With the increasing use of ultrasound as a standard examination in the first trimester, more incidental adnexal masses are detected. The reported incidence of adnexal masses in pregnancy varies, depending on the criteria used to define the mass. A literature review by Goh W. et al., found that 1% of all pregnancies are diagnosed with an adnexal mass 1. A more recent article has suggested adnexal masses are diagnosed in 5% of all pregnancies 2. Simple and functional cysts are very common, and they usually resolve after the first trimester 3. Mature teratomas are by far the most common persistent adnexal masses found in pregnancy 8. It has been estimated that up to 5% of adnexal masses in pregnancy are malignant 4.
Ovarian cysts are typically asymptomatic, but they can cause pain due to pressure on adjacent organs, rupture, bleeding or torsion. The latter case is a significant health condition which mainly requires emergency surgical intervention. During pregnancy, surgical management of ovarian cyst complications is more difficult and more challenging. This is mainly because of other differential diagnosis causing similar symptoms related to pregnancy such as ectopic pregnancy and miscarriage. In case of surgical intervention, the second trimester of pregnancy is supposed to be the safest window for surgery as the risk for drug-induced teratogenicity is smaller than in the first trimester, most functional cysts have disappeared by then and it is technically less difficult than operating during the third trimester 13.
Antenatally, ultrasound is considered to be the best first-line imaging to evaluate adnexal masses 5. Ovarian mass characterization into benign, malignant or borderline can be challenging in pregnancy. This is mainly due to the effect of high levels of gestational hormones which can cause decidualisation of the cystic or solid parts of the ovaries. Benign masses can mimic malignant masses due to this pregnancy related phenomena 12. One of the largest data in literature on ovarian mass characterization is published by the International Ovarian Tumor Analysis group (IOTA). All IOTA studies excluded pregnant women when they developed and validated the rules and models to characterize ovarian masses 14-17. This limits our knowledge and ability to use these models in pregnant women. It is known that tumour markers may be raised in pregnancy and should therefore not routinely been done 7. An alternative diagnostic tool is Magnetic Resonance Imaging (MRI) which is considered to be safe in pregnancy and can be helpful if the ultrasound imaging is inconclusive in evaluating whether a mass is benign or malignant 6; 10. The American College of Gynecology and Obstetrics recommends that pregnant patients should be reviewed on a case-to-case basis and stated that there are no known biological effects of MRI on fetuses. However, Gadolinium, which help in characterizing ovarian masses, should be avoided when examining a pregnant patient 11.
The aim of this retrospective study was to look into characteristics, size and subsequent management of cases of adnexal masses in early pregnancy.
Methods
This was a retrospective study of data collected between 12/01/2014 and 14/11/2016 in the Early Pregnancy and Gynaecology Unit (EPAGU) of a tertiary referral centre (Guy’s and St Thomas’ NHS Trust, GSTT) in central London. The Ultrasound reporting system (Astraia Software Gmbh, Version 1.24.10, Munich, Germany, 2016) was searched for data. Cases included were consecutive. The study was approved as a service evaluation audit by the Clinical Governance team at Guy’s and St Thomas’ NHS Trust. The study included women who were diagnosed with an adnexal mass while having a transvaginal ultrasound scan TVS at or before 15 weeks of gestation. Pregnancy was confirmed by a positive pregnancy test and an intrauterine gestation on transvaginal ultrasound scan. Women who had the first gestational TVS after 15 weeks of gestation, pregnancies of unknown location, ectopic or trophoblastic pregnancies and patients who had ovarian stimulation treatment were all excluded.
Repeat ultrasound scan reports were retrieved from the Astraia system. Further procedures, tests and imaging results were retrieved using the Electronic Patient Reporting system at GSTT (EPR application, iSOFT Group plc., USA, 2004), PACS (GE Medical Systems, Wisconsin, USA, 2006), Badgernet (Clevermed, Client version 2.9.1.0, Edinburgh, UK). We have used the subjective impression of the examiner as the index test. If surgery was performed the final outcome to identify benignity or malignancy was considered to be the histological diagnosis if any removed tissue. Cytology was used for a reference test in two cases when ovarian cysts were aspirated only. Borderline tumours were classified as malignant for statistical analysis. Tumours were classified using the criteria recommended by the World Health Organisation (WHO) 9; 10. All ultrasound scan images were available and reviewed by author TEG to confirm the US finding. For statistical analysis, the SPSS software package was used (version 24 for Windows, Chicago, IL, USA). A two tailed student’s t test was used to compare means in ovarian masses diameters and a p value of less than 0.05 was considered statistically significant.
Results
7150 patients underwent transvaginal scans for early pregnancy in that period. In total 48 cases of women with adnexal masses in pregnancy and completed data were analysed. Seven women have been excluded; one woman being postpartum at the time of the finding of a large endometrioma, five pregnancies due to assisted conception and one woman was found to have a corpus luteum cyst (Figure 1).
Figure 1: Study flow chart.
41 women with 46 ovarian cysts could be included in the study. Two women had bilateral ovarian cysts, one had two ipsilateral cysts and one woman had three ipsilateral cysts. The mean age at the time of detection of the ovarian mass was 30 (95%CI:28-32) (Fig.2).
Figure 2: Age distribution in the study group.
The mean gestation at the time of first ultrasound was 7.4 weeks (95%CI:6.6-8.3). The mean diameter of ovarian cysts measured 47.7mm (95%CI:39.9-55.4). In 36 women ultrasound alone was performed to reach diagnosis, one woman had an extra MRI scan, two women had tumour markers on top of the TVUS and in two women an MRI scan and tumour markers were performed after the TVUS. The ovarian cyst(s) was on the right ovary in 16/41 women, on the left in 22/41, bilateral in 2/41 and in one case the side of the cyst was not reported. The most common ultrasound subjective impression was mature teratoma (22/46 cysts), followed by simple cysts (12/46 cysts), haemorrhagic cysts (6/46 cysts), endometriomas (5/46 cysts) and one possible mucinous Borderline tumour. The latter was confirmed later on histology as the stage FIGO 1A intestinal type mucinous Borderline tumour (Fig.3).
Figure 3: Distribution of origin of cysts by histology.
In total 8/41 women (19.5%) underwent surgical intervention; of these eight cases six underwent major surgery under GA and two had a cyst aspiration under local anaesthesia. Seven out of these eight masses were classified as benign on USS and were subsequently confirmed to be benign by histology or cytology. In only one case a complex adnexal mass was found on USS examination at 9 weeks of gestation and the MRI scan reported possible malignancy. Tumour markers in this 23-year-old woman were normal and a laparotomy was performed at 17 weeks of gestation to remove the mass. Histology showed the mass to be a mucinous borderline tumour, FIGO stage IA. In another patient, an oophorectomy had to be performed at the time of the Caesarean section at term for fetal distress as the ovary was found to be necrotic. In this patient an ultrasound at 10 weeks of pregnancy had demonstrated a 6cm diameter haemorrhagic cyst, which had presumably torted during the pregnancy without any symptoms to prompt the patient to refer herself. Histology in this case had shown an infarcted cyst with fibrosis and calcification. In four of the major surgery cases performed under GA uncomplicated laparoscopies were performed to remove the adnexal mass; in one case a laparoscopic salpingoophorectomy was performed as an emergency for a suspected ovarian torsion at 16/40 weeks. In three cases a laparoscopic procedure for cystectomy was performed electively for ongoing pain. In the first case a cyst was diagnosed in early pregnancy subsequently there was a miscarriage and the cyst was removed 4 months after the diagnosis. In the second case a cyst was found in early pregnancy the woman had a termination at 11 weeks of pregnancy and a cystectomy 5 months later. In the third case a laparoscopic cystectomy was performed 8 weeks after the diagnosis, however the woman suffered a miscarriage at 12 weeks of gestation. Histology confirmed dermoid cysts in all four of these cases. The two cyst aspirations performed under local anaesthesia and ultrasound guidance were both symptomatic for torsion, one at nine weeks and one at ten weeks of pregnancy. In both patients the procedure has been successful. 33/41 (80.5%) with no indication for surgical intervention. There was a significant difference in the mean diameter of ovarian cysts in the expectant management group (41.2mm; 95%CI:34.7-47.7) compared with the mean diameter of cysts in the surgically managed group (74.5mm; 95%CI: 49.2-99.8) (Fig.4).
Figure 4: Mean diameter of the ovarian cysts.
In 33/41 patients no surgical intervention was needed during pregnancy. 13/33 patients had no follow up of their ovarian cyst arranged and no further mentioning of the cysts on routine growth and anomaly scans during pregnancy was found. In 20/33 patients at least one routine follow-up scan was performed 1-2 weeks after the diagnosis and in 12 of these 20 patients a second follow-up had taken place at least 1 month after the diagnosis. In one of the 20 patients with recorded follow-up’s an MRI scan had been arranged 2 months after the initial USS finding of a dermoid cyst.
Discussion
The results of our study confirm findings from previous studies: The vast majority of ovarian masses in pregnancy are benign and invasive cancer in pregnancy is rare; The results show a significant relation between size of adnexal mass and probability for surgery; Ultrasound examination of adnexal masses has been proven to be accurate and safe in pregnancy; Managing ovarian cysts in pregnancy can be challenging. Goh et al. have reported similar outcomes, namely that ovarian torsion is still reported as a rare event in pregnancy and that the management of most adnexal masses in pregnancy can be conservatively managed if asymptomatic and if there are no ultrasound findings suspicious for malignancy 8. If a surgical intervention is needed for persistent masses with complications such as torsion Goh et al. have found that laparoscopy during 1st and 2nd trimester can be safely performed 1. In our cohort two out of six women underwent successful major surgery during the 2nd trimester of pregnancy. One had an emergency laparoscopy for a torsion at 16 weeks of pregnancy and the other had a laparotomy at 17 weeks of pregnancy for a mucinous borderline tumour.
However, to our knowledge currently no evident guidelines exist on how to manage and follow-up ovarian masses during pregnancy. The characteristics and presentation of ovarian mass complications in pregnancy can be mimicked by similar symptoms related to pregnancy, such as ectopic pregnancy. In one of our cases a woman with a known ovarian cyst was found to have a necrotic ovary at the time of Caesarean section, despite no signs of torsion at any time during pregnancy. This only highlights how challenging and difficult the assessment of ovarian masses during pregnancy can be. Additional diagnostic examinations such as tumour markers in suspicious ovarian masses have been found difficult to interpret in pregnancy. However, there has been literature suggesting that if a mass is strongly suspicious for malignancy, it is likely that CA-125 will be severely elevated (1000-10 000) 7.
The strength of this study is that the data has been collected using the expertise and facilities of a tertiary referral centre in London (GSTT). The limitations of this study include retrospective data collection, small numbers of cases and loss of follow-up. Although, our study shows the benign nature of most ovarian masses in pregnancy and the ability of ultrasound to safely characterize ovarian masses, a prospective study is required to validate our results. As it is difficult to interpret ovarian cancer tumour markers in pregnancy 7, other models, such as the IOTA Simple Rules14,16 or the ADNEX model17 may play a role for further characterisation of ovarian masses. A prospective trial is required to validate these models in pregnancy.
Despite advances in the management of ectopic pregnancies an emphasis must be given on improving the understanding of the women and the healthcare professionals of the pathophysiology of haemorrhagic shock.
Educating the public and all health care professionals about the phrase “Think Ectopic” as a main differential in any women of childbearing age with atypical signs and symptoms of general ill health is paramount.
Précis
The significance of effective communication within multidisciplinary teams especially in emergency situations towards optimising patient care and saving lives cannot be understated.
Case Report
A 27-year-old woman who claimed to be unaware of her current pregnancy collapsed at her home. She was not known to have any co-morbidities. Paramedics were called and found her to be in cardiac arrest with pulseless electrical activity. Cardiopulmonary resuscitation (CPR) was immediately commenced. Spontaneous circulation returned after 13 minutes of CPR at home.
She was then transferred to the emergency department. On arrival to the emergency department her Glasgow Coma Scale (GCS) was 3. She had a pulse rate of 130 beats per minute; unrecordable blood pressure; haemoglobin of 55g/l; metabolic acidosis with a pH of 6.8; lactate > 15; and a potassium of 6.6 mmol/l. She was resuscitated and gradually regained consciousness with a GCS of 15.
In the midst of stabilising her condition and unaware of her pregnancy, a urine pregnancy test was obtained following siting of a urinary catheter. A positive pregnancy test prompted notification to the gynaecology team who performed ultrasonography imaging which revealed significant haemoperitoneum. An immediate decision was made to perform laparotomy in view of the most likely diagnosis of a ruptured ectopic pregnancy.
Laparotomy revealed a 3.5 litre of haemoperitoneum secondary to a ruptured right sided tubal ectopic pregnancy. A right salpingectomy was performed. The patient was subsequently transferred to the intensive care unit as her serology results were consistent with multi organ failure with a platelet count of 46 (109/L); creatinine of 194 mmol/L; estimated glomerular filtration rate (egfr) of 27 mls/min/ 1.73 m2; alanine transaminase (ALT) of 441 IU/L; and alkaline phosphatase (ALP) of 49 IU/L.
She made an uneventful recovery as demonstrated in figure 1 by the improving serological parameters and was discharged home after 6 days.
Figure 1: The cumulative serology- full blood count, liver function tests, urea and electrolytes, clotting profile.ankle
Investigations
Day 0
Day 0
Day 1
Day 1
Day 2
Day 3
Day 4
Day 5
Day 15
13:46
18:30
05:53
17:27
06:49
07:00
11:14
09:37
09:50
Hb g/L (115-150)
82
100
83
73
72
88
89
93
WCC 109/L (3.5-11.0)
19.8
23
18.1
13.2
11.8
11.2
9.5
9.1
Plts 109/L (140-400)
46
61
49
46
48
51
76
106
ALP IU/L (30-130)
49
42
44
51
57
73
74
100
ALT IU/L (0-40)
441
428
701
3197
2621
1807
1290
185
Bili mmol/L (0-21)
9
13
8
18
18
16
11
4
Na mmol/L (133-146)
139
142
143
141
143
142
140
141
139
K+ mmol/L (3.5-5.3)
6.8
4
4.3
4.2
3.9
3.9
3.7
4.6
Urea mmol/L (2.5-7.8)
9.6
12.4
14
14.2
11.5
7.9
7.4
8.3
Creat mmol/L (48-128)
194
174
230
279
319
269
163
137
88
egfr mls/min/ 1.73 m2
27
30
22
18
15
19
33
40
66
INR ratio
1.4
1.4
1.5
1.6
1.4
1.1
1
PT secs (9.7-12.3)
14.8
15.1
15.9
16.7
15.1
11.5
10.6
Fibrinogen g/L (1.9-3.1)
1.2
1.4
1.2
1.5
2.4
3.9
>4.5
Discussion
The confidential enquiry report into maternal deaths – UK has shown a decreasing trend in the case fatality rate in women with ectopic pregnancies. This has been suggested to reflect earlier detection and immediate treatment of ectopic pregnancies. However unforeseen tubal rupture with major haemorrhage continues to be a source of major morbidity and mortality. Ectopic pregnancies account for 3-4% of pregnancy related deaths. 4
The classical triad of symptoms encountered in ectopic pregnancy includes pain, vaginal bleeding and amenorrhoea. 1 Worryingly, as illustrated by our case, rarely these women may present in a state of collapse even before the diagnosis of pregnancy is made. 4
Pathophysiology of multi-organ failure following haemorrhagic shock
Our case clearly demonstrates the detrimental multi-systemic effects and subsequent threat to life created by haemorrhage from a ruptured ectopic pregnancy. Acute haemorrhage results in decreased cardiac output and pulse pressure that is detected by baroreceptors in the aortic arch and atrium. Neural reflexes subsequently cause an increased sympathetic outflow to the heart and other vital organs resulting in vasoconstriction, and redistribution of blood flow away from non-vital organs. Neuroendocrine responses activated by neural reflexes play a major role in homeostasis during haemorrhage. Elevated aldosterone and cortisol secondary to raised adrenocorticotrophic hormone secreted by the pituitary gland leads to increased water absorption in the kidneys. The reduced tissue perfusion to non-vital organs results in insufficient delivery of oxygen and nutrients required for cellular function. 2
The resultant hypoxia leads to anaerobic metabolism and hence lactate production and metabolic acidosis. Hyperlactaemia is defined when serum lactate is greater than 4 mmol/l. 3 A level of 15mmol/l as demonstrated by our case highlights the extent of shock the patient was in.
Endogenous heat production is restricted by anaerobic metabolism, which in turns exacerbates hypothermia that is likely to be predisposed by the administration of intravenous fluids and blood products. Hypothermia is one of the reversible causes of pulseless electrical activity and a core temperature of less than 35°C is itself an independent predictor of mortality after major haemorrhage.
Furthermore, our case revealed a severe acidosis with a pH of 6.8, which is reflective of widespread cellular anaerobic respiration secondary to hypoxia as a result of inadequate perfusion. Widespread literature has shown that a pH of less than 7.2 is associated with decreased contractility, low cardiac output, bradycardia, arrhythmias and decreased blood flow to the liver and kidneys. This can lead to multi-organ failure.6
Many patients with severe haemorrhage can establish coagulopathy very quickly as our case has demonstrated. At present there is nouniversally established definition of coagulopathy though many experts use prolonged prothrombin time as an indicator of coagulopathy. Our case presented with a prolonged prothrombin time of 14.8 seconds. The pathophysiology is complex and stems from immediate activation of multiple haemostatic pathways including fibrinolysis, platelet and endothelium dysfunction. Furthermore, acute phase response after resuscitation measures can create a prothrombotic state. Sometimes, disseminated intravascular coagulation can occur in those who are insufficiently resuscitated or not resuscitated in a timely manner. 7
Effective multi-disciplinary input
This case clearly highlights that the responsibility does not solely rely on the surgeon who is required to cease the bleeding but also on the multi-disciplinary specialists including paramedics, emergency clinicians, nursing staff, anaesthetists and haematologists. This is a vital component of resuscitation management during emergency situations.
Appropriate initial fluid management
The management with intravenous fluid resuscitation remains challenging as some evidence suggests that aggressive fluid resuscitation can be detrimental because it can lead to dislodging of clots and dilutional coagulopathy leading to increased risk of haemorrhage. 5
Clinicians supporting this hypothesis suggest to cautiously administer fluid resuscitation with the aim of maintaining a subnormal blood pressure (systolic of 70-90 mmHg), whilst allowing sufficient oxygen delivery. The very early use of crystalloids and blood products is paramount to help treat acute coagulopathy. 7
Immediate surgical treatment
Recourse to immediate surgical cessation of bleeding is a vital part of the resuscitation process, and must not be delayed. 7 The presence of free fluid in the abdomen and a positive pregnancy test immediately alerted an ectopic pregnancy as the most likely diagnosis. The majority of women of reproductive age are free of comorbidities with a greater ability to adapt to resuscitative measures and hence showing quicker recovery.
