A 40 years old non-alcoholic and non-diabetic agricultural laborer presented with skin lesions around his neck, forearms and feet (sun exposed areas) along with glossitis. Pellagra was suspected because of Casal's necklace (i.e., erythematous, hyperpigmented, scaly lesions around his neck- arrow mark in figure 1). However he did not have diarrhea or neurological manifestations. Pellagra is due to Niacin (Vitamin B3) deficiency. Typical cases of pellagra are associated with 3 Ds - Dermatitis, Diarrhea, Dementia, (and if not treated, the 4th D- Death).1,2 Not many will have all the three Ds. Most commonly involved is skin – dermatitis (Pelle-skin; agra -rough). The patient belonged to poor socioeconomic status.2 His vital parameters and basic investigations were all within normal limits and HIV-ELISA was negative.
The diagnosis of a pellagra-like dermatitis was entertained.3 He was treated with multivitamin capsules which included Niacinamide.2
The skin lesions had disappeared dramatically at the time of follow-up after one month (figure 2).
A 70-year-old man presented in the winter with a four-week history of redness of the left anterolateral leg. He first noticed a slight “tenderness” in the area when showering; the discomfort lasted only a few days. Over the next week, he noticed redness developing. It is now painless and not pruritic, warm, or peeling. He has not applied any topical lotions or creams. He has not had an exposure to new soaps or detergents. He feels well, without fever or weight loss. He has a diagnosis of hypertension and lumbar radiculopathy with an L5 discectomy and resultant leg numbness. He is retired and does not smoke or drink alcohol; his hobby is woodworking in his garage.
Physical examination reveals normal vital signs. On his left anterolateral leg, he has an 8 cm, irregular patch of reticulated erythema with both hyperpigmentation and scaling. The lesion is non-palpable. He has decreased sensation in an L5 distribution on that leg, which was unchanged from prior examinations. These skin findings are shown in Figure 1.
Figure 1
Question: Based on history and physical examination, which of the following is the most likely diagnosis?
Livedo reticularis
Erythema ab igne
Livedo racemosa
First-degree burn
Discussion
The answer is erythema ab igne (EAI; literally “redness from fire,”) which results from chronic exposure to moderate-intensity heat. EAI presents as a reticulated erythematous patch over the area of exposed skin. Possible secondary changes include epidermal atrophy and scaling.1,2 With repeated exposure, brown hyperpigmentation may develop.1 Most patients are asymptomatic, although some note a mild burning sensation. A history of repeated exposure to heat is key to the diagnosis. While cases were historically noted on skin exposed to fire, such as the arms of bakers and coal shovellers, EAI can result from our many, modern heat-sources, such as laptop computers, car seat heaters, heating pads, and, in this case, the portable space heater under the patient’s woodworking bench.2-4 With removal of the heat source, hyperpigmentation typically regresses but may take years.1,3 The diagnosis is clinical. A biopsy is not required to make the diagnosis, but is indicated if malignant transformation is suspected. EAI can increase risk of squamous cell carcinoma, Merkel cell carcinoma, and cutaneous marginal zone lymphoma.1,5 Treatment is typically not necessary; topical steroids or retinoids and laser have had variable success.1,3,4 If pre-malignant changes are detected, topical 5-flourouracil is recommended.1,4
See Table 1 for a summary of the key characteristics and distinguishing features of each diagnosis in this selected differential.
Table 1. Selected Differential Diagnosis of Reticulated Skin Lesions in Adults
Condition
Characteristics
Livedo reticularis
Violaceous mottled or reticulated patches; painless; typically temperature sensitive; may be physiologic or secondary to systemic disease; no hyperpigmentation.
Erythema ab igne
Erythematous reticulated patch, with possible secondary changes including epidermal atrophy and scaling; chronic exposure may lead to hyperpigmentation; painless or associated with a mild burning sensation; history of heat exposure.
Livedo racemosa
Violaceous reticulated patch with larger branching pattern than livedo reticularis, often with asymmetric or “broken” net appearance; typically involves the trunk and proximal limbs; generally secondary to chronic disease; frequently painful; no hyperpigmentation.
First-degree burn
Erythematous, dry, painful lesion which includes the entire area of skin that contacted the high-intensity heat source; not reticulated; no hyperpigmentation.
Livedo reticularis is typically more violaceous in appearance, with net-like, mottled discolouration of the skin due to deoxygenation and dilation of the venous plexus. Primary, physiologic livedo reticularis is often brought on by cold and alleviated by warming. It usually involves a larger area, such as the bilateral thighs, rather than a confined area of skin.1,2
Livedo racemosa is a persistent variant of livedo reticularis with a characteristic, large, broken, branching pattern, often on the trunk and proximal limbs. It is generally secondary to a systemic disease, such as antiphospholipid antibody syndrome or Sneddon syndrome.6
First-degree burns are erythematous, dry, and painful. Instead of a reticulated pattern, as shown here, the erythema of first degree burns covers the entire area of skin that contacted the high-intensity heat source.
A 19 year old male presented with a history of recurrent respiratory tract infections and progressive diminution of vision. Fundoscopy was performed and showed the changes in image below.
What is the finding suggestive of?
1. Retinitis pigmentosa
2. Drug toxicity
3. Congenital rubella
4. Syphilis
Answer: Retinitis Pigmentosa
Retinitis pigmentosa (RP) is a bilateral inherited progressive retinal degeneration presenting in the first to second decades of life.1 The inheritance can be autosomal dominant, autosomal recessive or X-linked recessive. Hallmark symptoms of RP are nightblindness and visual field constriction. Fundus changes in retinitis pigmentosa include waxy pallor of optic disc (black arrow), arteriolar attenuation (white arrow head) and bony spicule pigmentation (white arrow) in the mid-peripheral fundus, which is predominantly populated by rods. Vessel attenuation is the earliest feature seen clinically. Although intraretinal pigmentary migration is relatively easy to observe, it requires years to develop, so early RP may only exhibit vessel attenuation without pigmentation (previously known as RP sine pigmento). Prognosis is variable and tends to be associated with the mode of inheritance.
Drug toxicity with chloroquine can result in visual disturbances. History of drug usage prior to vision disturbance can be present. Fundus examination shows a subtle bulls eye macular lesion characterized by a central foveolar island of pigment surrounded by a depigmented zone of RPE atrophy, which is itself encircled by a hyperpigmented ring.2 In congenital rubella, a history of maternal infection will be present. Fundus findings include salt and pepper pigmentary disturbance involving the periphery and posterior pole with normal vessels, RPE mottling and no intraretinal pigmentary migration. Syphilitic retinopathy may have sectorial or generalised pigmentation.3 The onset can be from adulthood to old age. History of genital ulcer may be present.
A 40 year old patient presented to the hospital outpatient department with one year history of cough, choking sensation following swallowing, hoarseness of voice and loss of weight. History revealed his previous hospital admission 1 year back for management of organophosphorus poisoning during which he was intubated and put on mechanical ventilator for 10 days. Patient developed the symptoms a month after his discharge from the hospital. Cranial nerve examination was within normal limits. What is the possible diagnosis?
Gastro-oesophageal reflux disease
Tracheo-oesophageal fistula
Oesophageal diverticula
Oesophageal rupture
Fig 1: Barium swallow illustrating a dilated oesophagus and the TOF with resultant contamination of the trachea and bronchial tree
Fig 2: Oesophagoscopy showing TOF
Correct answer:
2. Tracheo-oesophageal fistula
Discussion:
A tracheo-oesophageal fistula (TOF) is a communication between the trachea and oesophagus which can be congenital or acquired. Congenital and acquired TOFs are associated with multiple complications, including poor nutrition, recurrent pneumonia, acute lung injury, acute respiratory distress syndrome, lung abscess, bronchiectasis from recurrent aspiration, respiratory failure, and death. Acquired TOFs occur secondary to malignant disease, infection, ruptured diverticula, and trauma.1, 2 Acquired TOFs are quite rare, and incidence rates have not been well documented. Post intubation TOFs uncommonly occur following prolonged mechanical ventilation with an endotracheal or tracheostomy tube. TOFs caused by endotracheal tube intubation depend on several factors, including prolonged intubation, an irritating or abrasive tube, and pressure exerted by the cuff. Pressures exceeding 30 mm Hg can significantly reduce mucosal capillary circulation and result in tracheal necrosis. Cuff pressure is particularly risky when exerted posteriorly against a rigid nasogastric tube in the oesophagus. Poor nutrition, infection, and steroid use cause tissue alteration, which predisposes patients for the development of TOFs. As a result of laryngeal bypass, spillage of oesophageal contents occurs into the trachea. Saliva, food and gastric juice contaminate the airways. This leads to congestion, infection, pneumonia, bronchial obstruction, atelectasis and respiratory distress. The severity of contamination depends on the width and length of the fistula as well as the posture of the patient. Spontaneous closure of non-malignant TOFs is exceptional.
Patients with acquired TOFs have high mortality and morbidity rates because of critical illnesses and co-morbidities. Acquired TOFs may occur in individuals of any age, and elderly individuals are at increased risk if they become ventilator dependent because of respiratory failure. Acquired TOFs can be diagnosed by instillation of contrast media into the oesophagus (Fig.1) or during direct visualization by flexible oesophagoscopy (Fig.2) or bronchoscopy. A high index of suspicion is needed to diagnose tracheo-oesophageal fistula in a post intubated patient presenting with symptom of cough following deglutition. Since acquired TOFs do not close spontaneously, surgical repair is needed if the patient is stable enough.3, 4 Critically ill patients are managed conservatively until stable enough for a major surgical procedure.
