The way a doctor dresses is a fundamental part of establishing therapeutic alliance with patients.1,2 It has been shown that doctor’s dress can influence patient confidence, offer greater reassurance, higher levels of trust, better adherence to prescribed medication regimens, enhanced willingness to complete return visits, and discuss sensitive issues.3,4 The literature outcomes in this field are mixed; for example, some studies suggest a non-correlation with perceived courteousness or professionalism,5,6 but we believe there is enough evidence to suggest that the manner in which a doctor dresses forms an important part of non-verbal communication, which is important for their interaction with patients, carers and with other staff members.
Various studies have examined patient preferences towards doctors’ dress. Formal dress or a white coat have been cited as favoured due to their perceived association with empathy, competence and trust.2,4,7,8 This is in contrast to other studies which found semiformal dress as preferred.9
In psychiatry, studies of inpatients have indicated a preference for smart attire and white coats as part of their doctors' dress code.10,11 Mcguire et al also found that community patients preferred their psychiatrists to be dressed as “smart/formal”.12
In recent years, dress code policy for doctors in the UK has become more informal, and white coats have been abolished for a number of reasons.13 In this study, we sought to determine the attitudes of multiple stakeholders towards doctors’ dress in both general and psychiatric hospital settings.
Methods
We surveyed healthcare staff, patients, and carers in an emergency department at a district general hospital (“medical setting”), and in a psychiatric hospital (“psychiatric setting”) in the South East of England. The data was collected on a week day between 09.00 and 17.00 at both settings, using a questionnaire based on Rehman et al.14 There were no exclusion criteria.
The survey questionnaire sampled demographic details, and used nine questions and two sets of images (a male doctor & a female doctor) depicting three styles of dress; white coat, formal (tie & trousers for male; dark skirt and white shirt for female) and smart casual (“bare below the elbows”). The survey questionnaire was piloted amongst volunteer staff and assessed for their user-friendliness and ease of comprehension before use. It was amended in line with the feedback received.
Results
337 individuals responded to the questionnaire, giving a response rate of 94%. Our sample was predominantly white (72%), female (62%) and married (43%). Respondent age, ethnicity and employment status were broadly representative of the local population.
Overall (Table 1), we found that the majority of respondents felt that the way that doctors dress was important to them, and that the location of respondents significantly affected their preferences (p <0.001). Although in these overall results there was no majority preference for one dress code over another in either location, preferences within each varied significantly (medical: p<0.01 and psychiatric: p<0.001). This numerical preference appeared to be for formal dress in both settings, capturing 35% and 45% of respondent vote respectively.
Within the three stakeholder-specific breakdowns (Tables 2-4), differences in preference reached significance for medical staff (p<0.001), psychiatric staff (p<0.001), psychiatric patients (p<0.05), and psychiatric carers (p<0.01). Like the overall results, there was no majority preference in any of these groups, but formal dress captured the highest numerical vote in medical staff (41%), psychiatric staff (55%), and in psychiatric patients (41%). Psychiatric carers preferred formal and smart casual dress broadly equally, which captured 36% and 40% of the vote respectively. Carers were the only stakeholder whose preferences were significantly influenced by their location (p< 0.01).
Dress code statistically significantly influenced the attributes associated with the doctor wearing them (p< 0.0001), as shown in Table 5. Formal dress captured the greatest proportion of every attribute tested, and considering total responses, formally dressed doctors were almost twice as likely to be associated with these attributes as those dressed in smart causal or a white coat.
52% of respondents were not aware that a doctors’ dress code policy existed, and while 53% of respondents felt they should not be consulted when considering dress code, 41% believed they should. 59% of respondents believed doctors adhered to their sites’ dress code policies, while 27% did not think so.
Discussion
To our knowledge, this is the first study in the world to compare preferences in doctors’ dress code between a psychiatric hospital and a medical hospital. Also, no other study to our knowledge has simultaneously explored the attitudes of different key stakeholders in both medical and psychiatric settings regarding this important issue.
In this study, we have successfully captured the attitudes and perceptions of key stakeholders regarding doctors’ dress code. We found that overall, doctors’ dress code was felt to be important, and that in medical and psychiatric locations a formal dress code is preferred. Looking at staff, patients and carers specifically, we found a preference for formal dress among medical staff, psychiatric staff, and in psychiatric patients. Among psychiatric carers, formal dress was preferred equally to smart casual. There were no significant preferences among the other stakeholders surveyed.
This preference for formal dress is easily explained by the results shown in Table 5. Seeing a doctor in formal dress made it almost twice as likely that that doctor would be seen as possessing any of the eight positive attributes included. Clearly, in the eyes of the respondents to our survey, a formally dressed doctor was most likely to provide good care.
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
42
40
59
26
167
<0.01
-
Psychiatric
57
18
76
19
170
<0.001
-
Total
99
58
135
45
337
-
<0.001
Table 1. Dress code preferences among all stakeholders. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
22
10
27
7
66
<0.001
-
Psychiatric
22
4
35
3
64
<0.001
-
Total
44
14
62
10
130
-
NS
Table 2. Dress code preferences among staff. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
14
14
15
10
53
NS
-
Psychiatric
16
9
24
10
59
<0.05
-
Total
30
23
39
20
112
-
NS
Table 3. Dress code preferences among patients. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
6
16
17
9
48
NS
-
Psychiatric
19
5
17
6
47
<0.01
-
Total
25
21
34
15
95
-
<0.01
Table 4. Dress code preferences among carers. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Dress code
Associated doctor attribute
Total
Trust
Advice
Conf.
Return
Knowl.
Caring
Resp.
Auth.
Smart casual
77
57
59
74
49
109
51
38
514
White coat
74
91
89
77
107
65
87
103
693
Formal
142
138
142
134
132
110
143
145
1086
Table 5. Doctor attributes associated with different dress codes.Respondents were shown images of each dress code asked “Which doctor would you…”: Trust the most (trust), Follow the advice of (advice), Have confidence in their diagnosis and treatment (conf.), Return to for follow-up care (return), Regard as knowledgeable & competent (knowl.), Regard as caring & compassionate (caring), Regard as responsible (resp.), Regard as authoritative & in control (auth.). P <0.0001.(calculated using Chi-squared test). Results were excluded for where more than one dress code was selected for an attribute, or where no choice was made.
Discussion (continued)
Interestingly, we also found that the location of healthcare influenced the preferences of carers to such an extent that it offset the non-significant results among staff and patients; such that this significance was carried through to the overall results. Exploring this in more detail, we see a marked preference for smart casual in the psychiatric setting over the medical setting (40% vs. 13%), for a white coat in the medical setting over the psychiatric setting (33% vs. 11%), and an almost equal preference for formal dress in both. This starkness in difference in preference between care locations indicates differences in the cultural perceptions of doctors by carers, but not by staff or patients. Perhaps an explanation for this difference is that historically, carers have been more involved and influential in the psychiatric setting, being an essential component to care, whereas in the medical setting they have tended to be more passive partners in care. A negative perception of mental health care portrayed to the public through film and media may have driven preferences away from white coat in the psychiatric setting, whereas in the medical setting perhaps a positive association with the white coat and physical health may have done the opposite.
Conclusion
We have identified a clear preference for a formal dress code for doctors from all stakeholders at medical and psychiatric care locations studied. However, we identified several interesting variations in preferences among individual stakeholders, and found that the location of care significantly impacted the preferences of carers. We believe these findings could be harnessed in the future development of dress code policies for doctors in order to enhance the doctor-patient relationship, and to improve the quality of doctors’ relationships with both carers and with other staff members. Additionally, there may be merit in involving these stakeholders during the policy development process.
Endocrine disorders are frequently accompanied by psychological disturbances. Conversely, psychiatric disorders, to significant extent demonstrate consistent pattern of endocrine dysfunctions. [1] Endocrinopathies manifests as myriad of psychiatric symptoms, as hormones affect a variety of organ systems function. The presence of psychiatric symptoms in patients with primary endocrine disorders provides a new insight for exploring link between hormones and affective function.[2] Disturbance of hypothalamic-pituitary-thyroidal axis is of considerable interest in psychiatry and is known to be associated with a number of psychiatric abnormalities.[3]Thus, the main focus of psychoneuroendocrinology is on identifying changes in basal levels of pituitary and end-organ hormones in patients with psychiatric disorders. Psychiatric symptoms may be the first manifestations of endocrine disease, but often are not recognized as such. Patient may experience a worsening of the psychiatric condition and an emergence of physical symptoms with the progression of the disorder.[4] Psychiatric manifestations of endocrine dysfunction include mood disturbances, anxiety, cognitive dysfunction, dementia, delirium, and psychosis. While dealing with treatment-resistant psychiatric disorder, endocrinopathies should also be considered as a possible cause in management. Psychotropics medicine may worsen the psychiatric symptoms and improves only once the underlying endocrine disturbance is corrected. [5]The lifetime prevalence of depression and anxiety is 11.8% to 36.8% and 5.0% to 41.2% respectively in the group with previously known thyroid disorder. [6,7].The occurrence of major depression in DM is mostly estimated around 12% (ranging from 8-18%). 15-35 % of individuals with DM report milder types depression. [8]. Depressive symptom is seen in almost half of patients with Cushing's syndrome and these experience moderate to severe symptoms. Some patients with Cushing's syndrome also experience psychotic symptoms [9]. Patients suffering from Addison's disease may be misdiagnosed with major depressive disorder, personality disorder, dementia, or somatoform disorders [4, 10]. Women with hyperandrogenic syndromes are at an increased risk for mood disorders, and the rate of depression among women with PCOS has been reported to be as high as 50 percent. Central 5-HT, system dysregulation that causes depression might simultaneously affect peripheral insulin sensitivity, or vice versa, possibly via behavioral or neuroendocrinological pathways, or both. [10]
Hollinrake 2007 showed prevalence of depression has shown it to be four times that of women without PCOS. Hollinrake screened patients with PCOS for depression and found total prevalence of depressive disorders which included women diagnosed with depression before the study, was 35% in the PCOS group[11]. No specific psychiatric symptoms have been consistently associated with acromegaly or gigantism or with elevated GH levels. Adjustment disorder may occur from changes in physical appearance and from living with a chronic illness [11]. Sheehan’s syndrome (SS) refers to the occurrence of varying degree of hypopituitarism after parturition (1). It is a rare cause of hypopituitarism in developed countries owing to advances in obstetric care and its frequency is decreasing worldwide. Reports of psychoses in patients with Sheehan’s syndrome are rare. [13] Psychiatric disturbances are commonly observed during the course of endocrine disorders .The underlying cause can be hyper- or hyposecretion of hormones, secondary to the pathogenic mechanisms. medical or surgical treatment of endocrine diseases, or due to genetic aberrations[14]. Psychiatric disorders frequently mimic the symptoms of endocrinological disorders. In view of sizable number of patients seeking treatment from our department present with comorbid endocrinolgical disorders, we planned the present study to investigate psychiatric morbidity preferably anxiety and depression pattern among endocrinolgical disorders patients. With this background, we studied the depression and anxiety in different endocrinogical disorders.
Methods
The present study was conducted in the SMHS Hospital of Government medical college Srinagar and the study sample was drawn from patients attending the endocrinogical OPD in the Department of Medicine at Government Medical College Hospital Srinagar (SMHS).The study was conducted over a period of one and half year, from April 2011 to September 2012 in patients attending the Department of Medicine Government Medical College Hospital Srinagar enrolling 152 cases of Endocrinological disorders. All patients were first examined by Consultant endocrinologist. The patients were then selected using simple random sampling choosing every alternate patient. General information including age, sex, residence, economic status, past history of thyroid disorders, family history of psychiatric disorders was included. An endocrinology specialist first examined the patients, while a psychiatrist administers Hospital Anxiety and Depression scale (HADS). Hospital Anxiety and Depression scale (HADS) was used for purpose of screening anxiety and depressive disorders in patients suffering from different endocrinogical disorders. Hospital Anxiety and Depression scale (HADS) is used for purpose of screening anxiety and depressive disorders in patient suffering from chronic somatic disease. HADS contain 14 items and consist of two subscales: anxiety and depression with seven question each. Each question is rated on four point scale (0 to 3) giving maximum total score of 21 each for anxiety and depression. Score of 11 or more is considered a case of psychological morbidity, while as score of 8-10 represents borderline and 0-7 as normal. The forward backward procedure was applied to translate HADS from English to Urdu by a medical person and professional translator. [15]
The participating physicians subjected select patient of chronic Endocrinological disorders to HADS Questionnaire and recorded scores both for anxiety and for depression.
The patients were subjected to inclusion and exclusion criteria as given below:
Inclusion criteria
1. All endocrinological disorders.
2. Both sexes will be included.
3. Age > 15 yrs.
4. Those who will give consent.
Exclusion criteria
1. Those who don’t consent.
2. If diagnoses is not clear.
3. Age less than 15 years.
4. Presence of pregnancy or a history of pregnancy in the last six months.
5. Those who are on steroids or drugs known to interfere with thyroid function
General description, demographic data and psychiatric history was be recorded using the semi structured interview which was pretested
Statistical methods: Statistical analyses were performed using the SPSS, version 16.0 for Windows. A secure computerized database was established and maintained throughout the study. Patient names were replaced with unique identifying numbers. Descriptive statics were used to generate a profiles of each illness group based on presence of depression only, anxiety only and those with both anxiety and depression. To determine whether there were any significant differences between each illness group in the prevalence of depression and anxiety disorders , an unadjusted 3×2×2 test chi square was conducted. Data were analyzed by the Pearson chi-squared test and t test. P<0.05 was considered as the significance level in the evaluations.
Consent: Informed consent was obtained from each patient; those who were considered incapable of consenting were allowed to participate with consent of their closest family member or custodian. All patients were informed about the nature of the research within the hospital and willingly gave their consent to participate. Information sheets and preliminary interviews made it clear that the choice to consent or otherwise would have no bearing on the treatment offered. The project ensured the anonymity of the subjects by replacing patient names with unique identifying numbers before the statistical procedures began.
Results
A total of 152 patients from the endocrinological departments of Govt. Medical College, Srinagar hospitals were taken up for study. They were evaluated in detail with regard to socio-demographic profile regard to presence of psychiatric co-morbidity by HADS and the results have been presented below in the tabulated form .Only patients who consented for complete interview and respond to all HADS questions were considered in final analyses.
Out of total 152 subjects 71 were males (46.72%)), and 81 were females (53.28%) (Table 1). Most of cases belong to 35-45 year age group (26.3%) followed by age group 25- 35 years (24.3%) and 67.7% were married and 18.4% were unmarried. More than half (51.97 %) of the study subjects were from nuclear families and 82 (53.9%) were illiterate and majority 84(55.4 %) belonging to middle class family. The socio-demographic profile of the studied patients is shown in Table-2 .
Out of 152 patients with endocrine disorders, 56(37%) patients elicited HADS score of 10 or less indicating absent or doubtful association anxiety or depression. 96 (63.15%) patients were found positive to HADS Questionnaire with anxiety/depression score of 11 or more. The mean HADS score for anxiety alone, depression alone and anxiety/depression patients were 13.42, 15.7 and 25.62 respectively. On the basis of HADS screening, 96(63.157%) patients had varying degree of psychiatric co morbidity. 27 (28.12%) had anxiety alone, 30(43.47%) had depression alone where 39(40.62%) as patients had anxiety and depression both.(Table 3) The breakdown of total number of different Endocrinological disorders is given in table. Maximum psychiatric comorbidity is found in thyroid patients (69.35%) followed by diabetic patients (68.05). (Table 4).
Table 1: Age and sex distribution
Sex
Total
Male
Female
Age group
< 25
14
20%
7
9%
21
14%
25 – 35
20
28%
17
21%
37
24%
35 – 45
17
24%
23
28%
40
26%
45 – 55
11
16%
19
24%
30
20%
55 & above
9
13%
15
19%
24
16%
Total
71
100%
81
100%
152
100%
Mean ± SD
51.4± 13.7
56.4± 13.1
54.1± 13.6
Table 2: Demographic Characteristics of the Studied Patients
Characteristic
N
%
Dwelling
Rural
98
64.47
Urban
54
35.52
Marital status
Unmarried
28
18.4
Married
103
67.7
Widowed
21
13.8
Occupation
Household
61
40.1
Unskilled
29
19
Semiskilled
39
25.6
Skilled
23
15.1
Professional
8
5.26
Family type
Nuclear
79
51.97
Joint
28
18.4
Extended
45
29.6
Literacy status
Illiterate
82
53.9
Primary
22
14.4
Secondary
16
10.5
Matric
13
8.55
Graduate
11
7.23
Postgraduate/Professional
8
5.26
Family Income(Rs)
< 5000
45
29.6
5000 to 10000
85
55.92
≥ 10000
22
14.4
Socioeconomic status ( Kuppuswamy Scale )
Lower
32
21
Upper lower
11
7.23
Middle
84
55.2
Upper middle
19
12.5
Upper
6
3.94
Table 3: Result of HADS Scoring
Variable
Total (n=96)
Anxiety alone
Depression Alone
Anxiety depression both
p value
Male
37(38.54%)
8(29.6%)
18(60 %)
11(28.2%)
-
Female
59(61.4%)
19( 70.3%)
12( 40%)
28(71.7 %)
-
Age (Years)
54.1± 13.6
51.4± 13.7
56.4± 13.1
54.1± 13.1
< 0.005
Mean HADS Score
-
13.42±3.4
15.73±3.3
25.62±4.3
< 0.005
Table 4: Types of endocrinological disorders
Endocrinological disorders
Number of patients(N=152)
Psychiatric comorbidity
percentage
Thyroid disorders
62 (40.7%)
43
69.35
Diabetes mellitus
47(30.92%)
32
68.05
PCOD
28(18.4%)
16
57.1
Cushings syndrome
5(3.289%)
2
40
Acromegally
2(1.31%)
0
0
Addisions disease
1(0.65%)
0
0
Sheehan’s syndrome
3(1.97%)
2
66.6
Miscellaneous
4(2.63%)
1
25
Table-5 Psychiatric Co-morbidity across Socio-demography of the Patients
Present
Absent
p value
n
%
N
%
Dwelling
Rural
59
60.02
39
39.7
<0.005 (Sig)
Urban
37
68.5
17
31.4
Marital status
Unmarried
8
28.5
20
71.4
>0.005 (NS)
Married
72
69.9
31
30
Widowed
16
76.1
5
23.8
Occupation
Household
57
93.4
4
6.55
>0.005 (NS)
Unskilled
14
48.2
15
51.7
Semiskilled
9
39.1
30
76.9
Skilled
14
60.8
9
39.1
Professional
2
25
6
75
Family type
Nuclear
45
56.9
34
43.0
>0.005 (NS)
Joint
22
78.5
6
21.4
Extended
29
64.4
23
51.1
Literacy status
Illiterate
70
85.2
12
14.6
>0.005 (NS)
Literate
26
36.1
46
63.8
Family Income(Rs)
< 5000
17
37.7
28
62.2
>0.005 (NS)
5000 to 10000
65
76.4
20
23.5
≥ 10000
14
63.6
8
36.3
Socioeconomic status
Lower
18
50
18
50
>0.005 (NS)
Upper lower
7
63.6
4
36.3
Middle
59
70.2
25
29.7
Upper middle
10
52.6
9
47.3
Upper
2
33.3
4
66.6
Discussion
This study is the first to offer data on psychiatric morbidity among endocrine patients in the Kashmiri population. 63.15% (96) patients were found positive to HADS questionnaire with anxiety/depression score of 11 or more in our study. The results of this study suggest patient suffering from endocrinological disorders are likely to have a co-morbid psychiatric disorder. [5, 16].Depressive disorders and anxiety disorders are the commonest psychiatric disorders in endocrinogical patients. [3].Numerous studies have shown a high correlation between depression and endocrinological disorders and this study supports these findings, with 43.47 %( 30) of the participants having depressive symptoms on the HADS. [3, 16] 40.62% (39) respondents had both depressive symptoms and an anxiety disorder. 28.12% (27) participants were diagnosed with an anxiety disorder, which is slightly higher than the lifetime prevalence of anxiety disorder in men [16]. Our findings of a high proportion of respondents with endocrinological disorders (45.7%) Female were more in number than their male counterparts 59(61.4%) vs. 37(38.54%) and the majority of men presenting with endocrinological disorders were between the ages of 35 and 45 years has also been reported in a previous studies. [4, 8].The findings of our study suggest that psychiatric disorders are highly prevalent in endocrinological disorders and is largely unrecognized in the primary care setting. Endocrine disorders of different kinds, irrespective of treatment have been associated with Psychological distress. Psychological wellbeing of endocrine disorders may provide new insights in clinical endocrinology. Further psychological disorders comorbid with endocrinological disorders adds to their disability as well as cost to the individual and the society.[17] Most of the clinicians do not suspect this important association of endocrinological disorders in the beginning resulting in delayed diagnosis. Thus, the high prevalence of anxiety and depression in endocrinological disorders in our study supports a case for screening for these disorders in endocrinological clinics. Furthermore, recognition and treatment of these comorbidities could improve patient outcomes. Future studies should focus on replicating or refuting these findings in larger samples as well as in testing interventions aimed at targeting psychological morbidities in this patient group. Under-recognition of psychiatric morbidity is not an uncommon phenomenon, and has been found in similar local studies of psychiatric morbidity in other medical illnesses[8].Thus, more attention should be paid to recognizing psychiatric morbidities in this group of patients.. The reasons for increase in the frequency of psychiatric disorders are multi-factorial. Being chronic illness leads to psychological stress .The major limitation of our study was relatively small sample size. Another limitation of our study is its crossectional design, which does not allow us to determine direction of causality in the relationship between endocrinological disorders and depression/anxiety. More community based studies are required to assess the magnitude of the problem and to lay down principles to help such patients.In order to clarify the temporal relationship prospective studies with a bigger sample size are essential in the future. As far as we are aware, this is a first of its kind study in kashmir. Endocrinological disorders accounts for a huge proportion of referrals to psychiatric clinics and misery is added upon an already devastating metabolic disease. To add the cost associated with psychiatric morbidity accounts individual and to the society are substantial. Thus, the high prevalence of anxiety and depression in endocrinological disorders in our study supports a case for screening for these disorders in Endocrinological clinics. Furthermore, recognition and treatment of these comorbidities could improve patient outcomes.
