The first documented case of COVID-19 in the UK was reported on 29 January 2020 followed by a rapid surge of infections leading to a UK national lockdown announced on 23 March 20201.
The COVID-19 pandemic has since required NHS hospitals to constantly adapt their protocols, workforce and logistics to keep pace with the evolving spread of the virus.
The variable clinical presentation of COVID-19 may result in those requiring admission being redirected under the care of different specialties within the hospital2. Furthermore the presence of asymptomatic carriers admitted with unrelated pathologies or cases of nosocomial cross-infections implies that COVID-19 related clinical noting and discharge summary documentation is likely to affect doctors across all hospital departments.
An initial review of 50 consecutive urology discharge summaries in Royal Shrewsbury Hospital in April 2020, revealed that only 27% included the patient’s in-hospital COVID-19 swab result (positive or negative) and only 2% documented any recommended patient self-isolation advice to be adhered to after discharge into the community.
Accurate COVID-19 related documentation is paramount to ensure the patient, their family and their GP / care setting where applicable are all aware of their COVID-19 status and any recommended self-isolation, to safeguard infection prevention in the community. Furthermore, there could be potential medicolegal sequalae for the Trust were a patient recently discharged from hospital to spread COVID-19 to their family and / or vulnerable adult cohabitants due to lack of clear self-isolation guidance.
An urgent collaboration between the urology team and the Trust IT department was undertaken to upgrade the Trust’s existing eScript discharge summary software.
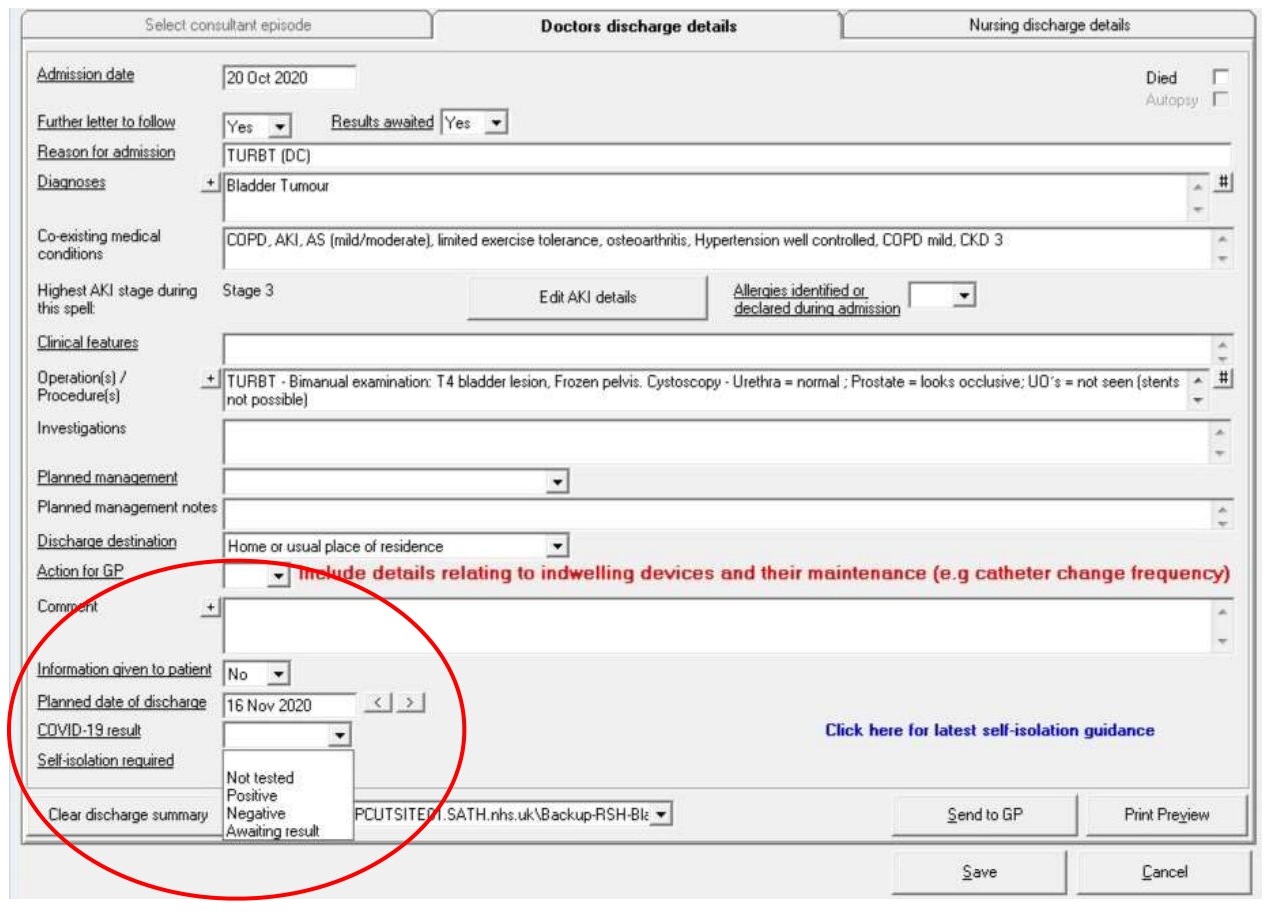
Two new tabs were integrated:
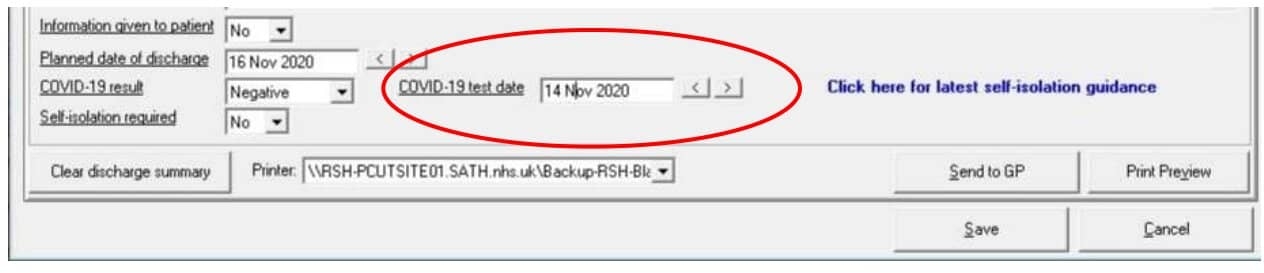
1. COVID-19 test result [Figure 1] and date [Figure 2]: Positive / Negative / Not tested
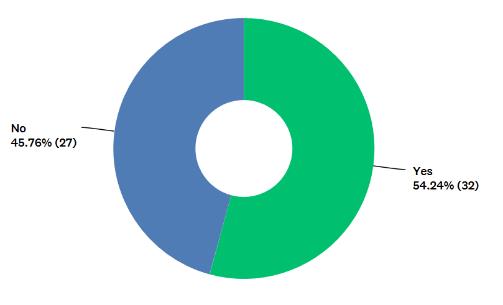
2. Self-isolation advice [Figure 3]: No / Yes (please specify as free text)
Completion was made mandatory prior to being able to sign-off the document for printing and successful upload on the electronic records.
Figure 1
Figure 2
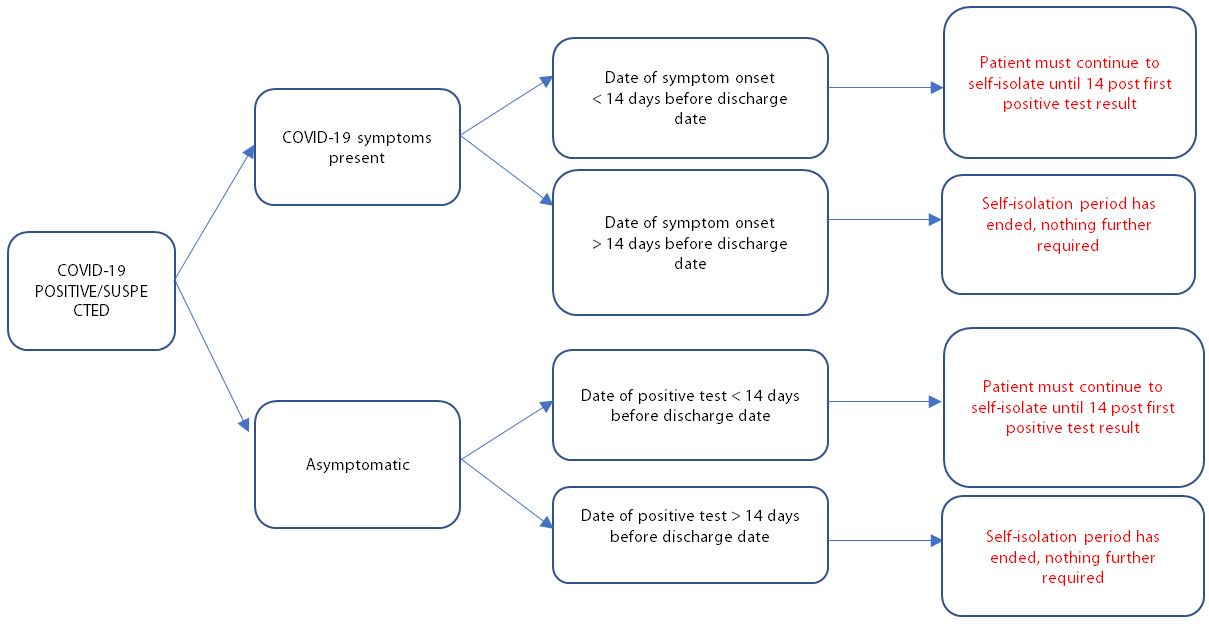
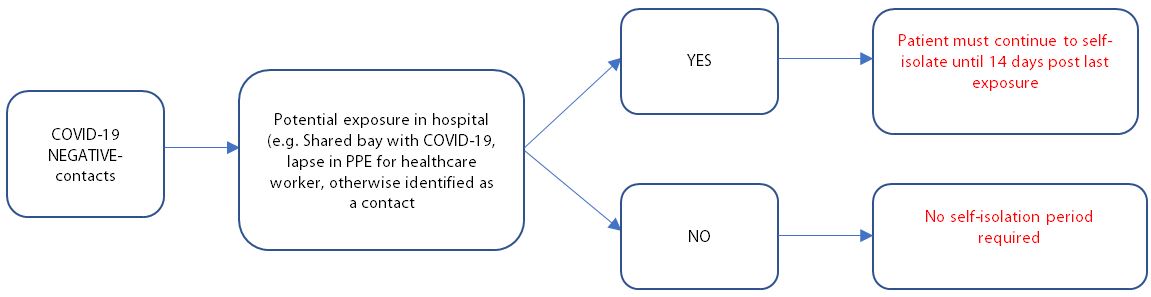
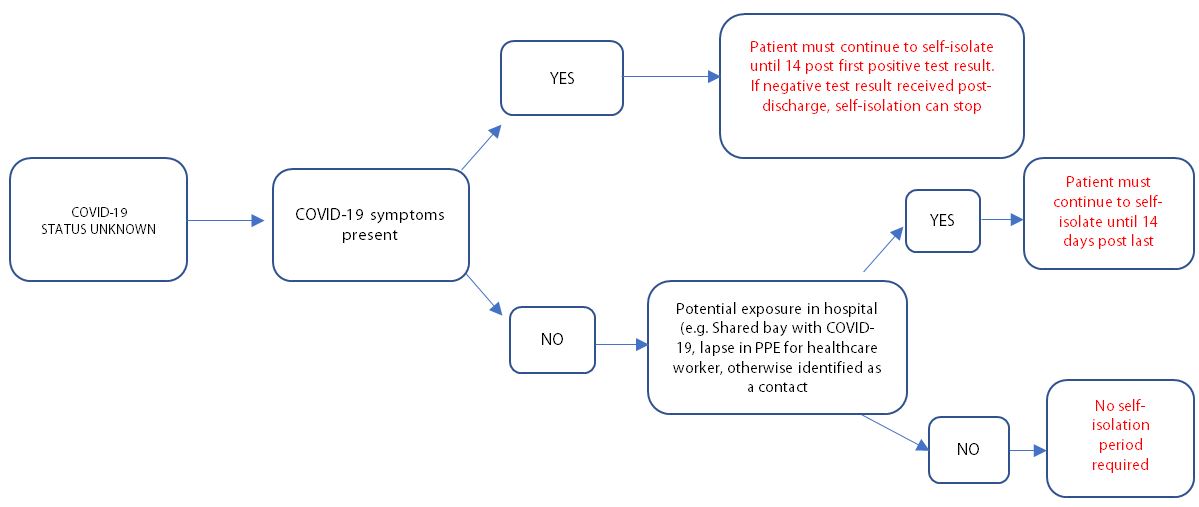
Collaboration with the infection prevention team (IPT) was undertaken to create a flow-chart style document accessible by hyperlink [Figure 3] to help discharging clinicians correctly determine and document patient self-isolation instructions following discharge from hospital, depending on individual circumstances. [Appendix 1]
Figure 3
The aim of this quality improvement project was to evaluate the impact of the dynamic upgrade made to the eScript discharge summary software in clinician compliance with COVID-19 related documentation.
Materials and Methods
The upgraded eScript discharge summary software was rolled out across the Shrewsbury and Telford NHS Trust (SATH) in the week beginning 28th September 2020.
All clinicians were informed regarding the upcoming software change by means of a Trust-wide email from the SATH Medical Director, with instructions provided on how to complete the new tabs.
The first 50 consecutive completed discharge summaries of patients admitted electively or as emergency under the urology team starting from 1st October 2020 were retrospectively reviewed by NL, EF, ZK by means of electronic records.
Note was taken of correct documentation of:
· any COVID-19 test outcome (positive or negative result)
· any recommended patient self-isolation advice after discharge from hospital
The findings were compared and contrasted with the results of the initial study in April 2020.
Results
49 / 50 (98%) patients had a COVID-19 test at any time during their admission – 1 patient did not have a COVID-19 test at any time in their admission.
3 patients were discharged prior to their COVID-19 result becoming available, 1 patient was discharged without a written discharge summary and 1 patient was incorrectly labelled as having been “not tested.”
46 patients’ results therefore became available in time before discharge and 44 (90% of all those tested) were documented on their discharge summary. All COVID-19 tests were negative. [Table 1]
All patients had either documented self-isolation advice or “none required” specified on their discharge summary following discharge from hospital. [Table 1]
The most common primary reasons for admission were urinary tract infection / sepsis (18%), catheter-related complications (14%) and urinary retention (12%).
Incidental note was made of two patient deaths within 28 days of admission.
Table 1
Initial Review
Review after software update
Number of patients
50
50
Patients tested for COVID-19
33 (66%)
49 (98%)
Patients testing positive
1 (3.3%)
0 (0%)
COVID-19 result on discharge summary
9 (27%)
44 (90%)
Self-isolation advice on discharge summary
1 (2.0%)
50 (100%)
Discussion
The results revealed that the upgraded eScript software resulted in a notable improvement in COVID-19 related documentation on discharge summaries.
In the initial study 33 / 50 (66%) had a COVID-19 test at any time during their admission – only 27% of these however had the result included on their discharge summary, compared to 90% compliance following the eScript software upgrade.
Following the finding of 3 patients’ (6%) COVID-19 result not becoming available prior to discharge, SATH IT was consulted and an extra option on the eScript COVID-19 result dropdown menu was added to include “awaiting result” to mitigate for this particular circumstance. [Figure 1]
Only 1 patient (2%) in the initial study had any self-isolation advice documented on their discharge summary – this figure soared to 100% following the eScript software upgrade. [Table 2]
The figures have to be interpreted in light of the change in COVID-19 testing availability, which only became widespread in mid-May 2020 and thus after the completion of the initial study3. This is likely to account for the lower proportion of in-patient COVID-19 tests being performed in the initial study (66%) vs. second study (98%).
Arguably a negative COVID-19 result such as those commonly encountered on the urology ward are less likely to be documented on a discharge summary compared to a positive test, particularly if admitted with unrelated pathologies (e.g. urinary retention) or asymptomatic carriers. By nonetheless documenting this pertinent negative, one ensures the patient is aware of their reassuring result and any community-based clinician such as district nurse or GP can be cognisant of this information if called to assess the patient soon after hospital discharge.
The findings of the study are directly relevant to all doctors working in acute NHS Trusts, as clear and accurate documentation is a key principle in the GMC’s “Good Medical Practice” document to which all registered practising doctors must abide to4. A discharge letter is a key component of the documentation of a patient’s journey and therefore must be completed accurately in line with GMC guidance. The updated software system safeguards the accuracy and clarity of the Trust’s discharge summaries in relation to COVID-19 results and self-isolation advice.
Self-isolation is a key principle of outbreak control for any infectious disease, and is a particularly important strategy in managing widespread vast numbers of cases such as in the COVID-19 pandemic in a libertarian society where strict quarantine is not routinely enforced5. The adherence with self-isolation has been notoriously poor in the UK – it is estimated that only 25% of symptomatic patients with proven COVID-19 complied fully with the government advice of not leaving the home during their isolation period6. It is therefore of paramount importance that patients being discharged from hospital in the COVID-19 pandemic era are given clear instructions on how to self-isolate and the recommended duration of this is documented.
Doctors preparing discharge summaries and their patients must be aware that COVID-19 may still be relevant to them even if the primary reason for admission was unrelated and their test on admission was negative – for example they may have been exposed to another in-patient or staff member later found to be positive for the virus. The discharging clinician should check for any such event and disclose this on the discharge summary where applicable.
From a medicolegal perspective, hospitals trusts may find themselves in a vulnerable position if COVID-19 positive or potentially exposed patients are discharged without any documented self-isolation advice. This in particular follows the controversy highlighted in the earlier months of the pandemic of thousands of elderly patients being discharged from hospital to care homes in the UK without a COVID-19 test7. Indeed, since then a judge has allowed legal action from a bereaved daughter to be brought against the Department for Health and Social Care, NHS England and Public Health England for failure to adequately protect vulnerable residents in an Oxfordshire care home8. Safeguarding the clear documentation of recommended patient self-isolation instructions on discharge summaries is likely to confer additional protection to a Trust facing any such legal challenge.
Writing a high-quality discharge summary is a difficult skill to teach and indeed they are often completed by the most junior members of the medical team9. The Trust’s IT software can therefore play a vital role in helping doctors ensure that COVID-19 result and self-isolation instructions are documented for all hospital discharges, by means of mandatory tabs for completion prior to sign off.
To our knowledge, although other Trusts have since similarly amended their discharge summary software in light of the COVID-19 pandemic, this is the only study in the literature which directly attests the degree of improvement in documentation as a result of such a software change. We urge that all Trusts in the UK consider amending their discharge summary software in line with the changes characterised in this study.
Conclusions
The updated eScript discharge summary software has greatly improved compliance within the Trust with COVID-19 test result and self-isolation advice documentation on discharge summaries.
This is a simple and highly effective modification whose benefits can have ramifications across the healthcare system.
By accurately documenting COVID-19 test results and any advised self-isolation for the patient after hospital discharge, one safeguards IPC in the community and protects the Trust from potential relevant medico-legal sequalae.
Appendix 1
Scenario 1: COVID-19 positive patient
Scenario 2: COVID-19 negative patient
Scenario 3: No COVID-19 test performed as rubbish and make someone else
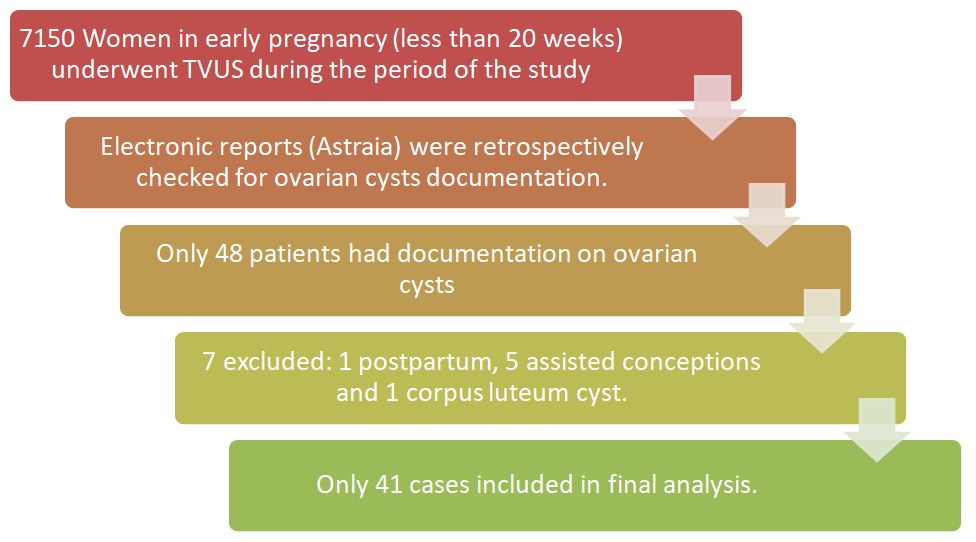
Across the UK there has been a reduction in the number of children and young people (CYP) presenting acutely to hospital during the COVID-19 pandemic. This was highlighted in a recent survey of consultant paediatricians in the UK and Ireland1. It showed that not only were fewer children being brought to emergency departments, but there were also delays in acute presentation of critical illness (such as sepsis and diabetic ketoacidosis) and reductions in referrals for cancer treatment and child protection assessments1.
The reasons for the reduced attendance are thought to be related to the initial government messaging of Stay Home, Protect the NHS, Save Lives2. However, as it became clear that not only parents, but other potential patients were not presenting even if warranted, the government adjusted the messaging to make it clear that the NHS was still open for urgent care that was not just COVID-19 related.
In CYP the cause of delayed presentations were likely to be manifold: parents following the initial governmental message; families concerned that hospitals were unsafe; the initial presumption that COVID-19 in CYP would present in the same manner as in adults potentially leading to primary care and NHS 111 pathways channelling them to domestic isolation. It may be that some delays in hospital presentations may be due to reduced referrals from primary care, and that in turn may be influenced by fewer CYP accessing their local General Practice facility. The ‘Take the Temperature’ survey which assessed the views of 1535 respondents (predominantly aged 16-25 years) found, “85% knew that they shouldn’t go to a doctor if they got the virus”3. However, it is possible that CYP and parents may not be able to make the often challenging differentiation between symptoms of COVID-19 and what may be another illness in need of medical attention.
There has been a significant increase in pressure on many aspects of the health service, including on primary care. Automated telephone messages have been used as a tool by General Practice to direct service users to the correct service or point of care for some time. As such, it is unsurprising that automated messages may be used to try to address some questions about the pandemic prior to speaking to a call handler at a practice. In addition to this, significantly limiting face to face contact with patients during the pandemic in Primary Care has been essential to prevent the potential spread of the virus and closure of services. We aimed to review the initial advice that parents and carers may be receiving from their first point of contact when telephoning their local General Practice and whether this considered CYP specifically.
Methods All General Practices within four Clinical Commissioning Groups (CCGs) in NHS Sheffield CCG, NHS Manchester CCG, NHS Leeds CCG and NHS Birmingham and Solihull CCG were identified using the NHS website. These were chosen as they are large cities, with diverse populations.
Practices were only contacted within their standard opening hours by three of the authors, within a four-day time period (7th July 2020 to 10th July 2020). The data collected is shown in table 1. All practices were telephoned and identified as to whether they had the following (see table 1):
Table 1: Questions asked during data collection
Was there an automated message?
Yes/No
Was COVID-19 was mentioned in the automated message?
Yes/No
Was there was advice to stay away from the practice if COVID-19 symptoms present?
Yes/No
Was there advice to self-isolate with COVID-19 symptoms
Yes/No
Was there any age segmentation or differing advice for children?
Yes/No
If worsening COVID-19 symptoms, was there advice to go to NHS website or telephone NHS 111 service?
Yes/No
What was the length of the automated message (In seconds)?
Percentages, means, standard deviation, and standard error of the mean were calculated. Proportions were compared using Fisher’s Exact test to calculate statistical significance of some data.
Table 2: Reasons for exclusion from analysis
Reason for exclusion from analysis
Number of practices
Private screening clinic
1
Duplication of practice already listed
5
Permanently closed
1
Call failed or no telephone number available
4
Line busy despite repeated attempts
1
Total
12
In total, 549 practices were listed under these four CCGs. 12 practices were excluded (see table 2), leaving 537 practices from which we could obtain results.
Table 3: Analysis of results from 537 GP practices
ALL GPS COMBINED
Automated message
Coronavirus mentioned in automated message
Advice to stay away from practice if coronavirus symptoms
Advice to self-isolate with coronavirus symptoms
Did have age segmentation
Advice if worsening COVID-19 symptoms to go to NHS Website or phone 111
Length of automated message (seconds)
TOTAL
440
290
153
120
5
169
23694
% of surgeries contacted
81.9%
54.0%
28.5%
22.3%
0.9%
31.5%
% of surgeries with automated message
100.0%
65.9%
34.8%
27.3%
1.1%
38.4%
Mean
54.1
Standard Deviation
26.9
Table 3 demonstrates that of the 537 practices, 81.9% (n=440) had an automated message. When an automated message was present, the mean length was 54.1 seconds (SD = 26.9). Of all of the practices with an automated message, 65.9% (n=290) mentioned ‘coronavirus’ or ‘COVID-19’ in their message, 34.8% (n=153) gave specific advice to stay away from the practice if the caller had symptoms of COVID-19, 27.3% (n=120) gave advice about self-isolating with COVID-19 symptoms, and 38.4% (n=169) re-directed callers to telephone NHS 111 or visit the NHS 111 website for advice on worsening symptoms. Only 1.1% (n=5) practices mentioned children specifically. Of these, two said that the advice about self-isolating also applied to children, and the other three said the following: “…anyone with a new continuous cough or fever of 37.8 degrees centigrade or higher must self-isolate for 7 days. This includes children. Travel history is now irrelevant. Anyone with these symptoms who are well are to stay at home and do not need to ring 111 or be tested. Anyone with these symptoms who are unwell should go to NHS 111 online for advice. You must not come to the surgery…” “…anyone with a new continuous cough and/or a high temperature should stay at home and self-isolate for the next 7 days. This includes children. All other members of your household will need to self-isolate for 14 days even if they remain asymptomatic. Do not attend the university health service, hospital, pharmacy or other NHS service in person. If you have these symptoms, use the NHS 111 online coronavirus service to find out what to do. Do not call NHS 111 unless you cannot get help online…”
“…anyone with a new continuous cough, a fever of 37.8 degrees or higher, or a loss or change to your sense of smell or taste must self-isolate for 7 days. This includes children. Anyone with these symptoms who are well must stay at home and order a COVID-19 test… Anyone with these symptoms who are unwell should go to 111 online for advice. You must not come to the surgery…”
Sheffield CCG had the fewest number of automated messages compared with all the other CCGs:
Sheffield CCG (n=75, 70.8%) vs Leeds CCG (n=119, 88.8%) p<0.0005;
Sheffield CCG (n=75, 70.8%) vs Manchester CCG (n=74, 81.3%) p=0.0974;
Sheffield CCG (n=75, 70.8%) vs Birmingham and Solihull CCG (n=172, 83.5%) p=0.012.
Sheffield CCG had the most automated messages with advice to stay away from the practice compared with the other CCGs:
Sheffield CCG (n=44, 58.7%) vs Leeds CCG (n=34, 28.6%) p<0.0001;
Sheffield CCG (n=44, 58.7%) vs Manchester CCG (n=26, 35.1%) p=0.0052;
Sheffield CCG (n=44, 58.7%) vs Birmingham and Solihull CCG (n=49, 28.5%) p<0.0001.
Manchester CCG had the fewest messages with advice to self-isolate compare with the other CCGs: Manchester CCG (n=9, 12.2%) vs Leeds CCG (n=30, 25.2%) p=0.0415;
Manchester CCG (n=9, 12.2%) vs Sheffield CCG (n=26, 34.7%) p=0.0018;
Manchester CCG (n=9, 12.2%) vs Birmingham and Solihull CCG (n=55, 32%) p=0.0009. See Table 4.
Table 4: Breakdown of results for individual CCGs
CCG
% of surgeries with automated message
% Coronavirus mentioned in automated message
% Advice to stay away from practice if coronavirus symptoms
% Advice to self-isolate with coronavirus symptoms
% Did have age segmentation
% Advice if worsening Covid-19 symptoms to go to NHS website or phone 111
Mean length of message in seconds (95%CIs)
Sheffield (n=106)
70.8 (n=75)
62.7 (n=47)
58.7 (n=44)
34.7 (n=26)
4.0 (n=3)
34.7 (n=26)
52 (46-57)
Leeds (n=134)
88.8 (n=119)
62.2 (n=74)
28.6 (n=34)
25.2 (n=30)
1.7 (n=2)
53.8 (n=64)
56 (51-60)
Manchester (n=91)
81.3 (n=74)
68.9 (n=51)
35.1(n=26)
12.2 (n=9)
0 (n=0)
56.8 (n=42)
58 (52-64)
Birmingham and Solihull (n=206)
83.5 (n=172)
68.6 (n=118)
28.5 (n=49)
32.0 (n=55)
0 (n=0)
21.5 (n=37)
52 (49-56)
Automated messages were all in English (although a small number of practices provided a translation in other languages after the message) and orated by a mixture of computerised voices, doctors or staff from the practice. Many automated messages indicated a range of options for the caller to be re-directed to a different line (such as to arrange an urgent appointment or to obtain a repeat prescription) but for the purposes of this study, the key data points listed in table 2 were the only parts of the message which were recorded.
There was no statistically significant difference in mean message length between the four CCGs. Sheffield CCG 51.7 seconds (95% confidence interval 46.5 to 56.8); Leeds CCG 55.7 seconds (95% confidence interval 51.2 to 60.1); Manchester CCG 58.0 seconds (95% confidence interval 52.2 to 63.7); Birmingham and Solihull CCG 52.4 seconds (95% confidence interval 48.7 to 56.0) (p<0.05).
Discussion
This study found that very few practices specifically mentioned children in their automated messaging in relation to the current pandemic. 81.9% of the practices contacted had automated telephone messaging. Of these, 65.9% mentioned COVID-19 in their message but only 1.1% (n=5) specifically mentioned children in their message.
38.4% of practices re-directed callers to either the NHS website or NHS 111 telephone advice line. The website advice states, "Call 111 if you're worried about a baby or child under 5. If your child seems very unwell, is getting worse or you think there's something seriously wrong, call 999”4. There is also further advice particularly focussed upon babies and very young children on the website. This is helpful advice for parents or carers of an unwell child and it is important that it is emphasised. However, it relies upon parents and carers to make an assessment as to when something may be getting worse or is ‘seriously wrong’. Whilst this would increase the workload for primary care, it perhaps would be more beneficial for CYP, particularly those under 5 years to be triaged by a call handler at the local practice and have a much lower threshold for a telephone consultation with a clinician at the surgery or advice to attend hospital.
This study provides a timely representation of first point of care health advice which is being provided in England during the current pandemic. It seeks to look specifically at automated advice given to CYP and whether this may contribute the delays in presentation to secondary care for acutely unwell CYP which have been seen.
It is difficult to know for certain how this may be directly attributable to the reported delays in presentation of serious illness.
Practices from within only four CCGs were contacted in this study. However, this covered a sizable number of different practices, 537 in total, all of which were in large cities and towns in England. It is notable that we did not assess any advice that may have been given by those answering the telephone call. Once the automated message had been completed there may have been opportunity to provide targeted advice. Also, for the 18.1% (n=97) practices where there was no automated message, we do not know if any further advice is relayed by those answering the call. It may have been at this point when age specific advice might have been received.
To our knowledge there have been no other studies looking at the spectrum of automated messages in General Practice during the COVID-19 pandemic.
This study highlights the need for tailored and consistent advice for CYP specifically during the COVID-19 pandemic.
There is significant variation in the advice being given by different General Practices. The Royal College of General Practitioners (RCGP) states that ‘as with all patients, children should be triaged prior to any face to face consultation’ and ‘every effort should be made to avoid face to face assessment’5. It is very important to note that the pandemic has been an extremely challenging time for General Practice with rapid adaptations to working being made in a very short time period. There have been repeated changes in guidance which highlight the challenges faced by General Practice in providing the most up to date information. Since 18th February 2020, patients with a travel history or suspected symptoms were advised to call NHS 111 and to not go to their local General Practice, pharmacy or hospital6. On 5th March 2020, General Practitioners (GPs) were advised by NHS England to switch to a telephone-only triage system, to reduce the change of potentially infected patients attending the practice7. The latest NHS England Standard operating procedure for General Practice (at the time of writing; 24 June 2020, Version 3.3)8 offersspecific advice for GPs regarding children; “Prolonged illness and/or severe symptoms should not be attributed to COVID-19 and should be evaluated as usual”. The rapidly changing advice, coupled with large amounts of uncertainty and anxiety among staff in Primary Care may have contributed to the challenges of providing consistent, standard information for service users such as through automated messaging. For some practices, a telephone triage service was a completely novel way of working, making this large process change over a very limited time frame must have been extremely challenging.
Logistically, the ability to alter automated telephone messaging is often not straightforward and, in many cases, requires outsourcing of this to external companies. This requires an already pressured service to keep up to date with rapidly altering advice whilst arranging for a staff member to formulate a new script and then arrange for this recording to be amended. A process which would have been required to be repeated multiple times over the preceding months, due to regularly changing government messaging.
Although evidence continues to emerge, we know that COVID-19 is less likely to develop into serious illness in healthy children and adolescents compared to adults9.
There have been concerns regarding a serious but rare complication of COVID-19 infection in children PIMS-TS (paediatric inflammatory multisystem syndrome temporarily associated with SARS-CoV-2). A recent paper in the Lancet10 reviewing children admitted to PICUs in the UK between 1st April 2020 and 10th May 2020 suggested that incidence of PIMS-TS requiring intensive care was around 1.5%. However, at the time only hospitalised patients were being tested for COVID-19 in the UK, so this does not take into account the number of children who may have had COVID-19 but were not tested. As a result, it is likely to be an overestimation. Whilst this condition can be serious, the likelihood of a child progressing to PIMS-TS after developing Covid-19 remains low. The greater concern is delayed presentation of other serious illness.
As other publications have suggested, there is a greater risk that children may delay in presenting to hospital or be delayed in being referred to secondary care for important investigations due to the widespread ‘stay away’ advice, seen in both the UK11 and in Europe12.
We suggest that adapting the messaging that parents or carers receive when they first contact their GP to include CYP would be possible and may reduce the number of unwell CYP who have delays in receiving medical care. It would also be important to aim to have consistent messaging across different practices, advice which perhaps should be standardised at a national level. This could greatly assist those working in Primary Care to be able to provide accurate and up to date messaging for their patients. Any adaptations required could be made by individual CCGs to take account of local differences.
Increased amounts of wider public health messaging directed towards encouraging parents and carers to seek medical advice if they are worried about their child, despite the pandemic, are paramount to aid in getting this vital message to those caring for CYP. It is important that additionally where appropriate, this advice is also available in languages other than English.
This study does not prove a direct link between the advice provided at the first point of contact in Primary Care and the delays in CYP presenting to hospital with serious illness. We do not know what influence the advice on automated messages has over CYP and their parents in their decision making about accessing care. Future research should seek to answer this question specifically, perhaps involving directly interviewing CYP and their parents or carers.
General Practice is the first point of contact for most patients who ask for professional medical advice in the United Kingdom (UK) National Health Service (NHS)1. Primary care makes up around 90% of all NHS activity and, as a result of increasing populations overtaking the number of newly qualified General Practitioners (GPs), the burden of tasks from patients has increased exponentially. GPs characterise their workload as “unmanageable” or “unsustainable” and 93% have reported that patient care has been subsequently affected.1 Funding into General Practice from the NHS expenditure has fallen by almost 20% which has halted the expansion of new practices and recruitment of substantial GPs. The growth of new GPs increased by 0.2% only, between 2009-2014, and this has indirectly pressured existing doctors to care for more patients. This is reducing job morale as well as patients’ satisfaction with services. The main causes of increased workload are increased administrative load, high patient expectations and increased risk of litigation.2
Four years ago, there were four doctors at our practice. As time passed, one doctor emigrated, another doctor passed away and the third had retired. This has left two doctors at the practice at this current time. The practice currently employs locum GPs to cover the pressures of daily patient appointments as, according to new studies, there are now on average an astonishing 2,100 registered patients per GP.3 The loss of permanent doctors in this practice may be due to the location of the GP surgery. Barnsley, according to uSwitch in 2015, was ranked 122 out of 138 local areas across the UK based on 26 factors such as household income, life expectancy, hours of sunshine and the cost of essential goods including food bills, fuel costs and energy bills.4 Adding to the lack of permanent GPs, recruitment into General Practice as a specialty has been scarce. Studies have shown that medical graduates chose medical careers that they considered as more stimulating and interesting. One study mentions that medical students are attracted to technical or biomedical forms of medical practice, as opposed to a holistic view of medicine such as that of General Practice.5
Non-permanent GPs in the practice are keen on taking on flexible working hours, which meant the permanent doctors are left with a majority of the work including all of the on-call tasks. These tasks include dealing with patient requests that come through to the receptionist such as booking appointments, patient referrals, prescribing medication and issuing sick notes. We aim to identify the prevalence of specific tasks and evaluate ways to reduce the tasks performed by the doctor. We intend to analyse the number of prescribed acute medication that can be placed on a repeat or variable repeat prescription.
METHODS
Data was collected from a single NHS England GP Centre. This centre utilizes the Egton Medical Information Systems (EMIS) web platform for recording consultations, tracking investigation results, prescribing medications, and communicating within the practice.6 Using EMIS, we collected all the tasks of the on-call doctor for a single month. In this month, there were no school or public holidays. These tasks are sent to the on-call doctor from the receptionist who receives them directly from patients. At this centre, all tasks from 2pm on a particular day form part of the following days’ workload. Therefore, the tasks of each day were recorded from 2pm the previous day until 2pm that day.
We separated tasks by allocating them into 1 of 5 categories: medication request; request for appointment, advice, or test results; request for a referral; request for sick note; and other which included all miscellaneous tasks.
RESULTS
Total task distribution
A total of 969 tasks were performed in the month. The proportion of tasks over 4 weeks was as follows: week 1 had 26.7% (n=259) of the total tasks; week 2 had 25.6% (n=248); week 3 had 25.1% (n=243); and week 4 had 22.5% (n=218).
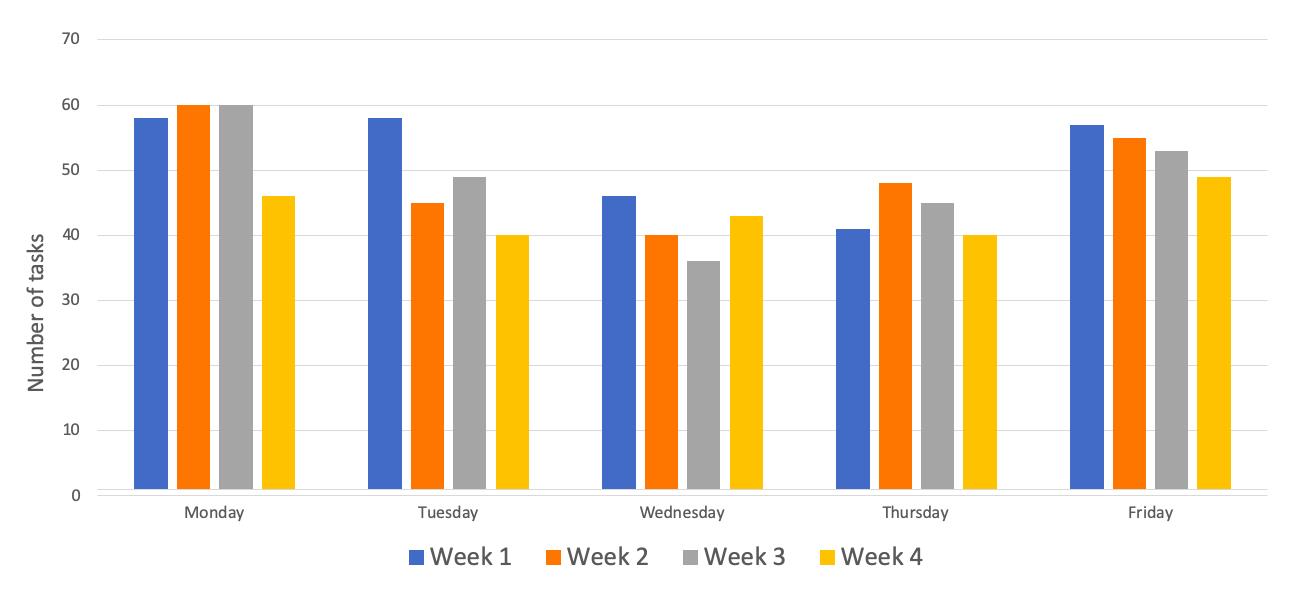
Figure 1: Total number (n) of tasks per day across each week for the four weeks of the month
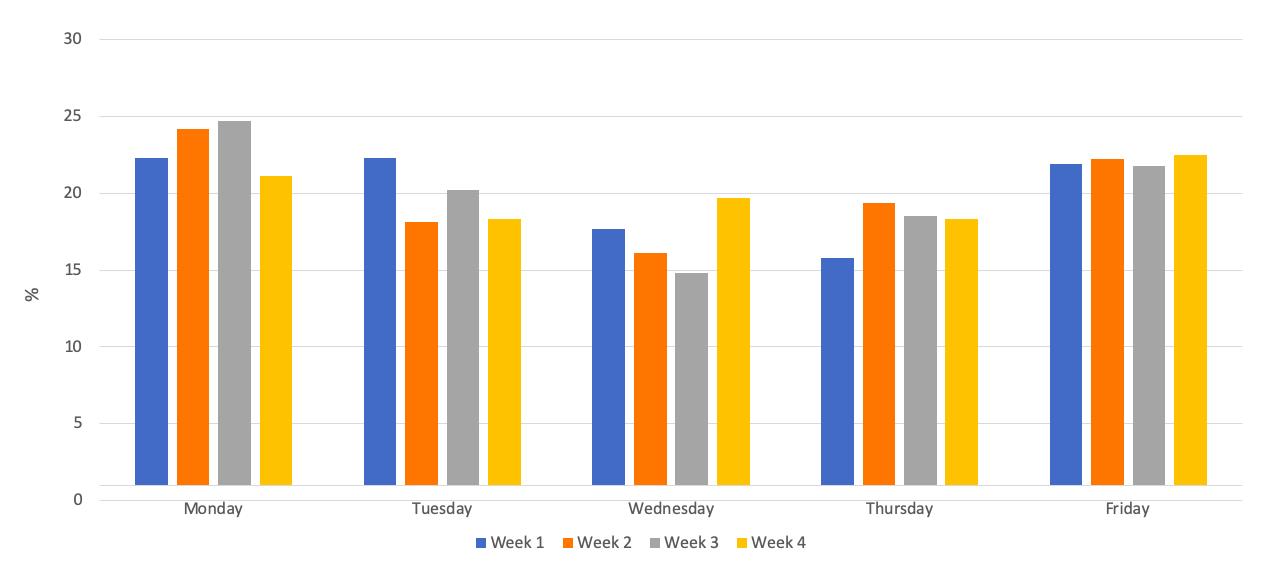
Further to this, regarding the proportion of tasks over the days of the week: Monday had 23.1% (n=224) of the total tasks; Tuesday had 19.8% (n=192); Wednesday had 17.0% (n=165); Thursday had 18.0% (n=174); and Friday had 22.1% (n=214). Figures 1 and 2 show the number and percentage of task distribution respectively across the days and weeks for the month.
