There have been continuing initiatives to transform and improve the National Health Service (NHS) in recent years. Mental health services in England have similarly shown evolution with regards to service provision. There has been a shift away from the perceived “medicalisation” of treatment, with traditional long-stay institutions replaced with more targeted and personalised care in the community.1 Furthermore, community services themselves have seen much remodelling over the years including decommissioning and integration, as well as increased involvement in outreach and early intervention teams.2
Mental health services are sometimes perceived as relatively well funded from outside but, as with most healthcare sectors, compared to the population requiring this service, these resources are inadequate to support the growing demand. This has been the case for some time, but it has become more evident with a significant reduction in funding observed since 2010/11.1 In addition, constant governmental pressures to meet key performance targets, as well as unachievable expectations from the public, have further stretched an already resource-depleted mental health service.
The implementation of new National policies3 was supposed to be a shift from large psychiatric hospitals to smaller specialist community centres with a promised reduction in the demand placed on inpatient services. In England, a peak number of 150,000 inpatient psychiatric beds was reported in 1955; this has since rapidly declined to 22,300 in 2012. Between 2010/11 and 2013/14, a further rapid reduction of 7% of all beds available was seen.4
Despite the promise of changes in service delivery within mental health to mitigate the continued reduction in the number of inpatient beds, demand for inpatient beds has not in fact reduced nationally.1 The recommended level of occupancy, for example, is 85% but 119 wards surveyed5 were operating at 91%, with some at 138% level of occupancy. The occupancy levels of over 100% usually occurred when long-stay inpatients were discharged home on short-term leave and their beds got filled during their absence.4 Where numbers of inpatient beds fail to meet the demands, or waiting list for their first assessment or review grows, the inadequacy lends these facilities to issues with regard to providing high quality and safe patient care. Examples of this may include inappropriate use of the Mental Health Act for detention of patients as a means of securing an inpatient bed,5 incomplete assessments of people detained in places of safety due to time or space constraints,6 and an increase in violent incidents on overcrowded inpatient wards.7
What is a Crisis Resolution and Home Treatment Team (CRHTT)?
In the late 1980s and 1990s, community mental health teams provided acute crisis support. This posed a number of issues including that these teams usually operated during normal working hours of 9am-5pm (Monday to Friday) and were not always available to provide support to patients in a crisis, and did not have the desired impact of reducing the number of acute admissions.8 This gap in service provision inspired the experimentation with and subsequent development of intensive home treatment services, some of which showed evidence of reduced hospital admissions, and holistic-working often preferred by families who were happy to have their loved ones receive the required support in the home environment.9 Over the last two decades, with remodelling of services, increased investment, NHS funding rising from £49 billion in 2000 to £122 billion in 2016, and a migration of mental health professionals, CRHTTs were established and are now available in every mental health trust across the United Kingdom (UK).10
CRHTT is a team of mental health professionals including psychiatrists, community psychiatric nurses, social workers and support workers, who provide rapid and intensive support at home during a mental health crisis.11 They are a 24-hour service operating seven days a week, and acting as the “gatekeeper” for acute services accepting referrals from various sources including inpatient, community, liaison and from outside the Trust for providing support to patients experiencing crises. These teams risk-assess patients and determine whether they require inpatient or home treatment. In the latter case, CRHTTs provide intensive home treatment by offering up to 2-3 visits a day as well as 24/7 phone support. These teams are also involved in facilitating early discharges from hospitals; in cases where patients are past the initial acute crisis, but may need further input prior to discharge to community mental health teams for longer term support.8
Definition of diagnosis and second opinion.
A second opinion is defined as “advice from a second expert (such as a doctor/psychiatrist) to make sure advice from the first such expert is correct” whilst diagnosis is defined as “the art or act of identifying a disease from its signs and symptoms”.12 Due to increased pressure on inpatient facilities and remodelling of community services, there has been a huge increase in the number of referrals made to CRHTTs. Between 2011/12 and 2013/14, it has been noted that referrals to CRHTTs increased by 16%.13 Reduction in inpatient beds and high workloads within community services often result in the formulation of arbitrary diagnoses and treatment plans. With increased pressures on other mental health services, the role of CRHTTs has begun to evolve. In addition to the previously discussed functions, CRHTTs appear to be becoming second opinion services by default enabled by the psychiatrists working in these teams.
We organised a project to establish whether a typical CRHTT is fulfilling the criteria of being a diagnostic or second opinion service provider.
Method
We examined 100 consecutively accepted referrals to a CRHTT from 1st December 2016. The patients were divided into three groups: those being discharged/referred from hospital (HR), those referred from the community (CR), and those who were not open to secondary mental health services at the time of referral (NR). The age range and gender of the groups were noted. Thereafter, the NR group was excluded from analysis for the obvious reason that the CRHTT was not providing a second opinion in their case. The HR and CR groups were further reduced by excluding patients who were not seen by a CRHTT psychiatrist. The remaining patients in both groups were scrutinised regarding a change in medication; this was also recorded for the previous and next care occasions. The likelihood of medication change at the next treatment event was analysed to establish whether it was affected by the previous event. The numbers of patients with CRHTT diagnosis change were also recorded for both groups.
Results
Figure 1: Project Flowchart
Figure 2: Group Demographics
n
Patient Gender
Patient Age
Time with CRHTT
Male
Female
Average
Range
1-7 days
> 7 days
No prior referral open (NR)
43
20 (47%)
23 (53%)
36.0
19-60
5 (12%)
38 (88%)
Community referral (CR)
36
13 (36%)
23(64%)
37.8
19-66
7 (19%)
29 (81%)
Hospital referral (HR)
21
10 (48%)
11 (52%)
39.0
19-63
6 (29%)
15 (71%)
There was little difference in age between the three groups (average ages were: CR=37.8, HR=39.0, NR=36.0). There was a lower proportion of men in the CR group than were present in the HR and NR groups (36% as against 48% and 47%). Whether a psychiatrist saw a patient appeared to be related to both the referral source and the length of CRHTT stay. Most (n=16, 76%) patients in the hospital-referred group (HR) were not seen by a psychiatrist while most (n=24, 67%) of those referred from the community (CR) did receive such an outcome. No community-referred patient was seen by a psychiatrist if they were with the CRHTT for less than a week. These short-stay patients accounted for 7 out of the 12 community-referred patients who were not seen. This suggests that a psychiatric assessment should be scheduled more quickly after community referrals so as to offer patients a more comprehensive service.
Psychiatric assessment led to changed diagnoses for 28% (8/29) of patients. This figure was 40% (2/5) for the HR group and 25% (6/24) for the CR group.
Medications were changed for 69% (20/29) of patients seen by a psychiatrist. In the subgroups; 60% (3/5) of HR psychiatric assessments resulted in a change of medication while 71% (17/24) of CR psychiatric assessments led to medication changes.
The chi-square statistic was used to evaluate whether a recent medication change, during the inpatient stay or at the most recent outpatient appointment, made the CRHTT less likely to adjust medication. This indicated that there was no relationship between the two events. A similar analysis indicated that the likelihood of a medication change at the patient’s next community appointment was increased by seeing a CRHTT psychiatrist but unrelated to whether that assessment had resulted in a change of medication.
Discussion
We have demonstrated in this study that a typical CRHTT is providing a diagnostic and second opinion service. Changes in medication were more than twice as frequent as changes in diagnosis – this is perhaps unsurprising as diagnostic changes would be likely to require a different prescription.
Most community referrals were actively evaluated in terms of both diagnosis and treatment. This is a significant change to the original function of the CRHTT where a psychiatric assessment was not a standard aspect of care when very few of the original CRHTTs included a psychiatrist. This may also reflect the current pressures on community teams, which are frequently short-staffed, leading to more competition for the available clinic appointments. Consequently, patients may not have seen a psychiatrist for some time and their requirements may have changed. It is, however, also known1 that community patients who have not been reviewed recently or who have a long wait before their first assessment are more likely to present in crisis.
The diagnostic and second opinion function of the CRHTT is more prevalent when patients have been referred by the community team (67% reviewed, 47% medication changed) rather than on discharge from hospital (24% reviewed, 14% medication changed). This appears to largely reflect the fact that relatively few discharges were seen by the CRHTT psychiatrist because these patients had just received a full consultant-led discharge treatment plan. This may be another example of community service pressures leading to patient crises and thus engagement with alternative services – in this case inpatient care may be offering a second opinion service. The current separation of community and inpatient services will augment this effect as previously the patient would have been more likely to receive continuous care from the same consultant. This is an interesting view of current service configuration. The reduced continuity of care is often seen as a disadvantage but it does present an opportunity for a fresh evaluation of a patient’s diagnosis and medication by a different psychiatrist.
Longer lengths of stay with the CRHTT made psychiatric assessments more likely. It was particularly clear that discharge within a week made a psychiatric review unlikely. The proportion of community-referrals seen by a CRHTT psychiatrist could be increased to 83% if patients were to be seen within 24 hours. This figure is derived from the assumption that psychiatrists would then see the same proportion of both long and short stay patients. The residue would include those patients who refuse to engage with such an appointment.
It is interesting that chi-square statistical analysis suggests that the only influence on prescription change at the next appointment is whether the patient was seen by a CRHTT psychiatrist. It is not related to whether or not the CRHTT psychiatrist changed the medication. It is difficult to see why this should be the case unless the community psychiatrists consider the patients’ needs in more detail or are tempted to regain control after the referral to another psychiatrist.
In conclusion, the addition of psychiatric care to CRHTTs may be a valuable adjunct to the current pressures on community teams. The current trend to separate community, inpatient and CRHTT care is often cited as a disadvantage due to reduced continuity of care for patients. This project has drawn attention to the fact that it also offers opportunities for new teams to re-evaluate both diagnosis and treatment which offers patients the advantage of an internal second-opinion service. This advantage could be offered to more community-referred patients, albeit with more resources, by ensuring that they are assessed by the CRHTT psychiatrist within 24 hours.
Limitations
This is a small study conducted in a single CRHTT. It does, however, offer an indication of the evolving role of the CRHTT and its relationship to other services.
Arrhythmogenic Right Ventricular Dysplasia (ARVD) was first described in a case series of 24 patients back in 1982 1, 2. Since then, our understanding of its pathophysiology has improved dramatically, with dedicated guidelines and literature being published to help with both diagnosis and management. Prompt diagnosis remains a struggle in majority of developing countries, including Malaysia, where resources and expertise are scarce, and obtaining both cardiac magnetic resonance imaging or endomyocardial biopsies remain a challenge. Furthermore, diagnosis is difficult in most cases as clinical presentation may vary and wide range of clinical mimics exist. We present a unique case of ARVD, diagnosed early through the knowledge of having a deceased sibling, whom had endomyocardial tissue characterization performed in the past confirming the presence of the disease in a first degree relative.
Case Report
A 21-year old gentleman presented to the emergency department following an episode of loss of consciousness, lasting approximately 30 minutes which recovered spontaneously. He denies having any similar episodes in the past. However, he had been suffering from reduced exercise tolerance, with a New York Heart Association (NYHA) Class II, over the past 1 year. He had no known medical illness at the time but smoked 6 cigarettes a day for the past 7 years.
His vital signs were stable on arrival, with a heart rate of 73 beats per minute, regular in rhythm, a blood pressure of 143/84 mmHg, respiratory rate of 19 breaths per minute, temperature of 37 degrees Celcius and oxygen saturation of 98% on room air. Cardio-respiratory examination revealed no murmurs, and normal heart and breath sounds. There were no carotid bruits audible. There was no evidence of any neurological deficits on neurological examination.
Figure 2 – Electrocardiogram revealing T-wave inversions in leads V2 to V4 with ventricular ectopic beats
Chest radiography revealed cardiomegaly (Figure 1). Electrocardiogram (ECG) revealed deep T-wave inversions in leads V2 to V4, with ventricular ectopic beats (Figure 2). Due to the suspicious-looking ECG, a serum Troponin-I test was performed, which was elevated at 480 pg/ml. The patient was treated for acute coronary syndrome complicated by cardiac syncope, and was later referred to the medical team for further inpatient management.
However, on further history, it was revealed that the patient had a sibling who had died from an unknown cause, 5 years prior. His younger brother, 14 years of age at the time, was brought in after collapsing whilst playing basketball in a school compound. Unfortunately, he was pronounced dead on arrival to the clinic. A post-mortem was performed due to the unexpected nature of the event. Fortunately, our patient was brought into the same hospital as his sibling, allowing us to trace previous autopsy reports and images, with consent.
Macroscopic examination of the right ventricular cavity revealed epicardial surfaces showing infiltration of excessive fat tissue with nodular fibrosis. The right ventricular cavity appeared dilated and cut sections showed diffuse transmural fibro-fatty replacement of the right ventricular free wall, extending into the endocardium and involving the right ventricular septum (Figure 3a).
Figure 3a – Macroscopic examination of right ventricular cavity, which was dilated and showing signs of transmural fibrofatty infiltration. Figure 3b – Histological evidence of focal lymphocytic infiltration, myocyte hypertrophy and degenerative cytoplasmic changes.
Histology revealed extensive fatty infiltration with interstitial fibrosis, primarily in the epicardium. There was associated myocyte loss with hypertrophy of cardiac muscle cells remaining (Figure 3b). Both macroscopic and microscopic findings were suggestive of ARVD.
After learning of the autopsy results, changes in clinical management took place, with priorities being shifted towards obtaining an echocardiogram, cardiac Magnetic Resonance Imaging (MRI) and Holter recording, as opposed to diagnostic angiography and coronary evaluation. Echocardiography revealed an ejection fraction of 25 to 30%, with evidence of left ventricular dyssynchrony, a tethered posterior mitral valve leaflet with mild eccentric regurgitation, consistent with dilated cardiomyopathy.
Cardiac MRI revealed both left and right ventricular dilatation, end diastolic dimensions being 5.8 cm and 4.4 cm and end-diastolic volume being 153 ml/m2 and 149 ml/m2 respectively, with evidence of bi-ventricular dyssynchrony. Left ventricular and right ventricular ejection fraction measured 31% and 8% respectively. There was also bilateral atrial dilatation. Gadolinium study revealed late enhancement in areas of the right ventricular wall (Figure 4).
Figure 4 – Four-chamber view of cardiac magnetic resonance imaging revealing evidence of right ventricular enhancement following gadolinium study.
A 24-hours Holter recording revealed up to significant ventricular ectopic burden, many of which were bigeminy and trigeminy in nature. In view of symptoms and the above investigative findings, the patient consented to insertion of an implantable cardiac defibrillator (ICD) 4 weeks later in our centre, and has since recovered well with regular monitoring.
Discussion
ARVD is rare, prevalence ranging between 1 in 2000 to 1 in 5000 (taking into consideration geographical variations) and accounts for 5% of deaths in young adults and 25% of deaths in athletes 3, 4. Typical histopathological feature of ARVD is the loss of right ventricular myocardium, replaced heavily by fibro-fatty tissue. Less commonly, left ventricle involvement have been reported 5, 6. Consequence from such pathological process leads to arrhythmias, heart failure and more importantly sudden cardiac death (SCD), with mortality rate ranging between 4 to 20% and peaking in the fourth decade, equally in both males and females 5.
Diagnosis is difficult in most cases as clinical presentation may vary and wide range of clinical mimic exist, including myocarditis, sarcoidosis, Brugada syndrome, idiopathic RV outflow tract VT and congenital heart diseases with right chambers overload amongst others 6. A Diagnostic Criteria was developed in 1994, with further modification in 2010 to assist in the diagnosis of ARVD and although the criterion has been shown to be specific, it lacks sensitivity 7. Nevertheless, it highlights several key areas, a mix of clinical, radiological, histological and electrophysiological features, that assist in diagnosis 4.
Despite not having any further evaluation or investigations performed at the time of presentation, in view of circumstances, our patient’s deceased sibling had supportive histological features. Therefore, our patient met the major criteria of having a first degree relative affected by the disease. More importantly, the suspicious family history had prompted further evaluation for the disease, allowing the medical team to prioritize investigations performed, specifically the Cardiac MRI and Holter evaluation. This led to early risk stratification and decision to implant an ICD for the patient, as he was deemed at high risk of SCD.
Conclusion
This case highlights the importance of good history taking, including a detailed family history of SCD or cardiac-related diseases, especially in young patients presenting with typical cardiac-related symptoms. Early identification and appreciation of risk will subsequently affect the outcomes of such patients affected by ARVD. Furthermore, important diagnosis like ARVD will have implications to relatives and future off-springs, further highlighting the need for detailed evaluation of patients similar to ours described in the above case report.
In a contemporary medical practice caring for complex patients with utmost efficiency, primary care physicians and specialists are expected to work together to organize a seamless transfer from acute to chronic care. The job of the generalist is to sort out and integrate different recommendations from numerous specialists and apply those strategies in the care of the patient long after the index admission. During such interactions with specialists, primary care physicians often realize the impact of differing viewpoints on the overall patient care well beyond the anticipated time frame, whether acute or chronic. To that end, and to better inform such recommendations, this paper proposes the top 10 things primary care physicians wish every specialist knew when addressing problems on the busy hospital ward.
1. Organ-systems work together, not independently
As we see in examples such as the cardio-renal syndrome, hepato-renal syndrome, or hepato-pulmonary syndrome, as the patient gets sicker, the interaction of organ-systems begins to dominate. Indeed, predicting the outcome in comorbid conditions depends not only on understanding the culprit organ, but rather quantifying a complicated interaction of multiple organ-systems. For example, the ADHERE registry algorithm shows the most important predictor for in-hospital death in heart failure patients is not the cardiac function per se, but rather creatinine clearance and BUN[1]. In other words, the commonly used comments from a specialist asked to evaluate their system of expertise, ‘such and such organ is fine’, might soon become irrelevant and obsolete in the context of multiple complex systems.
Moreover, recent research revealed that genotype, endotype and phenotype are quite different in COPD and asthma[2]. Therefore, even though a disease may manifest in a single system, the pathophysiological process from which it arose may have been triggered in different organs.
2. Mortality is not the only outcome measure
Specialists seem to treat all-cause mortality as the most important outcome measure in most cases. Or, they choose strategies based on organ specific survival as an alternative, such as MACE (major adverse cardiac events) or creatinine-doubling time[3]. Life is far more than just being alive. Subsequently, the quality of life (QOL) measures, which capture patient-centred outcomes, provide insight into the effectiveness of interventions but also their meaningfulness to patients, and such measures are gauging previously uncaptured positive aspects of interventions[4]. The difficulty of defining well-being remains a challenge for researchers and arises from the differences brought about by cultural and societal elements which are context-bound and unique to each community.
3. ADL is one of the most critical prognostic indicators
New biological markers are numerous around here - new renal injury markers, such as NGAL or KIM, to name a few. But a quick, old-fashioned, bedside assessment can easily reveal impairments in Activities of Daily Living (ADL) at each patient visit; and ADLs by Functional Assessment Measures have been consistently shown as strong outcome predictors in acute and chronic illnesses, especially within elderly populations[5]. In fact, functional measures were deemed to be as important as other objective measures in some prognoses[6]; for instance, in the BODE score for COPD survival prediction, the ADL measure carries the same weight as the PFT (Pulmonary Function Test). In the management of elderly patients, hospitalization[7] and initiation of haemodialysis[8] significantly influence the worsening of ADLs. In the development of a 1-year mortality index after hospital admissions among elderly patients, ADL was of pivotal importance[9].
Functional impairment is also a strong indicator for readmission: there is a dose-response correlation of severity of impairment and the risk of readmissions[10]. Intensifying the in-hospital post-ICU physical and nutritional therapy has been shown to improve many aspects of recovery[11]. In patients with numerous chronic illnesses, the number of comorbidities strongly correlates with the decline of ADL[12]. Interventions to maintain pre-hospitalization ADL is important in facilitating recovery from hospitalization, and in one study in-hospital mobility programs helped patients to maintain pre-hospitalization ADL while the usual care group experienced significant decline[13].
4. Effectiveness, not efficacy, matters most in the real-world
“Doctor, I cannot afford the medicine prescribed to me when I was discharged!” This is oft-repeated in offices of generalist physicians. If a patient cannot afford medication and therefore does not take it, the treatment lacks efficacy. In the inpatient setting, efficacy of intervention determines the outcome since patients are most likely to receive the prescribed intervention. This is not the case in the outpatient setting, and the effectiveness of an intervention depends on many other elements, such as the accuracy of diagnosis, patient compliance to the proven intervention, prescription drug coverage, access to care, and finally, efficacy of the intervention[14].
5. Mental wellness is essential to physical wellness
Health is not limited to the physical body; it also involves mental wellness. In fact, mental and physical health are inseparable. Naturally, serious illnesses affect mood and cognition: therefore, it is important to acknowledge that mental health issues lie squarely within the spectrum of physical disease management. Generalists can help patients with multiple comorbidities manage depressive symptoms through brief psychological interventions; such symptoms related to cognition and mood are expected consequences of any serious illnesses.
Studies have shown that among elderly patients without dementia at baseline, noncritical hospitalization is associated with the development of cognitive dysfunction[15]. Among elderly patients, the prevalence of cognitive dysfunction is significantly higher in ADHF (acute decompensated heart failure) admissions[16] or survivors of severe sepsis[17]. Depression and depressed mood are prevalent in patients suffering serious illnesses[18]. New models are emerging to integrate psychotherapy in multiple comorbid patients and have been proven to be effective[19].
6. Pay heed to illness trajectory
“My grandma has never been the same after her hip surgery. Please fix her!”
Primary care physicians often note a decline in the general function and cognition of their patients after index admissions to the hospital. As noted earlier, acute hospital admissions have a strong independent effect on the severity of disability amongst elderly persons[20]. The multidimensional frailty score, which incorporates ADL and cognitive function, predicts one-year mortality based on a simple scoring system[21]. Poor functional status attributes to frailty and has led to poor surgical outcomes in the elderly[22]. The prevalence of functional impairment steadily increases from 28% in the 2 years prior to death to 56% in the last month of life[23]. Studies demonstrate that gait speed is an important predictor for survival amongst the elderly[24][25] as well as grip strength[26][27].
Furthermore, elderly patients sustain significant impairments long after the index hospitalization[28]. Amongst elderly patients discharged from the ICU, more than 50% die within a month[29]. At one-year follow-up, critical ADL capacity, such as taking medications or shopping, was impaired in more than 70% of ICU survivors who remained ventilated for longer than 48 hours[30]. Delirium sustains a long-lasting effect even after patients are discharged from the hospital, the longer the duration of delirium, the more sustained is the cognitive impairment[31].
7. Care for the care-givers
There is increasing evidence that caregivers sustain long lasting effects from patient illnesses. Depressive symptoms increase overall for surviving spouses regardless of hospice use[32]. The RECOVER study[33] demonstrated that caregivers suffered from high levels of depressive symptoms up to 1 year after a loved one’s ICU admission. In the era of chronic illnesses, it is essential to be mindful of the contributions made by caregivers in disease management. Tools are widely available for the clinician to assess caregiver burden[34]. This is important because family-support interventions have been shown to improve the quality of communication and decrease the patient’s length of stay in ICU[35].
8. ‘Exercise and diet’ trumps ‘medicine and surgery’
The COURAGE trial demonstrated that after 7 years, there is no difference between medical management and percutaneous intervention (PCI) in managing coronary disease[36]. As time progresses after the initial event, the benefits of surgical intervention become less apparent. Similarly, in the long run, intensive statin therapy has not proven to be of greater clinical significance compared to those receiving moderate levels of statin[37]. As the saying goes, in the long run, “we are what we eat.” Innumerable studies have shown that diet and physical habits have a lasting effect on the health of individuals[38]. Bariatric surgery has been demonstrating dramatic and long-lasting effects on diabetes control, while the DiRECT study demonstrated that intensive exercise and diet successfully achieved remission in nearly half of the intervention group, compared to only 4% of controls[39]. Despite the substantial increase in chronic illnesses that are closely tied to our lifestyle and eating habits, physicians of all specialties are poorly trained to provide nutritional counselling to patients[40].
