Evidence suggests that Serotonin has an important role in bladder control through central and peripheral neurological pathways. The three main serotonin receptor sites involved in the micturition pathway are 5-HT1A, 5-HT4, and 5-HT7. 5-HT7 and 5-HT4 are excitatory to acetylcholine release and 5-HT1A is inhibitory. Increased serotonergic activity leads to parasympathetic inhibition, which results in urine retention. It is through this mechanism of action and their effect on pre-synaptic serotonin 1A and peripheral 5-HT3 receptors that SSRIs were observed to have anti-enuretic effect. However, the exclusive role of serotonin in this regard is not fully understood because along with serotonin, other neurotransmitters, particularly acetylcholine are also implicated in micturition physiology. Acetylcholine is released from nerves innervating the detrusor muscle and causes bladder contraction resulting in voiding. Contrarily, adrenergic pathways lead to constriction of the bladder sphincter and promote continence. There have been suggestions that at lower intrasynaptic 5-HT concentrations, there is prevalence of inhibitory control of micturition, whereas excitatory effect is more pronounced at higher concentrations of 5-HT. This may suggest a dose-dependent relationship between Sertraline and urinary side effects. 1
Case Reports:
Case 1
A 14 year old girl with a diagnosis of moderate depressive episode was prescribed Sertraline 150 mg once daily. On follow up with her community psychiatrist, mum reported that she had been having episodes of bedwetting on a regular basis for almost two weeks. There was no past history of enuresis, no medication changes, or changes to her diet or routine. She had been drinking fluids during the day and had limited fluid intake after 6 pm. On a visit to the Sheffield Children’s Hospital, she had been diagnosed with a urinary tract infection and was prescribed a five-day course of antibiotics. She denied symptoms of abdominal pain, dysuria or fever.
On discussion with the trust pharmacist, it was reported that urinary incontinence is a rare listed side effect of Sertraline with nocturia occurring in 1 in 100 to 1 in 1000.2 At further medication review appointments, the patient continued to report being incontinent on approximately every alternate night and had to use incontinence pads. It was agreed with the patient to reduce the dose of Sertraline to 100 mg once daily to test if her urinary incontinence was linked to Sertraline and review after 2 weeks in clinic. The reduction in Sertraline dose to 100mgs once daily did not alter the frequency of bedwetting that continued on most week nights and varied from being partial to full emptying of the bladder. As a result, she was then referred to the Paediatric Community Incontinence clinic for further investigation regarding the sudden onset of these night bedwetting episodes. Concurrently, Sertraline was gradually reduced and stopped. She was switched to Fluoxetine liquid for treatment of her depressive symptoms, which was titrated to a dose of 16 mg once daily. At the community continence clinic, urine dipstick was negative. Systemic examination including a neurological examination was unremarkable. Mum reported that since the change in medication from Sertraline to Fluoxetine, there was a remarkable improvement in her urinary symptoms.
Case 2
A 16 year old boy with a diagnosis of mixed anxiety and depressive disorder was initiated on Sertraline which was gradually titrated to a maximum dose of 200 mg once daily. He reported improvement in his symptoms of anxiety and depression. However, a few days into taking the higher dose, he experienced symptoms of hesitancy with micturition and failure to ejaculate. On reduction of Sertraline to 100 mg once daily, he reported complete resolution of urinary and sexual side effects, while still reporting a reactive and stable mood. Due to his significant progress, he was eventually discharged from CAMHS back to the care of his GP.
Case 3
A 12 year old girl with a diagnosis of Generalized Anxiety Disorder and Attachment Disorder reported three incidents of urinary incontinence whilst being on Sertraline 200 mg once daily. Sertraline was discontinued by the patient against medical advice. No follow up information was available to observe for resolution of symptoms after discontinuation of Sertraline.
Discussion:
Selective Serotonin Reuptake Inhibitors (SSRIs) are a very commonly used class of psychotropic medication in the CAMHS population to treat depression, anxiety, PTSD and OCD. 3 It is evident by the cases discussed above that SSRIs may have a key link in causing symptoms of urinary dysfunction, which may range from nocturnal enuresis to acute urinary retention. This could be explained by Serotonin’s pivotal role in micturition through central and peripheral pathways. There is not enough evidence on the links in a child and adolescent population as most of the studies are on an adult cohort.4
Conclusion:
In conclusion, it is important for clinicians to bear in mind the genitourinary side effects of SSRIs, which may be debilitating for patients in the CAMHS population. It is equally important for us as clinicians to educate young people and their parents about these potential side effects and how they can be managed. It has also been observed that higher doses of Sertraline have shown a possible link between onset of urinary side effects. In order to establish a significant causal and dose-related relationship on the onset and severity of genitourinary symptoms, studies with a larger sample size followed up over a longer period would be required.
A clearer understanding of the aetio-pathogenesis of schizophrenia would ultimately lead to effective treatment strategies and provide the impetus for elucidation. The autoimmune hypothesis promulgates that it is the auto-antibodies that are responsible for schizophrenia and, according to the viral hypothesis, it may be the body’s abnormal response to a slow viral infection or the undefeated viral antigens causing the schizophrenia pathology. The autoimmune and viral hypotheses are interlinked, as autoimmune disorders can be triggered by microbial infection. Viral aetiology is less convincing than the autoimmune model, but from a treatment perspective, the former is more promising than the latter. To gain a detailed understanding of aetiological models of a subset of schizophrenia, herein the author has reported on a review of the literature relating to the immunity- and viral-based aetiological models of schizophrenia. Genetic vulnerability has been highlighted in the schizophrenia literature alongside environmental factors. The veracity and contestability of the immunity- and viral-based aetiological hypothesis of schizophrenia merits further investigation.
Schizophrenic Syndromes
A prerequisite for incorporating autoimmune and viral aetiology into a scientific discussion would be acceptance of the heterogeneous hypothesis of schizophrenias; they may be a cluster of entities with different aetiologies and the end-stage of different disease processes. 1 Autoimmune or viral aetiology may account for one subgroup.
Schizophrenia has diverse signs and symptoms, and a long history of controversy. Nosologists designate it as polythetic, whereas most other mental illnesses are monothetic, seemingly affecting only one brain system. 2 In the second half of the twentieth century, the psychosocial model gave way to evidence that it is a brain disorder. Schizophrenia has a long history of controversies and there has been much contention over the aetiology, psychopathology, nomenclature, and diagnostic criteria. Schizophrenia is currently seen as a neurodevelopmental encephalopathy, in which the cognitive deficits are produced due to the errors during the normal development of the brain 3 or a neuro-degenerative disorder and the cognitive deficits are derived from a degenerative process that goes on unalterably. Modern neuroimaging techniques and an intensification of studies of necropsy tissue have been responsible for this shift. Researchers seem to agree that a neurodevelopmental or degenerative assault precedes the symptoms by several decades.
The aetiology of the cognitive deficits is unidentified and several potential factors, genetic and epigenetic, are envisaged. Environmental factors—including infectious agents and disturbance in utero through malnutrition—account for a few cases. Autoimmunity and viral theories would fit in with the neuro-developmental and neurodegenerative hypotheses. Proponents of viral aetiology view viruses as acting alongside susceptible genes to initiate a trajectory that manifests as psychotic symptoms.
Lessons from Autoimmunity
Disorders of an autoimmune nature are known to occur with increasing frequency in patients with another autoimmune disease. This is somewhat like the coexistence of multiple psychosomatic disorders in a person; as per Halliday’s psychosomatic formula, association of other psychosomatic afflictions justifies the diagnosis of a new psychosomatic condition. 4 It is well recognised that the central nervous system (CNS) may be directly affected by autoimmune processes, as in the case of multiple sclerosis (MS) and autoimmune limbic encephalitis. A physical autoimmune disease, such as systemic lupus erythematosus (SLE) and antiphospholipid syndrome are also associated with psychiatric morbidity. Paediatric autoimmune neuropsychiatry disorder is a post-infection (group A Beta-haemolytic streptococcal infection) autoimmune disorder characterised by abrupt onset of obsessive compulsive disorder (OCD) and Tourette’s syndrome, brought about by molecular mimicry. 5 Nicholson et al observed that 20% of OCD patients were positive for anti-basal antibodies, considered to be part of a post-streptococcal autoimmune reaction. 6
Autoimmunity is a misdirected response occurring when the immune system attacks the body; it is the loss of tolerance to self-antigens. Immunological tolerance to one’s own tissue is probably normally acquired during foetal life, helping to prevent the occurrence of the autoimmune process (see Table1). Some clones of cells that can produce auto-antibodies (forbidden clones) are thought to be produced throughout life, and are suppressed by large amounts of self-antigens or antigen-specific T cells. Auto-antibodies are produced for a wide variety of antigens; some are organ-specific and others are non-organ-specific. Some microorganisms or drugs may trigger changes in individuals who are genetically vulnerable to autoimmunity.
Table 1- Mechanisms preventing and causing autoimmunity
Tolerance to self molecules a. Clonal deletion-removing any lymphocytes that might react to self molecules b. Clonal anergy-decreasing the responsiveness of lymphocytes that recognise self-molecules. c. Receptor editing-rearrangement of B-cell receptors. d. Reduction or inhibition of molecules or antigens that may cause self recognition. Failure of self tolerance a. Release of isolated auto antigens-tissue trauma or infection may cause breakdown of anatomic barriers and may expose the hidden antigens for recognition of T cells that were not deleted during development. b. Structural alterations in self peptides- Once structurally altered by a trigger such as infection , the self-peptides become more antigenic and are subsequently recognised by the undetected T-cells evoking immune response. c. Molecular mimicry-based on a structural similarity between a pathogen or metabolite and self structures, evoking an immune response against the foreign particles but also an autoimmune response against the self molecules they resemble. d. Polyclonal activation-Infectious agents activate our immune system, B cells and T cells are stimulated resulting in abnormal production of immunoglobulin specific for self molecules. e. Genetic predisposition
A human disease may be considered of autoimmune origin on the basis of knowledge from molecular biology and hybridoma technology, 7 along with the Witebsky postulations. It is established by the presence of auto-antibodies and T cells that react with host antigens. Approximately 25% of patients with an autoimmune disease (AD) tend to build up additional auto-antibodies. Strausburg et al (1996) explained several hypotheses for the virally-triggered autoimmune mechanism (see Table 2). 8 Allergy is the consequence of a strong response to a harmless substance, but ADs are caused when the destructive potential of the immune system is misdirected to oneself. ADs share common effect or mechanisms with hypersensitivity reactions and can be classified into three main types corresponding to the type ii, type iii, and type IV categories of hypersensitivity reactions (see Table 3)
Table 2 - Virally triggered autoimmune mechanisms
a. Molecular mimicry -a protein or polysaccharide on the virus may be structurally homologous to a host molecule and the immune system being unable to differentiate between the two, may then cross react with host cells and tissues expressing this molecule. b. The virus may cause release into the circulation of auto antigens that are normally hidden from the immune system. c. The virus might pick up host proteins from the cell membranes that become immunogenetic since they are present on the virus particle. d. The virus in the process of replication may structurally change the host proteins that in turn become recognized as foreign to the immune system.
Table 3 - Classification of Autoimmune disorders
Type i-no autoimmune diseases are caused by lgE, the source of type i hypersensitivity reactions. Type ii-caused by antibodies directed against components of cell surfaces or the extracellular matrix Type iii-caused by soluble immune complexes deposited in tissues Type iv- caused by effector T cells.
Shared Aetiology
ADs are characterised by shared threads in terms of their propensity to co-exist in a patient or direct relatives. Two major autoimmune clusters have been recognised via, thyrogastric—mostly organ-specific—diseases and lupus-associated—mainly multi systems—diseases. 9 Some ADs are distributed within either cluster and there are also overlaps within each cluster. These patterns of concurrence depend predominantly on genetic determinants.
Poly-autoimmunity is the term proposed for the association of multiple autoimmune disorders in a single patient and such co-occurrences indicate a common origin of the disease. 10 Adriana et al, by grouping diverse ADs in the same patient, demonstrated that they are true associations as part of autoimmune tautology rather than chance findings.
Co-Occurrence of ADs
Theories for autoimmune aspects of schizophrenia raise the concept of early infection by microorganisms with antigens so analogous to CNS tissue that resulting antibodies act against the brain.Some data suggest that an autoimmune process precedes schizophrenia, non-affective psychosis, and bipolar disorder, 11 but do not establish whether this is affected by viral attack, as viral footprints may be hard to detect, especially in the target organ, once the autoimmune process has begun. Psychosis is reported in 25% of SLE cases.
A Danish study revealed that schizophrenia is associated with a large range of ADs. 12 The researchers found that a history of any AD in the patient is allied with a 45% increase in the incidence of schizophrenia. Specifically, nine ADs have a higher prevalence rate among patients and 12 ADs have a higher prevalence rate among their parents than among comparison groups. In comparison with the control group, Thyrotoxicosis, Celiac disease, Acquired haemolytic anaemia, interstitial cystitis, and Sjogren’s syndrome had a higher prevalence rate among schizophrenia sufferers and their family members.
