In recent years, increasing attention has focused on the treatment of chronic pain with a considerable number of research and publications about it. At the same time, opioid prescription, use, abuse and death related to the inappropriate use of opioids have significantly increased over the last 10 years. Some reports indicated that there were more than 100 ‘pain clinics’ within a one-mile radius in South Florida, between 2009 and 2010, which led to the birth of new opioid prescription laws in Florida and many other states to restrict the use of opioids. In the face of clinical and social turmoil related to opioid use and abuse, a fundamental question facing each clinician is: are opioids effective and necessary for chronic non-malignant pain?
Chronic low back pain (LBP) is the most common pain condition in pain clinics and most family physician offices, which ‘requires’ chronic use of opioids. Nampiaparampil et al conducted a literature review in 20121 and found only one high-quality study on oral opioid therapy for LBP, which showed significant efficacy in pain relief and patient function. Current consensus believes that there is weak evidence demonstrating favourable effectiveness of opioids compared to placebo in chronic LBP.2Opioids may be considered in the treatment of chronic LBP if a patient fails other treatment modalities such as non-steroidal anti-inflammatory drugs (NSAIDs), antidepressants, physical therapy or steroid injections. Opioids should be avoided if possible, especially in adolescents who are at high risk of opioid overdose, misuse, and addiction. It has been demonstrated that the majority of the population with degenerative disc disease, including a disc herniation have no back pain. A Magnetic Resonance Imaging (MRI) report or film with a disc herniation should not be an automatic ‘passport’ for access to narcotics.
Failed back surgery syndrome (FBSS) is often refractory to most treatment modalities and sometimes very debilitating. There are no well-controlled clinical studies to approve or disapprove the use of opioids in FBSS. Clinical experience suggests oral opioids may be beneficial and necessary to many patients suffering from severe back pain due to FBSS. Intraspinal opioids delivered via implanted pumps may be indicated in those individuals who cannot tolerate oral medications. For elderly patients with severe pain due to spinal stenosis, there is no clinical study to approve or disprove the use of opioids. However, due to the fact that NSAIDs may cause serious side effects in gastrointestinal, hepatic and renal systems, opioid therapy may still be a choice in carefully selected patients.
Most studies for pharmacological treatment of neuropathic pain are conducted with diabetic peripheral neuropathy (DPN) patients. Several randomized clinical controlled studies have demonstrated evidence that some opioids, such as morphine sulphate, tramadol,3 and oxycodone controlled-release,4 are probably effective in reducing pain and should be considered as a treatment of choice (Level B evidence), even though anti-epileptics such as pregabalin should still be used as the first line medication.5
Some studies indicate opioids may be superior to placebo in relieving pain due to acute migraine attacks and Fiorinal with codeine may be effective for tension headache. However there is lack of clinical evidence supporting long-term use of opioids for chronic headaches such as migraine, chronic daily headache, medication overuse headache, or cervicogenic headache. Currently there are large amounts of opioids being prescribed for headaches because of patients' demands. Neuroscience data on the effects of opioids on the brain has raised serious concerns for long-term safety and has provided the basis for the mechanism by which chronic opioid use may induce progression of headache frequency and severity.6 A recent study found chronic opioid use for migraine associated with more severe headache-related disability, symptomology, comorbidities (depression, anxiety, and cardiovascular disease and events), and greater healthcare resource utilization.7
Many patients with fibromyalgia (FM) come into pain clinics to ask for, or even demand, prescriptions for opioids. There is insufficient evidence to support the routine use of opioids in fibromyalgia.8 Recent studies have suggested that central sensitization may play for role in the aetiology of FM. Three central nervous system (CNS) agents (pregabalin, duloxetine and milnacipran) have been approved by United States Food and Drug Administration (US FDA) for treatment of FM. However, opioids are still commonly prescribed by many physicians for FM patients by ‘tradition’, sometimes even with the combination of a benzodiazapine and muscles relaxant - Soma. We have observed negative health and psychosocial status in patients using opioids and labeled with FM. Opioids should be avoided whenever possible in FM patients in face of widespread abuse and lack of clinical evidence.9
Adolescents with mild non-malignant chronic pain rarely require long-term opioid therapy.10 Opioids should be avoided if possible in adolescents, who are at high risk of opioid overdose, misuse, and addiction. Patients with adolescents living at home should store their opioid medication safely.
In conclusion, opioids are effective and necessary in certain cases. However, currently no single drug stands out as the best therapy for managing chronic non-malignant pain, and current opioid treatment is not sufficiently evidence-based. More well-designed clinical studies are needed to confirm the clinical efficacy and necessity for using opioids in the treatment of chronic non-malignant pain. Before more evidence becomes available, and in the face of widespread abuse of opioids in society and possible serious behavioural consequences to individual patients, a careful history and physical examination, assessment of aberrant behavior, controlled substance agreement, routine urine drug tests, checking of state drug monitoring system (if available), trials of other treatment modalities, and continuous monitoring of opioid compliance should be the prerequisites before any opioids are prescribed.
Opioid prescriptions should be given as indicated, not as ‘demanded’.
A 69 year old male with hypertension, body mass index 24 kg/m2, neck circumference 16 inches, and moderate COPD, on home oxygen, presented to his pulmonary clinic appointment with worsening complaints of fatigue, leg cramps, and intermittent shortness of breath with chest discomfort. A remote, questionable history of syncope five to ten years ago was elicited. His vital signs were: temperature 98.80F, blood pressure 119/76 mmHg, pulse 92/min and regular, and respirations 20/min. Physical exam was significant for crowded oropharynx with a Mallampati score of four, distant breath sounds with a prolonged expiratory phase on lung exam with a normal cardiac exam. Laboratory investigation showed normal complete blood counts, haemoglobin 15 g/dL, and normal chemistries. Compared to his previous studies, a pulmonary function study showed stable parameters with a FEV1 1.47 L (69%), FVC/FEV1 ratio 0.44 (62%), and a DLCO/alveolar volume ratio of 2.12 (49%). A room air arterial blood gas revealed pH 7.41, PCO2 44 mmHg, and PO2 61 mmHg, with 92% oxygen saturation. A six minute treadmill exercise test performed to assess the need for supplemental oxygen showed that he required supplemental oxygen at 1L/min via nasal cannula to eliminate hypoxemia during exercise. His chest radiograph was significant for hyperinflation and prominence of interstitial markings. A high resolution computed tomography of the chest demonstrated severe centrilobular and panacinar emphysema only. A baseline electrocardiogram (EKG) showed normal sinus rhythm with an old anterior wall infarct (Figure 1). Echocardiography of the heart revealed a normal left ventricle with an ejection fraction of 65%. Right ventricular systolic function was normal although elevated mean pulmonary arterial pressure of 55 mmHg was noted. A diagnostic polysomnogram performed for evaluation of daytime fatigue and snoring at night revealed mild OSA with an AHI of 6/hr. with sleep time spent with oxygen saturation below 90% (T-90%) of 19%. The EKG showed normal sinus rhythm. A full overnight polysomnogram for continuous positive airway pressure (CPAP) titration performed for treatment of sleep disordered breathing was sub-optimal, however it demonstrated an apnoea–hypopnea index (AHI) of 28 during REM (rapid eye movement) sleep, and a T-90% of 93%. The associated electrocardiogram showed Wenckebach second degree AV heart block during REM sleep usually near the nadir of oxygen desaturation. On a repeat positive airway pressure titration study, therapy with Bilevel pressures (BPAP) of 18/14 cmH20 corrected the AHI and nocturnal hypoxemia to within normal limits during Non REM (NREM) and REM sleep. His electrocardiogram remained in normal sinus rhythm .A twenty-four hour cardiac holter monitor revealed baseline sinus rhythm and confirmed the presence of second degree AV block of the Wenckebach type. A one month cardiac event recording showed normal sinus rhythm with frequent episodes of second degree AV block. These varied from Type I progressing to Type II with a 2:1 and 3:1 AV block, during sleep. Progression to complete heart block was noted with the longest pause lasting 3.9 seconds during sleep. The patient underwent an electrophysiology study with placement of a dual chamber pacemaker. He was initiated on BIPAP therapy. Subsequently, the patient was seen in clinic with improvements in his intermittent episodes of shortness of breath, fatigue, and daytime sleepiness.
Figure 1- Patient’s baseline EKG, normal sinus rhythm. Figure 2 -Progression to Mobitz Type II block 5:07 am. Figure 3 and 4- Sinus pauses, longest interval 11:07 pm 3.9 seconds (Figure 4).
Discussion
In healthy individuals, especially athletes, bradycardia, Mobitz I AV block, and sinus pauses up to 2 seconds are common during sleep and require no intervention5. Cardiac rhythm is controlled primarily by autonomic tone. NREM sleep is accompanied by an increase in parasympathetic, and a decrease in sympathetic, tone. REM sleep is associated with decreased parasympathetic tone and variable sympathetic tone. Bradyarrhythmias in patients with OSA are related to the apnoeic episodes and over 80% are found during REM sleep. During these periods of low oxygen supply, increased vagal activity to the heart resulting in bradyarrhythmias may actually be cardioprotective by decreasing myocardial oxygen demand. This may be important in patients with underlying coronary heart disease.
Some studies have found that Mobitz I AV block may not be benign. Shaw6 et al studied 147 patients with isolated chronic Mobitz I AV block. They inserted pacemakers in 90 patients, 74 patients were symptomatic and 16 patients received a pacemaker for prophylaxis. Outcome data included five-year survival, deterioration of conduction to higher degree AV block, and new onset of various forms of symptomatic bradycardia. They concluded that survival was higher in the paced groups and that risk factors for poor outcomes in patients with Mobitz I included age greater than 45 years old, symptomatic bradycardia, organic heart disease, and the presence of a bundle branch block on EKG.
The Sleep Heart Health Study7 found a higher prevalence of first and second-degree heart block among subjects with sleep-disordered breathing (SDB) than in those without (1.8% vs. 0.3% and 2.2 vs. 0.9%, respectively). Gami et al8observed thatupon review of 112 Minnesota residents who hadundergone diagnostic polysomnography and subsequentlydied suddenly from a cardiac cause, sudden death occurred between the hours of midnight and 6:00 AM in 46% of those with OSA, as compared with 21% of those without OSA. In a study of twenty-three patients with moderate to severe OSA who were each implanted with an insertable loop recorder, about 50% were observed to have frequent episodes of bradycardia and long pauses (complete heart block or sinus arrest) during sleep9. These events showed significant night-to-night intra individual variability and their incidence was under-estimated, only 13%, by conventional short-term EKG Holter recordings.
Physiologic factors predisposing patients with OSA to arrhythmias include alterations in sympathetic and parasympathetic nervous system activity, acidosis, apnoea’s, and arousal2, 10, 11. Some patients with OSA may have an accentuation of the ‘Diving Reflex’. This protective reflex consists of hypoxemia-induced sympathetic augmentation to muscles and vascular beds associated with increased cardiac vagal activity which results in increased brain perfusion, bradycardia and decreased cardiac oxygen demand. In patients with cardiac ischemia, poor lung function (i.e. COPD), or both, it may be difficult to differentiate between these protective OSA-associated Bradyarrhythmias and those which may lead to sudden death. It has been well established that patients with COPD are at higher risk for cardiovascular morbidity12 and arrythmias13. Fletcher14 and colleagues reported that the effects of oxygen supplementation on AHI, hypercapnea and supraventricular arrhythmias in patients with COPD and OSA were variable. Out of twenty obese men with COPD studied, in most patients oxygen eliminated the bradycardia observed during obstructive apnoea’s and eliminated AV block in two patients. In some patients supplemental oxygen worsened end-apnoea respiratory acidosis however this did not increase ventricular arrhythmias.
CPAP therapy has been demonstrated to significantly reduce sleep–related Bradyarrhythmias, sinus pauses, and the increased risk for cardiac death 9, 15. Despite this, in certain situations placement of a pacemaker may be required. These include persistent life-threatening arrhythmias present in patients with severe OSAS on CPAP, arrhythmias in patients who are non-compliant with CPAP, and in patients who may have persistent sympathovagal imbalance and hemodynamic fluctuations resulting in daytime bradyarrhythmias16.
Our case is interesting since it highlights the importance of recognizing the association between OSA, COPD, and life-threatening cardiac arrhythmias. Primary care providers should note the possible association of OSA-associated bradyarrhythmias with life-threatening Type II bradyarrhythmias and pauses. Since bradyarrhythmias related to OSA are relieved by CPAP, one option would be to treat with CPAP and observe for the elimination of these arrhythmias using a 24hour holter or event recorder17. Compliance with CPAP is variable and if life-threatening bradycardia is present, placement of a permanent pacemaker may be preferred18.
Our patient is unusual because most studies showing a correlation with the severity of OSA and magnitude of bradycardia have included overweight patients without COPD19. This patient’s electrocardiogram revealed a Type II AV block at 5am (Figure 2). This is within the overnight time frame where patients with OSA have been observed to have an increased incidence of sudden death. Figures 3 and 4 show significant sinus pauses. In selected cases where patients have significant co-morbidities (i.e. severe COPD with OSA), in addition to treatment with positive airway pressure, electrophysiological investigation with placement of a permanent pacemaker may be warranted.
Nosocomial pneumonia in patients receiving mechanical ventilation, also called ventilator-associated pneumonia (VAP), is an important nosocomial infection worldwide which leads to an increased length of hospital stay, healthcare costs, and mortality.(1,2,3,4,5) The incidence of VAP ranges from 9% to 27% with a crude mortality rate that can exceed up to 50%. (6,7,8,9) Aspiration of bacteria from the upper digestive tract is an important proposed mechanism in the pathogenesis of VAP.(9, 10) The normal flora of the oral cavity may include up to 350 different bacterial species, with tendencies for groups of bacteria to colonize different surfaces in the mouth. For example, Streptococcus mutans, Streptococcus sanguis, Actinomyces viscosus, and Bacteroides gingivalis mainly colonize the teeth; Streptococcus salivarius mainly colonizes the dorsal aspect of the tongue; and Streptococcus mitis is found on both buccal and tooth surfaces.(11) Because of a number of processes, however, critically ill patients lose a protective substance called fibronectin from the tooth surface. Loss of fibronectin reduces the host defence mechanism mediated by reticuloendothelial cells. This reduction in turn results in an environment conducive to attachment of microorganism to buccal and pharyngeal epithelial cells.(12) Addressing the formation of dental plaque and its continued existence by optimizing oral hygiene in critically ill patients is an important strategy for minimizing VAP.(13) Two different interventions aimed at decreasing the oral bacterial load are selective decontamination of the digestive tract involving administration of non absorbable antibiotics by mouth, through a naso-gastric tube, and oral decontamination, which is limited to topical oral application of antibiotics or antiseptics.(14) Though meta-analysis of antibiotics in decontamination of digestive tracts have found positive results(15) , the use of this intervention is, however, limited by concern about the emergence of antibiotic resistant bacteria.(16) One alternative to oral decontamination with antibiotics is to use antiseptics, such as chlorhexidine which act rapidly at multiple target sites and accordingly may be less prone to induce drug resistance.(17) Recently a meta-analysis of four trials on chlorhexidine failed to show a significant reduction in rates of ventilator associated pneumonia(18) but, subsequent randomised controlled trials, however, suggested benefit from this approach.(19) Current guidelines from the Centres for Disease Control and Prevention recommend topical oral chlorhexidine 0.12% during the perioperative period for adults undergoing cardiac surgery (grade II evidence). The routine use of antiseptic oral decontamination for the prevention of ventilator associated pneumonia, however, remains unresolved.(8) Despite the lack of firm evidence favouring this preventive intervention, a recent survey across 59 European intensive care units from five countries showed that 61% of the respondents used oral decontamination with chlorhexidine. As the emphasis on evidence based practice is increasing day by day, integrating recent evidence by meta-analysis could greatly benefit patient care and ensure safer practices. Hence we carried out this meta-analytic review to ascertain the effect of oral decontamination using chlorhexidine in the incidence of ventilator associated pneumonia and mortality in mechanically ventilated adults.(20)
Methods
Articles published from 1990 to May 2011 in English which were indexed in the following databases were searched: CINAHL, MEDLINE, Joanna Briggs Institute, Cochrane Library, EMBASE, CENTRAL, and Google search engine. We also screened previous meta-analyses and the references lists from all the retrieved articles for additional studies. Further searches were carried out in two trial registers (www.clinicaltrials.gov/ and www.controlled-trials.com/) and on web postings from conference proceedings, abstracts, and poster presentations.
Articles retrieved were assessed for inclusion criteria by three independent reviewers from the field of nursing with masters degrees. The inclusion criteria set for this meta-analysis were as follows: a) VAP definition meeting both clinical and radiological criteria b) Intubation for more than 48 hours in ICU.
We excluded the studies where clinical pulmonary infection score alone was considered for diagnosing VAP. Thereafter the articles were evaluated for randomisation, allocation concealment, blinding techniques, clarity of inclusion and exclusion criteria, outcome definitions, similarity of baseline characteristics, and completeness of follow-up. We considered randomisation to be true if the allocation sequence was generated using computer programs, random number tables, or random drawing from opaque envelopes. Finally, based on the above characteristics, only 9 trials which fulfilled the inclusion criteria was included for the pooled analysis. A brief summary of the 9 trials were listed in Table 1. The primary outcomes in this meta-analysis were incidence of VAP and mortality rate.
Table 1: Brief summary of trials
Source
Subjects
Intervention
ComparedWith
Outcome with respect to VAP
Outcome with respect to Mortality
C
E
C
E
DeRiso et al., 1996
353- Open Heart surgery patients
Chlorhexidine 0.12% 15 ml preoperatively and twice daily postoperatively until discharge from intensive care unit or death
Placebo
9/180
3/173
10/180
2/173
Fourrier et al., 2000
60- Medical and surgical patients
Chlorhexidine gel 0.2% dental plaque decontamination 3 times daily, compared with bicarbonate solution rinse 4 times daily followed by oropharyngeal suctioning until 28 days discharge form ICU or death
Standard treatment
15/30
5/30
7/30
3/30
Houston et al., 2002
561- cardiac surgery patients
Chlorhexidine 0.12% rinse compared with Listerine preoperatively and twice daily for 10 days postoperatively or until extubation, tracheostomy, death, or diagnosis of pneumonia.
Standard treatment
9/291
4/270
NA
NA
MacNaughton et al., 2004
194 – Medical and surgical patients
Chlorhexidine 0.2% oral rinse twice daily until extubation or death
Placebo
21/101
21/93
29/93
29/101
Fourrier et al., 2005
228 –ICU patients
Chlorhexidine 0.2% gel three times daily during stay in intensive care unit until 28 days
Placebo
12/114
13/114
24/114
31/114
Segers et al.,2005
954 – cardiac surgery patients
Chlorhexidine 0.12%, nasal ointment, and 10 ml oropharynx rinse four times daily on allocation and admission to hospital until extubation or removal of nasogastric tube
Placebo
67/469
35/485
6/469
8/485
Boop et al., 2006
5- cardiac surgery patients as pilot study
0.12% chlorhexidine gluconate oral care twice daily until discharge
Standard treatment
1/3
0/2
NA
NA
Koeman et al., 2006
385 –General ICU patients
2 treatment group: 2%Chlorhexidine, chlorhexidine and colistin, placebo four times daily until diagnosis of ventilator associated pneumonia, death, or extubation
Placebo
23/130
13/127
39/130
49/127
Tontipong et al., 2008
207 –General medical ICU or wards
2% chlorhexidine solution times per day until endotracheal tubes were removed.
Standard treatment
12/105
5/102
37/105
36/102
NA-Not available; C-Control group; E- Experimental group
Data analysis
Meta-analysis was performed in this study by using Review Manager 4.2 (Cochrane Collaboration, Oxford) with a random effect model. The pooled effects estimates for binary variables were expressed as a relative risk with 95% confidence interval. Differences in estimates of intervention between the treatment and control groups for each hypothesis were tested using a two sided z test. We calculated the number of patients needed to treat (NNT, with 95% confidence interval) to prevent one episode of ventilator associated pneumonia during the period of mechanical ventilation. A chi-squared test was used to assess the heterogeneity of the results. A Forest plot graph was drawn using Stats direct software version 2.72 (England: Stats Direct Ltd. 2008). We considered a two tailed P value of less than 0.05 as significant throughout the study.
Results
Effect of Chlorhexidine in reducing the Incidence of VAP
A total of nine trials were included in this meta-analysis(19,21,22,23,24,25,26,27,28). Pooled analysis of the nine trials with 2819 patients revealed a significant reduction in the incidence of VAP using chlorhexidine (Relative risk 0.60, 0.47 to 0.76; P< 0.01) (Figure 1). In relation to the Number Needed to Treat (NNT), 21 patients would need to receive oral decontamination with Chlorhexidine to prevent one episode of Ventilator associated pneumonia (NNT 21, 14 to 38).
Figure 1: Forest Plot showing the effect of Chlorhexidine oral decontamination in preventing the incidence of ventilator-associated pneumonia. Test for heterogeneity:χ2 =15.5, df =8, p < 0.01. Test for overall effect: z =4.33, p <0.05.
Effect of Chorhexidine in overall mortality rate
For assessing the outcomes in terms of mortality, only seven out of nine trials were included, since the other two(23,27) did not report the mortality rate. Pooled analysis of the seven trials with 2253 patients revealed no significant effect in reducing the overall mortality rate in patient who received chlorhexidine oral decontamination.(Relative risk 1.02, 0.83 to 1.26; P= 0.781 (Figure 2).
Figure 2: Forest plot showing the effect of Chlorhexidine oral decontamination in reducing overall mortality rate. Test for heterogeneity:χ2 =0.05, df =6, p = 0.81. Test for overall effect: z =0.27, p = 0.78
Discussion
The effectiveness of oral decontamination to prevent VAP in patients undergoing mechanical ventilation has remained controversial since its introduction, due to partly discordant results of individual trials. In the present meta-analysis nine trials were included to estimate the pooled effect size; the results revealed a significant reduction in the incidence of VAP among patients who were treated with oral chlorhexidine. But, it had no effect in reducing the overall mortality rate among these patients. There is a firm body of evidence that oropharyngeal colonization is pivotal in the pathogenesis of VAP. More than 25 years ago, Johanson et al described associations between increasing severity of illness, higher occurrence of oropharyngeal colonization, and an increased risk of developing VAP .(29,30)Subsequently, cohort and sequential colonization analyses identified oropharyngeal colonization as a important risk factor for VAP. (31,32,33) Our finding confirms the pivotal role of Oro- pharyngeal colonization in the pathogenesis of VAP , since this meta-analysis indicates that oral decontamination may reduce the incidence of VAP. Chlorhexidine was proven to have excellent antibacterial effects, with low antibiotic resistance rates seen in nosocomial pathogens, despite long-term use(34). Previous meta-analyses examining the effect of prophylaxis using selective decontamination of the digestive tract reported a significant reduction in the incidence of ventilator associated pneumonia(35,36,37). The most recent meta-analysis indicated that such an intervention combined with prophylactic intravenous antibiotics reduces overall mortality(38). In comparison our review suggests that oral antiseptic prophylaxis alone can significantly reduce the incidence of ventilator associated pneumonia, but not mortality. A similar result was documented by Ee Yuee Chan et al (2007)(14) who performed a meta-analysis with seven trials with a total of 2144 patients and found a significant result (Odds ratio 0.56, 0.39 to 0.81). Another comparable finding in the present study was, Mortality rate was not influenced by use of Chlorhexidine use, which was in line with the findings of Ee Yuee Chan et al (2007)(14) . Our meta-analysis on Chorhexidine differs from the findings of Pineda et al, who pooled four trials on chlorhexidine and did not report lower rates of ventilator associated pneumonia (odds ratio 0.42, 0.16-1.06; P=0.07)(18) . Our results also extend those of Chlebicki et al, who did not find a statistically significant benefit using the more conservative random effects model after pooling seven trials on chlorhexidine (relative risk 0.70, 0.47- 1.04; P=0.07), although their results were significant with the fixed effects model(39). Our meta-analysis included larger data set with a total of 9 trials including recent trials(28) which further adds strength to our analysis.
Limitations
Though our literature search was comprehensive, it is possible that we missed other relevant trials. Electronic and hand searches do not completely reflect the extent of research outcomes. For example, trials reported at conferences are more likely than trials published in journals to contain negative reports. In addition, more positive than negative results tend to be reported in the literature. This failure to publish more studies with negative outcomes is probably more due to authors’ lack of inclination to submit such manuscripts than to the unwillingness of editors to accept such manuscripts. Furthermore, many studies not published in English were not included e.g. a study by Zamora Zamora F (2011).(40) These limitations may lead to a risk for systematic reviews to yield a less balanced analysis and may therefore affect the recommendations resulting from the reviews. In addition, the heterogeneity which we found among the trials with respect to populations enrolled, regimens used, outcome definitions, and analysis strategies, may limit the ability to generalize results to specific populations.
Conclusion
The finding that chlorhexidine oral decontamination can reduce the incidence of ventilator associated pneumonia could have important implications for lower healthcare costs and a reduced risk of antibiotic resistance compared with the use of antibiotics. These results should be interpreted in light of the moderate heterogeneity of individual trial results and possible publication bias. It may not be prudent to adopt this practice routinely for all critically ill patients until strong data on the long term risk of selecting antiseptic and antibiotic resistant organisms are available. Nevertheless, Chlorhexidine oral decontamination seems promising. Further studies are clearly needed in testing the effect of Chlorhexidine in specific populations with standard protocols (which includes specific concentration, frequency, and type of agents) to generalize the findings. Studies also may be done to test the effect of different oral antiseptics in reducing VAP, so as to enrich the body of knowledge within this area.
Although one cell type may predominate, teratomas usually comprise of tissue from all three embryonic germ layers1. Generally arising from the gonads, they may be found in extra-gonadal sites such as sacro-coccygeal region, mediastinum, neck and retroperitoneum.2 Here we report a case of retroperitoneal teratoma in an adult with successful surgical treatment. Its clinical presentation, diagnosis and treatment are reviewed.
