1 ± 4.4
ASA (I/II)
19/6
20/5
Weight (Kg)
69.7 ± 4.2
66.9 ± 6.7
Height (cm)
167.9 ± 8.6
170.2 ± 4.5
Duration of laryngoscopy and intubation (sec)
14.9 (1.7)
16.2 (1.2)
HR/ minute
80.13±8.69
81.87±11.62
MAP mmHg
89.97±10.1
85.83±9.23
Systolic BP mmHg
120.2±11.2
117.44±17.1
Diastolic BP mmHg
78.7±9.91
73.13±12.42
(mean ± SD or number). No significant difference among groups
Table 2: Changes in Heart rate/minute
Group S
(Saline)
Group L
(Lornoxicam)
P
After induction
85.15±10.76
83.32±8.44
.062
0 minute after intubation
106±14.3
88.17±8.89
.000*
1 minute
101.71±11.15
86.92±9.11
.000*
2 minute
97.39±12.07
84.88±10.36
.019*
3 minute
95.48±12.95
81±9.91
.036*
Table 3: Changes in mean arterial pressure mmHg
Group S
(Saline)
Group L
(Lornoxicam)
P
After induction
84.65±8.3
79.77±9.92
.055
0 minute after intubation
129±16.54
91.73±10.7
.000*
1 minute
119.95±18.2
86.01±8.99
.000*
2 minute
105.33±13.15
83.62±10.63
.008*
3 minute
96.1±10.11
83.47±8.8
.024*
(mean ± SD). *P ≤ 0.05 is statistically significant change.
All tracheal intubations were performed successfully by the same anaesthetist at the first attempt. Following the induction of anaesthesia; SBP, DBP and MAP decreased in both groups (fig. 1 and 2).
After intubation the attenuation of the increase in SAP, DBP, MAP and HR in group L was statistically significant compared to group S, and then remained significant until 3 mins. after intubation. Haemodynamic variables are summarised in tables 2,3,4,5. The maximum rise in MAP and HR in group S at intubation was 30.5% and 42% respectively. While in group L the maximum rise in MAP and HR was 7.1% and 6.2% respectively over the entire observation period. After that, SBP, DBP, MAP and HR decreased gradually in both groups to values similar to those noted before induction. Furthermore, blood samples collected one minute following intubation showed a significant increase in serum epinephrine and norepinephrine concentrations in group S compared to group L in the same observation period (fig. 3) (table 6).
Table 4: Changes in systolic blood pressure mmHg
Group S
(Saline)
Group L
(Lornoxicam)
P
After induction
107.38±11.71
102.25±12.89
.069
0 minute after intubation
169.27±18.29
117.35±13.5
.0001*
1 minute
141.53±15.51
113.68±12.91
.005*
2 minute
128 ±11.2
115.39±14.17
.014*
3 minute
122.99±12.56
111.67±14.8
.037*
(mean ± SD). *P ≤ 0.05 is statistically significant change
Table 5: Changes in diastolic blood pressure mmHg
Group S
(Saline)
Group L
(Lornoxicam)
P
After induction
72.49±8.79
68.99±8.1
.085
0 minute after intubation
109.53±14.22
78.48±8.51
.000*
1 minute
92.18±10.63
74 ±7.75
.007*
2 minute
89.77 ±11.34
78.12±7.98
.02*
3 minute
81.45±8.8
73.6±8.21
.043*
(mean ± SD). *P ≤ 0.05 is statistically significant change
Table 6: Changes in serum catecholamine level nmol/L
Group S
(Saline)
Group L
(Lornoxicam)
P
Epinephrine
Pre intubation
.195±.119
.179±.104
.085
1 min postintubation
.206±.112
.181±.087
.038*
Norepinephrine
Pre intubation
1.11±.633
1.098±.51
.059
1 min postintubation
1.499±.903
1.107±.524
.000*
(mean ± SD). *P ≤ 0.05 is statistically significant change
Discussion:
Lornoxicam has been successfully used in prevention and treatment of postoperative pain 11. It was reported that i.v. 8 mg of lornoxicam was equianalgesic with 20 mg of morphine 12, 50 mg of pethidine 13, while 16 mg of lornoxicam had a superior analgesic effect compared with 100 mg of tramadol 14 and was comparable to 100 µg of fentanyl as intraoperative analgesia in mild to moderate day case ENT surgical procedures 15.