Chest pain accounts for 1% of all GP consultations, but in only 8%-18% of cases is it an indicator of underlying ischemic heart disease.1 Given the potential diagnostic uncertainty associated with chest pain at initial presentation, specialist evaluation of patients in a Rapid Access Chest Pain Clinic (RACPC) is of value and represents an important process in the evaluation of symptoms. These clinics were established with the aim of providing rapid outpatient assessment of patients with suspected cardiac disease in order to permit earlier provision of appropriate treatment and investigations where required.
Stable chest pain typically presents as angina, a triad of dull central chest pain, brought on with exertion and relieved by rest or GTN spray. The aetiology is usually stable atherosclerotic plaque disease which is associated with low mortality and can be treated with oral anti-anginals, as demonstrated by meta-analyses and the landmark COURAGE study. 2, 3
NICE Clinical Guideline 95 (NICE CG95) suggests that choice of initial investigation for stable chest pain should be guided by a patient’s pre-test probability of having CAD. Calculations of the pre-test probability take into consideration a patient’s age, gender, cardiac risk factors and symptoms. Patients are defined as high risk of cardiac disease if they have diabetes, smoke or have hyperlipidaemia (total cholesterol >6.47mmol/litre). Patients with none of the above are considered low risk. Symptoms are defined as “typical angina” if the pain is: 1) constricting discomfort in the front of the chest or in the neck, shoulders, jaw or arms; 2) is precipitated by physical exertion and 3) is relieved by rest or GTN spray within approximately five minutes. Pain is defined as “atypical angina” if only two of the above criteria are met and defined as “non-anginal” if one or none of the above criteria are met.
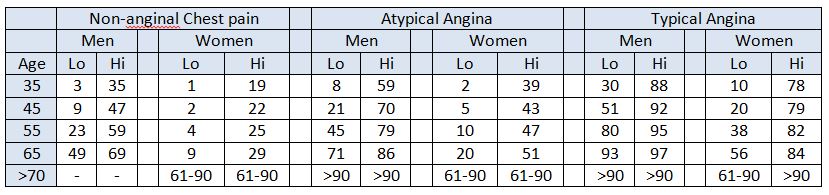
NICE pre-test probabilities of CAD (Table 1), are based on a version of Diamond and Forrester’s pre-test probabilities published in 1979, modified using data from Duke’s cohort study, published in 1993.4, 5, 6 Recent studies suggest that these NICE pre-test probabilities may overestimate the prevalence of CAD in a primary care population and may risk over investigating patients.7, 8 In addition to having financial implications, this may cause patients undue anxiety and unnecessarily put them at risk of complications.
Table 1: NICE Clinical Guideline 95 pre-test probabilities table. Each cell represents the percentage risk of each group of patients having CAD, based on their typicality of symptoms, gender, age and cardiac risk factors (lo, low and hi, high)4
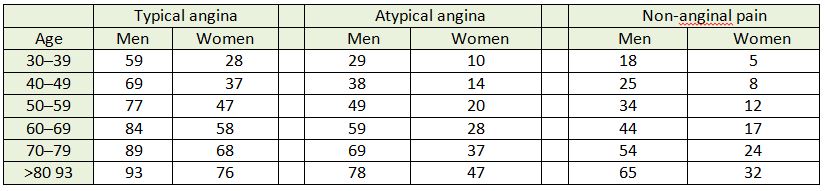
ESC guidelines utilise an updated, validated model of the Diamond-Forrester model by Genders et al. to create pre test probabilities of CAD (Table 2), based on patient’s age, gender and typicality of symptoms. 9, 10
Table 2: ESC guidelines clinical pre-test probabilities in patients with stable chest pain symptoms Each cell represents likelihood of each group of patients having CAD, based on typicality of symptoms, age and gender.9
We hypothesised that strict adherence to NICE guidelines results in over-estimation of the pre-test probability of CAD and therefore over-investigation of patients presenting with stable chest pain. ESC guidelines may offer more accurate pre-test probabilities of CAD and allow a more targeted and cost-effective use of investigations.
Methodology
Clinic records of all patients who attended the RACPC at Tunbridge Wells Hospital between July 2005 and December 2012 were reviewed. This service is run by a cardiology specialist. Patient demographics, cardiac risk factors and information regarding the nature of patient symptoms were collected prospectively and completed at the time of the patient’s RACPC appointment. Results of cardiac investigations were collected from paper and computerised records, and included diagnoses of significant CAD made following invasive coronary angiogram. These results were compared with patients’ pre-test probabilities of CAD calculated using both NICE and the ESC’s calculation methods. Outcome and readmissions were obtained from electronic records from the Maidstone and Tunbridge Wells NHS Trust computer records retrospectively.
Results
Study population
A total of 1968 records were reviewed. 59% (n = 1162) of patients were male and 41% (n = 806) were female. Their mean age was 60 years. At initial assessment, 69.8% patients (n=1373) had non-anginal chest pain, 19.5% (n=383) had atypical angina and 10.8% (n=212) had typical angina, based on the NICE guideline definitions of chest pain.
97.2% (n= 1912) patients underwent further investigation; 15% (n=256) of these were subsequently diagnosed as having significant CAD, accounting for their symptoms. The 2.8% (n=56) of patients who did not undergo investigation either chose not to, were unable to, were lost to follow up, or were diagnosed as having a non-cardiac cause of their symptoms at the initial RACPC appointment.
NICE CG95 pre test probabilities compared against cohort data
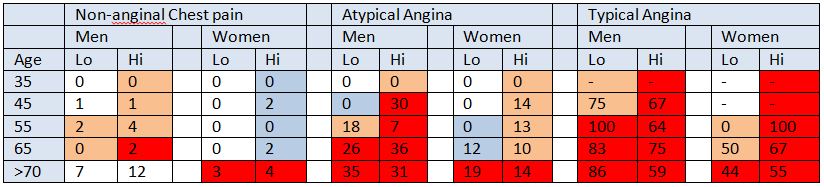
Table 3: NICE guidelines 95 pre test probabilities compared against cohort data Each cell represents the proportion (%) of cohort patients from each group who were diagnosed with CAD. We have colour-coded cells to represent the NICE estimated pre-test probability of CAD in each group. Red cells represent 61-90+% probability, pink cells represents 30-60% probability, blue cells represent 10-29% probability and white cells represents <10% probability of CAD according to NICE Guidelines. “ – “ marks a cell where pre-test probabilities of CAD could not be calculated for cohort patients.
Table 4: A comparison of NICE pre-test probabilities and cohort patient data. The risk of CAD as predicted by NICE guidelines 95 on the left compared with the actual number of cohort patients in each category and the proportion of those patients diagnosed with significant CAD.
The average discrepancy between the pre-test probability and actual incidence of CAD in cohort patients was 28% (range 20% - 88%). In 48% of cells in the NICE CG95 pre-test probability table (Table 1) the pre-test probability of CAD was overestimated by 30% or more (Table 3). A marked discrepancy between pre-test probability and actual incidence of CAD was found between “high risk” and “very low risk” patients. On average, high risk patients had an overestimated pre-test probability of 34.3 – 40.9% per cell compared with low risk patients whose pre-test probability was only overestimated by 6.5% (Table 3).
The cells highlighted in dark red in table 3 represent high risk patients whose pre-test probability was of 61-90+%, according to NICE CG95. In our cohort, only 31.2% (n=214, 95% CI 27.6-34.5) of high risk patients in this category were diagnosed with CAD. On average, actual incidence of CAD compared with pre-test probability was overestimated by 34.4% – 40.9% in each cell.
The pink cells in table 3 represent medium risk patients with a pre-test probability of CAD of 30-60%, according to NICE CG95. In our cohort, only 4.4% (n=24, 95% CI 3.0 – 6.5) of medium risk patients had a positive angiogram (Table 4). The average overestimate of actual incidence against pre-test probability was 35.9%.
The cells highlighted in blue in table 3 represent low risk patients with a pre-test probability of CAD of 10-29%, according to NICE CG95. In our cohort, only 2.5% (n=7, 95% CI 1.2 – 5.0) of low risk patients were diagnosed with CAD (Table 4). On average, the pre-test probability of CAD exceeded the found incidence of CAD by 18.6% (Table 3).
The white cells in table 3 represent very low risk patients with pre-test probability of CAD <10% according to NICE CG95. In our cohort, only 0.28% (n= 1, 95% CI 0.1 – 1.6) of patients were diagnosed with CAD. Average overestimation in this group was 6.5% in each cell.
ESC guidelines pre test probabilities compared against cohort data
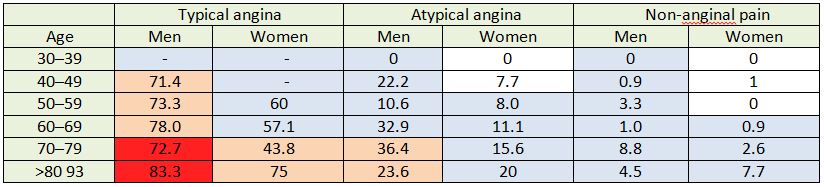
Table 5: A comparison of ESC pre-test probabilities with cohort patient data. Each cell shows the proportion (%) of cohort patients from each group diagnosed with CAD. Each cell is colour coded to correspond with the ESC estimated pre-test probability. Dark red cells represent >85% probability, pale pink cells represent 66-85% probability, pale blue cells represent 15-65% probability and white cells represent <15% probability.
Table 6: A comparison of ESC pre-test probabilities and cohort patient data The risk of CAD as predicted by ESC guidelines on the left compared with the actual number of cohort patients in each category and the proportion of those patients diagnosed with significant CAD.
The average discrepancy between pre-test probability of CAD, according to the ESC’s risk stratification table, and actual incidence of CAD in cohort patients was 20.7%. In 28% of cells, the pre-test probability of CAD exceeded the found incidence of CAD by 30% or more (Table 5).
The cells highlighted in dark red in table 5 represent very high risk patients with a pre-test probability of CAD greater than 85%, according to ESC guidelines (Table 5). 73.4% (n= 58, 95% CI 63.7 – 82.7) of cohort patients in this high-risk category were diagnosed with CAD (Table 6). On average, incidence of CAD in each cell has been overestimated by 13% in this category.
The cells highlighted in pale pink in table 5 represent high risk patients, with a pre-test probability of CAD of 66-85%, according to ESC guidelines. 58.5% (n=103, 95% CI 51.1 – 65.5) of cohort patients in this high-medium risk category were diagnosed with CAD (Table 6). On average, the pre-test probability of CAD exceeded the found incidence of CAD in each cell by 17.7% (Table 5).
The cells highlighted in pale blue in table 5 represent medium risk patients with a pre-test probability of CAD of 15-65%, according to ESC guidelines. 6.4% (n=93, CI 5.3 –7.8) of cohort patients in this risk category were diagnosed with CAD (Table 6). On average, the pre-test probability of CAD exceeded the found incidence of CAD by 24.1%in each cell (Table 5).
The cells highlighted in white in table 5 represent patients whose pre-test probability of CAD was less than 15% according to ESC guidelines. Only 0.76% (n=2, 95% CI 0.2 –2.7) of cohort patients in this risk category were diagnosed with CAD (Table 6). On average, pre-test probability of CAD exceeded found incidence of CAD in each cell by 6.2% (Table 5).
Discussion
Only 15% of a total of 1968 patients referred to RACPC were diagnosed with significant CAD. The majority (70%) of referred patients had “non-anginal” chest pain and low pre-test probabilities of CAD, reflecting the importance ascribed by General Practitioners of ruling out ischemic heart disease as the underlying cause for chest pain, even in low risk patients. This may not be surprising given the large media attention to heart disease and sustained campaigns for early warning signs of heart attack in the British media. It is therefore of great public interest for cardiac disease to be identified.
NICE CG95 pre test probabilities compared against cohort data
Comparing cohort data to the pre-test probabilities of CAD outlined in NICE CG95, NICE have overestimated the number of patients likely to have CAD in the majority of groups. Strict adherence to NICE CG95 therefore carries the risk of over-investigating patients. NICE recommend CT calcium scoring as the first line investigation for patients with a low (10-29%) pre-test probability of CAD. 284 patients fall into this category and only 7 patients were shown to have CAD. This means that 40.5 patients need to be treated in order to identify 1 positive patient (NNT= 40.5).
In patients with a medium (30-60%) pre-test probability of CAD, NICE recommends functional imaging as the first line diagnostic investigation. In our cohort 544 patients would undergo functional imaging, but only 24 of these patients would be diagnosed with CAD, NNT=22.7.
Finally, in patient groups with a high (61-90%) pre-test probability of CAD, NICE recommends invasive coronary angiography as the first line diagnostic investigation. In our cohort of 1968 patients, 691 patients had a high pre-test probability of CAD, and 214 had significant coronary artery disease on angiography, NNT= 3.2.
Although invasive coronary angiography is considered the gold standard investigation for diagnosing CAD, and permits simultaneous therapeutic intervention, the procedure is not without risk, particularly in elderly patients and those with renal impairment.11 Furthermore, invasive angiography is expensive and is costed by the East Kent Hospitals University NHS Foundation Trust at £1166.02 per procedure (private correspondence).
NICE CG95 offers no guidance on managing patients who have a <10% pre-test probability of CAD. 347 of our cohort patients fell into this very low risk category and only 1 was diagnosed with CAD. Therefore, NICE CG95, if strictly adhered to, would have missed one diagnosis of CAD in our patient cohort.
ESC pre test probabilities compared against cohort data
ESC guidelines tend to offer more conservative estimates of pre-test probability of CAD compared with NICE guidelines. Using the ESC’s risk stratification table, almost all patients, except those with over 85% pre-test probability and those with less than 15% pre test probability, would be investigated for chest pain. This is due to their claim that non-invasive, image-based diagnostic methods for CAD have typical sensitivities and specificities of around 85%, so that roughly 15% of these investigations could be yielding false results. Hence, due to these inaccuracies, in patients with pre-test probabilities of CAD below 15% or above 85%, ESC state that performing no test at all could provide fewer incorrect diagnoses.9
In our patient cohort, 79 patients had very high (>85%) pre-test probability of CAD, but only 58 patients (73%) were diagnosed with CAD. For this patient risk group, ESC guidelines suggest that further investigation may not be necessary and that a diagnosis of CAD may be assumed. Thus, applying ESC guidelines to our cohort could result in 21 patients being incorrectly diagnosed with stable angina, and more serious causes of chest pain, for example pulmonary emboli or gastric ulceration, may be missed. However, in practice, it is likely that many patients in this very high pre-test probability category would have undergone angiography, because patients who have "severe symptoms" or who are clinically thought to have "high risk coronary anatomy" should be offered an invasive angiography with or without pressure wire studies. The vagueness of the guidelines allows interventionists to interpret this in the clinical context.
In ESC guidelines, invasive coronary angiography is not specifically recommended as a first line investigation for stable angina, regardless of the pre-test probability of CAD. In patients with a high (66-85%) pre-test probability of CAD, ESC guidelines recommend non-invasive functional imaging first line. Of the 176 patients who fell into this category, only 102 (58.0%) patients were ultimately diagnosed with CAD.
In patients with medium (15-65%) pre-test probability of CAD, ESC guidelines advise exercise ECG testing (or non-invasive imaging for ischemia if local expertise is available) as first line diagnostic investigations. Of the 1451 patients which fell into this category, only 93 were diagnosed with CAD, NNT= 15.6. Fortunately, exercise ECG testing would not expose the patient to potentially harmful radiation or medication, but their poor diagnostic power may result in the need for further investigations, despite a negative result.
In patients with low risk of CAD (<15%) ESC guidelines suggest making an assumption that the patient does not have CAD and advocates conducting no further investigations. In our cohort, 263 patients fell into this low risk category, two (0.8%) of which were diagnosed with CAD.
The ESC guidelines appear to have higher specificity than the NICE guidelines, and only two patients would have been missed had ESC guidelines been adhered to, compared to one patient missed if NICE guidance was used. Thus, although highly sensitive, ESC guidelines when applied to our cohort have lower sensitivity than NICE guidelines.
Comparison of number of investigations
Following ESC guidance for our cohort of patients would have resulted in fewer diagnostic invasive angiograms being performed than if NICE guidance had been followed. ESC guidance only recommends invasive angiography if first line, non-invasive investigations generate positive results. Overall, however, ESC guidance would result in a greater number of overall investigations being performed.