Figure 2: Percentage (%) of task distribution per day-of-the-week across each week for the four weeks of the month.
Type of task
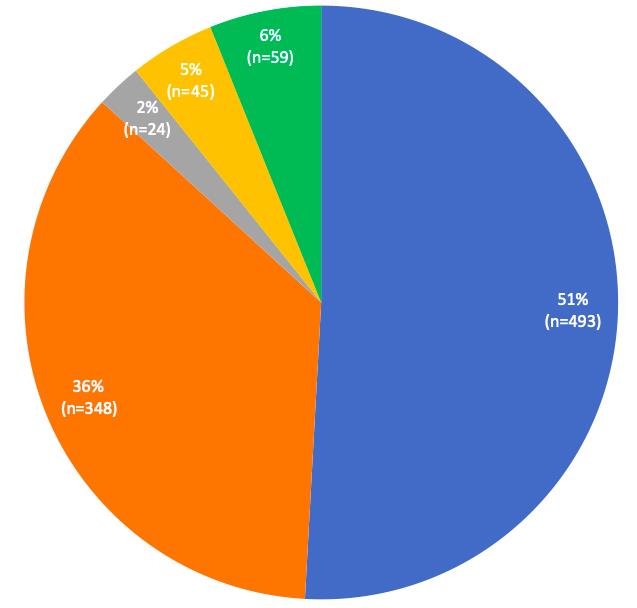
The tasks for the month were separated unevenly across the five categories: medication tasks were 50.9% (n=493) of the total tasks; requests for appointments, results and advice were 35.9% (n=348) of the total tasks; referrals were 2.4% (n=24) of the total tasks; sick note were 4.6% (n=45) of the total tasks; and other tasks made up the remaining 6.1% (n=59) of the month. Figure 3 shows the distribution of tasks for the month.
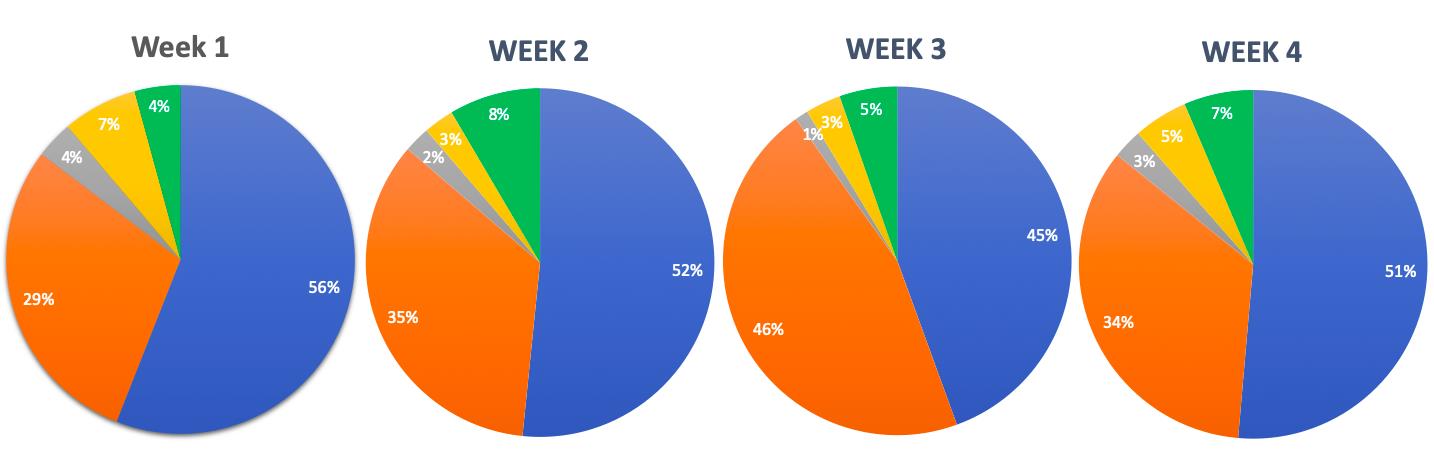
Figure 3: Distribution of tasks/requests according to task-type for the month (total tasks n=969).
We recorded the type of tasks completed per week. Figure 4 shows the distribution of tasks according to task-type for weeks 1, 2, 3, and 4, respectively. Of the total 260 tasks recorded for week 1, 55.8% (n=145) were tasks involving medication; followed by 29.2% (n=76) request for appointments, results and advice; referrals made up 4.2% (n=11); sick notes were 7.3% (n=19); and miscellaneous tasks came to 3.5% (n=9).
The second week had a total of 248 tasks. Of these, 51.6% (n=128) were medication tasks; 34.7% (n=86) were requests for appointments, results and advice; referrals made up 2.4% (n=6); sick notes made up 2.8% (n=7); and miscellaneous tasks were 8.5% (n=21).
The third week had a total of 243 tasks. Of these, 44.4% (n=108) were medication tasks; 45.7% (n=111) were requests for appointments, results and advice; referrals made up 1.2% (n=3); sick notes made up 3.3% (n=8); and miscellaneous tasks were 5.3% (n=13).
The fourth week had a total of 218 tasks. Of these, 51.4% (n=112) were medication tasks; 34.4% (n=75) were requests for appointments, results and advice; referrals made up 2.8% (n=6); sick notes made up 5.0% (n=11); and miscellaneous tasks were 6.4% (n=14).
Figure 4: Comparison of distribution of tasks/requests according to task-type for week 1, 2, 3, and 4, respectively.
Medication tasks
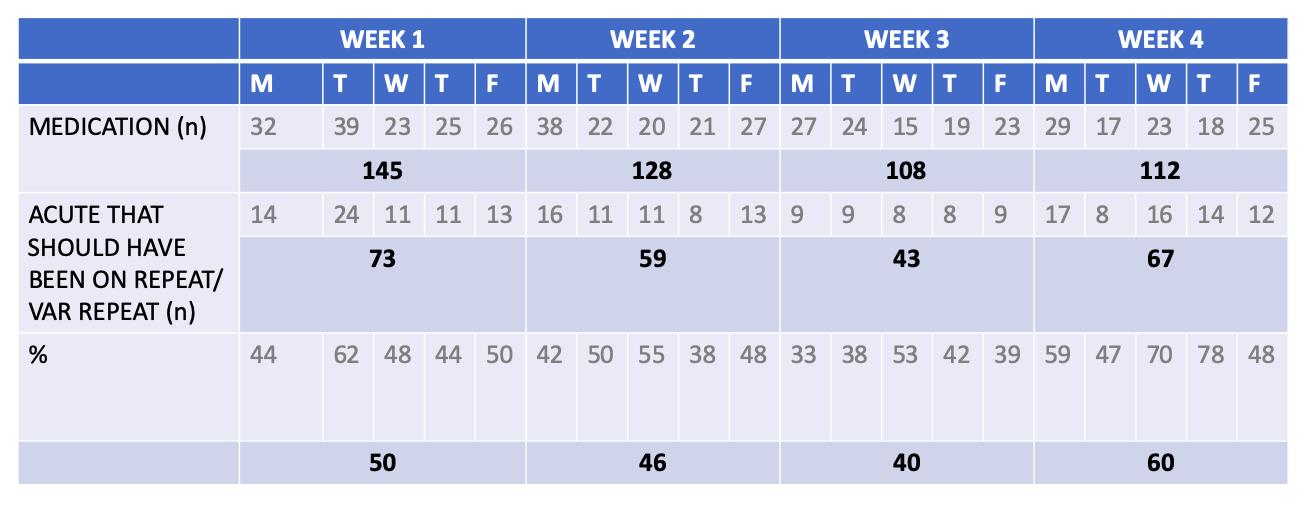
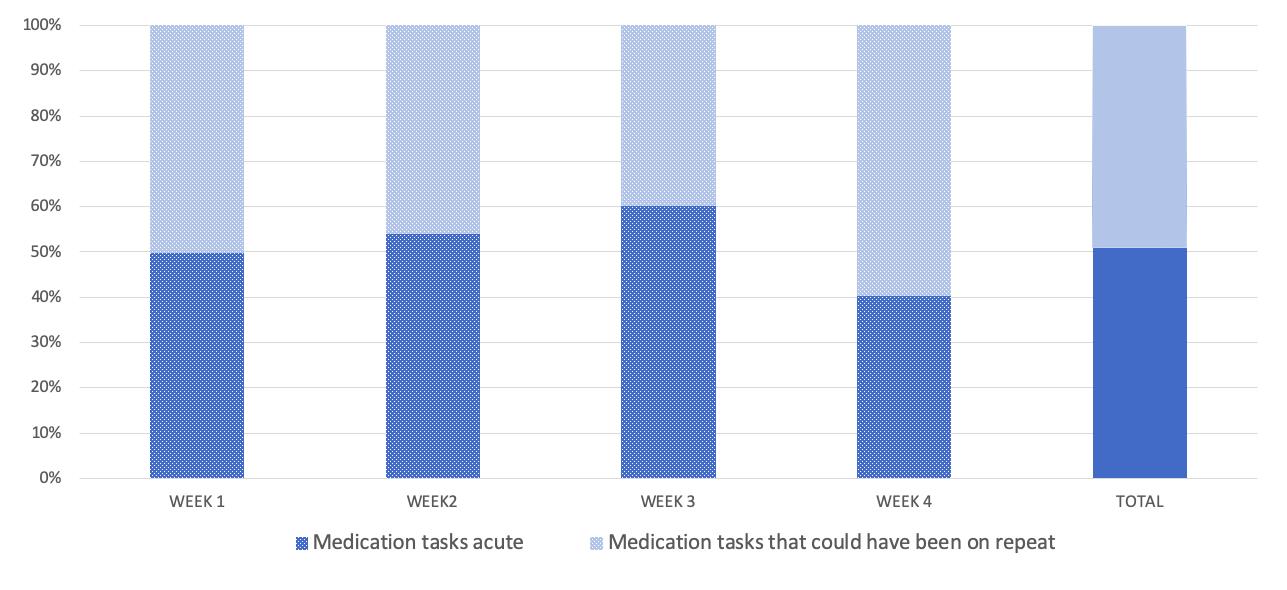
Focusing on the medication category, we had a look at whether medication requests sent to the on-call doctor were drug prescriptions that should have been on a repeat/variable repeat prescription rather than on acute. Out of a total 493 medication tasks for the month, 49.1% (n=242) medication requests could have been on repeat prescription rather than being acutely prescribed. A further analysis of this data yielded comparable findings per week. In the first week, there were 145 total medication tasks, about 50.3% (n=73) of drug prescriptions could have been on repeat. In the second week, out of 128 medications, 46.1% (n=59) of medication could have been on a repeat or variable repeat prescription. In the third week, out of 108 medications, 39.8% (n=43) of drug prescriptions could have been on a repeat or variable repeat prescription. In the fourth week, out of 112 medications, 59.8% (n=67) could have been on a variable repeat or repeat prescription. Table 1 represents the total number of medication tasks that could have been on repeat or variable repeat prescription per day. Figure 5 represents the percentage of medication tasks that were on acute prescription but could have been on repeat or variable repeat prescription across each week.
Table 1: Total medication tasks that could have been on repeat or variable repeat prescription, per day across each week for the four weeks of the month.
Figure 5: Percentage (%) of medication tasks that could have been on repeat or variable repeat prescription, across each week for the four weeks of the month.
DISCUSSION
SUMMARY
The total number of tasks did not differ significantly day-to-day: each day per week (Monday-Friday) held about 15-25% of the total weeks’ tasks. The medication requests contributed to the majority of the total tasks (50.9%); followed by requests for appointments, results and advice (35.9%). Upon further analysis of the medication category, 10-25 medication tasks per day could have been avoided by having certain drugs on repeat prescription rather than being acutely prescribed. Taking into account that a GP would typically spend 2 minutes per task, this could save 20-50 minutes per day, which amount to 100-250 minutes per week, and 400-1000 minutes or 6.5-16 hours per month.
The drug prescriptions that we thought should have been on repeat or variable repeat prescription, rather than on acute prescription, included requests for drugs that patients typically take long-term. This included Proton Pump Inhibitors (PPIs) such as Omeprazole, statins such as Simvastatin, and Angiotensin Converting Enzyme Inhibitors (ACEIs) such as Ramipril. These are for chronic conditions such as gastric reflux, hypercholesterolemia, and hypertension, respectively. Other drugs that we considered would be more feasible if put on repeat or variable repeat prescription were those for palliative patients in care homes that require a constant need for laxatives such as Senna or Lactulose, or drugs such as Paracetamol. These are for constipation or pain management, respectively.
The medication requests that could not have been on repeat or variable repeat prior to the request being sent were drugs that were required acutely, such as for short-lived infection, transient pain relief, changing of drug doses, and prescribing of alternative drugs due to a possible manufacturing problem or unavailability from the pharmacy. These are tasks that we deem necessary to be sent to the GP so that drug doses are changed based on clinical judgement, and not merely on a request sent to the receptionist. This upholds a standard of drug-control and patient safety within the practice.
STRENGTHS & LIMITATIONS
This retrospective study provides an in-depth analysis of the on-call doctors’ day-to-day tasks in terms of the nature and number of tasks. This is a study involving a large number of tasks collected from a month in a single GP surgery which has produced significant results. As non-GPs collected all the data, including data in the medication category, this eliminated bias in reporting acute medication that could have been prescribed as repeat or variable repeat medication. Limitations include the sample size being considered as a relatively small number which cannot be representative of all on-call GPs’ tasks in the rest of England. In addition, this study took place in the month of September and the tasks can be distinctly different when looking into other months.
COMPARISON WITH EXISTING LITERATURE
To date, the existing literature that looks at GP tasks from this perspective is limited. Most studies look at the receptionists’ role in handling patient requests or focus on scrutinizing the technology that GPs rely on to issue repeat or variable repeat prescriptions.
Our study included the number of tasks completed in a single month as well the stratification of tasks done within the month. We separated our results week per week to see if there were any differences between them. In 2014, a quantitative analysis of incoming calls into three GP surgeries described basic numbers of calls and type of patient enquiries that came into the practice. They had received a total of 2,780 calls and found that the most dominant type of request was making a doctor’s appointment. The main finding in the study is that it identifies an aspect of non-effective communication in GP receptionists’ encounters with patients. It describes how some receptionists failed to meet the initial requests of the patient by directing the telephone call forward or even closing calls prematurely before understanding the problem. This increased ‘patient burden’ and lead to lower patient satisfaction score when recorded. Effective receptionists understood and summarized the patients’ requests as well as making alternative actions to help the patients enquiry.7
Repeat prescriptions are defined as those that are printed by a practice computer from its repeat prescribing program8. In the UK, repeat prescriptions account for up to three quarters of all drugs prescribed, and four fifths of drug costs in General Practice.9,10 Repeat prescriptions are mostly done as a technology-supported practice that requires collaboration between clinical and administrative staff to ensure patient safety.11 Two conflicting opinions exist around repeat prescribing: the first is that the increased automation aids in improving safety; the second is that the process as a whole may be weakened if assumptions built into the technology do not take full account of the nature of healthcare work such as real life demands like time, space, and resource constraints.11,12 It is important that the GPs at our practice are aware of the risks involved in potentially putting more drugs onto repeat prescription, and consequently monitor this closely.
IMPLICATIONS FOR RESEARCH AND/OR PRACTICE
The findings collected in our study demonstrate the increasingly demanding role of the on-call GP outside of consultation hours. According to recent surveys, the GP occupation has had its lowest job satisfaction since 2001 because of a higher workload which indirectly lowers quality of patient care and increases negative patient experiences.13,14 This should be taken with paramount importance, as this can cause harm to both patients and GPs. As results have described the huge number of tasks, it is important to find a way to avoid unnecessary tasks telephoned into the GP surgery. The results of our study were presented to all of the staff in the practice and the underlying message was well received. Medications that are prescribed by the doctors are double checked by the Clinical Commissioning Group pharmacist in the practice to ensure that drugs are safely given to patients.
CONCLUSION
As the funding formula has changed in the last decade, the government budget into the NHS primary care has decreased more than in secondary care even with the ever-growing pressures on primary care services.13 Some strategies, such as telephone triage, have been introduced at the practice to reduce workload crisis. However recent evidence has shown this is not effective.15 In 2015, the primary care workforce commission laid out recommendations to restructure primary care services as the current model for primary care was under doubt. The underlying message in the report was that continuity of care was important for the majority of GPs - the GPs understood patients better when they had been under their care for many years.16 With this, extra tasks can be avoided if GPs know their patients well. At a glance of primary care, from literature and our findings, it seems that General Practice may follow an unsustainable path. The pressures of workload include increasing patient lists, higher public expectations and growing bureaucracy.17 Our data collection has proven that there are a lot of tasks to be done in a month by an on-call doctor, however the amount of time that could be saved by prescribing repeat or variable repeat rather than acute medication can save significant time. From our positive results in the medication task section, we hope this can inspire further research into other areas of the GP surgery that can help optimize the time of the doctors. Furthermore, we would like to repeat our retrospective study in one year’s time with the suggestion implemented (appropriate acute medications changed to repeat or variable repeat prescriptions) over a longer period of time. With limitations corrected for, we want to re-analyse the number and type of tasks completed to determine whether this has truly optimized the time of the overworked on-call doctor.
Aesophagogastroduodenoscopy (EGD), is a common same-day procedure used for both diagnostic and therapeutic purposes during which a small flexible fibreoptic tubular camera is introduced through the mouth and advanced through the pharynx into the oaesophagus, stomach, and duodenum. EGD procedures are performed under deep sedation, since they can elicit significant pain, discomfort, and anxiety. When pain is not controlled properly, this can lead to an increase use of adjunctive medications such as opioids. This can extend the length of stay and increase adverse outcomes.1 In a prospective, randomised, double-blinded study, Bedirli et al. found that use of opioid medications such as fentanyl are associated with increased adverse outcomes.2
Since procedural sedation-related complications (such as hypoxia, hypotension, desaturation, and emergent airway intervention) remain one of the biggest challenges in EGD procedures, it is important to select the correct medications to reduce these complications.3 Currently, propofol is the most common and popular main procedural sedation agent used for EGD procedures.4,5
Propofol is the preferred main intravenous agent in EGD procedures due to its amnestic, sedative, and hypotonic properties.6 It has also been favoured due to its ultra-rapid response and duration of effects, usually taking 30-60 seconds for onset of action and lasting up to 4-8 minutes.7 However, propofol has been associated with significant adverse effects that include dose-related hypotension, bradycardia, laryngospasms, and apnoea.8,9 Propofol does not have analgesic properties and will usually be combined with opioids for pain control.10
Ketamine is classified as a dissociative anaesthetic and is known to provide analgesia and amnesia. Important to note, it causes less respiratory or cardiovascular depression when used alone for children greater than 4 months of age.11 However, ketamine alone can cause such side effects of laryngospasm, increase secretions, and vomiting.12,13
The mixture of propofol and ketamine in one syringe (coined ketofol) has been shown to be effective in sedation for various procedures, such as spinal anaesthesia,14 along with orthopaedic15 and cardiovascular procedures16 in adults and children. Use of this combination has been favoured in brief but painful emergency room procedures due to the opposing haemodynamic and respiratory effects of both sedative medications.17 The negative cardiac effects produced by propofol can be attenuated with the use of ketamine, resulting in an increase in mean arterial pressures and cardiac indices.18,19 The complementary effect of both mediations has enabled the use of lower doses for each medication, thus lowering the toxicity and side effects.20,21 Although there are studies comparing activities of ketofol sedations,22-25 there has not been a study published on ketofol compared to propofol use in children during EGD procedures.
The primary goal of this study was to determine if there were differences in the outcomes of adverse cardiac and pulmonary events, vital sign parameters including objective pain, and administration of adjunct pain medication (for which fentanyl was used in this study) during EGD procedures between propofol and ketofol groups. A secondary goal was to determine if there was a difference in site performance metrics for EGD procedures (sedation time, stop of sedation to discharge time, and length of stay) between propofol and ketofol groups.
Methods:
This study protocol was approved by the Naval Medical Center Portsmouth Institutional Review Board in compliance with all applicable federal regulations governing the protection of human subjects. Research data was derived from an approved IRB protocol: number NMCP.2018.0021. Written informed consent was not required by the Naval Medical Center Portsmouth IRB, as this data concerned historical dae-identified patients.
Study Design
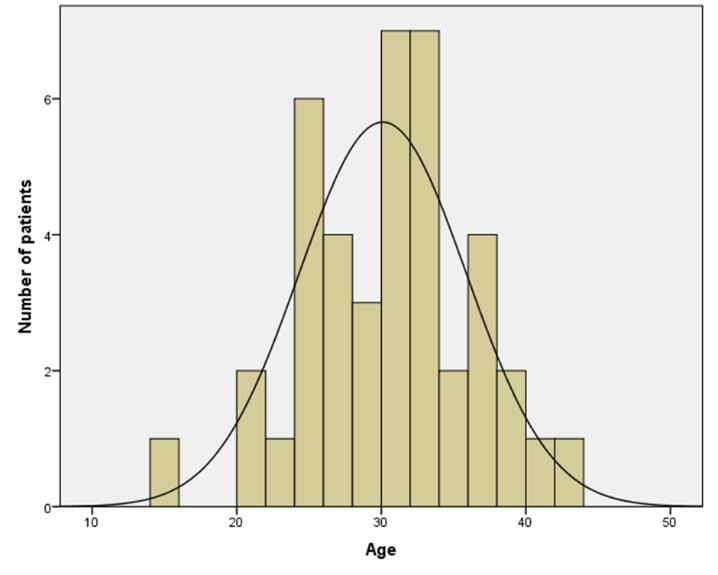
This was a single centre, retrospective study of a cohort of children (ranging from 2 to 18 years). Data was collected from March 2011 to September 2013 at Naval Medical Center Portsmouth’s Paediatric Sedation Centre. EGD and sedation protocol was not changed during this time period. EGD procedures were performed by the same paediatric gastroenterologists throughout this time period. Sedation was performed by the same paediatric intensivists throughout this time period. All patients used in this study were involved in a same day EGD procedure. Forty-one patients underwent deep sedation via propofol as main sedation agent from March 2011 to May 2012. Forty-nine patients underwent deep sedation via propofol and ketamine combination as main sedation agent from May 2012 to September 2013. Each main sedation agent was given in a similar fashion as an initial intravenous loading dose based on 1 mg/kg propofol followed by an intravenous infusion of 200-250 mcg/kg/minute that was started less than 10 minutes prior to start of the procedure and stopped at the end of the procedure. Ketofol solution used was a 1:5 ratio of ketamine to propofol (40 mg:200 mg). One mcg/kg of fentanyl was given when the sedationist during the EGD perceived the patient experiencing pain. Exclusion criteria included: patients less than 2 years and greater than 18 years, those less than 10 kg, and patients receiving adjunct medications other than fentanyl, ondansetron, or lidocaine.
Data Collection
Fourteen patients were excluded due to weight less than or equal to 10 kg. In addition, 12 patients were excluded due to age less than 2 years or greater than 18 years. Past medical history, ASA class, procedure indications, age, weight, sex, pain scores, vital signs (mean arterial blood pressure [MAP], heart rate [HR], and respiratory rate [RR]), unplanned events (hypoxia defined as SPO2 less than 85% at any time point, and hypotension defined as mean arterial blood pressure with greater than 20% decrease from baseline blood pressure), emergent airway intervention (defined as apnoea needing bag mask ventilation or CPAP use), and unplanned intubation. Vitals and pain scores were obtained from initial presentation in the sedation suite, start of procedure, every 5 minutes during the procedure to stop of sedation, and at time of discharge. Midway procedure vitals used for statistical analysis were obtained by selecting vitals that were at the half-way point of the patient’s EGD procedure. The Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) was performed every 5 minutes during the EGD procedure by an independent United States Navy Corpsman and used to evaluate patient’s pain prior, during, at stop of sedation, and after procedure for this study.26
Statistics
All statistics performed in this study were calculated using SPSS Statistics programme (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). Mann-Whitney U nonparametric test between independent groups was performed to compare age, weight, total EGD procedure time, total time of sedation during EGD procedure, time from stop of sedation to discharge, total length of stay, and total fentanyl use (in mcg/kg) between the two main groups in this study (propofol and ketofol group). The significance level was set to 0.008 after a Bonferroni was corrected, in order to address the probability of making one or more false discoveries when performing multiple hypotheses tests. A repeated measures ANOVA was run to determine the effect of treatments over time for HR, MAP, and RR. Mauchly's test of sphericity was performed for both age groups. The Fisher Exact test was performed to compare propofol to ketofol in unplanned hypotensive events and unplanned apnoea requiring bag valve mask or CPAP. Pearson Correlation statistics were performed to study possible correlations between propofol or fentanyl and sedation time or length of stay. Statistical significance for Pearson Correlation statistics was considered when two-tailed p<0.001.
Results:
Table 1. Demographic divided into 2 age groups. EE= eosinophilic esophagitis. * indicates statistically significant difference.
Sedation Risk Age Groups
2-11 years old
12-18 years old
Propofol
n=26
%
Ketofol
n=27
%
Propofol
n=15
%
Ketofol
n=22
%
General
Demographics
Male
11
42.3%
16
59.3%
6
40%
10
45.5%
Female
15
57.7%
11
40.7%
9
60%
12
54.5%
Mean Age (years old)
6
7
15
16
Mean Weight (kg)
21.6
23.7
57.7
57.4
ASA I, II
26
100%
25
92.6%
15
100%
22
100%
ASA III
0
0%
2
7.4%
0
0
EGD Indications
EE
4
15.4%
4
14.8%
2
13.3%
0
0%
GERD
11
42.3%
9
33.3%
2
13.3%
5
22.7%
Dysphagia or Feeding Intolerance
0
0%
3
11.1%
4
26.6%
4
18.1%
Foreign Body Ingestion
1
3.8%
2
7.4%
0
0%
0
0%
Failure to Thrive
3
11.5%
1
3.7%
0
0%
0
0%
Abdominal Pain
7
26.9%
9
33.3%
6
40%
11
50%
Recurrent Emesis
3
11.5%
1
3.7%
1
6.6%
1
4.5%
Gastritis
0
0%
0
0%
1
6.6%
3
13.6%
Other
2
7.7%
0
0%
2
13.3%
4
18.1%
Unplanned Events
Hypotension (blood pressure >20% decrease from baseline)
4
15.4%
1
3.7%
2
13.3%
0
0%
Apnea requiring bag valve mask or CPAP
14
53.8%*
1
3.7%*
5
33.3%*
0
0%*
Intubations
0
0%
0
0%
1
6.6%
0
0%
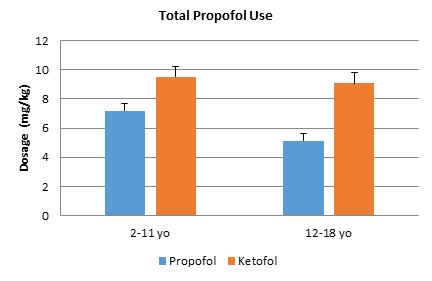
Figure 1. Propofol amount total per weight (mg/kg). Bars represent standard error of the mean. There was no significant difference between the propofol and ketofol in all age groups.
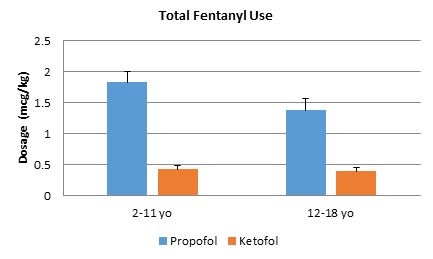
Figure 2. Fentanyl amount total per weight (mcg/kg). Bars represent standard error of the mean. In all age groups, there was a significant difference between propofol and ketofol. *p<.008.
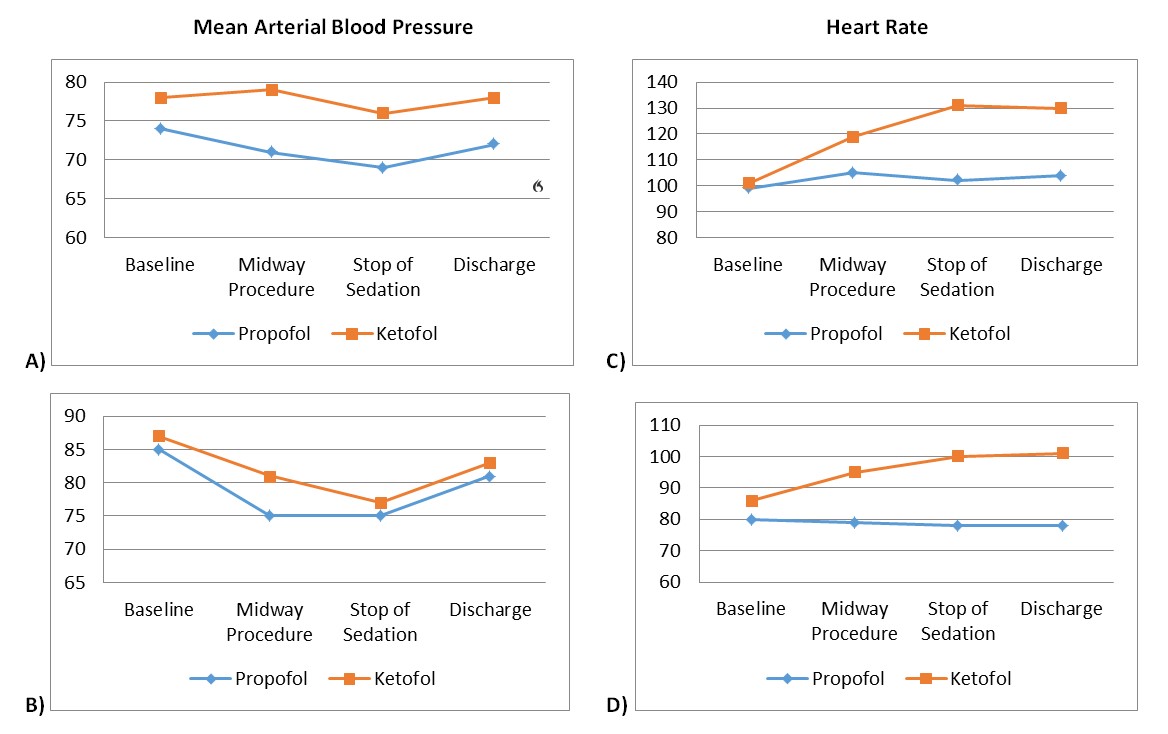
Figure 3. Vital signs. Mean arterial pressures for ages A) 2-11 years and B) 12-18 years. Main sedative agents’ MAPs were statistically different for ages 2-11 years (p =0.004), but not for ages 12-18 years (p =0.224) for all time periods. Heart rate for ages C) 2-11 years and D) 12-18 years. For Heart Rate, there was a statistically significant interaction between treatment and time for both age group using the Greenhouse-Geisser correction, p =0.002, p =0.014. Main sedative agents’ HRs showed to be statistically different for both age groups, p <0.001 and p =0.004.
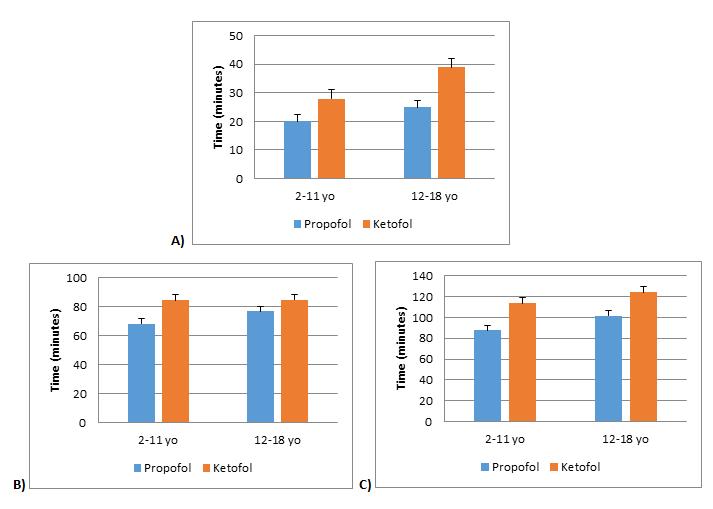
Figure 4. Duration of time. A) total sedation time, B) stop of sedation to discharge, and C) total length of stay. In all age groups, there was no significant difference between propofol and ketofol. Bars represent standard error of the mean. *p<0.008.
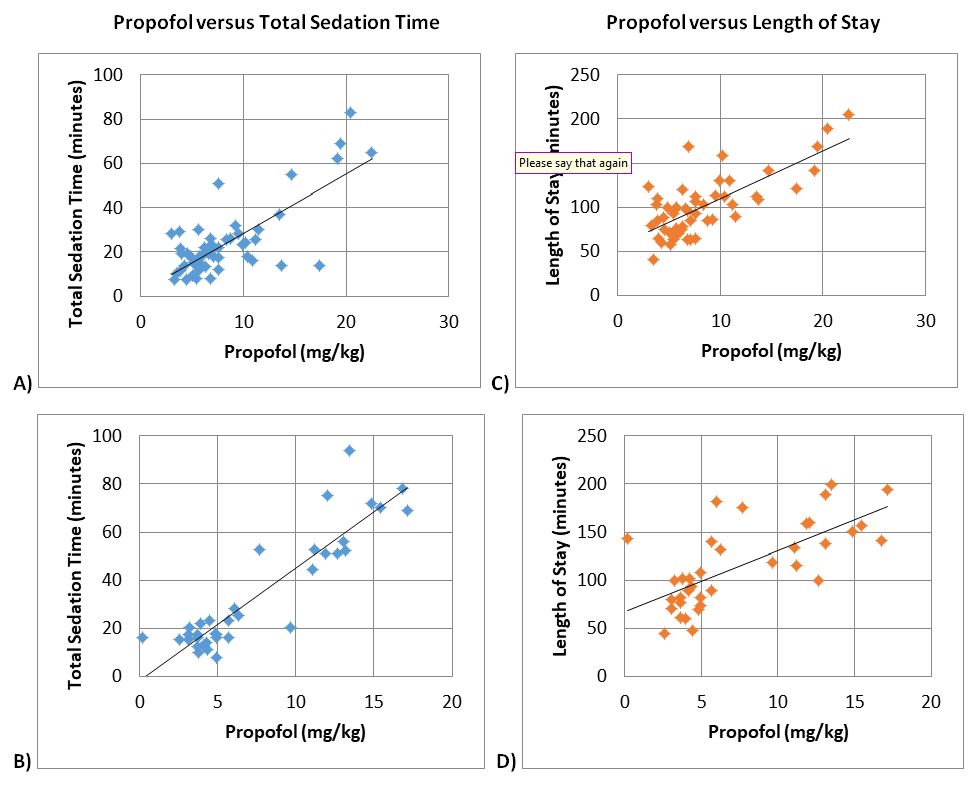
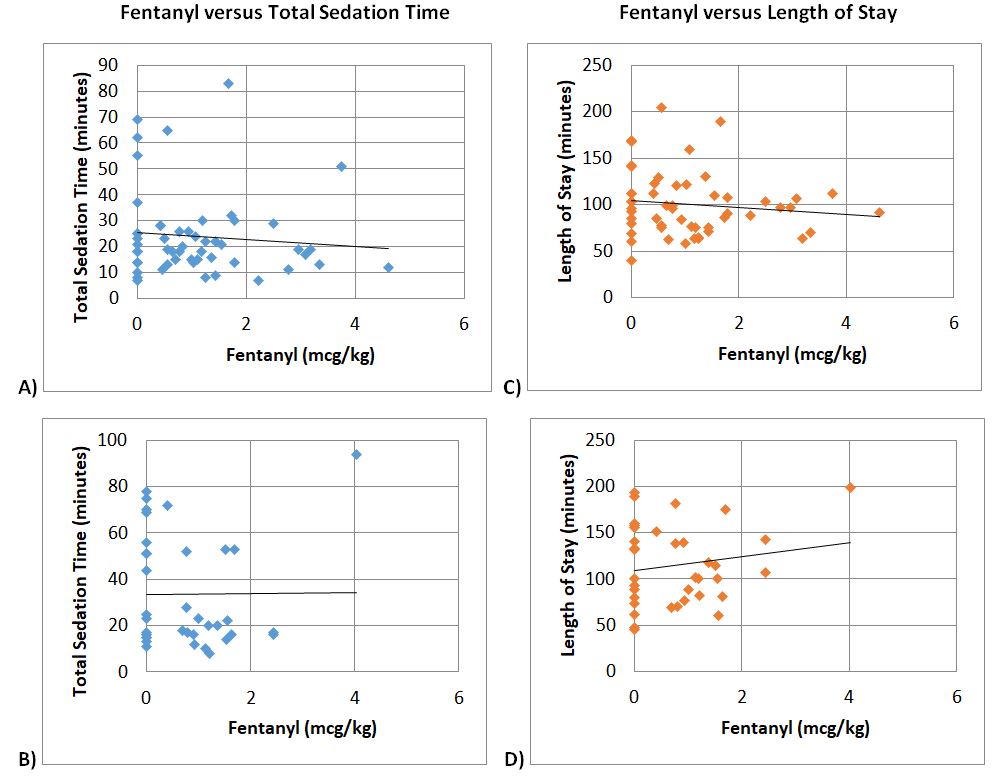
Figure 5. Pearson Correlation. Propofol versus total sedation time for ages A) 2-11 years (p<0.01*), and B) 12-18 years (p<0.01*). Propofol versus length of stay for ages C) 2-11 years (p<0.01*), and D) 12-18 years (p<0.01*). * Correlation is significant at the 0.01 level (2-tailed).
Figure 6. Pearson Correlation. Fentanyl versus total sedation time for ages A) 2-11 years (p=0.506), and B) 12-18 years (p=0.961). Fentanyl versus length of stay for ages C) 2-11 years (p=0.378), and D) 12-18 years (p=0.352). No significant correlation was not seen for all age groups.
Ninety patients were retrospectively analysed in this study. Baseline demographics were similar between the groups, except for gender proportions (Table 1). Similar amounts of propofol per weight were used in each group (Figure 1). Ketofol significantly reduced fentanyl use in all age groups by ≥.99 mcg/kg compared to propofol alone (p<0.008 for all age groups, Figure 2). In the 2-11 year old age group, the propofol group required a mean fentanyl dose of 1.96 mcg/kg ± 1.24 mcg/kg and the ketofol group required a mean fentanyl dose of 0.44 mcg/kg ± 0.49 mcg/kg; thus ketofol required about 1.52 mcg/kg less fentanyl during EGD procedures. In the 12-18 year old group, the propofol group required a mean fentanyl dose of 1.38 mcg/kg ± 1.05 mcg/kg and the ketofol group required a mean fentanyl dose of 0.39 mcg/kg ± 0.59 mcg/kg; thus ketofol required about 1 mcg/kg less fentanyl during EGD procedures.
Vital signs (HR, RR, and MAP) and CHEOPS pain scores were obtained and analysed for baseline vitals, at the procedure midpoint, at stop of sedation, and at time of discharge. CHEOPS pain scores’ mean was 6 throughout all time periods for both groups, thus there was no statistically significant difference.
A repeated measures ANOVA was run to determine the effect of treatments over time for RR. There was sphericity for the interaction term, as assessed by Mauchly's test of sphericity in both age groups (p =0.070, p =0.762). For RR, there was not a statistically significant interaction between treatment and time for both age groups, p =0.163, p =0.804. The treatments were not found to be statistically different for either age group, p =0.736 and p =0.224.
A repeated measures ANOVA was run to determine the effect of treatments over time for HR. As assessed by Mauchly's test of sphericity, no sphericity was found in either age group (p <0.05). For HR, using the Greenhouse-Geisser correction, a statistically significant interaction was found between treatment and time for both age group, p =0.002, p =0.014. The treatments were found to be statistically different for both age groups, p <0.001 and p =0.004. A repeated measures ANOVA was run to determine the effect of treatments over time for MAP. Sphericity was found in both age groups for the interaction term, as assessed by Mauchly's test of sphericity (p =0.209, p =0.269). For MAP, there was not a statistically significant interaction between treatment and time for either age group, p =0.261, p =0.591. The treatments were statistically different for the 2-11 year old group (p=0.004), but not statistically different for the 12-18 year old group (p=0.224). (Figure 3 A-D)
Unplanned events were analysed for clinically significant hypoxia, hypotension, emergent airway intervention, and unplanned intubations. Ketofol compared to propofol had fewer hypotensive events in the 2-11 year old age group (3.7% versus 15.4%, p=0.192) and in the 12-18 year old age group (0% versus 13.3%, p=0.144). Ketofol compared to propofol had statistically significant fewer apnoea events requiring bag valve mask or CPAP intervention for the 2-11 year old group (3.7% versus 53.8%, p<0.001) and for the 12-18 year old group (0% versus 33.3%, p=0.005). There were no significant hypoxia events. There was one unplanned intubation in the propofol group of a healthy ASA I twelve year old female who had a 20 mL emesis episode after a loading dose of propofol was given on induction. (Table 1)
With propofol leading to significantly more fentanyl usage, more hypotension and emergent airway intervention during EGD procedures, we performed analysis to see if there was an effect on sedation time, time from stop of sedation to discharge, and length of stay (LOS). In all age groups, there was no statistical difference between propofol and ketofol for sedation time (p=0.115 for ages 2-11 years, p=0.124 for ages 12-18 years), time from stop of sedation to discharge (p=0.033 for ages 2-11 years, p=0.511 for ages 12-18 years), and LOS (p=0.026 for ages 2-11 years, p=0.109 for ages 12-18 years) (Figure 4). Based on Pearson correlation test, it was established that propofol was positively correlated with sedation time and LOS (+0.753 for sedation time and +0.611 correlation for length of stay with <0.001 significance) (Figure 5). There was no significant correlation between fentanyl and sedation time or LOS (Figure 6).