Case Report:
A woman aged 28 years presented with pain in the right hypochondrium of one year duration. There was no associated bowel or urinary symptom. Examination showed minimal fullness in the right hypochondrium. Routine blood tests and urinalysis were within normal limits. A plain abdominal radiograph showed calcification in the right side of the abdomen (Fig. 1). Ultrasonography demonstrated 13.6 x 8.1 cm soft tissue mass in the retro-peritoneum between liver and the right kidney. It was heterogeneous, well circumscribed with sharply defined borders, and had some calcification and cystic areas. CT abdomen revealed a hypo-dense lesion between liver and the right kidney. It had fatty attenuation with internal hyper-dense areas representing calcification. (Fig. 2). Provisional diagnosis of a retroperitoneal teratoma was made and an open exploration was performed with a right sub-costal incision. There was a large cystic mass behind the ascending colon, duodenum and the pancreas. It was located in the retroperitoneal compartment. There were dense, fibrous adhesions of the mass with aorta but entire cystic mass was excised successfully.
Post operatively this tumor mass measuring 5 x 5 cm was excised in vitro and found to be filled with yellowish creamy material containing hair, sebum and bony tissue. Microscopically it was confirmed to be a cystic teratoma with no malignancy. Stratified squamous epithelium with sebaceous and sweat glands, hair shafts, calcification, few bony spicules and bone marrow elements were all demonstrated. (Fig. 3). The post operative course was uneventful and she was well at the 2 months follow up.
Figure 1. Plain abdominal radiograph showing radio-opaque shadow (arrow heads) in the right upper abdomen.
Figure 2: Computed Tomography showing an encapsulated mass that contains multiple tissue elements including fat and areas of calcification.
Figure 3: Microscopic examination of the tumor showing squamous epithelium (SE), hair shaft (HS), sebaceous glands (SBG)
Discussion:
Teratomas are congenital tumours arising from pluri-potential embryonic cells and therefore have several recognizable somatic tissues3, Teratomas are usually localized to the ovaries, testis, anterior mediastinum or the retro-peritoneal area in descending order of frequency.4 Teratomas constitute less than 10% of all primary retroperitoneal tumours and hence are relatively uncommon5. Furthermore, retroperitoneal teratomas occur mainly in children and have been very rarely described in the adults. Half of these cases present in children less than 10 years of age and only a fifth of them present after 30 years of age. Retroperitoneal teratomas are often located near the upper pole of the kidney with preponderance on the left. The case described here is therefore unusual in that it was a primary retroperitoneal teratoma in an adult, on the right side and with adhesions to the aorta.
Retroperitoneal teratomas are seen in females twice as commonly than males. Teratomas are usually benign if they are cystic and contain sebum or mature tissue. They are more likely to be malignant if they are solid and have immature embryonic tissue like fat, cartilage, fibrous and bony elements.6 In these regards our case is similar to other described cases as our patient is also female and as her teratoma was cystic, it showed lack of malignancy.
Teratomas are usually asymptomatic as the retroperitoneal space is extensive enough to allow for their free growth. When compression of the surrounding structure occurs, patients may get compression symptoms.The diagnosis of a retroperitoneal teratoma cannot be made on clinical grounds alone. Ultrasound and computed tomography are important in its diagnosis and may show the presence of calcification, teeth or fat. Calcification on the rim of tumour or inside the tumour is seen in 53-62% of teratomas and although radiologically three quarters of patients with a benign teratoma may have calcification within it, a quarter of malignant cases may also demonstrate calcification. Computed tomography is better than Ultrasonography in defining the extent and spread of teratoma to the surrounding organs.7
The prognosis is excellent for benign retroperitoneal teratoma if complete resection can be accomplished.
Nerve blocks have a variety of applications in anaesthesia enabling an extra dimension for patients with regards to their pain control and anaesthetic plan. Anaesthetists can perform nerve blocks by a range of methods including landmark techniques and ultrasound guidance, with both of these techniques having the potential to be used with a nerve stimulator.
Nerve blocks are associated with complications including nerve damage, bleeding, pneumothorax and failure. Ultrasound, if used correctly, may help limit such complications.1 NICE guidance on the use of ultrasound guidance for procedures, has evolved over the years. Ultrasound guidance is now considered an essential requirement for the placement of central venous lines2 and is recommended when performing nerve blocks.3
Method
This survey aimed to assess the methods used by anaesthetists in performing nerve blocks and audited the use and competencies of clinicians in performing such blocks under ultrasound guidance and landmark techniques. This survey also looked at whether performing nerve blocks under ultrasound guidance was hindered by the lack of availability of appropriate resolution ultrasound machines in the workplace.
A paper survey was completed by anaesthetists of all grades at Kettering general hospital, UK and Birmingham Heartlands Hospital, UK between October and December 2011. The survey consisted of a simple, easy to use, tick box table and a generic area in which participants made further contributions. From this we ascertained the following:
Grade of clinician.
Any courses undertaken in ultrasound guided nerve blocks.
Which nerve blocks the clinicians felt they could perform competently with either method (landmark versus ultrasound guided).
In the event the anaesthetist could perform a block with or without ultrasound guidance; which method was used if ultrasound equipment was available.
Was the ability to perform ultrasound guided nerve blocks limited by the availability of an ultrasound machine.
The term “landmark technique” is used when the landmark technique is combined with or without a nerve stimulator and the term “ultrasound technique” when ultrasound guidance is used with or without a nerve stimulator.
Results
We surveyed a total of 52 anaesthetists, subdivided into Consultants 26 (50%), ST/staff grade 17 (33%), CT trainees 9 (17%). Of all grades, only 50% had completed a course in ultrasound guided nerve blocks. 42% of clinicians had encountered situations when they could not use ultrasound guidance for a nerve block because there was no ultrasound machine available at the time of the procedure.
The competencies of clinicians with the landmark and ultrasound technique varied depending on the type of nerve block and the grade of clinician (figure 1).
Various routinely performed blocks were surveyed and this revealed a good comparison of the use of ultrasound and landmark technique. For the Interscalene block, the consultants and middle grades combined were competent in performing this block, with the landmark technique 56% and the ultrasound technique 33%. For the Lumbar plexus block, 0% of the consultants surveyed felt competent in performing this block with the ultrasound technique compared to 73% with the landmark technique. The majority of clinicians felt competent in performing the TAP block with the ultrasound technique, 65% versus 35%, for the landmark technique.
Consultant (%) n-26
ST/Staff Grade (%) n-17
CT1/2 (%) n-9
Nerve block
Competent Landmark
Competent US
Competent Landmark
Competent US
Competent Landmark
Competent US
Brachial Plexus
Interscalene
54
34
58
29
0
0
Supra/Infra clavicular
31
23
29
18
0
0
Axillary
31
31
47
18
0
0
Elbow
12
19
29
12
0
0
Lumbar Plexus
73
0
65
12
11
0
Sciatic
Anterior
39
8
64
12
0
0
Posterior
42
27
76
18
0
0
Femoral
100
69
100
76
36
11
Epidural
100
19
100
18
36
0
Spinal
100
12
100
18
56
0
Abdominal
TAP
38
85
29
65
33
11
Rectus Sheath
19
35
18
47
0
11
Figure 1. This table illustrates competencies for different nerve blocks with the landmark technique and ultrasound technique for different grades of anaesthetists.
Discussion
The findings of this survey and audit have a range of implications for anaesthetists in the workplace:
1) Junior grades of doctors do not feel competent in performing nerve blocks. This may lead to a reliance on senior doctors during on calls to assist in performing blocks such as femoral and TAP blocks. Specific training geared towards junior doctors to make them proficient in such blocks would enable them to provide an anaesthetic plan with more autonomy.
2) A large percentage of consultant grade clinicians felt competent in performing nerve blocks with the landmark technique but not in performing the same blocks with ultrasound guidance. This has implications for training because consultants are the training leads for junior grades of anaesthetists. If consultants do not feel competent in the use of ultrasound guidance for nerve blocks, this could lead to a self perpetuating cycle.
3) Only 50% of clinicians in this survey had completed a course for ultrasound guided nerve blocks, this coupled with the finding that clinicians did not feel comfortable in performing nerve blocks with ultrasound, indicates the possible need for local training accessible to clinicians to improve their everyday practice.
4) It has been shown that ultrasonic guidance improves the success rate of interscalene blocks.4 The practice amongst clinicians in this survey reveals that the majority of anaesthetists (middle and consultant grades) are competent with the landmark technique 56% compared to the ultrasound technique 36%. This also highlights a training deficit which if addressed would enable clinicians to offer a more successful method of performing the interscalene block.
5) This survey highlighted the lack of availability of appropriate ultrasound machines in different departments, leading to some clinicians utilising the landmark technique, when ultrasound guidance was the preference. This has the potential of a patient receiving a nerve block technique which may have been riskier and less efficient. This highlights a potential need for investment and accessibility of appropriate resolution ultrasound machines in the different work places of a hospital environment.
The main limitation of this project was the small number of clinicians in the respective hospitals the survey was performed in. However, we feel the results reflect the practice of clinicians across most anaesthetic departments. The recommendations highlight a training need for anaesthetic trainees in the use of ultrasound guided nerve blocks. This survey could form the basis of a much larger survey of clinicians across the UK to provide a more insightful review of the competencies and preferences of anaesthetic trainees in performing nerve blocks and the availability of appropriate resolution ultrasound machines.
The difference in the number of clinicians in each category limited comparisons between groups. A larger cohort of participants would enable comparison of nerve block techniques between different grades of clinicians.
This survey included all clinicians regardless of their sub-specialist interest. This may result in a skewing of results, depending on the area of interest of the clinicians surveyed.
This work only highlights the competencies and preferences of clinicians in performing nerve blocks. No extrapolation can be made to complications that arise from the choice of either technique. Studies have shown an improved success rate when performing nerve blocks with ultrasound.4 However this does not directly apply to a specific clinician who may have substantial experience in their method of choice in performing a nerve block.
Even though it is commonly seen in Graves' disease, TPP is not related to the etiology, severity, and duration of thyrotoxicosis. 1
The pathogenesis of hypokalaemic periodic paralysis in certain populations with thyrotoxicosis is unclear. Transcellular distribution of potassium is maintained by the Na+/K+–ATPase activity in the cell membrane, and it is mainly influenced by the action of insulin and beta-adrenergic catecholamines.2 Hypokalemia in TPP results from an intracellular shift of potassium and not total body depletion. It has been shown that the Na+/K+–ATPase activity in platelets and muscles is significantly higher in patients with TPP.3 Hyperthyroidism may result in a hyperadrenergic state, which may lead to the activation of the Na+/K+–ATPase pump and result in cellular uptake of potassium.2, 4, 5 Thyroid hormones may also directly stimulate Na+/K+– ATPase activity and increase the number and sensitivity of beta receptors.2, 6 Patients with TPP have been found to have hyperinsulinemia during episodes of paralysis. This may explain the attacks after high-carbohydrate meals.7
CASE REPORT:
A 19 year old male patient presented to our emergency room with sudden onset weakness of lower limbs. He was not able to stand or walk. Power of 0/5 in both lower limbs and 3/5 in upper limbs was noticed on examination. Routine investigations revealed to have severe hypokalemia with a serum potassium of 1.6 meq/l (normal range 3.5-5.0 meq/l), a serum phosphorus level of 3.4 mg/dl (normal range 3-4.5 mg/dl) and mild hypomagnesemia with serum magnesium level of 1.5mg/dl (normal range 1.8-3.0 mg/dl). ECG showed hypokalemic changes with prolonged PR interval, increased P-wave amplitude and widened QRS complexes. He was managed on intravenous as well oral potassium and history revealed weight loss, increased appetite and tremors from past 4 months. He had a multinodular goiter and radioactive iodine uptake scan (Iodine 131) showed a toxic nodule (Toxic nodule shows increased iodine uptake while the rest of the gland is suppressed) with no exophthalmos, sensory or cranial nerve deficits. Thyroid function tests revealed thyrotoxicosis with free T4 of 4.3ng/dl (normal range 0.8-1.8ng/dl), T3 of 279 ng/dl (normal range = 60 - 181 ng/dl) and a TSH level of <0.15milliunits/L (normal range = 0.3 - 4 milliunits/L). He was managed on intravenous potassium & propanolol. The patient showed dramatic improvement of his symptoms. The patient was discharged home on carbamazole with the diagnosis of TPP secondary to toxic nodular goiter.
In this case there was a significant family history as one of his elder brother had a sudden death (cause not known) and his mother was primary hypothyroid on levothyroxin replacement therapy.
DISCUSSION :
TPP is seen most commonly in Asian populations, with an incidence of approximately 2% in patients with thyrotoxicosis of any cause.1,8,9,10 The attacks of paralysis have a well-marked seasonal incidence, usually occurring during the warmer months.1 Pathogenesis of hypokalaemia has been explained by some authors to be due to an intracellular shift of body potassium, which is catecholamine mediated.11,12 Shizume and his group studied total exchangeable potassium which revealed that patients with thyrotoxic periodic paralysis were not significantly different from controls when the value was related to lean body mass.11 The paralytic symptoms and signs improve as the potassium returns from the intracellular space back into the extracellular space.13 The diurnal variation in potassium movement where there is nocturnal potassium influx into skeletal muscle would explain the tendency for thyrotoxic periodic paralysis to occur at night.14 Hypophosphataemia and hypomagnesaemia are also known to occur in association with thyrotoxic periodic paralysis.14,15,16,17,18 The correction of hypophosphataemia without phosphate administration supports the possibility of intracellular shift of phosphate.16 Electrocardiographic findings supportive of a diagnosis of TPP rather than sporadic or familial periodic paralysis are sinus tachycardia, elevated QRS voltage and first-degree AV block (sensitivity 97%, specificity 65%).20 In addition to ST-segment depression, T-wave flattening or inversion and the presence of U waves are typical of hypokalaemia.
The management is to deal with the acute attack as well as treatment of the underlying condition to prevent future attacks. Rapid administration of oral or intravenous potassium chloride can abort an attack and prevent cardiovascular and respiratory complications.4 A small dose of potassium is the treatment of choice for facilitating recovery and reducing rebound hyperkalaemia due to release of potassium and phosphate from the cells on recovery.1,2,3 Rebound hyperkalaemia occurred in approximately 40% of patients with TPP, especially if they received >90 mmol of potassium chloride within the first 24 hours.4 Another mode of treatment is to give propranolol, a nonselective b-blocker, which prevents the intracellular shift of potassium and phosphate by blunting the hyperadrenergic stimulation of Na+/K+–ATPase.20 Hence, initial therapy for stable TPP should include propranolol.21,22,23 The definitive therapy for TPP includes treatment of hyperthyroidism with antithyroid medications, surgical thyroidectomy, or radioiodine therapy.
Normal sleep is divided into Non-REM and REM. REM occurs every 90-120 minutes during adult sleep throughout the night with each period of REM progressing in length such that the REM periods in the early morning hours are the longest and may last from 30-60 minutes. Overall, REM accounts for 20-25% of the sleep time but is weighted toward the second half of the night. During REM sleep with polysomnography monitoring one observes a low voltage mixed frequency amplitude EEG and low voltage EMG in the chin associated with intermittent bursts of rapid eye movements. During the periods of REM breathing becomes irregular, blood pressure rises and the heart rate also increases due to excess adrenergic activity. The brain is highly active during REM and the electrical activity recorded in the brain by EEG during REM sleep is similar to that of wakefulness.
Parasomnias are undesirable, unexpected, abnormal behavioral phenomena that occur during sleep. There are three broad categories in parasomnias. They are
Disorders of Arousal (from Non-REM sleep)
Parasomnias usually associated with REM sleep, and
Other parasomnias which also includes secondary type of parasomnias.
RBD is the only parasomnia which requires polysomnographic testing as part of the essential diagnostic criteria.
Definition of RBD
“RBD is characterized by the intermittent loss of REM sleep electromyographic (EMG) atonia and by the appearance of elaborate motor activity associated with dream mentation” (ICSD-2).1 These motor phenomena may be complex and highly integrated and often are associated with emotionally charged utterances and physically violent or vigorous activities. RBD was first recognized and described by Schenck CH et al. in 1986.2 This diagnosis was first incorporated in the International Classification of Sleep Disorders (ICSD) in 1990. (American Academy of Sleep Medicine)
A defining feature of normal REM sleep is active paralysis of all somatic musculature (sparing the diaphragm to permit ventilation). This result in diffuse hypotonia of the skeletal muscles inhibiting the enactment of dreams associated with REM sleep. In RBD there is an intermittent loss of muscle atonia during REM sleep that can be objectively measured with EMG as intense phasic motor activity (figure 1 and 2).
Figure 1
Figure 2
This loss of inhibition often precedes the complex motor behaviors during REM sleep. Additionally, RBD patients will report that their dream content is often very violent or vigorous dream enacting behaviors include talking, yelling, punching, kicking, sitting, jumping from bed, arm flailing and grabbing etc. and most often the sufferer will upon waking from the dream immediately report a clear memory of the dream which coincides very well with the high amplitude violent defensive activity witnessed. This complex motor activity may result in a serious injury to the dreamer or bed partner that then prompts the evaluation.
Prevalence
The Prevalence of RBD is about 0.5% in general population.1, 3 RBD preferentially affect elderly men (in 6th and 7th decade) with ratio of women to men being 1 to 9.4 The mean age of disease onset is 60.9 years and at diagnosis is 64.4 years.5 RBD was reported in an 18 year old female with Juvenile Parkinson disease,6 so age and gender are not absolute criteria.
In Parkinson disease (PD) the reported prevalence ranges from 13-50%,7, 14-19 LewyBody Dementia (DLB) 95%,8 and Multiple System Atrophy (MSA) 90 %.9 The presence of RBD is a major diagnostic criterion for MSA. RBD has been reported in Juvenile Parkinson disease, and pure autonomic failure10-12 all neurodegenerative disorders are synucleinopathies.13
Physiology
The neurons of locus coeruleus, raphe nuclei, tuberomammillary nucleus, pedunculopontine nucleus, laterodorsal tegmental area and the perifornical area are firing at a high rate, and cause arousal by activating the cerebral cortex. During REM sleep, the aforementioned excitatory areas fall silent with the exception of the pedunculopontine nucleus and laterodorsal tegmental areas. These regions project to the thalamus and activate the cortex during REM sleep. This cortical activation is associated with dreaming in REM. Descending excitatory fibers from the pedunculopontine nucleus and laterodorsal tegmental area innervate the medial medulla, which then sends inhibitory projections to motor neurons producing the skeletal muscle atonia of REM sleep.20-21
There are two distinct neural systems which collaborate in the “paralysis” of normal REM sleep, one is mediated through the active inhibition by neurons in the nucleus reticularis magnocellularis in the medulla via the ventrolateral reticulospinal tract synapsing on the spinal motor neurons and the other system suppresses locomotor activity and is located in pontine region.22
Pathophysiology
REM sleep contains two types of variables, tonic (occurring throughout the REM period), and phasic (occurring intermittently during a REM period). Tonic elements include desynchronized EEG and somatic muscle atonia (sparing the diaphragm). Phasic elements include rapid eye movements, middle ear muscle activity and extremity twitches. The tonic electromyogram suppression of REM sleep is the result of active inhibition of motor activity originating in the perilocus coeruleus region and terminating in the anterior horn cells via the medullary reticularis magnocellularis nucleus.
In RBD, the observed motor activity may result from either impairment of tonic REM muscle atonia or from increase phasic locomotor drive during REM sleep. One mechanism by which RBD results is the disruption in neurotransmission in the brainstem, particularly at the level of the pedunculopontine nucleus.23Pathogenetically, reduced striatal dopaminergic mediation has been found24-25 in those with RBD. Neuroimaging studies support dopaminergic abnormalities.
Types of RBD
RBD can be categorized based on severity:
Mild RBD occurring less than once per month,
Moderate RBD occurring more than once per month but less than once per week, associated with physical discomfort to the patient or bed partner, and
Severe RBD occurring more than once per week, associated with physical injury to patient or bed partner.
RBD can be categorized based on duration:
Acute presenting with one month or less,
Subacute with more than one month but less than 6 months,
Chronic with 6 months or more of symptoms prior to presentation.
Acute RBD: In 55 - 60% of patients with RBD the cause is unknown, but in 40 - 45% the RBD is secondary to another condition. Acute onset RBD is almost always induced or exacerbated by medications (especially Tri-Cyclic Antidepressants, Selective Serotonin Reuptake Inhibitors, Mono-Amine Oxidase Inhibitors, Serotonin Norepinephrine Reuptake Inhibitors,26 Mirtazapine, Selegiline, and Biperiden) or during withdrawal of alcohol, barbiturates, benzodiazepine or meprobamate. Selegiline may trigger RBD in patients with Parkinson disease. Cholinergic treatment of Alzheimer’s disease may trigger RBD.
Chronic RBD: The chronic form of RBD was initially thought to be idiopathic; however long term follow up has shown that many eventually exhibit signs and symptoms of a degenerative neurologic disorder. One recent retrospective study of 44 consecutive patients diagnosed with idiopathic RBD demonstrated that 45% (20 patients) subsequently developed a neurodegenerative disorder, most commonly Parkinson disease (PD) or Lewy body dementia, after a mean of 11.5 years from reported symptoms onset and 5.1 years after RBD diagnosis.27
The relationship between RBD and PD is complex and not all persons with RBD develop PD. In one study of 29 men presenting with RBD followed prospectively, the incidence of PD was 38% at 5 years and 65% after 12 years.7, 28, 29 Contrast this with the prevalence of the condition in multiple system atrophy, where RBD is one of the primary symptoms occurring in 90% of cases.9 In cases of RBD, it is absolutely necessary not only to exclude any underlying neurodegenerative disease process but also to monitor for the development of one over time in follow up visits.
Clinical manifestations
Sufferers of RBD usually present to the doctor with complaints of sleep related injury or fear of injury as a result of dramatic violent, potentially dangerous motor activity during sleep. 96% of patients reporting harm to themselves or their bed partner. Behaviors during dreaming described include talking, yelling, swearing, grabbing, punching, kicking, jumping or running out of the bed. One clinical clue of the source of the sleep related injury is the timing of the behaviors. Because RBD occurs during REM sleep, it typically appears at least 90 minutes after falling asleep and is most often noted during the second half of the night when REM sleep is more abundant.
One fourth of subjects who develop RBD have prodromal symptoms several years prior to the diagnosis. These symptoms may consist of twitching during REM sleep but may also include other types of simple motor movements and sleep talking or yelling.30-31 Day time somnolence and fatigue are rare because gross sleep architecture and the sleep-wake cycle remain largely normal.
RBD in other neurological disorders and Narcolepsy:
RBD has also been reported in other neurologic diseases such as Multiple Sclerosis, vascular encephalopathies, ischemic brain stem lesions, brain stem tumors, Guillain-Barre syndrome, mitochondrial encephalopathy, normal pressure hydrocephalus, subdural hemorrhage, and Tourette’s syndrome. In most of these there is likely a lesion affecting the primary regulatory centers for REM atonia.
RBD is particularly frequent in Narcolepsy. One study found 36% pts with Narcolepsy had symptoms suggestive of RBD. Unlike idiopathic RBD, women with narcolepsy are as likely to have RBD as men, and the mean age was found to be 41 years.32 While the mechanism allowing for RBD is not understood in this population, narcolepsy is considered a disorder of REM state disassociation. Cataplexy is paralysis of skeletal muscles in the setting of wakefulness and often is triggered by strong emotions such as humor. In narcoleptics who regularly experienced cataplexy, 68% reported RBD symptoms, compared to 14% of those who never or rarely experienced cataplexy.32-33 There is evidence of a profound loss of hypocretin in the hypothalamus of the narcoleptics with cataplexy and this may be a link that needs further investigation in the understanding of the mechanism of RBD in Narcolepsy with cataplexy. It is prudent to follow Narcoleptics and questioned about symptoms of RBD and treated accordingly, especially those with cataplexy and other associated symptoms.
Diagnostic criteria for REM Behavior Disorder(ICSD-2: ICD-9 code: 327.42)1
A. Presence of REM sleep without Atonia: the EMG finding of excessive amounts of sustained or intermittent elevation of submental EMG tone or excessive phasic submental or (upper or lower) limb EMG twitching (figure 1 and 2).
B. At least one of the following is present:
i. Sleep related injurious, potentially injurious, or disruptive behaviors by history
ii. Abnormal REM sleep behaviors documented during polysomnographic monitoring
C. Absence of EEG epileptiform activity during REM sleep unless RBD can be clearly distinguished from any concurrent REM sleep-related seizure disorder.
D. The sleep disturbance is not better explained by another sleep disorder, medical or neurologic disorder, mental disorder, medication use, or substance use disorder.
Differential diagnosis
Several sleep disorders causing behaviors in sleep can be considered in the differential diagnosis, such as sleep walking (somnambulism), sleep terrors, nocturnal seizures, nightmares, psychogenic dissociative states, post-traumatic stress disorder, nocturnal panic disorder, delirium and malingering. RBD may be triggered by sleep apnea and has been described as triggered by nocturnal gastroesophageal reflux disease.
Evaluation and Diagnosis
Detailed history of the sleep wake complaints
Information from a bed partner is most valuable
Thorough medical, neurological, and psychiatric history and examination
Screening for alcohol and substance use
Review of all medications
PSG (mandatory): The polysomnographic study should be more extensive, with an expanded EEG montage, monitors for movements of all four extremities, continuous technologist observation and continuous video recording with good sound and visual quality to allow capture of any sleep related behaviors
Multiple Sleep Latency Test (MSLT): Only recommended in the setting of suspected coexisting Narcolepsy
Brain imaging (CT or MRI) is mandatory if there is suspicion of underlying neurodegenerative disease.
Management
RBD may have legal consequences or can be associated with substantial relationship strain; therefore accurate diagnosis and adequate treatment is important, which includes non-pharmacological and pharmacological management.
Non-pharmacological management: Acute form appears to be self-limited following discontinuation of the offending medication or completion of withdrawal treatment. For chronic forms, protective measures during sleep are warranted to minimize the risks for injury to patient and bed partner. These patients are at fall risk due to physical limitations and use of medications. Protective measure such as removing bed stands, bedposts, low dressers and applying heavy curtains to windows. In extreme cases, placing the mattress on the floor to prevent falls from the bed has been successful.