Conclusion
Despite advances in the management of ectopic pregnancies an emphasis must be given on improving the understanding of the women and the healthcare professionals of the pathophysiology of haemorrhagic shock. Educating the public and all health care professionals about the phrase “Think Ectopic” as a main differential in any women of childbearing age with atypical signs and symptoms of general ill health is paramount.
Furthermore, the significance of effective communication within multidisciplinary teams towards optimising patient care and saving lives cannot be understated.
Increasing number of term deliveries undergo induction of labour (IOL). This figure is as high as 1 in 4 in developed countries, making it one of the most common procedures a woman may experience in pregnancy. 1 IOL may be achieved with pharmacological, mechanical or surgical methods. 1, 2 Mechanical methods were the first methods used to ripen the cervix and induce labour. The National Institute of Clinical Excellence (NICE) does not recommend the routine use of mechanical methods for IOL as only heterogeneous small studies were available at their time of publication more than half a decade ago. 2 However, since then there is increasing evidence of safety and efficacy of mechanical IOL. Subsequent publications including those from World Health Organization (WHO) and Cochrane Database of Systematic Reviews support the use of balloon catheter for IOL. 1, 3 It is therefore important to revisit the role of mechanical methods of IOL.
The Cochrane Database of Systematic Reviews concluded that mechanical methods of induction of labour have a lower risk of uterine hyperstimulation with similar caesarean section rates and delivery within 24 hours as prostaglandins. Furthermore, mechanical methods reduce the risk of caesarean section when compared with oxytocin induction of labour. 3 This review is consistent with another earlier systematic review. 4
Both Pfizer’s Prostin (PGE) and Cook Medical’s Cervical Ripening Balloon (CRB) are licensed for IOL. While the use of Prostin is a standard care in Singapore, the CRB has not been used routinely. We therefore propose a study to evaluate the use of CRB for IOL in Singapore.
Methods
A prospective cohort randomised controlled study was conducted in a tertiary referral maternity unit in Singapore. Pregnant women aged 21 – 40 years old with a singleton pregnancy with no major fetal anomaly who were suitable for vaginal delivery and scheduled for a planned IOL at 37+0 to 41+6 weeks gestation were invited for the study. Cases were excluded if at the start of the planned IOL, they were in spontaneous labour, had a cervical dilatation of ³3 cm, had confirmed rupture of membrane, had abnormal cardiotocogram (CTG), had a scarred uterus such as previous caesarean section, had malpresentation in labour, or if caesarean section delivery was indicated. Women who were unable to give or had withdrawn their consent to participate in the trial were also excluded for the study.
All suitable pregnant women receiving team care who require elective IOL were identified in antenatal clinic, antenatal or labour wards by the attending doctor or clinical research coordinator (CRC). Following routine counselling for IOL by the attending doctor, the woman will be offered participation in the study and a member of the research team will counsel and obtain informed consent from her. The woman will be made to understand that participation in the study is voluntary, does not affect her medical care and consent for participation can be withdrawn at any stage of the study. Women who were uncertain in their participation were offered the opportunity to participate during her follow-up or on the day of IOL after further consideration. Patient information leaflet on IOL as well as information of the study were made available to the participants.
On the day of the IOL, the participants were reviewed for the appropriateness of the IOL and participation in the study. A presentation scan, vaginal examination for cervical dilatation and CTG were performed. If they were suitable, they were randomly allocated PGE or CRB IOL in labour ward. Randomization was achieved with third party sealed envelope allocation. A total of 75 envelopes containing a folded paper with the words “Cervical Ripening Balloon” and another 75 identical envelopes containing a folded paper with the word “Prostin” were prepared and shuffled after sealing. These randomized envelopes were then labelled sequentially with their randomization allocation number from 1 to 150. The participants who underwent randomization were allocated to the next randomization allocation numbered envelop which contain either allocation for CRB or PGE IOL.
Participants undergoing CRB IOL will have the CRB inserted after cleaning the vulva and vagina with Cetrimide solution. The uterine and vaginal balloons of the CRB will be gradually inflated with normal saline, initially 40 ml and 20 ml respectively, and a further 20 ml each hour later until each balloon is 80 ml. CTG monitoring was undertaken before and after each inflation for at least 20 minutes. If the participant was not in labour after complete inflation of the balloons, she would be transferred to the antenatal wards for rest before removing the CRB 12 hours after insertion in labour ward when possible.
Participants undergoing PGE IOL will have 3 mg Prostin tablet inserted in the posterior fornix after cleaning the vulva with Cetrimide solution. CTG monitoring was also undertaken for at least 40 minutes after PGE insertion. If the participant was not in labour, she would be transferred to the antenatal wards. If there was no response to the first PGE, a repeat dose was given after 6 hours in labour ward when possible.
Participants will undergo artificial rupture of membrane (ARM) and/or oxytocin infusion augmentation of labour as necessary. If the participant was not in labour or ARM was not possible after removing the CRB or 2 cycles of PGE, the participant would have been considered having a failed IOL and will leave the study protocol with her subsequent management determined by the specialist attending to her. This would typically involve insertion of a third or first PGE in the PGE or CRB arm respectively.
Upon delivery of the pregnancy, a member of the research team will interview the participant and obtain demographics, labour and delivery outcomes data from the clinical notes. Pain and maternal satisfaction scores and comments were also recorded by interviewing the participants in the post-natal period; these findings will however be discussed separately.
The data was collected on a pro forma and entered into an excel spreadsheet. The data was then analysed using IBM SPSS Statistics version 19.
This study was approved by the SingHealth centralised institutional review board with the reference number of 2013/553/D.
Results
A total of 138 women were approached to join the study but 40 (29.0%) women declined. There was no significant difference in maternal age (27.8 ± 5.4 vs 28.7 ± 5.2 years; p = 0.373), ethnicity, proportion of primigravidae (62.5% vs 53.1%; p = 0.349), weight (61.2 ± 15.4 vs 64.4 ± 13.8 kg; p = 0.228), BMI (24.8 ± 5.8 vs 25.3 ± 5.0 kg/m2; p = 0.646) and primary indication for IOL between women who declined and accepted enrolment to the study respectively.
The remaining 98 women were enrolled for the study. Eight-seven women were randomized after excluding 6 women in spontaneous labour, 1 woman with non-cephalic fetal presentation, and 1 woman had confirmed ruptured of membrane on admission for their IOL, as well as 3 other cases in which the women presented for IOL without the availability of the research team (figure 1).
Figure 1. Flow diagram of recruitment, randomisation and completion status
In the CRB arm, one woman withdrew from the study after 8 hours 55 minutes as she felt the discomfort was too unbearable. Another woman was excluded when she was found to have spontaneous version to breech in labour. One woman randomized to PGE did not receive it as she went into spontaneous labour prior to IOL. Another woman in the PGE arm was subsequently found to be only 36+3 weeks and was therefore excluded from analysis (figure 1). The remaining 83 cases were analysed and their characteristics are shown in table 1.
The induction to vaginal delivery time, as well as, vaginal delivery rate were similar in both arms of the study (table 2). Compared to PGE arm, participants undergoing CRB IOL were faster in achieving cervical dilatation ≥4 cm (14.4 ± 5.7 vs 23.5 ± 16.6 hr; p = 0.001) and requesting epidural (16.4 ± 5.4 vs 23.2 ± 15.8 hr; p = 0.040), as well as more likely to require oxytocin infusion for augmentation (77.4% vs 50.0%; p = 0.020). Uterine hyperstimulation defined as >5 contractions every 10 minutes was only found in PGE arm. Cervical dilatation from 0 – 2 cm to ≥4 cm was achieved without regular contractions in 2 (6.9%) cases in the CRB arm and 1 (2.4%) case in the PGE arm. The mean frequency of uterine contractions at cervical dilatation ≥4 cm was 2.5 ± 1.4 in 10 minutes for CRB arm compared to 3.8 ± 1.4 in 10 minutes for PGE arm (p <0.001). No case of uterine rupture was observed.
There was 1 (3.2%) case for failed CRB IOL where both uterine and cervical balloons were found in the vagina suggesting that either placement of the uterine balloon was not optimal or it was expelled after placement. The woman went on to have Prostin and delivered vaginally. In the 9 (17.3%) cases in the PGE group that did not respond after 2 cycles, all went on to have the third Prostin successfully except for 2 women who required Caesarean section for persistent failed IOL.
The birth outcomes of both arms of the study were also similar with no case of stillbirth (table 3). There were 2 case of neonatal intensive care unit admission in the PGE arm for continuous positive airway pressure therapy; both were discharged from NICU within 24 hours.
Table 1. Characteristics of participants undergoing cervical ripening balloon (CRB) and Prostin (PGE) induction of labour.
CRB (n = 31)
PGE (n = 52)
p
Maternal age, years (83) 1
28.2
± 5.3
28.7
± 5.0
0.646
Ethnicity (83) 2
0.222
· Chinese
35.5%
(11)
42.3%
(22)
· Malay
54.8%
(17)
36.5%
(19)
· Indian
3.2%
(1)
15.4%
(8)
· Others
6.5%
(2)
5.8%
(3)
Primigravidae (83) 2
61.3%
(19)
44.2%
(23)
0.174
Weight, kg (83) 1
64.4
± 15.0
63.9.4
± 13.2
0.861
BMI, kg m-2 (83) 1
25.5
± 5.0
25.0
± 5.1
0.706
Pre delivery Hb, g dl-1 (80) 1
11.6
± 1.8
12.0
± 1.3
0.211
GBS positive (79) 2
22.6%
(7)
21.2%
(11)
0.204
Gestational age, weeks (83) 1
39.4
± 1.1
39.2
± 1.9
0.357
Cervical dilatation, cm (83) 1
1.0
± 0.7
0.9
± 0.7
0.954
Primary indication for IOL (83) 2
0.108
· Decreased fetal movement 3
-
11.5%
(6)
0.082
· Post dates 3
54.8%
(17)
32.7%
(17)
0.065
· Gestational diabetes 3
16.1%
(5)
13.5%
(7)
0.756
· Impending macrosomia 3
-
1.9%
(1)
0.526
· IUGR 3
3.2%
(1)
-
0.137
· Low amniotic fluid index 3
19.4%
(6)
34.6%
(18)
0.089
· Maternal request 3
3.2%
(1)
5.8%
(3)
0.489
· Pre-eclampsia 3
3.2%
(1)
-
0.373
1 Values are mean ± SD, p calculated with Student t-test; 2 Values are percentage (n), p calculated with Pearson chi-square test; 3 Values are percentage (n), p calculated with Fisher’s exact test.
Table 2. Labour outcomes of participants undergoing cervical ripening balloon (CRB) and Prostin (PGE) induction of labour.
CRB (n = 31)
PGE (n = 52)
p
IOL to ≥4 cm dilatation, hr (78) 1
14.4
± 5.7
23.5
± 16.6
0.001
IOL to full dilatation, hr (66) 1
20.8
± 6.1
24.8
± 15.7
0.150
IOL to vaginal delivery, hr (63) 1
21.2
± 6.8
25.6
± 16.1
0.136
Duration of 2nd stage, hr (63) 1
0.9
± 2.9
0.8
± 0.9
0.741
Delivery within 24 hr (83) 2
77.3%
(17)
61.0%
(25)
0.265
Failed IOL (83) 3
3.2%
(1)
17.3%
(9)
0.082
Number of PGE used (83) 2
<0.001
· 0
96.8%
(30)
-
· 1
3.2%
(1)
53.8%
(28)
· 2
-
28.8%
(15)
· 3
-
17.3%
(9)
Augmentation use (83) 3
77.4%
(24)
50.0%
(26)
0.020
Epidural use (83) 3
58.1%
(18)
55.8%
(29)
1.000
· IOL to epidural use, hr (47) 1
16.4
± 5.4
23.2
± 15.8
0.040
· Epidural use to delivery, hr (47) 1
9.2
± 4.1
7.0
± 3.8
0.065
Contractions 1
· At IOL (83)
0.2
± 0.6
0.2
± 0.5
0.579
· 3 hr after IOL (81)
2.0
± 1.9
1.6
± 1.9
0.451
Contractions >5 every 10 min 3
· 30 min after IOL (81)
-
-
-
· 3 hr after IOL (81)
-
2.0%
(1)
1.000
Vaginal delivery (83) 3
71.0%
(22)
78.8%
(41)
0.438
Indication for LSCS (20) 2
0.513
· Failed IOL
-
18.2%
(2)
· FTP in 1st stage of labour
55.6%
(5)
36.4%
(4)
· FTP in 2nd stage of labour
22.2%
(2)
9.1%
(1)
· NRFS
11.1%
(1)
27.3%
(3)
· FTP and NRFS
11.1%
(1)
9.1%
(1)
1 Values are mean ± SD, p calculated with Student t-test; 2 Values are percentage (n), p calculated with Pearson chi-square test; 3 Values are percentage (n), p calculated with Fisher exact test.
Table 3. Birth outcomes of participants undergoing cervical ripening balloon (CRB) and Prostin (PGE) induction of labour.
CRB (n = 31)
PGE2 (n = 52)
p
Male fetus (83) 2
51.6%
(16)
42.3%
(22)
0.496
Birth weight, g (83) 1
3,166
± 478
3,094
± 417
0.472
Apgar at 5 min <7 (83)
-
-
-
Meconium aspiration (83)
-
-
-
Pyrexia in labour (83) 3
6.5%
(2)
5.8%
(3)
1.000
NICU admission (83) 2
-
3.8%
(2)
0.526
ITU admission (83)
-
-
-
1 Values are mean ± SD, p calculated with Student t-test; 2 Values are percentage (n), p calculated with Pearson chi-square test; 3 Values are percentage (n), p calculated with Fisher exact test.
Discussion
To the best of our knowledge, this is the first randomized controlled study to assess the use of CRB for IOL in Singapore. Our study concur with the published literature that both CRB and PGE have similar rate of vaginal deliveries and rate of deliveries within 24 hours. Both methods are effective and safe with PGE having a higher risk of uterine hyperstimulation and need for Caesarean section for failed IOL.
Pharmacological induction of labour using PGE is the most established form of IOL. However, it is important to be able to offer alternative methods to women particularly in cases of hypersensitivity or allergy to PGE. PGE can cause bronchospasm complicating asthma, a medical condition which affects 4 – 12% of pregnant women. 5, 6 Similarly, caution should be exercised in the use of PGE in women with other common medical conditions such as hypertension and epilepsy.
In addition, women may not respond to PGE for IOL, or the PGE may only result in uterine tightenings which do not lead to cervical dilatation. In these situations the CRB may be considered as an adjunct for IOL to avoid Caesarean section of ‘failed IOL’.
The risk of uterine hyperstimulation and the need for a repeat dose in 6 to 8 hours for PGE typically require the women to be admitted for IOL. The use of CRB does not require planned intervention until 12 hours later. This potentially allows an outpatient IOL if further studies support its safety in this aspect.
The application of PGE is relatively straightforward and is already performed by both doctors and midwives. The insertion of CRB may however be considered too invasive for midwives thus limiting the type and hence availability of staff to commence IOL. We have explored the learning curve in the insertion of CRB and will discuss this separately.
Conclusion
Both CRB and PGE are effective methods for IOL at term. Each method has its own benefits and limitations. The availability of both methods in an obstetric unit will allow the clinician to choose the most appropriate form of IOL, provide a complementary method of IOL, as well as offer women choice in their IOL.
A 36 year old multiparous woman presented to the Labour Ward at 33 weeks’ gestation with lower abdominal pain. She had mild asthma and her obstetric history included 2 previous normal vaginal deliveries.
At 16 weeks’ gestation she was found during antenatal scanning to have a right ovarian cystic lesion measuring 59x34x50mm. This was monitored and a repeat scan at 25 weeks’ showed it had increased in size to 73x55x47mm.
At 32 weeks’ she was diagnosed with a DVT and was commenced on therapeutic enoxaparin (stopped two days before current presentation). (D-Dimer > 4000micrograms/L). An inferior vena cava filter was inserted. The patient declined any surgical intervention of the cystic lesion during pregnancy and an early elective Caesarean Section with surgical management of the cyst at 34 weeks’ gestation was planned. She had no symptoms or signs suggestive of a PE and was not formally investigated for one prior her current presentation.
On this presentation at 33 weeks’ gestation, her pain suddenly worsened with associated hypotension and evidence of foetal distress and so an emergency exploratory laparotomy was performed.
Admission haematology results: haemoglobin 10g/dL, platelets 158 x 109 /L, INR 1.0, APTT 28.4 seconds, APTT ratio 1, fibrinogen 3g/L.
She underwent a rapid sequence induction in the supine wedged position using thiopentone and suxamethonium. She was a Grade 1 intubation and anaesthesia was maintained with oxygen/nitrous oxide/sevoflurane and muscle relaxation was achieved with atracurium. A ruptured, torted right ovarian mass containing an estimated one litre of altered blood was noted. At Caesarean section a live male infant was delivered. A right oophrectomy was then performed. The infant was subsequently intubated and transferred to the Neonatal Intensive Care Unit.
Oxytocin 5IU followed by a 40IU infusion over 4 hours was administered following delivery of the baby. Effective haemostats was achieved, the uterus appeared well-contracted and the patient’s abdomen was closed. Surgical blood loss was estimated as 600mls (excluding blood within the ovarian mass).
Thirty minutes following completion of surgery the patient, fresh blood was noted vaginally. A HemoCue* reading was taken as 5.9g/dL. Four units of blood and two units of FFP were transfused whilst a second laparotomy was performed. Fresh blood was noted intra-abdominally and the uterus was markedly atonic. Ergometrine 500mcg and carboprost trimethamine 250mcg were administered intramuscularly, as well as, misoprostol 800mg vaginally. A hysterectomy was performed due to the rate of bleeding and the evident haemodynamic instability.
Coagulation studies: platelets 27 x 109/L, INR 1.4, APTT 101.8 seconds, APTT ratio 3.6 and fibrinogen 1g/L.
A further 4 units of blood, 4 units of FFP, 1 pool of platelets and 2 units of cryoprecipitate were transfused. Factor VII was also administered on advice from the Haematologist.
An internal jugular central venous catheter was inserted and a noradrenaline infusion started. Initial attempts to insert an arterial cannula were unsuccessful as peripheral pulses were difficult to palpate. Venous blood gas readings revealed hyperkalaemia (K+ 6.4mmol/L) which was treated with sodium bicarbonate, 10mls 10% calcium chloride and a continuous 50% dextrose and insulin infusion. Her abdomen was packed and percutaneous drains were inserted. Anaesthesia, close monitoring and resuscitation continued.
