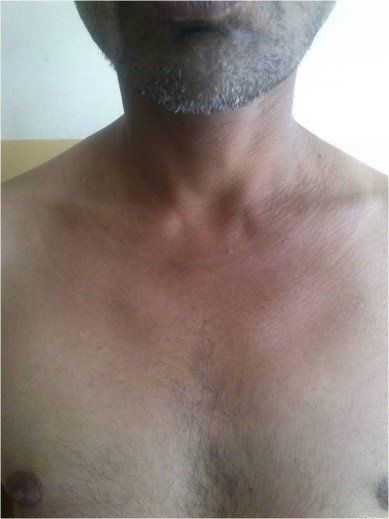
A 40 years old non-alcoholic and non-diabetic agricultural laborer presented with skin lesions around his neck, forearms and feet (sun exposed areas) along with glossitis. Pellagra was suspected because of Casal's necklace (i.e., erythematous, hyperpigmented, scaly lesions around his neck- arrow mark in figure 1). However he did not have diarrhea or neurological manifestations. Pellagra is due to Niacin (Vitamin B3) deficiency. Typical cases of pellagra are associated with 3 Ds - Dermatitis, Diarrhea, Dementia, (and if not treated, the 4th D- Death).1,2 Not many will have all the three Ds. Most commonly involved is skin – dermatitis (Pelle-skin; agra -rough). The patient belonged to poor socioeconomic status.2 His vital parameters and basic investigations were all within normal limits and HIV-ELISA was negative.
The diagnosis of a pellagra-like dermatitis was entertained.3 He was treated with multivitamin capsules which included Niacinamide.2
The skin lesions had disappeared dramatically at the time of follow-up after one month (figure 2).
A dermatoscope is a hand-held device for examining the appearance of the skin. Dermoscopy has become an increasingly used and valued tool in the assessment of various skin lesions, and more recently, inflammatory rashes. It is quick, cheap and when used correctly, dermoscopy is an essential tool in helping clinicians detect early stage skin cancer. Various national and international guidelines recommend routine use of dermoscopy in the assessment of pigmented lesions1,2 because it enhances melanoma detection rates3,4 and can help confirm the diagnosis of benign lesions such as haemangiomas and seborrhoeic keratoses. As with any skill, competency takes time to develop and a combination of various learning and assessment methods is best. The dermatology specialist training curriculum in the United Kingdom (UK) states that trainees should be competent in using a dermatoscope and interpreting findings, while recognizing the limitations of this tool5. Assessment of these clinical skill and behavioural competencies using direct observation of procedural skills (DOPS), case-based discussion (CBD), mini clinical examination (mini-CEX), and/or multisource feedback (MSF) is suggested. There is no specific guidance on what resources a trainee should use to achieve these competencies, nor on what is the minimum expected dermoscopy skillset at completion of specialist training.
The aim of this survey was to explore dermoscopy use amongst dermatology specialist trainee registrars in the UK including frequency of use, how it is being taught and whether trainees feel their dermoscopy training has been adequate.
An online survey was designed and distributed to dermatology trainees in the United Kingdom using an email link and hard copies were distributed at a national dermoscopy course. Respondents who did not identify themselves as dermatology trainees were removed from the analysis. Responses were collected anonymously, then collated and analysed using SurveyMonkey® computer software.
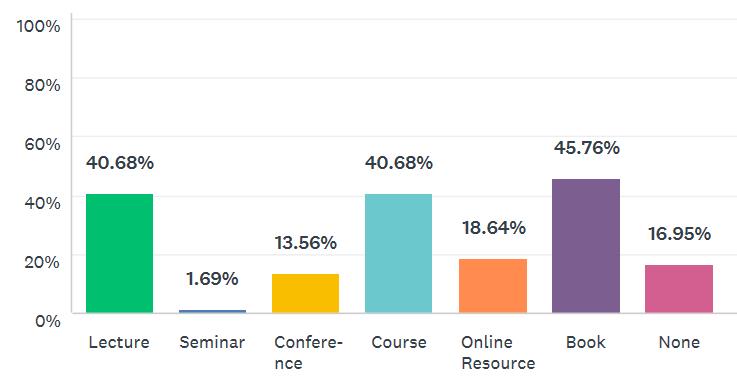
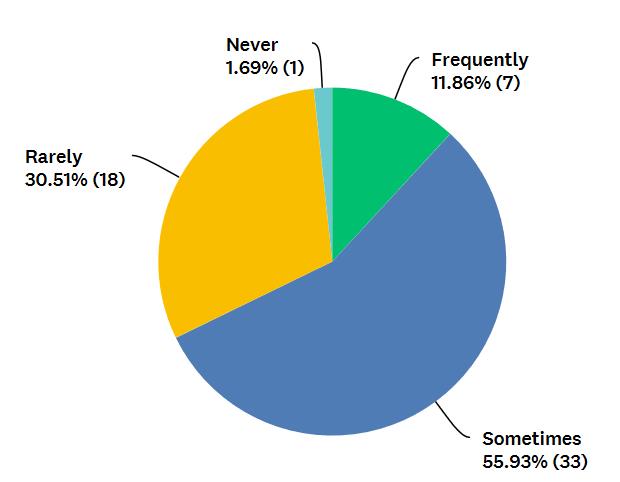
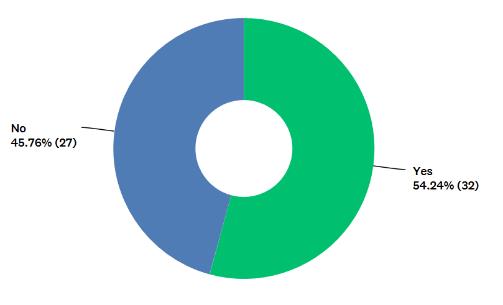
Twenty-five percent (59/238) of dermatology trainees completed the survey. On average, 92% (54/59) use dermoscopy more than once daily. Eighty-five percent (50/59) always use dermoscopy when assessing pigmented lesions while 34% (20/59) always and 59% (35/59) sometimes use it to assess non-pigmented lesions. When asked about specific tools used to learn dermoscopy, 41% (24/59) have been on a previous course, 42% (25/59) reported attendance at a lecture or seminar, 46% (27/59) have used a dermoscopy text book, 14% (8/59) have attended a conference, 19% (11/59) have used online resources. Seventeen percent (10/59) have never used any of the above learning methods. (Figure 1a). Amongst those who have attended a formal dermoscopy course (n=24), 92% (22/24) of these were ≤1 day in duration. When questioned about informal teaching in clinical practice, 12% (7/59) frequently, 56% (33/59) sometimes, 31% (18/59) rarely and 2% (1/59) never receive teaching from their supervising dermatology consultant. (Figure 1b). Fifty-four percent (32/59) feel they have received adequate training in dermoscopy while the remaining 46% (27/59) feel their dermoscopy training is inadequate for their training stage (Figure 1c). Seventy-three percent (43/59) have access to dermoscopic photography within their local dermatology department.
Fig 1a - Have you undertaken any formal study in dermoscopy? 49% of trainees have attended a lecture, 2% a seminar, 14% a conference, 41% a course, 19% have used an online resource, 46% have used a book, 17% have not used any resource.
Fig 1b- Do you receive dermoscopy training from your supervisor in clinic? 56% of trainees sometimes, 31% rarely, 12% frequently, and 2% have never received training from their seniors in clinic.
Fig 1c- Do you believe that you have received adequate training in the use of a dermoscopy for your training grade?
These results of this survey highlight the need for dermoscopy training to be reviewed within the UK national training curriculum for dermatology. Despite daily use by the vast majority, dermoscopy training is largely self-directed and highly variable amongst individual trainees. Of concern, a significant proportion of those who responded feel their dermoscopy skills are inadequate for their training stage. Of note, the 25% response rate means that the results of this survey may not be representative of dermatology trainees in the United Kingdom as a whole.
This is the first time that dermoscopy use has been explored through a national survey of dermatology trainees in the UK, to the best of our knowledge. A survey on dermoscopy use was carried out by The British Association of Dermatologists (BAD) in 20126 but the majority of responses were from dermatology consultants. This confirmed that 98.5% of respondents regularly used dermoscopy, while 81% had received any training. The most frequent source of training was UK based courses, which 62% of respondents reported attending. Of note, 39% of all respondents lacked confidence when making a diagnosis based on their interpretation of dermoscopy findings. It is not clear how many of those lacking in confidence were consultants, trainees or specialty doctors. Although the situation may have improved since 2012, these results do suggest that dermoscopy training needs have not been met for a proportion of doctors across the dermatology community.
Dermoscopy training is an important issue to address for several reasons. The volume of cutaneous lesions being referred to dermatology is increasing, and skin cancer referrals and treatment now account for 50% of a UK dermatologists’ workload7. For every melanoma diagnosed, a dermatologist may expect to see 20–40 benign lesions referred from general practitioners (GPs)7. These facts highlight the importance of maximising diagnostic skills which frequently include using dermoscopy as part of clinial assessment. Lack of adequate training is a common self-reported reason for dermatologists not using dermoscopy8. Both trainees and their supervising bodies have a responsibility to maximize training opportunities and embed the use of dermoscopy in routine practice.
In conclusion, we feel UK dermatology trainees and indeed any clinician who utilizes this tool, would benefit from a more standardized and integrated approach to dermoscopy teaching to ensure safe practice of this skill and deliver high quality evidence-based patient care.
A 70-year-old man presented in the winter with a four-week history of redness of the left anterolateral leg. He first noticed a slight “tenderness” in the area when showering; the discomfort lasted only a few days. Over the next week, he noticed redness developing. It is now painless and not pruritic, warm, or peeling. He has not applied any topical lotions or creams. He has not had an exposure to new soaps or detergents. He feels well, without fever or weight loss. He has a diagnosis of hypertension and lumbar radiculopathy with an L5 discectomy and resultant leg numbness. He is retired and does not smoke or drink alcohol; his hobby is woodworking in his garage.
Physical examination reveals normal vital signs. On his left anterolateral leg, he has an 8 cm, irregular patch of reticulated erythema with both hyperpigmentation and scaling. The lesion is non-palpable. He has decreased sensation in an L5 distribution on that leg, which was unchanged from prior examinations. These skin findings are shown in Figure 1.
Figure 1
Question: Based on history and physical examination, which of the following is the most likely diagnosis?
Livedo reticularis
Erythema ab igne
Livedo racemosa
First-degree burn
Discussion
The answer is erythema ab igne (EAI; literally “redness from fire,”) which results from chronic exposure to moderate-intensity heat. EAI presents as a reticulated erythematous patch over the area of exposed skin. Possible secondary changes include epidermal atrophy and scaling.1,2 With repeated exposure, brown hyperpigmentation may develop.1 Most patients are asymptomatic, although some note a mild burning sensation. A history of repeated exposure to heat is key to the diagnosis. While cases were historically noted on skin exposed to fire, such as the arms of bakers and coal shovellers, EAI can result from our many, modern heat-sources, such as laptop computers, car seat heaters, heating pads, and, in this case, the portable space heater under the patient’s woodworking bench.2-4 With removal of the heat source, hyperpigmentation typically regresses but may take years.1,3 The diagnosis is clinical. A biopsy is not required to make the diagnosis, but is indicated if malignant transformation is suspected. EAI can increase risk of squamous cell carcinoma, Merkel cell carcinoma, and cutaneous marginal zone lymphoma.1,5 Treatment is typically not necessary; topical steroids or retinoids and laser have had variable success.1,3,4 If pre-malignant changes are detected, topical 5-flourouracil is recommended.1,4
See Table 1 for a summary of the key characteristics and distinguishing features of each diagnosis in this selected differential.
Table 1. Selected Differential Diagnosis of Reticulated Skin Lesions in Adults
Condition
Characteristics
Livedo reticularis
Violaceous mottled or reticulated patches; painless; typically temperature sensitive; may be physiologic or secondary to systemic disease; no hyperpigmentation.
Erythema ab igne
Erythematous reticulated patch, with possible secondary changes including epidermal atrophy and scaling; chronic exposure may lead to hyperpigmentation; painless or associated with a mild burning sensation; history of heat exposure.
Livedo racemosa
Violaceous reticulated patch with larger branching pattern than livedo reticularis, often with asymmetric or “broken” net appearance; typically involves the trunk and proximal limbs; generally secondary to chronic disease; frequently painful; no hyperpigmentation.
First-degree burn
Erythematous, dry, painful lesion which includes the entire area of skin that contacted the high-intensity heat source; not reticulated; no hyperpigmentation.
Livedo reticularis is typically more violaceous in appearance, with net-like, mottled discolouration of the skin due to deoxygenation and dilation of the venous plexus. Primary, physiologic livedo reticularis is often brought on by cold and alleviated by warming. It usually involves a larger area, such as the bilateral thighs, rather than a confined area of skin.1,2
Livedo racemosa is a persistent variant of livedo reticularis with a characteristic, large, broken, branching pattern, often on the trunk and proximal limbs. It is generally secondary to a systemic disease, such as antiphospholipid antibody syndrome or Sneddon syndrome.6
First-degree burns are erythematous, dry, and painful. Instead of a reticulated pattern, as shown here, the erythema of first degree burns covers the entire area of skin that contacted the high-intensity heat source.
Striae distensae, or stretch marks, are linear scars in the dermis which arise from rapid stretching of the skin over weakened connective tissue. It is a common skin condition that rarely causes any significant medical problems but is often a significant source of distress to those affected. Striae distensae were described as a clinical entity hundreds of years ago, and the first histological descriptions appeared in the medical literature in 1889.1 With a high incidence and unsatisfactory treatments, stretch marks remain an important target of research for an optimum consensus of treatment. These appear initially as red, and later, as white lines on the skin, representing scars of the dermis, and are characterized by linear bundles of collagen lying parallel to the surface of the skin, as well as eventual loss of collagen and elastin. The estimated prevalence of striae distensae range from 50 to 80%.2,3 The anatomical sites affected vary, with areas commonly affected including the abdomen, breasts, thighs and buttocks.4 The three maturation stages of striae include the acute stage (striae rubra) characterized by raised, erythematous striae, the sub-acute stage characterized by purpuric striae, and the chronic stage (striae alba), characterized by white or hypo-pigmented, atrophied striae.5 Although stretch marks are only harmful in extreme cases, even mild stretch marks can cause distress to the bearer6 (Table 1).
Table 1: Histological comparisons between striae rubrae and striae albae
Epidermis
Oedema Increased melanocytes
Epidermal atrophy Loss of rete ridges Decreased melanocytes
Papillary dermis
Dilatation of blood vessels
No vascular reaction
Reticular dermis
Structural alteration of collagen fibres Reduced and reorganized elastic fibres Fine elastic fibres in dermis
Densely packed collagen parallel to skin surface. Thick elastic fibres in dermis
Inflammatory cells
Lymphocytes and fibroblasts
Eosinophills
Aetiology
Striae may result from a number of causes, including, but not limited to, rapid changes in weight, adolescent growth spurts, corticosteroid use or Cushing Syndrome, and generally appear on the buttocks, thighs, knees, calves, or lumbosacral area.7 In addition, approximately 90% of all pregnant women develop stretch marks either on their breasts and/or abdomen by the third trimester.8 Genetic predisposition is also presumed, since striae distensae have been reported in monozygotic twins.9,10 There is decreased expression of collagen and fibronectin genes in affected tissue.11 The role of genetic factors is further emphasised by the fact that they are common in inherited defects of connective tissue, as in Marfan’s syndrome.12,13 Obesity and rapid increase or decrease in weight have been shown to be associated with the development of SD.14 Young male weight lifters develop striae on their shoulders.15 Striae distensae also occurs in cachetic states, such as tuberculosis, typhoid and after intense slimming diets.16 Rare etiologies include human immunodeficiency virus positive patients receiving the protease inhibitor indinavir and chronic liver disease.13,15 A case of idiopathic striae was also reported.17
Rosenthal18 proposed four aetiological mechanisms of striae formation: insufficient development of tegument, including elastic properties deficiency; rapid stretching of the skin; endocrinal changes; and other causes, possibly toxic.
Pathogenesis
The pathogenesis of striae is unknown but probably relates to changes in the components of extracellular matrix, including fibrillin, elastin and collagen.19 There has been emphasis on the effects of skin stretching in the pathogenesis of striae because the lesions are perpendicular to the direction of skin tension.20 A possible role of glucocorticoids in the pathogenesis of striae has been suggested because of an increase in the levels of steroid hormones and other metabolites found in patients exhibiting striae.21 There are studies suggesting the role of fibroblasts in the pathogenesis of striae. Compared to normal fibroblasts, expression of fibronectin and both type I and type III procollagen were found to be significantly reduced in fibroblasts from striae, suggesting that there exists a fundamental aberration of fibroblast metabolism in striae distensae.22
Pathological aspects
The earliest pathological changes are subclinical to be detected by electron microscopy only. These changes include mast cell degranulation and the presence of activated macrophages in association with mid-dermal elastolysis.23 When the lesions become become clinically visible, collagen bundles start showing structural alterations, fibroblasts become prominent, and mast cells are absent.23 On light microscopic examination, Inflammatory changes are conspicuous in the early stage, with dermal oedema and perivascular lymphocytic cuffing.24 In later stages, there is epidermal atrophy, loss of rete ridges and other appendages including hair follicles are absent.25
Evaluation of striae distensae
Approaches to evaluating SD severity visually include the Davey 26 and Atwal scores,27 although these have not been validated specifically for SD. An objective evaluation of SD may be carried out using skin topography, imaging devices including three-dimensional (3D) cameras, reflectance confocal microscopy and epiluminescence colorimetry.28,29,30
Table 2: Visual scoring systems for the assessment of striae distensae
Davey method
Used for evaluating striae rubrae and albae. Divide the abdomen into quadrants using midline vertical and horizontal lines. Each quadrant given a score (0 no SD; 1 moderate number of SD; 2 many SD). Score given out of 8.
Atwal score
Used for evaluating striae rubrae and albae. Six sites chosen (abdomen, hips, breasts, thigh/buttocks). Each site given a maximum score of six. Total score out of 24. Score 0–3 for the presence of striae (0 no SD; 1 < 5 SD; 2 5–10 SD; 3 > 10 SD). Score 0–3 for the presence of erythema (0 no erythema; 1 light red/pink; 2 dark red; 3 purple).
Management
Striae distensae (striae alba) is a very challenging cosmetic problem for dermatologists to treat. Various modalities of treatment have been tried. Although therapeutic strategies are numerous, there is no treatment which consistently improves the appearance of striae and is safe for all skin types.31 Weight loss by diet alone or a combination of diet and exercise do not change the degree of striae distensae.32
Topical treatments
Topical tretinoin (0.1%) ameliorates striae and the improvement may persist for almost a year after discontinuation of therapy.33 More recently, tretinoin has been shown to improve the clinical appearance of stretch marks during the active stage (striae rubra), although with not much effect during the mature stage (striae alba).34 Some of the studies have proven the inefficacy of the vitamin A derivative in the treatment of SD, but most of the patients included in these early studies presented with old lesions that had evolved into whitish atrophic scars.35 A study comparing topical 20% glycolic acid and 0.05% tretinoin versus 20% glycolic acid and 10% L-ascorbic acid, found that both regimens improved the appearance of striae alba.36
Hydrant Creams: 1) Trofolastin (a cream containing Centella asiatica extract, vitamin E, and collagen-elastin hydrolysates). The exact mechanism of action was identified as the stimulation of fibroblastic activity 37 and an antagonistic effect against glucocorticoids.38 2) Verum (a cream containing vitamin E, panthenol, hyaluronic acid, elastin and menthol). The results suggest that the product may show the benefit of massage alone.39 3) Alphastria (a cream composed of hyaluronic acid, allantoin, vitamin A, vitamin E, and dexpanthenol). Only one study was conducted, which concluded that the product markedly lowered the incidence of stretch mark development after pregnancy.40
Glycolic acid (GA): The exact mechanism of action of GA in the management of striae distensae is still unknown because, although GA is reported to stimulate collagen production by fibroblasts and to increase their proliferation in vivo and in vitro, which may be useful for the treatment of stretch marks.41,42 A study comparing topical 20% glycolic acid and 0.05% tretinoin versus 20% glycolic acid and 10% L-ascorbic acid, found that both regimens improved the appearance of striae alba.43
Trichloroacetic acid (TCA; 10–35%): It has been used for many years as a treatment option for striae distensae and is repeated at monthly intervals with reported improvement in texture and color of marks.44
Other topical products: Several oils have been used in the prevention of SD. A non-randomized, comparative study investigated the effect of almond oil in the prevention of SD in which they noted significant differences in the frequency of SD between the groups (almond oil and massage 20%, almond oil alone 38.8%, control 41.2%).45
Overall, there is limited evidence for the efficacy of topical therapy for the treatment of SD.
Microdermabrasion
Microdermabrasion may improve many skin problems including acne scars, skin texture irregularities, mottled pigmentation and fine wrinkles. Karimipour et al reported that microdermabrasion induces epidermal signal transduction pathways associated with remodelling of the dermal matrix.46 However, studies documenting the efficacy of rnicrodermabrasion in treatment of striae are lacking. Published in 1999, a book on microdermasion written by a French dermatologist, Francois Mahuzier, and translated to English, has a chapter "Microdermabrasion of stretch marks”.47 The author states that 10-20 sessions of microdermabrasion at an interval of not less than 1 month, each session resulting in bleeding points, provide satisfactory results. The author concludes that, "microdermabrasion is the only effective treatment of stretch marks today."
Lasers
Lasers have recently become a popular therapeutic alternative to ameliorate and improve the appearance of stretch marks. Most commonly used lasers used include pulsed-dye laser (PDL), short- pulse carbon dioxide and erbium-substituted yttrium aluminium garnet (YAG), neodymium- doped YAG (Nd:YAG), diode, and Fraxel.
Pulsed dye laser: The dilated blood vessels render the striae rubrae a good candidate for PDL.48 The 585- nm pulsed dye laser has a moderate beneficial effect in the treatment of striae rubra.49 To evaluate the effectiveness of the 585-nm flashlamp-pumped pulse dye laser in treating cutaneous striae, 39 striae were treated with four treatment protocols.50 Subjectively, striae appeared to return toward the appearance of normal skin with all protocols. Objectively, shadow profilometry revealed that all treatment protocols reduced skin shadowing in striae. Laser treatment of SD should be avoided or used with great caution in darker skin types (IV–VI), because of the possibility of pigmentary alterations after treatment.51
Excimer laser: Studies have shown temporary repigmentation and improvement of leukoderma in SD with excimer laser, although it failed to show any improvement in skin atrophy.52,53 To evaluate the true efficacy of the 308-nm excimer laser for darkening striae alba, 10 subjects were treated using the excimer laser on the white lines of striae, while the normal skin near to and between the lines was covered with zinc oxide cream. The results of this study showed the weakly positive effect of the 308-nm excimer laser in the repigmentation of striae alba.54
Copper Bromide laser: copper-bromide laser (577-511 nm) has been used for stretch marks. A clinical study was conducted in 15 Italian women with stretch marks, treated with the CuBr laser (577-511 nm) and followed-up for 2 years.55 The results of the study concluded that the copper-bromide laser was effective in decreasing the size of the SD and there were some pathogenic considerations that justified the use of this laser.
1,450-nm Diode Laser: The non-ablative 1,450-nm diode laser has been shown to improve atrophic scars and may be expected to improve striae. To evaluate the efficacy of the 1,450-nm diode laser in the treatment of striae rubra and striae alba in Asian patients with skin types 4-6, striae on one half of the body in 11 patients were treated with the 1,450-nm diode laser with cryogen cooling spray with the other half serving as a control.56 None of the patients showed any noticeable improvement in the striae on the treated side compared to baseline and to the control areas. The study concluded that the non-ablative 1,450-nm diode laser is not useful in the treatment of striae in patients with skin types 4, 5, and 6.
1,064-nm Nd:YAG Laser: A study was aimed to verify the efficacy of this laser in the treatment of immature striae in which 20 patients with striae rubra were treated using the 1,064-nm long-pulsed Nd:YAG laser.57 A higher number of patients (55%) considered the results excellent when compared to the same assessment made by the doctor (40%).
Intense Pulsed Light: In order to assess the efficacy of IPL in the treatment of striae distensae, a prospective study was carried out in 15 women, all of them having late stage striae distensae of the abdomen.58 All the study subjects showed clinical and microscopical improvement after IPL. It seems to be a promising method of treatment for this common problem with minimal side-effects, a wide safety margin and no downtime.
Fractional Photothermolysis: To determine the efficacy of fractional photothermolysis in striae distensae, 22 women with striae distensae were treated with two sessions each of fractional photothermolysis at a pulse energy of 30 mJ, a density level of 6, and eight passes at intervals of 4 weeks and response to treatment was assessed by comparing pre- and post-treatment clinical photography and skin biopsy samples.59 Six of the 22 patients (27%) showed good to excellent clinical improvement from baseline, whereas the other 16 (63%) showed various degrees of improvement. This study concluded that Fractional photothermolysis may be effective in treating striae distensae, without significant side effects.
Ablative 10,600-nm carbon dioxide fractitional laser: Ablative 10,600-nm carbon dioxide fractional laser systems (CO₂ FS) have been used successfully for the treatment of various types of scars. To assess the therapeutic efficacy of CO₂ FS for the treatment of striae distensae, 27 women with striae distensae were treated in a single session with a CO₂ FS and clinical improvement was assessed by comparing pre- and post-treatment clinical photographs and participant satisfaction rates.60 The evaluation of clinical results 3 months after treatment showed that two of the 27 participants (7.4%) had grade clinical 4 improvement, 14 (51.9%) had grade 3 improvement, nine (33.3%) had grade 2 improvement, and two (7.4%) had grade 1 improvement. None of the participants showed worsening of their striae distensae.To assess and compare the efficacy and safety of nonablative fractional photothermolysis and ablative CO(2) fractional laser resurfacing in the treatment of striae distensae, 24 ethnic South Korean patients with varying degrees of atrophic striae alba in the abdomen were enrolled in a randomized blind split study and were treated with 1,550 nm fractional Er:Glass laser and ablative fractional CO(2) laser resurfacing.61 These results of the study support the use of nonablative fractional laser and ablative CO(2) fractional laser as effective and safe treatment modalities for striae distensae of Asian skin with neither treatment showing any greater clinical improvement than the other treatment.
UVB/UVA1 Combined Therapy: Besides lasers, light sources emitting ultraviolet B (UVB) irradiation have been shown to repigment striae distensae. A study was conducted on 9 patients with mature striae alba who received 10 treatment sessions, and biopsies were taken at the baseline and end of the study.62 At the end of the study, all patients reported some form of hyperpigmentation that was transient and did not affect any surrounding tissues. No changes were seen on biopsy to indicate an effective remodelling collagen effect of the device, although it needs further assessment. Another study was conducted to analyse the histologic and ultrastuctural changes seen after UVB laser- or light source-induced repigmentation of striae distensae in which analyses of biopsied skin after treatment with both the UVB laser and light source showed increased melanin content, hypertrophy of melanocytes, and an increase in the number of melanocytes in all patients.63
Radiofrequency devices: RF devices are based on the principle of heat generation that occurs in response to poor electrical conductance according to Ohm’s law (heat generation is directly correlated with tissue resistance). The heat that is generated is sufficient to cause thermal damage to the surrounding connective tissue,64 which is responsible for the partial denaturation of pre-existing elastic fibers and collagen bundles.65 Initial collagen denaturation within thermally modified deep tissue is thought to represent the mechanism for immediate tissue contraction; subsequent neocollagenesis further tightens the dermal tissue and reduces striae.66 The efficacy and safety of combination therapy with fractionated microneedle radiofrequency (RF) and fractional carbon dioxide (CO2) laser in the treatment of striae distensae has been evaluated revealing that this combination therapy is a safe treatment protocol with a positive therapeutic effect on striae distensae.67 A recent study evaluating the effectiveness of a RF device in combination with PDL subjected 37 Asian patients with darker skin tone with SD to a baseline treatment with a RF device and PDL.68 All histological evaluations demonstrated an increase in the amount of collagen fibers, and six of the nine specimens showed an increase in the number of elastic fibers.TriPollar RF device appears to be a promising alternative for the treatment of striae distensae in skin phototypes IV-V.69
Needling therapy:
To evaluate the effectiveness and safety of a disk microneedle therapy system (DTS) in the treatment of striae distensae, 16 Korean volunteers with striae distensae alba or rubra were enrolled which received three treatments using a DTS at 4-week intervals.70 Marked to excellent improvement was noted in seven (43.8%) patients, with minimal to moderate improvement in the remaining nine. This study revealed that Disk microneedle therapy system (DTS) can be effectively and safely used in the treatment of striae distensae without any significant side effects. Another study assessed and compared the efficacy and safety of needling therapy versus CO2 fractional laser in treatment of striae and the results supported the use of microneedle therapy over CO2 lasers for striae treatment.71
Platelet-rich plasma:
Platelet-rich plasma has these wound-healing properties, affecting endothelial cells, erythrocytes, and collagen,72 which potentially aids in the healing of the localized chronic inflammation believed to be a factor in the aetiology of striae distensae. Platelet-rich plasma is well tolerated by the patients and is a safe and cost effective treatment option for striae distensae.
Platelet-rich plasma alone is more effective than microdermabrasion alone in the treatment of striae distensae, but it is better to use the combination of both for more and rapid efficacy.73
The plasma fractional radiofrequency and transepidermal delivery of platelet-rich plasma using ultrasound has also been found to be useful in the treatment of striae distensae.74
Since thermal damage from intradermal RF has characteristics similar to those of many wounds, combination treatment with intradermal RF and autologous PRP would eventuate in enhanced localized collagen neogenesis and redistribution. In one of the studies, three sessions of intradermal RF were used combined with autologous PRP administered once every four weeks.75 All of the participants showed satisfactory changes and no patient was reported to show no improvement.
Transepidermal retinoic acid:
Transepidermal retinoic acid delivery using ablative fractional radiofrequency associated with acoustic pressure ultrasound has also been used for the treatment of stretch marks.76
Conclusion
Striae distensae are an extremely common, therapeutically challenging form of dermal scarring. Adequate scientific knowledge and the evidence behind both preventative and therapeutic agents are vital in order to understand striae and to offer patients the best therapeutic options. The treatment of this cosmetically distressing condition has been disappointing and there is no widely accepted surgical procedure for improving the appearance of stretch marks. Laser therapy has been advocated as a treatment for striae distensae.
The state of pregnancy results in a multitude of cutaneous changes in the female. These are a reflection of the profound alterations in the endocrine, metabolic and immunological profiles that occur during this period.1 Skin manifestations occur due to the production of a number of proteins and steroid hormones by the fetoplacental unit and also by the maternal pituitary, thyroid and adrenals.2 The placenta, a new endocrine organ in the woman, produces progesterone. Dehydroepiandrosterone is produced by the fetal adrenals from pregnenolone and this is aromatized to estriol. At term, the level of progesterone is 7 times, estradiol is 130 times and prolactin level is 19 times of that present at 8 weeks of gestation.3 There occurs an overall preference for the Th2 cytokine profile, which helps in fetal protection from the immune system.4 This is due to the high levels of progesterone, which promotes Th2 cytokines like IL-4, IL-5 and IL-10 and has inhibitory effects on TNF alpha production. Oestrogen suppresses IL-2 production. The postpartum period is marked by withdrawal of hormones and consequent elevation of Th1 cytokine levels.4
Cutaneous changes develop in more than 90% of all pregnant females.5 These include common cutaneous changes that occur in most cases to severe diseases, some of which are seen exclusively in the pregnant and postpartum state. Cutaneous manifestations can be grouped into three broad categories: physiological cutaneous changes related to pregnancy; diseases modified by pregnancy and specific dermatoses of pregnancy.6
PHYSIOLOGICAL CHANGES IN PREGNANCY
These changes are so common that they are not considered abnormal. Rather, they provide contributory evidence of a pregnant state. This however, does not mean they are cosmetically acceptable to all patients. The various physiological changes during pregnancy have been summarized in Table 1.
Table 1: Physiological changes in pregnancy
Pigmentation Generalized hyperpigmentation Pigmentation of inner thigh, genitalia, axilla Secondary areola Linea nigra Chloasma Prominence/ appearance of pigmentary demarcation lines Enlargement and darkening of freckles, naevi and scars
Vascular changes Oedema of distal extremities and hands Spider angiomas Palmar erythema Leg varicosities Rectal haemorrhoids Cutis marmorata Capillary haemangioma
Glandular changes Miliaria Dyshidrotic eczema Montgomery’s tubercles Aggravation of acne
Oral mucosal changes Oedema and hyperaemia of gingivae Pregnancy epulis
Hair changes Hirsuitism Hypertrichosis Delayed anagen release after delivery
Nail changes Brittle nail plate Onycholysis Beau’s lines after delivery
Pigmentation:
Hyperpigmentation is one of the most common and early signs of pregnancy, seen in more than 90% of patients.7 High levels of Melanocyte Stimulating Hormone (MSH), oestrogen and progesterone are believed to be responsible for hyperpigmentation. Progesterone augments the oestrogen mediated melanin output, the levels of which correlate with pigmentary changes.8
Generalized hyperpigmentation is seen which is more marked in the dark haired skin.6 Pigmented areas of the body, namely the genitalia, perineum, areolae and upper medial thighs, demonstrate more pronounced pigmentation. Linea nigra, a hyperpigmented line extending from the pubic symphysis to umbilicus and further up to the xiphisternum, replaces the linea alba.9 Chloasma, also termed as mask of pregnancy, is the well marginated brownish pigmentation of the face like melasma. It is seen in 45-75% of pregnant women in western literature but in less than 10% cases in women with pigmented skin.5,10,11 Pigmentary demarcation lines appear on the limbs with borders of abrupt transition; freckles, naevi and scars tend to darken and enlarge.12
The pigmentation gradually fades after delivery, though the resolution of skin colour is usually incomplete. Chloasma tends to persist in 30% cases postpartum.13 Sun protection and reassurance is all that is needed. Topical formulations containing hydroquinone and tretinoin are avoided in pregnancy and can be added after delivery.
Physiological connective tissue changes:
Gross distension of abdomen with adrenocortical activities are responsible for the red-blue depressed streaks seen on abdomen and breasts in 70-90% pregnancies, called striae distensae.5,14 These usually develop in the second trimester. Females with pre-existing striae on breasts and thighs are more likely to develop striae gravidarum15, seen in White women more than Asian and African-American.14 Preventive therapies are controversial and postpartum treatment options include topical tretinoin, excimer laser or surgery.10
Soft tissue fibromas of pregnancy are called molluscum fibrosum gravidarum. They appear in the second trimester on the neck, face and beneath the breasts. These disappear after delivery.16
Physiological vascular changes:
Vascular growth factors released during pregnancy by the pituitary, adrenals and placenta are believed to be causative and this has been demonstrated in vitro as well.17 Non-pitting oedema of the face, hands and feet is present in around half of all females in the later part of pregnancy.13 This is probably due to sodium and fluid retention and pressure of the gravid uterus on the inferior vena cava. Spider naevi or spider angiomas are small raised lesions with a central pulsatile punctum and radiating telangiectatic vessels frequently present over the area drained by the superior vena cava. They are present in 67% of White women and 11% Black women during the second trimester.5 Palmar erythema is seen in two-thirds of White and one-third of Black women.8 Other vascular changes include varicosities of legs and anus (40%)13, cutis marmorata (0.7%)18 and capillary haemangioma (5%)9. These changes revert after the postpartum period.
Physiological glandular changes:
Eccrine gland activity is usually increased but the palms show decreased sweating. Thus, the incidence of miliaria and dishidrotic eczema is increased. There is inconclusive evidence to suggest that apocrine gland activity is decreased during pregnancy.19 Sebaceous activity increases in the third trimester leading to acne and enlargement of Montgomery’s tubercles.14 One-third to half of all pregnant women develop these tubercles, which are modified sebaceous glands.5,8 However, sebum excretion has not been found to decrease in lactating females post-delivery.20
Oral mucosal changes:
Oedema and hyperaemia of the gingivae in pregnancy is attributable to local irritation and nutritional deficiencies and is seen in around 80% women.5 Gingivitis not related to poor oral hygiene may occur. Granuloma gravidarum or pregnancy epulis might occur that regresses postpartum.
Hair changes:
Hair changes are seen in 3-12% of pregnant females.21 Hirsuitism and hypertrichosis occurs due to oestrogen. This leads to an increase in the percentage of hair in anagen.2 Approximately 2-3 months after delivery, loss of telogen hair occurs.22 This is termed as late anagen release as the hair follicles are no longer stimulated to stay in anagen phase by the maternal hormones. The hair recovery occurs in 3-12 months. A small number of females may experience episodic shedding of hair for long periods. This has been proposed to be due to the inability of some hair follicles to revert to asynchronous shedding.23 Rarely, male pattern baldness may occur in women.2
Nail changes:
Nail growth increases during pregnancy.6 Brittleness of the nail plate and distal onycholysis may be seen.19 Beau’s lines may develop after delivery.12 Reassurance is all that is needed for these benign nail problems.
DISEASES MODIFIED BY PREGNANCY
Many pre-existing dermatoses may be exacerbated or ameliorated by pregnancy. Certain tumours may also show remission or exacerbation. This is due to the shift in pregnancy to the Th2 state and a return to Th1 state in the postpartum period and also the discontinuation of some drugs due to their teratogenic potential.
Infections:
Depressed cell-mediated immunity makes the pregnant woman susceptible to more severe and frequent infections.24
Candidiasis is quite common and was found to be the commonest cause of white discharge per vagina, being present in 22% pregnant females.5 Half of all neonates born to infected mothers are positive for Candida and some may show signs of infection.25 Pityrosporum folliculitis, caused by Pityrosporum ovale, is more common in pregnancy.25
Genital warts are the commonest sexually transmitted disease seen in 4.7% subjects, these increase in size during pregnancy.9,25 Prophylactic caesarian section to prevent laryngeal papillomas in the neonate is not recommended now.26 Herpes simplex virus infection carries 50% risk of transmission to neonate in the primary episode and 5% risk in recurrent episode, caesarean section might be warranted to prevent such transmission.26 Varicella zoster virus infection has been reported to cause pneumonia in 14% of mothers and death in 3%.27 Bowenoid papulosis, caused by human papilloma virus appears first during pregnancy or may get aggravated.6
Pregnancy prepones the clinical manifestations in HIV infected females, possibly due to additive immune suppression. Pneumocystis pneumonia or listeriosis may prove to be fatal.27 Kaposi’s sarcoma may occur in these females.27 20-30% women present with leprosy for the first time in pregnancy and the postpartum period.28 The disease tends to downgrade towards the lepromatous pole in pregnancy and upgrades during lactation.29 Type 1 lepra reactions are more frequent in the first trimester and after delivery, whereas type 2 lepra reactions peak in third trimester.29 Trichomoniasis is diagnosed in 60% of pregnant women.25
Autoimmune diseases:
Systemic Lupus Erythematosus (SLE) is associated with a better prognosis than previously thought, if the disease is in remission and nephropathy and cardiomyopathy are not present.10 If the disease is active, half of the patients’ disease will get worse and there might be fatalities.14 SLE tends to be more severe if it first presents in pregnancy.14 Babies of such mothers are likely to develop neonatal lupus.
Patients with scleroderma are usually unaffected and some are improved in pregnancy. However, occasional reports of renal crisis, hypertension and pre-eclampsia are reported.30 Course of dermatomyositis is usually unaltered but the disease may worsen in some patients.31
Pemphigus tends to be exacerbated or present for the first time in pregnancy.32 The clinical presentation in pregnancy is similar to that of the regular presentation. Differentiation from herpes gestationis is important.
Metabolic diseases:
Effect of pregnancy on porphyria cutanea tarda is not clear, though some females show biochemical and clinical deterioration.33 Acrodermatitis enteropathica shows clinical worsening.34
Connective tissue diseases:
Pregnancy can lead to bleeding, uterine lacerations and wound dehiscence in patients of Ehlers-Danlos syndrome. Pseudoxanthoma elasticum patients may suffer massive gastrointestinal bleeds.35 Lichen sclerosis et atrophicus of the vulva usually improves in pregnancy and a normal delivery is mostly possible.