Discussion:
This was a retrospective study looking at 90 paediatric patients, ages 2-18 years, undergoing EGD procedures with either propofol or ketofol as the main sedative medication. Patients in this study had similar weights, ages, ASA scores, and EGD indications; however there baseline demographics were not similar with regards to gender proportion (Table 1). Based on the large prospective database on sedation use for procedures outside the operating room obtained by the Paediatric Sedation Research Consortium,27 we separated our patient population into two age risk groups to allow our results to be generalisable. To our knowledge, this study is the first to show that ketofol, when compared to propofol, significantly reduces fentanyl use (≥.99 mcg/kg, Figure 2) and cardiopulmonary adverse outcomes (Table 1) in paediatric EGD procedures.
EGD procedures are known to be invasive and painful. To decrease the pain appreciated by a patient, various adjuncts are often utilised. In our study, we used fentanyl for adjunct pain control. In both main sedation medication groups (propofol and ketofol), there was no statistical significance seen in objective pain based on CHEOPS scores with a mean score of 6 in all age groups (p>0.05). However, the amount of adjunct needed to maintain adequate pain control between both groups statistically and clinically differed (Figure 2). In all age groups, the propofol group compared to the ketofol group required almost 1 mcg/kg more of fentanyl, which leads to the potential for the patient to experience higher incidence of side effects, such as respiratory depression and hypoxia.28-30
The mechanism that lead to this significant difference in opioid demand between ketofol and propofol is most likely due to ketamine’s ability to stimulate opioid sigma receptors,31 thus leading to opioid sparing effects. It is unclear if propofol and ketamine interaction heightens this opioid sparing effect, because ketamine alone has not been shown to lead to opioid sparing effects in children.32
In a review of our population’s vital signs, there was a significantly higher MAP in the ketofol group compared to the propofol group for ages 2 to 18 years (Figure 3 A-B). In addition, the ketofol group had statistically higher HR compared to the propofol group for ages 2 to 18 years (Figure 3 C-D). It is our thought that this increase in MAP and HR in the ketofol group mediated by ketamine is a protective factor against major hypotensive changes (31). It is this effect that minimised unplanned hypotensive events in our ketofol group compared to the propofol group by 11.7% in ages 2-11 years and 13.3% in ages 12-18 years (Table 1).
One of the more noticeable differences in our main sedative medication groups was the unplanned apnoea events requiring CPAP or bag mask ventilation intervention. In our 2 to 11 year age group, propofol had 50.1% more apnoea events needing intervention compared to ketofol. In our 12 to 18 year old group, propofol had 33.3% more apnoea events needing respiratory intervention compared to ketofol. This was found to be statistically significant. It is unclear if this is also clinically significant since no emergent airway intubation was needed for these events. However, there was 1 emergent airway intubation in the 12-18 year old propofol group. Based on the review of the medical records, it appears that these apnoea events needing respiratory intervention were mostly associated after the initial loading dose of either propofol or ketofol prior to or at the start of the infusion. Thus, bring into question if not starting with a loading dose bolus would decrease adverse effects.
Despite the propofol group requiring more respiratory intervention, increased fentanyl use, and less haemodynamic stability seen, there was no statistical differences in total sedation time and LOS between the two main sedation medication groups (Figure 4). Yet when we ran correlation statistics, there was a positive correlation to increased propofol dosages, total sedation time, and LOS in ages 2 to 18 years (Figure 5); therefore, if our procedures were longer, there could be a statistically and possibly clinically significant increase in total sedation time and LOS for the propofol only group. Thus, we can infer that propofol compared to ketofol is not the main sedation medication of choice for longer similarly painful procedures in children ages 2 to 18 years, such as EGD procedure followed by a colonoscopy.
A limitation of our study is that it is retrospective. With that, we were not able to blind our sedationists to the main sedation medication that was chosen and could not control the interventions that were performed. Yet, based on strict exclusion criteria, we were able to control the interventions used in our analysis. Also, in our study we did not analyse patients under the age of 2 years. Reviewing the data, we had seven patients, and thus this patient population size was not powered to perform the proper statistical analysis. Another limitation to consider is the time difference in procedure protocols. However, since this study included over 2 years of data, procedure protocols were the same. Additionally, the EGD indications were similar between ketofol and propofol (Table 1). Another consideration of this study is generalisability. This study was conducted at a single centre, but the way we analysed our results makes it easier to perform large scale prospective studies to further investigate our findings. Last limitation is directly correlating fentanyl dose with a significant adverse event. Due to the short length of the EGD procedure, constant sedation medication infusion, and fentanyl dose, it is difficult to directly say that a particular fentanyl dose alone leads to an adverse event. Therefore we can only speculate based on correlation.
Conclusions:
Our study found that ketofol significantly reduced fentanyl use in all age groups by ≥0.99 mcg/kg and cardiopulmonary adverse events compared to propofol alone. In addition, an increase in the amount of propofol was positively correlated to increasing LOS and total sedation time for a child undergoing an EGD procedure. This suggests that increasing amounts of propofol leads to greater LOS. To conclude, our study indicates that ketofol can be a safer alternative to propofol use alone for deep sedation in EGD procedures for children ages 2 to 18 years.
There have been continuing initiatives to transform and improve the National Health Service (NHS) in recent years. Mental health services in England have similarly shown evolution with regards to service provision. There has been a shift away from the perceived “medicalisation” of treatment, with traditional long-stay institutions replaced with more targeted and personalised care in the community.1 Furthermore, community services themselves have seen much remodelling over the years including decommissioning and integration, as well as increased involvement in outreach and early intervention teams.2
Mental health services are sometimes perceived as relatively well funded from outside but, as with most healthcare sectors, compared to the population requiring this service, these resources are inadequate to support the growing demand. This has been the case for some time, but it has become more evident with a significant reduction in funding observed since 2010/11.1 In addition, constant governmental pressures to meet key performance targets, as well as unachievable expectations from the public, have further stretched an already resource-depleted mental health service.
The implementation of new National policies3 was supposed to be a shift from large psychiatric hospitals to smaller specialist community centres with a promised reduction in the demand placed on inpatient services. In England, a peak number of 150,000 inpatient psychiatric beds was reported in 1955; this has since rapidly declined to 22,300 in 2012. Between 2010/11 and 2013/14, a further rapid reduction of 7% of all beds available was seen.4
Despite the promise of changes in service delivery within mental health to mitigate the continued reduction in the number of inpatient beds, demand for inpatient beds has not in fact reduced nationally.1 The recommended level of occupancy, for example, is 85% but 119 wards surveyed5 were operating at 91%, with some at 138% level of occupancy. The occupancy levels of over 100% usually occurred when long-stay inpatients were discharged home on short-term leave and their beds got filled during their absence.4 Where numbers of inpatient beds fail to meet the demands, or waiting list for their first assessment or review grows, the inadequacy lends these facilities to issues with regard to providing high quality and safe patient care. Examples of this may include inappropriate use of the Mental Health Act for detention of patients as a means of securing an inpatient bed,5 incomplete assessments of people detained in places of safety due to time or space constraints,6 and an increase in violent incidents on overcrowded inpatient wards.7
What is a Crisis Resolution and Home Treatment Team (CRHTT)?
In the late 1980s and 1990s, community mental health teams provided acute crisis support. This posed a number of issues including that these teams usually operated during normal working hours of 9am-5pm (Monday to Friday) and were not always available to provide support to patients in a crisis, and did not have the desired impact of reducing the number of acute admissions.8 This gap in service provision inspired the experimentation with and subsequent development of intensive home treatment services, some of which showed evidence of reduced hospital admissions, and holistic-working often preferred by families who were happy to have their loved ones receive the required support in the home environment.9 Over the last two decades, with remodelling of services, increased investment, NHS funding rising from £49 billion in 2000 to £122 billion in 2016, and a migration of mental health professionals, CRHTTs were established and are now available in every mental health trust across the United Kingdom (UK).10
CRHTT is a team of mental health professionals including psychiatrists, community psychiatric nurses, social workers and support workers, who provide rapid and intensive support at home during a mental health crisis.11 They are a 24-hour service operating seven days a week, and acting as the “gatekeeper” for acute services accepting referrals from various sources including inpatient, community, liaison and from outside the Trust for providing support to patients experiencing crises. These teams risk-assess patients and determine whether they require inpatient or home treatment. In the latter case, CRHTTs provide intensive home treatment by offering up to 2-3 visits a day as well as 24/7 phone support. These teams are also involved in facilitating early discharges from hospitals; in cases where patients are past the initial acute crisis, but may need further input prior to discharge to community mental health teams for longer term support.8
Definition of diagnosis and second opinion.
A second opinion is defined as “advice from a second expert (such as a doctor/psychiatrist) to make sure advice from the first such expert is correct” whilst diagnosis is defined as “the art or act of identifying a disease from its signs and symptoms”.12 Due to increased pressure on inpatient facilities and remodelling of community services, there has been a huge increase in the number of referrals made to CRHTTs. Between 2011/12 and 2013/14, it has been noted that referrals to CRHTTs increased by 16%.13 Reduction in inpatient beds and high workloads within community services often result in the formulation of arbitrary diagnoses and treatment plans. With increased pressures on other mental health services, the role of CRHTTs has begun to evolve. In addition to the previously discussed functions, CRHTTs appear to be becoming second opinion services by default enabled by the psychiatrists working in these teams.
We organised a project to establish whether a typical CRHTT is fulfilling the criteria of being a diagnostic or second opinion service provider.
Method
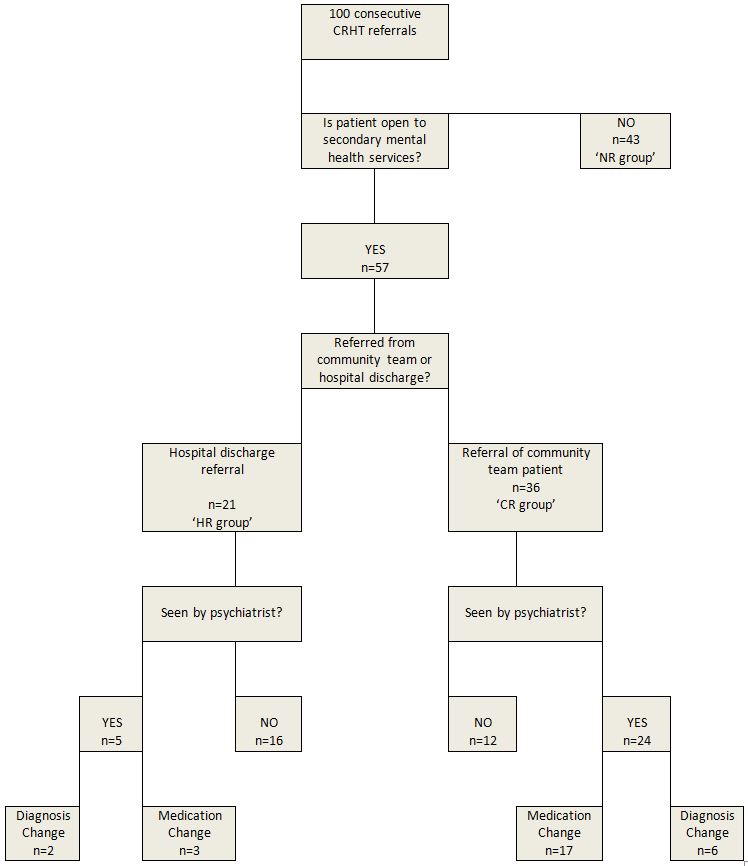
We examined 100 consecutively accepted referrals to a CRHTT from 1st December 2016. The patients were divided into three groups: those being discharged/referred from hospital (HR), those referred from the community (CR), and those who were not open to secondary mental health services at the time of referral (NR). The age range and gender of the groups were noted. Thereafter, the NR group was excluded from analysis for the obvious reason that the CRHTT was not providing a second opinion in their case. The HR and CR groups were further reduced by excluding patients who were not seen by a CRHTT psychiatrist. The remaining patients in both groups were scrutinised regarding a change in medication; this was also recorded for the previous and next care occasions. The likelihood of medication change at the next treatment event was analysed to establish whether it was affected by the previous event. The numbers of patients with CRHTT diagnosis change were also recorded for both groups.
Results
Figure 1: Project Flowchart
Figure 2: Group Demographics
n
Patient Gender
Patient Age
Time with CRHTT
Male
Female
Average
Range
1-7 days
> 7 days
No prior referral open (NR)
43
20 (47%)
23 (53%)
36.0
19-60
5 (12%)
38 (88%)
Community referral (CR)
36
13 (36%)
23(64%)
37.8
19-66
7 (19%)
29 (81%)
Hospital referral (HR)
21
10 (48%)
11 (52%)
39.0
19-63
6 (29%)
15 (71%)
There was little difference in age between the three groups (average ages were: CR=37.8, HR=39.0, NR=36.0). There was a lower proportion of men in the CR group than were present in the HR and NR groups (36% as against 48% and 47%). Whether a psychiatrist saw a patient appeared to be related to both the referral source and the length of CRHTT stay. Most (n=16, 76%) patients in the hospital-referred group (HR) were not seen by a psychiatrist while most (n=24, 67%) of those referred from the community (CR) did receive such an outcome. No community-referred patient was seen by a psychiatrist if they were with the CRHTT for less than a week. These short-stay patients accounted for 7 out of the 12 community-referred patients who were not seen. This suggests that a psychiatric assessment should be scheduled more quickly after community referrals so as to offer patients a more comprehensive service.
Psychiatric assessment led to changed diagnoses for 28% (8/29) of patients. This figure was 40% (2/5) for the HR group and 25% (6/24) for the CR group.
Medications were changed for 69% (20/29) of patients seen by a psychiatrist. In the subgroups; 60% (3/5) of HR psychiatric assessments resulted in a change of medication while 71% (17/24) of CR psychiatric assessments led to medication changes.
The chi-square statistic was used to evaluate whether a recent medication change, during the inpatient stay or at the most recent outpatient appointment, made the CRHTT less likely to adjust medication. This indicated that there was no relationship between the two events. A similar analysis indicated that the likelihood of a medication change at the patient’s next community appointment was increased by seeing a CRHTT psychiatrist but unrelated to whether that assessment had resulted in a change of medication.
Discussion
We have demonstrated in this study that a typical CRHTT is providing a diagnostic and second opinion service. Changes in medication were more than twice as frequent as changes in diagnosis – this is perhaps unsurprising as diagnostic changes would be likely to require a different prescription.
Most community referrals were actively evaluated in terms of both diagnosis and treatment. This is a significant change to the original function of the CRHTT where a psychiatric assessment was not a standard aspect of care when very few of the original CRHTTs included a psychiatrist. This may also reflect the current pressures on community teams, which are frequently short-staffed, leading to more competition for the available clinic appointments. Consequently, patients may not have seen a psychiatrist for some time and their requirements may have changed. It is, however, also known1 that community patients who have not been reviewed recently or who have a long wait before their first assessment are more likely to present in crisis.
The diagnostic and second opinion function of the CRHTT is more prevalent when patients have been referred by the community team (67% reviewed, 47% medication changed) rather than on discharge from hospital (24% reviewed, 14% medication changed). This appears to largely reflect the fact that relatively few discharges were seen by the CRHTT psychiatrist because these patients had just received a full consultant-led discharge treatment plan. This may be another example of community service pressures leading to patient crises and thus engagement with alternative services – in this case inpatient care may be offering a second opinion service. The current separation of community and inpatient services will augment this effect as previously the patient would have been more likely to receive continuous care from the same consultant. This is an interesting view of current service configuration. The reduced continuity of care is often seen as a disadvantage but it does present an opportunity for a fresh evaluation of a patient’s diagnosis and medication by a different psychiatrist.
Longer lengths of stay with the CRHTT made psychiatric assessments more likely. It was particularly clear that discharge within a week made a psychiatric review unlikely. The proportion of community-referrals seen by a CRHTT psychiatrist could be increased to 83% if patients were to be seen within 24 hours. This figure is derived from the assumption that psychiatrists would then see the same proportion of both long and short stay patients. The residue would include those patients who refuse to engage with such an appointment.
It is interesting that chi-square statistical analysis suggests that the only influence on prescription change at the next appointment is whether the patient was seen by a CRHTT psychiatrist. It is not related to whether or not the CRHTT psychiatrist changed the medication. It is difficult to see why this should be the case unless the community psychiatrists consider the patients’ needs in more detail or are tempted to regain control after the referral to another psychiatrist.
In conclusion, the addition of psychiatric care to CRHTTs may be a valuable adjunct to the current pressures on community teams. The current trend to separate community, inpatient and CRHTT care is often cited as a disadvantage due to reduced continuity of care for patients. This project has drawn attention to the fact that it also offers opportunities for new teams to re-evaluate both diagnosis and treatment which offers patients the advantage of an internal second-opinion service. This advantage could be offered to more community-referred patients, albeit with more resources, by ensuring that they are assessed by the CRHTT psychiatrist within 24 hours.
Limitations
This is a small study conducted in a single CRHTT. It does, however, offer an indication of the evolving role of the CRHTT and its relationship to other services.
A dermatoscope is a hand-held device for examining the appearance of the skin. Dermoscopy has become an increasingly used and valued tool in the assessment of various skin lesions, and more recently, inflammatory rashes. It is quick, cheap and when used correctly, dermoscopy is an essential tool in helping clinicians detect early stage skin cancer. Various national and international guidelines recommend routine use of dermoscopy in the assessment of pigmented lesions1,2 because it enhances melanoma detection rates3,4 and can help confirm the diagnosis of benign lesions such as haemangiomas and seborrhoeic keratoses. As with any skill, competency takes time to develop and a combination of various learning and assessment methods is best. The dermatology specialist training curriculum in the United Kingdom (UK) states that trainees should be competent in using a dermatoscope and interpreting findings, while recognizing the limitations of this tool5. Assessment of these clinical skill and behavioural competencies using direct observation of procedural skills (DOPS), case-based discussion (CBD), mini clinical examination (mini-CEX), and/or multisource feedback (MSF) is suggested. There is no specific guidance on what resources a trainee should use to achieve these competencies, nor on what is the minimum expected dermoscopy skillset at completion of specialist training.
The aim of this survey was to explore dermoscopy use amongst dermatology specialist trainee registrars in the UK including frequency of use, how it is being taught and whether trainees feel their dermoscopy training has been adequate.
An online survey was designed and distributed to dermatology trainees in the United Kingdom using an email link and hard copies were distributed at a national dermoscopy course. Respondents who did not identify themselves as dermatology trainees were removed from the analysis. Responses were collected anonymously, then collated and analysed using SurveyMonkey® computer software.
Twenty-five percent (59/238) of dermatology trainees completed the survey. On average, 92% (54/59) use dermoscopy more than once daily. Eighty-five percent (50/59) always use dermoscopy when assessing pigmented lesions while 34% (20/59) always and 59% (35/59) sometimes use it to assess non-pigmented lesions. When asked about specific tools used to learn dermoscopy, 41% (24/59) have been on a previous course, 42% (25/59) reported attendance at a lecture or seminar, 46% (27/59) have used a dermoscopy text book, 14% (8/59) have attended a conference, 19% (11/59) have used online resources. Seventeen percent (10/59) have never used any of the above learning methods. (Figure 1a). Amongst those who have attended a formal dermoscopy course (n=24), 92% (22/24) of these were ≤1 day in duration. When questioned about informal teaching in clinical practice, 12% (7/59) frequently, 56% (33/59) sometimes, 31% (18/59) rarely and 2% (1/59) never receive teaching from their supervising dermatology consultant. (Figure 1b). Fifty-four percent (32/59) feel they have received adequate training in dermoscopy while the remaining 46% (27/59) feel their dermoscopy training is inadequate for their training stage (Figure 1c). Seventy-three percent (43/59) have access to dermoscopic photography within their local dermatology department.
Fig 1a - Have you undertaken any formal study in dermoscopy? 49% of trainees have attended a lecture, 2% a seminar, 14% a conference, 41% a course, 19% have used an online resource, 46% have used a book, 17% have not used any resource.
Fig 1b- Do you receive dermoscopy training from your supervisor in clinic? 56% of trainees sometimes, 31% rarely, 12% frequently, and 2% have never received training from their seniors in clinic.
Fig 1c- Do you believe that you have received adequate training in the use of a dermoscopy for your training grade?
These results of this survey highlight the need for dermoscopy training to be reviewed within the UK national training curriculum for dermatology. Despite daily use by the vast majority, dermoscopy training is largely self-directed and highly variable amongst individual trainees. Of concern, a significant proportion of those who responded feel their dermoscopy skills are inadequate for their training stage. Of note, the 25% response rate means that the results of this survey may not be representative of dermatology trainees in the United Kingdom as a whole.
This is the first time that dermoscopy use has been explored through a national survey of dermatology trainees in the UK, to the best of our knowledge. A survey on dermoscopy use was carried out by The British Association of Dermatologists (BAD) in 20126 but the majority of responses were from dermatology consultants. This confirmed that 98.5% of respondents regularly used dermoscopy, while 81% had received any training. The most frequent source of training was UK based courses, which 62% of respondents reported attending. Of note, 39% of all respondents lacked confidence when making a diagnosis based on their interpretation of dermoscopy findings. It is not clear how many of those lacking in confidence were consultants, trainees or specialty doctors. Although the situation may have improved since 2012, these results do suggest that dermoscopy training needs have not been met for a proportion of doctors across the dermatology community.
Dermoscopy training is an important issue to address for several reasons. The volume of cutaneous lesions being referred to dermatology is increasing, and skin cancer referrals and treatment now account for 50% of a UK dermatologists’ workload7. For every melanoma diagnosed, a dermatologist may expect to see 20–40 benign lesions referred from general practitioners (GPs)7. These facts highlight the importance of maximising diagnostic skills which frequently include using dermoscopy as part of clinial assessment. Lack of adequate training is a common self-reported reason for dermatologists not using dermoscopy8. Both trainees and their supervising bodies have a responsibility to maximize training opportunities and embed the use of dermoscopy in routine practice.
In conclusion, we feel UK dermatology trainees and indeed any clinician who utilizes this tool, would benefit from a more standardized and integrated approach to dermoscopy teaching to ensure safe practice of this skill and deliver high quality evidence-based patient care.
With the increasing use of ultrasound as a standard examination in the first trimester, more incidental adnexal masses are detected. The reported incidence of adnexal masses in pregnancy varies, depending on the criteria used to define the mass. A literature review by Goh W. et al., found that 1% of all pregnancies are diagnosed with an adnexal mass 1. A more recent article has suggested adnexal masses are diagnosed in 5% of all pregnancies 2. Simple and functional cysts are very common, and they usually resolve after the first trimester 3. Mature teratomas are by far the most common persistent adnexal masses found in pregnancy 8. It has been estimated that up to 5% of adnexal masses in pregnancy are malignant 4.
Ovarian cysts are typically asymptomatic, but they can cause pain due to pressure on adjacent organs, rupture, bleeding or torsion. The latter case is a significant health condition which mainly requires emergency surgical intervention. During pregnancy, surgical management of ovarian cyst complications is more difficult and more challenging. This is mainly because of other differential diagnosis causing similar symptoms related to pregnancy such as ectopic pregnancy and miscarriage. In case of surgical intervention, the second trimester of pregnancy is supposed to be the safest window for surgery as the risk for drug-induced teratogenicity is smaller than in the first trimester, most functional cysts have disappeared by then and it is technically less difficult than operating during the third trimester 13.
Antenatally, ultrasound is considered to be the best first-line imaging to evaluate adnexal masses 5. Ovarian mass characterization into benign, malignant or borderline can be challenging in pregnancy. This is mainly due to the effect of high levels of gestational hormones which can cause decidualisation of the cystic or solid parts of the ovaries. Benign masses can mimic malignant masses due to this pregnancy related phenomena 12. One of the largest data in literature on ovarian mass characterization is published by the International Ovarian Tumor Analysis group (IOTA). All IOTA studies excluded pregnant women when they developed and validated the rules and models to characterize ovarian masses 14-17. This limits our knowledge and ability to use these models in pregnant women. It is known that tumour markers may be raised in pregnancy and should therefore not routinely been done 7. An alternative diagnostic tool is Magnetic Resonance Imaging (MRI) which is considered to be safe in pregnancy and can be helpful if the ultrasound imaging is inconclusive in evaluating whether a mass is benign or malignant 6; 10. The American College of Gynecology and Obstetrics recommends that pregnant patients should be reviewed on a case-to-case basis and stated that there are no known biological effects of MRI on fetuses. However, Gadolinium, which help in characterizing ovarian masses, should be avoided when examining a pregnant patient 11.
The aim of this retrospective study was to look into characteristics, size and subsequent management of cases of adnexal masses in early pregnancy.
Methods
This was a retrospective study of data collected between 12/01/2014 and 14/11/2016 in the Early Pregnancy and Gynaecology Unit (EPAGU) of a tertiary referral centre (Guy’s and St Thomas’ NHS Trust, GSTT) in central London. The Ultrasound reporting system (Astraia Software Gmbh, Version 1.24.10, Munich, Germany, 2016) was searched for data. Cases included were consecutive. The study was approved as a service evaluation audit by the Clinical Governance team at Guy’s and St Thomas’ NHS Trust. The study included women who were diagnosed with an adnexal mass while having a transvaginal ultrasound scan TVS at or before 15 weeks of gestation. Pregnancy was confirmed by a positive pregnancy test and an intrauterine gestation on transvaginal ultrasound scan. Women who had the first gestational TVS after 15 weeks of gestation, pregnancies of unknown location, ectopic or trophoblastic pregnancies and patients who had ovarian stimulation treatment were all excluded.
Repeat ultrasound scan reports were retrieved from the Astraia system. Further procedures, tests and imaging results were retrieved using the Electronic Patient Reporting system at GSTT (EPR application, iSOFT Group plc., USA, 2004), PACS (GE Medical Systems, Wisconsin, USA, 2006), Badgernet (Clevermed, Client version 2.9.1.0, Edinburgh, UK). We have used the subjective impression of the examiner as the index test. If surgery was performed the final outcome to identify benignity or malignancy was considered to be the histological diagnosis if any removed tissue. Cytology was used for a reference test in two cases when ovarian cysts were aspirated only. Borderline tumours were classified as malignant for statistical analysis. Tumours were classified using the criteria recommended by the World Health Organisation (WHO) 9; 10. All ultrasound scan images were available and reviewed by author TEG to confirm the US finding. For statistical analysis, the SPSS software package was used (version 24 for Windows, Chicago, IL, USA). A two tailed student’s t test was used to compare means in ovarian masses diameters and a p value of less than 0.05 was considered statistically significant.
Results
7150 patients underwent transvaginal scans for early pregnancy in that period. In total 48 cases of women with adnexal masses in pregnancy and completed data were analysed. Seven women have been excluded; one woman being postpartum at the time of the finding of a large endometrioma, five pregnancies due to assisted conception and one woman was found to have a corpus luteum cyst (Figure 1).
Figure 1: Study flow chart.
41 women with 46 ovarian cysts could be included in the study. Two women had bilateral ovarian cysts, one had two ipsilateral cysts and one woman had three ipsilateral cysts. The mean age at the time of detection of the ovarian mass was 30 (95%CI:28-32) (Fig.2).
Figure 2: Age distribution in the study group.
The mean gestation at the time of first ultrasound was 7.4 weeks (95%CI:6.6-8.3). The mean diameter of ovarian cysts measured 47.7mm (95%CI:39.9-55.4). In 36 women ultrasound alone was performed to reach diagnosis, one woman had an extra MRI scan, two women had tumour markers on top of the TVUS and in two women an MRI scan and tumour markers were performed after the TVUS. The ovarian cyst(s) was on the right ovary in 16/41 women, on the left in 22/41, bilateral in 2/41 and in one case the side of the cyst was not reported. The most common ultrasound subjective impression was mature teratoma (22/46 cysts), followed by simple cysts (12/46 cysts), haemorrhagic cysts (6/46 cysts), endometriomas (5/46 cysts) and one possible mucinous Borderline tumour. The latter was confirmed later on histology as the stage FIGO 1A intestinal type mucinous Borderline tumour (Fig.3).
Figure 3: Distribution of origin of cysts by histology.
In total 8/41 women (19.5%) underwent surgical intervention; of these eight cases six underwent major surgery under GA and two had a cyst aspiration under local anaesthesia. Seven out of these eight masses were classified as benign on USS and were subsequently confirmed to be benign by histology or cytology. In only one case a complex adnexal mass was found on USS examination at 9 weeks of gestation and the MRI scan reported possible malignancy. Tumour markers in this 23-year-old woman were normal and a laparotomy was performed at 17 weeks of gestation to remove the mass. Histology showed the mass to be a mucinous borderline tumour, FIGO stage IA. In another patient, an oophorectomy had to be performed at the time of the Caesarean section at term for fetal distress as the ovary was found to be necrotic. In this patient an ultrasound at 10 weeks of pregnancy had demonstrated a 6cm diameter haemorrhagic cyst, which had presumably torted during the pregnancy without any symptoms to prompt the patient to refer herself. Histology in this case had shown an infarcted cyst with fibrosis and calcification. In four of the major surgery cases performed under GA uncomplicated laparoscopies were performed to remove the adnexal mass; in one case a laparoscopic salpingoophorectomy was performed as an emergency for a suspected ovarian torsion at 16/40 weeks. In three cases a laparoscopic procedure for cystectomy was performed electively for ongoing pain. In the first case a cyst was diagnosed in early pregnancy subsequently there was a miscarriage and the cyst was removed 4 months after the diagnosis. In the second case a cyst was found in early pregnancy the woman had a termination at 11 weeks of pregnancy and a cystectomy 5 months later. In the third case a laparoscopic cystectomy was performed 8 weeks after the diagnosis, however the woman suffered a miscarriage at 12 weeks of gestation. Histology confirmed dermoid cysts in all four of these cases. The two cyst aspirations performed under local anaesthesia and ultrasound guidance were both symptomatic for torsion, one at nine weeks and one at ten weeks of pregnancy. In both patients the procedure has been successful. 33/41 (80.5%) with no indication for surgical intervention. There was a significant difference in the mean diameter of ovarian cysts in the expectant management group (41.2mm; 95%CI:34.7-47.7) compared with the mean diameter of cysts in the surgically managed group (74.5mm; 95%CI: 49.2-99.8) (Fig.4).
Figure 4: Mean diameter of the ovarian cysts.
In 33/41 patients no surgical intervention was needed during pregnancy. 13/33 patients had no follow up of their ovarian cyst arranged and no further mentioning of the cysts on routine growth and anomaly scans during pregnancy was found. In 20/33 patients at least one routine follow-up scan was performed 1-2 weeks after the diagnosis and in 12 of these 20 patients a second follow-up had taken place at least 1 month after the diagnosis. In one of the 20 patients with recorded follow-up’s an MRI scan had been arranged 2 months after the initial USS finding of a dermoid cyst.
Discussion
The results of our study confirm findings from previous studies: The vast majority of ovarian masses in pregnancy are benign and invasive cancer in pregnancy is rare; The results show a significant relation between size of adnexal mass and probability for surgery; Ultrasound examination of adnexal masses has been proven to be accurate and safe in pregnancy; Managing ovarian cysts in pregnancy can be challenging. Goh et al. have reported similar outcomes, namely that ovarian torsion is still reported as a rare event in pregnancy and that the management of most adnexal masses in pregnancy can be conservatively managed if asymptomatic and if there are no ultrasound findings suspicious for malignancy 8. If a surgical intervention is needed for persistent masses with complications such as torsion Goh et al. have found that laparoscopy during 1st and 2nd trimester can be safely performed 1. In our cohort two out of six women underwent successful major surgery during the 2nd trimester of pregnancy. One had an emergency laparoscopy for a torsion at 16 weeks of pregnancy and the other had a laparotomy at 17 weeks of pregnancy for a mucinous borderline tumour.
However, to our knowledge currently no evident guidelines exist on how to manage and follow-up ovarian masses during pregnancy. The characteristics and presentation of ovarian mass complications in pregnancy can be mimicked by similar symptoms related to pregnancy, such as ectopic pregnancy. In one of our cases a woman with a known ovarian cyst was found to have a necrotic ovary at the time of Caesarean section, despite no signs of torsion at any time during pregnancy. This only highlights how challenging and difficult the assessment of ovarian masses during pregnancy can be. Additional diagnostic examinations such as tumour markers in suspicious ovarian masses have been found difficult to interpret in pregnancy. However, there has been literature suggesting that if a mass is strongly suspicious for malignancy, it is likely that CA-125 will be severely elevated (1000-10 000) 7.
The strength of this study is that the data has been collected using the expertise and facilities of a tertiary referral centre in London (GSTT). The limitations of this study include retrospective data collection, small numbers of cases and loss of follow-up. Although, our study shows the benign nature of most ovarian masses in pregnancy and the ability of ultrasound to safely characterize ovarian masses, a prospective study is required to validate our results. As it is difficult to interpret ovarian cancer tumour markers in pregnancy 7, other models, such as the IOTA Simple Rules14,16 or the ADNEX model17 may play a role for further characterisation of ovarian masses. A prospective trial is required to validate these models in pregnancy.
Telephone triage has been used by many practices in primary care to manage workload and prioritise patients for same day appointments.1,2 Telephone triage may have benefits in terms of managing work load,3 but is also associated with certain risks,4 which has worried both clinicians and patients.5 The analysis of the use of telephone triage has so far focused on the ease of access, demand management, cost effectiveness, quality of consultations, safety and patient satisfaction. However, other effects in terms of patient outcome may exist. One of the main focuses in General Practice is to identify symptoms and signs of cancer for early diagnosis to improve outcome. Our study aims to assess whether telephone triage helps in prioritising early assessment and referral of patients who are subsequently diagnosed with cancer.
Methods
A retrospective analysis of all the patients at our practice who had a diagnosis of cancer made between April 2013 and December 2014 was carried out.
Patients have a choice of 2 different ways to book an appointment in our practice.
Telephone triage for same day appointment requests, where a triaging doctor decides about the urgency of a problem and books the appointment, arranges tests or gives advice after speaking to patients over the phone. This group is referred as “Group 1” in this study.
Patients book the next available appointment to see a GP through reception without any triage. This group is referred to as “Group 2” in this study.
The date of first contact with the GP practice for the symptoms which later lead to a diagnosis of cancer was noted for both groups. This was the telephone triage date for the first group and the date the appointment was booked by the patients for the second group. The date the patient was first seen in secondary care for further assessment and investigations was also noted. The duration between first contact with GP practice and GP appointment, and the duration between the first contact with practice and first hospital appointment were calculated. This information was gathered from practice computer records.
Patients who were diagnosed with cancer through screening were excluded. Slow growing tumours which do not merit a 2-week rule referral, such as basal cell cancer of skin were excluded. Patients whose appointments were initiated by the GP on reviewing the results of routine tests were not included. Patients diagnosed with cancer in hospital without going through primary care referral were also excluded from this study.
There are two research questions:
Is there a significant difference in the time required from the first contact with primary care to the GP Clinic appointment between Group 1 and Group 2 patients?
Is there a significant difference in the time required from the first contact with primary care to the date the patient was seen in the secondary care between Group 1 and Group 2 patients?
Descriptive statistics (such as the mean, standard deviation, median, minimum, and maximum) were used to present the time required from the first contact with primary care to the GP Clinic appointment; and the time required from the first contact with primary care to the date patient seen in the hospital, for Group 1 and Group 2 patients. Wilcoxon rank-sum test was used to answer each research question. A p-value less than 0.05 indicated significance at the 0.05 level.
All data analyses were conducted using SAS.
Results
A total number of 39 patients were included in the study. Among them, 13 (33%) used telephone triage to make their appointments and 26 (67%) booked their appointment by themselves.
Figure 1 shows the bar charts of the time required from the first contact to GP practice, to the GP clinic appointment for Group 1 and Group 2 patients. It took 0-3 days for 12 Group 1 patients and 8-11 days for 1 Group 1 patient. The time required from the first contact to GP practice to the GP Clinic appointment for Group 2 patients can be illustrated by the same manner.
Figure 1: Bar charts of the time (days) required from the first contact for surgery to the GP Clinic appointment for Group 1 and Group 2 patients. (Note that the midpoints 2, 6, 10, 14, 18, and 22 represented days within the range of 0-3, 4-7, 8-11, 12-15, 16-19, and 20-23, respectively.)
Table 1 shows the summary statistics for the time (days) required from the first contact with the practice, to the GP Clinic appointment for Group 1 and Group 2 patients. The average time required was 0.77 days for Group 1 patients and the average time required for Group 2 patients was 7.88 days. The results of Wilcoxon rank-sum test indicated that this was a statistically significant difference in time required from the first contact for surgery to the GP Clinic appointment between Group 1 patients (patients using Telephone triage to make their appointments) and Group 2 patients (patients booking their appointment by themselves) (p = 0.0020).
Number
Mean
SD
Median
Min
Max
Group 1
13
0.77
2.24
0
0
8
Group 2
26
7.88
7.53
6
0
23
Table 1:Summary statistics for the time (days) required from the first contact for surgery to the GP Clinic appointment for Group 1 and Group 2 patients. SD = standard deviation.
Figure 2 shows the bar charts of the time required from the first contact with the GP practice, to the date patients were seen in the secondary care for Group 1 and Group 2 patients. It took 0-5 days for 4 Group 1 patients, 10-19 days for 5 Group 1 patients, 20-29 days for 1 Group 1 patient, 30-39 days for 2 Group 1 patients, and 90-99 days for 1 Group 1 patient. The time required from the first primary care contact to the date patient seen in the secondary care for Group 2 patients can be illustrated by the same manner.
Figure 2: the bar charts of the time required from the first contact for surgery to the date patient seen in the hospital for Group 1 and Group 2 patients. (Note that the midpoints 5, 15, 25, 35, 45, 55, 65, 75, 85 and 95 represented days within the range of 0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89 and 90-99, respectively).
Table 2 shows the summary statistics for the time (days) required from first contact with GP practice to the date patients were seen in the hospital for Group 1 and Group 2 patients. The average time required for Group 1 patients was 19.54 days and the average time required for Group 2 patients was 35.69 days. The results of Wilcoxon rank-sum test indicated that this was a statistically significant difference in time required from the first contact to the primary care to the date patient seen in the hospital between Group 1 patients (patients using Telephone triage to make their appointments) and Group 2 patients (patients booking their appointment by themselves) (p = 0.0474).
Number
Mean
SD
Median
Min
Max
Group 1
13
19.54
23.41
10.00
3
90
Group 2
26
35.69
26.28
32.50
1
88
Table 2: Summary statistics for the time (days) required from the first contact for surgery to the date patient seen in the hospital for Group 1 and Group 2 patients. SD = standard deviation.
Type of Cancer
Number of Patients
Lung
5
Breast
5
Colorectal
4
Malignant melanoma of Skin
3
Squamous Cell carcinoma of Skin
3
Oesophagous
2
Stomach
2
Urinary Bladder
2
Larynx
2
Pancreas
1
Endomtrium
1
Cervix
1
Kidney
1
Prostate
1
Testis
1
Tonsil
1
Lymphoma
1
Appendix
1
Myelodysplastic
1
Olfactory Neuroblastoma
1
Table 3: Number of patients with types of cancer.
Discussion
More than 90% of contacts with healthcare in the UK occur in primary care.6 The estimated numbers of consultation for a typical practice in England rose from 21,100 in 1995 to 34,200 in 2008 as per analysis conducted by Hippisley-Cox J et al.7 With increasing demands being placed upon General Practice, there is a need to explore innovative ways of working which enable the prioritisation of patients with concerning symptoms. Telephone triage has been considered to reduce the demand for face-to-face consultation with GPs,3 which can potentially free up time for effective use. NHS England report ‘Transforming Urgent and Emergency Care Service in England’ suggests GPs should offer more telephone consultations to reduce pressure on accident and emergency.8 However, a cluster-randomised controlled trial (The Esteem Trial) across 42 practices showed that telephone triage increased the number of primary care contacts in the following 28 days, after patients’ request for same day GP consultation.1
With increasing demands for consultations, it is important to have a system to identify and prioritise patients for early assessment; who may have a suspected cancer diagnosis. Our study demonstrates that telephone triage reduces the time from first primary care contact to face to face assessment in primary and secondary care for patients with suspected cancer. Patient numbers are small and the sample is from one practice, yet the difference seen is statistically significant.
Cancer stage at diagnosis is one of the major reasons for difference in cancer survival in different countries.9,10 The delay in cancer diagnosis can be due to multiple factors. Telephone triage can provide an opportunity to patients to discuss symptoms early with a GP, and this can reduce delays in the cancer diagnosis pathway. It has been shown that certain alarm symptoms are associated with the likelihood of cancer diagnosis 11 and these can be used to prioritise the patients in triage process. It may also reduce anxiety amongst patients waiting for an appointment, who are concerned about their symptoms.
Telephone triage should not only be seen as a way of managing demands and appointments but also as a system to improve patient outcome. Further research is clearly needed on a larger scale to determine if the results are reproducible in other settings as patients’ knowledge and understanding about cancer warning symptoms and healthcare seeking behaviour may vary among different population sets.