Our results showed a significant fall in SBP, DBP and MAP in both groups after induction. This might be due to the vasodilatation associated with the administration of propofol. Patients in both groups exhibited an increase in heart rate since no medicine other than Lornoxicam was added to propofol to decrease pain on injection. Propofol can cause significant tachycardia from pain in addition to reflex tachycardia due to a decrease in SVR. As the SBP, DBP and MAP rose significantly for the first 3 minutes after intubation in the control group, a further reduction in SVR due to the vasodilator effect of sevoflurane is the probable reason for the return of the MAP to nearly baseline values over the entire observation period. The fall in HR over the same period might be partly due to the bradycardia associated with fentanyl administered 2 minutes after intubation in both groups.
In our study, lornoxicam attenuated the pressor response to laryngoscopy and tracheal intubation; SBP, DBP, MAP and HR were significantly lower in L group compared to S group in the first 3 min after intubation. This may be attributable to the analgesic action of lornoxicam mediated through the antiprostaglandin effect of COX inhibition, the release of endogenous dynorphin and β-endorphin 14, a decrease in peripheral and central prostaglandin production, 16 as well as it exerting some of its analgesic activity via the central nervous system 17.
In agreement with our results, Bruder and colleagues 18 reported that laryngoscopy and intubation violate the patient's protective airway reflexes with marked reflex changes in the cardiovascular system and lead to an average increase in blood pressure by 40-50% and a 20% increase in heart rate. Kihara and colleagues 19, when comparing the haemodynamic response to direct laryngoscopy with the intubating laryngeal mask and the Trachlight device, reported that the HR increased compared with preoperative baseline values in all groups. Moreover, both systolic and diastolic pressure increased after tracheal intubation for 2 mins. with the highest values in the hypertensive group receiving direct laryngoscopy.
In a previous study done by Riad and Moussa 7, i.v. administration of 8 mg lornoxicam half an hour before surgery added to fentanyl 1 µg Kg-1 during induction of anaesthesia was found to attenuate the haemodynamic response to laryngoscopy and tracheal intubation in the elderly. However, it was unclear whether this was attributed to the drug's narcotic effect. Therefore, our study was designed to evaluate the use of lornoxicam individually, in a single i.v. administration of 16 mg lornoxicam half an hour before surgery. Lornoxicam 8 mg was not used as it was proven to have an inadequate analgesic effect 15.
There have been a few studies which have measured catecholamine levels after intubation. Our results are consistent with those of Russell et al 2 and Shribman et al 20 who reported significant elevations in serum levels of norepinephrine and epinephrine following laryngoscopy and tracheal intubation. Hassan and colleagues 21 concluded that during laryngoscopy and endotracheal intubation, placing the tube through the cords and inflating the cuff in the infraglottic region contributes significantly to sympathoadrenal response caused by supraglottic stimulation.
When assessing techniques to ameliorate the cardiovascular responses to intubation; the drugs used to induce anaesthesia may influence the results. We induced anaesthesia with propofol which produces hypotension. This may compensate in part for the cardiovascular changes attributable to laryngoscopy and tracheal intubation. This could be considered a limitation of the present study. The omission of opioids during the induction of anaesthesia in healthy young patients should not be a concern.
In conclusion, pretreatment with lornoxicam in the doses given in this study, attenuates the pressor response to laryngoscopy and the intubation of the trachea.