Pharmacological management: Clonazepam is highly effective in treatment and it is the drug of choice. A very low dose will resolve symptoms in 87 to 90% of patients.4, 5, 7-34 Recommended treatment is 0.5 mg Clonazepam 30 minutes prior to bed time and for more than 90% of patients this dose remains effective without tachyphylaxis. In the setting of breakthrough symptoms the dose can be slowly titrated up to 2.0 mg. The mechanism of action is not well understood but clonazepam appears to decrease REM sleep phasic activity but has no effect on REM sleep atonia.35
Melatonin is also effective and can be used as monotherapy or in conjunction with clonazepam. The suggested dose is 3 to 12 mg at bed time. Pramipexole may also be effective36-38 and suggested for use when clonazepam is contraindicated or ineffective. It is interesting to note that during holidays from the drug, the RBD can take several weeks to recur. Management of patients with concomitant disorder like narcolepsy, depression, dementia, Parkinson disease and Parkinsonism can be very challenging, because medications such as SSRIs, selegiline and cholinergic medications used to treat these disorders, can cause or exacerbate RBD. RBD associated with Narcolepsy, clonazepam is usually added in management and it is fairly effective.
Follow-up
Because RBD may occur in association with neurodegenerative disorder, it is important to consult a neurologist for every patient with RBD as early as possible, especially to diagnose and provide care plan for neurodegenerative disorder, which includes but not limited to early diagnosis and management, regular follow up, optimization of management to provide better quality of life and address medico-legal issues.
Prognosis
In acute and idiopathic chronic RBD, the prognosis with treatment is excellent. In the secondary chronic form, prognosis parallels that of the underlying neurologic disorder. Treatment of RBD should be continued indefinitely, as violent behaviors and nightmares promptly reoccur with discontinuation of medication in almost all patients.
Conclusions
RBD and neurodegenerative diseases are closely interconnected. RBD often antedates the development of a neurodegenerative disorder; diagnosis of idiopathic RBD portends a risk of greater than 45% for future development of a clinically defined neurodegenerative disease. Once identified, close follow-up of patients with idiopathic RBD could enable early detection of neurodegenerative diseases. Treatment for RBD is available and effective for the vast majority of cases.
Key Points
Early diagnosis of RBD is of paramount importance
Polysomnogram is an essential diagnostic element
Effective treatment is available
Early treatment is essential in preventing injuries to patient and bed partner
Apparent idiopathic form may precede development of Neurodegenerative disorder by decades
Acute non-traumatic knee effusion is a common condition presenting to the Orthopaedic department which can be caused by a wide variety of diseases(Table 1). Septic arthritis is the most common and serious etiology. It can involve any joint; the knee is the most frequently affected. Accurate and swift diagnosis of septic arthritis in the acute setting is vital to prevent joint destruction, since cartilage loss occurs within hours of onset1,2. Inpatient mortality due to septic arthritis has been reported as between 7-15%, despite improvement in antibiotic therapy3,4. Crystal arthritis (Gout/Pseudogout) is the second most common differential diagnosis. It is often under-diagnosed and subsequently patients do not receive rheumatology referral for appropriate treatment and follow-up. In addition, some patients are misdiagnosed and treated as septic arthritis with inappropriate antibiotics. Untreated crystal-induced arthropathy has been shown to cause degenerative joint disease and disability leading to a considerable health economic burden.6,7
When the patient is systemically unwell, it is common practice to start empirical antibiotic treatment after joint aspiration for the fear of septic arthritis. This aims to minimize the risk of joint destruction while awaiting gram stain microscopy and microbiological culture results. In a persistent painful swollen knee with negative gram stain and culture, antibiotic therapy can be continued with or without arthroscopic knee washout based on clinical suspicion of infection 8.
We have therefore undertaken a retrospective study to review our management of patients with non-traumatic hot swollen knees and in particular patients with crystal-induced arthritis.
Materials and methods:
We performed a retrospective review of 180 patients presenting consecutively with acute non-traumatic knee effusion referred to the on-call Orthopaedic team in the hospital of study between November 2008 and November 2011. Sixty patients were included in the study (Table 2). There were 43 males and 17 females, with a mean age of 36 years (range, 23- 93 years).
Patient demographics, clinical presentation, co-morbidities, current medications and body temperature were recorded. The results of blood inflammatory markers (WBC, CRP), blood cultures, synovial fluid microscopy, culture and polarized microscopy were also collected. Subsequent treatment (e.g. antibiotics, surgical intervention), complications, and mortality rates were reviewed.
Results:
On presentation, a decreased range of movement was evident in all patients. Associated knee pain was reported by 55 patients (92%), and 24 patients (40%) had fever (temperature ≥ 37.5º). All joints were aspirated prior to starting antibiotics and samples were sent for gram stain microscopy, culture and antibiotic sensitivity, and polarized light microscopy.
Of the 60-patient cohort, 26 were admitted and started on intravenous antibiotics based on clinical suspicion of infection (Table 3). The median duration of inpatient admission was 4 days (range, 2 to 14 days). The median duration of antibiotic therapy was 6 days (range, 2 to 25 days). Eighteen patients were treated non-operatively by means of antibiotics and anti-inflammatory medications. Arthroscopic washout was performed in the remaining eight knees. In this group of patients, leucocyte count in the joint aspirate ranged from 0-3 leucocyte/mm3, blood leucocyte count ranged from 4-20 leucocyte/mm3, while mean CRP was 37.8 mg/l (range, 1-275 mg/l).
Review of laboratory results revealed that four patients had positive microscopic growth on gram stained films. Two samples showed staphylococcus aureus growth and two grew beta haemolytic streptococci. Eight patientshad crystals identified on polarized light microscopy of joint aspirate. Three showed monosodium urate (MSU) crystals while five had calcium pyrophosphate (CPP) crystals. They received antibiotic therapy for a mean duration of 10 days (range, 1-30 days). Two patients were taken to theatre for arthroscopic lavage. Only two patients received rheumatology referral.
Seven patients developed complications during their hospital stay. Four contracted diarrhoea; three of which had negative stool cultures but one was positive for clostridium difficile, developed toxic megacolon and died. One patient with known ischemic heart disease had a myocardial infarction and died. Two further patients acquiredurinary tract infections.
Discussion:
Acute monoarthritisof the knee joint can be a manifestation of infection, crystal deposits, osteoarthritis and a variety of systemic diseases. Arriving at a correct diagnosis is crucial for appropriate treatment 9. Septic arthritis, the most common etiology, develops as a result of haematogenous seeding, direct introduction, or extension from a contiguous focus of infection. Joint infectionis a medical emergency that can lead to significant morbidity and mortality. Mainstay of treatment comprises appropriate antimicrobial therapy and joint drainage 10,11. Literature reveals the knee is the most commonly affected joint (55%) followed by shoulder (14%) in the septic joint population12-13.
The second most common differential diagnosis is crystal-induced monoarthritis. Gout and pseudogout are the two most common pathologies 14. They are debilitating illnesses in which recurrent episodes of pain and joint inflammation are caused by the formation of crystals within the joint space and deposition of crystals in soft tissue. Gout is caused by monosodium urate (MSU) crystals, while pseudogout is inflammation caused by calcium pyrophosphate (CPP) crystals, sometimes referred to as calcium pyrophosphate disease (CPPD) 15,16. Misdiagnosis of crystals arthritis or delay in treatment can gradually lead to degenerative joint disease and disability in addition to renal damage and failure 5. The clinical picture of acute crystal-induced arthritis can sometimes be difficult to differentiate from acute septic arthritis. It is manifested by fever, malaise, raised peripheral WBC, CRP and other acute phase reactants. Synovial fluid aspirate can be turbid secondary to an increase in peripheral polymorphonuclear cells. Diagnosis can be challenging and therefore crystal identification on polarized microscopy is considered the gold standard 17, 18, 19. Rest, ice and topical analgesia may be helpful but systemic non-steroidal anti-inflammatory medications are the treatment of choice for acute attacks provided there are no contraindications 20.
In this study, all joints were aspirated and samples were sent for microscopy, culture and sensitivity, and polarized microscopy for crystals in-line with the British Society of Rheumatology and British Orthopaedic Association guidelines 8. Aspiration not only helps diagnosis but in addition reduces the pain caused by joint swelling. Twenty six patients were admitted, on clinical and biochemical suspicion of septic arthritis. They presented with acute phase response manifested by malaise, fever and raised inflammatory markers and were treated with antibiotic therapy and non steroidal anti-inflammatory medications while awaiting the results of microbiology and polarized light microscopy. Four of theses patients developed complications secondary to antibiotic therapy including death due to clostridium difficile infection and subsequent toxic megacolon.
Infection was confirmed to be underlying cause in four patients (6%) who showed positive microscopic growth on gram stained films. They underwent arthroscopic washout and continued antibiotic therapy according to the result of culture and sensitivity of their knee aspirate till their symptoms and blood markers were normal. Arthroscopic washout was required for four patients with negative microscopic growth due to persistant symptoms despite antibiotic treatment, as recommended by the British Society of Rheumatology and the British Orthopaedic Association 8. Two patients showed calcium pyrophosphate crystals on polarized microscopy and two had no bacterial growth or crystals.
We retrospectively reviewed laboratory results and found that eight patients (13%) were confirmed to have crystal arthritis as crystals (MSU/CPP) were identified in their knee aspirates by means of polarized microscopy. However, only two patients (25%) received this diagnosis whilst in hospital. In both cases, antibiotic therapy was discontinued and they were referred to a rheumatologist for appropriate treatment and follow up. The remaining six patients continued to receive antibiotics and two of them were taken to theatre for arthroscopic lavage on clinical suspicion of infection as symptoms did not improve significantly with medications.
Our study shows that crystal-induced arthritis can easily be overlooked or misdiagnosed as septic arthritis. This results in patients having unnecessary antibiotic therapy, developing serious complications and undergoing surgical procedures, all of which can be avoided. Moreover, they were not referred to a rheumatologist.
Acute knee effusion is a common presentation to the Orthopaedic department and although we seem to be providing a good service for septic arthritis, patients with crystal arthropathy are still slipping through the net. Clinicians should always remember that crystal arthritis is almost as common as septic arthritis and will eventually lead to joint damage if not managed appropriately. It must be excluded as a cause of hot swollen joints by routine analysis of joint aspirate using polarized light microscopy. If crystal arthritis is proved to be the underlying pathology, patients must be treated accordingly and receive a prompt rheumatology referral for further management.
Saliva is the watery and usually frothy substance produced in and secreted from the three paired major salivary (parotid, submandibular and sublingual) glands and several hundred minor salivary glands, composed mostly of water, but also includes electrolytes, mucus, antibacterial compounds, and various enzymes. Healthy persons are estimated to produce 0.75 to 1.5 liters of saliva per day. At least 90% of the daily salivary production comes from the major salivary glands while the minor salivary glands produce about 10%. On stimulation (olfactory, tactile or gustatory), salivary flow increases five fold, with the parotid glands providing the preponderance of saliva.1
Saliva is a major protector of the tissues and organs of the mouth. In its absence both the hard and soft tissues of the oral cavity may be severely damaged, with an increase in ulceration, infections, such as candidiasis, and dental decay. Saliva is composed of serous part (alpha amylase) and a mucus component, which acts as a lubricant. It is saturated with calcium and phosphate and is necessary for maintaining healthy teeth. The bicarbonate content of saliva enables it to buffer and produce the condition necessary for the digestion of plaque which holds acids in contact with the teeth. Moreover, saliva helps with bolus formation and lubricates the throat for the easy passage of food. The organic and inorganic components of salivary secretion have got a protective potential. They act as barrier to irritants and a means of removing cellular and bacterial debris. Saliva contains various components involved in defence against bacterial and viral invasion, including mucins, lipids, secretory immunoglobulins, lysozymes, lactoferrin, salivary peroxidise, and myeloperoxidase. Salivary pH is about 6-7, favouring digestive action of salivary enzyme, alpha amylase, devoted to starch digestion.
Salivary glands are innervated by the parasympathetic and sympathetic nervous system. Parasympathetic postganglionic cholinergic nerve fibers supply cells of both the secretory end-piece and ducts and stimulate the rate of salivary secretion, inducing the formation of large amounts of a low-protein, serous saliva. Sympathetic stimulation promotes saliva flow through muscle contractions at salivary ducts. In this regard both parasympathetic and sympathetic stimuli result in an increase in salivary gland secretions. The sympathetic nervous system also affects salivary gland secretions indirectly by innervating the blood vessels that supply the glands.
Table 1: Functions of saliva
Digestion and swallowing Initial process of food digestion Lubrication of mouth, teeth, tongue and food boluses Tasting food Amylase- digestion of starch Disinfectant and protective role Effective cleaning agent Oral homeostasis Protect teeth decay, dental health and oral odour Bacteriostatic and bacteriocidal properties Regulate oral pH Speaking Lubricates tongue and oral cavity
Drooling (also known as driveling, ptyalism, sialorrhea, or slobbering) is when saliva flows outside the mouth, defined as “saliva beyond the margin of the lip”. This condition is normal in infants but usually stops by 15 to 18 months of age. Sialorrhea after four years of age generally is considered to be pathologic. The prevalence of drooling of saliva in the chronic neurological patients is high, with impairment of social integration and difficulties to perform oral motor activities during eating and speech, with repercussion in quality of lifeDrooling occurs in about one in two patients affected with motor neuron disease and one in five needs continuous saliva elimination7, its prevalence is about 70% in Parkinson disease8, and between 10 to 80% in patients with cerebral palsy9.
Pathophysiology
Pathophysiology of drooling is multifactorial. It is generally caused by conditions resulting in
Excess production of saliva- due to local or systemic causes (table 2)
Inability to retain saliva within the mouth- poor head control, constant open mouth, poor lip control, disorganized tongue mobility, decreased tactile sensation, macroglossia, dental malocclusion, nasal obstruction.
Problems with swallowing- resulting in excess pooling of saliva in the anterior portion of the oral cavity e.g. lack of awareness of the build-up of saliva in the mouth, infrequent swallowing, and inefficient swallowing.
Drooling is mainly due to neurological disturbance and less frequently to hyper salivation.Under normal circumstances, persons are able to compensate for increased salivation by swallowing. However, sensory dysfunction may decrease a person’s ability to recognize drooling and anatomic or motor dysfunction of swallowing may impede the ability to manage increased secretion.
Depending on duration of drooling, it can be classified as acute e.g. during infections (epiglottitis, peritonsilar abscess) or chronicneurological causes.
Symptoms
Drooling of saliva can affect patient and/or their carers quality of life and it is important to assess the rate and severity of symptoms and its impact on their life.
Table 3 Effect of untreated Drooling of saliva
Physical
Psychological
Perioral chapping (skin cracking) Maceration with secondary infection Dehydration Foul odour Aspiration/ pneumonia Speech disturbance Interference with feeding
Isolation Barriers to education (damage to books or electronic devices) Increased dependency and level/intensity of care Damage to electronic devices Decreased self esteem Difficult social interaction
Assessment
Assessment of the severity of drooling and its impact on quality of life for the patient and their carers help to establish a prognosis and to decide the therapeutic regimen. A variety of subjective and objective methods for assessment of sialorrhoea have been described3.
History (from patient and carers)
Establish possible cause, severity, complications and possibility of improvement, age and mental status of patient, chronicity of problems, associated neurological conditions, timing, provoking factors, estimation of quantity of saliva – use of bibs, clothing changing required/ day and impact on the day today life (patient/carer)
Physical examination
Evaluate level of alertness, emotional state, hydration status, hunger, head posture
Examination of oral cavity- sores on the lip or chin, dental problems, tongue control, swallowing ability, nasal airway obstruction, decreased intraoral sensitivity, assessment of health status of teeth, gum, oral mucosa, tonsils, anatomical closure of oral cavity, tongue size and movement, jaw stability. Assessment of swallowing
Assess severity and frequency of drooling (as per table 4)
Investigation
Lateral neck x ray (in peritonsilar abscess)
Ultrasound to diagnose local abscess
Barium swallow to diagnose swallowing difficulties
Audiogram- to rule out conductive deafness associated with oropharyngeal conditions
Salivary gland scan- to determine functional status
Table 4 : System for assessment of frequency and severity of drooling
Drooling severity
Points
Dry (never drools)
1
Mild (wet lips only)
2
Moderate (wet lips and chins)
3
Severe (clothing becomes damp)
4
Profuse (clothing, hands, tray, object become wet)
5
Frequency
Points
Never drools
1
Occasionally drools
2
Frequency drools
3
Constantly drools
4
Other methods of assessing salivary production and drooling
1) 1- 10 visual analogue scale (where 1 is best possible and 10 is worst possible situation)
2) Counting number of standard sized paper handkerchiefs used during the day
3) Measure saliva collected in cups strapped to chin
4) Inserting pieces of gauze with a known weight into oral cavity for a specific period of time and then re-measuring weight and calculating the difference between the dry and wet weights.
6) Salivary duct canulation 12 and measuring saliva production.
Management
Drooling of saliva, a challenging condition, is better managed with a multidisciplinary team approach. The team includes primary care physician, speech therapist, occupational therapist, dentist, orthodontist, otolaryngologist, paediatrician and neurologist. After initial assessment, a management plan can be made with the patient. The person/ carer should understand the goal of treating drooling is a reduction in excessive salivary flow, while maintaining a moist and healthy oral cavity. Avoidance of xerostomia (dry mouth) is important.
There are two main approaches
Non invasive modalities e.g. oral motor therapy, pharmacological therapy
Invasive modalities e.g. surgery and radiotherapy
No single approach is totally effective and treatment is usually a combination of these techniques. The first step in management of drooling is correction of reversible causes. Less invasive and reversible methods, namely oral motor therapy and medication are usually implemented before surgery is undertaken5
Non invasive modalities
Positioningprior to implementation of any therapy, it is essential to look at the position of the patient. When seated, a person should be fully supported and comfortable. Good posture with proper trunk and head control provides the basis for improving oral control of drooling and swallowing.
Eating and drinking skills-drooling can be exacerbated by pooreating skills. Special attention and developing better techniques in lip closure, tongue movement and swallowing may lead to improvements of some extent. Acidic fruits and alcohol stimulate further saliva production, so avoiding them will help to control drooling10
Oral facial facilitation - this technique will help to improve oral motor control, sensory awareness and frequency of swallowing.Scott and staios et al 18 noted improvement in drooling in patients with both hyper and hypo tonic muscles using this technique. This includes different techniques normally undertaken by speech therapist, which improves muscle tone and saliva control. Most studies show short term benefit with little benefit in long run. This technique can be practiced easily, with no side effects and can be ceased if no benefits noted.
a) Icing – effect usually last up to 5-30 minutes. Improves tone, swallow reflex.
b) Brushing- as effect can be seen up to 20- 30 minutes, suggested to undertake before meals.
c) Vibration- improves tone in high tone muscles
d) Manipulation – like tapping, stroking, patting, firm pressure directly to muscles using fingertips known to improve oral awareness.
e) Oral motor sensory exercise - includes lip and tongue exercises.
Speech therapy-speech therapy should be started early to obtain good results. The goal is to improve jaw stability and closure, to increase tongue mobility, strength and positioning, to improve lip closure (especially during swallowing) and to decrease nasal regurgitation during swallowing.
Behaviour therapy-this uses a combination of cueing, overcorrection, and positive and negative reinforcement to help drooling. Suggested behaviours, like swallowing and mouth wiping are encouraged, whereas open mouth and thumb sucking are discouraged. Behavior modification is useful to achieve (1) increased awareness of the mouth and its functions, (2) increased frequency of swallowing, (3) increased swallowing skills. This can be done by family members and friends. Although there is no randomized controlled trial done, over 17 articles published in last 25 years, show promising results and improved quality of life. No reported side effects make behavioural interventions an initial option compared to surgery, botulinum toxin or pharmaceutical management. Behaviour interventions are useful prior and after medical management such as botulinum toxin or surgery.
Oral prosthetic device- variety of prosthetic devices can be beneficial, e.g. chin cup and dental appliances, to achieve mandibular stability, better lip closure, tongue position and swallowing. Cooperation and comfort of the patient is essential for better results.
Pharmacological methods
Systematic review of anticholinergic drugs, show Benztropine, Glycopyrrolate, and Benzhexol Hydrochloride, as being effective in the treatment of drooling. But these drugs have adverse side-effects and none of the drugs been identified as superior.
Hyoscine- The effect of oral anticholinergic drugs has been limited in the treatment of drooling. Transdermal scopolamine (1.5 mg/2.5 cm2) offers advantages. One single application is considered to render a stable serum concentration for 3 days. Transdermal scopolamine has been shown to be very useful in the management of drooling, particularly in patients with neurological or neuropsychiatric disturbances or severe developmental disordersIt releases scopolamine through the skin into the bloodstream.
Glycopyrrolatestudies have shown 70-90% response rates but with a high side effect rate. Approximately 30-35% of patients choose to discontinue due to unacceptable side effects such as excessive dry mouth, urinary retention, decreased sweating, skin flushing, irritability and behavior changes. A study on 38 patients with drooling due to neurological deficits had shown up to a 90% response rateMier et al21 reported Glycopyrrolate to be effective in the control of excessive sialorrhea in children with developmental disabilities. Approximately 20% of children given glycopyrrolate may experience substantial adverse effects, enough to require discontinuation of medication.
Antimuscarinic drugs, such as benzhexol, have also been used, but limited due to their troublesome side effects.
Antireflux Medication: The role of antireflux medication (Ranitidine & Cisapride) in patients with gastro esophageal reflux due to esophageal dysmotility and lower esophageal tone did not show any benefits in a study 21.
Modafinil - One case study noticed decreased drooling in two clients who were using the drug for other reasons, but no further studies have been done.
Alternate medications: (Papaya and Grape seed extract) – Mentioned in literature as being used to dry secretions but no research in to their efficacy has been conducted.
Botulinum toxin It was in 1822 that a German poet and physician, Justinus Kerner, discovered that patients who suffered from botulism complained of severe dryness of mouth which suggested that the toxin causing botulism could be used to treat hypersalivation. However, it was only in the past few years that botulinum toxin type A (BTx-A)has been used for this purpose. BTx-A binds selectively to cholinergic nerve terminals and rapidly attaches to acceptor molecules at the presynaptic nerve surface. This inhibits release of acetylcholine from vesicles, resulting in reduced function of parasympathetic controlled exocrine glands. The blockade though reversible is temporary as new nerve terminals sprout to create new neural connections. Studies have shown that injection of botulinum toxin to parotid and submandibular glands, successfully subsided the symptoms of drooling 30,31. Although there is wide variation in recommended dosage, most studies suggest that about 30- 40 units of BTx-A injected into the parotid and submandibular glands are enough for the symptoms to subside The injection is usually given under ultrasound guidance to avoid damage to underlying vasculature/ nerves. The main side effects from this form of treatment are dysphagia, due to diffusion into nearby bulbar muscles, weak mastication, parotid gland infection, damage to the facial nerve/artery and dental caries.
Patients with neurological disorders who received BTX-A injections showed a statistically significant effect from BTX-A at 1 month post injection, compared with control, this significance was maintained at 6 months. Intrasalivary gland BTX-A was shown to have a greater effect than scopolamine.
The effects of BTx-A are time limited and this varies between individuals.
Invasive modalities
Surgerycan be performed to remove salivary glands, (most surgical procedures focused on parotid and submandibular glands). ligate or reroute salivary gland ducts, or interrupt parasympathetic nerve supply to glands. Wilke, a Canadian plastic surgeon, was the first to propose and carry out parotid duct relocation to the tonsillar fossae to manage drooling in patients with cerebral palsy. One of the best studied procedures, with a large number of patients and long term follow up data, is submandibular duct relocation 32, 33.
Intraductal laser photocoagulation of the bilateral parotid ducts has been developed as a less invasive means of surgical therapy. Early reports have shown some impressive results34.
Overall surgery reducedsalivary flow and drooling can be significantly improved often with immediate results – 3 studies noted that 80 – 89% of participants had an improvement in their control of their saliva. Two studies discussed changes in quality of life. One of these found that 80% of those who participated improved across a number of different measures including receiving affection from others and opportunities for communication and interaction. Most evidence regarding surgical outcomesof sialorrhea management is low quality and heterogeneous. Despitethis, most patients experience a subjective improvement followingsurgical treatment 36.
Radiotherapy - to major salivary glands in doses of 6000 rad or more is effective Side effects which include xerostomia, mucositis, dental caries, osteoradionecrosis, may limit its use.
Key messages
Chronic drooling can pose difficulty in management
Early involvement of Multidisciplinary team is the key.
Combination of approach works better
Always start with noninvasive, reversible, least destructive approach
Surgical and destructive methods should be reserved as the last resort.
Chronic pain, arbitrarily defined as that lasting longer than six months, is a clinical, social, and economic problem. It is often accompanied by feelings of low mood and despondency.
Whether chronic pain induces clinical depression or depression initiates psychosomatic pain (through physiological mechanisms) is difficult to prove. The burden of illness increases when patients suffer from both. Financial hardship and medical costs affect the quality of life which leads to difficulties in coping and further decreased functioning, making the treatment of both conditions more complicated. Therefore, better recognition, assessment, and treatment of comorbid pain and depression should, at least in theory, lead to better outcomes.
Pain is broadly categorized into three groups: nociceptive (any painful stimulus), neuropathic (for example, diabetes), and psychogenic. Nociceptive pain occurs with direct noxious stimuli. Neuropathic pain is a result of disease or injury to the nervous system or spinal cord. Psychogenic pain has no discernible physical origin. Although the precise physiological mechanisms are not entirely understood, there are two basic categories of sensory neurones. The first type is myelinated and fast conducting; the second is unmyelinated and slow conducting.
Acute pain which follows damage to tissue (an ankle sprain, for example) is usually correlated with hyperalgesia (an increase in the pain elicited by a noxious stimulus and felt as a sharp, burning sensation) and allodynia (‘other’ pain evoked by a normally innocuous stimulus) and serves to protect the injury from further trauma while allowing the damage to be repaired.