Three of the Ads—namely, celiac disease, thyrotoxicosis, and acquired haemolytic anaemia—have been previously associated with schizophrenia. Celiac disease involves an immune reaction to wheat gluten. This could be due to increased permeability of the intestine, raising the level of antigen exposure, resulting in increased risk of an autoimmune response to brain components or it may be that gluten proteins are broken down into psychoactive peptides. Eaton et al opined that the association of schizophrenia and ADs could be due to common genetic causes, perhaps related to the HLA or other genes, and some cases of schizophrenia may be consequential to the production of autoantibodies that disrupt the brain function.
Researchers for a Taiwan study identified a greater variety of ADs in schizophrenic patients than anticipated and recommended further research. 13 Chen et al. found that 15 ADs are significantly associated with the schizophrenia group. Their studies also confirmed an earlier observation of a negative relationship between schizophrenia and rheumatoid arthritis (RA). It has been observed in a small sample study that mothers of schizophrenia patients have a lower risk for RA.14
Rheumatoid Connection
The negative correlation between schizophrenia and RA is puzzling. 15 Such dissociation was interpreted as the effect of antipsychotic medication. Similarly, the metabolic changes associated with one disease may inhibit another.16 Genes predisposing a person to have one disorder may have a protective influence against another and, in that way, the negative rheumatoid connection with schizophrenia is consistent with an autoimmune model.
RA has a genetic predisposition partly mediated by major histocompatibility complex (MHC) alleles and triggered by infection. Similarly, schizophrenia has genetic and environmental associations and has been cautiously connected with MHC genes other than those perhaps involved in RA. In addition to gene products accountable for antigen presentation, the MHC gene complex holds a multitude of genes-controlling aspects of immune response. Hypothetically, depending on the set of genes an individual has inherited at the MHC complex, a viral assault will lead the immune system to an immune cascade toward the development of RA, or along a genetically-predetermined path with a network of cytokines and immune mediators and directed against CNS components, resulting in schizophrenia. 17
The negative rheumatoid connection may be attributable to two mutually-exclusive alleles of the same gene. Such associations may lead to novel treatment strategies; sickle cell anaemia patients are thought to be less affected by malaria. Of note, the combined research of Karolinska Institute in Sweden and John Hopkins’s University School of Medicine in the United States have recently discovered the genes and the specific deoxyribonucleic acid (DNA) sequences that regulate them plot together to the progress of RA; rheumatology may be inching close to an early detection method and effective treatments. Such a development could hopefully happen in the schizophrenia research.
Commonalities
Even though ADs superficially seem different, the vast majority of them share several similarities. Like ADs, schizophrenia, as such, is neither infectious nor congenital. Schizophrenia and ADs have well-established genetic propensities, and a combination of genes, rather than a single gene, is thought to be responsible for their manifestations. Both schizophrenia and ADs can be triggered by environmental toxins and they have a remitting and relapsing course. Worsening of symptoms is observed when patients are exposed to stress and both conditions have a peak increase in late adolescence or early adulthood. These similarities argue in favour of an autoimmune aetiological model of schizophrenia. 18
Apparently, there is an interesting epidemiological dissimilarity between ADs and schizophrenia. The incidence of ADs is on the increase in developed countries, whereas schizophrenia has a consistent incidence of 1% globally. According to the hygiene hypothesis of ADs, the widespread practice of hygiene, vaccination, and antibiotic therapy in rich countries have disabled children’s immune systems to deal with proper infections and are more geared to charge with one’s own tissues in highly-destructive ways. 19 The incidence between the sexes was thought to be almost similar in the case of schizophrenia, but a recent study shows that for every three males with schizophrenia, there are two females with the disease. 20 ADs are slightly higher among the female population.
Immune Modulation of Clozapine
Antipsychotics may have an immunosuppressant effect; plasma levels of IL-6, soluble IL-6R and transferrin-receptor (TfR) were significantly lower after antipsychotic drug treatment. Activation of cell-mediated immunity may occur in schizophrenia; neuroleptic agents may modulate this through suppression of IL-6 or IL-6R-related mechanisms. 21 The antipsychotic effect may involve a counter-effect on the brain-mediated immune system.
Clozapine, the gold standard for refractory schizophrenia, is a dibenzodiazepine and lowers D2 receptor occupancy and is also a 5-hydroxytryptamine antagonist. Studies indicate that among the atypical antipsychotics, clozapine seems to have an immunosuppressant effect along with neuro-modulatory effect. It has been suggested that clozapine may diminish antibody synthesis in hematopoietic cells and also argued that a possible immunosuppressive action may contribute to its superior antipsychotic efficacy. 22 The long-term immunosuppressive effects of antipsychotics may inhibit putative autoimmune responses against neurological sites and could, thus, act synergistically with the direct antagonistic action on brain receptors for the evident improvement of psychotic symptoms. 23 It is also conjectured that the increase of soluble IL-2 receptor levels in Clozapine-treated patients indicates an immunosuppressant mechanism. 24
Haloperidol may also be a neuro-immune-modulating drug. A study of in-vitro effects of clozapine and haloperidol on cytokine production by human whole blood suggested that both drugs, at concentrations within their therapeutic range, may exert immunosuppressive effects through an enhanced production of IL-1 receptor antagonists. 25
It is well recognised that unlike other antipsychotics, clozapine works better over time, as immune modulation may take longer than neuro modulation. In addition to the neuro modulation, antipsychotics may be working on the principles of immune modulation, as well. If a derivative of clozapine, without its haematological and metabolic side effects is discovered, such a drug would become the first line of choice among the antipsychotics, and that could be a significant event in schizophrenia research. The immunosuppressant effects of clozapine seem to have public health awareness that patients on clozapine are advised to have the winter flue jab. Elderly patients on antipsychotic medications are more prone to get pulmonary infections, indicating that such drugs have a delicate immunosuppressant property.
Autoimmune-Neuropsychiatric Disorder?
If schizophrenia is an AD, a higher rate of other ADs may be expected among schizophrenics. Most studies confirm that it is tied to irregularities affecting multiple levels of the immune axis.There are multiple interlinked causative factors in the aetiology of schizophrenia. There are suggestions that the neuro-behavioural changes follow an abnormal response to microbial invasion, but that does not necessarily lead to an autoimmune process. The literature deciphering the role of viruses in neurotransmitter abnormalities linking neurodevelopment assaults and the neuropsychological manifestations of schizophrenia is unhelpful. For those who adhere to the autoimmune model of schizophrenia, the simplest suggestion would be that the pathogenesis of the subset of schizophrenia studied may be caused by antibodies in the plasma and CSF that react with brain proteins, resulting in a neuro-autoimmune process.
Lessons from Viral Infections
The concept that certain psychiatric disorders are the neuro-behavioural sequel of the body’s immune response to viral infections was prevalent in the early part of the 20th century. That was an outcome of research conducted into rabies in the late 1880s, which revealed the affinity of viruses for the nervous system. Research into tertiary syphilis also provided evidence of an infectious aetiology for specific psychiatric disorders. Investigation of the encephalitis lethargica pandemic (1919 - 1928) contributed to recognition of viral causation on account of similarities apparent between the psychotic symptoms associated with encephalitis lethargica and the clinical presentation of schizophrenia. 26
Post-influenza depression, depression following mononucleosis, and hallucination associated with herpes encephalitis are well recognised. Menninger, who studied post-influenza psychosis, promulgated the first acceptable viral hypothesis for schizophrenia. 27 In the mid-twentieth century, psychodynamic studies began to encompass the origins of schizophrenia and viral aetiology lost its novelty. Dementias associated with Acquired Immune Deficiency Syndrome (AIDS) have reawakened interest in the correlation between virology and psychiatric disorders, and different authors have revisited these hypotheses in the last three decades. 28-36
The immune response to influenza and other viruses involves cell-mediated immunity and cytokine activity, which tend to turn tryptophan into kynurenic instead of serotonin. The outcome of this deviation is mood disturbance. It is the body’s immune response that blocks the conversion of tryptophan into serotonin, thereby resulting in post-influenza depression. It is arguable that there may be other psychiatric disorders consequential to a slow immune response of the body to viral infections. The possibility of viral oncogenesis was originally ridiculed, but now there is some evidence to support the view that viruses are responsible, at some stage, for approximately 20% of human malignant diseases. 31
In theory, a virus could induce schizophrenic symptoms or depression by stimulating antibodies that cross-react with brain tissue, without necessarily gaining entry into the brain. At different developmental stages, the immune response may become less efficient and viral agents may become potentiated, leading to neuropsychiatric conditions. The supposedly inflammation-mediated brain diseases occur at different stages—for instance, schizophrenia in late adolescence or early adulthood, and Alzheimer’s typically at an advanced age. It is well established that the human immunodeficiency virus (HIV) may lead to a form of AIDS dementia, and other common viruses that infiltrate the neurons may cause other types of dementia. HIV/AIDS and Borna Disease Virus (BDV) in animals help to bring the infection-based model of schizophrenia to the realm of scientific imagination
Viruses can influence the human genome. After becoming effective, viral sequences are integrated into the genome of brain cells. These sequences are not thought to be inheritable, but may cause mutations that interfere with brain functions and contribute to the development of psychiatric disorders. 37 It may be arguable that the combination of the body’s sustained immune response and the constant release of antigens of a hypothetical slow virus (schizovirus) may account for the neuro-behavioural alterations. In the following paragraphs, the author discusses how viral pathogens and other potential contributors could interact and lead to schizophrenic psychopathology.
Immune Responses
Neuro-developmental theories of schizophrenia fit the hypothesis that viral insult occurs early in sufferers, not proximally to a psychotic episode. The interaction between host and virus is affected by coordinated activity of the immune system and the brain. There is evidence that schizophrenia is accompanied by mutations in the immune system. Innate immunity is the first defence against microbes; infection results in invasion by live microorganisms and their toxic products, stimulating an inflammatory response. Neuronal functions are disrupted by pathogens and the brain’s inflammatory responses. Non-cytolytic viruses may affect neurones without causing cyto-architectural alteration, but disturbing neurotransmitter production and weakening hormones involved in neurodevelopment. 38 In schizophrenia, immune infiltration is absent, as are vital inclusion bodies and minimal gliosis. There is subtle disruption of neuronal function and brain development, but no significant loss of neuronal cells. Thus, the schizophrenia subset may have a viral aetiological origin, bringing about anomalous, specific immune responses, an autoimmune basis, or both. What triggers the autoimmune process is uncertain, but microbial triggers are a strong possibility.
Immune dysfunctions including lymphocytic abnormalities, protein abnormalities, auto-antibodies, and cytokines have been suggested in seriously-ill patients 39. One study showed significantly higher plasma levels of interleukin-6 (IL-6) in schizophrenics, and soluble IL-6R and soluble IL-2R were significantly high in mania. 40 A few early investigators claimed to have microscopically visualised virus-like particles in the cerebrospinal fluid (CSF) of patients or in chicken embryos inoculated with CSF. Studies of viral antibodies, viral antigens, viral genomes, the cytopathic effect of specimens on cell cultures, and animal transmission experiments are other avenues for exploring the viral infection hypothesis.
The subset of schizophrenics in question may have a highly-sensitive surveillance system, but a less-discerning immune mechanism than the general population. It could be the over-reaction of the immune system to the microbial adversary that may eventually lead to the schizophrenia pathogenesis. The fault may lie in the surveillance system, as well as in the body’s anomalous response to the microbial invasion. 17 In general, innate and acquired immune mechanisms interact and cooperate, but any derangement can lead to deviant immune responses that may result in neuropsychiatric abnormalities.
From an evolutionary perspective, innate immunity is less evolved and the mammalian brain is endowed with a complex immune response system, implying that the neurobehavioral aberrations of schizophrenia could be more linked with deviant and vigorous specific immune responses. 17 It is possible that the proposed subset of schizophrenia may have either an autoimmune basis or a viral aetiological origin, bringing about anomalous, specific immune responses, or both. It has been argued that a gene family involved in the specific immune system and autoimmunity is involved in schizophrenia. 41 The genome-wide association studies (GWAS) have been disappointing in schizophrenia, whereas the major histocompatability complex (MHC) region continues to be the best replicated.
Epidemiological Findings
Epidemiological studies offer useful supporting evidence for viral aetiology (see Table 4). Epidemiological studies characterised by certain broad patterns of incidence and distribution of schizophrenia offer evidence to suspend the scepticism of the viral causal hypothesis. In a study of adults at risk of exposure in utero to the 1957 influenza A2 epidemic in Helsinki, those at risk during the second trimester had significantly more hospitalisations for schizophrenia than those potentially exposed during the other trimesters or immediate years. 42 Researchers for nine subsequent epidemiological studies scrutinised the risk of schizophrenia after possible intrauterine exposure to influenza in Europe and the USA; these identified a small majority claiming to find an association.43 Falsifying the influenza link with the origin of schizophrenia does not altogether make the viral aetiology null and void. There could still be an unknown virus (schizo-virus) as the causative agent. The Hepatitis C virus came to medical attention only 15 years ago. At least these epidemiological studies illustrated that viruses can help set the stage for schizophrenia as a long-term sequel
Table 4 - Suggested Evidences for Viral aetiology
A. Direct evidences: 1.Neuropathology 2.Transmission to laboratory animal 3.Detection of viral genome 4. Sero-epidemiological studies-Detection of Antigen or antibody B. Indirect evidences: 1.Seasonality of schizophrenic births 2.Prevalence studies 3. Immune alterations 4.Antiviral effects of antipsychotic drugs 5.Possible immunosuppressant effect of antipsychotic drugs 6.Studies of identical twins 7. Migration and high risk 8. Gender differences-males are younger at disease onset and have a more severe course.