In total, NICE advises that all 691 of our high risk cohort patients should undergo invasive angiography as a first line investigation. 544 with medium risk should undergo functional testing first and 24 of these patients (assuming an angiogram would follow a positive result) would go on to have invasive angiography. 284 low risk patients should undergo CT calcium scoring first, of which 7 would go on to have functional imaging and angiography if the above logic is followed. This generates a total of 1557 investigations; 722 angiograms, 551 functional imaging investigations and 284 cardiac CT scans.
In comparison, using ESC guidance, 176 of our high risk patients would have functional imaging investigations, 103 patients with positive results would then undergo invasive angiography. 1451 patients would receive exercise ECGs, of which 93 with positive results would undergo functional imaging and invasive angiography. This generates a total of 1916 investigations; 196 angiograms, 269 functional imaging investigations and 1451 exercise ECGs.
If we assume that stress echocardiograms are used as “functional imaging” we can estimate costs for our cohort when applying each set of guidelines. Costs for each investigation are supplied by East Kent Hospitals University NHS Foundation Trust and are as follows: Outpatient elective coronary angiograms are costed at £1,166.02; stress echocardiograms are costed at £132.30; exercise ECGs at £40.26 and CTs of one area at £102.47 (private correspondence). If we were to apply NICE guidelines to our cohort, £841,866.44 would be spent on angiograms, £72,897.30 would be spent on stress echocardiograms and £29,101.48 on CT scans. This is a total of £943,865.22 on investigations.
If we were to apply ESC guidelines to our cohort, £228,539.92 would be spent on coronary angiograms, £35,588.7 would be spent on stress echocardiography and £58,417.26 would be spent on exercise ECGs. A total of £322,545.88 would be spent on investigations. Overall, this is £621,319.34 cheaper than applying NICE guidelines.
Limitations of study
This study is based on data from a single site and may not be nationally representative. The final diagnosis was made clinically by an experienced interventional cardiologist, which introduces subjectivity and the risk of interpreter bias. Not all patients underwent the gold standard of invasive coronary angiography to demonstrate the presence of CAD. However, all patients were seen and fully assessed by a cardiologist and 97% underwent investigations if deemed necessary.This study has all the limitations of a registry study. In addition, costs for investigations may vary throughout the country, and indeed the world, with varying expertise available.
Conclusion
In conclusion, strict adherence to NICE CG95 over-estimates the pre-test probability of CAD in our local population group. This is consistent with previous studies conducted in South London where there is a larger Afro-Caribbean population, as well as with studies conducted in the North of England.8,9 Adherence to ESC guidelines in place of NICE guidelines may enable a more targeted and cost-effective use of investigations. Strict application of the ESC guidelines to the study cohort would have resulted in investigations costing an estimated £322,545.88, compared to £943,865.22 if NICE guidelines were applied. However, conducting fewer investigations carries greater risk of misdiagnosis, and using ESC guidelines in isolation introduces the possibility of assuming CAD in patients without conducting investigations to confirm this.
It is advisable that local cardiology departments audit their stable chest pain guidelines to ensure that the interpretation of pre-test probabilities is in keeping with the local population. Unfortunately there is no ideal policy and local protocols should reflect the local population.
In the last few decades, the practice of medicine has seen swift changes, as well as its visualisation in the near future. It was designed and focused on serving the community and helping people in need. However, it is not a secret that there is a huge business around this labour and the economic interest of a diverse industry in the field. 1,2
Not intending to generalise, many have observed in daily practice a comparable trend with modern society. A phenomenon including both patients and health personnel, where there is a demand for health services, a growing supply, and a considerable revenue. Basic market economics, right? 3
Not that simple.
It would be the triumph of basic sciences to explain each disease under a biological substrate, minimising the involvement of other factors. A definitive targeting of biological research would be the key to unlocking knowledge. What is certain is that this approach has transformed pharmacotherapy, treatment alternatives and prognosis.2, 3, 4
Early physicians had little to nil information on what today we call aetiology, pathophysiology and therefore treatment. Patients were rarely relieved due to human intervention. Trepanations were frequently performed in the Classical and Renaissance periods and although having modern indications (decompressive craniotomy), its uses and technique were at best questionable. Belief and verbally transmitted understanding of a handful of medicinal plants whose effect were known empirically were standards of care.5
These times have changed, the pharmaceutical industry is a pillar of the economies in many countries, and the number of transactions and cash flow that they move are beyond the wildest dreams of the first physicians. Born each year, thousands of new pharmaceutical companies develop and market new drugs and medical supplies. 1, 6
As advocated by experts, pharmaceutical and medical supply companies are considered one the safest businesses nowadays, with everyone being a potential consumer/patient. It is the race for continuous development of new drugs to its current rate that guarantees soon we will have more drugs and procedures available. The drug industry may be easily overloaded by an oversupply of organic compounds and procedures to patients. 2, 4, 6
This pharmaceutical industry thriving is widening its horizon. Personalised medicine, the study of the influence of a patient’s genetic makeup on their disease susceptibility, prognosis, or treatment response (efficacy and safety), is actually in the spotlight. This can be assessed in different ways, being preventive and/or therapeutic. 7
In the preventive field, preconception screening studies have been unravelling genetic disorders, as recommended by different guidelines such as those of the American College of Medical Genetics, which are designed for individuals with known genetic conditions or high-risk patients who wish to become pregnant. 8
In the therapeutic filed, pharmacogenomics can aid in the identification of alterations of Single Nucleotide Polymorphism (SNPs) that affect the function or expression of proteins associated with pharmacokinetics or pharmacodynamics of different drugs. In recent years the research community has doubled efforts in personalising certain therapies. Hormonal therapy in breast cancer has been from the beginning a receptor-guided therapy, especially with ER (Oestrogen Receptor) therapy. Initial clinical results of trials conducted so far have allowed to establish single therapies regimens with Tamoxifen or combined with Arimidex. 9
Another model of the advances in this arena is reflected in the new alternatives for prostate cancer. This hormone-dependent tumour has demonstrated recurrent alterations in the androgen receptor and its pathway. In specific patients the disease can be found in Castration-Resistant Prostate Cancer (CRPC), a lethal clinical state in which the tumour has developed resistance to androgen deprivation therapy. This clinical scenario is commonly established in advanced or metastatic prostate cancer patients. The genomic landscape of localised prostate cancer has been well defined, describing putative pathogenic BRCA2 germ line mutations as well as somatic and germ line DNA repair alterations found such as BRCA1, CDK12, FANCA, and RAD51B. Furthermore, the research advances described above can allow clinicians to determine treatment, therefore achieving better outcomes. 10
It is unquestionable that personalising treatment will improve clinical outcomes for patients in the near future and help achieve a more effective use of available health care resources. The next challenge for scientists and researchers is to demonstrate with strong evidence the clinical and cost-effectiveness to support the use of personalised medicine and its implementation in different health care systems around the world. 2, 3, 5
In conclusion, individual patient variability currently studied in drug efficacy and drug safety has represented a major objective in current clinical practices. Years of research results have converged in progresses in pharmacogenetics and human genomics that have dramatically accelerated the discovery of genetic variations that potentially determine variability in drug response, providing better clinical outcomes for patients. The future in this field is expected to allow us to have effective and safe medications to targeted patients with appropriate genotypes.
Global recruitment in psychiatry has been falling for several decades because medical students and graduates have been finding it consistently unattractive 1,2. An analysis of the career choices of newly qualified doctors in the United Kingdom (U.K.) found the same trend from 1974 to 2009; psychiatry was the first career choice for only 3-5% of medical graduates annually3. In the U.K., lack of recruitment into psychiatry had reached a crisis point by 2003 when 15% of all unfilled consultants posts in England were in psychiatry and the Royal College of Psychiatrists was finding recruitment into specialist psychiatry posts increasingly difficult4,5. In 2012, only 78% of the Core Training year one (CT1) posts in psychiatry were filled; a serious shortfall which was overcome by overseas recruitment up until changes in immigration rules.
The factors that seem to dissuade medical students from taking up psychiatry as a future career may include: stigma, bad prognosis of psychiatric disorders, poor scientific base of psychiatry, ‘bad-mouthing’ from medical colleagues, lack of respect among peers & public, threats of violence from patients and lack of resources1-5. However, there is evidence to suggest that many students’ attitudes towards career choice changed in a positive direction after working in psychiatry due to the perceived ‘job satisfaction’, ‘life-style’, ‘training available’ and ‘multidisciplinary approach’3.
Psychiatry has previously been ranked higher in career choice at the end of students’ clinical year6. To ensure a stable psychiatric workforce for the future, there is an obvious need to motivate current and future cohorts of young doctors to take up psychiatry as a career. Das & Chandrasena (1988) found that attitudes changed positively towards mental health following clinical placement in this specialty7. It is also known that medical students’ attitudes to psychiatry and career intentions can be improved by their experiences of teaching8. Students were found to develop more positive attitudes when encouraged by senior psychiatrists, had direct involvement in patient care, or saw patients respond well to treatment. Improvement in attitudes during the placement was also related to an increased intention to pursue psychiatry as a career.
Previous research into attitude to psychiatry as a specialty and career choice seems to have produced conflicting results and most of it was carried out among medical students. Since career choices in the U.K. are actually made in the first clinical year following graduation, we carried out a survey among a recent cohort of foundation year one (FY1) doctors in the South East England before and after their first clinical year.
Method
Our study sample consisted of all FY1 doctors (n=101) in one region of South East England. They participated in the study at the beginning and then at the end of their first clinical year. We used a 20–item questionnaire devised by Das & Chandrasena(1988) to ascertain their perceptions and attitudes towards psychiatry before they commenced their first clinical placement. The questionnaire was sent to them via their Medical Education Managers (MEMS). It was handed out to the FY1 doctors as part of their induction pack for completion along with a study information sheet.
At the end of their first year of working, the participants were asked to complete an amended version of the questionnaire. This included two additional questions which ascertained whether the doctor had an opportunity to work in a psychiatric post, or had any experience of psychiatry in practice (such as taster days or cases in A&E). These amended questionnaires were sent to the foundation doctors electronically via their MEMS for completion.
The data was collected and entered into a spreadsheet to prepare descriptive statistics. Comparisons for before and after exposure to psychiatry, and between the psychiatry and non-psychiatry groups were made using the chi-square test. As the data was binary, a latent class model was developed using LatentGOLD software9 to explore the associations between different items in the questionnaire. Responses from the questionnaires were coded as: responses which agree with a positive attitude to psychiatry or disagree with a negative attitude were coded as +1; those not sure were coded as 0; and responses which agree with a negative attitude to psychiatry or disagree with a positive attitude were coded as -1.
Results
A 100% (n=101) response rate was obtained for the first set of questionnaires completed at the beginning of the year. However, there was a significant drop in the number of questionnaires completed at the end of the year - a 53.5% response rate (n=54) generally but 61.1% (22 out of 36) for those FY1 doctors who had the opportunity or access to a post in psychiatry within their clinical year.
Initial cohort at beginning of the clinical year vs. those with no exposure to psychiatry at the end
Table 1 shows the group means for each questionnaire item, for the whole cohort at the beginning of the year compared to those with no exposure to psychiatry by the end of the year.
Table 1: All FY1 doctors before training placements started (initial cohort) versus FY1 doctors without a psychiatric post after FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.591
0.095
-0.169
0.359
0.476
I may consider pursuing a career in psychiatry in the future
-0.539
-0.136
0.403
0.046
0.760
0.028
Psychiatry is attractive because it is intellectually comprehensive
-0.500
0.273
0.773
0.436
1.000
0.000
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
-0.500
-0.069
-0.442
0.305
0.717
Physicians do not have time to deal with patients emotional problems
-0.294
0.273
0.567
0.142
0.991
0.009
Psychiatrists understand and communicate better than other physicians
-0.127
0.364
0.491
0.090
0.892
0.017
Psychiatrists don't overanalyse human behaviour
0.147
0.364
0.217
-0.200
0.633
0.306
Expressing an interest in psychiatry is not seen as odd
0.157
-0.136
-0.293
-0.727
0.141
0.184
Hospitalised patients are not given too much medication
0.167
0.591
0.424
0.116
0.732
0.007
Psychiatrists don't make less money on average than other physicians
0.255
0.045
0.209
-0.537
0.118
0.208
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.727
0.365
0.033
0.696
0.032
Psychiatric curriculum and training are not too easy
0.520
0.682
0.162
-0.112
0.436
0.243
Psychiatrists are not fuzzy thinkers
0.578
0.818
0.240
-0.082
0.561
0.142
Psychiatrists should have the legal power to treat patients against their will
0.608
0.955
0.347
0.051
0.642
0.022
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.864
0.246
-0.066
0.558
0.121
Psychiatry is scientific and precise
0.627
0.818
0.191
-0.098
0.480
0.194
There is a place for ECT in modern medicine
0.755
0.727
-0.028
-0.239
0.184
0.797
Psychiatric consultations are often helpful
0.853
0.864
0.011
-0.210
0.231
0.924
Entering psychiatry is not a waste of a medical education
0.873
1.000
0.127
-0.048
0.303
0.153
Psychiatrists don't often abuse their legal powers
0.892
1.000
0.108
-0.049
0.264
0.175
Those FY1 trainees who had not worked in psychiatry during the year were significantly more positive (p = < 0.05) for psychiatry’s future, psychiatrist being better at patient communication and not over-medicating their patients. However, they remained significantly less convinced as compared to the whole cohort about psychiatry’s intellectual attraction or taking it up as a future career.
Initial cohort at beginning of the year vs. those with exposure to psychiatry at the end
Table 2 shows the group means for each questionnaire item, for the whole
cohort at the beginning of the year compared to those with exposure to psychiatry at the end of the year.
Table 2: All FY1 doctors before training placements started versus FY1 doctors with a psychiatric post during FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.745
-0.058
-0.242
0.125
0.531
I may consider pursuing a career in psychiatry in the future
-0.539
-0.617
-0.078
-0.332
0.177
0.547
Psychiatry is attractive because it is intellectually comprehensive
-0.500
-0.468
0.032
-0.214
0.278
0.798
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
0.106
0.538
0.248
0.827
0.000
Physicians do not have time to deal with patients emotional problems
-0.294
-0.383
-0.089
-0.401
0.224
0.575
Psychiatrists understand and communicate better than other physicians
-0.127
-0.085
0.042
-0.260
0.345
0.783
Psychiatrists don't overanalyse human behaviour
0.147
0.340
0.193
-0.123
0.510
0.229
Expressing an interest in psychiatry is not seen as odd
0.157
0.106
-0.050
-0.378
0.277
0.761
Hospitalised patients are not given too much medication
0.167
0.362
0.195
-0.044
0.434
0.109
Psychiatrists don't make less money on average than other physicians
0.255
0.404
0.149
-0.092
0.391
0.224
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.064
-0.299
-0.569
-0.029
0.030
Psychiatric curriculum and training are not too easy
0.520
0.596
0.076
-0.128
0.281
0.464
Psychiatrists are not fuzzy thinkers
0.578
0.596
0.017
-0.233
0.268
0.892
Psychiatrists should have the legal power to treat patients against their will
0.608
0.532
-0.076
-0.323
0.171
0.545
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.574
-0.043
-0.290
0.203
0.730
Psychiatry is scientific and precise
0.627
0.702
0.075
-0.155
0.304
0.521
There is a place for ECT in modern medicine
0.755
0.511
-0.244
-0.427
-0.061
0.009
Psychiatric consultations are often helpful
0.853
0.745
-0.108
-0.289
0.073
0.239
Entering psychiatry is not a waste of a medical education
0.873
0.808
-0.064
-0.218
0.090
0.412
Psychiatrists don't often abuse their legal powers
0.892
0.766
-0.126
-0.279
0.027
0.105
After a psychiatry placement, significant positive differences (p=<0.05) were observed in their responses to medical staff’s view of psychiatry, future of psychiatry and place of Electro Convulsive Therapy (ECT) in modern medicine. While there was a positive trend in most responses in favour of psychiatry, trainees remained negative about psychiatry’s status, its scientific base, curriculum & training and taking up psychiatry as a future career.
Those exposed to psychiatry vs. those not exposed to psychiatry
Table 3 compares responses between FY1 doctors exposed to psychiatry during the clinical year and those who were not.
Table 3: FY1 doctors who had a psychiatric post versus those who did not have one
Sorted by the size of the difference between the two groups.
t-test
ranksum
Psychiatry
No Psychiatry
Difference
L
U
p-value
p-value
Most non-psychiatric medical staff are not critical of psychiatry
0.106
-0.500
-0.606
-1.000
-0.144
0.011
0.011
Psychiatrists don't make less money on average than other physicians
0.404
0.045
-0.359
-0.694
-0.024
0.036
0.034
Expressing an interest in psychiatry is not seen as odd
0.106
-0.136
-0.243
-0.735
0.249
0.329
0.322
Psychiatrists don't overanalyse human behaviour
0.340
0.364
0.023
-0.421
0.467
0.917
0.907
Psychiatric curriculum and training are not too easy
0.596
0.682
0.086
-0.210
0.382
0.564
0.497
Psychiatry is scientific and precise
0.702
0.818
0.116
-0.187
0.419
0.447
0.777
Psychiatric consultations are often helpful
0.745
0.864
0.119
-0.173
0.411
0.419
0.388
Within medicine, psychiatry has a high status
-0.745
-0.591
0.154
-0.130
0.437
0.283
0.391
Entering psychiatry is not a waste of a medical education
0.808
1.000
0.191
-0.020
0.403
0.075
0.058
There is a place for ECT in modern medicine
0.511
0.727
0.217
-0.117
0.551
0.200
0.192
Psychiatrists are not fuzzy thinkers
0.596
0.818
0.222
-0.114
0.559
0.192
0.190
Hospitalised patients are not given too much medication
0.362
0.591
0.223
-0.139
0.597
0.218
0.192
Psychiatrists don't often abuse their legal powers
0.766
1.000
0.234
-0.005
0.473
0.055
0.040
A placement in psychiatry can change one's negative views of psychiatry
0.574
0.864
0.289
-0.045
0.623
0.088
0.064
Psychiatrists should have the legal power to treat patients against their will
0.532
0.955
0.423
0.097
0.748
0.012
0.011
Psychiatrists understand and communicate better than other physicians
-0.085
0.364
0.449
0.000
0.897
0.050
0.050
I may consider pursuing a career in psychiatry in the future
-0.617
-0.136
0.481
0.084
0.878
0.028
0.017
Physicians do not have time to deal with patients emotional problems
-0.383
0.273
0.656
0.195
1.000
0.006
0.007
Psychiatry is a rapidly expanding frontier of medicine
0.064
0.727
0.663
0.269
1.000
0.001
0.002
Psychiatry is attractive because it is intellectually comprehensive
-0.468
0.273
0.741
0.352
1.000
0.000
0.001
Those exposed to psychiatry agreed more often that non-psychiatric medical staffs were critical of psychiatry compared to the group not exposed to psychiatry. They also had comparatively negative responses for psychiatrists not abusing legal powers and to have the legal power to treat someone against their will. Trainees exposed to psychiatry also felt significantly (p=<0.05) positive towards psychiatry being intellectually comprehensive and adopting it as a career. However, they were less enthusiastic about psychiatrists treating patients against their will and psychiatry being the expanding frontier of medicine.
Discussion
In this study, we have ascertained attitudes of a regional cohort of FY1 doctors towards psychiatry as a specialty and as a career choice. Our findings are similar to previous research carried out among medical students, which found that there were generally negative attitudes towards psychiatry as a specialty and career choice but fairly positive attitudes towards the role of psychiatry in medicine and in society in general1-5,10. Like others, we also found that personal experience of psychiatry placement can improve trainees’ view of psychiatry as a specialty and as a future career 3,11.