Depression is often a chronic disorder and though its symptoms may be alleviated by appropriate medication and other therapies, physical complaints tend to be more intractable. For example, fibromyalgia (FM), a syndrome characterized by widespread muscle pain and generalized tender points, is often associated with major depressive disorder.1 However, although the vast majority of patients with fibromyalgia do not meet criteria for a psychiatric disorder, psychological symptoms are common. In a randomized controlled trial of primary care patients with musculoskeletal problems and depression, antidepressant medication followed by a self-management pain programme led to improvement in both.2 The tricyclic antidepressant amitriptyline was traditionally used usually in small doses, to treat pain, with moderate success. In addition to its own intrinsic analgesic effect amitriptyline appears to enhance the effects of opioid analgesia. Other antidepressants are now in vogue; for example, duloxetine, a serotonin (5-HT)/noradrenaline (NA) reuptake inhibitor, is sometimes used for diabetic neuropathic pain.
Of the numerous neurotransmitters at least two, namely 5-HT and NA, may prove to be one common link between depression and pain. Both serotoninergic and noradrenergic pathways ascend from subcortical areas (brainstem, hypothalamus and thalamus) to the whole neocortex and mediate emotional and physiological responses.3 Their pathways descend the spinal cord and suppress nociceptive inputs. Serotoninergic cell bodies located in the raphe nucleus in the brainstem, and noradrenergic neurones located in the locus coeruleus (also in the brainstem) send projections to various parts of the brain involved in the control of mood, appetite, sexual activity, attention and concentration. Theoretically at least, a dysfunction at the level of the serotoninergic and noradrenergic neurons could affect both ascending and descending pathways resulting in the psychological and physically painful symptoms of depression. Neurotransmitters may open or close the ‘gate’ on perception of painful stimuli. Therefore adrenergic and serotoninergic pathways from the brainstem to the spinal cord will inhibit incoming painful stimuli. This is perhaps an oversimplification as some sensory fibres enter via the ventral spinal roots.
The hypothalamic pituitary axis (HPA) is probably also involved. The hypothalamus, which synthesises and secretes neurohormones, has a wide range of physiological functions including regulation of thirst and hunger, sexual behaviour, defence reactions such as fear and rage, and circadian rhythm: disturbances of all these functions are frequently seen in depressed or anxious patients. The HPA is also affected in patients with physical stress as well as major depression, as shown by increased levels of adrenocorticotropic hormone and cortisol in the plasma. Stimulation of the lateral areas of the hypothalamus produces a diffuse sympathetic discharge possibly because some areas of the hypothalamus control adrenaline and NA secretion. Prolonged stress associated with pain leads to depletion of central 5-HT and malfunction of other associated receptors.4
The hypothalamus and limbic system (whose boundaries are difficult to define) with its associated structures – the amygdala, hippocampus and septal nuclei, are involved in the mental and affective aspects of emotions. The amygdala, a cluster of nuclei in the medial temporal lobe, may have a role in the reciprocal relationship between pain and depression. The amygdala controls not only emotional behaviour but also memory. However, mixed results have been reported regarding the level of activity of the amygdala in response to pain.
Nociceptor afferents terminate within distinct regions of the dorsal horn and within the spinal cord, synapses are sites of considerable modification, hence the term ‘gate’ for the dorsal horn cells. The neurotransmitter for slow pain is believed to be substance P, and glutamate is the putative transmitter secreted by primary afferent fibres subserving fast pain.5
5-HT and NA neurotransmitter systems influence neuroplasticity in the brain. Most currently available antidepressants act through reuptake inhibition of either or both. Therefore, it would seem feasible to prescribe dual-action antidepressants when pain symptoms are associated with depression. However depressed patients with pain comorbidity are less likely to take antidepressant medications compared to those with depression alone. Also, individuals who develop pain or depression are at risk for developing the other, thus escalating the clinical management. Furthermore, when pain is refractory to treatment, it is associated with more depressive symptoms and worse depression outcomes, and vice versa. Depressive symptoms are very common in physically ill patients. Unfortunately, depression is often overlooked in pain patients because pain symptoms take priority or worse still, comorbid depression is not considered.
It is difficult to state with certainty whether or not unexplained pain is ‘psychological’. Such an assumption might be perceived as demeaning and patronizing to patients and the suggestion of providing cognitive therapy misinterpreted as him/her overplaying their reaction to pain or that the pain is ‘psychological’. Others do not like being labelled ‘psychiatric’, and are therefore reluctant to take antidepressants even when a physiological explanation is given. Pain perception involves physical and emotional factors and its primary function is to protect the organism from harm. It follows therefore, that pain thresholds and pain tolerance vary from individual to individual, and especially among patients with depression.
Antidepressants are frequently used in the treatment of depression and generalized anxiety disorders. Their use extends beyond these areas, however, and it is now accepted that antidepressants are efficacious in treating chronic pain syndromes in addition to their effects on psychological features such as low mood, inordinate guilt, or feelings of worthlessness. Because physical symptoms are often the main complaint in many depressed patients and pain is common as a presenting symptom, clinicians need to know about the dual use of antidepressants for both. Future antidepressants may involve neurotransmitters, other than 5-HT and NA, which could include dopaminergic pathways, opioid (antagonists of morphine-type drugs) receptors and the pentapeptides (enkephalins) which bind to these receptors.
Controlled teaching environment can be provided to undergraduate medical students for learning certain basic clinical skills through using manikins or models before they have to perform them on real patients. Many medical schools in the United Kingdom now have clinical skills laboratories which are equipped with a large host of such learning resources. Many medical schools promote their clinical laboratories and have dedicated lead consultants to teach, monitor and develop clinical skills. Furthermore, a wide variety of skills can be taught in these laboratories. For example, the University of Leeds Medical school offers teaching to second year undergraduate medical students in basic life support, vital signs, injections, blood glucose monitoring, cannulation and venepuncture while third year medical students are taught fundoscopy, rectal examination, urinary bladder catheterisation, doing an ECG and examination of the breast. Similarly, simulators have also been used in postgraduate medical teaching, for example, Colonoscopy simulators have been used to calculate efficiency ratio of learners. 1
However not all places in the world have clinical skills laboratories. Alternatively, some institutions teach the undergraduate medical students various basic skills in clinical supervised settings before they take up their first job as physicians. Some have assessed the level of training that their institutions have thus offered and tried to improve upon deficits. Mario Sicaja et al 2 from Zagreb University evaluated 252 students using a questionnaire asking the students to self assess their abilities on nine groups of skills and asked 129 faculty teachers to simultaneously assess the minimum necessary level of skills they expected from the graduating students. They concluded that the teachers expected higher level of clinical skills from students than that assessed by the students. Similarly, in postgraduate teaching, the students’ learning needs have been assessed by determining the difference in expectation of trainers and the trainees. 3
Effectiveness of basic clinical skills training programmes has been documented and it has been suggested that longitudinal skills training offers superior preparation for abilities during the clerkship 4. It has also been suggested that whereas students from medical schools using traditional curriculum may not differ in their knowledge based performance, (demonstrated by Multiple Clinical Questions i.e. MCQ scores) from students at medical schools with clinical skills training, the later perform better on clinical examination (measured by Objective Structured Clinical Examination i.e. OSCE). 5
However, in many other medical schools worldwide, which implement the traditional undergraduate medical curriculum, there are no clinical skills teaching sessions for undergraduate medical students. The students get to learn this first time when they are doing internship and are in direct contact with the patients. It was the same situation in Liaquat University of Medical and Health Sciences (LUMHS) in Hyderabad, Pakistan. This is a large medical school which is based in the second largest city of Sindh province of Pakistan. The first author was invited from United Kingdom to review and advise on the undergraduate medical curriculum at LUMHS. The professor of plastic surgery (second author) had started to run a voluntary clinical skills course in his department covering some general basic clinical skills and provided his data to the first author for analysis and review.
This study was devised to analyse the views of participating students regarding the course and determine their learning needs. Based on the learning needs, one could identify which resources are needed and what the University should aim to provide. Furthermore, there are no such published studies from Pakistan. This study was aimed at providing scientific information on the learning needs of undergraduate medical students from the developing world, which may be deemed to be different from the medical students in the western world.
Methods:
All medical students from fourth and final year at LUMHS were invited to attend four weeks of clinical skills course at the plastic surgery department voluntarily. The students had to attend the department after their normal working hours. There were dedicated junior doctors in the department who were given the responsibility to teach the attendees hands on clinical skills in a structured manner. The skills included history taking, organising blood tests, vene-puncture, giving intravenous and intra-muscular injections, intravenous cannulation, urinary bladder catheterisation, passing naso-gastric tube, dressing of surgical wounds, basic pre-operative assessment, basic post-operative assessment including haemo-dynamic stability, surgical theatre mannerism, principles of sterilization, identification of common surgical instruments and equipment and identification of types of drugs used in anaesthesia. The students were provided a questionnaire asking for feedback on the course which they had to fill at the end. The study was approved by the University Research and Ethics Committee. The data was computerised and statistically analysed using a statistical package. It involved all students who went through the course during consecutive sixteen months commencing from October 2008 and ending in January 2010.
Results:
90 students were recruited to the study. Students were from both sexes and both fourth year and final year. There were 32 male (35.6%) and 58 female (64.4%) students. Of the total 90 students, 62 (68.9%) were from 4th year while 28 (31.1%) students were from final year. They were all volunteers who were willing to attend the course after their normal working hours and were allocated seats on a first come first serve basis. No student was refused entry to the course and all participants were provided questionnaire on feedback at the time of completion of the course. The response rate was 100% although this may be because students were actively encouraged by the teaching staff to ensure that feedback questionnaires were filled in.
History taking and laboratory investigations were deemed least important by students, perhaps because these are taught to them during normal attachments in all wards for clinical teaching.
The Friedman mean rank was highest for catheterisation of urinary bladder (11.66) and passing of a naso-gastric tube (12.44). The students felt the greatest need to learn these two basic clinical skills perhaps because they are not taught elsewhere. This was followed by anaesthesia, sterilisation and passing an intravenous cannulation. The students ranked learning of the learning of the following skills in the middle: giving injections, taking blood, providing pre or post-operative care and being able to identify surgical instruments. Taking history and arranging laboratory investigations were both ranked the lowest at 6.22. The Friedman asymptotic significance was high (p<0.000). Despite being a good sample size, Monte Carlo significance at confidence interval of 99% was very high (p<000.0). Table below summarises the statistics
Ranks
Mean Rank
History taking
6.22
Lab investigations
6.22
Venesection
6.29
Giving injection
6.68
I/v cannulation
7.46
Catheterisation
11.66
Naso-gastric intubation
12.24
Dressing wound
6.29
Pre-operative assessment
6.71
Theatre environment
6.53
Post-operative assessment
6.62
Principles of sterilisation
7.73
Types of anaesthesia
7.81
Surgical instruments
6.54
Test Statistics a
N
90
Chi-Square
615.431
Df
13
Asymp. Sig.
0.000
Monte Carlo Sig.
0.000
99% Confidence Interval Lower Bound
0.000
99% Confidence Interval Upper Bound
0.000
a : Friedman Test
Discussion:
Our study has shown that undergraduate medical students from the developing world greatly value a basic clinical skills course, and are particularly keen on being taught naso-gastric intubation and urinary bladder catheterisation. They seem to get enough exposure in the wards on history taking and arranging laboratory tests, but identify learning needs in other clinical skills.
This study is limited to data collection from one large medical university, but the sample size has been large, observation has been over a period of one year, statistical significance has been very high and response rate has been extremely good. The teaching staff actively encouraged the students to fill the feedback questionnaires, and this could arguably lead to some response bias.
There are no such previous studies from Pakistan to compare our findings with. This study therefore can make a good baseline for local institutions to further develop and build upon. Roy Remmen’s group compared four medical schools on clinical skills of students, and demonstrated positive effect of both longitudinal skill training as well as utilisation of problem based approach in these skill courses. Our study did not provide any longitudinal data and problem based learning approach was not utilised either. Our data is a cross sectional study.
There seem to be three levels of engagement in learning basic clinical skills. One side of the spectrum has structured teaching in clinical skills laboratories with simulation, models and manikins, while the other has no teaching of clinical skills at all, until the physician starts to work with real patients. In the middle is the model of teaching clinical skills on the wards, before graduating as doctors. The former model with clinical skills laboratories requires the most resource. Which model of teaching is adopted by any individual medical university may be dependant upon the local resources, as well as the demands of the local regulatory bodies. During this study, we were able to realise the pattern of clinical skills teaching at some other medical universities in Pakistan, India and Bangladesh as random examples of southeast Asia. We learned that most institutions in this part of the world do not undertake any formal clinical skills teaching, and certainly there are hardly any clinical skills laboratories. This voluntary attempt by the professor of plastic surgery at LUMHS is therefore commendable.
This study has also identified the keenness of students to learn some specific skills through such courses prior to graduation. With a move to more globalisation of medical protocols and guidelines, a greater uniformity should also emerge in the ways in which doctors in the east or the west hemisphere of the world learn medical knowledge, attitudes and skills. There may thus be need for researchers in medical education to encourage and push for adoption of clinical skills teaching courses prior to medical graduation in the developing world.
Furthermore this study has yet again reiterated that student’s views should form a key part in the curriculum design when considering development of a clinical skills course, and resources should be geared to meet these learning needs of students.
Examination of the ovaries at caesarean section is a normal practice as ovarian pathology may be found. The incidence of an adnexal mass found at caesarean section ranges from 1 in 123 1 to 329 2. Ovarian cysts rarely develop de novo in late pregnancy, but rather persist from early pregnancy. About 4 in 5 ovarian cysts detected in the first trimester scan resolve spontaneously. Also, 4 in 5 of ovarian cysts persisting into the second trimester will also be present in the post-natal period as complex cysts such as serous cystadenomas, mature cystic teratomas, endometriomas and mucinous cystadenomas 3. It therefore seems sensible to remove the ovarian cyst for histology at caesarean section rather than subject the woman to the anxiety of multiple investigations and/or another laparotomy, particularly when ovarian cystectomy during caesarean section does not appear to increase morbidity of the procedure 1.
We present a case of incidental ovarian cyst found at elective caesarean section to illustrate the value of a comprehensive consenting process.
Case Report
A 35 year-old para 1 + 0 healthy Polish woman was admitted for elective lower segment caesarean section (LSCS) at 39 + 4 weeks gestation in view of a previous caesarean section 2 years ago for failure to progress in the first stage of labour.She was booked in a neighbouring hospital for her antenatal care where she was counselled and consented for the procedure by her consultant. Her pregnancy was uncomplicated and routine pregnancy scans were unremarkable. Apart from drainage of a breast abscess 2 years ago, she had no medical history of note.
Written consent for elective LSCS was obtained by the junior doctor on duty before the consultant pre-operative ward round. However, the directorate’s standardised consent (figure 1) form was not used. The woman was therefore again counselled and written consent for elective LSCS obtained for the third time now including previously omitted additional procedures that might be performed during the course of the surgery.
At the uncomplicated LSCS under spinal anaesthetic, routine inspection of the uterus and adnexa revealed a 30 x 20 x 15 mm pedunculated firm pale mass attached to the left ovary suggestive of a fibroma. The findings were relayed to the woman, and confirmation of consent for the ovarian cystectomy was obtained. The abnormal ovarian mass was removed with conservation of the left ovary. Histology of the mass subsequently confirmed it to be an ovarian fibroma / fibrothecoma.
Discussion
The Royal College of Obstetricians and Gynaecologists (RCOG) recommend that clinicians should seek prior consent to treat any problem which might arise 4. Indeed, in its Consent Advice for caesarean section, it states that discussion of appropriate but not essential procedures, such as ovarian cystectomy at caesarean section, should take place before undertaking the procedure 5. This supports the position of the Department of Health which states that a procedure should not be performed merely because it is convenient, and that it is good practice where possible to seek the person’s consent to the proposed procedure well in advance, when there is time to respond to the person’s questions and provide adequate information 6.
In spite of the publication of the above guidelines well over a year ago, our case supports the belief that most obstetricians omit discussion and/or documentation of ovarian cystectomy at LSCS, and indeed other risks or additional procedures that may be relevant as showed in figure 1. This may be because the clinician is unaware of the recommendations, not familiar with the potential risks or findings at surgery, or that there is simply insufficient time to document comprehensively.
Our directorate has adopted the use of standardised consent forms for common procedures. These forms are available on our intranet which can be edited allowing clinicians to amend the risks and additional procedures as appropriate in each individual case. We believe the verified printed consent form offers legible and comprehensive documentation of the counselling process, as well as prompting clinicians to discuss key issues such as those recommended by the RCOG Consent Advice. We advocate the use of such standardised consent forms in improving the care of patients and supporting clinicians to deliver optimal services.
Figure 1. Standardised consent form for lower segment caesarean section
A 73 year old lady presented for assessment of her recurrent right sided pleural effusion. She had a history of gallstones and underwent open cholecystectomy. One month after surgery the patient had recurrent pleural effusion requiring thoracocentesis on a monthly basis. On the chest x-ray, the pleural effusion was seen exclusively on the right side occupying the whole right hemithorax.
The pleural fluid was transudative on multiple occasions and there was no evidence of malignant cells. Her echocardiography revealed preserved cardiac function. An abdominal ultrasound showed findings of cirrhosis and splenomegaly consistent with portal hypertension.
Image 1
Computerised tomography (CT) of the chest and abdomen revealed a large right-sided pleural effusion and minimal ascites (Image 1). An ultrasound guided paracentesis was performed with difficulty and only 17cc of fluid.was obtained. The abdominal fluid showed similar consistency as the pleural fluid. The blood workup at the same time was unremarkable.
Image 2
Intra-peritoneal administration of 99mTc-sulphur colloid was attempted but failed in the absence of ascites. Computed tomography with three dimensional reconstruction at the diaphragmatic level revealed a defect in the posterior aspect of the right hemidiaphragm (Image 2 black arrow) and also revealed irregular contours of the liver, an indirect sign of diaphragmatic defect (Image 2 white arrow).
The patient declined any surgical intervention at that point including the option of pleurodesis. She was started on diuretics and a low salt diet with significant improvement.
Discussion:
Pleural effusion due to hepatic cirrhosis and ascites is well known, but hepatic hydrothorax in the absence of ascites is a rare complication. We report a case of liver cirrhosis with a large and recurring right sided pleural effusion that had an apparent abdominal source in the absence of ascites. We review the characteristics and treatment for hepatic hydrothorax in the absence of ascites.
Hepatic hydrothorax is defined as the presence of significant pleural effusion in a cirrhotic patient without primary pulmonary or cardiac disease1. Postulated mechanisms for the development of pleural effusions in patients with hepatic cirrhosis include: hypoalbuminemia and decreased oncotic pressure leakage of the plasma from the hypertensive azygos vein, lymphatic leak from the thoracic duct, passage of ascitic fluid to the pleural space by way of lymphatic channels in the diaphragm, and transfer of peritoneal fluid directly via diaphragmatic defects2.
The usual unilaterality of hepatic hydrothorax could be attributed to a congenital factor, but not to physiologic mechanisms3. The most likely explanation appears to be that ascitic fluid passes through congenital or acquired fenestrations in the diaphragm directly into the pleural space2. The description of hepatic hydrothorax in the absence of ascites is very rare1. The flow of the ascitic fluid into the pleural space equaled the rate of ascites production in patients with this entity3.
The composition of pleural fluid from hepatic hydrothorax is similar to that of ascitic fluid. Pleural effusions associated with portal hypertension are always transudative1. Nuclear scans can be performed to establish the diagnosis of hepatic hydrothorax with fairly high accuracy. Intra-peritoneal administration of 99mTc-human serum albumin or 99mTc-sulphur colloid can be used to demonstrate the communication between the peritoneal and pleural space. Recent advances in radiological imaging have enabled investigators to examine in detail the diaphragmatic defects responsible for the development of hepatic hydrothorax1.
The management is challenging and frequently associated with poor outcomes in most cases. Dietary restriction of sodium intake and the addition of diuretics is the initial approach. Thoracocentesis can be performed in patients with dyspnoea due to hepatic hydrothorax for immediate relief of symptoms. When thoracocentesis is required too frequently in patients on maximal sodium restriction and optimal diuretics, alternative treatment options must be considered1, 3.
Over the last few years, new insights into the pathogenesis of this entity have lead to improved treatment modalities such as portosystemic shunts (TIPS) and video-assisted thoracoscopy (VATS) for closure of diaphragmatic defects. Both, though temporary measures, are perhaps the best available bridging to liver transplantation in selected patients with refractory hepatic hydrothorax2, 3.
A 52 year-old Caucasian male with a history of chronic obstructive airway disease (COPD) presented to the emergency department complaining of progressive shortness of breath. Two days prior, the patient had presented to the ED with similar complaints that resolved with aerosol treatments and the patient was discharged on a metered dose inhaler (MDI). The patient had been prescribed MDI’s (metered dose inhalers) previously for management of his COPD, but due to financial constraints he had been unable to fill his prescription for the past month. Emergency medical services (EMS) suspected COPD exacerbation and administered 40 mg prednisone IV and two albuterol-ipratropriumnebulisertreatments en route to the hospital, which improved the patient’s breathing symptoms.
Upon arrival to the hospital, his blood pressure was 129/90, respirations 28, pulse 127, and he had an oxygen saturation of 100% on 7L/min. Physical examination revealed increased work of breathing, and wheezes in all lung fields with prolonged expiratory phase. The cardiovascular exam was normal except for tachycardia. A Routine electrocardiogram (ECG) revealed sinus tachycardia and T wave inversions in anterior leads. Chest x-ray showed old scarring in the left lower lobe. Routine cardiac enzymes showed mild elevation with a serum troponin level of 0.68ng/ml (normal range 0.0ng/ml-0.05ng/ml). The second set of troponin peaked at 1.66 ng/ml (normal 0.0ng/ml-0.05ng/ml). In view of the elevated cardiac enzymes atransthoracicechocardiogram was performed which demonstrated multiple wall motion abnormalities and reduced left ventricular ejection fraction of 25%. Coronary angiography demonstrated normal coronary arteries. Left ventriculography revealed hypokinetc mid-anterior and apical segment with a hypercontractile base with reduced ejection fraction (EF) of around 25% (normal range EF 55-65%) (Figure 1)
Figure 1. Left ventriculography demonstrating the classic appearance of Takotsubo cardiomyopathy
In light of the systolic dysfunction not in proportion with the degree of coronary artery stenosis and the multiple areas of wall motion abnormalities seen on echocardiogram, the diagnosis of Takotsubo cardiomyopathy (TCMP) was made. The diagnosis was further supported by the presence of ECG changes, troponin elevation, and the added social stresses of being unemployed. Over the course of his stay in hospital, the patient’s breathing improved with oral prednisone, inhaled tiotropium, and fluticasone/salmeterol. The patient was also treated with an angiotension converting enzyme inhibitor (ACE inhibitor), aspirin, statin, and beta-blockers. There were no adverse coronary events during the course of his hospital stay and the patient was discharged after four days. A Follow up echocardiogram after 4 weeks showed normal left ventricular systolic function.
DISCUSSION
Takotsubo cardiomyopathy (TCMP), also called stress-induced cardiomyopathy, apical ballooning syndrome, or broken heart syndrome, is a transient systolic dysfunction of the ventricles in the absence of significant coronary artery disease. Once thought to be a rare syndrome, TCMP is increasingly being identified in clinical practice, however, the prevalence and incidence are not known. It is estimated that 0.7-2.5% of patients who present with acute coronary syndrome are found to have TCMP1 .The majority of these patients are postmenopausal females, with a mean age of 62-75 years. They may present with chest pain and have a recent history of an emotional stress or severe medical illness. 1
The clinical manifestations of TCMP can mimic those of an acute myocardial infarction. Although, chest pain is a common presenting symptom, patients may also have complaints ofdyspnoeaand arrhythmias. In our casedyspnoeawas the predominant symptom and was easily confused with COPD exacerbation. Recently a few cases of concomitant stress cardiomyopathy with obstructive airway disease have been documented in literature. 2-4 While the pathophysiology of the coexistence of these two disorders is not fully understood, it is thought that both stress induced cardiac dysfunction due to exaggerated sympathetic activation and use of sympathomimetic bronchodilators instigates the myocardial stunning in such patients. Furthermore, an emotional stressor, such as death of a family member, or a physiological stressor, such as an acute medical illness, is thought to be a trigger for cardiomyopathy. 5 It is believed that the syndrome is not a result of anischemia, but there is some evidence to suggest thatoestrogenlevels may have a role in modulating the sympatho-adrenal outflow in TCMP. In mice models, chronic oestrogen supplementation seemed to have protective effects from exaggerated sympathetic outflow from the heart and brain6 . Postmenopausal women with low levels ofoestrogenmay be more vulnerable to the exaggerated catecholamine release in responses to stressors. 7
The characteristic finding in TCMP is a transient mid-ventricular or apical ballooning due to a hypokinetic portion seen on echocardiogram or on a left ventriculography. Systolic dysfunction is usually transient, inconsistent to the perfusion area of a single coronary artery, and usually resolves within 4-6 weeks. 8 Additional findings include ECG changes with ST segment deviations in precordial leads being the most common. Cardiac enzymes have been noted to have moderate elevations.9.
As data regarding the treatment of TCMP is limited, medical management mainly consists of symptomatic therapy with aspirin, ACE inhibitors, beta-blockers, and diuretics, also used in acute coronary syndrome.10 Patients who present acutely are treated as acute coronary syndrome and often receive emergency coronary angiography. However, less invasive imaging techniques, such as echocardiograms, should first be examined carefully. Due to the transient nature of the syndrome, the duration of treatment is unknown with some studies suggesting that there is no benefit with chronic treatment. 11 The prognosis is fairly good, with in hospital mortality rates being reported to range from 0-8%, and recovery of left ventricular function in the majority of patients. 9, 12
TCMP is difficult to distinguish from acute coronary syndrome on first presentation. Our patient had significant social stress. She presented with severedyspnoeaand was treated for COPD exacerbation. Elevation of cardiac enzymes and ECG changes lead to further evaluation and diagnosis of stress cardiomyopathy. This atypical presentation of TCMP showcases the importance ofutilisingthe routine noninvasive imaging and laboratory values to guide the diagnosis. Furthermore physicians need to maintain a high clinical suspicion for this syndrome.
It is often forgotten that smoking inducescytochrome P450 (CYP) 1A2, resulting in altered concentrations and required doses of drugs metabolized by this route. Conversely, upon cessation of smoking, concentrations of these drugs can rise to toxic levels unless appropriate dose adjustments are made. Medical staff, and others involved with smoking cessation counselling, need to be aware of this if potential harm to patients is to be avoided. Here, we describe a patient who developed tonic clonic seizures due to Theophylline toxicity, having ceased smoking 2 weeks earlier.
Case Report
Our patient is a 76-year-old lady who presented to A&E feeling generally unwell, with a two day history of dizziness. Her medical history included atrial fibrillation, which was treated with Digoxin 62.5mcg, and Chronic Obstructive Pulmonary Disease, for which she took a combination inhaler of 25mcg Salmeterol Xinafoate and 250mcg Fluticasone Propionate, 2 puffs twice a day, plus Theophylline MR 175mg twice daily. She had successfully given up smoking 2 weeks prior to admission, having smoked 100 cigarettes per day over the previous 40 years. On admission, she was in atrial fibrillation, well controlled with a heart rate of 90 beats per minute, and normotensive, with no evidence of postural hypotension. Respiratory system examination revealed prolonged expiration, in keeping with COPD, but the rest of the examination was unremarkable. Routine blood investigations, including full blood count, urea, creatinine and electrolytes, liver function tests and C-reactive protein, were all normal apart from a serum potassium level of 3.0mmol/l (NR 3.5-5.0mmol/l). Theophylline concentrations were not tested at this point. A chest X-ray showed hyper-inflated lung fields in keeping with Chronic Obstructive Pulmonary Disease.
The patient was admitted for observation, and treated with Trimethoprim for a presumed urinary tract infection on the basis of urinalysis, which was positive for leukocytes and nitrites.
Two days following admission, the patient developed facial spasms and twitching of her muscles of her upper limbs. Over the next 24 hours, the patient had two witnessed tonic-clonic seizures, which were terminated with intravenous Lorazepam. An urgent CT (Computed Tomography) scan of the brain was performed. This showed changes in keeping with small vessel disease only, nothing to account for new onset of seizures. Following a post-ictal period, the patient recovered, but then the following day had a further two tonic-clonic seizures. It was at this point that a blood Theophylline concentration was requested.
The Theophylline concentration was reported as 41.6mcg/ml (NR 10-19.9mcg/ml), more than twice the upper safe therapeutic concentration. A search of the laboratory system revealed that this patient’s Theophylline concentration had been within the therapeutic range when last checked 2 months prior to admission, while she was still smoking.
The Theophylline was immediately stopped and the patient closely monitored at the Medical High Dependency Unit for further fits, arrhythmias or electrolyte disturbances. Other causes of seizures had been investigated and excluded.
The patient’s neurological symptoms improved dramatically following cessation of Theophylline, with no further twitching, muscle spasms or seizures. Within three days her Theophylline concentration returned to a safe level, but the drug was not recommenced. Unfortunately, however, the patient died from sepsis two weeks following her admission without having left hospital.
Discussion
Theophylline has largely fallen out of favour as a treatment for airways disease due to its very narrow therapeutic index. Even within the therapeutic range, side effects frequently occur. These side effects range from mild, including tremor and gastrointestinal disturbance, to serious and potentially life threatening, such as seizures and cardiac arrhythmias. Following acute overdose, hypokalemia, hyperglycemia, hypercalcemia, hypophosphatemia, and acidosis commonly occur.
Theophylline is mainly metabolised in the liver by demethylation or oxidation using the cytochrome P450 system. The 8-hydroxylation of Theophylline to 1,3-dimethyluric acid (1,3-DMU) via cytochrome P450 1A2 is the major pathway.
The cytochrome P450 enzyme CYP1A2 mediates the rate-limiting step in the metabolism of Theophylline1, andthe polycyclic aromatic hydrocarbons found in cigarette smoke are potent inducers of this enzyme2. For this reason, smokers may need up to double the dose of Theophylline to achieve therapeutic effect compared with non-smokers3.
The relationship between smoking cessation and Theophylline has also been the subject of many studies. Lee et al demonstrated that stopping smoking for 1 week resulted in a 37.6% decrease in clearanceand a 35.8% increase in the half-life of Theophylline, and that the dose needs to be reduced by one fourth to one third after brief abstinence from tobacco to prevent potentially toxic concentrations4. For this reason, careful monitoring of plasma Theophylline concentration should be considered essentialfor optimal dosing in patients following smoking cessation. The study by Faber et al recommends that the dose of CYP1A2 substrates such as Theophylline should automatically be reduced by 10% on cessation of heavy smoking and thereafter be guided by plasma concentration monitoring5.
We found one report in which Theophylline toxicity resulted in a patient’s death following a similar presentation to the one described above6. This highlights the close attention that must be paid to drug concentration monitoring by physicians when advising patients to quit smoking.
Theophylline is not the only drug which needs to be considered when patients stop smoking. Other examples are Clozapine, Olanzapine, Haloperidol and Flecanide to name a few. These drugs are also substrates for CYP1A27.
Conclusion
When advising patients to stop smoking, it is essential that physicians routinely review the drugs that the patient is taking to look for those that may require dose adjustments. In the case of Theophylline, careful monitoring of Theophylline concentrations, for instance weekly in the first few weeks following smoking cessation, is essential to avoid potentially life-threatening complications.
Dr James Moon is a Senior Lecturer and Consultant Cardiologist at UCL and the Heart Hospital. He set up and runs the cardiac MRI department dividing his time between clinical practice and research.
He is part of a team of 5 research fellows in the new Heart Hospital Imaging department. He is interested in understanding the structure and function of the heart, particularly the heart muscle, and in detecting abnormalities of the heart to better target treatment.
How long have you been working in your speciality?
12 years (3 as consultant)
Which aspect of your work do you find most satisfying?
The creative aspects of research - joining the dots on information that does not fit and constructing a coherent body of work.
What achievements are you most proud of in your medical career?
Changing statin prescribing in England – as a registrar, I did not having access to cardiac MRI for 2 years and I worked relentlessly at all levels of the healthcare system –including up to Commons Health Select Committee - on this with the result that £1billion was saved or diverted to treat more individuals with statins – the UK now has the highest uptake of statins for primary prevention in the world.
Developing new ways of detecting different types of disease with MRI or CT scanners – in its latest iteration, we may be onto a technique that can measure a fundamental process common to most diseases and organs – not just the heart, and with CT as well as MRI: the volume of cells, fibrosis and their ratio.
Which part of your job do you enjoy the least?
New bureaucracy which we did without just a few years ago..
What are your views about the current status of medical training in your country and what do you think needs to change?
I worry about a tickbox ‘learning portfolio’ culture which dumbs down initiative and personal responsibility leaving a misplaced sense of entitlement.
How would you encourage more medical students into entering your speciality?
I’ve not seen the need to – cardiology is a fantastic, over-subscribed specialty with something for everyone so its pretty competitive.
What qualities do you think a good trainee should possess?
The same as those of a doctor. I have never seen this trainee:consultant divide; there is a continuum of learning and responsibility development.
What is the most important advice you could offer to a new trainee?
My advice is about learning rather than being a trainee. Medicine does not have that many raw facts to learn. What it does have is interconnected systems. Rarely consciously try and learn information – rather, try and link everything you have ever learned together, preventing isolated islands of knowledge. It takes longer to create the story, but you will never forget it and it’s far more rewarding. If you encounter something new - a tricky JVP waveform, an ECG repolarisation abnormality or some esoteric MRCP clinical sign, invoke your know of the physical world and apply it to explain the new phenomena – write the essay, deconvolute the phenomena and build it back up, perhaps with subtle changes to see where that gets you. You have spent decades learning about the Krebb’s cycle, anatomy, electron transport, fractals, Newtonian dynamics, Brownian motion, fluid dynamics, conservation of energy, entropy, cell structure, evolutionary biology, statistics etc etc – use them.
What qualities do you think a good trainer should possess?
I am not sure I know, but generating enthusiasm in people, and then rewarding and promoting it - that’s a good starting point.
Do you think doctors are over-regulated compared with other professions?
No.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what shouldbe done to counter this trend?
It’s the effects on individuals that concern me. I fully understand the need for process, protocol teamwork and hierarchy, but these remove individual responsibility
Which scientific paper/publication has influenced you the most?
The non-medical maths/science/philosophy books and magazines I read at school and university. I particularly remember Martin Gardner recreational maths books. Recently I have used fractals and the concepts behind trapdoor ciphers in my understanding of cardiology.
What single area of medical research in your speciality should be given priority?
Prioritize individual researchers/teams rather than topics to create progress through their enthusiasm and own perceptions of priorities.
What is the most challenging area in your speciality that needs further development?
Managing our increasing technical capability which comes with ever reducing incremental benefit.
Which changes would substantially improve the quality of healthcare in your country?
I would overhaul the way society pays for and develops drugs. I would focus on increasing drug company reward for the risk associated with genuine innovation whilst reducing reward for expensive ‘me too’ drugs with no added value. My group estimated that about 10% of the NHS drug budget could immediately be reallocated improving societal value for money in prescribing, paying for all those much needed NICE decision cancer type drugs and concurrently turbocharging rather empty pharmaceutical drug development pipelines.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Absolutely. If you have transparently good and altruistic ideas, are selfless about who gets he credit for them, and sufficiently driven to achieve results, the NHS is a wonderful place - its like a demagnetized iron – apply a sufficiently persuasive external field, and the domains line up, generating far more force and direction than expected.
How has the political environment affected your work?
The UK has been great for my field –new techniques are adopted early and the international bane of my field - cardiology-radiology turf wars are less acrimonious here as socialized medicine does not reimburse on a pay per procedure basis..
What are your interests outside of work?
My young family, recreational science, cooking.
If you were not a doctor, what would you do?
Who knows. Perhaps an economist or maybe evolutionary biologist.
Cosmetic outcome following breast-conserving surgery depends on various factors including location of the tumour, weight of the specimen excised, number of surgical procedures, volume of breast, length of scar and postoperative adjuvant treatment1. The best method of cosmetic assessment following breast-conserving surgery is still unclear. However various objective and subjective methods in combination are known to give a good assessment of cosmesis2, 3, 4. It has been shown that photographic assessment is as effective as live assessment in the post-surgical setting5. Methods to assess cosmesis following breast-conserving surgery are varied and more recently computer software are being used to assess cosmesis following breast-conserving surgery.
The aim of this study was to compare three different methods of cosmetic assessment following breast-conserving surgery and to assess the influence of various factors on final cosmetic outcome.
Methods:
One hundred and fifteen patients underwent breast-conserving surgery for carcinoma of breast by wide local excision and level 2 axillary clearance. Following wide local excision, cavity shavings were taken to ensure adequate local excision. Breast drainage was not used but suction drains were used routinely following axillary clearance. All patients received adjuvant breast radiotherapy (46 Gy, 23 fractions with a cavity boost of 12 Gy in 4 fractions) administered over a period of 6 weeks.
Figure-1: Measurement of Breast Retraction Assessment6 (reprinted with permission from Elsevier, ref 6 (page 670), copyright 1999)
Digital photographs were taken at one year in three views; frontal with arm by the side, frontal and oblique with arm abducted to 90 degrees. The photographs were used for subjective and objective assessment of cosmesis. The objective assessment of cosmesis was carried out using Breast Retraction Assessment (BRA) and Nipple Deviation (ND). BRA was calculated as indicated in figure 16. ND was calculated as a percentage difference from suprasternal notch to nipple on normal side compared with the operated side. BRA and ND were then categorised into three groups; BRA: (excellent to good <3.1 cm, fair 3.1-6.5, poor >6.5), ND: (difference of <5% - excellent to good, 5-10% fair and >10% poor). Subjective assessment was carried out using a panel consisting of a Consultant Breast Surgeon, Research Fellow, Secretary, Breast Care Nurse and Nurse Practitioner with each scoring independently. The method described by Harris et al7 with a score of 9-10 for excellent (no visible difference between two breasts), good (slight difference; score 7-8), fair (obvious difference but no major distortion; score 4-6) and poor (major distortion; score <4) was used to categorise patients.
Figure- 2: Measurement of breast volume (Sloane method) Formula for calculation of breast volume: 1/3 π r2h (reprinted with kind permission from Sloane project)
The volume of breast tissue excised was estimated with the length (L), width (W) and height (H) of the excised tissue specimen and the cavity shave measured by the pathologist and using the formulas for a prolate ellipse (V= 0.52* L* W* H); this was added on to the volume of cavity shave calculated using the formula 0.79* L* W* H. The total breast volume was estimated using the mammogram and applying the formula (1/3 πr2h) as shown in figure-2. Based on these measurements the percentage breast volume excised was calculated and compared with cosmetic outcome.
Statistics:
Multirater kappa statistics8 were used to assess inter-observer agreement between five different members of the panel and also to test agreement between the three different methods for assessing cosmesis. The average value given by the panel was used and categories good and excellent were combined in order to compare the three methods of cosmetic assessment. A kappa statistic of less than or equal to 0.20 was considered to demonstrate poor agreement, 0.21 to 0.40 fair agreement, 0.41 to 0.60 moderate agreement, 0.61 to 0.80 good agreement and 0.81-1.00 very good agreement9.
The effect of the percentage volume of the breast tissue excised and the tumour size on the three methods of cosmetic assessment was examined using where appropriate a Jonckhneere-Terpstra test for trend, a Kruskal Wallis test or a Mann-Whitney U test. The effect of the number of breast operations performed and the location of the tumour were assessed using Chi-square test or Fisher’s exact test when appropriate.
Results:
Of the 115 patients assessed using panel assessment 64 (56%) scored good to excellent, 39 (34%) scored fair and 12 (10%) scored poor. ND scored 50(43%) as good to excellent, 32 (28%) as fair and 33 (29%) as poor. Using BRA, the scores were 76 (66%), 38 (33%) and 1(1%) respectively. These results are shown graphically in figure-3.
Figure- 3: Number of patients classified into each of the three categories poor, fair and good/excellent for the three methods bra, nipple deviation and panel assessment. BRA= breast retraction assessment; Panel= assessment by different panel members; ND= nipple deviation
Taking the mean scores for these three methods of assessment and dichotomising the results into two categories of good to excellent and poor to fair, 52% of patients in this study had good to excellent cosmetic result and 48% were categorised as fair to poor cosmetic result. The Kappa statistic was calculated on 115 patients for the three methods of assessment and it was found to have a value of –0.23 (95% CI (–0.35, – 0.11) which falls within the poor agreement category.
Figure- 4: Comparison of panel assessment by different panel members. Pa, Ph, Pg, Pk and Pd= Codes for the different panel members
Examining the panel assessment using the kappa statistics for the 115 patients assessed there was moderate agreement between the panel members (Kappa statistic of 0.42; 95% confidence interval of (0.37, 0.47). This suggests there is moderate chance that the panel members will categorise each patient the same way. If one plots the panel assessment graphically one can see that excellent is used least by all and fair most frequently (figure 4).
Factors affecting cosmesis:
1) Percentage breast volume excised
Figure -5: Effect of percentage breast volume excised on cosmetic outcome using Panel assessment, BRA and ND
For panel assessment it appears that removal of a larger percentage volume gives a poor cosmetic result and a smaller percentage volume an excellent/good result (figure 5) as would be expected clinically. This is supported by a Jonckhneere-Terpstra test for trend (=0.01). Using ND median percentage volumes across the groups did not appear to differ (χ2=1.05 p=0.59, Kruskal Wallis test). However, for BRA, only one patient was classified as poor and no difference was seen between those with fair and good/excellent results (U=477, p=0.34). The median volume excised for different cosmetic outcome using the three methods is shown in table 1.
Table-1: Medians volumes for the three measurements.
Panel assessment
BRA
Nipple deviation
Poor
157.56
(only 1 poor value)
100.61
Fair
88.58
93.11
55.96
Good/Excellent
68.33
76.55
81.33
BRA= breast retraction assessment
BRA= breast retraction assessment
The percentage breast volume excised was then compared with cosmetic outcome using the three methods of assessment. As shown in table 2, 45-65% of patients with <10% estimated breast volume excised had good to excellent cosmetic result compared with 35-50% good to excellent result if >10% breast volume was excised.
2) Tumour location:
Tumour location was divided into inner or outer quadrants of the breast. The distribution of tumours in the breast and the cosmetic outcome with each of the three methods of assessment is shown in table 3. The location of tumour within the breast was not significantly associated with cosmetic outcome (χ2 =1.86, p=0.39 for panel assessment), (p=0.23, Fisher’s exact test for BRA) and (χ2 =0.21, p=0.90 for ND).
Table-2: Estimated percentage breast volume excised and cosmetic outcome
< 10% breast volume excised
> 10% breast volume excised
Panel Assessment
Good to excellent (%)
32 (65)
7 (35)
Fair (%)
15 (31)
6 (30)
Poor (%)
2 (4)
7 (35)
Breast Retraction Assessment
Good to excellent (%)
32 (65)
10 (50)
Fair (%)
16 (33)
10 (50)
Poor (%)
1 (2)
0
Nipple Deviation
Good to excellent (%)
22 (45)
8 (40)
Fair (%)
15 (31)
4 (20)
Poor (%)
12 (24)
8 (40)
3) Number of breast operations:
The influence of number of operations (1 vs 2) was examined for each of the three methods of assessment. Using BRA and Panel assessment there was no significant difference in the cosmetic outcome for patients who underwent one or two operations ( p=0.70 for panel assessment), (p=0.99, Fisher’s exact test for BRA). For ND there does appear to be a larger proportion in the poor group for those with two operations (p =0.30 Fisher’s exact test for ND). This is illustrated in Table 3.
Table-3: Factors affecting cosmesis
Table-3: Factors affecting cosmesis
Panel
BRA
ND
Percentage volume excised
Poor (median (IQR))
Fair (median (IQR))
Good/Excellent (median (IQR))
13.8 (11.0,16.5)
8.4 (4.4,10.4)
5.8 (3.9,8.0)
-
8.0 (4.6,11.6)
6.9 (4.3,10.1)
8.5 (5.1,11.4)
5.8 (3.9,9.4)
7.2 (4.4,11.0)
Location
Poor (outer (n), inner (n))
Fair (outer (n), inner (n))
Good/Excellent (outer (n), inner (n))
8, 2
22,8
47,8
0,1
26,5
51,12
9,1
23,6
33,8
No. of Operations
Poor (One (n), Two (n))
Fair (One (n), Two (n))
Good/Excellent (One (n), Two (n))
9,1
24,6
48,8
1,0
26,5
54,10
20,5
27,2
34,8
Tumour size (mm)
Poor (median (IQR)
Fair (median (IQR)
Good/ Excellent (median (IQR)
12 (9, 15)
11 (9, 19)
12 (7, 15)
-
11 (8,15)
12 (7, 15)
12 (10, 15)
12 (8, 16)
9 (6,14)
Panel= panel assessment; BRA= breast retraction assessment; ND= nipple deviation; IQR= inter quartile range
Panel= panel assessment; BRA= breast retraction assessment; ND= nipple deviation; IQR= inter quartile range
4) Tumour size:
Table 3 shows the median tumour size and interquartile range for the three categories, good/ excellent, fair and poor and one can see that there is no significant difference in tumour size for these categories using panel assessment (Jonckheere-Terpstra p=0.31) or BRA (U =873, p=0.55). However, using ND there was evidence to suggest that large tumour size resulted in poor outcome (Jonckheere-Terpstra, p=0.04).
Thus, tumour size had a significant influence on the cosmetic outcome when ND was used as the method of assessment.
Discussion:
Cosmetic outcome following breast-conserving surgery is assessed using a combination of subjective and objective methods. The subjective method uses a panel of members from different backgrounds to assess overall cosmesis. However, Pezner et al10 showed relatively low level of agreement between observers when a four-point scale was used for assessment of overall cosmesis. The objective methods, which mainly compare the position of the nipple, are easy to reproduce but do not take into account skin changes and give poor assessment of cosmesis for lower quadrant tumours.
In this study the cosmetic outcome was assessed in 115 patients one year post-operatively. The mean cosmetic result using the three different methods of assessment was good to excellent in 55% of the patients, which compares favourably with other studies reported in the literature2, 4. Looking at inter-observer variation for the panel assessment, moderate agreement was found between different panel members. This compares favourably with an earlier study that looked at cosmetic outcome in the EORTC trial 22881/108826. However, when the three methods of cosmetic assessment were compared with each using kappa statistic there was poor concordance. Although some agreement was noted, this was likely to be due to chance as the kappa statistic was low. It is difficult to explain this finding as other authors1, 6 have reported moderate to good agreement between subjective and objective methods. One explanation for this lack of agreement is that each method assesses a different aspect of cosmesis.
The two objective methods of cosmetic assessment (BRA and ND) that are used to assess upward retraction of nipple have been found to be a very good determinant of cosmetic outcome and are easy to reproduce according to Fujishiro et al11. Furthermore, evaluation of nipple position has also been shown to be moderately representative of overall cosmetic result6. BRA is a two dimensional measurement of nipple position and some cosmetic factors such as volume, shape or skin changes cannot be accurately assessed11. This is probably the reason why BRA shows a better cosmetic outcome when compared with subjective assessment by panel members. In this study only one (1%) patient was deemed to have a poor cosmetic outcome using BRA compared with 12 (10%) using panel assessment.
A criticism of the current study is that patients’ perceptions of their own cosmetic outcome were not assessed. Previous studies have shown a significant correlation between patient satisfaction after breast-conserving surgery and their self-assessment of cosmesis12, 13. This study shows that there is need to find a reproducible method of cosmetic assessment which takes into account all the limitations of the methods currently used. More recently computer software like BCCT.core and Breast Analysing Tool have been developed and early results using these software are promising14, 15. There are various factors that are known to affect cosmesis following breast-conserving surgery. As expected larger percentage volume of excised breast tissue was associated with poorer cosmetic result. This was particularly evident from panel assessment. Such a relationship was less clear with BRA and ND. The effect of percentage volume of breast tissue excised and the outcome is consistent with a recent report that showed higher patient satisfaction if estimated percentage breast volume excised was < 10%16. Cosmetic outcome based on tumour location varies depending on the method of assessment used. BRA is adversely affected by tumour in the upper and outer quadrants of the breast, suggesting that surgery causes larger nipple deviation in this quadrant, while panel assessment gives poor scores for tumours located in inferior quadrant2, 11. In this study only 19% of patients had tumours located in the inner quadrant and the small number may explain why, no significant difference in cosmetic outcome was found. Tumour location or the number of operations performed did not appear to affect the cosmetic outcome in this study. The volume of breast tissue excised depends on tumour size. Since the majority of tumours in this study were small, the size of the tumour did not affect cosmetic outcome except when nipple deviation was used. This once again indicates that these three methods of assessment may be looking at different aspects of cosmesis.
In conclusion, cosmetic outcome following breast-conserving surgery is an important, measurable end point. However, the best method of assessment of cosmesis has not been devised17. Although, the objective methods are easier to apply and reproduce, they do not give a good assessment of global cosmetic results. Panel Assessment however, does appear to provide concordant results between different observers and may be a useful, simple measure of cosmetic assessment following breast-conserving surgery.
Bisphosphonates, which have been on the market for roughly a decade, have raised safety concerns in the past. Several case series and multiple individual case reports suggest that some subtrochanteric and femoral shaft fractures may occur in patients who have been treated with long-term bisphosphonates. Several unique clinical and radiographic features are emerging. Recent media spotlight in the United States (US), implying that long-term use of alendronate could cause spontaneous femur fractures in some women, has reignited the debate about the safety of bisphosphonates. The question posed: is the risk of bisphosphonate-associated fractures so great that treatment should be stopped?
Postmenopausal women with osteoporosis are commonly treated with the bisphosphonate class of medications, one of the most frequently prescribed medications in the US. While alendronate therapy has been shown to decrease the risk of vertebral and femoral neck fractures in postmenopausal osteoporotic patients, recent reports have associated long-term alendronate therapy with low-energy subtrochanteric and diaphyseal femoral fractures in a number of patients. In the past four years reports have been published implying that long-term bisphosphonate therapy could be linked to atraumatic femoral diaphyseal fractures.1, 2 According to two studies reported recently at the American Association of Orthopedic Surgeons 2010 Annual Meeting, an unusual type of bone fracture has been reported in women who have taken bisphosphonates for osteopenia and osteoporosis for more than four years.3, 4 The first report was published in 2005. Odvina et al5 reported on nine patients who sustained atypical fractures, including some with delayed healing, while receiving alendronate therapy. These authors raised the concern that long-term bisphosphonate therapy may lead to over-suppression of bone remodelling, an impaired ability to repair skeletal microfractures, and increased skeletal fragility. There have been other reports of "peculiar" fractures - i.e. low-energy femur fractures that are typically transverse or slightly oblique, diaphyseal, or subtrochanteric, with thickened cortices and a unicortical beak - in patients who have been on long-term bisphosphonate treatment.1-4, 6
In a small prospective study, Lane et al3 obtained bone biopsies from the lateral femurs of 21 postmenopausal women with femoral fractures. Twelve of the women had been on bisphosphonate therapy for an average duration of 8.5 years, and nine had no history of bisphosphonate use. They found that the heterogeneities of the mineral/matrix ratio were significantly reduced in the bisphosphonate group by 28%, and the crystallinity of the bone was significantly reduced by 33% (p < 0.05). The authors concluded that this suggested suppression of bone turnover, resulting in a loss of heterogeneity of the tissue properties, which may be a contributing factor to the risk of atypical fractures that we are starting to see. It is believed that long-term alendronate administration may inhibit normal repair of microdamage arising from severe suppression of bone turnover (SSBT), which, in turn, results in accumulation of microdamage. This process would lead to brittle bone and the occurrence of unexpected stress fractures, characteristically at the subtrochanter of femur. The typical presentation of these fractures consist of prodromal pain in the affected leg and/or a discrete cortical thickening on the lateral side of the femur in conventional radiological examination or the presentation with a spontaneous transverse subtrochanteric femur with typical features. The morbidity of atypical femoral fractures, particularly when bilateral, is high. Surgical intervention is generally required and healing may not be achieved for several years. Despite the lack of conclusive evidence of a causal relationship with bisphosphonate therapy, the current consensus is that treatment should be discontinued in patients who develop these fractures. In view of the high frequency of bilateral involvement, imaging of the contralateral femoral shaft with X-rays, MRI, or an isotope bone scan should be performed. MRI and bone scanning havegreater sensitivity than radiography for an incipient stressfracture. If lateral cortical thickening and/or an incipient stress fracture is seen, prophylactic surgical fixation should be considered. Suppressed bone formation in these patients provides a possible rationale for the use of anabolic skeletal agents, such as parathyroid hormone peptides, but at the present time the efficacy of this approach remains to be established. Parathyroid hormone not only has activated bone-formation markersin trials in humans but has also enhanced the healing of fracturesin studies in animals.
The question of whether these fractures are causally linked to bisphosphonate therapy is widely debated but as yet unresolved. Consequences of long-term suppression of bone turnover include increased mineralization of bone, alterations in the composition of its mineral/matrix composite and increased micro damage, all of which may reduce bone strength. Whilst these lend biological plausibility to a causal association, however, they do not constitute direct evidence. The bilateral fractures seen in many patients corroborate the suspicion that patients with bisphosphonate-associated stress fractures carry some other risk factor in addition to taking the drug. Microfractures,inadequate mineralization, and outdated collagen are some of the candidate causes. However, until further studies can provide definitive evidenceof bisphosphonate-associated fractures, it is premature to attributeatypical fractures to over-suppression of bone turnover alone,while disregarding secondary and patient-related factors. Many experts believe that prolonged suppression of bone remodelling with alendronate may be associated with a new form of insufficiency fracture of the femur. Studies have not shown if the entire class of medications produce a similar result, but patients who have been treated with any bisphosphonate for an extended period of time should be considered at risk.
A wealth of information from well-designed clinical trials clearly shows that, as a class, bisphosphonates are highly effective at limiting the loss of bone mass, deterioration of bone micro architecture, and increased fracture risk that occur with aging. The benefit/risk ratio of bisphosphonate therapy in patients at high risk of fracture remains overwhelmingly positive because of the very low incidence of atypical femoral fractures. Current estimates suggest that alendronate prevents 200 clinical fractures if 4000 women are treated over three years and will cause one femur fracture over the same course of time.7 A study by Schilcher et al8 found that the incidence density of a stress fracture for a patient on bisphosphonate was 1/1000 per year (95% CI: 0.3-2), which is acceptable considering that bisphosphonate treatment is likely to reduce the incidence density of any fracture by 15/1000.9 Nevertheless, limitation of treatment duration to five years in the first instance, with evaluation of the need to continue therapy thereafter, may be appropriate in clinical practice. The Fracture Intervention Trial Long-term Extension (FLEX), in which postmenopausal women who had received alendronate therapy for five years were randomised to continue receiving alendronate for five additional years or switched to placebo, provided clinical evidence that the effect of bisphosphonate therapy was maintained after discontinuation of therapy.7, 10 Women who are being treated with bisphosphonates should take a drug holiday if they have been on them for five years. Patients in whom bisphosphonate therapy is discontinued should typically follow up with bone mineral density measurements at 1- to 2-year intervals, with some experts advocating periodic measurement of biochemical markers of bone turnover to detect loss of the antiresorptive effect. Additional research is necessary to determine the exact correlation between the use of bisphosphonates and spontaneous or low-energy trauma fractures.
Professor Elisabeth Paice is currently on secondment to NHS London having been appointed to the new post of Acting Director of Medical and Dental Education from her role as Dean Director at London Deanery. The new role will ensure that the right number of doctors and dentists have the right training to deliver the service ambitions outlined in Healthcare for London. Elisabeth will be leading on the Medical and Dental Education Commissioning System (MDECS). This is the name of the programme of work that will manage the changes to postgraduate medical and dental training.
She was born in Washington DC, brought up in Canada, and studied medicine first at Trinity College Dublin and later at Westminster Medical School. She was the originator of the 'Hospital at Night' concept; developed the 'Point of View Surveys'; chaired PMETB working parties on Generic Standards and the National Trainee Survey and has published variously including on doctors in difficulty; workplace bullying; women in medicine. She was Chair of COPMeD, Conference of Postgraduate Medical Deans, from July 2006 to July 2008.
How long have you been working in your speciality?
I have been a full-time postgraduate dean since 1995. Before that I was a consultant rheumatologist for 13 years.
Which aspect of your work do you find most satisfying?
I get great satisfaction out of developing and implementing new ideas, especially when they work well enough to be taken up by others. I think most doctors have a creative streak and sometimes bureaucracy can damp this down. One of the reasons why medical education and training is so enjoyable is that it has to keep changing because of changes in the way the service is developing. There are standards to be met, of course, and regulators to satisfy, but within those constraints there is plenty of room for innovation. The better the quality of education and training, the better and safer the care of patients.
What achievements are you most proud of in your medical career?
As Dean Director of London, I have been very proud to lead postgraduate medical and dental education in one of the world’s great cities, with its five world-renowned medical schools, numerous centres of clinical excellence, and over 10,000 trainees. In order to understand trainees’ views, I introduced a regular survey through which they could voice their views about the quality of training they were receiving. I was very pleased when this formed the basis of the very successful National Trainee Doctor Survey, now embarking on its fourth iteration. This survey has enabled postgraduate deans across the UK to identify departments where training is not meeting the minimum standards for training and to take appropriate action.
Other achievements of which I am proud include the development of a multiprofessional team-based approach to out of hours services, known as the Hospital at Night initiative, which has improved patient safety while providing a solution for reducing the hours of junior doctors. Most recently I am delighted with the success of London’s Simulation and Technology-enhanced Learning Initiative (STeLI) which recently won the prestigious Health Service Journal Award for Patient Safety.
Which part of your job do you enjoy the least?
I least enjoy dealing with performance issues, whether internal to my staff or among trainees or their trainers.
What are your views about the current status of medical training in your country and what do you think needs to change?
Medical education is recognized in the UK as being a vital factor in providing the high quality doctors necessary for a high quality health service. It needs to be better resourced, and in particular every doctor with responsibility for educational supervision needs to have the training, the time, and the tools to do a good job. The way in which training has traditionally taken place, known as the ‘apprenticeship model’, is no longer suitable because of restrictions on the hours of work. I am all in favour of these restrictions, because long hours have a negative impact on learning and pose a risk to the health and safety of both doctors and patients. But we need radical change in the way we depend on doctors in training to provide out of hours cover and we need to find robust ways to ensure they gain the practical experience they need.
How would you encourage more medical students into entering your speciality?
I would strongly encourage any medical student to consider taking an interest in medical education from the start. Whatever the field of medicine that they enter, there will inevitably be an expectation that they will teach the next generation of doctors and of other healthcare professionals. Teaching is increasingly being recognized as one of the duties of a doctor, and like anything else, the more effort you put in, the more rewarding the outcomes.
What qualities do you think a good trainee should possess?
Trainees need to have a solid grounding in the basic sciences, because it is the foundation on which their postgraduate training will build. They need to be both conscientious and curious, doing what is required of them, but also going the extra mile in the search for knowledge. They should be motivated by the desire to make a positive difference to the lives of others, because I believe that is the only motivation that stands the test of time.
What is the most important advice you could offer to a new trainee?
Read the curriculum, establish what is expected of you and what you can expect from your seniors and your team, and engage with the educational programme.
What qualities do you think a good trainer should possess?
Kindness, honesty, expertise - and a passion for developing these qualities in their juniors.
Do you think doctors are over-regulated compared with other professions?
No, it is a profession in which we can potentially harm others, regulation is a necessity.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what should be done to counter this trend? The responsibility for the professionalism of a doctor lies with the doctor. There are no policies in the UK that de-professionalise doctors.
Which scientific paper/publication has influenced you the most? I have been heavily influenced by the body of work by Charles Czeisler in the USA and Philippa Gander in New Zealand about the impact of long hours and sleep deprivation on health, safety, errors and retention of learning of doctors in training.
What single area of medical research in your speciality should be given priority? Simulation technology.
What is the most challenging area in your speciality that needs further development? Fitting adequate training into a 48 hour week without lengthening the duration of training
Which changes would substantially improve the quality of healthcare in your country?
Improving the training of general practitioners
Do you think doctors can make a valuable contribution to healthcare management? If so how?
All doctors need to learn to look after the system of care as well as the patient in front of them. Medical leadership is crucial to modernizing services. During training all doctors should be involved in quality improvement initiatives and all should learn how to champion change effectively.
How has the political environment affected your work?
The most recent impact has come from the national policy to introduce a separation between the commissioning of education and its provision. This has meant a reorganization of the way we work, with much of the work we did being commissioned from lead providers. While change is always disconcerting, there are real benefits to be realized from this one, in particular a better alignment between service and education planning.
What are your interests outside of work?
Looking after our four delightful grandchildren
If you were not a doctor, what would you do?
When I was at school I planned to write plays, but a medical career has sated my appetite for drama.
He'd try to sit, couldn't hold on for long,
Fidgety, restless, frustration would only prolong
Tried hard to listen to parents and teacher,
Distracted, voices sounding like a background clutter
Kept working on sitting listening and learning
Realized wasn't at par with kids and his sibling
This sentence would redundantly echo in his head
"Sit, listen, learn" you dumb head!!!
"How come life can't be better than what I feel?"
Why is it so hard for me to deal
My head hurts after constant listening,
Nothing I do is gratifying
They say, am not in same learning standard curve as other kids
My parents are worried for me, not understanding my needs
Have tried all avenues, anger, love , comfort, compassion,
Yet everyday is a challenge for them to find a solution
They interpreted his "not sitting still as restlessness",
Not listening and disruptive behaviour as impulsiveness
His attention level considered as poor learning skills
parents embarrassed, trying to overcome his hills
"Trust me”, He'd say, “you don’t understand, I'm trying my best"
Parents instead kept echoing sit, listen and learn, and accept it as a test
All this felt repetitive and redundant in his head,
Until someone said "maybe something is wrong with his brain instead"
Suggested see a doctor who might help clear the clutter away
Who observed his behaviour without decision to change him right away,
That's when he told the parents "Your child has had attention deficit disorder"
They felt was a mental taboo, and asked not to speak about it louder
The doctor insisted on strict compliance and periodic follow-up
Meds, mental stimulation exercises worked, felt no more like empty cup
Before he knew, he was sitting longer, nothing felt like clutter
Realized the deficit had prevented him from thinking better
Parents and doctors worked together, we salute them for the joint effort,
helped him evolve into the person altogether different
He listens to his inner and external suggestions alone and in group discussions,
Has learned realities of life, applying them in every day decisions
Sits down for hours working on his research projects
Sit, listen, learn, now all sound real, not mystical acts
The fundamental responsibility of an anesthesiologist is to maintain adequate gas exchange through a patent airway. Failure to maintain a patent airway for more than a few minutes results in brain damage or death1. Anaesthesia in a patient with a difficult airway can lead to both direct airway trauma and morbidity from hypoxia and hypercarbia. Direct airway trauma occurs because the management of the difficult airway often involves the application of more physical force to the patient’s airway than is normally used. Much of the morbidity specifically attributable to managing a difficult airway comes from an interruption of gas exchange (hypoxia and hypercapnia), which may then cause brain damage and cardiovascular activation or depression2.
Though endotracheal intubation is a routine procedure for all anesthesiologists, occasions may arise when even an experienced anesthesiologist might have great difficulty in the technique of intubation for successful control of the airway. As difficult intubation occurs infrequently and is not easy to define, research has been directed at predicting difficult laryngoscopy, i.e. when is not possible to visualize any portion of the vocal cords after multiple attempts at conventional laryngoscopy. It is argued that if difficult laryngoscopy has been predicted and intubation is essential, skilled assistance and specialist equipment should be provided. Although the incidence of difficult or failed tracheal intubation is comparatively low, unexpected difficulties and poorly managed situations may result in a life threatening condition or even death3.
Difficulty in intubation is usually associated with difficulty in exposing the glottis by direct laryngoscopy. This involves a series of manoeuvres, including extending the head, opening the mouth, displacing and compressing the tongue into the submandibular space and lifting the mandible forward. The ease or difficulty in performing each of these manoeuvres can be assessed by one or more parameters4.
Extension of the head at the atlanto-occipital joint can be assessed by simply looking at the movements of the head, measuring the sternomental distance, or by using devices to measure the angle5. Mouth opening can be assessed by measuring the distance between upper and lower incisors with the mouth fully open. The ease of lifting the mandible can be assessed by comparing the relative position of the lower incisors in comparison with the upper incisors after forward protrusion of the mandible6. The measurement of the mento-hyoid distance and thyromental distance provide a rough estimate of the submandibular space7. The ability of the patient to move the lower incisor in front of the upper incisor tells us about jaw movement. The classification provided by Mallampati et al8 and later modified by Samsoon and Young9 helps to assess the size of tongue relative to the oropharynx. Abnormalities in one or more of these parameters may help predict difficulty in direct laryngoscopy1.
Initial studies attempted to compare individual parameters to predict difficult intubation with mixed results8,9. Later studies have attempted to create a scoring system3,10 or a complex mathematical model11,12. This study is an attempt to verify which of these factors are significantly associated with difficult exposure of glottis and to rank them according to the strength of association.
Materials & methods
The study was conducted after obtaining institutional review board approval. Six hundred ASA I & II adult patients, scheduled for various elective procedures under general anesthesia, were included in the study after obtaining informed consent. Patients with gross abnormalities of the airway were excluded from the study. All patients were assessed the evening before surgery by a single observer. The details of airway assessment are given in Table I.
Table I: Method of assessment of various airway parameters (predictors)
Airway Parameter
Method of assessment
Modified Mallampati Scoring
Class I: Faucial pillars, soft palate and uvula visible.
Class II: Soft palate and base of uvula seen
Class III: Only soft palate visible.
Class IV: Soft palate not seen
Class I & II : Easy Intubation
Class III & IV: Difficult Intubation
Obesity
Obese BMI (≥ 25)
Non Obese BMI (< 25)
Inter Incisor Gap
Distance between the incisors with mouth fully open(cms)
Thyromental distance
Distance between the tip of thyroid cartilage and tip of chin, with fully extended(cms)
Degree of Head Extension
Grade I ≥ 90◦
Grade II = 80◦-90◦
Grade III < 80◦
Grading of Prognathism
Class A: - Lower incisor protruded anterior to the upper incisor.
Class B: - Lower incisor brought edge to edge with upper incisor but not anterior to them.
Class C: - Lower incisors could be brought edge to edge.
In addition the patients were examined for the following.
High arched palate.
Protruding maximally incisor (Buck teeth)
Wide & short Neck
Direct laryngoscopy with Macintosh blade was performed by an anaesthetist who was blinded to preoperative assessment.
Glottic exposure was graded as per Cormack-Lehane classification13 (Fig 1).
Figure 1: Cormack-Lehane grading of glottic exposure on direct laryngoscopy
Grade 1: most of the glottis visible; Grade 2: only the posterior extremity of the glottis and the epiglottis visible; Grade 3: no part of the glottis visible, only the epiglottis seen; Grade 4: not even the epiglottis seen. Grades 1 and 2 were considered as ‘easy’ and grades 3 and 4 as ‘difficult’.
Results
Glottic exposure on direct laryngoscopy was difficult in 20 (3.3%) patients.
The frequency of patients in various categories of ‘predictor’ variables is given in Table-II
Table II: The frequency analysis of predictor parameters
Airway Parameter
Group
Frequency (%)
Modified Mallampati Scoring
Class 1&2
Class 3&4
96%
4%
Obesity
Obese BMI (≥ 25)
Non Obese BMI (< 25)
28.7%
71.3%
Inter Incisor Gap
Class I : >4cm
Class II: <4cm
93.5%
6.5%
Thyromental distance
Class I: ≥ 6cm.
Class II: ≤6cm.
94.6%
5.4%
Head & Neck Movements
Difficult {class II & III (90˚)}
Easy {class I(>90˚)}
16%
84%
Grading of Prognathism
Difficult (class III)
Easy (class I + II)
96.1%
3.9%
Wide and Short neck
Normal neck body ratio 1:13
Difficult (Ratio≥ 1:13)
86.9%
13.1%
High arched Palate
Yes
No
1.9%
98.1%
Protruding Incisors
Yes
No
4.2%
95.8%
The association between different variables and difficulty in intubation was evaluated using the chi-square test for qualitative data and the student’s test for quantitative data and p<0.05 was regarded as significant. The clinical data of each test was used to obtain the sensitivity, specificity and positive and negative predictive values. Results are shown in Table III.
Table III: Comparative analysis of various physical factors and scoring systems
Physical factors and various Scoring Systems
Sensitivity ( % )
Specificity ( % )
PPV
( % )
NPV
( % )
Obesity
81.8
72.76
6.34
99.43
Inter incisor gap
18.8
94.14
6.6
98.1
Thyromental distance
72.7
96.5
32.0
99.4
Head and Neck movement
86.36
86.0
34.6
99.7
Prognathism
4.5
96.3
2.7
97.9
Wide and Short neck
45.5
87.9
7.8
98.6
High arched palate
40.1
99.38
60.0
98.67
Protruding incisor
4.6
95.9
2.5
97.79
Mallampati scoring system
77.3
98.2
48.57
99.5
Cormack and Lehane’s scoring system
100
99.7
88
100
Discussion
Difficulty in endotracheal intubation constitutes an important cause of morbidity and mortality, especially when it is not anticipated preoperatively. This unexpected difficulty in intubation is the result of a lack of accurate predictive tests and inadequate preoperative assessment of the airway. Risk factors if identified at the preoperative visit help to alert the anaesthetist so that alternative methods of securing the airway can be used or additional expertise sought before hand.
Direct laryngoscopy is the gold standard for tracheal intubation. There is no single definition of difficult intubation but the ASA defines it as occurring when “tracheal intubation requires multiple attempts, in the presence or absence of tracheal pathology”. Difficult glottic view on direct laryngoscopy is the most common cause of difficult intubation. The incidence of difficult intubation in this study is similar to that found in others.
As for as the predictors are concerned, different parameters for the prediction of difficult airways have been studied. Restriction of head and neck movement and decreased mandibular space have been identified as important predictors in other studies. Mallampati classification has been reported to be a good predictor by many but found to be of limited value by others14. Interincisor gap, forward movement of jaw and thyromental distance have produced variable results in predicting difficult airways in previous studies7,15. Even though thyromental distance is a measure of mandibular space, it is influenced by degree of head extension.
There have been attempts to create various scores in the past. Many of them could not be reproduced by others or were shown to be of limited practical value. Complicated mathematical models based on clinical and/or radiological parameters have been proposed in the past16, but these are difficult to understand and follow in clinical settings. Many of these studies consider all the parameters to be of equal importance.
Instead of trying to find ‘ideal’ predictor(s), scores or models, we simply arranged them in an order based on the strength of association with difficult intubation. Restricted extension of head, decreased thyromental distance and poor Mallampati class are significantly associated with difficult intubation.
In other words patients with decreased head extension are at much higher risk of having a difficult intubation compared to those with abnormalities in other parameters. The type of equipment needed can be chosen according to the parameter which is abnormal. For example in a patient with decreased mandibular space, it may be prudent to choose devices which do not involve displacement of the tongue like the Bullard laryngoscope or Fiber-optic laryngoscope. Similarly in patients with decreased head extension devices like the McCoy Larngoscope are likely to be more successful.
Conclusion
This prospective study assessed the efficacy of various parameters of airway assessment as predictors of difficult intubation. We have find that head and neck movements, high arched palate, thyromental distance & Modified Malampatti classification are the best predictors of difficult intubation.
The implementation of Modernising Medical Careers (MMC) significantly altered the structure of postgraduate medical education in the UK. MMC oversees the training of all UK doctors from the outset of their career, the first two years of which comprise the Foundation Programme. Successful completion of the Foundation Programme is based upon doctors’ Foundation Portfolios in which they must demonstrate achievement of essential competences and work-based assessments. Doctors are also encouraged to attain additional competencies and to develop their portfolio further. Voluntary educational activities undertaken outside the workplace form the basis of this.
Application into Specialist Training following the Foundation Programme is highly competitive, with an average of three applicants for each post in 20081. Points-based shortlisting criteria are used to select candidates, and are based upon the contents of the Foundation Portfolio and application form. This means that points can be scored for activities not required for completion of the Foundation Programme, such as Royal College membership examinations and course attendance. Foundation Programme doctors undertake voluntary activities to improve their portfolios however no quantifiable evidence currently exists as to what doctors undertake in this respect.
We aimed, therefore, to determine firstly what voluntary educational activities Foundation doctors are undertaking. We also aimed to establish their underlying motivating and deterring factors, financial costs incurred, and use of annual and study leave and ‘specialty taster days’, to assess the overall extent and impact of portfolio activities. The authors hope the results are useful in informing medical students and Foundation trainees of the scope of activities of their peers, and in advising supervisors of the activities of their trainees.
Methods
A two page anonymous questionnaire was posted at random to 100 Foundation doctors across five hospitals in East Midlands Deanery (50 Foundation Year 1, 50 Foundation Year 2). See Appendix 1
Demographics
The first section of the questionnaire asked for the sex and grade of respondents (Foundation Year 1 (FY1), or Foundation Year 2 (FY2))
Activities
Respondents were directly asked whether they were attending courses or conferences, using on-line e-learning packages, joining professional bodies/societies or sitting higher professional examinations such as royal college membership examinations/higher degrees.
Cost
Doctors were asked how much money (excluding that of teaching allowances) and days of annual leave they used on the above activities. They were also asked how many of their allowed ‘specialty taster days’ they had taken during each year.
Motivating and deterring factors
Doctors were asked to rank from a list the motivating and deterring factors determining what activities they were undertaking.
Professional development
Doctors were finally asked to rank which educational activities they thought would make them a better overall Foundation doctor.
Results
Response rate was 49% with 49 doctors returning the questionnaire. Of these 69.4% (n=34) were Foundation Year 1 (FY1) and 30.6% (n=15) were Foundation Year 2 (FY2), with 53.1% female and 46.9% male.
Activities
Overall 89.8% (n=44) of respondents were engaged in voluntary educational activity (FY1 85.3%, FY2 100%). The most common mode (89.8%, n=44) was e-learning packages (FY1 85.3% (n=29), FY2 100% (n=15)) followed by joining/ becoming a member of professional bodies or societies ie BMA etc (73.5%, n=36) (FY1 64.7% (n=22), FY2 93.3% (n=14)), followed by courses (69.4%, n=34) (FY1 55.9% (n=19), FY2 100% (n=15)), undertaking higher qualifications (36.7%) (FY1 14.7% (n=5), FY2 86.7% (n=13)) and attending conferences (14.3%) (FY1 14.7% (n=5), FY2 13.3% (n=2))– See figure 1.
Fig 1 – A graph to show the percentage of Foundation year 1 and 2 doctors involved in each mode of voluntary educational activity.
Of the courses attended, 25.5% pertained to teaching, 25.5% to advanced life support and 18.0% to surgical skills. The remaining 31% of courses related to a variety of other interests such as anaesthetic skill days, expedition medicine courses, and sub speciality specific courses such as movement disorder workshops and laparoscopic surgery.
Cost
The mean amount spent by Foundation Year 1 Doctors on these activities was £581 (range £0 - £3100) Foundation Year 2 Doctors spent significantly more at £1842 (range £0 - £3500). The mean cost per activity is shown in figure 2.
Fig 2 – A graph to show the mean amount of money spent by foundation year 1 and 2 doctors on each mode of
educational activity.
The mean number of days of annual leave used by doctors for these activities was 2.8 in FY1 and 5.3 in FY2, therefore combining to average 8.1 days in total that would be used over the whole foundation programme. Of their five allowed ‘taster – days’ the mean number attended was 1.3 and 2.9 by FY1 and FY2 doctors respectively. Only 20.4% of doctors took their full entitled allowance.
Motivating and deterring factors
The most common factor motivating Foundation doctors to undertake portfolio educational activities was the belief they would help candidates achieve a specialist training post (67.3%). Only 12.2% engaged primarily out of personal interest with 8.2% to improve their medical competence (See Table 1).
Primary Motivating Factor
FY1 Doctors
FY2 Doctors
Overall
Percentage (%)
Number
Percentage (%)
Number
Percentage (%)
Number
Improve chance of specialist training post
58.8
20
86.7
13
67.3
33
Personal interest
14.7
5
6.7
1
12.2
6
To improve medical competencies
11.8
4
0
0
8.2
4
On advice of seniors
11.8
4
6.7
1
10.2
5
Other
2.9
1
0
0
2
1
TOTAL
100
34
100
15
100
49
Table 1 – A table to show the primary motivating factors of foundation doctors to undertake voluntary portfolio educational activities.
The most common deterrents were a lack of study leave (42.9%), lack of annual leave (22.4%) and expense (20.4%) (See Table 2).
Primary Deterring Factor
FY1 Doctors
FY2 Doctors
Overall
Percentage (%)
Number
Percentage (%)
Number
Percentage (%)
Number
Lack of study leave
38.2
13
53.3
8
42.9
21
Lack of annual leave
23.5
8
20
3
22.4
11
Financial expense
17.6
6
26.7
4
20.4
10
Lack of career choice
11.8
4
0
0
8.2
4
Not relevant to Foundation doctors
8.8
3
0
0
6.1
3
Other
0
0
0
0
0
0
TOTAL
100
34
100
15
100
49
Table 2 – A table to show the primary deterring factors listed by foundation doctors that deter them from undertaking voluntary educational portfolio activities.
Professional development
The final section of the questionnaire asked respondents which educational activity they felt was most influential in making them a better Foundation doctor. Interestingly 83.7% (n=41)(FY1 88.2% (n=30), FY2 73.3%( n=11)) felt on-call experience was most influential, with only 6.1% (FY1 2.9% (n=1), FY2 13.3% (n=2)) citing courses, 6.1 % (FY1 2.9% (n=1), FY2 13.3% (n=2)) e-learning packages and 4.1% (FY1 2.9% (n=1), FY2 6.7% (n=1)) qualifications (Fig 3).
The academic conference was ranked least influential by 89.8% (n=44) (FY1 85.3% (n=29), FY2 100% (n=15)) of respondents, followed by 6.1% (n=3) (FY1 8.8% (n=3), FY2 0.0% (n=0)) citing courses, and 4.8% (FY1 5.8% (n=2), FY2 0.0% (n=0)) e-learning packages (Fig 3).
Fig 3 – The above graph was the response of Foundation doctors when asked which activities they thought were most and least influential in making them a better foundation doctor.
Discussion
This survey suggests that Foundation doctors undertake numerous activities at significant personal expense to expand their portfolios, and are primarily motivated by a belief that this will increase their chance of obtaining higher specialist training posts.
Educational activities and opportunities
The advent of the European Working Time Directive and New Deal document2 have resulted in junior doctors working considerably fewer hours than in previous years. This has led some authors to conclude that the quality of learning opportunities in the working environment has reduced 3 .With 89.8% of Foundation doctors in this survey actively undertaking some form of educational activity outside of work, this suggests that Foundation doctors may be going some way to re-dressing this balance. It may also come as a surprising yet reassuring figure to Foundation Programme educational supervisors who may be unaware of the education of their trainees outside of work.
We found the most popular mode of educational activity to be the e-learning package. E-learning is an effective and extensively employed method for both distance learning4 , and as an adjunct to “traditional” lecture-based techniques across several disciplines. It has also been shown to be a well received and practical method of supplementary education for doctors5 and our study suggests this is particularly true for the Foundation years. The reasons why e-learning is popular in this group was not explored, but its low cost, easily accessible and modular nature may have some part to play. As medical schools continue to utilise this modality to a greater extent, its follow-through into the Foundation years and postgraduate medical education in general is inevitable. With such high uptake, e-learning packages are a promising format for delivering education to this group.
Popular courses undertaken by Foundation doctors related to obtaining teaching skills, or advanced life support. This suggests that Foundation doctors place a high emphasis on teaching and training, and on recognising and managing acutely ill patients. These are two core objectives of the Foundation Programme. However, one could also argue that doctors undertaking courses outside work to achieve essential competencies casts doubt on the ability of the Foundation Programme to deliver them. We submit that educational supervisors are in a prime position to appraise this issue.
The least popular mode of activity in our survey was the attendance of a medical conference. It was also regarded as least influential by 89.7% of respondents. There is a global shortage of medical academics6, and as conferences serve to introduce junior doctors to academic medicine and research, perhaps academic doctors should take a more prominent role in promoting conferences as an educational activity.
Time and money
Doctors incur the majority of their costs attending courses with Foundation Year 1 and 2 doctors spending £365 and £1120 respectively on this area (fig 2). This highlights the possibility that Foundation doctors may be prone to financial exploitation by a growing number of courses which are often unvalidated. As senior advice was the primary motivating factor for only 10.2% of activities, this suggests that educational supervisors could play a greater role in assessing, appraising and advising their trainees on the courses best suited for them and their professional development.
The overall financial cost incurred for all portfolio educational activities was £581 for FY1 and £1842 for FY2. Whilst previous estimates have been made in this area, this is the first specific to the Foundation Programme and to include non-mandatory outlay, and represents 3 % and 7% of the basic salary for FY1 and FY2 doctors before tax. As our survey found financial expense to be a significant deterrent to portfolio activity (20.4% of respondents), a potentially serious implication is that expense will limit the uptake of postgraduate education in the future. From the authors’ own experience such professional costs are not explained to medical students and that this issue merits more attention in undergraduate education.
A lack of study leave was highlighted as the main deterring factors to educational portfolio activities (42.9%). This is of particular interest as only 20.4% of Foundation doctors use their full ‘taster-day’ entitlement. These ‘taster days’ are a fundamental aspect of the Foundation Programme, offering doctors the opportunity to explore a specialty for up to five days per year. However, whilst doctors fail to utilise them, they take an average of 8.1 days’ annual leave over the two year programme for educational purposes.
The reasons behind this are unclear, but may be due to a lack of awareness of these ‘taster days’. With a lack of study leave hindering educational activities, a potential solution might be for doctors to have the option to utilise ‘taster days’ as a form of study leave.
Professional education and motivation
Between 1998 and 2005, the number of medical students in the UK has risen by 57%7. Increasing numbers of doctors and decreasing working hours may reduce the amount of on-call experience for those in the Foundation Programme. However, it is this on-call experience that is regarded by the vast majority (83.7% in this study) as the most important educational modality in making them a better foundation doctor. Although time and money are perceived as barriers to portfolio educational activities it appears that doctors value this on-call experience above all. With key aims of the Foundation Programme being training and emergency competence, efforts must be made to preserve this experience.
Whilst Foundation doctors are engaging in numerous portfolio activities, their underlying motivations are interesting. It appears this group are primarily motivated not by the educational benefits of these activities, but rather by their perceived ability to help attain a specialist training post. This could suggest that the educational portfolio is at risk of becoming a ‘tick-box’ means for career progression, rather than addressing limitations, exploring interests and aspiring to clinical excellence. This contrasts with the conclusions of the most recent assessment of postgraduate medical education in the UK8.
As competition for jobs appears to be driving Foundation doctors to undertake educational activities it remains unclear whether engaging in these activities to obtain jobs, rather than competencies, reduces their validity and educational outcomes. Furthermore it is unclear whether trainees will be more likely to achieve their overriding aim of obtaining a specialist training post through these activities. Determining the career outcomes of doctors undertaking these activities will provide an evidence base, allowing educational supervisors to optimally advise their trainee in portfolio educational activities.
Conclusions
This is a baseline survey quantifying portfolio educational activities in the Foundation Programme, applicable to trainees and supervisors alike. Whilst the latter are well aware of assessments such as DOPS (Direct Observation of Procedural Skills) and CbD’s (Case-based Discussions), they are often less aware of the voluntary educational activities of their trainees.
Our study would suggest that Foundation Programme doctors are a cohort driven to undertake numerous voluntary educational activities, albeit largely to achieve career progression rather than accrue educational benefit. To this end they undertake activities such as e-learning, courses and higher qualifications at the expense of conferences. For this they spend significant amounts of money and leave, yet continue to site a lack of traditional study leave as a barrier to further educational development. The authors would suggest that further work is needed to develop the role of educational supervisors in the Foundation Programme in harnessing the motivation of their trainees, and guiding them appropriately.
Key Points
·Foundation Doctors spend significant amounts of time and money on voluntary educational activities.
·Foundation Doctors are primarily driven to undertake these activities due to the belief that it will help them obtain specialist training posts.
·A lack of study leave is the primary barrier to voluntary education.
·The academic medical conference is viewed as the activity least likely to improve medical competence, whereas on-call experience is regarded as the most likely.
·Foundation Programme educational supervisors are best placed to guide their trainees towards the most appropriate educational modalities
'The following article is another in a series of critical essays examining the current status of Psychiatry in the NHS'
In therapy
"Good advice is often a doubtful remedy but generally not dangerous since it has so little effect.’ Carl Jung (1875-1961)
The word ‘therapy’, as defined by the Oxford Dictionary as ‘to treat medically’, is derived from the Greek therapeuein, meaning to minister. Nowadays it can denote any treatment from massage therapy to music therapy. In mental health it has become synonymous with counselling or psychotherapy. Drug therapy, believe it or not, is included in the definition, though is frowned upon by many in the mental health industry, and is often the subject of derisory and ill-informed comments from both medical and non-medical practitioners. Many medical doctors who decide to embark on a career in psychotherapy generally forfeit all their knowledge of physiology, biochemistry, anatomy, pharmacology and many other subjects, in the pursuit of an ideal that somehow all life’s problems can be resolved through a particular brand of talking therapy. One wonders why they spend many years in medical school and in postgraduate teaching. Why devote all that time studying subjects, which have no relevance to common or garden psychotherapy? Would it not be more practical for those who specifically want to pursue such a career in psychotherapy to enrol in a psychotherapy training college, and then ‘specialise’ in whatever form of psychotherapy they aspire to? Such individuals, instead of wasting years training as medical doctors, could receive a diploma or certificate to practise psychotherapy. Likewise, you do not need to be a neurosurgeon to become a neuroscientist, or a physician to study virology. For some reason, however, scientists, including innovators in the fields of medicine and surgery, seem to be disparaged by both medical and non-medical psychotherapists, and seen as persons who can only conceptualise individuals as molecules, or objects to be examined with sophisticated machinery. Psychotherapy seems to induce a state of delusional intellectualism among some of its members, it would seem. Such intellectualism, if it be described as such, portrays an affected and misguided arrogance towards matters scientific. Yet curiously, published papers in mental health journals or in the press, when written by ‘experts’ are often interspersed with the words ‘science’ or ‘scientific’ even when they are little more than observations, studies, or comparisons between populations receiving a particular mode of this therapy or that therapy. We are not talking about advances in the treatment of neuroblastoma or other cancers here or a cure for dementia. It is one thing to describe Addison’s disease; it is another to discover the cause.
The panacea
‘Nice people are those who have nasty minds.’ Bertrand Russell (1872-1970)
The necessity for ‘therapy’ now seems to be deeply ingrained in our culture and the army of pop psychologists and psychiatrists, non-biological therapists, and agony aunts increases, it seems, by the day. In the media what is quoted as ‘research’ and passed off as science, is often no more than a street survey, or opinion poll on a current fad or passing headline grabber, rather like those ‘we asked a hundred people’ questions posed on popular family quiz shows. The therapy bandwagon rolls on and is quite lucrative if you are fortunate enough to capture the market with your own brand of snake oil cure to life’s woes. Admission is free to the Mind Industry and furthermore, there are no compulsory, nationally agreed standards for the conduct and competence of non-medical psychotherapists and counsellors. Even if removed from the membership of their professional body for inappropriate conduct say, therapists can continue to practise, there being no legal means to prevent them from doing so. Most members of the public are unaware of this lack of statutory regulation. It is not surprising then that many ‘therapists’ flagrantly sell their product and any attempt to question the authenticity of a particular ‘cure’ is met with vitriol and feigned disbelief. After all, one has to guard one’s source of income. The author Richard Dawkins was subject to such venom and hostility when he dared to question the reasons and need for religion in his book The God Delusion. Woe betide any practitioner who dares to criticise the favourable results of ‘carefully conducted positive outcome studies’ on, say, cognitive therapy, even when one’s own clinical experience attests to the opposite. Of course, some therapies work, some of the time, but not because of the outlandish claims made for them; rather, they work best when a ‘client’ harnesses the energy and motivation to get better and ‘chooses’ one brand of therapy over another, or feels at ease with a therapist who is empathic and understanding, much as one might confide in a best friend, rather than any inherent benefit from the ‘therapy’ itself. Certain therapies work because they have an intrinsic behavioural component to them, for example, dialectic therapy for ‘borderline personality’ disorder (as real a condition as ‘sociopathic’ disorder), or cognitive behaviour therapy for obsessive-compulsive disorder and phobic disorders. With other therapies one would almost have to admit feeling better given the enormous sums of money involved say, for a one-week course in a therapeutic healing centre. After all, it would be painful to admit an expensive holiday being a waste of time when a lot of hard-earned money has been spent.
The enemy within
‘Sorrow and silence are strong, and patient endurance is godlike.’ Henry W Longfellow (1807-1882)
Why does one who is vehemently opposed to psychiatry want to become a psychiatrist? Do as many medically qualified psychotherapists as non-medical therapists dismiss the role of biology in the causation of mental health disorders? Why do we speak of anti-psychiatrists and not anti-cardiologists? What about the claims for psychotherapy itself? Is it possible truthfully to scientifically evaluate whether or not it works? Criticism comes from within its own camp. To paraphrase one well-known psychologist, ‘Psychotherapy may be good for people, but I wish to question how far it changes them, and I strongly cast doubt on any assumption that it cures them’.1 The irony now is that the therapies themselves are being ‘dumbed down’, sometimes aimed at a younger audience to court popular appeal. Trite and stultifying sound bites such as ‘getting in touch with your feelings’, ‘it’s good to cry’, ‘promote your self-esteem’, ‘search for your inner child’, and many other inane phrases flourish. Failure to display distress or intense emotional turmoil outwardly (say, after a bereavement), is seen as weak, maladaptive, and abnormal, instead of being viewed as a strength, a mark of dignity, and an important way of coping. The corollary of course, is the spectacle of some psychiatrists, because of their medical training, endeavouring to explain every aspect of mental health psychopathology in terms of neurotransmitters and synapses. And then there is the scenario of non-medical ‘scientists’ critically evaluating and expounding on subjects completely outside their remit, for example, uttering pronouncements say, on the neuropharmacology of depression, or the reputed reduction in hippocampal volume caused by posttraumatic stress disorder, when they are not qualified to do so, having only a superficial knowledge of pharmacology and/or neuroimaging respectively. Instead of asking the engineer’s advice on the safety strength of a steel column supporting a bridge, why not ask the carpenter! The absurdity knows no bounds.
It seems that all life’s problems are self-inflicted or caused by ‘society’ or faulty upbringing. Back to the schizophrenogenic mother then. It is up to the client to seek the therapist’s help and advice by way of talking cures to set him/her on the road to recovery. To be fair to non-medical therapists and lay counsellors, some psychiatrists do not believe in the genetics of, or neurobiological contribution to, mental health. Some even believe mental illness to be a myth! Imagine an electrician who does not believe in electricity, or to compare like with like, an oncologist who does not believe in cancer. Many decades ago the psychiatrist Thomas Szasz described psychology as pseudoscience and psychiatry as pseudomedicine 2 .Since then others have reinforced Szasz's conclusions. Who can blame them? To illustrate by one example, many court cases (particularly in the forensic field) involve a psychiatrist/psychologist giving ‘expert’ testimony for the defence with the prosecution in turn calling for a psychiatrist/psychologist to offer a contradictory opinion on say, the defendant’s fitness to plead. The prosecution says the defendant is acting, the defence argues the defendant is suffering from a mental disorder. No surprises there as to why psychiatry has descended into farce.
Psychotherapy is all talk
‘There is no art to find the mind’s construction in the face.’ William Shakespeare (1564-1616)
One outspoken critic has had the courage, some might say the audacity, to assert that the psychology/psychiatry therapy hoax is still as widespread and dangerous as it was when the neurologist Sigmund Freud first invented what she describes as ‘the moneymaking scam of psychoanalysis.’ 3. Briefly, at the core of psychoanalysis lies the principle that the id, ego and superego (not originally Freud’s terms) are considered to be the forces underlying the roots of psychological turmoil. The id, or pleasure principle, is in conflict with the superego or conscience (the conscious part of the superego) and the resultant outcome is mediated by the ego. Any interference with this delicate balance results in symptoms. However, this simplistic theory has come in for much criticism over the years and many scholars now consider the claims of psychoanalysis as having little credibility. It is not philosophy and it is certainly not science. Research in this area is fraught with even more methodological problems than say, with cognitive therapy studies. There is no way of testing analysts’ reports or interpretations reliably, and their conclusions are speculative and subjective. One eminent psychotherapist pronounced ‘as far as psychoanalysis is concerned, the logistical problems of mounting a full-scale outcome study are probably insurmountable.’4 It is impossible to develop a truly valid research protocol in either cognitive or psychoanalytic treatments to account for all the subtle, different variables that make individuals so unique. How can one research the mind? There are no specific blood tests and brain investigations that diagnose mental illness in the same way one might diagnose neuroleptic malignant syndrome or Parkinson’s disease respectively, at least not yet. Measuring scales are a very crude way of conducting research into mental health, and are not always objective, particularly when researchers are keen to have a favourable result. This applies also to drug trials, I hasten to add.
Many people feel better simply by seeing and discussing their troubles with a friend, their physician, a member of the clergy, or their next-door neighbour for that matter. Such individuals are usually more than prepared to give considerable time to listening sympathetically and offering possible solutions to often intricate and personal problems. Nonetheless, talking about a negative experience or trauma does not necessarily alleviate the distress or pain felt by that event. One wonders then why a ‘client’ would be expected to get better simply by insisting changing his/her ‘negative set’, for instance, by doing homework exercises for the teacher/therapist. No doubt countless individuals move in and out of therapy and support groups; some may even benefit from self-help books. However, it is the earnest fatuity in such books that is so tragically funny, and that people take them so seriously is even more worrying.5 Some ‘clients’ find therapy a waste of time, but since they do not return for their follow-up sessions it is assumed they are well, or have moved on, or are simply unsuitable. On the other hand, there are countless individuals who find an inner resilience to withstand and improve themselves through their own volition, with a few prompts on the way, rather like finding one’s way through unfamiliar territory with the aid of a street map. Likewise, drug treatment is of very little value if one’s relationships are in disarray, or an individual is in great debt, for instance. The ‘worried well’ simply require practical help from appropriate advisors, not health care professionals and should they wish to spend money on counsellors and therapists, that is for them to decide.
Common sense and nonsense
‘He who exercises his reason and cultivates it seems to be both in the best state of mind and dear to the gods.’ Aristotle (384 -322 BC)
We have now reached a point where minor setbacks and irritations are seen as obstacles to be treated. By adopting this attitude we are succumbing to the might of the Therapies and Mind Industry, eliminating those experiences that define what it is to be human. Individuals freed from moral duty are now patients or victims. This abnegation, abdication and suffocation of individual responsibility for the sake of self-esteem is creating a society which needs only to be placated and made content.3 Anything that causes dismay or alarm is a trauma, and therefore needs therapy. Any crime or misdemeanour is not our fault. We have a psychological condition that absolves us from every sin or ailment. The opposite scenario is whether through scientific ignorance or a refusal to acknowledge that the human genome may play a part, perhaps both, some therapists accuse organic theorists of being ‘too ready’ to favour biological models, believing that dysfunctions in neuronal circuits have no part to play in ‘disorders of the psyche’. We are not all at the mercy of our neurotransmitters, they cry. Neither view is accurate. Psychoanalytic psychotherapy is no exception either. The nub of psychoanalysis is the therapist’s analysis of transference and resistance, which distinguishes this form of psychotherapy from all other types. With this brand of therapy absurd interpretations abound, leading one psychotherapist to openly admit that ‘jargon is often used to lend a spurious air of profundity to utterances which are nothing of the kind’.6 The author Frederick Crews writes: ‘I pause to wonder at the curious eagerness of some people to glorify Freud as the discoverer of vague general truths about human deviousness. It is hard to dispute any of these statements about “humans”, but it is also hard to see why they couldn't be credited as easily to Shakespeare, Dostoevsky, or Nietzsche - if not indeed to Jesus or Saint Paul - as to Freud’.7
One particular concept that is difficult to sustain is that repressed memories of traumatic events lead to psychiatric disorders. That such repressed memories in some instances encompass sexual preferences towards one or other parent, is even more perplexing to most people. The Oedipus and Electra complexes, expounded by Freud and Jung respectively, were founded on Greek mythology, hardly the basis for scientific study. Psychoanalysis set out to cure a disorder by uncovering repressed memories. However, traumatic memories by their very nature are actually difficult to ‘repress’. Of course individuals do forget. This is a normal part of the human condition. Memories are recollected or resurrected by association of ideas; multiple-choice format questionnaires work on the same principle. Familiar sights, smells and sounds, as famously depicted in Marcel Proust’s A La Recherché de Temps Perdu (‘and suddenly the memory revealed itself. The taste was that of the little piece of madeleine cake‘) often conjure up previously ‘forgotten’ memories, what used to be described as involuntary memory. Forgetting does not always equate with psychopathology; forgetfulness is common and becomes more common with age. In psychiatric treatment electroconvulsive therapy (ECT) is associated with a high prevalence of memory disturbances, often irreparable. With organic disorders, memory channels or traces are damaged, for example, through alcohol, or subcortical injury.8 However, even in Alzheimer’s disease, at least in the early stages, memories are often not totally erased, a fact utilised in reminiscence therapy. Memories in healthy people are not suppressed or repressed. Not wanting to talk about some painful issue is not necessarily ‘denial’, nor does it denote a fear of unleashing repressed/suppressed memories.
After the Trauma
‘We seldom confide in those who are better than ourselves.’ Albert Camus(1913-1960)
Mental health care workers often speak of posttraumatic stress disorder where memories of an especially overwhelming and upsetting event are ever-present and particularly distressing, leading to panic feelings, flashbacks, and recurrent nightmares. Such memories may be easily evoked, sometimes merely by watching a documentary, reading a news item, listening to a radio programme, and so forth. In other words, patients are all too quickly reminded of them - the memories are very vivid, not repressed. Often people simply do not want to be reminded. They are not in denial – they are simply avoiding the issue and should be allowed to do so. Whereas formerly such traumas were associated with catastrophic events such as the Holocaust or major natural disasters, nowadays the term posttraumatic has become over-inclusive. Some people have ‘trauma’ imposed on them in the form of invidious suggestions that they were subject to abuse of one form of another. On the contrary, there is no evidence that any of Freud’s patients who came to him without memories of abuse had ever suffered from sexual abuse. Furthermore, Freud ensured that his theory of repression could not be easily tested, and in practice the theory became ‘unfalsifiable’.9 Traumatic memories of abuse are very difficult to forget, and patients struggle to suppress them, in the author’s experience.
Undoubtedly, some memories are painful, and generally speaking, there are individuals who want to ‘forget the past’ in order to ‘move on’, which would strike most of us as being a reasonably healthy approach in certain circumstances. Many patients, for instance, would want to ‘move on’ to a healthier, more satisfying relationship, change job, alter their lifestyles, and so forth. When it comes to major catastrophic events, memories are not preconscious or unconscious: they are very often disturbingly real, and very difficult to live with; in many cases time is the only ‘healer’. Some traumatic memories never fade and in many cases no amount of talking will erase the painful memories. Witness the Holocaust survivors and those subject to horrendous atrocities throughout the Pol Pot regime, for example.
It is difficult to ascertain therefore whether so-called defence mechanisms such as repression or denial are truly separate entities operating in the human psyche, or merely part of a conscious natural survival instinct to ward off painful stimuli. How can such mechanisms be unconscious when it is commonplace to hear of people ironically talking about ‘being in denial’? Individuals who attempt to overcome their own addictions for example, are seen as suffering from a ‘perfectionist complex’, and reluctant to admit their failings. In other words, acknowledge you are unable to cope and are in denial about the true nature of your affliction and you will then be offered a place in the recovery programme.5 Therapists see denial as a mechanism deployed to avoid the pain of acknowledging a problem and taking action to seek help. It is not medical bodies but grass roots campaigners who are foremost in demanding that every ‘traumatic’ or ‘problematic’ condition be medicalised, creating more opportunities for counselling intervention.10 Hence the new breed of disorders to include shyness, inattentiveness, road rage, trolley rage, sex addiction, shopping addiction, internet addiction and so forth.
Beyond therapy
‘We are all born mad. Some remain so.’ Samuel Beckett (1906-1989)
Talking therapy is now the new religious cult and is what people have now turned to in order to find solace or answers (‘discover your real self’), and even cope with often inconsequential day-to-day events. The constant, pervasive emphasis on counselling diminishes the capacity of healthy people to confront commonplace problems they encounter in ordinary day life. Normal variants in behaviour are considered pathological and ‘psychologised’ or ‘medicalised’. Psychobabble prevails. We all need therapy or a pill. More and more ‘disorders’ are being invented. The endless proliferation and demand for ‘expertise’ in all areas of life is eroding the willingness of those who are best positioned to offer at least measured advice, accumulated from years of experience. There are no ‘experts in living’ and some individuals need to steer away from their excessive dependency and seeking self-approval of others who claim to be. Kierkegaard once wrote of people ‘taking refuge in a depersonalized realm of ideas and doctrines rather than confronting the fact that everyone is accountable to himself for his life, character and outlook’.11 In the words of John Stuart Mill, ‘Ask yourself whether you are happy, and you cease to be so.’
Headaches associated with or occurring around sexual activity have been recognized since the time of Hippocrates [1, 2]. Wolff [3] discussed headache during sexual activity in 1963. However, these headaches started to be formally reported in the 1970s, first by Kitz in 1970 [4] and then Paulson [5] and Martin [6] in 1974. The first published study was by Lance in 1976 [7].
Classification
This type of headache has been given many different names: benign sex headache (BSH), benign coital headache, coital cephalgia, orgasmic cephalgia, primary headache associated with sexual activity (PHSA), coital ‘thunderclap’ headache, primary thunderclap headache (PTH), orgasmic headache (OH) and preorgasmic headache.
In 2004the International Headache Society [8] classified HSA as a distinct form of primary headache.
These benign HSA are bilateral headaches, precipitated by sexual excitement (masturbation or coitus) occurring in the absence of any intracranial disorder and which can be prevented or eased by ceasing activity before orgasm. Type 1 consists of a bilateral, usually occipital, pressure-like headache that gradually increases with mounting sexual excitement. Type 2 headaches have an explosive, throbbing quality and appear just before or at the moment of orgasm. These often start occipitally but may generalize rapidly [9].
However, there are individuals who experience patterns of HSA that do not fall within the classifications and are included as a subgroup of HSA with unusual psychopathology [10]. For example, Paulson and Klawans [5] described a rare type postural sexual headache after coitus, which is present on standing, eased by lying, accompanied by a low CSF pressure, and persists for several weeks.
International Headache Society diagnostic criteria - ICHD-2(7) classification for HSA
4.4 Primary headache associated with sexual activity
4.4.1 Pre-orgasmic headache
A. Dull ache in the head and neck associated with awareness of neck and/or jaw muscle contraction
and fulfilling criterion B.
B. Occurs during sexual activity and increases with sexual excitement
C. Not attributed to another disorder
4.4.2 Orgasmic headache
A. Sudden severe (“explosive”) headache fulfilling criteria B
B. Occurs at orgasm
C. Not attributed to another disorder
7 Secondary headache disorder
7.2.3 Headache attributed to spontaneous (or idiopathic) low CSF pressure
Prevalence
HSA are not common but it is generally felt that they are under-reported due to patient embarrassment [1] at telling health professionals when their headaches occur. Prevalence in the general population is reported at around 1% [11, 12] and is greater in men than in women, by 3-4 times [11, 13-16]. There appear to be two peak times of onset: in the early 20s and then around age 40 [17]. About 22% of HSA are Type 1 and 78% are Type 2 [18]. The male:female ratio is the same for Type 1 and Type 2 headache.