Oestrogen receptors (ERs) are expressed in a large proportion (approximately 70%1) of breast cancers (BCs). Oestrogen stimulates the growth of breast epithelial cells (both normal and cancerous) by binding to these receptors. Aromatase inhibitors (AIs) prevent the conversion of androstenedione to oestrogen by the enzyme aromatase in peripheral tissues, which is the predominant source of oestrogen in post-menopausal women. Consequently, they are routinely offered to post-menopausal women with ER-positive early invasive breast cancer as adjuvant therapy2. However, decreased residual oestrogen levels are associated with increased bone resorption by osteoclasts. The menopause initiates an accelerated phase of bone loss lasting 4 to 8 years, which is followed by a slower phase which continues indefinitely3. AI-induced bone loss (AIBL) occurs at a higher rate than natural menopausal bone loss4. Women are therefore at increased risk of fractures while they are on AI therapy5, with an associated higher rate of fractures as demonstrated in the ATAC trial6.
Recent data have supported more prolonged use of AIs (10 years instead of 5) to achieve lower BC recurrence rates7. This may lead to changes in future clinical practice in that ER-positive BC patients may be on an even longer course of AIs. This is likely to translate into a higher fracture risk in patients on long term treatment, and bone health in these patients should remain an important consideration.
Several guidelines have emerged over the years, as summarised by Hadji et al8, to aid the assessment of fracture risk in women receiving BC treatment, and management of AIBL. In the UK, the guidance in use and recommended by the National Institute of Health and Clinical Excellence (NICE) is a UK expert group consensus position statement issued in 2008 (Guidance for the Management of Breast Cancer Treatment-Induced Bone Loss)9. This includes two treatment algorithms for the assessment and management of bone loss in early BC: one for women with adjuvant treatment-induced premature menopause and the other for postmenopausal women starting adjuvant AI.
Despite the existence of various guidelines on the management of AIBL in BC patients, few articles have been published on the practical adherence to guidance. We carried out an audit of the management of AIBL in BC patients in a large general practice (with roughly 9000 registered patients) in Bradford (UK). Given the small number of eligible patients in our study, we undertook a review to identify all studies in the English literature assessing practical adherence to guidance on AIBL to establish whether gaps identified in our practice reflects a more widespread issue.
Our study
Methods
We carried out a retrospective study in a general practice in April 2015. Using the clinical electronic system used at the practice (SystemOne), we performed a search for all registered patients documented to currently be on AIs or to have previously been on them at any point, for the treatment of BC, using the search terms “anastrazole”, “Arimidex”, “exemestane”, “Aromasin”, “letrozole” and “Femara”. We excluded male patients (not addressed by current guidelines) and patients who started their treatment with AIs prior to the issuance of the UK guidance in 2008. For each patient we gathered data on the indication of treatment, menopause status, the date of initiation +/- completion of treatment, details of dual energy Xray absorptiometry (DEXA) scan and bone mass density (BMD), blood biochemistry results, documented risk factors for fractures and details of bone protection treatment. We audited our practice against the UK guidance.
Summary of the UK guidance
All post-menopausal patients starting AIs should have a baseline DEXA within 6 months of treatment initiation. Patients are stratified as low, medium and high risk for fractures based on the baseline T-scores. Medium and high risk patients should have vitamin D and calcium supplements, and high risk patients should be started bisphosphonates. A repeat DEXA scan should be performed 2 years later for medium and high risk patients to re-assess BMD and augment bone protection therapy as appropriate. Patients aged 75 years and above with at least one clinical risk factor for fractures should be started on a bisphosphonate regardless of their baseline BMD.
Results
There were 12 female patients who started AIs for BC treatment from 2008 onwards. Treatment was initiated between the years 2008 and 2014 (inclusive). The mean age was 67 years (range 57-81 years) and all 12 were post-menopausal at the time of adjuvant hormonal therapy initiation. Three were initially on tamoxifen and switched to an AI after 2 years of tamoxifen therapy.
Three patients (25%) did not receive an initial DEXA scan and had no subsequent risk fracture management. One of them was 75 years of age at the time of AI initiation and was on long term steroids (i.e. should have been on a bisphosphonate regardless of BMD), but she was not on a bisphosphonate.
Of the remaining 9 (75%) who did have a DEXA scan,
One was at high risk (T-score -2.7), and was appropriately started on a bisphosphonate and calcium and vitamin D supplements.
7 patients were at medium risk of osteoporotic fractures (T-score range -2.0 to -0.1). All were started on calcium and vitamin D supplements.
7 were eligible to have had a repeat DEXA scan at the time of the study but only 4 had a scan. Of these four, one was found to have incurred significant bone loss and was started on a bisphosphonate.
The mean interval between AI initiation and baseline DEXA was 1.9 months (range 0.2-4.4). The mean interval between the initial and repeat DEXA scans was 4.1 years (range 2.5-5.1).
Figure 1 illustrates the proportion of scans requested by different clinical teams involved in the patients’ care.
Figure 1: Who requests DEXA scans?
Literature review
Methods
We performed a search with the following terms on the Ovid Medline and Embase databases: “bone loss”, “osteoporosis”, “osteopenia”, “aromatase inhibitor”, “breast cancer”, “guidelines” and “guidance”. Of the 137 results returned after deduplication, we selected original and review articles assessing management of AIBL against established guidelines. We retrieved further papers by reviewing the references of these articles.
Results
The original articles generated are shown in Table 1. While conference abstracts have not been included here, they have been reviewed for the purpose of our discussion.
Table 1: Original articles publishing the results of audits of bone health management in BC patients on AIs against established guidelines
Authors
Place of study
Guidelines used to define audit standards
Sample size
Adjuvant therapy
Roberts R et al10
Australia
ASCO*, ESMO*, Hadji et al8, Belgian Bone Club
42
Both AI and tamoxifen
Spangler L et al11
Washington, USA
ASCO*
342
AI
Bosco D12
Italy
Results from the ARBI* trial13
39
AI
Gibson K et al14
Colorado, USA
ASCO*
54
AI
Ligibel et al15
USA
ASCO*, NCCN*, Hadji et al8
9138
AI
Dong et al16
UK
NICE guidelines based on UK expert group consensus9
100
AI
Zekri J et al17
Saudi Arabia
NICE guidelines based on UK expert group consensus9
367
AI
*ASCO: American Society of Clinical Oncology, ESMO: European Society for Medical Oncology, NCCN: National Comprehensive Cancer Network, ARBI: Arimidex Bone Mass Index and Oral Bisphosphonates
Discussion
The results of our audit show that we are failing to meet our current national standards pertaining to management of AIBL in BC patients. Our literature review confirms that this is a widespread issue and that results from larger studies are in agreement with ours.
25% of our patients never had a baseline BMD measurement. Similar findings have been reported in the literature11,12,14. However, Roberts et al report much higher rates of DEXA screening pre –AI10. Reasons for this were felt to be the presence of an institutional treatment algorithm as well as a survivorship programme.
We had a poor rate of repeat DEXA scans. Gibson et al and Spangler et al also noted that the highest rate of DEXA scanning was around the time of AI initiation compared to after initiation of therapy11,14. For the patients who had a repeat BMD measurement in our study, practice was not in line with recommendations as the interval between the initial and repeat DEXA scans (mean 4.1 years) was much longer than the recommended 2 years. This may be because recommendations made by the breast surgery team were different (intervals of 3 to 5 years being recommended in some cases in clinic letters written to the GP by the breast team).
Gibson et al found that 75% of their patients were on calcium and vitamin D, which deviates from the ASCO guidelines that they audited their results against14. The ASCO guidelines recommend that all BC patients should be on calcium and vitamin D therapy. In some studies10.12 not all women diagnosed with osteoporosis were started on bisphosphonates. Although women diagnosed with osteoporosis were started on bisphosphonates in our cohort, the suboptimal uptake of DEXA scans means that we may have missed the diagnosis in a number of patients.
From the articles included in our literature review, several reasons have been suggested as causes for deviation from guidelines when it comes to management of AIBL in BC patients. Lack of awareness of guidelines, especially amongst general practitioners (GPs), has been recognised as a barrier, as well as the expectation that other healthcare professionals should be addressing this aspect of care10. In our study, DEXA scans were mostly requested by the specialist breast team initiating AIs, or by the GP at the request of the breast team. Based on our experience, it is not clear who the responsibility of bone health management lies with – the breast surgery team, the oncologist or the GP. In a survey of 307 UK-based breast surgeons and oncologists 57% of responders felt that oncologists should be responsible for this18. In practice, patients may be discharged from specialist clinic follow-ups while they are still on hormonal therapy and GPs would be expected to continue their care. When this happened in our cohort of patients, there was no evidence of clear written communication from specialist teams to the GP regarding outstanding aspects of care that the GP would be expected to follow up.
An analysis of five different guidelines regarding antiresorptive treatment in postmenopausal women with hormone-receptor positive BC showed that little consistency exists among the five guidelines19. The variety of guidelines and recommendations regarding bone loss in BC patients probably leads to inconsistency in practice. In our study, specialist teams have sometimes recommended an interval of 3 to 5 years between BMD tests, deviating from the national recommendation of 2 years. This can translate into confusion when care is taken over by the community team after the patient is discharged from the specialist team.
Recommendations
We therefore suggest that institutional guidelines on bone health management in BC patients on AIs (as well as other hormonal therapies) should be created to improve awareness amongst clinicians as this has shown to improve rates of DEXA scanning10. Local guidelines should closely mirror national guidelines to allow delivery of standardised care across the country, but should include clear recommendations as to which local team should be responsible for bone health management, as well as recommendations regarding the creation of a care plan for general practitioners when the patient is discharged from specialist teams.
A UK-based study has shown that a “one stop” nurse-led bone health clinic within the breast care service can be a cost-effective way of ensuring adherence to guidelines20. Patients to be started on an AI are identified by the multidisciplinary team (MDT). They are referred to the clinic which arranges a baseline DEXA and other appropriate investigations. Such a clinic may be a consideration in institutions where resources allow. Studies have also shown that simple interventions such as presentations at MDT meetings and display of posters to increase awareness of guidelines amongst clinicians have led to significant improvement in compliance16,17.
Lack of patient awareness of the negative effects of AIs has also been highlighted in the literature21. Improving patient education can improve patients’ compliance with treatment and decrease the rates of unattended appointments for BMD screening. It can also give more control to patients over management of their bone health, as they may be able to discuss with their clinicians where they notice a gap (e.g. if they have failed to receive an appointment for a DEXA scan). Ligibel et al have noted that women from areas with lower levels of education are less likely to undergo BMD tests15.Patient education can also help reduce the impact that such health-seeking behaviours have on compliance to bone health management.
Current guidelines make no mention of bone health management in male BC patients on hormonal therapy. Although they constitute a small percentage of BC patients, it would be reasonable to include recommendations of their bone loss management in updated guidelines so that this aspect of their care is not neglected.
Strengths and limitations
Our audit is limited by its small sample size and its retrospective nature which meant that we relied on documentation of variable accuracy. We had no information regarding patients who failed to attend appointments despite their clinicians’ invitations for DEXA scans or biochemistry tests, and no information on compliance to medication. However, the results from recent conference abstracts on UK based studies22,23 generated from our literature review reflect our results, suggesting that this is indeed a national issue. The literature review presented is the most extensive currently available on the subject, gathering up-to-date evidence on worldwide compliance to guidelines on AIBL.
Conclusion
Although the sample size of our study does not allow us to draw conclusions purely based on our data, the literature review that it has prompted has shown that several years after issuance of various guidelines on the management of BC treatment-induced bone loss, in particular AIBL, important gaps still exist in practice. We have presented a summary of up-to-date evidence in the literature to identify potential reasons for this and possible solutions to the current problems, hoping that this will improve current practice.
However, the current guidelines are now several years old. In the last few years, there has been a lot of research on the role of bisphosphonates in BC. A consensus paper assessing recent evidence has suggested that bisphosphonates should be considered for the prevention of bone loss in patients with a T score of <-2.0 or with at least two clinical risk factors for fracture24. The paper also suggests considering the use of bisphosphonates as adjuvant BC treatment, based on a large meta-analysis including 18 766 patients which demonstrated significant benefits of bisphosphonates in terms of prevention of bone metastases and BC survival in postmenopausal women25. This may well change routine adjuvant treatment of BC in the next few years and must be taken into consideration if and when new guidelines on the management of AIBL are issued, or when writing local guidelines.
Chest pain accounts for 1% of all GP consultations, but in only 8%-18% of cases is it an indicator of underlying ischemic heart disease.1 Given the potential diagnostic uncertainty associated with chest pain at initial presentation, specialist evaluation of patients in a Rapid Access Chest Pain Clinic (RACPC) is of value and represents an important process in the evaluation of symptoms. These clinics were established with the aim of providing rapid outpatient assessment of patients with suspected cardiac disease in order to permit earlier provision of appropriate treatment and investigations where required.
Stable chest pain typically presents as angina, a triad of dull central chest pain, brought on with exertion and relieved by rest or GTN spray. The aetiology is usually stable atherosclerotic plaque disease which is associated with low mortality and can be treated with oral anti-anginals, as demonstrated by meta-analyses and the landmark COURAGE study. 2, 3
NICE Clinical Guideline 95 (NICE CG95) suggests that choice of initial investigation for stable chest pain should be guided by a patient’s pre-test probability of having CAD. Calculations of the pre-test probability take into consideration a patient’s age, gender, cardiac risk factors and symptoms. Patients are defined as high risk of cardiac disease if they have diabetes, smoke or have hyperlipidaemia (total cholesterol >6.47mmol/litre). Patients with none of the above are considered low risk. Symptoms are defined as “typical angina” if the pain is: 1) constricting discomfort in the front of the chest or in the neck, shoulders, jaw or arms; 2) is precipitated by physical exertion and 3) is relieved by rest or GTN spray within approximately five minutes. Pain is defined as “atypical angina” if only two of the above criteria are met and defined as “non-anginal” if one or none of the above criteria are met.
NICE pre-test probabilities of CAD (Table 1), are based on a version of Diamond and Forrester’s pre-test probabilities published in 1979, modified using data from Duke’s cohort study, published in 1993.4, 5, 6 Recent studies suggest that these NICE pre-test probabilities may overestimate the prevalence of CAD in a primary care population and may risk over investigating patients.7, 8 In addition to having financial implications, this may cause patients undue anxiety and unnecessarily put them at risk of complications.
Table 1: NICE Clinical Guideline 95 pre-test probabilities table. Each cell represents the percentage risk of each group of patients having CAD, based on their typicality of symptoms, gender, age and cardiac risk factors (lo, low and hi, high)4
ESC guidelines utilise an updated, validated model of the Diamond-Forrester model by Genders et al. to create pre test probabilities of CAD (Table 2), based on patient’s age, gender and typicality of symptoms. 9, 10
Table 2: ESC guidelines clinical pre-test probabilities in patients with stable chest pain symptoms Each cell represents likelihood of each group of patients having CAD, based on typicality of symptoms, age and gender.9
We hypothesised that strict adherence to NICE guidelines results in over-estimation of the pre-test probability of CAD and therefore over-investigation of patients presenting with stable chest pain. ESC guidelines may offer more accurate pre-test probabilities of CAD and allow a more targeted and cost-effective use of investigations.
Methodology
Clinic records of all patients who attended the RACPC at Tunbridge Wells Hospital between July 2005 and December 2012 were reviewed. This service is run by a cardiology specialist. Patient demographics, cardiac risk factors and information regarding the nature of patient symptoms were collected prospectively and completed at the time of the patient’s RACPC appointment. Results of cardiac investigations were collected from paper and computerised records, and included diagnoses of significant CAD made following invasive coronary angiogram. These results were compared with patients’ pre-test probabilities of CAD calculated using both NICE and the ESC’s calculation methods. Outcome and readmissions were obtained from electronic records from the Maidstone and Tunbridge Wells NHS Trust computer records retrospectively.
Results
Study population
A total of 1968 records were reviewed. 59% (n = 1162) of patients were male and 41% (n = 806) were female. Their mean age was 60 years. At initial assessment, 69.8% patients (n=1373) had non-anginal chest pain, 19.5% (n=383) had atypical angina and 10.8% (n=212) had typical angina, based on the NICE guideline definitions of chest pain.
97.2% (n= 1912) patients underwent further investigation; 15% (n=256) of these were subsequently diagnosed as having significant CAD, accounting for their symptoms. The 2.8% (n=56) of patients who did not undergo investigation either chose not to, were unable to, were lost to follow up, or were diagnosed as having a non-cardiac cause of their symptoms at the initial RACPC appointment.
NICE CG95 pre test probabilities compared against cohort data
Table 3: NICE guidelines 95 pre test probabilities compared against cohort data Each cell represents the proportion (%) of cohort patients from each group who were diagnosed with CAD. We have colour-coded cells to represent the NICE estimated pre-test probability of CAD in each group. Red cells represent 61-90+% probability, pink cells represents 30-60% probability, blue cells represent 10-29% probability and white cells represents <10% probability of CAD according to NICE Guidelines. “ – “ marks a cell where pre-test probabilities of CAD could not be calculated for cohort patients.
Table 4: A comparison of NICE pre-test probabilities and cohort patient data. The risk of CAD as predicted by NICE guidelines 95 on the left compared with the actual number of cohort patients in each category and the proportion of those patients diagnosed with significant CAD.
The average discrepancy between the pre-test probability and actual incidence of CAD in cohort patients was 28% (range 20% - 88%). In 48% of cells in the NICE CG95 pre-test probability table (Table 1) the pre-test probability of CAD was overestimated by 30% or more (Table 3). A marked discrepancy between pre-test probability and actual incidence of CAD was found between “high risk” and “very low risk” patients. On average, high risk patients had an overestimated pre-test probability of 34.3 – 40.9% per cell compared with low risk patients whose pre-test probability was only overestimated by 6.5% (Table 3).
The cells highlighted in dark red in table 3 represent high risk patients whose pre-test probability was of 61-90+%, according to NICE CG95. In our cohort, only 31.2% (n=214, 95% CI 27.6-34.5) of high risk patients in this category were diagnosed with CAD. On average, actual incidence of CAD compared with pre-test probability was overestimated by 34.4% – 40.9% in each cell.
The pink cells in table 3 represent medium risk patients with a pre-test probability of CAD of 30-60%, according to NICE CG95. In our cohort, only 4.4% (n=24, 95% CI 3.0 – 6.5) of medium risk patients had a positive angiogram (Table 4). The average overestimate of actual incidence against pre-test probability was 35.9%.
The cells highlighted in blue in table 3 represent low risk patients with a pre-test probability of CAD of 10-29%, according to NICE CG95. In our cohort, only 2.5% (n=7, 95% CI 1.2 – 5.0) of low risk patients were diagnosed with CAD (Table 4). On average, the pre-test probability of CAD exceeded the found incidence of CAD by 18.6% (Table 3).
The white cells in table 3 represent very low risk patients with pre-test probability of CAD <10% according to NICE CG95. In our cohort, only 0.28% (n= 1, 95% CI 0.1 – 1.6) of patients were diagnosed with CAD. Average overestimation in this group was 6.5% in each cell.
ESC guidelines pre test probabilities compared against cohort data
Table 5: A comparison of ESC pre-test probabilities with cohort patient data. Each cell shows the proportion (%) of cohort patients from each group diagnosed with CAD. Each cell is colour coded to correspond with the ESC estimated pre-test probability. Dark red cells represent >85% probability, pale pink cells represent 66-85% probability, pale blue cells represent 15-65% probability and white cells represent <15% probability.
Table 6: A comparison of ESC pre-test probabilities and cohort patient data The risk of CAD as predicted by ESC guidelines on the left compared with the actual number of cohort patients in each category and the proportion of those patients diagnosed with significant CAD.
The average discrepancy between pre-test probability of CAD, according to the ESC’s risk stratification table, and actual incidence of CAD in cohort patients was 20.7%. In 28% of cells, the pre-test probability of CAD exceeded the found incidence of CAD by 30% or more (Table 5).
The cells highlighted in dark red in table 5 represent very high risk patients with a pre-test probability of CAD greater than 85%, according to ESC guidelines (Table 5). 73.4% (n= 58, 95% CI 63.7 – 82.7) of cohort patients in this high-risk category were diagnosed with CAD (Table 6). On average, incidence of CAD in each cell has been overestimated by 13% in this category.
The cells highlighted in pale pink in table 5 represent high risk patients, with a pre-test probability of CAD of 66-85%, according to ESC guidelines. 58.5% (n=103, 95% CI 51.1 – 65.5) of cohort patients in this high-medium risk category were diagnosed with CAD (Table 6). On average, the pre-test probability of CAD exceeded the found incidence of CAD in each cell by 17.7% (Table 5).
The cells highlighted in pale blue in table 5 represent medium risk patients with a pre-test probability of CAD of 15-65%, according to ESC guidelines. 6.4% (n=93, CI 5.3 –7.8) of cohort patients in this risk category were diagnosed with CAD (Table 6). On average, the pre-test probability of CAD exceeded the found incidence of CAD by 24.1%in each cell (Table 5).
The cells highlighted in white in table 5 represent patients whose pre-test probability of CAD was less than 15% according to ESC guidelines. Only 0.76% (n=2, 95% CI 0.2 –2.7) of cohort patients in this risk category were diagnosed with CAD (Table 6). On average, pre-test probability of CAD exceeded found incidence of CAD in each cell by 6.2% (Table 5).
Discussion
Only 15% of a total of 1968 patients referred to RACPC were diagnosed with significant CAD. The majority (70%) of referred patients had “non-anginal” chest pain and low pre-test probabilities of CAD, reflecting the importance ascribed by General Practitioners of ruling out ischemic heart disease as the underlying cause for chest pain, even in low risk patients. This may not be surprising given the large media attention to heart disease and sustained campaigns for early warning signs of heart attack in the British media. It is therefore of great public interest for cardiac disease to be identified.
NICE CG95 pre test probabilities compared against cohort data
Comparing cohort data to the pre-test probabilities of CAD outlined in NICE CG95, NICE have overestimated the number of patients likely to have CAD in the majority of groups. Strict adherence to NICE CG95 therefore carries the risk of over-investigating patients. NICE recommend CT calcium scoring as the first line investigation for patients with a low (10-29%) pre-test probability of CAD. 284 patients fall into this category and only 7 patients were shown to have CAD. This means that 40.5 patients need to be treated in order to identify 1 positive patient (NNT= 40.5).
In patients with a medium (30-60%) pre-test probability of CAD, NICE recommends functional imaging as the first line diagnostic investigation. In our cohort 544 patients would undergo functional imaging, but only 24 of these patients would be diagnosed with CAD, NNT=22.7.
Finally, in patient groups with a high (61-90%) pre-test probability of CAD, NICE recommends invasive coronary angiography as the first line diagnostic investigation. In our cohort of 1968 patients, 691 patients had a high pre-test probability of CAD, and 214 had significant coronary artery disease on angiography, NNT= 3.2.
Although invasive coronary angiography is considered the gold standard investigation for diagnosing CAD, and permits simultaneous therapeutic intervention, the procedure is not without risk, particularly in elderly patients and those with renal impairment.11 Furthermore, invasive angiography is expensive and is costed by the East Kent Hospitals University NHS Foundation Trust at £1166.02 per procedure (private correspondence).
NICE CG95 offers no guidance on managing patients who have a <10% pre-test probability of CAD. 347 of our cohort patients fell into this very low risk category and only 1 was diagnosed with CAD. Therefore, NICE CG95, if strictly adhered to, would have missed one diagnosis of CAD in our patient cohort.
ESC pre test probabilities compared against cohort data
ESC guidelines tend to offer more conservative estimates of pre-test probability of CAD compared with NICE guidelines. Using the ESC’s risk stratification table, almost all patients, except those with over 85% pre-test probability and those with less than 15% pre test probability, would be investigated for chest pain. This is due to their claim that non-invasive, image-based diagnostic methods for CAD have typical sensitivities and specificities of around 85%, so that roughly 15% of these investigations could be yielding false results. Hence, due to these inaccuracies, in patients with pre-test probabilities of CAD below 15% or above 85%, ESC state that performing no test at all could provide fewer incorrect diagnoses.9
In our patient cohort, 79 patients had very high (>85%) pre-test probability of CAD, but only 58 patients (73%) were diagnosed with CAD. For this patient risk group, ESC guidelines suggest that further investigation may not be necessary and that a diagnosis of CAD may be assumed. Thus, applying ESC guidelines to our cohort could result in 21 patients being incorrectly diagnosed with stable angina, and more serious causes of chest pain, for example pulmonary emboli or gastric ulceration, may be missed. However, in practice, it is likely that many patients in this very high pre-test probability category would have undergone angiography, because patients who have "severe symptoms" or who are clinically thought to have "high risk coronary anatomy" should be offered an invasive angiography with or without pressure wire studies. The vagueness of the guidelines allows interventionists to interpret this in the clinical context.
In ESC guidelines, invasive coronary angiography is not specifically recommended as a first line investigation for stable angina, regardless of the pre-test probability of CAD. In patients with a high (66-85%) pre-test probability of CAD, ESC guidelines recommend non-invasive functional imaging first line. Of the 176 patients who fell into this category, only 102 (58.0%) patients were ultimately diagnosed with CAD.
In patients with medium (15-65%) pre-test probability of CAD, ESC guidelines advise exercise ECG testing (or non-invasive imaging for ischemia if local expertise is available) as first line diagnostic investigations. Of the 1451 patients which fell into this category, only 93 were diagnosed with CAD, NNT= 15.6. Fortunately, exercise ECG testing would not expose the patient to potentially harmful radiation or medication, but their poor diagnostic power may result in the need for further investigations, despite a negative result.
In patients with low risk of CAD (<15%) ESC guidelines suggest making an assumption that the patient does not have CAD and advocates conducting no further investigations. In our cohort, 263 patients fell into this low risk category, two (0.8%) of which were diagnosed with CAD.
The ESC guidelines appear to have higher specificity than the NICE guidelines, and only two patients would have been missed had ESC guidelines been adhered to, compared to one patient missed if NICE guidance was used. Thus, although highly sensitive, ESC guidelines when applied to our cohort have lower sensitivity than NICE guidelines.
Comparison of number of investigations
Following ESC guidance for our cohort of patients would have resulted in fewer diagnostic invasive angiograms being performed than if NICE guidance had been followed. ESC guidance only recommends invasive angiography if first line, non-invasive investigations generate positive results. Overall, however, ESC guidance would result in a greater number of overall investigations being performed.
In total, NICE advises that all 691 of our high risk cohort patients should undergo invasive angiography as a first line investigation. 544 with medium risk should undergo functional testing first and 24 of these patients (assuming an angiogram would follow a positive result) would go on to have invasive angiography. 284 low risk patients should undergo CT calcium scoring first, of which 7 would go on to have functional imaging and angiography if the above logic is followed. This generates a total of 1557 investigations; 722 angiograms, 551 functional imaging investigations and 284 cardiac CT scans.
In comparison, using ESC guidance, 176 of our high risk patients would have functional imaging investigations, 103 patients with positive results would then undergo invasive angiography. 1451 patients would receive exercise ECGs, of which 93 with positive results would undergo functional imaging and invasive angiography. This generates a total of 1916 investigations; 196 angiograms, 269 functional imaging investigations and 1451 exercise ECGs.
If we assume that stress echocardiograms are used as “functional imaging” we can estimate costs for our cohort when applying each set of guidelines. Costs for each investigation are supplied by East Kent Hospitals University NHS Foundation Trust and are as follows: Outpatient elective coronary angiograms are costed at £1,166.02; stress echocardiograms are costed at £132.30; exercise ECGs at £40.26 and CTs of one area at £102.47 (private correspondence). If we were to apply NICE guidelines to our cohort, £841,866.44 would be spent on angiograms, £72,897.30 would be spent on stress echocardiograms and £29,101.48 on CT scans. This is a total of £943,865.22 on investigations.
If we were to apply ESC guidelines to our cohort, £228,539.92 would be spent on coronary angiograms, £35,588.7 would be spent on stress echocardiography and £58,417.26 would be spent on exercise ECGs. A total of £322,545.88 would be spent on investigations. Overall, this is £621,319.34 cheaper than applying NICE guidelines.
Limitations of study
This study is based on data from a single site and may not be nationally representative. The final diagnosis was made clinically by an experienced interventional cardiologist, which introduces subjectivity and the risk of interpreter bias. Not all patients underwent the gold standard of invasive coronary angiography to demonstrate the presence of CAD. However, all patients were seen and fully assessed by a cardiologist and 97% underwent investigations if deemed necessary.This study has all the limitations of a registry study. In addition, costs for investigations may vary throughout the country, and indeed the world, with varying expertise available.
Conclusion
In conclusion, strict adherence to NICE CG95 over-estimates the pre-test probability of CAD in our local population group. This is consistent with previous studies conducted in South London where there is a larger Afro-Caribbean population, as well as with studies conducted in the North of England.8,9 Adherence to ESC guidelines in place of NICE guidelines may enable a more targeted and cost-effective use of investigations. Strict application of the ESC guidelines to the study cohort would have resulted in investigations costing an estimated £322,545.88, compared to £943,865.22 if NICE guidelines were applied. However, conducting fewer investigations carries greater risk of misdiagnosis, and using ESC guidelines in isolation introduces the possibility of assuming CAD in patients without conducting investigations to confirm this.
It is advisable that local cardiology departments audit their stable chest pain guidelines to ensure that the interpretation of pre-test probabilities is in keeping with the local population. Unfortunately there is no ideal policy and local protocols should reflect the local population.
One in four adults are affected by musculoskeletal (MSK) problems, which account for up to 30% of General Practice (GP) consultations in the United Kingdom..1 Some GPs have direct access to community MSK services, but when not available, referrals are made to secondary care departments such as rheumatology. MSK training involves the skills that a rheumatologist needs to achieve competencies in the diagnosis and treatment of soft tissue rheumatism as opposed to inflammatory rheumatic joint disease.
It has been reported that junior doctors in the United Kingdom fail to routinely screen for MSK conditions on admission onto general medical or surgical wards2 which may be reflective of training issues. It was in our anecdotal opinion that MSK training at higher specialist training was being compromised as well. Within the United Kingdom doctors in training typically begin work as a first year rheumatology trainee four years after graduation from medical school following completion of both a two year foundation programme (encompassing a generic training programme which forms the bridge between medical school and specialist/general practice training) and a two year Core Medical Training programme, (involving 2 years of training, undertaking between four and six rotations in different medical specialties). At the time of writing, higher specialty training, such as in rheumatology, began at the level of Specialist Trainee 3 (ST3) and was either a four year training programme or a 5 year training programme if trainees were dually accrediting in general medicine.3 Higher specialist training involves rotating through different rheumatology departments within each Local Education Training Board (LETB).
In our opinion, the basic MSK skill set is essential to the training of a competent rheumatologist and trainees gain overall MSK competencies within routine clinical practice as they rotate through different hospitals during training. However, in some training programmes, there is very little MSK training opportunities, as MSK centres operating in the community in the United Kingdom, mean that these patient groups are not being treated in training hospitals. Faculty in these centres are competent to train, but training opportunities in MSK centres are reduced.
Rheumatology registrars in-training have expressed the anecdotal view that MSK training may be compromised, partly due to the reduction of referrals to secondary care and partly due to the inevitable focus on training in the more complex inflammatory conditions.
Rheumatology trainees in the UK were surveyed in 2015 on behalf of the Rheumatology Specialist Advisory Committee to assess confidence and ability in dealing with MSK conditions during and on recent completion of training. The survey was disseminated to rheumatology trainees via the trainee representative from each LETB.
77 responses were received across 15 LETBs from a total of an estimated 223 trainees. 20 of these surveys were incomplete, with not all questions being answered but those questions answered were considered in the results of this survey. Responses from trainees across all career grades from ST3 (1st year of specialist training) to 2 years post Certificate of Completion of Training were received.
58 out of 63 doctors (92%) thought MSK medicine to be an important part of rheumatology training. Free text comments recognised that MSK conditions were frequently referred to rheumatology and differentiating between inflammatory and non-inflammatory pain is important.
Only 41 out of 64 doctors (64%) felt they managed patients with soft tissue pathology on a daily basis and 20 out of 63 (32%), felt they were not yet confident in diagnosing and distinguishing between different types of soft tissue pathologies.
Exposure to, and experience with MSK medicine in current jobs and throughout training ranged from poor to excellent.
Only 9 out of 58 trainees (16%) felt they were lacking in competency for their level of training in managing the MSK pathologies outlined in the Joint Royal Colleges of Physicians Training Board (JRCPTB) 2010 rheumatology curriculum. The majority of trainees felt they were either partially competent in all, or some areas, satisfactory for their level of training.
Interestingly, only 39 out of 58 trainees (67%) felt their training in injection techniques had been at least ‘adequate’. Some trainees mentioned they had been self-taught in some injection procedures and training had been limited in certain soft tissue injections (most commonly plantar fasciitis, tendon sheath and elbow enthesis injections).
This survey has limitations in that the numbers of trainees surveyed were small. However, our total response number considering the usual poor response rate for online surveys is reasonable. Our survey was not validated and it is likely that there will be an element of selection bias in the responses received.
However, one of the strengths of our survey is the ability to review responses by seniority. We analysed further the confidence rating according to training level grade and we looked into two main subgroups, the more junior trainees (ST3 and ST4s) and the more senior trainees (ST6 and ST7). As expected the more junior cohort rated their confidence slightly lower compared to the more experienced group. Within the junior group (n=17) only 41% suggested they felt confident for their level of training when generically asked about their general diagnostic skills on MSK, which improved to 59% when this question was mapped to the curriculum. In the senior group of ST6 and ST7 (n=25), the confidence levels were significantly higher (80% felt confident appropriate to their level of training) and there was no change in confidence levels when skills were mapped to the curriculum. (Table 1). This may reflect the natural increase in experience and exposure to MSK medicine with progression in training, but also the better understanding of the curriculum requirements by the more senior trainees.Only one fully completed survey was received from a rheumatologist post Certificate of Completion of Training making this subgroup too small for further analysis.
Table 1:
(n)
Q6) Confidence in dealing with MSK
% Q6
Q9) Confidence mapped to curriculum
% Q9
ST3 and ST4- junior
17
7
0.41
10
0.59
ST6 and ST7- senior
25
20
0.8
20
0.8
Q6) How confident do you feel in diagnosing and distinguishing between different types of soft tissue pathologies/MSK in your daily practice? Q9) Do you feel competent in diagnosing and managing the above MSK pathologies outlined in the 2010 rheumatology curriculum?
Within this limited survey, the views of 77 trainees have shown that training in MSK could be improved for rheumatologists in training at all levels. Although trainees felt they were lacking confidence in dealing with certain areas of MSK medicine, when competencies were mapped out to the rheumatology curriculum, trainees felt they were achieving appropriate competency for their level of training although this was not assessed objectively.
The trainees’ perception of the level of competency needed in dealing with MSK conditions seemed to overestimate the requirement of the 2010 rheumatology curriculum. In clinical practice, trainees may feel they encounter different MSK pathologies, which they are being expected to manage which are not being given sufficient emphasis within their curriculum. Further questioning in this area may conceivably lead to adjustments within the curriculum and the training programmes.
In particular, to improve training in MSK medicine, rheumatology trainees valued teaching from physiotherapists and being able to attend specialist sports medicine clinics. Trainees who had ‘independently’ taken time to gain experience in this way felt that their training had benefitted. To support trainees in achieving these competencies it may be worthwhile adding a prerequisite in the Annual Review of Career Progression (ARCP) process (a formal method in UK medical training by which a trainee’s progression through their training programme is monitored and recorded) to ensure dedicated time is set aside for this aspect of MSK rheumatology training. Completion in a range of direct assessments such as Clinical Evaluation Exercises (miniCEX), and DOPs (Directly Observed Procedures) may ensure competency in this aspect of rheumatology training as well as secure confidence in dealing with MSK conditions and soft tissue pathology.
With changes in the nature and geography of rheumatology specialist services we feel these aspects of rheumatology training should not be overlooked so trainees are equipped to deal with MSK conditions independently by their completion of training.
An audit and re-audit on the monitoring of the physical health of patients on antipsychotic medication in the Early Intervention in Psychosis Service of the 5 Boroughs Partnership NHS Foundation Trust
Introduction
A growing number of studies suggest a causal relationship between antipsychotic treatment and metabolic disturbances. The most frequent problems linked to antipsychotic drugs have been abnormalities of glucose metabolism such as insulin resistance, hyperglycaemia or new onset diabetes mellitus and dyslipidemia, including increased levels of total cholesterol, LDL-cholesterol and triglycerides.1
Developing effective models of identifying and managing physical ill health among mental health service users has increasingly become a concern for psychiatric service providers. Individuals with Serious Mental Illness (SMI) defined as any Diagnostic and Statistical Manual (DSM) mental disorder leading to substantial functional impairment, have higher than expected risks of physical morbidity and mortality in comparison with members of the general population.2 People with mental health problems such as Schizophrenia or Bipolar Disorder have been shown to die on average 16 to 25 years sooner than the general population.3 One set of explanations for these vulnerabilities points to the lifestyles of people with serious mental illnesses, which are often associated with poor dietary habits, obesity, high rates of smoking, and the use of alcohol and street drugs.4 Illness related factors have also been cited. It has been suggested that individuals with serious mental illness are less likely to spontaneously report physical symptoms.5 Poor physical activity has also been shown to be a common occurrence in people with serious mental illness.6, 7
A greater inherent predisposition to develop metabolic abnormalities coupled with metabolic adverse effects of antipsychotic drug treatments may negatively influence physical health.8 Many of these problems can be avoided if close attention is paid to the physical health of patients on antipsychotic treatment. A longstanding debate persists concerning who is responsible for the physical care of patients with serious mental illness. Psychiatrists and physicians are advised to play an active role in ensuring that patients with mental illness are not disadvantaged.9
The Warrington and Halton Early Intervention in Psychosis Team is based in the 5 Boroughs Partnership (5BP) NHS Foundation Trust in the North West region of the United Kingdom, and in collaboration with Advancing Quality Alliance (AQuA), they embarked on a joint audit between November 2012 and May 2013 with the aim of reviewing the practice regarding the routine monitoring of physical health of service users on antipsychotic treatment. The study set out to reduce the cardio-metabolic effect of antipsychotic medication in service users. The study was also aimed at contributing to a reduction in the mortality rates in people with severe mental illness as well as testing out approaches to improve the physical health of people with serious mental illness who are receiving care from the Early Intervention in Psychosis Teams. The promotion of a more integrated approach to the physical health care of people with a SMI was also targeted.
Method
In November 2012, the Warrington and Halton Early Intervention in Psychosis service (EIP) conducted the initial audit, designed by AQuA as a baseline measure of the current standard of physical health screening amongst the Early Intervention patients in the two boroughs. The recommendations from the National Institute for Health and Care Excellence (NICE) and Maudsley prescribing guidelines were the frameworks for the AQuA design. The Research and Audit Governance Group in the 5 Boroughs Partnership NHS Foundation Trust approved the audit.
A retrospective review of the clinical records of all patients opens to the EIP, who were prescribed antipsychotics, was undertaken. Six physical health parameters were examined and these include; serum lipid profile and blood glucose levels. Others measures were body weight, height, Body Mass Index (BMI) and blood pressure. These parameters were entered into the survey monkey audit tool developed by AQuA.
Other items audited were the frequency of screening, the number of physical health parameters evaluated at each period of recording and the smoking status of the service users. Clinical records were checked for documented history of physical illness in all patients. The number of service users receiving physical health interventions as a result of the screening and the number of service users who were offered physical health interventions at the screening but either refused treatment or did not respond to the referral was also recorded. The results were presented at a Trust-wide forum and recommendations were made, and disseminated shortly afterwards. A re-audit was done in May 2013.
Results
Table 1, summarises the demographic details of patients at baseline and re-audit. 55 patients were involved in the baseline audit and 52 patients were involved in the re-audit. No significant differences were observed in both audits in terms of gender distribution and age. Majority of the patients involved in both audits were of white British ethnicity.
Table 1: Demographic details of patients at baseline audit and re-audit
Nov 2012
May 2013
Total number of patients
Male : female
35:20
22:30
Age
14-36
15-36
White British Ethnicity
52
48
Baseline audit: November 2012
Screening and monitoring
The table below indicates the number of service users receiving a screening for weight, height, BMI, glucose blood levels, lipid blood levels and blood pressure at the 4 week, 3 month, 12 month and 24 month assessments.
Table 2: Physical health screening of service users at baseline
4 weeks recorded screening
3 months recorded screening
12 months recorded screening
24 months recorded screening
1 type of screening
5 (9.1%)
12 (21.8%)
18 (32.7%)
18 (32.7%)
2 types of screening
14 (25.5%)
17 (30.9%)
5 (9.1%)
5 (9.1%)
3 types of screening
4 (7.3%)
4 (7.3%)
3 (5.5%)
6 (10.9%)
4 types of screening
5 (9.1%)
3 (5.5%)
5 (9.1%)
3 (5.5%)
5 types of screening
4 (7.3%)
0
1 (1.8%)
4 (7.3%)
6 types of screening
4 (7.3%)
3 (5.5%)
4 (7.3%)
2 (3.6)
There was no screening recorded for 19 (34.5%) patients at 4 weeks, 16 (29%) patients at 3 months, 19 (34.5%) patients at 12 months and 17 (30.9%) patients at 24 months.
Smoking status of service users
Based on the analysis of those referred to the smoking cessation service, it was concluded that around 35% of service users within the EIP Service smoke. The findings from this data also indicate high refusal rates to smoking cessation programmes (at over 80% of those service users who confirmed that they smoke).
Documented history of physical illness
The presence or absence of physical illness was documented in the records of 35 patients. Where physical health problems were identified, patients were offered a number of interventions. These include referral to the dietician/exercise programmes, smoking cessation and referral to primary care services for illnesses such as, hypertension, diabetes and hyperlipidemia.
Table 3, summarises the types of interventions available for patients when physical health issues were identified. A number of patients (N/A) required no interventions, as physical problems were not identified.
Number of service users receiving physical health interventions
Table 3: Physical health interventions
Yes
No
N/A
Referral to dietician/exercise programme
15 (28.8%)
26 (50%)
14 (25.5%)
Treatment for Diabetes
0
22 (45.8%)
33 (60%)
Treatment for
Hyperlipidemia
2 (4.2%)
23 (47.9%)
30 (54.5%)
Treatment for
Hypertension
0
22 (45.8%)
33 (60%)
Help with smoking
cessation
12 (24.5%)
19 (38.8%)
24 (43.6%)
Re-audit: May 2013
Screening and monitoring
The table below indicates the number of service users receiving a screening for weight, height, BMI, glucose blood levels, lipid blood levels and blood pressure at the 4 week, 3 month, 12 month and 24 month assessments. The table shows that 29 patients had their screening recorded at 4 weeks, 19 (66%) of which had 6 types of screening. At 24 months, out of the 16 patients who had their screening recorded, 15 (95%) had 6 types of screening. Patients with no screening parameters were omitted.
Table 4: Physical health screening of service users at re-audit
4 weeks recorded
screening
3 months recorded screening
12 months recorded screening
24 months recorded screening
1 type of screening
2 (7%)
0
0
0
2 types of screening
2 (7%)
2 (8%)
1 (4%)
1 (5%)
3 types of screening
1 (3%)
1 (4%)
3 (11%)
0
4 types of screening
3 (10%)
3 (12%)
1 (4%)
0
5 types of screening
2 (7%)
1 (4%)
1 (4%)
0
6 types of screening
19 (66%)
18 (72%)
21 (77%)
15 (95%)
Smoking status of service users
The overall data confirms that 25 patients, who were identified as smokers, were offered smoking cessation, 19 of which refused, thus giving an overall refusal rate of 76%
The table below compares the results of both audits with respect to “6 types of screening” done at 4 weeks, 3 months, 12 months and 24 months. The result shows an overall improvement over the audit period.
Comparing results of both audits with respect to “6 types of screening”
Table 5: Comparison of screening results
November 2012
May 2013
4 weeks
4 (7.4%)
19 (66%)
3 months
3 (5.5%)
18 (72%)
12 months
4 (7.4%)
21 (77%)
24 months
2 (3.7%)
15 (95%)
Discussion
The first audit revealed a suboptimal screening of the 6 targeted parameters at 4 weeks, 3 months, 12 months and 24 months in the service users audited when compared to the recommendations of the Maudsley guidelines (See Table 3). Some of the issues identified are summarised in the table below;
Table 6: Issues identified following the first audit
Sporadic health and wellbeing sessions
Ad-hoc physical health checks prior to commencing antipsychotics
Physical health screening was not perceived as priority
Physical screening were unsystematic and erratic
Poor referral links with local health promotion programmes
Poor attendance to physical health screening appointments
Poor recording of screening tests
Inadequate links with primary care services
Psychiatric clinics poorly equipped with instruments for basic health screening
No clarity about who takes responsibility for screening: Psychiatrists or GP?
Patients’ lack of interest and motivation in the screening process
SMI register not up-to-date
Recommendations made following the initial audit are outlined in the table below;
Table 7: Recommendations following the first audit
Need to finda comprehensive screening tool
Development of a documentation system
Building an alert system to remind when physical health checks are due
Improvement of links with primary care services
A more robust approach to ensure patient’s attendance at screening clinics
Improvement of links within secondary care agencies
Identification of further skills needed within the team e.g. venipuncture, ECG
A Plan, Do, Study, Act (PDSA) model was used which was useful in clarifying issues and actions needed.10 It helped us to identify issues and actions needed including:
1. Establishing physical health as a priority within the EIP
2. Involvement of primary care and health promotion
3. Establishing a database for physical health monitoring
4. Making physical health monitoring part of care planning
To tackle the identified issues a local project group was constituted. This group was made up of a consultant psychiatrist, business manager, nurse consultant, team manager, an occupational therapist (OT), a support worker (STR), a pharmacist, social services, public health leads, wellbeing nurses, a service user representative, and a locally based General Practitioner. The group had monthly meetings.
Patients in the Warrington and Halton Early Intervention in Psychosis Service were screened using the 5 Boroughs Partnership (5BP) Comprehensive Physical Health Assessment tool. This tool covered the 6 parameters targeted in the audit and other relevant health information such as, smoking, diet, exercise, sexual health, sleep, dental and optical health, ECGs, and other routine bloods checks. An in-house database in which results could be recorded was devised and implemented. A notification list which alerted on computer when a screening is due was developed; a GP DVD and information leaflet for the GP website and the Clinical Commissioning Group (CCG) Newsletter were produced. Wellbeing Nurse-led clinics were held in Halton and a STR-led physical health clinic was initiated in Warrington. Access into the path labs for both localities was established to help facilitate prompt access to blood results. Regular AQuA meetings took place in Salford, Manchester, and links were established with the Medical Director and the Clinical Commissioning Group, who were regularly, provided progress reports.
The re-audit in May 2013 showed an increase in the number of service users being screened and monitoring for the six identified parameters (see Table 8).A robust and comprehensive recording system has been developed, resulting in more service users receiving appropriate screening and physical health monitoring. Better links and working relationships have been established with primary care services and there is increased awareness of the need for physical health monitoring in professionals and service users. Regular and well-equipped physical health clinics with well-trained staff have been established across both localities. Other secondary care agencies within the Trust are now more aware of the requirements for physical health screenings.
Why should we be doing regular physical health monitoring? The benefits of monitoring the physical health of individuals with serious mental illness cannot be overemphasised; it allows early identification and subsequent management of cardiovascular and other risk factors in a timely manner.11 The Maudsley Guidelines recommend monitoring of blood lipids at baseline, at 3 months and yearly. Similar recommendations are made for the weight, which includes BMI and waist size when possible. Plasma glucose measurements are recommended at baseline, at 4 to 6 months and yearly. Blood pressure measurements are recommended at baseline and frequently during dose titration. Full blood count and electrolyte measurements are recommended at baseline and yearly.12 In the last few years, agencies worldwide have also developed clinical guidelines. In the United States, the American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologist and the North American Association for the Study of Obesity have released joint guidelines.13
Even though the side effects of antipsychotics are well established, many mental health services today have yet to adopt a practice of regular blood monitoring as recommended by international guidelines.14 The issue of responsibility for monitoring metabolic abnormalities remains a much debated topic today.9 The primary responsibility for managing the physical health of individuals with severe mental illness has been said to lie with primary care.7 Another side of the debate, however, exists, and two consensus conferences have called on mental health care providers to take responsibility for the physical health of their patients.8 It is widely recognized that mental health teams have a role to play in the monitoring of the physical health of their service users; however, many psychiatrists still consider psychiatric symptom control as their primary responsibility.14 15 Studies have also shown that Individuals with Serious Mental Illness do not readily access primary care.16 Despite the availability of Clinical Guidelines, screening for and monitoring of metabolic problems in patients with serious mental illness remains suboptimal.11
The usual practice in most centers for monitoring physical health parameters and guidelines used vary and are rarely regulated. Local resource availability is likely to play a significant role in guideline selection. Physical equipment, staffing levels and other resource issues may need to be taken into consideration prior to devising a local guideline. Development of a specialised phlebotomy service, for example, to the outpatient clinics will be a welcome addition, introduction of a key worker system as seen in the Warrington and Halton Early Intervention in Psychosis Team and consideration of the physical health needs of patients as part of the key worker’s duties, a simple one-page monitoring prompt attached to the patient’s medical file, educational intervention and oversight by the senior clinicians may all increase the adherence to routine blood testing guidelines. Regular liaison with General Practitioners regarding a joint approach to physical health monitoring would also help improve adherence to the guidelines.
A 38 year male presented to our centre with a two-month history of jaundice. Past medical & family history was insignificant. Clinical examination revealed a icterus and greenish brown ring in both eyes (Figure 1). Laboratory investigations revealed a mild thrombocytopenia (platelet count-1.2 lakh/mm3) and a prolonged prothrombin time. Liver function tests showed elevated serum levels of alanine aminotransferase & aspartate aminotransferase. Serology for hepatotropic viruses was negative. Serum ceruloplasmin was 9.8 mg/dl (reference range 20-60mg/dl) and 24 hour urinary copper was elevated.
Figure 1
What is the eye finding?
Arcus Senilis
Pterygium
Kayser Fleischer ring
Phlycten
Correct Answer:
3. Kayser Fleischer ring
Discussion:
Wilson’s disease is a consequence of defective biliary excretion of copper. This leads to its accumulation in the liver and brain 1. It is due to mutations of the ATP7B gene on chromosome 13, which codes for a membrane-bound copper transporting ATPase 2.
Kayser-Fleischer ring is an outcome of abnormal copper deposition in the membrane in the limbus of cornea. Slit-lamp examination by an experienced observer is required to identify a K-F ring. The colour may range from greenish gold to brown. When well developed, a K-F ring may be readily visible to the naked eye. K-F ring is observed in most individuals with symptomatic Wilson disease and are almost invariably present in those with neurologic manifestations. They are not entirely specific for Wilson’s disease, since they may also be found in patients with chronic cholestatic diseases.
Clinical presentation is variable and patients presenting with chronic hepatitis, cirrhosis & at times acute liver cell failure. The most common presenting neurologic feature is asymmetric tremor. The characteristic tremor is coarse, irregular proximal tremulousness with a “wing beating” appearance.
Typically, the combination of K-F rings and a low serum ceruloplasmin (<0.1 g/L) level is sufficient to establish a diagnosis of Wilson’s disease 3.However delayed diagnosis in patients with neuropsychiatric presentations is frequent and was in one case as long as 12 years 4.Our patient was treated with a none copper diet, oral zinc and d pencillamine. His liver functions became normal over 6 months of treatment and without progression of liver disease.
Arcus Senilis is a grey band of apacity near the sclero-corneal margin, commonly found in the elderly and associated with hypercholesterolemia. Pterygium is a benign wedge shaped fibrovascular growth of conjunctiva that extends onto the cornea. Phylecten is consequence of allergic response of the conjunctive & corneal epithelium usually associated with tuberculosis, staphylococcus protein and moraxella.
Suicide and deliberate self-harm (DSH) have been recognised as major public health problems in India for some time, but there are significant obstructions to effective intervention including difficulties in following Western models to understand these behaviours.1, 2, 3
The World Health Organisation (WHO) recognises suicide as one of the three leading causes of death in young adults globally.4 The greatest burden of suicide is now in low- and middle-income countries like India where annual suicide rates are 10-11 per 100,000.5, 6, 7 India is second only to China in the absolute number of annual deaths by suicide.5 The number of individuals who die by suicide each year in India alone is more than the total number of suicides in the four top ranked European countries combined.3, 5, 8
DSH, defined as intentional self-poisoning or self-injury, is a closely related public health problem.9WHO estimates that for every suicide there are at least 10-20 DSH acts.10 If this estimated proportion, based on Western research, is also true in India then there are 1-2 million DSH acts in India each year.
Official data for 2005 suggest that 19.6% (n=22,327) of India's 113,914 officially recorded suicides were self-poisonings with pesticides7 (predominately organophosphates, which are freely available and widely used in agriculture). The official suicide rate for India, 10.3 per 100,000 in 2005,7 is thought to be an under-estimate.3, 11 Studies from several regions suggest that India's suicide rates may be as high as 40 per 100,000 and that 30% or more of these deaths are due to pesticide self-poisoning.11 The studies reporting the highest suicide rates within India are from Tamil Nadu (>60 per 100,000 – three times higher than the official figure for the state).12, 13, 14, 15 Whilst some of the discrepancies between official statistics and findings in local studies may be due to urban-rural differences in the incidence of suicide, data collated by the Indian police suggest that around 90% of suicides in India occur in non-urban areas.7, 11, 15 Extrapolating from these figures, it is conservatively estimated that there may be up to 420,000 suicides per annum in India (126,000 from pesticide self-poisoning).
India's centrally collated self-harm and suicide data are unreliable owing to a number of factors. Death registration processes are below Western standards. Only about 25% of deaths are registered and only about 10% are medically certified.16, 17 Attempted suicide is a crime in India.18 Survivors are interviewed by the police. Fear of legal and social consequences following an act of self-harm probably influence willingness to acknowledge DSH and preparedness to seek medical intervention.
India contributes almost 20% to the world's population, and suicides rates are increasing particularly amongst the young.11, 19 Obtaining reliable and nationally representative data on DSH rates in India should be a priority for health-funding agencies over the next decade. In order to reduce fatalities following self-harm, information and investment are needed to improve quality, affordability and accessibility of health care close to the affected communities.20
If, as seems likely, self-harm (especially pesticide poisoning) occurs predominantly in rural areas of India,11 Western models of data collection and intervention aimed at reducing pesticide poisoning (which is predominately accidental in developed economies) are likely to require significant modification to be reliable and effective. The WHO's global suicide prevention strategy is largely based on findings from research and models of suicide prevention developed in the West.21 Health care resources in rural areas of India are thinly spread, and are often rudimentary compared to those in the West. There is an urgent need for research in low- and middle-income communities – particularly in rural areas of India – to provide the evidence base to underpin public health strategies for preventing pesticide suicides in these countries.
The establishment of DSH registers is a first step towards the systematic collection of data in relation to self-harm, both for epidemiological purposes and to understand pesticide self-poisoning at an individual level. If DSH registers can be shown to generate reliable information in India, in due course it may be possible to identify the factors that put individuals at risk of behaving in this way, and create relevant evidence-based policies to develop interventions for reducing mortality and morbidity associated with DSH (particularly pesticide poisoning).
This paper explores the feasibility of setting up a DSH register in a resource-poor large State hospital in south India, where rates of suicide and DSH are high.
METHODS
Setting
This study was carried out at Mysore Medical College and Research Institution (MMCRI), a State-run hospital in Mysore, southern India. The hospital serves a catchment area of 1,500,000 population and 135 primary health centres. The hospital has most specialities, with 1050 beds and a 10-bedded intensive care unit. 800-1000 patients attend the hospital outpatient department daily. Daily attendance to the casualty department for the purpose of medico-legal registration (which includes self-harm) is between 110 and 130. All other presentations including emergencies are managed through respective speciality outpatient departments.
Figure 1. Care Pathway for deliberate self-harm (DSH) at Mysore Medical College and Research Institution (MMCRI)
Setting up of the register
The flow diagram (Fig. 1) illustrates the care pathway of those presenting with DSH to MMCRI highlighting that only a few receive psychosocial assessment. A working group of psychiatrists, psychologists, social workers, casualty medical officers, statisticians and hospital managers was formed to arrive at a consensus on the minimum dataset that could be gathered from DSH survivors for the purpose of setting up a register. Literature on establishing self-harm registers was reviewed along with international guidelines in relation to self-harm assessment in the general hospital.22, 23 Opinion was sought from senior psychiatrists and public health personnel from the private and public sector in Mysore and from the United Kingdom (UK). The team was visited, supported and advised by the Centre for Mental Health and Society, Bangor, UK.
The items listed in Table 1 were considered as ‘minimal yet essential’ for informing clinical practice, service development and patient engagement in future research. The study was not externally funded and, due to time and resource implications, it was agreed that outcomes of mental health assessments would not be recorded in the register. The method of DSH was coded according to the International Classification of Diseases 10th Revision (ICD-10) criteria24 and socio-economic indicators were derived from a modified Kuppuswamy’s scale25 that is validated for the south Indian urban population.
Table 1. Contents of the deliberate self-harm (DSH) register.
An electronic DSH register was set up in February 2013 and is currently held in the Department of Psychiatry, MMCRI, and Mysore. Two pre-registration House Officers (junior resident equivalent) visited the casualty department daily and identified those cases registered as self-harm from both the standard patient register and medico-legal case registers. If the individual was discharged from casualty (condition necessitated no further treatment, no intensive care bed available, or patient chose admission in private sector after first aid) the available information is captured from the registers and medical records. If they admitted to the general hospital they were traced and personally contacted. Information (as in Table 1) was collected from DSH survivors and from medical records. The data was verified by a Consultant Psychiatrist before being entered in the register. DSH survivors are asked to provide two contact details (postal address and phone number) for future tracing if they consent to further contact either in person or by phone. Table 2 is a list of the sources of data for the DSH register in Mysore and their limitations.
Table 2. Sources of data for deliberate self harm (DSH) register in Mysore and their limitations.
Feasibility
A DSH register should be representative, complete and accurate. The register should be acceptable to the entrants and only take a minimal time for data collection and registration. For the purpose of this study the following were identified as indicators of feasibility:
· Time between identifying that the patient should be included in the register and completion of data entry in the register. This was recorded for 80 randomly chosen inpatient DSH survivors.
· The proportion of patients presenting with alleged DSH who were correctly identified and, if admitted to the general hospital, traced for the purpose of inclusion to the register (representativeness).
· Proportion of those included in the register for whom a full data set could be captured (completeness).
· Proportion of the DSH survivors who were willing to be included in the register and provided contact details for future follow-up (acceptability).
· Over a period of a week, every month during study period February 2013 to July 2013, a Consultant Psychiatrist independently collected data from casualty registers and checked against the total number registered on the DSH register for the corresponding month (accuracy).
RESULTS
Between February 2013 and July 2013, a total of 19,563 patients attended the casualty department. Of these, 1072 attended in relation to self-harm. 1041 of them were hospitalised for further intervention. All of those who were hospitalised and survived (n=817) were traced and contacted. None objected to their details being entered on the register. However, only 253 of the 817 (30.9%) agreed to be contacted for future follow-up. Of the 817, only 109 (13%) had been formally referred to the psychiatry department for an assessment prior to contact with the research team. None of the 817 had any involvement with Social Services.
Out of the 1023 on the register, complete data was available and/or obtained for 740 (72.3%) individuals and data was incomplete for 283 (27.7%) patients. Either by reviewing the medical records or interviewing the patient, it was confirmed in all 1023 cases that there had been an act of self-harm necessitating medical intervention. The time between identifying that the patient should be included in the register and completion of data entry in the register varied between 30 minutes and 2 hours. When the data collected was cross-verified (n=315) by a Consultant Psychiatrist (author RR), entries of 310 individuals were accurate, with a minor discrepancy in less than 3 items for another 5 individuals.
Various terminologies were used to report a case of DSH in the case records (for example, suicide attempt, failed suicide, self-harm, poisoning, deliberate harm).
DISCUSSION
This is the first description of a method of successfully setting up and maintaining a DSH register in an Indian setting. It was a labour-intensive exercise due of lack of electronic patient data management, administrative support and the absence of an agreed care pathway for DSH in the hospital. Despite these obstructions, we have illustrated that it is feasible to set up a DSH register in a busy tertiary care hospital in India. Results of our study indicate that the register details are accurate and representative of those who seek help from the specialist centre. However, it cannot capture those patients whose DSH was managed successfully within primary health centres, those individuals who failed to seek help and those who died before admission.
Clinical Implications
The experience of establishing a DSH register has lead to changes in local clinical practice. DSH is associated with increased morbidity and increased utilisation of health services.26 DSH survivors who were contacted (n=817) by the psychiatry residents were offered psychosocial assessments. Under normal circumstances, 708 (87%) of this group would not have received any psychosocial assessment. The process of setting up the register has helped to identify DSH cases so that an intervention can be offered before discharge from the general hospital. The register has also played a major role in the identification of people who harmed themselves but were discharged without admission to a ward. This group can also be helped. We have now developed an education and service information leaflet which includes emergency contact details (similar to a crisis card in the UK), which is given to DSH patients on discharge. These are known to decrease the repetition of DSH in the developed world.27 Deaths from suicide are largely preventable if knowledge and understanding of this maladaptive behaviour is used to ensure timely intervention.8
By auditing DSH data in a systematic way, clinical decision-making will be based on pooled experience, not just on each clinician’s recall. Comprehensive registers of DSH provide clinicians with the opportunity to review cases of suicide where they have had clinical involvement, using techniques such as psychological autopsy, improving clinical skills and judgements. Overall there is a need for an attitude of vigilance about suicide risk, and of enthusiasm about pursuing initiatives for suicide prevention based on evidence. Better understanding of self-harm will assist in devising means of reaching out to those at risk of dying without having had contact with health care services.
Reporting of DSH in case records was inconsistent. There is a need for uniform recording, medical coding and reporting of DSH. In the DSH register, the method of self-harm is recorded using an international recognised coding system (e.g. ICD-10).
If we continue to offer psychiatric assessment to all cases of DSH, the much higher rate of ascertainment arising from the DSH register will place further strain on an already stretched psychiatric service. Further investment in services specifically targeting self-harm in India is urgently needed.
Service Implications
Use of the register
The register creates an opportunity for a standing DSH audit, allowing for identification of trends over time and comparisons with other services that establish DSH registers using similar methods. Systematic collection of demographic and clinical data will allow calculation of admission rates, repetition rates and other indices of importance in service development. Collaboration with non-governmental organisations in the region who work with those who self-harm will allow development and evaluation of specific culturally appropriate interventions.
Where the register should be held?
In the developed world DSH registers are normally held on electronic systems in the Accident and Emergency department or liaison psychiatric services. In India, it is a mandatory obligation to hold a medico-legal register (which includes DSH) in casualty. Maintaining an additional DSH register risks unnecessary duplication, but modification of a medico-legal register creates an ethical problem and risks under-reporting. There are few liaison psychiatry services in India. On balance, we suggest that our practice of holding the DSH register within the department of adult psychiatry is the optimal arrangement in the Indian setting.
Confidentiality
Confidentiality must be respected. In the UK, when establishing a DSH register, it is necessary to discuss issues of confidentiality and legality with the local Data Protection Officer, and to register under the Data Protection Act. Use of the data for research purposes requires approval from local Research Ethics Committees. In India, there is little regulation of this sort. In order to establish our register it was only necessary to obtain consultant approval and consent through the local medical committee. We suggest that good practice would demand that standards of confidentiality and oversight should, as far as possible, match Western standards.
Manpower and resources
Setting up this register in Mysore required input by a Consultant Psychiatrist, for 2 sessions per week for 6 months, to negotiate with casualty medical officers, consultant physicians and reception staff. The resident from the psychiatry department spent at least 2 hours a day collating and updating the register. The absence of a patient electronic data system and lack of administrative support has placed additional strain on residents and has prolonged the time to identify a case of DSH from the casualty records and trace them on the medical wards. We believe that once the register is established, these tasks could be managed by a trained Social Worker spending 1 session per day collecting the data and 1 session per week editing the register. The work load might vary in other hospitals, depending on the number of daily hospital attendances for DSH.
Integration with other data sources
Linking this register with post mortem records, local civil registration of deaths and police records is desirable but this needs co-ordinated effort from several civil bodies and public health organisations. In the absence of any legislation or national record linkage systems, there are few motivators to drive this change or the allocation of resources. However, a unique person identification number system is presently being rolled out across India. The development of cross-agency electronic databases will facilitate easier record linkage in the future, which creates the opportunity for collection of reliable and representative data at a regional level.
None of those who were contacted during the study period had any formal input from Social Services. Though the models and mode of delivery by Social Services in India is radically different to those in Europe, DSH survivors form a stigmatised vulnerable group who are frequently in need of social assessment and support.
Future investment and development
There are good humanitarian reasons to seek the de-criminalisation of acts of self-harm in India, and there is presently strong lobbying to bring this about. It is reasonable to suppose that this might lead to readier help-seeking and better reporting of self-harm and suspected suicide. However, there are other measures that would be necessary to reduce rates of DSH and completed suicide. Regulating the supply of organophosphate insecticides, so that they are only available in dilutions that make fatal overdose more difficult, would be one such measure. There is also a need to develop liaison psychiatric services, offering psychosocial assessments to a higher proportion of those who present with features indicative of probable self-harm. Other necessary developments include investment in patient electronic records and systematic strategies for destigmatisation of DSH.
The register has provided us with a cohort of individuals who are willing to be contacted for future studies. The register has continued beyond the study period. We presently have 3720 individuals on the register. The unit has established formal links with research centres in the UK. We intend to carry out longitudinal studies to examine the patterns of DSH, rates of repetition, compliance with follow-up and suicide rates. This will help to identify the culture-specific access, adherence and prognostic factors, and will influence the development and validation of brief psychosocial interventions in a social, economic and cultural context that is radically different to the West.
CONCLUSIONS
We have illustrated that it is feasible to set up a DSH register in a busy tertiary care hospital in India where rates of self-harm are high. Results of our study indicate that the register details are accurate and representative of those who seek help from the specialist centre.
Very few were referred for psychosocial assessment following an act of self-harm and none of them had any formal input from Social Services. Though the models and mode of delivery by Social Services in India is radically different to those in Europe, DSH survivors form a stigmatised vulnerable group who are frequently in need of social assessment and support.
A 46 year-old man presented to the Emergency department with chest pain and collapse, associated with loss of consciousness lasting several minutes. He had no significant past medical history and he had no risk factors for coronary artery disease. However, he did note a similar episode of collapse and loss of consciousness one year prior for which he did not seek medical attention. There was no known family history of heart disease or sudden death.
On examination he was haemodynamically stable with a blood pressure of 130/80 mmHg and heart rate of 85 beats per minute. Jugular venous pressure was measured at 2cm above the sternal angle and heart sounds were normal with no added sounds. His oxygen saturation was 98% on air and chest was clear to auscultation. Chest X-Ray demonstrated clear lung fields and laboratory investigations, including electrolytes and cardiac troponin T were within normal limits. Echocardiography showed a structurally normal heart. Figure 1 shows his 12-lead electrocardiogram (ECG) on admission.
Figure 1 – 12 lead ECG on admission
Questions
1. What is the likely diagnosis based on the clinical presentation and ECG findings?
2. What life-threatening arrhythmias can arise from this condition?
3. What is the pathophysiology of this condition?
4. How is the diagnosis of this condition made?
5. What treatment options are available for patients with this condition?
Answers
1. What is the likely diagnosis based on the clinical presentation and ECG findings?
Short answer
Brugada syndrome
Long answer
The ECG shows coved Type 1 ST segment elevation in keeping with a diagnosis of Brugada syndrome.
First described in 1992, Brugada syndrome is a primary cardiac electrical disease or channelopathy that is accompanied a structurally normal heart and carries an association with sudden cardiac death1.
Presentation often occurs in the third or fourth decades of life, with a male preponderance of 8:1, however sudden cardiac death due to Brugada syndrome has also been seen in patients at the extremes of age. It is estimated that it accounts for up to 20% of all sudden cardiac deaths in patients without structural heart disease, ischaemia or electrolyte abnormalities2. It is most commonly seen in south-east Asia, especially Thailand, where its incidence is around 1%, and is much less common in western countries1.
2. What life-threatening arrhythmias can arise from this condition?
Short answer
Brugada syndrome is associated with increased risk of ventricular tachycardia (VT), often polymorphic, and ventricular fibrillation (VF).
Long answer
Brugada syndrome often manifests clinically in the form of syncope or sudden cardiac death. It is most commonly associated with polymorphic VT and VF, which may or may not terminate spontaneously. There are a large proportion of patients with Brugada syndrome who never experience any symptoms and indeed, may not ever even be identified as having the condition, unless they are found to have incidental ECG abnormalities as part of routine medical testing or are under investigation for another problem3.
3. What is the pathophysiology of this condition?
Short answer
Brugada syndrome is understood as a genetic cardiac channelopathy, a disorder produced by the dysfunction of a cardiac ion channel participating in the action potential which can result in electrical change favouring the development of arrhythmias. Inheritance of the condition occurs via an autosomal dominant mode of transmission with incomplete penetrance4.
Long answer
Brugada syndrome is a genetic disorder, with a loss-of-function mutation of the SCN5A gene implicated in about 30% of sufferers. This gene codes for the α-subunit of the cardiac sodium channel. Other mutations of sodium and calcium channels have also been found. In inherited cases, the gene is passed in an autosomal dominant fashion, though sporadic mutations are also seen.
There is increased susceptibility to ventricular arrhythmias, because of altered depolarisation within the right ventricle. In SCN5A mutations, the defect in sodium channels leads to decrease in the sodium current and a shortening of the cardiac action potential by blunting phase 0 depolarisation. Potassium channels are also affected, with an increased number of transient outward potassium channel currents. This imbalance in the myocytes between sodium and potassium concentrations means the overall effect is to shorten the refractory period, making the myocytes more prone to re-entrant circuits, leading to the development of VT and degeneration to VF2,5.
4. How is the diagnosis of this condition made?
Short answer
Brugada syndrome is characterised by electrocardiographic changes demonstrating coved ST segment elevation in the right precordial leads.
Long answer
Electrocardiographic abnormalities constitute the hallmark of Brugada syndrome. There are three different ECG patterns and in all three types, the ECG shows ≥2mm J point (junction between the termination of QRS complex and beginning of ST segment) elevation and a characteristically shaped ST segment in the right precordial leads6.
Type I has a ‘coved’ pattern ST segment elevation ≥2mm, with a descending terminal portion in at least one right precordial lead.
Type II has a ‘saddle-back’ ST segment elevation ≥1mm and has a high elevation in its initial portion.
Type III has either coved or saddleback ST elevation but is less accentuated than types I or II (<1mm).
Although all the 3 patterns can be present in patients with Brugada syndrome, only the presence of a type-1 ECG pattern defines the diagnosis of the condition2,7. The patterns for type II or III are not diagnostic, and carrying out a Class I anti-arrythmic drug (AAD) test to confirm the diagnosis is recommended. This can be done with AADs such as ajmaline, flecainide or procainamide, though currently ajmaline is preferred due to its higher sensitivity in revealing Brugada type ECG changes1.
It is worth noting that the resting ECG changes associated with Brugada syndrome (in particular type I) are often transient, and therefore, in someone in whom the diagnosis is suspected, an AAD test may be indicated even if there are no resting spontaneous ECG abnormalities evident6.
Differential diagnoses of Brugada syndrome must be approached with care as ST segment elevation is associated with a wide variety of benign and malignant pathophysiologic conditions3.
5. What treatment options are available for patients with this condition?
Short answer
Currently, the implantable cardioverter defibrillator is the only proven effective treatment in the prevention of sudden cardiac death.
Long answer
Management of Brugada syndrome is focused on risk stratification of patients to prevent arrhythmic death in high risk individuals. ICD implantation can prevent sudden cardiac death in these groups1. Newer devices are now also being used, including the subcutaneous ICD which is implanted in a subcutaneous pocket and does not require any endovascular leads in the heart or access to the central venous circulation8.
Pharmacological options are focused on rebalancing the ion channel current active during the early phases of the epicardial action potential in the right ventricle3,9. Some studies have evaluated the role of quinidine in the treatment of Brugada syndrome and found it to be effective in preventing polymorphic VT and VF in this condition10. Quinidine has also been proposed as an alternative to ICD implantation in children and infants too young to receive an ICD11,12.
Data relative to the use of cryosurgical treatments or ablation therapy in Brugada syndrome are very limited at this point in time3.
Patient outcome
The patient underwent successful implantation of a subcutaneous cardioverter defibrillator. Figure 2 and Figure 3 show chest radiographs of the leadless device.
The discharge summary is an integral part of continuing patient care. Apart from containing vital information regarding current admission, it also conveys key findings and plans to clinicians who will be taking over the care of the patient. This would mean communicating important information about patients to ensure appropriate and safe follow-up management. Studies involving discharge summaries have looked into role of communication from secondary to primary care and have highlighted the importance of accuracy and quality of information,1 errors2 and general practitioner (GP) preference.3 Systematic reviews have found low availability (12-34%) of discharge summary during first visit post-discharge as well as wide variations in content of discharge summaries thereby directly affecting patient management.4,5 The timing of discharge summary completion and reaching the follow-up physician is therefore of prime importance wherein this has been also found to influence and reduce the risk of rehospitalisation.6 The content necessary for a ‘good’ or ‘high-quality’ discharge summary has been studied via surveys. The inclusion of important data such as diagnosis, discharge drugs, complications, laboratory results and follow-up plans have been considered to be important clinical information by hospital physicians and GPs.7
Hospital discharge summaries can be hand-written, dictated or in electronic format. These formats have their benefits and downfalls. Hand-written summaries have been found to be well-accepted by primary care physicians although involve the factor of legibility.8 A randomised-controlled trial found no difference between electronic and dictated discharge summaries for primary care physician satisfaction.9 Although the use of electronic discharge summaries has significantly improved both the content and timing of discharge summaries reaching follow-up physician or healthcare staff,10 they have been found to contain higher number of errors in patient progress, additional diagnosis and free-text components.11
This audit examined the timing and content of discharge summaries at The Mount and whether they met local Trust standards. A follow-on audit was conducted to study the impact of recommendations that had been put forward at the end of Cycle 1 of the audit.
Aim and Objectives
Aim
Cycle 1: To study the content, accuracy and timing of discharge summaries at The Mount, Old Age Psychiatry hospital.
Cycle 2: To examine changes in clinical practice following recommendations from Cycle 1 of audit involving content and timing of discharge summaries from The Mount.
Objectives
Cycle 1: To ascertain whether Trust guidelines regarding content of discharge summaries are met and also whether the timeline guidance is being maintained.
Cycle 2: To examine adherence to the Trust guidelines as well as to study the changes brought about by recommendations at the end of Cycle 1.
Criteria/ Standards
Trust guidelines state:
Discharge summaries must be typed and sent in 5 working days post-discharge from hospital.
They must include the following information (Box 1):
Box 1 Trust guidelines for inclusion of information in discharge summaries
Patient ID
Date dictated
Patient Name
Date of Birth
Name of consultant
Admission address
Discharge address
Admission date
Discharge date
Reasons for admission
History of present illness
Past medical history
Past psychiatric history
Family history
Social history
Occupational history
Premorbid history
Mental health examination
Physical examination
Results of investigations
Progress & treatment during admission
Final diagnosis
Discharge medications
Follow-up arrangements
Name of key worker
Number of pages
Method
Audit Sample
Patients admitted and discharged from Ward 3 & 4 of The Mount, between 01.04.2011 to 31.10.2011. A total of 103 patient discharge summaries were therefore analysed in Cycle 1 of the study. For cycle 2, the audit sample comprised of patients admitted and discharged from Ward 3 & 4 of The Mount, between 01.04.2012 to 31.10.2012. A total of 97 patient discharge summaries were therefore analysed in this part of the study.
Data Collection
Data was collected using an anonymous data collection tool (Appendix 1) which was designed according to Trust guidelines. Administrative staff provided the clinical audit leads with list of patients discharged during the study dates. The electronic patient record system of the Trust (PARIS: Patient Record Information System) was used to study the discharge summary letters. Data collection was performed under the supervision of consultant responsible for the audit, between November 2011 and January 2012 for cycle 1 and for cycle 2 data collection was performed between October 2013 and November 2013. Patient confidentiality and anonymity was maintained.
Data Analysis
Qualitative data was gathered, coded and collated on to a Microsoft Excel spread sheet. The data collected was reviewed by the authors to ensure each aspect of data collection tool was filled. The data was analysed by the Clinical Audits Facilitator at the Trust Clinical Audit Support Team and placed into a report format for dissemination.
Results
The number of discharge summaries analysed in Cycle 1 and 2 of this study was 103 and 97 respectively.
Data were collected using the data collection tool (appendix 1). Dates of discharge, dictation and typing were recorded. Date of typing was used as a proxy of date sent to GP since there was no record of this. Seven days were permitted for discharges to be sent (equivalent to 5 working days). Discharge summaries were read and it was recorded if each stipulated heading from the Trust guidelines was present. No comment was made on quality of information; only consideration was whether information was present or absent.
Compliance with each point from the above categories is shown in the following series of tables and comparison is made between the studies in Cycles 1 and 2 (Table 1-4). The statistical significance of the differences found in the two audit cycles was evaluated using chi-square tests.
Table 1 Presence of information on discharge summary according to Trust guidelines
Criteria
Adherence % 2011 (n=103)
Adherence % 2013 (n=97)
Statistical significance
Patient code
100% (n=103)
97% (n=94)
p=0.721
Date dictated
72% (n=74)
98% (n=95)
p<0.001
Patient Name
100% (n=103)
100% (n=97)
No change
Date of birth
97% (n=100)
100% (n=97)
p=0.090
Name of consultant
98% (n=101)
99% (n=96)
p=0.596
Name of current GP
98% (n=101)
98% (n=95)
No change
Admission address
98% (n=101)
100% (n=97)
p=0.167
Discharge address
98% (n=101)
100% (n=97)
p=0.167
Admission date
97% (n=100)
100% (n=97)
p=0.090
Discharge date
97% (n=100)
99% (n=96)
p=0.342
Legal status
99% (n=102)
98% (n=95)
p=0.525
Reasons for admission
98% (n=101)
98% (n=95)
No change
History of present illness
100% (n=103)
99% (n=96)
p=0.301
Past medical history
89% (n=92)
95% (n=92)
p=0.150
Past psychiatric history
95% (n=98)
98% (n=95)
p=0.282
Family history
19% (n=20)
86% (n=83)
p<0.001
Social history
56% (n=58)
89% (n=86)
p<0.001
Occupational history
67% (n=69)
68% (n=66)
p=0.873
Premorbid history
37% (n=38)
52% (n=50)
p=0.036
Mental health examination
95% (n=98)
93% (n=90)
p=0.482
Physical examination
86% (n=89)
92% (n=89)
p=0.227
Results of investigations
84% (n=87)
78% (n=76)
p=0.265
Progress & treatment during admission
96% (n=99)
100% (n=97)
p=0.049
Final diagnosis
92% (n=95)
97% (n=94)
p=0.147
Discharge medications
98% (n=101)
97% (n=94)
p=0.602
Follow-up arrangements
86% (n=89)
79% (n=77)
p=0.007
Name of key worker
64% (n=66)
56% (n=54)
p=0.225
Number of pages
0% (n=0)
0% (n=0)
No change
Are there any spelling/typing errors in the list of medications?
90% (n=8)
98% (n=2)
p=0.064
Are there any spelling/typing errors in the diagnosis and medical terminology?
78% (n=21)
99% (n=1)
p<0.001
Table 1: The presence of information mentioned in the Trust guidelines is analysed. The percentage adherence in cycle 1 is compared with findings from cycle 2. Significant increase in inclusion of family history, social history, follow-up arrangements and date of dictation is observed. A healthy increase is also observed in inclusion of premorbid history and progression and treatment during admission. A significant reduction in spelling/typing errors is also seen. The decrease in inclusion of name of key worker, discharge medications, mental health examination and results of investigation amongst others is also noted. GP, general practitioner.
The comparison of findings from Cycle 1 and 2 establish a significant increase in adherence to family history (p<0.001), social history (p<0.001), premorbid history (p=0.036) as well as progress and treatment during hospital stay (p=0.049) components of the discharge summary. There was also a significant increase in inclusion of date of dictation of discharge summaries (p<0.001). Increase in adherence to most of the components of discharge summaries was observed. However, there was significant decrease in inclusion of follow-up arrangements (p=0.007) as well as a decrease in inclusion of name of key-worker assigned to patient (from 64% in cycle 1 to 56% in cycle 2; p=0.0225). A significant decrease in spelling/typing errors in diagnosis or medical jargon was observed (p<0.001).
Timing of Discharge Summaries
Table 2 Time taken between discharge of patient and dictation of letter
Days
Adherence % 2011 (n=74)
Adherence % 2013 (n=94)
Statistical significance
0-7
30% (n=22)
73% (n=69)
p<0.001
8-15
24% (n=18)
22% (n=21)
p=0.762
16-22
18% (n=13)
4% (n=4)
p=0.004
23+
29% (n=21)
0% (n=0)
p<0.001
Table 2: The time taken between discharge of patient and dictation of letter is analysed. A significant increase is observed in the dictation of letter as per Trust guidelines (within 5 working days).
Table 3 Time taken between dictation and typing of discharge letter
Days
Adherence % 2011(n=75)
Adherence % 2013 (n=94)
Statistical significance
0-5
84% (n=63)
73% (n=69)
p<0.001
6-11
7% (n=5)
24% (n=23)
p=0.192
12+
9% (n=7)
2% (n=2)
p<0.001
Table 3: The time taken between dictation of letter and typing of discharge letter is analysed. A significant decrease is observed in the time taken for typing of letter within 5 days of dictation of letter.
Table 4 Time take between discharge and typing of discharge letter
Days
Adherence % 2011 (n=100)
Adherence % 2013 (n=96)
Statistical significance
0-7
18% (n=18)
52% (n=50)
p<0.001
8-15
32% (n=32)
34% (n=33)
p=0.724
16+
60% (n=60)
14% (n=13)
p<0.001
Table 4: The time taken between discharge of patient and typing of discharge letter is analysed. A significant increase is observed in the early typing of discharge letter from the date of discharge of patient.
The number of discharge summaries being dictated and typed within 7 days of discharge was significantly increased (p<0.001) and a significant decrease in discharge letters being dictated more than 2 weeks (p=0.004) or 3 weeks (p<0.001) of patient being discharged was observed. The time taken between dictation of letter and it being typed up was also found to have dropped, with 73% being done within 7 days, significant decrease (p<0.001) being observed since the first cycle. Furthermore, a significant increase is observed in early (less than 7 days) typing of discharge letter since patient being discharged (p<0.001).
Discussion:
The discharge summary is a very important means to communicate medical (both physical and psychiatric) and nursing interventions to the GP or community mental health team. This in turn helps in making invaluable decisions to patient care in the community. Hence, it is worth spending time on doing a good discharge letter which includes relevant information. A timely discharge letter can also be very useful in this regard.
At the end of Cycle 1 of the audit, recommendations that were made included (Appendix 2):
Disseminating information amongst all junior doctors, consultants and administrative staff on each ward to include the above mentioned headings in accordance with Trust guidelines.
Information was also provided regarding finding out Name of Keyworker in PARIS system.
A specific note was also placed regarding to spell out medical terminologies that would assist in the typing of discharge summaries by administrative staff.
From the results, it is evident that the content of the discharge summary has largely been maintained. In other words, good practice was maintained and recommendations from previous audit were implemented in most spheres of discharge letters. However, despite the recommendation of finding out name of key-worker from PARIS system, there was a decrease (from 64% in first cycle to 56% in second cycle) in its inclusion (p=0.225). Thus, training in usage of information technology system is essential. Providing appropriate instruction and training to junior doctors has been found to be useful in improving the quality of discharge summaries.12 Therefore, it might be beneficial to include instructions or guidelines for appropriate discharge summaries at local Trust or departmental inductions. This will help junior doctors in ensuring completion of accurate and succinct discharge summaries that will aid in patient management.
There was a reduction in documentation of discharge medication, follow up arrangement, mental state examination and physical health investigation carried out as an in-patient. This certainly needs improving as these are the relevant areas to facilitate smooth transition of care in the community and follow-up arrangement. With regard to the timing of the discharge summary, this was found to have significantly improved from the previous audit cycle. For example, the timing between discharge and dictation (within 7 days) has increased from 30% to 73% and almost all discharge summaries are dictated no later than 3 weeks. The possible reasons for delays in dictation could be ongoing workload, availability of medical staff and of the medical notes, as these are sometimes requested by the Intermediate Community Service (ICS) team. There was a slight drop in the time between dictation and typing (from 84% to 73%), which could possibly due to availability of administrative staff, dictation tapes or medical notes and proof reading by medical staff. Significant increase was observed in inclusion of date of dictation of discharge summaries which will be a useful component for future audits. A significant decrease in spelling/typing errors in diagnosis or medical terminologies was observed. Furthermore, there was significant increase in inclusion of family history, social history, premorbid history as well as information on progress and treatment during hospital in the discharge summary. Therefore, timely audit and feedback can be very useful in improvement of discharge summaries and patient care.
Recommendations & Actions:
Raise awareness amongst senior house officers (SHO’s) and other doctors in the Trust regarding recording of pre-morbid history, occupational history, name of keyworker as this was only done in 52%, 62%, 56% cases respectively. This could be done by disseminating findings from this audit amongst SHO’s and other doctors of Trust through hand-outs to wards as well as through local teaching session.
Remove number of pages from the list of sub-headings needed in discharge summary as this is dependent on typing and not necessarily possible to estimate while dictating discharge summary. However, it is an important part of discharge summary. Therefore, send information with audit findings to medical secretaries informing the need to keep number of pages in the discharge summary.
Consider adding a section on documentation of risk assessment should be included in the discharge summary as well as ‘early relapse signature’ which would enable early intervention in the community to avoid inpatient admission. This could be included in the discharge summary. This would involve liaising with consultants and the responsible person for making/printing discharge summaries for Trust.
People with intellectual disabilities are a heterogeneous group, who can pose a challenge to services in terms of meeting a wide range of needs. Following the closure of large institutions, the optimum means of service provision for people with intellectual disabilities with additional mental illness and challenging behaviour has been a matter of debate.
Challenging behaviour can be defined as a ‘culturally abnormal behaviour of such an intensity, frequency or duration that the physical safety of the person or others is likely to be placed in serious jeopardy, or behaviour which is likely to seriously limit use of, or result in the person being denied access to, ordinary community facilities’ – Emerson, 19951. Examples of challenging behaviours include self-injury, aggressive outbursts, destruction of property and socially inappropriate behaviour.
The credit-crunch of recent years has led to an increased use of private sector services delivering care to NHS funded patients. The Winterbourne Scandal unearthed by BBC Panorama in June 2011 (an investigation into the physical abuse and psychological abuse suffered by people with learning disabilities and challenging behaviour at this private hospital in South Gloucestershire), highlighted that whist this maybe an economically viable option, fundamental questions were raised about whether private sector services’ safeguards and monitoring protocols were as robust as the NHS in protecting vulnerable patients. It also reawakened longstanding disputes around the way people with complex needs are cared for in residential settings. The discussions centred around ‘institutional’ versus ‘community’ care styles; specialist intellectual disabilities services versus generic adult psychiatric services; local versus specialist expertise congregated around a single unit; and also financial questions regarding how best to meet the needs of this population at a time of austerity. Opinions vary widely, and at times are even polarised, as a result of several factors including position within this competitive and complex system, personal and cultural politics and also personal experience. As a result of the government review, subsequent to the Winterbourne investigation, a number of recommendations have been made which will affect the future of care of this vulnerable group of patients. These include, “by June 2013, all current placements will be reviewed, everyone in hospital inappropriately will move to community-based support as quickly as possible, and no later than June 2014… as a consequence, there will be a dramatic reduction in hospital placements for this group of people”2
The Department of Health Policy, Valuing People3, set out ‘ambitious and challenging programme of action for improving services’, based on four important key principles – civil rights, independence, choice and inclusion. Government Policy as detailed in both Valuing People and the Mansell Report3, 4 recognises that NHS specialist inpatient services are indeed necessary on a short-term basis for some people with intellectual disabilities and complex mental health needs. Inpatient facilities for people with Intellectual Disability have been described as highly specialised services that are a valuable, but also expensive, component of mental health services5. The Enfield Specialist Inpatient unit - the Seacole Centre - is one such service.
The Seacole Centre consists of two inpatient units, with a total of 12 inpatient beds, for people with intellectual disabilities with acute mental illness and/or challenging behaviour. It is located within Chase Farm Hospital in Enfield, Greater London. The Seacole Centre has a multidisciplinary team consisting of nurses, psychologists, psychiatrists, a resident GP, occupational therapists, intensive support team staff, physiotherapists, speech and language therapists, a physical exercise coach and administrative staff. Patients are admitted from a variety of sources, including general psychiatric wards, general medical wards and community intellectual disability teams. Since patients are often referred from other boroughs, in addition to this multidisciplinary team, each patient has their own community and social care team based within their own borough. The use of out-of-area units faces similar challenges to out-of-area placements, use of which has been increasing in the UK, and it is important to explore ways in which service users, out-of-area, can be supported effectively6.
In 2002, a review of admissions to the unit was completed to describe the management of mental illness and challenging behaviour. Since then there have been several service reconfigurations within the trust, in order to accommodate national, political and financial recommendations. However, despite these changes, it was observed clinically that certain clinical problems including delayed discharges continue to occur. We decided to complete a similar review, to describe current admission trends in further detail, in order to enable us to identify areas of improvement, and also to ascertain the nature and severity of ongoing problems to focus future recommendations.
METHOD:
A retrospective review of the case records of all inpatient admissions to the Seacole Centre was completed over a three-year period – from 1st January 1999 to 31st December 2001.
Data collected included age on admission, gender, borough, diagnosis, psychotropic medication on discharge, date of admission and discharge, length of stay, legal status on admission, delays on discharge, and reason for delay, and living arrangements prior to and after discharge
A successful outcome of admission was discharge from hospital to community care. We used the following definition of the delayed discharge:
"A delayed transfer occurs when a patient is ready for transfer from a general and acute hospital bed but is still occupying such a bed. A patient is ready for transfer when:
a clinical decision has been made that the patient is ready for transfer
a multi-disciplinary team decision has been made that the patient is ready for transfer
the patient is safe to discharge/transfer.7
The review was repeated during a further three-year period between 1st January to 2009 and 31st December 2011.
RESULTS:
Characteristics of 1999-2001 cohort, and comparison with 2009-2011
The basic demographic details can be seen in Table 1.
Table 1 - Demographic details
1999-2001
2009-2011
Number of admissions
60
41
Number of patients
46
40
Average (mean) age/years
29.58
36.16
Age Range / years
14-63
19-72
M:F ratio
1.4:1
3.1:1
Total number of boroughs from which patients admitted
10
7
Trends in Admission Rates
As seen in Tables 1 and 2, there has been a reduction in the total number of admissions between the studies. There has also been a marked reduction in re-admissions. The average length of stay has increased, and although the number of delayed discharges has slightly decreased, it can be seen that this is still a factor in a significant proportion of the admissions.
Table 2 - Trends in admission
1999-2001
2009-2011
Total Number of admissions
60
41
Average (mean) length of stay / days
198.6
244.6
Number of readmissions
16
1
Number of delayed discharges
40 (67%)
24 (59%)
Reason for admission
The trends in reason for admission are shown in Figure 1.
Figure 1 – Trends in Reason for Admission, 1999-2001 compared to 2009-2011
In both time periods, the most frequent reason for admission is challenging behaviour (62%, n=37 between 1999-2001; 63%, n=29, between 2009-2011), followed by psychosis (22%, n=13 between 1999-2001; 11%, n=5, between 2009-2011. Social admissions were the third most common reason for admission in the recent study (0% between 1999-2001; 4%, n=2 between 2009-2011). The range of psychiatric presentations was widest during the original time period.
Patterns on discharge
As shown in Figure 2, most patients in the original study were discharged to either the same residential home or back to the family home, where as in the latter time period patients were most frequently discharged to either a different residential home or to supported living. Figure 3 summarises this effect, demonstrating the change in discharging the majority of patients to a different place of residence.
Figure 2 – A graph to show the place of discharge, 1999-2001 compared to 2009-2011
Figure 3 – A Graph to Demonstrate Trends in Place of Discharge – comparing 1999-2001 and 2009-2011
Delayed discharges
The primary cause for delay in both studies was finding appropriate placement, although this was more marked in the recent cohort.
One of the major factors contributing to delayed discharges was lack of identification of suitable placement, which was identified as a major contributing factor to delayed discharges in 69% of cases in 2009-2011 and in 44% in 1999-2001, and apparent delays in the role played by social services (table 2).
DISCUSSION:
Throughout this study spanning 10 years, challenging behaviour followed by psychotic disorder remained the most common cause for admission. Interestingly, by 2008-2011, the third most common cause for admission was related to social reasons (4%). There were no admissions in the original study for this reason. Between 1999 and 2001, there were a wider range of reasons for admission across the mental illness spectrum compared to 10 years on. In previous studies, the largest diagnostic group for all admissions was schizophrenia spectrum disorders7,8. However, between 2009-2011, more than a quarter of patients admitted to the Seacole Centre did not have any psychiatric diagnosis on admission. It is important to keep in mind that individuals with intellectual disabilities accessing specialist inpatient services are more likely to present with complex clusters of symptoms and behavioural problems that may span several diagnostic categories.
The most significant improvement from the original review and the re-review is that the number of re-admissions significantly reduced from 24% (14 patients) to 2% (1 patient). Of interest to note is that during 1999-2001 a large proportion of patients were discharged to their original place of accommodation (often the family home) whereas in 2009-2011, it was more common for patients to be discharged to a new place of living, more suited to managing increasing complex needs and behaviours. This may account for some of the reduction in re-admission rates.
The length of stay over the 10-year period has slightly increased from an average of 198.6 days up to 244.6 days, which demonstrate that admissions are considerably longer than in more generic medical settings. The findings are in keeping with a number of other studies regarding patients with intellectual disability who are admitted to a specialist unit and continue as inpatients for significantly longer periods. One study showed a mean length of stay 23.2 weeks for a specialist unit versus 11.1 weeks in generic settings 8. Another study in South London revealed similar finds of 19.3 weeks compared with generic unit stays of 5.5. weeks9. An exploratory national survey of intellectual disability inpatient services in England has shown that 25% of residents had been in the units for more than two years. Only 40% of residents had a discharge plan, and only 20% had both this and the type of placement considered ideal for them in their home area10. Reasons for length of stay are not fully understood in any of these studies. They may include fear of taking risks, lack of local safe or competent amenities, lack of experience or authority amongst those charged with sourcing bespoke services for complex people with challenging needs, and also a potential lack of such resource in terms of time available to see people, read reports, meet with stake holders and find the right services. The results of another retrospective study comparing the generic and specialist models in two districts in the UK by Alexander et al11 suggested that, within the same district, patients do stay longer in the specialist unit, but they are less likely to be discharged to an out of area placement.
There is no evidence to suggest that comprehensive care for people with intellectual disabilities can be provided by community services alone. Likewise, there is also no clear evidence to suggest that a balanced system of mental health care can be provided without acute beds12. There is, however, clear evidence that services created by the private sector are used very widely and seen as at time as an economically viable option in the current climate of credit crunches.
The different models of inpatient service provision that have been suggested range from mainstream adult mental health services; alternatively an integrated inpatient scheme whereby people with Intellectual disabilities with additional mental illness or severe challenging behaviour are admitted to adult mental health beds, with provision for extra support from a multidisciplinary learning disabilities team; ranging across to specialist assessment and treatment units13,14.
Inpatient care is known to consume most of the mental health budget15 and specialist inpatient units are an expensive component of these services. Cost containment and cost minimisation of inpatient beds within the current economic recession presents a real challenge for those charged with responsibility to provide high-quality, effective, specialist care for adults with intellectual disability. Such cost reduction could be approached in a number of ways, through the reduction of length of stay, optimising drug budgets, reducing rates of re-admissions, and establishment of projects in association with the voluntary and statutory sector to facilitate prompt and safe discharge.
Reducing the average length of stay where possible can reduce the cost, and the resources and budget freed up in this way could be used for other service components15. However, this single agenda can lead to problems of pressured early discharge to unsuitable placements. It is known that resource consumption is most intense during the early stages of admission. As such, we observe a position whereby reducing length of stay requires proactive planning throughout the whole process of care, as well as active discharge planning, with a need for clearly defined pathways of care.
A crucial aspect of the patient's transition through inpatient placement to life in the community is efficient and regular communication between the relevant professionals and teams who form part of continuity of on-going care back in the community. This can at times be particularly challenging owing to differences in values and perceptions about patient need and problem, and also varying pressures. Understanding and resolving problems for individuals with complex and severe challenging behaviour or mental illness that requires a period of containment in a specialist service also requires specialist on-going work and risk management to ensure that when the problems are contained and understood, they remain contained and understood on discharge and thereafter so long as the individual remains vulnerable to the point of requiring any care giving. Many people from the general population who develop a serious mental illness requiring hospitalisation, have capacity once well, to make decisions for themselves and articulate a need or otherwise for specific care or intervention. This is rarely completely the case for people with Intellectual disabilities. Collaborative approaches together with those involved in community care is crucial to getting the right care at the right financial cost for this relatively small but very complex and vulnerable group of individuals.
Irritable bowel syndrome (IBS) is a chronic and often debilitating condition with a complex aetiology1. It is the most common diagnosis made by gastroenterologists worldwide2. The incidence and prevalence of IBS vary depending on the diagnostic criteria used but it is estimated that the prevalence in the UK is 17% overall, with a prevalence of 11% among men and 23% among women3-4. IBS can have a significant negative impact on quality of life and social functioning, although it is not known to be associated with the development of serious disease or excess mortality. However, patients with IBS are more likely to undergo specific surgical operations such as hysterectomy and cholecystectomy. IBS further represents an economic burden on society due to the high consumption of healthcare resources and the non-productivity of IBS patients5. It appears that 33–90% of patients do not consult a physician, and that a proportion of patients who meet the IBS criteria are not diagnosed with IBS. The frequency of IBS symptoms peaks in the third and fourth decades, and there is a female predominance of about 2:1 in the 20s and 30s, although this discrepancy is less apparent in older patients6. The female predominance is less apparent in the general population, which suggests that women with IBS are more likely to seek healthcare for their symptoms7. IBS symptoms which persist beyond middle life continue to be reported by a substantial proportion of individuals in their seventh and eighth decades.
Pathogenesis
The pathogenesis of IBS appears to be multifactorial. The following factors play a central role in the pathogenesis: heritability and genetics, dietary and intestinal microbiota, low-grade inflammation and disturbances in the neuroendocrine system of the gut2.
IBS is known to aggregate in families and to affect multiple generations but not in a manner consistent with a major Mendelian effect. Relatives of an individual with IBS are two to three times as likely to have IBS8.
Psychological distress is not only a common co-morbidity in IBS patients, but also a factor which is likely to play a direct role in the pathogenesis4. Interestingly, parental modelling and the reinforcement of illness behaviour can also contribute to IBS. Having a mother with IBS has been shown to account for as much variance as having an identical set of genes as a co-twin who has IBS. This insinuates that the contribution of social learning to IBS is at least as great as the contribution of heredityFurthermore, the role of childhood events such as nasogastric tube placement, poor nutrition, abuse, and other stressors have been clearly associated with IBS8.
A substantial proportion of patients with IBS report onset of their symptoms after acute gastroenteritis9. Post-infectious (PI)-IBS has been reported after viral, bacterial, protozoa and nematode infections, with the incidence of PI-IBS varying between 7% and 31%. In this subset of IBS patients GI symptoms appear following gastroenteritis, with approximately 10% developing persistent symptomsRecent studies suggest that some individuals are genetically predisposed to developing PI-IBS, with some people demonstrating a specific cytokine response to infection4.
It is important to note that women appear to have more frequent and severe IBS symptoms during menses compared to other phases of the menstrual cycle and that female gender is a significant independent risk factor for the development of IBS7.
Diagnosis and Investigations
Adult patients who present to their general practitioner (GP) with lower gastrointestinal tract disorders account for one in 20 of all general practice consultations. The possibility of sinister conditions such as colorectal cancer or inflammatory bowel disease may create diagnostic uncertainty and reluctance for the doctor to attribute the symptoms to IBS. In the United Kingdom up to 29% of patients with IBS are referred to a specialist but the majority of these will return to their GP for long term management6.
Primary care differs from specialist care because the GP’s greater familiarity with the patient, and their previous consultations, enable presenting problems to be seen in context rather than in isolation. Furthermore, it involves the first contact for care of problems at a stage when they are likely to be poorly defined. Lastly, primary care is characterised by a biopsychosocial model of care that takes into account the context of the person’s problem. These characteristics are especially important when managing chronic disorders, such as IBS, where there is a high priority on continuity of care6.
There is currently no biochemical, histopathological or radiological diagnostic test for IBS. The diagnosis is based principally on symptom assessment. The Rome III criteria (Figure 1) is the most recent, updated and universal diagnostic criteria for IBS. However, although the Rome III criteria are widely used in clinical studies, it is not used by most cliniciansIn fact, most primary care physicians are not aware of diagnostic criteria for IBS and about one third of secondary care doctors do not use them in practice6.
IBS patients are grouped on the basis of the most predominant bowel symptom as diarrhoea- predominant, constipation-predominant, a mixture of both diarrhoea and constipation, and un-subtyped IBS in patients with an insufficient abnormality of stool consistency to meet the criteria for the other sub-groups. Approximately one third of patients have diarrhoea- predominant, one third have constipation-predominant, and the remainder have a mixture of both diarrhoea and constipation. The classification of IBS patients into sub-groups is useful for clinical practice, but it is common for IBS patients to switch from one subtype to another over time. More than 75% of IBS patients change to either of the other 2 subtypes at least once over a 1-year period2,10.
Figure 1 - Rome III diagnostic criteria* for IBS 6
Recurrent abdominal pain or discomfort** at least 3 days a month in the past 3 months, associated with two or more of the following:
Improvement with defecation
Onset associated with a change in frequency of stool
Onset associated with a change in form (appearance) of stool
* Criteria fulfilled for the past 3 months with symptom onset at least 6 months before diagnosis
** “discomfort” means an uncomfortable sensation not described as pain
According to the National Institute for Health and Clinical Excellence (NICE), healthcare professionals should consider assessment for IBS if a patient presents with any of the following symptoms for at least six months11:
abdominal pain/discomfort
bloating
or a change in bowel habit
NICE has also given the following guideline pertaining to “red flag” indicators. All people presenting with possible IBS symptoms should be asked if they have any of the following indicators. Referral to secondary care should be made if any are present11:
unintentional and unexplained weight loss
rectal bleeding
family history of bowel or ovarian cancer
change in bowel habit to looser and/or more frequent stools persisting for more than 6 weeks in a person aged over 60 years.
Furthermore, all patients presenting with IBS symptoms should be appropriately assessed and clinically examined for the following 'red flag' indicators. A referral should be made to secondary care if any are present11:
Anaemia
Abdominal masses
Rectal masses
Inflammatory markers for inflammatory bowel disease
Serum CA125 should be measured in women with symptoms that suggest ovarian cancer
In addition, NICE have stated that IBS should be considered only if the person has abdominal pain or discomfort that is either relieved by defecation or associated with altered bowel frequency or stool form. This should be accompanied by at least two of the following four symptoms11:
abdominal bloating (more common in women), distension, tension or hardness
symptoms made worse by eating
passage of mucus
Other features such as lethargy, nausea, backache and bladder symptoms are common in people with IBS, and may be used to support the diagnosis.
According to NICE, patients who meet the IBS diagnostic criteria should have the following tests to exclude other diagnoses (Figure 2):
Figure 2 11 - Tests to exclude other diagnoses
Full blood count (FBC)
Erythrocyte sedimentation rate (ESR) or plasma viscosity
C-reactive protein (CRP)
Antibody testing for coeliac disease (endomysial antibodies [EMA] or tissue transglutaminase [TTG])
The value of serological tests for coeliac disease (EMA or TTG antibodies) in patients with IBS diarrhoea-predominant depends on the population and is generally considered cost-effective if the incidence of coeliac disease is above 1%. It is therefore likely to be beneficial in the United Kingdom, where up to 3% of cases of IBS diarrhoea-predominant in primary care have coeliac disease6.
The following tests are not necessary to confirm diagnosis in people who meet the IBS diagnostic criteria11:
Ultrasound
Rigid/flexible sigmoidoscopy
Colonoscopy/barium enema
Thyroid function test
Faecal ova and parasite test
Faecal occult blood
Hydrogen breath test (for lactose intolerance and bacterial overgrowth)
It is important to note that IBS is associated with several other conditions. At least half of IBS patients can be described as depressed, anxious, or hypochondriacal. In addition, between 20% and 50% of IBS patients have fibromyalgia. Furthermore, IBS is common in several chronic pain disorders, being present in 51% of patients with chronic fatigue syndrome, in 64% with temporomandibular joint disorder, and in 50% with chronic pelvic pain. The lifetime rates of IBS in patients with these syndromes are even higher. Patients with such co-morbidities generally have more severe IBS. A careful history to identify such associated disorders is helpful in identifying patients who are likely to have severe IBS and associated psychiatric disorder6.
Management
The treatment of IBS is determined by the patient’s most troublesome symptoms. Although there is overlap in the therapies offered to the different IBS sub-groups, treatment decisions are primarily based on the frequency and severity of symptomsThe management discussed in this section is largely based on the NICE guidelines11.
Dietary and lifestyle advice
People with IBS should be given information about the importance of self-help in effectively managing their IBS. This should include information on general lifestyle, physical activity, diet and symptom-targeted medication. Healthcare professionals should assess the physical activity levels of people with IBS (ideally using the General Practice Physical Activity Questionnaire). People with low activity levels should be given advice to encourage them to increase their activity levels. Healthcare professionals should also encourage people with IBS to make the most of their available leisure time and to create time for relaxation11.
Figure 3 summarises the general advice that should be given to patients regarding their diet and nutrition. If diet continues to be considered a major factor in a person's symptoms and they are following general lifestyle/dietary advice, they should be referred to a dietician for further advice and treatment, including single food avoidance and exclusion diets. Such advice should only be given by a dietician11.
Probiotics are live microorganisms which when taken in sufficient quantities, confer a health benefitPeople with IBS who try probiotics should be advised to take the product for at least 4 weeks while monitoring the effect. Probiotics should be taken at the dose recommended by the manufacturer11.
Figure 3 - Diet and nutrition should be assessed and the following general advice given 11
Have regular meals and take time to eat
Avoid missing meals or leaving long gaps between eating
Drink at least eight cups of fluid per day, especially water or other non-caffeinated drinks, for example herbal teas
Restrict tea and coffee to three cups per day
Reduce intake of alcohol and fizzy drinks
It may be helpful to limit intake of high-fibre food (such as wholemeal or high-fibre flour and breads, cereals high in bran, and whole grains such as brown rice)
Reduce intake of 'resistant starch' (starch that resists digestion in the small intestine and reaches the colon intact), which is often found in processed or re-cooked foods
Limit fresh fruit to three portions per day (a portion should be approximately 80 g)
People with diarrhoea should avoid sorbitol, an artificial sweetener found in sugar-free sweets (including chewing gum) and drinks, and in some diabetic and slimming products.
People with wind and bloating may find it helpful to eat oats (such as oat-based breakfast cereal or porridge) and linseeds (up to one tablespoon per day).
Healthcare professionals should review the fibre intake of patients, adjusting (usually reducing) it while monitoring the effect on symptoms. People with IBS should be discouraged from eating insoluble fibre (for example, bran). If an increase in dietary fibre is advised, it should be soluble fibre such as ispaghula powder or foods high in soluble fibre (for example, oats)
Pharmacological therapy
Healthcare professionals should consider prescribing antispasmodics for patients. These should be taken as required, alongside dietary and lifestyle advice. Laxatives should be considered for the treatment of constipation, but patients should avoid taking lactulose. Patients should be advised how to adjust their doses of laxative or antimotility agent according to the clinical response. The dose should be titrated according to stool consistency, with the aim of achieving a soft, well-formed stool (corresponding to Bristol Stool Form Scale type 4). Loperamide should be the first choice of antimotility agent for diarrhoeaOne advantage of loperamide is its peripheral site of action with little penetration of the blood brain barrier and thus, little potential for CNS side effects or habituation4.
Psychotropics possess a variety of peripheral and central effects which make them attractive treatments for IBS. These effects include modulation of pain perception, mood stabilisation, treatment of associated psychiatric conditions, and possible direct effects on GI motility and secretionHealthcare professionals should consider tricyclic antidepressants (TCAs) as second-line treatment for patients if laxatives, loperamide or antispasmodics have not helped. Treatment should be started at a low dose (5–10 mg equivalent of amitriptyline), which should be taken once at night and reviewed regularly. The dose may be increased, but does not usually need to exceed 30 mg11.
Selective serotonin reuptake inhibitors (SSRIs) should be considered only if TCAs have been ineffective. The anticholinergic effects of TCAs and their ability to prolong intestinal transit times are the reasons they are particularly preferred over SSRIs in IBS diarrhoea-predominant. Furthermore, given the propensity of SSRIs to commonly cause GI adverse events of nausea, vomiting, and diarrhoea, indicate that TCAs may have more utility in IBS diarrhoea-predominant than SSRIs12. Healthcare professionals should take into account the possible side effects when prescribing TCAs or SSRIs. After prescribing either of these drugs for the first time at low doses, the patient should be followed up after 4 weeks and then at 6–12 monthly intervals11.
Psychological interventions
Anxiety and depression are common in IBS and patients report a correlation between stress and their symptoms, providing a rationale for psychological therapyReferral for psychological interventions (cognitive behavioural therapy, hypnotherapy and/or psychological therapy) should be considered for people with IBS who do not respond to pharmacological treatments after 12 months and who develop a continuing symptom profile (refractory IBS).11 Hypnotherapy reduces patient anxiety and improves symptom control in the majority of patients with refractory IBS. The benefits extend well beyond symptom control and include improvements in quality of life and reduction in emotional distress13. Data from general practice shows that hypnotherapy is effective during the first three months, although the effect is less marked after that6.
Prognosis of IBS depends on the length of the history, those with a long history being less likely to improveFollow-up should be agreed between the healthcare professional and the patient based on the response of the person's symptoms to interventions. The emergence of any 'red flag' symptoms during management and follow-up should prompt further investigation and/or referral to secondary care11.
Acute gastrointestinal ulcerations and erosions (stress ulcers) are common in major trauma victims and in intensive care units. In fact, 75% of all critically ill admissions may have endoscopic evidence of gastroduodenal or upper gastrointestinal bleeding1. The bleeding could be in mutiple forms such as haematemesis,coffee ground aspirates, melaena, or haematochezia. Clinically significant haemorrhage causes hypotension and tachycardia and requires blood transfusion. Aggressive management is required in order to improve the outcomes of this potentially fatal complication. Prevention of stress ulcers helps reduce the morbidity and mortality of major bleeding2. Multiple causes may be responsible for gastrointestinal ulceration in patients with spinal cord injury1. Furthermore, steroids, thrombophylactic agents, anticoagulants and heavy cigarette smoking may act as predisposing factors to gastrointestinal bleed.
The aim of this study was to review our practice of stress ulcer prophylaxis after spinal cord injury and analyse morbidity and mortality associated with stress ulcer bleeding.
Patients and Methods
The Queen Elizabeth National Spinal Injuries Unit is the sole spinal cord injury centre in Scotland. It serves a population of 5.1 million and admits approximately 175 acute spinal injuries patients per year.
This study is retrospective. Only cases of life threatening or massive gastrointestinal haemorrhage were included. The period studied is between January 2006 and May 2008.
The department policy is to start all patients on Ranitidine 150 mg twice daily provided they are not on alternative medications before their admission, in which case the policy is to continue with the original pre admission medication.
Clinical notes of included patients were reviewed and information on patient’s demographics, cause and level of injury, past medical history, preadmission medications, clotting profile, prophylaxis, and management of bleeding were collected.
Results
A total of 360 patients were admitted. Out of them 19 (2 Female:17 Male) met the inclusion criteria as they suffered a life threatening GI bleed or major haemorrhage. The age range was 19 to 78 years with a mean age of 51.2 years. The majority of patients had a cervical spine injury (63%) followed by lumbar (21%) and thoracic (16%) spine injuries . Fall down stairs was the most common cause of injury occurring in 6 (31.5%) patients followed by road traffic accidents (26.3%) and fall from a height (21%). One patient suffered spinal injury whilst playing rugby and 1 patient suffered a cycling accident. The majority of cases (17 out 19) were admitted with acute injuries. However, 2 patients were admitted for complications of chronic injuries (one with a post surgical abscess and one with pressure sores). The various causes of spinal injuries are shown in table 1.
The American Spinal Injury Association (ASIA) impairment scales of all 19 patients are shown in Table 2. Associated injuries were encountered in 4 (21%) of patients. These associated injuries include sternum fracture, rib fractures, clavicle fracture, tendon injury and a calcaneum fracture. Significant past medical history was found in 14 (73.6%) patients whereas 5 (26.4%) did not have any previous medical illness. The list of all the significant past medical problems is shown in Table 3.
4 (21%) patients were already taking Omeprazole before admission, whereas 2 (10.5%) were taking Ranitidine and 1 (5.2%) patient was taking Lansoprazole.
7 out of 19 patients (36.8%) had either one or two episodes of significant coffee ground vomiting, 6 (31.5%) patients had an episode of haematemesis and 4 (21%) patients had combined coffee ground vomiting and haematemesis. Two (10.5%) patients had positive nasogastric aspirate for bleeding.
All 19 patients were started on intravenous Omeprazole and Sucralfate was added in 13 patients. Low molecular weight heparin, Ibuprofen and Aspirin was discontinued in all patients. Six (31.5%) patients were transfused 40 units of fresh frozen plasma and packed red cells (Figure 1). Eight patients (42.1%) underwent endoscopic treatment (Table 4) and 3 (15.7%) patients underwent laparotomy. There was one (5.2%) fatality reported.
Table 1:Causes of Spinal Cord Injury
Cause of Injury
Number of Patients
Percentage
Fall from stairs
6
31.5%
Road traffic accidents
5
26.3%
Fall from height
4
21%
Rugby injury
1
5.2%
Cycling accident
1
5.2%
Old injury admitted with skin problem
1
5.2%
Post surgical abscess
1
5.2%
Table 2:American Spinal Injury Association Impairment Scale
ASIA Impairment Scale
Number of Patients
Percentage
A= Complete: No motor or sensory function is preserved in the sacral segments S4-S5.
3
15.7%
B=Incomplete: Sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-S5
1
5.2%
C=Incomplete: Motor function is preserved below the neurological level, and more than half of key muscles below the neurological level have a muscle grade less than 3
10
52.6%
D=Incomplete: Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more
2
10.5%
E=Normal: motor and sensory function are normal
3
15.7%
Table 3: Previous Risk Factors in Spinal Cord Injured Patients with Stress Ulcers
Adverse Factor
Number of Patients with the Problem
Smoking
13 (68.4%)
Alcohol
5 (26.3%)
Reflux Oesophagitis
4 (21%)
Hypertension
3 (15.8%)
Diabetes Mellitus
3 (15.8%)
Hiatus Hernia
2 (10.5%)
Ischemic Heart Disease
2 (10.5%)
Asthma
1 (5.3%)
Duodenal Ulcers
1 (5.3%)
Anaemia
1 (5.3%)
Pyloric Stenosis
1 (5.3%)
Table 4:Endoscopic Findings, Procedures and Outcome
Number of Patients
Endoscopic findings, Procedures and Outcome
2
Bleeding Duodenal Ulcer injected with adrenaline Bleeding stopped
1
Had Endoscopy twice and bleeding Duodenal Ulcer injected with adrenaline on both occasions Continuous bleeding Underwent Laparotomy and over Sewing of the ulcer
1
Endoscopic findings were Oesophagitis, Hiatus Hernia and superficial ulcerations No procedure performed Treated Conservatively
1
Bleeding Duodenal Ulcer injected with adrenaline Continuous bleeding Prepared for Laparotomy but could not survive
1
Bleeding Duodenal Ulcer injected with adrenaline Bleeding stopped Barrett’s oesophagus was found and biopsied but biopsy results were negative
2
Bleeding Duodenal Ulcer injected with adrenaline Continuous bleeding Laparotomy and over sewing
Figure 1: Packed Red Cells and Fresh frozen Plasma Transfusion Units Patients
Discussion
The development of “stress” ulceration in the upper GI tract has been part of critical care folklore for a long time. In 1823 Curling described a series of severe duodenal ulceration associated with burns3; in 1832 Cushing reported ulcer disease associated with surgery and trauma4In the early years of intensive care, a strong association between severity of illness and the incidence of GI bleeds was established. Patients who had major bleeds had a high mortality rate and, consequently, prophylaxis against this complication has become a central issue in ICU care.
Gastrointestinal haemorrhage in patients with spinal cord disease was not reported until 1933 when Polstorff described gastric ulceration in an epileptic patient with spontaneous hematomyelia5. El Marsi and colleagues in 1982 reported 5.5% incidence of gastrointestinal bleeding in acute spinal cord injury patients6. Lesions of the spinal cord including traumatic, viral and infectious have been described with gastrointestinal bleeding7. It has been found mainly associated with injury to the cervical spinal cord8.
Controversy still exists regarding the appropriate prophylaxis of stress ulcers in trauma patients. There have been numerous randomized, controlled trials and several meta-analyses evaluating the use of drug therapy for stress ulcer prophylaxis in trauma patients9. One meta-analysis concluded that Sucralfate is as effective as pH-altering medications in preventing stress ulcer bleeding10. There is currently no large study that proves the superiority of proton pump inhibitors over H2- receptor antagonists for stress ulcer prophylaxis 11, 12. A survey of all the Level I trauma centers in the United States by Barletta et al9 revealed that H2-receptor blockers were the preferred agents. It is important to mention that some studies have questioned the need for prophylaxis altogehter but these were mainly retrospective studies that primarily evaluated medical patients as compared to trauma patients13, 14, 15, 16. The reported incidence of gastrointestinal haemorrhage in the medical literature in acute spinal cord injuries is between 5 and 22% 6, 17,18. In our study 19 out of 360 patients (5.2%) suffered a major bleed from the gastrointestinal tract. This incidence is similar to lower percentage reported in the medical literature17, 18. The strict adherence to the department policy of early prophylaxis for all admitted patients could be the reason for this low percentage of significant bleeding.
It is interesting to note that despite the increasing use of steroids and anticoagulants in the last decade, the incidence of gastrointestinal bleeding in acute spinal cord injuries have remained the same. The possible reason for this could be the increased awareness of this condition by spinal cord injury specialists and the regular prophylaxis initiated in the early phases of the injury. Our unit aims to admit patients as soon as they are fit for transfer and approximately 50% of our patients are transferred within the 48 hours of their injury from the peripheral hospitals. The referring hospitals are advised to commence H2 receptor antagonist at the time of referral.
Increasing use of antacids, H2 receptor antagonists and proton pump inhibitors in primary care19 may also contribute to the reduction of the incidence of gastrointestinal bleeding in patients with spinal cord injuries. This assumption is supported by our study as 7 (36.8%) patients in our study were already on these medications prior to their spinal cord injury.
The aetiology of gastroduodenal bleeding in spinal cord injury is multifactorial including, synergetic effects of the stress of the accident along with added effects of concomitant surgery, sepsis, unopposed reduced vagal tone and mucosal ischemia20. Also prolonged mechanical ventilation and coagulopathy has been shown to be associated with increased risk of stress ulcers in spinal injuries21.Other identified risk factors include multiple injuries, acute renal failure and use of high dose steroids22. Croft23 in 1977 first described the dynamics of the surface epithelium in the stomach. He reported that various agents were responsible for the damage of the gastric mucosa; stress, steroids and uraemia were causing decrease in the production of the mucosal cells; and alcohol and aspirin were causing increase in the shed of the gastric mucosal cells. This serious complication usually develops during the first four weeks after the spinal cord injury20,24. However, the period of greatest risk for gastrointestinal haemorrhage is reported to be between the fourth and tenth day after the injury8Nuseilben also reported focal ischemia of the gastric mucosa as early as 24 hours following the acute spinal cord injuries25.
Spinal injuries seldom occur in isolation; in a study by Silver26 in 1985 a 15% incidence of associated injuries was reported. The incidence of associated injuries in our study was 21%.
In a study by Walters and Silver1 all patients that bled had a combination of at least 3 risk factors. In our study 73.6% of patients who developed gastroduodenal bleeding had significant history of risk factors with smoking (68.4%) and alcohol (26.3%) being the major contributors. The other risk factors in our study were reflux oesophagitis (21%), hypertension (15.8%), diabetes mellitus (15.8%), hiatus hernia (10.5%) and ischemic heart disease (10.5%). However, only 7 (36.8%) patients had a combination of three or more risk factors at the time of admission. The reason for this decreased incidence as compared to Walter and Silver1 is difficult to explain.
In this study the majority of patients with gastrointestinal bleeding had cervical cord injuries (63.1%) as compared to thoracic and lumbar spine injuries. Kewalramani20 also showed predominance of gastrointestinal bleeding in patients with cervical cord injuries. This favours the neurogenic hypothesis as a major cause of gastrointestinal bleeding following the spinal injury 20.
Finally, there is no consensus, in literature, over the discontinuation of stress ulcer prophylaxis. Some studies suggest the continuation of prophylaxis throughout the duration of the critical illness or intensive care unit stay27, 28, 29.
Conclusion:
Gastrointestinal haemorrhage is a serious complication in spinal cord injured patients. Appropriate prophylaxis, early diagnosis and prompt management may help to avoid a possible fatality. Patients with spinal cord injury especially with cervical cord injury are at a high risk of gastrointestinal bleeding at all times even during period of rehabilitation30, 31. All acute spinal cord injured patients and patients who are undergoing rehabilitation who become critically ill may benefit from receiving chemical prophylaxis for stress ulceration. The duration of treatment is ill defined but is maybe better to continue while risk factors are present. Prevention could be the cornerstone in the overall management of this problem.
Grapefruit (Citrus paradise) is thought to have originated as a cross between the Jamaican sweet orange (Citrus sinensis) and the Indonesian pomelo (Citrus maxima) fruit. It was first bred in Barbados and brought to Florida in 1820s. Subsequently, different mutant and hybrid varieties were developed. Although the white and pink varieties were being popularly consumed, the ruby red variety has become very popular and commercially successful.
The taste is a mixture of the sweetness and tanginess of an orange and the sourness of a citrus fruit. It is a rich source of vitamins C and potassium. It is found to have antioxidant properties due to the presence of lycopene1and an ability to inhibit atherosclerosis due to the presence of pectin2,3. The seed extract is thought to have antimicrobial and antifungal properties.
With good publicity, marketing and coverage by health magazines, grapefruit juice has gained widespread use and in most Western Europe and America it is one of the common fruit juices consumed at breakfast. In the United Kingdom, in terms of fruit juice sales, it ranks second among citrus fruits and the fourth overall.4
Pharmacokinetic effects
The interaction of grapefruit juice with medication was first reported by Bailey et al in 1991 after their accidental discovery of up to four fold increase in the blood levels of filodipine when taken with grapefruit juice5. Further studies have identified similar interactions with more than 85 drugs6. The half life of the effects of grapefruit juice is estimated to be around 12 hours7, but these effects may last from 4 hours to 24 hours8. The effects are more pronounced with regular consumption of grapefruit juice prior to ingestion of the drug and there can be a cumulative increase in drug concentrations with continued grapefruit juice intake7,9.
As little as 200-250ml may be sufficient to induce its effects7,10. Some of the interactions involve medication that have narrow therapeutic window and can therefore cause potent adverse effects such as torsade de pointes, rhabdomyolysis, myelotoxicity, respiratory depression gastrointestinal bleeding, nephrotoxicity and sudden cardiac death.6 There is a lack of awareness among both doctors and patients about its effects and interaction with various medications.
Mechanism of action
These pharmacokinetic interactions with grapefruit juice are more observable in drugs with high first pass metabolism and in those with an innate low oral bioavailability. The oral bioavailability of affected drugs is increased but their half life usually remains unaltered11,12. Grapefruit juice is associated with the inhibition of Cytochrome P450 enzyme system, particularly the CYP3A4 enzyme7. The CYP3A4 enzyme is present both in the liver and intestinal mucosa. Once the drug is taken up by the mucosa, the susceptible drug may be metabolised by the CYP3A4 or pumped back into the intestine lumen by P-glycoprotein. The observed effects of grapefruit juice are thought to be mainly due to the inhibition of intestinal CYP3A4 activity, which leads to decreased first pass metabolism and hence increased bioavailability. This inhibitory action is fairly quick and may be due to the rapid degradation of the enzyme or any decrease in its production from the mRNA. The production of mRNA itself from DNA is not thought to be affected13. The susceptibility varies between individuals depending upon their genetic expression of CYP3A4, the effects being more prominent in those with high small intestinal CYP3A4 content7, 14.
The effect of grapefruit juice on the P-glycoprotein is unclear. The activation of P-glycoprotein pumps the drug back into the intestinal lumen which should reduce bioavailability and similarly the inhibition of P-glycoprotein increases the bioavailability. Some studies suggest that the inhibition of P-glycoprotein is the mechanism responsible for the increased bioavailability of certain drugs like cyclosporine15,16.
The active ingredients responsible for interactions of grapefruit juice with medication are not clearly identified. The compounds exerting this action are thought to be either the flavanoids such as naringin and naringinen17,18,19,20 or the furanocoumarins such as bergamottin and its derivatives21,22,23,24, but there is no clear consensus.
Drug interactions
Table 1 below lists some of the commonly used drugs whose bioavailability is affected by grapefruit juice. Although the best known interactions have been mentioned in the table, there are many other drugs like carvedilol, estrogens, itraconazole, losartan and methyl prednisolone whose bioavailibility is increased by grapefruit juice and the adverse effects are not yet clear.
Table 1: Potential risk of drug interactions with grapefruit juice6, 7,13,25,26,27
Risk of Interaction
Group
Drug
V High
High
Mod
Anaesthetic
Ketamine
+++
Anaesthetic
Alfentanil
++
Fentanyl
++
Antiarrhythmic
Dronedorone
+++
Amiodorone
++
Quinidine
+
Anti-Cancer
Dasatanib
++
Everolimus
++
Nilotinib
++
Pazopanib
++
Sunitinib
++
Vanetanib
++
Antidepressants
Buspirone
++
Sertraline
+
Clomipramine
+
Antiemetic
Domperidone
+++
Antiepileptics
Carbamazapine
++
Anti-HIV
Maraviroc
+++
Ripivirine
++
Anti-infective
Erythromycin
++
Quinine
++
Primaquine
++
Antiplatelet
Clopidogrel
++
Antipsychotics
Pimozide
++
Quetiapine
++
Ziprasidone
++
Benzodiazepines
Midazolam
+
Diazepam
+
Triazolam
+
Ca-channel bolckers
Felodipine
+
Nifedipine
+
Immunosuppressants
Cyclosporin
++
Tacrolimus
++
Sirolimus
++
Opiods
Oxycodone
++
Methadone
++
Statins
Simvastatin
+++
Atorvastatin
++
Urinary Tract
Solifenacin
+
Fesoterodine
+
Darifenacin
+
Tamsulosin
+
Implications on clinical practice
Clinicians should make themselves aware and educate their patients of these potential interactions, keeping in mind the individual variations in susceptibility. This may be particularly important for medications that have a very narrow therapeutic window, medication that have an innate low oral bioavailability and a high first pass metabolism mainly via CYP3A4.
A patient may develop exceptional beneficial effects or equally, significant adverse effects should he start consuming grapefruit juice mid- treatment. Conversely, a drop in efficacy of a drug is also possible, should a patient using grapefruit juice on a regular basis, stops it suddenly.
To achieve steady concentration of the medication and avoid such potential effects, it may be best to advise patients to avoid consuming grapefruit juice if there is a potential of interaction. The half life of the effect of grapefruit juice appears to be around 12 hours and therefore, it is advisable to discontinue grapefruit juice 72 hours prior to starting any drug with potential interactions. 8,9
Due to the prolonged effect of CYP3A4 inhibition which may last up to 24 hours, it is not possible to avoid these interactions by separating the times of drug and grapefruit juice consumption.8,9
There is more research needed to clarify the mechanism of action and to determine the active ingredients. The identification of the active ingredient can allow oral administration of drugs that undergo CYP3A4 mediated high first pass metabolism because of which currently, they can only be given systemically.
In light of the possible increase in bioavailability of specific drugs, although it might be possible for patients to use this to their advantage in reducing the dose of their medication under medical supervision, it is perhaps too early to recommend the use of grapefruit juice as an adjunctive or augmentation strategy.
The incidence and prevalence of hypertension is rife among first and second world countries and arguably, could be labelled the most common chronic disease in the UK1. It is estimated that a quarter of all adults in the UK have hypertension2. This is alarming in light of the incredible contribution of hypertension to mortality and morbidity. Evidence shows that for each 2mmHg rise of systolic blood pressure, mortality from ischaemic cardiac events rises by 7% and mortality from ischaemic intracranial events rises by 10%3-4. The key to reversing this lies in diagnosing hypertension accurately and quickly and knowing how to best treat each patient.
Understanding hypertension
It is still not entirely clear what mechanisms cause hypertension. Evidence has proven that systolic blood pressure increases in a linear fashion with age, which is due to the loss of elastic tissue in arteries with age1,5. This is known as ‘essential hypertension’. The majority of patients who are diagnosed with hypertension have ‘essential hypertension’, in other words, there is no clear cause found besides increasing age1-2. Research has shown that other factors can be associated with hypertension but alone may not necessarily cause it. Unalterable risk factors include genetic predisposition, age, sex and race. Other factors which have proven to raise blood pressure include environmental factors such as lifestyle and diet, obesity (randomised control trials have shown that a weight loss of one kilogram can be attributed to one mmHg fall in diastolic blood pressure5), excessive alcohol intake, smoking, stress at work or in the home, socio-economic status and recent major life events1-2,6.
How to take the perfect blood pressure
In the clinic setting, make sure the patient is relaxed, sit the patient comfortably with their arm outstretched, resting on the table and wait a few minutes. Make sure the sleeves are not too tight as this will alter the readings1,5. Be careful that the blood pressure cuff is the correct size for the patient as small cuffs can give a false high reading for larger patients and larger cuffs can give a false low reading for smaller patients3,5. Check the pulse is regular as irregular pulses can give incorrect readings from automated devices - if in doubt perform it manually5. Take the blood pressure in both arms and repeat several times, discard the first reading and always record the lowest reading in the patient’s file1.
The well recognised ‘white coat syndrome’ has a prevalence of about 10% in the UK and according to NICE data, the syndrome can cause a difference of 20/10mmHg between readings in a clinical setting and those at home1,3,5. In light of this, NICE altered the guidelines in 2011, stating that any patient with a reading close to 140/90mmHg is to be sent home with an Ambulatory Blood Pressure Monitor (ABPM)3. This is a device attached to the patient for a minimum of 24 hours and it records the patient’s blood pressure every 30 minutes of the patient’s waking day. The idea behind this is to rule out any ‘white coat syndrome’ and to get a range of readings as the patient goes about their usual day to day activities. In this way, when the readings are analysed (an average of at least 14 readings are taken by the clinician), it confirms diagnosis immediately and treatment can be initiated1,3.
The value of repeated measurements in different settings has been shown in evidence from as early as the 1970s2,5. Research has also shown that patients usually have a high blood pressure reading initially which drops after subsequent measurements, hence the new guidelines are in place to allow for a range of readings before diagnosing and treating hypertension1,3.
Investigations
While the patient is still in the clinic, assess the patient’s overall cardiovascular risk score using the cardiovascular risk assessment tool3. Perform a thorough physical examination, including looking for evidence of target organ damage, for example, left ventricular hypertrophy, renal disease, peripheral vascular disease and changes in the retina from raised blood pressure1,3,5. If there is suspicion of hypertension, send the patient home on an ABPM3. While waiting for the results of the ABPM, any patient under investigation for hypertension needs to have a baseline set of tests1,7-8. This includes a full blood count, renal function tests, liver function tests, a fasting glucose and cholesterol blood test, an ECG (electrocardiogram) and a urine dip. These tests are a basic screen for assessment of target organ damage6,9. If these investigations are not adequate, a patient can be referred for more extensive investigation for target organ damage, for example, an echocardiogram or a renal ultrasound/angiography1,3,5.
Any patient that is young or presenting with persistent hypertension, especially that which does not respond to treatment, needs further investigation for other causes, such as renal disease, adrenal disease, alcoholism or steroid use (not to forget the oral contraceptive pill can also cause hypertension1,7,9.
In general, a patient should be treated if their blood pressure readings are persistently 140/90mmHg or higher. For those that have borderline readings, for example, 135/85mmHg, clinicians must assess their cardiovascular risk score and look for target organ damage. If there is evidence for either of these, a patient should be started on treatment immediately1.
Treatment
Non-pharmacological
First line treatment of hypertension is always non-pharmaceutical; also known as ‘lifestyle changes’ 1,3,5,9. Attempt to find out the details of the patient’s diet, weight, employment, stress levels at work/home, exercise, alcohol intake and smoking habits. Once established, assist the patient in altering their lifestyle choices in order to lower their blood pressure. Patients often feel overwhelmed and many benefit from group activities, such as smoking cessation and weight loss groups3. Other ideas include a dietician referral, counsellors if they are struggling with motivation and low moods, gym sessions/personal trainers. Encourage the patient in that if they succeed in altering their lifestyle and therefore bringing down their blood pressure, they can avoid prescription medication.
Lifestyle changes can delay hypertension for many years but if the blood pressure continues to creep upwards in subsequent multiple visits and lifestyle options have been exhausted, it would then be appropriate to start pharmacological management1,3,5.
Pharmacological Treatment
In general terms, always start with monotherapy and increase the dose according to patient response. According to NICE guidelines from 2011, if a patient is over 55 years of age and/or Afro-Caribbean in origin, start with a calcium channel blocker, such as Amlodipine3. If these are contra-indicated, start with a thiazide diuretic3. In regards to thiazide diuretics, the new NICE guidelines state that Chlortalidone (12.5–25.0 mg once daily) or Indapamide (1.5 mg modified-release or 2.5 mg once daily) should be used in preference to what clinicians have been prescribing for years, namely Bendroflumethiazide and Hydrochlorothiazide3. For those who are already on these conventional thiazide diuretics, NICE state that if the patient’s blood pressure is stable, to continue with Bendroflumethiazide or Hydrochlorothiazide3.
Patients diagnosed with hypertension who are under 55 years of age, should be started on an ACE inhibitor (Angiotensin Converting Enzyme inhibitor), for example, Ramipril3, but if this is not tolerated, replace it with an ARB (Angiotensin II Receptor Blocker) such as Losartan3.
Review the patient every few weeks initially and extend the reviews to 6 months once the blood pressure is within therapeutic range6.Do not forget to check the patient’s renal function in the first few months of starting a new drug and always be aware that if a patient’s blood pressure drops drastically after starting an ACE inhibitor this suggests underlying renal disease and must be investigated1,3,5,9.
Continue to titrate the dose of the drug until the patient’s blood pressure is satisfactory. Consider adding in a second agent when the patient is nearing maximum dose of the first agent and the blood pressure is rising again3,5. Depending on what the patient is on, add in either an ACE inhibitor, ARB or a calcium channel blocker, for example, if patient is on Ramipril, add in Amlodipine and vice versa3. If a calcium channel blocker is not tolerated as second line, consider using thiazide diuretics. Afro-Caribbean patients who are already on calcium channel blockers, add in an ARB, rather than an ACE inhibitor3.
Following that, if the blood pressure is still not within therapeutic range, consider adding in a third agent or alternatively, discontinue the first agent and continue with the second and add a third from among an ACE inhibitor, ARB or calcium channel blocker. Consider a thiazide diuretic if patients are intolerable to any of the above3.
Beta-blockers should not be considered in treating hypertension, according to NICE, unless the patients are very young or intolerant to ACE inhibitors, ARBs or calcium channel blockers3.
Beware and monitor closely any elderly patients who are on antihypertensives as the physiology of ageing interferes with the drugs, for example, decreased clearance of drugs from the kidney or liver, decreased sensitivity to baroreceptors (postural hypotension), chronic sodium retention and reduced cardiac reserve. Do not forget communication and compliance issues with the elderly also1,7.
Make sure there is an annual review for each patient that has been diagnosed with hypertension in order to get blood pressure readings, medication review and how the patient is coping with lifestyle changes or side effects of the antihypertensives.
When to Refer
Resistant hypertension is defined as a patient remaining hypertensive despite being on triple or quadruple drug therapy3,7. Consider starting a low dose of Spironolactone (if the serum potassium is less than 4.5mmol/l) and refer to a specialist for advice3-4.
If subsequent readings are 180/110mmHg or more, start antihypertensives immediately and refer the patient to hospital. Also refer immediately if retinal haemorrhages or papilloedema are seen1,3.
Summary
If a patient is suspected to have hypertension, send them home with an ABPM and perform baseline tests1,3.
Start treatment if blood pressure is 140/90mmHg and ABPM average is 135/85mmHg and/or patient has one of the following:
target organ damage
established cardiovascular disease
renal disease
diabetes
10-year cardiovascular risk equivalent to 20% or greater (NICE guidelines, 2011)3
Start on monotherapy and review every few months, until blood pressure is stable3.
Review yearly after stability has been reached and consider adding in further antihypertensives if the blood pressure rises again.
Book patients in for annual reviews of end organ damage as this is an excellent overview of disease progression.
Hypertension is to be respected in light of its incredible contributor to morbidity and mortality. Never underestimate the importance of keeping a patient’s blood pressure within the desired range4.
Total knee replacement (TKR) is an effective and cost-effective intervention for advanced osteoarthritis (OA). Pain is the main indication for the procedure, and the majority of patients undergoing a TKR gain significant pain relief 1-3.
However, an important minority of those who undergo a TKR have persistent pain in the operated knee 4. Baker showed that 19.8% of patients with data in the National Joint Registry had persistent knee pain, and 18.2% were dissatisfied with the procedure 5. Anderson, in a study of 98 patients, found that 8.1% claimed that the operated knee was worse at follow-up (2-3 years after surgery) than prior to surgery and 9.2% were dissatisfied Wylde et al reviewed the available literature in 2009, and found that 10-20% of patients report significant pain in the operated knee, and that the patient centred outcomes of TKR appear to be considerably worse than those of total hip replacement, where as implant survivorship figures are fairly similar 7.
There are numerous possible causes of pain after a TKR, including anterior knee pain arising from the patello-femoral joint and extensor apparatus, prosthesis loosening, or infection. Other likely causes include soft-tissue periarticular problems, referred pain, pain sensitisation, or neuropathic painBecause of the risk of infection, and the possible need for further surgery, orthopaedic surgeons are generally keen to investigate these patients thoroughly and exclude surgical causes of the problem. However, there seems to be background pain vulnerability in the knee causing this high incidence of post-operative pain. The pain itself clearly needs appropriate management but patients also need surgical evaluation to exclude important reversible causes.9
In spite of this being a sizeable and worrying problem in orthopaedics, very little has been written about the assessment or management of these patients. No protocols or guidelines are available and the costs of management have not been explored.
In this paper we describe the first case series of patients with chronic knee pain after a TKR, and document the investigations and treatment undertaken, and the direct financial costs of their care to the NHS Trust in which they were seen.
RD&E provides an Arthroplasty tertiary referral service for a large area but is a large District General Hospital and as such the costs and results we report should be representative of most trusts within the UK
Methods:
A specialist service for revision knee surgery is available at the Royal Devon and Exeter Hospital, resulting in the referral of patients with problems in a knee after a TKR. A registry of such patients has been established at the hospital. The data presented here is based on examination of the records of 41 of these patients. These were patients with a painful TKR who had been referred to one of the authors from Orthopaedic specialists in various institutions including the resident hospital.
The notes of these patients were analysed to ascertain the number of appointments patients’ had attended to address the TKR problem, and what investigations and treatments had been undertaken for that problem both by the originating surgeon and by the revision knee specialist.
In addition data was obtained from the Trust on the current costs of the clinic appointments, investigations and any treatment or interventions undertaken.
Results:
The 41 patients studied included 27 women and 14 men, with a mean age of 63.9 years (range 49-81) at time of initial TKR. In the year 2009, 536 TKR’s were performed in the trust with an average age of 70.5 years (range 37-94) with 298 females and 238 males.
Investigations were commenced for abnormal pain post total knee replacement on average 15 months (range 1-84) after their knee replacement. Appointments and investigations were undertaken over a mean time of 20 months from initial investigation (range 7-45).
Neuropathic pain was diagnosed in 6 patients and instability was identified as a cause in 5 patients. 4 patients suffered aseptic loosening and no diagnosis was made in 26 patients (63%).
Table 1 shows the average number of appointments attended and investigations undertaken on these 41 patients.
Data on the costs of these appointments, investigations and treatments to the local NHS Trust are presented in Table 2.
Table 1- Number of appointments and investigations per patient with a painful TKR
Ave appt/pt
Range
Orthopaedic appointment
4.37
2 – 11
Pain team appointment
2.05
0 – 6
Physiotherapy appointment
3.05
0 – 12
Hydrotherapy appointment
0.8
0 – 8
ESR/CRP/WCC/PV
7.75
2 – 38
X-rays
7.92
2 – 35
MRI/CT/Bone scan
0.41
0 – 2
Aspiration/Arthroscopies
0.51
0 – 3
Table 2 – Costs of appointments, investigations and treatments per patient
Ave cost/pt (£)
Orthopaedic appointment
370
Pain team appointment
235
Physiotherapy appointment
45
Hydrotherapy appointment
68
ESR/CRP/WCC/PV
21
X-rays
*
MRI/CT/Bone scan
70
Aspiration/Arthroscopies
1529
Operative Costs
2624
Drug Costs
174
Average cost/patient
5136
*= X-ray radiographs costs were insignificant and not charged to the NHS Trust
The outcomes of these 41 patients included medical management alone in 19 (14 of whom reported significant improvement) and further surgical interventions in 22 (14 of whom reported improvement). The calculated direct costs of investigation and management of those treated solely medically (i.e. non-surgically) was £190/patient, while the cost of those treated surgically was £5,051/patient. This is shown in table 3.
Table 3 – Comparison of operative versus non-operative costs
Average Surgical intervention cost/pt
Average drug therapy cost/pt
Total cost/pt
Operative patients (22)
4891.09
160.22
5051.31
Non-operative patients (19)
N/A
190.63
190.63
Discussion:
We have analysed the management of a case series of patients with persistent pain in the knee after TKR. The results show that most of the 41 people studied attended numerous appointments with different specialists, and had the same investigations (serology and x-rays) repeated on many occasions over a relatively short period of time (less than 2 years), often before referral to a surgeon with a specific revision knee interest. We have also shown that the investigations and treatment undertaken were costly to the NHS, particularly if specialist imaging investigations (CT or MRI) or further surgical procedures (including aspiration or arthroscopy) were undertaken. The costs to the patients of the numerous appointments and repeated investigations have not been included, but are likely to have been considerable.
The fact that many different appointments were offered, and many investigations repeated, along with the wide range of different approaches to the different patients, are indicative of the absence of clear patient pathways or of a co-ordinated clinical service for these patients. Patients were seen by orthopaedic surgeons, pain specialists and physiotherapists, but definitive diagnoses or management plans did not often result from these appointments, and investigations were often repeated unnecessarily. We do not believe that this situation is unique to our area, as there are no clear guidelines or protocols to help us know how best to investigate or manage these patients before referral and the natural history of the condition is unknown.
The investigations carried out most frequently were serological tests (ESR and CRP) to try to exclude infection, and x-rays to look for prosthesis loosening or other bony problems. Previous work has shown that a single test of ESR greater than 22.5 or CRP greater than 13.5, in this situation, has a sensitivity of 0.77 and a specificity of 0.93 for the diagnosis of infection Repeating these tests offers little help, and if these were positive it would seem more appropriate to proceed to joint aspiration 11, 12-15.
Similarly, there is little point in doing more than one x-ray study a year, as the rate of change in radiographic findings is slow. If a bone problem is suspected, other more sophisticated imaging modalities can be used 16-18.
The cost data obtained from our Trust show that high costs are incurred from new clinic referrals and visits, sophisticated imaging procedures (CT, MRI and bone scans), and surgical procedures – in particular revision surgery. These high costs of investigations would indicate that patients with a painful TKR would be more appropriately investigated and managed by specialist centres with early and meticulous evaluation by surgeons with a special interest in revision knee surgery.
The surgical costs of management of painful TKR’s dwarf the amount of money spent on medical (i.e. non-surgical) approaches. This considerable difference suggests that it is of paramount importance to manage the pain early, irrespective of whether surgery is required. Good pain management will allow the surgeon, and particularly the patient, to evaluate the problem in a clearer manner, weighing up the treatment options and making a decision from a more balanced position.
According to data from the National Joint Registry, over 53,000 TKRs were performed in NHS hospitals in England and Wales in 2009 19. Using the estimates of Baker, and Wylde and others on the numbers of these patients who are in pain or dissatisfied, we calculate that over 10,000 patients each year, in this country alone, are acquiring the problem of persistent pain in a TKR ,7This represents a huge public health problem, and one that, if our Trust’s cost figures are representative, is probably costing the NHS over £10 Million/annum. In view of that, we believe that this issue needs urgent attention from the research community and health care providers.
Figure 1 – Algorithm for assessment of a patient with a painful TKR
Our recommendation is that research is undertaken to document the natural history of pain in a TKR knee, differentiate the main causes of this pain, and develop simple algorithms to help clinicians make the correct diagnosis. We suggest a protocol that can be utilised by healthcare professionals to investigate painful TKR’s to allow correct assessment and diagnosis (Figure 1). We believe that health care providers in major orthopaedic centres should set up interdisciplinary clinics in which surgeons, pain specialists and physiotherapists can work together to help investigate and manage these patients.
Injuries in children are common.1 In the UK, incidence is found to be 20.2 fractures per 1000 per year. The peak age of incidence is on average of 9.7 years .2 Up to 42 per cent of boys and 27 per cent of girls will sustain at least one fracture during the paediatric age. 3
A study conducted in Northern Sweden in the age group of 0 - 19 years showed that there is a rise in injury related visits to emergency department over the years. Fractures and dislocations accounted for 21.4 per cent of the cases.1Consequently, this will put a pressure on fracture clinics as new cases take a considerable in fracture clinic.
The purpose of this audit was to assess the pattern of new cases referred to fracture clinic at a large paediatric university teaching hospital
Materials and Methods
This prospective audit was carried out over a four-week period in May and June of 2010 and it was approved by the institutional clinical audit department. There were a total of 18 working days. A total of 864 patients were seen in the fracture clinic during this period, which included 310 new cases and 554 follow up cases. Data was collected from the fracture clinic patient list for the respective days and the new patient list was extracted from this. Using the picture archiving and communication system (PACS), the radiographs and reports were analysed to collect the data regarding the fracture sustained.
Results
Total number of cases seen during the 4 week period were 864, which included 310 new cases and 554 follow up cases. Two hundred and ninety two cases out of 310 were analysed, as 18 cases did not have radiographs available.
There were 170 males and 140 females. The average age was 9 years (range 1 month to 16 years).
One hundred and seventy seven (61%) showed fractures. One hundred and one (34%) cases did not have any fractures and 14 (5%) were suspected fractures.
The following figure 1 shows the pattern of cases on each working day. Those, which are left blank, are non working days or cancelled clinics. The average number of cases seen per day were 48 and of these, the average of new cases seen were 17.2 and the average number of follow up cases seen were 30.7.
As shown in figure 2, fractures of the distal radius and ulna were the predominant cases (23%) followed by hand fractures (15%). Other fractures included: lower limb excluding foot [23 (8%)], elbow and humerus [14 (5%)], clavicle [11 (4%)], foot [12 (4%)] and others [5 (2%)].
Further analysis of the fractures sustained showed that forearm injuries were the predominant cases and majority of them were buckle or greenstick fractures. The detailed distribution is shown in the figure 3 below.
Figure 1 showing the daily pattern of cases
Figure 2 showing the area involved
Figure 3 showing the pattern of fracture
Discussion
Fracture clinics are a part of any trauma and orthopaedic department. One must consider the benefits of providing such a service and routine audits are necessary to improve the efficiency, accuracy and above all, best possible patient care.
Although there is evidence that simple fracture like buckle fractures of the distal radius do not need orthopaedic input and can be safely treated in emergency department using a splint, and can be discharged without follow up 4, concerns have been raised against the possibility of a misdiagnosis and providing patient information 5.
Radiographic interpretation is often done by junior doctors in the emergency department. Guly6 demonstrated that there is significant issue in misreading radiographs and missing the injuries. The second problem was noted to be not requesting a radiograph. It has been suggested that better training in interpreting radiographs and rapid reporting by radiologist could solve this problem.
Others have adapted local departmental audits and guidelines and have shown to reduce the risk.7
Another possibility is a rapid review of radiographs by orthopaedic consultants on the same day as suggested by Beiri et al.8 But if the hospital is covering a large population area including peripheral walk in centres, this becomes difficult due to accessibility and logistic reasons.
Toeh and collegues9 investigating attitudes of parents towards paediatric fracture clinic found that mothers were the one who predominantly accompanied their children and most children had to take time off school to attend the clinic. It was also interesting to note that parents perception of severity of injury prompted attendance at follow up clinics.
In another study, ninety nine per cent of the parents thought attendance at the fracture clinic was important. However, when evaluating the socio economic costs, they found that this led to loss of 0.25 working days of parents, 0.18 daily wages and 0.54 schooling days per visit.1
A combination of factors may lead to fracture clinic appointments especially in paediatric population. Departmental protocols and guidelines may help in reducing the fracture clinic visits, however careful consideration must be given while drawing up these for a successful outcome.
Inappropriate referrals lead to usage of time and resources, which can lead to delay of service meant for those in need of specialist opinion. In our audit, 34% of the cases seen did not have any fractures and 5% were suspected fractures.
One of the drawbacks of this audit includes lack of case note review of those cases where fractures were not present. It would have been ideal to investigate the nature of cases seen, and whether this was treated as soft tissue injuries, or seen just for reassurance or used as a safety net.
The following recommendations could be used as possible solutions to decrease inappropriate referrals to fracture clinic.
If the patient is seen in Accident and Emergency (A&E), where appropriate and when diagnosis is in doubt, there should be an opportunity for the patient to be seen or discussed with a more senior doctor in A&E.
With regards to Peripheral Walk In Centres, there should be an opportunity to discuss it with the on call Orthopaedic team with the integration of PACS, so that images are readily available for viewing, and to consider rapid reporting of images.
The use of Specialist Physiotherapists for soft tissue injuries in A&E with follow up in physiotherapy clinics were shown to have high patient satisfaction rates and reduce fracture clinic follow up. Similar strategy could be considered.11, 12
Conclusion
This study has shown that although the majority of patients needed treatment, a significant number (34%) did not have fractures. Considerable amounts of time can be saved, especially in a busy fracture clinic if unnecessary appointments could be avoided. It would also benefit patients by avoiding unnecessary visits to the fracture clinic. A repeat study following the consideration of recommendations would reveal any benefit of such a strategy.
Lumbar punctures are commonly performed by both medical and anaesthetic trainees but in different contexts. Medically performed lumbar punctures are often used to confirm a diagnosis (meningitis, subarachnoid haemorrhage) whilst lumbar puncture performed by anaesthetists are usually a precedent to the injection of local anaesthetics into cerebrospinal fluid for spinal anaesthesia. The similarity relies on the fact that both involve the potential for iatrogenic infection into the subarachnoid space. The incidence of iatrogenic infection is very low in both fields; a recent survey by the Royal College of Anaesthetists1 reported an incidence of 8/707 000 whilst there were only approximately 75 cases in the literature after ‘medical’ lumbar puncture.2 However, the consequences of iatrogenic infection can be devastating. It is likely that appropriate infection control measures taken during lumbar puncture would reduce the risk of bacterial contamination. The purpose of the present study is to compare infection control measures taken by anaesthetic and medical staff when performing lumbar puncture.
Method
A survey was constructed online (www.surveymonkey.com) and sent by email to 50 anaesthetic and 50 acute medical trainees in January 2011. All participants were on an anaesthetic or medical training programme and all responses were anonymous. The survey asked whether trainees routinely used the following components of an aseptic technique3 when performing lumbar puncture:
Sterile trolley
Decontaminate hands
Clean patient skin
Apron/gown
Dressing pack
Non-touch technique
Sterile gloves
No ethical approval was sought as the study was voluntary and anonymous.
Results
The overall response rate was 71% (40/50 anaesthetic trainees and 31/50 medical). All anaesthetic trainees routinely used the components of an aseptic technique when performing lumbar puncture. All medical trainees routinely cleaned the skin, decontaminated their hands and used a non-touch technique but only 80.6% used sterile gloves. 61.3% of medical trainees used a sterile trolley, 38.7% used an apron/gown and 77.4% used a dressing pack.
Discussion
This survey shows that adherence to infection control measures differ between anaesthetic and medical trainees when performing lumbar puncture. The anaesthetic trainees have a 100% compliance rate compared to 80% for the medical trainees for all components of the aseptic technique. Both groups routinely cleaned the patient’s skin, decontaminated their hands and used a non-touch technique. However, there were significant differences in the use of other equipment, with fewer medical trainees using sterile gloves, trolleys, aprons and dressing packs.
Although the incidence of iatrogenic infection after lumbar puncture is low, it is important to contribute to this low incidence by adopting an aseptic technique. There may be differences with regards to the risks of iatrogenic infection between anaesthetic and medical trainees. Anaesthetic lumbar punctures involve the injection of a foreign substance (local anaesthesia) into the cerebrospinal fluid and may therefore carry a higher risk. Crucially however, both anaesthetic and medical lumbar punctures involve accessing the subarachnoid space with medical equipment and so the risk is present.
There are many reasons for the differing compliance rates between the two specialties. Firstly, anaesthetic trainees perform lumbar punctures in a dedicated anaesthetic room whilst the presence of ‘procedure/treatment rooms’ is not universal on medical wards. Secondly, anaesthetic trainees will always have a trained assistant present (usually an operating department practitioner, ODP) who can assist with preparing equipment such as dressing trolleys.
The mechanism of iatrogenic infection during lumbar puncture is not completely clear.4 The source of microbial contamination could be external (incomplete aseptic technique, infected equipment) or internal (bacteraemia in the patient); the fact that a common cause of iatrogenic meningitis are viridans streptococcus strains5 (mouth commensals) supports the notion that external factors are relevant and an aseptic technique is important.
It is very likely that improved compliance amongst acute medical trainees would result from a dedicated treatment room on medical wards, but this is likely to involve financial and logistical barriers. The introduction of specific ‘lumbar puncture packs’, which include all necessary equipment (e.g. cleaning solution, aprons, sterile gloves) may reduce the risk of infection; the introduction of a specific pack containing equipment for central venous line insertion reduced colonisation rates from 31 to 12%.6 The presence of trained staff members to assist medical trainees when performing lumbar puncture may assist in improved compliance, similar to the role of an ODP for anaesthetic trainees.
The main limitation of this study is that the sample size is small. However, we feel that this study raises important questions as to why there is a difference in infection control measures taken by anaesthetic and medical trainees; it may be that the environment in which the procedure takes place is crucial and further work on the impact of ‘procedure rooms’ on medical wards is warranted.
On discharge from hospital, secondary care providers have a duty and obligation to communicate with primary care provides – particularly the general practitioner – to give information regarding the reasons for admission, results of investigations, procedures performed, treatment instigated and importantly follow-up management. Therefore the transition of information between secondary and primary care is vital for care management and hence patients’ safety.
This information is shared in the form of a ‘discharge summary’. It is the responsibility of the secondary care team to provide this. The level of detail given has been found to vary not just between different NHS trusts or hospital but also between different wards and individual doctors completing the discharge summary – this can create many problems as communication plays a pivotal role in patient care.
The information given in the discharge summary is all that a patients’ GP knows in regards to their hospital admission and management. A discharge summary is effectively a form of ‘handover’. A hospital physician may instruct the GP to do certain things in regards to follow-up; for example check blood results, review results of investigations arranged as outpatients or simply review the patient clinically. The more information that is transferred across from secondary to primary care the more awareness the GP has to what has happened and what needs to happen, which leads to better patient care.
A discharge summary can also be a valuable document for when a patient is admitted to hospital; if their notes are not available a past discharge summary will provide useful information (re. past medical history and drug history in particular) to the medical team who may have no prior knowledge of the patient, this is invaluable if it not possible to take a history from a patient and is also useful in directing investigations if a patient has been admitted with the same complaint(s). Of course this depends on the patient having a copy of the discharge summary with them on admission or the ability to access previous discharge summaries electronically.
Good documentation is vital in the healthcare setting. All documentation, no matter in what form, must be clear, accurate and legible. Any type of document is useless if it cannot be read. The GMC and Royal College of Physicians stress the importance of documentation1, 2.
The importance of the discharge summary has been highlighted in the last few years. There has been a move from the traditional hand-written discharge summary – commonly referred to as the TTA (to take away) – to the use of computer software providing an electronic discharge summary (EDS). The latter not only provides more detail but also aims to deliver it to the primary care setting in a timelier manner; for example, in the future, once all EDSs are completed at Barking, Havering and Redbridge University Hospitals NHS Trust there are plans for them to be automatically emailed to a patients GP surgery – currently this scheme is being trailed at certain GP surgeries. This complies with the requirement and recommendations made to secondary care trusts to provide the GP with a discharge summary within 24hrs of a patients’ discharge from hospital – consequently reducing previous financial penalties when not achieved and thus being more cost efficient.
The advent of the EDS has impacted the daily working of the junior doctor, who is commonly, the individual on the secondary care team whose role it is produce the discharge summary. Previously with a TTA a patient could be discharged home without all the constituents on the form being completed and so a GP would be provided with an incomplete discharge summary. At BHR University Hospital NHS Trust in order to produce a finished EDS - and essentially discharge the patient - all constituent sections have to be completed before it can be electronically sent to pharmacy so that the patient sent home with their medications (the discharge summary acts as a prescription). Therefore producing an EDS is more time consuming in comparison to a TTA. However an EDS does have advantages (see Table 1).
Table 1: Comparison of EDS and TTA
Any form of discharge summary is user dependent; what is written is determined by the individual doctor producing the document therefore there is no guarantee that they have documented everything that occurred during admission. In the case of the TTA user dependence also refers to the legibility of the writing, the durability of the carbon copies produced, as well as the level of detail of the discharge summary produced.
In 2008 Newham University Hospital Trust introduced the EDS, the trust audited this process and found it to be successful3. 2010 saw the introduction of the EDS at BHR University Hospital NHS Trust. The EDS was piloted on Sunrise B ward of Queen’s Hospital, Romford. The purpose of this audit is to establish if the introduction of the EDS at BHR University Hospital NHS Trust has been successful. The audit aims to determine if the EDS method is superior to that of the traditional TTA – this will be achieved by comparing the completion rates for specific criteria of the discharge summary. This audit also aims to identify areas of improvement and recommendation for the EDS.
Design and Method:
An opportunistic sample of 50 TTAs and 50 EDSs were selected from the patients admitted to Sunrise B (‘Care of the elderly’) ward, Queen’s Hospital, Romford in a two-month period (January to February 2011). Thus this is a retrospective audit. No exclusion criteria for selection of discharge summaries was set. For each discharge summary completion rates for the different fields of the discharge summary were recorded. Table 2 shows the criteria fields included in each type of discharge summary.
Table 2: Comparison of EDS and TTA criteria
The Royal College of Physicians have published their recommendations for the structure and content of the discharge summary. Section headings include
GP details - name, address, practice code
Patient details – surname, forename, date of birth, gender, NHS number, address, telephone number
Admission details – method of admission, source of admission, hospital site, trust, date of, time of
Discharge details – date of, time of, discharge destination, discharging consultant, specialty
Clinical information – diagnosis at discharge, operations/procedures, reason for admission/presenting complaint, allergies, investigations and results, treatments, discharge medications, medication changes
Advice, recommendations and future plan – hospital/GP/community
Person completing summary – doctors name, grade, specialty, signature, date of completion4
This audit establishes which method of discharge summary is more compliant with these recommendations.
Data analysis was mainly descriptive. Data collected was tabulated and represented as percentages. Graphical representation of the data was performed using Microsoft Excel. Due to the nature of the study and data collected more sophisticated statistical analysis, such as that requiring the use of SPSS software, was not warranted.
Results:
Results demonstrate significant differences between the TTA and EDS completion rates for criteria of the discharge summary. Table 2 presents the data as percentages in a tabulated form. Compared to the TTA, the EDS had a higher rate of the following six criteria of the discharge summary documented; diagnosis, co-morbidities, investigations, drug history, discharge destination and instructions for GP.
Table 3: Summary table of data
Patient details and admission date.
The TTA had lower completion rates for these fields than the EDS. The EDS software automatically enters these fields therefore it is not possible for this criterion to be incomplete. The correct patient details ensure continuity of care and patient safety. If patient details – i.e. full name, date of birth, hospital number and address - are not present those with similar names could be mixed up.
Diagnosis.
The TTA performed poorly on documenting diagnosis. The EDS had a completion rate significantly higher than that of the TTA (EDS completion rate = 88%, TTA completion rate = 48%). Figure 1 represents these findings. The main objective of a discharge summary is to inform primary care of the diagnosis to enable healthcare management, therefore it is crucial and pivotal information, for it not to be included in the discharge summary is illogical.
Co-morbidities.
Neither TTAs nor EDSs documented co-morbidities well. However the EDS, yet again, outperformed the TTA. See Figure 1. Documenting co-morbidities has important repercussions for clinical coding and financial incentives (see below).
Investigations.
Coincidently, 62% of TTAs did not document investigations that the patient had had in contrast to 62% of EDSs that did. See Figure 1. There is no guarantee for either discharge method that all investigations are listed; it is dependent upon the doctor who is producing the discharge summary.
Figure 1: Graphical representation of data
Drug history.
As previously mentioned, EDS has to have a completed drug history before the patient can be discharged and hence they have to have a 100% completion rate for this criterion. TTAs only achieved a 64% completion rate as Table 3 demonstrates.
Review of case.
This is not a criteria field on the TTA document. Therefore 86% of TTAs provided no review. 88% of EDSs did provide a case review. Just fewer than 10% of EDSs were incomplete for this item.
Discharge date.
Like the admission date, a discharge date is automatically completed on an EDS thus the completion rate is 100%. However, this date is the date in which the EDS is completed and may not be the actual day the patient leaves hospital because sometimes the EDS is completed (and so the medications dispensed) the day prior to discharge or patient discharge may be delayed. The TTA achieved a 66% completion rate.
Discharge destination.
This is not a criterion present on the TTA and thus 100% of TTAs did not fulfil this requirement. EDSs had a 98% completion rate.
Follow-up arrangements.
The majority of EDSs documented the follow-up plans for a patient (88% in total, 70% specifically for GP follow-up). 46% of TTAs documented patient follow-up required, specifically 44% for hospital follow-up. 54% of TTAs documented no follow-up. In summary, 88% of EDSs documented follow-up in comparison to 46% of TTAs. These findings may be a limitation of the study i.e. patient selection rather than failings in documentation.
Instructions for GP and functional status.
Coincidently, 92% of TTAs did not document ‘instructions for GP’ in contrast to 92% of EDSs that did. ‘Instructions for GP’ is not a criterion on the TTA document.
Functional status.
‘Functional status’ is also not a criterion on the TTA document and so all TTAs were not complete for this. 64% of EDS had a completion rate for documenting ‘functional status’. Functional status indicates a patient’s mobility status, self-care abilities, hearing and sight impairment.
Discussion:
This audit has established that the EDS has a higher completion rate for criteria on the discharge summary, significantly so for documenting diagnosis, co-morbidities, investigations, drug history and instructions for the GP.
One major concern that has been highlighted in performing this audit is the documentation of co-morbidities. Due to variations in training many doctors are unaware of how and where to enter this information on the EDS – there is a specific window that opens on the software program to input this information. Junior doctors were documenting patients’ past medical history under the field of ‘diagnosis’. Co-morbidities should not be listed under ‘diagnosis’ - this infers a new diagnosis - as they are not the acute problem.
The coding of the diagnosis [the acute problem], in context of a patients co-morbidities, results in a condition specific ‘fee’ being paid to secondary care. For example the ‘fee’ received for a patient diagnosed with a respiratory tract infection is different for that when the patient is diagnosed with a respiratory tract infection on the background of dementia. Inaccuracies in diagnosis lead to incorrect coding and measures of incidence. Co-morbidity is ‘any condition which co-exists in conjunction with another disease’. It is a requirement of the discharge summary to document certain co-morbidities – as determined by the Clinical Coding Co-morbidity Working Group (CCCWG)5. Although the discharge summary is not the recommended source documents for use in clinical coding – patients medical notes are used instead – it can help direct and inform those responsible for clinical coding. In should be borne in mind that it is the treating clinicians’ responsibility to document co-morbidities relevant to the current admission. Accurate and correct clinical coding will result in financial gains. Clinical coding has more important purposes other than just financial; it allows the monitoring of health services, epidemiological research, NHS planning of provisions, as well as clinical audit and governance6.
The amount of information documented is user dependent; the level and amount of detail written is subjective. For example there is no guarantee that all the investigations that a patient had are documented. One doctor may provide a whole paragraph to summaries [‘review of case’] whereas another may just write one sentence. Educating those whose task it is to complete the discharge summary about how vital and important it is, along with the role it serves in healthcare management, may influence the effort and time dedicated to producing an EDS. The principles of clear, complete and concise documentation should be applied to both the patients’ discharge summary and their medical notes.
Other healthcare professionals should also contribute to producing the discharge summary, in particular occupational therapists and physiotherapists who are more aware of a patients ‘functional status’ than the doctors. More accurate completion of this item could be achieved with their input.
At the moment with the EDS software system used at BHR University Hospital Trust once an EDS has been printed there is no means of changing any of the information. It cannot be re-accessed to document new or change existing details. Often an EDS will be finalized and so printed for a patient to be discharged home on that day for the discharge then to be delayed. The discharge date document on the EDS should be the actual date the patient is discharged from hospital. Therefore it should be possible to be able to re-access and change details on the EDS.
The results of this audit show that the EDS system used at BHR University Hospital Trust is better then the EDS system audited at Newham in 2008. The Newham audit did not focus on all the criteria fields of the discharge summary or compare with a hand-written discharge summary method, however there is place for comparison with the results of this audit.
Table 4: Comparison of results with findings of Newham audit
This audit has established that the EDS method provides a discharge summary more compliant with the Royal College of Physician’s recommendations on the structure and content of discharge summary in comparison to the TTA.
The EDS will inevitably replace the TTA in time. However it should be remembered that there is still a place for the TTA in clinical practice e.g. locums do not have passwords to access the software programme, if computers are not working, fail or are unavailable. At the end of the day, a discharge summary is better than no discharge summary.
Conclusion:
The findings of this audit show that the EDS is a far superior method of producing a discharge summary than the TTA. The EDS provides a more informative and detailed discharge summary, which is always legible. The discharge summary is often the only source of information a GP is given in regards to a hospital admission and therefore secondary care providers have an obligation to provide clear, complete and concise information.
This audit does highlight that there are areas for improvement and recommendation:
The importance of a discharge summary should be highlighted to all individuals whose responsibility it is to complete them. This could promote better compliance at completing all items and completing them more thoroughly.
EDS training should make users aware of the ‘co-morbidity’ section. Past medical history should not be listed under new diagnosis. This should be a compulsory part that has to be completed before an EDS can be finished.
Occupational therapists and physiotherapists should be able to complete the ‘functional status’ criterion. This should be expanded to give more information and details to primary care providers.
The documentation of certain co-morbidities (those determined by the CCCWG) should be done by ‘tick list’ selection therefore it will not rely upon the individual doctor to remember to document such co-morbidities. All the co-morbidities that should be documented could be listed and the user selects those that the patient has. This will improve the trusts performance in regards to the financial rewards linked to discharge summaries.
The audit should be performed again in 12 months to access if EDS are maintaining high completion rates, to identify further improvement in completion rates and identify any further areas for improvement or recommendation.
Discussion of both TTA and EDS could be a part of the regular weekly supervision of junior medical staff by their prospective consultants.
A discharge summary should also be checked by nursing or clerical staff prior to letting the patient leave the ward to see if all components are completed.
Gastro-oesophageal reflux (GOR) is the passage of gastric contents into the oesophagus. In most infants with GOR the outcome is benign & self-limiting. (1)
Incidence/Prevalence
Peak incidence of GOR is around 4 months of age, and it resolves spontaneously by 1-2 years of age in most patients. (2)
Regurgitation (possetting or spitting up) is the most common presentation in infants with GOR. Regurgitation of at least one episode a day is seen in:
50% of infants 0-3 months
67% of infants at 4 months
5% at 10 to 12 months of age (3)
It is important to note that in infants (younger than 1 year of age) who are otherwise well and symptomatic, regurgitation may be considered entirely normal. (4)
Causes/Risks
GOR occurs due to the transient, inappropriate relaxation of the lower oesophageal sphincter, which allows the stomach contents to pass into the oesophagus.
GOR can be physiological or pathological:
Physiological GOR – when the infant has normal weight gain and experiences no complications and is generally well.
Pathological GOR – also known as gastro-oesophageal reflux disease (GORD) is when reflux is associated with other symptoms like failure to thrive or weight loss, feeding or sleeping problems, chronic respiratory disorders, oesophagitis, haematemesis etc (3)
Several anatomical and physiological conditions make infants (younger than 1 year of age) more prone to GORD than older children and adults:
Short, narrow oesophagus
Delayed gastric emptying
Shorter, lower oesophageal sphincter that is slightly above, rather than below, the diaphragm
Liquid diet and high calorie requirements, putting a strain on gastric capacity
Larger ratio of gastric volume to oesophageal volume(4)
Most children have no specific risk factors for GORD. Children with the following conditions are at increased risk for developing GORD and for progressing to severe GORD:
Severe neurological impairment
Prematurity
Cystic fibrosis
Gastro-oesophageal abnormalities (even after surgical repair), e.g. Oesophageal atresia, diaphragmatic hernia, pyloric stenosis
Bronchopulmonary dysplasia (preterm infants with lung disease)
Hiatus hernia
Oesophageal sphincter disorders
Raised intra-abdominal pressure(5)
Symptoms
GORD in infants and children can present with a variety of symptoms many of which can be relatively non-specific. Equally, other pathologies may lead to the development of reflux. Those in the early years tend to be based on observations by parents, while older, more vocal children express symptoms more akin to adult presentations.
As such, the history/symptoms will be broadly divided into those expected for infants (<1yr), young children (1-5yrs) and older children (>5yrs).
Infants(6-10)
Excessive possetting/regurgitation
Possetting is a normal phenomenon in infants
Frequent episodes, together with vomiting may indicate underlying GORD
Projectile vomiting may indicate an obstructive pathology
Difficult/rapid cessation of feeds
There may be difficulty initiating feeds and latching
Early cessation may be precipitated with the onset of reflux
Failure to thrive
No weight loss can be expected
Weight loss crossing centiles on the growth chart must be addressed urgently
Sleep disturbance
Particularly after an evening feed
This is often associated with irritability and inconsolable crying
Irritability and inconsolable crying
One of the commonest presentations to the GP
This may occur during feeds or shortly afterwards
Apnoeic episodes
A witnessed pausing in respiratory effort
Occurring at night, it can mimic obstructive sleep apnoea
This may indicate a more serious underlying pathology and requires urgent assessment
It is likely to be more prevalent in this age group
Young Children(6-10)
Regurgitation/vomiting
Beating/rubbing the chest may be an early sign of this pathology
Reflux symptoms can be typical of those in adults
Failure to thrive
Refusing food
Similar to the infant, however, the younger child can be more vocal in their refusal
Abdominal/chest pain
With increasing age, children may demonstrate gastric irritation with abdominal pain
Acid reflux producing oesophagitis may present as chest discomfort
Both are similar to symptoms adults experience
Irritability
Persistent/nocturnal cough/wheezing
There may be a dry, non productive cough
Secondary to pharyngeal irritation
There may be no co-morbidities or underlying pathologies
Symptoms can be mistaken for asthma by parents
Older Children (9)
Dyspepsia/vomiting
These symptoms in older children are thought to have a similar reliability in diagnosis as in adults
Dysphagia/odynophagia
As children become more articulate they may be able to describe these symptoms in relation to meals
Particularly with chronic GORD and the development of a Barrett’s Oesophagus
Abdominal/chest pains
Persistent/nocturnal coughing/wheezing
Other Symptoms
Symptoms which can be identified but which maybe considered less life-threatening include:
Dental erosions
Hiccups
Halitosis
Those deserving urgent investigation and intervention include:
Forceful/Bilious vomiting
Suggesting a possible obstructive pathology
This requires urgent surgical referral
Force of vomiting may not always indicate the severity of the problem
Upper gastrointestinal bleeding/hematemesis
This may be a consequence of increased pressure from vomiting
Similar to a Mallory-Weiss pathology
An urgent review by local Paediatric Gastroenterologists is warranted
Profuse diarrhoea or constipation
Failure to thrive/weight loss
Lethargy
Apnoeic episodes
Physical Signs
As with the previous section, physical signs will be considered for each age range as above: infants (<1yr), young children (1-5yrs) and older children (>5yrs).
Infants(9)
Irritability when lying flat
Particularly following feeds
Especially when supine
Weight loss
Regular monitoring with repeat measurements
A single weight cannot imply loss
This is usually a late sign
Arching of the back
Secondary to oesophageal irritation
Can be associated with increased tone and crying
Dehydration
Loss of fluid through vomiting
Look for
Dry mouth
Sunken fontanelle
Prolonged capillary refill time
Reduced skin turgor
Reduced urine output
Crying without tears
Apnoeas
Periods of reduced respiratory effort
Noted by parents as pauses in breathing
Young Children(9)
Weight loss
Dehydration
Anaemia
Associated with chronic symptoms and gradual loss of iron
Look for Pallor/pale conjunctivae, Glossitis, Angular stomatits, Pica
Dysphagia/choking with food
Particularly with prolonged GOR and development of stricturing
Difficulty in breathing/wheezing/lower respiratory tract infection (LRTI)
Similar to asthma on examination
Signs of LRTI on auscultation
Possibly stridor
Older Children(9)
Weight loss
Dehydration
Anaemia
Dysphagia/Choking with food
Difficulty in breathing/Wheezing/LRTI
Persistent sinusitis
Signs requiring urgent intervention include(9):
Hematochezia
Unaltered blood in stool
Stools take on a red appearance
Onset of vomiting after 6 months of life
Fever
Uncommon with GOR
Indicating an infective pathology
Hepatosplenomegaly
An underlying condition other than GOR is likely
Important pathologies must not be missed
Bulging fontanelle
Indicating increased intracranial pressure and an alternative pathology underlying the reflux
Macro/microcephaly
Suggestive of hydrocephalus or a congenital malformation
Seizures
Related to a number of other problems
Metabolic pathologies should figure highly in any differential diagnosis
Abdominal distension with reduced bowel sounds
Tinkling bowel sounds and an pain may suggest bowel obstruction
Differential diagnoses
Common differential diagnoses have been noted in Table 1, however, this is by no means a definitive list of conditions or presentations. It should be taken as an indication to the diverse presentations that can mimic or precipitate GOR (adapted from (9) and (10)).
Condition
History/Symptoms
Signs
Pyloric Stenosis
Sudden onset vomiting Constantly hungry baby Usually males First 4-6 weeks of life
Non-bilious projectile vomiting Visible peristalsis Positive test feed
Malrotation
Sudden onset pain in volvulus Reduced bowel movement Vomiting
Bilious vomiting Abdominal distension Pulling up legs with pain onset
Cow's Milk Allergy
Vomiting and Diarrhoea Eczema Relationship to feeds Failure to thrive
Urticaria Watery stool Weight loss crossing centiles
Constipation
Infrequent stools Straining Blood in nappy
Palpable stool on examination Irritable baby
Urinary Tract Infections
Vomiting Fever (can be without focus) Poor feeding
Lethargy Reduced urinary output Abdominal pain
Viral Gastroenteritis
Vomiting Diarrhoea Fever Lethargy
Dehydration Viral Rash
Hypocalcemia
Poor feeding Lethargy Tetany Seizures
Seizures Apnoeas Tremor Abdominal distension
Hydrocephalus
Vomiting Lethargy Confusion Visual changes
Increased head size Gait change Altered consciousness
Meningitis
Fever Lethargy Vomiting Confusion
Neck stiffness Photophobia Rash (late onset)
Drugs/Toxins
Vomiting Lethargy Ingestion history
Dependant upon drug ingested
Table 1
Investigations and management of infants (<1 yr old)
Complicated cases of GORD (not gaining weight/faltering growth or non-GI symptoms e.g. cough), should be referred to a Paediatrician while investigating for causes and instituting simple management.
Simple investigations to do in primary care:
Abdominal examination for hernias/pyloric stenosis (test feed)
Urine dip to rule out UTI
Blood tests for electrolyte abnormalities, coeliac screen (if weaned)
Referral to a Paediatrician will result in imaging investigations such as Abdominal x-ray and upper GI contrast study to rule out malrotation/hiatus hernia/achalasia in older children, sometimes GORD can be seen on contrast studies. The Paediatrician may go on to arrange a pH/impedance study, upper GI endoscopy or allergy testing.
Management
Calculate feed requirements, parents may be over feeding, e.g. approximate fluid requirement 100-120ml/kg/day every 3-6hrs (depending on age and whether weaned on to solids)
In thriving infants there is no evidence that pharmacological therapy will make a significant difference to symptoms.
Therefore the mainstay of management is reassurance. Simple pharmacological intervention can be tried with feed thickener (in formula fed babies) or Alginates e.g. Gaviscon (can be mixed with water for breast fed babies)
If there are continued concerns refer to Paediatrician for on going investigations and management.
Recent evidence shows that some infants may have cow’s milk protein intolerance (9). Therefore for breast fed babies the mother could try cutting out dairy from her diet (important to have supervision from dietician re: nutritional requirements while breast feeding). Formula fed babies can have a 2 week trial of hydrolysed/amino acid based formula e.g. Progestimil, Nutramigen, Neocate.
Reviews from ESPGHAN (9) and DTB (11) recommend H2RA (H2 receptor antagonists eg. Ranitidine) may help, though there is little evidence – these could be commenced while waiting for an appointment with the Paediatrician.
(Currently there is no role for Domperidone. The next medication a Paediatrician may try is Omeprazole ± omission of cow’s milk protein) (11)
Investigation and management of older children (>18mths)
As before, complicated cases of GORD (not gaining weight/faltering growth or non-GI symptoms e.g. cough), should be referred to a Paediatrician while investigating for causes and instituting simple management.
Investigations
Urine dip, if there are symptoms of vomiting
Stool H. Pyloti antigen test
Bloods tests inc. inflammatory markers, H. Pylori antigen, celiac screen
Management
If main symptom heartburn with no evidence of H. Pylori:
Reassurance and lifestyle changes (weight loss, dietary changes, timing of meals), up to 4 week trial of PPI (Proton pump inhibitor e.g. lansoprazole, omeprazole).
If symptoms improve then continue PPI for up to 6 months, then wean off over 4 weeks (evidence that if stopped suddenly patients may get rebound symptoms) (10).
If PPI doesn’t help or symptoms recur after stopping the PPI, then refer to a Paediatrician.
The Paediatrician may investigate with more blood tests e.g. Autoimmune screen, allergy testing, imaging, pH/impedance study, endoscopy.
Examination of the ovaries at caesarean section is a normal practice as ovarian pathology may be found. The incidence of an adnexal mass found at caesarean section ranges from 1 in 123 1 to 329 2. Ovarian cysts rarely develop de novo in late pregnancy, but rather persist from early pregnancy. About 4 in 5 ovarian cysts detected in the first trimester scan resolve spontaneously. Also, 4 in 5 of ovarian cysts persisting into the second trimester will also be present in the post-natal period as complex cysts such as serous cystadenomas, mature cystic teratomas, endometriomas and mucinous cystadenomas 3. It therefore seems sensible to remove the ovarian cyst for histology at caesarean section rather than subject the woman to the anxiety of multiple investigations and/or another laparotomy, particularly when ovarian cystectomy during caesarean section does not appear to increase morbidity of the procedure 1.
We present a case of incidental ovarian cyst found at elective caesarean section to illustrate the value of a comprehensive consenting process.
Case Report
A 35 year-old para 1 + 0 healthy Polish woman was admitted for elective lower segment caesarean section (LSCS) at 39 + 4 weeks gestation in view of a previous caesarean section 2 years ago for failure to progress in the first stage of labour.She was booked in a neighbouring hospital for her antenatal care where she was counselled and consented for the procedure by her consultant. Her pregnancy was uncomplicated and routine pregnancy scans were unremarkable. Apart from drainage of a breast abscess 2 years ago, she had no medical history of note.
Written consent for elective LSCS was obtained by the junior doctor on duty before the consultant pre-operative ward round. However, the directorate’s standardised consent (figure 1) form was not used. The woman was therefore again counselled and written consent for elective LSCS obtained for the third time now including previously omitted additional procedures that might be performed during the course of the surgery.
At the uncomplicated LSCS under spinal anaesthetic, routine inspection of the uterus and adnexa revealed a 30 x 20 x 15 mm pedunculated firm pale mass attached to the left ovary suggestive of a fibroma. The findings were relayed to the woman, and confirmation of consent for the ovarian cystectomy was obtained. The abnormal ovarian mass was removed with conservation of the left ovary. Histology of the mass subsequently confirmed it to be an ovarian fibroma / fibrothecoma.
Discussion
The Royal College of Obstetricians and Gynaecologists (RCOG) recommend that clinicians should seek prior consent to treat any problem which might arise 4. Indeed, in its Consent Advice for caesarean section, it states that discussion of appropriate but not essential procedures, such as ovarian cystectomy at caesarean section, should take place before undertaking the procedure 5. This supports the position of the Department of Health which states that a procedure should not be performed merely because it is convenient, and that it is good practice where possible to seek the person’s consent to the proposed procedure well in advance, when there is time to respond to the person’s questions and provide adequate information 6.
In spite of the publication of the above guidelines well over a year ago, our case supports the belief that most obstetricians omit discussion and/or documentation of ovarian cystectomy at LSCS, and indeed other risks or additional procedures that may be relevant as showed in figure 1. This may be because the clinician is unaware of the recommendations, not familiar with the potential risks or findings at surgery, or that there is simply insufficient time to document comprehensively.
Our directorate has adopted the use of standardised consent forms for common procedures. These forms are available on our intranet which can be edited allowing clinicians to amend the risks and additional procedures as appropriate in each individual case. We believe the verified printed consent form offers legible and comprehensive documentation of the counselling process, as well as prompting clinicians to discuss key issues such as those recommended by the RCOG Consent Advice. We advocate the use of such standardised consent forms in improving the care of patients and supporting clinicians to deliver optimal services.
Figure 1. Standardised consent form for lower segment caesarean section
Vertigo is the hallucination of movement of the environment around the patient, or of the patient with respect to the environment 1. It is not a fear of heights.
Vertigo is not necessarily the same as dizziness
Dizziness is a non-specific term which can be categorised into four different subtypes according to symptoms described by the patients:
Vertigo
Presyncope: the sense of impending faint, caused by a reduced total cerebral perfusion
Light-headedness: often described as giddiness or wooziness 2
Disequilibrium: a feeling of unsteadiness or imbalance when standing 2
Classification Vertigo may be classified as:
Central - due to a brainstem or cerebellar disorder
Peripheral - due to disorders of the inner ear or the Vestibulocochlear (VIIIth) cranial nerve
Incidence/Prevalence: Most patients who complain about dizziness do not have true vertigo:
5 community based studies into dizziness indicated that around 30% of patients were found to have vertigo, rising to 56.4% in an older population 3
A postal questionnaire study which examined 2064 patients, aged 18-65, 7% described true vertigo in the previous year 3
A full time GP can therefore expect between 10-20 patients with vertigo in one year 3
93% of primary care patients with vertigo have either benign paroxysmal positional vertigo (BPPV), acute vestibular neuronitis, or Ménière's disease 4. These conditions are highlighted in Table 2
Causes A wide range of conditions can cause vertigo, and identifying whether deafness or CNS signs are present, can help narrow the differential diagnosis, as shown in Table 1.
Brain tumour:- e.g. ependymoma or metastasis in the fourth ventricle
Acute cochleo-vestibular dysfunction
Cervical spondylosis
Migraine
Syphilis (rare)
Following flexion-extension injury
Multiple sclerosis
Aura of epileptic attack – especially temporal lobe epilepsy
Drugs – e.g. phenytoin, barbiturates
Syringobulbia
Symptoms
Vertigo may be due to central lesions or peripheral lesions. Vertigo may also be psychogenic or occur in conditions which limit neck movement, such as vertigo caused by cervical spondylosis, or following a “whiplash” flexion-extension injury.
It is essential to determine whether the patient has a peripheral or central cause of vertigo 1.
Information obtained from the history that can be used to make this distinction includes 1:
The timing and duration of the vertigo
Provoking or exacerbating factors
Associated symptoms such as
Pain
Nausea
Neurological symptoms
Hearing loss
Central vertigo:
The vertigo usually develops gradually
Except in: an acute central vertigo is probably vascular in origin, e.g. CVA
Central lesions usually cause neurological signs in addition to the vertigo
Auditory features tend to be uncommon.
Causes severe imbalance
Nystagmus is purely vertical, horizontal, or torsional and is not inhibited by fixation of eyes onto an object
The duration of vertigo episodes and associated auditory symptoms will help to narrow the differential diagnosis 5. This is illustrated for various pathologies that cause vertigo, in Table 2
Table 2 Timing of symptoms
Pathology
Duration Of Episode
Associated Auditory Symptoms
Peripheral or Central Origin
Benign Paroxysmal Positional Vertigo
Seconds
No
Peripheral
Vestibular Neuronitis
Days
No
Peripheral
Ménière's Disease
Hours
Yes
Peripheral
Perilymphatic Fistula
Seconds
Yes
Peripheral
Transient Ischemic Attack
Seconds / Hours
No
Central
Vertiginous Migraine
Hours
No
Central
Labyrinthitis
Days
Yes
Peripheral
Stroke
Days
No
Central
Acoustic Neuroma
Months
Yes
Peripheral
Cerebellar Tumour
Months
No
Central
Multiple Sclerosis
Months
No
Central
It is important to differentiate vertigo from non-rotatory dizziness (presyncope, disequilibrium, light-headedness). Patients can be asked whether they “felt light headed or felt as if the world was spinning around” during a dizzy spell 3.
Important points in the history:
Onset - specific provoking events such as flying or trauma
Associated auditory symptoms - rare in primary CNS lesion
Other associated symptoms
Nausea and vomiting in a vestibular cause
Neurological symptoms such as visual disturbance, dysarthria in a central lesion
Physical/signs
Examination of ear drums (Otoscopy/ Pneumatic otoscopy) for:
Vesicles (Ramsay Hunt syndrome)
Cholesteatoma
Tuning fork tests for hearing loss – Rinne/Weber tests
Cranial nerve examination. Cranial nerves should be examined for signs of :
Nerve palsies
Sensorineural hearing loss
Nystagmus 3
Hennebert's sign 1
Vertigo or nystagmus caused by pushing on the tragus and external auditory meatus of the affected side
Indicates the presence of a perilymphatic fistula.
Gait tests:
Romberg's sign (not particularly useful in the diagnosis of vertigo 1)
Heel-to- toe walking test
Unterberger's stepping test 1 (The patient is asked to walk on the spot with their eyes closed – if the patient rotates to one side they have labyrinth lesion on that side
Dix-Hallpike manoeuvre 1
The most helpful test to perform on patients with vertigo1
If rotational nystagmus occurs then the test is considered positive for BPPV. During a positive test, the fast phase of the rotatory nystagmus is toward the affected ear, which is the ear closest to the ground.
Head impulse test/head thrust test
Useful in recognizing acute vestibulopathy 6
Caloric tests
Cold or warm water or air is irrigated into the external auditory canal
Not commonly used
Investigations/Testing to consider:
Special auditory tests
Audiometry helps establish the diagnosis of Ménière's disease
The history is most important and may give a quite good indication of the cause of vertigo. General medical causes such as anaemia, hypotension and hypoglycaemia may present with dizziness, and therefore should be investigated.
If features of CNS causes is suspected from the history or examination:
CT/MRI Brain imaging as appropriate
Treatment
Treatment should ideally aim at the cause of the vertigo 7:
Medical management – as described below.
Vestibular rehabilitation exercises – e.g. Cawthorne-Cooksey exercises 5.
These exercises aim to help the patient return to normal activity more quickly.
Moving the eyes from side to side and up and down while in bed or sitting down - then moving the head, first with your eyes open and then closed
Other forms use gaze and gait stabilising exercises. Most exercises involve head movement
For most patients the main priority is effective control of the symptoms.
For acute attacks, treatments include 5,8: -
Betahistine hydrochloride 8-16mg upto TDS
Cinnarizine, 15-30 mg TDS or
Prochlorperazine should be reserved for rapid relieve of acute symptoms only 8,12 - tablets 5-10 mg or buccal 3mg TDS or injection 12.5 mg IM or 25mg PR suppository - if vomiting
Preventive measures for recurrent attacks include:
Restrict salt and fluid intake - stop smoking and restrict excess coffee or alcohol 9,10
Betahistine hydrochloride 16mg regularly TDS seems most effective in Ménière's
Cinnarizine 15-30 mg TDS
Points to consider
Warn patients when drugs may sedate 10.
Prochlorperazine is less sedating than some other recommended antihistamines, but may cause a dystonic reaction (particularly in children and young women) 11.
Benzodiazepines are not recommended 9.
Recurrent vertigo
The most important first step in the management of recurrent vertigo is to distinguish vertigo from 'dizziness'.
In attacks of vertigo there is a sense of mobile disequilibrium ("the room spinning") which, if severe, results in uncontrolled staggering in one direction which may be only prevented by grabbing a solid object 10.
Epley's manoeuvre
a. Aims to remove debris from the semicircular canals and deposit it in the utricle where hair cells are not stimulated 11 b. Contraindications include 10: i. Severe carotid stenosis ii. Unstable heart disease iii. Severe neck disease (cervical spondylosis with myelopathy) iv. Advanced rheumatoid arthritisConsultation and referral:
Refer to secondary care if 10 :
Recurrent separate episodes
Neurological symptoms e.g. dysphasia, paraesthesiae or weakness
Associated sensorineural deafness
If there is an inadequate visualisation of the entire tympanic membrane or an abnormality (e.g. cholesteatoma)
Atypical nystagmus e.g. non-horizontal, persisting for weeks, changing in direction or differing in each eye
Positive fistula sign: pressure on the tragus reproducing symptoms (suggests endolymphatic fistula
If the patient has hearing problems in addition to vertigo then referral should be made to an ENT specialist. Other cases should be referred to a neurologist 10.
While awaiting referral:
Consider symptomatic drug treatment for no longer than 1 week because prolonged use may delay vestibular compensation
It is important that the person stops symptomatic treatment 48 hours before seeing a specialist, as it will interfere with diagnostic tests such as the Dix-Hallpike manoeuvre.
If the person's symptoms deteriorate, seek specialist advice.
When to consider hospitalization
Admit the patient to hospital if they have severe nausea and vomiting, and are unable to tolerate oral fluids 9.
Admit or urgently refer the person to a neurologist if they have:
Very sudden onset of vertigo (within seconds) that persists.
Acute vertigo associated with neurological symptoms or signs (e.g. new type of headache - especially occipital, gait disturbance, truncal ataxia, numbness, dysarthria, weakness) which may suggest CVA, TIA, or multiple sclerosis 9.
Admit or refer the person as an emergency to an ENT specialist if they have acute deafness without other typical features of Ménière’s disease (tinnitus and a sensation of fullness in the ear). Sudden onset unilateral deafness would suggest acute ischaemia of the labyrinth or brainstem, but can also occur with infection or inflammation.
Emergency treatment may restore hearing. The person should be seen within 12 hours of the onset of symptoms 9
The urgency of referral depends on the severity of symptoms (e.g. requirement for intravenous fluids because of excessive vomiting) and the suspected diagnosis 9.
Patient InformationThe Ménière's Society www.menieres.org.ukwww.patient.co.uk/doctor/Vertigo.htm
Urinary incontinence is a common and distressing condition. It is an underreported problem because of the stigma associated with the condition and many patients simply suffer in silence.
Definition
Urinary incontinence is defined as involuntary leakage of urine.
Prevelence
It has been estimated that in the United Kingdom (UK) 9.6 million women are affected by bladder problems.1, 2 An overactive bladder itself affects five million adults, nearly 1 in 5 of the over-40 population.3 Prevalence is estimated to be 15% among healthy older adults and 65% of old frail adults.4 It is twice as common in women than men. It can affect women of all ages including after childbirth. In a cross-sectional survey of adult females attending a primary care practice in the UK, nearly half had urinary incontinence but only a small minority sought help.5 Forty-two per cent of women affected wait up to 15 years before seeking treatment.6
Types
1. Stress incontinence: This is involuntary urine leakage on exertion such as coughing/laughing/sneezing or exercise. Stress incontinence is due to an incompetent urethral sphincter. It is largely caused by childbirth thus young women can develop this problem. Other causes include pelvic surgery or hysterectomy.
2.Urge incontinence:This is involuntary urinary leakage associated with urgency (a compelling desire to urinate that is difficult to defer) and is due to detrusor overactivity leading to detrusor contraction. Urge incontinence often appears later in life. Frequency or nocturia, with low volume of urine voided, are signs of an overactive bladder that can occur with or without urge incontinence.7 An overactive bladder affects both genders and its prevalence rises with age, affecting 16.7% of those aged 40 in North America and Europe.3 An overactive bladder should be managed in the same manner as urge incontinence.
3. Overflow incontinence
4. Mixed incontinence: This is both stress and urge incontinence.
Risk factors
The most important risk factor is being female. Others are:
Obesity
Pregnancy and childbirth
Obstruction - tumours in the pelvis or impacted stool
Hysterectomy 8
Neurological disease
Cognitive impairment
Burden
In 2001 the annual estimated cost of dealing with bladder problems was £353.6 million.9 This included expenditure on pads. It is expected to be much higher now. Only a small proportion of the above amount was spent on drugs,10 the remainder being spent on secondary care and surgical treatment.
Bearing this in mind, it makes sense that the general practitioner (GP) is ideally placed to screen and manage these patients in primary care. It is not necessary to refer all patients to secondary care. With the ever-increasing pressure on GPs to reduce unnecessary referrals, there is now a scope for commissioning this service. However, management of an overactive bladder is not part of the Quality and Outcome Framework - could be one reason why GPs are not keen or enthusiastic.
Primary care management
History
A good history makes the initial diagnosis. Ask the woman whether she leaks on coughing, sneezing or exertion (stress) or whether she has an urgent need to pass urine before the leakage (urge). If she gives a history of both, she probably has mixed incontinence.
A history of nocturia or frequency with low urinary volume means an overactive bladder. This should be managed in the same way as urge incontinence. Previous surgery, or an obstetric and gynaecology history, may give further clues as to the type of incontinence.
Examination
Abdominal examination - any palpable mass. This may be a palpable bladder, an ovarian cyst, or a large fibroid.
Pelvic examination - Prolapse, enlarged uterus due to fibroid. Inspection of the pelvic floor may show visible stress incontinence on straining or coughing.
Per-rectal (PR) examination if suspicion of constipation or faecal incontinence.
Investigations
Routine urine check for sugar and protein.
Mid-stream urine (MSU) to exclude urinary infection.
Bladder diary for three days. Ask the woman to complete a diary of time and fluid volume - intake and output with episodes of urinary leakage and her activity at that time. The charts are available from pharmaceutical companies (keep the booklets in your examination room).
National Institute for Health and Clinical Excellence (NICE) states that the use of cystometry, ambulatory urodynamics or video-urodynamics is not recommended before commencing non-surgical treatment.11
Treatment
Treatment depends on the type of incontinence. Pregnancy and childbirth are known risk factors and there is evidence that pelvic floor exercises during pregnancy reduce the risk. The exercises should be taught by the midwife during antenatal classes.
For stress incontinence, the first line therapy is three months of pelvic floor exercises. These should be taught by the practice nurse. An instruction leaflet on its own is not enough. There is good evidence that advising about pelvic floor exercises is an appropriate treatment for women with persistent postpartum urinary incontinence.12
For urge incontinence, bladder training is the first step. The patient should be taught to gradually increase the time between voids.
Life style advice in all with a body mass index (BMI) over 30kg/m2.11
Household modifications, mobility aids, downstairs toilets can help an elderly patient struggling to reach the toilet in time.
Regular prompting of patients, by residential or nursing home staff, to visit the toilet can make a considerable difference rather than putting a pad on.
Patients with an overactive bladder should be advised to reduce their caffeine and alcohol intake.
Encourage the patient to drink two litres of fluid a day. Many women reduce their fluid intake hoping that this would help the symptom control, but less fluid intake can lead to concentrated urine which can result in bladder irritation.
Antimuscarinic drugs such as oxybutynin can be used if bladder training is not successful. NICE recommends that immediate-release oxybutynin should be given as a first line.11 Transdermal oxybutynin can be given if oral oxybutynin is not tolerated. Compliance is often a problem because of side effects e.g. dry mouth, constipation, dry eyes, blurred vision, dizziness and cognitive impairment. Contraindications are acute angle glaucoma, myasthenia gravis, severe ulcerative colitis and gastro-intestinal obstruction.
NICE does not recommend duloxetine as a first or second line treatment for stress incontinence. It can be considered if there are persisting side effects with oxybutynin.
Desmopressin or tricyclic antidepressants can be used in women with nocturia.
The role of hormone replacement therapy (HRT) is debatable. Although oestrogens may improve atrophic vaginitis, there is no evidence that oestrogens by themselves are beneficial in incontinence.13
Pads and catheters should only be issued on prescription if all treatment options have failed and the patient is waiting to see a specialist. These are coping aids.
Referral to secondry care
GPs should refer patients to a urogynaecologist or a surgeon who has experience in this field. Extra-contractual referrals are not favoured by Primary Care Trusts (PCTs) - try convincing your PCT!
Refer if there is:
Pelvic mass
Frank haematuria
Symptomatic prolapse
Suspected neurological disease
Urogenital fistula
Previous pelvic surgery
Failure of conservative measures and anticholinergic drugs.
Chlamydia Screening In General Practice
Sexually transmitted infections are reaching epidemic proportions in Britain and Chlamydia is the commonest sexually transmitted bacterial infections.
Prevalence
Chlamydia is thought to be prevalent in 5-10% of 20-24 years old. About 75% of women and 50% of men are asymptomatic. The National Chlamydia Screening Programme currently finds about 8% of young people tested to be positive 1 but this may represent selective testing of higher risk individual.
National Chlamydia Screening Programme (NCSP)
This was initiated in 2003.The aims & objectives were early detection and treatment of asymptomatic infection, to reduce the onward transmission and to prevent the development of sequelae by screening all sexually active under the age of 25 years annually or with each change of sexual partner.
The positive rate for this group in 2008 was 8.7% 1.
An ideal setting to provide screening is General Practice. The nationally agreed target is for 25% of 15-25 years olds-males and females to be screened by 2009/2010 and 35% by 2010/2011.
Pathogenesis
Chlamydia is an intracellular bacteria and causes disease by chronic inflammation which is exacerbated by re-infection. It infects the female & male genital tract and is primarily sexually acquired. It can be carried in the throat, thus oral sex can transmit the bacteria.
Symptoms
Over 70% of women and 50% of men are asymptomatic.
Women may experience:
• post coital or inter- menstrual bleeding
• pelvic pain
• dysuria
• increased vaginal discharge
• P.I.D with infertility (10-40% incidence)
Men may experience:
• urethral discharge
• dysuria
• epididymo- orchitis
• urinary frequency
Symptoms in both men and women:
• rectal discharge
• rectal bleed following rectal infection
• pharyngeal infection - rare.
History
Early diagnosis and treatment will reduce the risk of long term complications. A detailed history of following should be taken-
1) History of discharge-Enquire about:
• colour & consistency of the discharge
• odour
• is it aggravated by sexual intercourse
• any associated itching
• when was it first noticed
• any past history of the discharge
• was it diagnosed and treated earlier
• any association of the discharge with menstrual cycle
2) Sexual history:
• date of last sexual intercourse
• were condoms used
• and if so were they used consistently
• regular partner or not
• any other partners in the last six months
• has she or her partner had sex with some one else of the same sex
• any history of sex with a partner from a different country
• any drug abuse in either the woman or her partner
3) Contraception and cytology:
• which contraception does she use
• any recent change of contraception
• whether she is up to date with cervical cytology
• whether all previous screens have been normal
4) Menstrual history:
• date of LMP
• are periods regular or have they altered recently
• any bleeding in between periods or after intercourse
5) History of sexually transmitted infection:
• any past history of STI
• was it treated
• was the partner also treated
• did they have a test of cure
6) Others symptoms:
• ower abdominal pain
• dysparunia
• dysuria
• any soreness or warts.
7) History of treatment:
• any medication been prescribed.
• any usage of over the counter medications
Examination
Examination of the female patient is usually normal but may show some muco -purulent discharge with contact bleeding. If pelvic inflammation is present there will be tenderness on uterine and adnexal bimanual palpation. The patient may sometimes be unwell with temperature. In suspected rectal chlamydia, Proctoscopy may be normal or may show changes of bloody/muco-purulent discharge or ulceration of mucosa.In men with epididymo-orchitis there may be epididymal and testicular tenderness with or with out systemic features.
Investigations
• The older less sensitive (EIAs) Enzyme immunoassays are replaced by Nucleic acid amplification tests (NAATs) .They are based on polymerase chain reaction technology.
• In some areas a combined NATT is in use for diagnosis of both Chlamydia & gonorrhoea. NATTs are not licensed for rectal or pharyngeal sampling.
• Men should have a first void urine sample tested. In symptomatic women an endocervical swab is the sample of choice. If the patient does not require a per speculum examination a blind vulvovaginal swab could be an appropriate sample. These are almost as accurate and have become the basis for self test kits, now available widely.
• A first catch urine (FCU) sample may be taken for women (having not passed urine for at least one hour before) but this is less sensitive in women than in men2
• Sexually transmitted infection screen should include serological testing for HIV and syphilis. Current guidelines for HIV testing can be found at www.bashh.org.
Prevention
No opportunity should be lost to discuss safe sex with young people at the time of new patient check up and when prescribing contraception. It is a good practice to screen Chlamydia with informed consent when performing cervical screening in sexually active women under 25 and those over 25 with two or more partners in the last year or a change of partner in the past year.
Management
• It is appropriate to treat Chlamydia in a general practice setting. Treatment is with either macrolides or tetracyclines.
• Oral Azithromycin (Zithromax) 1gm stat should be the first choice as it avoids compliance issues. Patients must be advised to avoid sex for 7 days after the treatment. An alternative is oral Doxycycline (Vibramycin) 100 mg twice daily for 7 days or oral Erythromycin (Erymax) 500 mg twice daily for 14 days.
• Interaction with oral contraceptive pill should be discussed. In pregnant women or those at risk of pregnancy, Azithromycin is still an option.
• Retesting to verify cure is not advocated, partly because of the high cure rate and partly the test using NAA may remain positive for up to five weeks causing confusion.
• All at risk partners in the last six months for females and asymptomatic males or four weeks for symptomatic males should be informed. They should be invited and treated even if the test is negative 3.The discussion and treatment can take place by the GP if the patient is registered with the practice or by referral to local genitourinary clinic.
Locally Enhanced Service
Each primary care trust has a Chlamydia screening officer. This year the target from the Department of Health is to screen 25% of patients aged 16 to 25 years registered at the practice who are sexually active.
Fee Structure
On agreeing a service plan with the PCT the general practice can receive: ( this may vary from one PCT to another PCT)
• £4.50 per test received in the laboratory for coverage of ≤ 10% of the practice population aged 15-24 years.
• £5.00 per test received in the laboratory for coverage of 10% to ≤20% of the practice population aged 15-24 years.
• £6.50 per test received in the laboratory for coverage of 20% to ≤25% of the practice population aged 15-24 years.
• £8.00 per test received in the laboratory for coverage of over 25% of the practice population aged 15-24 years.
How To Achieve Targets
• Do a computer search of all the target patients.
• Have a practice meeting
• Involve the whole team: practice nurses, health care assistants and receptionists
• Delegate, delegate and delegate! Practice nurses or health care assistants can screen at risk groups
• “new patient health check” is an ideal opportunity to offer screening. Involve the receptionist to hand out leaflets, forms and urine pots
• Make sure the reception area is suitable for handing out these items otherwise use a side room to ensure privacy
• Decide who would be dealing with positive results, treatment and partner notification
• To earn the money for extra effort you and your staff has made, make sure you use the appropriate read codeand ask the practice manager to send the claims monthly
• Remember only patients tested with in the practice premises are included when calculating the percentage screened
• Make sure you reward your staff appropriately with the money otherwise their enthusiasm may soon vanish
Emergency contraception (E.C) is also known as post-coital pill (PCC) or ‘the morning after pill’. It is the provision of preventing the establishment of a pregnancy following either an unprotected sexual intercourse or a potential contraceptive failure (1). Patients presenting to a general practitioner asking for emergency contraception should be seen and treated the same day. All the reception staff working in a surgery should be trained and patient requesting a PCC over the phone should be fitted in the surgery the same day.Teenage pregnancy is a public health priority (2) and government targets have been set to half the rate of conceptions in people under the age of 18 years in England by 2010 (3).Most people begin to consider sexual activity in adolescence(4).This is a period of psychological maturation.The UK has a higher teenage birth rate in Western Europe (5).About 90,000 teenagers in England become pregnant, resulting in 56,000 live births. Of these 2,200 are to girls aged 14 or under and 7,700 are to under 16 years age.There is a need to improve the provision of emergency contraception (6), but access to the service with in 72 hours can be difficult for young girls who may be worried about the confidentiality (2).
WHEN NEEDED
Emergency contraception is needed either because of split or slipped durex or a potential contraceptive failure e.g. late starter of the contraceptive pill on top of usual seven day break, forgetting to take the pill because of excessive alcohol intake or not taking precautions if vomiting/diarrhoea or antibiotic usage. Missing more than one pill in the first week of the pack could be another reason.Young women for whom sexual intercourse is often unpremeditated and therefore unprotected represents one of the most important groups requiring emergency contraception (7).
HISTORY
Before issuing a prescription, an accurate history to assess the risk of a pregnancy and whether an emergency contraception is needed must be taken (2).There may be a significant age difference between the patient and the partner or there could be an issue of abuse. General practitioner must have an access to local and national child protection guidelines. An accurate history of last menstrual period, usual cycle, date and time of last unprotected sexual intercourse and whether she has had other episodes of UPSI during that cycle should be recorded. History of current medication—enzyme inducing drugs e.g.antiepileptics, St John’s wort which could reduce the efficacy of E.C. should be taken.The only absolute contraindications are pregnancy or a history of serious allergy to any ingredient of the medication.Acute intermittent porphyria, severe liver disease, venous thromboembolism on anticoagulants, breast cancer is some of the relative contraindications.
EXAMINATION
Physical examination should include measurement of height, weight, and blood pressure. A routine urine check for protein & sugar should be done. Advice and help regarding smoking, alcohol and drugs should be given if needed. A pelvic examination is only necessary if an infection is suspected or if the IUCD method is used.
TREATMENT
Two methods are available in the UK-
1) Hormonal method. This contains 1.5 mg of Levonorgestrel (LNS) and is given as a single dose as soon as possible after an UPSI. This is available on the prescription as Levonelle 1500 or as purchase by women over sixteen at pharmacies as Levonelle One Step, both by Schering Health UK. Only those pharmacists who have undertaken training and signed Patient Group Direction (PGD) can dispense the pill.
The sooner it is taken, the greater the efficacy
0 - 24 hours 95% efficacy
25 – 48 hours 85% efficacy
49 -- 72 hours 58% efficacy
It is licensed to be prescribed with in 72 hours of UPSI, although it is known to have some efficacy for up to 120 hours but effectiveness decreases the longer the delay. It acts by interrupting the follicular development and ovulation. There is no effect on implantation. Side effects with E.C are rare. Nausea is reported in 15% of cases and vomiting in 1-2 % cases. If vomiting occurs with in two hours of taking the pill, the patient should return for a repeat dose of Levonelle 1500(1).Irregularity of cycle is another side effect.50% of women reported bleeding a few days earlier or later than expected and 16% had bleeding unrelated to menses within the next seven days (8). Cramps, headaches, dizziness and breast tenderness could be some other side effects. Because this is a progestogen, the oestrogen related cardiovascular risks are not a concern.
2) Copper containing IUCD (not Mirena). This is more effective and prevents nearly 100 % of pregnancies. It has both pre and post ovulation effects .The toxicity of copper prevents fertilisation. If inserted later in the cycle, it causes an inflammatory reaction in the endometrium; preventing implantation (9).It can be inserted with in five days (120 hours) after UPSI. If intercourse has occurred more than five days previously, an IUCD can still be inserted up to five days after the earliest likely calculated ovulation. Before inserting the coil a pelvic examination and swabs should be taken to exclude sexually transmitted diseases. If patient is at a risk, treatment with 1 Gm, Azithromycin should be given. Absolute contraindications to the coil insertion are few and same as to the routine use of coil. This is a better option if patient is taking enzyme inducing drugs such as antiepileptic or St John’s wort.
FOLLOW UP
All patients should be followed up in three or four week time after prescribing a PCC or the coil insertion.
No emergency contraception is 100% effective. Pregnancy should be excluded by doing a pregnancy test if period is late by one week or more. If patient is pregnant various options regarding termination/continuation/adoption should be discussed.Regular methods of contraception should be discussed and advice should be given regarding safe sex. If indicated screening for STD should be done. A general practitioner can do a lot to reduce the burden of STI. Chlamydia screening in England varies from area to area. One can visit www.chlamydiascreening.nhs.uk to find out what is happening in one’s practice area. NICE and the national Collaborating Centre for women and children’s health have produced a guideline recommending that Long Acting Reversible Contraception (LARC) should be offered to all women as part of their contraceptive choices after emergency contraception.
CONCLUSION
There is an increased awareness of emergency contraception although the confusion exists particularly among those aged 16-20 years regarding the time limit for its effectiveness. Every GP practice should have a practitioner with an interest in family planning and sexual health or a family planning trained nurse.