A worldwide average of 1% prevalence of “core schizophrenia” is generally accepted, 44 even though such a concept of universal distribution and gender equality has opposition. 45 However, there is evidence to assume that there may not be gross variations in this global prevalence. Cross-culturally stable rates, despite decreased fecundity in affected individuals, support an external biological aetiology. These point toward biologically-interlinked and multifactorial causation including an evolutionary genetic factor, as a single biological factor would be insufficient. The preservation of susceptibility genes for schizophrenia in the human gene pool is an evolutionary enigma; gene carriers or first-degree relatives may have some compensatory evolutionary advantage. 46 In a multifactorial aetiological model of schizophrenia, infectious theories are contestable. 17
Such a consistent prevalence, if true, could also be argued in favour of a biologically-inter-linked and multi-factorial causation of schizophrenia, as it is obvious that a single biological factor would be insufficient to maintain a delicate and consistent global prevalence of a disease. Many viruses are relatively constantly distributed, while genetic diseases present distinct geographical clustering due to inbreeding. One may hypothesise that where viral loading is high, genetic input may be less and vice versa. The consistent global incidence points toward universal microbes, a readily-available environmental factor, or, more specifically, a “schizovirus.” The interaction of vulnerable host genes with a virus could yield epidemiology like that of schizophrenia.
Birth patterns rank highly among epidemiological observations in schizophrenia. 47 Many more schizophrenics are born in winter and spring than in summer and fall. 48 Infectious aetiology is a plausible explanation, as many viruses show a surge in the same months and viral aetiology is a more convincing explanation of the consistency in question. While gene coding for particular proteins is inherited, environmental and developmental factors are undoubtedly implicated in modulating genes’ expression.
Exposure to prenatal infections and other obstetric complications are neuro-developmental assaults that increase vulnerability to schizophrenia. 49-52 In obstetrics, infection in the mother generates antibodies transmitted to the foetus, producing auto-antibodies that upset neural development and increase the schizophrenia risk. 53
Schizo-Virus or any Microbe?
It is not certain whether it is body’s abnormal response to any virus and other microbes or a specific unknown virus that results in “schizophrenic reactions.” It is even unclear that the unbeatable antigens of this hypothetical virus alone are capable of inducing the neuro-behavioural changes associated with schizophrenia. The hepatitis C virus came to medical attention only 15 years ago. The rotavirus was isolated in 1973 and the HIV virus was isolated in 1983. Non-detection of a pathogen does not exclude its role in the pathogenesis. If a specific virus is responsible for schizophrenia, it should have been with human society for a very long time, as the illness has been reported from the beginning of recorded human history. Some people may have a genetic vulnerability to the hypothetical schizovirus; inheritability would lie in contracting the specific virus. Poliomyelitis has a concordant rate of 36% among monozygotic twins; the rest are attributed to environmental factors. The majority of children exposed to the polio virus may not develop poliomyelitis and a genetic propensity may be required for the viral manifestation. It is even reported that 10% of the world population rarely catch influenza, in spite of its yearly mutation.
Cardiac disease due to endocarditis (caused by an autoimmune process affecting many parts of the body), a sequel to acute rheumatic fever, is an analogy to demonstrate how, theoretically, a microbial infection may lead to impaired neurodevelopment and psychiatric disorders in a different scenario. Endocarditis is triggered by a reaction to streptococcal bacteria, not a bacterial infection. It may begin a chronic process, leading to valvular cardiac disease. Generally, rheumatic heart diseases are diagnosed 10 - 20 years following rheumatic fever. Similarly, schizophrenia could be an autoimmune complication of a subtle microbial infection; finding and countering the antigenic triggers of ADs may lead to an effective cure.
HIV/AIDS
Patients with HIV are at risk for developing psychiatric symptoms and disorders similar to those seen in the general population, as well as those that are direct effects of HIV. HIV is a neurotropic and lymphotropic virus that causes immune suppression and allows the entry of opportunistic pathogens with an affinity for the CNS. There is some evidence that HIV may trigger a psychotic episode and contribute to first-onset schizophrenia. 54 Serious CNS complications occur late in the course of HIV infection, when the immunity function has diminished considerably. The viral load is closely associated with the degree of cognitive impairment. HIV-associated dementia (AIDS dementia complex) is defined as acquired cognitive abnormality in two or more domains and is associated with functional impairment and acquired motor or behavioural abnormality in the absence of other aetiology. It is estimated that 30% to 60% of patients experience some CNS complications during the course of their illness and 90% reveal neuropathological abnormalities at autopsy.
Pearce argued that HIV-related encephalitis could engender a scenario for a viral aetiology of schizophrenia. 17 HIV produces symptoms after being latent for several years. HIV was not identified as the aetiological agent of AIDS until the conditions for viral replication in lymphoid cell lines were identified. Prior to the evolution of PCR serology techniques, it was debatable whether the virus was in circulation at all. This indicates that the absence of a demonstrable virus does not mean the absence of a subtle virus-induced disease process. No virus, as such, is currently detectable in the schizophrenia disease process. Even in the absence of opportunistic infections, HIV infection of the brain causes severe neuro-behavioural syndromes, such as AIDS dementia, without infecting neurons, but by complex interaction with host molecules and non-neuronal cells. All these suggest that a rare or unknown infectious agent is involved; it would not be identified unless it was specifically tested for.
The finding that the neurophysiological and psychological stress of HIV infection can aggravate an underlying psychotic illness implies that viruses, without being a direct causative agent in psychotic episodes, can unmask pre-existing psychiatric vulnerabilities, acting on the brain physiology through unknown pathways. A curious aspect of HIV-related psychosis is that it responds to anti-psychotic treatment and to anti-retroviral drugs. Several anti-psychotic drugs have been shown to have antiviral properties, both in vitro 55 and in vivo. 56 The deduction is that a virus could initiate events resulting in psychosis, and anti-psychotic drugs can interrupt that sequence. All these features of HIV infections are consistent with the idea that a virus can cause neurobehavioral abnormalities after several years.
Borna Disease Virus
It has been recognised that Borna disease virus (BDV) could cause neuropsychiatric complications including neurological, behavioural, and mood alterations in animals. 57 A ribonucleic acid (RNA) virus from the family Bornaviridae, it is a neurotropic virus with an affinity to a variety of hosts, particularly hoofed animals, and can cause persistent infection of the CNS. Such an infection may be either latent or chronic and slow, but BDV presents with the latent type, characterised by a lack of viral particles. It may resemble the alleged pathogens in non-affective psychosis. The severity of clinical symptoms depends on the immune response of the host.BDV can directly influence the CNS through the binding of viral proteins with neurotransmitter receptors and indirectly through immune response and inflammatory reactions.
Depending on the host’s age and the integrity of the immune response, an infection may be asymptomatic or involve a broad spectrum of behavioural disorders. The severity of clinical symptoms depends on the immune response of the host.58, 59 Unusual features of BDV biology include nuclear localisation of replication and transcription, varied strategies for the regulation of gene expression, and interaction with signalling pathways, resulting in subtle neuropathology.60 BDV can directly influence the CNS through the binding of viral proteins with neurotransmitter receptors and indirectly through immune response and inflammatory reactions. The issue of human BVD infection has been recently questioned by American researchers who reported an absence of association of psychiatric illness with antibodies to BDV or with nucleic acids in serially-collected serum and white blood cell samples from 396 participants. 61 However, BDV in animals helps to bring the infection-based model of schizophrenia to the realm of the scientific imagination.
Neurotransmitters
It is an overstatement to say that schizophrenia is a neurotransmitter disease, although it is well established that it incorporates a derangement of dopamine activity. Some viruses have been shown to alter dopamine metabolism. 62 The literature deciphering the role of viruses in bringing about neurotransmitter abnormalities linking neurodevelopment assaults and the neuropsychological manifestations of schizophrenia is unhelpful. 63 It has been reported that in rodents, BDV could crash neurotransmitter systems, including dopamine, neuropeptides, and glutamate. 64 How viruses alter neurotransmitters is a central issue. Communication between the immune system and the brain is crucial to defend against viral infection; this is mediated through neurotransmitters. Viruses are bound to tamper with the intrinsic communication system as part of their cellular offensive. Some viruses have been shown to alter dopamine metabolism. 65
Genetics
The undisputed genetic factor in schizophrenia may be posited to discount the viral hypothesis. However, genetic factors do not exclude environmental contributions. Monozygotic twins have a concordance rate of only 48%. Brief reactive psychosis due to acute sequels to viral infection, though regarded as unrelated to schizophrenia, may still be schizophrenic reactions and they do not progress to schizophrenia only because the sufferers are not genetically predisposed to schizophrenia. Genetic predilection may be attributable to genes that determine idiosyncratic differences in immune responsiveness to common viral pathogens.
Susceptibility and immune response to infectious agents are known to be subject of genetic control and may involve multiple interacting susceptibility genes. 66 The genetic component of schizophrenia may engross multiple interacting susceptibility genes. These together or singularly may moderate the virus, and the virus and gene product may act at different points. Many cases would have a genetic foundation and it may be extremely rare to develop schizophrenia independently of a genetic anomaly. A small subset of patients may have a purely genetic form. Research should also be directed at identifying risk genes and why they assert themselves and cause the disease. Any future research which sheds more light on some people are affected more readily than others would bring researchers closer to more effective treatments and early intervention (see Table 5).
Table 5 - Future Directions
1. Critical research studies should target in establishing the viral and autoimmune aetiology of a subset of schizophrenia as the illness may be due to both factors. Detection criteria/ tests are vital in isolating this subset from the rest of schizophrenia syndromes 2. Robust epidemiological studies to be conducted to find putative infectious agents and possible models of transmission. 3. Developing new methods for detection of viral agents, directed at the analysis of previously identified pathogens and identification of novel viruses. Vigorous studies with PCR and other sensitive methods for nucleic acid detection to be carried out for the detection of viral nucleic acids in the body fluids of schizophrenia sufferers. 4.To find a method to turn off autoimmune attacks from the body or selectively disable the immune response 5. Identify risk genes and to find the specific DNA molecules and their tagging patterns vital for the progress of the illness. 6. To develop drugs to target specific genes which would mean they would be far more effective and have fewer side effects. 7. Finding psycho-physiological parameters for early detection to minimise the damage. 8. In the event of future discovery of effective antiviral agents, the subset of schizophrenia in question could take advantage of the clinical benefits of such discoveries. 9. Viral aetiology, if proven true, could lead to finding a vaccine against the disease. 10. Selective immune-suppressants could be a future addition into the psychiatric armamentarium. 11. A derivative of cloazapine without its haematological and metabolic side effects would be highly promising.
Summary
There are multiple interlinked causative factors in schizophrenia and viral infection may be only a trigger. Viral infections may be the cause of vigorous immune responses or triggering an autoimmune process that lead to neuro-behavioural aberrations and a subset of schizophrenia would emerge as viro-immuno-neuropsychiatric disorder or autoimmuno-neuro-psychiatric disorder. If such a subset of schizophrenia contains an autoimmune component, either triggered by infectious agents or due to unidentified intrinsic factors, the disease process would be determined by genetic vulnerability. There is not sufficient evidence established to identify viruses as being implicated in the aetiology of schizophrenia, but researchers have reason to anticipate further laboratory studies, as newer, more sensitive laboratory technologies are evolving. A viral or autoimmune model of schizophrenia may illuminate its pathogenesis, but not necessarily the diversity of psychiatric symptomatology. In the last few decades, schizophrenia research has been focussed on neurotransmitter derangements and neuro-developmental anomalies. The cause of a tsunami is not in the sea water, but due to the tectonic shifts under the sea bed; the aetiology of schizophrenia may be similarly due to immune alterations.
Pellagra psychosis due to niacin deficiency was hidden under the schizophrenia umbrella. 67 There may be other psychotic disorders grouped under schizophrenia, and they may have a pure biological aetiology—chemical or infectious—but with genetic vulnerability. No one can be sure whether it is the toxic chemical of the pathogens or the immune response of the host, or both, that may lead to the psychopathology. Searching for this hypothetical virus is a challenging task, but if researchers found it, the benefits would be enormous. A viral aetiology of certain types of schizophrenia, if demonstrable, could affect radical changes in treatment and management. In fact, the hypothesis of viral aetiology is more promising than any other biological hypothesis, as it gives a message of potential drug cure. In this contest, it is interesting to note that the antigenic similarity between components of the streptococcus and cardiac tissue resulted in rheumatic heart diseases, but with the advent of penicillin, this disease has virtually disappeared. Only time will determine the validity and therapeutic prospects of the viral and autoimmune aetiology of schizophrenia.
Davison opined that as evidence accumulates about the autoimmune basis of at least a subset of psychiatric disorders, clinicians should keep abreast of immune-neuropsychiatric research. 68 Psychiatry must constantly expand to meet the growing needs with the emergence of novel ideas in other medical specialities and it is high time to introduce a new terminology—“Psycho-immunovirology”—to study the viral aetiological mechanisms involved in psychiatric disorders like schizophrenia. Neuro-virology and psycho-immuno-virology could develop as an interdisciplinary field which represents a melding of virology, psychiatry, the neurosciences and immunology.