Ongoing output from drains prompted a third exploration after an hour. There was generalised oozing particularly around the bed of the resected ovary in the pouch of Douglas.
Coagulation profile: platelets 50 x 109/L, INR 1.4, APTT 89.6 seconds, APTT ratio 3.1 seconds, fibrinogen 1.4g/dL.
A further 10 units of blood, 3 pools of platelets, 5 units of FFP and 3 units of cryoprecipitate were transfused. Sequential coagulation profiles and thromboelastography were used to guide transfusion.
During this exploration, ECG revealed a broad complex tachycardia with no palpable pulse confirming cardiac arrest likely secondary to hypovolaemia and/or hyperkalaemia. Return of spontaneous circulation was achieved after 3 cycles of continuous cardiac massage, 4 direct current shocks and adrenaline 1mg.
A femoral artery cut-down was performed and arterial cannula was inserted by a general surgeon. IABP monitoring commenced.
A fourth exploration was carried out around two hours later for ongoing blood loss. Again only generalised oozing was noted particularly from the oophrectomy site. Her abdomen was re-packed.
Coagulation profile: haemoglobin 7.4g/dL, INR 1.2, APTT 48.9 seconds, APTT ratio 1.7, fibrinogen 1.9g/dL, platelets 94 x 109/L.
She was transferred to the ICU eight hours from the start of the primary operation. Estimated total blood loss was 13,200mls. Transfusions continued and her abdomen was closed two days later. She received haemofiltration therapy for acute kidney injury. She recovered to her premorbid level with no neurological deficit before being discharged with her baby a few weeks later. In total, she was transfused 64 units of blood, 35 units of FFP, 10 pools of platelets and 11 units of cryoprecipitate. Histology of the ovarian mass revealed high grade clear cell carcinoma for which she received chemotherapy but unfortunately she died two years later.
Discussion
The association between cancer and thromboembolism has been well established for many decades.1Ovarian cancer patients have one of the highest incidences of VTE amongst cancer patients, particularly clear cell carcinoma (CCC). One study found the incidence of thromboembolic complications to be significantly higher in CCC when compared with other epithelial types of ovarian cancer (27.3% vs 6.8%).2
The pathological mechanism behind the hypercoaguable state induced in ovarian cancer patients appears to be largely multi-faceted. A variety of procoagulant subtances may be involved. Of particular interest is tissue factor (TF), a potent procoagulant found in endothelial and blood cells, as well as, in tumour cells. TF may play an important role in this hypercoaguable state through activation of the coagulation cascade.3 TF is frequently over-expressed in ovarian cancer tissue and there is research suggesting it influences tumour progression.3,4
A hyperviscosity syndrome may also be seen in association with ovarian cancer which favours thrombosis and may accelerate tumour progression and metastasis.DVT is a recognised complicating factor of ovarian cancer which may adversely affect the course of the disease possibly as a component of this hyperviscosity syndrome5,6 Ovarian cancer patients are also vulnerable to developing cerebrovascular complications and carry a higher risk of developing ischaemic strokes which has a significant impact on morbidity and mortality.7
The hypercoagulable state seen in cancer patients can have a spectrum of manifestations that ranges from DIC to massive thromboembolism. DIC in these instances is usually chronic and subclinical.8
The degree of coagulopathy which was seen in this case could not be attributed solely to dilutional effects incurred through fluid resuscitation. Instead we propose the acute severe coagulopathy was a consequence of procoagulant factors inherent to neoplastic tissue, including TF, which were suddenly released into the circulation following rupture and surgery to the ovarian tumour. The overall result would be widespread activation of the clotting cascade and a consumptive coagulopathy.
This case aims to increase awareness of a refractory coagulopathy which may be seen following rupture and/or surgical resection of a malignant ovarian tumour. The presence of an ovarian cyst especially in conjunction with evidence of vascular thrombosis in pregnancy should raise suspicion for an ovarian malignancy and hence vigilance for this potential complication. Anticipation of such a severe coagulopathy and associated significant blood loss should pre-empt early establishment of invasive monitoring, ample intravenous access and ensuring quick access to blood and blood products. Bedside coagulation tests such as thromboelastography are useful guides to blood product transfusion.9 Prompt mobilisation of resources, multi-disciplinary input and effective team work were crucial factors which facilitated the management of this case.
Acute, severe DIC associated with ovarian intratumoural bleed which resolves following resection of the tumour has been reported previously.10 This is the first case to the best of our knowledge occurring following ovarian cancer torsion and rupture during pregnancy.
The use of dietary supplements has grown rapidly over the past several decades, and are now used by more than half of the adult population in the United States (US).1 In 1994, the Dietary Supplements Health and Education Act (DSHEA) significantly changed the Food and Drug Administration’s (FDA) role in regulating supplement labelling. According to the DSHEA dietary supplements may contain products taken by mouth including vitamins, minerals, herbs or other botanicals, amino acids, other dietary substances, or combinations or extracts of any of these ‘dietary ingredients.’ The DSHEA reaffirmed that dietary supplements are to be regulated as foods and not as drugs. Annual sales of supplements to Americans are now reported at about $23 billion, a substantial share of which is spent on vitamins and minerals.
The purpose of this review is to present the discussion from available research to internists and other clinicians to help guide their decisions behind the efficacy and safety of dietary supplement use in primary prevention of chronic disease in the general non-pregnant adult population.
Profile of a dietary supplement user
In general dietary supplements are used by individuals who practise healthier lifestyles. Its use is higher among women and the children of women who use supplements; in elderly persons; among people with more education, higher income, healthier diets, and lower body mass indices; and among residents of the western US.2 Individuals with chronic illnesses, or those who are seeking to prevent recurrence of a serious disease (for example, cancer) also tend to be more frequent supplement users.3 Many dietary supplement users perceive their health as better.
Why use dietary supplements?
The growth in supplement use has accelerated rapidly with marketing spurred by claims that chronic conditions could be prevented or treated by supplement use. The commonly used over-the-counter multivitamin and mineral supplements contain at least 10 vitamins and 10 minerals. On a daily basis consumers receive advertising and promotional material of unproven claims made about dietary supplements or other products and the medical wonders they can achieve. Some of the promotional material makes a consumer feel guilty if he or she is not using one. Many users feel so strongly about the potential health benefits of some of these products that they reported that they would continue to take them even if they were shown to be ineffective in scientifically conducted clinical studies.4 More than half of American adults take dietary supplements in the belief that they will make them feel better, give them greater energy, improve their health, and prevent and treat disease.
Is there clinical evidence for use of dietary supplements?
Most studies do not provide strong evidence for beneficial health-related effects of supplements taken singly, in pairs, or in combinations of 3 or more.5 In some studies, or subgroups of the study populations, there is encouraging evidence of health benefits such as increased bone mineral density and decreased fractures in postmenopausal women who use calcium and vitamin D supplements.
Huang et al 5 performed a systematic review to synthesize the published literature on the efficacy of multivitamin and mineral supplements and certain commonly used single vitamin or mineral supplements in the primary prevention of cancer and chronic disease in the general adult population. The authors concluded that the strength of evidence for the efficacy of multivitamin/mineral supplementation in the general adult US population was very low for primary prevention of cancer, cardiovascular disease, and hypertension; and low for cataract and age-related macular degeneration.
The National Institutes of Health (NIH) consensus panel statement2 on ‘multivitamin/mineral supplements and chronic disease prevention’ did not find any strong evidence for beneficial health-related effects of supplements taken singly, in pairs, or in combinations of 3 or more. The panel concluded that the present evidence is insufficient to recommend either for or against the use of dietary supplements by the American public to prevent chronic disease. It also concluded that the current level of public assurance of the safety and quality of dietary supplements is inadequate, given the fact that manufacturers of these products are not required to report adverse events and the FDA has no regulatory authority to require labeling changes or to help inform the public of these issues and concerns.
A recent study published in Archives of Internal Medicine6 raised some disturbing concerns. In this large prospective study, 38,772 older women in the Iowa Women's Health Study were followed up for a mean time of 19.0 years. The authors found that most of the supplements studied were not associated with a reduced total mortality rate in older women. In contrast, they found that several commonly used dietary vitamin and mineral supplements, including multivitamins, vitamins B6, and folic acid, as well as the minerals iron, magnesium, zinc, and copper, were associated with a higher risk of total mortality. Of particular concern, supplemental iron was strongly and dose dependently associated with increased total mortality risk. The association was consistent across shorter intervals, strengthened with multiple use reports and with increasing age at reported use. Supplemental calcium was consistently inversely related to total mortality rate; however, no clear dose-response relationship was observed. The strengths of this study include the large sample size and longitudinal design. In addition, the use of dietary supplements was queried three times: at baseline in 1986, in 1997, and in 2004. The use of repeated measures enabled evaluation of the consistency of the findings and decreased the risk that the exposure was misclassified.
Summary
The use of dietary supplements has grown rapidly over the past several decades even though clinical deficiency of vitamins or minerals, other than iron, is now uncommon in the US.2 Fortification of foods has led to the remediation of vitamin and mineral deficits. The cumulative effects of supplementation and fortification have also raised safety concerns about exceeding upper levels besides interactions of dietary supplements with the prescriptions drugs taken by a consumer. There is no evidence-based data about what the optimal compositions and dose of a multivitamin and mineral supplement should be. Though dietary supplements are perceived to be safe, that should not be sufficient reason for using them without a valid medical need. Providers should take into consideration their efficacy and cost-effectiveness. There are also no outcomes data or data about quality adjusted life years gained by using dietary supplements taken singly, in pairs, or in combinations. The current data available on the efficacy and safety of dietary supplements is conflicting. Clinicians considering the use of dietary supplements should be aware of their risks, consider the likelihood of the adverse effects, interaction with prescription medications, safety, efficacy, costs, and possibility of unintended effectsof dietary supplements.
Conclusion
The conclusion from the available data (new and old) is that consumption of dietary supplements for prolonged periods appears not to be safe and is not cost-effective in primary prevention of chronic disease in the general non-pregnant adult US population. Practitioners should evaluate each case individually and take a decision based on available evidence-based data when considering dietary supplements in this population. Given the potential for widespread use of dietary supplements, there is a need for robust study methods in the future.
Pre-eclampsia is a multisystem disorder of pregnancy that forms an integral part of the spectrum known as hypertensive diseases of pregnancy. The National High Blood Pressure Education Program (NHBPEP) Working Group1classifies hypertensive diseases in pregnancy into 4 groups:
1) Gestational hypertension
· New onset hypertension in pregnancy presenting after 20 weeks
· No proteinuria
· BP returns to normal less than 12 weeks postpartum
· Final diagnosis made only postpartum
2) Chronic hypertension
· BP >140/90 mm Hg before pregnancy or diagnosed before 20 weeks gestation not attributable to gestational trophoblastic disease or
· Hypertension first diagnosed after 20 weeks gestation but persistent after 12 weeks postpartum.
3) Pre-eclampsia/eclampsia
· BP > 140/90 mm Hg after 20 weeks gestation in a women with previously normal blood pressure
· Proteinuria (>0.3 gm urine protein in 24 hr).
· Eclampsia is defined as seizures that cannot be attributed to other causes in a woman with pre-eclampsia
4) Superimposed pre-eclampsia (on chronic hypertension)
· New onset proteinuria (>300 mg/24 hr) in a woman with hypertension but no proteinuria before 20 weeks gestation
· A sudden increase in proteinuria or blood pressure, or platelet count less than 100,000 in women with hypertension and proteinuria before 20 weeks gestation
Epidemiology
Pregnancy induced hypertension complicates about 10% of pregnancies, but there is a widespread geographic variation in its incidence.The incidence is higher in developing countries. The highest reported rate of pre-eclampsia is 7.1% (deliveries) from Zimbabwe2, while the incidence is as low as 0.81% (deliveries) in Colombia3. In UK, the incidence of severe pre-eclampsia is 5/1000 maternities4, while the incidence of eclampsia is 4.9/10,000 maternities5. The incidence of severe pre-eclampsia in European countries ranges from 2/1000 (deliveries) in Norway to 6.4/1000 (deliveries) in Belgium and Hungary6.
The 8th Confidential Enquiry into maternal and child heath7 revealed pre-eclampsia and eclampsia as the second leading cause of direct maternal death, thereby contributing to a maternal death rate of 0.83 / 100,000 maternities.
Worldwide studies show that mortality from pre-eclampsia can be as high as 0.4%, while that in eclampsia varies from 6.1% in developing countries to 1.8% in UK 5, 8-9.
Estimates of maternal mortality from the developing countries (in Asia, Africa, Latin America and the Caribbean) suggest that 10-15% of maternal deaths are associated with hypertension in pregnancy, while eclampsia is associated with 10% maternal mortality10.
Severe pre-eclampsia is also associated with significant maternal morbidity, including eclamptic seizures, intracerebral haemorrhage, pulmonary oedema due to capillary leak or heart failure, acute renal failure, liver dysfunction, and coagulation abnormalities.
Fetal complications include abruptio placentae, intrauterine growth restriction, premature delivery, and intrauterine fetal death. The incidence of stillbirths and neonatal deaths in mothers who suffered eclampsia was 22.2/1000 and 34.1/1000, respectively, in the UK with a higher incidence in developing countries5.
More than half a million women die each year from pregnancy related causes across the globe. The Millennium Development Goals have placed maternal health as a basic human right, one that is integral to the core of the fight against poverty and inequality. The high incidence of pre-eclampsia and its complications makes its prevention and effective management important. The following article attempts to outline the pathophysiology and management of pre-eclampsia.
Aetiology & Risk factors
Pre-eclampsia is commonly referred as the “disease of theories” making its prevention and management an ongoing challenge worldwide. Although the aetiology is still largely unknown, there are a few hypotheses regarding the pathophysiology and prediction of pre-eclampsia.
It has been postulated that pre-eclampsia may be autoimmune in nature. Seminal-vesicle-derived transforming growth factor 1 (TGF-1) initiates a post mating inflammatory reaction, which is a type 2 immune response towards paternal antigens resulting in maternal-fetal (paternal) immune maladaptation11. This idea originates from epidemiological studies demonstrating the protective effect of long-term sperm exposure and is supported by the fact that frequency of pre-eclampsia is higher in nulliparous women or multiparous women with a new partner, teenagers, women who conceive after donor insemination or oocyte donation, and women with autoimmune conditions.
Another potential mechanism responsible for pathogenesis of pre-eclampsia is placental hypoperfusion which in turn releases various factors that trigger endothelial activation / dysfunction. Nitric oxide, disordered endothelin metabolism, thromboxane/prostaglandin imbalance, cellular fibronectin, inflammatory cytokines (TNF-α, IL-6, IL-1α, and IL-1β) and otherfactors such as lipid peroxides and reactive oxygen intermediateshave all been implicated in mediating the endothelial cell injury12. This is well-supported by the fact that pre-eclampsia commonly occurs in pre-existing metabolic (diabetes, hypercholesterolemia), renal, vascular disorders (hypertension) and connective tissue disorders that result in poor placental circulation. In cases of multiple gestation or increased placental mass, it is not surprising for the placenta to become underperfused.
However, majority of the pre-eclamptic women do not suffer from any underlying medical conditions. In these women, lack of placental cytotrophoblastic invasion of uterine spiral arterioles and arrest of arteriolar remodelling results from failure of pseudo-vascularisation of the invasive cytotrophoblasts13. Deregulation of angiogenesis-related gene products such as vascular endothelial growth factor (VEGF), angiopoietin and ephrin family proteins, placental growth factor (PlGF) and their receptors have been implicated in this process14.Shallow placentation leads to reduced placental perfusion and subsequent ischaemia.
Obese (BMI ≥30 Kg/m2) women are at higher risk for pre-eclampsia compared to lean women (odds ratio = 3.3). The exact mechanism is not completely understood but possible explanations are: increased stress due to the hyperdynamic circulation associated with obesity; dyslipidaemia or increased cytokine-mediated oxidative stress; and direct haemodynamic effects of hyperinsulinaemia15 (increased sympathetic activity and increased tubular sodium resorption).
On the other hand, smoking actually decreases a woman’s risk of pre-eclampsia. Inhibition of thromboxane A2production by nicotine might explain the decreased risk. However, the adverse effects of smoking on pregnancy significantly outweigh any beneficial effects16.
Epidemiological and clinical risk factors for pre-eclampsia are classified as maternal, paternal, and/or pregnancy-specific2, 17 (Table 1, below).
Table 1: Pre-eclampsia Risk Factors
Maternal Considerations
Inherent
Ø Age < 20 or 35–40 years
Ø Nulliparity
Ø Afro-Caribbean origin
Ø Prior or family history of PE or cardiovascular disease
Ø Woman born small for gestational age
Medical conditions
Ø Obesity
Ø Chronic hypertension
Ø Chronic renal disease
Ø Diabetes mellitus (insulin resistance, type 1, and gestational)
Ø Antiphospholipid antibody syndrome
Ø Connective tissue diseases
Ø Thrombophilia
Ø Stress
Pregnancy specific
Ø Multiple gestation
Ø Oocyte donation
Ø New partner
Ø Urinary tract infection
Ø Congenital conditions affecting the fetus
Ø Hydatidiform mole
Ø Hydrops fetalis
Ø Structural anomalies
Paternal Considerations
Ø Limited sperm exposure
Ø Barrier contraception
Ø First-time father
Ø Donor insemination
Ø Partner who fathered a pre-eclamptic pregnancy in another woman
What exactly happens in Pre-eclampsia?
The triad of physiological derangements in pre-eclampsia include 1. Vasospasm 2. Plasma volume contraction 3. Local or disseminated intravascular coagulation.
Although the cause of pre-eclampsia is unknown, we have already discussed that the placenta is largely implicated. The sequence of events starts with vasospasm caused by increased production or sensitivity to vasoconstrictors (angiotensin II, serotonin and endothelin) and/or decreased production or sensitivity to vasodilators (prostacyclin and nitric oxide). This is followed by plasma volume contraction, increased capillary permeability and, in severe cases, low plasma oncotic pressures. Redistribution of fluid occurs from the intravascular to interstitial fluid spaces causing peripheral tissue oedema. Along with this, intravascular coagulation may occur due to platelet activation, thrombocytopenia and, often, reduced production of anti-thrombin III.
The net effect is organ hypoperfusion. Commonly affected systems are kidney (manifested by reduced GFR, proteinuria, hyperuricaemia and occasionally oliguria), liver (manifested by elevated transaminases with or without epigastric and right upper quadrant pain), and the brain (manifested by headaches, transient visual disturbances due to occipital lobe ischaemia and rarely convulsions, i.e. eclampsia). This leads to increased maternal morbidity.