9. Whose definition of health matters?
If health is defined, as defined by the WHO, is not simply the lack of illness, but “a state of complete physical, mental and social well-being,” it must incorporate many other elements dictated by societal, cultural, moral and philosophical norms and values. Furthermore, the definition of health and the path to attain it should come from the society and community it reflects, since neither healthcare personnel nor the healthcare industry own health. Therefore, the definition should emerge from community interventions and multidisciplinary groups filled with varied stakeholders, rather than from the ivory tower of healthcare researchers. Therefore, medical decision-making processes are rapidly moving away from the paternalistic approach to consensus-based, collegial decisions. Shared decision-making, informed consent, discussions of different treatment options and acquiring second opinions have become standard practice and reflect the empowerment of patients, and communities, to define their own healthcare. Ultimately, as long as patients are competent, they decide their treatment after consulting with physicians, who advocate for the patients’ goals in care and advise them accordingly.
10. Empower healthcare recipients
In the long-term management of chronic illness, participation of the patient is essential. And transparent communication is pivotal for better participation and shared decision-making[41]. In the new model of health, healthcare providers must play an active role in advocating for patients and promoting well-being while acknowledging that health is a dynamic concept[42]; these physicians do not simply “coordinate care.” This shift from the physician-centred to the patient-centred approach, in and of itself, will be empowering for patients.
CONCLUSION
Transition of care is one of the most important steps connecting hospital care to primary care. Those problems currently labelled as miscommunication might be more than just a lack of handoff tools or timely messaging; they rather stem from a difference in priorities and varied interpretations of patients’ problems by these two groups of providers. Many questions remain unanswered when facing the future of collaborative healthcare: what kind of doctors are most suited to address the complex interaction of illnesses involving multiple organs? Who can develop a new framework to capture this dynamic and complex interaction of systems, covering many organs in a single patient? Moreover, the next generation of healthcare providers will need to be trained to bear in mind this fundamental concept of patient management. As the twenty-first century progresses, discoveries within medical science will continue to advance the field further away from the current organ-based specialization to pathophysiology-based specialization. This article advances the discussion on the altering role of generalist physicians and the advice of their specialist colleagues, as together they face more and more changes within the practice of medicine.
Psychiatric trainees in Iraq face many challenges that limit their immediate access to improved training opportunities. These include limited access to classroom teaching, regular clinical supervision meetings and fewer opportunities to attend international conferences and placements. These challenges are more acute in those specialities with the greatest shortage of consultants (for example, forensic and child and adolescent psychiatry).
Furthermore, the fragile security situation in the capital and larger cities and the post-conflict disruption to educational institutions consequent to these difficulties makes it difficult for those in the UK and elsewhere to visit the country and support educators and training on the ground.
Against this background and as a medical educational team in the UK (Oxford University Medical Education Fellows, OUMEF) with an interest in developing training opportunities for peers and colleagues in Iraq, we set up the Oxford Psychiatry in Iraq (OxPIQ) Project, beginning with a project development team that included Medicine Africa, an experienced online distance learning platform.
So what is the role of TEL in the delivery of online distance learning targeted at medical professionals in these circumstances?
Meeting the Challenge – the role of TEL
The concept of Technology-enhanced Learning (TEL), or Web-based learning (WBL), defined as the use of information and communication technologies in teaching and learning 1, is a relatively new phenomenon. Nevertheless, there is a considerable body of evidence supporting the use of TEL in various clinical and non-clinical settings.
Mccutcheon et al. 2 systematically reviewed thirteen studies and found that ten of these studies concluded that online learning is as effective as traditional or classroom teaching, despite the limitations of some of these studies.
In a large meta-analysis, Means and colleagues 3 concluded that students using online teaching performed modestly better compared to students learning similar material using face-to-face teaching. Combining face-to-face and online teaching resulted in larger benefit compared to the use of face to face methods only.
TEL can address the learning limitations in classroom settings due to expanding curriculum coverage and limits on contact time between students and lecturers/trainers alike. It can contribute to better use of such face-to-face classroom contact through the facilitation of the flipped classroom approach. 4 In this approach (also called inverted instruction and upside-down teaching), students acquire the basic information of the lesson outside the class (usually using online materials) and then develop their knowledge further in the class by sharing their learning, interacting with other classmates and teacher, and discussing various aspects of the study topic.These advantages have enabled TEL to revolutionise distance learning at many levels – enabling greater access to education by overcoming geographical and time-zone boundaries.
An allied concept within distance TEL is the concept of virtual teams 5 where health professionals come together to teach and learn from each other independent of location. Of itself, this offers some advantages. These include the possibility of addressing speciality-specific training gaps through the incorporation of the relevant expertise within the team - and to the creation of what is termed “connectivism”. This term refers to the use of internet technologies to enhance learning through online peer networks 6 and the development of communities of practice. 7 The latter allows for workplace-based learning with trainees learning from more experienced practitioners and moving towards the same through greater competency acquisition.
In a similar vein, creating networks of professionals may help to establish more longer-lasting relationships of mutual benefit between the UK and Iraqi professionals (e.g. through collaboration on training programmes, conferences, etc.). Also, cross-cultural online learning has been shown to be very useful in improving language skills and cultural awareness of learners and educators. 8 With language translation technology, any language difficulties can also be overcome, especially if the educator can observe the learners’ responses to the translated text and offered the opportunity to give further explanations and clarifications when necessary. 9 Finally, as well as sharing knowledge and experience within groups, TEL enables opportunities for mentoring and coaching individuals. 10
For our purposes, these findings and opinions support the use of online learning as a suitable distance learning “add-on” to existing training opportunities in Iraq.
TEL and Learning Theories
Learning theorists suggest that experiential and constructive learning theories are most appropriate to learning in the clinical context. Both are possible with TEL (as well as being facilitative of behaviourist and cognitivist approaches).
For example, the virtual classroom environment can enhance the learning experience of the participants by improving their analytical skills by thinking through case formulation and management plans. 11 Participants in online learning could be assessed and receive the feedback immediately. Ideas can be shared, and there is no passive acquisition or transfer of knowledge as is the case with traditional lectures. These aspects have implications for the design of the educational sessions and are discussed below in the learning methods section.
Challenges of Online Distance Learning
There are many challenges associated with online distance learning. Firstly, there is the potential lack of the required technologies (internet access, laptops or desktop computers), the expenses of subscribing to these online learning templates, the need to have technical support, and similar technical and logistic issues. 12 These technical problems may impair access to and functioning of the virtual team. The choice of an experienced online platform must, therefore, be considered carefully.
Secondly, there may be ethical issues about the protection of patients’ confidentiality in these sessions, especially when there are different laws of privacy that are applied in the UK and Iraq. This will require knowledge of the relevant professional requirements by the tutor team for example.
Furthermore, the student-teacher relationship has traditionally been underpinned by direct face-to-face contact and being present at the same time and place. 11 Therefore, learners and educators might be less satisfied with online learning. For these reasons, the concept of blended learning (careful integration of online learning with face to face learning experience) has been developed to overcome the limitations of a standalone online or face to face learning and has been found effective and applicable in various settings. 13
Thirdly, any distance online learning programme must understand and support existing “local” training provision and arrangements, in the classroom and the workplace. This requires liaison and cooperation with the training providers and institutions on the ground.
For clinical training to be relevant, it needs to reflect the learning needs of trainees in the workplace – in keeping with adult learning principles and cognitive apprenticeship models of learning. 14 The latter includes the importance of clinical decision-making underscored by the higher levels of Bloom’s (1956) cognitive domain. 15 To this end, then appropriate learning and assessment methods are needed to enable effecting learning.
In other words, while necessary, TEL may be insufficient in enhancing learning outcomes if allied learning methods are not chosen appropriately. Also, in our view, TEL is not a substitute for bedside teaching.
Table 1 summarises this appraisal of online distance learning (using the online platform provided by MedicineAfrica).
Table 1 Strengths and limitation of using MedicineAfrica (web-based virtual classroom environment)
Strengths
Limitations
Better use of the participants time and resources
Limited or lack of internet access
Overcome geographical barriers between two countries
Technical and logistic issues
Improve critical thinking and communication skills
Subscription expenses Appropriate choice of learning methods
Form long-standing professional networks
Ethical and legal issues (e.g., confidentiality)
Interactivity
Lack of direct face to face contact
OxPIQ & Project Development Team
OxPIQ is a partnership between Medicine Africa and psychiatrist members of the Oxford University Medical Education Fellows, with experience of working in Iraq. The Oxford University Medical Education Fellows (http://OUMEF.org) is a group of trainees from across medical and surgical specialities with interest in medical education and training.
Medicine Africa (http://medicineafrica.com) is an innovative clinically targeted online platform developed in collaboration with King’s College London’s Centre for Global Health, within the King’s Somaliland Partnership. Built at low bandwidth, it enables collaboration between medical professionals in the UK and those in remote or fragile states to enhance education in various clinical specialities using online sessions (live courses and mentoring sessions). Please see Appendix 3 for a screenshot of one of the active sessions of OxPIQ.
The next step was to invite representation and support from the Iraqi Board of Psychiatry and the Medical Education Unit in Baghdad. These developments led to the formal launch of OxPIQ Partnership in March 2016. Later on, the many UK and Iraqi doctors joined the Partnership as tutors and learners.
The Virtual Learning Team: Trainees, Specialty Consultants & Tutors
Iraqi psychiatry trainees were then recruited, and their more pressing learning needs to be appraised based on their views and those of the Iraqi Board of Psychiatry supervisors. Learning needs to emerge included the management of older patients with dementia and functional disorders, assessment and management of children and adolescents (with autism and ADHD for example), forensic patients and those with drug and alcohol addiction. The team thus formed was composed of up to ten psychiatry trainees from Iraq and five senior psychiatrists/tutors each, from Iraq and the UK respectively. A schedule of fortnightly seminars was agreed and published on the learning platform. Case-based discussions were used as the main educational activity during these seminars.
Learning Methods and Processes
As noted earlier, the importance of experiential and constructivist learning methods are key to clinical education. Our literature appraisal revealed that they are essential elements of successful TEL in this context too. 16, 17 To these must be added learner engagement. 18
Virtual or online (anonymised) case-based discussions (CBDs) are valid and reliable learning tools. 16 They are interactive and centred around the students and their learning needs while a facilitator guides the process of learning. Learners are engaged through discussion of actual clinical cases, so preparing learners for real-life experience. 19 Also, expert facilitation and peer feedback to trainees promotes clinical knowledge and skills’ development. 20, 21
Effective small group teaching is characterised by four main strengths: flexibility, interaction, reflexivity and engagement. 22 Flexibility is when the teacher responds to the needs and learning of the students dynamically and helps them to explore wider pedagogic spaces. A higher degree of interactivity is usually seen in small group teaching compared to a larger group. Teachers are better able to continually engage in self-reflection and listen sensitively to students in a small group and observe the dynamics between the members of the group, leading therefore to better reflexivity. Engagement refers to encouraging the students to develop their academic identity and engage in lively debate about the various aspects of the topic discussed.
We aimed to replicate these characteristics. For example, a small group discussion allowed better interaction with each participant (interactivity); the presence of chat windows enables the facilitator to self-reflect on the process, monitor engagement and respond reflexively using questions and answers to stimulate interest and respond flexibly to individual trainee knowledge gaps. Tutors are encouraged to identify trainees’ learning needs and facilitate interactivity, and timely feedback as these are highly valued by the participants and help to keep them motivated and engaged. 18
For further reading in this area, we recommend Brindly and colleagues’ 23 ten strategies to increase students’ motivation towards and engagement with online learning (see table 2).
Table 2- Strategies to increase engagement in online teaching (modified from Brindly and colleagues, 2009) 23
1. Transparency of expectations: Making the learning objectives very clear and relevant to the participants learning needs. The teachers must be open to the learners’ suggestions and must be willing to discuss the process and purpose of the educational activities.
2. Clear instructions: The educational activity, its timing, duration, and the technical aspects are described in detail to the participants. They should not be left to ‘try out things’ and must be guided explicitly.
3. Appropriateness of task for group work: For the online activity to succeed, individual versus group tasks should be differentiated. In our example, this may be done by asking the participants to do a particular task before the session (e.g., read about severe and enduring mental illness), and then to work together on producing a formulation for the case discussed. This will increase their motivation to be involved in various tasks.
4. Meaning-making/relevance: The case-based discussions (and any online activity) should have relevance for the participants and aim to enrich their experience in their clinical work.
5. The motivation for participation embedded in course design: It is essential that participants in the online activity understand that the success of the group and the course depend on the individual effort of each participant.
6. The readiness of learners for group work: This aspect describes the development of a sense of community through a professional relationship which leads to better collaborative work.
7. The timing of group formation: Before the participants join in the educational activity, it is preferable to have some discussions before the tutorial on their learning needs to allow a time for rapport to develop to enable better group activities.
8. Respect for the autonomy of learners: Joining and leaving the educational activity (and the whole online course) should be voluntary. No penalties should be attached to leaving the course. Learners should have the freedom to choose what aspects of the online course is relevant to them.
9. Monitoring and feedback: The tutor should monitor the progress of the participants, and timely feedback is given respectfully to enhance the engagement and motivation of the participants. Please see Appendix 1 (lesson plan) for more details on feedback and evaluation.
10. Sufficient time for the task: Participants should be given time to be actively involved in the session. This is particularly important in a distant learning session when issues related to sound quality or speed of internet connection may prevent some participants from engagement.
The focus of the Lesson Plan Design
To these ends, the focus on the lesson design was on using problem-based learning methods (e.g. CBDs) within a small group setting (between 4-12 members) and a format that promoted learner engagement. A sample lesson plan is provided in Appendix 1.
In practical terms, tutorials were held fortnightly in term-time. All participants received an email notification to inform them of the session topic, and the tutor uploaded the slides from the session to the website beforehand. Participants logged-in to the site (http://medicineafrica.com) and interact with the tutor by voice (requiring only simple microphone equipment) and by writing in a chat window.
Evaluation and feedback gathering
The evaluation of the effectiveness of these sessions was reliant originally on trainees’ immediate reaction (table 3, level 1 evaluation, Kirkpatrick 24) using formal feedback tools provided online by MedicineAfrica. This feedback was shared with tutors and the Project Team. Please see Appendix 2 for the template used in collecting feedback after each session.
Subsequently, members of the project team approached trainee representatives, tutors and Iraqi Psychiatry Board leads separately for further feedback and appraisal of learning needs. Furthermore, some months after a tutorial we have asked trainees for evidence of learning across the higher levels of Kirkpatrick’s evaluation model.
Regular feedback from the Iraqi and UK participants has been positive. The sessions have been associated with improved clinical knowledge and skills of the Iraqi Psychiatry Trainees. Requests for certificates of tutorial participation have been agreed upon and provided by the project team addition, so supporting learners’ (and tutors) portfolio development.
Table 3 Kirkpatrick’s (1996) Levels of Training Assessment
Level
How to assess
Level 1: Reaction (the participants feeling about the training
Feedback during and after the tutorial using the feedback questionnaire
Level 2: Learning (improving the participants’ knowledge)
Post-tutorial questionnaire and interviews
Level 3: Behaviour-also called Transfer (improving the participant's performance)
Direct or indirect observation and assessment of the skills and competencies of the trainees
Level 4: Results (cost-effectiveness, engagement, sustainability, adherence to evidence-based practices)
regular meetings between the participants, tutors, and stakeholders.
Further cooperation
A surprising (and very welcome) outcome of the project was, through the facilitation and support of the Iraqi Board of Psychiatry, the introduction of educational workshops in Baghdad. These workshops were held in Medical City, Baghdad, in May 2017 and April 2018 and were facilitated by tutors (YH & H Al-T) from the OxPIQ Partnership. They covered targeted topics such as old age psychiatry, addiction, organic and forensic psychiatry. Trainees and senior psychiatrists from Iraq attended; their feedback showed how they valued the interactive nature of the teaching and use of CBDs as learning methods, resulting in high levels of engagement.
Conclusions
This paper describes the process of designing, delivering, and the early evaluation of an online distance TEL programme for mental health professionals based in the UK and Iraq.
TEL has had an important role in overcoming the geographical barriers and other challenges to developing training opportunities in Iraq and other developing countries. We are of the view that it could be used more often to connect professionals working in similar circumstances and with other disadvantaged groups, including refugee and asylum seekers. It is a flexible way of providing training to professionals working with those groups in relatively remote and resource-deprived environments.
Greenhalgh 25 suggests that three factors are needed for the success of online educational activity: ease of access, perceived usefulness of the activity to the learning requirements of the students, and the interactivity of the session. In our experience, these are important. Also, we believe that additional consideration should be given to (i) working with an experienced online platform provider; (ii) working with local educational institutions, trainers and learners to identify unmet learning needs and support existing learning opportunities/programmes; and (iii) adopting an iterative approach to feedback and evaluation.
Appendix 1: Example of a Lesson Plan
Session title
Case-based discussion on management of severe and enduring mental illness.
Duration of session
60 minutes
Tutor
A UK-based Psychiatrist
Learner group
Psychiatry Board Trainees and Senior Psychiatrists in Iraq and UK
Step 1– Learning outcomes
a) Describe the various stages in the management of the cases discussed during the session.
b) Enhance the participants learning using case-based discussion with peers and seniors in the UK and Iraq.
c) Improve the presentation and discussion skills of the participants and their communication skills.
d) Explore ethical, cultural, and social issues related to the management of mental disorders and improve cultural competency and awareness.
Step 2 – Learning Plan
Introduction to the online tutorial -10 minutes
a) Highlight the learning objectives of the tutorial
b) Stimulate the thinking of the participants by asking about their current knowledge of the subject, whether they managed similar cases in their clinical work, and what are their learning needs.
c) Outline the tutorial structure and further engage the participants by informing them about other details (e.g., if they can ask the question during or after the case presentation)
2. The tutorial in a case with severe and enduring mental disorder – 30 minutes
a) Participants are encouraged to interact with the tutor who should be invited to keep the tutorial interactive.
b) The case presented will provide an overview of the patient’s journey from the initial presentation, followed by the investigation, then treatment plans. Discussions of the differential diagnosis are important.
c) The tutor will assess the knowledge of the participants by asking questions on the various aspects of the case presentation (e.g., what is your differential diagnosis for a patient presenting with auditory and visual hallucination? What investigations would you request?).
3. Recap and Q&A time- 20 minutes
a) Tutor to give a summary of the main learning points from the tutorial and linking these to the learning outcomes presented at the beginning.
b) Participants are given enough time to ask questions and to participate actively in the session.
Step 3 – Assessment
Before Lesson
Before the tutorial, the tutor should know the current educational curriculum of the participants and their learning outcomes in that subject. UK and Iraqi Psychiatry curriculum are different, and therefore knowing what is relevant is important.
Stating the learning outcomes at the beginning of the tutorial will also help in the baseline assessment of the knowledge and skills of the participants.
Pre-session questionnaires could be used as well (for example, asking questions on the prognosis of various mental disorders and comparing the participant’s knowledge before and after the session).
After the lesson
· Ongoing assessment during the tutorial using questions on various aspects related to the case presented.
· Questions in the recap section at the end of the tutorial.
· Post tutorial feedback forms will allow the participants to give their views about their learning needs and if they feel the tutorial was relevant to their learning outcomes.
It is important to provide personalised feedback to the participants about their performance on these assessment tools as this will help them to identify gaps in their knowledge and improve their learning. 26
Step 4 – Resources required
MedicineAfrica is free to join and designed to work well even with low bandwidth. Hence it won’t be affected by slow internet connections which are likely to be the case in developing countries.
Trainees and Tutors will need a computer (desktop or laptop) with an internet connection. No other resources are needed. Recommended readings could be disseminated by email to the trainees after the session.
Step 5 – Evaluation
Student evaluation
Gathering feedback is an essential step to influence the learning outcomes favourable and continue to improve the structure and content of the tutorials (After the tutorial, the participants will be asked to fill an electronic feedback form (please see Appendix 2).
The form contains various questions with rating (from 1-5, ranging from strongly disagree to strongly agree) on various aspects of the tutorial. These include structure, organisation, the range of aids used and meeting of the learning outcomes.
Also, direct feedback from the trainees, tutors, facilitators, and the stakeholders responsible for running the online learning platform is gathered to assess the effectiveness of these tutorials.
Teacher evaluation
Professionals invest a significant amount of time and efforts in these lessons, and it is imperative to assess how the tutorials could be improved to meet the needs of the trainees and keep them and the tutors motivated and interested. Tutors in these tutorials meet regularly using Skype to reflect on their teaching sessions and discuss ways of improving the delivery and quality of the tutorials.
Mutual learning is another aspect that needs to be assessed (is the tutor also benefitting from these lessons, for example, by improving their cultural competencies or their teaching skills).
Appendix 2: Feedback form to be completed by the participants after the session
Session title
Case-based discussion on management of severe and enduring mental illness.
Speaker
Date
Content
The session was relevant to my training needs
Strongly disagree 1 2 3 4 5 Strongly agree
Organisation
Sufficient time was allowed for the session
Strongly disagree 1 2 3 4 5 Strongly agree
Presentation
The session was well presented
Strongly disagree 1 2 3 4 5 Strongly agree
The session was delivered at the right pace
Strongly disagree 1 2 3 4 5 Strongly agree
The session was interactive and encouraged discussion/questions
Strongly disagree 1 2 3 4 5 Strongly agree
Structure
The session was well organised and structured
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were clear
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were met
Strongly disagree 1 2 3 4 5 Strongly agree
Overall evaluation
Overall, I would rate this session as
Extremely poor 1 2 3 4 5 Extremely good
Appendix 3: MedicineAfrica screenshot during an active session
Epidural anaesthesia is one of the favored and effective treatment options for labour pain. It is usually safe and only a handful situations lead to absolute contraindications to this technique such as patient’s refusal, lack of expertise and equipment, severe coagulopathy and infection at the site of puncture (1). However, as with any other technique and procedure, epidural anaesthesia is not flawless. The side effects and complications include hypotension, pruritus, inadequate analgesia, post puncture headache, nerve damage, infection, and epidural haematoma (1,2). Headache is common in one third of the patients after lumbar puncture however, the frequency is less in epidural anaesthesia as the fluid is injected in and not removed in the latter (3). Accidental dural damage and subsequent headache following epidural anaesthesia is uncommon and is an important cause of morbidity which can limit patient severely. Further, in rarest of rare cases Pneumocephalus can develop after epidural anaesthesia which has rarely been reported. We report a patient who developed Pneumocephalus after receiving epidural anaesthesia for labour pain.
Case Report:
A 39 year old female presented to our Emergency Department with severe headache not responsive to analgesics. The headache started developing 10 to 12 hours after she was given an epidural which was attempted three times for labour pain which was four days prior at a nearby medical center . The severity of the headache did not change with lying or the upright position. She had no symptoms of vomiting, no fever and no confusion. Neurological examination and vital signs were unremarkable. The site of the spinal anaesthesia did not reveal any swelling or any signs of infection. An urgent head CT scan was performed which revealed Pneumocephalus denoted by numerous left fronto-parietal extra axial air locules (Figure 1 and Figure 2). MRI spine revealed mild subcutaneous oedema at the site of the needle insertion without any haemorrhage or collection. The patient was admitted and treated conservatively for six days and follow up serial head CT scans showed complete resorption of the Pneumocephalus and the patient’s symptoms resolved completely. The patient was discharged and the follow up was uneventful.