Methamphetamine and related compounds are the most widely abused drugs in the world after cannabis 1. Methamphetamine is a synthetic stimulant which acts both on central and peripheral nervous system. It causes the release and blocks the reuptake of dopamine, norepinephrine, epinephrine and serotonin in neuronal synapse. Methamphetamine can be smoked, snorted, injected or ingested orally. Methamphetamine is more potent, and its effects last longer than cocaine 2, 3.
Methamphetamine intoxication causes various systemic complications like sympathetic over activity, agitation, seizure, stroke, rhabdomyolysis and cardiovascular collapse. Acute cardiac complications of methamphetamine like chest pain, hypertension, arrhythmias, aortic dissection, acute coronary syndrome, cardiomyopathy, and sudden cardiac death have been reported 4, 5. Chronic methamphetamine use is associated with coronary artery disease, chronic hypertension and cardiomyopathy 6.
Here we present a case of methamphetamine overdose, which presented with cardiomyopathy and severe systolic heart failure whose cardiac function was normalized after treatment.
Case presentation
A 38-year-old male presented with shortness of breath, chest tightness and sweating which started after he used intravenous crystal meth the day before presentation. He was an active poly substance abuser and used different drugs like marijuana, alprazolam, amphetamine, cocaine, percocet (oxycodone and acetaminophen) and clonazepam regularly. He was on methadone maintenance program as well. The patient did not have any cardiac problem in the past. He had a seizure disorder but he was not on medication. He had an episode of a seizure after methamphetamine use. His review of system was otherwise unremarkable.
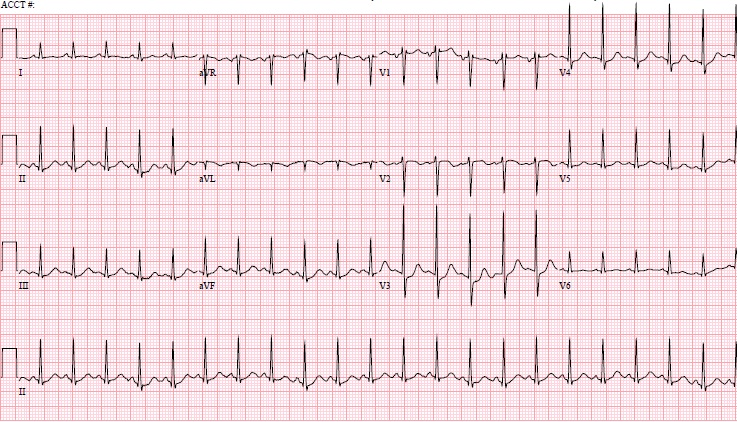
On presentation he was tachycardic, his pulse was 128/min and his temperature was 98 degree Fahrenheit. He had bilateral diffuse crackles on lung bases. Troponin I was high 4.23 ng/ml (reference 0.01-0.05 ng/ml) and BNP was high 657 pg/ml (reference 0-100pg/ml). His electrolytes, renal function, liver function and creatinine kinase were normal. Urine toxicology was positive for opiate, methadone, amphetamine, benzodiazepine, cocaine and cannabinoid. Electrocardiogram showed sinus tachycardia at rate 130/min and QTc was prolonged at 488ms (Figure 1).
Figure 1 - Electrocardiogram: Sinus tachycardia at 130/min with prolonged QTc
Subsequently the patient became tachypnoeic and hypoxic, was intubated, put on a mechanical ventilator, and sedated with versed, fentanyl and propofol. Arterial blood showed respiratory acidosis and hypoxia. The patient was in cardiogenic shock and dopamine drip was started and intravenous Lasix was given. A subsequent chest X-ray showed newly developed pulmonary congestion. Echocardiogram showed left ventricular dilatation with diffuse hypokinesis and depressed systolic function. The left atrium was dilated. He had moderate diastolic dysfunction, mild mitral regurgitation and tricuspid regurgitation with a pulmonary artery pressure of 38mmHg. There was global left ventricular function was reduced and ejection fraction was 25-30%. His CT head was negative for an infarct or hemorrhage. He was managed in the cardiac care unit and responded very well to treatment. He became haemodynamically stable and dopamine was discontinued; aspirin, clopidogrel and carvedilol were started. The patient gradually improved and was extubated. Cardiac catheterization showed normal coronaries and normal left ventricular function. LVEDP was 18mmHg. His repeat echocardiogram one week later showed normal left ventricular systolic and diastolic function with an ejection fraction of 70%. The patient was discharged to drug rehab after eight days of treatment.
Discussion
This patient used intravenous crystal meth after which his problem started, so the most likely culprit was methamphetamine. Although he used multiple drugs including cocaine and amphetamine, which have acute and chronic effects on the heart, his cardiac function was normal before. Different mechanisms for cardiac injury due to methamphetamine have been proposed which include catecholamine excess, coronary vasospasm and ischaemia, increase in reactive oxygen species, mitochondrial injury, changes in myocardial metabolism, and direct toxic effects 3.Methamphetamine use is known to cause acute and chronic cardiomyopathy and the reversal of cardiac failure has been documented after discontinuing the drug. In one case report, a patient with chronic methamphetamine-associated cardiomyopathy did not demonstrate late gadolinium enhancement, consistent with an absence of significant fibrosis, and had left ventricular function recovered with 6 months of medical therapy and decreased drug abuse 7. Another case of a female 42 year old methamphetamine user who had transient left ventricular dysfunction and wall motion abnormalities and an index ventriculogram showed apical ballooning consistent with Takotsubo cardiomyopathy; her left ventricular function significantly improved after 3 days of medical treatment 8. In our patient, acute cardiomyopathy resolved quickly with intensive medical management. It is not clear how long it takes for cardiomyopathy to revert to normal after discontinuing the drug, or at what stage cardiac damage is irreversible. Many patients who use methamphetamine also ingest other drugs as well. It is unclear to what extent the use of multiple drugs play synergistic role in the cardiac complications that occur. Among patients who present with cardiomyopathy and cardiogenic shock, the usage of drugs like methamphetamine and co-ingestion of other drugs should be considered. Further study is needed to recommend treatment for methamphetamine and related drugs induced cardiomyopathy.
Alopecia areata is a non-scarring autoimmune, inflammatory hair loss affecting the scalp and/or body. Although the etiopathogenesis of alopecia areata is still unknown, the most widely accepted hypothesis is that it is a T-cell mediated autoimmune condition that occurs in genetically predisposed individuals. The term ‘alopecia areata’ was first used for this disorder by Savages1.Alopecia areata has a reported incidence of 0.1-0.2%, with a life-time risk of 1.7%2-4. The disease can begin at any age, but the peak incidence is between 20 and 50 years of age5. Both the sexes are equally affected and there is no racial variation reportedClinically, alopecia areata may present as a single well demarcated patch of hair loss, multiple patches, or extensive hair loss in the form of total loss of scalp hair (alopecia totalis) or loss of entire scalp and body hair (alopecia universalis). Histopathologically, alopecia areata is characterized by an increase in the number of catagen and telogen follicles and the presence of perifollicular lymphocytic infiltrate around the anagen phase hair follicles. The condition is thought to be self-limited in majority of cases, but in some the disease has a progressive course and needs active treatment in the form of oral or topical therapeutic options. Progressive alopecia areata is associated with severe social and emotional impact.
Clinical features
Alopecia areata mostly presents as a sudden loss of hair in well demarcated localized areas. The lesion is usually a round or oval flat patch of alopecia with normal skin colour and texture involving the scalp or any other region of the body. The patch of alopecia may be isolated or there may be numerous patches. It usually has a distinctive border where normal hair demarcates the periphery of the lesion. In acute phases, the lesions can be slightly erythematous and oedematous.
The patches of alopecia areata are usually asymptomatic, although several patients may sometimes complain of local paraesthesia, pruritus or pain. The affected hairs undergo an abrupt conversion from anagen to telogen, clinically seen as localized shedding. Characteristic hairs, known as ‘exclamation point hairs’ may be seen within or around the areas of alopecia. The hairs are tapered towards the scalp end with thickening at the distal end. These hairs may also demonstrate deposition of melanin pigment in the distal extremity, also known as Wildy’s sign. Although not absolutely pathognomonic, it strongly suggests the diagnosis of alopecia areata. Hair pull test conducted at the periphery of the lesion may be positively correlated (six or more) with disease activity. In the chronic phases, the test is negative, since the hair is not plucked as easily as in the acute phases.
Another important clinical sign that can aid in the diagnosis is the presence of ‘cadaverous hair’. These are the hairs in which there occurs a fracture of the shaft inside the hair follicle, producing blackened points inside the follicular ostia resembling comedones. In alopecia areata, the hair loss progresses in a circumferential pattern. Often, distinct patches merge to form large patches. Upon regrowth, hairs will often initially lack pigment resulting in blonde or white hairs7.
Extrafollicular involvement in alopecia areata:
a) Nail changes: Nail changes are more frequent in children (12%) than in adults (3.3%)8.The prevalence of nail changes is greater in the more severe forms of alopecia areata such as alopecia universalis and alopecia totalisFinger nails are more commonly involved than the toe nails. Pitting is the most common finding. Other nail changes include koilonychias, onycholysis, onychomadesis, punctuate leukonychia, trachyonychia, Beau’s lines and red lunulae8-11.
b) Ocular changes: Various ocular changes have been reported to occur in alopecia areata. These include focal hypopigmentation of the retina12, lens opacities, posterior subcapsular cataracts13 decrease in visual acuity, Horner’s syndrome, heterochromia of the iris14, miosis and palpebral ptosis.
Treatment of alopecia areata
Treatment of alopecia areata is not mandatory in every affected patient because the condition is benign in majority and spontaneous remission is common. Treatment is mainly directed towards halting the disease activity as there is no evidence that the treatment modalities influence the ultimate natural course of the disease. Treatment modalities are usually tailored as per the extent of hair loss and the patient’s age. Addressing the impressive inflammatory process occurring in alopecia areata, corticosteroids have by far been the most commonly used treatment modality-16Few treatments have been subjected to randomized control trials and except for contact immunotherapy, there is a paucity of published data on their long term outcomes. Currently, new treatments targeting the immune system are being explored for the use in alopecia areata.
Topical treatments
Topical steroids
Intralesional steroid injections
Topical contact sensitizers
Anthralin
Minoxidil
Topical retinoids
Tacrolimus
Systemic treatments
Systemic corticosteroids
Sulfasalazine
Azathioprine
Methotrexate
Oral zinc sulphate
Photo-and photochemotherapy
PUVA
NBUVB
Excimer laser
Miscellaneous and Non-pharmacological treatment
Dermatography, wigs
Hypnotherapy etc
Topical treatment options
Topical corticosteroids:
Several topical corticosteroids with varying levels of efficacy have been used to treat alopecia areata. These include fluocinolone acetonide cream17, fluocinolone scalp gel, betamethasone valerate lotion18, clobetasol propionate ointment19, dexamethasone in a penetration-enhancing vehicle and halcinonide cream20. They are a good option in children because of their painless application and wide safety margin21. Topical corticosteroids are ineffective in alopecia totalis/universalisFolliculitis is a common side effect of corticosteroid treatment, appearing after a few weeks of treatment. Telangiectasia and local atrophy have also been reported. Treatment must be continued for a minimum of 3 months before regrowth can be expected and maintenance therapy often is sometimes necessary.
Intralesional corticosteroids:
Intralesional corticosteroids are widely used in the treatment of alopecia areata. In fact, they are the first-line treatment in localized conditions involving <50% of the scalp22. Hydrocortisone acetate (25mg/ml) and Triamcinolone acetonide (5-10mg/ml) are commonly used. Triamcinolone acetonide is administered usually in the concentration of 5mg/ml using a 0.5 inch long 30-gauge needle in multiple 0.1 ml injections approximately 1 cm apart22-23. The solution is injected in or just beneath the dermis and a maximum of 3 ml on the scalp in one visit is recommended23. Lower concentrations of 2.5mg/ml are used for eyebrows and face. Regrowth usually is seen within 4-6 weeks in responsive patients. Treatments are repeated every 3-6 weeks. Skin atrophy at the sites of injection is a common side effect, particularly if triamcinolone is used, but this usually resolves after a few months. Repeated injections at the same site or the use of higher concentrations of triamcinolone should be avoided as this may lead to prolonged skin atrophyPain limits the practicality of this treatment method in children who are less than 10 years of age. Severe cases of alopecia areata, alopecia totalis, alopecia universalis as well as rapidly progressive alopecia areata respond poorly to this form of treatment25.
Anthralin:
Dithranol (anthralin) or other irritants have been used in the treatment of alopecia areata. The exact mechanism of action is unknown, but is believed to be through immunosuppressant and anti-inflammatory properties with the generation of free radicals. It is used at concentrations ranging from 0.5 to 1 % for 20-30 minutes after which the scalp should be washed with shampoos in order to avoid excessive irritant effects. The applications are made initially every other day and later on daily. Adverse effects include pruritus, erythema, scaling, staining of treated skin and fabrics, folliculitis, and regional lymphadenopathy26-27. In an open study, 25% patients with severe alopecia areata were shown to respond positively to local applications of 0.5-1% anthralinMore placebo control studies are needed to justify the use of anthralin in alopecia areata.