It was interesting to find out that after a year in clinical practice but without any experience of psychiatry, trainees’ attitudes towards psychiatry as a specialty had been positive. It is difficult to know the exact reason but we can speculate that this respect for the specialty may have developed when they experienced limitations of the other specialties in medicine and/or perhaps due to the positive professional encounters with psychiatrists at the Accident & Emergency (A&E) or with psychiatric liaison teams during ward consultations. As opposed to previous research11, it was heartening to note that the group with no exposure to psychiatry agreed that non-psychiatric medical staff were not critical of psychiatry; a possible sign of reduced stigma for psychiatry within the medical profession.
Despite exposure to psychiatry, FY1 doctors’ attitudes to psychiatry’s status, scientific base, curriculum & training and career choice remained somewhat negative. Similar results were found by Lyons et al11 when they assessed students’ attitudes towards psychiatry after a clerkship in the specialty. There was a significant decrease in negative & stigmatising views towards mental illness after the clerkship, but no significant improvement in students' interest in psychiatry was detected1. Goldacre et al (2013) also acknowledged mixed outcomes of early experience of working in psychiatry as it might discourage some doctors. While highlighting positive effect of the doctors’ experience of the speciality, they also cited it as a negative factor that influenced some doctors who had previously considered psychiatry as a career3.
Our study has limitations because of having a small sample and being carried out in one small region of the country. It is also worth mentioning that the group exposed to psychiatry may not have had a psychiatry placement as it also included those who had had taster days or experience in A&E. The brevity of these latter exposures cannot give someone a real sense of the specialty. The nature of this and the overall experience needs to be differentiated and the exposure quantified in the future studies. Our study findings also need to be replicated with future cohorts and in other regions for confirmation because FY training programme in the U.K. is relatively recent and placements in psychiatry have evolved4 over the last few years through closer collaboration between different stakeholders in the Foundation Training Programmes.
Hypertension is the most common risk factor for perioperative cardiovascular emergencies. Acute episodes of hypertension may arise due to the aggravation of a pre-existing chronic hypertensive condition or as de novo phenomena1.
Emergency, anaesthesia, intensive care and surgery are among the clinical settings where proper recognition and management of acute hypertensive episodes is of great importance. Many surgical events may induce sympathetic activity, leading to sudden elevations in BP2.
The long term end-organ effects add to patient morbidity and mortality. Ensuring cardiovascular stability and pre-optimization of BP allows safe manipulation of physiology and pharmacology during anaesthesia2. Different medications are available for the management of hypertensive emergencies. The greatest challenge is the acute care setting where the need for proper and sustained control of BP exists.
Definition
Acute severe elevations in BP have several terms. The syndrome characterized by a sudden increase in systolic and diastolic BPs (equal to or greater than 180/120 mmHg) associated with acute end-organ damage that requires immediate management otherwise it might be life-threatening was defined as malignant hypertension3. The international blood pressure control guidelines removed this term and replaced it with hypertensive emergency or crisis4.
Criteria for hypertensive emergencies (crises) include: dissecting aortic aneurysm, acute left ventricular failure with pulmonary oedema, acute myocardial ischemia, eclampsia, acute renal failure, symptomatic microangiopathic haemolytic anemia and hypertensive encephalopathy5.
While they suggest 'hypertensive urgency' for patients with severe hypertension without acute end-organ damage3. The difference between hypertensive emergencies and urgencies depends on the existence of acute organ damage, rather than the absolute level of blood pressure5.
Causes of hypertensive crises
Cessation of antihypertensive medications is one of the main causes. Other common causes are autonomic hyperactivity, collagen-vascular diseases, drug use (stimulants, e.g. amphetamines and cocaine), glomerulonephritis, head trauma, pre-eclampsia and eclampsia, and renovascular hypertension6.
Signs and symptoms of hypertensive crisisinclude severe chest pain, severe headache accompanied by confusion and blurred vision, nausea and vomiting, severe anxiety, shortness of breath, seizures and unresponsiveness.
Pathogenesis
Humoral vasoconstrictors released in the hypertensive crises episodes result in a sudden increase in systemic vascular resistance. Endothelial injury accompanies severe elevations of BP resulting in fibrinoid necrosis of the arterioles with the deposition of platelets and fibrin, and a breakdown of the normal autoregulatory function. The resulting ischemia speeds the further release of vasoactive substances completing a vicious cycle7.
Perioperative hypertension
At least 25% of hypertensive patients who undergo noncardiac surgery develop myocardial ischemia associated with the induction of anaesthesia or during the intraoperative or early post-anaesthesia period8. Previous history of diastolic hypertension greater than 110 mmHg is a common predictor of perioperative hypertension. The level of risk depends on the severity of hypertension9.
Sympathetic activation during the induction of anaesthesia increases the BP by 20 to 30 mmHg and the heart rate by 15 to 20 beats per minute in normotensive individuals8. These responses may be more obvious in patients with untreated hypertension in whom the systolic BP can increase by 90 mmHg and heart rate by 40 beats per minute.
Intraoperative hypertension is associated with acute pain induced sympathetic stimulation besides certain types of surgical procedures like carotid surgery, intrathoracic surgery and abdominal aortic surgery. Paix et al, analysed 70 incidents of intraoperative hypertension and reported that drugs were the precipitating cause (inadvertent vasopressor administration by the anaesthetist or surgeon, intravenous adrenaline with local anaesthetic and failure to deliver a volatile agent or nitrous oxide) in 59% of the cases. Light anaesthesia and excessive surgical stimulation represented 21% of incidents, while equipment related causes (ventilation problems e.g. stuck valve, hypoventilation, soda lime exhaustion and endobronchial intubation) were 13% of incidents. Awareness under general anaesthesia, myocardial infarction and pulmonary oedema represented 7% of incidents10.
In the early postanaesthesia period, hypertension often starts within 10 to 20 minutes after surgery and may persist for 4 hours. Besides pain induced sympathetic stimulation, hypoxia, intravascular volume overload from excessive intraoperative fluid therapy and hypothermia can promote postoperative hypertension. If untreated, patients are at high risk for myocardial ischemia, cerebrovascular accidents and bleeding11. Hypertension might happen 24 to 48 hours postoperative due to fluid mobilisation from the extravascular space, besides cessation of antihypertensive medication in the early postoperative period12.
The absolute level of BP is as important as the rate of increase. For example, patients with chronic hypertension may tolerate systolic BPs (SBP) of 200 mm Hg without developing hypertensive encephalopathy, while pregnant women and children may develop encephalopathy with diastolic BPs of 100 mm Hg13.
Preoperative general considerations for hypertensive patients
During preoperative assessment we have to review associated medical problems such as ischaemic heart disease, cerebrovascular disease and renal failure. This can assess the risk for anaesthesia and so the hypertensive end-organ damage. Some patients with hypertension are asymptomatic and accidentally discovered during preoperative assessment. Incidental hypertension may suggest long standing hypertensive disease1. Idiopathic hypertension comprises about ninety percent of hypertensive patients6.
Management of perioperative hypertension crises
The treatment plan of perioperative hypertension differs from treatment of chronic hypertension. Hypertensive patients undergoing elective surgery are at risk for increased perioperative hypertensive attacks. Postponement of elective surgery is recommended in chronic hypertensive patients if the diastolic BP is ≥110 mm Hg until the BP is controlled14. We have to determine if it is a hypertensive emergency or urgency, besides the underlying causes of the patient’s BP elevation.
The most appropriate medication for management of hypertensive emergency should have a rapid onset of action, a short duration of action, be rapidly titratable, allow for dosage adjustment, have a low incidence of toxicity, be well tolerated and have few contraindications2,15. A parenteral antihypertensive agent is preferred due to rapid onset of action and ease of titration5.
The goal of therapy is to halt the vascular damage and reverse the pathological process, not to normalise the BP. Guidelines by the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High BP for treating hypertensive emergencies include starting intervention with reducing systolic BP by 10 to 15%, up to 25% within the first hour. Followed
by gradual reduction of the absolute BP to 160/110 mmHg over the following two to six hours5,16.
Hypertension that occurs with tracheal intubation, surgical incision and emergence from anaesthesia is best treated with short-acting β-blockers, calcium channel blockers, vasodilators, or angiotensin-converting enzyme inhibitors. Postoperative hypertension is best managed by correction of precipitating factors (pain, hypothermia, hypervolemia, hypoxia and hypercarbia)17.
Unintentional hypotension and associated organ hypoperfusion happens with aggressive attempts to lower BP since the homeostatic mechanisms depend on higher blood pressure for adequate organ perfusion. While inadequate lowering of BP may result in increased morbidity and mortality. However, the alteration between overshooting BP and severe hypotensive states and using vasopressors to get the normotensive levels may damage end-organs and the vasculature - precise control of BP in a hypertensive crisis is a challenge18.
Since chronic hypertension shifts cerebral and renal perfusion autoregulation to a higher level, the brain and kidneys are prone to hypoperfusion with rapid decrease in blood pressure. So control of blood pressure to baseline levels should take 24 to 48 hours5.
In cases of aortic dissection, the systolic BP should be reduced to less than 120 mmHg within twenty minutes. In ischemic stroke, BP must be lowered to less than 185/110 before administration of thrombolytic therapy19. Gentle volume expansion with intravenous saline solution will maintain organ perfusion and prevent sudden drop in BP with using antihypertensive medications5. Preoperative hypertension is a hypertensive urgency, not an emergency, as it rarely involves end-organ damage with adequate time to reduce the BP18. Longer acting oral medications such as Labetalol and Clonidine may be more suitable 20.
Common antihypertensive medications used in hypertensive crises
Sodium Nitroprusside is a combined venous and arterial vasodilator which decreases both afterload and preload. The onset of action is within seconds and duration of action lasts for one to two minutes, so continuous BP measurement is recommended. If the infusion is stopped, the BP rises immediately and returns to the pretreatment level within one to ten minutes. Prolonged intravenous administration with infusion rates more than 2 mcg/Kg/min may result in cyanide poisoning. Thus, infusion rates greater than 10 mcg/Kg/min should not be continued for prolonged periods21.
Labetalol, an alpha- and beta-blocking agent has proven to be beneficial to treat patients with hypertensive emergencies. Labetalol is preferred in patients with acute dissection and patients with end-stage renal disease. The onset of action is five minutes and lasts for four to six hours. The rapid fall in BP results from a decrease in peripheral vascular resistance and a slight fall in cardiac output22. A reasonable administration protocol is to give an initial intravenous bolus of Labetalol 0.25 mg/Kg, followed by boluses (0.5 mg/Kg) every 15 minutes until BP control or a total dose 3.25 mg/Kg. Once an adequate BP level is achieved, we can start oral therapy with gradual weaning from parenteral agents22.
Fenoldopam, a peripheral dopamine-1-receptor agonist, induces peripheral vasodilation; administered by intravenous infusion. Duration of action from 30 to 60 minutes. Gradual decrease in blood pressure to pretreatment values occurs without rebound once the infusion is stopped because of short elimination half-life. A starting dose of 0.1 μg/kg/min, titrated by 0.05 to 0.1 μg/kg/min up to 1.6 μg/kg/min. Fenoldopam provides rapid decline in blood pressure with reflex tachycardia so beware in patients at risk of myocardial ischemia23.
Clevidipine, a dihydropyridine calcium channel blocker, produces rapid and precise BP reduction. It has a short half-life of about one to two minutes with potent arterial vasodilation without affecting venous capacitance, myocardial contractility or causing reflex tachycardia24. Start intravenous infusion of Clevidipine at 1-2 mg/h; titrate the dose at short intervals (90s) initially by doubling the dose. Systolic pressure decreases by at least 15% from baseline within 6 minutes post-infusion24. A 1-2 mg/h increase in infusion rate produces an additional 2-4 mmHg reduction in SBP14. Clevidipine is an ideal agent to manage acute severe hypertension moreover safe for patients with hepatic and renal dysfunction2.
Rational approach to the management of hypertensive crises
Neurological emergencies
Subarachnoid haemorrhage, acute intracerebral haemorrhage, hypertensive encephalopathy, and acute ischemic stroke require rapid BP reduction. In hypertensive encephalopathy, reduce the mean arterial pressure (MAP) 25% over 8 hours. Labetalol, Nicardipine and Esmolol are the preferred medications; Nitroprusside and Hydralazine should be avoided25.
For acute ischemic stroke, the preferred medications are Labetalol and Nicardipine. The target BP is < 185/110 mm Hg especially if the patient is receiving fibrinolysis25.
In acute intracerebral haemorrhage, Labetalol, Nicardipine and Esmolol are preferred; avoid Nitroprusside and Hydralazine. If signs of increased intracranial pressure (ICP) exist, keep SBP < 180 mm Hg, while maintain SBP < 160 mm Hg in patients without increased ICP for the first 24 hours after onset of symptoms25. Early intensive BP control is recommended to reduce hematoma growth26,27.
In subarachnoid haemorrhage, Nicardipine, Labetalol and Esmolol are also the preferred agents; while Nitroprusside and Hydralazine should be avoided. Maintain the SBP < 160 mm Hg until the aneurysm is treated or cerebral vasospasm happens25.
Cardiovascular emergencies
Rapid BP reduction is also indicated in cardiovascular emergencies such as aortic dissection, acute heart failure, and acute coronary syndrome. Labetalol, Nicardipine, Nitroprusside (with beta-blocker), Esmolol, and Morphine are preferred in aortic dissection. Beta-blockers should be avoided if there is aortic valvular regurgitation or suspected cardiac tamponade. Keep the SBP < 110 mmHg unless signs of end-organ hypoperfusion exists28.
In acute coronary syndrome if the BP is >160/100 mm Hg, Nitroglycerin and beta blockers are used to lower the BP by 20-30% of baseline but, thrombolytics are avoided if the BP is >185/100 mm Hg28. In acute heart failure use intravenous Nitroglycerin and intravenous Enalaprilat. Give vasodilators (besides diuretics) when SBP is 140 mm Hg28.
Cocaine toxicity/Pheochromocytoma
Diazepam, Phentolamine and Nitroglycerin/Nitroprusside are the preferred drugs. In cocaine toxicity, tachycardia and hypertension rarely require specific treatment. Phentolamine is proper for cocaine-associated acute coronary syndromes.In pheochromocytoma, beta blockers can be added after alpha blockade for BP control29.
Pre-eclampsia/eclampsia
The proper medications are Hydralazine, Nifedipine and Labetalol however avoid Nitroprusside, Esmolol and angiotensin-converting enzyme inhibitors. The BP should be <160/110 mm Hg in the antepartum period and during delivery. The BP should be maintained below 150/100 mm Hg if the platelet count is less than 100,000 cells mm3. Intravenous Magnesium Sulphate should also be used to prevent seizures30.
Perioperative hypertension
Nitroprusside, Nitroglycerin and Esmolol are used. Target the perioperative BP to within 20% of the patient's baseline pressure. Perioperative beta blockers are best to use in patients undergoing vascular procedures or at risk of cardiac complications28.
CONCLUSION
Perioperative hypertension commonly occurs in patients undergoing surgery. The permitted value is based on the patient’s preoperative BP. It is approximately 10% above that baseline however more reduction in BP may be warranted for patients at high risk of bleeding or with severe cardiac problems. Accurate adjustment of treatment and monitoring of patient’s response to therapy are essential to safe and effective management of perioperative hypertension.
Striae distensae, or stretch marks, are linear scars in the dermis which arise from rapid stretching of the skin over weakened connective tissue. It is a common skin condition that rarely causes any significant medical problems but is often a significant source of distress to those affected. Striae distensae were described as a clinical entity hundreds of years ago, and the first histological descriptions appeared in the medical literature in 1889.1 With a high incidence and unsatisfactory treatments, stretch marks remain an important target of research for an optimum consensus of treatment. These appear initially as red, and later, as white lines on the skin, representing scars of the dermis, and are characterized by linear bundles of collagen lying parallel to the surface of the skin, as well as eventual loss of collagen and elastin. The estimated prevalence of striae distensae range from 50 to 80%.2,3 The anatomical sites affected vary, with areas commonly affected including the abdomen, breasts, thighs and buttocks.4 The three maturation stages of striae include the acute stage (striae rubra) characterized by raised, erythematous striae, the sub-acute stage characterized by purpuric striae, and the chronic stage (striae alba), characterized by white or hypo-pigmented, atrophied striae.5 Although stretch marks are only harmful in extreme cases, even mild stretch marks can cause distress to the bearer6 (Table 1).
Table 1: Histological comparisons between striae rubrae and striae albae
Epidermis
Oedema Increased melanocytes
Epidermal atrophy Loss of rete ridges Decreased melanocytes
Papillary dermis
Dilatation of blood vessels
No vascular reaction
Reticular dermis
Structural alteration of collagen fibres Reduced and reorganized elastic fibres Fine elastic fibres in dermis
Densely packed collagen parallel to skin surface. Thick elastic fibres in dermis
Inflammatory cells
Lymphocytes and fibroblasts
Eosinophills
Aetiology
Striae may result from a number of causes, including, but not limited to, rapid changes in weight, adolescent growth spurts, corticosteroid use or Cushing Syndrome, and generally appear on the buttocks, thighs, knees, calves, or lumbosacral area.7 In addition, approximately 90% of all pregnant women develop stretch marks either on their breasts and/or abdomen by the third trimester.8 Genetic predisposition is also presumed, since striae distensae have been reported in monozygotic twins.9,10 There is decreased expression of collagen and fibronectin genes in affected tissue.11 The role of genetic factors is further emphasised by the fact that they are common in inherited defects of connective tissue, as in Marfan’s syndrome.12,13 Obesity and rapid increase or decrease in weight have been shown to be associated with the development of SD.14 Young male weight lifters develop striae on their shoulders.15 Striae distensae also occurs in cachetic states, such as tuberculosis, typhoid and after intense slimming diets.16 Rare etiologies include human immunodeficiency virus positive patients receiving the protease inhibitor indinavir and chronic liver disease.13,15 A case of idiopathic striae was also reported.17
Rosenthal18 proposed four aetiological mechanisms of striae formation: insufficient development of tegument, including elastic properties deficiency; rapid stretching of the skin; endocrinal changes; and other causes, possibly toxic.
Pathogenesis
The pathogenesis of striae is unknown but probably relates to changes in the components of extracellular matrix, including fibrillin, elastin and collagen.19 There has been emphasis on the effects of skin stretching in the pathogenesis of striae because the lesions are perpendicular to the direction of skin tension.20 A possible role of glucocorticoids in the pathogenesis of striae has been suggested because of an increase in the levels of steroid hormones and other metabolites found in patients exhibiting striae.21 There are studies suggesting the role of fibroblasts in the pathogenesis of striae. Compared to normal fibroblasts, expression of fibronectin and both type I and type III procollagen were found to be significantly reduced in fibroblasts from striae, suggesting that there exists a fundamental aberration of fibroblast metabolism in striae distensae.22
Pathological aspects
The earliest pathological changes are subclinical to be detected by electron microscopy only. These changes include mast cell degranulation and the presence of activated macrophages in association with mid-dermal elastolysis.23 When the lesions become become clinically visible, collagen bundles start showing structural alterations, fibroblasts become prominent, and mast cells are absent.23 On light microscopic examination, Inflammatory changes are conspicuous in the early stage, with dermal oedema and perivascular lymphocytic cuffing.24 In later stages, there is epidermal atrophy, loss of rete ridges and other appendages including hair follicles are absent.25
Evaluation of striae distensae
Approaches to evaluating SD severity visually include the Davey 26 and Atwal scores,27 although these have not been validated specifically for SD. An objective evaluation of SD may be carried out using skin topography, imaging devices including three-dimensional (3D) cameras, reflectance confocal microscopy and epiluminescence colorimetry.28,29,30
Table 2: Visual scoring systems for the assessment of striae distensae
Davey method
Used for evaluating striae rubrae and albae. Divide the abdomen into quadrants using midline vertical and horizontal lines. Each quadrant given a score (0 no SD; 1 moderate number of SD; 2 many SD). Score given out of 8.