Figure 1: Pneumocephalus seen as locules of air (black color) in the left fronto-parietal region denoted by arrows (Axial section)
Figure 2: Multiple pockets of air seen in the Saggital section marked by arrows demonstrate the Pneumocephalus.
Discussion:
Pneumocephalus is the presence of air in the intracranial cavity. It can be acute ( less than72 hours ) or delayed (more than 72 hours). The most common site is the frontal region (4). Plain skull x-rays can detect Pneumocephalus of about 2 ml, whereas it requires only 0.5 ml of air to be detected by a CT scan (5). Pneumocephalus is most commonly a result of traumatic brain injury, surgical intervention of the brain or infection (5). Trauma accounts for up to 75% percent of the total cases. Chronic infections of ENT especially otitis media also amounts to a number of significant cases. Surgical procedures of brain, spine and ENT like sinus surgery, nasal polypectomy and nasal septum resection accounts for the causes. The incidence after supratentorial craniotomy has been reported to be 100% (6, 7). However, it is very unusual for pneumocephalus to develop post epidural anaeasthesia possibly due to ball valve mechanism in which the air enters the space through the CSF leakage which allows input but not output. Headache post lumbar puncture and epidural anaesthesia is relatively not uncommon but certain situations may demand a more thoughtful approach (3).
In our patient we suspect there was a puncture of the dura during epidural anaesthesia which led to air being trapped and siphoned upwards in an inverted soda bottle fashion. This is supported by the meta-analysis done by Choi et al. which states the incidence of accidental dural puncture in epidural insertion to be 1.5% and among those 52 % will have post puncture headaches (8). In another extensive study performed over ten years, the overall incidence of accidental dural puncture and postdural puncture headache were 0.32% and 0.38%, respectively (9). The authors further stressed that if more than one attempt was required to identify the epidural space, the accidental dural puncture rate increased to 0.91%. In our patient we witnessed the same wherein three attempts were made to identify the epidural space which increased the risk of dural injury and subsequent leaking. Pneumocephalus usually gets absorbed without any clinical manifestations. The conservative treatment involves placing the patient at rest, avoiding Valsalva manoeuver, administering analgesics. With these measures, reabsorption was observed in 85% of cases after 2–3 weeks (5). Use of oxygen mask, nasal catheter, hyperbaric oxygen sessions and good hydration have also been reported. If conservative measures fail to provide the desired results then specific treatment like a epidural blood patch or even surgical closure of the dural gap is indicated (3, 10).
The recent increase in the number of patients presenting with a borderline personality disorder (BPD) in general adult psychiatry and primary care is creating pressure within the National Health Service (NHS)1.Currently, BPD is perceived to be like an ‘epidemic’ entity, particularly in areas with a high incidence of socioeconomic deprivation. Similarly, there is a parallel increase in the human and medical resources needed to manage this disorder efficiently. In fact, the authors have found that BPD tends to be comorbid with factitious disorders and depression (Tripolar syndrome) with a tendency to overuse hospital and medical facilities, inclusive of Accident and Emergency (A&E) departments, family doctors and General Practitioner (GP) surgeries2.
Consequently, patients with BPD require a constant and unlimited allocation of medical and psychiatric resources, together with targeted care plans. In fact, they might be prone to frequent self-referrals to A&E, seek hospital admissions and augment all their psychotropic medications in order to deal with their on-going crises not solvable in their homes. Also, the skills needed by healthcare personnel to reduce chronic self-harming and suicidal ideation in this vulnerable population are complex and need to be updated on an on-going basis also due to the tendency of these patients to raise allegations towards their healthcarers3. Nonetheless, the provision of treatment is often hindered by various healthcare system limitations, such as the lack of beds on medical and psychiatric units, forced reduction in the length of stay in a hospital and insufficient human resources. This scenario has mostly affected female patients with BPD who seek admission to psychiatric hospitals often for respite from chronic suicidal ideation4.Moments of amplified suicidal ideas become evident when internal voices, perceived as auditory hallucinations commanding to self-harm or to commit suicide, become more intense5.
As observed by the authors of the current editorial, increased suicidal ideation in persons with BPD also occurs during minor crises in life, when experiencing intensified flashbacks about past abuses, during minor losses, after significant conflicts with others and after the separation from influential people in their social network. Besides, admissions in psychiatric wards, very commonly, occur when there is an intensification of internal voices commanding BPD patients to take overdoses of the prescribed medication or to jump in front of a train, a car or off a pier to commit suicide. Police is often involved to stop these dramatic plans. At the same time, healthcare professionals are discouraged by the complex management of patients with BPD, which, in combination with their tendency to challenge or make unwarranted allegations against their health carers, results in feelings of sadness, rejection and alarm in the latter. Kanin reported that the reason to produce a false allegation is to create a defence or to get compassion6. Nonetheless, it is also likely that some healthcare professionals might have some preconceived ideas about people with Borderline Personality Disorder, which might reduce the depth of health carers’ empathy towards these patients and lead to burnout after prolonged treatment of BPD in hospital or community. Attempts to treat and to reduce suicidal ideation and self-harm in this group of patients are often thwarted as they challenge medical decisions and endeavour to sabotage the proposed care plans. The strain on the doctor-patient relationship is determined by the underlying ‘Mistrust/Abuse’ scheme of patients with BPD who expect from others, and are thus sensitive to, signals of relational wound, treachery and abuse7.
Consequently, a chronic feeling of inadequacy in patients with BPD translates itself in enduring dissatisfaction with any therapy and healthcare professionals. Hence, in the authors’ experience, any attempt to establish a long-term therapeutic relationship with BPD patients might have limited outcomes. Frustration in healthcare professionals aiming to create an enduring therapeutic alliance with patients with BPD happens as these patients tend to interpersonal biases and to ascribe undesirable experiences to people (hence to healthcare professionals) as opposed to circumstances8. Therefore, social interactions with primary carers result in dissatisfaction of people with BPD about any medical or psychiatric plan is set up for them. Consequently, community teams, general practitioners and hospital staff feel hopeless due to recurrent readmissions of people with BPD and the lack of definitive treatment for such pathology. Stress caused by difficulties encountered in ensuring that BPD patients comply with the therapy regularly places doctors and nurses at crisis point.
Once in the hospital, discharging patients with BPD can be difficult as they are frequently reluctant to return to the community, leading to recurrent readmissions within a short period. In fact, the period before discharge from a psychiatric hospital is complicated by mounting anxiety and distress in patients with BPD. The authors observed a regular escalation of self-harming behaviours and increased suicidal ideation in these patients just before discharge, possibly indicating their underlying anxiety in going back to the home environment. Many BPD patients suggest that they would rather stay in the hospital instead of returning to the community that is considered by them as unsafe or unstructured. Furthermore, as these patients have an intense vulnerability to social rejection, they rarely feel adequate during social interactions thus developing an enduring sense of solitude9. Therefore, any hospital discharge or a visit to the GP will be interpreted by them as disappointing and will lead patients with BPD to confirm their sense of rejection. As a reaction, the authors observed that BPD patients demand endless and unconditional attention from their primary carers. Attempts by patients with BPD to self-harm or commit suicide intensify over weekends or public holidays as their sense of solitude increases during these periods, especially when there is also a shortage of healthcare professionals available for immediate support.
The authors of the current editorial propose possible strategies of intervention both on the psychopharmacological and managerial side. The challenge is that patients with BPD often use overdoses of oral medication in a suicide attempt10. Hence, the authors recommend the use of long-lasting depot antipsychotic injections (e.g., Zuclopenthixol Decanoate) to stabilise their mood and reduce impulsivity, the risk of overdoses, pseudo-psychotic symptoms and command hallucinations leading to deliberate self-harm. The use of oral lithium to treat mood swings poses an ethical dilemma for doctors as it could be lethal when used as an overdose. Healthcare management is another way of intervention. One point of difficulty is the tendency of patients with BPD to split their teams and to create niches of protectors and opposers within staff with possible conflicts within the team that is treating them. In this case, inter-professional coordination, integrated care and constant information sharing are required11. Furthermore, several healthcare services treating patients with BPD are trying to find an integrated approach for their hospital and community treatment. The authors speculate that the increased number of admissions of patients with BPD is reducing the total capabilities of physical and mental wards to treat patients with other pathologies. Besides, the dramatic presentation of patients with BPD who tend to overuse the healthcare services poses ethical dilemmas in their management. This scenario has created discrepancies in health care policies about treatments and hospital (re)admissions of patients with BPD reaching an epidemic magnitude in many healthcare trusts. Hence, a new culture is required for the management and treatment of patients with BPD in the community.
Culture is defined as the character of an institution that affects employee gratification and organisational accomplishments12.What is needed is a frank and constructive dialogue between healthcare managers, leaders and medical staff in the hospital and in the community. Furthermore, clear and regional guidelines should exist to improve the efficacy of care which is offered to BPD patients at home and to reduce the constant risks which patients pose to themselves, their sense of solitude and their tendency to seek hospital admission in order to solve chronic existential difficulties. A model of integrated care comes from Max Weber who differentiated between ‘formal rationality’, the endorsement by healthcare managers of the most efficient ways of achieving organisational goals (e.g., ensuring more hospital beds by quick discharges of ‘bed blockers’), and ‘substantive rationality’, the expectation by healthcare professionals that values and morals should instead be based on tradition, compassion and dedication13;pertinent to the care of BPD patients in our case. The collaboration of all those involved parties is also important to reduce the risk of ‘silo management’ where confined and regional policies do not embrace a wider perspective for the management of specific problems while responding only within the confines of the own guidelines and procedures14.In these cases, integrated care in communities can halt self-harming and suicidal attempts of patients with BPD. The organigram sees inter-professional actions, targeted psychopharmacological policies and psychiatric crisis teams in A&E that can reduce the need to hospitalise patients with BPD at any ensuing crisis.
Physicians pursue the interest that during the hospital stay the best patient care needs to be provided; and achieving that in a short time - as a result the patient is expected to recover from illness and return to normal life.
The ability to prevent possible complications that the patients are exposed to, has always generated ambiguity in the current medical practice, since it is assumed, that the relief of the patients once the treatment is established, should always be the same1. However, it is the awareness and proper care of comorbidities and the baseline condition of the patients that determine the success rate of the treatment, without requiring additional interventions beyond the ones proposed at the beginning of the treatment 2, 3.
This important factor has generated in practitioners the need to be able to monitor the clinical evolution of the patients. Laboratory tests are an important basis of medical diagnosis, and are frequently used to monitor the clinical progress of the hospitalised patient. The patient clinical state sometimes changes suddenly or continuously; requiring the surveillance of the basic variables such as vital signs. Vital signs monitoring activate a warning signal for the immediate reassessment of the patient and reorient the medical decisions at any moment during the hospitalisation, with the goal of avoiding further deterioration or adequately treating any new disease state that the patient may develop 3, 4.
From that point of view and long time ago the medical community has observed the need to generate a code that could be universal and that could be used as an early warning of the patient worsening. As a result of this situation, in different countries around the world, researchers and clinicians have developed scales, scores, algorithms and others tools to identify early patients in risks to be in critical conditions. Those tools are based on the ability of easy data collection and simple clinical interpretations allowing the clinical personnel to make objective and early assessment of the overall clinical state of the patients 4.
These scales or scores are not ideal, since there is no perfect scale, and all have statistical weaknesses either in their sensitivity or specificity. The clinical judgment and the physician experience, added to a score from any of these scales, may guide the path to follow according to the particular scenario to treat the patient illness 5.
Selecting the ideal scale to be adopted is one of the controversial topics in which a practitioners and institutions can be involved in. Occasionally other services in the hospital such as clinical laboratory and clinical imaging values play an important role in the process of diagnosis of the disease and are counted in the risk scales making easier to have good standard of care. Scientific studies assess the statistical performance of these scales yield controversial results that sometimes distort or endorse these results 5. This is why the decision of the ideal scale is based first on the target population that physicians in charge will care of and select the appropriate scale or score that will be applied, to know the implications of the most representative age group of patients that will be attended and to use scales which data acquisition be a simple and quick task to perform6.
Based on that, the Royal College of Physicians of the United Kingdom headed by Bryan Williams and collaborators, and many other researchers worldwide have analysed a significant number of scales on the basis that the scale should use systems (track and trigger warning systems protocol) divided into three types. Single parameter systems, multi-parameter systems, total weighted scoring systems and combined systems 6.
The researchers came to the conclusion that the performance of these scales was better than those that conserve the third type of system, since not only the parameters are categorized but also those who develop the scale proposed management to be carried out in an easy, orderly scheme and logical within a framework of independent work or in addition to more robust strategies that involve management schemes within a hospital institutions - the so-called (Rapid Response Systems RRS) 7.
For Williams et al, the MEWS changed its name after being accepted by the Royal College of Physicians of the United Kingdom as the NEWS scale with its variables defined as (respiratory rate, oxygen saturation, systolic blood pressure, heart rate, consciousness or new confusion and temperature). This score has been recognized and quickly adopted worldwide. The NEWS has an immediate applicability as a parameter of high sensitivity in the detection of clinical deterioration, despite its known low specificity. Thus inviting the attending physician to approach and reassess the state of the patient. The score makes changes in medical decisions according to the new conditions found during the patient’s assessment7.
This kind of scales must be endorsed internationally and be easily replicable by all practitioners who wish to adopt them. This allows other physicians to obtain results when implementing actions, reaching better clinical outcomes similar to clinical studies previously published. In the daily practice and clinical application we find different scenarios to use the scales, where the main problem of its application represent extra costs in lab test or clinical images and the time invested by the practitioners and medical personnel 7.
For this reason, the scales for clinical assessment should be easy and flexible to be implemented by any person, ideally for any member of the healthcare team to avoid barriers during the process of data acquisition. From this perspective, the scales that are based on easily collected parameters are the most appropriate, but they are often the scales that suffer the rigors of the biases when they are undervalued or overvalued, just the operability can be affected by personnel knowledge and skill.
The interesting thing about this exercise is to see that the people who have the most continuous contact with the patient, such as the nursing staff, physicians with the practice have the ability to use them in their practice and this would make the scales a valuable resource to perform clinical assessments and achieve the goal proposed.
In this new era where the reincorporation of a patient into daily life in a short time is ideal scenario, the medical and nurse staffs and also service providers seek to alleviate the patient's health breakdown. It is here from the hospital point of view where the proper care not only in the quality of care but also in the prevention of complications plays an important role in the applicability of these early detection scales. This is an invitation to success from its inception and to tend to patients being hospitalized for the minimum time required.
A dermatoscope is a hand-held device for examining the appearance of the skin. Dermoscopy has become an increasingly used and valued tool in the assessment of various skin lesions, and more recently, inflammatory rashes. It is quick, cheap and when used correctly, dermoscopy is an essential tool in helping clinicians detect early stage skin cancer. Various national and international guidelines recommend routine use of dermoscopy in the assessment of pigmented lesions1,2 because it enhances melanoma detection rates3,4 and can help confirm the diagnosis of benign lesions such as haemangiomas and seborrhoeic keratoses. As with any skill, competency takes time to develop and a combination of various learning and assessment methods is best. The dermatology specialist training curriculum in the United Kingdom (UK) states that trainees should be competent in using a dermatoscope and interpreting findings, while recognizing the limitations of this tool5. Assessment of these clinical skill and behavioural competencies using direct observation of procedural skills (DOPS), case-based discussion (CBD), mini clinical examination (mini-CEX), and/or multisource feedback (MSF) is suggested. There is no specific guidance on what resources a trainee should use to achieve these competencies, nor on what is the minimum expected dermoscopy skillset at completion of specialist training.
The aim of this survey was to explore dermoscopy use amongst dermatology specialist trainee registrars in the UK including frequency of use, how it is being taught and whether trainees feel their dermoscopy training has been adequate.
An online survey was designed and distributed to dermatology trainees in the United Kingdom using an email link and hard copies were distributed at a national dermoscopy course. Respondents who did not identify themselves as dermatology trainees were removed from the analysis. Responses were collected anonymously, then collated and analysed using SurveyMonkey® computer software.
Twenty-five percent (59/238) of dermatology trainees completed the survey. On average, 92% (54/59) use dermoscopy more than once daily. Eighty-five percent (50/59) always use dermoscopy when assessing pigmented lesions while 34% (20/59) always and 59% (35/59) sometimes use it to assess non-pigmented lesions. When asked about specific tools used to learn dermoscopy, 41% (24/59) have been on a previous course, 42% (25/59) reported attendance at a lecture or seminar, 46% (27/59) have used a dermoscopy text book, 14% (8/59) have attended a conference, 19% (11/59) have used online resources. Seventeen percent (10/59) have never used any of the above learning methods. (Figure 1a). Amongst those who have attended a formal dermoscopy course (n=24), 92% (22/24) of these were ≤1 day in duration. When questioned about informal teaching in clinical practice, 12% (7/59) frequently, 56% (33/59) sometimes, 31% (18/59) rarely and 2% (1/59) never receive teaching from their supervising dermatology consultant. (Figure 1b). Fifty-four percent (32/59) feel they have received adequate training in dermoscopy while the remaining 46% (27/59) feel their dermoscopy training is inadequate for their training stage (Figure 1c). Seventy-three percent (43/59) have access to dermoscopic photography within their local dermatology department.
Fig 1a - Have you undertaken any formal study in dermoscopy? 49% of trainees have attended a lecture, 2% a seminar, 14% a conference, 41% a course, 19% have used an online resource, 46% have used a book, 17% have not used any resource.
Fig 1b- Do you receive dermoscopy training from your supervisor in clinic? 56% of trainees sometimes, 31% rarely, 12% frequently, and 2% have never received training from their seniors in clinic.
Fig 1c- Do you believe that you have received adequate training in the use of a dermoscopy for your training grade?
These results of this survey highlight the need for dermoscopy training to be reviewed within the UK national training curriculum for dermatology. Despite daily use by the vast majority, dermoscopy training is largely self-directed and highly variable amongst individual trainees. Of concern, a significant proportion of those who responded feel their dermoscopy skills are inadequate for their training stage. Of note, the 25% response rate means that the results of this survey may not be representative of dermatology trainees in the United Kingdom as a whole.
This is the first time that dermoscopy use has been explored through a national survey of dermatology trainees in the UK, to the best of our knowledge. A survey on dermoscopy use was carried out by The British Association of Dermatologists (BAD) in 20126 but the majority of responses were from dermatology consultants. This confirmed that 98.5% of respondents regularly used dermoscopy, while 81% had received any training. The most frequent source of training was UK based courses, which 62% of respondents reported attending. Of note, 39% of all respondents lacked confidence when making a diagnosis based on their interpretation of dermoscopy findings. It is not clear how many of those lacking in confidence were consultants, trainees or specialty doctors. Although the situation may have improved since 2012, these results do suggest that dermoscopy training needs have not been met for a proportion of doctors across the dermatology community.
Dermoscopy training is an important issue to address for several reasons. The volume of cutaneous lesions being referred to dermatology is increasing, and skin cancer referrals and treatment now account for 50% of a UK dermatologists’ workload7. For every melanoma diagnosed, a dermatologist may expect to see 20–40 benign lesions referred from general practitioners (GPs)7. These facts highlight the importance of maximising diagnostic skills which frequently include using dermoscopy as part of clinial assessment. Lack of adequate training is a common self-reported reason for dermatologists not using dermoscopy8. Both trainees and their supervising bodies have a responsibility to maximize training opportunities and embed the use of dermoscopy in routine practice.
In conclusion, we feel UK dermatology trainees and indeed any clinician who utilizes this tool, would benefit from a more standardized and integrated approach to dermoscopy teaching to ensure safe practice of this skill and deliver high quality evidence-based patient care.
With the increasing use of ultrasound as a standard examination in the first trimester, more incidental adnexal masses are detected. The reported incidence of adnexal masses in pregnancy varies, depending on the criteria used to define the mass. A literature review by Goh W. et al., found that 1% of all pregnancies are diagnosed with an adnexal mass 1. A more recent article has suggested adnexal masses are diagnosed in 5% of all pregnancies 2. Simple and functional cysts are very common, and they usually resolve after the first trimester 3. Mature teratomas are by far the most common persistent adnexal masses found in pregnancy 8. It has been estimated that up to 5% of adnexal masses in pregnancy are malignant 4.
Ovarian cysts are typically asymptomatic, but they can cause pain due to pressure on adjacent organs, rupture, bleeding or torsion. The latter case is a significant health condition which mainly requires emergency surgical intervention. During pregnancy, surgical management of ovarian cyst complications is more difficult and more challenging. This is mainly because of other differential diagnosis causing similar symptoms related to pregnancy such as ectopic pregnancy and miscarriage. In case of surgical intervention, the second trimester of pregnancy is supposed to be the safest window for surgery as the risk for drug-induced teratogenicity is smaller than in the first trimester, most functional cysts have disappeared by then and it is technically less difficult than operating during the third trimester 13.
Antenatally, ultrasound is considered to be the best first-line imaging to evaluate adnexal masses 5. Ovarian mass characterization into benign, malignant or borderline can be challenging in pregnancy. This is mainly due to the effect of high levels of gestational hormones which can cause decidualisation of the cystic or solid parts of the ovaries. Benign masses can mimic malignant masses due to this pregnancy related phenomena 12. One of the largest data in literature on ovarian mass characterization is published by the International Ovarian Tumor Analysis group (IOTA). All IOTA studies excluded pregnant women when they developed and validated the rules and models to characterize ovarian masses 14-17. This limits our knowledge and ability to use these models in pregnant women. It is known that tumour markers may be raised in pregnancy and should therefore not routinely been done 7. An alternative diagnostic tool is Magnetic Resonance Imaging (MRI) which is considered to be safe in pregnancy and can be helpful if the ultrasound imaging is inconclusive in evaluating whether a mass is benign or malignant 6; 10. The American College of Gynecology and Obstetrics recommends that pregnant patients should be reviewed on a case-to-case basis and stated that there are no known biological effects of MRI on fetuses. However, Gadolinium, which help in characterizing ovarian masses, should be avoided when examining a pregnant patient 11.
The aim of this retrospective study was to look into characteristics, size and subsequent management of cases of adnexal masses in early pregnancy.
Methods
This was a retrospective study of data collected between 12/01/2014 and 14/11/2016 in the Early Pregnancy and Gynaecology Unit (EPAGU) of a tertiary referral centre (Guy’s and St Thomas’ NHS Trust, GSTT) in central London. The Ultrasound reporting system (Astraia Software Gmbh, Version 1.24.10, Munich, Germany, 2016) was searched for data. Cases included were consecutive. The study was approved as a service evaluation audit by the Clinical Governance team at Guy’s and St Thomas’ NHS Trust. The study included women who were diagnosed with an adnexal mass while having a transvaginal ultrasound scan TVS at or before 15 weeks of gestation. Pregnancy was confirmed by a positive pregnancy test and an intrauterine gestation on transvaginal ultrasound scan. Women who had the first gestational TVS after 15 weeks of gestation, pregnancies of unknown location, ectopic or trophoblastic pregnancies and patients who had ovarian stimulation treatment were all excluded.
Repeat ultrasound scan reports were retrieved from the Astraia system. Further procedures, tests and imaging results were retrieved using the Electronic Patient Reporting system at GSTT (EPR application, iSOFT Group plc., USA, 2004), PACS (GE Medical Systems, Wisconsin, USA, 2006), Badgernet (Clevermed, Client version 2.9.1.0, Edinburgh, UK). We have used the subjective impression of the examiner as the index test. If surgery was performed the final outcome to identify benignity or malignancy was considered to be the histological diagnosis if any removed tissue. Cytology was used for a reference test in two cases when ovarian cysts were aspirated only. Borderline tumours were classified as malignant for statistical analysis. Tumours were classified using the criteria recommended by the World Health Organisation (WHO) 9; 10. All ultrasound scan images were available and reviewed by author TEG to confirm the US finding. For statistical analysis, the SPSS software package was used (version 24 for Windows, Chicago, IL, USA). A two tailed student’s t test was used to compare means in ovarian masses diameters and a p value of less than 0.05 was considered statistically significant.