Placental insufficiency resulting from uterine hypoperfusion is characterised by intrauterine fetal growth retardation and less commonly placental abruption or fetal death. Preterm delivery, low birth weight, respiratory distress syndrome, and admission to the neonatal intensive care lead to increased perinatal morbidity.
In spite of major advances in understanding the pathophysiology of the disease in recent years, interventions to prevent hypertensive disorders in pregnancy have had disappointing results, hence early detection, continued surveillance and timely intervention still remains the key towards decreasing the inherent maternal and fetal morbidity and mortality associated with severe pre-eclampsia and eclampsia.
Prevention of pre-eclampsia
Till date there is no well-established measure for prevention of pre-eclampsia in the general population. Calcium is clearly of benefit amongst high risk women in communities where low dietary calcium intake is prevalent. A Cochrane systematic review in 2010 concludes that calcium supplementation approximately halves the risk of pre-eclampsia, reduces the risk of preterm birth and the rare occurrence of the composite outcome 'death or serious morbidity18.
Low dose aspirin (antiplatelet agent) therapyefficiently reduces the development of pre-eclampsia in women with abnormal uterine artery Doppler studies. If started in early gestation (< 16 weeks), it also causes a significant reduction in the incidence of severe pre-eclampsia, gestational hypertension and IUGR19.
Some studies have suggested that prophylactic use of antioxidants (vitamin C, E) may be beneficial as well but this is not routinely recommended20 in practice.
Evidence is also lacking to support lifestyle preventative interventions for pre-eclampsia, such as rest, exercise and reduced dietary salt intake.
The pre-eclampsia community guideline (PRECOG)
This has been developed for screening and detection of onset of pre-eclampsia in the community21. It includes:
Initial risk assessment at community booking using pre-determined criteria, to identify factors that predispose women to pre-eclampsia in a given pregnancy. Following this, women are offered referral before 20 weeks gestation for specialist input to their antenatal care plan if they have been identified as high risk: this may be for clarification of risk, necessary investigations, advice on early intervention or pharmacological treatment.
Systematic community assessment for onset of pre-eclampsia from 20 weeks gestation. The frequency of assessment is determined by the likelihood of developing pre-eclampsia. Women with no risk factors for pre-eclampsia are offered assessments at weeks 16, 28, 34, 36, 38, 40, and 41 weeks.Women with one risk factor for developing pre-eclampsia (excluding previous pre-eclampsia, multiple pregnancy and underlying medical conditions like hypertension, renal disease, diabetes, antiphospholipid syndrome) are reviewed in the community at least once every three weeks before 32 weeks, and then at least once every two weeks, until delivery. At every visit, recommendation is to look for presence of any signs or symptoms like new hypertension, new proteinuria, headache/visual disturbance, or both, epigastric pain/vomiting, or both, reduced fetal movements, small for gestational age infant. In the presence of two such, they are referred for early specialist input, individual assessment, and discussion of obstetric risk.
Recommendations have been made within the scope of this guideline for improving accuracy inblood pressure measurement, increasing reliability of proteinuria test with dipstick and community assessment of fetal growth and well being which provide the parameters for referral. Referral is made forstep-up assessment in hospital day unit within 24/48 hoursor admission in accordance with set criteria. All pregnant women are also made aware that pre-eclampsia may develop between antenatal assessments, and they could self-refer at any time.
It is recognised that all women benefit from a continuity of care in the community and need midwifery or GP care as part of their individual antenatal care plan, whatever be their obstetric risk.
Management of Pre-eclampsia
Antenatal Care
These patients should be under consultant led care with multidisciplinary input from the anaesthetic and neonatal teams as necessary.
Women with risk factors for developing pre-eclampsia may be considered for uterine artery doppler velocimetry at 20-24 weeks to look for increased impedance to flow (resistance index >95th centile or early diastolic notch), which is predictive of developing pre-eclampsia or IUGR in late gestation, however the specificity and sensitivity varies widely between different studies22-25.
At diagnosis of pre-eclampsia, the best practice is to offer initial hospital admission for assessment and formulation of follow-up care. Assessment of proteinuria should be done by automated reagent strip reading device. Visual assessment of the dipstick is not recommended nowadays because of high error rates26-28. If the automated reagent strip reading of urine yields a result of 1+ or more, this should be followed up with a spot urinary protein:creatinine ratio or a 24 hour urine collection to quantify the proteinuria. Significant proteinuria is diagnosed if the urinary protein:creatinine ratio is more than 30mg/mmol or the validated 24 hr urine sample has more than 300 mg of protein. Baseline blood investigations should include full blood count, liver function (bilirubin and transaminases), electrolytes and kidney function tests. Antihypertensive medications may need to be commenced with the aim of maintaining the systolic blood pressure below 150 mm Hg, and the diastolic pressure between 80 - 100 mm Hg. Labetalol is the first line treatment. However, in patients in whom labetalol cannot be used (e.g. in patients with bronchial asthma), alternatives include nifedipine (contraindicated before 20 weeks of gestation), methyldopa, atenolol and metoprolol. 4-6 hourly blood pressure, daily assessment of proteinuria, along with haematological and biochemical monitoring are also carried out. Inpatient management is required till the blood pressure stabilises.
Following discharge blood pressure can be checked in the community or in antenatal day assessment 2-3 times a week depending on clinical circumstances. Quantification of urinary protein is not necessary after the initial assessment, however, blood tests for full blood count, liver and kidney functions need to be repeated at least twice weekly (thrice weekly if the hypertension is moderate or severe). There is often a rise in serum uric acid level, which has been associated with poor maternal and fetal outcome29, 30. However, there is no evidence to use serum uric acid levels for clinical management.
Fetal monitoring:
Ultrasound assessment of fetal growth and amniotic fluid volume along with umbilical artery doppler velocimetry needs to be done at initial diagnosis of pre-eclampsia to exclude IUGR and then every 2 weeks if the pregnancy is managed conservatively and the results remain normal CTG monitoring is commonly done at diagnosis, along with the ultrasound assessment. If normal, further CTG should be performed weekly unless otherwise clinically indicated.
Delivery
In pre-eclampsia with mild or moderate hypertension, women may be delivered between 34 and 37 weeks of gestation, depending on maternal and fetal condition, presence of risk factors and availability of neonatal intensive care facilities. If severe pre-eclampsia develops, refractory to treatment or fetal wellbeing delivery may need to be done earlier.
Pre-eclampsia is considered to be severe in case of
1) Severe hypertension with proteinuria or
2) Mild / moderate hypertension and proteinuria with one or more of the following signs / symptoms:
Ø Severe headache , not responding to medications
Ø Visual disturbance (blurring or flashing of light)
Ø Severe pain in upper abdomen or vomiting
Ø Papillo-oedema
Ø Signs of clonus (³ 3 beats)
Ø Liver tenderness
Ø HELLP syndrome
Ø Decrease in platelet count to less than 100 x 109 per litre
Ø Abnormal liver enzymes (ALT or ASTrising to above 70 iu/litre).
HELLP syndrome
HELLP Syndrome (haemolysis, elevated liver enzyme, low platelets) is a form of severe pre-eclampsia that is associated with high maternal and perinatal morbidity and mortality and may be present without hypertension or, in some occasions, without proteinuria.
A diagnosis of HELLP syndrome is made after confirmation of haemolysis, either by blood film microscopy showing fragmented red cells or increased serum LDH level. An AST or ALT level of above 70 iu/l is significant while a level more than 150 iu/l is associated with increased morbidity to the mother, though neither of them are independent risk factors for increased maternal morbidity 31. A low platelet count (less than 100 x 10 6 /ml) supports the diagnosis.
There is some evidence to suggest that the severity of pre-eclampsia differs according to the time of onset. More severe form occurs with the onset of pre-eclampsia prior to 34 weeks of gestation. This form is associated with abnormal uterine artery blood flow, IUGR and adverse maternal and fetal outcomes32-33.
There may be some difference in the pathophysiology of these two disease types. The early onset disease may be associated with placental abnormalities, while the late onset one is more linked to maternal constitutional factors such as increased BMI34.
In severe pre-eclampsia, delivery is appropriate anytime beyond 34 weeks of gestation following corticosteroid administration to achieve fetal lung maturity. Delivery before 34 weeks is only indicated in maternal/fetal compromise or hypertension refractory to treatment35-37. Prolonging pregnancy at early gestation may improve the perinatal outcome but has to be carefully balanced against maternal wellbeing. If conservative management is planned, ultrasound assessment of fetal growth, amniotic fluid volume and umbilical artery doppler flow should be done at admission, and thereafter, every two weeks. In case of normal ultrasound findings, weekly CTG monitoring should suffice, unless clinically indicated otherwise (for e.g. reduced fetal movement, vaginal loss, abdominal pain or deterioration of maternal condition).
Eclampsia
Generalised tonic-clonic seizures, with or without raised blood pressure and proteinuria, occurring during or after pregnancy with no other identifiable cause is classified as eclampsia. The cause is usually multi-factorial including cerebral vasoconstriction, ischaemia, vasogenic oedema, or other pathology. Although it is more likely to occur in women with severe rather than mild pre-eclampsia, there is no convincing test for predicting the onset of eclampsia. Convulsions may occur antepartum (38-53%), intrapartum (18-36%), or postpartum (11-44%)38. Women with a history of previous eclampsia are at increased risk of eclampsia (1-2%) and pre-eclampsia (22-35%) in subsequent pregnancies39.
Intrapartum Care
During labour, hourly blood pressure monitoring in women with mild or moderate hypertension, and continuously in severe hypertension is ideal. Antenatal hypertensive treatment should be continued, with the aim of maintaining the systolic blood pressure below 150 mm Hg, and the diastolic pressure between 80-100 mmHg. If oral medications fail to control the blood pressure, then intravenous anti-hypertensives are indicated to prevent the known risk of vascular damage due to uncontrolled hypertension.
Hydralazine, a peripheral arteriolar vasodilator, has been widely used as the first-line treatment for acute hypertension in pregnancy, in the past.It is administered as bolus doses (5-10 mg) intravenously, every 20 minutes to a maximum dose of 30 mg, with careful monitoring of blood pressure. The side effects include headache, nausea, and vomiting. Importantly, hydralazine may result in maternal hypotension, which may subsequently cause fetal distress. Preloading with 500 ml of crystalloid fluid before or with the first dose of intravenous hydralazine may avoid this40. Labetalol is another antihypertensive that can be given intravenously, either as bolus doses or as an infusion to manage severe hypertension. It is commonly used as the first line drug in many centers in UK. However, it is not suitable for patients with bronchial asthma. Nifedipine may also be used orally to control blood pressure (sublingual administration is not recommended).However, it can interact with magnesium sulphate to produce profound muscle weakness, maternal hypotension and fetal distress41-43. Recent evidence suggests labetalol and nifedipine as better alternatives than hydralazine40. In all cases, the blood pressure should be monitored closely, along with fetal monitoring, as sudden decrease in maternal blood pressure will reduce the utero-placental blood flow, resulting in fetal distress.
Magnesium sulphate isthe agent of choice for treatment of eclampsia. It is also used in women with severe pre-eclampsia for prophylaxis of eclampsia andis usually commenced once delivery decision is made or in immediate postpartum period. In women with less severe disease the decision will depend on individual case assessment. Evidence shows that magnesium sulphate more than halves the risk of eclamptic seizures44.It has also been shown to reduce maternal morbidity related to pneumonia, mechanical ventilation and intensive care45.However, there is little evidence to suggest that it decreases the risk of stillbirth or neonatal death.Magnesium sulphate is usually continued for 24 hours following delivery or 24 hours after the last seizure, whichever is the later, unless there is a clinical reason to do otherwise. This is based on the findings of the Collaborative Eclampsia Trial, 1995. However, recent evidence suggests that magnesium infusion may be stopped earlier (12 hours postpartum), especially when used in conjunction with other clinical parameters46, 47. Regular assessment of the urine output, deep tendon reflexes, respiratory rate, oxygen saturation and serum concentration is done as long as magnesium sulphate is continued to avoid toxicity. Features of magnesium toxicity include suppression/loss of patellar reflexes, drowsiness and respiratory depression. Intravenous calcium gluconate is used for reversal of magnesium toxicity.
Fluid restriction is the usual practice, unless there is associated maternal haemorrhage, to reduce the chance of fluid overload and pulmonary oedema. As per NICE guidelines, total fluids should be limited to 80 ml/hour in women with severe pre-eclampsia. Strict intake-output chart should be maintained. The regime of fluid restriction should continue until postpartum diuresis commences.
The mode of delivery should be individualised taking into account the gestation, presentation, cervical favourability for induction of labour and well-being of the fetus. Vaginal delivery is generally preferable but in case of extreme prematurity or fetal compromise, caesarean section is more likely.
Haematological and biochemical monitoring needs to be continued in labour and is dictated by the patient condition and need for analgesia/anaesthesia. For those on magnesium sulphate, bloods must be repeated every 6 hours.
Anaesthetic management
The anaesthetic management in pre-eclamptic patients is important, and should start with a detailed pre-anaesthetic assessment. Appropriate history and physical examination are important. Pre-eclamptic patients are at increased risk of oedema of the pharyngolarynx and assessment of airway is vital48-49. Clinical assessment of the cardiopulmonary and fluid status is required, along with laboratory investigations including renal biochemistry and coagulation status.An appropriate understanding of the obstetric interventions such as antihypertensive medications, and magnesium sulphate infusion is required.
Anaesthetic management should include appropriate monitoring, and should include NIBP, pulse oximetry and urine output. Invasive blood pressure monitoring (arterial line) is indicated in patients with poorly controlled blood pressure, or when NIBP is difficult to obtain (e.g. in the obese patients).
Pulmonary oedema is a rare but serious complication of severe pre-eclampsia, which can lead to increased maternal mortality (10%) and perinatal mortality as high as 50%50. Central venous pressure monitoring is indicated in patients with pulmonary oedema, poor urine output or when difficulty in fluid management is anticipated in the peripartum period. Pulmonary arterial catheters are rarely needed. Non-invasive monitoring of cardiac output may be required in patients with difficult fluid management or coexisting cardiac problems.
The safety of regional anaesthesia in pre-eclamptic patients is now well established51. Lumbar epidural may be used for labour analgesia in women with pre-eclampsia if the mothers opt for it. Early epidural should be considered as it helps to diminish the hypertensive responses to pain. Platelet count >75x109/L in the absence of other coagulation abnormalities is not associated with increased likelihood of regional anaesthetic complications in the setting of pre-eclampsia52. The presence of a functioning epidural catheter allows the epidural block to be titrated for LSCS if indicated. If central neuraxial block is contraindicated, then intravenous opioids may be used for labour analgesia53-54. Few studies have mentioned the successful use of remifentanil PCA in these patients55.Regional blockade is currently the preferred mode of anaesthesia for caesarean section. It has long been argued that while titrated epidural blocks are safe, single shot spinal or CSE techniques may produce profound hypotension. However, multiple studies have demonstrated the safety of spinal and CSE in pre-eclamptic patients for LSCS with no adverse effects on mother or fetus56-58. In fact the incidence of hypotension in pre-eclamptic patients following regional anaesthesia is less than that in healthy patients, and is successfully managed by intravenous boluses of ephedrine or phenylephrine59-60.Doses of local anaesthetics in regional anaesthesia remain the same in pre-eclamptic patients as in normal healthy parturients.
Though regional anaesthesia is preferred for LSCS, a general anaesthesia may still be needed if regional anaesthesia is contraindicated (e.g. coagulopathy as in HELLP syndrome), and in emergency situations where the baby has to be delivered as early as possible. General anaesthesia increases the risk of hypertension during induction and emergence, loss of airway due to pharyngolaryngeal oedema, aspiration and transient neonatal depression. Extreme care is to be undertaken to obtund the hypertensive response during induction-intubation, as this has been a significant past cause of maternal mortality61. Several agents (alfentanil, fentanyl, remifentanil, magnesium sulphate, intravenous lignocaine and esmolol) have been suggested for induction, and clinicians should use familiar ones. All opioids rapidly cross the placenta and increase the risk of neonatal depression, and appropriate facilities for neonatal resuscitation must be available. Remifentanil has the advantage as it is rapidly metabolised by the neonate, and any respiratory depression is usually brief62- 63.Maintenance of anaesthesia is done by inhalational anaesthetic agents. Isoflurane is considered to be a good choice, because of its vasodilating properties. Vigilance is also required during emergence from anaesthesia, to prevent hypertension, as well as aspiration.
Anaesthetists must also be aware of the potential drug interactions of agents commonly used in pre-eclampsia. Magnesium sulphate and calcium channel blockers may potentiate the action of muscle relaxants and appropriate monitoring is vital.
Post delivery analgesia
This is maintained by simple analgesics like paracetamol. Non-steroidal anti-inflammatory agents have been used; however, caution must be exercised due to their effect on cyclo-oxygenase pathway, especially those with renal insufficiency and coagulopathy. A few case reports of significant increase in blood pressure in postpartum women have been reported following their use64. Patient controlled analgesia with opioids has been used widely, and is considered to be a safe option.
Use of oxytocic agents
Syntocinon is the drug of choice. Ergometrine should be avoided because of its propensity to cause hypertension. Synthetic prostaglandins such as Carboprost (15 methyl PGF 2 alpha) may be given with caution after considering the risk-benefit ratio, especially because it can aggravate hypertension.
Use of thromboprophylaxis
This should be considered in all patients with pre-eclampsia.
Table 2: Management strategies for chronic hypertension and gestational hypertension
Preconception
Antenatal
Delivery
Postpartum
Further follow-up
Chronic Hypertension
Optimise antihypertensives, change ACE inhibitors, diet and lifestyle modification
Continue treatment to maintain BP <150/100. Offer uterine artery dopplers to detect risk of developing pre-eclampsia/IUGR
At 37 weeks, if BP is controlled.
Aim to maintain BP <140/90 with antihypertensives
Medical review at 6-8 weeks
Gestational Hypertension
Assessment of risk factors
Hospital admission if severe hypertension. Antihypertensive if BP > 150/100. Test for proteinuria at each visit, blood tests as indicated
At 37 weeks, if BP <160/110, with/without antihypertensives
Titrate antihypertensives to keep BP <140/90
Medical review at 6-8 weeks, or earlier if need to continue antihypertensives
Pre-eclampsia
Assessment of risk factors.