Atwal score
Used for evaluating striae rubrae and albae. Six sites chosen (abdomen, hips, breasts, thigh/buttocks). Each site given a maximum score of six. Total score out of 24. Score 0–3 for the presence of striae (0 no SD; 1 < 5 SD; 2 5–10 SD; 3 > 10 SD). Score 0–3 for the presence of erythema (0 no erythema; 1 light red/pink; 2 dark red; 3 purple).
Management
Striae distensae (striae alba) is a very challenging cosmetic problem for dermatologists to treat. Various modalities of treatment have been tried. Although therapeutic strategies are numerous, there is no treatment which consistently improves the appearance of striae and is safe for all skin types.31 Weight loss by diet alone or a combination of diet and exercise do not change the degree of striae distensae.32
Topical treatments
Topical tretinoin (0.1%) ameliorates striae and the improvement may persist for almost a year after discontinuation of therapy.33 More recently, tretinoin has been shown to improve the clinical appearance of stretch marks during the active stage (striae rubra), although with not much effect during the mature stage (striae alba).34 Some of the studies have proven the inefficacy of the vitamin A derivative in the treatment of SD, but most of the patients included in these early studies presented with old lesions that had evolved into whitish atrophic scars.35 A study comparing topical 20% glycolic acid and 0.05% tretinoin versus 20% glycolic acid and 10% L-ascorbic acid, found that both regimens improved the appearance of striae alba.36
Hydrant Creams: 1) Trofolastin (a cream containing Centella asiatica extract, vitamin E, and collagen-elastin hydrolysates). The exact mechanism of action was identified as the stimulation of fibroblastic activity 37 and an antagonistic effect against glucocorticoids.38 2) Verum (a cream containing vitamin E, panthenol, hyaluronic acid, elastin and menthol). The results suggest that the product may show the benefit of massage alone.39 3) Alphastria (a cream composed of hyaluronic acid, allantoin, vitamin A, vitamin E, and dexpanthenol). Only one study was conducted, which concluded that the product markedly lowered the incidence of stretch mark development after pregnancy.40
Glycolic acid (GA): The exact mechanism of action of GA in the management of striae distensae is still unknown because, although GA is reported to stimulate collagen production by fibroblasts and to increase their proliferation in vivo and in vitro, which may be useful for the treatment of stretch marks.41,42 A study comparing topical 20% glycolic acid and 0.05% tretinoin versus 20% glycolic acid and 10% L-ascorbic acid, found that both regimens improved the appearance of striae alba.43
Trichloroacetic acid (TCA; 10–35%): It has been used for many years as a treatment option for striae distensae and is repeated at monthly intervals with reported improvement in texture and color of marks.44
Other topical products: Several oils have been used in the prevention of SD. A non-randomized, comparative study investigated the effect of almond oil in the prevention of SD in which they noted significant differences in the frequency of SD between the groups (almond oil and massage 20%, almond oil alone 38.8%, control 41.2%).45
Overall, there is limited evidence for the efficacy of topical therapy for the treatment of SD.
Microdermabrasion
Microdermabrasion may improve many skin problems including acne scars, skin texture irregularities, mottled pigmentation and fine wrinkles. Karimipour et al reported that microdermabrasion induces epidermal signal transduction pathways associated with remodelling of the dermal matrix.46 However, studies documenting the efficacy of rnicrodermabrasion in treatment of striae are lacking. Published in 1999, a book on microdermasion written by a French dermatologist, Francois Mahuzier, and translated to English, has a chapter "Microdermabrasion of stretch marks”.47 The author states that 10-20 sessions of microdermabrasion at an interval of not less than 1 month, each session resulting in bleeding points, provide satisfactory results. The author concludes that, "microdermabrasion is the only effective treatment of stretch marks today."
Lasers
Lasers have recently become a popular therapeutic alternative to ameliorate and improve the appearance of stretch marks. Most commonly used lasers used include pulsed-dye laser (PDL), short- pulse carbon dioxide and erbium-substituted yttrium aluminium garnet (YAG), neodymium- doped YAG (Nd:YAG), diode, and Fraxel.
Pulsed dye laser: The dilated blood vessels render the striae rubrae a good candidate for PDL.48 The 585- nm pulsed dye laser has a moderate beneficial effect in the treatment of striae rubra.49 To evaluate the effectiveness of the 585-nm flashlamp-pumped pulse dye laser in treating cutaneous striae, 39 striae were treated with four treatment protocols.50 Subjectively, striae appeared to return toward the appearance of normal skin with all protocols. Objectively, shadow profilometry revealed that all treatment protocols reduced skin shadowing in striae. Laser treatment of SD should be avoided or used with great caution in darker skin types (IV–VI), because of the possibility of pigmentary alterations after treatment.51
Excimer laser: Studies have shown temporary repigmentation and improvement of leukoderma in SD with excimer laser, although it failed to show any improvement in skin atrophy.52,53 To evaluate the true efficacy of the 308-nm excimer laser for darkening striae alba, 10 subjects were treated using the excimer laser on the white lines of striae, while the normal skin near to and between the lines was covered with zinc oxide cream. The results of this study showed the weakly positive effect of the 308-nm excimer laser in the repigmentation of striae alba.54
Copper Bromide laser: copper-bromide laser (577-511 nm) has been used for stretch marks. A clinical study was conducted in 15 Italian women with stretch marks, treated with the CuBr laser (577-511 nm) and followed-up for 2 years.55 The results of the study concluded that the copper-bromide laser was effective in decreasing the size of the SD and there were some pathogenic considerations that justified the use of this laser.
1,450-nm Diode Laser: The non-ablative 1,450-nm diode laser has been shown to improve atrophic scars and may be expected to improve striae. To evaluate the efficacy of the 1,450-nm diode laser in the treatment of striae rubra and striae alba in Asian patients with skin types 4-6, striae on one half of the body in 11 patients were treated with the 1,450-nm diode laser with cryogen cooling spray with the other half serving as a control.56 None of the patients showed any noticeable improvement in the striae on the treated side compared to baseline and to the control areas. The study concluded that the non-ablative 1,450-nm diode laser is not useful in the treatment of striae in patients with skin types 4, 5, and 6.
1,064-nm Nd:YAG Laser: A study was aimed to verify the efficacy of this laser in the treatment of immature striae in which 20 patients with striae rubra were treated using the 1,064-nm long-pulsed Nd:YAG laser.57 A higher number of patients (55%) considered the results excellent when compared to the same assessment made by the doctor (40%).
Intense Pulsed Light: In order to assess the efficacy of IPL in the treatment of striae distensae, a prospective study was carried out in 15 women, all of them having late stage striae distensae of the abdomen.58 All the study subjects showed clinical and microscopical improvement after IPL. It seems to be a promising method of treatment for this common problem with minimal side-effects, a wide safety margin and no downtime.
Fractional Photothermolysis: To determine the efficacy of fractional photothermolysis in striae distensae, 22 women with striae distensae were treated with two sessions each of fractional photothermolysis at a pulse energy of 30 mJ, a density level of 6, and eight passes at intervals of 4 weeks and response to treatment was assessed by comparing pre- and post-treatment clinical photography and skin biopsy samples.59 Six of the 22 patients (27%) showed good to excellent clinical improvement from baseline, whereas the other 16 (63%) showed various degrees of improvement. This study concluded that Fractional photothermolysis may be effective in treating striae distensae, without significant side effects.
Ablative 10,600-nm carbon dioxide fractitional laser: Ablative 10,600-nm carbon dioxide fractional laser systems (CO₂ FS) have been used successfully for the treatment of various types of scars. To assess the therapeutic efficacy of CO₂ FS for the treatment of striae distensae, 27 women with striae distensae were treated in a single session with a CO₂ FS and clinical improvement was assessed by comparing pre- and post-treatment clinical photographs and participant satisfaction rates.60 The evaluation of clinical results 3 months after treatment showed that two of the 27 participants (7.4%) had grade clinical 4 improvement, 14 (51.9%) had grade 3 improvement, nine (33.3%) had grade 2 improvement, and two (7.4%) had grade 1 improvement. None of the participants showed worsening of their striae distensae.To assess and compare the efficacy and safety of nonablative fractional photothermolysis and ablative CO(2) fractional laser resurfacing in the treatment of striae distensae, 24 ethnic South Korean patients with varying degrees of atrophic striae alba in the abdomen were enrolled in a randomized blind split study and were treated with 1,550 nm fractional Er:Glass laser and ablative fractional CO(2) laser resurfacing.61 These results of the study support the use of nonablative fractional laser and ablative CO(2) fractional laser as effective and safe treatment modalities for striae distensae of Asian skin with neither treatment showing any greater clinical improvement than the other treatment.
UVB/UVA1 Combined Therapy: Besides lasers, light sources emitting ultraviolet B (UVB) irradiation have been shown to repigment striae distensae. A study was conducted on 9 patients with mature striae alba who received 10 treatment sessions, and biopsies were taken at the baseline and end of the study.62 At the end of the study, all patients reported some form of hyperpigmentation that was transient and did not affect any surrounding tissues. No changes were seen on biopsy to indicate an effective remodelling collagen effect of the device, although it needs further assessment. Another study was conducted to analyse the histologic and ultrastuctural changes seen after UVB laser- or light source-induced repigmentation of striae distensae in which analyses of biopsied skin after treatment with both the UVB laser and light source showed increased melanin content, hypertrophy of melanocytes, and an increase in the number of melanocytes in all patients.63
Radiofrequency devices: RF devices are based on the principle of heat generation that occurs in response to poor electrical conductance according to Ohm’s law (heat generation is directly correlated with tissue resistance). The heat that is generated is sufficient to cause thermal damage to the surrounding connective tissue,64 which is responsible for the partial denaturation of pre-existing elastic fibers and collagen bundles.65 Initial collagen denaturation within thermally modified deep tissue is thought to represent the mechanism for immediate tissue contraction; subsequent neocollagenesis further tightens the dermal tissue and reduces striae.66 The efficacy and safety of combination therapy with fractionated microneedle radiofrequency (RF) and fractional carbon dioxide (CO2) laser in the treatment of striae distensae has been evaluated revealing that this combination therapy is a safe treatment protocol with a positive therapeutic effect on striae distensae.67 A recent study evaluating the effectiveness of a RF device in combination with PDL subjected 37 Asian patients with darker skin tone with SD to a baseline treatment with a RF device and PDL.68 All histological evaluations demonstrated an increase in the amount of collagen fibers, and six of the nine specimens showed an increase in the number of elastic fibers.TriPollar RF device appears to be a promising alternative for the treatment of striae distensae in skin phototypes IV-V.69
Needling therapy:
To evaluate the effectiveness and safety of a disk microneedle therapy system (DTS) in the treatment of striae distensae, 16 Korean volunteers with striae distensae alba or rubra were enrolled which received three treatments using a DTS at 4-week intervals.70 Marked to excellent improvement was noted in seven (43.8%) patients, with minimal to moderate improvement in the remaining nine. This study revealed that Disk microneedle therapy system (DTS) can be effectively and safely used in the treatment of striae distensae without any significant side effects. Another study assessed and compared the efficacy and safety of needling therapy versus CO2 fractional laser in treatment of striae and the results supported the use of microneedle therapy over CO2 lasers for striae treatment.71
Platelet-rich plasma:
Platelet-rich plasma has these wound-healing properties, affecting endothelial cells, erythrocytes, and collagen,72 which potentially aids in the healing of the localized chronic inflammation believed to be a factor in the aetiology of striae distensae. Platelet-rich plasma is well tolerated by the patients and is a safe and cost effective treatment option for striae distensae.
Platelet-rich plasma alone is more effective than microdermabrasion alone in the treatment of striae distensae, but it is better to use the combination of both for more and rapid efficacy.73
The plasma fractional radiofrequency and transepidermal delivery of platelet-rich plasma using ultrasound has also been found to be useful in the treatment of striae distensae.74
Since thermal damage from intradermal RF has characteristics similar to those of many wounds, combination treatment with intradermal RF and autologous PRP would eventuate in enhanced localized collagen neogenesis and redistribution. In one of the studies, three sessions of intradermal RF were used combined with autologous PRP administered once every four weeks.75 All of the participants showed satisfactory changes and no patient was reported to show no improvement.
Transepidermal retinoic acid:
Transepidermal retinoic acid delivery using ablative fractional radiofrequency associated with acoustic pressure ultrasound has also been used for the treatment of stretch marks.76
Conclusion
Striae distensae are an extremely common, therapeutically challenging form of dermal scarring. Adequate scientific knowledge and the evidence behind both preventative and therapeutic agents are vital in order to understand striae and to offer patients the best therapeutic options. The treatment of this cosmetically distressing condition has been disappointing and there is no widely accepted surgical procedure for improving the appearance of stretch marks. Laser therapy has been advocated as a treatment for striae distensae.
The increasing collaboration between diabetologists and general practitioners (GPs) (e.g. the IGEA project) has resulted in the GP taking a more relevant role in management of patients with diabetes. Just as measurement of arterial blood pressure has become an important tool in follow-up of patients with hypertension by the GP, SMBG has become a valuable tool to evaluate glycaemic control. In particular, self-monitoring of both blood pressure and glycaemia are important to assess the efficacy of prescribed therapies, and can help the patient to better understand the importance of control of blood pressure and blood glucose.
Several instruments for measurement of blood pressure have been validated by important medical societies involved in hypertension, and much effort has been given to compliance and patient comfort. However, less attention has been dedicated to glucometers. In particular, little consideration has been given to patient compliance, and SMBG is often perceived as an agonising experience. Moreover, hourly pre-visit glucose curves for glycaemic control, even if important, do not have the same value as a standard control over 2 to 3 months between visits. In addition, after an initial period of "enthusiasm" the fear and hassle of pricking oneself and the unpleasant feeling of pain often cause the patient to abandon SMBG.
A literature search on PubMed using the term “self-measurement of blood glucose (SMBG) and pain” retrieved only two publications, demonstrating a general lack of interest of the medical community. However, SMBG can be of important diagnostic-therapeutic value. Pain related to skin pricks on the fingertip, needed for determination of glucometric blood glucose, can significantly reduce compliance to SMBG, thus depriving the physician of a useful tool for monitoring the efficacy of anti-hyperglycaemic therapy and glycaemic control. Moreover, HbA1c has clear limitations, even if it provides a good idea of glycaemic control over the past 2-3 months, as it is a mean value of pre- and post-prandial blood glucose. It does not, therefore, measure glycaemic variability, which is an important cardiovascular risk factor. Thus, more research is needed into puncture sites as an alternative to the fingertip that are associated with less pain, which could favour greater use of SMBG.
Another problem of significant importance concerns the reproducibility and accuracy of blood glucose measurements. In the traditional method, blood samples for self-monitoring are taken from the fingertip of any finger using a lancing device with a semi-rigid prick (Figs. 1 and 2). The large blood vessels in the derma of the fingertip (Fig. 3) are lanced, and a drop of blood is obtained for the glucometer. All lances are optimised to prick the skin at a depth greater than 0.5 mm with a variability of ± 0.2 mm (Fig. 4).
Figure 1. The fingertip as a traditional site of puncture using a lancet.
Figure 2. Traditional method for self-monitoring of blood glucose.
Figure 3. Vascularisation of derma.
Figure 4. Traditional lancet.
Unfortunately, by pricking the fingertip at this depth, numerous tactile corpuscles in the dermis are also touched, causing the unpleasant sensation of pain. In a recent study by Koschinsky1 on around 1000 patients with type 1 (T1D) and type 2 diabetes (T2D), about one-half (51%) referred that they normally pricked themselves on the side of the fingertip because it is less painful. However, almost one-third (31%) used the centre of the fingertip, which is the site associated with the most pain. Other sites of puncture on the fingers are used much less frequently (5%), while 12% used other places on the body. It is also interesting to see how many times patients reused the lancet: 10% once, 19% for 2-4 times, 22% for 5-7 times, 25% for 8-10 times and 21% for more than 11 times. Pricking oneself 2 several times daily for years is not only troublesome for patients, but also leads to the formation of scars and callouses, and reduces fingertip perception and tactile sensitivity. Notwithstanding, alternative sites of puncture such as the arm, forearm and abdomen have not been evaluated in a systemic manner.
The objective of the present study is to compare alternative sites of puncture using a new semi-rigid lancet and determine if blood glucose values are similar to those obtained using traditional methods. A new puncture site was chosen, namely the area proximal to the nail bed of each finger. The sensation associated with puncture (with or without pain) was used to compare the two groups. Pain was assessed with a visual analogue scale (VAS). Blood glucose was measured in the morning after 12 hours of fasting.
Materials and methods
The present study enrolled 5 general practitioners and 70 patients with diabetes and without diabetes-related (micro-albuminuria, retinopathy, arterial disease of the lower limbs) complications. In addition, patients with diabetic neuropathy or neurological/vascular complications that could alter pain perception were excluded. The study population was composed of 20 women and 50 men with a mean age of 47.8 ± 15.3 years and a mean duration of diabetes of 11.4 ± 10.3 years; 34.3% had T1D and 65.7% had T2D. The study was carried out according to the standards of Good Clinical Practice and the Declaration of Helsinki. All patients provided signed informed consent for participation.
Semi-rigid lancets were provided by Terumo Corporation (Tokyo, Japan) and consisted in a 23-gauge needle that was remodelled to permit less painful puncture than a traditional lancet (Fig. 5). Punctures (nominal penetration from 0.2 to 0.6 mm) were made at a depth variation of ± 0.13 mm. In addition, a novel puncture site was used, namely the area proximal to the nail bed of each finger (Figs. 6-8). In this area of the finger, blood flow is abundant and it is easy to obtain a blood sample. Moreover, the area has fewer tactile and pain receptors than the fingertip, and thus when lanced less pain is produced.
Six fingers were used in a random fashion to evaluate puncture of the anterior part of the finger, the periungual zone and the lateral area of the fingertip (depth 0.2-0.6 mm), and compared to fingertip puncture at a depth of 0.6 mm. The sensation provoked by puncture (with or without pain) was used to compare groups. Pain was evaluated using a VAS ranging from ‘no pain’ to ‘worst pain imaginable’. The VAS is a unidimensional tool that quantifies the subjective sensation such as pain felt by the patient and considers physical, psychological and spiritual variables without distinguishing the impact of the different components.
Figure 5. New lancet
Figure 6. Proximal lateral area of the nail bed as a new site of puncture.
Figure 7. Method of lancing.
Figure 8. Site of lancing
Blood glucose was measured in the morning after 12 hours of fasting. The Fine Touch glucometer used was provided by Terumo Corporation (Tokyo, Japan). Statistical analysis was carried out using Fisher’s two-sided test. Differences in blood glucose with the two methods were analysed using Wilcoxon matched pairs signed ranks test. A P value <0.05 was considered statistically significant.
Results
Pain was not perceived in 90% and 94.28% of subjects punctured in the lateral area of the fingertip at a depth of 0.2 and 0.3 mm, respectively. At a depth of 0.4 mm, 67.14% of subjects did not perceive pain, while at 0.5 mm and 0.6 mm, 47.14% and 17.14% of subjects did not feel pain, respectively. There was no significant difference in pain considering punctures at 0.2 or 0.3 mm, while significant differences were seen between 0.2 and 0.4 mm (p <0.05), 0.5 mm (p <0.001) and 0.6 mm (p <0.001). All subjects who performed puncture in the central zone of the fingertip referred a painful sensation.
Using a periungual puncture site, pain was not referred by any subject, although a bothersome sensation was noted by some. The same results were obtained for all fingers used. Blood glucose levels obtained using traditional and alternative puncture sites were highly similar with no significant differences between groups (134.18 mg/dl ± 5.15 vs. 135.18 mg/dl ± 5.71 mg/dl; p = 0.5957).
Discussion
The present study evaluated the use of alternative puncture sites that are associated with less pain. These encouraging results undoubtedly warrant further investigation in a larger cohort, but nonetheless suggest that compliance with SMBG can be optimised. The use of the area close to the nail bed allowed high quality blood samples to be obtained for measurement of blood glucose, with an accuracy that was the same as that seen using the fingertip. The design of the lancet used herein was also associated with a lower perception of pain, which is composed of a hypodermic needle in a rigid casing that prevents accidental needle sticks both before and after use. Thanks to the needle point that was made using a triple-bevel cut, epidermal penetration is less traumatic and as a consequence less painful. This further favours rapid recovery of tactile function of patients with T2D. This allows the use of a larger transversal section using a puncture with less depth, and less involvement of nerves present in skin. In addition, the characteristics of the novel lancing device (Fine Touch, Terumo Corporation, Tokyo, Japan) allows adjusting the depth of puncture to the characteristics of each patient (e.g. in children, adolescents and adults).
The depth of penetration of the lancet can be varied from 0.3 to 1.8 mm with a self-incorporated selector; the maximum deviation of the lancing device in terms of depth is approximately 0.1 mm. Due to the possibility to select a minimal depth of only 0.3 mm, it can be used at alternative sites that allow a reduction in the frequency of samples taken from the fingertip. In theory, compared to traditional lancets, this would allow less perception of pain even at traditional sites as well as at periungual zones, and it was our intention to compare the different types of lancets to reinforce this idea. No puncture-related complications were reported, and another fundamental aspect that is not reported in other studies comparing traditional and alternative puncture sites is that no differences in blood glucose were observed.
In conclusion, it is our belief that a new type of finger lancet that decreases or eliminates pain associated with lancing merits additional consideration. Further studies are warranted on larger patient cohorts to confirm the present results. If validated, this would enable patients with diabetes - especially those who need to take several daily blood glucose samples - to perform SMBG with greater peace of mind and less distress.
Claimants in medical negligence cases are increasingly making use of negligent failure to warn of risk in claims for compensation following medical mishaps when an inherent risk in a medical procedure has manifested itself resulting in injury. In order to succeed the claimant must establish firstly that the failure to warn was negligent and secondly that the negligence has caused a loss. This paper focuses on causation in failure to inform cases but briefly considers the shift in judicial attitudes to the requirement to give warnings in order to explain how the duty to inform and the available remedies have diverged.
Members of the medical profession commonly believe that to find a negligent failure to inform has caused a loss to the claimant a court must be satisfied that the patient would not have consented to the treatment had they been told of the risk. This was probably true until 2004 when the House of Lords came to a surprising decision which has since received a mixed reception.
The Changing nature of the requirement to give warnings
In the early days of medical litigation whether non-disclosure amounted to negligence was left to the standards of the medical profession. A medical professional was under a duty to at least equal the standards of a reasonably skilled and competent doctor; this would be assumed if s/he had acted in accordance with a body of professional opinion. This is referred to as the Bolam test.[i] There was disquiet amongst academic lawyers that doctors were being allowed to set their own standards and over time the courts have been wrestling back control.[ii],[iii] Following the Recent Supreme Court ruling in Montgomery[iv] there is now no doubt that patient autonomy is paramount and the need to inform will now be judged by reference to a reasonable person in the patient’s position.
In Montgomery the claimant, a diabetic, alleged she had been given negligent advice during her pregnancy. In particular she was not warned of risk of shoulder dystocia, the inability of the baby’s shoulders to pass through the pelvis, assessed at 9-10% for diabetic mothers and not informed of the possibility of delivery by elective caesarean section. The Consultant responsible for her care gave evidence (at paragraph 13) that she would not routinely advise diabetic mothers of this risk because if mentioned, “most women will actually say, ‘I’d rather have a caesarean section.’” The Supreme Court in finding (at paragraph 87) for the claimant held, “The doctor is therefore under a duty to take reasonable care to ensure that the patient is aware of any material risks involved in any recommended treatment, and of any reasonable alternative or variant treatments. The test of materiality is whether, in the circumstances of the particular case, a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it.” Although expressed as, “a duty to take reasonable care,” the medical professional is expected to, “ensure,” that the patient has the requisite knowledge. The test in failure to inform cases now focuses, not on the actions of the medical professional but, on the patient’s knowledge of the risks.
Chester v Afshar[v]
On 21st November 1994 Mr Afshar carried out a microdiscectomy at three disc levels on Miss Chester. There was no complication during the operation and the surgeon was satisfied that his objectives had been met. When Miss Chester regained consciousness she reported motor and sensory impairment below the level of L2. A laminectomy shortly after midnight the next day found no cause and the surgeon’s only explanation was cauda equine contusion during the retraction of the L3 root and cauda equine dura during the L2/L3 disc removal. During the legal proceedings Miss Chester brought against Mr Afshar it was found that the operation carried an unavoidable 1-2% risk of cauda equine syndrome (CES) and that the surgeon had not warned the patient about this risk. It was further found that, had the warning been given, Miss Chester would have sought a second (and possibly third) opinion meaning that the operation would not have taken place on 21st November.
The surgeon and the patient did not agree what was said about the risks of the operation before consent was obtained but the issue was decided in favour of the patient: the surgeon had failed to give a proper warning about the risk of CES. In order to succeed in her claim Miss Chester needed to establish that this failure had caused her loss but her lawyers did not argue that she would have refused consent if she had been informed. They took a different approach; the 1-2% risk of CES is not patient specific and is realised at random. If warned of the risk Miss Chester would have sought a second opinion meaning that the operation would have happened at a later date and possibly with a different surgeon. This subsequent operation would have carried the same 1-2% risk of CES. The High Court of Australia had previously accepted (in a different case) that the claimant can satisfy the burden by showing that, if informed, s/he would have chosen a different surgeon with a lower risk of adverse outcome but there was no evidence in this case that by choosing another surgeon Miss Chester could have reduced the risk.[vi]
At the time Mr Afshar failed to advise Miss Chester of the risks two paths should have been open to her. She could choose to have the operation with the defendant on 21st November which resulted in CES or to seek a second opinion and undergo the operation at a later date giving her a 98-99% (a better than balance of probabilities) chance of avoiding CES. Thus the failure to inform did not increase the 2% risk of CES but the court found, as a matter of fact, that it did cause the CES. Although the physical harm that Miss Chester had suffered (because of the inevitable risk) did not fall within the scope of the doctor’s duty to inform (to allow the patient to minimise risk) a majority of the House of Lords felt that the surgeon should be held liable because otherwise the patient would be left without a remedy for the violation of her right to make autonomous decisions about treatment.
There are two leaps in Chester the first is the notion that negligence causes a loss if it induces the claimant to follow a path with an associated risk that is realised when they could have followed another path with exactly the same risk. The second is that violating a patient’s right to make autonomous decisions should, as a matter of policy, make the surgeon liable for personal injury which happens after the patient is deprived of their right to make a decision about treatment. The next two paragraphs will consider these leaps in turn.
Equally risky paths: The first leap
In Wright[vii] the patient had developed a streptococcus pyogenes infection that had seeded into her proximal femur resulting in osteomyelitis. Her admission to hospital was delayed for two days by the defendant clinic’s negligent handling of her first presentation. On admission to hospital the patient had the additional misfortune to receive woefully inadequate treatment resulting in septic arthritis and permanently restricted mobility. The patient took the questionable decision to sue the clinic but not the hospital. One of the patient’s arguments against the clinic was that had she been admitted to hospital without the two day delay she would have been treated by different staff who would, almost certainly, not have been negligent. The claimant argued that, as in Chester, although the clinic’s negligence did not increase the random risk of receiving negligent hospital care it had, as a matter of fact, caused the negligent care. Lord Justice Elias rejected this suggestion precisely because the delay had not increased the risk that the hospital would provide the patient with inadequate treatment. However, the other members of the Court of Appeal found for the patient but for another reason; given two extra days the hospital would probably have realised their mistakes and been able to correct them before any permanent harm resulted.
Violated autonomy and personal injury: The second leap
There have been attempts to expand the scope of the majority reasoning in Chester. In Meiklejohn[viii] the patient was treated for suspected non-severe acquired apastic anaemia with Anti Lymphocyte Globulin and Prednisolone the latter causing an avascular necrosis. At an initial consultation a blood sample was taken from the patient for “research purposes” but possibly to exclude dyskeratosis congenital, the condition from which he was actually suffering. The patient argued he had not given informed written consent to the taking of a blood sample for research purposes and that had he been told about the uncertainty in the diagnosis he would have delayed treatment pending the result of the blood test or asked to have been treated with Oxymetholone instead. He further argued these violations of his autonomy required that he be given a remedy for the injury which had actually occurred through a reasonable misdiagnosis of his rare condition. Lady Justice Rafferty sitting in the Court of Appeal dismissed this argument stating at paragraph 34 that, “Reference to [Chester] does not advance the case for the Claimant since I cannot identify within it any decision of principle.”
Conclusion
Courts deciding failure to warn cases have shifted the emphasis from the reasonable practices of the medical profession to the autonomy of the patient; from the duty of the medical professional to the rights of the patient. Medical professionals are now required to give enough information to allow a reasonably prudent patient to make an informed decision about their own treatment. While this change has been taking place there has been no corresponding revision of the remedies available when a patient’s autonomy is infringed. If autonomous decision making is to be properly protected a remedy should be vested in every patient who has had their autonomy infringed whether or not that patient has suffered physical injury; autonomy infringements should be actionable per se (without proof of loss) and result in the award of a modest solatium (a small payment representing the loss of the right to make an informed decision about treatment.) Under the present arrangements the wrong that the patient complains of (infringement of autonomy) is not what they are seeking damages for (personal injury.)
In a small way, the court in Chester has sought to close this gap between the patient’s right and the remedy available by extending the existing law and widened the circumstances in which damages can be recovered by a patient following an infringement of autonomy. Medical professionals who fail to warn patients of small risks may be held liable if disclosing the risk might cause the patient to delay treatment while further deliberations take place. Paradoxically it could conceivably be argued that medical professionals who fail to disclose significant risks (greater than 50%) should escape liability because the loss was more likely than not to happen anyway!
Both Chester extensions to the law have been tested independently in Wright and Meiklejohn and rejected but this does not mean that it has been overruled. The two subsequent cases were heard by the Court of Appeal which cannot overrule the House of Lords (now the Supreme Court.) Both cases were distinguished meaning that the court was satisfied that they were not factually the same as Chester. Clearly Wright is not concerned with rights to autonomy and Meiklejohn is a failure to warn of uncertainties in diagnosis or failure to obtain written informed consent to research rather than risks inherent in treatment. If the facts of Chester were to come before the Courts again the decision would have to be the same; a surgeon could not necessarily escape liability by proving that, informed of the risk, the patient would have consented to the operation.
Summary points
Patients have a right to be informed of material risks inherent in medical treatment
An injured patient does not necessarily need to prove they would not have consented to the operation if the risks had been disclosed
A legal claim against a health care professional may be successful if the patient would have delayed the operation to a later date
This extension of the law has critics but the situation is unlikely to change in the near future
Drug abuse is a universal phenomenon and people have always sought mood or perception altering substances. Similarly the attitude of people towards addiction varies depending upon various factors and can come across as prohibition and condemnation to tolerance and treatment1. The United Nations Narcotics Bureau describes drug abuse as the worse epidemic in the global history 2.India like rest of the world has huge drug problem. Located between two prominent drug producing hubs in the world, i.e. Golden Triangle (Burma, Laos and Thailand) and Golden Crescent (Iran, Afghanistan and Pakistan), India acts as a natural transit zone and thus faces a major problem of drug trafficking. Similarly the geographic location of Jammu and Kashmir is such that the transit of drugs is easily possible across the state. In addition the prevailing turmoil is claimed to have worsened the drug abuse problem alongside an unusual increase in other psychiatric disorders in Kashmir 3.
There are not many studies about drug use from Kashmir and hardly any about the actual community prevalence. In addition, it is difficult to conduct a study in a community affected by drug abuse due to stigma associated with drug addiction. Furthermore people hesitate to volunteer information due to laws prohibiting sale and purchase of such substances and risk of being criminally charged. In view of this difficulty the present study was conducted on the treatment seeking patients at the Drug De-addiction Centers. The present study was aimed at highlighting the epidemiological profile and pattern of drug use in Kashmir Valley.
Material and Methods
This cross-sectional study was undertaken at two Drug De-addiction Treatment Centers (Government Psychiatric Disease Hospital and Police Hospital, Srinagar). Government Psychiatric Disease Hospital is the only psychiatric hospital in the Kashmir valley that also provides treatment for substance use disorder patients. The De-addiction center at the Police Hospital is run by Police Department in the capital city Srinagar. Both these centres have a huge catchment area comprising all districts of the valley, due to lack of such services outside the capital city, thus reflecting the community scenario to a greater extent.
The study was conducted for a period of one year from July 2010 to June 2011. Substance Use Disorder Patients were diagnosed as per the Diagnostic and Statistical Manual-IV (DSM IV 2004) criteria 4. Following informed consent, a total of 125 patients were included in the study. In case of minors (<18 years of age), the consent was obtained from the guardian. Information was collected regarding the age, sex, residence, religion, marital status, educational status, history of school dropout, occupation and type of family, reasons for starting the substance of abuse, type of the substance abused, and age of initiation. The socio-economic status of the patients was evaluated by using the modified Prasad’s scale for the year 2010, based on per capita income per month 5.
Results
A total of 125 Substance Use Disorder patients were studied and all were males. The majority of the patients (50.4%) were in the age group of 20-29 years and most (73.6%) were unmarried. Most of the patients were Muslims (96%). There was nearly an equal urban to rural ratio. Most of the patients had completed their educationup to high school level or higher. There was a high rate of school dropouts (41.7%) and among those, substance use being common reason (46%) for school dropout. 71.2% belonged to nuclear families. Most of the patients (53.6%) belonged to socio-economic class I as per Prasad’s scale [Table 1]. Majority of the patients started taking substances in the age group of 10-19 years [Table 2]. Besides nicotine (89.6%), the most common substances used were cannabis (48.8%), codeine (48%), propoxyphene (37.6%), alcohol (36.8%) and benzodiazepines (36%) [Table3].
Table 1: Socio-demographic profile
N
%
Age (years)
10 to 19
20
16.0
20 to 29
63
50.4
30 to 39
27
21.6
40 to 49
12
9.6
≥ 50
3
2.4
Gender
Male
125
100.0
Religion
Islam
120
96.0
Sikh
3
2.4
Hindu
2
1.6
Residence
Urban
56
44.8
Rural
69
55.2
Marital Status
Unmarried
92
73.6
Currently Married
27
21.6
Separated/Divorced
6
4.8
Education
Illiterate
5
4.0
</= high school
71
56.8
> high school
49
39.2
Occupation
Unemployed
21
16.8
Student
25
20.0
Government Job
16
12.8
Self employed
63
50.4
Type of family
Joint
36
28.8
Nuclear
89
71.2
Socio-economic status
Class I
67
53.6
Class II
36
28.8
Class III
18
14.4
Class IV
3
2.4
Class V
1
0.8
Table 2: Age at onset of initiation of Substance use by the patients seeking treatment for Substance Use disorder
Substance
< 10 years
10 to 19 years
> 19 years
N
%
N
%
n
%
Nicotine
11
9.8
86
76.8
15
13.4
Volatile Solvents
0
0
10
76.9
3
23.1
Cannabis
0
0
43
70.5
18
29.5
Codeine
0
0
33
55
27
45
Propoxyphene
0
0
24
51.1
23
48.9
Benzodiazepines
0
0
20
44.4
25
55.6
Alcohol
0
0
19
41.3
27
58.7
Table 3: Type of substance used by the patients seeking treatment for Substance Use disorder*
Table 4: Reason for starting the Substances among the patients seeking treatment for Substance Use disorder*
Reason
N
%
Peer Pressure
91
72.8
Relief from psychological stress**
49
39.2
Curiosity/Experimenting
27
21.6
Fun/Pleasure Seeking
13
10.4
Prescription medicine abuse***
12
9.6
Others****
6
4.8
*multiple responses ** (family tragedy like death or disease in the family; history of arrests, torture in jail or death and disability in the family due to the prevailing turmoil; conflicts within family; loss of job or job dissatisfaction. ***deliberate use of prescription medications for recreational purposes in order to achieve intoxicating or euphoric psychoactive effects, irrespective of prescription status ****Family history, routine work or boredom, availability.
Peer pressure was the most common (72.8%) reason for starting the use of substance [Table 4]. Majority of the patients started using substances in the age group of 10 to 19 years with 76.8% nicotine users, 76.9% volatile substances and 70.5% cannabis users among this group. The age of onset was higher (>19 years) in case of benzodiazepines and alcohol.
Discussion:
Kashmir Valley has a population of over 6 million with around 70% people living in rural areas.6
There is almost no data available on the community prevalence of drug use in the valley. Population is predominantly Muslim with strong taboo on use of alcohol and other drugs. Interestingly, none of the patients in our sample are female which could be due to stigma associated with drug use and hence reluctance to seek treatment. The police drug addiction centre is locally in the police lines with heavy security which requires frisking, which may also prevent people, especially women, from seeking help. This does not mean females do not use drugs as evident from clinical practice and previous studies 7. The sample is mostly comprised of a young age group of 20-29 years (50.4%) followed by 30-39 years (21.6%). Similar findings have been shown by the previous study conducted by Kadri et al.8 Another study on college going male students showed a prevalence of 37.5 %9, suggesting young age at initiation and high prevalence in students. The results also show high school dropout rate due to drug use which could be due to the associated problems with drug use and negative impact on the overall quality of life and future prospects.
There is a minor rural predominance in the sample. This is consistent with findings of Drug Abuse Monitoring System India and other studies 10-12, which reveal a nearly equal rural urban ratio with slight rural predominance. This could be due to the stigma associated with these centres and reluctance from local population to seek help due to fear of being identified and shamed.
73.6% of the patients were unmarried with 4.8% separated or divorced. Similar results have been shown by Hasin DS et al 13 and Martins SS et al14. The reason for predominant unmarried sample in our study could be due the higher number of younger age patients as compared to the current marriageable age.