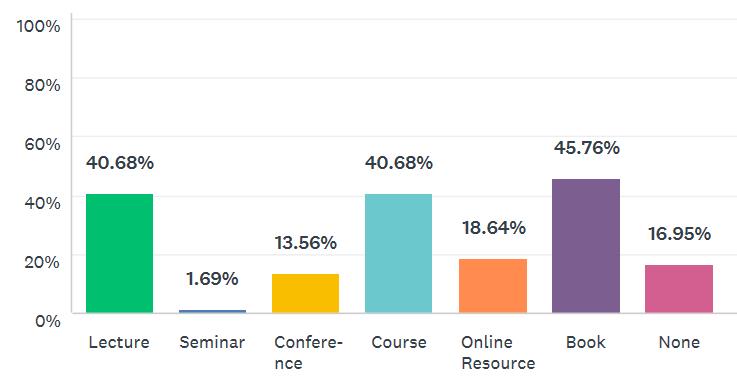
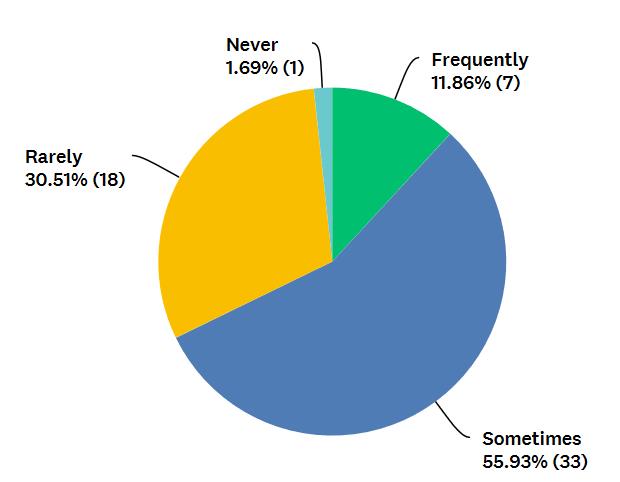
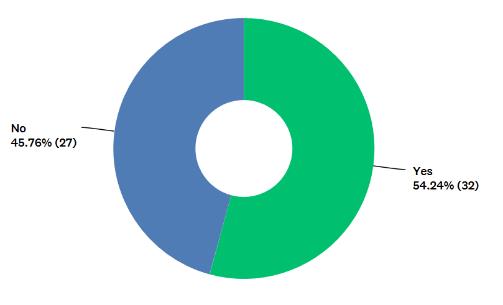
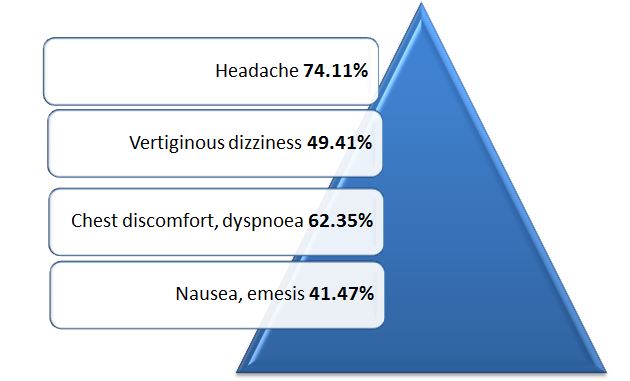
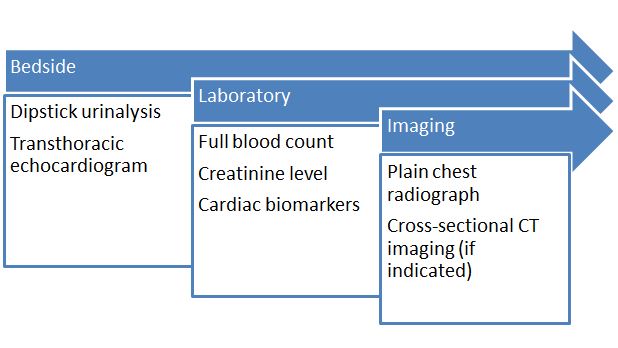
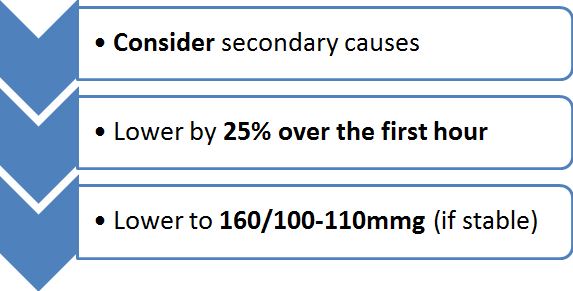





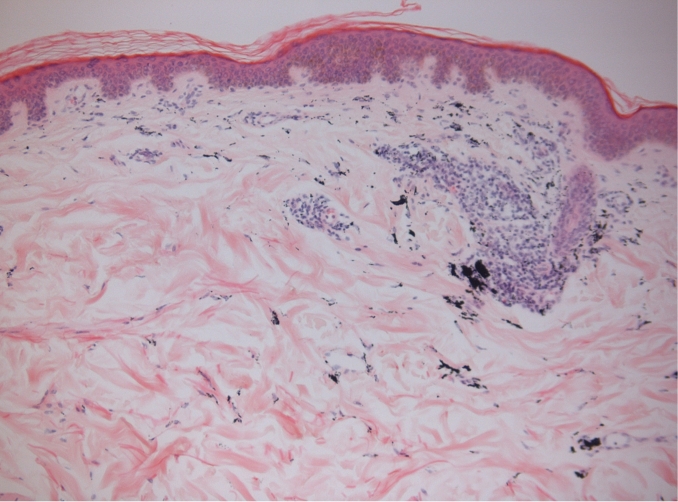
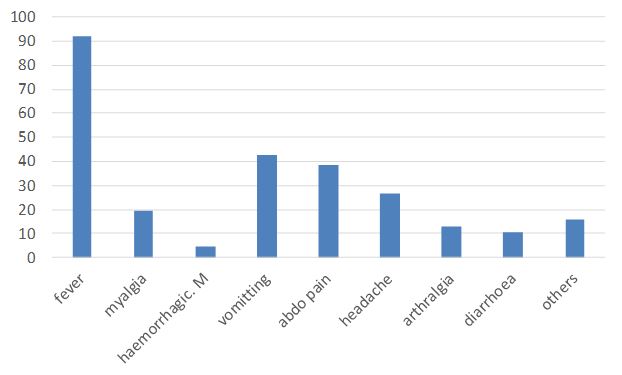
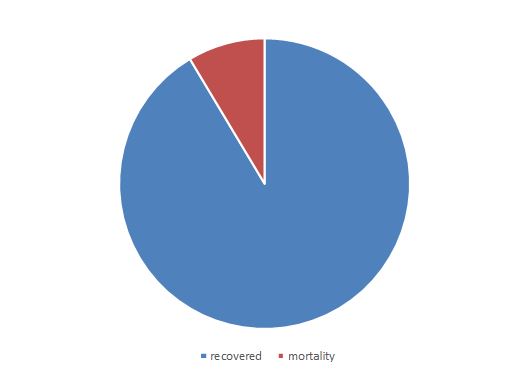
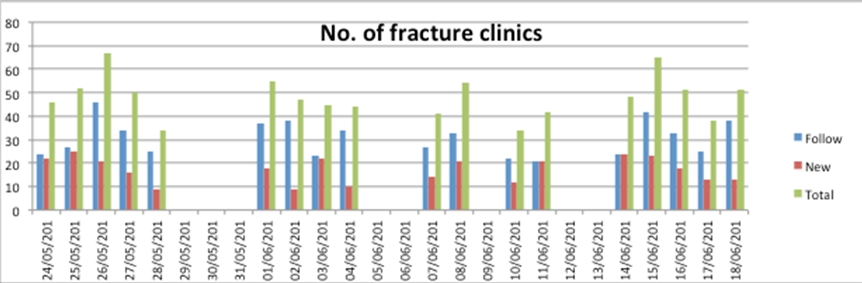
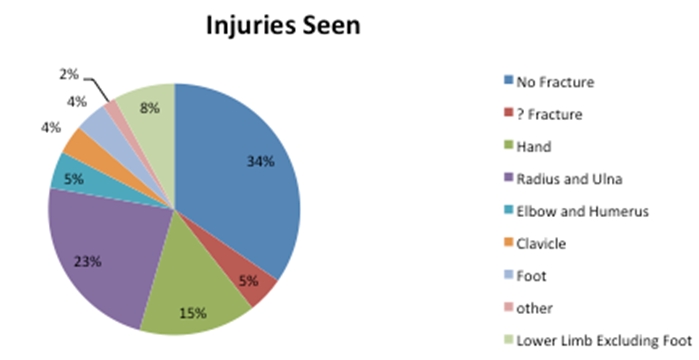
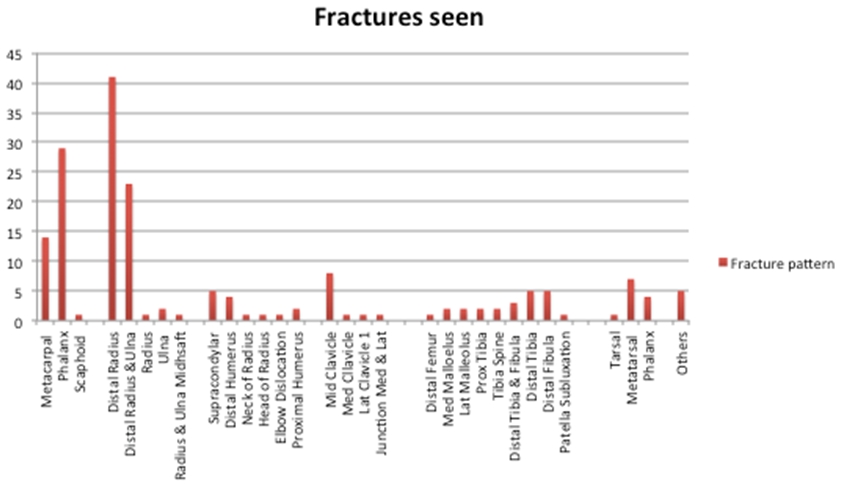
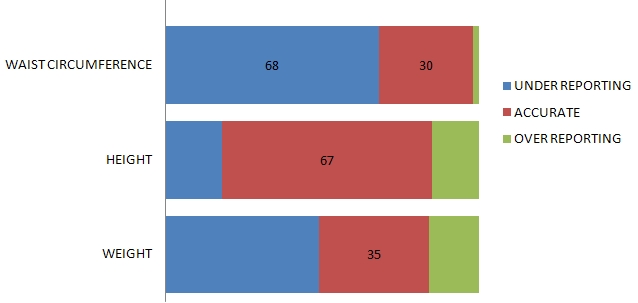
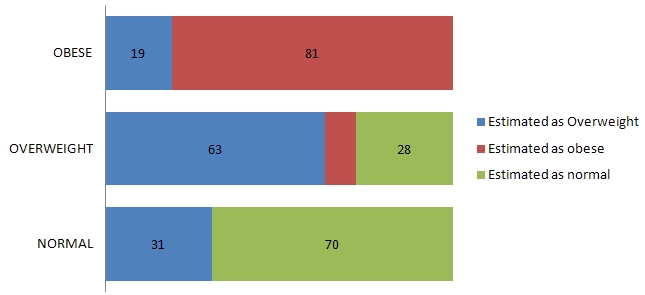
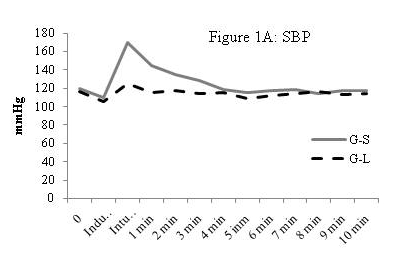
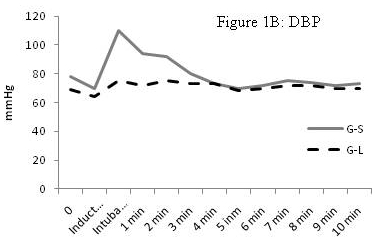
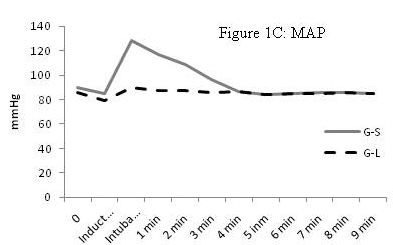
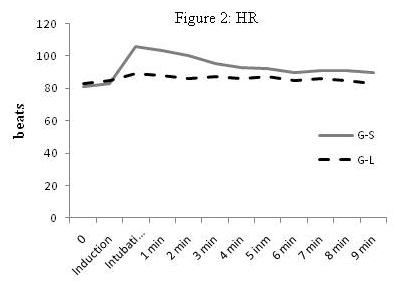
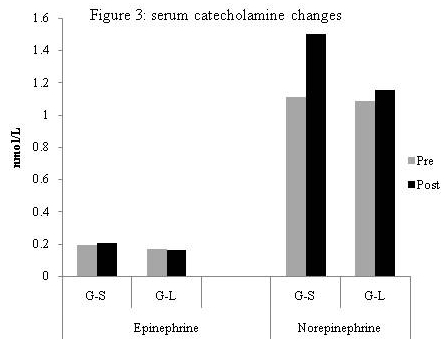
BJMP July 2021 Volume 14 Number 1
Research Articles
Education and Training