Results
7150 patients underwent transvaginal scans for early pregnancy in that period. In total 48 cases of women with adnexal masses in pregnancy and completed data were analysed. Seven women have been excluded; one woman being postpartum at the time of the finding of a large endometrioma, five pregnancies due to assisted conception and one woman was found to have a corpus luteum cyst (Figure 1).
Figure 1: Study flow chart.
41 women with 46 ovarian cysts could be included in the study. Two women had bilateral ovarian cysts, one had two ipsilateral cysts and one woman had three ipsilateral cysts. The mean age at the time of detection of the ovarian mass was 30 (95%CI:28-32) (Fig.2).
Figure 2: Age distribution in the study group.
The mean gestation at the time of first ultrasound was 7.4 weeks (95%CI:6.6-8.3). The mean diameter of ovarian cysts measured 47.7mm (95%CI:39.9-55.4). In 36 women ultrasound alone was performed to reach diagnosis, one woman had an extra MRI scan, two women had tumour markers on top of the TVUS and in two women an MRI scan and tumour markers were performed after the TVUS. The ovarian cyst(s) was on the right ovary in 16/41 women, on the left in 22/41, bilateral in 2/41 and in one case the side of the cyst was not reported. The most common ultrasound subjective impression was mature teratoma (22/46 cysts), followed by simple cysts (12/46 cysts), haemorrhagic cysts (6/46 cysts), endometriomas (5/46 cysts) and one possible mucinous Borderline tumour. The latter was confirmed later on histology as the stage FIGO 1A intestinal type mucinous Borderline tumour (Fig.3).
Figure 3: Distribution of origin of cysts by histology.
In total 8/41 women (19.5%) underwent surgical intervention; of these eight cases six underwent major surgery under GA and two had a cyst aspiration under local anaesthesia. Seven out of these eight masses were classified as benign on USS and were subsequently confirmed to be benign by histology or cytology. In only one case a complex adnexal mass was found on USS examination at 9 weeks of gestation and the MRI scan reported possible malignancy. Tumour markers in this 23-year-old woman were normal and a laparotomy was performed at 17 weeks of gestation to remove the mass. Histology showed the mass to be a mucinous borderline tumour, FIGO stage IA. In another patient, an oophorectomy had to be performed at the time of the Caesarean section at term for fetal distress as the ovary was found to be necrotic. In this patient an ultrasound at 10 weeks of pregnancy had demonstrated a 6cm diameter haemorrhagic cyst, which had presumably torted during the pregnancy without any symptoms to prompt the patient to refer herself. Histology in this case had shown an infarcted cyst with fibrosis and calcification. In four of the major surgery cases performed under GA uncomplicated laparoscopies were performed to remove the adnexal mass; in one case a laparoscopic salpingoophorectomy was performed as an emergency for a suspected ovarian torsion at 16/40 weeks. In three cases a laparoscopic procedure for cystectomy was performed electively for ongoing pain. In the first case a cyst was diagnosed in early pregnancy subsequently there was a miscarriage and the cyst was removed 4 months after the diagnosis. In the second case a cyst was found in early pregnancy the woman had a termination at 11 weeks of pregnancy and a cystectomy 5 months later. In the third case a laparoscopic cystectomy was performed 8 weeks after the diagnosis, however the woman suffered a miscarriage at 12 weeks of gestation. Histology confirmed dermoid cysts in all four of these cases. The two cyst aspirations performed under local anaesthesia and ultrasound guidance were both symptomatic for torsion, one at nine weeks and one at ten weeks of pregnancy. In both patients the procedure has been successful. 33/41 (80.5%) with no indication for surgical intervention. There was a significant difference in the mean diameter of ovarian cysts in the expectant management group (41.2mm; 95%CI:34.7-47.7) compared with the mean diameter of cysts in the surgically managed group (74.5mm; 95%CI: 49.2-99.8) (Fig.4).
Figure 4: Mean diameter of the ovarian cysts.
In 33/41 patients no surgical intervention was needed during pregnancy. 13/33 patients had no follow up of their ovarian cyst arranged and no further mentioning of the cysts on routine growth and anomaly scans during pregnancy was found. In 20/33 patients at least one routine follow-up scan was performed 1-2 weeks after the diagnosis and in 12 of these 20 patients a second follow-up had taken place at least 1 month after the diagnosis. In one of the 20 patients with recorded follow-up’s an MRI scan had been arranged 2 months after the initial USS finding of a dermoid cyst.
Discussion
The results of our study confirm findings from previous studies: The vast majority of ovarian masses in pregnancy are benign and invasive cancer in pregnancy is rare; The results show a significant relation between size of adnexal mass and probability for surgery; Ultrasound examination of adnexal masses has been proven to be accurate and safe in pregnancy; Managing ovarian cysts in pregnancy can be challenging. Goh et al. have reported similar outcomes, namely that ovarian torsion is still reported as a rare event in pregnancy and that the management of most adnexal masses in pregnancy can be conservatively managed if asymptomatic and if there are no ultrasound findings suspicious for malignancy 8. If a surgical intervention is needed for persistent masses with complications such as torsion Goh et al. have found that laparoscopy during 1st and 2nd trimester can be safely performed 1. In our cohort two out of six women underwent successful major surgery during the 2nd trimester of pregnancy. One had an emergency laparoscopy for a torsion at 16 weeks of pregnancy and the other had a laparotomy at 17 weeks of pregnancy for a mucinous borderline tumour.
However, to our knowledge currently no evident guidelines exist on how to manage and follow-up ovarian masses during pregnancy. The characteristics and presentation of ovarian mass complications in pregnancy can be mimicked by similar symptoms related to pregnancy, such as ectopic pregnancy. In one of our cases a woman with a known ovarian cyst was found to have a necrotic ovary at the time of Caesarean section, despite no signs of torsion at any time during pregnancy. This only highlights how challenging and difficult the assessment of ovarian masses during pregnancy can be. Additional diagnostic examinations such as tumour markers in suspicious ovarian masses have been found difficult to interpret in pregnancy. However, there has been literature suggesting that if a mass is strongly suspicious for malignancy, it is likely that CA-125 will be severely elevated (1000-10 000) 7.
The strength of this study is that the data has been collected using the expertise and facilities of a tertiary referral centre in London (GSTT). The limitations of this study include retrospective data collection, small numbers of cases and loss of follow-up. Although, our study shows the benign nature of most ovarian masses in pregnancy and the ability of ultrasound to safely characterize ovarian masses, a prospective study is required to validate our results. As it is difficult to interpret ovarian cancer tumour markers in pregnancy 7, other models, such as the IOTA Simple Rules14,16 or the ADNEX model17 may play a role for further characterisation of ovarian masses. A prospective trial is required to validate these models in pregnancy.
We would like to draw the attention of your readers to the outcome of a survey undertaken in Kettering General Hospital. We wanted to determine what methods clinicians use to confirm central line cannula/needle position before dilatation and what their removal plan would be for an accidental insertion of a central line (>7 Fr) into the carotid artery.
We performed a paper survey of 52 doctors in anaesthesia/intensive care at Kettering General Hospital. We achieved a 100% return rate. We asked the doctors to answer questions based on their practise over the previous year period. The majority of people surveyed were consultants (47%). The results of the survey revealed doctors mostly utilised ultrasound confirmation of guidewire before dilatation (89%) but only 19% utilised pressure transduction. A large proportion of doctors surveyed either did not know how to manage carotid artery cannulation with a >7 Fr central line (35%) or would ‘pull and press’ (40%). Only 5% of the doctors who would ‘pull and press’ would arrange computed tomography (CT) angiogram follow up.
We highlighted a lack of clarity, which may be widespread. It is advisable to seek a vascular surgeon or interventional radiology input to facilitate line removal due to the excessive complications related to the ‘pull and press’ technique (47% complication rate).1 Complications include pseudoaneurysm formation, airway compromising haematomas, arteriovenous fistula, stroke and death.1 If such lines are removed by the ‘pull and press’ technique it is recommended to arrange CT angiogram even if the patient is asymptomatic due to the possibility of pseudoaneurysm or arteriovenous fistula formation.1
We correctly utilised ultrasound confirmation of guidewire position before dilatation. However ultrasound alone has not eliminated accidental arterial dilatation. This still occurs despite ultrasound usage especially in cases involving inexperienced clinicians and the guidewire going through the vein and into the artery.2 The combined use of ultrasound and transduction may further reduce the incidence of carotid cannulation.3 This may prove invaluable in centres without vascular or interventional radiology support.
Our centre has reduced its usage of central venous pressure (CVP) monitoring. This may reflect our lack of transduction prior to dilatation for central line insertion. Hence we devised a novel use of the double male Luer lock connector. This connector allows the female connector end of an infusion line to connect to the female connector of the blood aspirating port of an arterial transducer. This will then allow transduction of a central line cannula, before dilatation, via the arterial transducer by turning the 3-way tap (Figure 1). This removes the need to set up a separate transducer and also prevents the need to disconnect connections in the arterial line to allow CVP confirmation, as this was considered an infection risk.
Figure 1: Double male Luer lock connector attached to the blood aspirating port of an arterial transducer, with a fluid line connecting this to the central venous cannula
Adult Still’s disease (AOSD) is an inflammatory disorder of unknown etiology characterized by quotidian (daily) fevers, arthritis, and an evanescent rash and multi-organ involvement [1].First described in children by George Still in 1896, subsequently in 1971 Bywaters described 14 patients with similar presentation [2]. The clinical course of adult Still’s disease (AOSD) can be divided into three main patterns: monophasic (or monocyclic), intermittent, and chronic. Patients with monophasic AOSD have a disease course that typically lasts only weeks to months, completely resolving within less than a year in most patients [3]. Systemic features, including fever, rash, serositis, and hepatosplenomegaly, predominate in this group. The patient we diagnosed as AOSD, with monophasic course, went into remission after proper treatment and is symptom free even after stopping the treatment.
CASE REPORT
46 year old Indian male, non-smoker, married, nondiabetic, normotensive admitted at department of internal medicine in our hospital with history of high grade fever, polyarthritis, and skin rash for the last 4 weeks. The fever was high grade, with maximum temperature reaching 39.2°C. The patient also complained of joint pains involving the knee, ankle, wrist and proximal interphalangeal joints. There was no history of oral ulcers, morning stiffness, ocular symptoms, or contact with infected persons. In the hospital, during the febrile period, he developed macular rash mainly on chest and back [Figure 1]. On examination, the patient was sick looking, febrile-39.2°C. Chest on auscultation was normal, cardiovascular examination was unremarkable. Examination of abdomen revealed mild spleenomegaly. Neurological examination was unremarkable. Investigations revealed hemoglobin 12.7g/dl, erythrocyte sedimentation rate (ESR) 120 mm in 1st hour. Total leukocyte count-12.7 x10 9/L. Liver function showed elevated liver enzymes with Aspartate transaminase-125U/L, Alaninie aminotransferase 60 U/L, low albumin 2.3gms/dl. He was worked on lines of pyrexia of unknown origin and his blood, urine and sputum culture showed no growth. Procalcitonin level was less than 0.5ng/ml. Sputum for AFB was negative for three samples; qunatiferon gold test for tuberculosis was negative. IgM CMV, EBV, HIV, hepatitis B and C were negative malarial parasite, Widal and Brucella serology was negative. CT-chest and abdomen were normal, except for mild spleenomegaly. Echocardiogram was normal. ANA, rheumatoid factor was negative. Lactate dehydrogenase (LDH) 978 U/L, His CRP showed a progressive increase from 82mg/L to 284 mg/L, which decreased after starting steroids. His ferritin levels were 40, 000 (normal range 21.8 -274.6 ng/ml), which were reconfirmed by second sample and he had normal transferrin saturation. On the basis of his history, clinical examination and review of his laboratory investigations, diagnosis of AOSD was made. We started him on prednisolone 60 mgs daily along with Diclofenac potassium 50 mg twice daily, to which he responded and become afebrile. He was discharged with a tapering dose of steroids 5mgs weekly. He is doing well and is completely symptom free.
Figure 1: Skin Rash on the back
DISCUSSION
First described in children by George Still in 1896, “Still’s disease” has become the eponymous term for systemic juvenile idiopathic arthritis [4]. In 1971, the term “adult Still’s disease” was used to describe a series of adult patients who had features similar to the children with systemic juvenile idiopathic arthritis and did not fulfill criteria for classic rheumatoid arthritis.
The etiology of adult Still’s disease (ASD) is unknown; both genetic factors and a variety of infectious triggers have been suggested as important, but there has been no proof of an infectious etiology, and the evidence supporting a role for genetic factors has been mixed. It is uncertain whether all patients with AOSD share the same etiopathogenic factors. Proposed pathogens have included numerous viruses; suspected bacterial pathogens include Yersinia enterocolitica and Mycoplasma pneumoniae [5]. As an example of studies of the immunogenetics of ASD, in a series of 62 French patients, human leukocyte antigen (HLA)-B17, -B18, -B35, and -DR2 were associated with AOSD. However, other studies have not confirmed these findings [6].
Adult Still’s disease is very uncommon. Prevalence of AOSD is estimated to be 1.5 cases per 100, 000-1, 000, 000 people, with an equal distribution between the sexes [6]. There is a bimodal age distribution, with one peak between the ages of 15 and 25 and the second between the ages of 36 and 46. The diagnosis of AOSD is possible only by recognizing the striking constellations of clinical and laboratory abnormalities. It is also to be to remember that AOSD is a diagnosis of exclusion. AOSD has been associated with markedly elevated serum ferritin concentrations in as much as 70 percent of patients. Serum ferritin values above 3000 ng/mL in a patient with compatible symptoms should lead to suspicion of AOSD in the absence of a bacterial or viral infection. Abnormally high serum ferritin values were reported in some case reports and it was suggested that high ferritin levels may be a diagnostic marker of Still's disease [7]. Our patient showed almost all features as laid down in Yamaguchi criteria[Table 1] for the diagnosis of AOSD [8] along with a markedly high ferritin levels.
Table 1 : Diagnostic criteria for AOSD (Yamaguchi)8
Major criteria
Minor criteria
Fever > 39ºC, > 1 week
Sore throat
Arthralgia/ arthritis > 2 weeks or splenomegaly
Lymphadenopathy
Typical rash
Abnormal LFT
WBC > 10, 000 with > 80% PMNs and RF
Negative ANA
Exclusions: Infections, malignancy, rheumatological diseases. Five criteria with at least two major criteria. ASOD: Adult onset still’s disease. WBC: White blood cell, ANA: Antinuclear antibody, RF: Rheumatoid factor, PMN: Polymorphonuclea
Non-steroidal anti-inflammatory drugs (NSAIDs), such as aspirin, ibuprofen or naproxen, help to reduce inflammation [9]. Patients with high-fever spikes, severe joint glucocorticoids, such as prednisone (0.5- 1mg/kg/day)Methotrexate has been used successfully in a small series of people to treat adult Still's disease [10]. Some patients are refractory to these conventional therapies. Tumor necrosis factoralpha (TNF) blockers include infliximab, adalimumab, etanercept, anti-interleukin-1, antiinterleukin-6 agents, and most recently anti CD20-expressing B-cell antibodies are also effective in some cases. Other experimental drugs, including cyclosporine and anakinra, have also been successful in small groups of people [9]. Interleukin 6 inhibitors like tocilzumab showed a good result in patients with AOSD resistant to other immunosuppressive agents such as methotrexate, TNF inhibitors and anakinara [11]. Even with treatment, it's difficult to predict the course of adult Still's disease. Some people might only experience a single episode, while for others adult Still's disease may develop occasional flair up or a chronic condition. About one-third of people with the disorder may fall into each of the above groups.
CONCLUSION
A diagnosis of AOSD should be kept in mind in case of pyrexia of unknown origin particularly in a patient who presents with high-grade intermittent fever, polyarthritis and skin rash of more than two weeks duration. However, the patient should be extensively evaluated to rule out other differentials of AOSD like acute or chronic infections, autoimmune disorders, vasculitis and malignant disorders. Serum ferritin values can be powerful adjuncts in making the diagnosis of AOSD [12], where they are usually higher than other inflammatory diseases. Indeed, extreme elevation of serum ferritin up to 75, 500ng/ mL has been reported in AOSD[12]. Several investigators agree that ferritin levels above l, 000 ng/mL are suggestive of AOSD while levels greater than 4, 000ng/mL are very specific for this diagnosis when accompanied by a compatible clinical picture.
Several studies found that refugees develop post-traumatic stress disorder (PTSD) after having endured war trauma1, or certain circumstances related to migration like moving to a new country, being unemployed and poor housing2. PTSD is described as distress and disability due to a traumatic event that occurred in the past3. In 2013, the American Psychiatric Association revised the PTSD diagnostic criteria in the fifth edition of its Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and PTSD was included in a new category, Trauma- and Stressor-Related Disorders4. All of the conditions included in this category required exposure to a traumatic or stressful event as a diagnostic criterion4. The person with PTSD often avoids trauma-related thoughts and emotions, and discussion of the traumatic event4. PTSD patients are invariably anxious about re-experiencing the same trauma. The trauma is usually re-lived by the person through disturbing, repeated recollections, flashbacks, and nightmares4. Symptoms of PTSD generally begin within the first 3 months after the provocative traumatic event, but may not begin until several years later4. A large number of children (10-40%), 16 or younger, who have experienced a traumatic event in their life, tend to develop PTSD later on5. Moreover, many families with children growing in war zones and then moving to safer places, experience trauma, stress and reduced functioning6. These families have different resilience rates in their survival mechanisms, coping strategies and adaptation levels7.
The latest war in Syria has led to the migration of large parts of the Syrian population to neighboring countries such as Lebanon, Jordan and Turkey8.The United Nations High Commissioner for Refugees (UNHCR) estimates that approximately 1.5 million refugees are located in Lebanon9. These refugees have been exposed to several types of traumatic events that may increase the incidence of mental health problems10.
We hypothesize that the proportion of positive PTSD screens would be high among Syrian refugees with the presence of some specific related risk factors. Thus, the objective of our study was to examine PTSD symptoms and to determine the associated risk factors in a sample of Syrian refugees living in North Lebanon.
METHODS
1. Study design and population
This was a cross-sectional study that aimed to assess the proportion of Syrian refugees in North Lebanon who were at high risk of developing PTSD, and to examine the association of PTSD high risk with other factors. The survey was carried out during February and March 2016. A convenient sample of Syrian refugees of both gender, aged between 14 and 45 years, living in North Lebanon, was selected out of a population of 262,15111.
The estimated minimum sample size, calculated using Raosoft sample size calculator, with a margin of error of 5% and a confidence interval of 95%, was 384 refugees. A total number of 450 Syrian refugees, residing in individual tented settlements (ITSs), collective shelters (CS) or Primary Health Care Centers (PHCs) located in North Lebanon, was selected according to inclusion and exclusion set criteria.
The inclusion criteria were: Syrian refugees, aged (14-45 years), physically and mentally independent. Hence, all subjects that were younger than 14 or older than 45, speechless, deaf, physically and mentally dependent, or have undergone recent moderate or severe surgery (less than one week earlier), were excluded from the study.
2. Ethical considerations
The study protocol received approval from the Notre Dame University (NDU) Institutional Review Board (IRB). The approval comprised details about the procedure of the study and the rights of the participants. Informed consent was obtained from each participant. The questionnaires were answered anonymously, ensuring confidentiality of collected data.
3. The Interview questionnaire
The interview questionnaire was divided into six sections consisting of a total of 46 questions. The questions were dichotomous, close-ended and open-ended. A cover page described the purpose of the study, ensuring the anonymity and confidentiality, and soliciting the consent of participants. The questionnaire collected data on the demographic and socio-economic characteristics of the participants. Information about health status and stressful life events (SLE) were also obtained. The PC-PTSD (Primary Care Post-Traumatic Stress Disorder) tool was used to screen PTSD.
For the purposes of the study, subjects were classified as having/not having positive PC-PTSD. The results were used to calculate the proportion of Syrian refugees who are at high risk of developing PTSD.
PC-PTSD questionnaire: The PC-PTSD was initially developed in a Veteran Affairs primary care setting and is currently used to screen for PTSD, based on the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-4) diagnostic criteria12. The screen consisted of 4 questions related to a traumatic life event: In the past month you (1) Have had nightmares about it or thought about it when you did not want to?; (2) Tried hard not to think about it or went out of your way to avoid situations that reminded you of it?; (3) Were constantly on guard, watchful, or easily startled?; (4) Felt numb or detached from others, activities, or your surroundings? The answers to these questions were dichotomous (Yes/No) and the total screen was considered "positive" when a patient answered "yes" to three out of four questions. PC-PTSD showed a high sensitivity (86%) and moderate specificity (57%) when using a cutoff score of 213.
In order to validate the Arabic version of the PC-PTSD questionnaire, it was translated into Arabic and translated back into English. The original version of the Arabic questionnaire was pilot-tested on 10 Syrian refugees to ensure the validity of the answers, and to guarantee its reliability.
Anthropometric measurements: The main anthropometric measurements were weight and height. Participants were dressed in light clothes and barefooted, and standing height was measured to the nearest 0.1 cm using a stadiometer. Body weight was measured to the nearest 100g using an electronic scale. Body Mass Index (BMI) is a measure of weight adjusted to height (kg/m2), calculated by dividing weight (in kilograms) by the square of height (in metres). For the purposes of the study, BMI was recoded into four categories: underweight, normal, overweight and obese.
4. Data entry and statistical analysis
The Statistical Package for Social Science (SPSS) for Windows (version 22) was used for data entry and analysis.
First, bivariate analyses of categorical variables were performed using the Fisher exact tests, Chi-squared tests and Student’s t-test. The dependent variable was the high risk of PTSD, using the PC-PTSD tool. Thus, the PC-PTSD score was considered the dependent variable: a dichotomous variable of PC-PTSD (-) and PC-PTSD (+), and all variables that might be a risk factor or might lead to PTSD were set as the independent variables. Two main independent variables were: age and gender. Other variables included: marital status, place of residence, number of people and families living in the same household (crowding index), income, education status, profession, work status, lifestyle habits, medical or psychological problems, medication taken and SLE. Frequencies and percentages were calculated for qualitative variables, and mean and standard deviations for quantitative variables (BMI, crowding index). A p-value of 0.05 or less was considered to be statistically significant.