The majority of the patients in our study were using cannabis, medicinal opioids (codeine and Propoxyphene), benzodiazepines and alcohol. One of the major reasons for high rate of opioids and benzodiazepines abuse in present study can be explained by over the counter sale of these drugs without the prescription from the doctor. This is a worrying trend as there is no proper drug control and it is easy to access any medication. Although there are only a few outlets selling alcohol in the whole of Kashmir, it is surprising how alcohol use is so common. It is speculated that current political turmoil may be responsible and people buy alcohol legally or illegally from army depots.
Most of the substance users had started taking drugs at the age of 10 to 19 years and more so in the case of nicotine, volatile substances and cannabis. Similar results have been found in the earlier studies. 15 Nicotine was typically the first substance of abuse. Tobacco is often considered as a gateway to other drugs 16.
The overall prevalence of volatile substance abuse in this study was 10.4% but significantly higher in the adolescent age group (53.8%). About three fourths of the patients had started using volatile solvents in the age group of 10-19 years. Inhalant use has been identified as most prevalent form of substance abuse among adolescents by different studies 17-18. The observation in present study could be explained by the easy accessibility, cheap price, faster onset of action, and a regular “high” with volatile substances like glues, paint thinners, nail polish removers, dry cleaning fluids, correction fluids, petrol, adhesives, varnishes, deodorants and hair sprays.
Peer pressure is the most common cause of initiation of drug use only to be followed by self-medication for psychological stress. Previous studies have shown similar results in relation to peer pressure and also the ongoing conflict situation to be responsible for increased drug use in the valley 19-20.
Conclusion:
There is a need for further studies to find the community prevalence of drug use. The service provision is very limited, restricted to the capital city and with none in the rural areas. There is a worrying trend of early age of initiation with adverse consequences including dropping out of school. The control of prescription drug use is another major issue which needs to be addressed. It is also worrying that female drug users are not able to seek help due to lack of appropriate facilities.
The clinical features of early HAT are well defined, yet the features of delayed HAT are less clear. Delayed HAT is a rare complication of OLT that may present with biliary sepsis or remain asymptomatic. Sonography is extremely sensitive for the detection of HAT in symptomatic patients during the immediate postoperative period. However, the sensitivity of ultrasonography diminishes as the interval between transplantation and diagnosis of HAT increases due to collateral arterial flow. MRA is a useful adjunct in patients with indeterminate ultrasound exams and in those who have renal insufficiency or an allergy to iodinated contrast.
In the absence of hepatic failure, conservative treatment appears to be effective for patients with HAT but retransplantation may be necessary as a definitive treatment.
Case Presentation:
A 52 year old male with a history of whole graft OLT for primary sclerosing cholangitis presented with two days of fever, nausea, and mild abdominal discomfort.
One week prior to presentation, he was seen in the liver clinic for regular follow-up. At that time, he was totally asymptomatic and his laboratory workup including liver function tests were within normal range.
He has undergone OLT three years prior. At the time of transplant he required transfusion of 120 units of packed red blood cells, 60 units of fresh frozen plasma and 100 units of platelets due to extensive intraoperative bleeding secondary to chronic changes of pancreatitis and severe portal hypertension, but had an otherwise uneventful postoperative recovery.
On physical examination the temperature was 39C, heart rate was 125 beats per minute, respiratory rate was 22 bpm. Initial laboratory workup revealed a white blood cell count of 25,000/mm3, AST of 6230 U/L, ALT of 2450 U/L, total bilirubin of 11 mg/dL , BUN 55 mg/dL and Creatinine of 4.5 mg/dL. Lactate level was 5 mmol/L. Doppler ultrasonography revealed an extensive intrahepatic gas (Image 1A). Computed tomography of the abdomen and pelvis revealed extensive area of hepatic necrosis with abscess formation measuring 19x14 cm with extension of gas into the peripheral portal vein branches (Image 1B,C). Upon admission to the hospital, the patient required endotracheal intubation, mechanical ventilator support and aggressively fluid resuscitation. He was started on broad-spectrum antibiotics and a percutaneous drain was placed that drained dark, foul smelling fluid. Cultures from the blood and the drain grew Clostridium perfringens.
Magnetic resonance imaging (MRI), MRA revealed occlusion of the hepatic artery 2 cm from its origin and also evidence of collaterals (Image 2A,B).
Image 1: (Pannel A) Doppler ultrasonography reveal extensive intrahepatic gas. (Pannel B&C) Computed tomography of the abdomen and pelvis reveal an extensive area of hepatic necrosis with abscess formation measuring 19x14 cm with extension of gas into the peripheral portal vein branches.
Image 2: MRI & MRA reveal occlusion of the hepatic artery 2 cm from its origin and also evidence of collaterals.
Following drain placement, the patient’s clinical condition markedly improved with significant reduction of liver function test values. Retransplantation was considered but delayed in the setting of infection and significant clinical and laboratory testing improvement.
The patient was transferred to the medical floor in stable condition, and the drain was then removed.
A week later the patient developed low grade fevers and tachycardia. One day later he began to experience mild abdominal discomfort and high grade fevers. Repeat CT of the abdomen revealed worsening hepatic necrosis and formation of new abscesses. His clinical condition decompensated quickly thereafter requiring endotracheal intubation, mechanical ventilation and aggressive resuscitation. Percutaneous drain was placed and again, drained pus-like, foul-smelling material. His overall condition deteriorated, and he eventually expired a few days later.
Discussion:
Delayed (more than 4 weeks after transplantation) HAT is a rare complication of OLT with an estimated incidence of at around 2.8%1.
Risk factors associated with development of HAT include Roux-en-Y biliary reconstruction, cold ischaemia and operative time, the use of greater than 6 units of blood, the use of greater than 15 units of plasma, and the use of aortic conduits on arterial reconstruction during transplant surgery2.
Collateralization is more likely to develop after Live Donor Liver Transplantation (LDLT) than after whole-graft cadaveric OLT3. Therefore, the latter is also associated with increased risk of late HAT.
Although the clinical features of early HAT are well described, the features of delayed HAT are less clearly defined1: the patient may present with manifestations of biliary sepsis or may remain asymptomatic for years. Right upper quadrant pain has been reported to occur in both immediate and delayed HAT. The clinical presentations may include recurrent episodes of cholangitis, cholangitis with a stricture, cholangitis and intrahepatic abscesses, and bile leaks1. Doppler ultrasonography has been extremely sensitive for the detection of HAT in symptomatic patients during the immediate postoperative period but becomes less sensitive as the interval between transplantation and diagnosis of HAT increases because of collateral arterial flow4.
3D gadolinium-enhanced MRA provides excellent visualization of arterial and venous anatomy with a fairly high technical success rate. MRA is a useful adjunct in patients with indeterminate ultrasonography examination in patients who have renal insufficiency or who have allergy to iodinated contrast 5.
Antiplatelet prophylaxis can effectively reduce the incidence of late HAT after liver transplantation, particularly in those patients at risk for this complication6. Vivarelli et al reported an overall incidence of late HAT of 1.67%, with a median time of presentation of 500 days; late HAT was reported in 0.4% of patients who were maintained on antiplatelet prophylaxis compared to 2.2% in those who did not receive prophylaxis6. The option of performing thrombolysis remains controversial. Whether thrombolysis is a definitive therapy or mainly a necessary step in the proper diagnosis of the exact etiology of HAT depends mostly on the particular liver center and needs further analysis7. Definitive endoluminal success cannot be achieved without resolving associated and possible instigating underlying arterial anatomical defects. Reestablishing flow to the graft can unmask underlying lesions as well as assess surrounding vasculature thus providing anatomical information for a more elective, better plan and definitive surgical revision7. Whether surgical revascularization compared to retransplantation is a viable option or only a bridging measure to delay the second transplantation has been a longstanding controversy in the treatment of HAT.
Biliary or vascular reconstruction do not increase graft survival and ongoing severe sepsis at the time of re-graft results in poor survival7. However, although uncommon, delayed HAT is a major indication for re-transplantation7. In the absence of hepatic failure, conservative treatment appears to be effective for patients with hepatic artery thrombosis.
C. perfringensis an anaerobic, gram-positive rod frequently isolated from the biliary tree and gastrointestinal tract. Inoculation of Clostridium spores into necrotic tissue is associated with formation of hepatic abscess8.
Necrotizing infections of the transplanted liver are rare. There have been around 20 cases of gas gangrene or necrotizing infections of the liver reported in the literature. Around 60% of these infections were caused by clostridial species with C. perfringens accounting for most of them. Around 80% of patients infected with Clostridium died, frequently within hours of becoming ill9,10. Those who survived underwent prompt retransplantation and the infection had not resulted in shock or other systemic changes that significantly decreased the likelihood of successful retransplantation8.
Because the liver has contact with the gastrointestinal tract via the portal venous system, intestinal tract bacteria may enter the liver via translocation across the intestinal mucosa into the portal venous system. Clostridial species can also be found in the bile of healthy individuals undergoing cholecystectomy9,10.
The donor liver can also be the source of bacteria. Donors may have conditions that favor the growth of bacteria in bile or the translocation of bacteria into the portal venous blood. These conditions include trauma to the gastrointestinal tract, prolonged intensive care unit admissions, periods of hypotension, use of inotropic agents, and other conditions that increase the risk of potential infection 8,9,10. C. perfringens sepsis in OLT recipients has been uniformly fatal without emergent retransplantation. Survival from C. perfringens sepsis managed without exploratory laparotomy or emergency treatment has been extremely rarely reported8. In those patients who survived, and in whom the infection has not resulted in shock or multiple organ failure, retransplantation may be successful8.
Although our patient survived his intensive care course, his recovery was tenuous as he quickly developed additional hepatic abscesses that led to his eventual demise. Post-mortem examination in our patient revealed intra-hepatic presence of Clostridium perfringens.
He was managed conservatively since he markedly improved both clinically and by liver function tests. Because of this, retransplantation was delayed. He was also already on antiplatelet prophylaxis.
Conclusion:
We report an interesting case of Clostridium perfringens hepatic abscess due to late HAT following OLT. Although the patient initially improved with non-surgical treatment, he eventually died. In similar cases, besides aggressive work-up and medical management retransplantation may be necessary for a better long term outcome.
Fear of physicians, injections, operations, the operation theatre and the forced separation from parents make the operative experience more traumatic for young children and can cause nightmares and postoperative behavioural abnormalities. Preanaesthetic medication may decrease the adverse psychological and physiological sequelae of induction of anaesthesia in a distressed child1. An important goal of premedication is to have the child arrive in the operating room calm and quiet with intactcardiorespiratoryreflexes. Various drugs have been advocated as premedication to allay anxiety and facilitate the smooth separation of children from parents. The idealpremedicantin children should be readily acceptable and should have a rapid and reliable onset with minimal side effects. Midazolam has sedative and anxiolytic activities, provides anterograde amnesia, and has anticonvulsant properties2. Ketamine, on the other hand, provides well-documented anaesthesia and analgesia. It has a wide margin of safety, as the protective reflexes are usually maintainedOral premedication with midazolam and ketamine became widely used inpaediatric anaesthesiato reduce emotional trauma and ensure smooth induction. It provided better premedication than either oral ketamine or midazolam alone4, but excessive salivation and hallucination were observed5.
Dexmedetomidine is a highly selective α2-adrenoreceptor agonist drug. Clinical investigations have demonstrated its sedative, analgesic and anxiolytic effects after IV administration to volunteers and postsurgical patients6. It has been used to sedate infants and children during mechanical ventilation and also to sedate children undergoing radiological imaging studies,8In the literature, few articles have used dexmedetomidine orally for the premedication of children. The purpose of this study is to evaluate the efficacy of dexmedetomidine when administered orally as a hypnotic and anxiolytic agent compared to oral combination ketamine/midazolam as preanaesthetic medication in paediatrics.
Methods:
The Hospital Ethics Committee approved the protocol. Written informed consent was obtained from parents prior to inclusion. Sixty six children of ASA physical status I or II, aged between 2 and 6 years and scheduled for elective minor surgery of more than 30 minutes expected duration were enrolled in this prospective, randomized, double-blind study. Exclusion criteria were: a known allergy or hypersensitivity reaction to any of the study drugs, organ dysfunction, cardiac arrhythmia or congenital heart disease, and mental retardation.
Children were randomly allocated to one of the two study groups using computer-generated random numbers. Group D received oral dexmedetomidine 3 μg/kg and group MK received 0.25 mg/kg oral midazolam (up to a maximum of 15 mg) with 2.5 mg/kg oral ketamine. The oral premedication was mixed with 3 ml of apple juice as a carrier to be given thirty minutes before induction of anaesthesia. The oral route was chosen as it is the most acceptable and familiar mode of drug administration. An independent investigator not involved in the observation or administration of anaesthesia for the children prepared all study drugs. Observers and attending anaesthetists who evaluated the patients for preoperative sedation and emergence from anaesthesia were blinded to the drug administered. Children had premedication in the preoperative holding area in the presence of one parent. All children received EMLA cream unless contraindicated.
After drugs were administrated, the following conditions were observed: 1) response to drug and onset of sedation, 2) response to the family separation circumstance and the entrance to the operating room, 3) response to the venous line (IV) insertion, 4) ease of mask acceptance during induction of anaesthesia. The time to recovery from anaesthesia and to achieve satisfactory Aldrete score were also noted. Onset of sedation was defined as the minimum time interval necessary for the child to become drowsy or asleep.
Sedation statuswas assessed every 5 min for up to 30 min with a five-point scale. A score of three or higher was considered satisfactory. In addition anxiolysis was assessed on a four-point scale. An anxiety score of three or four was considered satisfactory. Cooperation was assessed with a four-point scale. A cooperation score of three or four was considered satisfactory. Taste acceptability was evaluated on a four-point scale. A score of 1–3 was considered satisfactory.
Score
Sedation
Anxiolysis
Cooperation
Taste
1
Alert/active
Poor
Poor
Accepted readily
2
Upset/wary
Fair
Fair
Accepted with grimace
3
Relaxed
Good
Good
Accept with verbalcomplaint
4
Drowsy
Excellent
Excellent
Rejected entirely
5
Asleep
Heart rate, blood pressure, respiratory rate and arterial oxygen saturation were recorded before premedication, every five minutes for 30 min preoperatively, and then during induction of anaesthesia, every 5 min intra-operatively, every 15 min in recovery room and every 30 min in day-case unit until time of discharge.
The anaesthetic agents administered were standardized.Children were induced with sevoflurane, nitrous oxide in oxygen and fentanyl 1-2 µg/Kg and maintained with the same drugs. The trachea was intubated after administering cisataracurium 0.1 mg/kg.
At the end of the procedure, the neuromuscular blockade was reversed with neostigmine with glycopyrolate and the child was extubated. After that, they were kept in the recovery room (PACU) under observation until discharge. The time to recovery from anaesthesia and to achieve satisfactory Aldrete score were noted. The discharge time was also noted and postprocedure instructions were given. Children were called for checkups the following day, when parents were asked to answer a questionnaire about the surgical experience of the parent and child and side effects experienced, if any.
Statistical analysis was performed using SPSS version 17. All values were reported as mean ± SD and range. Data analysis for numerical data was performed by unpaired Student’s t-test to detect the differences between the groups for age, weight, onset of anxiolysis and sedation. Data analysis for categorical data was performed by Fisher’s exact test to detect differences for the scores. Other data are reported as mean ± SD or frequency (%). A P value < 0.05 was considered statistically significant. Prior to the study, we chose the null hypothesis (i.e. nosignificantsedation scores between the groups). The number of patients required in each group was determined using power analysis based on previous studies. Assuming that 79% of patients would become drowsy or asleep in the midazolam/ketamine group (15 patients), a sample size of 30 patients per group would have an 80% power of detecting a 20% difference in sedation (from 79% to 99%) at the 0.05 level ofsignificance. We decided to study 66 patients to account for possible dropouts.
Results:
Sixty-six patients were enrolled; four did not receive the study medication and two did not have surgery on the same day, leaving 60 subjects who fulfilled the criteria for the study.Groups were comparable regarding age, sex, weight, ASA physical status, surgical interventions and duration of anaesthesia (Table 1). Operative procedures were evenly distributed and included inguinalherniorrhaphy, hydrocele repair or orchidopexy.
Table 1: Demographic characteristics and duration of anaesthesia:
Group D
Group MK
No of patients
33
33
No of patients excluded
4
2
Age (years)
4.02±1.98
4.2±1.45
Gender (female/male)
13/16
15/16
ASA (I/II)
25/4
25/6
Weight (Kg)
17.72±4.4
16.56±5.1
Duration of Anaesthesia (min)
35.17±5.9
32.7±8.4
Data are expressed as mean ± SD (range). P > 0.05. No significant difference among groups. Dex group (D). Midazolam Ketamine group (MK). ASA, American Society of Anesthesiology physical status.
Onset of sedation was significantly faster after premedication with midazolam/ketamine (Fig1), and the level of sedation was significantly better after premedication with midazolam/ketamine 30 minutes after ingestion of the premedicant.
The anxiolysis score revealed 84 % of children in group MK as being friendly and only 51% of children in group D have similar behaviour (Table 2). The taste of oral dexmedetomidine was judged as significantly better; 13% of children rejected the oral midazolam/ketamine combination (Table 2).
Table 2: Distribution of behaviour and sedation status at time of induction:
Group D
Group MK
P
Time to onset of sedation (min)
24.52 ± 3.1
18.36 ± 2.6
0.015*
Preoperative sedation score
1.6±0.5
3.1±0.8
0.003*
% asleep at induction
61%
90%
0.024*
Preoperative anxiolysis score
1.4±0.6
2.9±0.7
0.016*
% Face mask acceptance
58%
88%
0.033*
% Venous line insertion acceptance
72%
90%
0.005*
% Satisfactory parental separation
50%
80%
0.04*
% Parental satisfaction
70%
90%
0.036*
% Taste acceptance
97%
87%
0.002*
Data are expressed as mean ± SD (range) or percentage. Dex group (D). Midazolam Ketamine group (MK). * significantP <0.05.
Application of a facemask at induction of anaesthesia was accepted more readily in patients of group MK (Fig 2).Overall, satisfactory cooperation with venous line insertion was found in 90% of children in group MK, while comparatively 72% of children in group D showed satisfactory cooperation with insertion of a venous line (Table 2). Moreover, most of the MK treated children were more calm and sedated than the D-treated group at the time of separation from parents. Parental satisfaction was significantly higher in group MK.
The time interval from end of surgery to spontaneous eye opening in the PACU was significantly less in group D (Fig 1), while the time to discharge from the PACU to ward was similar for groups (Table 3).
Table 3: Time to eye opening and PACU discharge
Group D
Group MK
P
Time to eye opening (min)
21±4.3
30±6.1
0.032*
Time of PACU discharge (min)
30± 3.9
28.12±5.5
0.316
Data are expressed as median ± SD (range). Dex group (D). Midazolam Ketamine group (MK). * significantP < 0.05.
While no child experienced respiratory complications or arterial oxygendesaturationbefore induction, heart rate and systolic blood pressure were marginally higher after administration of MK. On the other hand, the mean heart rate and systolic blood pressure measurements were 15% lower (than preoperative values) in group D at the same study periods. However, during recovery, haemodynamic responses were similar.
Adverse events were recorded for the three periods. Two children in group MK as well as one in group D experienced nausea but only one patient in group MK vomited before induction. Hallucination was recorded in 10 % of patients in group MK. Excessive salivation occurred in 12% of children receiving the combination of drugs, compared to 7% in D-treated children.
Discussion:
Our study proved that midazolam/ketaminereceiving patients were significantly calmer and more cooperative compared to dexmedetomidine receiving patients during the preoperative period, the insertion of a venous line, during separation from parents and also during the application of a facemask at induction. Several studies have been published demonstrating the advantage of the midazolam/ketamine combination in paediatric premedication4,9, while others have reported superiority of oral dexmedetomidine premedication to oral midazolam10,11.
Based on their experience with using oral dexmedetomidineas a preanaesthetic in children, Kamal et al10 and Zub et al 12 reported that the dose of 3 μg/kg could be safely and effectively applied without haemodynamic side effects.
Midazolam is currently the most commonly usedpaediatric premedication due to easy application, rapid onset, short duration of action and a lack of significant side effects13. Meanwhile oral ketamine was used in the 1970s by dentists to facilitate the treatment of mentally handicapped children. In 1982, Cetina found that rectal or oral preanaesthetic ketamine is an excellent analgesic and amnesic agent with no incidence ofdysphoric reactions, possibly related to its high rate of first-pass metabolism14. The metabolite norketamine has approximately one-third the potency of ketamine, but reaches higher blood concentration and also causes sedation and analgesia 15. The use of midazolam and ketamine in combination as a premedicant combines their properties of sedation and analgesia and attenuates drug induced deliriumGhai et al and Funk et al have also reported that a combination of midazolam and ketamine results in better premedication than the individual drugs given alone4,9.
Like clonidine, dexmedetomidine possesses a high ratio of specificity for the α2 versus the α1 receptor (200: 1 for clonidine and 1600: 1 for dexmedetomidine). Through presynaptic activation of the α2 adrenoceptor, it inhibits the release of norepinephrine and decreases sympathetic tone. There is also an attenuation of the neuroendocrine and haemodynamic responses to anaesthesia and surgery, thereby leading to sedation and analgesia16. One of the highest densities of α2 receptors has been detected in the locus coeruleus, the predominant noradrenergic nucleus in the brain and an important modulator of vigilance. The hypnotic and sedative effects of α2-adrenoceptor activation have been attributed to this site in the CNS16. This allows psychomotor function to be preserved while letting the patient rest comfortably, so patients are able to return to their baseline level of consciousness when stimulated17. Clonidine and dexmedetomidine seems to offer the beneficial properties, but dexmedetomidine has a shorter half-life, which might be more suitable for day surgery. Zuband his colleagues reported that dexmedetomidine may be an effective oral premedicant prior to anaesthesia induction or procedural sedation and it was effective even in patients with neurobehavioural disorders in whom previous attempts at sedation had failedAlso Sakurai et al reported that oral dexmedetomidine could be applied safely and effectively as a preanaesthetic in children18.
While dexmedetomidine is tasteless and odourless17 , with 82% bioavailability after extravascular doses in healthy human adults19, oral midazolam formulations have a bitter taste and were usually prepared by mixing the IV midazolam with a variety of sweet additives. In our study, children judged the taste of oral dexmedetomidine as significantly better than oral midazolam ketamine mixture, although both drugs were given with the same sweet tasting syrup. This observation probably might also reflect the developmental age of these patients and the difficulty of gaining their cooperation in swallowing something that they did not wish to swallow. Recently, new commercially prepared oral midazolam formulations are reported to be more palatable20, but unfortunately, it is not available yet in our country.
Our data confirmed that onset of sedation and peak sedative effect was significantly slower after oral dexmedetomidine compared to oral midazolam ketamine. These results are consistent with studies by Kamal et al and Schmidt et al who reported slow onset of action of oral dexmedetomidine,21In addition, Anttila et al reported that, in adults after oral administration, peak plasma concentration is achieved at 2.2 ± 0.5 h after a lag-time of 0.6 ± 0.3 h19.
In this study, dexmedetomidine premedication with the present study design resulted in slight hypotension and bradycardia, which could be attributed to postsynaptic activation of α2 adrenoceptors in the central nervous system (CNS) that inhibit sympathetic activity and thus can decrease blood pressure and heart rate22. In a finding consistent with our results, Khan et al and Aantaa et al reported that useofdexmedetomidine can beassociatedwithsome cardiovascular side effects including hypotension and bradycardia,24Conversely, Ray and Tobias did not find significant haemodynamic changes when used dexmedetomidine in providing sedation during electroencephalographic analysis in children with autism and seizure disorders25.
There were some limitations to this study; the bioavailability of oral dexmedetomidine is based on the adult dataWe need to decide the timing of the oral administration as apremedicantbased on the data in children. Therefore, the bioavailability of oral dexmedetomidine needs to be studied in children. The premedication period was 30 min, however, if a longer premedication period had been allowed, possibly more subjects could have attained satisfactory sedation at separation from parents and at induction of anaesthesia.
Conclusion:
In this study, premedication with oral midazolam/ketamineappeared to be superior to oral dexmedetomidine with evident haemodynamic stability and a higher degree of parental satisfaction demonstrated, although oral dexmedetomidinewas more accepted by the children. No significant side effects were attributable to either premedication. Emergence from anaesthesia was comparable between groups.
Payment by results was introduced across the National Health Service (NHS) in 2005. It’s aim was to provide a pricing structure (tariff) for the whole country with some allowance for geographical variation1-2. The system uses Healthcare Resource Group codes (HRG) in which treatments in similar cost brackets have the same codeA price / tariff is derived from each hospital patient episode and the patient’s registered Primary Care Trust (PCT) is billed accordingly.
In order to generate an HRG code data is collected by the hospital clinical coding department including primary diagnosis, comorbidity (which incurs an extra charge if applicable), and complications, surgical procedure, age and duration of stay4. Diagnoses (either primary, co morbidities or complications) are coded using ICD-10 codes. Surgical procedure is defined using OPCS-4 codesA piece if software is then utilised to allocate the HRG code. Each HRG code represents a tariff, which is the average cost of a treatment nationwide. Minor regional adjustments are made to reflect the cost of living2.
Payment by results covers all admissions, attendance in accident & emergency departments and outpatients attendances5. The 2004 NHS Improvement plan designated 18 weeks as a target for referral to treatment (RTT)6. It is a common misconception that trauma patients do not account for considerable income within the NHS. Trauma is often seen as the poor relation when compared with elective work where a target based culture now prevails. Elective targets must be met or hospital trusts can incur financial penalty. This situation is not apparent for trauma due to the acute nature of service delivery in the majority of cases. The burden of trauma work can block elective admissions and is seen by some as a barrier to target attainment. At least 36% of orthopaedic surgeons in the United Kingdom describe trauma as part of their sub-specialist interestWe aimed to assess the throughput and income generated from one week of trauma workload and compared this with the elective throughput in our unit for the same week. This was performed by means of a prospective study. We are not aware of any published work in this specific area.
Methods:
We followed all acute patients admitted to our trauma unit between 21/02/2008 and 28/02/2008. This represented a “trauma week” which is how the consultant rota is organised in our trust. We then compared this with the throughput in our elective unit for the same calendar period. No surgeons were on leave this week and no theatre sessions were cancelled other than the on call trauma consultant’s elective operating sessions. Our trust is a busy district general hospital with over 500 beds and approximately 55,000 emergency attendances per year. The orthopaedic directorate is staffed by ten full time consultants and serves a population of 315,000 patients.
All patient details were recorded prospectively and followed until the end of their inpatient episode. Case notes were then reviewed with the coding department and ICD-10 and OPCS-4 codes were generated. Their length of stay and other required variables were reviewed in order to generate the correct HRG code. Once the analysis was complete income for the trauma and elective groups were calculated.
Results:
Trauma:
48 patients were admitted (22 male) of which 36 required operative intervention. This utilised 14 theatre sessions. Mean age was 53.75 years (range: 7-93, median: 59). Median stay was 4 days with a mean of 13.3. The median and mean trim points (expected duration of stay before extra charges incurred by PCT) were 14.5 and 26.7 days respectively. Other consultants operated on 6 patients. This was either due to expertise in a specific area or space on an elective list utilised to reduce backlog. The income generated by these cases is included in the trauma total due to them being acute trauma interventions rather than elective cases. These results are summarised in tables 1 and 2.
Table 1: Demographic & Income Data of Trauma and Elective Patients
Trauma
Elective
Median age (yrs)
59
47
Number of Patients
47
71
No of Males
26
30
Median stay (days)
4
1
Range of stay (days)
1 – 107
1 - 7
Total bed days
637
118
Estimated Bed Costs (£)
203,840
26,550
Mean income per pt (£)
3658.32
2117.15
Total Income (£)
171,941
150,318
Table 2: Income by Anatomic Region
Trauma
Elective
Length of stay (median) days
No of pts
Total income (£)
Mean income per patient (£)
Length Of Stay (median) days
No of pts
Total income (£)
Mean income per patient (£)
Upper limb
1
18
32,455
1,803
1
9
11,469
1,274
Spine
1
5
10,327
2,065
0
34
44,887
1,320
Hip
26
13
90,891
5,494
4
12
43,660
3,638
Knee
5
5
19,576
3,915
2
12
45,434
3,786
Foot and ankle
6
7
18,692
2,670
1
4
4,868
1,217
Total
47
171,941
3658
71
150,318
2117
Of the 48 patients admitted 12 required no operative intervention. These cases were general ‘run of the mill’ admissions such as soft tissue infections for intravenous antibiotics, undisplaced fractures where home circumstances obstructed discharge, soft tissue injuries for further investigation and back pain. These will not be discussed further but the income generated (£31,127) does go towards the total. The median stay was 2 days with a mean stay 8.5 days (range: 1 – 47). This reflects the broad comorbidities and social circumstances of this subset.
The group requiring operative intervention included hip fractures (11 patients). Of these, seven required dynamic hip screw fixation but were deemed “complex” due to their comorbidities and therefore attracted the higher tariff rate (£6685). One displaced intracapsular fracture required total hip replacement, attracting a tariff of £7261. One patient required revision from a dynamic hip screw to an intramedullary device and then revision to a total hip arthroplasty. The tariff price was £19,479. The remaining fractured neck of femur patients attracted between £4379 and £6711 dependent on operative procedure. The median stay was 26 days (mean: 14, range 9 – 107). One patient required closed manipulation of a dislocated total hip replacement attracting a tariff price of £1034 and an inpatient stay of one day. In addition one acetabular fracture was sustained requiring open reduction and internal fixation. It attracted a tariff price of £4262 and an inpatient stay of seventeen days.
One patient required open reduction and internal fixation of a patella fracture attracting a tariff of £2405 and was an inpatient for 10 days. Another patient with septic arthritis required two arthroscopic knee washouts, attracting a tariff of £5941 and was an inpatient for 26 days.
Seven ankle fractures were admitted requiring operative intervention, all of these attracted a tariff of £2405 except one, which attracted £4262 due to co morbidity and complexity of injury. The median stay in this group was six days (mean: 4.9, range: 2-7).
Thirteen patients sustained hand and wrist injuries requiring operative intervention. Of these there were two tendon repairs, two abscesses drained and one digital terminalisation. Five wrist fractures required either manipulation and plaster application, closed reduction and Kirschner wiring or open reduction and internal fixation by means of a volar plate. Three fractures of the base of the thumb were manipulated and percutaneously K-wired. These patients attracted a tariff of between £1048 and £3227. Median stay was one day (mean: 1.36, range: 1 – 3). Three of these cases were managed by our hand surgeon on a trauma list.
One patient admitted with cauda equina syndrome required microdiscectomy attracting a tariff of £1271 and was an inpatient for one day. This was performed by one of our spinal surgeons on a trauma list.
Elective:
71 procedures were performed (36 female). This utilised 22 theatre sessions. Mean age was 49.51 years, (11 – 87 median: 47). Mean stay was 2.3 days. The median and mean trimpoints were 2 and 6.35 days respectively. Cases were divided by anatomical region. A table of income for both trauma and elective patients by anatomical region is included (Table 2).
Twelve patients had hip procedures performed. These included hip injections (n=2, tariff £615), sciatic nerve exploration (n=1, tariff £1217), cemented total hip arthroplasty (n=2, tariff £4304), uncemented total hip arthroplasty (n=1, £5305), resurfacing hip arthroplasty (n=5, £4023) and revision hip arthroplasty (n=1, £7185).
Twelve patients had knee procedures performed. These consisted of total knee replacements (n=3, tariff £5613), unicompartmental knee replacements (n=4, £5613), one anterior cruciate ligament reconstruction (£1863), knee arthroscopies (n=2, tariff £1063), one removal of metal work (tariff £1063) and one scar revision (tariff £1091).
Four patients had foot and ankle procedures performed and these all attracted £1217 tariff price. They consisted of one ganglion excision, one hallux valgus correction, one excision of Morton’s neuroma and one ankle arthroscopy.
Nine patients had upper limb procedures performed. These comprised carpal tunnel decompression (n =1 £1217), radial head excision (n=1 £1217), shoulder stabilisations (n=3 £1217), subacromial decompression (n=1 £1217), acromiclavicular joint excision (n=1 £1063), diagnostic shoulder arthroscopy (n=1 £1217) and arthroscopic cuff repair (n=1 £1887).
34 patients had spinal procedures performed. Inpatient stay ranged from 0 to 5 days with trimpoints of 1 – 13 days. These ranged from nerve root injections (n=23, tariff £522), discography (n=3, tariff £615), microdiscectomy and interspinous distraction (n=2, tariff £3192), decompression, fusions and instrumentation (n= 5, tariff £4252 - £5140), and kyphoplasty (n=1, tariff negotiated: no HRG code. Income £1506). Total income for the spinal group was £44,887.
It can be seen from the data that a wide range of trauma and elective surgery was performed and that the elective group was admittedly younger and had a shorter hospital stay (Table 1). Our unit has the benefit of two spinal surgeons who operate a local and tertiary practice, which changes the demographic of our cohort slightly; other units may not have this factor adjusting their income.
The tariff income for the elective group was £150,318, which was lower than that for the trauma group of £171,941.
Discussion:
This paper is, as far as we are aware the first to compare elective and trauma orthopaedic throughput in a busy district general hospital. It would be bold not to draw attention to our studies limitations. We analysed only one week in the financial year and we accept that seasonal variation may occur. The weather for the week in question involved no snow or ice and was warmer than average for this time of year (5.2°C)10. We do not feel that severe weather influenced our admissions. Previous studies have assessed the effect of seasonal variation on admissions rate. One was in a winter sports resort in Switzerland and unsurprisingly showed a positive correlation between season and fracture incidence11. Another study based in Tasmania showed no variation in either vitamin D levels or incidence of femoral neck fracture12. This goes against the findings of a study based at three latitudes, which showed a high seasonal peak in Scotland, Hong Kong and New ZealandOur locality has a temperate climate with no local winter sports resorts; our experience of seasonal variation is minor.
Miscoding and therefore error in calculations may have occurred; as both the authors and experienced coders reviewed the casenotes the likelihood of this is limited.
Our most important finding was that the mean income per trauma patient (£3658.32) was higher than that for an elective patient (£2045.13) and was statistically significant (p=0.001). The HRG code and income generated represents the money actually received by the hospital from the primary care trust. We openly admit that trauma patients represent a larger burden for the hospital. They have a tendency to be older, have complex co-morbidity and have increased length of stay. They are therefore more costly than elective patients. One study performed in a large university hospital calculated the mean cost for a hip fracture to be £8978.56 (range £3450 - £72,564), this rose to £25,940.44 if there was a superficial wound infection (range £4387 - £93,976) and £34,903 if there was a deep infection (range £9408 - £93,976)14.
Although actual income from the PCT was higher the trauma group will have been loss making on account of the hip fracture group. Whilst this is hard to quantify it seems likely given the calculations portrayed in the Nottingham study of 3686 patientsInpatient costs for the trauma group ignoring theatre costs amount to approximately £204,000. This exposes a lack of appreciation of this group’s requirements in comparison with fit elective hip patients and probably inequality in trauma coding for these patients.
Our study has not tackled implant costs partly due to the fact that inpatient costs have significantly dwarfed these but also due to the fact that we consider these a relatively fixed overhead, costs being determined by local bulk purchase agreements. The consequence on overall study outcome would be minimal given that trauma implants are several orders of magnitude cheaper than elective joint prostheses.
It became apparent to us during the course of our study that trauma can be under resourced when compared with elective care. The background team currently provided for trauma patients include the on call medical team (Consultant Orthopaedic Surgeon, Specialist Registrar and Senior House officer). In addition there are ward nursing staff, anaesthetist, theatre staff, occupational therapists and physiotherapists. On the elective side there are 4 waiting list clerks, 3 surgical assistants, 3 preoperative clinic sisters as well as reception staff and the background medical team (anaesthetist, consultant orthopaedic surgeon, specialist registrar and senior house officer). In the elective setting the aim is identification and optimisation of comorbidities pre-operatively and discharge planning to ensure throughput and turnover of patients. We admit that pre admission screening is not applicable to trauma but faster throughput could ensure improved efficiency and reduced duration of stay.
Our elective patients have a 30-bed ward with an additional 8-bed day case unit; the trauma ward has 24 inpatient beds. The elective unit has 7 registered nurses and 4 health care assistants; on the trauma ward this figure is 4 and 3 respectively. Our elective patients have 2.5 full time equivalent physiotherapists whilst our trauma patients have 1.5.
This situation is probably not dissimilar to the situation in many units elsewhere in the country. This work has shown that trauma income is higher than that for elective work and from this we can infer that if resources were directed accordingly then length of stay could be reduced and profit could be a possibility. A recent paper using hospital episode statistics (HESS) data has shown that length of stay fell quickly once payment by results was implemented15. What was unclear was whether this represented a real change in efficiencies or simply a change in data manipulation by trusts. HESS data has repeatedly been noted to be inaccurate with a range from 10 to 98% dependent on region and disease group.16-17. In a 2006 statement by the then Health Minister Mr. A Burnham it was quoted that £88m pounds was being wasted from 390,000 extra unnecessary bed days18. This was based on the cost of an elective bed being £225 per day with acute beds being significantly more (approximately £320 in one study)The total stay for 66 elective patients was 118 days whereas that for 48 trauma patients was 637 days. Several outliers hugely increased the figure for trauma. Ten trauma patients represented 464 days of inpatient care. If the inpatient stay was reduced by one day for fractured neck of femur patients alone, this amounts to 500 less days per year and approximately £160,000 per year reduction in overhead costs for the trust.
One study in the USA assessed the use of a caseworker to expedite discharge for elderly patients with hip fractures19. The study did not utilise extra physiotherapy and occupational therapy support. Findings were increased theatre, anaesthetic and blood product costs in elderly patients. Increasing age did not correlate with length of stay, cost of stay or income for the hospital. They found that a case manager did reduce the average stay but did not reduce the overall cost. The NHS would do well to note these findings - in many trusts patient flow practitioners are being employed to try and expedite discharge and increase patient turnover. We feel that this money could be channelled into rehabilitation services to effect prompt rehabilitation and discharge.
One final issue is the variation in income between secondary and tertiary centres for certain injuries. One acetabular fracture underwent fixation generating £4262. If this had been referred to a tertiary centre a supplementary specialised service code would have been applicable generating more income (up to 70% in some cases) when intervention was identical. We agree that certain injuries require tertiary treatment by a team with high volume experience and specialised skills. There is an income chasm between the income generated between secondary and tertiary centres for the same injury, which seems perverse.
Overall trauma income was higher than elective income, but still ran at a loss. This was on account of the length of stay of the hip fracture patients and current coding underestimating their true cost to the trust. There is a disparity between rehabilitation services provided for trauma and elective patients, which needs to be addressed to improve efficiency.