



ISSN 1757-8515
Tracheo esophageal fistula
M Suresh Babu, Deepak Suvarna, Chandrashekhar Shetty and Aditya Nadella
Cite this article as: BJMP 2014;7(2):a717
|
|
Keywords: TEF - Tracheoesophageal fistula Abbreviations: TEF - Tracheoesophageal fistula |
A 40 year old patient presented to the hospital outpatient department with one year history of cough, choking sensation following swallowing, hoarseness of voice and loss of weight. History revealed his previous hospital admission 1 year back for management of organophosphorus poisoning during which he was intubated and put on mechanical ventilator for 10 days. Patient developed the symptoms a month after his discharge from the hospital. Cranial nerve examination was within normal limits. What is the possible diagnosis?
- Gastro-oesophageal reflux disease
- Tracheo-oesophageal fistula
- Oesophageal diverticula
- Oesophageal rupture
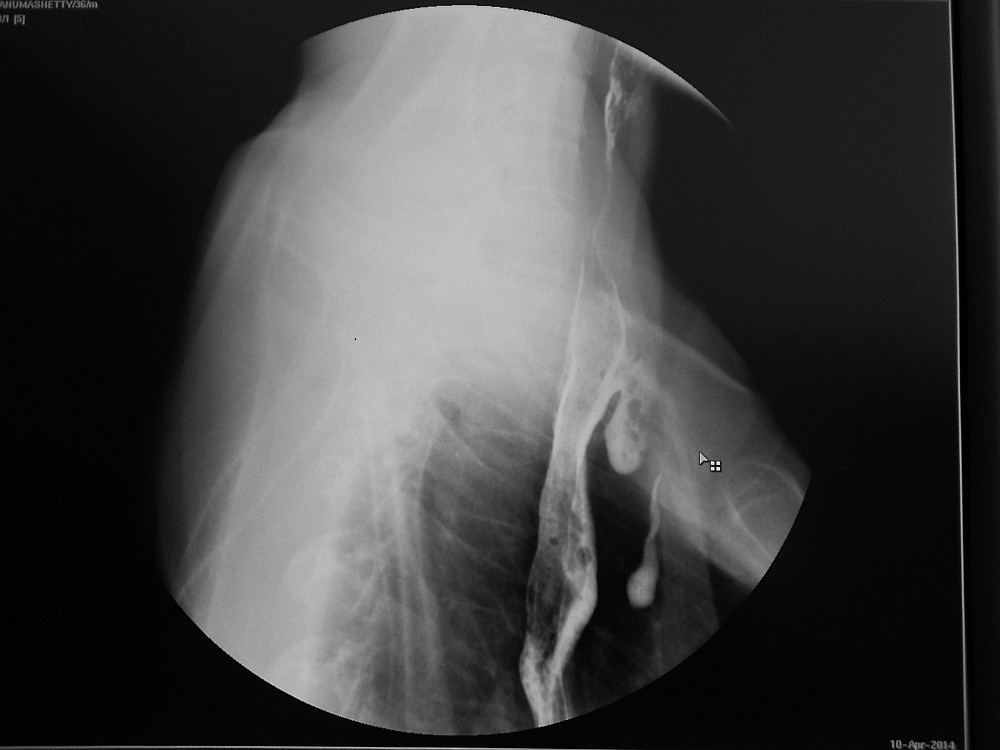
Fig 1: Barium swallow illustrating a dilated oesophagus and the TOF with resultant contamination of the trachea and bronchial tree
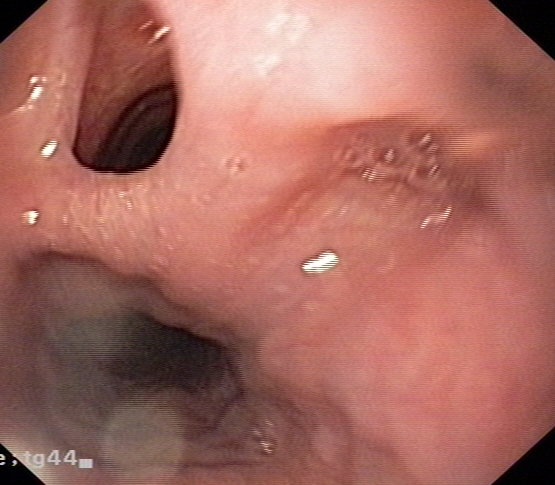
Fig 2: Oesophagoscopy showing TOF
Correct answer:
2. Tracheo-oesophageal fistula
Discussion:
A tracheo-oesophageal fistula (TOF) is a communication between the trachea and oesophagus which can be congenital or acquired. Congenital and acquired TOFs are associated with multiple complications, including poor nutrition, recurrent pneumonia, acute lung injury, acute respiratory distress syndrome, lung abscess, bronchiectasis from recurrent aspiration, respiratory failure, and death. Acquired TOFs occur secondary to malignant disease, infection, ruptured diverticula, and trauma.1, 2 Acquired TOFs are quite rare, and incidence rates have not been well documented. Post intubation TOFs uncommonly occur following prolonged mechanical ventilation with an endotracheal or tracheostomy tube. TOFs caused by endotracheal tube intubation depend on several factors, including prolonged intubation, an irritating or abrasive tube, and pressure exerted by the cuff. Pressures exceeding 30 mm Hg can significantly reduce mucosal capillary circulation and result in tracheal necrosis. Cuff pressure is particularly risky when exerted posteriorly against a rigid nasogastric tube in the oesophagus. Poor nutrition, infection, and steroid use cause tissue alteration, which predisposes patients for the development of TOFs. As a result of laryngeal bypass, spillage of oesophageal contents occurs into the trachea. Saliva, food and gastric juice contaminate the airways. This leads to congestion, infection, pneumonia, bronchial obstruction, atelectasis and respiratory distress. The severity of contamination depends on the width and length of the fistula as well as the posture of the patient. Spontaneous closure of non-malignant TOFs is exceptional.