RESULTS
Table 1: Socio-demographic characteristics of the 450 Syrian refugees
Variables
Frequency (n) or Mean
Percentage (%) or Standard Deviation
Gender
· Male
69
15.3
· Female
381
84.7
Age (years)
27.9
8.1
Crowding index (co-residents/room)
4
2.4
Crowding index
· ≤ 2.5
135
30
· 2.51-3.5
108
24
· > 3.5
207
46
Current place of residence
· Tented settlements
62
13.8
· Collective shelters
92
20.4
· Building
296
65.8
Educational level
· Don’t know how to read and write
33
7.3
· Know how to read and write/Elementary
216
48
· Complementary/Secondary/Technical
178
39.6
· College degree
23
5.1
Marital status
· Single
54
12
· Married
378
84
· Divorced
5
1.1
· Widowed
13
2.9
Current employment status
· No
379
84.2
· Full-time job
40
8.9
· Part-time job
31
6.9
Presence of income
· No
379
84.2
· Yes
71
15.8
Perceived income (n=71)
· Satisfactory
25
35.2
· Non-Satisfactory
46
64.8
Table 2: Health characteristics and migration factors of the 450 Syrian refugees
Variables
Frequency (n)
Percentage (%)
BMI category (kg/m2)
· <18.5
11
2.4
· 18.5-24.9
176
39.1
· ≥ 25
263
58.5
Tobacco consumption
· Yes
97
21.6
· No
353
78.4
Presence of medical conditions
· No
337
74.9
· Yes
113
25.1
Migration status
· Before 2011
15
3.3
· 2011-2013
339
75.3
· After 2013
96
21.4
Seeking professional help for psychological disorders
· No
439
97.6
· Yes
11
2.4
Number of stressful life events
· None
22
4.9
· [1-2]
181
40.2
· [3-4]
235
52.2
· [5-6]
12
2.7
PC-PTSD
· Negative
237
52.7
· Positive
213
47.3
Table 3: Socio-demographic characteristics associated with positive screen for PTSD among the 450 Syrian refugees (bivariate analyses)
Variables
Positive PC-PTSD n(%) or mean±SD
Negative PC-PTSD n(%) or mean±SD
p-value
Gender
0.011*
· Male
23 (33.3)
46 (66.7)
· Female
190 (49.9)
191 (50.1)
Age (years)
28.9 ± 7.6
26.9 ± 8.5
0.009*
Crowding index (co-residents/room)
4.2 ± 2.7
3.8 ± 2.2
0.069
Crowding index
0.294
· ≤ 2.5
58 (43.0)
77 (57.0)
· 2.51-3.5
49 (45.4)
59 (54.6)
· > 3.5
106 (51.2)
101 (48.8)
Current place of residence
0.137
· Tented settlements
27 (43.5)
35 (56.5)
· Collective shelters
52 (56.5)
40 (43.5)
· Building
134 (45.3)
162 (54.7)
Educational level
0.479
· Don’t know how to read and write
16 (48.5)
17 (51.5)
· Know how to read and write/Elementary
95 (44.0)
121 (56.0)
· Complementary/Secondary/Technical
· University level
92 (51.7)
86 (48.3)
10 (43.5)
13 (56.5)
Marital status
0.000*
· Single
9 (16.7)
45 (83.3)
· Married
191 (50.5)
187 (49.5)
· Divorced
4 (80.0)
1 (20.0)
· Widowed
9 (69.2)
4 (30.8)
Current employment status
0.205
· No
184 (48.5)
195 (51.5)
· Full-time job
14 (35.0)
26 (65.0)
· Part-time job
15 (48.4)
16 (51.6)
Presence of income
0.233
· No
184 (48.5)
195 (51.5)
· Yes
29 (40.8)
42 (59.2)
Perceived income (n=71)
0.264
· Satisfactory
8 (32.0)
17 (68.0)
· Non-Satisfactory
21 (45.7)
25 (54.3)
*Significant with p-value < 0.05
Table 4: Health characteristics and migration factors associated with positive screen for PTSD among the 450 Syrian refugees (bivariate analyses)
Variables
Positive PC-PTSD n (%)
Negative PC-PTSD n (%)
p-value
BMI category (kg/m2)
0.183
· <18.5
7 (63.6)
4 (36.4)
· 18.5-24.9
75 (42.6)
101 (57.4)
· ≥ 25
131 (49.8)
132 (50.2)
Tobacco consumption
0.369
· Yes
42 (43.3)
55 (56.7)
· No
171 (48.4)
182 (51.6)
Presence of medical conditions
0.000*
· No
143 (42.4)
194 (57.6)
· Yes
70 (61.9)
43 (38.1)
Migration status
0.094
· Before 2011
5 (33.3)
10 (66.7)
· 2011-2013
154 (45.4)
185 (54.6)
· After 2013
54 (56.2)
42 (43.8)
Seeking professional help for psychological disorders
0.003*
· No
· Yes
203 (46.2)
236 (53.8)
10 (90.9)
1 (9.1)
Number of stressful life events
0.000*
· None
0 (0.0)
22 (100.0)
· [1-2]
66 (36.5)
115 (63.5)
· [3-4]
138 (58.7)
97 (41.3)
· [5-6]
9 (75.0)
3 (25.0)
* Significant with p-value < 0.05
All the socio-demographic, health and migration characteristics of our sample of Syrian refugees were described in Tables 1 and 2. Out of the 450 participants, 47.3% had positive PC-PTSD. In order to study the association between the socio-demographic characteristics among the Syrian refugeesand PTSD screening, abivariate association was explored as shown in Table 3. The results indicate a significant difference between gender groups, as almost half of the women (49.9%) had a positive screen for PTSD compared to 33.3% of the men (p=0.011). Mean age was significantly higher in refugees with positive PC-PTSD (28.9 ± 7.6 years) versus those with negative PC-PTSD (26.9 ± 8.5 years) (p=0.009). PTSD screening was shown to be significantly associated with marital status. In fact, positive PC-PTSD was mostly perceived in divorced participants (80%) compared to 69.2% of widowed, 50.5% of married, and 16.7% of single subjects (p=0.000). Yet, crowding index, current place of residence, educational level, employment status, and income were not significantly associated with positive PC-PTSD (p>0.05).
The association of health characteristics and migration factors among the Syrian refugees with PTSD screening was displayed in Table 4. A significant association was observed between the presence of medical condition and positive screen for PTSD, as 61.9% of subjects suffering from a medical condition had a positive PC-PTSD, compared to 42.4% of participants without medical conditions (p=0.000). However, BMI and tobacco consumption were not significantly associated with PTSD screening (p>0.05). PTSD screening was significantly associated with the presence of psychological disorders. Thus, 90.9% of refugees who sought professional help for psychological disorders had positive PC-PTSD, versus 46.2% of those who did not (p=0.003). Positive PC-PTSD was significantly associated with the increase in the number of SLE. In fact, none of the participants without any stressful event had a positive PC-PTSD, compared to 36.5% of participants with 1-2 SLE, 58.7% of participants with 3-4 SLE and 75% of participants with 5-6 SLE (p=0.000). On the other hand, no significant association was observed between PC-PTSD and migration status (p>0.05).
DISCUSSION AND CONCLUSION
PTSD represents the most frequently occurring mental disorder occurring among refugees14. PTSD prevalence rates ranging between 15% and 80% have been reported in refugees. A study of Cambodian refugees living in the Thailand-Cambodia border camp indicated that 15% had PTSD15. A cohort study aimed to show the prevalence of PTSD among Iranian, Afghani and Somalian refugees that have moved to the Netherlands at a 7-year interval [(T1=2003) - (T2=2010)]. Results displayed a high prevalence at both T1 (16.3%) and T2 (15.2%). The reason for this high unchanged prevalence may be due to the late onset of the PTSD symptoms, and the low use of mental health care centers16. De Jong and colleagues reported that 50% of the refugees in Rwandan and Burundese camps had serious mental health problems, mainly PTSD17. While Teodorescu and colleagues aimed to illustrate the prevalence of PTSD among refugees in Norway; results showed that 80% of the refugees had PTSD18. In our study, the high proportion of positive screen for PTSD among Syrian refugees was estimated at 47.3%. In 2006, a mental health assessment demonstrated that Lebanese citizens exposed to war were more likely to develop psychiatric problems such as PTSD19. Subsequently, a cross-sectional study was done in South Lebanon on 681 citizens in 2007 (1-year after the 2006 war in Lebanon). The aim of the study was to examine the prevalence of PTSD 12 months after 2006 war cessation. Results showed that the prevalence of PTSD was 17.8%19. A recent cross sectional study, aimed to show the prevalence of PTSD and explore its relationship with various variables. The study included 352 Syrian refugees settled in camps in Turkey. An experienced psychiatrist evaluated the participants, and results demonstrated that 33.5% of study participants had PTSD, mainly female refugees, people who experienced 2 or more SLE, or those who had a family history of psychiatric disorder20.
PTSD has been associated with a wide range of traumatic events: emotional or physical abuse21, sexual abuse22, parental break-up23, death of a loved one24, domestic violence25, kidnapping26, military services27, war trauma28, natural disasters29 and medical conditions including cancer30, heart attack31, stroke32, intensive-care unit hospitalization33, and miscarriage34.
Our findings should be interpreted taking into account several limitations. The first limitation is the use of screening tools, instead of the more accurate diagnosis of the clinician, in order to detect PTSD. Given that a standardized screening tool for PTSD was used, our rates are likely an overestimate of the true prevalence rates. Secondly, this study was conducted with a limited sample of Syrian refugees and therefore should not be generalized to all refugees of other eras or from other countries. The third limitation is represented by the lack of information on the presence of other Axis I psychiatric comorbidities such as anxiety or mood disorder that could facilitate the development of PTSD or influence its manifestations35-36.
Refugees are an important group to examine, given the high prevalence of mental health disorders. Although refugees are evaluated for health problems, currently there are no standardized screening and clinical practice guidelines for assessing PTSD in all refugees. Therefore, we may be missing opportunities to detect and treat these harmful and potentially fatal conditions. Our findings suggest the need to consider a standardized screening tool for PTSD in this population. In addition, a far greater percentage of patients may have “PTSD symptoms,” that are abnormal but do not meet full criteria of the DSM5 for PTSD diagnosis, but still cause functional impairment and may later develop into a diagnosable PTSD. Given the overall high prevalence, one possible model for evaluation would be a stepped screening approach: Positive screens for PTSD could trigger a standardized clinical diagnosis for PTSD with more comprehensive assessment and early intervention. Considering the high cost of treating individuals with PTSD, screening and intervention strategies should be addressed. Greater awareness among providers and increased targeted assessment and treatment efforts may increase early detection of a wide range of PTSD, preventing more serious future health problems and functional impairment among refugees.
The identification of dark patches on the skin may be the first indication of type 2 diabetes mellitus (DM type 2). DM type 2 is a complex heterogeneous group of metabolic conditions characterised by elevated levels of serum glucose. Causative factors are impairment in both insulin action and insulin secretion. The darkening of the skin is usually evident on the hands and feet, in folds of skin, along the neck, and in the patient’s groin and armpits.1 The affected skin differs from that which surrounds it, and it feels velvety and also thicker. That skin may have hanging from it the small, soft, skin-coloured growths known as tags, and the area affected may be pruritic. This condition is a nonspecific dermatological disorder termed acanthosis nigricans (AN), which often occurs in patients with high insulin levels. Hud et al. (1992) found that 74% of the obese population exhibits AN.2The association of AN, skin tags, and diabetes mellitus due to insulin resistance – along with obesity in adolescents and young adults – is a well-defined syndrome.3,4,5
High-insulin levels in the blood may increase the body’s production of skin cells, many of which have increased pigmentation that gives the skin a darkened appearance – dark patches appear on the skin. These are often the outcome of insulin receptors in the skin being triggered, causing mutations of normal tissue that are dark in colour and/or irregular in shape. The condition may be an indication that the blood sugar is persistently high. The term ‘acanthosis nigricans’ was originally proposed by Unna et al. in 1891, but the first descriptions of it were made a year earlier by two researchers working independently of each other: Pollitzer and Janovsk.6 Kahn and colleagues tried to clarify the link between AN and insulin resistance in 1976.7 Eventually, its presence became established as an indicator of insulin resistance or diabetes mellitus in obese patients.8 In 2000, the American Diabetes Association formally accepted AN as such.9 It should be borne in mind that AN must not be considered a characteristic feature of DM type 2; it is not a condition that is developed by all those who suffer from the disease.
Figures 1,2,3 - Acanthosis Nigrans
Pathogenesis
Although the pancreas produces insulin in DM type 2, the body cannot make use of it efficiently. The outcome is a build-up of glucose in the bloodstream, which may lead to high levels of blood glucose and insulin. At low concentrations, insulin regulates the metabolism of carbohydrates, lipids, and protein and may promote growth by binding to ‘classic’ insulin receptors. High concentrations of insulin may stimulate keratinocyte and fibroblast proliferation through high-affinity binding to the insulin-like growth factor 1 (IGF-1) receptors.10 In obese patients elevated IGF-1 levels may contribute to keratinocyte and fibroblast proliferation;11 the binding stimulates the proliferation of keratinocytes and fibroblasts, which leads to AN.
To put this simply, AN is the outcome of a toxic effect of hyperinsulinemia. Excess insulin causes the normal skin cells to reproduce rapidly rate, and it has been demonstrated to cross the dermo-epidermal junction and reach keratinocytes. In those who have dark skin, these new cells have increased melanin. The higher level of melanin results in the creation of a patch of skin that is noticeably darker than the skin surrounding it. The presence of AN is therefore a strong indicator of increased insulin production and, therefore, it is also a predictor for future DM type 2.
When the occurrence of AN is recognised, a prediabetic person has the opportunity to become more alert to their symptoms and to take precautions in the form of diet restrictions and weight loss. This is because overweight people tend to develop resistance to insulin over time. If too much insulin is the cause of AN, it is relatively easy for the patient to counter it by changing to a healthier diet, taking exercise, and controlling their blood sugar. Obesity-associated AN may be a marker for higher insulin needs in obese women with gestational diabetes,12andAN has been shown to be a dependable early indicator for metabolic syndrome in paediatric patients.13
Autoimmunity?
Unknown autoantibodies other than insulin receptors have been implicated in AN, which may explain the effectiveness of cyclosporine treatment. Kondo and colleagues identified a very rare occurrence – without type B insulin resistance – of generalised AN with Sjögren's syndrome and systemic lupus erythematosus-like features.14Theirs was the first report of generalised AN involving an area from the mucosa of the larynx to the esophagogastric junction, accompanied by autoimmune disorder (AD) responding to systemic immunosuppressive therapy. AN skin lesions and mucosal papillomatosis were medicated with oral cyclosporine A and were accompanied by lower autoantibody titres. That was an outcome of the development of antibodies to insulin receptors in AD such as systemic lupus erythematosus.15
Raymond et al. have reported on the association of AN with disordered immunoreactivity.16 The onset of AN may precede a variety of classic ADs, and different categories of ADs may be present at the same time. If AN is an AD, DM type 2 may also represent a slow and subtle autoimmune process. AN and DM type 2 then become two different expressions of the same disease process, but the former is apparently benign and the latter is ultimately potentially fatal. Autoimmunity is a well-known pathogenic component in DM type 2. The assumption that its pathogenesis encompasses autoimmune aspects is increasingly recognised. That is based on the presence of circulating autoantibodies against β cells, self-reactive T cells, and also on the glucose-lowering efficacy in DM type 2of some immunomodulatory therapies.17 The autoimmune hypothesis of AN has the potential to modify the direction of DM type 2 research.
The symptoms of ADs are inconstant and this is in divergence to the mechanisms of antigen recognition and effector function that are alike in the response to pathogens. 18 The symptoms basically depend on the triggering autoantigen and the target tissue. In certain conditions, autoantibodies function as receptor antagonists and in other situations, they function as receptor agonist. Autoantibodies of both types can be made against insulin receptor. When they serve as antagonists as in DM Type 2, the cells of patients are unable to take up glucose, the consequence is hyperglycaemia whereas in patients with agonistic antibodies, cells deplete blood glucose resulting in hypoglycaemia.18 One wonders whether AN may be an early by-product of such an autoimmune process.
Vitiligo which is the result of depigmentation of the skin is in fact an opposite disorder to AN. Vitiligo is recognised as an AD.19Thyroid disorders, particularly Hashimoto thyroiditis and Graves’ disease, other endocrinopathies, such as Addison disease, diabetes mellitus, alopecia areata, pernicious anaemia, inflammatory bowel disease, psoriasis, and autoimmune poly-glandular syndrome are all associated with vitiligo. 20 Kakourou et al identify that Hashimoto's thyroiditis is 2.5 times more frequent among children and adolescents with vitiligo than in a healthy age- and sex-matched population and it usually follows the onset of vitiligo. 21
As in the case of other ADs, vitiligo susceptibility may involve both target organ-specific genes and immune response genes. 22 The autoimmune theory suggests alteration in humoral and cellular immunity in the destruction of melanocytes of vitiligo. 23. Vitiligo lesions have an infiltrate of inflammatory cells, particularly cytotoxic and helper T-cells and macrophages;histological evidences further back up an autoimmune aetiology. 24 Like AN, Vitiligo is thus gene linked; immunity derangements may be providing the matrix and genes are the craftsmen in both conditions.
Vitiligo occurs more commonly in DM Type 1. A few recent studies have revealed its increased incidence in DM Type 2. 25 These may be isolated case studies, but offer new insight into the pathogenesis of DM Type 2. There is a logical thread running between the autoimmune assertion of AN and its depigmentation counterpart (vitiligo) which is recognised as an AD. If AN is proven as an AD, the AD hypothesis of DM Type 2 becomes more binding. The autoimmune process of AN warrants further consideration and further study is needed to confirm or falsify the hypothesis of an autoimmune spectrum disorder between AN, vitiligo and DM Type 2.
Even though the common assumption that bacteria flora occupying human body outnumber the body cells has been proven wrong, their revised ratio of 1:1 is still astounding.26 The exact role of the resident microbial colony in human body is unclear. There are less ADs observed among the hunters’ tribal population of Tanzania whose faecal matter contain more varieties of microbes than people in developed countries. 27,28 This is an observation that need further verification. It is possible that the occupied microbial army may be maintaining the harmony among the human body cells from attacking each other and serving as moderators. Now that anti-autoimmune activity in molecules produced by parasites have been confirmed in haematology lab, these findings may have clinical significance. The aetiology of ADs is multifactorial. Genetic, environmental, hormonal, psychological stress and immunological factors are all considered important in their development. I content that the clue to the mechanism of development of certain ADs and ways of counteracting them may be embedded in the bacterial colony and their interaction with human cells.
International studies
A pilot study by Bhagyanathan and colleagues demonstrated that children with AN have a high incidence of insulin resistance.29 They posit that the detection of insulin resistance in children may present an opportunity to prevent the onset of microvascular changes before the development of DM type 2. Once DM type 2 by hyperglycemia is diagnosed it may be too late for that. Insulin resistance is one of the mechanisms involved in the pathogenesis of DM type 2; therefore, early recognition of insulin resistance is paramount in the prevention or delay of the onset of diabetes. Their study was of 62% of children who had AN alongside high insulin resistance. In children with AN and a high BMI, the incidence of insulin resistance was about 80%. This is evidence that the easily detectable symptoms are of value in the screening of children who are at high risk of developing DM type 2. Bhagyanathan et al. conclude that AN has potential as a screening method because those who have high insulin resistance as well as AN are at high of future DM type 2.
An earlier US study, by Brickman and colleagues, had yielded somewhat similar results.30 This involved 618 youths from different ethnic groups at nine paediatric practices. They were aged from 7 to 17 years. A survey was made of their demographics and their family history with regard to DM type 2, and their weight and height were also measured. AN was scored and digital photographs of their necks were taken. AN was identified in 19%, 23%, and 4% of the African American, Hispanic, and Caucasian youth respectively. It was also found in 62% of those studied who had a BMI greater than the 98th percentile. Using multiple logistic regression, the researchers found that the level of BMI, the presence of maternal gestational diabetes, female gender, and not being Caucasian, were all independently associated with AN. AN was common among the overweight young people and was associated with risk factors for glucose homeostasis abnormality. Brickman et al. concluded that identification of AN offers an opportunity to advise families about the causes and consequences of the condition. 30 That has the potential to motivate those with responsibility for the young people to encourage and effect healthy lifestyle changes that decrease the risk of the development of DM type 2 and cardiovascular disease.
In their research in India, Vijayan et al. determined that BMI, waist circumference and AN are three physical markers for the recognition of insulin resistance in children.31 They conducted a cross-sectional school-based study in a semi-rural environment in the state of Kerala, which has become known as the diabetic capital of the country. Their study encompassed 283 children between the ages of 10 to 17. The prevalence of insulin resistance was 35%; this estimate was arrived at by using a homeostasis model assessment of insulin resistance (HOMA-IR). Of the children studied, 30% had a waist circumference above the 75th percentile and 18.7% had a BMI above 85th percentile. AN was diagnosed in 39.6% of the population studied. A significantly high prevalence of insulin resistance was observed among the children with a waist circumference exceeding the 75th percentile, a BMI above the 85th percentile, or a diagnosis of AN. The most sensitive physical marker of insulin resistance was AN (90%) and the most specific was BMI (91%). By combining these parameters their sensitivity may be increased to 94% and their negative predictive value to 96%. Vijayan et al. conclude that these easily recognisable physical markers are an efficient warning of insulin resistance among children.
Acanthosis nigricans in different conditions
AN is not a disease, but a symptom of disease. A high prevalence has been observed recently, and there are a number of varieties. These include benign, obesity associated, syndromic, malignant, acral, unilateral, medication-induced, and mixed AN.32,33 It has been established that AN may occur in a number of conditions, and a brief discussion of these is appropriate for this paper. Different types of AN are listed in Table 1. It often appears gradually in the prediabetic state, but abruptly in malignancy.
AN may be triggered by a plethora of medications, such as birth control pills, human growth hormones, thyroid medications, and even some bodybuilding supplements. All these medications may cause changes in insulin levels. Medications used to ease the side effects of chemotherapy have also been linked to AN. In most cases, the condition clears up when the medications are discontinued. In rare cases, AN may be caused by gastric cancer (especially gastric adenocarcinoma) or an adrenal gland disorder such as Addison’s disease. Hypothyroidism, Cushing’s disease, and polycystic ovarian disease are also common causes of AN. 34,35
When AN is present without any identifiable cause in middle-aged and older patients with extensive skin findings, internal malignancy needs to be ruled out. AN has been reported in association with many kinds of cancer, by far the most common being an adenocarcinoma of gastrointestinal origin. In these patients it is a rapid-growing dermatological pigmentation disorder. The skin changes are typically more extensive and severe than those seen in benign AN. Findings may include thickening, unusual roughness and dryness, and/or potentially severe itching (pruritus) and irritation of the skin regions affected. Pigmentary changes may be more pronounced than those observed in benign AN and they are not restricted to areas of hyperkeratosis. Malignant AN is frequently associated with the mucous membranes and with distinctive abnormalities of the oral (mouth) region. For example, reports indicate that the lips and the back and sides of the tongue may have an unusually ‘shaggy’ appearance, sometimes with elevated, wart-like, non-pigmented tissue growths (papillomatous elevations). Malignant AN is also commonly characterised by wart-like thickening around the eyes, unusual ridging or brittleness of the nails, thickening of the skin on the palms of the hands, hair loss, and sometimes other symptoms. Investigators have reported that the development of malignant AN may occur as much as five years before the onset of other symptoms, although the time span before malignancy is typically of shorter duration.
Table 1. Different types of acanthosis nigricans
1. Obesity-associated acanthosis nigricans. Obesity-associated acanthosis nigricans, once labelled pseudo-acanthosis nigricans, is the most common type. Lesions may appear at any age but are most common in adulthood. The dermatosis is weight dependent, and lesions may completely regress with weight reduction. Insulin resistance is often present in these patients. It is slow growing. 2. Acral acanthosis nigricans. Acralacanthosis nigricans (acral acanthotic anomaly) occurs in patients who are otherwise in good health. Acral acanthosis nigricans is most common in dark-skinned individuals, especially those of African-American or sub-Saharan-African descent. The hyperkeratotic velvety lesions are most prominent over the dorsal aspects of the hands and feet, with knuckle hyperpigmentation often most prominent. 3. Unilateral acanthosis nigricans. Unilateral acanthosis nigricans, sometimes referred to as nevoid acanthosis nigricans, is believed to be inherited as an autosomal dominant trait. Lesions are unilateral in distribution and may become evident during infancy, childhood, or adulthood. Lesions tend to enlarge gradually before stabilising or regressing. 4. Generalised acanthosis nigricans. Generalised acanthosis nigricans is rare and has been reported in paediatric patients without underlying systemic disease or malignancy. 5. Syndromic acanthosis nigricans. Syndromic acanthosis nigricans is the name given to acanthosis nigricans that is associated with a syndrome. The type A syndrome and type B syndrome are special examples. 6. Hereditary acanthosis nigricans. Familial acanthosis nigricans is a rare genodermatosis that seems to be transmitted in an autosomal dominant fashion with variable phenotypic penetrance. The lesions typically begin during early childhood but may manifest at any age. 7. Drug-induced acanthosis nigricans. Drug-induced acanthosis nigricans, although uncommon, may be induced by several medications, including nicotinic acid, insulin, pituitary extract, systemic corticosteroids, and diethylstilbestrol. Rarely, triazinate, oral contraceptives, fusidic acid, and methyltestosterone have also been associated with it. 8. Malignant acanthosis nigricans. Malignant acanthosis nigricans, which is associated with internal malignancy, is the most concerning variant of acanthosis nigricans because the underlying neoplasm is often an aggressive cancer. 9. Mixed-type acanthosis nigricans. Mixed-type acanthosis nigricans refers to those situations in which a patient with one of the above types develops new lesions of a different ethology.