Typical oesophageal symptoms of gastro-oesophageal reflux disease include heartburn, regurgitation and dysphagia. The classic presentation of spontaneous oesophageal rupture is chest pain and subcutaneous emphysema after recent vomiting or retching (Mackler’s triad) in a middle-aged man with a history of dietary over-indulgence and over consumption of alcohol. Oesophageal diverticula presents with oropharyngeal dysphagia, usually to both solids and liquids, which is the most common symptom. Retention of food material and secretions in the diverticulum, particularly when it is large, can result in regurgitation of undigested food, halitosis, cough, and even aspiration pneumonia. The patient may note food on the pillow upon waking up in the morning.
An 87-year-old gentleman was admitted after sudden dysarthria and left facial palsy due to a right internal carotid artery occlusion. On examination, incidental spontaneous movements were seen at rest in the left leg (video), with bilaterally diminished Achilles reflexes. Patient was unaware of this finding. Muscle atrophy and hypoesthesia were not present. When walking on heels, left foot dorsiflexion was impaired.
What kind of physical finding is shown in this video?
A. Myoclonus B. Dystonia C. Tremor D. Chorea E. Fasciculation F. Myokymia
Answer / Discussion
Focal fasciculations in the tibialis anterior muscle are shown. When walking on heels, left foot dorsiflexion was slightly impaired.
Fasciculation is a brief, twitching, spontaneous involuntary contraction affecting muscle fibres served by one motor unit, which may be visible under skin. When present, they reflect denervation.
A complete history intake and neurological examination will lead to a sensible diagnostic work-up and to set a prognosis. Clinical differential diagnosis is presented in table 1.
Table 1: Key points for clinical diagnosis
Myoclonus
Brief, shocklike involuntary contraction of a muscle or group of muscles
Dystonia
Involuntary muscle contraction that can cause slow repetitive movements or abnormal postures
Tremor
Involuntary rhytmic contraction of antagonistic muscles
Chorea
Involuntary irregular movement that starts in one part of the body and moves unpredictably and continously to another part, like “dancing”
Myokymia
Involuntary spontaneous quivering, writhing movements within a single muscle not extensive enough to cause a movement of a joint
Localization helps in diagnosis: fasciculations can be generalised, in metabolic-toxic conditions, the benign fasciculation syndrome and degenerative disorders of anterior horn of spinal cord, as amyotrophic lateral sclerosis; segmental, as in syringomyelia; or focal, affecting the muscles controlled by a nerve or spinal root. When fasciculations are in a distribution that cannot be explained by plexus, root or nerve lesion amyotrophic lateral sclerosis (ALS) must be ruled out as soon as possible.
Evolution findings are also pivotal. The absence of muscle atrophy suggests that an acute or subacute nerve lesion is present, although a limited chronic nerve lesion cannot be excluded based on that observation alone. A clinical examination should be repeated at least every six months to assess progression, muscle weakness, upper motor neuron signs and other findings, such as bilateral wasting of the tongue, the “split hand”, head drop, emotionality and cognitive or behavioral impairment1
It is also very important to rule out any possible metabolic disorder, as toxic conditions. Earl Grey tea intoxication has been reported as a cause of widespread fasciculations and cramps2
Electromyography (EMG) is the recording of the electrical activity of the muscles. It supports the clinical suspicion and helps in the topographic diagnosis. If ALS is suspected, a systematic examination of clinically uninvolved muscles has to be done for 2 minutes as fasciculations are the hallmark of this condition. As fasciculation potentials in ALS and benign fasciculation syndrome are indistinguishable on grounds of waveform parameters3 and there is not a reliable biological marker of the disease, a minimum follow-up of 6 months is required before setting a prognosis. When non-progressive isolated fasciculations of the tibialis anterior muscle, it has to been examined the 5th lumbar root and the deep peroneal nerve, as localizer sensory symptoms may be absent4, and to rule out any more diffuse neurogenic processes.
Magnetic resonance imaging (MRI) is supportive to EMG findings as it is very sensitive in detecting anatomic changes that could be responsible for the radiculopathy, but there are other causes of radiculopathy besides nerve root compression. Moreover, lumbar disk protrusions can be found in asymptomatic patients independent of age5. Therefore, MRI is not appropriate if pain or foot drop are not present.
Finally, an isolated chronic left L5 radiculopathy was diagnosed related to lumbar spondyloarthrosis.
A 26-year-old previously healthy male presented with a two day history of pain in his left wrist following trauma inflicted while playing volleyball. It was aggravated by movements around the affected joint. Clinical examination revealed mild tenderness over the left wrist with full range of movements and absence of any swelling. Distal neurovascular status was intact. X-ray of the left hand and wrist was done to rule out an injury to the bones (Fig. 1). Fig. 1: X-Rays of left hand and wrist
What diagnosis does the X-ray findings indicate?
Fracture of left scaphoid bone
Osteoblastic metastases
Osteopathia striata
Tuberous sclerosis
Osteopoikilosis
Answer / Discussion
The X-ray in Fig. 1 shows multiple small hyperdense oval and circular lesions scattered in all small bones of the left hand, with preservation of cortical thickness. These findings are suggestive of osteopoikilosis. Similar lesions were also present in the contralateral hand and wrist, as well as the pelvis (Fig. 2), on X-rays done subsequently.
Fig. 2: X-Ray Pelvis showing bone islands
Patient was counselled and reassured about the radiological findings. He was prescribed oral Paracetamol and topical Piroxicam for three days and asked to rest the affected joint. Osteopoikilosis (also called spotted bone) is a benign, possibly autosomal dominant dysplasia of bones, occurring in 1 per 50,000 people.1 Small bones of hand and feet, long tubular bones and pelvis are most frequently affected. The condition is asymptomatic and is diagnosed incidentally on radiographs taken for other problems. The diagnosis is straightforward, based on the typical radiological appearances of small (up to 10mm) hyperdense opacities distributed symmetrically. No further investigations or any specific treatment are indicated. Patients need to be reassured about the benign nature of radiological findings.
Osteoblastic metastases occur in the older age group, are generally larger in size and do not have such a uniformly symmetric distribution. Osteopathia striata is another rare bone dysplasia, characterized by long hyperdense striations mainly in the metaphyses of long bones and pelvis.2 Sclerotic bone lesions in tuberous sclerosis are frequently seen in the axial skeleton especially calvarias and spine, are at times distributed focally and have irregular borders and variable size.3 Subperiosteal new bone formation may be present and other clinical features like epilepsy may also provide a clue. As seen in Fig. 1, there is no break in the continuity of scaphoid bone, thus ruling out a fracture.
A 32-year old female with medical history of Diabetes Mellitus (type 2) presents to the outpatient clinic with a 2-day history of pain in the roof of her mouth. She described the pain as severe, throbbing, non-radiating, and unrelieved by analgesics. Fever was absent and there were no symptoms suggestive of an antecedent respiratory tract infection (RTI). She had no history of oral mucosa trauma or burns. She gave a remote history of herpes oralis and aphthous ulcers. Her diabetes is well controlled with Sitagliptan-Metformin and Lantus. An annual dental examination done in the past year was described as “normal” by the patient. She maintains oral hygiene with daily teeth brushing without flossing; she had never used dentures. Further review of systems was negative. On examination she was not in distress and vital signs were normal. No external orofacial or neck swelling was observed. Oral examination revealed dental plagues and periodontal lesions. A 2x2cm tender paramedian mass with a small central ulcer was seen and felt on the hard palate anteriorly (see Figure 1 and 2). There were no pharyngotonsillar lesions or regional lymphadenopathy. Tongue and deglutitive movements were normal. Systemic examination was normal. STD/HIV screening was negative. The clinical picture is most consistent with:
Torus palatinus with aphtous ulceration
Hyperplastic candidiasis
Palatal pleomorphic adenoma
Median palatine cyst
Palatal abscess
Answer
The clinical picture is most consistent with a palatal abscess. Palatal abscess is a pyogenic collection representing a palatally directed drainage of infective pulpal, pericoronal or periodontal process.1, 2The most common origin is from an infection of the palatal root of maxillary premolars or molars.3It presents as a very painful, fluctuant swelling, with lateral or paramedian localization. The surrounding edema may give an impression of midline involvement or contralateral extension.4The prevailing dental plagues and periodontitis present in this patient (her diabetic state abetting), creates a rich source of oral aerobes and anaerobes as well as the environment in which they thrive. An antecedent herpetic or aphthuos ulcer may also be portal of entry for causative microbes. The patient’s oral hygiene status, her diabetic state, the acuity of symptoms and markedly painful presentation are consistent with acute palatal abscess. The absence of fever in this patient does not preclude this diagnosis.
Hyperplastic candidiasis is the result of chronic colonization and superficial oral mucosa invasion by Candida sp, causing chronic inflammatory changes with edema and epithelial proliferation.2The result of these reactive responses is a raised pebbled-like –surfaced lesion. It is most commonly seen under denture sites in denture wearers.5,6The lesion depicted in the picture above is not typical for hyperplastic candidiasis, more so, though not an absolute discriminant, the patient had never used dentures.
Torus palatinus is a wide-based, smooth surfaced, bony protrusion in midline of the hard palate caused by cortical bone growth with a thin, poorly vascularized mucosa lining. The etiology is unclear, but is thought to be multifactorial; genetics (autosomal dominant trait) and recurrent superficial palatal injuries most often implicated.1Torus palatinus is often an incidental finding, though some affected persons may present out of concern for its increasing size or interval development of ulceration or pain in the area of the torus. Pleomorphic adenoma is the most common neoplasm of salivary glands. Though it may occur at any age, pleomorphic adenoma of salivary glands has peak incidence in the fourth to sixth decade of life. Palatal pleomorphic adenoma often presents as a painless, slow-growing tumor. Median palatine cyst is a rare, non-odontogenic lesion of the hard palate that usually presents as a painless, fluctuant swelling. They are composed histologically of a fibrous collagenous tissue wall, with infiltration of chronic inflammatory cells, and lined by stratified squamous and/or respiratory epithelium. Pain is unusual in the above three oral diagnostic entities, when present it arises from ulcerative, hemorrhagic or infective complications. A detailed history eliciting the chronicity of a preceding midline palatal swelling is often helpful. The patient reported normal palatal examination a year earlier, the relative short history, and the acuity of presentation (severity of pain) make torus palatinus, median palatine cyst or palatal pleomorphic adenoma unlikely. See Table 1 for discriminants and differential diagnoses.
Table 1: Differential Diagnoses of Palatal Swelling
Onset and course
Acute
Palatal abscess
Chronic
Torus palatinus, median palatal cyst, pleomorphic adenoma, hyperplastic candidiasis
Shape
Globular
Palatal abscess, torus palatinus, median palatal cyst, pleomorphic adenoma
Palatal abscess, hyperplastic candidiasis, infective or traumatic complications of: torus palatinus, median palatal cyst, pleomorphic adenoma
No
Uncomplicated: torus palatinus, median palatal cyst, pleomorphic adenoma
Associated fever
Yes
Palatal abscess (but may not be present)
No
Hyperplastic candidiasis, uncomplicated: torus palatinus, median palatal cyst, pleomorphic adenoma
Patient attributes
Poor oral hygiene/caries
Palatal abscess
Diabetes/HIV
Palatal abscess
Denture wearer
Hyperplastic candidiasis
The patient underwent definitive treatment with incision and drainage of abscess as well as extraction of her upper left second molar by a dental surgeon. She completed a course of Clindamycin as well as multiple scaling and polishing sessions by a dental hygienist. Maintaining oral hygiene by daily teeth brushing, and flossing, use of mouth antiseptic, as well as a biannual visit to her dentist was recommended.
A 26 year old male was brought to Emergency department with history of altered sensorium of 1 day duration. He had a 2 week history of fever prior to admission. On examination, meningeal signs were present. Fundus examination showed evidence of papilloedema and a round pale yellow spot near the optic disc (Figure 1). CT scan of head did not reveal any abnormality.
Mantoux test and HIV ELISA were negative. CSF analysis showed:
Glucose – 40mg/dl; Protein: 2gm/l;
Cell Count: 1200cells/µl;
Cell Type: 80% lymphocytes;
CSF VDRL- negative;
CSF Grams stain, India ink staining and Ziehl Neelsen staining were unremarkable.
What is the Fundus finding?
Roth Spot
Cotton Wool Spot
Choroidal tubercle
A-V malformation
Discussion:
Correct answer: 3) Choroidal Tubercle.
Intraocular tuberculosis is a rare event and occurs in 1% of all diagnosed cases of tuberculosis.1 It occurs by haematogenous spread of mycobacterial organism. Choroidal tuberculosis is the most common initial manifestation of intraocular tuberculosis. They may be seen in 1.4% to 60% of patients with different forms of tuberculosis and are highly specific for tuberculosis. 2, 3
Choroidal tubercles may be unilateral or bilateral and appear as polymorphic yellowish lesions with discrete borders. They are of 2 types, solitary tubercle or granuloma (seen in chronic tuberculosis) and choroidal miliary tubercles (seen in acute miliary tuberculosis). Their size varies from 0.4 to 5 mm and may be associated with retinal vasculitis, panuveitis, choroiditis and neuroretinitis.
When they involve macula they present with visual loss and any delay in appropriate treatment results in irreversible visual loss. Peripherally situated tubercles are asymptomatic. Definitive diagnosis can be daunting due to difficulty in getting ocular samples for histological evaluation, however when available reveal features of granulomatous inflammation. Fundus angiography exhibits hypofluorescence in early stages and hyperfluorescence in later stages.
On treatment they heal by varying degrees of scar formation and marginal pigmentation.4 Untreated tubercles grow into large tumour like mass called tuberculoma.
Roth spots are retinal haemorrhages with a pale centre and are associated with bacterial endocarditis. Cotton wool spots appear as fluffy white patches on the retina and are associated with diabetes. A-V malformations are developmental vascular anomalies and appear as marked arterial and venous dilation associated with a tortuous pattern of vessels. They may have an associated bruit or chemosis of the eye.
The presence of ocular tuberculosis may be subtle. A high index of suspicion is required for its diagnosis. Delay in treatment or misdiagnosis may lead to irreversible visual loss.
An 86-year-old lady was admitted from her residential home with acute on chronic confusion, new symptoms of expressive and receptive dysphasia, dysphagia, vacant episodes and urinary incontinence. She had a previous significant history of haemorrhagic stroke with residual right sided weakness, atrial fibrillation, hypertension, and moderate dementia. Following a CT head, this lady was started on acyclovir for encephalitis. She failed to respond to treatment, and developed constipation. With careful consideration of her poor prognosis and quality of life, this lady was placed on the End of Life Pathway. She was catheterised for comfort. Nine days after initial insertion of the urinary catheter, purple urine was noted in the catheter bag with yellow urine in the tubing leading to the bag. Urine dipstick showed Blood ++, Protein ++, Leuc +, Nit –ve, Glu -ve, Ketone +, pH 8.0. Urine microscopy showed: WCC 454, RBC 279, epithelial cells 52, no casts. Urine culture revealed heavy mixed growth with multiple organisms.
Question: What is the diagnosis?
Answers:
Porphyria
Propofol infusion syndrome
Purple urine bag syndrome
Blue diaper syndrome
Differential diagnoses: Discoloration of urine can be caused by trauma if blood stained, urinary tract infections, ingestion of dye (methylene blue), medications (amitriptyline, indomethacin, triamterene, flutamide, and phenol).
Explanation:
Porphyria usually presents with severe pain with neuropsychological symptoms or photosensitivity, and urine discoloration is likely to occur from initial onset of disease.
Propofol is an anaesthetic agent, excreted in the urine as phenol derivatives which can cause a green urine discolouration1. This medication is unlicensed for End of Life Pathway. Propofol infusion syndrome is associated with prolonged high dose infusion, but is not always accompanied by urine discoloration.
Blue diaper syndrome is an inherited metabolic disorder of tryptophan with presentation at infancy2-3.
Correct answer
Purple urine bag syndrome (PUBS)
Purple urine bag syndrome (PUBS)
PUBS is an uncommon condition with purple discoloration of the urine catheter system. This phenomenon is due to the presence of indigo and indirubin in the collected urine. PUBS was first published in 19784. Some academics would argue that PUBS was reported even earlier historically as an observation in Sir Henry Halford's bulletin in 18115-6. Two recent literature reviews suggested the prevalence of PUBS is as high as 9.8% in institutionalized patients with long-term urinary catheterisation8-9, 12.
A triad of key factors are suggested as cause of PUBS:
high level of tryptophan in the gut due to diet intake or bowel stasis
long term catheterisation8
urinary tract infection (UTI) with bacteria possessing indoxyl phosphatase and sulphatase enzymes, commonly Providencia stuarttiand rettgeri, Pseudomonas auruginosa, Proteus mirabilis, Escherichia coli,Klebsiella pneumoniae, Morganella, Citrobacter species, Group BStreptococci and Enterococci8, 13.
It is understood that bowel stasis causes accumulation of tryptophan, which leads to an increase in urinary indoxyl sulphate (UIS). In the presence of indoxyl phosphatase and sulphatase enzyme activities, whilst collected in the catheter system, UIS is degraded to form a mixture of indigo and dissolved indirubin in the plastic11, coating the catheter system with a purple appearance. Intensity of discoloration is deeper the longer the urine is in contact with the catheter plastic7, 10-12. The urine does not appear purple prior to entering the catheter.
Recent literature7-8 also suggested female gender, alkaline urine, bed bound debilitated patient population, PVC material7 and institutionalization are further predisposing factors of PUBS.
Management of PUBS requires catheter change and treatment of underlying UTI.
Good catheter hygiene and shorter duration of catheterisation can reduce PUBS1.
We present a case of a 48-year-old lady with a history of bony metastatic breast carcinoma who presented with abdominal pain, diarrhoea and bleeding per rectum. She had recently finished a course of chemotherapy 2 weeks ago.
On examination, she was febrile with a temperature of 38.4°C. Her blood pressure was 84/54mmHg and pulse rate was 130/min. She had lower abdominal tenderness with bowel sounds present and a small perineal haematoma. Per rectal examination revealed a small amount of fresh blood, but no surrounding crepitus or induration. Rectoscopic examination was not performed.
Initial haematological investigations revealed a haemoglobin of 11g/dl, white cell count 0.3x109/litre, neutrophil count 0.05x109/litre and a C-reactive protein of 171mg/L. A provisional diagnosis of neutropenic sepsis was made. She was managed with analgesia, intravenous fluids and broad spectrum intravenous antibiotics (piperacillin and tazobactam 4.5g 3-times per day). An urgent CT of abdomen and pelvis was arranged for that morning. It showed rectal wall thickening with air in the pelvis but no tumour or diverticulae (see figure 1).
Fig 1: CT scan of abdomen and pelvis showing free air around rectum
Explanation:
Stercoral perforation of the colon is caused by progressive ischemic necrosis of the bowel wall by a faecal mass. It is the least likely diagnosis here as it usually occurs on the antimesenteric border of the sigmoid colon and is usually associated with a history of chronic constipation and megacolon.
Typhylitis is a potentially life threatening inflammatory bowel process that is a recognised complication of systemic chemotherapy. It can progress to bowel necrosis and perforation but is usually characterised by involvement of the caecum or ascending colon and the rectum is rarely involved.
Clostridial gas gangrene infection occurs with tissue inoculation in a low oxygen tension environment. Approximately 80% of patients without trauma have a malignancy of which 40% are hematologic, however the vast majority of cases are preceded by trauma of which there was no history of in this case 1.
Perineal Necrotizing fasciitis is a rare condition with an estimated 500 cases each year in the UK2. It can affect healthy individuals of any age but carcinoma and immunosupression are known to increase susceptibility3. The initial lack of obvious skin findings make this condition difficult to diagnosis but exquisite pain, especially pain that is disproportionate to what would be expected from the clinical findings is seen 2, 4. Where concurrent signs of sepsis exist, a high index of suspicion is required.
As the disease progresses, the skin may begin to appear smooth, shiny and swollen. Blistering and serous bullae may develop, and a haemorrhage into bullae may occur and giving the appearance of a haematoma as in our case. Crepitus, induration and foul smelling watery discharge secondary to liquefactive necrosis can also become apparent2. On CT scans, fascial thickening, fat stranding and gas tracking may be seen in nearly 80%2, 5of cases, and was seen in this case as well.
Discussion
Necrotizing fasciitis is a lethal soft tissue infection characterised by rapidly progressive inflammation and necrosis of the subcutaneous fascial tissues. The adjacent skin and muscle are relatively spared until late in the course of the disease. Treatment with surgical debridement must be instigated without delay or the patient inevitably succumbs to sepsis and multi-organ failure2.
A 24 hour delay in treatment has been shown to increase mortality by 18% and further surgery is usually indicated with an average of 3.8 debridements needed overall5, 6. Surgical treatment should be instigated in conjunction with broad spectrum intravenous antibiotics and intensive care. The antibiotics selected should be effective against gram-positive, gram negative and anaerobic organisms. Adjuvant therapies like hyperbaric oxygen, intravenous immunoglobulin and activated protein C are of uncertain value.
Following surgery the patient is invariably left with a large tissue defect. Perineal wounds are particularly complex and present multiple challenges including the risk of infection from faecal contamination. Thus diverting colostomies are advised and a Vacuum Assisted Closure (VAC) system may facilitate wound healing 5.
A 45- year -old man hit by a speeding vehicle presented with chest and abdominal pains, along with dyspnea and vomiting. On examination, vitals signs were pulse rate of 122 per minute, blood pressure of 100/60 mm of Hg and respiratory rate of 28 per minute. Chest examination showed tenderness on the lower ribs. The patient had ecchymotic patches and abrasions on his lower chest and abdomen. Abdominal examination showed diffuse tenderness in all quadrants. The patient also had an open fracture of right femur. Arterial blood gas analysis showed hypoxia. Liver enzymes were normal. Chest X-ray and FAST (Focused Assessment with Sonography for Trauma) did not reveal any obvious pathology. CT scan of the chest showed small contused areas of lungs on both sides. Contrast CT abdomen showed the following picture.
Medicine in pictures
CECT (Contrast Enhanced Computed Tomography) of Abdomen.
Question: What is this radiological finding?
Answers:
1. Pneumobilia
2. Liver Laceration
3. Portal vein air embolism
4. Oriental cholangiohepatitis.
Correct answer and description – at the end of the article
Differential diagnosis:
Air in the portal vein has many causes including Necrotizing entero-colitis, Inflammatory bowel disease, Pneumatosis intestinalis, Mesenteric ischemia, Perforated peptic ulcer, Trauma etc.
Explanation:
Pneumobilia means air in the biliary tree. This condition refers to central location of the air which does not extend to within 2 cm of the liver capsule. It is most commonly seen in patients following surgery in which a biliary-enteric anastomosis has been created or a sphincterotomy (sphincter of Oddi) has been performed.
Liver laceration is seen as a non-enhancing region, linear or branching, hypo-dense wedge lesion extending to liver surface.
The CT findings in oriental cholangiohepatitis can present as intra- or extra hepatic duct stones, dilatation of the extra hepatic duct with relatively mild or no dilatation of the intrahepatic ducts or as localized dilatation of the lobar or segmental bile ducts.
Discussion:
Gas in the portal vein is a rare and usually fatal condition, and its presence in trauma is a rare occurrence. Various terms are used to describe the condition like hepatic portal vein gas (HPVG), pneumoportogram, gas embolism of the portal vein etc. It has to be differentiated from air in the biliary radicals. Portal venous gas manifests on CT as small, tubular air densities in the peripheral regions of the liver, predominantly in the left hepatic lobe in the left portal vein as it is more anterior. Due to the centrifugal flow of blood in the portal venous system, air bubbles appear to extend within 2 cm of the liver capsule 1, 2 . Susman and Senturia state that air in the biliary radicals is more centrally placed and extends up to the hilum and into the common hepatic duct due to the centripetal flow of bile 3 . In the pediatric age group the commonest cause attributable is necrotizing entero-colitis, and along with pneumatosis intestinalis it is in fact pathognomic of the condition4 . The pathophysiology behind air entering portal vein is intestinal mucosal damage leading to air entering the venules that connect into the portal vein. This was demonstrated in an experiment where hydrogen enema was given to a dog and subsequent mesenteric venous gas was noted5. Outcomes are poor in non-trauma cases. In the absence of CT findings associated with bowel ischemia, portal venous gas due to trauma or iatrogenic causes may be treated conservatively 6 . However, blunt trauma can be varying in severity and intensity, and the likelihood of polytrauma should be considered by the treating physician.
Correct answer is option 3 - Portal vein air embolism. Portal Vein Air embolization also called HPVG ( hepatic portal vein Gas).Long arrow showing air in the left portal vein and the arrow head showing the contrast filled right portal vein.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the heart, lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In the previous two editions of pictorial essay, we have discussed the normal and abnormal positions of tracheal tube, nasogastric tube and central venous catheters on chest radiographs. In this edition, we shall look into permanent pacemakers and oesophageal Doppler probe on chest radiographs. PERMANENT PACEMAKERS A permanent pacemaker (artificial pacemaker) is a small battery powered medical device that is placed subcutaneously in the chest or abdomen to help control abnormal heart rhythms. They are inserted for different types of conduction problems (eg: sinus node disease, atrio-ventricular block, tachyarrhythmia etc). Permanent cardiac pacemakers consist of two parts:1. Pulse generator (power unit) – usually felt like a “bar of soap” beneath the skin and2. Pacing electrode leads The pulse generator consists of an energy source (battery) and all electrical circuits necessary for pacing and sensory function. The electrode is the exposed metal tip in contact with the myocardium. The electrode is connected to the pulse generator via an insulated wire (lead). Details regarding classification and functioning of a pacemaker is beyond the scope of this article and can be found in any standard cardiology text book. We shall now discuss what to look for in a chest radiograph in a patient with permanent cardiac pacemaker. Chest radiograph is one of the important diagnostic tools used in the evaluation of a patient with a pacemaker. However, it is not complete by itself and in addition to reviewing chest radiographs, it is important to take a detailed history from the patient, do a thorough examination of the patient, review all necessary case notes and analyse the ECG. If required, a cardiology opinion should be sought. Important points to note on a chest radiograph are: Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3. Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835). Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values. Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
First of all, check whether you are looking at the correct chest radiograph (not another patient’s chest radiograph)Identify the pulse generatorIdentify whether it is a single chamber, dual chamber or biventricular pacemaker. This can be done by counting the number and tracing the pacing leads to the cardiac chamber it is implantedCheck that the pacing leads are not dislodgedCheck that the pacemaker leads are intact and not brokenFinally, look for any abnormal shadowing behind the pacemaker as these can be easily missed1
CONCLUSION Valuable information can thus be obtained on reviewing chest radiographs. Our aim is to provide a quick overview on what to look for in pacemakers and oesophageal Doppler probe on chest radiographs. It is by no means an exhaustive description. This article is for the benefit of medical students, junior doctors in training, nurses and paramedical teams who would be involved in the care of critically ill patients. Self Assessment Multiple Choice questions (only one option is correct):1. The wires of permanent pacemakers are usually inserted viaA. Femoral veinB. Basilic veinC. Subclavian veinD. Subclavian artery 2. A chest radiograph is not useful in one of the followingA. To detect intact pacemaker wiresB. To indicate whether a pacemaker is working optimallyC. To detect whether pacemaker wires are dislodgedD. To identify a single chamber or dual chamber pacemaker Answers:1. C2. B
Chest radiographs are one of the most common radiological procedures performed in medical practice. The chest radiograph should ideally include views of the heart, lungs, trachea, mediastinum, bones of the chest and upper part of the abdomen. Chest radiographs are normally taken in the posterior-anterior (PA) view with the patient in upright / standing position but for patients admitted in the intensive care unit (ICU) or other emergency situations, this is not possible and so they are taken in the supine (anterior-posterior views) or semi-erect position.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In this article, we aim to discuss and compare the normal and abnormal positions of central venous catheter (CVC) on chest radiographs.
Indications for Central Venous Catheter (Internal Jugular Vein Cannulation)
There are many indications for central venous cannulation 1. These include:
Central venous pressure (CVP) monitoring
Pulmonary artery catheterisation and monitoring
Transvenous cardiac pacing
Administration of drugs (vasoactive drugs, chemotherapy etc)
Aspiration of air emboli
Administration of fluids (in case of difficult peripheral venous access)
Confirming the position of the central venous catheter tip:
For accurate CVP measurement, the tip of the central venous catheter (CVC) should lie within the superior vein cava (SVC), above its junction with the right atrium and parallel to the vessel walls 1. After insertion of a CVC, the position of the catheter tip must be confirmed radiologically, as catheter tips located within the heart can cause cardiac perforation and tamponade 1. Hence, optimum positioning of the CVC tip is required to prevent complications.
If the CVC tip is situated high up (above the pericardial reflection), this can cause vessel wall erosion and if they are very low (in the right atrium), they can cause arrhythmias, placement in the coronary sinus and damage to the tricuspid valve 2.
The carina is a useful radiological landmark for CVC tip position. In this edition of pictorial essay, we aim to discuss the optimum position of both the right and left sided IJV cannula on chest radiographs.
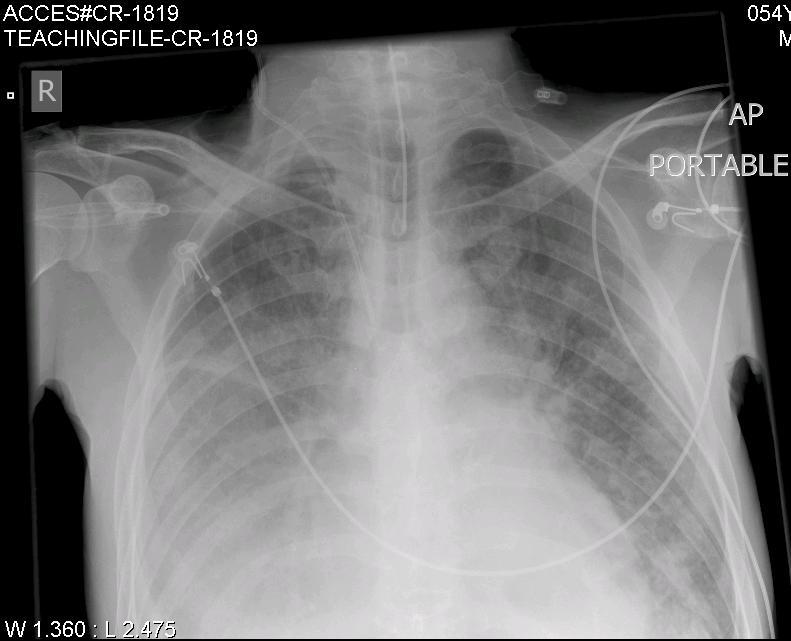
Fig: 1 (CR-1819) shows the normal position of a right sided IJV catheter. The tip of the right sided IJV cannula should ideally lie just above the level of the carina 2. This is the junction of the left and right innominate veins with the superior vena cava (SVC).
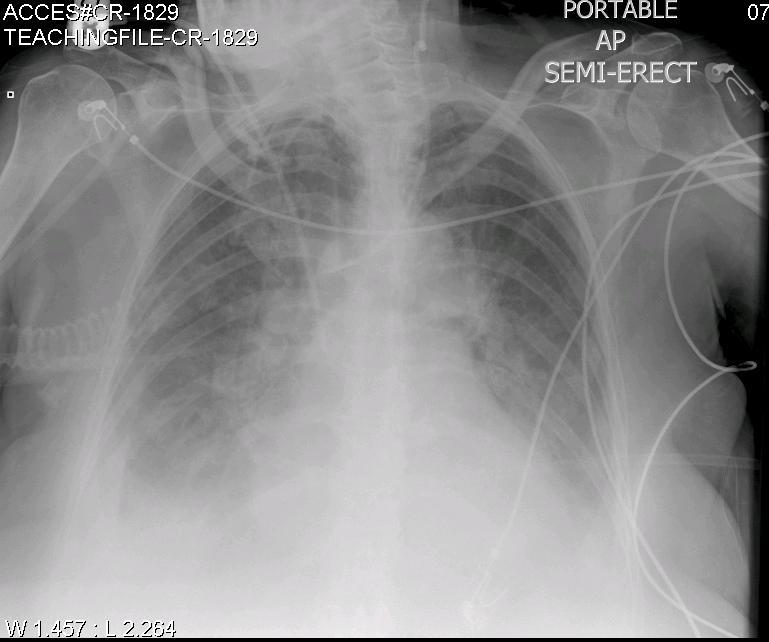
Fig: 2 (CR-1829): The optimum position of the left sided IJV cannula is at or just below the level of the carina 2. This radiograph shows the comparison between the right and left sided IJV cannula in the same patient.
The right sided IJV cannula is too low (below the level of the carina) and is probably in the right atrium while the tip of the left sided IJV cannula is optimally placed.
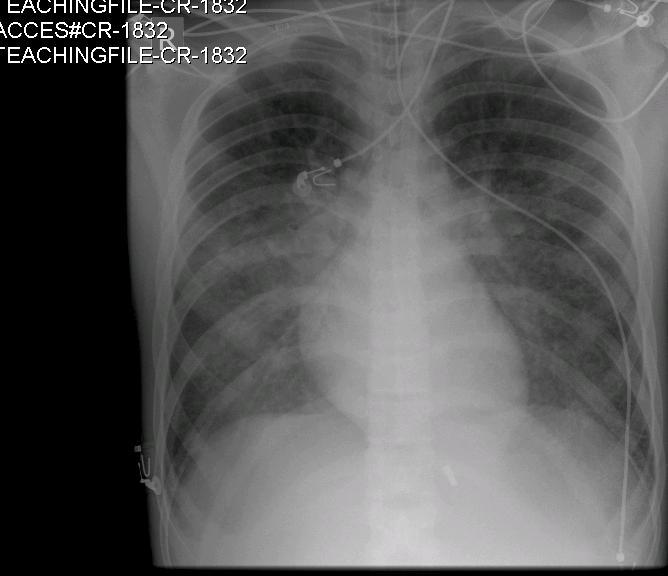
Fig: 3 (CR-1832): In this radiograph, the right sided IJV cannula is too high in the neck. This will not give an accurate CVP measurement. Besides, there is also a risk that the CVC might get dislodged and lead to extravasation of administered fluids and drugs.
Seldinger technique for CVC insertions:
The CVC’s are usually inserted using the Seldinger technique. The IJV can be located by using anatomical landmarks or under direct vision with the help of an ultrasound machine. In the Seldinger technique, after puncture of the IJV, a thin J-shaped guide wire is introduced through the puncture needle. The needle is then slowly withdrawn leaving the J-shaped guide wire in place. A dilator is then introduced over the guide wire to dilate the skin and the subcutaneous tissue. Next, the dilator is removed and the CVC is introduced over the guide wire. Finally, it is important that the guide wire is removed and the CVC is secured.
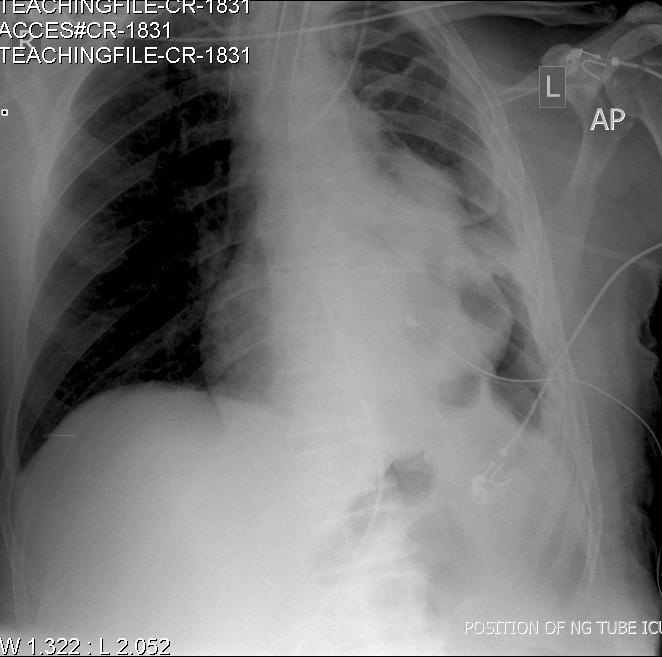
Fig: 4 (CR-1831). This chest radiograph shows an unusual complication where the guide wire has been left accidentally in situ on the right side. (Note the presence of the J-shaped guide wire on the right side of the neck). This can result in serious complications if the guide wire migrates distally.
Conclusion:
In this article, we have highlighted the optimum placement of central venous catheters on chest radiographs. It is imperative that after every CVC insertion (via the IJV or subclavian vein), the position of the tip be confirmed radiologically and if any re-positioning is required, it must be done. The above discussion is true for even CVC’s inserted through the subclavian veins.
Self Assessment MCQ:
The tip of the right sided IJV cannula should be located a. below the level of the carina b. at the level of the clavicle c. just above the level of the carina d. in the right atrium
Answer: c
ACKNOWLEDGEMENTS We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs. COMPETING INTERESTS None Declared AUTHOR DETAILS DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Bedford Hospital NHS Trust, UK DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Bedford Hospital, Bedford, UK Email: drkrishnanmr@gmail.com
References
Mark JB, Slaughter TF and Gerald Reves J. Cardiovascular monitoring. In: Miller RD ed. Anesthesia. 5th edition. Churchill Livingstone; 1144-51.
Stonelake PA and Bodenham AR. The carina as a radiological landmark for central venous catheter tip position. British Journal of Anaesthesia 2006; 96: 335-340
Chest radiographs are one of the most common radiological procedures performed in medical practice. The chest radiograph should ideally include views of the heart, lungs, trachea, mediastinum, bones of the chest and upper part of the abdomen. Chest radiographs are normally taken in the posterior-anterior (PA) view with the patient in upright / standing position but for patients admitted in the intensive care unit (ICU) or other emergency situations, this is not possible and so they are taken in the supine (anterior-posterior views) or semi-erect position.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In this article, we aim to discuss and compare the normal and abnormal positions of both the endotracheal tube (ETT) and nasogastric tube (NG) on chest radiographs.
Endotracheal tube (ETT):
Endotracheal tubes are used to secure the patients airway. Modern ETTs have a radio-opaque line running along their length which enables us to determine their position on chest radiographs 1.
Clinical methods 2 that can be used to determine the appropriate position of the ETT include:
Symmetrical rise and fall of the chest wall with each breath (on inspection and palpation of the chest).
Auscultation of the lung fields
Use of capnography
However, clinical methods cannot confirm how high or low the ETT is situated in the trachea. This can be confirmed by chest radiography. Optimum position of the ETT is required to ensure ventilation of both lungs.
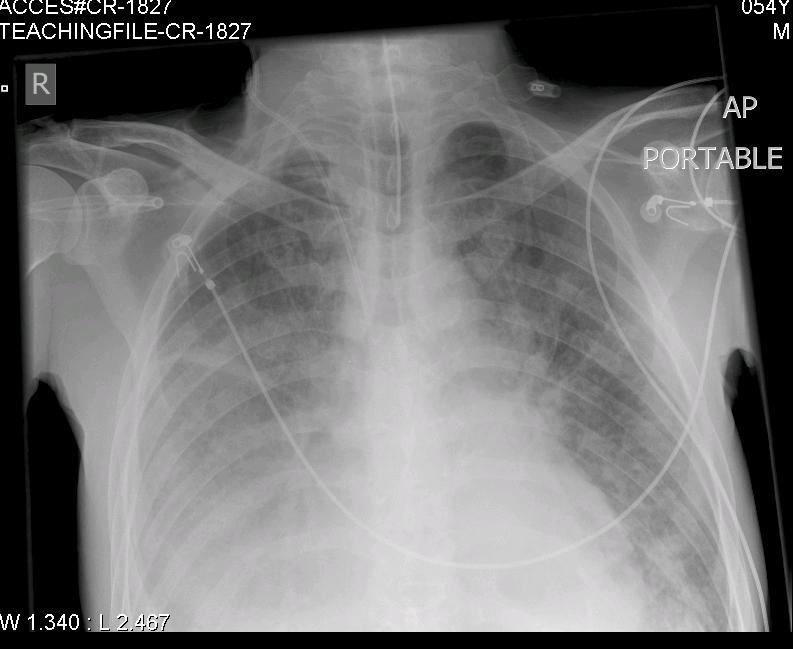
A correctly positioned ETT lies in the mid trachea and its tip is approximately 5-7 cm above the carina 3 as seen in Fig: 1 (CR-1827).
In Fig: 2 (CR-1820), the tip of the ETT is low lying and is at the origin of the right main bronchus. Further migration of the ETT will result in right sided endobronchial intubation and collapse of the left lung. This will result in decreased oxygen saturation values (SpO2) on a pulse oximeter and low arterial partial pressure of oxygen (PaO2) on analysis of an arterial blood gas specimen.
Nasogastric tube (NG):
Nasogastric tube (NG) or orogastric tube (OG) is inserted for providing enteral nutrition, administration of drugs or for gastric drainage. NG feeding is a common practice in all age groups. There is a risk that the NG feeding tube can be misplaced into the lungs during insertion or may move out of the stomach at a later stage.
In the past, various methods 4 have been used to determine the position of NG feeding tubes.
These included:
Auscultation of air insufflated through the feeding tube - whoosh test
Testing acidity/alkalinity of the aspirate using blue litmus paper
Interpreting absence of respiratory distress as an indicator of correct positioning
Monitoring bubbling at the end of the NG tube
Observing the appearance of the feeding tube aspirate
The National Patient Safety Agency (NPSA) have issued a patient safety alert and have recommended that the above methods are not reliable and therefore should not be used to detect the position of NG tubes.
The NPSA recommend 5:
Measuring the pH of the aspirate using pH indicator strips/paper
Use of radiography
The most accurate method for confirming the correct position of a NG feeding tube is radiography 5.
The pH of the gastric aspirate can be affected by ongoing enteral feeding and medications viz: antacids, H2 antagonists and proton pump inhibitors. In these cases, measuring the pH of the aspirate may not be useful and so use of radiography is recommended. The NPSA have issued guidance on how to confirm the position of nasogastric feeding tubes.
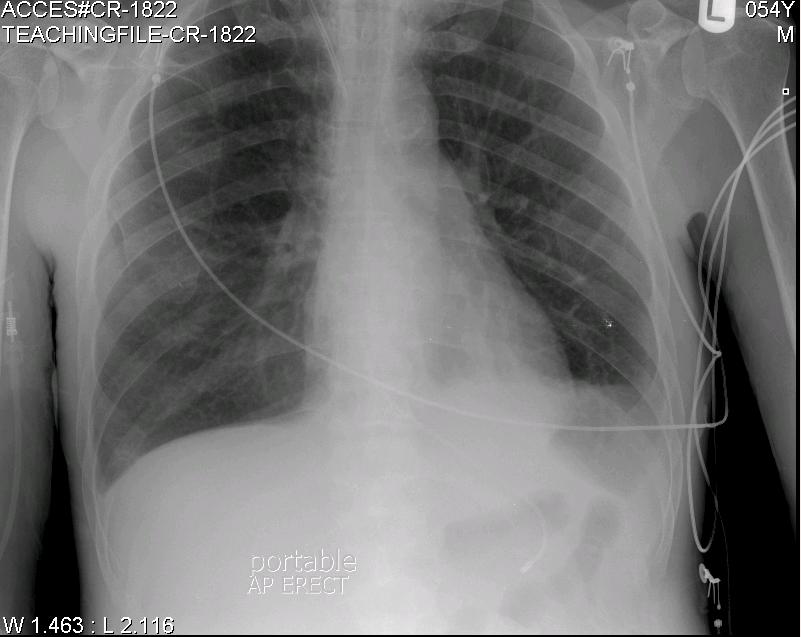
Fig: 3 (CR-1822) indicates the normal position of the NG tip below the diaphragm in the upper part of the stomach (fundus).
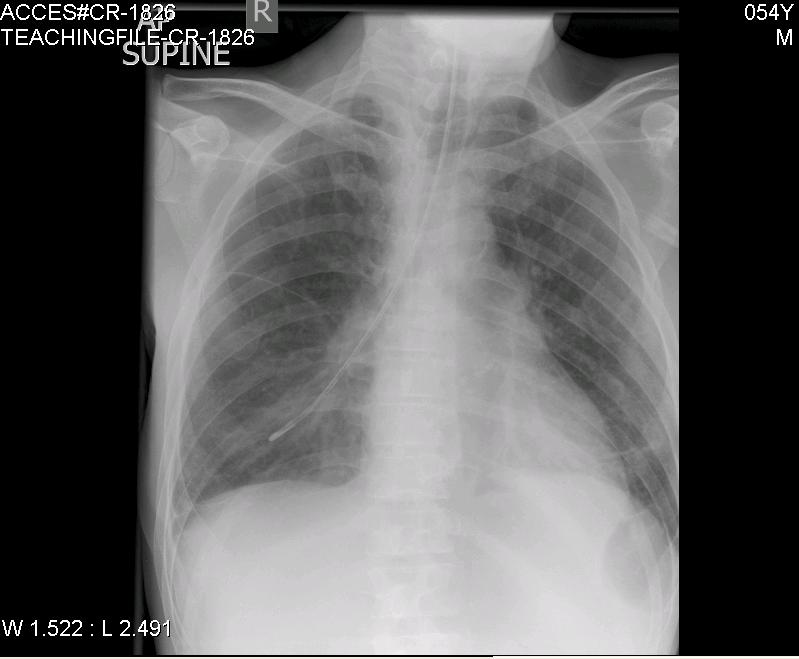
Fig: 4 (CR-1826) shows the abnormal position of the NG tube situated in the right lower lobe bronchus. If NG feeds are commenced, this will result in lung injury.
Conclusion
We have highlighted the optimum position of both the ETT and NG tube on chest radiographs. Optimum positioning is required not only for safety reasons to avoid complications but also for optimum monitoring and treatment of patients. This series of chest radiographs will benefit not only medical students and doctors from all specialties but also nurses, physiotherapists and paramedical teams who will be involved in the care of critically ill patients.
Self Assessment
MCQ 1:
On a chest radiograph, the tip of the ETT:
a. should lie very close to carina
b. should lie 5-7 cm above the carina
c. should lie 5-7 mm above the carina
d. The ETT cannot be visualised on a chest radiograph
MCQ 2:
Which one of the following tests is the most accurate method to determine the correct position of NG feeding tubes?
a. testing the aspirate from the NG tube using a blue litmus paper
b. whoosh test
c. measuring the pH using pH indicator strips/paper
d. radiography
Answers for MCQs:
MCQ 1: b
MCQ 2: d
ACKNOWLEDGEMENTS
We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Bedford Hospital NHS Trust, UK
DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK
CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Bedford Hospital, Bedford, UK
Email: drkrishnanmr@gmail.com
References
Tracheal and tracheostomy tubes and airways. In: Al-Shaikh B and Stacey S eds. Essentials of anaesthetic equipment. 2nd edition. Churchill Livingstone, 2002: 56-67.
Hutton P. Airway management II: assessment, control and problems. In: Hutton P, Cooper GM, James III FM and Butterworth J eds. Fundamental Principles and Practice of Anaesthesia. Martin Dunitz Ltd, 2002; 79.
Goodman LR. The postoperative and critically ill patient. In: Grainger RG and Allison DJ eds. Diagnostic Radiology. 2nd edition. Churchill Livingstone, 1992; 368.
Reducing the harm caused by misplaced nasogastric feeding tubes. Patient safety alert National Patient Safety Agency (NPSA)
How to confirm the correct position of nasogastric feeding tubes in infants, children and adults National Patient Safety Agency (NPSA), Interim advice for healthcare staff, February 2005.





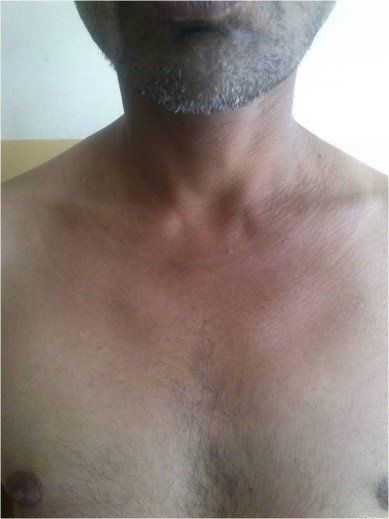

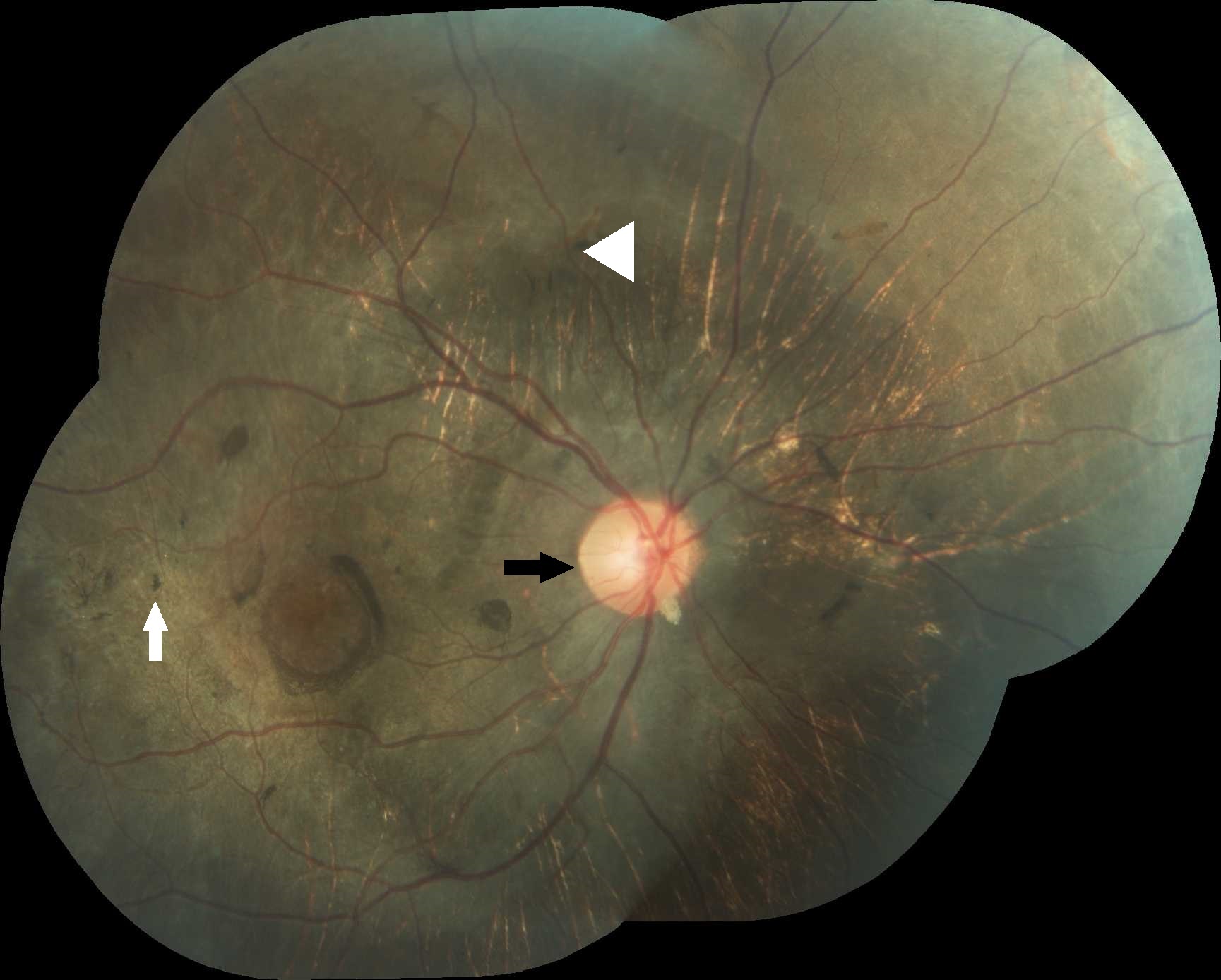
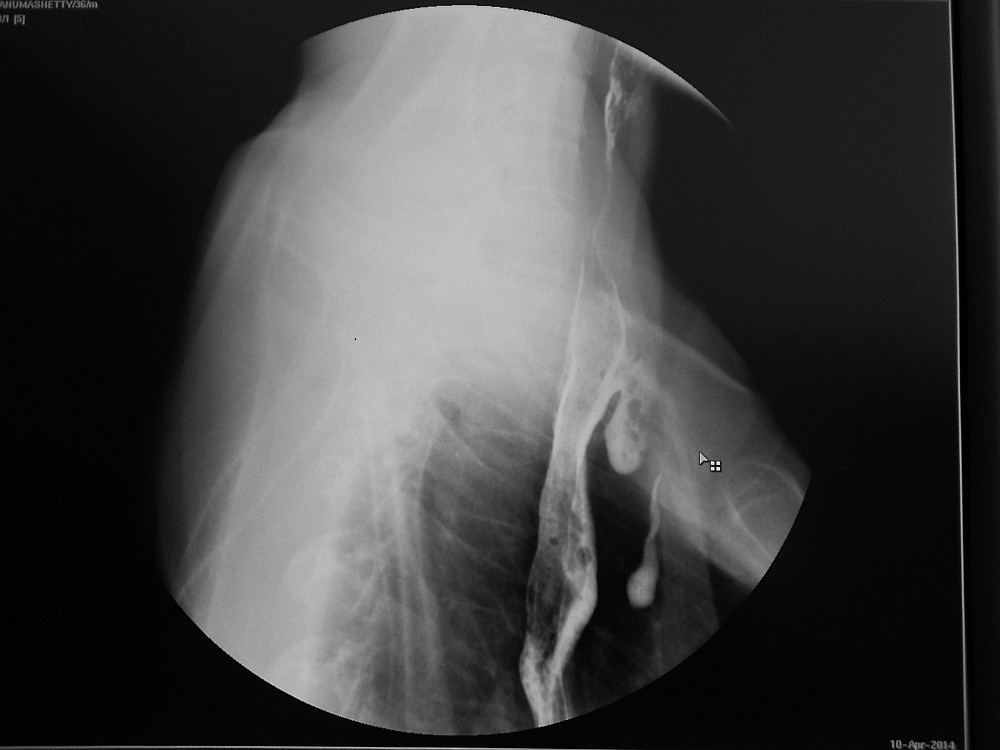
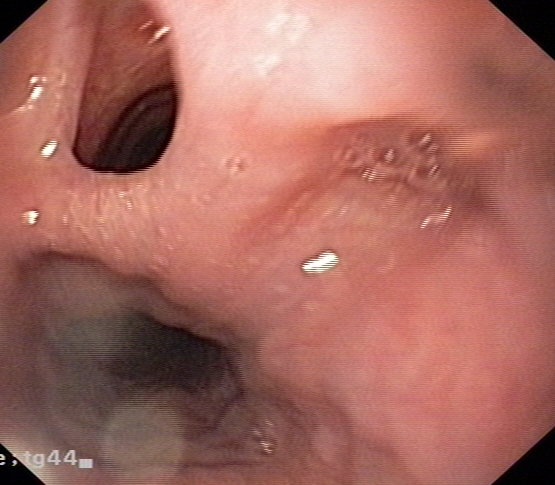




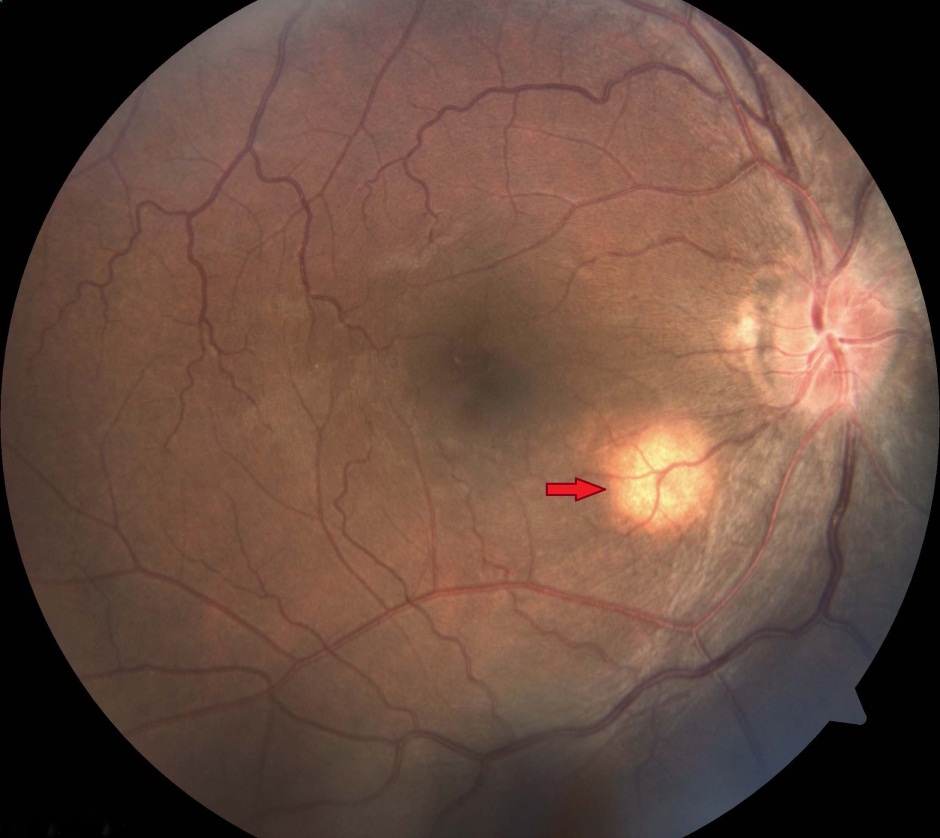




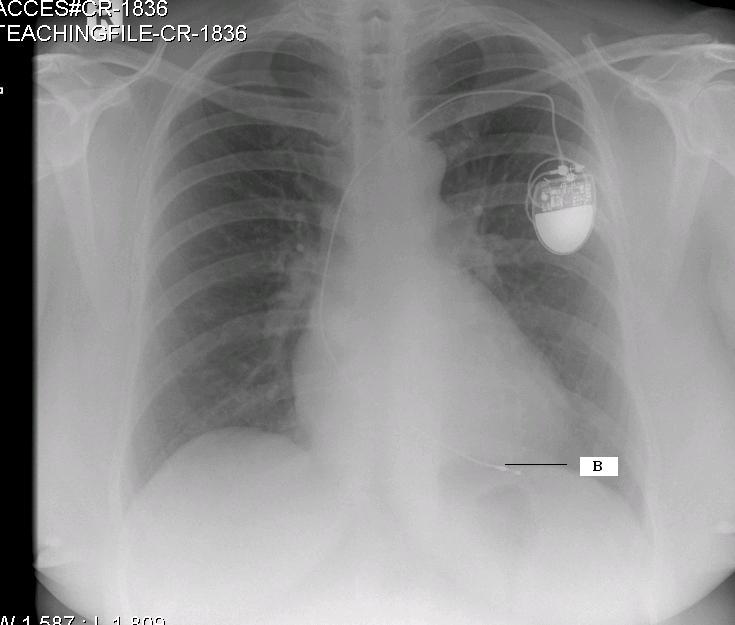 Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3.
Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3. 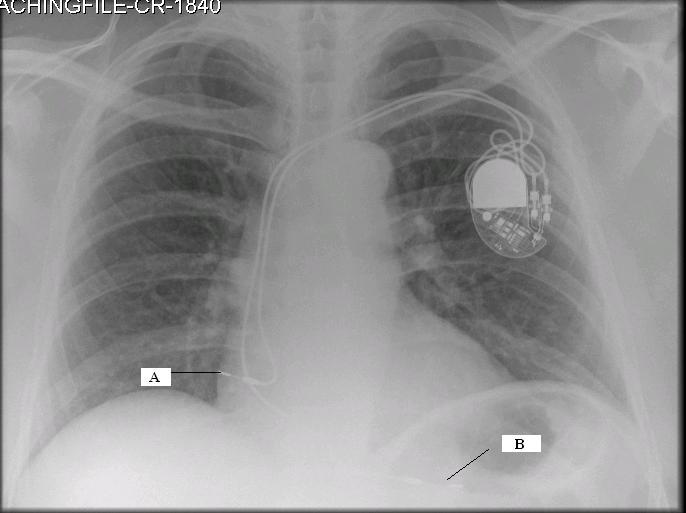 Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835).
Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835). 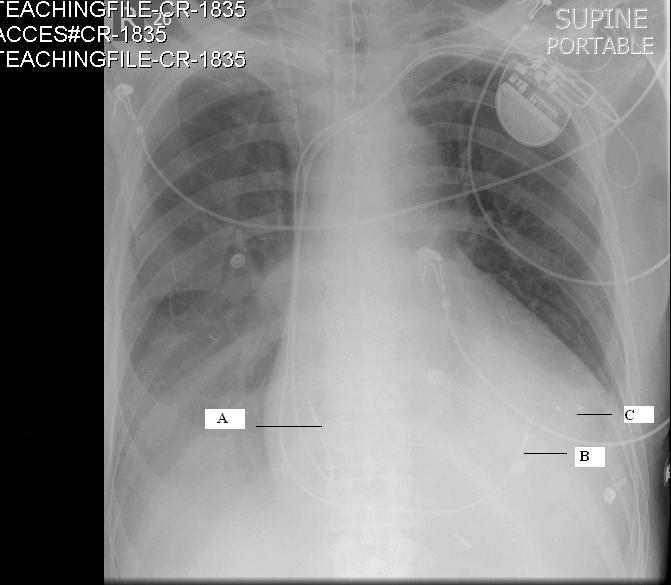 Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values.
Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values. 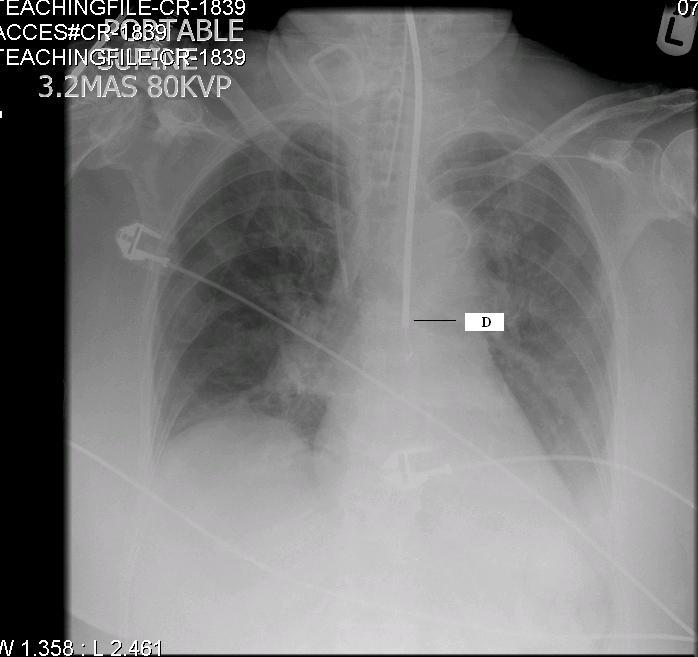 Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].