Minoxidil:
Minoxidil appears to be effective in the treatment of alopecia areata. It’s mechanism of action has yet to be determined, but it is known to stimulate DNA synthesis in hair follicles and has a direct action on the proliferation and differentiation of the keratinocytes28. In one clinical study, hair growth was demonstrated in 38% and 81% of patients treated with 1% and 5% minoxidil respectively. Thus 5% minoxidil solution is usually recommended as a treatment option in alopecia areata. No more than 25 drops are applied twice per day regardless of the extent of the affected area. Initial regrowth can be seen within 3 months, but continued application is needed to achieve cosmetically acceptable regrowth. Minoxidil has also been studied in combination with anthralin29, topical betamethasone propionate30 and prednisolone31. Minoxidil is of little benefit to patients of severe alopecia areata, alopecia totalis or alopecia universalisThe possible side effects from minoxidil are allergic and irritant contact dermatitis and hypertrichosis which is usually reversible with the interruption of the treatment.
Topical immunotherapy:
Topical immunotherapy is the best documented treatment so far for severe and refractory cases of alopecia areata. Topical immunotherapy is defined as the induction and periodic elicitation of allergic contact dermatitis by applying a potent contact allergen33. In 1965, the alkylating agent triethyleneimino benzoquinone was the first topical sensitizer used to treat cutaneous disease, but it was abandoned on account of its mutagenic potential. Later nitrogen mustard, poison ivy, nickel, formalin, and primin were tried, mainly as topical immunotherapy, for alopecia areata and warts. Contact immunotherapy was introduced in 1976, by Rosenberge and Drake. Later, potent contact allergens namely dinitrochlorobenzene (DNCB) and diphenylcyclopropenone (DPCP) replaced the allergens that were used earlier33. DNCB is mutagenic against Salmonella tymphimurium in the Ames test and is no longer usedNeither SADBE, nor DPCP are mutagenic. DPCP is more stable in solution and is usually the agent of choice.
Mechanism of action: Topical immunotherapy acts by varied mechanisms of action. The most important mechanism is a decrease in CD4 to CD8 lymphocyte ratio which changes from 4:1 to 1:1 after contact immunotherapy. A decrease in the intra-bulbar CD6 lymphocytes and Langerhan cells is also noted. Happle et al, proposed the concept of ‘antigenic competition’, where an allergic reaction generates suppressor T cells that non-specifically inhibit the autoimmune reaction against a hair follicle constituent. Expression of class I and III MHC molecules, which are normally increased in areas affected by alopecia areata disappear after topical immunotherapy treatment34.A ‘cytokine inhibitor’ theory has also been postulated34.
Method of sensitization: The protocol for contact immunotherapy was first described by Happle et al in 1983 The scalp is the usual sensitization site. For the initial sensitization a cotton-tipped applicator saturated with 2% DPCP in acetone is applied to a small area. Patients are advised to avoid washing the area and protect it from sunlight for 48 hours. After 2 weeks 0.001% solution of DPCP is applied on the scalp and then the application of contact allergen is repeated weekly with increasing concentrations. The usual concentration of DPCP that ultimately causes mild contact eczema is 0.01-0.1% and this is repeated weekly till a response is seen. An eczematous response indicates that sensitization has taken place. Only 1-2% of the patients fail to sensitize. It is important to remember that DPCP is degraded by light and should thus be stored in the dark and the patient should also wear a wig or hat during the day after application of DPCP. DPCP immunotherapy has even been combined with oral fexofenadine treatment with good effect36.
Evaluation of efficacy: The clinical response after six months of treatment is rated as per the grading system proposed by Mcdonald Hull and Norris37:
Grade 1- Regrowth of vellus hair.
Grade 2- Regrowth of sparse pigmented terminal hair.
Grade 3- Regrowth of terminal hair with patches of alopecia.
Grade 4- Regrowth of terminal hair on scalp.
If no regrowth is observed within six months of treatment, the patient is considered to be a non-responder. Evaluation of plucked hair is done using light microscopy, for evaluation of anagen/telogen ratio.
A review of most of the published studies of contact immunotherapy concluded that 50-60% of patients achieve a worthwhile response but the range of response rates was very wide (9-87%)Patients with extensive hair loss are less likely to respond. Other reported poor prognostic factors include the presence of nail changes, early onset disease and a positive family history39.
Topical immunotherapy can lead to certain side effects such as persistent dermatitis, painfull cervical lymphadenopathy, generalized eczema, blistering, contact leukoderma, and urticarial reaction. Systemic manifestations such as fever, arthralgia and yellowish discoloration of hair are noted more often with DNCB.
In poor responders to DPCP, squaric acid dibutylester (SADBE) can be tried as a contact sensitizer. The method of application is the same as with DPCP but the applications are done once or twice weekly40.
Good care should be taken to avoid contact with the allergen by handlers, including pharmacy and nursing staff. Those applying the antigen should wear gloves and aprons. There is no available data on the safety of contact immunotherapy during pregnancy and it should not be used in pregnant women or in women intending to become pregnant.
Tacrolimus:
Tacrolimus is a topical calcineurin inhibitor that inhibits transcription following T-cell activation of several cytokines including IL-2, IFN-gamma and TNF-α. Yamamoto et al reported in their findings that tacrolimus stimulated hair growth in mice41, although subsequent studies have shown conflicting resultsRecently, Price et al reported an 11-patient study in which none of the patients had terminal hair growth in response to tacrolimus ointment 0.1 % applied twice daily for 24 weeks43.
Topical garlic
Garlic is a very commonly used home remedy in the treatment of alopecia areata in India and even in the rest of the world. One study analyzed the effect of a combination of topical garlic gel and betamethasone valerate ointment in alopecia areata in a double-blind study. The study found the combination useful in majority of the patients with a statistically significant difference between the treatment and control groups44.
Topical retinoids:
Among topical retinoids, tretinoin and bexarotene have been tried in alopecia areata with mixed results-46Irritation of the skin is a very common side effect and the efficacy is doubtful in the absence of double-blind randomized trials.
Prostaglandin analogs:
The propensity of certain prostaglandin analogues used as anti-glaucoma eye drops to cause hypertrichosis has been employed in the treatment of alopecia areata. These prostaglandin analogues include Latanoprost and Bimatoprost and they are used in the treatment of alopecia areata involving the eyelashes-48However, the results obtained with these drugs have not been really encouraging49.
Systemic treatments
Systemic treatments, as a rule, are used only in progressive forms of alopecia areata and going by the immune nature of the disease, majority of these treatment options are immunosuppressants or immunomodulators in nature.
Systemic corticosteroids:
The use of systemic corticosteroids for the treatment of alopecia areata is under much debate. Some authors support a beneficial role of systemic steroids on halting the progression of alopecia areata, but many others have had poor results with this form of therapy. The suggested dosages are 0.5-1mg/kg/day for adults and 0.1-1 mg/kg/day for children50. Treatment course ranges from 1-6 months, but prolonged courses should be avoided to prevent the side effects of corticosteroids. Side effects profile of corticosteroids in conjunction with the long-term treatment requirements and high relapse rates make systemic corticosteroids a more limited option. In addition to the daily oral administration of corticosteroids, there are several reports of high-dose pulsed corticosteroid treatments employing different oral and intravenous regimens51-53. Many of these regimens have been tried in alopecia areata with encouraging results but the majority of these studies have been non-blind open studies. One such pulsed administration employs a high dose oral corticosteroid on two consecutive days every week with a gap of 5 days between the two pulses. This modality of treatment is known as oral minipulse therapy (OMP) and it has been tried in many skin diseases in addition to alopecia areata like vitligo54-55 and lichen planusSome open label studies on corticosteroid OMP therapy have reported encouraging results in alopecia areata53.
Sulfasalazine:
Because of its immunomodulatory and immunosuppressive actions, sulfasalazine has shown good hair regrowth in the treatment of alopecia areata. The drug is administered orally usually as enteric coated tablets to minimize the gastrointestinal side effects. The treatment is started at a lower dose, usually in the range of 500 mg twice daily and then the dose is gradually increased to 1 g three times a dayAdverse effects include gastrointestinal distress, liver toxicity and haemotological side effects. Sulfasalazine helps in alopecia areata because it causes inhibition of T cell proliferation, and natural killer cell activity and also inhibits antibody production. It also inhibits the secretion of interleukin (IL)-2, IL-1, TNF- and IFN-gamma and even IL-667.
A number of clinical studies have documented a positive effect of sulfasalazine in alopecia areata. In one clinical study, 23% patients showed a really good response with satisfactory hair growth after sulfasalazine therapyOther studies have also shown a beneficial effect of this treatment option in resistant cases of alopecia areata66,69.
Azathioprine:
Azathioprine, being an immunosuppressive agent has also been tried in alopecia areata. The drug is used in many cutaneous disorders owing to its effect on circulating lymphocytes as well as Langerhan cells. In a limited study on 20 patients hair regrowth was demonstrated in about half of the patients with a dosage regimen of 2g/day70.
Cyclosporine:
This drug has proven effective in the treatment of alopecia areata because of its immunosuppressive and hypertrichotic properties. The side effect profile and high rate of recurrence render the drug a poor choice for the use in alopecia areata. So the drug is to be attempted only in severe forms of alopecia areata not responding to treatment71.
Methotrexate:
Methotrexate either alone or in combination with prednisolone has been used in the treatment of alopecia areata in various studies with variable success rates72.
Oral zinc sulphate
Serum zinc levels have been found to be lower in patients with alopecia areata than in control populationIn a study on 15 patients, hair regrowth was observed in 9 patients (67%) after oral zinc gluconate administration74.
Biological agents:
Tumour necrosis factor inhibitors such as Adalimumab, Infliximab and Etanercept have been tried in alopecia areata, but the results have not been encouraging-76Clinical trials conducted till now have failed to demonstrate the efficacy of any biological agent in alopecia areata.
Photo-and photochemotherapy
Photochemotherapy:
Several uncontrolled studies regarding PUVA therapy for the treatment of alopecia areata exist. All types of PUVA (oral PUVA, topical PUVA, local or whole body UVA irradiation) have been used with success rates of up to 60-65%57-59. The mechanism of action is considered to be the interference in the presentation of follicular antigens to T-lymphocytes by depletion of the Langerhan cells. The relapse rate following treatment is high, sometimes demanding repeated treatments for a prolonged period with implications for carcinogenic risks60. To mitigate the side effects of systemic psoralens, PUVA-turban therapy is used for alopecia areata involving the scalp. In this form of photochemotherapy, very dilute solutions of 8-methoxy psoralen are applied on the scalp by utilizing a cotton towel as a turban. The patient’s scalp is exposed to UVA after keeping the ‘turban’ in contact with the scalp for about 20 minutesThe efficacy of this form of PUVA therapy has been seen to be about 70%61.
Phototherapy
Although narrowband UVB is among the most effective treatment options in a number of immune mediated skin diseases, the same efficacy has not been found in alopecia areata. Properly designed randomized trials are needed to elucidate whether NBUVB has any role in the management of alopecia areata62-63.
Excimer laser and excimer light
Excimer laser and excimer light are two more recent additions to the phototherapeutic armamentarium for many skin and hair disorders. While the main use of these phototherapeutic modalities remains to be psoriasis and vitiligo, their immunomodulatory effect can be made use of in many other skin disorders. Some clinical studies have documented the efficacy of excimer laser and excimer light in alopecia areata64-65. In one such study, 41.5% patches were shown to respond to excimer laser therapy administered over 12 weeks64. Another study on childhood alopecia areata found regrowth in 60% lesions after a treatment period of 12 weeksThe treatment is well tolerated with erythema of the skin as the only adverse effect reported.
Miscellaneous therapies
Various non-conventional therapeutic agents have been used in alopecia areata with some degrees of success. These include fractional Er-Glass laser77, topical azelaic acid78, topical onion juice79, topical 5-fluorouracil ointment80 and photodynamic therapyThe efficacy and safety of these therapeutic agents need to be confirmed in large-scale, double-blind, placebo-controlled trials before they can be recommended for treatment of alopecia areata.
Non-pharmacological methods
Cosmetic treatments for patients with alopecia areata include the following:
a) Dermatography: It has been used to camouflage eyebrows of patients with alopecia areata. In this treatment tiny pigment dots of pigment are used on the skin on the region of the eyebrows to mask the underlying alopecia81.
b) Wigs or Hair pieces: These are useful for patients with extensive disease and allow them to carry on their usual social life.
Conclusion:
Alopecia areata is now regarded as an autoimmune disease involving the cellular immunity through the CD8 lymphocytes that act on follicular antigens. The pathogenesis of alopecia areata is being unravelled with various animal and human studies.
The localized forms often heal spontaneously or respond to simple treatments such as topical or intralesional corticosteroids. The severe forms have a reserved prognosis and are difficult to treat. In these cases the best results are achieved by topical immunotherapy technique.