Patients with acquired TOFs have high mortality and morbidity rates because of critical illnesses and co-morbidities. Acquired TOFs may occur in individuals of any age, and elderly individuals are at increased risk if they become ventilator dependent because of respiratory failure. Acquired TOFs can be diagnosed by instillation of contrast media into the oesophagus (Fig.1) or during direct visualization by flexible oesophagoscopy (Fig.2) or bronchoscopy. A high index of suspicion is needed to diagnose tracheo-oesophageal fistula in a post intubated patient presenting with symptom of cough following deglutition. Since acquired TOFs do not close spontaneously, surgical repair is needed if the patient is stable enough.3, 4 Critically ill patients are managed conservatively until stable enough for a major surgical procedure.
Typical oesophageal symptoms of gastro-oesophageal reflux disease include heartburn, regurgitation and dysphagia. The classic presentation of spontaneous oesophageal rupture is chest pain and subcutaneous emphysema after recent vomiting or retching (Mackler’s triad) in a middle-aged man with a history of dietary over-indulgence and over consumption of alcohol. Oesophageal diverticula presents with oropharyngeal dysphagia, usually to both solids and liquids, which is the most common symptom. Retention of food material and secretions in the diverticulum, particularly when it is large, can result in regurgitation of undigested food, halitosis, cough, and even aspiration pneumonia. The patient may note food on the pillow upon waking up in the morning.
|
Competing Interests None declared Author Details M SURESH BABU, MBBS MD FCCP FICP FICS FIMSA FIACM FISE FACP(USA), Associate Professor, Department of Internal Medicine, JSS Medical College and Hospital, JSS University, Mysore, Karnataka, India. DEEPAK SUVARNA, MBBS MD DNB(Gastroenterology), Professor, Department of Gastroenterology, JSS Medical College and Hospital, JSS University, Mysore, Karnataka, India. CHANDRASHEKHAR SHETTY, MBBS MD(Radiology), Professor and Head of Department, Department of Radiology, JSS Medical College and Hospital, JSS University, Mysore, Karnataka, India. ADITYA NADELLA, MBBS, Junior Resident, Department of Internal Medicine, JSS Medical College and Hospital, JSS University, Mysore, Karnataka, India. CORRESPONDENCE: Dr. M. Suresh Babu MBBS, MD, FCCP, FICP Associate Professor, Department of Internal Medicine, JSS Medical College and Hospital, JSS University, Mysore, Karnataka, India-570004 PH: +91-9448052680 Email :drmsureshbabu@yahoo.co.in Postal Address: #739, E and F Block, Kuvempunagar, Mysore-570023, Karnataka, India Email: drmsureshbabu@yahoo.co.in |
References
- Diddee R, IH Shaw IH Continuing Education in Anaesthesia, Critical Care & Pain | Volume 6 Number 3 2006
- Sharma S Tracheoesophageal fistula - e medicine.medscape.com/article Medscape reference 2012
- Reed MF and Mathisen DJ “Tracheoesophageal fistula,” Chest Surgery Clinics of North America, vol. 13, no. 2, pp. 271–289, 2003.
- Chauhan SS, Long JD, “Management of tracheoesophageal fistulas in adults,” Current Treatment Options in Gastroenterology, vol. 7, no. 1, pp. 31–40, 2004

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.