Hospital admission at diagnosis. Antihypertensives to be started if BP>150/100. Regular blood investigations (2-3/week)
Delivery between 34-37 weeks, depending on maternal/ foetal condition
Initial monitoring as inpatient, to be discharged to the community when BP <149/99 with/without treatment and blood results are stable
Medical review at 2 weeks, if continuing antihypertensives. Otherwise at 6-8 weeks
Postpartum Care
Following childbirth, mobilisation of the extravascular fluid occurs increasing the intravascular volume, and consequently increasing the blood pressure. This fluid shift also increases the risk of pulmonary oedema, cerebral oedema and eclampsia.
Most of the existing guidance focuses on management of blood pressure and its associated problems in the antenatal and intrapartum period but the postpartum phase can often be poorly looked after 65. Regular blood pressure monitoring at an interval of 4-6 hours should be done as an inpatient initially and blood platelet count, transaminases and creatinine should be measured to note any changing trends. The aim is to maintain blood pressure <160/110mmHg, thereby preventing cerebral injury from occurring. In order to achieve this, beta-blockers, calcium-channel blockers and ACE inhibitors can be used in a stepwise manner. Use of methyldopa is usually avoided as it has the potential to cause depression and psychosis in postpartum period. Women are discharged to the community care if they are asymptomatic, blood pressure, with or without treatment, is 149/99 mmHg or lower and blood test results are stable or improving. Blood pressure isthen checked daily/alternate days in the community till 2 weeks postpartum. Antihypertensives should continue till blood pressure falls below 130/80 mm of Hg and the dose adjustments need to be made by the GP. If blood pressure becomes uncontrolled, then women would require urgent referral to the hospital.
In most cases, the hypertension and/or proteinuria resolve within six weeks postpartum. Any women whohad pre-eclampsia complicating their pregnancy, needs to have blood pressure and urine protein checked at 6-8 week postnatal visit at the GP surgery. If still requiring antihypertensive treatment at that stage or persistent proteinuria further assessment is warranted to find out cause for raised blood pressure if any and also identify and advise on risk factors for cardiovascular disease and lifestyle changes.
For all these women preconception counselling should be offered for subsequent pregnancies especially if risk factors are identified so that potentially preventative strategies can be initiated.
Table 2 outlines briefly the management strategies for mothers with chronic hypertension and gestational hypertension. However, a detailed discussion is outside the scope of this article.
Examination of the ovaries at caesarean section is a normal practice as ovarian pathology may be found. The incidence of an adnexal mass found at caesarean section ranges from 1 in 123 1 to 329 2. Ovarian cysts rarely develop de novo in late pregnancy, but rather persist from early pregnancy. About 4 in 5 ovarian cysts detected in the first trimester scan resolve spontaneously. Also, 4 in 5 of ovarian cysts persisting into the second trimester will also be present in the post-natal period as complex cysts such as serous cystadenomas, mature cystic teratomas, endometriomas and mucinous cystadenomas 3. It therefore seems sensible to remove the ovarian cyst for histology at caesarean section rather than subject the woman to the anxiety of multiple investigations and/or another laparotomy, particularly when ovarian cystectomy during caesarean section does not appear to increase morbidity of the procedure 1.
We present a case of incidental ovarian cyst found at elective caesarean section to illustrate the value of a comprehensive consenting process.
Case Report
A 35 year-old para 1 + 0 healthy Polish woman was admitted for elective lower segment caesarean section (LSCS) at 39 + 4 weeks gestation in view of a previous caesarean section 2 years ago for failure to progress in the first stage of labour.She was booked in a neighbouring hospital for her antenatal care where she was counselled and consented for the procedure by her consultant. Her pregnancy was uncomplicated and routine pregnancy scans were unremarkable. Apart from drainage of a breast abscess 2 years ago, she had no medical history of note.
Written consent for elective LSCS was obtained by the junior doctor on duty before the consultant pre-operative ward round. However, the directorate’s standardised consent (figure 1) form was not used. The woman was therefore again counselled and written consent for elective LSCS obtained for the third time now including previously omitted additional procedures that might be performed during the course of the surgery.
At the uncomplicated LSCS under spinal anaesthetic, routine inspection of the uterus and adnexa revealed a 30 x 20 x 15 mm pedunculated firm pale mass attached to the left ovary suggestive of a fibroma. The findings were relayed to the woman, and confirmation of consent for the ovarian cystectomy was obtained. The abnormal ovarian mass was removed with conservation of the left ovary. Histology of the mass subsequently confirmed it to be an ovarian fibroma / fibrothecoma.
Discussion
The Royal College of Obstetricians and Gynaecologists (RCOG) recommend that clinicians should seek prior consent to treat any problem which might arise 4. Indeed, in its Consent Advice for caesarean section, it states that discussion of appropriate but not essential procedures, such as ovarian cystectomy at caesarean section, should take place before undertaking the procedure 5. This supports the position of the Department of Health which states that a procedure should not be performed merely because it is convenient, and that it is good practice where possible to seek the person’s consent to the proposed procedure well in advance, when there is time to respond to the person’s questions and provide adequate information 6.
In spite of the publication of the above guidelines well over a year ago, our case supports the belief that most obstetricians omit discussion and/or documentation of ovarian cystectomy at LSCS, and indeed other risks or additional procedures that may be relevant as showed in figure 1. This may be because the clinician is unaware of the recommendations, not familiar with the potential risks or findings at surgery, or that there is simply insufficient time to document comprehensively.
Our directorate has adopted the use of standardised consent forms for common procedures. These forms are available on our intranet which can be edited allowing clinicians to amend the risks and additional procedures as appropriate in each individual case. We believe the verified printed consent form offers legible and comprehensive documentation of the counselling process, as well as prompting clinicians to discuss key issues such as those recommended by the RCOG Consent Advice. We advocate the use of such standardised consent forms in improving the care of patients and supporting clinicians to deliver optimal services.
Figure 1. Standardised consent form for lower segment caesarean section
Introduction: Most experts define infertility as not being able to get pregnant after at least one year of trying. Women who are able to get pregnant but then have recurrent miscarriages are also said to be infertile. The infertility definition made a difference. The World Health Organization definition based on 24 months of trying to get pregnant is recommended as the definition that is useful in clinical practice and research among different disciplines.1Magnitude of the Problem: It is a growing problem and across virtually all cultures and societies almost all over the World and affects an estimated 10%-15% of couples of reproductive age. In recent years, the number of couples seeking treatment for infertility has dramatically increased due to factors such as postponement of childbearing in women, development of newer and more successful techniques for infertility treatment, and increasing awareness of available services. This increasing participation in fertility treatment has raised awareness and inspired investigation into the psychological ramifications of infertility. Consideration has been given to the association between psychiatric illness and infertility. Researchers have also looked into the psychological impact of infertility per se and of the prolonged exposure to intrusive infertility treatments on mood and well-being. There is less information about effective psychiatric treatments for this population; however, there is some data to support the use of psychotherapeutic interventions2. Why infertility has a psychological effect on the couple? Parenthood is one of the major transitions in adult life for both men and women. The stress of the non-fulfilment of a wish for a child has been associated with emotional squeal such as anger, depression, anxiety, marital problems and feelings of worthlessness. Partners may become more anxious to conceive, ironically increasing sexual dysfunction and social isolation. Marital discord often develops in infertile couples, especially when they are under pressure to make medical decisions. Couples experience stigma, sense of loss, and diminished self-esteem in the setting of their infertility3. Male and female partner respond differently: In general, in infertile couples women show higher levels of distress than their male partners4; however, men’s responses to infertility closely approximate the intensity of women’s responses when infertility is attributed to a male factor3. Both men and women experience a sense of loss of identity and have pronounced feelings of defectiveness and incompetence. Women trying to conceive often have clinical depression rates similar to women who have heart disease or cancer. Even couples undertaking IVF face considerable stress. Emotional stress and marital difficulties are greater in couples where the infertility lies with the man. Therefore the psychological impact of infertility can be devastating to the infertile person and to their partner. Factors influencing psychological stress: According to one study done in Sweden, three separate factors seem to contribute to the psychological stress men and women experience as a result of their infertility. The three factors, in order of importance for the women were,1. "Having Children is a Major Focus of Life"2. "The Female Role and Social Pressure"3. "Effect on Sexual Life"The men in the study reversed the order of importance of factors 1 and 2. The third factor was equally significant to both the men and women. It was also shown that women experienced their infertility more strongly than the men. Women also showed a more intense desire to have a baby than men.5.Behaviour of the couple as a result of infertility: Stress, depression and anxiety are described as common consequences of infertility. A number of studies have found that the incidence of depression in infertile couples presenting for infertility treatment is significantly higher than in fertile controls, with prevalence estimates of major depression in the range of 15%-54%6,7,8,9. Anxiety has also been shown to be significantly higher in infertile couples when compared to the general population, with 8%-28% of infertile couples reporting clinically significant anxiety9,10. The causal role of psychological disturbances in the development of infertility is still a matter of debate. A study of 58 women from Lapane and colleagues reported a 2-fold increase in risk of infertility among women with a history of depressive symptoms; however, they were unable to control for other factors that may also influence fertility, including cigarette smoking, alcohol use, decreased libido and body mass index11. Psychological factors may also affect the reproductive capacity: Although infertility has an effect on a couple’s mental health, different psychological factors have been shown to affect the reproductive ability of both partners. Proposed mechanisms through which depression could directly affect infertility involve the physiology of the depressed state such as elevated prolactin levels, disruption of the hypothalamic-pituitary-adrenal axis, and thyroid dysfunction. One study of 10 depressed and 13 normal women suggests that depression is associated with abnormal regulation of luteinizing hormone, a hormone that regulates ovulation12. Changes in immune function associated with stress and depression may also adversely affect reproductive function13. Further studies are needed to distinguish the direct effects of depression or anxiety from associated behaviours (e.g., low libido, smoking, alcohol use) that may interfere with reproductive success. Since stress is also associated with similar physiological changes, this raises the possibility that a history of high levels of cumulative stress associated with recurrent depression or anxiety may also be a causative factor. Result of treatment: While many couples presenting for infertility treatment have high levels of psychological distress associated with infertility, the process of assisted reproduction itself is also associated with increased levels of anxiety, depression and stress14. A growing number of research studies have examined the impact of infertility treatment at different stages, with most focusing on the impact of failed IVF trials15. Comparisons between women undergoing repeated IVF cycles and first-time participants have also suggested that ongoing treatment may lead to an increase in depressive symptoms16. The data, however, is still controversial since other studies have found minimal psychological disturbance induced by the infertility treatment process or IVF failure17,18. In light of the discrepancy in results, there has been increasing interest in the factors that contribute to drop out from infertility treatment since this population is often not included or decline to participate in studies. Whereas cost or refusal of physicians to continue treatment have been cited as reasons for discontinuing treatment, recent research suggests that a significant number of drop outs are due to psychological factors19,20,21. The outcome of infertility treatment may also be influenced by psychological factors. A number of studies have examined stress and mood state as predictors of outcome in assisted reproduction. The majority of these studies support the theory that distress is associated with lower pregnancy rates among women pursuing infertility treatment7,16,22,23,24,25. Conclusion: In light of all the data suggesting that psychological symptoms may interfere with fertility, success of infertility treatment and the ability to tolerate ongoing treatment; interest in addressing these issues during infertility treatment has grown. Since psychological factors play an important role in the pathogenesis of infertility, exploration of this is also an important task to manage this devastating problem, which has cultural and social impact.
Female sexual dysfunction (FSD) is a serious morbidity which could occur postnatally. It may lead to a variety of physical, psychological, and social adverse effects on the patient. Moreover, the consequent cycle of fear might compound the initial sexual disorder and makes it more difficult to treat. Therefore, early diagnosis and management of the problem become essential to avoid later sequalae on reproductive and sexual life. However, early diagnosis may be challenged by many factors. For example, many patients will be preoccupied by the newborn or embarrassed of talking about sexual matters after delivery, which makes it very important for the midwifery, medical, or other staff to raise the issue during the postnatal care sessions. The staff, on the other hand, might feel uncomfortable to discuss the sexual function with the client, or even may lack the knowledge and skills required for sexual health counselling. In addition to the client-service gap, there are gaps between different sexual service providers.
There are many types of postnatal sexual disorders. These types can differ widely in clinical features and management. Additionally, management of postpartum female sexual dysfunction (PPFSD) can vary with clinician’s experience. There are very few randomised clinical trials on treatment for PPFSD, which partly explains the service-service gap in PPFSD management.
In the last three decades there has been an increase in caesarean section rate in the developed world due to many maternal and fetal indications, especially with the significant improvement in surgical and postoperative care. Recently, more attention has been paid to the positive role the caesarean section may play in protecting the female pelvic floor from birth trauma. Perineal birth trauma has been accused by many authors of adversely affecting the female sexual well being. 1 On the other hand there is a growing opinion that the quality of postnatal sexual health is unrelated to mode of delivery. 2 The previous two contradictory statements from literature illustrate the real size of the dilemma when we try to counsel a woman requesting a caesarean section as she is worried about sexual dysfunction after vaginal delivery. This problem might become more difficult to solve if the woman already suffers from a sexual disorder (for example: dyspareunia) in the antenatal or preconception period.
Female sexual dysfunction is impaired or inadequate ability of a woman to engage in or enjoy satisfactory sexual intercourse and orgasm. There are certain natural events in a woman’s life when she is at increased risk of developing sexual dysfunction, such as the use of contraception pills, menstruation, postpartum and lactation status, perimenopause, and postmenopause. This could be related to fluctuations in gonadal hormone secretion, making women more vulnerable to sexual symptoms.3 Postpartum female sexual dysfunction (PPFSD) is a common health problem with different incidence reported in literature. Xu et al reported an incidence of 70.6% of PPSFD in the first 3 months after delivery falling off to 55.6% during the 4th-6th months, and reduced to 34.2% at the 6th month, but not reaching pre-pregnancy levels of 7.17%. 2
For the purpose of this piece of writing, the classification of sexual dysfunction put forth by the American Psychiatric Association APA (1994) in the Diagnostic and Statistical Manual, 4th Edition (DSM-IV) is used to help understand the differing presentations of PPFSD. 4 The main postpartum female sexual dysfunction categories are: sexual desire dysfunction (Hypoactive Sexual Desire Disorder), sexual pain disorders (which includes dyspareunia, vaginismus. and vulvodynia), sexual arousal disorder, and female orgasmic disorder.
To help in understanding this classification better, it is important to refer to the early research done in this field by Masters and Johnson in 1966. One of the most interesting findings of the latter has been the four stage model of sexual response, which they described as the human sexual response cycle.5 They divided the human sexual response cycle into four stages: Excitement phase (initial arousal), Plateau phase (at full arousal, but not yet at orgasm), Orgasm, and Resolution phase (after orgasm). 5
Although it is normal to have hypoactive sexual desire (loss of libido) in the first 6-7 weeks after giving birth, this becomes abnormal when the desire for sexual activity is persistently reduced or absent causing distress in the relationship. Sexual desire disorder after delivery may be due to the mother being preoccupied with the neonate or postpartum complications (e.g. infection, pain, and bleeding). It can often be associated with sexual pain disorder as well.
Dyspareunia is the most common type of PPFSD. Solana-Arellano et al (2008) reported an incidence of 41.3% for dyspareunia in the 60-180 days period after giving birth.1 Postpartum dyspareunia may be due to medical (physical) problems such as a mal-healed perineal or vaginal tear, postpartum infection, cystitis, arthritis, or haemorrhoids, which may get worse after delivery. Moreover, dyspareunia might be caused by psychosocial factors like problems in relationship with the partner, work stress, financial crisis, depression, and anxiety. Dyspareunia, in many cases, can occur as a result of a combination of medical and psychosocial factors. Although, vaginismus is recognised as a different identity, it is usually associated with dyspareunia when it happens in the Puerperium. Vaginismus is the involuntary spasm of the pubococcygeal muscles causing difficult and painful penetration. Sexual desire disorders, Isolated postpartum sexual arousal and orgasmic disorder are rarely seen in postnatal clinics as when they occur they tend to be part of other PPFSDs.