The Royal College of Psychiatrists defines the 'graduates' as people who have had enduring or episodic severe mental disorder in adulthood and have reached the age of 65 years. Estimates of the most severely affected range from 11 to 60 per 100 000.1 This group of people seems to be uniquely disabled by a combination of social, mental health and physical disadvantages and there is a risk of falling between general adult, rehabilitation services and old age psychiatry.2
There has been an ongoing debate about identifying the best practice in the management of this group of patients who often have spent most of their lives in the old psychiatric asylums. The recommendations include identifying all graduates within the service followed by a full assessment of the patients' health and social care needs and the implementation of a care plan to meet these needs, to be reviewed at least annually. According to the report, the medical responsibility will rest with a principal in general practice or a consultant psychiatrist, and maintenance of continuous review should be the responsibility of the case manager.1
The Recovery and Rehabilitation Team (RRT) in Newham was founded in 1988 to facilitate the discharge of groups of patients from Goodmayes hospital (Essex). Patients discharged to residential care units and other supported schemes usually had spent many years in the institution and the team's remit after relocation into the community was mainly monitoring of mental health by conducting multiprofessional reviews in the care homes, crisis intervention, and the promotion of social networks and leisure activities. Over the following years, the team also received many referrals from Community Mental Health Teams (CMHT) for continuing care of people suffering from long term and severe mental illness. Today, a considerable proportion of these patients have 'graduated' into old age and the current percentage of the total caseload is now nearly 25%.
Our survey was carried out following an independent review by the Health and Social Care Advisory Service (HASCAS) in January 2005 for the rehabilitation services provided in the London Borough of Newham. The recommendations included an assessment of needs for all patients 65 years of age or over, using the Camberwell Assessment of Needs for the Elderly (CANE) .3This is a comprehensive needs assessment tool suitable for use in a variety of settings. It has been successfully used for older people in primary care, sheltered accommodation, residential homes, nursing homes, and mental health services for older people. However, it has not been used before to specifically assess the needs of older people who have graduated within the general adult mental health or rehabilitation services. CANE was found to be a valid and reliable tool and easy to use by different professions.4
Method:
The RRT database was searched for all patients aged 65 years or over. This yielded 52 names, who were then approached between June and September 2005 for a comprehensive assessment after an explanation about the survey. CMHTs were asked for numbers of graduates in their services, obtained from the respective databases.
The CANE is a structured, 24-item questionnaire covering different areas (see table 2), including social, psychological, mental health and physical needs. It is easily applicable by different professions and requires on average about one hour of assessment time. It measures met and unmet needs and obtains views from patients, carers, staff and the rater. Assessments were carried out by members of the multi-disciplinary team that consists of a consultant psychiatrist, the team manager, two senior clinical medical officers, two clinical psychologists, two occupational therapists, two social workers, five community psychiatric nurses and four community support workers. All raters had received a one day training provided by Juanita Hoe, one of the contributors in producing the CANE.
The collected data were analysed using Microsoft Excel.
Results
The total number of patients aged 65 years and above under the care of the rehabilitation services was 52 (24.5% of the total caseload of 212 patients). There were a further ten patients under the care of the adult CMHTs in Newham. Attempts were also made to determine the number of the graduates under the care of mental health services for older people, but these were unsuccessful.
Out of the 52 patients, 50 could be assessed using the CANE, two patients declined the assessment and the assessment sheet of one patient could not be traced, giving a total of 49 patients and a response rate of 79% of all known 'graduate' patients under the care of adult mental health services.
Results describing patient characteristics including mean age, gender, type of accommodation and diagnosis, are summarized in Table 1.
Table: 1 Demographic Details
Variable
Mean Age (years)
72.16
Gender (n(%))
Female
16(32.65%)
Male
33(67.34%)
Type of accommodation (n(%))
Residential care
25(51%)
Supported accommodation
13(26.53%)
Private accommodation
12(24.48%)
Diagnosis (n(%))
Schizophrenia
33(67.34%)
Schizoaffective Disorder
6(12.24%)
Bipolar Affective Disorder
5(10.20%)
Depression
2(4.08%)
Personality Disorder
1(2.04)
OCD
1(2.04%)
Dysthymic Disorder
1(2.04%)
Nearly two-thirds of patients were female, three-quarters of this population were living in supported living or residential care and 90% were suffering from a severe mental illness (two-thirds from schizophrenia).
The met and unmet needs of this population are described in table 2.
Table 2: Levels of needs as rated by the rater (n=49)
Item
No Need
Met Need
Unmet Need
Not Known
n
(%)
n
(%)
n
(%)
n
(%)
Accommodation
22
44.90%
22
44.90%
2
4.08%
3
6.12%
Household skills
5
10.20%
41
83.67%
3
6.12%
0
0.00%
Food
9
18.37%
34
69.39%
6
12.24%
0
0.00%
Self-care
12
24.49%
31
63.27%
6
12.24%
0
0.00%
Caring for other
47
95.92%
2
4.08%
0
0.00%
0
0.00%
Daytime activities
16
32.65%
14
28.57%
18
36.73%
1
2.04%
Memory
34
69.39%
4
8.16%
5
10.20%
6
12.24%
Eyesight/hearing
24
48.98%
14
28.57%
10
20.41%
1
2.04%
Mobility
26
53.06%
18
36.73%
5
10.20%
0
0.00%
Continence
28
57.14%
16
32.65%
3
6.12%
2
4.08%
Physical health
14
28.57%
29
59.18%
6
12.24%
0
0.00%
Drugs
17
34.69%
30
61.22%
2
4.08%
0
0.00%
Psychotic symptoms
18
36.73%
28
57.14%
3
6.12%
0
0.00%
Psychological distress
29
59.18%
14
28.57%
6
12.24%
0
0.00%
Information
28
57.14%
11
22.45%
6
12.24%
4
8.16%
Safety(deliberate self harm)
44
89.80%
4
8.16%
0
0.00%
1
2.04%
Safety(accidental self-harm)
35
71.43%
11
22.45%
2
4.08%
2
4.08%
Safety(abuse or neglect)
35
71.43%
10
20.41%
4
8.16%
1
2.04%
Behaviour
32
65.31%
12
24.49%
4
8.16%
1
2.04%
Alcohol
47
95.92%
2
4.08%
0
0.00%
0
0.00%
Company
29
59.18%
8
16.33%
11
22.45%
1
2.04%
Intimate relationship
40
81.63%
3
6.12%
4
8.16%
2
4.08%
Money
21
42.86%
19
38.78%
9
18.37%
0
0.00%
Benefits
37
75.51%
3
6.12%
4
8.16%
5
10.20%
Regarding unmet needs, the highest value (nearly 37%) was on daytime activities, which 18/49 people scored. This is followed by company (22.5%), which was a problem for 11 people. Eyesight or hearing also scored strongly (20.5%), followed by money (18.4%) and different problems in areas such as food and self-care, physical health and psychological distress (each 12%). Problems with suicidal behaviour and drug or alcohol abuse were not evident in terms of unmet needs.
Discussion
Our results show that the majority of needs identified by the CANE were adequately met by the current service provision or were only identified as unmet needs by a tiny minority (table 2). Since the vast majority of the patients were living in either residential or supported accommodation (25.51% and 26.53% respectively), items associated with domestic needs and activities appeared to be met to a great extent, e.g. accommodation (44.90% no need, 44.90% met need).
In terms of items related to mental state, the majority of patients seemed to be satisfactorily managed and receiving appropriate treatment. The raised number of patients who suffered from psychological distress could be explained by other psychosocial factors such as lack of daytime activities and lack of company which have been identified as the major unmet needs in our population.
A recent article,5 named risk of harm, unpredictability of behaviour, poor motivation, lack of insight and low public acceptability as the major reasons for social disability. However, in our review, over one-third of people clearly expressed the wish for more daytime activities, where the named disabilities might prevent a more active and satisfied lifestyle. In the interviews, it transpired that people mostly wished for an outreach service providing social contact, befriending and activities. The majority of people in our population seemed to be rather reluctant to access general facilities, like day centres for the elderly.
As we have assessed most of the patients under the care of adult mental health services, this survey should be able to inform service planning about the needs of this population. The development of an outreach service offering day time activities including a befriending component could be a challenge for the responsible service providers, e.g. social services, adult community mental health services and old age psychiatry.
The specific physical needs (especially eyesight and hearing) make it necessary for services to monitor these closely and implement this in the care plan in liaison with General Practitioners.
Similar reviews should be undertaken by community mental health services in other boroughs to highlight the needs of this specific group of patients, as the respective unmet needs might be dependent upon the level of service provision.
The Care Programme Approach (CPA) was introduced in England in 1993 to co-ordinate the care of patients with mental health disorders.1 Its aim was to ensure that there was a full assessment of the patient’s needs, that a care co-ordinator would see that the care was delivered, regular checks would be carried out to review progress, there would be collaboration between health and social services, and that patients (or the term used to ‘demedicalise’ them in psychosocial Newspeak 2 namely, ‘service users’) and carers (they also use the service) would have a greater say in the written management plan. Targets were set.
What has happened since? Prior to this I recall that most psychiatrists carried out full assessment needs, regular checks reviewed progress (outpatients), social services were involved when necessary, and patients and their families were nearly always involved in the discussion of after-care, when appropriate. Despite the condescending manner in which patients and carers were treated by the hierarchy, i.e. they would not understand the difference between social services management and other after-care, it was always quite clear to doctors that patients had no difficulty with the concepts of medical intervention (investigations, diagnosis, treatment), psychological therapies, and social help (housing, work, family, finances).
Rather than simplifying the process we now have two tiers of CPA, namely, standard and enhanced. Where the patient has ‘complex needs’ or is a ‘complicated case’ then you are in the enhanced bracket. For the rest – back to the General Practitioner (GP)! Not enough resources apparently. Not ill enough more likely. Remember – you have to have a severe and enduring mental health disorder – nothing else counts. Nowadays the GP is expected to be a specialist in mental health and run a risk assessment on every ‘psychiatric’ patient. The GP is frowned upon by the ‘experts in living’ should he/she for example, dare refer a mild or moderately (yes - those descriptions again!) ill patient to the Mental Health Services. Because there is no bottomless pit of money, the scenario was changed in 2008 so that those receiving only standard CPA were no longer entitled to it. However, not to appear callous and indifferent to the plight of those suffering from ‘less severe’ mental health problems, the usual lip service was paid to patients, assuring them that they should be respected and supported, and that their carers be also recognised as having ‘needs’. All the buzz words were put in place again – integrated care pathways, working together, reviews about the reviews, good practice, better training, and so forth. Now there is the Supervised Community Treatment Order, (whether you like it or not) and those subject to the new ‘order’ will be entitled to the ‘new’ CPA. Wonderful in theory.
So what happens to a patient who is not on CPA? We are informed that such patients should still be open to secondary mental health services, should continue to receive clinical support, that reviews should take place regularly, and a social assessment should be available under the new guidance to local authorities FACS (Fair Access to Care Services), readily available on the Internet. The truth of the matter is that only those patients on enhanced CPA will receive immediate support, the rest will have to jump through the usual hurdles to prove they have a severe, enduring mental illness (enduring is not enough) in order to gain access to NHS ‘support’ facilities. Some patients are seen as more deserving than others, for example, those admitted to hospital under the Mental Health Act (voluntary admission may count against you), current or potential risk (theoretically, any patient with a mental health disorder, which seems to defeat the purpose of the exercise) or the presence of a dual diagnosis (depression with alcoholism, or is it the other way round?). Anyway, if in doubt, the patient is entitled to a formal reassessment CPA and may be admitted to the ‘new’ CPA list. If all fails, the patient (remember, one with severe, enduring mental health symptoms) may make a complaint to the local authority or even hire a lawyer.
What is the true state of affairs? To begin with, many patients have enduring mental health problems which are not severe, are not life-threatening, and despite the hardship and drudgery endured, manage to trundle through work, relationships, and family life. Years of talking therapies or psychotropic medication, indeed both, may have only taken the edge off their symptoms. Often symptoms resurge and require alterations or adjustments in medication; sometimes a different psychological approach needs to be considered. Such patients are best left to the fountain of all wisdom, the GP, so it seems. Rather akin to telling the GP to treat for example, a ‘minor’ cardiac problem (say, palpitations) because the ‘specialist unit’ only deals with severe arrhythmias, severe pain, severe disability, ‘severe everything’. It is unfair to expect GPs to make informed decisions concerning psychotropic medication (no more than they should about adjusting chemotherapy drugs) and most would be familiar only with specific therapies such as Cognitive Behavioural Therapy (CBT) or Anger Management, where appropriate. The type of patients described here comprise the majority of those seen in outpatients, yet there is now a growing trend to discharge such patients back to the GP, because he/she is not ‘care co-ordinated’ on enhanced CPA. The burden is on the GP. It does not seem to have registered with politicians or management (doctors included) that chronic schizophrenia is not the same as chronic gastro-oesophageal reflux.
The trend now is for the setting up of Community Clinics (the patient does not necessarily get to see a doctor) where ‘all the other psychiatric problems’ are dealt with. The traditional psychiatric outpatient department is to be abolished, unless of course, GPs do something about this torrid state of affairs now. It could only happen in Psychiatry which seems to me a specialty doomed to oblivion. Family doctors are becoming increasingly irritated by a system or discipline (Psychiatry especially) which seems to ignore their concerns and is more preoccupied with targets (nothing has changed) and outcomes (back to the GP). Even referrals from GPs, who want a medical opinion, are filtered in order to weed out those not worthy to enter the hallowed walls of the Mental Health Institution. Those patients who ‘know the system’ or who are vociferous and make complaints (‘I know my rights’) get to be seen by the Great and Good. Lesser mortals, usually those with serious mental illnesses, do not make any undue demands and are therefore often forgotten or fall by the wayside. A patient with bipolar disorder on lithium is discharged back to a GP who is unsure whether or not the medication needs ‘fine tuning’ at times, should be discontinued, or reinstated were compliance is a problem in one heading for a relapse. As a corollary of that, I am sure most hospital doctors would not know what the acronym ABVD means in the chemotherapy treatment of Hodgkin’s disease. Adjusting psychotropic medication is not quite the same as adjusting an antihypertension regime. Unfortunately, if the patient needs to be referred back into the system the whole Kafkaesque scenario begins again.