Pathophysiology
HSA are not clearly understood but by definition lack serious underlying disease. They are however, unpleasant, frightening, repetitive and episodic. The clinical characteristics of Type 1 suggest a relationship with tension/muscular contraction headaches [2, 13, 15, 16]. There is a significant association between the risk of having more than one cluster of HSA and the presence of tension headaches or migraine [11, 14-17, 19-21]. Biehl [11] concluded that the association between migraine and HSA is bilateral. The prevalence of migraine in HSA patients is 25-47% [15, 16, 20]. Ostergaard [14] showed that the presence of concomitant migraine or tension headache was significantly associated with the recurrence of periods lasting weeks to months in which HSA occurred. Patients without another primary headache often have only one HSA period or episode and a more favourable prognosis . Migraine is co-morbid in 30% of Type 2 as opposed to 9% with Type 1. Co-morbidity is also seen in exertional headaches, 35% of Type 2 and 9% Type 1[17, 18]. There can be simultaneous onset of benign exertional headache (BEH) and HSA [22] as well as HSA after a history of BEH [16, 22].
Several drugs have been linked in case reports to sexual headaches associated with neurologic symptoms: Amiodarone [23], birth control pills [24], pseudoephedrine [7] and cannabis [25].An interesting more recent addition to HSA is that resulting from the use of PDE5 medication to assist in erectile difficulties [26, 27].
In type 2 headaches, increased intracranial pressure secondary to a Valsalva maneuver during orgasm has been proposed as a possible mechanism. Blood pressure may increase by 40-100mmHg systolic and 20-50mmHg diastolic during orgasm [7, 28-30]. A possible disruption of autoregulation of the cerebral vasculature has also been proposed [31-33].
Classic presentation
A male patient, middle-aged, in poor physical shape, mildly to moderately overweight, and mildly to moderately hypertensive [34]. In women muscle contraction and psychological factors are often involved [34].
The typical story is that the headache occurs during sexual activity, is bilateral and stops or is less severe if sexual activity stops prior to orgasm. The duration varies from 5 minutes to 2 hours if sexual activity stops and from 3 minutes to 4 hours, with the possibility of milder symptoms up to 48hours, if activity continues.
Differential diagnosis
With the first episode it is absolutely mandatory to exclude potentially life threatening and disabling causes. A thorough history and neurological examination with the option of imaging studies and CSF examination must be conducted.
Type 2 explosive “thunderclap” headaches can be secondary to subarachnoid haemorrhage, aneurysms without obvious rupture, intracerebral haemorrhage, pituitary apoplexy, venous sinus thrombosis, cervical artery dissection, subdural haematoma, haemorrhage into an intracranial neoplasm [35], cerebral tumour [36], intracranial hypotension and hypertension, significant cervical spine disease, and ischaemic stroke [37-43] and these serious conditions need to be excluded before an HSA diagnosis can be given. HSA may present similarly to paroxysmal headaches caused by phaeochromocytoma [44].
Sexual intercourse is reported as a precipitating cause of subarachnoid haemorrhage in 3.8% to 12% of patients with bleeding from a ruptured aneurysm [35].
Course of the disease
The unpredictable clinical course falls into 2 temporal patterns: an episodic course with remitting bouts, and a chronic course [20]. In most cases the headaches occur in bouts that recur over periods of weeks to months before resolving [16, 45].
The episodic type is defined as a bout of at least 2 attacks occurring in ≥ 50% of sexual activity followed by no attack for ≥ 4 weeks despite continuing sexual activity. The chronic course is defined as ongoing HSA attacks for ≥ 12 months without remission of ≥ 4 weeks [20].
Further uncertainty is experienced by the patient as HSA does not necessarily occur in every sexual encounter [7, 19]. A characteristic of HSA is the sporadic vulnerability of patients to the headache. Episodes can occur singly, in clusters or at irregular intervals. Recurrence can occur years later.
The acute HSA attacks are usually short lasting but the overall duration of pain can vary widely [17]. The mean duration of severe pain in HSA is similar (30 minutes) in type 1 and type 2 but the mean duration of milder pain is more prolonged with type 2 (4 hours vs 1 hour). About 15% of patients suffer from severe pain for >4hours needing acute treatment. Severe pain continuing for 2-24 hours occurs in up to 25% of patients with HSA [17]. Patients with episodic HSA compared to chronic HSA have an earlier age at onset and tend to suffer more often from concomitant BEH [20].
About 30% of patients report headaches with masturbation as well as intercourse. There are also reports of HSA occurring exclusively during masturbation [46, 47] and a case of this occurring with nocturnal emission [21].
Overall HSA occurs more commonly when the patient is tired, under stress or attempting intercourse for the second or third time in close succession [48]. HSA appears in bouts lasting weeks to months and can disappear without specific treatment [14, 16]. The number of attacks within one bout ranges from 2 to 50 [17]. About 25% of patients suffer attacks without longer remissions.
Prognosis
Prognosis is usually good for HSA as it is a benign self- limiting disorder and disappears without any specific treatment in the majority of patients [17]. It is usually better if there has been only one attack, especially if it was not associated with any other type of headache.
Frese [20] concluded that episodic HSA occurs in approximately 75% and chronic HSA in approximately 25% of patients. However even in chronic HSA, the prognosis is favourable, with remission rates of 69% in patients followed over 3 years.
Management
A thorough history and examination is mandatory in a first attack.
Referral is warranted if:
Atypical story and suspicious examination
First episode of severe headache where headache still present
A recurrent episode of severe headache with longer than average duration
Neck stiffness, photophobia or vomiting
Altered consciousness or confusion
Focal neurological signs
Previous history of AV malformation, neoplasms or neurosurgery
Investigations
Computed tomography
MRI
Lumbar puncture
Cerebral angiography
Urinary catecholamine
Medical treatment
Turner [49] has provided a good review.
Pre-emptive treatment
Propanolol hydrochloride ( Inderal) is effective in the prophylaxis of HSA[19]. Naratriptan 2.5mg has been reported as useful prior to sexual activity [50] but due to lower absorption rates needs to be taken more than 60 minutes before sexual activity [30]. Indomethacin 25-100mg can be taken 30-60 minutes prior to sexual activity [15, 16, 45, 51] and for acute severe pain management [20] but can cause serious gastrointestinal side-effects and is not tolerated by about 10% of headache patients [52].
Acute treatment
Triptans shorten the attack in about 50% of patients[30]. There is an 80% response rate [30]. Analgesics (ibuprofen, diclofenac, paracetamol, acetylsalicylic acid) given after onset of headache are of limited or no value in nearly all patients [45].
Other triptans, ergots and benzodiazepines have also been reported to have efficacy [5, 24, 53, 54] for acute and pre-emptive treatment for those patients not tolerating indomethacin. Taken 30 minutes before sexual activity they shorten orgasmic headache attacks in 66% of users [30].
Long term prophylaxis for longer lasting bouts or continued attacks
Options include indomethacin 25mg three times a day, propanolol 120-240mg per day, metoprolol 100-200 mg per day and diltiazem 180 mg per day [15, 19, 20, 22, 24, 45]. There is about an 80% response rate [30].
Sexual management
Trauma due to pain associated with sexual activity has the potential to affect immediate and long term satisfaction with sexual activity unless specifically addressed. HSA can be very distressing for both patient and partner with the development of fears around sexual activity and orgasm. Patients may develop patterns of impaired sexual arousal. If these fears are not exposed and dealt with, sexual problems may occur. Secondary avoidance behaviours may become established in the relationship leading to a decrease in couple’s physical affection, eroticism and sexual activity. Patients must be given the opportunity to talk about sexual fears in an ongoing way, especially if HSA is chronic.
The social and relationship history will disclose areas of stress which should be evaluated and managed as best possible. In type 1 HSA where neck and jaw tension may be a factor, conscious relaxation of these muscles during intercourse may help [7]. Relaxation exercises especially concentrating on neck and shoulder tension can be done regularly and particularly before anticipating sexual activity.
Individuals often sense early in the lovemaking process whether or not HSA will occur and encouragement not to pursue orgasm on that occasion can be helpful. Some patients can terminate the headache by stopping the sexual activity or suppressing orgasm and about 51% can lessen the intensity of pain by being more sexually passive [18].
Advice on continuing to engage with the partner despite ceasing or modifying one’s own sexual arousal needs to be given. Having a disappointed or resentful partner increases the distress of the condition so partner needs have to be discussed. Patients often have difficulty talking about sexual issues with both their partner and their doctor, therefore the doctor needs to be the one to raise the subject.
A brief sexual history will outline the love-making practice and modification to sexual positions, especially where neck tension is exaggerated, may help. In one report, the advice to engage in intercourse more frequently but less strenuously resulted in a reduction in headaches [5].
Avoiding sexual activity and strenuous activities until totally symptom free has been recommended by some [13, 22, 24, 55]. This may be difficult to follow as the capricious nature of HSA makes knowing when they have stopped difficult.
Conclusion
HSA are benign, but because they can mimic serious conditions, patients need to be properly assessed before reassurance is given and management of HSA started. Because pain can alter sexual experience and behaviour around sexuality for the patient and the couple, this aspect of patient wellbeing must be addressed by the treating physician for good holistic management. As not everyone is comfortable with addressing sexuality with patients, respectful acknowledgement of the situation and appropriate referral can be a useful approach.




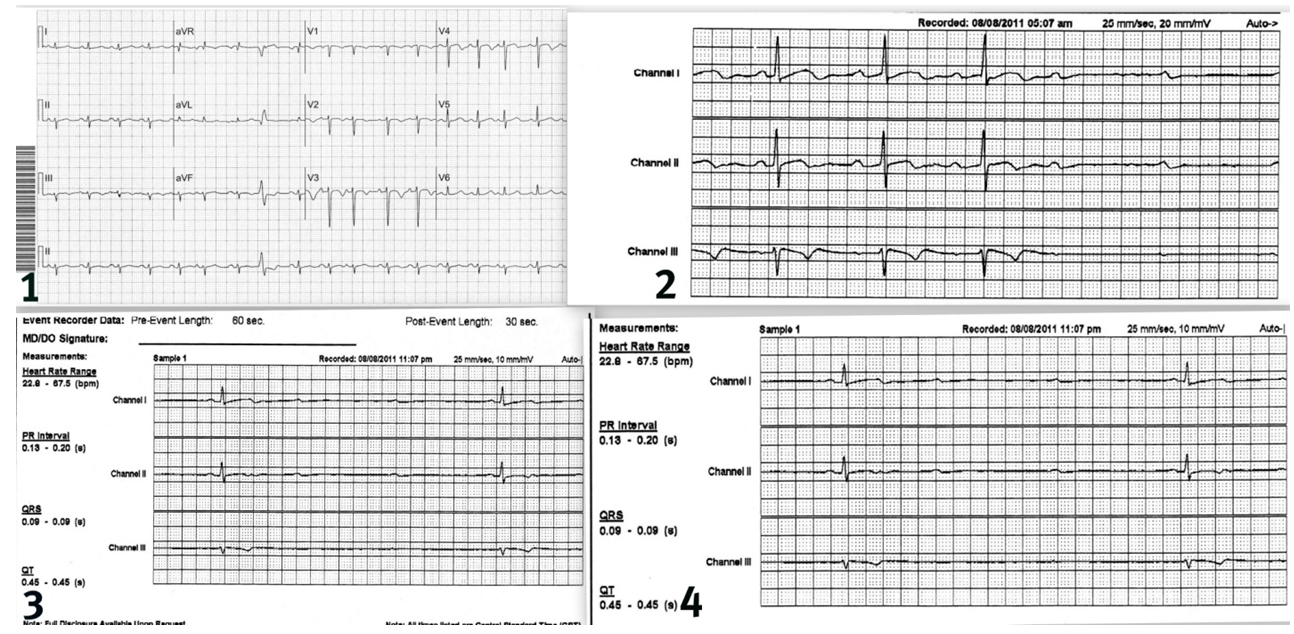
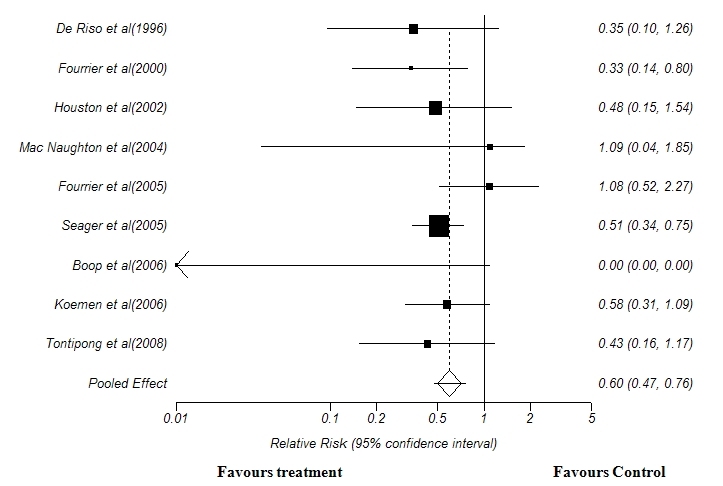
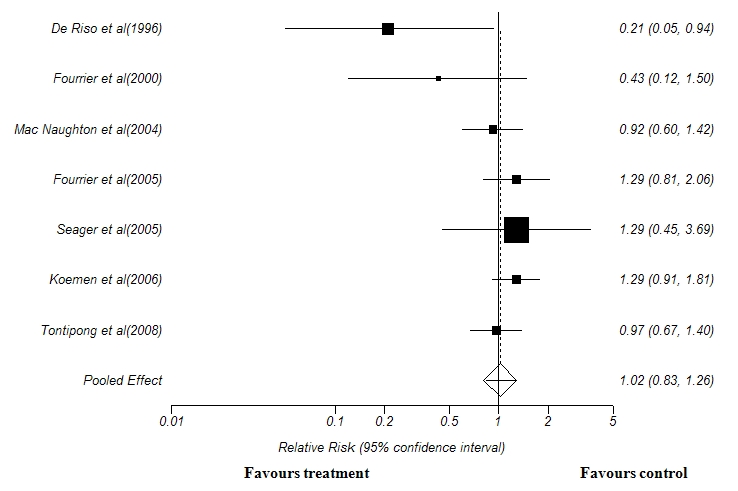
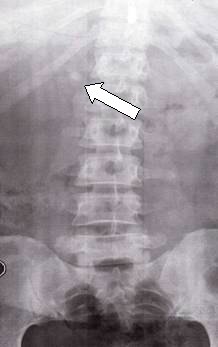

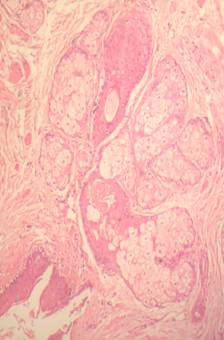
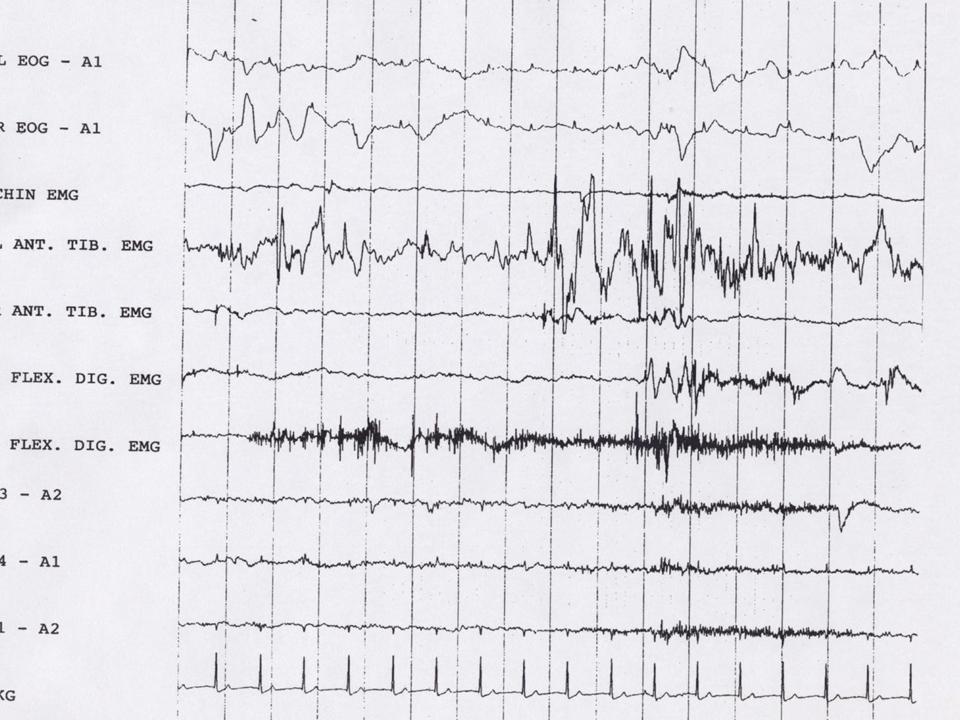
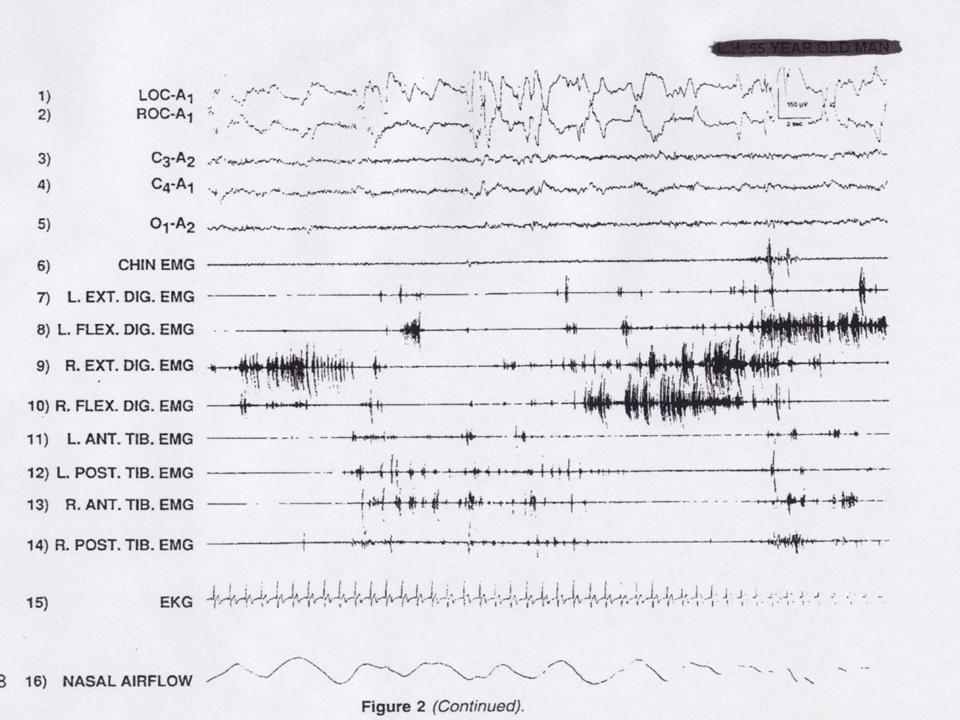
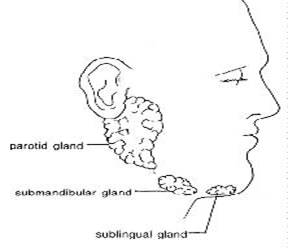


.jpg)

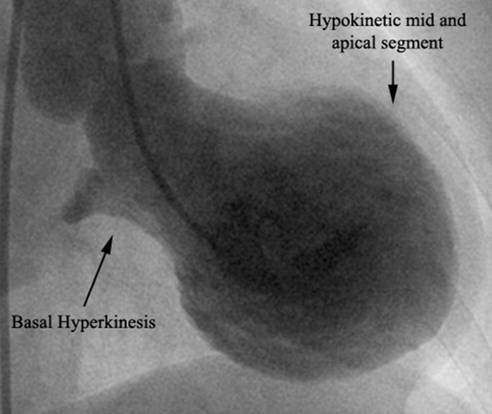

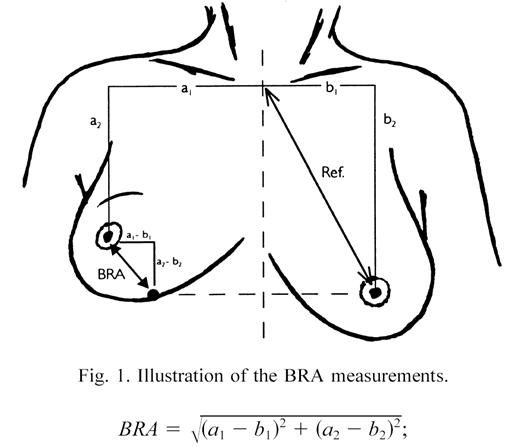
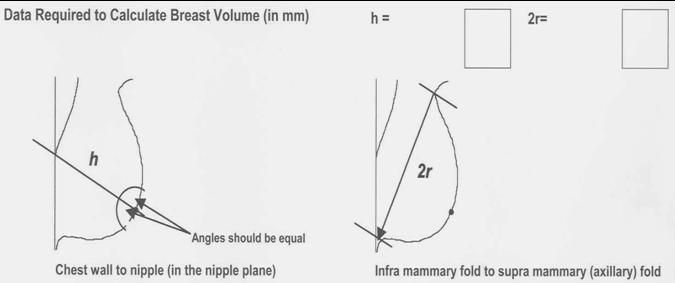

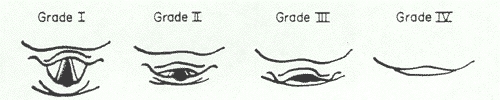
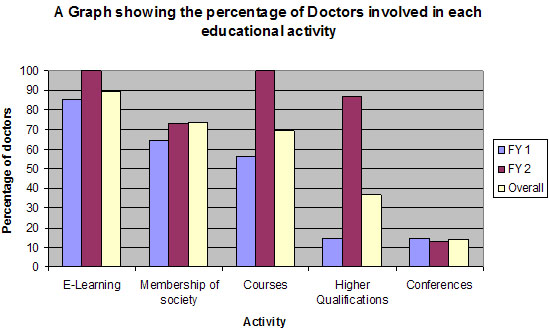
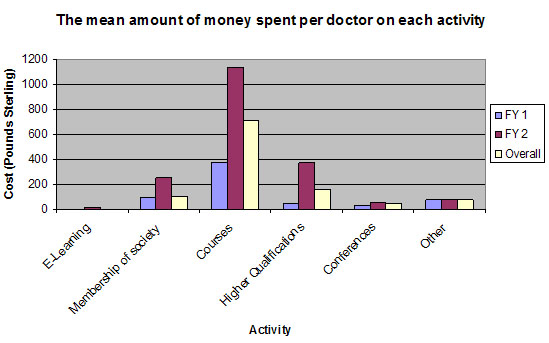
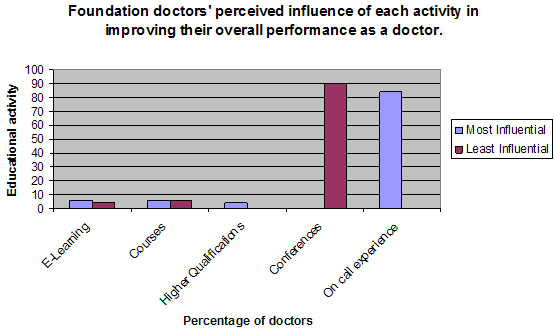
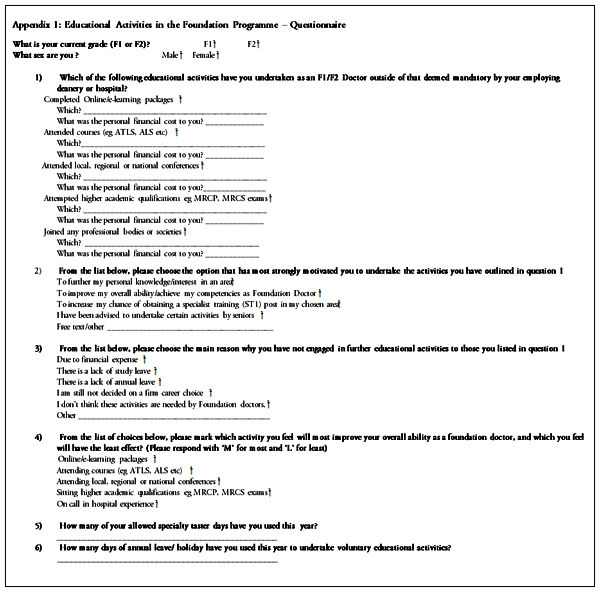
BJMP March 2012 Volume 5 Number 1
BJMP March 2012 Volume 5 Number 1
Editorial
Yili Zhou and Bohdan Warycha
Research Articles
E Balamurugan, A Kanimozhi and Govinda Kumari
Asif Mahmood, Mohammed Auldin and Asquad Sultan
A S Eid, V Burrows, J R M Murray, P Smitham, R Ahmad, R Miller and U Butt
Murali Krishna and Sreedharan Amarjothi
Review Articles
Umesh Vyas and Rose Franco
Ganesh Bavikatte, Poh Lin Sit and Ali Hassoon
Tauseef Mehdi
Case Reports/Series
Amitasha Mann, Jean Karen Fleischman and Karen Mrejen-Shakin
Sadaqat Ali Khan, Tariq Mahmood, Muhammad Zeeshan Sarwar, Syed Hamad Rasool, Muhammad Danish Siddique and Zohaib Khan
Hakim Irfan Showkat, Arif Hussain Sarmast, Rubina Lone, Mehmood Iqbal Qadri and Manzoor Ahmed Wani
Clinical Practice
Rajiv Malhotra and Sara Kelly