Disorders of glands:
Acne can aggravate during pregnancy. Hidradenitis suppurativa and Fox-Fordyce disease become better as a result of decreased apocrine gland activity.27
Keratinization diseases:
The course of psoriasis remains unaltered in 40% females during pregnancy while it improves in a similar percentage of females and worsens in the remaining.36 It is more likely to deteriorate in the postpartum period.37 Psoriatic arthritis has been found to worsen or present for the first time in pregnancy.2
Generalized pustular psoriasis of Von Zambusch may rarely occur. Though most patients have a preceding or family history of psoriasis, some may develop the disease without ever having a preceding episode.38 Peak incidence is seen in the last trimester and the disease tends to recur.38 Multiple, discrete, sterile pustules at the margins of erythematous macules on the umbilicus, medial thigh, axillae, inframammary folds, gluteal creases and sides of neck are seen. These break to form erosions and crusts. Painful, circinate mucosal erosions may form. Prednisolone is used for management.12 Von Zambusch pustular psoriasis of pregnancy was earlier termed ‘Impetigo Herpetiformis’ but the term is best avoided as it is impossible to differentiate it from the former, both clinically and histologically.6 Erythrokeratoderma variabilis is reported to worsen during pregnancy.27
Tumours:
A melanoma that develops during pregnancy carries worse prognosis but if pregnancy occurs after the tumour is resected, the prognosis is unaltered.39 Metastasis in the fetus has been seen and a minimum period of two years following tumour resection is recommended.32 A female with neurofibromatosis may develop neurofibroma for the first time in pregnancy or older neurofibromas may grow in size. Rupture of major vessels may occur.6 Pregnancy may worsen mycosis fungoides and eosinophilic granuloma.6
Miscellaneous diseases:
Prognosis of atopic dermatitis is unpredictable in pregnancy, with reports of both improvement and worsening.27 Predisposed patients may first develop atopic dermatitis during pregnancy.40 Allergic contact dermatitis may improve in pregnancy.12 Hand eczema may worsen in the puerperal period.6 Erythema multiforme may be precipitated by pregnancy.6 Autoimmune progesterone dermatitis has been described in pregnancy.12 This disease is characterized by hypersensitivity to progesterone demonstrated by a positive intradermal skin test and cutaneous lesions resembling urticaria, eczema, erythema multiforme and dermatitis herpetiformis.41 The disease is associated with fetal mortality and recurs in subsequent pregnancies.12
PREGNANCY SPECIFIC DERMATOSES
These are a heterogeneous group of inflammatory skin diseases specific for pregnancy.42 Most of these conditions are benign and resolve spontaneously in the postpartum period but a few of these are associated with fetal complications.42 Almost all of them present with pruritus and a cutaneous eruption of varying severity.5
Classification:
The first attempt to classify these conditions was made by Holmes and Black in 1982-83 who classified them into: a) Pemphigoid Gestationis (PG) or Herpes Gestationis(HG), b) Polymorphic Eruption of Pregnancy (PEP) or Pruritic Urticarial Papules and Plaques of Pregnancy (PUPPP), c) Prurigo of Pregnancy (PP) and d) Pruritic Folliculitis of Pregnancy (PF).43,44 Shornick was of the view that all patients with PF also had papular dermatitis, so he included PF in the PP group. He included Intrahepatic Cholestasis of Pregnancy (ICP) in his classification for dermatoses where secondary skin lesions due to scratching are produced. He proposed that failure to consider ICP in the classification has led to confusion in terminology of pregnancy specific diseases. Thus, his classification included PG, PEP, PP and ICP.45 Ambros-Rudolph et al carried out a retrospective review of 505 pregnant patients over a 10 year period and gave a more rationalised classification system in 2006. They clubbed PP, PF and eczema of pregnancy in one group called Atopic Eruption of Pregnancy (AEP) due to their overlapping features and found this group to be the most common pruritic condition in pregnancy. Thus, they proposed four conditions: a) AEP, b) PEP, c) PG and d) ICP.46 The various specific pregnancy dermatoses have been elaborated in Table 2.
Table 2: Comparison of different pregnancy specific dermatoses in relation to clinical characteristics, prognosis, investigations and treatment.
AEP
PEP
PG
ICP
Pruritus
+
+
+
+
Primary cutaneous involvement
+
+
+
-
Skin lesions
Eczematous or papular
Papules, vesicles and urticarial lesions
Vesiculo bullous lesion on urticarial base
Excoriations, papules secondary to scratching
Site of lesions
Trunk, extensors of limbs, rest of the body also involved
Abdominal involvement, in striae distensae, periumbilical sparing
Abdominal, particularly periumbilical involvement
Palms and soles followed by rest of the body
Time
First trimester
Third trimester, Post partum
Second and third trimester, post partum
Second and third trimester
Risk with primigravidae
-
+
-
-
Association with multiparity
-
+
-
+
Flare at delivery
-
-
+
-
Recurrence
+
-
+
+
Family history
+
+
-
+
Histopathology
Non-specific
Non-specific
Specific, sub epidermal vesicle
Non-specific
Immunofluorescence
-
-
Linear deposition of C3
-
Other lab findings
Ig E elevated
-
Indirect IMF +
Increased serum bile acids
Maternal risk
-
-
Progression to pemphigoid, thyroid dysfunction
Gallstones, Jaundice
Fetal risk
-
-
Prematurity, Small for age baby, neonatal blistering
Premature births, fetal distress, stillbirth
Treatment
Steroids, antihistaminics
Steroids, antihistaminics
Oral steroids, antihistaminics
Ursodeoxycholic acid
Atopic eruption of Pregnancy (AEP): (Syn: Besnier’s prurigo, prurigo gestationis, Nurse’s early onset prurigo of pregnancy)
It is the most common pregnancy specific dermatoses that includes eczematous or papular lesions in females with personal or family history of atopy and elevated IgE - accounting for nearly half of all patients.46 The disease tends to recur in subsequent pregnancies with 75% of all cases occurring before the start of the third trimester.47 It carries no risk for the mother or baby however, infant may develop atopy later in life.48 Treatment is symptomatic with antihistamines and corticosteroids.
E-type AEP: This group comprises of 67% of AEP patients and includes patients with eczematous features; previously referred to as Eczema of Pregnancy (EP). It was not until 1999 that a high prevalence of atopic eczema was noted in pregnancy.49 80% of pregnant women develop the first episode of atopic dermatitis during pregnancy.46 This is attributed to the Th2 cytokine profile in pregnancy and a dominant humoral immunity.4 It is more common in primigravida, in single gestation, begins in early pregnancy and affects whole body including face, palms and soles.46
P-type AEP: This group includes what was referred to previously as Prurigo of Pregnancy and Pruritic Folliculitis of Pregnancy. Prurigo of Pregnancy (PP) is seen in one out of 300 to 450 pregnancies and occurs predominantly in the second to third trimester.50 Excoriated or crusted papules are seen over the extensors of extremities and abdomen and are associated with some eczematization. The eruption lasts up to 3 months after delivery and recurrences in subsequent pregnancies are common.51 PP is associated with ICP with the differentiating feature being the absence of a primary lesion in the latter.50 Personal and family history of atopic dermatitis or raised IgE may be seen in PP.52 Serology is normal. There are no specific changes on histopathology and immunofluorescence results are found to be negative.50 There appears to be no maternal or fetal risk.45
Pruritic Folliculitis of Pregnancy (PF), first described by Zoberman and Farmer, is now believed to be as common as PG or PP, though only a few cases have been reported.50 It begins in the latter two trimesters and affects roughly one in 3000 pregnancies.51 Pruritus is not a defining feature, despite what the name suggests.2 Multiple, follicular papules and pustules occur on the shoulders, arms, chest, upper back and abdomen and are acneiform in nature.42 The lesions tend to resolve in a couple of months following delivery. Histopathological examination reveals non-specific features with sterile folliculitis and immunofluorescence studies are negative.50 No maternal or fetal risk is described except for low birth weight neonates in a single study.52 Pathogenesis of PF is unknown with no definite role of androgens or immunologic abnormalities.53 There is no evidence to suggest that it is a hormonally aggravated acne as proposed by some workers.54
Polymorphic Eruption of Pregnancy (PEP): (Syn: Pruritic Urticarial Papules and Plaques of Pregnancy or PUPPP, Bourne’s Toxaemic Rash of Pregnancy, Toxic Erythema of Pregnancy, Nurse’s Late Prurigo of Pregnancy)
With a prevalence of a case in every 130-300 pregnancies, this disease is the second most common pregnancy specific dermatoses and was seen in 21.6% pregnancies reviewed by Ambros-Rudolph et al.46 They found it began in late pregnancy in 83% cases and 15% in the postpartum period.46 The disease occurs predominantly in primigravida and a familial predisposition is present.55 Lesions are pleomorphic, usually urticarial but purpuric, vesicular, polycyclic and targetoid lesions may be present. The striae on the abdomen are the first to be involved and there is a characteristic periumbilical sparing.56 The lesions seldom occur on the body above the breast and on hands and feet.12 The lesions resolve with scaling and crusting in six weeks. The disease is more common in excessive weight gain during pregnancy and in multiple gestation.57,58 Histopathology is non-specific and shows spongiosis, occasional subepidermal split and eosinophilic infiltration. Serology and immunofluorescence is negative.50 Treatment is symptomatic, oral steroids are needed in severe cases. There are no associated maternal or fetal complictions,59 although infants may later develop atopic dermatitis.2
The pathogenesis is unknown however, the abdominal distension leading to collagen and elastic fibre damage in striae is hypothesized, leading to formation of antigens and triggering inflammatory cascade.60 The role of progesterone has been suggested by the increased progesterone receptor immunoreactivity in skin lesions of PEP.61 The discovery of fetal DNA in skin lesions of women with PEP has furthered the hypothesis that abdominal distension leads to increased permeability of vessels and permit chimeric cell migration in the maternal skin.62 Linear IgM dermatosis of pregnancy is an entity characterized by pruritic, red, follicular papules and pustules on the abdomen and proximal extremities seen after 36 weeks gestation and a linear band of IgM deposition on basement membrane zone. It has been characterized as a variant of PEP or PP by different authors.12
Pemphigoid Gestationis (PG): (Syn: Herpes Gestationis or HG, Gestational Pemphogoid, Dermatitis Herpetiformis of Pregnancy)
PG is the most clearly characterized pregnancy dermatosis and the one which also affects the fetal skin.63 It is a rare, self-limiting, autoimmune bullous disease with an incidence of 1:1700 to 1:50000 pregnancies.63 Mean onset occurs at 21 weeks gestation, though it occurs in the postpartum period in a fifth of all cases.64 Constitutional symptoms, burning and itching herald the onset of the disease. Half of patients develop urticarial lesions on the abdomen, particularly in the periumbilical region, that change rapidly to a generalized bullous eruption usually sparing the face, palms, soles and mucosae. Vesicles may arise in herpetiform or circinate distribution. Face is involved in 10% cases and oral mucosa in 20%.12 The disease shows spontaneous improvement in late gestation but flares may occur at the time of delivery in 75% of the cases.63 Though the disease may remit after a few weeks after delivery, a protracted course, conversion to bullous pemphigoid or recurrence with menstrual cycle and use of oral contraceptive pills has been reported.50 PG tends to recur in subsequent pregnancies in a more severe form and at an early stage with longer stay in postpartum.50 Skipped pregnancies have been described.63,65 The disease is also linked with hydatiform mole and choriocarcinoma.66
The classical histopathological finding is the presence of a subepidermal vesicle, spongiosis and an infiltrate consisting of lymphocytes, histiocytes and eosinophils.64 An inverted tear drop appearance due to oedema in the dermal papilla is seen in early urticarial lesions.15 Direct immunofluorescence reveals a linear deposition of C3 along the dermo-epidermal junction in 100% cases and is diagnostic of the disease, while a salt split skin shows an epidermal staining.67 Antithyroid antibodies may be present but thyroid dysfunction is not common.63 Systemic corticosteroids are the mainstay of management. About one in ten children born to women with PG develop blisters due to passive transfer of antibodies, this resolves on its own. Severity of the disease has been correlated with the risk of prematurity and small for gestational age babies.68
Pathogenesis of PG involves the production of IgG1 antibodies against NC16A domain of carboxyl terminus of Bullous Pemphigoid Antigen 2 (BPAg2), leading to activation of complement, recruitment of eosinophils to the local site and damage of the basement membrane and consequent blistering.2 The aberrant expression of MHC class II antigens of paternal haplotype is believed to stimulate an allogenic response to placental basement membrane and this is believed to cross react with the skin in PG.63,69
Intrahepatic Cholestasis of pregnancy (ICP): (Syn: Obstetric Cholestasis, Pruritus Gravidarum, Icterus Gravidarum, Recurrent Jaundice of Pregnancy, Idiopathic Jaundice of Pregnancy)
Pruritus in pregnancy is fairly common and can be due to various reasons like pregnancy specific dermatoses and other co-existing dermatoses such as scabies, urticaria, atopic dermatitis, drug reactions etc. It was found to be present in more than half of 170 pregnant women in an Indian study.70 This must be differentiated from ICP where the skin lesions arise secondary to itching.
ICP was first described by Kehr in 1907.63 ICP being referred to Pruritus Gravidarum (for pruritus without skin changes occurring early in pregnancy and related to atopic diathesis and no cholestasis) and Prurigo Gravidarum (for pruritus associated with PP like skin lesions and associated with cholestasis) lead to much confusion regarding nomenclature.63 The disease has an incidence of 10-150 cases per 10,000 pregnancies71, being more common in South America and Scandinavia, probably due to dietary factors.50 Patients complain of sudden onset pruritus beginning from the palms and soles and later generalizing to the whole body. Skin lesions are secondary to itching and range from excoriations to prurigo nodularis, extensors are more severely involved. Jaundice is seen in 20% cases only.72 Clay coloured stools, dark urine and haemorrhage secondary to vitamin K malabsorption can occur. Family history can be elicited in half of the cases and an association with multiple gestation is described.73 Resolution of ICP occurs soon after delivery. Recurrence in subsequent pregnancies is seen in 45-70% cases and routinely with the use of oral contraceptive pills, though no detectable abnormalities are seen in the duration between two pregnancies.63 Histopathology is non-specific and immunofluorescence is negative. Diagnosis is made by increased serum bile acid levels, transaminases are elevated. Prothrombin time may be prolonged. A 2.7 times increased risk of gallstones is reported in primigravida with ICP compared to non-pregnant women.74 ICP is associated with significant fetal morbidity including premature births in 20-60% cases, intrapartum fetal distress including meconium aspiration in 20-30% and fetal mortality in 1-2%.71 Risk is particularly more if serum bile acid levels exceed 40 micromoles per litre.75 Meconium may cause umbilical vein compression and induction of labour at 36 weeks gestation has been recommended in severe cases.50 The goal of treatment is reduction of serum bile acids. Ursodeoxycholic acid, given in the dose of 15mg/kg orally daily is the only proven therapeutic agent that decreases fetal mortality.63,76 Cholestyramine reduces vitamin K absorption and increases the risk of haemorrhage. Other agents like S-adenosylmethionine, dexamethasone, silymarin, phenobarbitone, epomediol and activated charcoal are not that effective and do not affect fetal risk.63 Topical emollients and antipruritic agents offer symptomatic relief but antihistamines are not that effective.50
The key event in the pathogenesis of ICP is elevation of bile acids. Oestrogens are said to have cholestatic properties by reducing hepatocyte bile acid uptake and also by inhibiting basolateral transport proteins.50 Progesterone may additionally saturate the transport capacity of these transport proteins in hepatocyte.71 Genetic predisposition occurs due to mutation in genes encoding bile transport proteins, with cholestasis developing in pregnancy as their capacity to secrete substance is exceeded.63 Bile acids passing through the placenta produce vasoconstriction of placental veins, fetal cardiomyocyte dysfunction and also abnormal uterine contractility, all leading to fetal hypoxia.71
CONCLUSION
Pregnancy is associated with a wide variety of cutaneous changes. These may range from common, benign changes termed physiological or more severe, posing significant risk to the mother as well as the baby. Physiological pregnancy changes may be of cosmetic concern to the patient and seldom need anything more than counselling. Pre-existing dermatoses may aggravate during this period, posing a challenge to the treating physician. Women suffering from such diseases need to be warned of complications and risks before trying to conceive. A strict watch for possible complications and appropriate management at an early stage is warranted. Women should also be looked for pregnancy specific dermatoses and their complaints should not be lightly overlooked as non-specific or physiological. Careful history and examination with a judicious use of investigations will help to arrive at a diagnosis and in prompt institution of treatment.
Dermatomyositis (DM) is a rare autoimmune process with not yet fully understood aetiology. It is characterised by a combination of striated muscle inflammation and cutaneous changes. The pathogenesis of the cutaneous manifestations of DM is not well understood either. DM occurs in all age groups. Therefore, two clinical subgroups of DM are described: adult and juvenile. The adult form is predominant among female patients with a clinical presentation which includes a Heliotrope rash (Fig. 1), Gottron’s papules (Fig. 2), nail fold telangiectasia and other various cutaneous manifestations in association with inflammatory myopathy.1 In addition to the previous mentioned symptoms, juvenile patients also commonly suffer from ulcerative skin and recurrent abdominal pain due to vasculitis. An increased occurrence of oncological processes in combination with adult DM has been observed with a slight predominance for the female gender.2 These patients carry a higher risk for comorbid cancers. The most common ones include malignant processes of the ovary, lung, pancreas, stomach, urinary bladder and haematopoietic system.3 The significance of these observations is that the development of DM should raise suspicion with regard to a possible parallel oncological process.
Figure 1
Figure 2
Materials and Methods
A retrospective consecutive case series was performed on a group of 12 patients that were hospitalised at the Department of Dermatology, Venereology and Allergology at the Medical University of Gdansk between 1996 and 2013. The diagnostic criteria for DM included: hallmark cutaneous lesions of DM, clinically significant muscle weakness evaluated by electromyography (EMG), indicative laboratory findings - muscle enzymes, muscle biopsy, autoantibodies. All 12 cases had muscle biopsy, serum studies and EMG performed. The retrospective study analysed the age and sex of the patients, course of the disease, accompanying diseases, clinical picture and treatment. The patients with malignancies were analysed by the primary organs of origin, and the period between the diagnosis of DM and that of malignancy (Table 1).
Table 1. Patient characteristics
No.
Sex
Previous medical history
Age of onset of DM
Clinical picture
Diagnostics
Treatment
Malignancy and age at diagnosis
1
F
Chronic eosinophilic leukaemia
54
Muscle weakness of shoulder and hip area, facial oedema and erythema, palmar erythema
CK 2550, ANA Hep-2 1:640, LDH 901, AST 69, ALT 143, X-ray = N, USG = N, EMG = N
Azathioprine, Prednisone
Stage IIA ovarian cancer at 55
2
F
Peptic ulcer disease
66
Facial erythema, Gottron’s papules on the hands, muscular weakness creating difficulty in movement, weight loss, decreased appetite
ANA Hep-2 1:1280, CT = N, EMG = N
Glucocortico- steroids
Small cell carcinoma at 66
3
F
None
23
Muscular weakness of shoulder and hip area; difficulty in standing up and walking up stairs, Gottron’s papules, Heliotrope rash, upper chest erythema
ANA Hep-2 1: 2580, CPK 12022; AST 595, ALT 210, CK-MB 534; Jo 1 = N, Mi = N
Azathioprine, Prednisone Methotrexate
None
4
F
Chronic obstructive pulmonary disease
42
Muscular weakness of shoulder and hip area, facial oedema and erythema
Cyclo- phosphamide, Methyl- prednisolone
Stomach tumour at 43
5
F
None
22
Muscle weakness, painful extremities, facial oedema and erythema
ANA Hep-2 = N, CT = N
Cyclo- phosphamide, Prednisone
None
6
F
None
42
Muscle weakness, paraesthesia of hands, facial oedema and erythema
ANA Hep-2 1:640
Cyclo- phosphamide, Prednisone
None
7
F
Hypertension, diabetes type II, osteopenia, leiomyoma.
65
Muscle weakness of shoulder and hip area, facial oedema and erythema
ANA Hep-2 1:1280, LDH 650
Cyclo- phosphamide, Prednisone
None
8
F
Hyper-thyroiditis
46
Muscle weakness; difficulty in moving, facial oedema and erythema
ANA Hep-2 1:160
Cyclosporine A, Prednisone
None
9
F
Autoimmune hepatic disease, leiomyoma.
45
Muscular weakness of shoulder and hip area, facial oedema and erythema
ANA Hep-2 1:2560, CK 3700, Mi-2 = P
Azathioprine, Methyl-prednisolone
None
10
F
Hypertension, diabetes type 2, hypo-thyroidism, ovarian cysts
57
Muscle weakness of shoulder and hip area, facial oedema and erythema, upper chest erythema, Gottron’s papules, Gottron’s papules, fatigue, dysphagia
ANA Hep-2 1: 640, CK 747, LDH 363, AST 78, Ro52 = P, Mi 2 = N, Jo 1 = N, PM/Scl = N, CT= two pulmonary lesions that were biopsied and diagnosed as pneumoconiosis
Prednisone, Methotrexate
Cervical Carcinoma at 51, Breast Cancer at 57, Pulmonary Metastasis at 58
No. = number (patient), DM = dermatomyositis, F = female, M = male, CK = creatine phosphokinase, ANA = antinuclear antibodies, LDH = lactate dehydrogenase, AST = aspartate transaminase, ALT = alanine transaminase, N = negative, P = positive, USG = ultrasonography, EMG = electromyography, CT = computerised tomography
Limitations
The small sample size is a significant limitation in this retrospective analysis. DM is a rare disease with a prevalence of 1:1000. Increasing sample size, by combining cases from multiple institutions, and implementing control would further strengthen the presented material.
Results
The average age of onset of the disease was 48 years. All 12 subjects were female. Previous medical history included chronic eosinophilic leukaemia, diabetes mellitus type II, hypertension, leiomyomas, hypo- and hyper- thyroid disease, chronic obstructive pulmonary disease, peptic ulcer disease, autoimmune hepatitis and osteopenia. The two most common are diabetes mellitus type II and hypertension. The clinical picture of each case was similar in that all of the patients presented with some form of muscle weakness. In addition, typical features of DM with Gottron’s papules, periorbital oedema, facial oedema and erythema were noted in five patients. Antinuclear Antibodies (ANA) Hep-2 of values >1:160 were identified in nine patients. Additional laboratory markers such as creatine kinase (CK), lactate dehydrogenase (LDH), aspartate transaminase (AST) and alanine transaminase (ALT) were elevated in five patients. Two patients had muscle biopsies performed. The immunohistopathology picture consisted of Immunglobulin G (IgG), fibrinogen, C1q, and C3 deposition around the perimysium and granular deposits of Immunoglobulin M (IgM) in the dermal epidermal junction. Of the 12 patients, four had neoplasms in addition to the diagnosed DM. The primary cancers were originating from the cervix, breast, stomach and ovary. Of these four patients, all had the diagnosis of DM prior to the diagnosis of a malignancy.
Discussion
The diagnosis of DM is made by combining the clinical picture with the results of various laboratory findings: skin and muscle biopsies, EMG, serum enzymes and ANAs.
The clinical picture varies. The typical dermatological presentation consists of a erythematous and oedematous periorbital rash - the Heliotrope rash (Fig. 1). Symmetrical redness and flaking can be observed on the elbows and dorsal sides of the phalanges, especially over the distal metacarpal joints - Gottron’s papules (Fig. 2). Erythematous lesions can also be found on other locations such as the face, upper chest and knees.4 The dermatitis heals with atrophy, leaving behind areas that resemble radiation-damaged skin. The striated muscle inflammation most often involves the shoulder and hip area, leading to muscle weakness and atrophy. The intercostal muscles and the diaphragm may be involved causing alarm with regards to respiratory compromise. Dysphagia can be present due to inflammation of the smooth and skeletal muscles of the oesophagus. These inflammatory processes often lead to muscle calcification.5 The sum of all these changes clinically is seen most often as weakness, weight loss and subfebrile temperatures. All patients in our study had co-existing muscle and cutaneous symptoms, with variation in severity and localisation. Five patients had the classical picture of shoulder and hip area weakness. The rest of the patients had a more general muscle weakness. Two patients had atypical complaints of hand paraesthesia and extremity pain respectively.
Subtypes of DM exist for the purpose of epidemiological research and sometimes prognosis. They are categorised by the clinical presentation and presence or absence of specific laboratory findings. These subtypes are as follows: Classic DM, Amyopathic DM, Hypo-amyopathic DM and Clinically Amyopathic DM. These subtypes have little impact on routine diagnosis. Common laboratory findings in DM are enzymatic elevation of CK, AST, ALT and LDH; these mainly reflect the muscle involvement. Amyopathic DM lacks both abnormal muscle enzymes and weakness.6 Enzymatic elevation may sometimes precede the clinical symptoms of muscle involvement. Hence, an enzymatic raise in a patient with a history of DM, should raise suspicion of recurrence. Positive ANA findings are frequent in DM but not necessary for diagnosis. More myositis-specific antibodies include anti-Mi 2 and anti-Jo 1. A typical histopathological examination shows: myofiber necrosis, perifascicular atrophy, patchy endomysial infiltrate of lymphocytes and occasionally the capillaries may contain membrane attack complexes.7
Cutaneous changes and muscular complaints can correspond to: 1. Systemic scleroderma which often has a positive ANA; 2. Trichinosis, in which periorbital swelling and myositis occurs, but there is a prominent eosinophilia and a history of consuming undercooked swine or bear meat; 3. Psoriasis with joint involvement which may give a clinically similar picture to DM. However, the skin changes in psoriasis have a more flaking pattern. In doubtful cases, a skin and muscle biopsy together with an electromyography will set the diagnoses apart. A facial rash may also be observed in systemic lupus erythematosus together with nail fold telangiectasia. They are usually distinguished by a clinical picture with more organ system involvement in systemic lupus and by serological studies. A drug-induced picture of DM exists and is particularly associated with statins and hydroxyurea.8
It is estimated that around 25% of DM cases are associated with a neoplastic process that can occur prior, during or after the episode of DM. The risk of developing a malignancy is highest in the first year of DM and remains elevated for years after diagnosis. 9, 10, 11 This was the case with patient number 1, 2 and 4 in our study, where the malignant process appeared in the first year following onset of DM. Risk factors seen in DM patients include male gender, advanced age and symptoms of dysphagia.12 The age range of the four patients in our study with malignancy was between 43 and 66. Symptoms that clinically raised suspicion of a malignant process included weight loss, lack of appetite and dysphagia. All neoplasms were discovered within one year after the diagnosis of DM was made. One patient had a previous history of cervical cancer, six years prior to the onset of DM.
The most common neoplasms seen in patients with DM vary in the world. In Europe the malignancies are located mainly in the ovaries, lungs, and stomach. The cancer types associated with the DM correlate with common cancers seen in the same area. For instance, in Asia, nasopharyngeal carcinoma (which is a rare malignancy in Europe) is a frequent occurrence in DM.1, 3 The location of neoplasms seen in our study varied from gastric, breast, ovary and pulmonary. The screening in regards to malignancies in patients with DM is individualised and should be based on risk factors such as previous malignancies, alarming symptoms such as weight loss or dysphagia, or abnormal findings on physical exam. This was the case with patient number 10 in our study who had a previous history of cancer, and patient number 2 who had symptoms of weight loss and decreased appetite. Initial screening was negative for patient number 1 and 2, where the malignancy developed first after the onset of DM. Age-appropriate screening with mammography, faecal-occult blood test and Papanicolaou smear should be considered. Additional investigations with chest films, computerised tomography (CT) scanning of chest, abdomen or pelvis; colonoscopy, cancer antigens; and gynaecological ultrasonography should be done when indicated.
The main objective of treatment in DM is to improve muscle strength and obtain remission, or at least clinical stabilisation. No specific protocol exists with regard to treatment of DM. Treatment is individualised and adapted to the specific condition of the patient. High-dose corticosteroids are the basis of treatment. However, randomised placebo clinical trials failed to show their efficacy. Clinical efficacy of corticosteroid therapy demonstrates itself and hence is the initial treatment of choice. Doses start at around 1 mg/kg/day depending on the corticosteroid of preference. This dosing is maintained for approximately two months until clinical regression is achieved, followed by approximately 10 mg decrease in dose for the coming three months. A maintenance dose of approximately 5-10 mg should be achieved. The exact parameters are patient-specific. In the case of a severe flare of dermatomyositis, 1 g per day for three days of methylprednisolone intravenous pulses can be administered. The systemic effects of long term therapy with corticosteroids have to be kept in mind. Hence, yearly dual-energy X-ray absorptiometry bone scans can be administered to monitor the development of osteopenia.
Further treatment options are offered in situations where the initial disease presentation is severe, involves internal organs, if relapse occurs during steroid dose reduction, and steroid side-effects. It has been proposed that combination therapy is a better method of approach due to lower reported relapse rates and lower need to use high-dose corticosteroids. Methotrexate is second-line therapy when steroids fail alone. Methotrexate is used with a maximum dose of 25 mg per week plus folate supplementation. The limitations of Methotrexate are immunosuppression and pulmonary fibrosis. Methotrexate is considered preferable to Azathioprine because the latter has a longer onset of efficacy. Azathioprine is administered at doses ranging from 1.5 - 3 mg/kg/day and has a side-effect profile is similar to that of other immunosuppressants. Cyclosporin A is a T-cell cytokine moderator that has a similar efficacy profile to Methotrexate. Side-effects include renal impairment, gingival hyperplasia, and hypertrichosis. Dosing of Cyclosporin A ranges from 2 - 3 mg/kg/day.
An expensive but effective and rather low side-effect alternative is intravenous immunoglobulins. The dosage of this medication has not been officially established in the treatment of DM, but options are: 2 g/kg given either in 1 g/kg/day for two days every four weeks; or 0.4 mg/kg/day for five days initially, and then for three days monthly for three to six months. Other alternatives include Mycophenolate Mofetil, Cyclophosphamide, Chlorambucil, Fludarabine, Eculizumab, Rituximab.9 Further options might be treatment targeted toward malignancy when associated with DM. This was observed in our patient number 10, where full remission of DM was obtained first after lobectomy and chemotherapy for the mammary carcinoma.
Conclusion
DM mainly affects women and all 12 cases presented in our study were female. One third of our cases had malignancies associated with their course of DM. We conclude that it is reasonable to screen these patients, especially in those with already established cancer risk factor. Age-appropriate screening and beyond is indicated by high risk factors or clinical presentation. High suspicion should be raised in patients with a previous history of oncological treatment since DM can be the first clinical sign of cancer recurrence.
A 41-year-old woman with a 6-year history of mild psoriasis presented with a rash under her breasts. The differential diagnosis included flexural psoriasis, an allergy to the nickel in her under wired bra, and intertriginous dermatitis (moisture-associated skin damage). She was prescribed Trimovate cream (GlaxoSmith Kline) and developed a florid weeping eczema within 48 hours of application (Figure 1). The eczema settled with the withdrawal of Trimovate and application of Betnovate RD cream (GlaxoSmith Kline). The history was very suggestive of a contact dermatitis to Trimovate cream.
Figure 1 showing eczema
She was referred to the Dermatology department and was patch tested to the European standard, medicament and steroid batteries. She had a number of positives including cetearyl alcohol, sodium metabisulphite, and clobetasone butyrate. These are all components of Trimovate. She was given advice sheets on all her allergens and on avoiding them she has had no recurrence of eczema.
Discussion
Contact dermatitis is a type IV allergy and usually appears within 2 to 3 days after contact with an external allergen. This case is likely to be an example of concomitant sensitisation, where one sensitivity facilitates the acquisition of another sensitivity to a chemically unrelated ingredient within a product.Whilst there has been a previous case report of concomitant sensitivity to sodium metabisulphite and clobetasone butyrate in a patient using Trimovate cream,1 this is the first report of a patient reacting to three of the ingredients found in Trimovate - sodium metabisulphite, clobetasone butyrate, and cetearyl alcohol. Allergy to clobetasone butyrate is rare, with only 5 previously reported cases.1, 2, 3 Allergy to sodium metabisulphite is not uncommon, producing a positive reaction in approximately 4% of patients who are patch tested.4, 5 Allergy to cetearyl alcohol is also rare, with one study estimating the incidence of positive reactions to be 0.8% among 3062 patients that were patch tested.6
Detection of the allergen, or allergens, is important, as avoidance results in resolution of the eczema. Our patient highlights the fact that it is insufficient to simply advise a patient to avoid the topical medicament that has caused a reaction. Ideally, patients with a topical medicament allergy should be patch tested to identify which components the patient is allergic to, so that they can be avoided in all products. In this case, in addition to Trimovate, there are a number of other products that our patient will now avoid. This is of particular significance in view of her history of psoriasis, for which she has used moisturizers and topical steroid preparations in the past, and will likely need again in the future. Clobetasone butyrate is often used in facial and flexural psoriasis. Cetearyl alcohol is a particularly important allergen to identify, as it is found in many products including a number of commonly used moisturizers such as Diprobase (MSD), Cetraben (Genus) and Epaderm (Mölnlycke) cream, and most steroid creams although not steroid ointments. Our patient was therefore advised to use only steroid ointments and has had no recurrence of the contact dermatitis. To conclude, GPs should consider sending their patients with contact dermatitis for patch testing, as the identification of all allergens is valuable to management.
Blue discolouration of the skin can have a multitude of causes, including Mongolian spots, blue naevi, the naevi of Ito and Ota and metallic discolouration1 or the use of drugs such as minocycline. Here we report the case of a 61 year old gentleman who developed blue macular skin lesions that were not attributable to any obvious cause and may be the result of an unidentified occupational exposure.
A 61 year old Caucasian gentleman developed blue macular skin lesions over a 14 year period. The very first lesion appeared in the middle phalanx of the right middle finger (figure 1). It was light blue and pinpoint, eventually darkening and increasing in size to approximately 1mm x 1mm, at which point becoming permanent and non-evolving. The lesion had no notable associated features and the patient was in otherwise good health.
Figure 1: The first blue macular lesion on the middle phalanx of the right middle finger.
Figure 2: A blue macular lesion on the terminal phalanx of the left middle finger.
Figure 3: A lesion on the anterior abdomen from which a punch biopsy was taken.
Figure 4: Haematoxylin and Eosin stained slide at 10x magnification. Abdominal skin biopsy showing dermal interstitial and perivascular distribution of black coloured pigment deposits
At present, he has approximately thirteen blue macular lesions in total, all of which have developed in the same manner. They are distributed predominantly on his hands with one on his left forearm and one on the right abdominal flank. New spots still continue to arise on his hands (figure 2).
A punch biopsy of the abdominal lesion (figure 3) was carried out. The histological findings were those of skin with normal intact epidermis and the presence of black coloured pigment granular deposits, located largely within the papillary dermis and occasional smaller deposits in the superficial reticular dermis (figure 4). The deep reticular dermis and subcutaneous fat were normal. The pigment had a perivascular distribution and in dendritic histiocytic cells, with close association to fibroblasts. Histiocytic cells form part of the mononuclear phagocyte system and these cells are abducted mainly for phagocytosis removal or storing material2. Apart from the pigment, the remaining skin was normal. The use of light microscopy alone does not identify all substances on examination of a Haematoxylin and Eosin (H&E) stained section of tissue. Applying polarisation light microscopy enables the identification of numerous structures, for example crystals, pigments, bone and amyloid3. However, the black coloured material here was non polarisable (no refractile foreign material could be identified). These appearances as seen on light microscopy alone are most frequently seen where there is a history of tattoo artistry, but tattoo pigment is typically identified as showing reflective properties using polarisation4. Interestingly, the patient had no clinical history of deliberate tattooing and other causes were considered.
Discussion
The discovery of black coloured deposits in the dermis excludes the diagnoses of Mongolian spots or blue naevi and the naevi of Ito and Ota, all of which are disorders of dermal melanocytes. Another important differential is malignant melanoma, but it is not the diagnosis as the histopathological findings did not find any evidence of dysplasia or malignancy.
In a disorder known as anthracosis, similar findings of black coloured deposits can be seen in other organs such as within the lung and draining lymph nodes. It is often found in smokers and urban populations and reflects the deposition of carbon which is the most commonly identified exogenous mineral substance within tissue sections. The skin is not a site where such carbon pigment is typically seen and therefore, this is not a credible diagnosis in this case.
Agyria is a condition that occurs as a result of silver particle impregnation of skin leading to blue-grey skin discolouration. Silver exposure may be due to occupational or surgical exposure (by use of silver sutures) or medication with silver salts. On interview, the patient denied any occupational exposure to silver and the use of silver salts. Although the patient had had previous shoulder surgery, silver sutures are no longer used in modern day surgical practice and therefore this cannot be the cause of his skin discolouration.
Unfortunately, histological examination of paraffin embedded tissue sections can only confirm the presence and distribution of an exogenous substance and it is not possible to precisely differentiate the exact type of material which is present. The use of an electron probe micro analyser may have been useful in identifying the substance, however, such equipment is not currently available and was not used in this case.
Interestingly, in tattoo artistry, carbon black may be used to give blue tattoos their colour5 and this is also a component of tyres and industrial rubber products6. This provided us with a link to occupational exposure, given that this gentleman is a tyre worker and has been involved in both the manufacture and assembly of tyres for 34 years. Carbon can cause discoloration of the skin, depending on the extent of deposition.
It is notable that in his 34 years of working with tyres, this gentleman did not routinely use gloves or protective uniform until only 10 years ago. This was as workplace safety precautions were not as strongly enforced in previous times. He admitted to have been in direct contact with the materials involved in tyre building and also suffered accidental superficial cuts on his hands whilst working, which may be a route by which carbon may have been introduced into the dermis. This is supported by the observation that the majority of the blue macular lesions were on the hands. Adding credibility to this theory is the identification of a colleague of this gentleman’s (who did not wish to be identified), whose job also involved the manufacture and assembly of tyres, who also has a similar single blue macular lesion on his hand.
In addition to this we have identified a forum on the internet7 that reports other similar cases of blue pin-point macular lesions appearing on the skin of tyre factory workers – some of whom worked for the same tyre company that this gentleman did. This may suggest that there is an association between exposure to a chemical, possibly carbon black, involved in the manufacture of tyres, and the appearance of these blue macular lesions.
In this case report, the identity of the material deposited and the route by which it accumulated in the dermis is unclear, but may have been related to an occupational exposure – this was in keeping with the general consensus upon presentation of this case at the West Midlands Dermatology Conference at New Cross Hospital Wolverhampton. We welcome any new case reports or literature that may be able to shed further light on this subject.
Maintaining its longstanding presence as one of the oldest forms of art, body tattooing has increased exponentially within mainstream society, as well as in social acceptance. Generally worn to display individuality and creativity, these distinctive forms of indelible markings are present in every culture, whether on tribal men, or people of status. Procedurally when inserting the decorative markings, the approach in studio tattooing has not changed significantly as artists are still using “an electrically powered, vertically vibrating instrument to inject tattoo pigment 50 to 3,000 times per minute up to or into the dermis at a depth of 1/64th to 1/16th of an inch”1
While no national registry provides prevalence, a 2012 Harris Poll cited one in five United States (U.S.) adults have at least one tattoo (21%), an increase of 16% and 14% from previous surveys taken in 2003 and 2008 respectively.2 Tattoo numbers were even higher in some variables including age between 30-39 years (38%), Hispanics (30%), females (23%), and those living in the Western part of the U.S. (26%). No questions were identified in the 2012 poll that queried tattooed body site locations. Other studies cite almost a 25% presence of tattoos.1,3-7 The amount of tattoo studios also echoes the growing body art phenomenon.
Given the societal blaze of tattooing, the medical literature on body art has also increased. Yet, most of the information still remains focused on small case reports6 about traditional locations (arms, legs, chest, back), their decision-making, various risk-taking behaviors,8 and the small amount of complications.7 Those with various adverse skin reactions or major complications seem to have had tattoos with colored pigment.6
While body art can be found virtually everywhere on the human anatomy, several articles have surfaced concerning genital body piecing.4-5, 9-11 Current studies validate the increasing rate of all types of tattooed 4,8 people, from a variety of occupations and social classes, with markings on visible and non-visible locations.7 This article reports on the limited medical literature found about men with genital tattoos (pubic and/or the glans penis). Also presented is a subsample data analysis of 14 men from a primary study examining male genital piercings,11-12 who responded affirmatively to one survey question about penile tattoos. This synopsis and subsample data analysis are provided for clinicians to have further, recent evidence about men with genital tattoos for decision making during patient encounters in health care settings. The terminology of penile and genital tattoos will be used interchangeably in this article.
METHODS
Literature Synopsis
Historically, the cross-cultural literature is rich in visual genital tattoo descriptions. In South America, the Moche on the North Coast of Peru (A.D. 150-800) produced ceramics illustrating vivid sexual imagery and highly decorated male genitals.13 Phallus decorations with dots, concentric lines, and other tattoo markings on the penile skin and mucosa during the Upper Paleolithic era in Europe 12,700 to 11,000 years ago have been reported.14-15 Likewise, the Samoan Island culture, where the word ”tattoo” is believed to have originated from “tatau,”, has maintained ritualistic16 traditions for over two thousand years; they are initiated at the time of puberty for future leadership roles. These 10+ days of ceremonies include very painful, repeated tattooing of the scrotum (tafumiti) and the penis (tafito). Other nearby primitive Polynesian tribes have believed this tattooing as highly erotic,16 whereas the indigenous Maori (New Zealand) trust that the pigment for these tattoos can trap cosmic energy.14 Circumcision and tattooing were thought to produce the same effect of magic protection and healing powers after scar healing.14 In the Japanese culture, an examination of Yakuza (racketeers or gangsters) also describes the genitalia as a site that is tattooed,17 fulfilling their principles of tattoos always being covered.
Searching for information about genital tattoos was more challenging within the medical literature. A comprehensive longitudinal 40 year search of the national and international electronic medical literature (1973-2013) published in English and their associated reference lists was conducted with MEDLINE, EMBASE, CINAHL, SCOPUS, and OVID. Only 20 articles were located that mentioned genital tattoos. Articles were from international authors (n = 11) and the U.S. (n = 9); they all produced interesting reading. One reference cited women with genital tattoos.7
Genital tattoos in the early literature were labeled as criminal, or personality disorders tattoos;18 one recent article discussed them under the header of genital self-mutilation.16 Others described them as a valuable clue for forensic pathology identification.19-20 World War II articles cited descriptive stories of soldiers with penile tattoos,21-22 with one reporting up to 10 sailors being seen.23 Besides reporting on how the fate of Bulgaria was determined by three tattooed men (Churchill with an anchor on his left arm, Roosevelt with a family coat of arms tattoo, and Stalin with a death’s head on his chest),24 Kazandjieva25 then provides vivid examples of auto-aggression markings that his countrymen self-inflicted after the Communist takeover. This included glans penis tattoos which are described as producing great pain.15,25 One political candidate, while campaigning, is reported as suggesting punitive action for those HIV+ by “putting indelible, glow-in-the-dark tattoos on [their] genitals.”26 Traumatic tattoos associated with gunpowder explosions and blast burns are also mentioned on the glans penis.27
Two studies also described inmates with genital tattoos and discussed how these markings demonstrated aggressive behavior within this type of environment. Here large, colorful tattoo designs and wording on the glans penis tattoos were described28-29 which seemed to satisfy the inmate’s flaunt of personal pain endurance. Additionally, Cuban refugees (Marielitos) fleeing to the U.S. were reported as having genital tattoos; they also were from prison subcultures and their markings had various sexual overtones.29
Four other reports described those with penile tattoos also routinely inserting foreign bodies12,30 and paraffinoma12,31,32 into the penis. In Pehlianov’s study (also in Bulgaria) they included a control group of another 25 men with genital tattoos. Recently, a unique case of non-ischemic priapism for 3 months was reported33 following prolonged bleeding from a manual penile tattoo procedure in Iran. The authors suggested the hand-held tattoo needle had penetrated too deeply producing an arteriovenous fistula and the subsequent persistent half-rigid priapism. The authors also noted that the 21 year old patient expressed no regret, depression, or other complications related to the genital tattoo.
Original Study
The initial study queried males with genital piercings using available internet survey software,12 as it was considered a hidden variable. Anonymity and access to people nationally and internationally were major advantages for using this nontraditional approach. The university institutional review board deemed the study status as Exempt. To obtain quantitative and qualitative data about those men with genital piercings, an 83 item web-based survey was used; overall results, and another subsample of this data, are published elsewhere.11-12
Subsample of those with Penile Tattoos
From the original 445 male genital pierced individuals that responded to the question regarding having tattoos on their penis, 14 replied affirmatively. This subsample had previously been determined not be an outlier of the larger group of genital pierced men.12 While a short general description (age span at the time of tattoo procurement, urethral “play,” design types, motives, and tattooists) about the 14 member genital tattoo subsample was published in 2010,12 further investigation leading to quantitative and qualitative (Figure 1) data is presented here.
Figure 1: Subsample Respondent Qualitative Quotes *Black tribal flames on the top of the shaft, done at [age] 38 * For erotic reasons, self done with no complications, done at [age] 54 *I got it because I wanted it. After it was finished I realized I needed it, done at [age] 30 * I self tattoo’d my penis on the glans and around the corona ridge in order to make up for its’ lack of size and to enhance its appearance. I used a sailmaker’s needle and Indian ink and there were no complications, done at [age] 43. *one small cross pigment tattoo! *I’m a little more than average in size, but I still have issues with my genitals. The way they look and their size. Piercings and tattoos have helped me quite a lot. *I sketched a rose one day, like[d] the design, decided to get it tattooed on my penis. The stem is green with some yellow highlights, the bud is red, all black outline. The tattoo was applied with a standard machine . . .healing was actually quicker and easier than any of my other tattoos. *It’s a little heart just next to ‘captain hemingway’ which I hand poked and used india ink for it when I was 17. . . thought our penis deserved a reminder of our affection . . .no complications experienced but since it was hand done with a [sterile] needle it’s kind of blurry
This subsample had significantly more foreskin genital piercings (chi-square = 11.5) = 1; P = .001), whereas the most common genital piercing of the larger group of those without genital tattoos11 had Prince Albert piercings (inserted through external urethra). No question inquired which came first, the genital piercing or genital tattoos.
Data Analysis
For this subsample analysis, (and original study11-12), IBM SPSS 21was used to obtain frequencies and chi-square analysis. Cross tabulations for the subsample were obtained by comparing those with and without penile tattoos.
RESULTS
Demographics
Almost all of the subsample respondents with penile tattoos were reportedly Caucasian (92%) and their ages ranged from 18 to 67 years (average 42.3). Of those that replied, six lived in the U.S. and five cited various international locations. Over half had vocational or college education (64%) and significantly more were likely to be single (25%) or divorced (25%), (chi-square 12.6) = 5; P = .027). Data regarding religious faith was weak to non-existent (75%). Respondents self-reported a good state of health (92%) (chi-square = 8.7) = 3; P = .034), yet 50% cited no annual health check-ups.
Risk Behaviors
Within this subsample, there was no consensus about being a “risk taker”. Recreational drugs were reportedly not used (91%), over half were non-smokers (55%), but monthly alcohol use with binge drinking (5+ or more drinks) was cited (78%). Their “motives for genital tattoos were for esthetics, sexual, and personal pleasure”12; a variety of penile tattoo designs were described (Figure 1), created either “by studio artists (n = 11) or self-inflicted (n = 3)”.12 All of them described having other body art, such as piercings and other general body tattoos. Some reported an average of 4 piercings (81%) and a significant amount of general body tattoos (average 3.5) (chi-square = 11.1) = 5; P = .049), that still interest them (85%) (chi-square = 8.9) = 3) P = .031).
Sexual Activity
This subsample’s average age of first intercourse was 17 years, with most citing women as their sexual partners (92%), most preferred penile/vaginal intercourse (79%), and only one respondent reported a sexually transmitted infection (gonorrhea). When asked about any forced sexual activity (rape), this subsample had a significant amount of those who answered affirmatively (23%) (chi-square = 7.7) = 1; P = .005). Virtually no sexual, physical, or mental abuse was reported.
Need for Uniqueness
A four-item scale called the Self-Attributed Need for Uniqueness (SANU)34 was present in the survey to determine the respondent’s self-view (Cronbach alpha = .86). Using a Likert scale, the subsample’s moderate, strong and very strong perspectives were collectively summarized. These respondents with penile tattoos preferred to be different (79%), distinctive (86%), intended to do things to make themselves different than those around them (72%), and reported a Need For Uniqueness (93%) (Cronbach alpha = .77). To validate this finding, when all 5 responses of SANU were totaled,12 the mean was 12.43 documenting a more positive perspective for intentionally wanting to be different, distinctive, and unique.
DISCUSSION
This article reviewed both the cross cultural and medical literature about those with genital tattoos, as well as included both a quantitative and qualitative subsample data analysis of a small group of men who specifically reported penile tattoos. Yet, with certainty this small sample size produced limitations and reporting/survey bias. Additionally, any generalizability with the findings of this subsample should be noted as the respondents could have self-selected their participation and used their personal judgment to interpret the survey questions in this non-experimental cross-sectional study using internet survey methodology.12
From this review and to our knowledge, few have studied groups of men with genital tattoos, a difficult group of subjects to find with this hidden variable.12,31 Cultural descriptions documented a long, rich history 12, 14-17, 29,31 of genital markings for esthetics, sexual enhancement, and tribal status, whereas the medical literature reflected limited observational type information, and few actual case histories or scientific studies. Although there were no mental health evaluations12 cited in this medical literature, more psychopathic, deviant behavior discussions were made about the individuals with genital tattoos.16-18,26,32,35 In contrast, two authors30,33 comment on the “normalcy” of their patients that presented with genital tattoos.
Genital tattoos may be more common than this very small subsample size suggested as great emphasis has been placed on male penile size in many cultures, for a long time.31,36 The augmentation of these genital markings and decorative designs seemed to have motivated their sexual health, self-enhancement9-10 and well-being.31 Thus, when further studies are considered for this population with a hidden variable, these findings should assist with further ideas of investigation.
Current society has a strong 25 year renaissance of procuring tattoos with at least one in five, and perhaps even four, individuals possessing a tattoo, on virtually every part of their body, without major complications. This small subsample of those who have genital tattoos validates some similarities to those who wear general body tattoos such as a single heterosexual orientation, possessing some college/vocational education, monthly binge drinking,1,3-5,10 and a strong propensity for a Need for Uniqueness.4-5,37 They were major body art wearers and continue to enjoy them, as others have also reported.4-5,10-12
Yet other demographic assumptions were challenged for this subsample of men with genital tattoos. These international respondents tended to be older Caucasians and not as ethnically diverse; there also was not a consensus as to them being risk takers, as has been repeatedly reported by many other body art respondents.1,3-5,11-12
Subsample respondents reported their average first occurance of sexual intercourse at age 17, similar to the national figures.38 Significant experiences of rape were also reported in this subsample, as in women with genital piercings.4-5,9-10 The national rate for forced sexual activity is 10.5%38 and those with genital tattoos reported over twice that amount (23%). No sexual abuse was reported in contrast to a recent German study39 examining general body tattooing.
As with any type of invasive procedure, there can be complications with certain types of body art. When these complications occur, body art wearers typically first seek the internet and/or their studio artist for health advice before presenting to clinicians.1,8,10-12 Yet, overall for the amount of general tattooing done, this type of body art produced limited documented complications and more potential concerns.7-8,11, 30,33 More complications were reported when the tattoos contained colored pigments.6
These tattoos are an integral part of their cultural and personal expression.12,31,33 From our experience many of these male patients with genital tattoos are not seen primarily because of their decorative markings,31 but during clinical evaluations for other issues presented with the normal range of urologic issues involving overall genitourinary and sexual function. Genital tattoos can be an ambivalent findings for many clinicians, but these indelible skin markings (tattoos) are only skin deep,40 and provide valuable cues such as a history of sexual trauma.39 Currently more genital tattoos are seen among our freedom-impaired patients, where the prevalence of general body tattoos among the inmates can be as high as 67%.41
Anecdotally, when healthcare staff discover a patient with genital body art, this discovery can be met with judgmental attitudes and behaviors which could impact care. To adequately assess, evaluate and treat the individuals that have chosen to have genital tattooing, clinicians should strive to provide a thoughtful, nonjudgmental patient-centered approach, along with a generous application of health education, for their present, or even future body art.11
The US Food and Drug Administration (USFDA) considers the following as biologics: any therapeutic serum, toxin, antitoxin, vaccine, virus, blood, blood component or derivative, allergenic product, analogous product, or derivatives applicable to the prevention, treatment, or cure of injuries or disease of man1. However, generally, biologics refer to protein molecules therapeutically used in various diseases so as to target specific points in the inflammatory cascade of these disorders 2. Hope for an improved tolerability, convenience in usage and lasting remissions, combined with increased knowledge of immune-pathogenesis of various cutaneous diseases has lead to the introduction of biologics as alternative immune-modulating agents in the field of dermatology.
CLASSIFICATION
Biologics are generally divided into three major groups 3:
a) Monoclonal antibodies
b) Fusion antibody proteins
c) Recombinant human cytokines and growth factors
The main groups and the principal agents in each group are summarised in Box 1 and described below.
A) MONOCLONAL ANTIBODIES
Monoclonal antibodies target specific cell-surface receptors. In the early days of biologic therapy, purely murine monoclonal antibodies were used. However, due to the development of antimurine antibodies, which blocked their action, these could be given only for very short periods. The monoclonal antibodies used now have different amounts of murine sequences in the variable region. They may be categorised into three classes:
(a) chimeric antibodies comprising of 30% murine genes fused with human antibodies
(b) humanised antibodies, which have 10% murine sequences, and
(c) human antibodies, which are solely derived from human immunoglobulin genes 4.
Principal monoclonal antibodies with therapeutic relevance in Dermatology
The principal monoclonal antibodies known till date are enumerated in Box 1 and described briefly below.
· Anti-IL-12 and anti-IL-23 monoclonal antibody: Ustekinumab
· Anti-CD2 antibody: Siplizumab
· Anti-CD4 antibody: Orthoclone (OKTcdr4a)
· Anti-CD25 antibodies: Basiliximab, Daclizumab
· Anti-CD80r: Galiximab (IDEC 114)
· Anti-IgE: Omalizumab
Fusion antibody proteins
· Etanercept
· Alefacept
· Abatacept
· Onercept
· Denileukin Diftitox
Recombinant human cytokines and growth factors
a) Interferons
· Interferon α (IFNα)
· Interferon γ (IFNγ)
· Interleukin 1 Receptor antagonist (IL1Ra)
· Interleukin 2 (IL-2)
· Interleukin 4 (rhIL-4)
· Interleukin 10 (rhIL-10)
· Interleukin 11 (rhIL-11)
b) Granulocyte macrophage colony stimulating factor (GM-CSF)
c) Platelet derived growth factor (PDGF)
1. Infliximab
Infliximab (trade name Remicade) is a human-mouse monoclonal antibody that binds to and inhibits the activity of TNF-α, and also causes lysis of TNF-α producing cells5.
Important uses of Infliximab
Psoriasis: Infliximab is approved for the treatment of psoriatic arthritis and plaque psoriasis by FDA6, 7. Infliximab may also be of value in recalcitrant or unstable disease and in generalised pustular psoriasis. It is given as an IV (intravenous) infusion in doses of 5 or 10 mg/kg, over a period of 2 hours at weeks 0, 2, 6 and may be followed by repeat single infusions at 8-12 week intervals 8. In various controlled trials, improvement at 10 weeks has been noted in 87% of patients 7, 9.
Atopic dermatitis: Infliximab has also been evaluated in a study of atopic dermatitis 10. At 2 weeks, there was significant improvement in all patients. At 10, 14, and 30 weeks, variable response was seen.
Hidradenitis suppurativa: Long-term efficacy has also been evaluated in hidradenitis suppurativa. In one study, some patients had no evidence of recurrence after 2 years, while others relapsed within a mean of 8.5 months11.
2. Adalimumab
Adalimumab (Humira®) is a human IgG1 monoclonal antibody directed against TNF-α. Adalimumab is given in a dose of 40 mg subcutaneously (SC) every other week as self-injection 5, 12.
Important uses of Adalimumab
Psoriasis: Adalimumab rapidly reverses the decrease in epidermal Langerhans cell density in psoriatic plaques 13. In a trial, patients with psoriatic arthritis received adalimumab every other week for 24 week14. It was well-tolerated and helped improve joint and skin manifestations significantly.
Hidradenitis suppurativa: An increasing number of reports in refractory hidradenitis supprativa have shown successful control with adalimumab 15, 16, 17.
3. Basiliximab
Successful treatment for severe psoriasis and generalised pustular psoriasis has been reported with basiliximab, an interleukin-2 receptor (IL-2R; CD25) chimeric monoclonal antibody 18, 19.
4. Daclizumab
Daclizumab is a humanised monoclonal antibody thatbinds to the CD25 subunit of the IL-2 receptor onT-cells, thus blocking T-cell proliferation. It has been tried in recalcitrant psoriasis and HIV-associated psoriatic erythroderma with a mean reduction in PASI of 30% 20, 2122.
5. Siplizumab
Siplizumab (Medi-507) is a humanisedmonoclonal antibody directed against CD2. It is designed to block stimulationby inhibiting the CD2–LFA-3 interaction. In earlyphase studies in psoriasis, significant response to therapy has been noted23.
6. Efalizumab
Efalizumab is a recombinant humanised monoclonal IgG1 antibody that binds to CD11a, a subunit of leukocyte function-associated antigen 1 (LFA-1) 24. It destabilises and decreases the trafficking of T-cells into dermal and epidermal tissues.
Important uses of Efalizumab
Psoriasis: Efalizumab was approved by the US FDA in October 2003 for the treatment of psoriasis5. It is currently the only biologic agent approved for continuous administration to adult patients24. The licensed dose of efalizumab is 1 mg/kg weekly as a subcutaneous self- administered injection for 12 weeks, following a first conditioning dose of 0.7 mg/kg 24.
Lichen planus: There is one case report of 3 months duration of treatment with efalizumab for lichen planus with resolution of skin lesions and pruritis 25.
7. Rituximab
Rituximab is a monoclonal humanised antibody directed again in the B cell-specific antigen CD20.
Important uses of Rituximab
Lymphoma: It has been used in patients with CD20-positive non-Hodgkin's lymphoma in a dosage of 375 mg/m2 for four infusions26.
SLE: In systemic lupus, dose escalation studies revealed no differences with respect to clinical outcome in patients who received either a single infusion of 100 mg/m2, a single infusion of 375 mg/m2, or four weekly infusions of 375 mg/m227.
Blistering diseases: For patients with blistering diseases, most patients receive the lymphoma dosage schedule. However, serious side effects were considerably higher.
There are reports of refractory pemphigus patients who received infusions of rituximab and had rapid resolution of lesions and a long lasting clinical remission 28, 29, 30.
8. Galiximab
Galiximab a humanised monoclonal antibody directedagainst CD80 and blocks its interaction with CD28 on the T cell, for T-cell stimulation 31. Clinicaldata for this drug are just beginning to emerge with 40% of patients achieving at least 50% reduction in PASI after receiving4 biweekly doses in a trial32, 33.
9. Ustekinumab
It is a fully human monoclonal antibody targeting IL-12 and IL-23, presently undergoing clinical trials for psoriasis and psoriatic arthropathy2, 34. In placebo-controlled studies, (PHOENIX 1) and (PHOENIX 2) have shown that ustekinumab could control plaque psoriasis with only four injections a year resulting in greater ease of use and more sustained relief 35, 36.
10. Certolizumab pegol
Certolizumab is the recombinant antibody Fab' fragment of a humanised TNF inhibitor monoclonal antibody. A study in chronic plaque psoriasis showed that certolizumab pegol, given subcutaneously every two weeks, over a period of 12 weeks shows significant improvement 37.
11. Golimumab
Golimumab, a fully human monoclonal antibody is at present undergoing Phase III clinical trials in psoriatic arthropathy 38.
12. Orthoclone or OkT4a
It is a humanised antihuman CD4 IgG4 monoclonal antibody preventing the recognition of the MHC-bound antigen by an appropriate T-cell receptor, hence T cells do not get activated 39. Several studies have found orthoclone to be effective in moderate to severe psoriasis 40, 41.
13. ABX-IL8
ABX-IL8 is a fully human monoclonalantibody designed to bind free IL-8, a key chemokine in psoriasis and deactivate it in theskin42, 43. In early trials, the drug has demonstrated good clinical responsein psoriasis 44, 45.
14. Omalizumab
Omalizumab is a recombinant, humanised, monoclonal antibody against immunoglobulin IgE. This agent acts as a neutralising antibody by binding IgE at the same site on IgE as its high-affinity receptor, FcεR I, thus inhibiting the biological effects before the generation of allergic symptoms 46. There are reports of the efficacy of omalizumab in chronic urticaria 47, cold urticaria 48 and atopic dermatitis 49.
15. Mepolizumab
Mepolizumab is a humanised monoclonal IgG antibody to the IL-5 molecule, which is essential for eosinophil growth and differentiation. Two weekly infusions showed significant clinical improvement in atopic dermatitisand clinical trials are underway for hyper-eosinophillic disorders 50,51.
16. SMART Anti–IFN-γ
SMART anti–IFN- γ,a humanised monoclonal antibody, binds and inactivates IFN- γ, an important Th1 cytokinein psoriasis. Early phase studies are being performed at this time 52.
B) FUSION ANTIBODY PROTEINS
Fusion proteins, also known as chimeric proteins, are proteins which are created by the fusion of the receptor domain of a human protein with the constant region of human IgG. The resultant fusion protein binds specifically to a ligand or co-receptor 53. The most commonly used fusion proteins in dermatology are briefly described below and enumerated in Box 1.
1. Alefacept
Alefacept is a bivalent recombinant fusion protein composed of the first extracellular domain lymphocyte function antigen 3 (LFA-3), fused to the hinge domain of human IgG1. The LFA-3 portion of alefacept binds to CD2 receptors on T-cells, thereby blocking their natural interaction with LFA-3 on antigen presenting cells (APCs). The IgG1 portion of alefacept binds to FcγR receptor on natural killer cells to induce T-cell apoptosis 54.
Important uses of Alefacept
Psoriasis: The US FDA approved alefacept in January 2003 for treatment in adult patients with moderate to severe chronic plaque psoriasis. It is given by intramuscular or intravenous route with a dose of 10-15 mg IM weekly or 7.5 mg IV weekly and a 12 week course is recommended 5, 54. Two 12-week courses showed a75% or greater reduction in the PASI 55.
Alopecia areata: Case reports have shown that alefacept may be effective in the treatmentof AA56, 57.
Pyoderma gangrenosum: Alefacept has been used for pyoderma gangrenosum and improvement was shown in 25% of these patients 58.
Other Indications
Some of the off-label conditions where alefacept has been used with success are graft-versus-host disease (GVHD), lichen planus, alopecia areata, atopic dermatitis, mycosis fungoides,alopecia universalis, erosive lichen planus,Hailey-Hailey diseaseand hand dermatitis 58, 59, 60, 61, 62, 63.
2. Denileukin diftitox
Denileukin diftitox is a novel recombinant fusion protein consisting of fragments of diphtheria toxin linked to human interleukin-2 and works by targeting the high-affinity interleukin-2 receptors. It was tried in patients with recalcitrant psoriasis and the rate of improvement for treated patients was found to be significant 64.
3. Abatacept (Ctla4ig)
It is a fusion protein composed of the extracellular domain of CTLA4 and the Fc region of IgG4. It interferes with T-cell activation by competitively binding the B7.1 and B7.2 molecules on the surface of APC 65. In a study, patients with stable psoriasis vulgaris showed good improvement with IV infusion of abatacept 33. A second generation CTLA4Ig, Belatacept, is currently under Phase II clinical trial for allograft diseases 66.
4. Etanercept
Etanercept is a recombinant fully human dimeric fusion protein comprising of the human TNF-α p75 receptor and the Fc portion of human IgG1 molecule. It functions as a TNF inhibitor, thereby preventing interaction with its cell surface receptors on target cells and blocking its pro-inflammatory effects.
Important uses of Etanercept
Psoriasis: Etanercept (Enbrel®) is FDA approved for use as subcutaneous monotherapy in psoriasis. Several clinical trials have shown that it is effective67, 68, 69, 70. The adult dose is 50 mg/week, given subcutaneously for three months 5. The drug is also indicated for treatment of psoriatic arthritis 71, 72.
Hidradenitis supprivata:There is a study of etanercept in patients with severe hidradenitis with more than 50% score improvement12.
5. Onercept
Onercept is a recombinant human soluble p55 tumour necrosis factor binding protein under development for the potential treatment of psoriasis and psoriatic arthritis73. C) RECOMBINANT HUMAN CYTOKINES AND GROWTH FACTORS
Cytokines are non-immunoglobulin proteins and glycoproteins produced by a wide variety of cells in the human body and released in response to any immune stimulus 74, 75. Recombinant cytokines or cytokine antagonists have been used as immunomodulators 76. The principal recombinant cytokines used in dermatology, enumerated in Box 1, are described below.
1. Interferons (IFNs)
IFNs, a family of related proteins, are produced by virus-infected leucocytes. They exhibit anti-proliferative, immune-modulatory and anti-neoplastic functions 77.
· Interferon α
Recombinant IFNα is given as a subcutaneous or intramuscular injection to treat verruca vulgaris 78 , condyloma acuminatum 79, cutaneous T cell lymphoma 80, Kaposi's sarcoma (AIDS related) 81, melanoma 82, basal cell carcinoma 83, squamous cell carcinoma 84, actinic keratosis 85, Behçet's disease 86, hemangiomas 87 and keloids 88.
The injections are usually given thrice weekly and the dose (depending on the condition being treated) varies from low-dose therapy for condyloma acuminatum to high-dose therapy for melanoma 89, 90. Of late, pegylated IFNα is being used for convenience, because it has a longer half-life and hence can be given once weekly 80.
· Interferon-γ
It is FDA approved for the treatment of chronic granulomatous disease 91 and has also been used in atopic dermatitis 92 and cutaneous T cell lymphoma 90.
Anakinra is the non-glycosylated form of human IL-1Ra and acts by blocking the functions of the naturally occurring IL-193. Good results have also been reported in Schnitzler's syndrome94, familial cold auto-inflammatory syndrome 95 and psoriatic arthropathy96. It is given by subcutaneous injection 100 mg once a day.
3. Interleukin 2
Recombinant IL-2 is an antitumour cytokine that has been used in cutaneous T cell lymphoma (CTCL) and metastatic melanoma 97. When given intravenously in high doses of 600,000-720,000 IU/kg in melanoma, IL-2 has produced a 15-20% overall response, with complete cure in 4-6% 98.
4. Interleukin 4 (rhIL-4)
In a dose-escalation study (0.5 to 5mg/kg given by subcutaneous injection thrice a week), IL-4 has been shown to cause improvement in psoriasis by inducing Th2 differentiation in human CD4 + T cells 99.
5. Interleukin 11 (rhIL-11, Oprelvekin)
It has also shown reasonably good results in the treatment of psoriasis at doses of 2.5 or 5mg/ kg, by subcutaneous injection 100.
GM-CSF acts by stimulating stem cells to produce granulocytes, monocytes and macrophages 101. Recombinant human GM-CSF has been used to promote wound healing in ulcerated skin for example leg ulcers 102, 103, and for the treatment of melanoma 104 and Sezary syndrome 105.
7. Platelet derived growth factor (PDGF)
PDGF is a dimeric glycoprotein which regulates and promotes granulation tissue formation, re-epithelialisation and wound angiogenesis 106. Recombinant PDGF-BB topical gel (100ìg/g), applied once daily, has been approved by FDA for the treatment of diabetic foot ulcers 107, 108.
8. Recombinant Human IL-10
Recombinant Human IL-10 (Tenovil)can be given in subcutaneousinjections. Early phase clinical trials have shown thatrecombinant human IL-10 three times a week improved psoriasis 109, 110.
SIDE EFFECTS OF BIOLOGICS 5, 111, 112, 113
Some of the adverse effects of biologics are described below:
Allergic reaction and antibody formation: Mostly seen with TNF-α blockers.
Mild transient injection site reactions: Comprising of erythema, oedema and bruising, noted with etanercept in 10-20% of cases in the first month of therapy. Antibodies to etanercept may develop in 6% of patients.
Infusion reaction: Occurs during or within 1-2 hours of treatment and may affect up to 20% of all the patients treated with infliximab, rarely anaphylactic shock may occur.
Acute flu-like symptoms: Headache, chills, fever, nausea and myalgia may occur within 48 hours after administration of the first two doses of efalizumab and Interferon α.
Infections: Reactivation of tuberculosis may occur on treatment with anti-TNF-α agents and sepsis secondary to Listeria monocytogenes and Histoplasma capsulatum have been reported 113.
Malignancy: Patients previously treated with PUVA represent an at-risk group.
Demyelinating disease: Worsening of multiple sclerosis and demyelination reported with infliximab.
Thrombocytopenia: Occurs with efalizumab and warrants discontinuation of therapy.
Autoimmune haemolytic anemia: Occurs 4-6 months after the start of treatment with efalizumab.
Congestive cardiac failure: Worsening of congestive cardiac failure with TNF-α blockers is reported to occur.
Antinuclear antibodies and lupus-like syndrome: May develop during therapy with anti-TNF-α agents, but not associated with symptoms and signs of lupus in the majority.
Hepatitis: Reported following infliximab therapy, occurring from 2 weeks to more than a year after initiation of treatment. Treatment should be stopped in the event of jaundice and/ or marked elevations (>5 times the upper limit of normal) in liver enzymes.
PATIENT SCREENING FOR BIOLOGIC THERAPY 113, 114
All patients to be put on biologics should undergo a thorough evaluation including detailed clinical history, physical examination and relevant investigations with particular reference to known toxicity profile of the agent being considered. The investigations generally advised are113: full blood count, liver and renal function tests, screening for hepatitis and HIV infection, anti-nuclear antibodies, anti-ds DNA, urine analysis, chest X-ray and Tuberculin skin testing.
For efalizumab, haemogram (including platelet count) is recommended monthly for the first 3 months and then every 3 months. For TNF blockers, it is done at 3 months initially and repeated every 6 months.
Liver and renal function tests, serum electrolytes and urine analysis are done at 3 months initially and then every 6 months.
EXCLUSION CRITERIA/ CONTRAINDICATIONS
There are various contraindications for use of biologics, warranting their exclusion and precautions are to be exercised because of their immune-modulator properties. The main exclusion criteria are: active tuberculosis, severe congestive heart failure, patients having >200 treatments of PUVA (because of a risk of developing malignancies with anti- TNF agents), history of demyelinating disease or optic neuritis, hepatitis B and C positivity, HIV positivity, premalignant states, active infections and high risk states such as chronic leg ulcers, persistent or recurrent chest infections and indwelling urinary catheter infections, pregnancy and breast-feeding.
ASSESSMENT OF THE RESPONSE TO BIOLOGICS
Many scoring systems for assessing the severity of various dermatological diseases exist. These scoring systems and other indices can be used for assessment of response to the use of biologics. For example, for evaluation of improvement in psoriasis, PASI (psoriasis area and severity index) and DLQI (dermatology life quality index) are recommended at 3 months initially and then every 6 months 113. Reduction in baseline PASI score of >75% is the standard used by FDA to assess the efficacy of a new psoriasis agent 115. Similarly in atopic eczemas, improvement is monitored based on the Eczema Area and Severity Index, Pruritus Severity Assessment and DLQI. Reduction of the Eczema Area and Severity Index score by 50% is considered excellent, 30-49% moderate and <29% non-significant.
SUMMARY
To summarise, biologics represent the future of therapeutics, not only in dermatology but also in other fields of medicine. Among the various dermatological disorders where they are used, biologics have been most evaluated in psoriasis 116. However, the possibility of serious infections and the oncogenic potential combined with the high cost of the drugs limit their routine use at the present stage 117. Regular re-evaluation of efficacy and safety is essential if these agents are to be used to the maximum benefit of patients118.
Psoriasis is a common skin disorder characterized by erythematous papules and plaque formation with silver scaling. Guttate psoriasis is much less common and many studies cite a prevalence of less than 30% among patients who have psoriasis. It refers to the acute appearance of multiple skin eruptions mostly in a patient with no preexisting psoriasis and less commonly in a patient with psoriasis. We report here a case of guttate psoriasis associated with a flare of psoriatic arthritis.
Case report
A 53 year old man presented with a generalized body rash and multiple joint pains. His symptoms started a week prior to presentation. The skin rash initially appeared on his back and flanks but gradually progressed to involve the thighs and arms. He had ‘sausage fingers’, bilateral knee and ankle swelling associated with pain and sporadic metatarsophalyngeal joint pain as manifestations of his arthritis. His past medical history included hypertension, diabetes mellitus, hyperlipidemia and psoriasis with psoriatic arthritis. He did not report any recent changes in his medication. The patient denied any history of fever, sore throat, weight loss, visual problems, dyspnea, cough, gastrointestinal complaints or recent travel. Physical examination revealed a diffuse, non-blanching, pruritic, maculopapular and maculopustular rash over the trunk. He also had a scaly and diffuse erythematic rash over the lower abdomen which was non-blanching and pruritic. Auspitz’s sign was positive. He had multiple painful joints including both knees, right wrist, left proximal interphalangeal joint, and both his ankles. Left knee arthrocentesis was done which revealed joint fluid consistent with inflammatory joint disease without any evidence of crystals. Laboratory tests, including red and white blood cell count, haemoglobin, cyclic citrullinated peptide antibody, rapid plasma regain, hepatitis panel, antinuclear antibody, rheumatoid factor, lyme markers and serum uric acid revealed no abnormalities. ASO titer level was positive at 196. An x-ray of his left hand showed periarticular erosive changes along the distal aspect of the proximal phalanx. A skin biopsy was performed which revealed mild spongiosis and a perivascular lymphoplastic infiltrate. A diagnosis of guttate psoriasis was made. He was started on prednisone, methotrexate and folic acid and discharged from hospital. He was followed up in the rheumatology clinic 2 weeks after discharge and his rash had improved.
Discussion
Unlike psoriasis, guttate psoriasis is a much lesser known entity. It refers to the acute appearance of multiple skin eruptions, mostly in patients with no preexisting psoriasis and less commonly in chronic plaque psoriasis (guttate flare of chronic plaque psoriasis).
The characteristic skin lesions of guttate psoriasis are less than 1 cm in diameter, hence the name guttate (drop like). The lesions look like a shower of red, scaly tear drops that have fallen down on the body mainly involving the trunk, arms, thighs and face. Guttate psoriasis should be differentiated from diabetic dermopathy, also called shin spots, which typically begin as dull red, scaly papules or plaques and later develop into bilateral asymmetrical circumscribed shallow pigmented scars and/or brownish macular lesions with a fine scale. In diabetic dermopathy the lesions usually are greater than 4 cm in size.
Diagnosis is usually made on clinical examination; however skin biopsy is helpful in difficult cases. Histopathologic findings of guttate psoriasis vary with the age of the lesion. Findings in early lesions may be nonspecific and may include mild acanthosis, papillary dermal oedema and lymphocyte-predominant dermal infiltrate. Mature lesions exhibit parakeratosis alternating with hyperkeratosis, epidermal acanthosis, Munro microabscesses and dermal perivascular infiltrate containg neutrophils, lymphocytes and macrophages.
Streptococcal infections are well known to precipitate guttate psoriasis,1 however there have been no significant improvements in patients who were given penicillin or erythromycin when compared to those who were not treated.2 Other known precipitants are physical and psychological trauma.
The exact pathophysiologic mechanism is undetermined. The disease is believed to result from an immune reaction triggered by a previous streptococcal infection in a genetically susceptible host. Recent research points toward chromosome 6 as HLA-Cw*0602 allele positive patients are more prone to develop the guttate form.
Atopic dermatitis (AD), also known as atopic eczema is a chronic, relapsing, inflammatory skin disease that can cause significant physical, psychological and social stress for patients and their families.1 This article focuses primarily on AD in adults. It is the most frequent inflammatory skin disease in the western world and is often characterized by chronic inflammation and pruritus interrupted by acute flares and bacterial infection.2,3 The majority of the care of AD is provided in primary care, with a minority of patients being referred to secondary care. There are currently extensive cost implications to the National Health Service (NHS) for both treating patients and for lost working days.4 AD can be a therapeutic challenge, especially in primary care, and there appears to be a great potential for improving the outcome and cost effectiveness of treatment in the community setting.4
Epidemiology and pathogenesis
AD typically begins in young infants or early childhood and subsides spontaneously by adolescence in approximately 90% of patients although it can persist into adulthood in about 10% of patients.5 The incidence of AD is generally considered to be increasing worldwide.6 AD affects both sexes equally, and in the United kingdom (UK) approximately 15-20% of school-aged children and 2-10% of adults will be affected by the condition at some stage.7
AD appears to result from a complex interplay between defects in skin barrier function, environmental agents, modified immune responses of the immune system to exogenous and endogenous factors, IgE-mediated mechanisms and other factors. However, the pathogenesis leading to the precise manifestation of AD is not completely understood.3,8
Diagnosis
There are no laboratory or diagnostic tests for AD. The diagnosis is based on visual assessment and clinical history. The UK diagnostic criteria (Table1) has been shown to be the most extensively validated for AD in comparison to the Hanifin and Rajka criteria, Schulz-Larsen criteria, Diepgen criteria, and Kang and Tian diagnostic criteria. Although several different diagnostic criteria have been developed they should mainly be used for research purposes as opposed to daily clinical management.4
Skin tests and laboratory investigations (specific IgE) may be helpful in the investigation of provocative factors such as food or environmental allergens. It is important to note that laboratory investigations should be interpreted in the context of the patient’s history.9
It is often difficult to differentiate AD from other skin conditions (e.g. seborrhoeic dermatitis, contact dermatitis, psoriasis, scabies). However, a family history of atopy and the clinical distribution of the lesions are helpful in making the diagnosis. Other conditions that need to be considered in the differential diagnosis of AD are metabolic and nutritional deficiencies, malignancies and immunodeficiency syndromes that present with skin manifestations.8
Table 1 – UK Working Party Diagnostic Criteria4
The patient must report an itchy skin condition (or parental report of scratching or rubbing in a child) in the last 12 months, plus three or more of the following:
History of involvement of the skin creases (front of elbows, behind knees, fronts of ankles, around neck or around eyes)
Personal history of asthma or hay fever (or history of atopic disease in first degree relative if child aged under four years)
A history of generally dry skin in the last year
Onset under the age of two years (not used if child aged under 4 years)
Visible flexural dermatitis (including dermatitis affecting cheeks or forehead and outer aspects of limbs in children under four years)
Management
The management of AD should involve a combination that includes short-term treatment of flares and a long-term maintenance approach to prevent flares. For patients with mild to moderate AD, topical therapy may be sufficient to control the condition. Patients with more severe disease may require advanced therapy such phototherapy or systemic therapy.
Education
For optimal disease management, patients and/or their carers should be educated about the nature of AD, the need for continued adherence to prescribed treatment and about the appropriate use of topical therapies. Time spent educating patients and carers have been shown to have a positive effect on disease outcomes. Patients may also benefit from written information to reinforce learning.8
Emollients
Emollients soften the skin, aid in restoring the impaired barrier function, reduce itching, prevent moisture from leaving the skin and increase the efficacy of topical corticosteroids (TCS). They also replace the natural surface oils that are essential to preventing irritant materials, infection and allergy-inducing substances from entering the skin.4
Healthcare professionals should offer a range of emollients, and prescriptions should be reviewed frequently. To optimise adherence to emollient therapy, creams, lotions, and ointments, or a combination can be used depending on patient preference. Continued use of emollients during periods of disease quiescence can reduce the likelihood for exacerbations.10
When the treatment regimen involves both an emollient and TCS, there is no evidence on which to base the order of application. Patients should be advised to apply emollients liberally and frequently (at least 2-4 times a day). It is especially important to use emollients during or after bathing. The emollient should be applied in the general direction of growth of body hair in order to prevent accumulation at hair bases which might predispose to folliculitis. Emollients can become contaminated with bacteria and the use of pump dispensers minimises this risk. If the emollient is in a pot it should be removed with a clean spoon or spatula.4
Topical corticosteroid therapy (TCS)
TCS is considered first-line therapy for AD flares. Available preparations include ointments, creams, gels, lotions, liquids, and foams. Ointments and creams are generally the most effective in treating AD as they tend to be more moisturising.10 The least potent preparation required to control AD, particularly in sensitive areas, should be utilised. When possible the TCS should be stopped for short periods to reduce the risk of adverse events.8
TCS is categorised into four groups according to potency: mild, moderately potent, potent and very potent. The choice of TCS potency should be tailored to the age of the patient, the body region being treated, and the severity of inflammation. Patients should be advised to apply TCS once daily. If there is an inadequate response to once daily application, the frequency should be increased to twice daily.4 Once control has been achieved, twice weekly maintenance therapy with a TCS should be considered in patients with moderate to severe AD experiencing frequent relapses. The local adverse effects of TCS usage include skin thinning, bruising, perioral dermatitis, folliculitis, pruritus, allergic contact dermatitis and the spread of fungal infection. Patients being treated with intermittent courses of TCS should be reviewed regularly (depending on TCS potency and site of application) to determine response to therapy and assess skin for potentially reversible atrophic changes.4
Table 2 - The ‘fingertip unit’ (FTU) is a method of determining the amount of TCS to apply. It is described as “the amount of ointment expressed from a tube with a 5 mm diameter nozzle, applied from the distal skin crease to the tip of the palmar aspect of the index finger.” The following table is a guide to the use of FTU in adults.4
Skin area
FTU per dose
Face and neck
2.5
Torso and abdomen
7
Back and buttocks
7
Entire arm and hand
4
A hand and fingers (front and back)
1
Entire leg and foot
8
Topical calcineurin inhibitors (TCIs)
TCIs are non-steroidal immunomodulating agents licensed for the treatment of AD.4 TCIs work by inhibiting the phosphatase activity of calcineurin to block expression of cytokines and are thought to represent a more targeted way to limit inflammation and avoid many of the adverse effects of TCS. TCIs may be used either as monotherapy, as a combination or as sequential therapy. TCS are generally less expensive and more effective than TCIs although individual clinical situations will arise in which TCIs are preferred.10
Two TCIs are available: tacrolimus (0.03% and 0.1% ointments) and 1% pimecrolimus cream. The tacrolimus 0.03% and 0.1% ointments are both licensed for moderate to severe eczema and the 0.03% ointment is licensed for use in children aged two years and over. The 1% pimecrolimus cream is licensed for mild to moderate eczema in patients aged two years and over. The use of tacrolimus should be limited to doctors with a specialist interest and experience in treating AD.4
TCIs should not be used as first line treatment unless there is a specific reason to avoid the use of TCS.4 Given the high cost of TCIs, and the fact that their long-term safety is not fully known, they are generally reserved for patients with persistent disease or frequent flares that would require continuous TCS treatment. They are also of use in patients with severe disease in sensitive skin areas (e.g. around the eyes, face, neck and genitals) where systemic absorption and the risk of skin atrophy with TCS are of concern. Considering the possibility that the normal immunological response to infection may be suppressed, TCIs should not be applied to skin which appears actively infected.4, 8
Dressings and wet wrap treatment
Patients with non-infected moderate to severe AD can be advised to cover affected areas with dry wrap dressings to provide a physical barrier to scratching and improve the retention of emollients. Wet wrapping generally consists of two layers of bandage applied over topical preparations. The bottom layer is soaked in warm water, squeezed out and then put onto the skin over the topical preparation. The top layer is dry. Wet wraps can be worn under nightwear or ordinary clothes and used during the day or night. They are available in bandage form or as garments.4 Disadvantages include a high cost, inconvenience, a need for specialised training, and an increased potential for adverse effects from occluded corticosteroids (such as systemic absorption, atrophy, striae), and increased incidence of skin infection.10 There is currently insufficient consistent evidence on which to base a recommendation for wet wrap use in the primary care setting.4
Antimicrobial measures
Skin lesions of around 90% of patients with AD are colonised compared to less than 5% of individuals with healthy skin. Staphylococci are the main organisms isolated although other organisms such as streptococci may also cause infection. The routine swabbing of skin is not indicated although swabs of potential Staphylococcus aureus carriage sites should be considered in patients with recurrent infection. Oral antibiotics are not recommended in the routine treatment of non-infected AD but patients with clinically infected AD can be prescribed short term oral antibiotic treatment based on local/regional antibiotic sensitivities. However, first- or second-generation cephalosporins or penicillins for 7 to 10 days are usually effective in managing bacterial infection. Macrolides are less useful alternatives due to resistant patterns in patients with AD. Patients with AD are also prone to recurrent viral infections. Eczema herpeticum is a severe disseminated herpes infection that is a serious risk in patients with widespread AD and may be misdiagnosed as a bacterial infection. Patients with eczema herpeticum normally require systemic antiviral treatment4, 10.
Antihistamines
Although first-generation antihistamines do not directly affect the itching associated with AD, the sedative effects have been found to help improve sleep. Therefore, short-term bedtime use of sedating antihistamines should be considered in patients with AD where there is debilitating sleep disturbance. Daytime use of first generation antihistamines should be avoided given their sedative effects. Non-sedating antihistamines appear to have limited value in patients with AD but they may provide some benefit in patients with allergic triggers.4, 8
Dietary interventions
Although there is an association between IgE mediated food allergy and AD severity in infants, it is unclear whether hypersensitivity to food is a major factor in causing and maintaining AD. Dietary exclusion is not recommended for managing AD in patients without confirmed food allergy. The exclusion of foods during pregnancy and breast feeding to prevent the development of AD in infants is not recommended. Breast feeding for three months or more may help prevent the development of infant eczema where there is a family history of atopy. However, current UK guidelines state that weaning should start at six months.4
Table 3 - Guidance on when to refer to secondary care4
Poor control of the condition or failure to respond to appropriate topical treatments
Psychological upset or sleep problems
Recurrent secondary infection
Other therapies
Systemic corticosteroids are usually reserved for the acute treatment of severe AD exacerbations. Prolonged use of oral steroids is associated with potentially serious adverse effects and their long-term use should be avoided. Furthermore, relapses are common following discontinuation of oral corticosteroid therapy.8
Ultraviolet (UV) phototherapy may also be beneficial for the treatment of AD in adults. In addition, systemic therapies are available and may be broadly classified into traditional medications (e.g. cyclosporine, azathrioprine, methotrexate) and biologic agents (targeted monoclonal antibodies). These options are available for severe, refractory AD. These therapeutic options should generally be reserved for unique situations and require consultation with a dermatologist. These therapeutic options are beyond the scope of this article.8
Alopecia areata is a non-scarring autoimmune, inflammatory hair loss affecting the scalp and/or body. Although the etiopathogenesis of alopecia areata is still unknown, the most widely accepted hypothesis is that it is a T-cell mediated autoimmune condition that occurs in genetically predisposed individuals. The term ‘alopecia areata’ was first used for this disorder by Savages1.Alopecia areata has a reported incidence of 0.1-0.2%, with a life-time risk of 1.7%2-4. The disease can begin at any age, but the peak incidence is between 20 and 50 years of age5. Both the sexes are equally affected and there is no racial variation reportedClinically, alopecia areata may present as a single well demarcated patch of hair loss, multiple patches, or extensive hair loss in the form of total loss of scalp hair (alopecia totalis) or loss of entire scalp and body hair (alopecia universalis). Histopathologically, alopecia areata is characterized by an increase in the number of catagen and telogen follicles and the presence of perifollicular lymphocytic infiltrate around the anagen phase hair follicles. The condition is thought to be self-limited in majority of cases, but in some the disease has a progressive course and needs active treatment in the form of oral or topical therapeutic options. Progressive alopecia areata is associated with severe social and emotional impact.
Clinical features
Alopecia areata mostly presents as a sudden loss of hair in well demarcated localized areas. The lesion is usually a round or oval flat patch of alopecia with normal skin colour and texture involving the scalp or any other region of the body. The patch of alopecia may be isolated or there may be numerous patches. It usually has a distinctive border where normal hair demarcates the periphery of the lesion. In acute phases, the lesions can be slightly erythematous and oedematous.
The patches of alopecia areata are usually asymptomatic, although several patients may sometimes complain of local paraesthesia, pruritus or pain. The affected hairs undergo an abrupt conversion from anagen to telogen, clinically seen as localized shedding. Characteristic hairs, known as ‘exclamation point hairs’ may be seen within or around the areas of alopecia. The hairs are tapered towards the scalp end with thickening at the distal end. These hairs may also demonstrate deposition of melanin pigment in the distal extremity, also known as Wildy’s sign. Although not absolutely pathognomonic, it strongly suggests the diagnosis of alopecia areata. Hair pull test conducted at the periphery of the lesion may be positively correlated (six or more) with disease activity. In the chronic phases, the test is negative, since the hair is not plucked as easily as in the acute phases.
Another important clinical sign that can aid in the diagnosis is the presence of ‘cadaverous hair’. These are the hairs in which there occurs a fracture of the shaft inside the hair follicle, producing blackened points inside the follicular ostia resembling comedones. In alopecia areata, the hair loss progresses in a circumferential pattern. Often, distinct patches merge to form large patches. Upon regrowth, hairs will often initially lack pigment resulting in blonde or white hairs7.
Extrafollicular involvement in alopecia areata:
a) Nail changes: Nail changes are more frequent in children (12%) than in adults (3.3%)8.The prevalence of nail changes is greater in the more severe forms of alopecia areata such as alopecia universalis and alopecia totalisFinger nails are more commonly involved than the toe nails. Pitting is the most common finding. Other nail changes include koilonychias, onycholysis, onychomadesis, punctuate leukonychia, trachyonychia, Beau’s lines and red lunulae8-11.
b) Ocular changes: Various ocular changes have been reported to occur in alopecia areata. These include focal hypopigmentation of the retina12, lens opacities, posterior subcapsular cataracts13 decrease in visual acuity, Horner’s syndrome, heterochromia of the iris14, miosis and palpebral ptosis.
Treatment of alopecia areata
Treatment of alopecia areata is not mandatory in every affected patient because the condition is benign in majority and spontaneous remission is common. Treatment is mainly directed towards halting the disease activity as there is no evidence that the treatment modalities influence the ultimate natural course of the disease. Treatment modalities are usually tailored as per the extent of hair loss and the patient’s age. Addressing the impressive inflammatory process occurring in alopecia areata, corticosteroids have by far been the most commonly used treatment modality-16Few treatments have been subjected to randomized control trials and except for contact immunotherapy, there is a paucity of published data on their long term outcomes. Currently, new treatments targeting the immune system are being explored for the use in alopecia areata.
Topical treatments
Topical steroids
Intralesional steroid injections
Topical contact sensitizers
Anthralin
Minoxidil
Topical retinoids
Tacrolimus
Systemic treatments
Systemic corticosteroids
Sulfasalazine
Azathioprine
Methotrexate
Oral zinc sulphate
Photo-and photochemotherapy
PUVA
NBUVB
Excimer laser
Miscellaneous and Non-pharmacological treatment
Dermatography, wigs
Hypnotherapy etc
Topical treatment options
Topical corticosteroids:
Several topical corticosteroids with varying levels of efficacy have been used to treat alopecia areata. These include fluocinolone acetonide cream17, fluocinolone scalp gel, betamethasone valerate lotion18, clobetasol propionate ointment19, dexamethasone in a penetration-enhancing vehicle and halcinonide cream20. They are a good option in children because of their painless application and wide safety margin21. Topical corticosteroids are ineffective in alopecia totalis/universalisFolliculitis is a common side effect of corticosteroid treatment, appearing after a few weeks of treatment. Telangiectasia and local atrophy have also been reported. Treatment must be continued for a minimum of 3 months before regrowth can be expected and maintenance therapy often is sometimes necessary.
Intralesional corticosteroids:
Intralesional corticosteroids are widely used in the treatment of alopecia areata. In fact, they are the first-line treatment in localized conditions involving <50% of the scalp22. Hydrocortisone acetate (25mg/ml) and Triamcinolone acetonide (5-10mg/ml) are commonly used. Triamcinolone acetonide is administered usually in the concentration of 5mg/ml using a 0.5 inch long 30-gauge needle in multiple 0.1 ml injections approximately 1 cm apart22-23. The solution is injected in or just beneath the dermis and a maximum of 3 ml on the scalp in one visit is recommended23. Lower concentrations of 2.5mg/ml are used for eyebrows and face. Regrowth usually is seen within 4-6 weeks in responsive patients. Treatments are repeated every 3-6 weeks. Skin atrophy at the sites of injection is a common side effect, particularly if triamcinolone is used, but this usually resolves after a few months. Repeated injections at the same site or the use of higher concentrations of triamcinolone should be avoided as this may lead to prolonged skin atrophyPain limits the practicality of this treatment method in children who are less than 10 years of age. Severe cases of alopecia areata, alopecia totalis, alopecia universalis as well as rapidly progressive alopecia areata respond poorly to this form of treatment25.
Anthralin:
Dithranol (anthralin) or other irritants have been used in the treatment of alopecia areata. The exact mechanism of action is unknown, but is believed to be through immunosuppressant and anti-inflammatory properties with the generation of free radicals. It is used at concentrations ranging from 0.5 to 1 % for 20-30 minutes after which the scalp should be washed with shampoos in order to avoid excessive irritant effects. The applications are made initially every other day and later on daily. Adverse effects include pruritus, erythema, scaling, staining of treated skin and fabrics, folliculitis, and regional lymphadenopathy26-27. In an open study, 25% patients with severe alopecia areata were shown to respond positively to local applications of 0.5-1% anthralinMore placebo control studies are needed to justify the use of anthralin in alopecia areata.
Minoxidil:
Minoxidil appears to be effective in the treatment of alopecia areata. It’s mechanism of action has yet to be determined, but it is known to stimulate DNA synthesis in hair follicles and has a direct action on the proliferation and differentiation of the keratinocytes28. In one clinical study, hair growth was demonstrated in 38% and 81% of patients treated with 1% and 5% minoxidil respectively. Thus 5% minoxidil solution is usually recommended as a treatment option in alopecia areata. No more than 25 drops are applied twice per day regardless of the extent of the affected area. Initial regrowth can be seen within 3 months, but continued application is needed to achieve cosmetically acceptable regrowth. Minoxidil has also been studied in combination with anthralin29, topical betamethasone propionate30 and prednisolone31. Minoxidil is of little benefit to patients of severe alopecia areata, alopecia totalis or alopecia universalisThe possible side effects from minoxidil are allergic and irritant contact dermatitis and hypertrichosis which is usually reversible with the interruption of the treatment.
Topical immunotherapy:
Topical immunotherapy is the best documented treatment so far for severe and refractory cases of alopecia areata. Topical immunotherapy is defined as the induction and periodic elicitation of allergic contact dermatitis by applying a potent contact allergen33. In 1965, the alkylating agent triethyleneimino benzoquinone was the first topical sensitizer used to treat cutaneous disease, but it was abandoned on account of its mutagenic potential. Later nitrogen mustard, poison ivy, nickel, formalin, and primin were tried, mainly as topical immunotherapy, for alopecia areata and warts. Contact immunotherapy was introduced in 1976, by Rosenberge and Drake. Later, potent contact allergens namely dinitrochlorobenzene (DNCB) and diphenylcyclopropenone (DPCP) replaced the allergens that were used earlier33. DNCB is mutagenic against Salmonella tymphimurium in the Ames test and is no longer usedNeither SADBE, nor DPCP are mutagenic. DPCP is more stable in solution and is usually the agent of choice.
Mechanism of action: Topical immunotherapy acts by varied mechanisms of action. The most important mechanism is a decrease in CD4 to CD8 lymphocyte ratio which changes from 4:1 to 1:1 after contact immunotherapy. A decrease in the intra-bulbar CD6 lymphocytes and Langerhan cells is also noted. Happle et al, proposed the concept of ‘antigenic competition’, where an allergic reaction generates suppressor T cells that non-specifically inhibit the autoimmune reaction against a hair follicle constituent. Expression of class I and III MHC molecules, which are normally increased in areas affected by alopecia areata disappear after topical immunotherapy treatment34.A ‘cytokine inhibitor’ theory has also been postulated34.
Method of sensitization: The protocol for contact immunotherapy was first described by Happle et al in 1983 The scalp is the usual sensitization site. For the initial sensitization a cotton-tipped applicator saturated with 2% DPCP in acetone is applied to a small area. Patients are advised to avoid washing the area and protect it from sunlight for 48 hours. After 2 weeks 0.001% solution of DPCP is applied on the scalp and then the application of contact allergen is repeated weekly with increasing concentrations. The usual concentration of DPCP that ultimately causes mild contact eczema is 0.01-0.1% and this is repeated weekly till a response is seen. An eczematous response indicates that sensitization has taken place. Only 1-2% of the patients fail to sensitize. It is important to remember that DPCP is degraded by light and should thus be stored in the dark and the patient should also wear a wig or hat during the day after application of DPCP. DPCP immunotherapy has even been combined with oral fexofenadine treatment with good effect36.
Evaluation of efficacy: The clinical response after six months of treatment is rated as per the grading system proposed by Mcdonald Hull and Norris37:
Grade 1- Regrowth of vellus hair.
Grade 2- Regrowth of sparse pigmented terminal hair.
Grade 3- Regrowth of terminal hair with patches of alopecia.
Grade 4- Regrowth of terminal hair on scalp.
If no regrowth is observed within six months of treatment, the patient is considered to be a non-responder. Evaluation of plucked hair is done using light microscopy, for evaluation of anagen/telogen ratio.
A review of most of the published studies of contact immunotherapy concluded that 50-60% of patients achieve a worthwhile response but the range of response rates was very wide (9-87%)Patients with extensive hair loss are less likely to respond. Other reported poor prognostic factors include the presence of nail changes, early onset disease and a positive family history39.
Topical immunotherapy can lead to certain side effects such as persistent dermatitis, painfull cervical lymphadenopathy, generalized eczema, blistering, contact leukoderma, and urticarial reaction. Systemic manifestations such as fever, arthralgia and yellowish discoloration of hair are noted more often with DNCB.
In poor responders to DPCP, squaric acid dibutylester (SADBE) can be tried as a contact sensitizer. The method of application is the same as with DPCP but the applications are done once or twice weekly40.
Good care should be taken to avoid contact with the allergen by handlers, including pharmacy and nursing staff. Those applying the antigen should wear gloves and aprons. There is no available data on the safety of contact immunotherapy during pregnancy and it should not be used in pregnant women or in women intending to become pregnant.
Tacrolimus:
Tacrolimus is a topical calcineurin inhibitor that inhibits transcription following T-cell activation of several cytokines including IL-2, IFN-gamma and TNF-α. Yamamoto et al reported in their findings that tacrolimus stimulated hair growth in mice41, although subsequent studies have shown conflicting resultsRecently, Price et al reported an 11-patient study in which none of the patients had terminal hair growth in response to tacrolimus ointment 0.1 % applied twice daily for 24 weeks43.
Topical garlic
Garlic is a very commonly used home remedy in the treatment of alopecia areata in India and even in the rest of the world. One study analyzed the effect of a combination of topical garlic gel and betamethasone valerate ointment in alopecia areata in a double-blind study. The study found the combination useful in majority of the patients with a statistically significant difference between the treatment and control groups44.
Topical retinoids:
Among topical retinoids, tretinoin and bexarotene have been tried in alopecia areata with mixed results-46Irritation of the skin is a very common side effect and the efficacy is doubtful in the absence of double-blind randomized trials.
Prostaglandin analogs:
The propensity of certain prostaglandin analogues used as anti-glaucoma eye drops to cause hypertrichosis has been employed in the treatment of alopecia areata. These prostaglandin analogues include Latanoprost and Bimatoprost and they are used in the treatment of alopecia areata involving the eyelashes-48However, the results obtained with these drugs have not been really encouraging49.
Systemic treatments
Systemic treatments, as a rule, are used only in progressive forms of alopecia areata and going by the immune nature of the disease, majority of these treatment options are immunosuppressants or immunomodulators in nature.
Systemic corticosteroids:
The use of systemic corticosteroids for the treatment of alopecia areata is under much debate. Some authors support a beneficial role of systemic steroids on halting the progression of alopecia areata, but many others have had poor results with this form of therapy. The suggested dosages are 0.5-1mg/kg/day for adults and 0.1-1 mg/kg/day for children50. Treatment course ranges from 1-6 months, but prolonged courses should be avoided to prevent the side effects of corticosteroids. Side effects profile of corticosteroids in conjunction with the long-term treatment requirements and high relapse rates make systemic corticosteroids a more limited option. In addition to the daily oral administration of corticosteroids, there are several reports of high-dose pulsed corticosteroid treatments employing different oral and intravenous regimens51-53. Many of these regimens have been tried in alopecia areata with encouraging results but the majority of these studies have been non-blind open studies. One such pulsed administration employs a high dose oral corticosteroid on two consecutive days every week with a gap of 5 days between the two pulses. This modality of treatment is known as oral minipulse therapy (OMP) and it has been tried in many skin diseases in addition to alopecia areata like vitligo54-55 and lichen planusSome open label studies on corticosteroid OMP therapy have reported encouraging results in alopecia areata53.
Sulfasalazine:
Because of its immunomodulatory and immunosuppressive actions, sulfasalazine has shown good hair regrowth in the treatment of alopecia areata. The drug is administered orally usually as enteric coated tablets to minimize the gastrointestinal side effects. The treatment is started at a lower dose, usually in the range of 500 mg twice daily and then the dose is gradually increased to 1 g three times a dayAdverse effects include gastrointestinal distress, liver toxicity and haemotological side effects. Sulfasalazine helps in alopecia areata because it causes inhibition of T cell proliferation, and natural killer cell activity and also inhibits antibody production. It also inhibits the secretion of interleukin (IL)-2, IL-1, TNF- and IFN-gamma and even IL-667.
A number of clinical studies have documented a positive effect of sulfasalazine in alopecia areata. In one clinical study, 23% patients showed a really good response with satisfactory hair growth after sulfasalazine therapyOther studies have also shown a beneficial effect of this treatment option in resistant cases of alopecia areata66,69.
Azathioprine:
Azathioprine, being an immunosuppressive agent has also been tried in alopecia areata. The drug is used in many cutaneous disorders owing to its effect on circulating lymphocytes as well as Langerhan cells. In a limited study on 20 patients hair regrowth was demonstrated in about half of the patients with a dosage regimen of 2g/day70.
Cyclosporine:
This drug has proven effective in the treatment of alopecia areata because of its immunosuppressive and hypertrichotic properties. The side effect profile and high rate of recurrence render the drug a poor choice for the use in alopecia areata. So the drug is to be attempted only in severe forms of alopecia areata not responding to treatment71.
Methotrexate:
Methotrexate either alone or in combination with prednisolone has been used in the treatment of alopecia areata in various studies with variable success rates72.
Oral zinc sulphate
Serum zinc levels have been found to be lower in patients with alopecia areata than in control populationIn a study on 15 patients, hair regrowth was observed in 9 patients (67%) after oral zinc gluconate administration74.
Biological agents:
Tumour necrosis factor inhibitors such as Adalimumab, Infliximab and Etanercept have been tried in alopecia areata, but the results have not been encouraging-76Clinical trials conducted till now have failed to demonstrate the efficacy of any biological agent in alopecia areata.
Photo-and photochemotherapy
Photochemotherapy:
Several uncontrolled studies regarding PUVA therapy for the treatment of alopecia areata exist. All types of PUVA (oral PUVA, topical PUVA, local or whole body UVA irradiation) have been used with success rates of up to 60-65%57-59. The mechanism of action is considered to be the interference in the presentation of follicular antigens to T-lymphocytes by depletion of the Langerhan cells. The relapse rate following treatment is high, sometimes demanding repeated treatments for a prolonged period with implications for carcinogenic risks60. To mitigate the side effects of systemic psoralens, PUVA-turban therapy is used for alopecia areata involving the scalp. In this form of photochemotherapy, very dilute solutions of 8-methoxy psoralen are applied on the scalp by utilizing a cotton towel as a turban. The patient’s scalp is exposed to UVA after keeping the ‘turban’ in contact with the scalp for about 20 minutesThe efficacy of this form of PUVA therapy has been seen to be about 70%61.
Phototherapy
Although narrowband UVB is among the most effective treatment options in a number of immune mediated skin diseases, the same efficacy has not been found in alopecia areata. Properly designed randomized trials are needed to elucidate whether NBUVB has any role in the management of alopecia areata62-63.
Excimer laser and excimer light
Excimer laser and excimer light are two more recent additions to the phototherapeutic armamentarium for many skin and hair disorders. While the main use of these phototherapeutic modalities remains to be psoriasis and vitiligo, their immunomodulatory effect can be made use of in many other skin disorders. Some clinical studies have documented the efficacy of excimer laser and excimer light in alopecia areata64-65. In one such study, 41.5% patches were shown to respond to excimer laser therapy administered over 12 weeks64. Another study on childhood alopecia areata found regrowth in 60% lesions after a treatment period of 12 weeksThe treatment is well tolerated with erythema of the skin as the only adverse effect reported.
Miscellaneous therapies
Various non-conventional therapeutic agents have been used in alopecia areata with some degrees of success. These include fractional Er-Glass laser77, topical azelaic acid78, topical onion juice79, topical 5-fluorouracil ointment80 and photodynamic therapyThe efficacy and safety of these therapeutic agents need to be confirmed in large-scale, double-blind, placebo-controlled trials before they can be recommended for treatment of alopecia areata.
Non-pharmacological methods
Cosmetic treatments for patients with alopecia areata include the following:
a) Dermatography: It has been used to camouflage eyebrows of patients with alopecia areata. In this treatment tiny pigment dots of pigment are used on the skin on the region of the eyebrows to mask the underlying alopecia81.
b) Wigs or Hair pieces: These are useful for patients with extensive disease and allow them to carry on their usual social life.
Conclusion:
Alopecia areata is now regarded as an autoimmune disease involving the cellular immunity through the CD8 lymphocytes that act on follicular antigens. The pathogenesis of alopecia areata is being unravelled with various animal and human studies.
The localized forms often heal spontaneously or respond to simple treatments such as topical or intralesional corticosteroids. The severe forms have a reserved prognosis and are difficult to treat. In these cases the best results are achieved by topical immunotherapy technique.
Vitiligo is one of the oldest and commonest skin disorders affecting approximately 1-2% of the human population.1 The disease shows no regard to the ethnic, racial or socioeconomic background of the affected sufferers. The cosmetic impact of this disease is tremendous and its psychological impact devastating particularly in coloured races.2,3,4 The aetiopathogenesis of this disease is now much better understood (table 1)5 compared with a decade earlier but much remains unknown. In parallel with these developments on the aetiological front, a lot of new advances have been made on the therapeutic front as well. With these new therapeutic options, we are currently in a much better position to treat this disease than we were a decade or two earlier. So, how far and how satisfactorily are we able to treat this disorder now? What are the new treatment options available for this disorder and how far have they helped a dermatologist to claim a cure for this disorder? These are some of the questions that will be addressed in this paper.
New advances in management
Medical therapies
The most recent advances on the medical front have been Narrowband Ultraviolet B (NB-UVB) therapy, Targeted Ultraviolet B (UVB), Excimer laser therapies, topical immunomodulator treatment in the form of topical calcineurin inhibitors, topical pseudocatalase, and topical Vitamin D analogues in combination with Ultraviolet (UV) light.
NB-UVB
NB-UVB, using UV-lamps with a peak emission of around 311nm has now emerged as the treatment of first choice in generalized vitiligo as well as vitiligo vulgaris (patchy vitiligo).6,7,8 The efficacy of NB-UVB in vitiligo was first demonstrated by Westerhof and Nieuwboer-Krobotova in 1997.9 Since then there have been a large number of clinical studies that have demonstrated the therapeutic benefit of NB-UVB in vitiligo patients. The mechanism of action of NB-UVB in vitiligo is through induction of local immunosuppression and stimulation of the proliferation of melanocytes in the skin and the outer root sheath of hair follicles.6 There is a stimulatory effect on melanogenesis and on the production of Melanocyte Stimulating Hormone (MSH).6 Comparison studies have shown a significantly enhanced rate of repigmentation with NB-UVB compared with topical Psoralen and Ultraviolet A (PUVA) therapy.10 Furthermore, the incidence of adverse effects seen commonly with topical PUVA, such as phototoxicity, is significantly reduced with the use of NB-UVB.
NB-UVB has shown a number of advantages over PUVA in vitiligo patients in addition to its excellent efficacy. These advantages include its extremely low side-effect profile particularly on the systemic front, its established safety in children, and safety in pregnant females. NB-UVB also has considerably better patient compliance as there is no need to time the exposure with any drug intake or any need for eye protection beyond treatment exposure time. A recent double-blind randomized11 study comparing NB-UVB with PUVA demonstrated a much better efficacy with NB-UVB. The study found that repigmentation achieved with NB-UVB was much better with respect to colour matching with uninvolved skin, and this was also more persistent than that achieved with PUVA.11
In addition NB-UVB has been used in childhood vitiligo with excellent results.12 No additional adverse effects were seen in children with NB-UVB as compared with those in adults. Furthermore, given the long-term safety profile of NB-UVB in comparison with PUVA as far as skin malignancies are concerned,13 NB-UVB is now preferred over all other treatment options in the management of generalized vitiligo in both adults and children.
Table 1: Aetiological hypothesis of vitiligo5
Aetiological hypothesis
Brief explanation
Autoimmune hypothesis
Believes that vitiligo occurs because of destruction of melanocytes by an immune mechanism.
Most favoured theory at present, supported by many recent in-vitro studies.
Auto-cytotoxic hypothesis
Believes that vitiligo occurs because of accumulation of toxic metabolites in the melanocytes secondary to a defect in their metabolic clearance of the toxins.
Neurogenic hypothesis
Believes that vitiligo is because of an altered reaction to neuropeptides, catecholamines and their metabolites by epidermal melanocytes.
Biochemical hypothesis
Believes that over-secretion of hydrobiopterin, a cofactor of tyrosine hydroxylase results in accumulation of catecholamines that in turn results in formation of reactive oxygen species in the melanocytes. These reactive oxygen species are thought to cause destruction of affected melanocytes in vitiligo patients.
NB-UVB has been used in combination with different topical agents to increase its efficacy and thus shorten the total duration of treatment. Treatment options that have been used with NB-UVB in vitiligo till date include topical tacrolimus,14,15 pimecrolimus,16 Vitamin D analogues17,18 and even topical pseudocatalase.19 While some studies have shown a synergistic effect with these combinations, others have found the efficacy of the combinations to be similar to NB-UVB alone. In one half-body comparison study, topical placental extract was used in combination with NB-UVB but the combination was shown to offer no added benefit than NB-UVB alone.20 Therefore, the ideal topical agent to be combined with NB-UVB remains unknown.
Laser Therapy
Excimer laser, which uses Xenon-Chlorine (Xe-Cl) gas and produces a monochromatic laser light of 308nm wavelength, is another innovative treatment option for vitiligo. The laser system has been used with increasing frequency over the last few years for targeted treatment of individual vitiligo lesions.21 The laser is used either alone or in combination with topical immunomodulator or PUVA-sol therapy.22,23 Treatment with this laser is claimed to give extremely good and early results in both localized and segmental vitiligo. In a pilot study21 on 18 patients with 29 affected areas 57% of lesions showed varying degrees of repigmentation after just six exposures over two weeks. The figure was increased to 87% after 12 treatments over four weeks.21 Another recent study has reported a repigmentation of >75% in 61% of lesions after 30 treatments with Excimer laser. Repigmentation was found to be better on the face and trunk than on the extremities.24
Topical therapies, particularly topical tacrolimus, have been used in combination with Excimer laser. This combination has been claimed to be more effective than Excimer laser alone.22 In a randomized right-left comparison study22 with 14 patients, Excimer light monotherapy was compared with a combination of Excimer laser with topical tacrolimus. While 20% of lesions treated with Excimer laser alone achieved >75% repigmentation, the same degree of repigmentation was obtained in 70% lesions with the combination treatment.22 Topical methoxsalen has also been used in combination with Excimer laser phototherapy and this has been claimed to have worked better than laser therapy alone.23
The advantage of Excimer laser therapy over conventional UVB therapy is the targeted mode of treatment with no exposure of the uninvolved skin. Moreover, the onset of repigmentation is earlier with Excimer laser therapy than with UVB therapy.
Targeted UVB therapy
This is another recent innovation in vitiligo management that has arrived over the last few years. The beauty with this therapy is that it delivers high intensity UVB light only to the affected vitiliginous areas, avoiding any exposure to the uninvolved skin. This not only decreases the cumulative UVB dose received by an individual patient, but is also claimed to improve the efficacy of treatment quite significantly.
Targeted UVB therapy, as expected, finds its use more in the treatment of focal and segmental types of vitiligo. In fact, the first study25 with targeted UVB therapy was done on eight patients with segmental vitiligo. Five of these patients achieved >75% repigmentation of their lesions with this therapy.25
Targeted UVB therapy offers certain advantages over Excimer laser phototherapy. The treatment is safer and more efficacious compared with conventional UVB therapy, and almost as efficacious but much less costly than Excimer laser therapy.26
Systemic immunomodulator therapy
Vitiligo is thought to be an immune-mediated disease and thus immune-suppressive and immunomodulator agents have been used on a regular basis in this disease. Among the immunosuppressants, systemic steroids have been the most commonly used. However, systemic steroid therapy has always been associated with a high incidence of adverse effects especially in children which is the age-group most commonly affected. To overcome this limitation, steroids have been given in pulse or even in mini-pulse form. A prospective study involving 14 patients with progressive or static vitiligo showed cessation of disease activity and a repigmentation rate of 10-
60% after high-dose methylprednisolone pulse therapy administered on three consecutive days.27 Systemic steroids have also been administered in a mini-pulse form on two consecutive days every week, known as Oral Minipulse (OMP) therapy. The first study demonstrating the efficacy of OMP with oral betamethasone (0.1mg/kg with a maximum of 5mg) was described in 1991.28 In a later study29 on childhood vitiligo, betamethasone was replaced by oral methylprednisolone and combined with topical fluticasone ointment on the vitiligo lesions. The disease was arrested in >90% of patients, and >65% of children achieved good to excellent (>50%) repigmentation of their vitiligo lesions.29
Topical Vitamin D analogues
Vitamin D analogues, particularly Calcipotriol, have been used topically either alone or in combination with topical steroids in the management of vitiligo. The basis for the use of these agents is that Vitamin D3 affects the growth and differentiation of both melanocytes and keratinocytes. This has been further proved by the demonstration of receptors for 1 alpha-dihydroxyvitamin D3 on the melanocytes. These receptors are believed to have a role in stimulating melanogenesis.29 Vitamin D analogues have given variable results in the treatment of vitiligo in different studies. These agents have also been used in combination with UV-light (including NB-UVB) and topical steroids with variable results.30,31,32
Topical immunomodulators
Topical immunomodulators, such as tacrolimus and pimecrolimus, have been the most promising recent additions to topical vitiligo therapy. In fact because of their efficacy and a remarkable safety profile the use of these agents in vitiligo has shown a consistently increasing trend over the last few years. These agents can be safely administered in young children, as they don’t cause any atrophy or telangiectasia of the skin even after prolonged use. There is also no risk of hypothalamic-pituitary-adrenal (HPA) axis suppression as seen with the widespread use of potent topical steroids.33 The first study that demonstrated the efficacy of tacrolimus in vitiligo was published in 2002.34 In this study tacrolimus was used in six patients with generalized vitiligo and five of them achieved >50% repigmentation of their lesions by the end of study period.34 Since then many additional studies have been published on this subject and have clearly demonstrated the role of topical tacrolimus in vitiligo. The best results with topical immunomodulator therapy have been seen on exposed parts of the body such as the face and neck and, as with any other therapy, the acral parts of the body respond the least.34,35 Similar results were obtained with the use of topical pimecrolimus in vitiligo patients.36
Pseudocatalase
Pseudocatalase has been used in combination with Dead Sea climatotherapy or UVB exposure for the treatment of vitiligo. The basis for the use of this agent in vitiligo is the evidence of oxidative stress and high H2O2 levels in the lesional skin.37 While some earlier studies37 demonstrated excellent results with this agent in inducing repigmentation in vitiligo, later studies have cast doubts on its efficacy.38 Pseudocatalase is used topically on the lesional skin, and this is followed by UVB exposure to the whole body or to the lesional skin. The combination is claimed to correct the oxidative stress on melanocytes in vitiligo patients and thus lead to correction of the depigmentation.
Topical 5-Fluorouracil
Topical 5-fluorouracil is supposed to induce repigmentation of vitiligo lesions by overstimulation of follicular melanocytes which migrate to the epidermis during epithelialization.39 This form of topical therapy can be combined with spot dermabrasion of the vitiligo lesions to improve the repigmentation response. In a study by Sethi et al,40 a response rate of 73.3% was observed with a combination of spot dermabrasion and topical 5-fluorouracil after a treatment period of six months.40
Surgical therapies
Surgical therapies for vitiligo have further increased the percentage cure of the disease by an appreciable degree, with the consequent increase of their use in the management of unresponsive vitiligo both in India and abroad. These surgical therapies, as a rule, are indicated in those patients who have a stable (non-progressive) disease of at least one year and not responding to medical treatment. In general the most important advantage with these procedures is that the chances of repigmentation of lesions are in the range of 90-100%. Moreover, these interventions are becoming better and easier to perform with every passing day.
Different surgical therapies that have been attempted in the management of vitiligo include autologous suction blister grafting, split-thickness grafting, punch grafting, smash grafting, single follicular unit grafting, cultured epidermal suspensions and autologous melanocyte culture grafting. All these grafting procedures, except the melanocyte culture grafting, are easy to perform and do not require any sophisticated instruments. These grafting techniques have now been divided into two types, tissue grafts and cellular grafts, depending on whether whole epidermal/dermal tissue is transplanted or the individual cellular compartment.
Tissue grafting technique
Suction blister grafting
Here, thin epidermal grafts are taken from suction blisters on the donor site, usually on the buttocks or thighs. These suction blisters are produced by applying sufficient negative pressure on the skin at the donor site by using a suction apparatus or syringes with three-way cannulae. The epidermal grafts are then transplanted on to dermabraded vitiligo lesions. This leads to repigmentation of the recipient areas with an excellent cosmetic matching. The ease of the procedure, the high success rate and the excellent cosmetic results have all made suction blister grafting the procedure of choice in vitiligo grafting.41
Split thickness grafting
In this grafting technique a thin split thickness graft is taken from a donor site with the help of a dermatome, Humby’s knife, Silver’s knife or a simple shaving blade. This graft is then transplanted on to dermabraded recipient areas. This technique also gives excellent cosmetic matching after repigmentation and the incidence of repigmentation in this technique is also quite high. In fact, most comparison studies on grafting techniques in vitiligo have shown that maximum repigmentation is achieved with either suction blister grafting or split thickness grafting.41 The advantage of partial thickness grafting over the suction blister method is that a relatively larger area of vitiligo can be tackled in a single sitting. Both partial thickness skin grafting as well as suction blister grafting can be followed up by NB-UVB to achieve faster and better results.
Miniature punch grafting
Here full-thickness punch grafts of 1.0 to 2.0 mm diameter are taken from a suitable donor site and then transplanted on to similar punch shaped beds on the recipient vitiligo lesions. The recipient area is then treated with either PUVA/PUVA-sol or topical steroids leading to spread of pigment from the transplanted punches to the surrounding skin. With time the whole of the recipient area gets repigmented. The advantages of this procedure are that it is easy to perform and can take care of a relatively larger vitiligo area compared with the above two procedures. Also vitiligo lesions with irregular or geographical shapes can be treated with this procedure. However there are certain limitations. There is the risk of ‘cobblestone appearance’, ‘polka-dot appearance’, and hypertrophic changes at the recipient site.42 All these side effects can be minimized by proper patient selection and by use of smaller sized punches of 1.0 to 1.5 mm diameter. Miniature punch grafting is presently the commonest surgical procedure performed in India on vitiligo patients.
Follicular unit grafting
In this technique, single-hair follicular units are harvested/prepared from a suitable donor area as in the case of hair transplantation. These follicular units are then cut above the level of the follicular bulb and then transplanted into vitiligo lesions. The idea behind this technique is that the melanocytes in the follicular unit are ‘donated’ to the vitiliginous skin and serve as a source of pigment at the recipient site. The repigmentation process here simulates the normal process of repigmentation of vitiliginous skin quite closely and thus gives an excellent cosmetic result. This procedure combines the advantages of punch grafting with the excellent cosmetic results of split thickness or blister grafting techniques.43 The procedure is however tedious and needs good expertise on the part of the cosmetic surgeon.
Smash grafting
In this technique, a partial thickness graft is taken and is ‘smashed’, or cut into very small pieces, by means of a surgical blade on a suitable surface such as a glass slide. This ‘smashed’ tissue is then transplanted on to the dermabraded recipient skin and covered with a special powder or corrugated tube dressing so as to keep the smash-graft undisturbed on the recipient area. The advantage of this technique, over a simple partial thickness grafting, is that thicker grafts can be used with a good cosmetic result. The procedure has been indicated for those who are relatively inexperienced and cannot take an ideal, thin and transparent partial thickness graft from the donor area.44
Cellular grafting techniques
Non-cultured epidermal suspensions
Here a split-thickness graft is taken from a donor area and then incubated overnight. On the next day the cells are mechanically separated using trypsin-EDTA solution and then centrifuged to prepare a suspension. This cell suspension is then applied to the dermabraded vitiligo lesions, and a collagen dressing is applied to keep it in place. A relatively large area of vitiligo, about ten times the size of the donor graft can be taken care of with this procedure.45 The recipient area however has to be treated with either NB-UVB or PUVA for two to three months to achieve the desired pigmentation.
Melanocyte culture transplantation
This is a relatively more advanced grafting procedure where, once again, a split-thickness graft is taken from a donor area and incubated in an appropriate culture medium to grow the melanocytes or the keratinocytes-melanocyte combination in vitro. The cultured cells are then applied onto laser dermabraded, or even mechanically abraded, lesional skin.46,47 The procedure is obviously more difficult to perform, as it needs the advanced laboratory facilities for melanocyte culture. However the results with this procedure are excellent and a relatively large area of involved skin can be tackled by a single donor graft.
Summary
Table 2 summarises the above discussion of treatment options in vitiligo.
Table 2: New treatment options in vitiligo
Medical therapies and phototherapy
Surgical therapies
Narrowband UVB therapy either alone or in combination with immunomodulators, Vitamin D analogues etc.