A medical colleague once bemoaned to me that psychiatrists are totally out of touch with Medicine. Alas, it seems they are also now out of touch with their medical colleagues.
Many subjects with chronic Hepatitis C Virus (HCV) infection show persistently normal alanine aminotransferase (ALT) levels (PNALT),1-4 and thus formerly defined as ‘healthy’ or ‘asymptomatic’ HCV carriers.1 However, it is now clear that only a minority of these people show normal liver (15-20%).5-7 Therefore, ‘normal ALT’ does not always mean ‘healthy liver.’4
It is known that during the course of HCV infection ALT levels could fluctuate widely, with long periods of biochemical remission.1-4Thus, at least two different subsets of HCV-PNALT carriers exist: patients with temporal ALT fluctuations, that could be within the normal range for several months, and true ‘biochemically silent’ carriers showing persistently normal ALT values.4It means that the observation period should not be shorter than 12 - 18 months, and ALT determinations should be performed every 2 - 3 months.4, 6
Although liver damage is usually mild, 1, 2the presence of more severe chronic hepatitis (CH) or cirrhosis has been reported despite consistently normal liver biochemistry.8Although some studies showed that HCV carriers with normal ALT have mild and rather stable disease, others reported a significant progression of fibrosis in approximately 20-30% of the patients with ALT normality.9The development of hepatocellular carcinoma (HCC) has been also described.10Sudden worsening of disease with ALT increase and histological deterioration has been reported after many years of follow-up.11
Finally, HCV carriers with PNALT may suffer from extra-hepatic manifestations, sometimes more severe than the underlying liver disease: lymphoproliferative disorders, mixed cryoglobulinaemia, thyroid disorders, sicca syndrome, porphyria cutanea tarda, lichen planus, diabetes, chronic polyarthritis, etc.1, 2, 12
Therefore, the possibility of progression to more severe liver damage despite persistently normal biochemistry, the risk of HCC, the possibility of extra-hepatic diseases, and economic considerations, suggest that HCV-infected persons with PNALT should not be excluded a priori from antiviral treatment.1, 2
The earliest guidelines discouraged interferon (IFN) treatment in patients with PNALT because of the cost and side effects of therapy,1, 2 and of the low response rates to IFN monotherapy (<10-15%) with a risk of ALT flares in up to 50% of patients during treatment.9
The introduction of the combination of weekly subcutaneous pegylated-IFN (PEG-IFN) plus daily oral ribavirin (RBV) has led to response rates >50%, with a favourable risk-benefit ratio even in patients with slowly progressing disease.1, 2, 9 The first trial of PEG-IFN plus RBV found a sustained virological response (SVR) in 40% of HCV-1 carriers with PNALT treated for 48 weeks, and in 72% of HCV-2 and HCV-3 treated for 24 weeks.13The efficacy of antiviral treatment with PEG-IFN plus RBVwas subsequently confirmed in clinical practice.14, 15
However, in everyday practice, management of carriers with PNALT may be paradoxically more difficult than that of patients with abnormal ALT levels. Indeed, it is not always so easy to ascertain in the single case whether it should be considered as healthy subject or true patient. Several topics to date remain unresolved: Should these ‘seemingly healthy’ people undergo routine liver biopsy? Is antiviral treatment justified in ‘asymptomatic’ subjects with persistently normal liver biochemistry? Is long-term follow-up needed in this setting, and how long it should last?2
Liver biopsy provides helpful information on liver damage, as it may reveal the presence of advanced fibrosis or cirrhosis. Without a biopsy, it is impossible to clinically distinguish true ‘healthy’ carriers from those with CH.4 On the other hand, it is difficult to recommend routine biopsy for all HCV-PNALT .4 The decision to perform a biopsy should be based on whether treatment is being considered, taking into account the estimated duration of infection, probability of disease progression, willingness to undergo a biopsy, motivation to be treated, and availability of non-invasive tools to assess liver fibrosis.12 The recently developed transient elastography has improved our ability to non-invasively define the extent of fibrosis in HCV persons.5
Careful evaluation of parameters associated with disease progression is mandatory to assess the actual need for antiviral treatment.4 Indeed, it is really impossible to suggest antiviral therapy in all HCV carriers, as the costs would be exceedingly high, due to the high number of HCV patients with PNALT. Data from the literature indicate that the main factors of progression are male gender, advanced age, severe fibrosis, ALT flares, and steatosis.1-2
Cost/benefit might be particularly favourable in:
Young patients, having high rate of SVR (e.g. females, low viral load, HCV genotype non-1, etc).
Middle age patients with ‘significant’ liver disease and/or co-factors of progression of liver damage, thus at risk of developing more severe liver disease.12
The age issue has a critical role for decision making. Younger patients have a higher chance of achieving SVR and tolerating therapy better; they a have longer life expectancy, are often well motivated, usually have minimal disease and fewer contraindications. Thus, in this group decision to treat should be based more on expected response and motivation than on the severity of liver disease.
On the contrary, older patients respond less well to therapy, are more likely to have significant liver disease and/or co-factors, could experience more side effects and may be less motivated. Thus, in this group decision to treat should be based on the severity of liver disease and on the possibility of SVR.
A recent Italian Expert Opinion Meeting suggested the following recommendations:12
HCV carriers with PNALT may receive antiviral treatment with PEG-IFN plus RBV using the same algorithms recommended for HCV patients with abnormal ALT.
Decision making should rely on individual characteristics such as HCV genotype, histology, age, potential disease progression, probability of eradication, patient motivation, desire for pregnancy, co-morbidities, co-factors, etc.
Treatment might be offered without liver biopsy in patients with a high likelihood of SVR (e.g. age <50 years + non-1 HCV genotype + low viral load), in the absence of co-factors of poor responsiveness.
Inpatients aged 50–65 years, and in those with a reduced likelihood of achieving a response, biopsy may be used to evaluate the need for therapy, with treatment being recommended only for patients with more severe fibrosis and higher possibility of SVR. Biopsy and therapy are not recommended in the elderly (>65-70 years).
In patients who are not candidates for antiviral treatment, follow-up may be continued, and ALT should be monitored every 4-6 months. Avoidance of alcohol and obesity may be strongly recommended.12 It is not clear whether these subjects should be routinely offered anti-HBV vaccine, given the risk of disease progression in the case of HBV infection.12 Antiviral treatment should be re-considered in the case of ALT flares, US abnormalities or platelet count decrease. Repeated measurements of serum HCV RNA to evaluate disease progression is not recommended.1, 9, 11, 12.
Hyperthyroidism is one of the most frequently encountered conditions in clinical endocrinology.1 The modes of treatment available are antithyroid drugs, surgery and radioiodine (RAI) and although each of these is highly successful in controlling or curing hyperthyroidism none leads to permanent euthyroidism on a consistent basis. 2 Although over the last three decades RAI therapy has replaced surgery as the leading form of definitive treatment 3,4, 5 there is no universally accepted dose or regime for its use. Previous attempts to individualise the dose of RAI to reduce the rate of post-RAI hyper- or hypothyroidism have been unsuccessful 6, 7. Fixed dose RAI administration has therefore become the most commonly used regime although the actual dose of RAI used varies considerably and ranges between 185MBq to 600MBq 8, 9. For the last two decades we have used a fixed RAI dose of 550MBq for all patients. Others have used this regime with a high success rate 10 and a prospective head to head comparison with the calculated dose method found the fixed dose regimen to be superior for curing Graves’ hyperthyroidism 11.
Conflicting results have been produced in several studies that have attempted to predict outcome following RAI therapy by correlating cure rate with various pre-treatment factors including age, gender, aetiology of hyperthyroidism, goitre size, use of antithyroid drugs, free thyroxine levels at diagnosis and thyroid antibody status. Various forms of calculated or low fixed dose RAI therapy have been used in these studies but no study used a high fixed dose of 550MBq. In this study we have evaluated the overall success rate of high fixed dose RAI therapy and attempted to identify simple clinical predictors of failure to respond the initial RAI dose.
Patients and Methods
The study is a retrospective analysis of 584 consecutive patients referred to the Shropshire endocrinology service (Princess Royal Hospital and Royal Shrewsbury Hospital) over a 14 year period for the treatment of hyperthyroidism. These patients received RAI therapy at Royal Shrewsbury Hospital, which is the only centre providing facilities for RAI administration in the county of Shropshire and also draws referral from adjoining trusts in Powys, North Wales. Information for this study was obtained from the thyroid database which is maintained on all patients who have received RAI since 1985 at the above hospitals.
RAI was administered both as a primary (53%) and as secondary (47%) treatment. A majority of patients with moderate to severe hyperthyroidism were rendered euthyroid by antithyroid drugs (ATD). Ninety percent (518/584) patients were pre-treated to euthyroidism by antithyroid drugs (carbimazole in 95% and propylthiouracil in 5%) before RAI therapy. Carbimazole was withdrawn one week and propylthiouracil 4 weeks prior to RAI therapy. A standard RAI dose of 550MBq was administered to all patients without a prior uptake study. Thyroid function was measured at 6 weeks and at 3, 6 and 12 months following RAI therapy. ATD drugs were not recommenced routinely following RAI therapy and were reserved for patients who were persistently and significantly hyperthyroid following RAI administration. Patients who developed clinical and biochemical hypothyroidism after the initial 6-8 weeks were commenced on thyroxine. Patients with high free thyroxine level (FT4) and a suppressed thyroid stimulating hormone (TSH) level and those on antithyroid medication were defined as being hyperthyroid, those with low FT4 or on thyroxine as hypothyroid and those with normal FT4 and a normal or low TSH as euthyroid. At the end of one year if a patient remained hyperthyroid, another RAI dose of 550MBq was administered. The patient was considered to have been “cured” if euthyroidism or hypothyroidism was achieved during the first year following RAI therapy and “not cured” if patient remained persistent hyperthyroidism at the end of this period.
Information recorded on the database included age, gender, aetiology, indication (primary or secondary), dose of RAI, number of RAI doses, name and duration of antithyroid drugs used, if any, and FT4 and TSH levels at diagnosis, at the time of RAI therapy and at 6 weeks, 3, 6 and 12 months after RAI therapy. Diagnosis of Graves’ disease was based on the presence of Graves’ ophthalmopathy or a combination of a diffuse goitre and a significant titre of thyroid peroxidase antibodies or if radionuclide scan showed diffuse uptake. Toxic nodular disease was diagnosed on the grounds of a nodular goitre and a focal increase in radionuclide uptake. Patients who could not be classified to either of the groups on clinical grounds and where a radionuclide scan could not be performed for a variety of reasons, were categorised as “unclassified” on aetiological grounds.
Statistical analysis
Continuous random variables were compared using t-tests and association of categorical variables by using chi-squared tests. The effect on outcome (cure of hyperthyroidism) of all variables was assessed by using logistic regression analysis and a step-wise routine was applied to choose the best set of predictors. All analyses were carried out by using NCSS2000.
Results
Data on 584 patients was included with a mean age of 56 years (range 20-90) and a female preponderance (82%). Assessment of the aetiology of hyperthyroidism was made by the above-mentioned criteria. In 110(15%) patients precise aetiological diagnosis could not be made. 344/474 (72%) patients had hyperthyroidism secondary to Graves’ disease and 134/474(28%) had toxic nodular disease. 518 patients received pre-RAI antithyroid medications. Mean free thyroxine level at time of diagnosis was 45.4pmol/L in 259 patients in whom this information was available. Data for thyroid status at 3, 6, and 12 months post-radioiodine were available in 97, 94 and 100% patients respectively (see Table 1).
Table 1: Thyroid status at 3, 6 and 12 months
Euthyroid (%)
Hypothyroid (%)
Hyperthyroid (%)
3 months
308 (54%)
176 (31%)
87 (15%)
6 months
210 (38%)
280 (51%)
59 (11%)
12 months
134 (23%)
411 (70%)
39 (7%)
FT4 values were entered onto the database more recently and this result was available in 259 patients. The group of patients where FT4 data was available was comparable to the group where this information was not available in all respects apart from age (mean age (SD) 54 (±15) vs 58 (±14) years respectively, p<0.02). Similarly, the group of patients in whom the aetiology could not be ascertained was not different from the group where the aetiology could be identified in any respect apart from the age (mean age (SD) 60 (±13) vs 55 (±15) respectively).
Table 2 – Forward Stepwise (Wald) logistic regression analysis to identify factors independently associated with failure to respond to first dose of RAI
Variables
P value
Adjusted r2; OR (95% CI)
Free T4 at diagnosis
0.005
0.084; 1.04 (1.01-1.07)
Free T4 > 45 pmol/l at diagnosis*
0.02
0.056; 3.43 (1.17-10.04)
Age
0.81
N/A
Gender
0.18
N/A
Aetiology
0.23
N/A
Pre RAI use of anti-thyroid drugs
0.42
N/A
* Regression analysis carried out with free T4 as a continuous variable and separately as a categorical variable at a cut off of 45pmol/l
One year following RAI treatment, 543(93%) patients were either euthyroid (162;28%) or hypothyroid (383;65%) and considered “cured”; 39(7%) patients remained hyperthyroid and required further doses of RAI, with 34(6%) patients requiring two doses and 5(1%) patients three doses. At 3 months, 484 out of 571 (85%) patients, and at 6 months, 490 out of 549 (89%) patients were “cured” (table 2). On univariate analysis no correlation could be established between the failure to respond to the first dose RAI and age, gender, aetiology or use of antithyroid medication (p = ns for all) although the rate of hypothyroidism was significantly higher at the end of one year in patients with Graves’ disease as compared to those with toxic nodular disease (77.1% vs. 50.3%, p<0.01). These results were not affected by limiting the analyses to any of the following groups: only those patients in whom the aetiological diagnosis could be made (n=478), only those patients in whom FT4 value was available (n=259) or only those patients where both FT4 was available and aetiology could be ascertained (n=209). On univariate analysis FT4 at diagnosis was associated with the outcome when it was used as a continuous variable (p<0.05) or as a categorical variable with the cut off set at mean FT4 value of 45pmol/L (p=0.01) and high values were associated with failure to respond to the first dose of RAI (mean ± SD, 57.28±20.1 v 44.58±16.1 pmol/L, p<0.05). On multivariate analysis with all variables, FT4 was found to be independently associated with outcome and again this association was seen when FT4 was used as a continuous variable (p=0.01) as well as a categorical variable (p=0.02). On using step-wise selection routine only FT4 could be chosen as a predictor when criterion for selection was set at p=0.05 and a value of over 45pmol/L predicted failure to respond to the first dose of RAI.
Discussion
The use of a standard fixed-dose RAI therapy is gaining increasing popularity and several studies have now shown that formal estimation of the required dose based on the thyroid size and iodine kinetics does not lead to a higher cure rate 6,7,10,11 or a lowerhypothyroidism rate 7. For several years we have used 550MBq dose for all patients of hyperthyroidism. The overall success rate with this regime was 93% and only 7% of patients required a repeat RAI dose. These figures are comparable to those from most other centres, which have used a similar dose of RAI 10. In addition to achieving a high cure rate, hyperthyroidism was controlled rapidly with 85% of the patients becoming either euthyroid or hypothyroid within 3 months of treatment. Early onset of hypothyroidism (>70% at 12 months) facilitated institution of thyroxine replacement therapy during the first year during which the patients were being closely followed.
The use of a relatively higher dose of RAI leads to more stringent restrictions to the normal life of patients and these have to be followed for a longer period of time than is the case with the use of a lower dose. Majority of patients accept these restrictions at the prospect of a cure of hyperthyroidism. However, even at this dose, 7% of patients required repeat dosing which in turn led to another restrictive period for these patients. In view of this it is useful to be able to predict failure of the first dose in an individual patient. This would enable us to warn these patients about the higher possibility of requiring repeat dosing, further period of post-RAI restrictions and target them for a closer follow up. To allow us to make this prediction we correlated simple clinical pre-treatment variables to the need for repeat dosing. We found that there was no statistically significant correlation between age, gender, aetiology and the use of anti-thyroid medication prior to RAI and the outcome following RAI therapy although a high free thyroxine level at diagnosis predicted a failure of the first dose to achieve a cure of hyperthyroidism. There are several conflicting reports in the literature on the correlation between these factors and the response to RAI therapy. Most of the studies have failed to show a significant association between the age of the patient and the outcome irrespective of whether the age was used as a continuous or a categorised variable 12-15 although in a study where a standard 150 gray RAI was used age >50 was found to be associated with a higher failure rate 16. In one study, male gender was associated with a lower cure rate following a single dose of RAI in patients with Graves’ disease 12 although others have failed to confirm this association 13,14. Use of antithyroid drugs prior to RAI has been shown to independently reduce the success rate of RAI 17, 18 while other studies have shown such an association with the use of propylthiouracil but not with carbimazole 19, 20. Literature on the association between the aetiology of hyperthyroidism and the outcome is even more confusing. Patients with toxic nodular disease have been considered to be more radio-resistant as compared to patients with Graves’ disease 21 although opposite results have also been noted 22. In other studies no correlation could be established on multivariate analysis between the aetiology and outcome following RAI 14, 18. Our study is the only one which analyses the influence of these factors on the outcome following the use of a standard 550MBq RAI dose and the above studies which have attempted to identify clinical predictors of outcome have either used various forms of the calculated dose regime or a lower fixed-dose RAI regime. We feel that this is the reason for the inconsistencies in the results and when a 550MBq dose RAI is used only FT4 value at diagnosis could predict the failure of RAI therapy to achieve cure. This dose of RAI appears to override the variations in the response induced by the remaining pre-treatment variables studied.
Studies using smaller doses or calculated doses of RAI have shown the outcome to be inversely associated with the thyroid size 14, 16 although this could not be ascertained in our study due to the lack of consistent documentation of the size ofgoitre in the clinical notes. In addition there are several possible confounding factors. Firstly the overall cure rate could have been influenced by the long period of time over which patients have been included (15 years) and the resulting changes in the criteria and threshold for the use of RAI. However if we divide the figures into 3 time periods of 5 years each, the findings remain consistent during each of these periods. Secondly, in over 50% of our patients, RAI was administered as a primary measure and it could be argued that a larger number of patients with milder hyperthyroidism may have been included in our cohort as compared to the patients at other centres where RAI is mainly reserved for patients who fail to respond to ATD. However there was no significant difference in the cure rate between those patients who received RAI as a primary measure and those in whom RAI was administered as a secondary treatment (94% v 93%). Thirdly in 15% of patients the aetiology could not be ascertained by using our well-defined criteria, mainly because of the practical difficulty of performing radionuclide scans in some of the patients where the diagnosis could not be made clinically. We do not feel that our results on the association between the aetiology and the cure rate were affected, as the patients with undefined aetiology were comparable to the remaining patients in all respects apart from age and had similar outcomes. Lastly the information on the FT4 value at diagnosis was available in only 259 patients. To exclude a selection bias this group was compared to the group of patients where this information was not available. Again the only difference between the two groups was the age distribution. In both instances this difference was not large (though statistically significant) and we do not feel it affected the outcome, especially as age does not appear to influence the outcome following RAI therapy. We could not assess the impact of post-RAI use of antithyroid drugs as these were not routinely restarted following RAI therapy at our centre.
In conclusion, high fixed dose RAI therapy is a very effective treatment for patients with hyperthyroidism and has a high success rate. Failure to respond to this dose cannot be predicted by most of the pre-treatment variables apart from the severity of the hyperthyroidism as judged by the FT4 value at diagnosis. Patients who present with severe hyperthyroidism should be warned regarding the higher possibility of requiring further doses of radioiodine even when treated with a dose of 550MBq.
A 78 year old man was admitted for re-fashioning of a prolapsing colostomy. Nine months previously he had undergone a juxtarenal aortic aneurysm repair complicated by ischaemic colitis, for which he had a sigmoid colectomy and a further laparotomy for refashioning of the stoma.
His past medical history consisted of anaemia, stable angina, superficial bladder cancer, Stage 4 chronic kidney disease, type 2 diabetes mellitus and osteoarthritis. He weighed 77 kg and his exercise tolerance was 100 yards, with the aid of a stick. His medications included doxazosin, quinine sulphate, perindopril, simvastatin, ferrous sulphate, isosorbide mononitrate and aspirin.
On examination, he was apyrexial with a blood pressure of 170/70 mm Hg, a heart rate of 65 bpm, a respiratory rate of 14 bpm and Sa02 of 98% on room air. Serum laboratory tests showed a prothrombin time of 13.4 sec (normal range 9.0 – 13.0 sec), haemoglobin 10.2 g/dL (13.0 – 16.7 g/dl), platelets 131 x109/L (150 – 400 x109/L), sodium 139 mmol/L, potassium 4.2 mmol/L, urea 15.7 mmol/L (2.5 – 7.0 mmol/L), creatinine 196 umol/L (50 – 130 umol/L) and eGFR 29 ml/min/1.73m2 (>60ml/min/1.73m2).
His preoperative pulmonary function tests showed an FVC of 2.78L (93.8% predicted), a reduced FEV1 of 1.66L (75.2% predicted) and FEV/FVC of 59.87%. His ECG showed normal sinus rhythm. A CPEX test taken 12 months previously showed moderately reduced peak aerobic capacity, with a peak V02 of 11 ml/kg/min and an anaerobic threshold (AT) of 7 ml/kg/min.
In the anaesthetic room, the patient was connected to standard monitoring in accordance with AAGBI Guidelines and venous access secured with an 18 g biovalve cannula. Following pre-oxygenation, anaesthesia was induced using fentanyl 200 mcg, midazolam 2 mg, propofol 120 mg and atracurium 50 mg. Tracheal-intubation was achieved (grade 1 view) using an 8.0 mm cuffed endotracheal tube (lo-contour). A TAP block was administered following induction using ultrasound guidance (Sonosite ‘micromax’). A 50 mm insulated Stimi-Plex needle was used to inject a total of 40 ml levobupivacaine 0.375% bilaterally. Anaesthesia was maintained using a mixture of air, oxygen and sevoflurane (1.3 – 2.3 ETAA range). Intravenous (IV) paracetamol 1 g was given intraoperatively. The prolapsing colon was dissected through a circumstomal incision. A 10 cm length of colon was resected after ligation and division of the mesenteric vessels. The new end colostomy was fashioned with interrupted mucocutaneous sutures. Blood loss was minimal and there were no intraoperative complications. The duration of surgery was 1.5 hrs.
The patient spent 30 minutes in the postoperative recovery unit. He was awake, orientated and pain free throughout this period and clinical observations were stable. The patient remained pain-free on the ward and did not require any postoperative opioids. He was medically fit for discharge the following day.
Discussion
There are no previous case reports to our knowledge describing the use of TAP blocks in a patient with such poor CPEX testing preoperatively (AT = 7 ml/kg/min). CPEX testing has been shown to be an independent predictor of morbidity, mortality and length of hospital stay after major abdominal surgery.1 The anaerobic threshold marks the onset of anaerobic metabolism as a result of inadequate oxygen delivery. It is not affected by patient effort and therefore provides a reliable patient specific measurement of functional capacity.2 An AT of at least 11 ml/kg/min is recommended to safely undertake major surgery.2 A combination of an AT of <11 ml/kg/min with ECG evidence of myocardial ischaemia is associated with high mortality and poor outcome. 3One study showed a mortality of 42% in those with ischaemic heart disease (IHD) and an AT <11 ml/kg/min, compared with just 4% in those with no IHD.4
Postoperative morbidity and mortality most often occurs in patients with pre-existing cardiorespiratory disease and a reduced functional capacity, due to their inability to withstand the additional physiological demands placed upon them by major surgery. Many of these patients develop features of organ hypoperfusion due to poor cardiorespiratory reserve.5
Our patient had an AT of 7 ml/kg/min and poor respiratory reserve (exercise tolerance of 100 yards, FEV/FVC 59.87% of predicted) but underwent uneventful intra-abdominal surgery with a good recovery and short length of hospital stay. Contributing factors may have been the anaesthetic technique used, as well as the surgical approach via a parastomal incision. Good intraoperative and postoperative control of cardiovascular parameters, temperature and pain are well known to reduce the surgical stress response and postoperative morbidity, and to improve postoperative outcome.6 Our patient was cardiovascularly stable throughout the perioperative period. His pain was well controlled with no opioid requirements due to the use of bilateral TAP blocks, and this probably contributed to his uneventful recovery, with no critical care requirement.
CPEX testing is not universally accepted as a useful preoperative assessment tool. In studies assessing it as a reliable predictor of outcome, there is heterogeneity in the degree of clinician blinding used. Blinding was used in some studies,1 whilst in other instances, clinicians were aware of the CPEX results and changed their management accordingly. This obscures the true relationship between patient outcome and CPEX-derived measures of risk.7
TAP blocks were first described in 20018 and have been shown to significantly reduce postoperative morphine consumption following abdominal surgery by up to 70%. They reduce pain scores at rest and during mobilisation in the early postoperative period (0-6 hours), and in the first 24 hours.9 The reduced requirement for morphine also leads to a reduction in postoperative nausea, vomiting and sedation.9 It may be possible that the ultrasound guided TAP block confers advantages in procedures with moderate surgical trauma to minimize pain and reduce opioid usage, thereby promoting faster recovery and discharge.8 TAP blocks were the chosen method of analgesia in our patient as they would elicit the least physiological disturbance, but would provide good postoperative analgesia, without opioid-related side effects. This was particularly beneficial, as his pre-existing renal impairment put him at increased risk of opiate toxicity. TAP blocks eliminate somatic pain relating to the surgical incision but do not treat visceral pain. However, our patient tolerated a 10 cm bowel resection with bilateral TAP blocks and intravenous paracetamol. A similar effect has been observed in other studies but the mechanisms behind it are unclear. One theory is that there is an analgesic effect due to high systemic levels of local anaesthetic.10
The use of CPEX testing to determine fitness for surgery should be interpreted with caution as newer anaesthetic and surgical techniques develop. Our patient had IHD and an AT which showed a significantly increased level of risk. However, a combination of regional anaesthesia and a cardio stable general anaesthetic with minimally invasive surgery, allowed a rapid and uneventful recovery with no opioid requirements and a short length of hospital stay.