Methods:
Risk Factors for PPFSD:To assess the risk factors for PPFSD a literature review was performed using the National Health Library database including all resources ( AMED, BNI, CINAHL, EMBASE, HEALTH BUSINESS ELITE, HMIC, MEDLINE, and PsycINFO). The MESH word/s used was (postpartum sexual dysfunction OR postpartum dyspareunia OR dyspareunia after delivery OR sexual dysfunction after delivery OR sexual problems after delivery). Other different MESH words (using the word sexuality and/or puerperium) were used as well to expand the search possibilities. Only studies discussing the risk factors of PPFSD after vaginal birth were included. Perineal pain as a complication after episiotomy or tears was differentiated from dyspareunia, and studies on perineal pain after delivery were excluded from the review if they did not discuss the effect of the pain on sexual activity. Effect of Mode of Delivery:Searching the Cochrane library databases has shown no review related to the subject. However, Hicks et al (2004) have conducted a systematic review of literature focused on mode of delivery and the most commonly reported sexual health outcomes, which included dyspareunia, resumption of intercourse, and self-reported perception of sexual health/sexual problems.6 In their systematic review they suggested an association between assisted vaginal delivery and some degree of sexual dysfunction but they reported that associations between Caesarean delivery and sexual dysfunction were inconsistent and continued research was necessary to identify modifiable risk factors for sexual problems related to method of delivery.6 Hicks et al have searched PubMed, CINAHL, and Cochrane databases from January 1990 to September 2003, 6 so we have tried to continue the review by looking into the literature database after that date. To assess the effect of mode of delivery on PPFSD (Caesarean section vs. vaginal birth), a literature review was performed using the National Health Library database including all resource ( AMED, BNI, CINAHL, EMBASE, HEALTH BUSINESS ELITE, HMIC, MEDLINE, and PsycINFO) from October 2003 to January 2010. New MESH words were used, related to comparison between different modes of delivery (Caesarean section, vaginal birth, modes of delivery, sexual dysfunction, sexual disorder, dyspareunia). Additional studies from the reference lists were obtained. Only studies directly compared between caesarean section and vaginal birth in term of assessing the PPFSD were included. Results: Risk Factors for PPFSD:Nineteen studies and one systematic review were retrieved in the period from 01/01/1984 to 01/01/2010. The Cochrane library database review did not have related articles. It is worth mentioning, however, that there was a Cochrane review on postpartum perineal short term pain, not related to sexual activity. Therefore, it was excluded from this review. The systematic review included in this list of literature studies is the Langer and Minetti review on the complications of episiotomy.7 Having systematically reviewed four hundred seventy two articles on the Medline database, they concluded that episiotomy, whether medial or mediolateral, appeared to be the cause of more dyspareunia in comparison to spontaneous perinea tears.7 However, there was no significant difference in the incidence of dyspareunia beyond the three month period after delivery.7 After the latter review, Solana-Arellano (2008) have showed that complications of episiotomy are an important risk factor for postpartum dyspareunia. 1 They have found that infection, dehiscence, and constricted introitus complicated an episiotomy can cause long-term postpartum dyspareunia.1 Moreover, Ejegard et al have investigated the long term quality of women's sex life (12-18 months after first episiotomy-assisted delivery).8 They have reported an adverse effect of episiotomy on women's sex life during the second year post partum .8 Effect of Mode of Delivery:Only eight studies fulfilled the criteria. Full papers were retrieved. There was one randomised controlled trial, one prospective cohort study, one cross-sectional study, and the other 5 were performed retrospectively (4 questionnaire surveys, and 1 interview survey). The total pool sample of patients studied included 3476 cases (1185 Caesarean sections vs. 2291 vaginal deliveries). Four studies aimed to compare PPFSD aspects within other variants, such as pelvic floor morbidity, urinary incontinence, and faecal or flatus incontinence.9, 10, 11, 12 the other four studies purely compared PPFSD variants such as dyspareunia with no other pelvic floor morbidity variants.13, 14, 15, 16 There has been an agreement between the studies on the less sexual problems after caesarean section compared to vaginal delivery in the short term after delivery (i.e. up to 3 months postpartum). However, in long term (i.e. more than 12 months postpartum), the outcome was controversial. A meta-analysis was conducted to compare and summarise the long term PPFSD results ( graph 1) . Graph 1: Forest plot of comparison between studies. Studies to left of the midline were in favour of less long term PPFSD symptoms with caesarean section compared to vaginal delivery. Discussion: From the previous results, birth tract trauma is a risk factor which may lead to PPFSD. Therefore it is a logic presumption to think that avoiding pelvic floor injury by performing a caesarean section especially as an elective mode of delivery may alleviate PPFSD. This presumption, if true, will have very significant clinical and financial implications in practice especially with a pre-existing problem of increasing caesarean section rate in many parts of the developed world. So what research evidence in the literature is available to support or overrule this presumption?. The answer to this question becomes more challenging if we know that the British National Sentinel Caesarean Section Audit showed that 50 percent of consultant obstetricians agreed with the statement ‘‘elective caesarean section will least affect the mother’s future sexual function’’ .17 From the previous meta-analysis, there is little evidence to support that a caesarean section may alleviate long term PPFSD compared to vaginal delivery (p=0,02). But, if we examine the studies’ subgroups and primary/secondary results in more details, this evidence sounds insufficient. Griffiths et al (2006) in their questionnaire survey of a 208 women from the Cardiff Birth Survey Database have showed a significant increase in the prevalence of dyspareunia two years after vaginal birth compared to caesarean section. 9 However, their comparison was between vaginal birth and elective caesarean section as they excluded emergency cases.9 Moreover; they found similar increase in the prevalence of urinary incontinence, incontinence of flatus and subjective depression in the vaginal birth group, which lead us to think whether the dyspareunia was related to these factors and not related to vaginal birth itself. In their paper they did not mention if vaginal birth with no tears or complications was associated with a higher incidence of dyspareunia. In contrast, Klein et al (2005) concluded that women who had intact perineum after vaginal birth had less dyspareunia than those underwent caesarean section.12 However, the incidence of dyspareunia in the latter study was higher among women who had an episiotomy with or without forceps.12 Similar findings were revealed by Buhling et al (2006) and Safarinejad et al (2009), who showed that persistence of dyspareunia longer than 6 months after delivery was the highest after operative vaginal delivery.15, 16 Buhling et al concluded that the incidence of persistent dyspareunia was similar in the caesarean section and the spontaneous vaginal birth without injury groups (approximately 3.5%), whereas, Safarinejad et al (2009) have shown that women after elective Caesarean section had the highest Female Sexual Function Index (FSFI) compared to other groups of delivery including the normal vaginal delivery without injury or episiotomy.15, 16 Although Safarinejad et al (2009) study was robust in many aspects, such as using FSFI and studying the sexual function score for both the women and their partners, I think the main weakness in the study that they included only primiparous women. 16 Therefore, we cannot generalise their findings on women in their second or more pregnancies. Moreover, as a previous caesarean section will increase the operative risk of the successive caesarean sections or will add more risk to the trial of labour if this is opted for in the future, we can expect a higher increased of sexual disorders in the following pregnancies. From previous discussion we found insufficient evidence to advocate a decision of performing a caesarean section on basis of alleviating PPFSD. This evidence is outweighed by the higher risk of caesarean section including bleeding, infection, anaesthesia risk, deep vein thrombosis, pulmonary embolism, impairment of future fertility, risk of scar dehiscence in next labour, injury to bladder and bowels and risk of fetal laceration. Author’s Conclusion: Risk Factors for PPFSD:In this review, there is good evidence to suggest that episiotomy is an important risk factor for short term PPFSD. However, there is little evidence to support a possible long term effect especially if other complications to episiotomy occurred later. Breastfeeding, and the use of progestogen-only pill as contraceptive are other risk factors identified by other studies .18, 19, 20 This may be caused by the low oestrogen level and the consequent dry vagina. 18, 19, 20 Other risk factors for PPFSD include the lack of postpartum sexual health counselling and treatment. 2, 21 Effect of Mode of Delivery:Postpartum female sexual disorder is a common problem which can be overlooked in practice sometimes. Awareness of the problem makes half of the solution. The other half consists of identifying the risk factors, careful antenatal and postnatal counselling and sexual health assessment, and educating women, their partners, and staff about diagnosis and management of the problem. Episiotomy and severe obstetric traumas are the main risk factors. Restricted use of episiotomy and early management of episiotomy complications can play an important role in preventing persistent PPFSD. There is insufficient evidence to suggest caesarean section as a better mode of delivery in term of preventing or alleviating PPFSD.
The herniation of a gravid uterus through an incisional hernia site is a rare occurrence. Incisional hernia is a frequent complication of abdominal wall closure and the management of pregnancy with a large incisional hernia with gravid uterus in its sac is challenging. The following is a case report of gravid uterus through an incisional hernia of a midline incision. Case Report Mrs LB, 35 years, Parity 2, period of amenorrhea of 34 weeks 3 days, married for 12 years was admitted to the hospital from the outpatient department due to the ulceration of abdominal skin as a result of herniation of gravid uterus through the midline longitudinal incision of a previous caesarean section . She was a booked case of our hospital and had been receivingantenatal care since 20 weeks of gestation. At 20 weeks there was no herniation of the uterus through the incision line. In her subsequent visits she came with the uterus protruding through the incisional hernia. She was referred to the General Surgeon who recommended elective Caesarean section with repair of hernia. Her past obstetric history revealed that she had her first emergency caesarean section eight years before because of a breech presentation and a second caesarean section, due to thepremature rupture of membranes at term. Both the babies were living & well. On both occasions she was operated on through infra umbilical midline vertical incision. There was no history of caesarean section wound infection during the post operative period in the previous two pregnancies. On examination, she was moderately built and adequately nourished. There was mild pallor. Her pulse rate was 88 beats per minute and her blood pressure was 126/86 mm Hg. Heart and chest were normal. Abdominal examination revealed distention of the abdomen in thecentral area. The uterus was felt just underneath the skin with acomplete lack of anterior abdominal wall. (Figure I) Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair.
Introduction Dysmenorrhoea and other premenstrual symptoms are common among women of reproductive age and lead to suffering and impact on home, school, and work performance. Earlier studies have focused on the prevalence and risk factors of dysmenorrhoea 1, 2, 3. Surveys in Pakistan have found the prevalence of premenstrual symptoms varying from 53% to 67% in college girls 4, 5, 6. About 57% of students in one study reported that dysmenorrhoea affected their work5. Although these surveys document the prevalence and severity of symptoms they do not correlate it with the impact of specific symptoms on daily activities or with healthcare seeking behaviour. A population-based survey of 2262 women from Goa, India, revealed a linear association between pain severity and treatment seeking and time off from work 3. However the impact of specific symptoms of premenstrual syndrome on treatment seeking and rest was not reported. Aims Primary objective: The authors carried out a cross-sectional study to explore the impact of dysmenorrhoea and other premenstrual symptoms among women of reproductive age.Secondary objective: The authors intended to find out the predictors of healthcare-seeking behaviour including self-treatment for premenstrual symptoms. Methodology A cross-sectional survey study design was chosen. A 13-item questionnaire was administered to women, aged 16 to 50, who were not pregnant and had no known gynaecological, medical, musculoskeletal or neurological diagnosis. Participants were recruited from multiple sites using convenience sampling within urban areas of Islamabad and Rawalpindi in Pakistan. Trained interviewers (physicians, medical students, nursing staff, and high school students) filled out questionnaires interviewing female students at a medical college, a nursing college, and at city schools; as well as housekeeping staff and patients’ attendants at a tertiary care teaching hospital in Islamabad. A proportion of women completed the questionnaire themselves. Ethical approval was obtained from the Shifa International Hospital Ethics committee. No personally identifiable data such as the respondents’ names were recorded. ResultsStudy population characteristics A total of 1236 women from multiple locations within Islamabad and Rawalpindi, Pakistan, participated in the survey. Most of the women were in the younger age groups: 402 women (33%) were 16–20 years old and 622 (50%) were 21–35 years old. Fewer women were in the older age groups: 147 women (12%) were 36–45 years old and 63 (5%) were more than 45 years old. About 55% were unmarried and 61% had no children. The distribution of educational achievement was weighted towards the more educated: 16% were able to read a religious book (basic literacy); 49% had some school education (up to 12th grade); and 34% had professional level education. About 27% of the respondents were homemakers (among women with professional level education, 10% reported staying at home). Age at menarche was less than 12 years old for 16%; between 12 and 14 years for 62%; and more than 14 years old for 23% of the respondents. Severity of dysmenorrhoea and its correlation with premenstrual symptoms On the 10-point visual pain scale, 465 women (38%, 95% CI 35–41) reported mild dysmenorrhoea severity from 0 to 3; 517 women (42%, 95% CI 39–45) reported moderate severity from 4 to 7; and 248 women (20%, 95% CI 18–23) reported severe pain rated from 8 to 10. The linear regression coefficient between dysmenorrhoea severity score and the number of days unable to work in a month was 0.59 (standard error: 0.031). Table 1: Prevalence of premenstrual symptoms and their contribution to pain severity and days lost from work
Women reporting symptoms, n (%, 95% CI) a
Contribution to pain score b
Contribution to days out of work c
Low back pain
879 (72, 69–74)
0.39 *
0.05
Depressed mood
484 (40, 37–43)
0.17 *
-0.05
Headache
268 (22, 20–24)
0.25 *
0.22 *
Swelling
218 (18, 16–20)
0.03
0.12
Nausea
218 (18, 16–20)
0.17 *
0.01
* Statistically significant values (P < 0.005)a Respondents were allowed to select more than one option. Total respondents: 1236.b Linear regression coefficients for a 10-point visual pain score categorized into three levels.c Linear regression coefficients for self-reported days unable to work in a month. Table 1 shows the prevalence of primary symptoms of preceding menstruation and their contribution to a 10-point visual pain scale and to self-reported days unable to work in a month. Low back pain and headache contributed most to the pain score while headache and swelling correlated with days out of work. Impact of dysmenorrhoea Among the working women (366 professionals and housekeeping staff) 49% (95% CI 44–54) reported one or more days out of work in a month due to pain. Similarly, among the 452 students surveyed, 53% (95% CI 48–58) reported dysmenorrhoea affecting school performance (Table 2).
Table 2: Impact of premenstrual symptoms and dysmenorrhoea on household, school and work performance
All respondents, n (%)
Students, n (%)
Maids and housekeeping staff, n (%)
Self-employed, n (%)
Professionals, n (%)
Affected domain
Household chores
441 (37)
124 (28)
59 (40)
31 (52)
75 (35)
Household income
129 (11)
24 (5.3)
33 (22)
12 (20)
18 (8.5)
Performance in school
313 (25)
239 (53)
N/A
N/A
N/A
Social obligations
395 (33)
130 (29)
58 (39)
31 (52)
85 (40)
Unable to work for one or more days in a month
643 (53)
282 (63)
75 (51)
38 (63)
103 (50)
Percentages do not add up to 100% as respondents were allowed to select more than one affected domain.Values for 50% or more respondents acknowledging an impact in a domain are given in bold.
Treatment taken for dysmenorrhoea relief
Table 3 outlines the remedies sought for the relief of dysmenorrhoea symptoms and the reported effectiveness of each type of remedy. All treatments except homeopathic were felt to be effective. Logistic regression analysis showed that the use of any treatment type was related to low back pain (odds ratio 2.2, 95% confidence interval 1.6–2.9), pain severity (OR 2.0, 95% CI 1.6–2.5), headache (OR 1.7, 95% CI 1.2–2.4), depressed mood (OR 1.7, 95% CI 1.3–2.2), increasing education (OR 1.1, 95% CI 1.0–1.2) and not being unmarried (OR 0.52, 95% CI 0.34–0.79).
Table 3: Remedies sought for dysmenorrhoea relief and their patient-reported effectiveness
Women reporting use of treatment, n (%, 95% CI)a
Odds ratio for self-reported effectiveness, (95% CI)b
Conventional medicine
496 (56, 53–59)
13 (8.7 to 21)
Household remedies
285 (32, 29–35)
6.5 (4.1 to 11)
Herbal
90 (10, 8–12)
4.1 (2.2 to 7.7)
Homeopathic
125 (14, 12–17)
1.5 (0.89 to 2.6)
a Respondents were allowed to select more than one option. Total respondents: 1236. b Unconditional logistic regression (converged, 6 iterations, 878 cases included, using Epi Info 3.4.3). All odds ratios with P < 0.005, except homeopathic, P = 0.12.[CI, confidence interval]
Conventional medicine was sought by women with higher pain scores (OR 2.2, 95% CI 1.8–2.8) and greater years of education (OR 1.2, 95% CI 1.1–1.3); other factors such as age and specific symptoms were not statistically related. Women with a greater number of days unable to work were more likely to use herbal treatment (OR 1.4, 95% CI 1.1–1.9) while household remedies like hot water bottles and warm drinks were more commonly taken by women with headache (OR 1.66, 95% CI 1.2–2.4), depressed mood (OR 1.6, 95% CI 1.2–2.3) and lesser years of education (OR 0.88, 95% CI 0.78–0.99). Discussion This paper is the first, to the best of our knowledge, to show an association between specific premenstrual symptoms and dysmenorrhoea severity and healthcare-seeking behaviour. We found that certain symptoms, namely low back pain and headache, contributed more to the perceived severity than other complaints. This finding may be of importance to clinicians treating women with menstrual complaints especially when the treatment is symptom-oriented. In women working outside their homes clinicians may wish to target headache and swelling as these symptoms correlated with days unable to work. Prevalence of premenstrual symptoms in the present study was higher than a Japanese survey7 that reported back pain in 6.9% of women and headache in 11% of women (compared with our results of 72% and 22% respectively). This difference may be due to cultural differences in perception and reporting of symptoms, overall better health, and being strong and hardworking. It may simply be the perception difference in underdeveloped or developed country i.e. lack of resources, poor diet, and poor health. Menstrual symptoms caused a heavy impact on social, school, and work responsibilities in women, a finding we share with previous studies. A cross-sectional survey from India found that 17% of adolescent girls reported missing school classes due to dysmenorrhoea while 60% reported disruption of their daily activities8. In an Australian study, 53% of high school girls reported that dysmenorrhoea limited daily routines and 37% stated that it affected schoolwork9. A study from New York found 46% of students missing one or more days of school due to dysmenorrhoea10. Corresponding figures from the present study were: 62% students reported missing at least one day of school and 53% reported an impact on school performance. The authors would like to reiterate the need for screening for and treating menstrual symptoms because of the impact on daily activities and the potential to reduce avoidable suffering. Women seek a variety of sources for relief of menstrual symptoms. A survey of 2411 high school girls in Malaysia showed that 11% sought medical care although the majority (80%) obtained advice from their mothers regarding premenstrual symptoms11. A study of adolescent girls in Haryana, India, found that 5.3% consulted a physician for menstrual symptoms and 22% self-treated with over-the-counter medicines12. 52% reported self-treatment and 7.7% used complementary medicines in a Japanese study13. In the present study, although conventional medicine was felt to be most effective, it was used by only half of the women. This indicates poor access or awareness of available effective treatments. Even household and herbal remedies were infrequently used possibly due to their limited effectiveness. As menstruation and its associated symptoms are often thought to be a ‘normal’ part of women’s lives these issues may remain untreated in the community. Women who were more educated tended to seek more effective treatments, as did those who had more severe symptoms. Clinicians and public health professionals need to proactively reach women from less privileged background to reduce suffering from menstrual symptoms. Educational campaigns to improve awareness of safe and effective conventional medicine, such as non-steroidal anti-inflammatory drugs, could reach women not aware of these options. These public health campaigns may be addressed toward high-school girls, homemakers, and professionally employed women through separate targeted channels. The present study was limited by non-random (convenience) sampling yielding a study sample skewed towards more educated women. This may be due to sampling in urban areas only. The questionnaire was designed using closed-ended questions, to reduce subjectivity in data recording, limiting exploration of unanticipated variables. Psychosocial issues, such as socio-economic disadvantage and mental health, play an important role in the perception and reporting of menstrual symptoms3 but these factors were not explored in this study. Further research in this area should focus on awareness, access to care, and quality of life outcomes with different treatment options. ConclusionLow back pain and headache contribute the most to severity of dysmenorrhoea while headache and body swelling (fluid retention) were predictive of days unable to work. Conventional medicine is commonly used by more educated women, as well as those with more severe symptoms, and was perceived to be effective more often than other treatment modalities. Effective treatments for the relief of menstrual symptoms remain underutilized causing avoidable suffering.
The incidence of caesarean section is rising1 and there is evidence that women who have a caesarean section may be at increased risk of complications in a subsequent pregnancy2. Compared with vaginal delivery in the first pregnancy, caesarean section has been found to be associated with significantly increased rates of: uterine rupture in labour;3 placenta previa and placental abruption;4 placenta previa leading to peri-partum hysterectomy;5 stillbirth;6 and perinatal death7. Sometimes some unusual complication develops with which, we are not familiar. Here an uncommon complication following caesarean section in a post caesarean pregnancy has been reported.
Case report
A 25 years old lady P 1+4 presented at the emergency department of NRS Medical College & Hospital, Kolkata as an unbooked sixth gravida with the complaint of leaking per vagina for last 4 hours and the period of amenorrhoea was 38weeks. Her past obstetric history revealed that she had caesarean section 4 years earlier (indication of caesarean section was not known to the patient) and 4 successive M.T.Ps, the last being done 1 year back. The baby was alive. The couple wanted ligation operation.
