David Kingdom is a Professor of Mental Health Care Delivery at University of Southampton and Honorary Consultant Psychiatrist to Hampshire Partnership Foundation Trust.
How long have you been working in your speciality?
30 years
Which aspect of your work do you find most satisfying?
Clinical work can be very stimulating but so can research particularly when you feel, rightly or wrongly, that you have contributed something original which can benefit patients.
What achievements are you most proud of in your medical career?
Developing cognitive behaviour therapy for people with psychosis and then seeing it gradually becoming part of accepted practice in many parts of the world.
Which part of your job do you enjoy the least?
Doing reports and filling in forms.
What are your views about the current status of medical training in your country and what do you think needs to change?
Generally I think there have been many positive developments of it especially in improving the interaction between patients, health care staff and doctors but there is still a real problem with conveying the importance of psychological aspects.
How would you encourage more medical students into entering your speciality?
I would like to see psychology being increasingly accepted as a relevant qualification on a par with other sciences.
What qualities do you think a good trainee should possess?
Intelligence and warmth.
What is the most important advice you could offer to a new trainee?
Spend as much time learning from patients and their carers as you can.
What qualities do you think a good trainer should possess?
Intelligence and warmth.
Do you think doctors are over-regulated compared with other professions?
No, although revalidation may be going that way.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what should be done to counter this trend?
No – we need to maximise the efficiency of our work and this will mean gradual change in roles of ourselves and others.
Which scientific paper/publication has influenced you the most?
‘Not made of wood’ by Jan Foudraine, a Dutch psychiatrist who spent time listening to patients in long-stay hospitals and drawing out the extraordinary stories of their lives.
What single area of medical research in your speciality should be given priority?
Psychological treatments for currently treatment resistant conditions.
What is the most challenging area in your speciality that needs further development?
Classification of mental disorders.
Which changes would substantially improve the quality of healthcare in your country?
Introduction of effective care pathways which are linked directly to outcome measurement and funding contingent on these.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Yes – by seeing that clinically effective interventions are made available to those who can benefit from them.
How has the political environment affected your work?
Funding has improved over the past decade but is now looking much more uncertain.
What are your interests outside of work?
Family, sailing & watching Southampton FC.
If you were not a doctor, what would you do?
Law probably as it also involves work with people and is a steady job.
Immediate postoperative care of patients undergoing nasal surgery, e.g. septoplasty or rhinoplasty, could be hazardous as desaturation happens frequently especially if the patient is not fully recovered struggling for nasal breathing while the nose is packed with gauze.1,2 Moreover, ice may be applied to the nose in the operating room to decrease swelling, and an external splint could be taped by the surgeon onto the patient’s face.3 All make it difficult to apply and fit a Hudson recovery face mask in the post-anaesthesia care unit (PACU) to maintain adequate oxygenation.
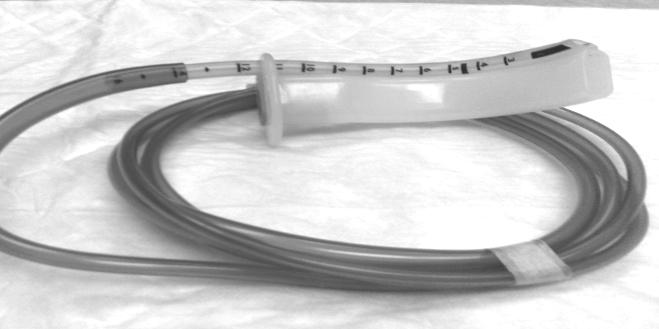
Figure 1
Facing this problem, we prepared an oral oxygenating airway device, to maintain an open unblocked airway in addition to adequate oxygenation, in the early recovery period for patients undergoing nasal surgery. Our device (Fig 1,2) is an oral airway size 4 or 5 with a siliconised soft endotracheal tube (ETT) size 5.5 mm fixed alongside the airway with its bevel directed laterally to provide easy insertion of the airway. The distal end of the ETT is cut 4-5 cm from the airway to be connected to a breathing circuit through a 15 mm connector or connected directly to tubing of oxygen flow-meter supplying humidified oxygen at a low flow rate of 1-2 L/minute to provide FIO2 35-40%. This device was tried successfully in 54 patients scheduled to septoplasty and rhinoplasty.
Figure 2
In conclusion, this device is simple, cheap, easily inserted, efficiently maintains adequate arterial oxygen saturation as long as the oral airway is tolerated in the early recovery period, reduces the oxygen flow rate and, in addition, an oxygen analyzer can be connected to the 15 mm connector to provide monitoring of the delivered FIO2.
Forty one years after the last influenza pandemic, while everyone was worrying about the avian influenza A (H5N1) virus causing a pandemic, an apparent new chapter is opened with the emergence of new strain of influenza A virus. On 24th April, the World Health Organization (WHO) declared the first ever public health emergency of international concern indicating the occurrence of confirmed human cases of swine influenza in Mexico and United States.1 Subsequently the Centre for Disease Control and Prevention (CDC) confirmed that these human influenza cases were caused by a novel strain of influenza A virus to which there is little or no population immunity.2 On June 2009, the WHO rated the pandemic alert from phase 5 to 6, signalling that the first pandemic of the 21st century was underway. It was however stressed that the rise in the pandemic alert level was mainly attributed to the global spread of the virus rather than its severity. The pandemic potential of influenza A viruses has been ascribed to their genetic and antigenic instability and there ability to transform by constant genetic re-assortment or mutations, which can result in the emergence of novel progeny subtypes capable of both infecting and leading to sustained person to person transmission.3 The newly emerged strain contains a combination of gene segments that have not been previously identified in swine or human influenza viruses.4
Historical Perspectives
Influenza has been recognised for hundreds of years, but the cause was unknown for most of this time. Hippocrates had defined this disease about 2400 years ago, but lacked laboratory confirmation.5 The year 1580, marks the first instance of influenza recorded as an epidemic even though there is possibility that there were many prior influenza epidemics.6 The word influenza (meaning influence), first used in 1743 originated from the Latin word “Influenza”, named so because the disease was considered to be caused by unfavourable astrological conditions. Since 1700, there have been approximately a dozen influenza A virus pandemics and the lethal outbreak of 1918-1919 is dubbed as the greatest medical holocaust in recorded history, killing up to 50 million people worldwide.7
The earliest evidence of influenza A virus causing acute respiratory illness in pigs was traced to the 1930s. Swine influenza A viruses are antigenically very similar to the 1918 human influenza A virus and they may all have originated from common ancestor.8 From 1930 to 1990, classic swine influenza A was the commonest swine influenza virus circulating amongst the swine population during which the virus did not undergo much genetic change. Antigenic variants of these classical influenza viruses emerged in 1991 and the real antigenic shift occurred at the ends of last century when the classical swine influenza virus re-assorted with human influenza A virus and a North American lineage avian influenza virus. This resulted in the emergence of multiple subtypes including H1N2 and H3N2. In the past few years, sporadic cases of human infections caused by swine influenza A virus have occurred, mainly due to subtypes. Occupational exposure to swine was the most important risk factor for infection and fortunately all patients recovered without resulting in efficient, sustained human to human transmission.9
Origin of 2009 Strain
The pandemic that began in March 2009, was originally referred to as “swine flu” because laboratory testing showed that many of the genes in this new virus were very similar to influenza viruses that normally occur in pigs (swine) in North America. But further study has shown that this new strain of virus represents a quadruple re-assortment of two swine strains, one human strain and one avian strain of influenza. The largest proportion of genes come from swine influenza viruses (30.6% from North American swine influenza strains, and 17.5% from Eurasian swine influenza strains), followed by North American avian influenza strains (34.4%) and human influenza strains (17.5%).10 Analysis of the antigenic and genetic characteristics of the pandemic influenza A virus demonstrated that it’s gene segments have been circulating for many years, suggesting that lack of surveillance in swine is the reason that this strain had not been recognized previously.11 This novel strain is antigenically distinct from seasonal influenza A and possesses previously unrecognised molecular determinants that could be responsible for the rapid human to human transmission. Moreover, antigenic drift has occurred amongst different lineages of viruses, therefore, cross protection antibodies against avian, swine and human viruses are not expected to exist. Emerging scientific data support the hypothesis of a natural genesis, with domestic pigs a central role in the generation and maintenance of the virus. Protein homology analysis of more than 400 protein sequences from the new influenza virus as well as other homologous proteins from influenza viruses of the past few seasons also confirmed that this virus has a swine lineage.1 Phylogenetic analysis has suggested that initial transmission to humans occurred several months before the recognition of the outbreak and multiple genetic ancestry of this influenza A is not indicative of artificial origin.11
Situation Update
In March 2009, an outbreak of respiratory illness was first noted in Mexico, which was eventually identified as being related to influenza A.12 The outbreak spread rapidly to the United States, Canada and throughout the world as a result of airline travel.13 On 11th June 2009, the WHO raised its pandemic alert to the highest level i.e. phase 6, indicating widespread community transmission on at least two continents.14
Pandemic influenza was the predominant influenza virus circulating in the US, Europe, northern and eastern Africa and in Australia. Activity of the virus has initially peaked and then declined in North America and in parts of western, northern and Eastern Europe, but activity continued to increase in parts of central and southeastern Europe, as well as in central and south Asia. As of 28th February 2010, worldwide more than 213 countries and overseas territories or communities have reported laboratory confirmed cases of pandemic influenza 2009, including at least 16455 deaths; a number the WHO acknowledges significantly underreported the actual number.15 Most of the deaths have been related to respiratory failure resulting from severe pneumonia and acute respiratory distress syndrome.16
In India, the number of confirmed cases till March 2010 was 29,953 and a total of 1410 deaths were reported. The rate of infection has been highest among children and young individuals of <24 years of age. To date, pandemic influenza A infections are uncommon in persons older than 65 years, possibly as a result of pre-existing immunity against antigenically similar influenza viruses that circulated prior to 1957.17 High rates of morbidity and mortality has been noted among children and young adults with underlying health problems including chronic lung disease, immunosuppressive conditions, cardiac disease, pregnancy, diabetes mellitus and obesity.18
Transmission and Shedding
Novel virus is contagious and can transmit from human to human in ways similar to other influenza viruses. The main route of transmission between humans is via inhalation of infected respiratory droplets (range in size from 0.08 µm to 0.12 µm) produced after coughing and sneezing.19 Transmission via contact with surfaces that have been contaminated with respiratory droplets or by aerosolised small-particle droplets may also occur. In addition to respiratory secretions, all other body fluids (including diarrhoeal stool) should also be considered potentially infectious.
The estimated incubation period is unknown and could range from 1 to 7 days, although the median incubation period in most cases appears to be approximately 2 days.20 Shedding of the virus begins the day prior to the onset of symptoms and can persist for 5-7 days in immunocompetent individuals. The amount of virus shed is greatest during the first 2-3 days of illness. Persons who continue to be ill, for a period of longer than 7 days after illness onset, should be considered potentially contagious until symptoms have resolved. Longer periods of shedding may occur in children (especially young infants), elderly adults, and patients with chronic illnesses and immunocompromised hosts who might be contagious for longer periods.
Clinical Manifestations
According to the CDC, in humans the symptoms of the 2009 “flu” virus are similar to those of influenza and of influenza-like illness in general. The illness with the virus has ranged from mild to severe and symptoms include fever, cough, sore throat, body aches, headache, chills and fatigue, which are usual features of influenza virus. The 2009 outbreak has shown an increase percentage of patients reporting diarrhoea and vomiting.16 As these symptoms are not specific to swine flu hence a differential diagnosis of probable swine flu requires not only symptoms but also a high likelihood of swine flu due to person’s recent history. The CDC advised physicians to consider swine influenza infection in the differential diagnosis of patients with acute febrile respiratory illness who have either been in contact with persons with confirmed swine flu or who were in states that have reported swine flu cases during the 7 days preceding their illness onset.
The overall severity with this 2009 virus has been less than what was observed during the influenza pandemic of 1918-1919. Most patients appear to have uncomplicated, typical influenza-like illness and recovered without requiring any medical treatment. About 70% of people who have been hospitalised have had one or more medical conditions, which include pregnancy, diabetes, heart disease, asthma and kidney disease.21 The most common cause of death is acute respiratory distress syndrome. The other causes of death are severe pneumonia with multifocal infiltrates (leading to sepsis), high fever (leading to neurological problems), dehydration (from excessive vomiting and diarrhoea) and electrolyte imbalance. Fatalities are more likely in young children (<5 years), elderly (>65 years) and in people with underlying conditions, which include pregnancy, asthma, lung diseases, diabetes, morbid obesity, autoimmune disorders, immunosuppressive therapies, neurological disorders and cardiovascular disease.22
Laboratory Diagnosis
All diagnostic laboratory work on clinical samples from suspected cases of virus infection should be done in a Biosafety Level 2 (BSL-2) Laboratory. Suspected cases of novel infection should have respiratory specimens (nasopharyngeal, nasal or oropharyngeal swab, bronchoalveolar lavage and endotracheal aspirate) collected to test for the 2009 flu virus. Specimens should be placed into sterile viral transport media (VTM) and to be kept at 4°C. Real time reverse transcriptase polymerase chain reaction (RT-PCR) is the recommended sensitive method for the detection of virus, as well as to differentiate between pandemic 2009 and regular seasonal flu.23 The other rapid influenza diagnostic tests (RIDTs), although provide results within 30 minutes or even less, none of these tests can distinguish between influenza A virus subtypes. Moreover, RIDTs do not provide any information about antiviral drug susceptibility. Isolation of the virus in cell cultures or embryonated eggs is another method for diagnosis of infection, but may not yield timely results for clinical management and negative viral culture does not exclude the influenza A infection.
However, most people with flu symptoms do not need a test for pandemic 2009 flu, specifically because the test results usually do not affect the recommended course of treatment. The CDC recommends testing only for people who are hospitalised with suspected flu and persons having underlying medical conditions and those with weak immune systems.24 It is also expressed that treatment should not be delayed by waiting for laboratory confirmation of test results, but rather make diagnosis based on clinical and epidemiological backgrounds and start treatment early.