Genetic links
It is worth noting that certain types of AN may be genetically linked.36 The interaction of genes and the environment is not clearly understood and the different variables of DM type 2 are not established. It is a heterogenous disorder and there is a general consensus that diabetic comorbidities may be the outcome of genetic and environmental susceptibilities.37,38,39,40,41 Such factors may have an influence independently or in combination with one another that brings about hyperglycaemic conditions.It would be interesting to explore the possibility of a link between the diabetic genes and the AN gene. DM type 2 may be potentiated by poor quality of insulin or decreased production of insulin, and the distinction between those manifestations is not well recognised. The controversy concerning the relative roles of insulin deficiency and insulin resistance in DM type 2 continues to be unresolved.42 Despite the early demonstration that obese people have elevated plasma insulin concentrations, many studies over the years have failed to control satisfactorily for the influence of obesity.43 Another difficulty with the interpretation of plasma insulin concentrations is that sustained hyperglycaemia may have detrimental effects on insulin secretion.44 Diabetes mellitus affects every cell of the body, and therefore it affects the beta cells of the pancreas in turn. The spiralling effect of hyperglycaemia adds to the malfunctioning of beta cells, and that results in impaired quantity and quality of insulin. Only a subset of diabetic patients shows AN, and other groups of obese diabetic patients do not develop AN. AN is linked with higher insulin production and obesity, whereas AN may not be present in diabetes with a reduced quantity of insulin. The presence of AN may serve as one of the biological markers to determine subtypes of DM type 2.
The incidence of AN varies in different races, which is evidence that AN may have a genetic contribution – indeed, it has been regarded by some as being strongly influenced by genetic factors. It is thought to be autosomal in nature. AN is common among African-Americans, Hispanics, and American Indians, but it is rare among white people.45,46 A study from the USA reports the prevalence of AN as 3% among Caucasians, 19% in Hispanics, and 28% in American Indians. 47 More recently, studies from Sri Lanka and south India show the prevalence of AN as high as 17.4% and 16.1% respectively in the adult population in general.48,49
Type 2 diabetes mellitus and schizophrenia
DM type 2 is relatively common among people who have mental health issues. Increased risk for cardiovascular disease and other serious illnesses related to insulin resistance – for example, certain epithelial cell carcinomas, AN, and polycystic ovary syndrome – are long-term concerns associated with the cluster of metabolic abnormalities stemming from insulin resistance. These are often referred to as the metabolic syndrome.50 Impaired action of insulin in patients with schizophrenia was reported over fifty-five years ago and later confirmed in Australia.51 The prevalence of DM type 2 in patients with schizophrenia was found to be higher than it was in the general population, even before antipsychotic medication was in widespread use.
The mechanisms underlying the relationship between schizophrenia and diabetes remain unexplained. The present author has argued in favour of the autoimmune hypothesis of a subset of schizophrenia.52,53 The proposal is that if AN is an AD, it may be co-existing with DM type 2, or the DM type 2 itself may even be an extension of the same autoimmune process. In other words, there may be a continuum of pathological process between AN and DM type 2. It follows that schizophrenia sufferers may have a predisposition to develop DM type 2; schizophrenia may even be considered as a clinical surrogate of DM type 2.
When AN occurs in a schizophrenic patient, they sometimes develop a delusional misinterpretation of the condition, such as that it is a result of skin cancer or even a manifestation of an external agency. Such situations may result in severe anxiety. Schizophrenia is frequently associated with poor lifestyle choices on the part of the patient, such as a diet high in fat, reduced levels of physical activity, and high rates of smoking-all of these may contribute to the development of a metabolic syndrome and insulin resistance.54,55 It is worth considering investigation into the early warning signs for DM type 2 – including the AN – before commencing a patient on antipsychotic drugs that lead to a metabolic syndrome.
It is now well recognised that patients treated with clozapine or olanzapine are more often classified as having DM type 2 or impaired glucose tolerance in comparison with patients treated with other second-generation antipsychotics. Clozapine increases the risk of diabetes if there is a history of pre-existing diabetes or a family history of diabetes. According to a US study, the risk is higher if the patient is African-American or of Hispanic origin. Such patients may need close blood sugar monitoring during the initiation of clozapine treatment. I contend that if a patient already has AN, weight-increasing antipsychotics should be avoided. Even though aripiprazole is the most metabolic-sparing agent among the second-generation antipsychotics, Manu et al. report a case of AN in a patient treated with it. That patient did have a family history of DM type 2, which adds to the interest of the case.56
Diagnosis and treatment
There is no specific treatment for AN. Treatment is directed towards the specific symptoms that are apparent in each individual. It should be borne in mind that such treatment may require the coordinated efforts of a team of medical professionals. Correcting the underlying disease improves the skin symptoms. Steps that may be taken, depending on what the disease is, include correcting hyperinsulinemia through diet and medication, encouraging the loss of weight in those with obesity-associated AN, removing or treating a tumour, and discontinuing a medication that causes AN. The control of obesity contributes significantly to reversing the whole process, essentially by reducing both insulin resistance and compensatory hyperinsulinemia. However, the pigmentary changes may persist. In drug-induced AN, offending medicines should be stopped. In hereditary AN, lesions tend to enlarge gradually before stabilising and/or regressing on their own.
For those with AN, the recommended treatment may include the use of certain synthetic, vitamin A-like compounds (retinoids). For individuals with malignant AN, disease management requires treatment by oncologists. Reports indicate that AN has improved with therapy used to treat underlying malignancies and has reappeared with tumour recurrences. Other treatment for this disorder is symptomatic and supportive. The treatments considered are used primarily to improve appearance, and include topical retinoids, dermabrasion, and laser therapy. The final outcome of AN varies depending on the cause of the condition. Benign conditions, either on their own or through lifestyle changes and/or treatment, have good outcomes. The prognosis for patients with malignant AN is often poor as the associated cancer is often advanced.
AN may be diagnosed on the basis of thorough clinical evaluation, identification of characteristic physical findings, a complete patient history including medication history, a thorough family history, and various specialised tests.57 The age at detection will vary, depending upon the form of AN present and on other factors. For example, benign forms of AN often become evident during childhood or puberty. It is less common for benign AN to be apparent at birth or to develop in adulthood. The latter cases most typically involve AN in association with obesity.
In individuals with skin changes that suggest AN, diagnostic assessment may include various laboratory tests. Examples are the glucose tolerance test and the glycated haemoglobin (HbA1c)test. Additional laboratory studies or other specialised tests may also be utilised in diagnosis in order to help detect or rule out certain other underlying disorders – including a number of endocrine and autoimmune conditions – that may be associated with AN. In addition, in some instances, particularly where the patient presents with signs suggestive of malignant AN, testing may include biopsy and microscopic evaluation of small samples of skin tissue affected.
The onset of malignant AN usually occurs after the patient reaches 40 years of age. Various factors may be indicative of malignant AN in association with an underlying cancer. These include symptom onset in adulthood that is not associated with the use of particular medications, obesity, a positive family history, and certain underlying disorders known to be associated with AN. It is rare for malignant AN to develop during childhood. In such instances, warning signs may include skin changes that progress rapidly and also involvement of the mucous membranes.58
AN may be metaphorically linked to the dark pigmentation that appears on the skin of the ripe Sharon fruit. Sharon fruit is the trade name for a variety of persimmon that is grown in Israel. In the fruit the dark patches on the ripe and sugary fruits are the result of condensed tannins. Insulin-resistant AN may be referred to as the Sharon fruit sign in order to emphasise the diagnostic value of the condition. It has been suggested that the official terminology for AN is inappropriate for a significant warning of an increasingly common disease for which early diagnosis is imperative. Because the complex name may have a negative impact on its identification by both clinicians and patients, a less formal term is in use among some of those who are concerned with patient care. It must be borne in mind that AN, otherwise Sharon fruit sign, manifests only in those with the insulin-resistant condition and should not be considered a characteristic feature of DM Type 2. Identification of the Sharon fruit sign may be helpful in the early diagnosis of DM type 2.
Discussion
Diabetes puts an enormous burden on patients, their families, and the health-care system. Detection of the disease at an early state using physical markers and instituting preventive measures will reduce the economic strain on society to a great extent. According to the latest global data from the World Health Organization (2016), an estimated 422 million adults are living with DM type 2 and diabetes prevalence is increasing rapidly.59 In 2013 the International Diabetes Federation estimated that 381 million people were living with diabetes.60 That number is anticipated to almost double by 2030.61 About 3.8 million people in the UK have DM type 2, and the charity Diabetes UK has made predictions that it may become as high as 6.2 million by 2035/36.
Most often a diagnosis of DM type 2 is made only when such symptoms as loss of weight, polydipsia, and polyurea have become manifest. By that time the damage to the body may have already come about. Complications arising from diabetes cover the entire area of medical science, so early detection is crucial. Intervention at the prediabetic stage helps to arrest the progress of this condition. AN may herald DM type 2, endocrinopathies, and malignancies. This cutaneous disorder is easily detectable and highly useful in the early detection of the disorders associated with it. Early screening for AN in preadolescent and adolescent people would provide a relatively simple, inexpensive, and non-invasive tool for identifying those young people who have hyperinsulinemia and could benefit from early intervention. That would prevent the development of DM type 2. Young people tend to be reluctant to undergo traditional screening measures and definitive diagnostic tests as they find them invasive and unpleasant.
A sedentary life style and unhealthy dietary habits – as well as the side effects of antipsychotics – make chronically ill psychotic patients more vulnerable to DM type 2 than the general population. Long-standing detained patients in particular are restricted in their mobility and may become more prone to obesity and insulin resistance. It is not clear whether the pathogenesis of psychosis itself has a diabetogenic effect. It is evident that because of the high incidence of DM type 2 among mental health service users, psychiatrists need to become more alert in the diagnosis, management, and prevention of the complications of DM type 2.
Within the United Kingdom, all doctors are expected to teach.1 It is assessed throughout their professional career, during annual appraisals for doctors in training and during consultant revalidation. But how are those just embarking on their medical career expected to develop the necessary teaching skills? As three educators at various stages in our clinical careers, we developed and delivered a small course with the aim of addressing this issue.
The General Medical Council within the United Kingdom, suggest that a basic comprehension of teaching should be gained during the undergraduate and postgraduate training of doctors.2 Dandavino et al. further suggest that early development of these teaching skills may have additional benefits for the clinician; such as improving communication and assisting undergraduates to develop their own ability to learn.3 Our local training region, Yorkshire and the Humber Deanery (HEYH), have a mandatory post-graduate training day in teaching skills which focuses on generic and clinical teaching skills. This is delivered towards the end of the first foundation year. It is delivered by doctors who have various roles in medical education. Whilst useful in its content, for many it comes late. Doctors have often already been involved in providing teaching to medical students on placement at this time.
AMC recalls from her first postgraduate (foundation) year. One peer was thrilled to have ‘shaken-off’ a final year medical student who was supposed to accompany them on a shift as a learning experience; stating that they were now able to ‘do some work’. She couldn’t understand the desperation to escape one-to-one teaching. On reflection, it was probable that her colleague found it overwhelming to incorporate the additional responsibility of teaching alongside an already stressful clinical workload. Many share these feelings, with new doctors finding time pressures along with competing clinical demands a challenge to implementing clinical teaching.4
We thought that giving our graduates simple tools to understand and overcome these challenges may empower them as teachers. It may also improve their confidence in other areas, such as in their own learning and presentation skills.5-6 This paper proposes a solution; after creating a short course to be delivered immediately following graduation, to empower new doctors as teachers by providing some basic training in clinical teaching. These doctors are then able to use this training as soon as they begin their foundation training, which is ultimately the beginning of their teaching career.
Methods
Two versions of a half-day course, titled ‘Teach the Medic’ were developed in HEYH which ran in successive years. The original course was designed by a surgical trainee (AMC) and a general practitioner running the undergraduate education curriculum (MS). Initial topics were chosen based on experiences of the authors and colleagues. The optional course (see figure 1), was offered to the cohort of Leeds medical students who were in the transition period between finishing their final examinations and commencing their first post as a doctor.
Figure 1: A representation of the initial course structure. Stations were developed as interactive lectures and delivered to participants by doctors of various training levels.
The initial course received encouraging verbal and written feedback from the participants, which was collected on the day of the course. Further feedback was collected a few months into foundation training, allowing enough time to pass for delegates to use this knowledge. This feedback, whilst encouraging, included that delegates were keen for additional workshop style sessions. Subsequently, a modified half-day course ran the following year, with the recruitment of additional postgraduate teachers (including LES). A further 17 newly qualified doctors from various medical schools completed the course, prior to commencing their HEYH foundation post. This modified course (see figure 2) included scenario based sessions around potentially difficult situations for the clinical teacher, and also explored alternative styles of teaching that could be adopted successfully in the workplace.
Figure 2: A representation of the modified course structure. Building on feedback from the initial course, the three co-authors incorporated new small group scenario based discussions, alongside the interactive lectures.
Results
Initial feedback received from evaluation of the day was positive for both courses. For the second course, initial feedback found that all participants found every session very good (71%) or good (29%) overall. 12/17 (71%) thought that the course should be made compulsory to medical students. We also sent a follow-up survey, distributed six months after the course which generated 14 responses. All respondents felt that the course should be run again. All participants either strongly agreed (n=2, 14%) or agreed (n=12, 86%) that they felt more confident in teaching compared with their peers. Regarding individual sessions, 10 participants (71%) had directly incorporated learning from the ‘Teaching Theory’ session, 12 (86%) from the ‘Teaching for your Learning and Portfolio’ session, 11 (79%) from the ‘Teaching your Peers’ session, and 10 (71%) from the ‘Scenarios’ workshop. All participants stated they would still recommend this course to colleagues. They also reported directly incorporating their learning from the sessions into their teaching practice. The responses gathered from the second course implied that participants felt more confident in teaching when compared to their peers.
Discussion
We feel the course content in ‘Teach the Medic’ complements other courses available later in one’s career, such as the Royal College of Surgeons’ ‘Train the Trainer’ course. We propose this course could be run by a junior doctor who has a strong interest in clinical teaching with involvement of a senior colleague with extensive medical education experience. We felt the course was especially beneficial as participants had continued to find it useful long after its delivery.
To expand this project to include a whole year group as a compulsory course is ambitious. It would require development and the use of more resources, but initial feedback suggested participants will find it extremely useful. Bing-You et al.6 agree, having found that undergraduate students would be willing to undertake formal instruction in clinical teaching prior to graduation.
As our short course gains momentum within HEYH, this prospect becomes more achievable. When considering a wider delivered course, one must remember that attendance to ‘Teach the Medic’ was optional; suggesting that those who attended had already identified an interest in teaching. This has the potential to bias our data to some degree. However, we still believe that making the session compulsory would allow skill development and empowerment for those who may not consider themselves aspiring medical educators, but who are still in positions to deliver teaching.
Conclusion
Our evolving teaching skills course suggests that close work with both local medical schools and deaneries is important to allow this course to be incorporated into the training of newly qualified doctors. This may be included as a compulsory part of the final year medical school curriculum, an option for a SSC, or as an integrated part of the new starter induction programme delivered by individual hospitals.
Medical scientists who espouse a strict biological model of the mind tend to care less about the prolongation of life than do those who have faith in higher authority.1 The prevailing reductionist model of mind has recently been challenged effectively.2,3,4,5. That has led to a position in which there is some justification for claiming that there is scientific evidence to enable a suspension of disbelief in life after death. 6 Medical profession should respect the theology veiled in thanatology and should be careful not to become instrumental in creating a culture of death; alleviating suffering is not by eliminating the patient.
In the absence of spiritual conviction, human suffering lacks deep meaning and death is regarded as the ultimate tranquilliser. Prolonging life at any cost may be perceived as a worthless endeavour. To counter that, without suffering evolution would not take place and human consciousness would fail to expand. Without stress and struggle the spirit buds to which we may be likened would not mature and grow leaves and fruit, and our characters would not develop; we would lead the lives of lotus-eating sybarites. 7
Evidence for discarnate survival
According to those who are sceptical about after-death survival, there is only as much evidence to justify belief in life after death as there is for the historical existence of dinosaurs. Some scientific researchers however argue that there are compelling reasons to support those who are proponents of belief in life after death. Dr Vernon Neppe, a neuropsychiatrist turned parapsychologist, has declared that the combined body of evidence for discarnate survival is overwhelming – so great that it may be regarded as scientifically cogent.8 This emerging scientific view, coupled with the wisdom of the faith traditions, challenges the rationality of supporting assisted suicide. The following are examples of evidence for discarnate existence that are commonly cited:
clinical death experiences
pre-death visions
shared death experiences
collective apparitions
some forms of mediumistic incidents, particularly ones that involve cross-correspondence, drop-in communications and physical phenomena
children’s memories of previous lives
electronic voice phenomena
instrumental trans-communications
transplant cases
Scientifically studied Marian apparitions
The list is becoming longer as survival research progresses. Encouraged by the success of afterlife experiments with mediums,9 the multi-specialist professor Gary Schwartz of Arizona University claims to have invented a device to communicate with discarnate spirits; the holy grail of survival research that could possibly offer a fool proof scientific evidence of afterlife existence,10 but also takes account of all the potential negative consequences. He claims to have worked with black boxes in his laboratory, using a software programme that has generated proof that there is a spirit world by measuring light. 11It appears that he has developed a technique whereby faint light can be detected in a totally dark box. Measurements are taken at the beginning of an experimental session, and then a specific “hypothesized spirit collaborator” is asked to show a “spirit light” in the box and a second reading is taken. The finding is that instruction for specific spirits to enter a light sensing system was associated with reliable increase in the apparent measurement of photons. Such a curious result means that these communicating spirits are able to hear, respond and produce light in an otherwise dark enclosure. 12,13 The conclusion is that survival research opens up new vistas which seem much more important than cosmology or quantum electrodynamics.
Scientifically examined Marian apparitions are a recent addition to the evidences for discarnate existence. 14 Mainstream scientists seem never to have attempted to develop the conceptual tools and vocabulary needed to investigate the possibility of post-mortem existence. It may be that science will not accept the possibility of discarnate survival without a new theory of physical reality. In the early part of the twentieth century the prevailing view of scientists was that there was no possibility whatsoever of proving the existence of life after death. Over the years that have passed since then attitudes have evolved, and in the world, we are now in it is asserted by some researchers that there is scientific evidence for the existence of life after death. Some of the evidence relating to discarnate existence may not however satisfy the criteria of the physical sciences since the latter are based on speculative science and court room logic.
Paradigmatic shift
Demonstrating post-mortem existence as an irrefutable phenomenon is a route to establishing empirically that humans have a higher consciousness. Unfortunately, in survival research there are many phenomena that have multiple possible explanations, and these augments add to the complexity of this immensely significant area of scientific enquiry. All the types of evidence postulated as supporting discarnate survival are simultaneously a form of evidence of a non-biological component that operates in association with the brain. The existence of a non-biological component indirectly proves the possibility of survival after physical extinction. A huge paradigmatic shift towards non-reductionism is now taking place in the cognitive sciences – consciousness is no longer considered an epiphenomenon of brain activity, but asthe designer and prime mover of the material body. Nowadays, some mainstream scientists are themselves paradoxically trying to debunk mainstream science.
Suicide victims
Through suicide, a person is simply changing the location of their suffering. While wrapped in the physical planet by space and time, we are in an advantageous position for inducing personality changes swiftly, whereas in the timeless state of discarnate existence changes are sluggish and personality development is much slower. Contemporary data for survival research may be congruent with the wisdom of the faith tradition. 15 To use a simple analogy for this, carrying out assisted suicide is like destroying the shell of a pupa and forcefully freeing it in a premature state. Such a pupa will not be able to fly about like a butterfly. It is arguable that a person subjected to violent death – as in the case of suicide – may not be able to enjoy the beauty of God’s grand other-worldly dimensions until they have become spiritually compatible with them. They have to navigate through the physical plane like wingless birds. 10 To look at this way, if fruit that is unripe drops from a tree, it will be sour. Suicide breaks a solemn law because it deprives the conscious self of the natural growth that life in a physical body can best provide.7The Chinese saying “One day of earthly existence is not equivalent to a thousand days of ghostly existence” is a statement of the sanctity of terrestrial life.
Lord Alton has campaigned against the Assisted Suicide Bill of 2014 since its inception. Referring to his dying father’s account of how he had seen his own brother, a member of the Royal Air Force who had died in the Second World War, Lord Alton argued that a forced death, as opposed to a natural one, may deprive a person of their “healing moment.” 16 A graceful and natural death may be supposed to be accompanied by benign caretaker spirits with exuberant love who assist those who are dying by making them comfortable for the big transition.17,18 A person who terminates their own life prematurely may not be so fortunate as to get such benevolent assistance from the spiritual realm. Most hospice workers are very familiar with departing and death-bed visions such as that described by Lord Alton. Furthermore, it has been suggested that beings from the imperceptible spiritual sphere who assist in delivery from the terrestrial plane have a role in such matters as the timing of death, and it is arguable that their part in what happens should not be impeded by intervention.
It appears that human brain is designed to have some doubts about discarnate survival for some reason and a fool proof evidence of post-mortem existence may have its down side in that somebody who is fed up of life might use it to justify ending his earthly life voluntarily. 19An ultra-optimistic view of discarnate life is spiritually counterproductive and such an over optimism could be seen as a justification by the patient and carers in the decision making of assisted suicide. In a weak moment of extreme psychological or physical sufferings, such a belief can also become the final rationalization for ending one’s own life voluntarily. In my own clinical practice, I have come across suicidal patients telling me, “It will be always better on the other suicide.” A belief in discarnate existence based on parapsychological proof alone did not deter one such patient making a serious suicidal attempt
End-of-life concerns
The evening of life was considered as a great opportunity for spiritual, emotional and psychological growth and a celebration of one’s life journey. These are also times to harvest the wisdom of yesteryears and share them with the succeeding generation. Spiritually enlightened people consider this to be the time to conquer the fear of death. Fear of death is not the fear of the physical pain of death, but the fear of truthful self-judgement after death. Recent observations in thanatology favour a belief in post-mortem self-assessment and appraisal. For some, it would be voluntary or assisted, whereas for others it could turn out to be forced upon them. The final phase of life is the time to settle the errors committed against fellow beings that have not been remedied in life. Fortunately, modern medicine has prolonged this period, which grants an opportunity for most people to experience conscious ageing. Sadly, traditional attitudes towards the evening of life have changed in today’s youth-obsessed culture. For some, medical procedures have extended life and made dying a lingering process rather than a sudden event, and have contributed their own problems. For several reasons, terminally ill people who are in crisis may wish to die rather than being kept alive longer (Table 1).
From an evolutionary point of view, there can be only a survival instinct – no Freudian death instinct. Avoiding death rather than seeking it is a natural human urge and the fear of death may affect every individual action. The very concept of euthanasia is totally against the human make-up and is entirely artificial. Assisted dying and assisted suicide are the same thing when a member of the medical professional gives a lethal drug to a person so that they can take their own life. Euthanasia is different; it happens when, for example, someone injects a lethal substance into a patient. Involuntary euthanasia refers to a situation in which the patient has the capacity to give consent, but has not done so; and in non-involuntary euthanasia a person is unable to give consent, for example because of dementia or being in a coma. Mercy killing is claimed to be a compassionate act to end the life of a patient.
Table 1: End of Life Concerns
Losing autonomy
Less able to engage in activities making life enjoyable
Loss of dignity
Burden on family, friends/caregivers
Losing control of bodily functions
Inadequate pain control or concern about it
Financial implications of treatment
Moral and ethical issues
It has been observed that the risk of suicide is higher among people with a family history of suicide. Family culture and genetics may account for the increased incidence of suicide in such situations. Assisted suicide would create a trail in the culture of more families and more succeeding generations would perhaps be at increased risk of considering suicide as a serious option at a time of crisis. Kevil Yull (2013) comments that changes in the law of assisted suicide would have an additional impact on those left behind, because of their effect on the moral connections, assumptions and accepted responses to situations on which we base our relationships with fellow human beings and establish ourselves in the world. 20 He argues that the legalisation of assisted suicide would undermine freedom instead of promoting freedom of choice, and also that the proposed safeguards and regulations would breach the privacy of the death-bed.
Assisting someone to kill themselves is assisting them in murder. According to all the major faith traditions, life is a gift from God and ending it is like throwing a precious object back to the giver. All spiritual traditions teach and believe that bringing the human heart to a standstill is God's business (Table 2). There are patients who assert that even if all their limbs were amputated, they would still want to hold on to the treasured gift of life. It is very difficult to define what unbearable suffering is; extreme suffering is a subjective matter that it is not possible to separate from an individual’s outlook on life. A fundamental question is that of who would be the one to pronounce a verdict on when suffering is intolerable – the patient or medical personnel?
Laws are not precision-guided arrows and they may become perverted. In a world full of violence and crime, assisted suicide is unsafe and could be exploited. There would be many unintended consequences. For reasons of public safety alone, some people oppose assisted dying. Financial abuse by relatives of the elderly seems to be becoming more common; those with a vested interest could be tempted to put an inheritance before life.
The regulation of assisted dying has been modified in recent times in some countries, an example being the Netherlands in 2014. There it is now lawful to kill a patient without their consent, and euthanasia and assisted suicide may be offered to people with mental health problems (consensus with the family is required in all these situations). Inboth Belgium and the Netherlands the euthanasia of children is legal with family consent (in Belgium there is no age limit; in the Netherlands the child must be 12 or above and must give consent). In Belgium blind adults who were developing further problems were granted euthanasia at their own instigation a few years ago. There is public concern about collaboration between euthanasia teams and transplant surgeons in Belgium.
Table 2: Medical dilemmas
Assisted suicide promotes a human right to commit suicide and gives wrong messages to suicidal patients in psychiatry.
It undermines the Universal Declaration of Human rights and strikes at the foundations of all spiritual values.
It is hard to define unbearable sufferings.
Assisted suicide has many unintended consequences.
Death with dignity could deteriorate as death with indignity.
It might permit the unlawful killing of innocent people in certain circumstances.
It is founded on unethical principles-survival of the fittest.
In 2013, 1.7% of all deaths in Belgium were hastened without the explicit request of the patients. 21 Professor Cohen Almagor, the author of 2015 report on euthanasia in Belgium stated that the decision as to which is no longer worth-living is not in the hands of the patient but in the hands of the medical personal. 22 More than 500 people in the Netherlands are subjected to euthanasia without their consent.23 Data from Oregon where assisted suicide was legalised in 1977 shows that the top five reasons people choose assisted suicide are not because they are suffering from a terminal illness and 49% stated that feeling like a burden and a fear of loss of control are among the main reasons for choosing assisted suicide Oregon .24 In Washington state in 2013, 61% of people who were killed in assisted dying said that being a burden was a key factor for their choice of death. 25
Medical Dilemmas
Majority of British medical practitioners are against assisted suicide. 26 A 2013 survey showed that 77% hold the view that they would oppose a change in the current law to allow assisted dying, 18% favoured the RCGP moving to a neutral position, and only 5% favoured a change in the current law. They opined that a change in the law would make patients afraid of their doctor and would alter doctor –patient relationship, and would make vulnerable patients most at risk from assisted dying. According to Marris bill, some people should be given help to die meaning that some lives are worth less than others. Vulnerable people would feel pressurised to choose death and could be killed without their explicit consent. GPs feel that it is their privilege to protect the disadvantaged and vulnerable people of the society.
Assisted dying would lead to less focus on investment in palliative care. The RCGPs also cautioned in the survey that a change in the position of the law makers would become like abortion legislation, which started as something for extreme circumstances and is now effectively on demand. They are also anxious for the fact that legalisation of assisted dying would make it impossible to tell the real reason why patients decided to die, because illness can cause people to become depressed and frightened. As debate on assisted suicide has become hotter, in clinical practice suicidal patients have already started enquiring about the prospects of assisted death.
Thanatology
Medical sciences have not advanced enough in matters of death to offer details to make informed choice for those who want to die voluntarily and thanatology is only a fledgling science. Thanatology is the scientific study of death and investigates the mechanisms and forensic aspects of death, such as bodily changes that accompany death and the post-mortem period, as well as wider psychological, parapsychological and social aspects related to death. They are not particularly interested in the meaning of life and related philosophical issues, but this is an area where science and philosophy not be separate. In recent years, studies of parting visions by Elizabeth Kubler Ross and Raymond Moody’s NDE studies. 27,28,29,30,31,32 have given a spiritual dimension to thanatology. Theology and Thanatology are two major corpuses of human wisdom that cannot but overlap. Assisted dying would probably become also an issue of forensic sciences.
It is the job of the doctor to keep the patient alive whereas it is the job of the psychotherapist to have a sense of a bigger picture. 33 People wanting to hasten death should also have the choice of receiving pastoral and psychotherapeutic assistances to distract themselves from their preoccupations of death and allow nature take its own natural course. New generation psychotherapists will have to be well versed in all aspects of death related sciences. Thanatology has a rightful place in medical studies, but I content that medical professionals need not to be unduly concerned about the different forms of afterlife existences, the borderland between religion and thanatology. Medical professionals are expected to be above religion and politics. Thanatologists now fear that if assisted suicide is legalised, they might be pressurised to slip from the original goal of acquiring more knowledge of human dying to serve the dying into the pursuit of death.
Concluding Remarks
Assisted suicide or euthanasia is incongruous with the theological view that it is the weakest and the vulnerable who can teach us the values of life and the concepts of euthanasia or assisted suicide have an indirect message of discarding them. The right to die would soon deteriorate as duty to die to prepare room for fittest ones. Instead of looking for reasons to live, people will be looking for reasons to die. What is need is better understanding of death process and advancements in the palliative care of the terminally ill, rather than doing away with them. Until we know more about the death process, assisted dying debate should be kept on hold. More research in palliative care and allowing people to die naturally with dignity should be the concern of medical profession.
Evolution may be taking place in biological and spiritual streams and they are interconnected: biological sufferings maybe aiding spiritual evolution. 34. From a philosophical perspective, the rationale of terminal sufferings is to help the individual to disengage from the “pleasant illusions” of earthly life. The debate of assisted suicide raises the question whether human beings are mere electrical animals, quantum beings or fundamentally spiritual personalities-humans maybe all the three.The sanctity of human sufferings need to be brought into the equation of assisted suicide discussion. Assisted suicide would only add to the growing violence in the present world that could do with reintroduction of principles of non-violence.
USA may have better legal infrastructure to negate the unwanted and unintended errors of assisted suicide, but in many third world countries, where there is no such legal infrastructure, the procedure would easily get dishonoured. Oriental religions as well as Abrahamic faith traditions are opposed to ending life voluntarily. In general, all faith traditions believe that life that is nearing the biological end need not be preserved at all costs and that one does not have to go to extraordinary lengths to preserve a terminally ill person’s life. This means, for instance, that while a terminally ill person should not be denied basic care, he or she could refuse treatment that might prove to be futile or unduly burdensome for the dying person - passive voluntary euthanasia.
A scientific belief in after death existence is not without its pitfalls unless it is accompanied by the spiritual corollary of sanctity of earthly life. Science alone cannot highlight the sanctity of life; Divine standards are helpful in comprehending the sacredness of life. In fact, science has taken us to a cross road with Professor Schwartz’s new instrumental communication and it is time mark the boundaries of healthy survival research and the unhealthy ones.
This case highlights a rare and interesting medical condition bought about by liquorice ingestion. While there have been many previous reports of liquorice toxicity secondary to eating confectionary, I have only found one case report of liquorice toxicity secondary to liquorice tea ingestion and the patient there had only a mild case of hypokalaemia and did not require hospital admission unlike patient X.1
Case presentation
Patient X is a usually fit and well 49-year-old woman who was admitted following a collapse. Prior to this collapse she had experienced a 3-week history of gradual onset, slowly worsening dull headache and a feeling of tingling in her hands which increased over this timeframe. On the day of admission, she experienced nausea. Her past medical history included migraines, for which she self-medicated with paracetamol, ibuprofen and codeine as necessary. She was also using Cerazette. She was in full time work, was a lifelong non-smoker and used alcohol very rarely. She had no family history of note.
On examination, Patient X was a slim individual who was hypertensive with a blood pressure of 170/100 mmHg. Her other observations were normal. Her general and neurological examinations were unremarkable.
While initially the medical team felt that Conn’s syndrome was a likely cause of the abnormalities, this was reconsidered on a ward round where, following research on the internet into her abnormalities, patient X brought it to the attention of the team that she had been consuming between six and eight liquorice tea infusions per day for the past two months and had been consuming around three a day for a significant period time prior to this (roughly 18 months). The diagnosis was made based on her history.
Investigations
A venous gas demonstrated a metabolic alkalosis with a pH of 7.57.
Blood tests revealed hypokalaemia (K+ = 2.2 mmol/L) and hypophosphataemia (PO4 = 0.35mmol/L). No other abnormalities were detected.
More specialist assays were undertaken, and demonstrated that her plasma renin was 2.3 ng/mL/hour (normal range 0.2 – 3.3 ng/mL/hour). Her morning supine plasma aldosterone level was 29 pg/mL (normal range 30 – 160 pg/mL). Her morning plasma cortisol level was 612 nmol/L (normal range 138-635 nmol/L).
In addition, the patient also underwent a CT head and a CT renal angiogram, both of which were normal.
DIFFERENTIAL DIAGNOSIS
Apparent mineralocorticoid excess
Exogenous mineralocorticoid excess
Liddle’s syndrome
Congenital adrenal hyperplasia
Cushing syndrome
Liquorice
Treatment
Intravenous potassium and phosphate replacement, cessation of liquorice intake and amlodipine 5mg OD.
Outcome and follow-up
The patient was discharged with a blood pressure of 132/66 mmHg on amlodipine, a potassium level of 2.9, and a phosphate level of 1.16. She was given oral potassium supplementation to be taken 3 times per day. After two weeks, the amlodipine was stopped as she became mildly hypotensive. Her blood pressure was 120/60 following cessation of amlodipine. Three months later her plasma potassium level was 4.6 without supplementation. Mrs X required no follow up although she reports an ongoing feeling of tingling in her hands.
Discussion
Liquorice is an extract of the roots of the Glycyrrhiza glabra plant and has been used as both a confectionary flavouring agent and a herbal remedy. It is also commonly used as a laxative, and as a flavouring agent in chewing gums, sweets, and food products.
The active ingredient in liquorice is glycyrrhetinic acid which inhibits the enzyme 11-β-hydroxysteroid dehydrogenase. This enzyme converts cortisol into inactive cortisone within the distal tubule of the kidney and so in liquorice toxicity there is a build-up of cortisol in distal tubular cells.2 This results in increased mineralocorticoid like activity as there are structural similarities between cortisol and aldosterone, with increased Na+ and water retention in conjunction with increased H+ and K+ excretion.3 Here hyperaldosteronism occurs, but with a low or low-normal plasma aldosterone and renin level. Serum glycyrrhetinic acid levels can be measured with enzyme-linked immunosorbent assay (ELISA) and high-performance liquid chromatography (HPLC). Urinary glycrrhetinic acid levels can be measured with gas chromatography-mass spectrometry (GC-MS).4
Pseudoaldosteronism secondary to liquorice consumption is a relatively rare occurrence. Case reports demonstrate a range of clinical manifestations from an asymptomatic patient fortuitously diagnosed to those with more severe presentations such as rhabdomyolysis, hypertensive encephalopathy, asthenia, paralysis, heart failure, and cardiac arrhythmias such as polymorphic ventricular tachycardia and ventricular fibrillation secondary to hypokalaemia. For these reasons, it has been suggested that the public should be made aware of the potential dangers associated with liquorice consumption. 5-13
The combination of alkalosis hypokalaemia and hypertension suggests increased mineralocorticoid activity leading to increased renal tubular Na+ reabsorption along with increased k+ and H+ excretion. Both primary and secondary hyperaldosteronism cause these abnormalities, the former via an appropriate response (renin release) to decreased renal perfusion pressure or decreased sodium concentration in the ultra filtrate, the latter an inappropriate release of aldosterone from the adrenal cortex, often a result of an adrenal adenoma.
Other genetic syndromes, such as Bartter’s or Gitelman’s, cause hypokalaemia with alkalosis but without hypertension.14
Features of low potassium include generalised weakness and lethargy, ascending paralysis, and rhabdomyolysis.15-17 Decreased intake is rarely a cause of low potassium as the western diet usually contains significantly more potassium than is needed and because the renal tubular reabsorption mechanism can be extremely effective in limiting potassium excretion.17
The maximum recommended dose of liquorice is 100mg/day although cases of liquorice toxicity have been reported in association with doses as low as 80mg/day. Each liquorice tea bag contains approximately 500mg of glycyrrhetic acid, of which approximately 20mg is ingested per infusion.
This is a relatively rare occurrence and it has been suggested that certain groups are more susceptible to toxicity than others – for example those with 11-β-hydroxysteroid dehydrogenase deficiency.18 It is also thought that those with essential hypertension are also more at risk.19
LEARNING POINTS/TAKE HOME MESSAGES
Consumption of liquorice can cause pseudoaldosteronism.
The clinical picture is similar to that of primary aldosteronism, but is characterised by low levels of both aldosterone and renin.
While liquorice toxicity can be asymptomatic, clinical manifestations are wide ranging and include cardiac arrhythmias, rhabdomyolysis, weakness and paralysis.
Pseudohyperaldosteronism caused by liquorice consumption is reversible and generally resolves upon cessation of liquorice consumption. Prior to resolution, potassium supplements are usually necessary.




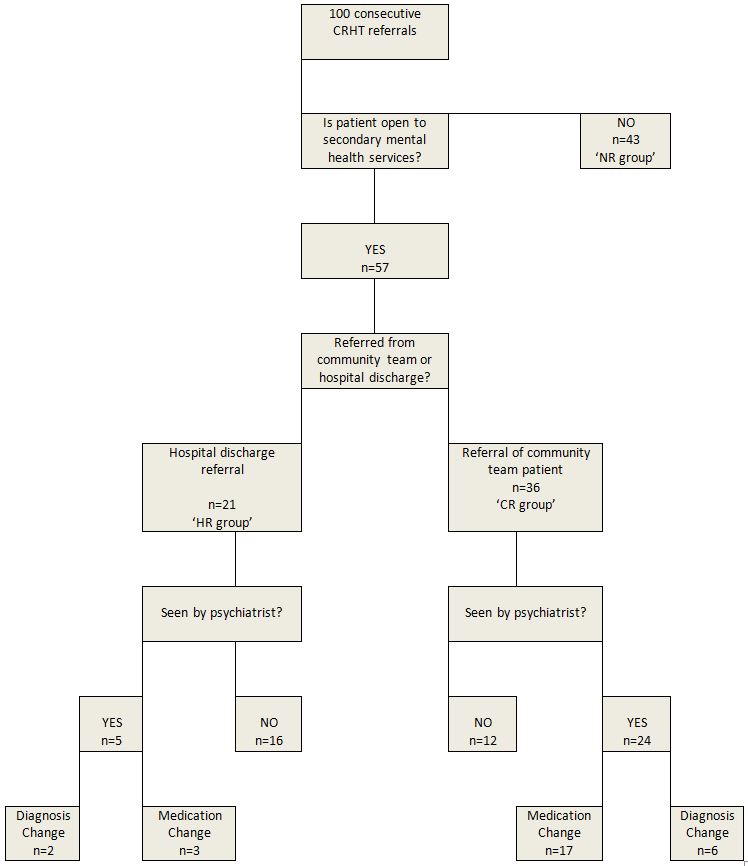
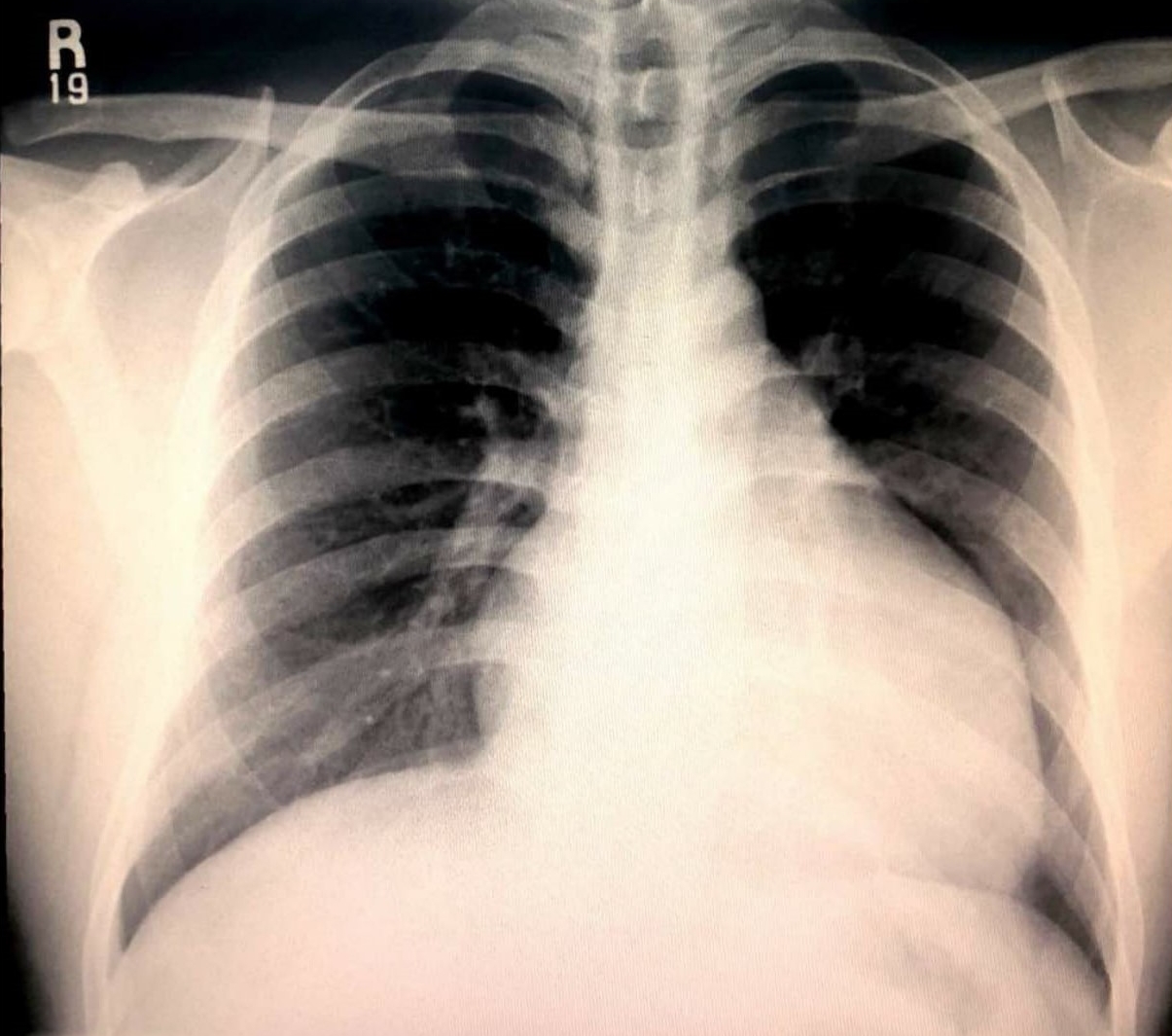
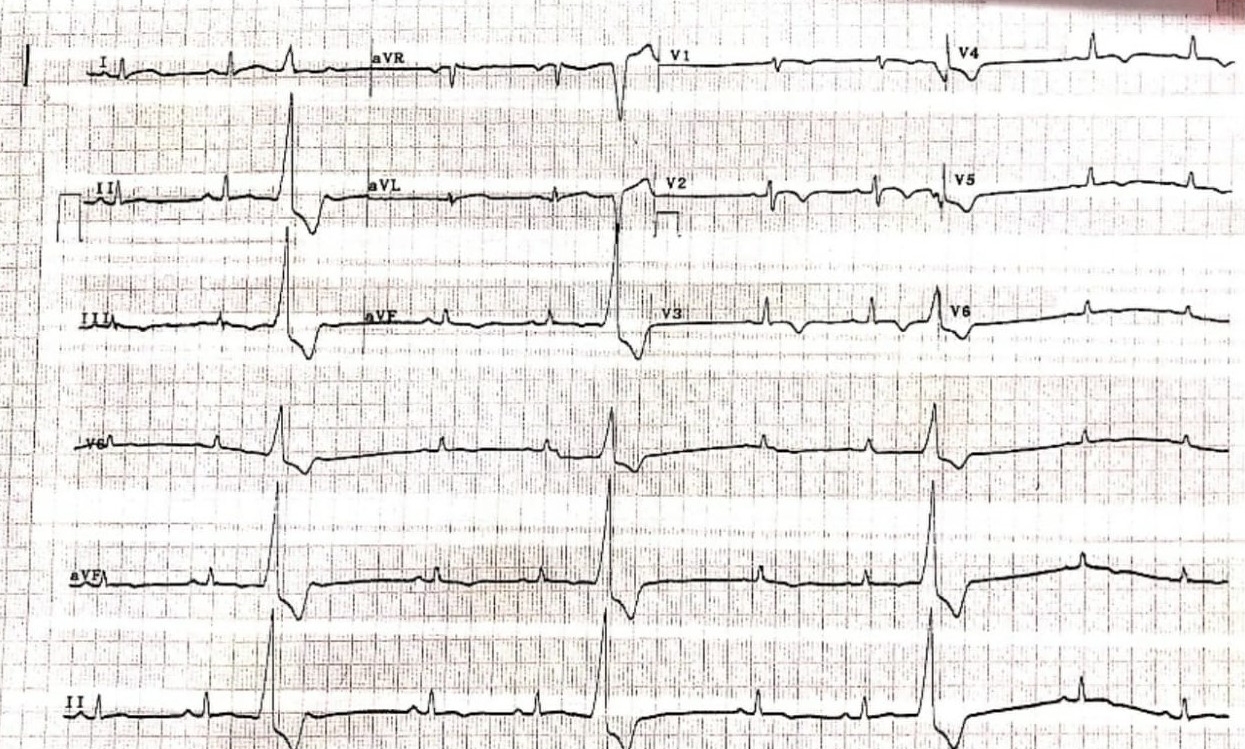
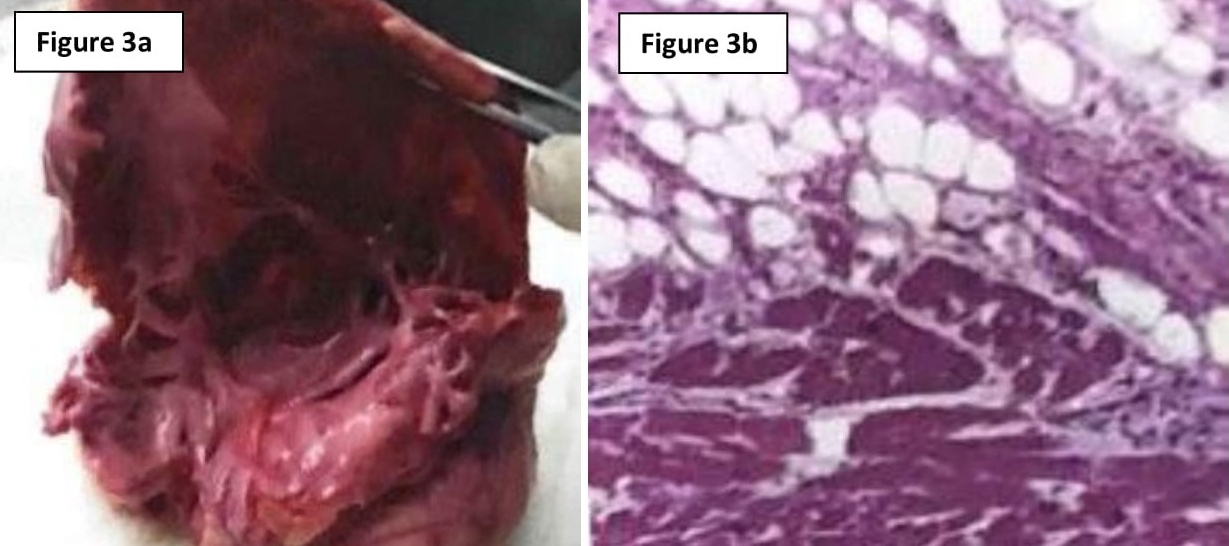
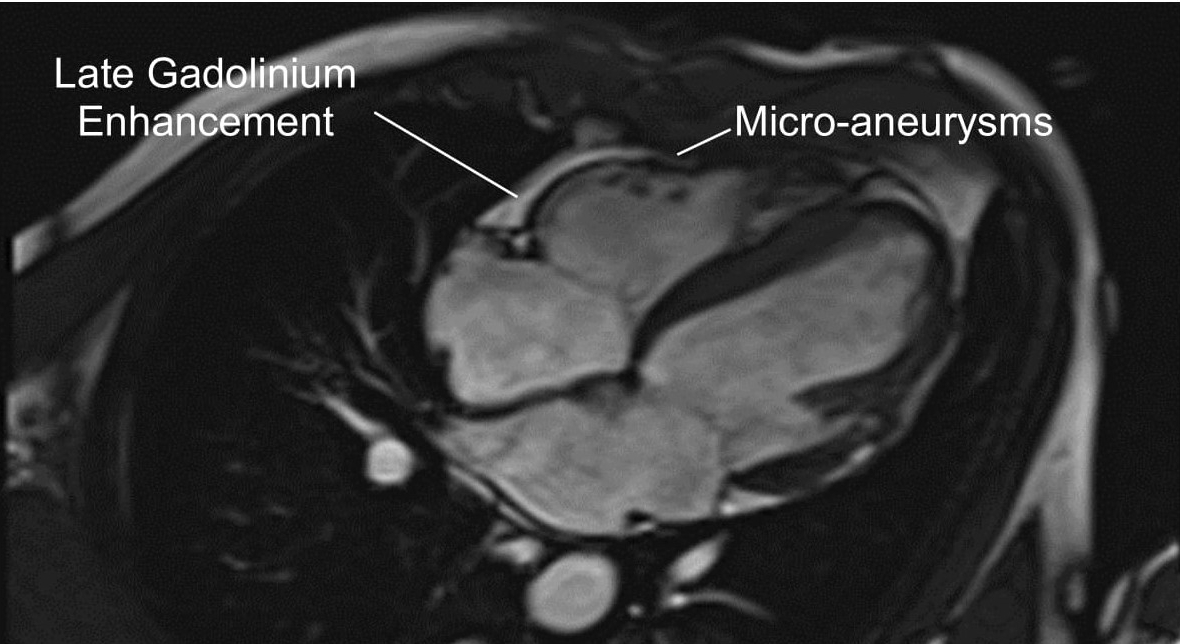
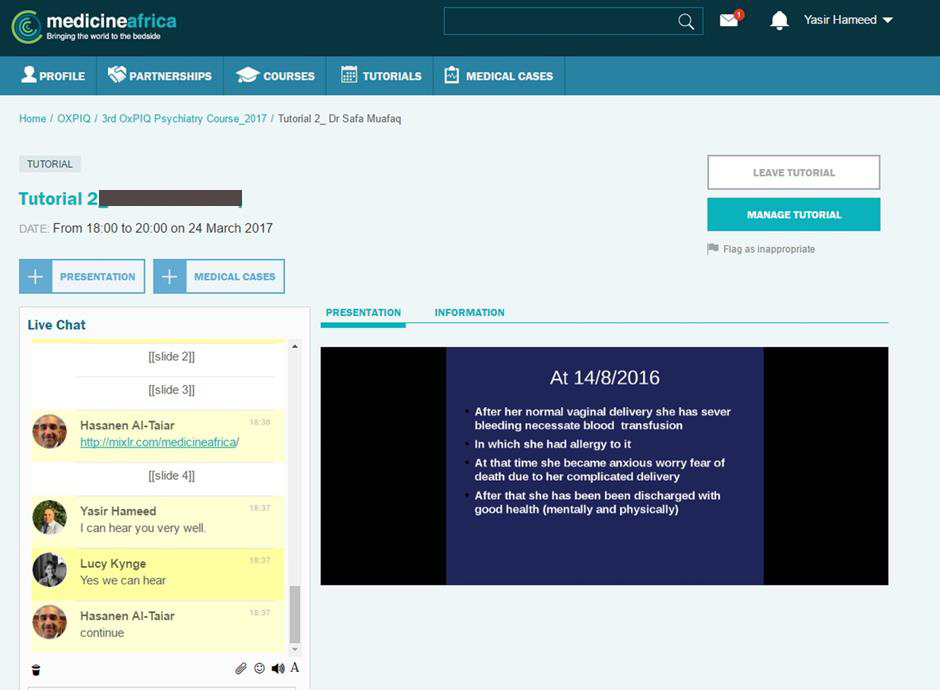
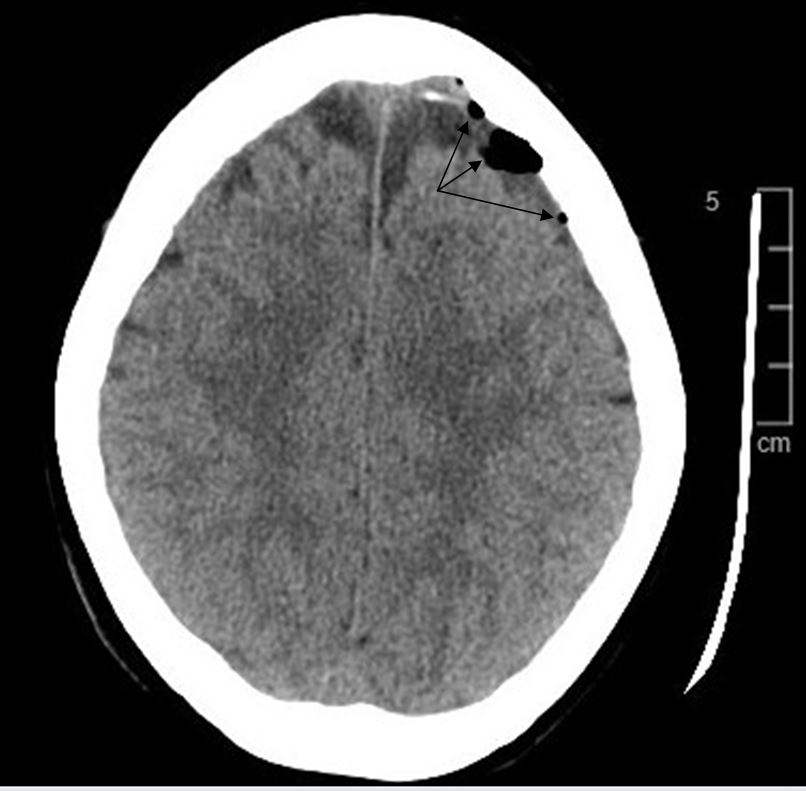

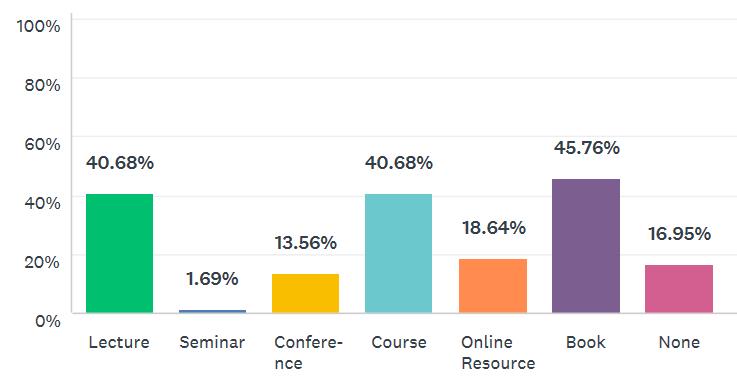
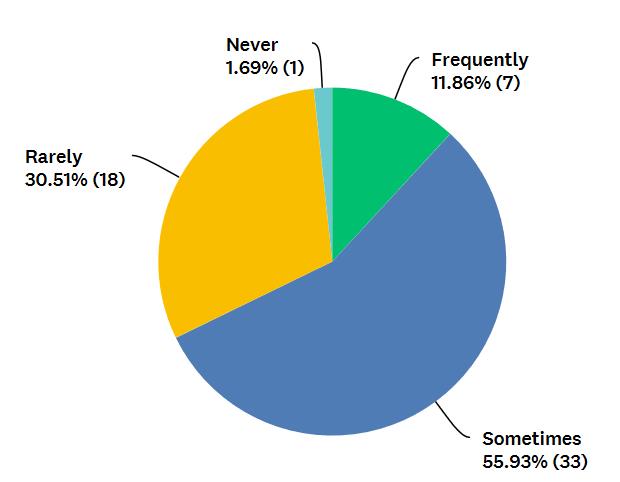
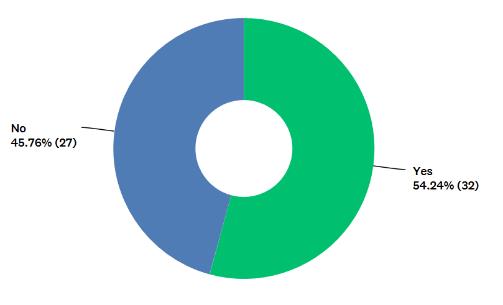
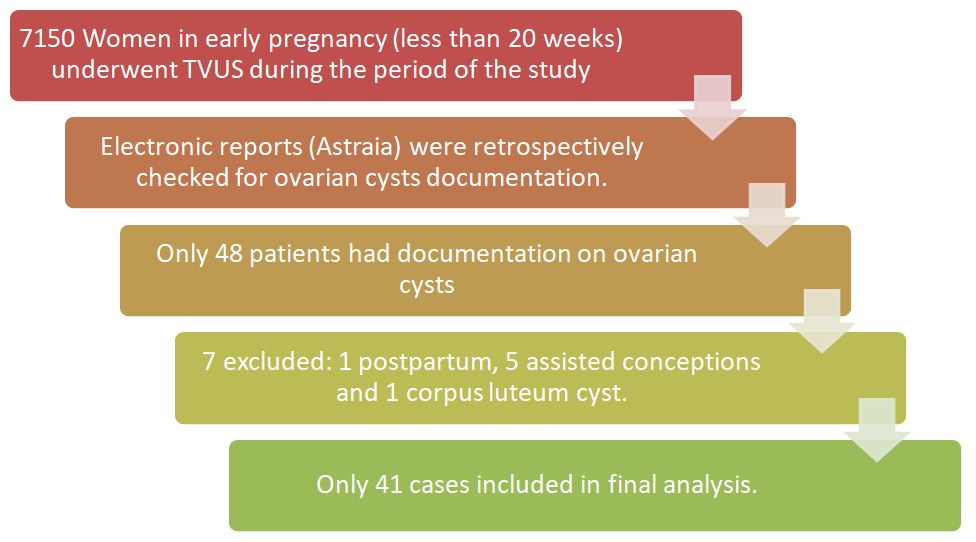
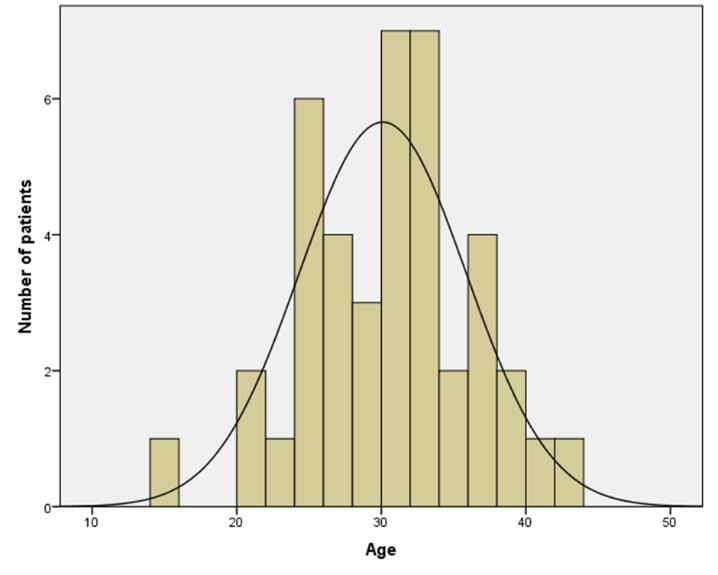
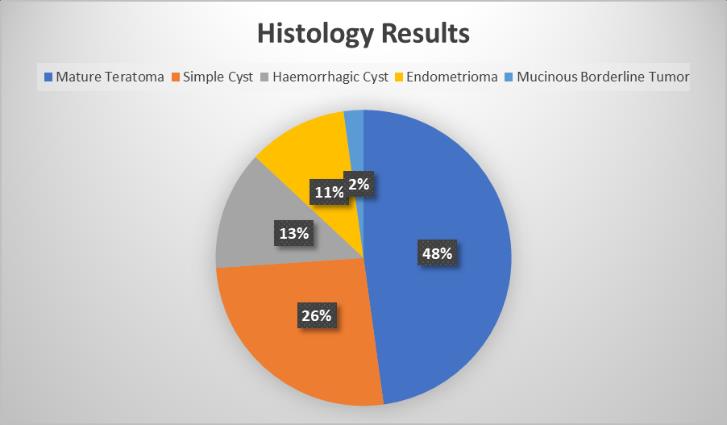
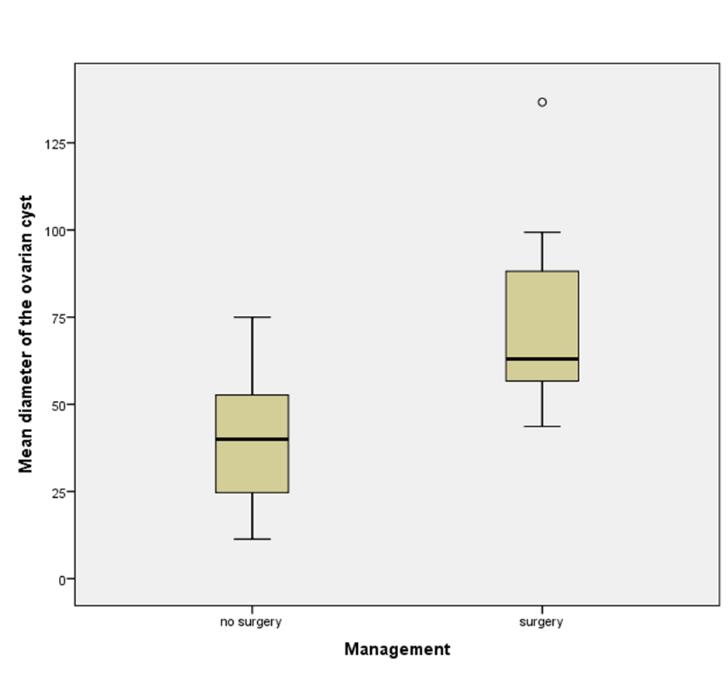
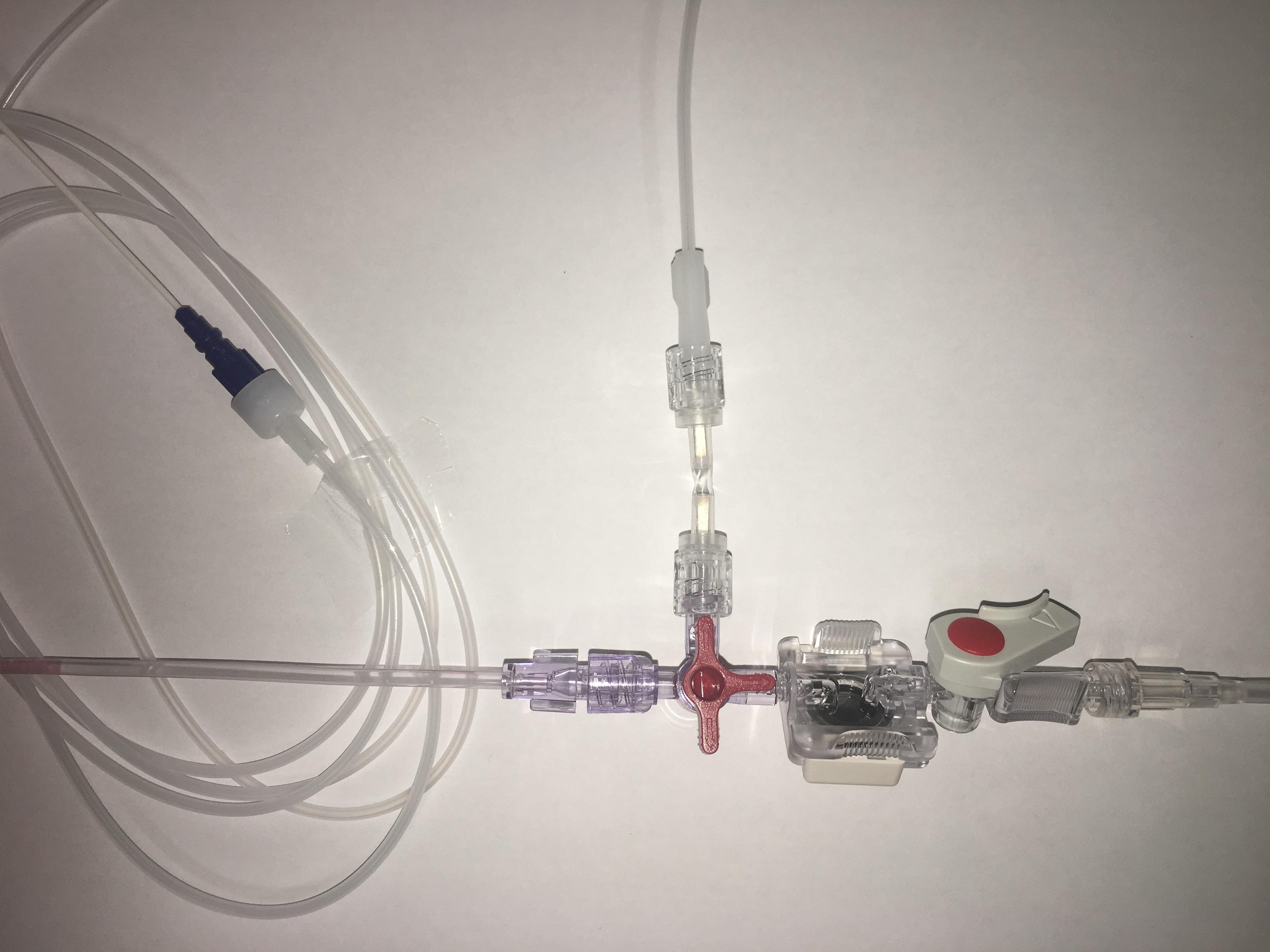




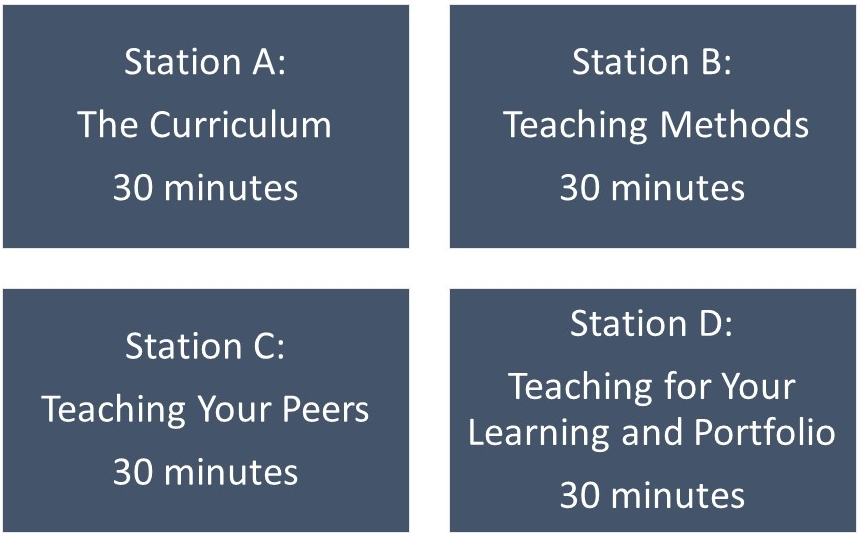
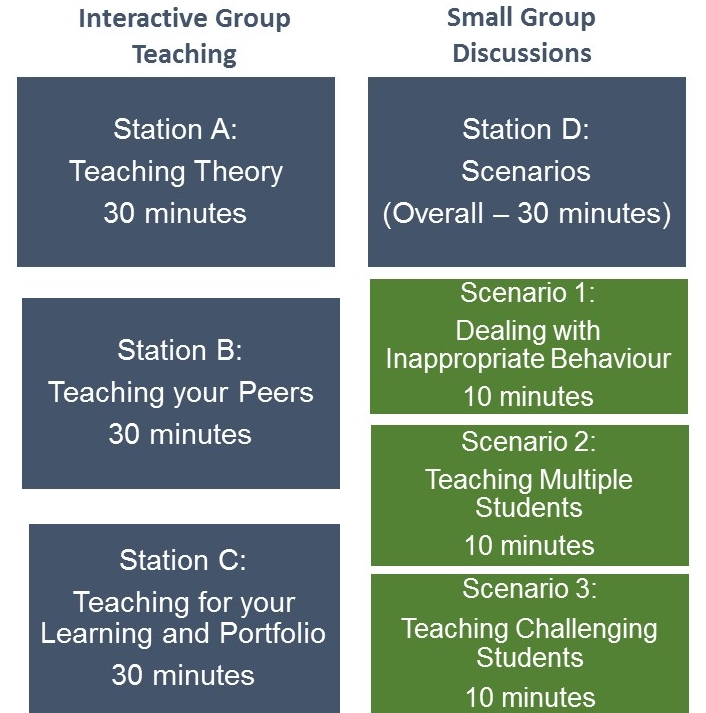
BJMP December 2018 Volume 11 Issue 2
BJMP December 2018 Volume 11 Number 2
Editorial
Case Reports/Series
Clinical Practice
Education and Training