On examination, she was mildly anaemic. Pulse was 88/min and BP was 126/80 mm Hg. She was free of any medical or surgical complications like morbid obesity, COPD and umbilical hernia. Per abdominal finding revealed a term size uterus with cephalic presentation and average liquor. FHS was 144/min and regular. Her previous caesarean section scar was low transverse and there was no scar tenderness.
Per speculum examination showed dribbling of clear liquor. Vaginal examination revealed cervix was 1.5 cm dilated, tubular, station was high up (-3) and membranes were absent.
An emergency L.S.C.S. was performed under spinal anesthesia. The skin incision was Pfannenstiel with excision of the previous scar. On opening the abdomen, uterus was found to be adherent with anterior abdominal wall from which uterus was separated for delivery of the baby (a living male baby of 2.75 Kg) and bilateral tubectomy operation. Bladder was also pulled high up which was dissected and pushed down before opening the uterus. Parietal peritoneum was not closed and rectus sheath was repaired with no 1 chromic catgut. Duration of operation was one hour which was longer than usual operation time of 35 minutes.
First two post operative days were uneventful. On the 3rd day there was a small amount of serosanguinous discharge from the umbilicus. The caesarean section wound, which was located much below the umbilicus, was healthy. Methylene blue dye was introduced into the bladder to rule out any communication with umbilicus, through which no dye came out. On 4th post operative day a mass was seen protruding through the umbilicus and on gentle prodding it seemed to be omentum like structure (Fig-I) A provisional diagnosis of omental hernia through umbilicus was made.
Figure I showing omentum like structure protruding through umbilicus
Figure II showing omental tag held during herniorrhaphy operation
On the 5th post operative day, she underwent herniorrhaphy operation under general anesthesia. A tag of omentum was seen to herniate through anterior rectus sheath and skin (Fig-II). The protruding tag of omentum (sent for histopathological examination and confirmed) was excised and a double breasting of rectus sheath was done, keeping a drain which was removed after 48 hours. Her subsequent recovery was uneventful. She came for check up after 6 weeks, when no abnormality was detected.
Discussion
A review of literature has failed to demonstrate the type of complication mentioned above . Intra operative complication like dense intra abdominal adhesion resulting in injury to the bladder and the bowel is not uncommon8. Probably this case report presents an unusual complication for the first time. Probable explanation is that during too much dissection of anterior rectus sheath (to get access to the fallopian tubes) which was firmly adherent with uterus, there was inadvertent injury to the anterior rectus sheath and skin through which omentum had protruded.
COMPETING INTERESTS None Declared AUTHOR DETAILS CHANDANA DAS, MBBS, MD , Associate Professor ,Gynaecology & Obstetrics , NRS Medical College. SNEHAMAY CHAUDHURI, MBBS, MD, DNB , Assistant Professor, Gynaecology & Obstetrics, NRS Medical College. CORRESPONDENCE: DR SNEHAMAY CHAUDHURI, Sopan Kutir , Flat No 1G, 53 B Dr S C Banerjee Road , Kolkata -700010, West Bengal, India Email: snehamay_chaudhuri_dr@yahoo.com
References
Arjun G Caesarean section: evaluation, guidelines and recommendations Indian Journal of Medical Ethics available at www.ijme.in/163co117.html accessed on 29/09/2008
Taylor MK, Simpson JM, Roberts CL,Olive EC, Handerson- Smart D J Risk of complications in a second pregnancy following caesarean section in the first pregnancy: a population-based study MJA 2005; 183 (10): 515-519
Gregory KD, Korst LM, Cane P, et al. Vaginal birth after cesarean and uterine rupture rates in California. Obstet Gynecol 1999; 94: 985-989.
Lydon-Rochelle M, Holt VL, Easterling TR, Martin D. First-birth cesarean and placental abruption or previa at second birth. Obstet Gynecol 2001; 97: 765-769.
Crane JM, Van den Hof MC, Dodds L, et al. Maternal complications with placenta previa. Am J Perinatol 2000; 17: 101-105.
Smith GCS, Pell JP, Dobbie R. Caesarean section and risk of unexplained stillbirth in subsequent pregnancy. Lancet 2003; 362: 1779-1784.
Smith GCS, Pell JP, Cameron AD, Dobbie R. Risk of perinatal death associated with labour after previous cesarean delivery in uncomplicated term pregnancies. JAMA 2002; 287: 2684-2690
Sobande A, Eskander M. Multiple Repeat Caesarean Sections: Complications and Outcomes. J Obstet Gynaecol Can 2006;28(3):193–197
The Mirena intrauterine system (IUS) has been licensed as a contraceptive in the UK since May 1995. Recent National Statistics suggest the Mirena IUS is used by only 1% of women aged 1649 years who are currently using contraception.1 The Mirena IUS now also has a licence for the management of idiopathic menorrhagia2 and may therefore be used by women who do not require contraception. Uterine perforation is a serious, albeit rare, potential complication of intrauterine device or system use. Women may be informed that uterine perforation occurs in fewer than 1 in 1000 of either copper intrauterine device (IUD) or IUS insertions.3,4 Rate of perforation reported with the Mirena IUS in a large observational cohort study was 0.9 per 1000 insertions.5 In this case report, an intraperitoneal Mirena IUS was detected nearly 4 years after its insertion and perforation of the uterus was diagnosed, despite vaginal hysterectomy and admissions to hospital. This case report demonstrates clearly that whenever there is suspicion from ultrasound scan report of an empty uterus that the IUS has fallen out, and in the persistence of symptoms, we should consider performing an abdominal X-Ray which is an easy, cheap method, to identify the IUS outside the uterus.
Case report
A 33-year-old woman, para 2, with a long standing history of menorrhagia, dysmenorrhoea and tiredness was referred by her GP to the hospital (2002). At the time she was treated for anaemia and felt tiredness. Also she was suffering from dysmenorrhoea; her periods had been regular although in the previous few months she was bleeding PV continuously. Her periods had become heavy after sterilisation (1996). She was anaemic. Cervical cytology had always been normal. In the past she had undergone a laparoscopy for pelvic pain for suspected endometriosis (1997), an appendicectomy (1997) and she was diagnosed with duodenal ulcer (1996). For management of her menorrhagia, she opted for Microwave Endometrial Ablation which was done in August 2002. After that she had an ultrasound scan for erratic bleeding which showed irregular endometrium. The patient was booked for hysteroscopy under general anaesthesia. The procedure was attempted in September 2003 and was abandoned due to difficulties passing the hysteroscope through the endocervical canal. The hysteroscopy was repeated in January 2004 and few intrauterine adhesions were reported. A Mirena IUS was inserted under the same general anaesthetic.
A month later she was admitted to the hospital with right upper quadrant pain and a problematic bleeding pattern. Ultrasound at this stage showed a normal size uterus but the Mirena IUS was not obviously in situ. It was assumed the Mirena IUS had fallen out and the patient was booked for vaginal hysterectomy, which was performed in September 2005.
In January 2007 was admitted to the hospital with right upper quadrant pain again and all investigations including chest X-ray, abdominal ultrasound scan and blood tests were normal. She had an upper GI endoscopy which showed a gastric ulcer (Cardia).
Fig.1 Abdominal X-Ray with the Mirena IUS (arrowed).
She was admitted again 1 year later with pelvic pain. An abdominal X-ray showed the lost IUS (fig. 1) and the CT scan showed the IUS to lie anteriorly under the rectus muscles and adjacent to the dome of the bladder. In April 2008 the IUS was retrieved laparoscopically. The omentum was adherent to anterior abdominal wall and the Mirena IUS was found in the omentum, (Fig.2). This was felt to be unlikely to be the cause of the pain. The IUS was removed easily from the abdominal cavity laparoscopically. The right tube and ovary were adherent to right pelvic side and they were freed up. The procedure was uneventful and the patient was discharged the same day and symptom free since.
Discussion
Uterine perforation is a serious, albeit rare, potential complication of Intrauterine contraceptive use. For informed consent, women should be informed that uterine perforation occurs in fewer than 1 in 1000 intrauterine LNG-IUS insertions4 Fig. 2 Mirena IUS (circled) within the omentum.
The rate of perforation reported with the LNG-IUS in a large observational cohort study was 0.9 per 1000 insertions.5 Current guidelines recommend that advice regarding the management of problems arising with the LNG-IUS use4 is similar to that for IUD use3. The problems are suspected perforation, lost threads, abnormal bleeding, pregnancy, presence of actinomyces-like organisms, pelvic infection, and postmenopausal removal.
The Royal College of Obstetricians & Gynaecologists recommends6 that women who present with persistent menorrhagia, despite LNG-IUS use, should be advised to return for further assessment of the uterine cavity (biopsy or ultrasound scan) to exclude pathology.
If menorrhagia persists despite medical treatments, women should be re-examined.6 An assessment of the uterine cavity should be performed using ultrasound scan. An endometrial biopsy should be considered in all women with persistent menorrhagia. When indicated, a hysteroscopy allows the assessment of the uterine cavity and biopsy under local anaesthesia.6 The WHO Selected Practice Recommendations for Contraceptive Use (WHOSPR) 7does not specifically refer to the Mirena IUS. Follow-up 36 weeks following IUD insertion is recommended and the Clinical Effectiveness Unit (CEU) advises similar follow-up for women using the Mirena-IUS.
In this case report, the detection of the Mirena IUS inside the peritoneal cavity was noted nearly 4 years after the insertion and the perforation of the uterus. The patient had several admissions to the hospital under the care of gynaecologists or gastroentero-logists always complaining for upper or lower abdominal pain. She even had a vaginal hysterectomy. Had she undergone an abdominal hysterectomy, the Mirena IUS may have been noted at that time.
This case report clearly demonstrates that following an ultrasound report showing an empty uterus in a symptomatic patient, an abdominal X-ray should be performed to identify whether or not the IUS is inside the peritoneal cavity. Also, we need to be aware of the peritoneal adhesion potential of Mirena IUS it is expected to be low. In another case report8, an intraperitoneal Mirena IUS resulted in plasma levonorgestrel levels 10 times higher (4.7 nmol/l) than the plasma level of levonorgestrel observed with Mirena IUS placed in utero. This high plasma LNG level suppresses ovulation. Therefore, aside from the adhesion potential, a misplaced Mirena IUS should be removed when pregnancy is desired9, 10.
The authors conclude that judicious use of the abdominal X-ray can lead to the early detection of a migrated IUS and expedite early removal.
A thorough literature search of the Medline, Embase and Cochrane databases did not reveal case reports similar to this and also did not report any formal guidance as to the use of the Mirena IUS device following endometrial microwave ablation, but we did find an article regarding insertion of Mirena IUS, after endometrial resection.11
Endometrial resection is a surgical method to manage menorrhagia. Intrauterine scarring may occur following treatment, but it is not known if the risk of uterine perforation is increased.
The Clinical Effectiveness Unit (CEU) responded12 recently that the British National Formulary (BNF)13 suggested that intrauterine devices (IUDs) should be used with caution in severely scarred uteri.
The United Kingdom Medical Eligibility Criteria for Contraceptive Use (UKMEC)14 recommends that if women have a distorted uterine cavity (any congenital or acquired uterine abnormality distorting the uterine cavity in a manner that is incompatible with IUD insertion), then the IUD or the levonorgestrel-releasing intrauterine system (LNG-IUS) should not be used (UKMEC 4).
A narrative review paper on treatment after hysteroscopic surgery suggests that an acceptable post-operative method of contraception after endometrial ablation is the LNG-IUS, as it protects the endometrium and there is a high amenorrhoea rate.15 However, following successful endometrial ablation the uterine cavity is usually severely narrowed making insertion of IUS (or IUD) impossible and it would not normally be considered as an appropriate method in these circumstances. Significant bleeding would suggest failure of the procedure, and if IUS or IUD was to be considered it should only be done with hysteroscopic assistance by an experienced gynaecologist.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
SHAMBHU S MBChB Senior House Officer, Department of Obstetrics and Gynaecology, Hull Royal Infirmary, UK
PAPPAS M MBChB Specialist Registrar, Department of Obstetrics and Gynaecology, Hull Royal Infirmary, UK
CORRESPONDENCE: DR SHAMBHU S, Senior House Officer in Obstetrics and Gynaecology, Hull Royal Infirmary, Hull, UK
Email: siddesh@doctors.org.uk
References
Dawe F, Meltzer H. Contraception and Sexual Health, 2002. London, UK: Office for National Statistics, 2003; 149 http://www.statistics.gov.uk.
Faculty of Family Planning and Reproductive Health Care (FFPRHC). FFPRHC Guidance (January 2004). The copper intrauterine device as long-term contraception. J Fam Plann Reprod Health Care 2004; 30(1): 2942.
Faculty of Family Planning and Reproductive Health Care (FFPRHC). FFPRHC Guidance (January 2004). The levonorgestrel-releasing intrauterine system (LNG-IUS) in contraception and reproductive health. Journal of Family Planning and Reproductive Health Care 2004; 30(2): 99109
Zhou L, Harrison-Woolrych M, Coulter DM. Use of the New Zealand Intensive Medicines Monitoring Programme to study the levonorgestrel-releasing intrauterine device (Mirena). Pharmacoepidemiol Drug Saf 2003; 12: 371377
Royal College of Obstetricians and Gynaecologists (RCOG). The Management of Menorrhagia in Secondary Care. National Evidence- Based Clinical Guidelines. London, UK: RCOG, 1999.
World Health Organization (WHO). Selected Practice Recommendations for Contraceptive Use. Geneva, Switzerland: WHO, 2002.
Management of a perforated levonorgestrel - medicated intrauterine device: pharmacokinetic study: Case report Ronit Haimov-Kochman et al, Human Reproduction Vol.18, No.6 pp. 12311233, 2003.
Adoni, A. and Ben Chetrit, A. (1991) The management of intrauterine devices following uterine perforation. Contraception, 43, 7781.
Andersson, K., Ryde-Blomqvist, E., Lindell, K., Odlind, V. and Milsom, I. (1998) Perforations with intrauterine devices. Report from a Swedish survey. Contraception, 57, 251255.
MEMBERS ENQUIRY RESPONSE Enquiry Reference: 2268, Sent: 2nd April 2008 . Faculty of Family Planning and Reproductive Health Care. Clinical Effectiveness Unit
British National Formulary. BNF 54. 2007.
Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit. UK Medical Eligibility Criteria for Contraceptive Use. http://www.ffprhc.org.uk/admin/uploads/UKMEC200506.pdf. 2006.
Romer, T., Schmidt, T., and Foth, D. Pre- and postoperative hormonal treatment in patients with hysteroscopic surgery. Contributions to Gynecology and Obstetrics 20, 1-12. 2000.
Abbreviations BSCCP British Society of Colposcopy and Cervical Pathology
CIN Cervical intraepithelial neoplasia
CGIN Cervical glandular intraepithelial neolpasia
DNA Deoxyribonucleic acid
HPV Human papillomavirus
HSIL High-grade squamous intraepithelial lesion
LBC Liquid-based cytology
LLETZ Large loop excision of transformation zone
LSIL Low-grade squamous intraepithelial lesion
NHSCSP National Health Service Cervical Screening Programme
Introduction
Papanicolaou’s publication in 1940s, which showed that exfoliated cervical cells could be reliably harvested and spread, fixed and stained on a glass slide, laid the foundations of cervical screening.
In the last two decades, there has been immense progress in the understanding of cervical carcinogenesis and the currently accepted view is that HPV is an essential factor in the causation of the disease. If HPV is persistent, integration into the cellular genome may occur, which results in the inactivation of tumour suppresser genes, suppression of apotosis, genetic instability and development of precancerous change. Additional genotoxic agents, such as smoking, contribute further to the progression of cervical cancer.
The death rate from cervical cancer was essentially unchanged until the national programme was instituted in 1988. The White Paper The Health of the Nation set a national target to reduce the mortality from cervical cancer by at least 20% by the year 2000 (from 15 per 100,000 populations in 1986 to no more than 12 per 100,000, directly standardize against the European population). The NHS Cervical Screening Programme (NHSCSP) exceeded the target by the year 1997, when the rate fell to 8.9 per 100,000. It continues to fall.
Cervical screening programme1
The programme originally involved every woman between the ages of 20 and 64 years (20-60 years in Scotland) being called and recalled every 3-5 years for a cervical smear test. The evidence has indicated that a more effective screening programme can be offered to women by changing the frequency of screening according to a woman’s age. In 2004, the NHSCSP has issued guideline number 20 which covers all of the major aspects of screening, diagnosis, treatment and follow up.
Age group (years)
Frequency of screening
25
First invitation
25 – 49
Three yearly
50 – 64
Five yearly
65+
Only screen those who have not been screened since age 50 or those who have had recent abnormal tests
Age at starting screening
The incidence of cervical cancer under the age of 25 years is low, and the prevalence of transient HPV infection is high. Much of this prevalent disease would resolve spontaneously. Hence, screening women under the age of 25 years may do more harm than good (unnecessary attendance to colposcopy clinic, increased anxiety and possible over treatment).
Screening interval
A 2003 publication indicated that, to be effective in younger women, screening needs to be more frequent. Therefore, the new screening intervals are to be 3 yearly until the age of 50 years when 5 yearly screening until the age of 64 years, because the most incidences of CIN will have been prevented by prior screening2.
Age at finishing screening
The prevalence of CIN3 and invasive cancer in women over the age of 50 is low. Although it is possible that it may be safe to withdraw well screened women with a negative smear history from screening programme at age 50 years, there is no robust evidence to withdraw this level of healthcare.
Population coverage
A major success in the cervical screening programme has been to increase population coverage. There remain certain women who do not participate, including some ethnic minorities and some women who choose not to. A significant proportion of women who develop cancer have not been regularly screened. Additional effort is required to convince some women that screening can be life saving.
LBC
Liquid base cytology provides almost total elimination of inadequate smear. The UK pilot studies concluded that inadequate cytology would be cut by 87 %, from 9.1% with Pap slides to an average of 1.6 % with LBC.
It has been established from systematic reviews that routine primary cervical screening carries a 50 – 70 % sensitivity to detect CIN3. LBC increases overall sensitivity, gives rise to less equivocation in low grade smear and leads to less referral for colposcopy. There is no difference between the specificity of LBC and Pap smear3.
Smear reports
Acceptable range4
Negative smear
Number of abnormal smear
8.1 – 8.3%
Inadequate smears
5.8 – 12.9%
Borderline nuclear abnormality Mild Dyskaryosis
4.1 – 9.5%
Moderate & Severe dyskaryosis
1 – 2 %
Referral guideline for colposcopy
Women with the following smear results should have the colposcopy assessment.