Treatment
The virus isolates in the 2009 outbreak are found to be resistant to amantidine and rimantidine. The CDC recommends the use of neuraminidase inhibitors as the drugs of choice for treatment and prevention of 2009 influenza in both children and adults.25 Tamiflu (oseltamivir phosphate) and Relenza (zanamivir) are the two FDA-approved influenza antiviral drugs and a third neuraminidase inhibitor peramivir is an experimental drug approved for hospitalised patients in cases where the other available methods of treatment are ineffective or unavailable. Antiviral drugs not only make the illness milder but also prevent serious flu complications. However, the majority of people infected with the virus make a full recovery without requiring medical attention or antiviral drugs. Treatment is recommended for patients with confirmed or suspected 2009 influenza who have severe, complicated or progressive illness or who are hospitalised. People who are not from the at-risk group and have persistent or rapidly worsening symptoms should also be treated with antivirals. Therapy should be started as soon as possible, since evidence of benefit is strongest when treatment is started within 48 hours of illness onset.26 Treatment should not be delayed while awaiting the results of diagnostic testing nor should it be withheld in patients with indications for therapy who present >48 hours after the onset of symptoms. Beside antivirals, supportive care at home or in hospital, focuses on controlling fevers, relieving pain and maintaining fluid balance as well as identifying and treating any secondary infections or other medical problems.
Major Concern
The neuraminidase inhibitors oseltamivir and zanamivir provide valuable defences and have been used widely for treatment and chemoprophylaxis of 2009 pandemic influenza A.But the recent emergence of resistance to these antiviral drugs is a matter of immediate concern. Influenza A strain resistant to oseltamivir has been reported from a variety of geographical locales and poses a challenge for the management of severely compromised patients.27 The CDC warned that the indiscriminate use of antiviral medications to prevent and treat influenza could ease the way for drug resistant strains to emerge, which would make the fight against the pandemic much harder. Most of the patients recover spontaneously without any medical attention and use of antiviral medications should be reserved primarily for people hospitalised with pandemic flu and persons, with pre-existing or underlying medical conditions who are at higher risk for influenza-related complications. It has also been emphasised that early treatment once a patient has developed symptoms, rather than chemoprophylaxis, should reduce opportunities for the development of oseltamivir resistance.26 The degree to which these drugs will remain effective for the treatment of the novel strain of influenza in the coming months is still a question.
What’s next?
The only possible way to combat the situation is large scale immunization. Antiviral drugs are not a substitute for vaccinination and are used only as an adjunct to vaccines in the control of influenza. Vaccines are one of the most effective ways to protect people from contracting illness during epidemics and pandemics of influenza. The seasonal vaccines do not confer any protection against 2009 H1N1; new vaccines have been licensed and are available.28 The vaccines are available in both live-attenuated and inactivated formulations. Two types of vaccines are approved by the FDA for use in the prevention of 2009 pandemic influenza virus. These are TIV (“flu shot” of trivalent inactivated vaccine) and LAIV (nasal spray of live attenuated vaccine). The inactivated vaccine is contraindicated in patients with severe allergic reaction to eggs or any other component of the vaccine. The live attenuated vaccine is licensed for persons aged 2 through 49 years who are not pregnant, are not immunocompromised and have no underlying medical conditions. Children less than 5 years who have asthma and are taking long term aspirin therapy should also not receive live vaccines. Otherwise, both vaccines are safe and highly immunogenic and a single administration leads to robust immune response in 80% to 90% of adults aged 18-64 years and in 56% to 80% of adults aged 65 years and older with in about 10 days.29 Children younger than 10 years will require two administrations of the vaccine separated by at least 21 days. Adverse effects following vaccination are minor, just like those of seasonal influenza vaccine and are self limiting. Concerns regarding the risk of Guillain-Barre syndrome (GBS) after vaccination have been raised. Various studies have suggested that the risk of GBS is higher from influenza itself rather than from the vaccine and the other adverse effects.30 The CDC is now encouraging everyone including people of 65 years and above to get vaccinated against the 2009 strain of influenza.
The Government of India has recently approved a split virus, inactivated, non-adjuvant monovalent vaccine (Panenza by Sanofi Pasteur) to inoculate frontline health workers and those who have a high risk of getting infected.31 Groups of health care workers has also been singled out by the European council for attention and immunization.32 Infection control practices in the health care settings should be followed along with as per the guidelines.33 Patients should also be educated regarding the other preventive measures, including using tissues to cover their mouth and nose when coughing and sneezing, developing good hand washing techniques, use of alcohol based hand-rubs, avoiding contact with ill persons if possible and staying home when ill unless medical attention has been given.
The flu season seems to be dying down in 2010 but the war is yet not over. Lessons must be learnt from the previous influenza pandemics and it is still important to get vaccinated against the flu and be prepared, as activity as well as virulence might increase again in the coming season. The words of Margaret Chan (Director General, WHO) to be remembered that “the virus writes the rule and this one like all influenza viruses can change the rules, without rhyme or reason, at any time”.
‘Everyone thinks of changing the world, but no one thinks of changing himself.’ Leo Tolstoy (1828-1910)
Readers surely must have noticed by now how ‘client’, ‘service user’, ‘customer’, and other business terms have gained momentum in health care settings over the years. Newspeak has insidiously worked its way into all health policy documents. For reasons that escape me, in mental health services particularly, there seems to be an unwritten diktat that hospital personnel use any terminology other than ‘patient’ for those attending for treatment. Anyone who sets foot inside a hospital is now deemed to be a service user even though the word patient (from the Latin, patiens, for ‘one who suffers’) has not changed its meaning for centuries. Yet curiously, management Newspeak is not questioned or discussed openly by medical or nursing staff, perhaps for fear of being labelled old-fashioned, trying to cling on to relics of a bygone era. Subtle, unspoken, ‘nannying’ of health professionals in general, and a casual, perfunctory dismissal of matters medical now seem to be the order of the day.
The term ‘patient’ is now viewed sceptically by some in the management hierarchy as depicting an individual dependent on the nurse or doctor, rather than a token of respect for that person’s privacy and dignity. Non-clinical therapists are not obliged to use the term patient. What follows from that however, is the abstruse rationale that it is probably best to describe everyone as a ‘client’, ‘customer’, or ‘service user’ so as not to appear judgemental or create confusion. This apparently avoids ‘inferiority’ labelling and ensures all are ‘treated’ the same. Using the term ‘patient’, implies a rejection by doctors of multi-disciplinary team working, we are led to believe. There is a perceived, albeit unfounded notion, that the medical profession want to dominate those with mental healthproblems in particular by insisting on a biological model of illness and, by inference, pharmacological ‘chemical cosh’ treatments. At the heart of all this mumbo-jumbo lies the social model of care with its aim of ‘demedicalising’ the management of mental illness. This, ironically, seems at odds with medical practice where the emphasis has always been on a holistic approach to patient care. Yet an insistence on a social model of mental illness is as patronising to the patients that hospital managers purport to be caring for, as is the imagined ‘disempowerment’ model they want to dismantle. Some in the health management hierarchy contend that the word ‘patient’ fits poorly with today’s views of‘users’ taking an ‘active part’ in their own health care.1 Or does it? One may decide to have the cholecystectomy or the coronary bypass, when the acute cholecystitis and chest pain respectively have settled down, and select the time and date of the procedure, but I doubt whether one has any real ‘choice’ in the matter when the condition becomes critical, or that one will play an active part in the procedure itself.
The concept of empowerment, which has been around for decades, also seems to be enjoying a renaissance, being one of the current buzzwords in ‘modern’ health care. Other buzz phrases, among many, include ‘freedom of choice’, ‘equity’, ‘right to participation’, ‘increased role of the consumer.’ Empowerment, theoretically, enables new customers to stand up for themselves, demand their therapeutic rights and choose their own treatment. Fine when you are well. However, should I develop a serious illness, particularly one in which I have no great expertise, and because I cannot conceivably amass the entire body of medical knowledge before I see the doctor or nurse about my condition, I would prefer the physician/nurse to outline the treatment plan. I do not want to be called a client, customer or punter, because such derisory terms are more apt to make me feel, ironically, ‘disempowered’.
Why the change?
‘If you want to make enemies, try to change something.’ Woodrow Wilson (1856-1924)
What is it about doctors using the word ‘patient’ that health managers and non-medical therapists find so irritating and difficult to accept? Perhaps the answer lies in the doctor-patient relationship, akin to the attorney-client privilege afforded to the legal profession, so loathed by the judicial system. We are being swept along on a current of neutral, incongruous words such as ‘client’ (the most popular at present), ‘service user’ (this applies across the board), ‘consumer’ (Consuming what? I know my rights!), ‘customer’ (Do I get a warranty with this service? May I return the goods if they are unsatisfactory?) Better still, ‘ambulatory health seekers’ (the walking wounded) and ‘punters’ (a day at the races). The general trend it seems is for doctors to name one attending an appointment as ‘patient,’ midwives opt for ‘people’, social workers tend to speak of the ‘service user’, psychologists and occupational therapists prefer ‘client’, and psychoanalysts sometimes use the rather cumbersome description ‘analysand’. What is usually forgotten is that the person waiting in the analyst’s reception is no different from the humble stomach-ache sufferer.2
To most people ‘service user’ infers someone who uses a train or bus, or brings their car to a garage or petrol station. The term ‘user’ often denotes one who exploits another; it is also synonymous with ‘junkie’ and a myriad of other derogatory terms for those dependent on illegal drugs; ‘client’ has ambiguous overtones, and ‘people’ refers generally to the population or race, not to individuals receiving treatment. For general purposes a ‘client’ could be defined as a person who seeks the services of a solicitor, architect, hairdresser or harlot. There is also talk of ‘health clients’. Someone who goes to the gym perhaps! A customer is a person who purchases goods or services from another; it does not specifically imply an individual patient buying treatment from a clinician. Try to imagine the scenario of being told in your outpatient setting that a client with obsessive compulsive disorder, or a service user who is psychotic, or a customer with schizophrenia, is waiting to be seen. Although it is defies belief, this is how non-medical therapists portray patients. Would a medical doctor describe a person with haemorrhagic pancreatitis as a customer? Picture a physician and psychiatrist talking about the same person as a patient and customer respectively. Patients make appointments with their general practitioners. In psychiatry the terms are an incongruous depiction of the actual clinic setting in that most patients are not consumers or customers in the market sense; indeed many have little wish to buy mental health services; some go to extraordinary lengths to avoid them.3 Those who are regarded as in greatest need vehemently avoid and reject mental health services and have to be coerced into becoming ‘customers’ through the process of the mental health act.
What do our medical and surgical colleagues make of all this? Despite Newspeak insidiously weaving its way through other specialties, it does not seem to have permeated medicine or surgery to the same extent. Is psychiatry therefore alienating itself even further from other fields in medicine by aligning itself with this fluent psychobabble? Do cardiologists refer to patients with myocardial infarctions as customers? Does a patient with a pulmonary embolism or sarcoidosis feel more empowered when described as a punter? Changing the name does not address the illness or the factors in its causation. Perhaps one could be forgiven for using terms other than ‘patient’ for someone who wants plastic surgery to enhance their facial appearance, or a ‘tummy tuck’ to rid themselves of fatty tissue induced by overindulgence, or in more deserving cases, successive pregnancies. Readers will have no difficulty adding to the list. Such people are not ill. However, when describing a person with multiple myeloma, acute pulmonary oedema, intravascular disseminated coagulopathy or diabetic ketotic coma, I’m not so sure ‘consumer’ or ‘ambulatory health client,’ fits the profile. After all, a customer usually wants to ‘buy something’ of his/her own choosing. Now this may apply to ‘gastric banding’ or silicone implants, but there is not much choice on offer when one is in a hypoglycaemic coma or bedridden with multiple sclerosis.
Despite the above, when people were actually asked how they would prefer to be described by a psychiatrist or by a general practitioner,67% and 75% preferred ‘patient’ respectively.4 Another survey revealed a slightly higher preference (77%) for ‘patient’.5 One might argue that such results depend on the setting where the surveys were carried out and by whom. However, logic dictates that if I am in the supermarket waiting to be served, I would assume I am a customer; while attending the general practitioner’s surgery for some ailment, I would imagine I am there as a patient. Such surveys are conveniently ignored by service providers. So what does it matter? It matters because the lack of direct contact between managers and patients puts the former at a great disadvantage and leads one to question their competence and credibility when accounting for patient preferences. Perhaps managers should ‘shadow’ physicians and surgeons to fully understand why the people they treat are called patients. Psychiatry is not a good example of normal medical practice since so many of its adherents possess the illusory fantasy of being ‘experts in living’, and not physicians whose aim is to diagnose and treat.
Be patient
‘The art of medicine consists in amusing the patient while nature cures the disease.’ Voltaire (1694-1778)
It is noticeable that ‘patient’ remains the preferred usage by the media, press, and cabinet ministers, and of course, by medical and surgical teams. The implicit meaning of the word ‘patient’ is that someone is being cared for, and the media at least seem to respect this. Ironically, in the field of mental health, clinicians will often write letters to other professionals referring to an ill person as a ‘patient’ in one paragraph, and a ‘client’ in the next! Doubt and equivocation reign. It is as if the stigma of mental illness will evaporate if we gradually stop talking about sufferers as patients, and ‘empower’ them by describing them as ‘customers.’ There is ambiguity in the terminology itself. The term service user is the most disliked term among those who consult mental health professionals.6 The terms are also used interchangeably, with ‘customers’ and ‘service users’ described in the same breath. What do we call a drug-user? - a service user drug-user or a drug-user service user, a customer who uses drugs, or a drug-using customer? How does one accurately describe an individual using alcohol and illegal drugs? Is an infant suffering from respiratory distress syndrome or a child moribund with bacterial meningitis an active participant in his/her health care? In theory, they are service users. What about young people among whom substance misuse is prevalent?7 Do we label and stigmatise them as drug clients or drug customers? Will the outpatient and inpatient departments be redesignated as out-service or in-service user clinics? Oxymoronic terms such as ‘health clients’ do not convey any meaning when applied to hospital patients. Doubtless, critics with their customary predictability will lamely and with gloating schadenfreude, accuse the medical profession of bemoaning their loss of hegemony in health care matters, but their arguments are specious, stem from a lingering resentment of the medical profession, and amount to little.
In other areas of health some argue that making choices about lifestyle, and seeking advice on matters such as fertility, liposuction, gastric banding, or cosmeticsurgery, do not require one to be called a patient, and rightly so. Such information is freely available at clinics and on the Internet, and therefore does not require the advice of a doctor per se, until the actual procedure is imminent. However, it would be inconceivable for a patient undergoing say, a laparoscopic bypass or sleeve mastectomy for obesity, not to heed the views of the surgeon performing the procedure itself, the success rate, and complications. Whether to have the operation is a different matter. Similarly, individuals who want to engage in psychological therapies such as cognitive or psychoanalytic, or who would rather indulge in an expensive course of ‘emotional healing’, can choose for themselves. Neither does one need to see a nurse practitioner or general practitioner for a mild upper respiratory tract infection. Such people are not suffering from any serious medical illness (an enduring feeling of being physically or mentally unwell) in the true sense of the word.
When all is said and done, most people are unschooled in etymology, and condemning words because of their remote origins is pointless. Words change in meaning over time. Often they take on a new meaning, all too obvious in teenage slang. The word ‘wicked’ used to mean sinful, now it refers to something ‘cool’ (another word that has changed its meaning). Besides, if ‘patient’ really is that offensive, it seems odd that it has retained unchallenged supremacy in the United States,the centre of consumerist medicine, where the patient is quite definitely a partner.8
Physicians do not want to return to the days of paternalistic and condescending medicine, where deferential, passive patients were at the mercy of the stereotypical omniscient, omnipotent doctor or nurse matron. Likewise, patients do not want to be treated like products in order to achieve targets for the government health police. Patients nowadays are generally more confident and better informed about their conditions, in other words, already empowered, than in days gone by, particularly with the advent of the Internet (alas, here misinformation also abounds) and this is welcome. Therefore, if you are relatively well you can choose a treatment to suit your lifestyle. Unfortunately, not many patients suffering from chronic illnesses, for example, schizophrenia in some cases, or a degenerative condition such as motor neurone disease, feel empowered. I might feel empowered when I can decide to have one therapy or another, say, cognitive as opposed to solution-focussed therapy. I somehow doubt whether I would feel equal in status to, or more empowered than, the surgeon who is performing a splenectomy on me for traumatic splenic rupture.
The thrust of all this is that nothing is thought through; everything consists of ‘sound bites’ and ‘catchphrases’, and the sound bites become increasingly absurd the more one scrutinises the terminology. The medical and nursing profession should only be tending to people who are ill or recovering from illness. Of course other staff are directly or indirectly involved in patient care and follow-up. Physiotherapy is a good example. Nonetheless the title patient remains the same. Therefore let us be clear about the definition: those who suffer from an illness are patients; those who are not ill can be called service users, or whatever term takes your fancy.
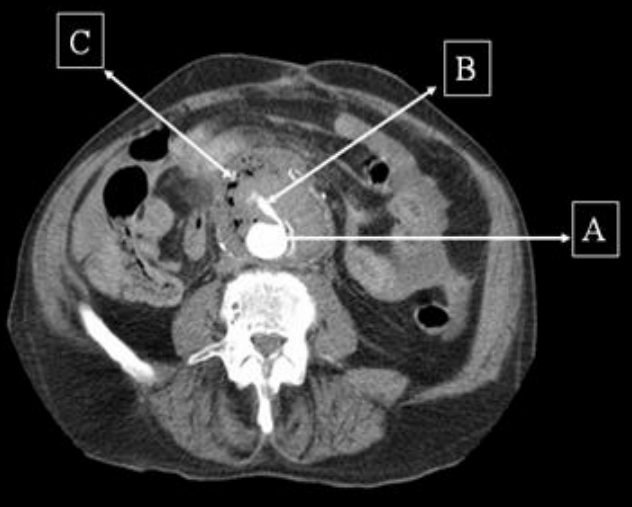
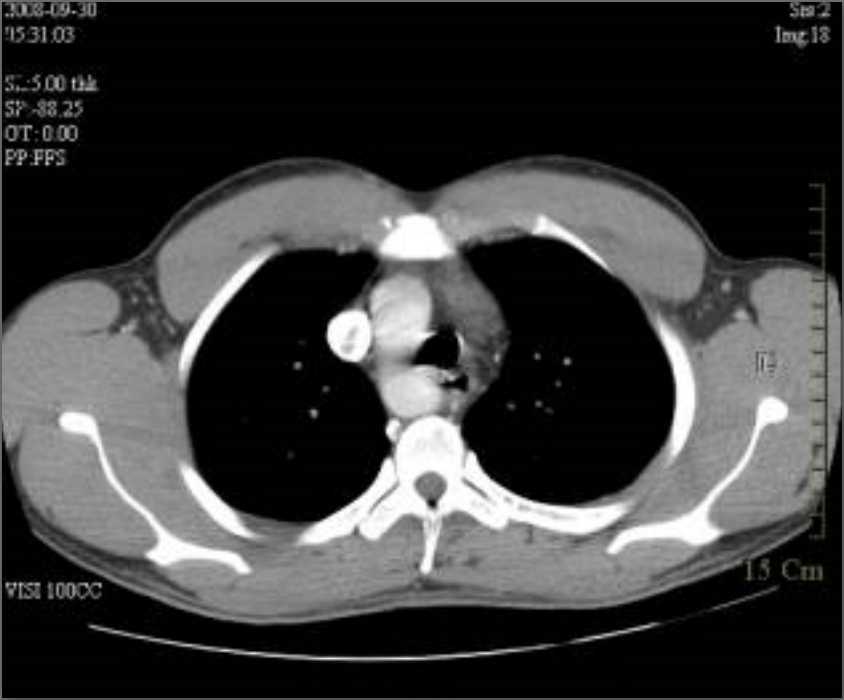
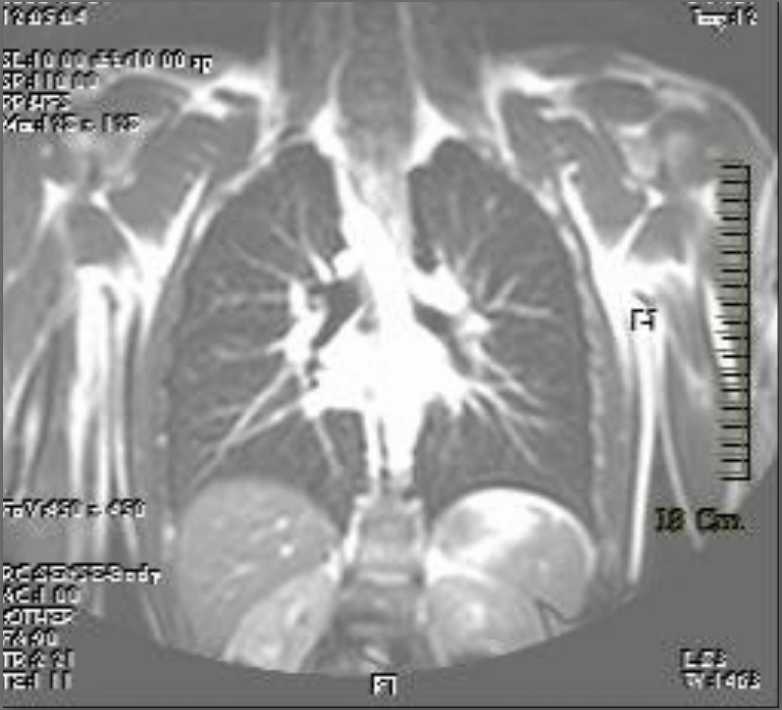
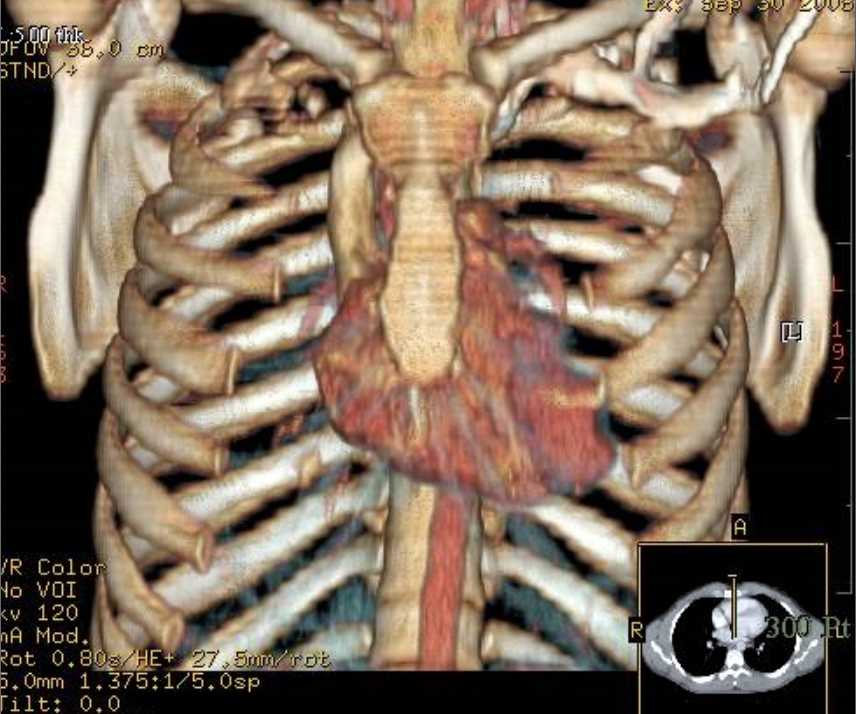
A 87-year old man was referred to hospital with a five day history of lethargy and increased urinary frequency. He denied symptoms of gastrointestinal bleeding or abdominal pain. His past medical history included diabetes mellitus, chronic kidney disease, peripheral vascular disease and surgery for repair of ruptured aortic aneurysm 6 weeks ago. Systemic examination, including per rectal examination, was normal. Haemoglobin was 83g/L and C-reactive protein was 148 (Normal <5). Twelve hours after admission he developed pyrexia (37.8 degree) accompanied with tachycardia (103 beats per minute) and hypotension (BP 87/43). Soon afterwards, he had a small amount (<50 mls) of fresh haemetemesis. He also complained of lower back pain and clinical examination revealed tenderness in the left iliac fossa. He was cross-matched for blood and initiated on intra-venous fluids. As his Rockall score was six an urgent oesophago-gastro-duodenoscopy (OGD) was planned. Over the next few hours he complained of increasing central abdominal pain and had several episodes of melaena. In view of the history of recent aortic surgery and current GI bleed the possibility of aorto-enteric fistula (AEF) was considered. An urgent contrast CT scan of the abdomen (Figure 1) was therefore arranged prior to OGD.
Figure 1: Contrast CT scan demonstrating the aorta (A) with extravasation of contrast (B) and a large collection (C) around it with trapped air suggestive of infection.
Contrast computed tomogram (CT) scan of the abdomen revealed an inflammatory soft tissue mass anterior to the infra-renal aortic graft with pockets of gas and leakage of contrast into it. These findings were suggestive of an AEF. The patient was informed of the diagnosis of AEF and the need for emergency surgical repair to which he consented. During the operation the vascular surgeons found that the duodenum was adherent to the aortic graft with evidence of fistulisation and infection, thus confirming the diagnosis. Although operative repair appeared to be successful, the patient continued to bleed on the table due to disseminated intravascular coagulation and died twenty fours after admission.
Discussion
AEF is defined as a communication between the aorta and the GI tract.1 The diagnosis of AEF should be considered in every patient with a GI bleed and a past history of aortic surgery.2 Our case patient had had emergency repair of a ruptured aortic aneurysm with a prosthetic graft 6 weeks prior to his current admission.
AEFs are a rare cause of gastro-intestinal (GI) hemorrhage. AEFs can be primary or secondary. Primary AEF (PAEF) is a communication between the native aorta and the GI tract.1 The incidence of PAEF ranges from 0.04 to 0.07%.3 PAEFs commonly arise from an abdominal aortic aneurysm of which 85% are atherosclerotic.1
Secondary AEFs (SAEF) are an uncommon complication of abdominal aortic reconstruction.4The incidence of SAEF ranges from 0.6% - 4%.5 Generally two types of SAEFs have been described. Type 1, termed as true AEF develops between the proximal aortic suture and the bowel wall. These usually present with massive upper GI hemorrhage.4 Type 2, or the paraprosthetic–enteric fistula does not develop a communication between the bowel and the graft and accounts for 15% to 20% of SAEFs.4 In this type of fistula, bleeding occurs from the edges of the eroded bowel by mechanical pulsations of the aortic graft. Sepsis is more frequently associated with this type of AEF (75% of cases).4 The mean time interval between surgery and presentation with SAEF is about 32 months6 but the time interval can vary from 2 days to 23 years.7 AEFs can involve any segment of the GI tract but, 75% involve the third part of the duodenum and the affected part is generally proximal to the aortic graft.8
The pathogenesis of AEF is not fully understood but two theories exist. One theory suggests repeated mechanical trauma between the pulsating aorta and duodenum causes fistula formation and the other suggests low-grade infection as the primary event with abscess formation and subsequent erosion through the bowel wall.9 The latter theory is felt to be most likely. The majority of grafts show signs of infection at the time of bleeding and up to 85% of cases have blood cultures positive for enteric organisms.10
The main symptom of AEF is GI bleeding. Secondary AEFs have been traditionally said to present with a symptom triad (as in our patient) of abdominal pain, GI bleeding and sepsis; however, only 30% of patients present in this manner.11 Patients often have a “herald bleed” which is defined as a brisk bleed associated with hypotension and hematemesis that stops spontaneously followed by massive gastro-intestinal haemorrhage in 20% – 100% of patients.8 Sometimes the GI bleeding can be intermittent.
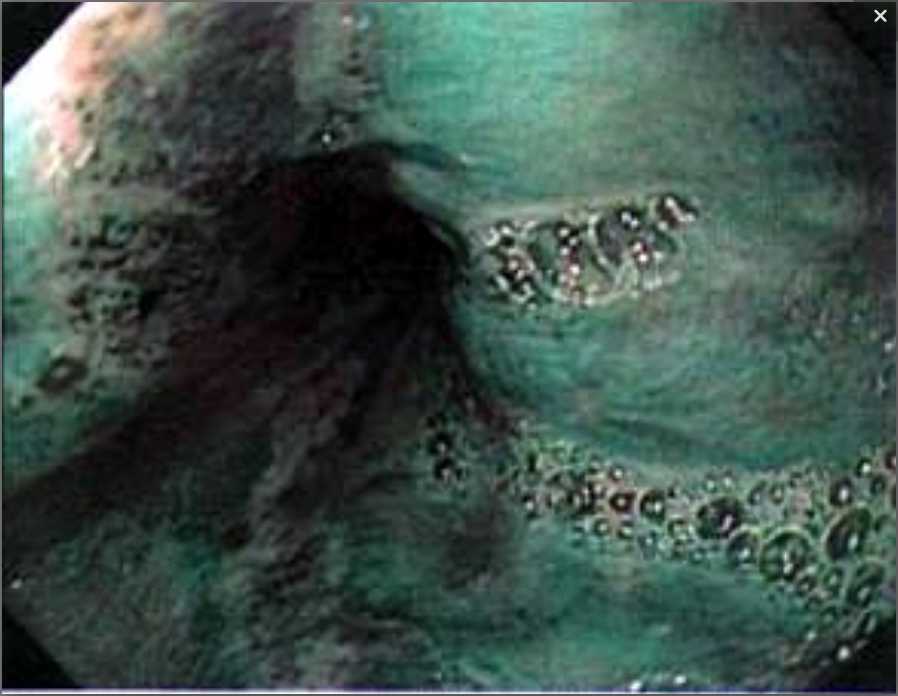
The commonest investigations for diagnosis of AEFs are OGD, conventional contrast CT scan and angiography.12 OGD is often the initial investigation, as in any upper GI bleed mainly because of lack of clinical suspicion of the diagnosis. The endoscopic findings vary from those of a graft protruding through the bowel wall to fresh bleeding in distal duodenum to that of an adherent clot or extrinsic compression by a pulsating mass with a suture line protruding into the duodenum.13 Less than 40% of patients have signs of active bleeding at OGD.8 Conventional CT with contrast is widely available and most commonly performed to diagnose AEFs. Perigraft extravasation of contrast is a pathognomic sign of AEF and this may be associated with signs of graft infection i.e perigraft fluid and soft tissue thickening along with gas.12 Multi-detector CT and MRI are more sensitive diagnostic imaging tools with MRI now being used mainly in patients with renal failure to avoid the use of contrast.12
PAEFs can be treated with endovascular stent placement in selected cases especially in those who cannot tolerate emergency surgery.12 The treatment of choice in SAEFs is graft resection and establishment of an extra-anastomotic circulation with repair of the duodenal wall although overall survival rates vary from 30% to 70%.13
Conclusion
SAEFs are a catastrophic complication of aortic surgery. AEFs are relatively rare and need a high index of suspicion in the appropriate clinical situation in order to diagnose this condition. Left untreated they are universally fatal. Surgical repair carries a very high mortality.
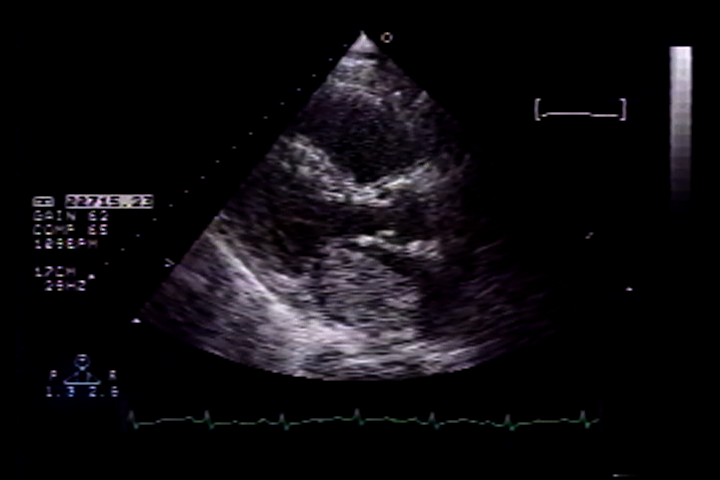
A 55 year old white male with a history of hypertension, hyperlipidemia, smoking and transient ischaemic attacks was admitted to the hospital with worsening dyspneoa on exertion over a period of 6 weeks. He also reported significant weight loss, loss of appetite and fatigue over several weeks. Physical examination revealed tachycardia, and moderate respiratory distress with prominent jugular venous distention. Cardiac auscultation revealed normal S1 and loud P2. Also heard were an early diastolic heart sound ( tumour plop) and a mid-diastolic murmur at the apex. An ECG revealed evidence of left ventricular hypertrophy with repolarization abnormalities. A transthoracic echocardiogram (Figures 1 and 2) revealed a large, pedunculated, mobile left atrial mass measuring 3x4 cm, impinging on the mitral orifice with a mean gradient across the mitral valve of 15 mm Hg. Left ventricular systolic function was normal.
Figure 1: Parasternal long axis echocardiograph of the left atrial myxoma prolapsing into the mitral valve during diastole.
A diagnosis of probable left atrial myxoma was made. The patient had four episodes of syncope within 24 hrs, the first at 3: 53 am after returning from the bathroom, subsequently leading to cardiac arrest at 14:20 pm.
Figure 2: parasternal long axis echocardiograph showing the large left atrial myxoma during systole.
He was intubated and initiated on vasopressors. An emergent Left heart catheterization was performed prior to a referral for surgical excision, which revealed triple vessel coronary artery disease. During cardiac catheterization the patient became more hypotensive requiring an intra-aortic balloon pump. While arrangements were made for a referral for surgery, the patient’s clinical condition deteriorated rapidly and he went into pulseless electrical activity at 18:54 pm and could not be resuscitated. The patient’s death was presumably due to persistent intracardiac obstruction. On autopsy, the left atrial mass was identified as a haemorrhagic left atrial myxoma, 5x4x3.5cm in size attached by a stalk to an inter-atrial septum. Multiple organizsing thrombi were present in the 1tumour. Histology showed abundant ground substance with stellate myxoma cells and haemosiderin-laden macrophages (Figures 3 and 4). The cause of death was attributed to valvular “ball-valve” obstruction.
Figure 3: Histopathology of left atrial myxoma showing spindle shaped myxoma cells (white arrow) in a myxoid matrix (black arrow) and blood vessels (top arrow) (H & E 40X)
Figure 4: Histopathology of left atrial myxoma showing vascular spaces filled with relatively fresh blood and evidence of old bleeding (hemosiderin) suggesting repeated episodes of hemorrhage within the myxoma (H & E 4X)
Case 2
A 57 year old African American female presented with recurrent syncopal episodes and dyspnea on exertion, orthopnea, leg swelling, abdominal distention, loss of appetite and fatigue for the preceding nine months. Physical examination revealed jugular venous distention, a displaced apical cardiac impulse, a parasternal heave, and a loud S2. Also detected were a pan-systolic murmur at the lower left sternal border, an early diastolic heart sound with a mid diastolic murmur at the apex, bibasilar crackles, ascites, and oedema up to the thighs.
Significant laboratory values were a total bilirubin of 1.6 mg/dl, and B- Type Natriuretic Peptide of 1323 pg/ml. A chest x-ray revealed an enlarged cardiac silhouette, right lung atelectasis and effusion. An ECG revealed left atrial and right ventricular enlargement.
The patient was admitted with the diagnosis of new onset congestive heart failure and was treated with intravenous lasix, and fosinopril. A 2-D Echocardiogram revealed a large mass suggestive of myxoma in the left atrium measuring 4.5 x 7.5 cm, occupying the entire left atrium protruding through the mitral valve into the left ventricle (Figure 5) .
Figure 5: Apical four chamber echocardiograph of the left atrial myxoma prolapsing into the mitral valve during diastole.
This mass was obstructing flow with a mean trans mitral gradient of 17 mm Hg, with a reduced stroke volume and severe pulmonary hypertension with an estimated Right Ventricular systolic pressure of 120 mm hg. A presumptive diagnosis of left atrial myxoma was made and the patient was scheduled for its surgical removal the following morning. The patient was transferred to the intensive care unit for closer monitoring; and fosinopril and lasix were discontinued. At about 22:30 hours that night patient was noted to be hypotensive with systolic blood pressure of around 80mm Hg. The patient was treated with normal saline and concentrated albumin. She then developed acute respiratory distress at 23:00 hours requiring intubation and ventilator support. Intravenous dobutamine, dopamine and later norepinephrine were added for continued hypotension. The patient went into pulseless electrical activity, she was successfully coded with a return of her pulse but continued to be hypotensive. Cardiothoracic surgery decided not to take the patient for emergency surgery due to her unstable haemodynamic condition. The patient’s family was notified of the poor prognosis and the decision was made not to resuscitate her if her condition deteriorated further. The patient ultimately became bradycardic and went into asystole at 5: 30 am. An autopsy was not performed. The cause of death was attributed to large left atrial myxoma causing valvular obstruction and cardiovascular collapse.
Discussion
These two cases illustrate an uncommon, malignant course of a left atrial myxoma with rapid progression of symptoms which proved fatal. The most common primary tumour of the heart is myxoma accounting for 40-50% of primary cardiac tumours(2,3) .Nearly 90% of myxomas occur in the left atrium(3) .In over 50% of patients, left atrial myxoma causes symptoms of mitral stenosis or obstruction. Systemic embolic phenomena are known to occur in 30-40% of patients(3) .
Table 1. Summary of 17 published cases of sudden cardiac death associated with cardiac myxoma in adults (1950-2008)
Author/Reference
Year
No
Age
Gender
Symptoms
Interval Between Symptoms To Scd
Size Of Myxoma In Cm
Autopsy
Vassiliadis (8)
1997
1
17
M
Dizziness
3 months
6
yes
McAllister (10)
1978
5
40 to60
NA
NA
NA
5 to 6
yes
Cina (2)
1996
6
Below 40
NA
Embolic, syncope
16.6 months
5.7
yes
Puff (9)
1986
1
41
M
Syncope,
months
1.5
yes
Puff (9)
1986
1
19
F
Syncope
6 months
3
yes
Maruyama (7)
1999
1
20
M
Dizziness
1 day
8
None, Patient survived SCD; Myxoma resected
Turkman (6)
2007
1
73
M
DOE
months
8
yes
Ito (13)
1987
1
28
M
Syncope
7 days
NA
yes
NA: not available
Constitutional symptoms reported in approximately 20% of patients include myalgia, muscle weakness, athralgia, fever, fatigue, and weight loss. Around 20% of cardiac myxomas are asymptomatic (3) .Severe dizziness/syncope is experienced by approximately 20% of patients due to obstruction of the mitral valve. (4) Of all the symptoms associated with cardiac myxomas, syncope is one of the most ominous prognostic indicators.
Although sudden death is known to occur in patients with primary cardiac tumour it is rare and is estimated to constitute 0.01 to 0.005% of all sudden deaths (1). Association between sudden death and cardiac myxoma has been reported as early as 1953 by Madonia et al (5). A review of the literature on this subject between 1950 to2008 revealed 17 cases of sudden death attributed to cardiac myxoma in adults (1, 6, 7, 8, 9, 10, 13)(Table 1) .
In all patients with unexpected death syncope was a predominant presenting symptom and their age ranged from seventeen to seventy three. The majority of patients with sudden death were men even though the tumour is more common in women. The size of the tumour did not influence clinical presentation and in some reports of sudden cardiac death tumour was as small as 1.5 cm and without previous symptoms (3). Sudden death in myxoma is attributed to either severe acute disturbance in cardiac haemodynamics from cardiac obstruction (ball-valve syndrome) or to coronary embolization from the tumour. The latter is probably responsible for sudden death in patients with very small tumours. In the study of Alverez Sabin et al (11) the initial neurological manifestation was Transient Ischemic Attack (TIA), but in none of the patients’ was a diagnosis of myxoma made because of the initial neurological symptom. Even though cardiac myxomas are a rare cause of TIA and syncope, it is important to consider cardiac myxoma in the differential diagnosis of any patient with a TIA or syncope (11). The patients presented here had a TIA and recurrent syncope placing them at high risk for sudden death.
The timing of surgical excision of myxoma is not clear and it is not unusual for patients to die or experience a major complication while awaiting surgery (2, 12). Intraaortic balloon pump (IABP) use has been described in one case of left atrial myxoma and life-threatening cardiogenic shock with favorable outcome(14) .As illustrated by the cases presented here it is essential that surgery be performed urgently once it has been identified that a patient has a myxoma that is large enough to cause complete intracardiac obstruction.
Female sexual dysfunction (FSD) is a serious morbidity which could occur postnatally. It may lead to a variety of physical, psychological, and social adverse effects on the patient. Moreover, the consequent cycle of fear might compound the initial sexual disorder and makes it more difficult to treat. Therefore, early diagnosis and management of the problem become essential to avoid later sequalae on reproductive and sexual life. However, early diagnosis may be challenged by many factors. For example, many patients will be preoccupied by the newborn or embarrassed of talking about sexual matters after delivery, which makes it very important for the midwifery, medical, or other staff to raise the issue during the postnatal care sessions. The staff, on the other hand, might feel uncomfortable to discuss the sexual function with the client, or even may lack the knowledge and skills required for sexual health counselling. In addition to the client-service gap, there are gaps between different sexual service providers.
There are many types of postnatal sexual disorders. These types can differ widely in clinical features and management. Additionally, management of postpartum female sexual dysfunction (PPFSD) can vary with clinician’s experience. There are very few randomised clinical trials on treatment for PPFSD, which partly explains the service-service gap in PPFSD management.
In the last three decades there has been an increase in caesarean section rate in the developed world due to many maternal and fetal indications, especially with the significant improvement in surgical and postoperative care. Recently, more attention has been paid to the positive role the caesarean section may play in protecting the female pelvic floor from birth trauma. Perineal birth trauma has been accused by many authors of adversely affecting the female sexual well being. 1 On the other hand there is a growing opinion that the quality of postnatal sexual health is unrelated to mode of delivery. 2 The previous two contradictory statements from literature illustrate the real size of the dilemma when we try to counsel a woman requesting a caesarean section as she is worried about sexual dysfunction after vaginal delivery. This problem might become more difficult to solve if the woman already suffers from a sexual disorder (for example: dyspareunia) in the antenatal or preconception period.
Female sexual dysfunction is impaired or inadequate ability of a woman to engage in or enjoy satisfactory sexual intercourse and orgasm. There are certain natural events in a woman’s life when she is at increased risk of developing sexual dysfunction, such as the use of contraception pills, menstruation, postpartum and lactation status, perimenopause, and postmenopause. This could be related to fluctuations in gonadal hormone secretion, making women more vulnerable to sexual symptoms.3 Postpartum female sexual dysfunction (PPFSD) is a common health problem with different incidence reported in literature. Xu et al reported an incidence of 70.6% of PPSFD in the first 3 months after delivery falling off to 55.6% during the 4th-6th months, and reduced to 34.2% at the 6th month, but not reaching pre-pregnancy levels of 7.17%. 2
For the purpose of this piece of writing, the classification of sexual dysfunction put forth by the American Psychiatric Association APA (1994) in the Diagnostic and Statistical Manual, 4th Edition (DSM-IV) is used to help understand the differing presentations of PPFSD. 4 The main postpartum female sexual dysfunction categories are: sexual desire dysfunction (Hypoactive Sexual Desire Disorder), sexual pain disorders (which includes dyspareunia, vaginismus. and vulvodynia), sexual arousal disorder, and female orgasmic disorder.
To help in understanding this classification better, it is important to refer to the early research done in this field by Masters and Johnson in 1966. One of the most interesting findings of the latter has been the four stage model of sexual response, which they described as the human sexual response cycle.5 They divided the human sexual response cycle into four stages: Excitement phase (initial arousal), Plateau phase (at full arousal, but not yet at orgasm), Orgasm, and Resolution phase (after orgasm). 5
Although it is normal to have hypoactive sexual desire (loss of libido) in the first 6-7 weeks after giving birth, this becomes abnormal when the desire for sexual activity is persistently reduced or absent causing distress in the relationship. Sexual desire disorder after delivery may be due to the mother being preoccupied with the neonate or postpartum complications (e.g. infection, pain, and bleeding). It can often be associated with sexual pain disorder as well.
Dyspareunia is the most common type of PPFSD. Solana-Arellano et al (2008) reported an incidence of 41.3% for dyspareunia in the 60-180 days period after giving birth.1 Postpartum dyspareunia may be due to medical (physical) problems such as a mal-healed perineal or vaginal tear, postpartum infection, cystitis, arthritis, or haemorrhoids, which may get worse after delivery. Moreover, dyspareunia might be caused by psychosocial factors like problems in relationship with the partner, work stress, financial crisis, depression, and anxiety. Dyspareunia, in many cases, can occur as a result of a combination of medical and psychosocial factors. Although, vaginismus is recognised as a different identity, it is usually associated with dyspareunia when it happens in the Puerperium. Vaginismus is the involuntary spasm of the pubococcygeal muscles causing difficult and painful penetration. Sexual desire disorders, Isolated postpartum sexual arousal and orgasmic disorder are rarely seen in postnatal clinics as when they occur they tend to be part of other PPFSDs.
Methods:
Risk Factors for PPFSD:To assess the risk factors for PPFSD a literature review was performed using the National Health Library database including all resources ( AMED, BNI, CINAHL, EMBASE, HEALTH BUSINESS ELITE, HMIC, MEDLINE, and PsycINFO). The MESH word/s used was (postpartum sexual dysfunction OR postpartum dyspareunia OR dyspareunia after delivery OR sexual dysfunction after delivery OR sexual problems after delivery). Other different MESH words (using the word sexuality and/or puerperium) were used as well to expand the search possibilities. Only studies discussing the risk factors of PPFSD after vaginal birth were included. Perineal pain as a complication after episiotomy or tears was differentiated from dyspareunia, and studies on perineal pain after delivery were excluded from the review if they did not discuss the effect of the pain on sexual activity. Effect of Mode of Delivery:Searching the Cochrane library databases has shown no review related to the subject. However, Hicks et al (2004) have conducted a systematic review of literature focused on mode of delivery and the most commonly reported sexual health outcomes, which included dyspareunia, resumption of intercourse, and self-reported perception of sexual health/sexual problems.6 In their systematic review they suggested an association between assisted vaginal delivery and some degree of sexual dysfunction but they reported that associations between Caesarean delivery and sexual dysfunction were inconsistent and continued research was necessary to identify modifiable risk factors for sexual problems related to method of delivery.6 Hicks et al have searched PubMed, CINAHL, and Cochrane databases from January 1990 to September 2003, 6 so we have tried to continue the review by looking into the literature database after that date. To assess the effect of mode of delivery on PPFSD (Caesarean section vs. vaginal birth), a literature review was performed using the National Health Library database including all resource ( AMED, BNI, CINAHL, EMBASE, HEALTH BUSINESS ELITE, HMIC, MEDLINE, and PsycINFO) from October 2003 to January 2010. New MESH words were used, related to comparison between different modes of delivery (Caesarean section, vaginal birth, modes of delivery, sexual dysfunction, sexual disorder, dyspareunia). Additional studies from the reference lists were obtained. Only studies directly compared between caesarean section and vaginal birth in term of assessing the PPFSD were included. Results: Risk Factors for PPFSD:Nineteen studies and one systematic review were retrieved in the period from 01/01/1984 to 01/01/2010. The Cochrane library database review did not have related articles. It is worth mentioning, however, that there was a Cochrane review on postpartum perineal short term pain, not related to sexual activity. Therefore, it was excluded from this review. The systematic review included in this list of literature studies is the Langer and Minetti review on the complications of episiotomy.7 Having systematically reviewed four hundred seventy two articles on the Medline database, they concluded that episiotomy, whether medial or mediolateral, appeared to be the cause of more dyspareunia in comparison to spontaneous perinea tears.7 However, there was no significant difference in the incidence of dyspareunia beyond the three month period after delivery.7 After the latter review, Solana-Arellano (2008) have showed that complications of episiotomy are an important risk factor for postpartum dyspareunia. 1 They have found that infection, dehiscence, and constricted introitus complicated an episiotomy can cause long-term postpartum dyspareunia.1 Moreover, Ejegard et al have investigated the long term quality of women's sex life (12-18 months after first episiotomy-assisted delivery).8 They have reported an adverse effect of episiotomy on women's sex life during the second year post partum .8 Effect of Mode of Delivery:Only eight studies fulfilled the criteria. Full papers were retrieved. There was one randomised controlled trial, one prospective cohort study, one cross-sectional study, and the other 5 were performed retrospectively (4 questionnaire surveys, and 1 interview survey). The total pool sample of patients studied included 3476 cases (1185 Caesarean sections vs. 2291 vaginal deliveries). Four studies aimed to compare PPFSD aspects within other variants, such as pelvic floor morbidity, urinary incontinence, and faecal or flatus incontinence.9, 10, 11, 12 the other four studies purely compared PPFSD variants such as dyspareunia with no other pelvic floor morbidity variants.13, 14, 15, 16 There has been an agreement between the studies on the less sexual problems after caesarean section compared to vaginal delivery in the short term after delivery (i.e. up to 3 months postpartum). However, in long term (i.e. more than 12 months postpartum), the outcome was controversial. A meta-analysis was conducted to compare and summarise the long term PPFSD results ( graph 1) . Graph 1: Forest plot of comparison between studies. Studies to left of the midline were in favour of less long term PPFSD symptoms with caesarean section compared to vaginal delivery. Discussion: From the previous results, birth tract trauma is a risk factor which may lead to PPFSD. Therefore it is a logic presumption to think that avoiding pelvic floor injury by performing a caesarean section especially as an elective mode of delivery may alleviate PPFSD. This presumption, if true, will have very significant clinical and financial implications in practice especially with a pre-existing problem of increasing caesarean section rate in many parts of the developed world. So what research evidence in the literature is available to support or overrule this presumption?. The answer to this question becomes more challenging if we know that the British National Sentinel Caesarean Section Audit showed that 50 percent of consultant obstetricians agreed with the statement ‘‘elective caesarean section will least affect the mother’s future sexual function’’ .17 From the previous meta-analysis, there is little evidence to support that a caesarean section may alleviate long term PPFSD compared to vaginal delivery (p=0,02). But, if we examine the studies’ subgroups and primary/secondary results in more details, this evidence sounds insufficient. Griffiths et al (2006) in their questionnaire survey of a 208 women from the Cardiff Birth Survey Database have showed a significant increase in the prevalence of dyspareunia two years after vaginal birth compared to caesarean section. 9 However, their comparison was between vaginal birth and elective caesarean section as they excluded emergency cases.9 Moreover; they found similar increase in the prevalence of urinary incontinence, incontinence of flatus and subjective depression in the vaginal birth group, which lead us to think whether the dyspareunia was related to these factors and not related to vaginal birth itself. In their paper they did not mention if vaginal birth with no tears or complications was associated with a higher incidence of dyspareunia. In contrast, Klein et al (2005) concluded that women who had intact perineum after vaginal birth had less dyspareunia than those underwent caesarean section.12 However, the incidence of dyspareunia in the latter study was higher among women who had an episiotomy with or without forceps.12 Similar findings were revealed by Buhling et al (2006) and Safarinejad et al (2009), who showed that persistence of dyspareunia longer than 6 months after delivery was the highest after operative vaginal delivery.15, 16 Buhling et al concluded that the incidence of persistent dyspareunia was similar in the caesarean section and the spontaneous vaginal birth without injury groups (approximately 3.5%), whereas, Safarinejad et al (2009) have shown that women after elective Caesarean section had the highest Female Sexual Function Index (FSFI) compared to other groups of delivery including the normal vaginal delivery without injury or episiotomy.15, 16 Although Safarinejad et al (2009) study was robust in many aspects, such as using FSFI and studying the sexual function score for both the women and their partners, I think the main weakness in the study that they included only primiparous women. 16 Therefore, we cannot generalise their findings on women in their second or more pregnancies. Moreover, as a previous caesarean section will increase the operative risk of the successive caesarean sections or will add more risk to the trial of labour if this is opted for in the future, we can expect a higher increased of sexual disorders in the following pregnancies. From previous discussion we found insufficient evidence to advocate a decision of performing a caesarean section on basis of alleviating PPFSD. This evidence is outweighed by the higher risk of caesarean section including bleeding, infection, anaesthesia risk, deep vein thrombosis, pulmonary embolism, impairment of future fertility, risk of scar dehiscence in next labour, injury to bladder and bowels and risk of fetal laceration. Author’s Conclusion: Risk Factors for PPFSD:In this review, there is good evidence to suggest that episiotomy is an important risk factor for short term PPFSD. However, there is little evidence to support a possible long term effect especially if other complications to episiotomy occurred later. Breastfeeding, and the use of progestogen-only pill as contraceptive are other risk factors identified by other studies .18, 19, 20 This may be caused by the low oestrogen level and the consequent dry vagina. 18, 19, 20 Other risk factors for PPFSD include the lack of postpartum sexual health counselling and treatment. 2, 21 Effect of Mode of Delivery:Postpartum female sexual disorder is a common problem which can be overlooked in practice sometimes. Awareness of the problem makes half of the solution. The other half consists of identifying the risk factors, careful antenatal and postnatal counselling and sexual health assessment, and educating women, their partners, and staff about diagnosis and management of the problem. Episiotomy and severe obstetric traumas are the main risk factors. Restricted use of episiotomy and early management of episiotomy complications can play an important role in preventing persistent PPFSD. There is insufficient evidence to suggest caesarean section as a better mode of delivery in term of preventing or alleviating PPFSD.
Humans have always been interested in altering their body. Whether through piercings or tattoos, for aesthetics, religious reasons, or self-expression, the practice of body modification is a well known art.1 One not as familiar or easily observed body modification type is genital piercings. Genital piercings (GP) are defined as developing a tract under the skin with a large bore needle to create an opening into the anatomical region for decorative ornaments such as jewelry.2-3 Historically, GPs are not a new procedure.
Currently, this once taboo practice is on the rise and more men with GP are presenting with a variety of medical needs to clinics and hospitals.3 From the rare Pubic Piercing (a piercing through the dorsal base of the penis) to the Guiche (a piercing through the perineum), the male genitalia provides ample area to pierce. Men commonly choose from nine different types of GP and often use three major types of piercing jewellery (Figure 1).3-6
Figure 1 Common Types of Genital Piercings (GP) Worn by Men
Illustrations by Larry Starr, Senior Design Specialist Texas Tech University Health Sciences Center. Text modified with permission: Urologic Nursing 2006, 26(3), 175-176.
This rapid growth trend is creating its own set of complications and questions among clinicians. The medical literature suggests the most common risks are infection and bleeding, but there are other structural considerations as well.3-4, 6-8 An example of this is with the most widely known and commonly encountered male GP, the Prince Albert; the jewellery pierces the urethral meatus, exiting through the ventral surface of the penis. The piercing effectively creates a fistula for urine to drain, and many men report experiencing the need to sit down during urination due to the change in stream and difficulty in aiming.3,4 Other reported single case histories of more severe complications are Fournier’s gangrene, urethral tears, priapism, post-coital bleeding or lost jewellery in female partners, paraphimosis, and recurrent sexually transmitted diseases.8-20
Given the variety of negative issues that could arise from GP, any subject related to the health and well being of men having an intimate piercing should be directed to a well informed clinician. Currently, when questions or problems arise, men are more likely to seek assistance from the internet or a piercer rather than a health care provider.3,21-22 Considering the limited medical literature, as well as the minimal availability of clinicians knowledgeable about body piercings and modifications, men with GP are at high risk for delays in appropriate treatment of complications related to piercings as well as for overall preventive healthcare. Over concentration on the presence of GP by clinicians could delay important health care.23
Our purpose for this study was to elucidate information about men with GP in order to aid the clinician in providing relevant information for patients considering GP, as well as to provide further scientific evidence by examining their demographics, risk behaviours, procedural motives and post-piercing experiences. Additionally, several motives or characteristics of those with body art such as depression, abuse, self-esteem, and need for uniqueness were examined.24-29 Authors of this study have experience in urology, various aspects of piercing, and two decades of published body art research.
Problems in attempting any study about those with GP is reaching a sizeable sample for a study and an acceptable data collection methodology as those with GP have a hidden variable of study, making it difficult to make contact. Networking or “snowball” sampling for data collection, as well as anonymous questionnaires, becomes one approach,30 but this also makes it difficult to validate if respondents actually have GP. In an effort to address this issue, survey questions were specifically written for individuals with GP, making it extremely difficult and time-consuming to answer if the respondents did not have applicable experiences. Previous research experience also indicates that after about 10-15 questions, interest can wane and the questionnaire will not be completed.3,7,31
Only two published studies could be located to provide preliminary information about individuals with GP.21,22 In the first study21 data, collected in 2000 and actually published in 2005 had a national convenience sample of 63 women and 83 men with nipple and/or GP. Forty-eight men in the study had GP; the average man was 31 years of age, single, heterosexual, Caucasian, in good-excellent health, who sought out annual physicals, possessed some college education, and spoke of moderately strong religious faith. Almost all were employed, reporting an average annual salary of $36,000, or higher. Over half admitted and continued their belief they were risk takers; many of them also had 3 or more general body piercings. Most did not smoke or use drugs routinely and in this study, no questions about alcohol use were asked. Their average age at first sexual intercourse was 15.7 (the national male average is 16.9).32 Of those that participated (37%) in sport activities or exercise, they reported with no problems. They voiced minimal, if any, regrets to obtaining a genital piercing and would repeat the procedure. The Prince Albert was the most common male GP. Few (12%) voiced any problems with their GP, with urinary flow changes and site hypersensitivity being the most frequently mentioned. Six participants stated partners had refused sexual intercourse with them after their GP. One case of STD (Gonorrhoea) was reported post-procedurally.
As the internet survey demonstrated marked success in reaching those with GP, a similar study was undertaken to query a larger cohort of men with GP to increase clinician awareness in caring for men with GP. Thus, a cross-sectional descriptive study of men with GP was conducted so the collected information could be compared with the previously mentioned studies of those with GP.21,22 To ensure that the rights and dignity of all research participants were protected, exempt study status was obtained for this study from the university institutional review board. Notices of the study and a request for participation were posted on a number of popular body piercing sites with the assistance of an internationally-known Expert Piercer. The survey was available on the web for a total of 6 months during late 2008 and early 2009.
Questionnaire
Questionnaire items were based on a review of literature, the Armstrong Team Piercing Attitude Survey,31 previous work examining women with GP, 3,21-22, 33 and recent findings about those with body art. 24-29 The study purpose and benefits were presented on the front page of the survey. The subjects were informed that completion of the survey indicated their consent to participate in the study and that they could stop at any point during the survey if they were uncomfortable with a question (s). Ethnicity was included to note GP acquisition patterns; the ethnic categories were not defined and participants self-reported. Assurances were provided that the information would be analyzed as group data and no identifying information would be sought. Respondents were encouraged to answer questions honestly and not to be offended by any questions as some of them directly related to unsubstantiated assumptions written about GP in the medical literature. 21-22 There was no ability to tabulate how many individuals viewed the survey if they did not start the survey.
The survey had 4 sections: (a) Obtaining the GP (13 questions); (b) Personal experiences with the GP (32 questions); (c) General information including depression and abuse (26 questions), and (d) Sexual behaviour including forced sexual activity (12 questions). Four scales were also included: motives (14), outcomes (16), pre and post procedural self-esteem (16), and need for uniqueness (4). The previous reliabilities for the motive scale was 0.75,22 outcome scale 0.88,22 and need for uniqueness scale was 0.80;25 data was not available for the self-esteem scale.34 Various response formats were used throughout the survey such as a 5 point Likert scale (1 = strongly disagree or unlikely to 5 = strongly agree or likely), multiple choice, and short answers.
Data Analysis
The Statistical Package for the Social Sciences (16.0 Ed.) was used for data analysis to obtain frequencies, cross-tabulation, and chi-square analysis.30 Additionally, T-tests were used to compare means of similar questions from both the 2005 and 2008 studies with data from the current study. Significant differences were found in both study samples so they were judged as different groups from this current study.
RESULTS
Study Population
While 545 respondents started the survey, responses were analyzed from 445 men with GP (82%) residing in 42 states and 26 international countries; they declared a total of 656 piercings. Clusters of participants were evident from CA (22), NY (17), TX (16), FL (11), Europe (43), Canada (21), and Australia (20). Ages of the men with GP at survey time ranged from 15 to 72 (Table 1). The average participant in this study was 36 years of age, Caucasian, some college education, married, in excellent health, who sought out annual physicals, reported no/few friends with GPs, and declared a salary of $45,000 or higher. Religious beliefs were grouped into either non-existent or moderately to very strong faith. There was almost equal numbers of blue collar and white collar workers: others were from health care, arts, academia or military, while some were self-employed; very few mentioned unemployment, or retirement.
Table 1 Self-Reported Characteristics Of Men with Genital Piercings (GPs) continued
Demographics
Current Study* N = 445
Age at time of survey 20 or < 21-35 36-50 51+
61/29% 77/36% 41/19% 33/16%
Ethnicity Caucasian
319/89%
Martial Status Single Living/significant other Married with/out children
96/27% 69/20 143/41%
Education High school Diploma Some college Bachelor’s degree Graduate/Doctoral degree
34/10% 113/32% 77/22% 88/20%
Occupations Technical/vocational Professional Students Artists
90/28%
92/29%
44/14% 23/07%
Salary <45,000 $45,000+
135/44% 169/56%
Strength/Religious Faith Non-existent Mod Strong-Strong
135/39% 99/28%
State of Health Excellent
310/88%
Health care visits Annual physicals Only when problems
150/43% 142/40%
Close friends w/GPs None 1-3 4+
239/68% 100/28% 14/ 4%
Feel sad/depressed
Little/Some Pre-piercing Post-piercing
248/57% 210/59%
*Numbers will not always add up to 100 because of missing data or multiple answers.
Risk Behaviours
Those who reported pre-procedural risk taking tendencies continued to have significant tendencies for them post-procedurally (χ2 = 2.13) = 16; p = 0.000) (Table 2). Some risky behavior was observed; over half had body art, with an average of 2 piercings or more, as well as tattoos. Alcohol use was infrequent, but when they did, they had 5+ drinks. Other answers did not bear out the risk taker image with their monogamous, heterosexual relationships, limited tobacco, and drugs. Their average age at first intercourse was 17.05 (national male average 16.9).32 Most (391/88%) did not report STDs before their piercings, but of those that did itemize their STDs, Chlamydia was the most frequently mentioned (n =18).
Table 2 Self-Reported Risk Behavior From Men with Genital Piercings (GPs)
Risk Behaviour
Current Study* N = 445
Age at first intercourse Never had intercourse 12 or less 13-15 16-18 19+
12/03% 14/04% 80/25% 160/48% 74 /23%
Sexual Orientation Women
286/82%
Risk Taker Before Piercing
222/52%
Remains Risk Taker
198/52%
Cigarettes Smoked None ½-1 pack daily
252/75% 75/22%
Monthly Alcohol Consumption 1-3 times 5+ drinks @ one setting, 1-3x
118/33% 191/55%
Drugs Used monthly None 1-15 times
294/87% 27/08%
Sexual Partners in 6 months One Two or more
211/62% 98/32%
General body piercings None 1-4 piercings 5+ piercings
119/27% 259/59% 108/33%
Tattoos None 1-4 5+
115/35% 134/38% 76/21%
STDs before piercing
54/12%
*Numbers will not always add up to 100 because of missing data or multiple answers.
Genital Piercing Procedure
A deliberate time delay between their consideration to making the decision to have a GP was present as many had waited almost 5 years before procurement (Table 3). Over half reported the Prince Albert GP, with another third choosing a Frenum/Frenum Ladder (Figure 1). While a small-moderate amount of pain and bleeding was reported procedurally, virtually no drugs or alcohol were used before their GP.
Table 3 Self-Reported Procedural Information From Men with Genital Piercings (GPs)
Genital piercing procedure
Current Study* N = 445
Amt of decision time Waited long time, then a few minutes A long time (over a year)
49/24% 143/37%
Age of GP Decisions Consideration Procurement
29 years 34 years
Type of Genital Piercings Ampallang Apadavya Dydoe Foreskin Frenum/Frenum ladder Guiche Hafada Prince Albert Other
*Numbers will not always add up to 100 because of missing data or multiple answers.
Motives and Outcomes
Table 4 illustrates participant motives and outcomes for each group in the various GP studies.21,22 For the highest motive response of “just wanted one” there was consistency over the three studies; of the top five responses, they were similar but just ranked differently. Alpha measurements for the motive response scale ranged from 0.40 to 0. 75 except for our current study, where the covariance matrix was zero or approximately zero so the statistics based on its inverse matrix could not be computed. Motives centered around wanting a GP, trying something new, have more functional sexual control, and seeking uniqueness. Measureable outcomes (Alpha range 0.88-0.89) of their GP evolved around their sexual expression, uniqueness, and aesthetics, as well as the improvement of their personal and partner’s sexual pleasure. In review, their motives for the GP were met in their stated outcomes.
Table 4A Three Study Comparison Of Self-Reported Motives and Outcomes From Those Wearing Genital Piercings.
Variable
Caliendo et al, 2005 Study: Data Collected 2000 Men with GPs N = 48*
Young, et al, 2010 Study Data collected 2008 Women with GPs N = 240*
Current Study Data collected 2009 Men with GPs N = 445*
Motives for their genital piercing
34/71% “Just wanted one” 24/50% “Trying to feel sexier”
23/45% “For the heck of it”
18/38% “Wanted to be different” 18/38% “Make myself more attractive” (alpha 0.40)
163/70% “Just wanted one” 120/51% “Trying to feel sexier” 111/48% “More control over my body” 93/40% “Seeking uniqueness” 91/39% “Make myself more attractive” (alpha 0.75)
196/90% “Just wanted one”
73/60% “For the heck of it” 67/60% “Trying to feel sexier” 56/58% “More control over body” 51/56% “Seeking uniqueness” (alpha unobtainable)
Outcomes of their genital piercing
36/77% “Improved my sexual pleasure”
35/73% “Helped express myself sexually” 35/73% “Helped me feel unique”
176/76% “Helped express myself sexually 173/75% “Improved my sexual pleasure 157/68% “Helped me express myself 134/58% “Helped me feel feminine” 134/58% “Helped me feel unique” (alpha 0.88)
278/81% “Improved my sexual pleasure
234/71% “Helped express myself sexually”
218/67% “Helped me feel unique” 229/67% “Improved partners sexual pleasure 211/64% “Helped genital look better” (alpha 0.88)
*Numbers will not always add up to 100 because of missing data or multiple answers.
Post-piercing Experiences
The men reported continued satisfaction with their GP and would repeat the procedure. While not many were engaged in exercise/sport activities, those that did, were active (Table 5). A few reported partner refusal of sexual activities when their GP was in place. Almost half reported no piercing complications; of those that did, only 2 major problems were cited. First, with over half reporting Prince Albert piercings, it was not surprising that 25% discussed changes in their urinary flow. Site hypersensitivity was the second most reported problem (23%), otherwise there were no further trends of other severe complications. While 80 (18%) reported STDs after their GP, only 19 itemized the specific type: the most responses were Chlamydia (9). Those that had a history of STDs (Table 2 & 5) before their piercings were significantly more likely to have them post-procedurally (χ2 = 11.5) = 1; p = 0.001).
Table 5 Self-Reported Post Procedural Information From Men with Genital Piercings (GPs)
Complications from piercing No problems Change in urinary flow Site hypersensitivity Skin irritation Rips/tears at site Problems using condoms Keloids @ site Site infection Urinary tract infection Site hyposensitivity Sexual problems Jewellery embedded Erection problems Other, not named
*Numbers will not always add up to 100 because of missing data or multiple answers.
Depression, Abuse, Self-Esteem, and Need for Uniqueness
Four additional characteristics about individuals with GP were examined.24-29 Men with GP respondents reported a small amount of “sad or depressed feelings”; those that had these depressed feelings before their piercings were significantly more likely to continue these depressed feelings post-procedurally (χ2 = 4.1), = 16; p = 0.00). Only 5 (1%) reported being forced to participate in sexual activity against their will, while a few cited (56/12%) physical, emotional, or sexual abuse.
To extract a profile of self-esteem, 8 questions were asked in the pre and post piercing survey sections; internal consistency (Cronbach alpha) of both scales was 0.75. Their responses to both the pre procedure (M = 22.3, SD = 4.51) and the post piercing time (M = 23.1, SD = 3.97) was highly correlated at 0.79 (P<0.01). Two statements triggered split, negative and positive responses with “I make demands on myself that I would make on others” and “I blame myself when things do not work the way I expected.” Lastly, their Need for Uniqueness (NU) was asked using a four item scale24,25in the pre-piercing survey section. When all five responses of the scale were totaled (20), the mean was 11.3 documenting a more positive perspective about their GP, close to the moderate level (Cronbach alpha 0.86), for intentionally wanting to be different, distinctive, and unique. When asked if their overall feelings of NU had changed since obtaining their GPs, those that had NU before their piercings were significantly more likely to have them post-procedurally (χ2 = 11.5) = 16; p = 0.03).
DISCUSSION
When examining this data from men with GP alongside the 2005 published study,21 the cohort almost equalled 500 participants. To our knowledge this is the largest repository of data currently available to provide further evidence of the demographics and health issues regarding men with GP. The anonymous data, obtained by networking sampling and accessible, economical web-based survey, could be viewed as a study limitation. Yet, finding similarities between this data and data collected almost ten years ago suggests that our findings tapped into a core body of knowledge about men with GP. Similar data, obtained at different times, from different respondents increases the credibility and lends the information to further generalizability to influence use in practice.30
The “social reality” 2 of the GP phenomenon is here. All of the men had one type of GP, and some had multiple GP, and many had other general body piercings.35 Awareness of the current types of body modification including GP will help the clinician educate and inform adequately, to give professional advice, and also provide a realistic picture of structural considerations. Respondents stated their GP were an important and satisfying part of their life, they still liked them, and would repeat the procedure; the GP improved their sexual activities, few refused sexual intercourse, those that exercised were active, and they were not troubled by the GP complications. From a medical standpoint the insertion of a GP could be considered a minor surgical procedure, and yet the data suggests that when the GP is performed by experienced hands only minimal side effects are reported. Thus, finding a knowledgeable, expert piercer is an important educational theme. However, patients need to also be aware that certain types of piercing may require some behavioral changes such as toileting and consistent body cleaning. Unfortunately virtually no health care providers, including clinicians, were mentioned in the GP decision making process or care, they usually went to the internet or returned to a piercer for information.21,22 Hopefully, as more clinicians are made aware of GPs, those who are considering GP will find their physician to be a helpful and more informative resource.
These study participants with GP were older, well-educated men, often in a stable relationship, different than what is usually thought about people with body piercings.7, 22,26-27,29,31 This scientific evidence about their overall demographics pose challenges to the current medical literature. Sample demographics from this study and the other two cited GP studies 21,22 do not reflect individuals from stereotypical low performing social and economical backgrounds. Demographically, the people with GP were in their early thirties, Caucasian, heterosexual, well educated, employed, in good health, with some religious beliefs, but not ethnically diverse. In contrast to literature describing men with GP as antisocial miscreants or mostly homosexual, 2,4,18 our data support that these men are more part of the mainstream culture. The avoidance of “rushing to judgment”28 is an important aspect, especially in the way they are often perceived.
Men with GP did not deny their propensity to be risk takers, but being a risk taker was not synonymous with being deviant, but more with achieving individualization.21,28,31 Threads about stable relationships were provided throughout their information, including sexual orientation, marital status, GP complications, and even their lack of many risk behaviours. Their first time for sexual intercourse was close to the male national average. While procurement of any type of body art is thought to be impulsive 7,21-23, their time for GP decision-making was deliberate, as well as their practice of on-going, conscientious care of their piercings.21,22 Absence of alcohol and/or drug consumption before the GP procedure has been a frequent finding in other body art studies.7,21-22,31 Reputable piercing artists advocate for no use of alcohol and drugs as they want their customers to be making realistic procedural decisions about their GP and listening carefully to post GP care instructions.
The unsubstantiated assumptions in the literature about GP complications such as male infertility, scrotal infections, reduction of erotic stimulation, and frequent infections with bicycle rides were also challenged.6,21,36-40 Overall, only two problems of urinary flow changes and site hypersensitivity were reported with their GP. They took their sexual concerns seriously, as part of their internal influences of self esteem and their need for uniqueness. Their documented motives reflected sexual enhancement, aesthetics, as well as uniqueness. Their stated outcomes of the GPs reflected an ability to better express themselves sexually and create a sense of uniqueness; these elements obviously took precedence over the two problems of urinary flow changes and hypersensitivity. Both these motives and outcomes were similar when compared with the other two studies.21,22 Further procedural research is suggested to obtain more information about the reasons some with Prince Albert GP have urinary flow changes, while others do not, to eliminate this as a possible side-effect.
Negative bias continues with the assumption that individuals with GP frequently have STDs.18-20, 36-40 Historically, concern for those who have “exotic adornments” such as body piercings have led some health facilities to require STD screening, no matter what the nature of the presenting complaint.22,35 Yet, in this study and the other two related GP studies,21,22 respondents reported only a few STDs. Their reporting incidence of STD was low compared to the national Guttmacher Institute report of one in three sexually active people will have contracted a STD by age 24.32 As in this study, Chlamydia remains the most highly reported STD in the US.32 While it is important to always conduct a thorough sexual history, 20 perhaps the conscientious care related to the deliberate decision for the GP, and the mostly monogamous relationships reported may account for the limited reporting of STDs. One STD clinic study found that neither socioeconomic status, method of contraception, multiple partners, or the presence of genital infections correlated with GP.38 Further longitudinal research is suggested to examine the long-term effects of GPs, as well as further GP complications and STD prevalence.19
Men, like women, with GP21 reported depressed feelings26,27,29 both pre and post procedure, but gender differences were present with abuse and forced sexual activity. The men with GP reported few incidents of abuse (emotional, physical, or sexual) or forced sexual activity against their will whereas over a third of the women with GP22 reported this. Although women frequently spoke of their use of GPs to take more control in reclaiming their body to “free them from the bonds of molestation and give them strong feelings of empowerment,” 22 men verbalized their use of GPs to give them more sexual control.
STUDY LIMITATIONS
As with any study, several limitations to generalizability of data must be considered and one of methodology has been previously discussed. This was a non experimental, descriptive study design and the respondents self-selected to complete a web-based survey. Bias, inaccurate recall, and/or inflation can result from self-reporting.30 Respondents had to use their personal judgment to interpret questions with the use of an anonymous survey so socially desirable responses could have been entered. Participants with strong negative or positive feelings may have been more likely to complete the survey. Yet, as random sampling is almost impossible in a population with hidden variables, and in spite of these limitations, the respondents did contribute further quantitative data.21,22
CONCLUSIONS
The trend of those obtaining GP continues to increase and is not limited by age, gender, socio-economical backgrounds, or sexual preferences. Many in this study still reported seeking advice of a piercer or the internet. As an identified population at risk for quality health care, further evidence of demographics, piercings and jewellery, motivations, outcomes, and health issues were presented about men with GP so clinicians can provide clinically competent and applicable approaches for care. The collective data examined here, along with some collected almost ten years ago, begins to dispel some of the negative assumptions about this segment of the body modification population regarding their overall demographics, GP complications, and STD prevalence.
The Royal College of Psychiatrists first introduced the CASC in June 2008. It is based on the OSCE style of examination but is a novel method of assessment as it tests complex psychiatric skills in a series of observed interactions.2 OSCE (Observed Structured Clinical Examination) is a format of examination where candidates rotate through a series of stations, each station being marked by a different examiner. Before the CASC was introduced, candidates appeared for OSCE in Part 1 and the ‘Long Case’ in Part 2 of the MRCPsych examinations. The purpose of introducing of the CASC was to merge the two assessments.3
The first CASC diet tested skills in 12 stations in one circuit. Subsequently, 16 stations have been used in two circuits - one comprising eight ‘single’ and the other containing four pairs of ‘linked’ scenarios. Feedback is provided to unsuccessful candidates in the form of ‘Areas of Concern’.4 The pass rate has dropped from almost 60% in the first edition to around 30% in the most recent examination (figure 1). Reasons for this are not known. The cost of organising the examination has increased and candidates will be paying £885 to sit the examination in 2010 in the United Kingdom (figure 2).
Figure 1
We are sharing our experience of the CASC examination and we hope that it will be useful reading for trainees intending to appear for the CASC and for supervisors who are assisting trainees in preparation. In preparing this submission, we have also made use of some anecdotal observations of colleagues. We have also drawn from our experience in organising local MRCPsych CASC training and small group teaching employing video recording of interviews.
Figure 2
CASC is an evaluation of two domains of a psychiatric interview: ‘Content’ (the knowledge for what you need to do) and ‘Process’ (how you do it). The written Papers (1, 2 and 3) test the knowledge of candidates. We therefore feel that the candidates possess the essentials of the ‘Content’ domain. Therefore, the more difficult aspect is demonstrating an appropriate interview style to the examiner in the form of the ‘Process’.
This article discusses the preparation required before the examination followed by useful tips on the day of the examination.
Before the examination day (table 1)
Table 1: Tips before the examination day
Factor
Technique
- The mindset
- Have a positive attitude
- Time required
- Start preparing early
- Analysing areas for improvement
- Use ‘Areas of Concern’
- Practice
- Group setting and individual sessions
- Feedback from colleagues using video
The mindset
In our view, preparation for the CASC needs to begin even before the application form is submitted. Having a positive mindset will go a long way in enhancing the chances of success.5 It is therefore a must to believe in ones ability and dispel any negative cognition. Understandably, previous failure in the CASC can affect ones confidence, but a rational way forward would be to consider the failure as a means of experiential learning, a very valuable tool. Experiential learning for a particular person occurs when changes in judgments, feelings, knowledge or skills result from living through an event or events.6
Time required
Starting to prepare early is crucial as it gives time to analyse and make the required changes to the style of the interview. For instance, a good interview requires candidates to use an appropriate mixture of open and closed questions. Candidates who have been following this technique in daily practice will find it easier to replicate this in examination conditions when there is pressure to perform in limited time. However, candidates who need to incorporate this into their style will need time to change their method of interview.
Analysing areas for improvement
Candidates need to identify specific areas where work is needed to improve their interview technique. The best way to accomplish this is by an early analysis of their interview technique by a senior colleague, preferably a consultant who has examined candidates in the real CASC examination. We think its best to provide feedback using the Royal College’s ‘Areas of Concern’ - individual parameters used to provide structured feedback in the CASC. This will help to accustom oneself with the expectation in the actual examination.
Requesting more than one ‘examiner’ to provide feedback is useful as it can provide insight into ‘recurring mistakes’ which may have become habit. In addition, different examiners might provide feedback on various aspects of the interview style. The Calgary-Cambridge guide7, 8 is a collection of morethan 70 evidence-based communication process skills and is a vital guide to learn the basics of good communication skills.
Practice
We believe that it is important to practice in a group setting. Group work increases productivity and satisfaction.9 The aim of group practice is to interact with different peers which will help candidates to become accustomed to varying communication styles. Group practice is more productive when the group is dynamic so that novelty prevails. Practising with the same colleagues over a period of weeks carries the risk of perceiving a false sense of security. We feel this is because candidates get used to the style of other candidates and, after a period of time, may not recognise areas for improvement.
Another risk of a static group is candidates may not readily volunteer areas for improvement - either because they may feel they are offending the person or, more importantly, because the same point may have been discussed multiple times before! Whenever possible, an experienced ‘examiner’ may be asked to facilitate and provide feedback along the lines of ‘Areas of Concern’. However candidates need to be conscious of the pitfalls of group work and negative aspects such as poor decisions and conflicting information.
In addition to group practice, candidates would benefit immensely from individual sessions where consultants and senior trainees could observe their interview technique. Candidates could interview patients or colleagues willing to role-play. We have observed that professionals from other disciplines like nurses and social workers are often willing to help in this regard. Compared to group practice, this needs more effort and commitment to organise. Consultants, with their wealth of experience, would be able to suggest positive changes and even subtle shifts in communication styles which may be enough to make a difference. We found that video recording the sessions, and providing feedback using the video clips, helps candidates to identify errors and observe any progress made.
The feedback of trainees who appeared in the CASC examination included that attending CASC revision courses had helped them to prepare for the examination. It is beyond the remit of this article to discuss in detail about individual courses. The majority of courses employ actors to perform role-play and this experience is helpful in preparing for the CASC. Courses are variable in style, duration and cost. Candidates attending courses early in their preparation seem to benefit more as they have sufficient time to apply what they have learnt.
During the examination (table 2)
Table 2: Tips during the examination
Factor
Technique
- Reading the task
- Fast and effective reading
- Focus on all sub-tasks
- Time management
- ‘Wrap up’ in the final minute
- The golden minute
- Establish initial rapport
- Leaving the station
- Avoid ruminating on previous station
- Expecting a surprise
- Fluent conversation with empathy
Reading the task
Inadequate reading and/or understanding of the task leads to poor performance. Candidates have one minute preparation time in single stations and two minutes in linked stations. We have heard from many candidates who appeared in the examination that some tasks can have a long history of the patient. This requires fast and effective reading by using methods such as identifying words without focusing on each letter, not sounding out all words, skimming some parts of the passage and avoiding sub-vocalisation. It goes without stating that this needs practice.
CASC differs from the previous Part 1 OSCE exam in that it can test a skill in more depth. For example it may ask to demonstrate a test for focal deficit in cognition that may not be detected by conducting a superficial mini mental state examination.
Candidates need to ensure they understand what is expected of them before beginning the interview. In some stations, there are two or three sub-tasks. We believe that all parts of a task have a bearing on the marking.
An additional copy of the ‘Instruction to Candidate’ will be available within the cubicles. We suggest that when in doubt, candidates should refer to the task so that they don’t go off track. Referring to the task in a station will not attract negative marking but it is best done before initiating the interview.
Time management
It is crucial to manage time within the stations. A warning bell rings when one minute is left for the station to conclude. This can be used as a reference point to ‘wrap up’ the session. If the station is not smoothly concluded before the end of the final bell candidates may come across as unprofessional. Candidates also run the risk of losing valuable time to read the task for the next station.
Single stations last for seven minutes and linked stations last for ten minutes. Candidates who have practiced using strict timing are able to sense when the warning bell will ring. They are also able to use the final minute to close the session appropriately.
Having stressed the importance of finishing the stations on time, it is also vital to understand that an early finish can lead to an uncomfortable silence in the station. This may give the examiner the impression that the candidate did not cover the task. We feel that there will always be something more the candidate could have explored!
The awkward silence in the above scenario can potentially make the candidate feel anxious and ruminate on the station which must be avoided.
The golden minute
First impressions go a long way in any evaluation and the CASC is no different in this regard.10 Candidates need to open the interview in a confident and professional manner to be able to make a lasting impact and establish a better rapport. Observing peers, seniors and consultants interacting with patients is a good learning experience for candidates in this regard.
Candidates who do well are able to demonstrate their ability to gain the trust of the actors in this crucial passage of the interaction. Basic aspects such as a warm and polite greeting, making good eye contact, and clear introduction and explanation of the session will go a long way in establishing initial rapport which can be strengthened as the interview proceeds.
The first minute in a station is important as it sets the tone of the entire interaction. A confident start would certainly aid candidates in calming their nerves. Actors are also put at ease when they observe a doctor who looks and behaves in a calm and composed manner.
Leaving the station behind
Stations are individually marked in the CASC. Performance in one station has no bearing on the marking process in the following stations. It is therefore important not to ruminate about previous stations as this could have a detrimental effect on the performance in subsequent stations. The variety of tasks and scenarios in the CASC means that candidates need to remain fresh and alert. Individual perceptions of not having performed well in a particular station could be misleading as the examiner may have thought otherwise. Candidates need to remember that they will still be able to pass the examination even if they do not pass all stations.
Expecting a sorprise
Being mentally prepared to expect a new station is good to keep in mind while preparing and also on the day of the examination. Even if candidates are faced with a ‘surprise station’, it is unlikely that the station is completely unfamiliar to them. It is most likely that they have encountered a similar scenario in real life. Maintaining a calm and composed demeanour, coupled with a fluent conversation focused on empathy and rapport, will be the supporting tools to deal with a station of this kind.
Conclusion
The CASC is a new examination in psychiatry. It tests a range of complex skills and requires determined preparation and practice. A combination of good communication skills, time management and confident performance are the key tools to achieve success. We hope that the simple techniques mentioned in this paper will be useful in preparing for this important examination. Despite the falling pass rate, success in this format depends on a combination of practice and performance and is certainly achievable.
Problem based learning (PBL) has been an important development in health professions education in the latter part of the twentieth century. Since its inception at McMaster University1 (Canada), it has gradually evolved into an educational methodology being employed by many medical schools across the globe2,3. PBL presents a paradigm shift in medical education, with a move away from ‘teacher centered’ to ‘student centered’ educational focus. The assumptive difference between a pedagogy learner and an androgogy learner (Table 1) was summarised by Knowles4, and the androgogy approach underpins PBL. This shift has redefined the role of a teacher in the PBL era, from being a teacher to a facilitator.
Table 1: Differences between Androgogy and Pedogogy learner (Knowles)
Characteristics
Pedagogy
Androgogy
Concept of the learner
Dependent personality
Self-directed
Readiness to learn
Uniform by age-level & curriculum
Develops from life tasks & problems
Orientation to learning
Subject-centered
Task- or problem-centered
Motivation
By external rewards and punishment
By internal incentives curiosity
It is well known that implementing PBL as an educational methodology required additional resources compared to a traditional lecture based curricula5. In addition, there was a need to recruit and train a large number of tutors to facilitate the PBL process6.Training PBL tutors is an important component of a successful curriculum change, and is a continuous process. Training workshops and role plays were employed to train conventional teachers, but challenges were faced in developing them into effective PBL tutors5.
The aim of this paper is to evaluate the literature for any evidence supporting the theory that a PBL background student may develop into an effective PBL tutor. The Medline, EMBASE and CINHAL databases were searched to look for any pre-existing literature or research supporting this theory.
Results:
To the best of my knowledge, there has been no reported evidence supporting this theory. With limited literature evidence, this paper aims to identify common grounds between a PBL student and a PBL tutor, and whether being a PBL student may contribute to the overall development as a PBL tutor. The discussion evolves around the following domains:
1. Teaching Styles:
The ideal teaching style of a PBL tutor is a facilitative-collaborative style, which augments and supplements the PBL process. The teaching style inventory developed by Leung et al7 hypothesised four domains of teaching styles: the assertive, suggestive, collaborative and facilitative styles. Though a PBL tutor assumes himself in possessing this style (facilitative), it does not necessarily match with the students perceptions, as reported by Kassab et al8.
Some of the characteristics of being a PBL student may foster the development of a collaborative teaching style. Being a student, you are expected to be a collaborative learner which is critical for achieving and improving group performance9. Initial years as a student in PBL may contribute to developing attributes required to develop a preferential teaching style.
2. Facilitating critical thinking:
PBL is grounded in cognitive psychology and is set out to stimulate curiosity and build durable understanding. One of the roles of the tutor is to foster critical thinking and enhance the group’s ability to analyse and synthesise the given information. This attribute stems from the tutors ability to facilitate, rather than teach. Irby10 opined that clinical teachers tended to teach as they themselves were taught using traditional approaches, which may affect the process of stimulating critical thinking among the students.
A tutor from a PBL background would have the ability to think critically, through a process of developing thoughtful and well-structured approach to guide their choices11. Tiwari et al12 showed in their study that PBL students showed significantly greater improvement in critical thinking compared to traditionalist courses. Hence, prior exposure to a certain learning style can create a cognitive psychology that can contribute to tutor development.
3. Group dynamics:
One of the prime roles of a PBL tutor is to facilitate the PBL process by keeping the group focused on tasks, and guiding them to achieve their goals. Tutors who are skilled in group dynamics are evaluated more highly than those who are not so skilled11,13 . Tutors need to develop sound appreciation of the group dynamics, failing which may lead to fostering uncertainty with in the group. Bowman et al13 commented about the lack of consideration on the emotional implications placed on prospective PBL tutors when tutoring small groups, especially the skills required to balance between short term anxieties and potential serious problems. This imbalance which usually serves as unconscious incompetence may affect group dynamics.
PBL students would have experience of group dynamics and the pressures of working within it. They would have developed a model of working with members with varying attributes. Blighet al14 showed in their study that students from a PBL curriculum rated themselves better in team working and motivation compared to conventional course peers. This highlights the fact that an apprenticeship model may be necessary in developing the right skills to be an effective tutor.
The characteristics of a student that may foster ideal attributes in a PBL tutor are briefly summarised in Table 2, and has evolved from the work of Samy Azer9,11 .
Table 2: Common ground
Ideal PBL student
Ideals of a PBL tutor
Knows his role within a group
Would help in identifying different roles students may play
Knows to ask empowering questions
Would help in guiding groups in achieving learning objectives
Monitors his own progress by self evaluation and motivation
Would help in monitoring individual progress and motivate group
Bonds with other members to achieve goals
Would help in building trust and encourage bonding of group members
Develops thoughtful and well structured approach to guide choices
Would help in facilitating critical thinking
Fosters collaboration with other group members to create a climate of trust
Would facilitate collaborative teaching style
4. Tutor training
Considerable resources are exhausted in teaching new tutors the art of facilitating a PBL group6, and the usual cohort is teachers from a conventional taught background. The shift from didactic expertise to facilitated learning is difficult for those tutors who feel more secure in their expert role. Finucane et al5 published their study which showed that only a minority of staff had volunteered to be PBL tutors, possibly reflecting the fact that absence of prior exposure to PBL style of learning may have contributed to this. In spite of tutor training workshops, they could only retain 73% at the end of two years.
Prior exposure as a student may help negate much of the stigma associated with PBL. They would have observed and learnt from their PBL tutors, and would have analysed their contribution to the PBL process. They could reflect on their experience and evolve into an ideal PBL tutor. This would help in minimising resource expenditure and contribute towards retention of staff.
5. Tutor comfort zones:
PBL contextualises learning to practical situations, with integration across disciplinary boundaries. Dornan et al15 reported on how some teachers felt PBL to be a frustrating drain on time as it did not fit their educational style, and was a distraction from clinical teaching, demonstrating the ‘conditioning effect’ of prior experiences. This further fuels the debate between content vs. process expertise, but prior knowledge of the process would benefit the students and the PBL process.
6. Role modeling:
Role models have long been regarded as important for inculcating the correct attitudes and behaviors in medical students. Being an ideal role model is considered as one of the prime requisites of a teacher. In a recent study, Mclean et al16 showed that PBL students tended to have a higher percentage of role models compared to students from a traditional programme (73% vs. 64%). In an ideal setting, a “content and process expert” would be the perfect role model for the PBL students, but this may not be realised in all settings.
Paice et al17 commented on the resistance to change within the medical profession, and highlighted the need for training to emphasise the values and attitudes required. This puts an added emphasis on the tutor to demonstrate tenacity and virtues to be an effective role model, avoiding ‘cognitive clouding’ from previous experiences.
As a PBL student, they would be exposed to variety of PBL tutors. They would have incorporated the good points of an effective PBL tutor, and would have reflected on the negative aspects. Reflective practice enables them to develop the right attributes. Though these attributes may be difficult to develop through training workshops, having a background of PBL education may help mould the tutor characteristics.
Conclusion:
As PBL continues to be employed across different specialties, there would be increased emphasis on the medical schools to match the resources needed to implement it. There is an argument for developing an apprenticeship model or recruiting tutors from PBL background, which would help in reducing the cost in training new tutors, along with nullifying the negative influences a new tutor may bring. The biggest limitation in the present setting is finding a cohort of PBL background tutors, but an apprenticeship model may benefit teachers from conventional background. A prospective research study exploring the attributes of tutors, successful and less successful, from traditional, PBL and hybrid curricula and those who have crossed the Rubicon from traditional to PBL can effectively answer this question.
Oesophageal compression by a vascular structure resulting in dysphagia is uncommon. There have been multiple reports in the medical literature of almost every major vascular structure in the chest causing some degree of oesophageal compression and subsequent dysphagia(1, 2). In 1794, David Bayford, described a case of a 62 year-old lady having dysphagia due to an aberrant right subclavian artery. He coined the term “dysphagia lusus naturae”, which means “Freak of nature” (3).
Pill-induced esophagitis is associated with the ingestion of many pills and presents an uncommon cause of erosive oesophagitis (4). Multiple different classes of drugs have been described to be hazardous to the oesophageal mucosa and cause pill-induced oesophagitis (5, 6). Although uncommon in itself, dysphagia lusoria has not been described in literature to present as pill-induced oesophagitis. We present the first case of dysphagia lusoria causing pill-induced oesophagi's by testosterone pills in a young healthy man. Pubmed review of the English medical literature has been conducted to discuss the epidemiology, pathogenesis and management of this uncommon disorder.
Case Presentation:
A 26 year-old man with no significant past medical history presented with 5 days of dysphagia (for both solids and liquids), odynophagia and retrosternal chest discomfort. He admitted to having occasional difficulty swallowing for past 2-3 months for solids only. He denied any heartburn, cough, regurgitation, loss of appetite, weight loss, fever, chills, haematemesis or melaena. He denied tobacco or alcohol use. 2 weeks prior to presentation he had started taking testosterone pills for body-building. Physical examination was completely unremarkable.
A barium oesophagram showed extrinsic oblique compression of the oesophagus at the level of the carina as it passes through the aorta. CT scan and MRI of the chest revealed a right-sided aortic arch crossing posteriorly to the oesophagus with proximal oesophageal dilatation consistent with Dysphagia Lusoria. Endoscopy noted erosive oesophagitis/distinct ulceration extending from 18cm into a pulsatile area of narrowing at 20 cm with normal mucosa visualized distally.
Biopsies revealed oesophageal squamous mucosa with marked acute inflammation, reactive changes and no evidence of viral inclusions. Surgical management was discussed with the patient, but given the short duration of symptoms and the patient's stable weight, providing symptomatic relief with lifestyle changes, together with a trial of medications such as proton pump inhibitors were considered. At 2 weeks follow-up whilst taking proton pump inhibitors and having discontinued the testosterone pills, the patient experienced complete resolution of symptoms.
Epidemiology:
Dysphagia Lusoria: Moltz et al, found that lusorian artery has a prevalence of about 0.7% in the general population, based on the post-mortem findings(7). Also, out of 1629 patients who underwent endoscopy for various reasons, 0.4% had a finding of a lusorian artery in a report from Fockens et al(8). It has also been concluded based on the autopsy results and retrospective analysis of patients’ symptoms during life that about 60-70% of these patients remain asymptomatic (7). Coughing, dysphagia, thoracic pain, syncope and Horner's syndrome may develop, but usually present in old-age(9).
Pill-Induced Oesophagitis: The data on pill-induced oesophagitis is rather limited. A Swedish study found an incidence of 4 cases per 100,000 population/year(10). Wright found the incidence of drug-induced oesophageal injury to be 3.9/100,000(11). This may be underestimated and does not include subclinical or misdiagnosed cases. Also, cases are reported selectively, due to clustering of cases, newly implicated pills or rare complications. The incidence today is probably much higher due to increased use of prescription medications, widespread use of endoscopy and an ageing population. All these factors limit our ability to correctly assess the true epidemiology of this iatrogenic disorder.
Pathogenesis
Dysphagia Lusoria: During embryological development, the aortic sac gives rise to six aortic arches and with further development the arterial pattern is modified and the fourth arch persists on both sides and some vessels regress. In right arch anomaly, the left arch atrophies and disappears whereas the right arch persists. If both arches persist, they form a double arch or a vascular ring encircling the trachea and oesophagus (12).
Pill-induced oesophagitis: Several lines of evidence confirm that oesophageal mucosal injury is caused by prolonged contact with the drug contents(13, 14) .On clinical grounds, patients frequently report a sensation of a pill stuck in the oesophagus before the development of symptoms and the frequent occurrence of symptoms after improper pill ingestion. Endoscopically, the evidence includes occasional observation of pill fragments at the site of injury, sharp demarcation of the injury site from the normal tissue and the frequent localization of the injury to the areas of oesophageal hypomotility or anatomic narrowing(4, 15). Therefore factors predisposing to the drug-induced oesophageal injury can be divided into two main categories: patient or oesophageal factors (16, 17, 18,19,20,21) and drug or pharmaceutical factors as shown in tables 1 and 2 (13,14,22,23,24).
Table 1: Patient/Esophageal facors for pill-induced esophagitis
Old Age
Decreased Salivation
Pill intake in recumbent position
Lack of adequate fluid intake with the drug
Structural abnormalities of esophagus
Hypomobility of the esophagus
Table 2: Drug related factors for pill-induced esophagitis
Chemical structure(sustained release pills, gelatinous surface)
Formal structure (capsule increases risk over the tablet)
Solubility
Simultaneous administration of multiple medications
It is important to note that most patients who experience pill-induced damage have no antecedent oesophageal disorder, neither obstructive nor neuromuscular (25). It is the combination of anatomic narrowing coupled with the caustic effects of the implicated drug that caused the oesophageal injury in our case. Although testosterone pills have never been reported to cause pill-induced oesophagitis, 6 cases of corticosteroid-induced oesophagitis have been described in the literature(26) .
Clinical Presentation
Dysphagia Lusoria: As previously mentioned the disorder remains asymptomatic in majority of the patients. Symptomatic adults usually present with dysphagia for solids, (91%), chest pain (20% or less). Less commonly, patients may have cough, thoracic pain or Horner’s syndrome (27,28). In infants, respiratory symptoms are the most predominant mode of clinical presentation. This is believed to be due to absence of tracheal rigidity, allowing for its compression with resulting stridor, wheezing, cyanosis etc (9) . Richter et al. reported average age of presentation to be 48 years (27). Various mechanisms to explain this delayed presentation have been proposed such as increased rigidity of the oesophagus, rigidity of the vessel wall due to atherosclerosis, aneurysm formation (especially Kommerell’s diverticulum), elongation of the aorta etc (9, 29,30) .
Pill-induced oesophagitis: Patients with pill-induced injury usually present with odynophagia, dysphagia and/or retrosternal chest pain(4) . Symptoms can occur after several days after starting a drug, but frequently occur after the first dose. (13) .Fever and haematemesis signifying a possible mediastinal extension can occur without chest pain(32,33). Pharyngitis due to the pill lodged in the hypopharynx has been reported(34).
Our case presents a typical example of asymptomatic Dysphagia Lusoria, who developed acute dysphagia, odynophagia and retrosternal chest discomfort immediately after the initiation of the offending agent; which is very typical of pill-induced oesophageal injury.
Diagnostic approach
Dysphagia Lusoria: The best method to diagnose an aberrant right subclavian artery presenting with difficulty swallowing is initially with a barium oesophagram followed by a CT or MRI scan. (27) .Angiography although considered gold standard for the diagnosis of vascular abnormalities is now largely supplanted by newer less invasive techniques such as CT or MR angiography. Upper endoscopy may reveal a pulsating compression of the posterior wall of the oesophagus as in our case(9, 27). Endoscopic ultrasound, especially with Doppler technology may be helpful to confirm the vascular nature of the abnormality(27). Oesophageal manometry usually shows non-specific findings. High peristaltic pressures have been reported in the proximal oesophagus above the level of the compression (9, 35).
Pill-induced oesophagitis: Barium studies can be normal, and slowing of barium column may be the only abnormality seen(31). Double contrast studies may however, increase the yield of a positive result(36). Kikendall et al. reported that endoscopy revealed the evidence of injury in all the patients (5) . Endoscopy most commonly reveals one or more discrete well demarcated ulcers with normal surrounding mucosa. Ulcers may range from pin-point to several centimetres in diameter(5). Biopsies, if performed, help to distinguish the condition from infection and neoplasia.
Our case shows a distinct oblique compression in the posterior wall of oesophagus on the barium study (fig 1) and classic findings on MR/CT with contrast which also excluded any other thoracic vascular abnormalities (fig 2-5). Endoscopic images of a shallow ulcer are shown in fig 6,7.
Figure 1- Barium esophagram depicting the extrinsic indentation of the esophagus as it crosses the aorta.
Figure 2- CT scan of the thorax demonstrating esophageal compression from a posteriorly placed aorta.
Figure 3- Magnetic resonance image showing esophageal compression with proximally dilated esophagus.
Figure 4- CT image showing the right sided origin of the aortic arch.
Figure 5- Three Dimensional image of the heart and the right sided approach of the arch.
Figure 6- Endoscopic view of esophageal inflammation at the site of compression.
Figure 7- Endoscopic image of the esophageal injury using narrow band imaging.
Treatment
Dysphagia Lusoria: The treatment of patients with DL primarily depends upon the severity of symptoms. Mild to moderate cases are managed by lifestyle and dietary changes such as eating slower, chewing well, sipping liquids, weight reduction and reassurance as in our case.(9,27) Janssen et al also reported in a series of 6 patients that 3/6 improved with proton-pump inhibitor alone or in combination with the prokinetic drug cisapride (9) .Severe symptoms and failure of medical therapy may need surgical evaluation and treatment. Richter et al. reported 14/24 patients who underwent surgical repair of the aberrant vessel for DL(27) . Bogliolo et al proposed endoscopic dilation as a temporary alternative to relieve symptoms in patients who are poor surgical candidates (37) .
Pill-induced oesophagitis: Most uncomplicated cases of pill-induced oesophagitis may heal spontaneously, with resolution of symptoms in a few days to a few weeks. Withdrawal of the offending drug and avoidance of topically irritating foods such as citrus fruits, alcohol is imperative to aid healing (4, 13). Sucralfate, topical anaesthetics, and acid suppression are often used to aid in relief of pain(4, 15). Rarely, in severe cases, parenteral nutrition or endoscopic dilation of chronic strictures may be required. (15, 25)
Conclusion
Our case demonstrates a typical case of DL presenting with pill-induced oesophagitis who responded to conservative and acid suppressive therapy. Identifying the risk factors and adequate patient education is the key to prevention.