3 consecutive inadequate smears
3 borderline changes in squamous cells
3 abnormal smears at any grade in a 10 year period
1 borderline change in endocervical cells
1 or 2 mild dyskaryosis (1 mild change – acceptable to repeat a smear)
1 moderate dyskaryosis
1 severe dyskaryosis
1 abnormal glandular smear
Time interval: referral – colposcopy
Abnormal smear
within 8 weeks
Moderate or severe dyskaryosis
within 4 weeks
Glandular abnormality or possible invasion
within 2 weeks
Treatment
Recent evidence suggests that possibly all major-grade (CIN 2, CIN 3, HSIL) lesions should be treated, whereas minor-grade (CIN 1, LSIL) lesions should be managed more conservatively.
Over the last decade the trend has been directed toward more conservative methods of managing CIN. This has coincided with the introduction of the large loop diathermy excision technique. A large multicenter study covering over 13000 treatments has recorded the continuing small risk of patients treated with conservative modalities to develop invasive cancer many years after initial treatment. The risk was still present up to 14 years following treatment.
Method of treatment
Local destructive techniques
It is imperative that any such method destroys the CIN contained within the cervical glands or, more correctly the crypts. Therefore, to be totally effective, these methods must destroy the tissue to the depth of at least 6-7 cm. These methods are the treatment of choice for selected cases in which the entire abnormality is visible on the ectocervix, and in which there is no suggestion of invasion. The principal disadvantage of this method is that a histologic examination of the entire lesion is not possible and early invasive cancer may remain undetected. There are four local destructive techniques:
Cryotherapy, or freezing the area by the application of probes; anaesthesia is not usually required.
Cold coagulation, usually without, or with some local anaesthesia.
Electrodiathermy, under either local or general anaesthesia.
Carbon dioxide (CO2) laser evaporation, usually with local analgesia.
Excisional techniques
Cold knife biopsy
Laser cone biopsy
Large loop diathermy
Hysterectomy: abdominal or vaginal
The optimal method of CIN treatment
There is no obviously superior conservative surgical technique for the treatment of CIN. Excisional treatments permit histological assessment of biopsy and can determine risk factors for residual disease.
The studies have led many authors to advocate the use of excision rather than local destruction techniques as the loops have discovered early invasive lesion in excised specimens. But it can be argued that many of the early micro-invasive lesions now found by the use of excision techniques would have been quite effectively destroyed by the use of local destructive techniques. Now at the moment, it must be left to the individual clinician to choose which technique gives the best results.
Complication
Immediate
The morbidity for excisional method is 2-4 % with immediate discomfort and bleeding.
Long term
Cervical stenosis and constriction: This problem tends to occur most frequently in postmenopausal and post partum women, and result in the development of pyometra. In the younger woman, the stenosis may lead to pelvic endometriosis following on haematometra. The patient often presents with symptoms of painful and prolonged menstruation. The simple management is to perform a dilatation of cervix under general anaesthesia. Even use of a narrow endocervical brush may relieve the symptom.
Excessive eversion of the columnar epithelium : It is not uncommon for the cervix to appear with a large area of exposed columnar epithelium, especially after cone biopsy. Such a situation may result in complaints of postcoital and intermenstrual bleeding or discharge. Nevertheless, it is possible for this exposed transformation zone to become infected yet again with mutagenic agent that resulted in the development of CIN.
It may be necessary to stimulate metaplasia of this area by applying cryosurgery, cautery, or even laser vaporization to columnar epithelium. However, for most patients active treatment is not necessary.
Subsequent pregnancy: There is always concern about subsequent fertility and pregnancy outcome following treatment for CIN. The morbidity associated with the excision of a small fully visible TZ will be different from that associated with a large zone which extends 2 cm up the endocervical canal.
The evidence found no effect on subsequent fertility and pregnancy outcome following loop diathermy treatment. However, it is found to have a higher incidence of low birth-weight babies when compared with controls. More recently, other authors have shown that using the CO2 laser, a cone biopsy greater than 10 mm in depth acts as an independent risk factor for the occurrence of preterm labour5.
Success rate
Modern conservative therapies for the treatment of CIN are extremely successful, with the clearance rate in the order of 95 % or better, except cryosurgery which has a lower clearance rate than other conservative method (85%).
Recurrence
The rate of dyskaryosis in 12 months following both LLETZ and laser ablation was 4.4 %. A cumulative rate of recurrence at 4 years was 10.1 per 100 women.
Follow up
Follow up after conservative treatment
Women aged 50 years or more with positive excision margin are particularly at risk of persistent and recurrent disease. Cytology alone is recommended for follow up and should start at six month following treatment.
Women treated for high grade disease (CIN2, CIN3, CGIN) require 6 and 12 month follow up cytology and annual cytology for subsequent nine years before returning to screening at routine interval.
Women treated for low grade disease require 6, 12 and 24 month follow up cytology. If all results are negative, then women may return to screening at routine interval.
Women treated for CGIN are at higher risk of developing recurrent disease than those with high grade CIN. Ideally, six-monthly samples would be taken for five years followed by annual samples for a further five years.
Follow-up after hysterectomy
Women who have had a hysterectomy with CIN present are potentially at risk of developing vaginal intraepithelial neoplasia (incidence 1%) and invasive vaginal disease.
For women on routine recall for at least 10 years prior to hysterectomy and no CIN in the sample at hysterectomy, no vault cytology is required.
For women with less than 10 years’ routine recall and no CIN at hysterectomy, a sample should be taken from the vault six months after surgery and there should be no further cytology follow-up if it is negative.
For women with completely excised CIN at hysterectomy, a sample should be taken from the vault at 6 and 18 months after surgery and there should be no further cytology follow-up if both are negative.
For women with incomplete or uncertain excision of CIN, follow-up should be conducted as if the cervix is still in situ.
Summary of follow up
Histology/ Pre-treatment smear history
Follow up
After conservative treatment
Low grade CIN
6, 12 and 24 months and then routine screening
After conservative treatment
High grade lesion (CIN2, CIN3, CGIN)
6, 12 and annual cytology for 9 years and then routine screening
After hysterectomy
Routine recall in last10 years, No CIN
No vault smear
After hysterectomy
Less than 10 years, Routine recall, No CIN
Vault smear 6 months after hysterectomy
After hysterectomy for CIN
Complete excision of CIN
Vault smear 6 and 8 months after hysterectomy
After hysterectomy for CIN
Incomplete or uncertain excision of CIN
Follow up as if the cervix is still in situ
The potential role of HPV testing
The type II hybrid capture is a new method for the detection of HPV DNA in cervical mucosa. The following list of clinical uses of hybrid capture is suggested:
As a screening method, together with cytology:
For patients with abnormal cytology, to select patients who will be referred to a colposcopic clinic.
To evaluate the low-grade lesions forecast.
The use of hybrid capture as a screening method is based on the principle that the cytology has a sensitivity of approximately 56%, and the sensitivity of virus typification is 77%; but using both at the same time, the diagnostic sensitivity amount to 93%. Whether hybrid capture should be used as a screening method is still being debate6. A recent RCT7 reported that adjunctive HPV testing did not add significantly to the effectiveness or cost effectiveness of LBC to the detection of CIN 3.
Vaccination against cervical cancer8
Without further preventive measures, death from cervical cancer are predicted to jump four-fold to over a million a year by 2050 as a result of the explosion in HPV infection rates across the world. Vaccination as a primary prevention has obvious advantages in countries where screening programmes are not established but may also offer advantages in countries like the UK, where secondary prevention by screening and treating premalignant lesions is not only expensive but sometimes imprecise, resulting in unnecessary anxiety and intervention for some women, while at the same time failing to detect lesions in others.
Rationale
Women previously infected with a particular HPV type are unlikely to become reinfected by the same type, because of immunity largely provided by antibodies targeted against the major papillomavirus capsid protein L1. When made in the laboratory, L1 protein self-assembles into virus-like particles (VLPs) that are morphologically identical to HPV and highly immunogenic but not in themselves infectious because of lack of viral genome.
Gardasil (Merk) is a quadrivalent vaccine offering protection against HPV types 6, 11, 16 and 18. The longevity of this immune response varied, with only 76% of vaccines showing detectable antibody response to 36 months after immunisation. There is preliminary evidence of cross protection against infection with related HPV 31 and 45. Gardasil and Cervarix has an excellent safety record with only transient injection site reaction and no evidence of adverse effects on chronic disorders.
In the UK, the HPV vaccination programme targets the girls from 12 to 13 year old and additional programme for the girls from 13 to 18 years old, starting in September 2008 and finishing in 2011. HPV-specific antibodies generated by vaccination may wane with time, although current data indicate that immune responses persist through 5 years. The need for booster immunisations to maintain protection against infection will become apparent after prolonged periods of follow up.
The abnormal smear in pregnancy
Ten to fifteen in 1000 pregnant women have their smear abnormal. Recommendations for referral colposcopy are the same in pregnancy as in non-pregnant women. Much more reassurance is required, with emphasis on the fact that the colposcopy will not harm the fetus or cause miscarriage. The treatment for preinvasive lesions may be postponed until after delivery. The essential role of biopsy is to rule out an invasive disease.
The cervical smear in menopausal women
Oestrogen deficiency causes atrophy of tissue and a retraction of squamocolumnar junction. The epithelium becomes thinner and more easily traumatized. There is a greater incidence of unsatisfactory smear reports and unsatisfactory colposcopy. It is generally preferable to repeat smear after oral, transdermal or vaginal estradiol for a period of 7 to 10 days.
Conclusion
The cervical smear is a simple and effective screening which has a number of deficiencies. False-negative smears are principally due to imperfect sampling, errors of cytological interpretation, and in rare cases to rapid progression of lesions in sites which are difficult to access. New technologies can improve the sensitivity of screening. The emphasis is on developing systems that will screen for preinvasive stage of cervical cancer and thereby allow assessment and appropriate management.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
TINT TINT WAI, ST3, Obstetrics and Gynaecology Department, Bedford Hospital, United Kingdom
DILIP PATIL, Consultant Obstetrician and Gynaecologist, Bedford Hospital, United Kingdom
CORRESPONDENCE: D Patil, Consultant Obstetrician and Gynaecologist, Bedford Hospital, United Kingdom,
Email: patild@yahoo.com
References
Colposcopy and Programme Management. NHS Cervical Screening Programme publication 20. April 2004
Progress in cervical screening. Scientific Advisory Committee. RCOG Opinion paper 7. June 2006
Guidance on the use of LBC for cervical screening. NICE, Technology appraisal 69. October 2003
David M Luesley, Mohamood I. Shafi and Joseph A. Jordan. Handbook of Colposcopy; Second edition 2002
Albert Singer & John M Monaghan. Lower Genital Tract Precancer. Second edition 2000
W Prendiville, J Ritter, S Tatti, L Twiggs. Colposcopy management options. First edition 2003
Henry Kitchener, et al. ARTISTIC: A randomised trial of HPV testing in primary cervical screening: Final results; BSCCP Annual Scientific Meeting, book of abstracts, 2008
Vaccination against cervical cancer, Scientific Advisory Committee, Opinion paper 9, RCOG; February 2007




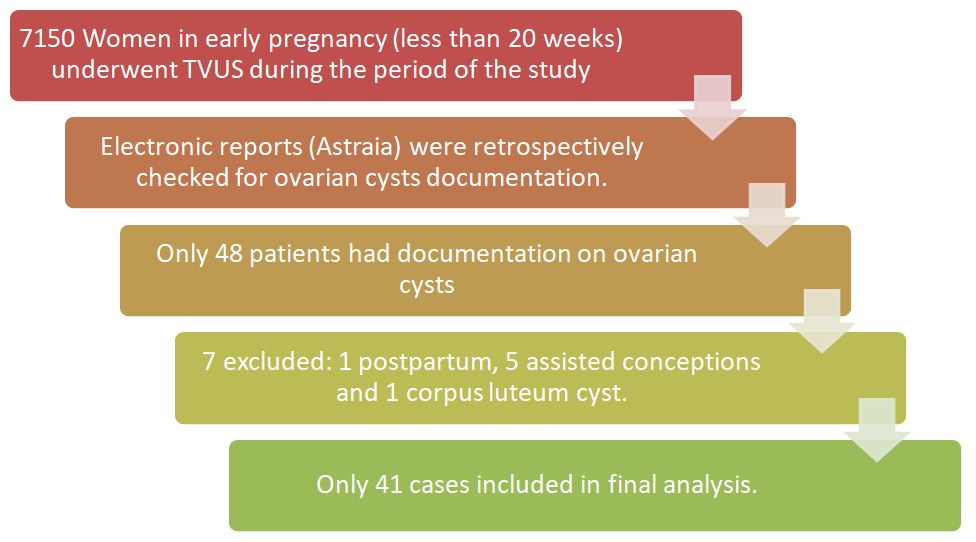
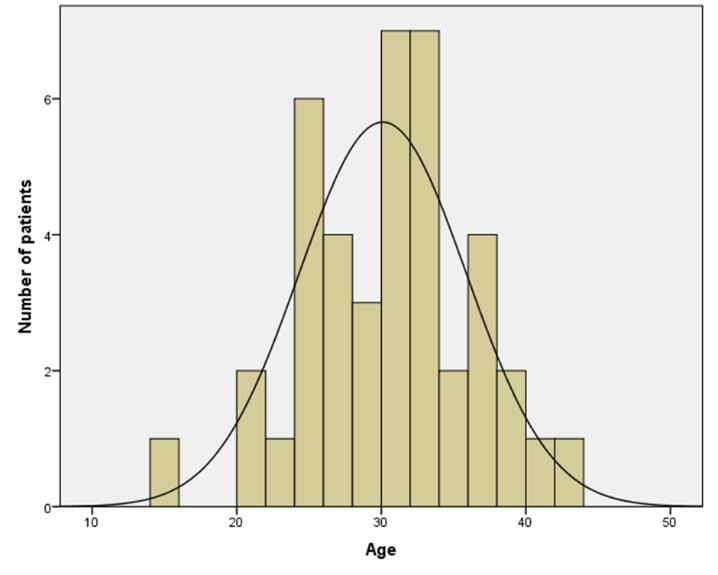
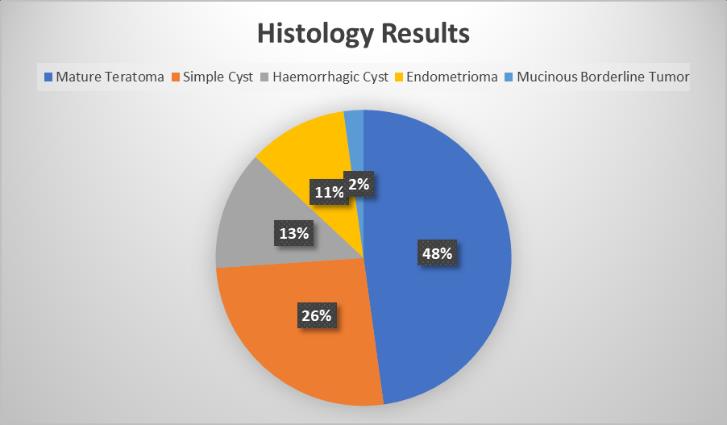
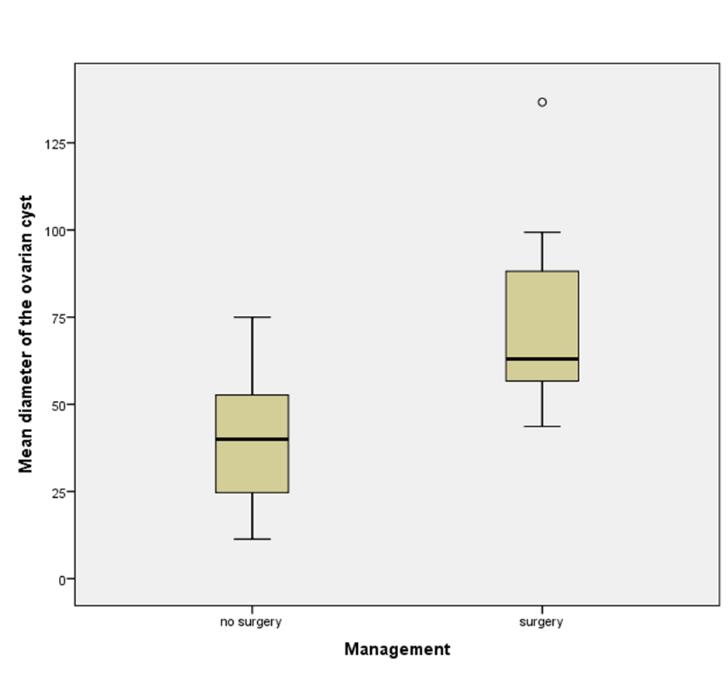
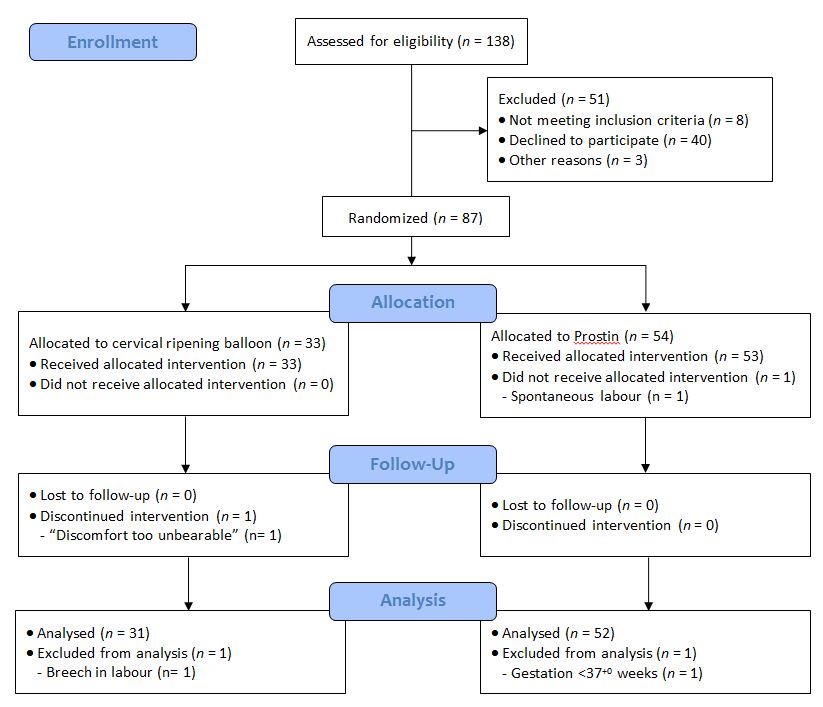

 Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair.
Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair.