BJMP 2009:2(2) 4-5
Obesity and Pulmonary Hypertension. What’s the Link?
Roop Kaw.
In the second paragraph of the left column on page 5, the second sentence must have read
"The most direct evidence comes from observations that treatment of OSA with continious positive airway pressure (CPAP) may lower daytime PAP"
BJMP 2009:2(1) 38 - 40
The ‘Lost’ Mirena: What Investigations Are Required ? An Intraperitoneal Levonorgestrel-Releasing Intrauterine System Following Uterine Perforation: Case Report
Shambhu S and Pappas M
The correct name of the author must have read Pappas A on pages 4,39, 41
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the heart, lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In the previous two editions of pictorial essay, we have discussed the normal and abnormal positions of tracheal tube, nasogastric tube and central venous catheters on chest radiographs. In this edition, we shall look into permanent pacemakers and oesophageal Doppler probe on chest radiographs. PERMANENT PACEMAKERS A permanent pacemaker (artificial pacemaker) is a small battery powered medical device that is placed subcutaneously in the chest or abdomen to help control abnormal heart rhythms. They are inserted for different types of conduction problems (eg: sinus node disease, atrio-ventricular block, tachyarrhythmia etc). Permanent cardiac pacemakers consist of two parts:1. Pulse generator (power unit) – usually felt like a “bar of soap” beneath the skin and2. Pacing electrode leads The pulse generator consists of an energy source (battery) and all electrical circuits necessary for pacing and sensory function. The electrode is the exposed metal tip in contact with the myocardium. The electrode is connected to the pulse generator via an insulated wire (lead). Details regarding classification and functioning of a pacemaker is beyond the scope of this article and can be found in any standard cardiology text book. We shall now discuss what to look for in a chest radiograph in a patient with permanent cardiac pacemaker. Chest radiograph is one of the important diagnostic tools used in the evaluation of a patient with a pacemaker. However, it is not complete by itself and in addition to reviewing chest radiographs, it is important to take a detailed history from the patient, do a thorough examination of the patient, review all necessary case notes and analyse the ECG. If required, a cardiology opinion should be sought. Important points to note on a chest radiograph are: Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3. Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835). Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values. Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
First of all, check whether you are looking at the correct chest radiograph (not another patient’s chest radiograph)Identify the pulse generatorIdentify whether it is a single chamber, dual chamber or biventricular pacemaker. This can be done by counting the number and tracing the pacing leads to the cardiac chamber it is implantedCheck that the pacing leads are not dislodgedCheck that the pacemaker leads are intact and not brokenFinally, look for any abnormal shadowing behind the pacemaker as these can be easily missed1
CONCLUSION Valuable information can thus be obtained on reviewing chest radiographs. Our aim is to provide a quick overview on what to look for in pacemakers and oesophageal Doppler probe on chest radiographs. It is by no means an exhaustive description. This article is for the benefit of medical students, junior doctors in training, nurses and paramedical teams who would be involved in the care of critically ill patients. Self Assessment Multiple Choice questions (only one option is correct):1. The wires of permanent pacemakers are usually inserted viaA. Femoral veinB. Basilic veinC. Subclavian veinD. Subclavian artery 2. A chest radiograph is not useful in one of the followingA. To detect intact pacemaker wiresB. To indicate whether a pacemaker is working optimallyC. To detect whether pacemaker wires are dislodgedD. To identify a single chamber or dual chamber pacemaker Answers:1. C2. B
REFRESHER DAY ON OBSTETRIC ANAESTHESIA AND ANALGESIA
Contact: Obstetric Anaesthetists' Association Secretariat Tel: 011-44-20-8741-1311 Fax: 011-44-20-8741-0611 Email: available through webpage Website: www.oaa-anaes.ac.uk
Anesthesiology
October 07, 2009 United Kingdom / London
UPPER & LOWER LIMB PERIPHERAL NERVE BLOCK WORKSHOP
Contact: Aynsley Pix, B. Braun Medical Limited Email: aynsley.pix@bbraun.com Website: www.aesculap-academy.com
Anesthesiology / Pain Management
October 08, 2009 United Kingdom / Sheffield
2009 DIFFICULT AIRWAY SOCIETY ANNUAL MEETING
Contact: Anne Griffin, Abbey Conference & Corporate Tel: 011-353-1-648-6130 Fax: 011-353-1-648-6197 Email: das2009@abbey.ie Website: www.das2009.co.uk/cms/
Anesthesiology
November 04-06, 2009 United Kingdom / Perth
ASSOCIATION OF CARDIOTHORACIC ANAESTHETISTS AUTUMN MEETING 2009
Contact: Mrs. Andrea Reid, Secretary to Cardiac Anaesthetists Tel: 011-44-125-365-7789 Fax: 011-44-125-365-7134 Email: andrea.reid@bfwhospitals.nhs.uk Website: www.actablackpool2009.nhs.uk
Anesthesiology
November 05-06, 2009 United Kingdom / Blackpool
2009 THREE-DAY COURSE ON OBSTETRIC ANAESTHESIA AND ANALGESIA
Contact: Obstetric Anaesthetists' Association Secretariat Tel: 011-44-20-8741-1311 Fax: 011-44-20-8741-0611 Email: available through webpage Website: www.oaa-anaes.ac.uk
Anesthesiology
November 09-11, 2009 United Kingdom / London
GENERAL MEDICINE
DIABETES & ENDOCRINOLOGY: CLINICAL CHALLENGES & EXPERT ADVICE
Contact: Christine Berwick Tel: 011-44-131-247-3634 Fax: 011-44-131-220-4393 Email: c.berwick@rcpe.ac.uk Website: www.rcpe.ac.uk
Endocrinology / Family Medicine / General Medicine / Geriatrics / Internal Medicine
October 01, 2009 United Kingdom / Edinburgh
2ND NATIONAL CONFERENCE: ANXIETY & DEPRESSION
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Family Medicine / General Medicine / Psychiatry
October 01-02, 2009 United Kingdom / London
3RD ROYAL COLLEGE OF GENERAL PRACTITIONERS (RCGP) ANNUAL NATIONAL PRIMARY CARE CONFERENCE
Contact: Terri Myers, RCGP Tel: 011-44-20-7581-3232 Fax: 011-44-20-7225-3047 Email: courses@rcgp.org.uk Website: www.rcgpannualconference.org.uk
Family Medicine / General Medicine
November 05-07, 2009 United Kingdom / Glasgow
NEW CLINICAL SOLUTIONS IN DIABETES CARE CONFERENCE: OPPORTUNITIES & CHALLENGES
Contact: Alison Bone, Diabetes UK Tel: 011-44-1325-488-606 Email: alison.bone@diabetes.org.uk Website: www.diabetes.org.uk
Family Medicine / General Medicine
November 05, 2009 United Kingdom / York
INNOVATIONS AND PROGRESS IN HEALTHCARE FOR WOMEN
Contact: Confab Consulting, Conference Organisers Tel: 011-44-20-8906-7778 Fax: 011-44-20-8906-7790 Email: IPHW09@confab-consulting.co.uk Website: www.womenshealth.uk.com
Family Medicine / General Medicine / Obstetrics/Gynecology / Oncology
November 09-11, 2009 United Kingdom / London
GYNAE & OBSTETRICS
TRAINING THE TRAINERS
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
October 01-02, 2009 United Kingdom / London
POSTMENOPAUSAL HEALTH
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
October 12-13, 2009 United Kingdom / London
ADVANCED TECHNIQUES IN VAGINAL HYSTERECTOMY
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
October 15, 2009 United Kingdom / London
BASIC PRACTICAL SKILLS IN OBSTETRICS AND GYNAECOLOGY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
October 26-28, 2009 United Kingdom / London
ADVANCE LABOUR WARD PRACTICE
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
November 02-04, 2009 United Kingdom / London
BRITISH SOCIETY OF UROGYNAECOLOGY / ROYAL COLLEGE OF OBSTETRICIANS & GYNAECOLOGISTS JOINT MEETING
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
November 05-06, 2009 United Kingdom / London
MEDICAL COMPLICATIONS IN PREGNANCY
Contact: Symposium Office, Imperial College London Tel: 011-44-20-7594-2150 Fax: 011-44-20-7594-2155 Email: sympreg@imperial.ac.uk Website: www.prossl.com/symposiassl/events.asp
Obstetrics/Gynecology
November 11-13, 2009 United Kingdom / London
PROMPT (PRACTICAL OBSTETRICS MULTI-PROFESSIONAL TRAINING) COURSE: TRAINING THE TRAINERS
Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings
Obstetrics/Gynecology
November 12, 2009 United Kingdom / London
PROMPT (PRACTICAL OBSTETRICS MULTI-PROFESSIONAL TRAINING) COURSE: TRAINING THE TRAINERS
Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings
Obstetrics/Gynecology
November 13, 2009 United Kingdom / London
NEONATAL UPDATE 2009
Contact: Symposium Office, Imperial College London Tel: 011-44-20-7594-2150 Fax: 011-44-20-7594-2155 Email: sympreg@imperial.ac.uk Website: www.prossl.com/symposiassl/events.asp
Obstetrics/Gynecology
November 16-20, 2009 United Kingdom / London
QUALITY MANAGEMENT OF A FERTILITY SERVICE STUDY DAY 2009
Contact: British Fertility Society Tel: 011-44-14-5464-2217 Fax: 011-44-14-5464-2222 Email: bfs@bioscientifica.com Website: www.britishfertilitysociety.org.uk
Obstetrics/Gynecology / Other Specialties / Urology
November 17, 2009 United Kingdom / London
REPRODUCTIVE GENETICS
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
November 19, 2009 United Kingdom / London
LAPAROSCOPIC SURGERY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk/events Website: www.rcog.org.uk/events
Obstetrics/Gynecology / Surgery
December 02, 2009 United Kingdom / London
RECENT ADVANCES IN GYNAECOLOGICAL SURGERY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology / Surgery
December 03-04, 2009 United Kingdom / London
HANDS ON LAPAROSCOPIC HYSTERECTOMY WORKSHOP
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
December 03, 2009 United Kingdom / London
BASIC PRACTICAL SKILLS IN OBSTETRICS & GYNAECOLOGY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
December 07-09, 2009 United Kingdom / London
PAEDIATRICS
EUROPEAN SYMPOSIUM ON LATE COMPLICATIONS AFTER CHILDHOOD CANCER
Contact: Margaret Falconer, Event Co-ordinator Tel: 011-44-131-226-0821 Fax: 011-44-131-226-0801 Email: eslccc2009@colpitts.co.uk Website: www.eslccc2009.com
Oncology / Pediatrics
October 29-30, 2009 United Kingdom / Edinburgh
3RD NATIONAL CONFERENCE: PAEDIATRICS ASTHMA & ALLERGY
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Immunology/Allergy / Pediatrics
November 09-10, 2009 United Kingdom / London
PSYCHIATRY
2ND NATIONAL CONFERENCE: ANXIETY & DEPRESSION
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Family Medicine / General Medicine / Psychiatry
October 01-02, 2009 United Kingdom / London
DRUG TREATMENTS IN AFFECTIVE DISORDERS
Contact: Mrs. Susan Chandler, British Association for Psychopharmacology Tel: 011-44-1223-358-428 Email: susan@bap.org.uk Website: www.bap.org.uk
Psychiatry
October 08-09, 2009 United Kingdom / Manchester
DRUG TREATMENTS IN OLD AGE PSYCHIATRY
Contact: Mrs. Susan Chandler, British Association for Psychopharmacology Tel: 011-44-1223-358-428 Email: susan@bap.org.uk Website: www.bap.org.uk
Psychiatry
November 11-13, 2009 United Kingdom / London
BRITISH ASSOCIATION FOR PSYCHOPHARMACOLOGY (BAP) MASTERCLASSES IN CLINICAL PSYCHOPHARMACOLOGY
Contact: Lynne Harmer, BAP Tel: 011-44-1223-358-421 Email: lynne@bap.org.uk Website: www.bap.org.uk
Clinical Pharmacology / Psychiatry
November 11, 2009 United Kingdom / London
CAREIF 2009 INTERNATIONAL CONFERENCE*
Contact: Hampton Medical Conferences Tel: 011-44-20-8979-8300 Fax: 011-44-20-8979-6700 Email: careif@hmconline.co.uk Website: www.careif.ukevents.org
Other Specialties / Psychiatry
December 04, 2009 United Kingdom / London
7TH NATIONAL CONFERENCE: BIPOLAR DISORDERS
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Psychiatry
December 10, 2009 United Kingdom / London
SLEEP DISORDERS
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Psychiatry / Respirology
RADIOLOGY
ECHOCARDIOGRAPHY
Contact: Robina, Intensive Care Society Tel: 011-44-20-7280-4350 Email: events@ics.ac.uk Website: www.ics.ac.uk
Internal Medicine / Radiology/Imaging
September 04, 2009 United Kingdom / London
PET / CT COURSE
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
October 01, 2009 United Kingdom / Glasgow
WELSH BRANCH, BRITISH INSTITUTE OF RADIOLOGY, AUTUMN MEETING
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
October 16-17, 2009 United Kingdom / Llantrisant
OBESITY: THE CHALLENGES & SOLUTIONS IN IMAGING
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
October 19, 2009 United Kingdom / London
ROYAL COLLEGE OF RADIOLOGISTS BREAST GROUP MEETING*
Contact: Hampton Medical Conferences, Conference Manager Tel: 011-44-20-8979-8300 Fax: 011-44-20-8979-6700 Email: hmc@hamptonmedical.com Website: www.hamptonmedical.com
Radiology/Imaging
November 02, 2009 United Kingdom / Belfast
CONTROLLING RADIATION RISKS IN DIAGNOSTIC RADIOLOGY
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
November 24, 2009 United Kingdom / London
RPS UPDATE TRAINING SESSION
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
November 25, 2009 United Kingdom / London
BRITISH SOCIETY OF THORACIC IMAGING AUTUMN MEETING
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
November 27, 2009 United Kingdom / London
7TH ANNUAL CONFERENCE OF UK & IRELAND NEUROENDOCRINE TUMOUR SOCIETY (UKI NETS)
Contact: UKI NETS Secretariat Tel: 011-44-145-464-2277 Fax: 011-44-145-464-2222 Email: enquiries@ukinets.org Website: www.ukinets.org
Endocrinology / Gastroenterology / Oncology / Other Specialties / Pathology / Radiology/Imaging / Surgery
November 30, 2009 United Kingdom / London
SURGERY
2ND ANNUAL ROYAL MARSDEN BREAST CANCER MEETING: HOT TOPICS IN BREAST CANCER
Contact: The Royal Marsden Tel: 011-44-20-7808-2921 Fax: 011-44-20-7808-2334 Email: conferencecentre@rmh.nhs.uk Website: www.royalmarsden.nhs.uk
Oncology / Pathology / Radiology/Imaging / Surgery
October 02, 2009 United Kingdom / London
CURRENT CONCEPTS IN EXTERNAL FIXATION IN TRAUMA
Contact: Jean Fretwell Tel: 011-44-113-392-3819 Email: jean.fretwell@leedsth.nhs.uk Website: www.rcseng.ac.uk
Orthopedics / Surgery
October 05, 2009 United Kingdom / Leeds
ADVANCED TECHNIQUES IN VAGINAL HYSTERECTOMY
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
October 15, 2009 United Kingdom / London
CARE OF THE CRITICALLY ILL SURGICAL PATIENT INSTRUCTOR COURSE
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6311 Email: ccrisp@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Other Specialties / Surgery
October 26-27, 2009 United Kingdom / London
21ST CENTURY DECONTAMINATION: SHARING EXPERTISE
Contact: Aynsley Pix, B. Braun Medical Limited Email: aynsley.pix@bbraun.com Website: www.aesculap-academy.com
Surgery
November 03-04, 2009 United Kingdom / Sheffield
CORE SKILLS IN OPERATIVE ORTHOPAEDIC SURGERY
Contact: Mrs. Kelly Westlake Tel: 011-44-29-2068-2129 Email: westlakekm@cardiff.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
November 04-06, 2009 United Kingdom / Cardiff
CORE SKILLS IN OPERATIVE ORTHOPAEDIC SURGERY
Contact: Lesley Izzard Tel: 011-44-114-271-4027 Email: Lesley.izzrd@sth.nhs.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
November 04-06, 2009 United Kingdom / Sheffield
HANDS ON GYNAECOLOGICAL ENDOSCOPY SKILLS WORKSHOP
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
November 11-13, 2009 United Kingdom / London
ONEHEALTH STUDY DAY
Contact: Aynsley Pix, B. Braun Medical Limited Email: aynsley.pix@bbraun.com Website: www.aesculap-academy.com
Surgery
November 11, 2009 United Kingdom / Tankersley
Day-case surgery is of great value to patients and the health service. It has rapidly expanded as a cost-effective and resource-conserving surgical intervention. However, the ability to deliver a safe and cost-effective general anesthetic with minimal side effects and rapid recovery is demanded in a day-case surgery unit. Pain and emesis are the two major complaints after day case surgery. Opioids are the agents of choice for severe pain. However, this class of analgesics is associated with dose-dependent adverse effects such as PONV, sedation, respiratory depression, resulting in delayed discharge or prolonged hospital stay. Non-opioid analgesics, e.g. acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs), are often used alone or as adjuncts to opioids because of fewer adverse effects compared to opioids alone. However, NSAIDs also have side effects [1]. Lornoxicam is a new NSAID that belongs chemically to oxicams, a chemical class including piroxicam and tenoxicam. Lornoxicam is a potent inhibitor of cyclo-oxygenase and the only oxicam with a 15 times shorter half-life than piroxicam and tenoxicam [2]. In addition, lornoxicam can be given by I.V. route. Lornoxicam has a better safety profile than diclofinac and naproxen with regards to renal and hepatic function tests. In addition to better GIT tolerability compared to selective COX2 inhibitors; it is completely metabolized to inactive metabolites [2,3]. Lornoxicam has been successfully used in prevention and treatment of postoperative pain. However, evaluation of the perioperative analgesic efficacy of lornoxicam in day-case surgery has not yet been studied. This randomized, double blinded study was designed to compare the quality of perioperative analgesia as well as side effects of IV lornoxicam versus fentanyl in patients scheduled for minor to moderate day-case ENT surgical procedures. Materials and Methods: Male or female patients (aged 18-60 yr) were eligible for inclusion in the study. After obtaining the approval of the Hospital Research & Ethical Committee and patient’s informed consent, patients were randomized into three groups of ASA class I and II, scheduled to undergo minor to moderate day-case ENT surgical procedures e.g. tonsillectomy, excision of ENT lesion (e.g. vocal cord nodules and cysts), polypectomy and endoscopic sinus operations were enrolled in this randomized, double blinded study between May and December 2008. Exclusion criteria were patients with body mass index (BMI) > 30%, drug or alcohol abuse, and known allergy to NSAIDs, paracetamol or any contraindications for opioid use. The protocol was similar for all patients. Prior to surgery, patients were educated in the use of the 10 – point visual analog scale (VAS) for pain assessment (0 = no pain to 10 = maximum pain). No premedication was given. In the holding area, an IV cannula was inserted and an IV infusion of Lactated Ringer’s was started. HR, MAP and SpO2 were recorded before induction (baseline value). Since fentanyl is a clear fluid while lornoxicam is yellow, the pharmacist prepared, covered and coded the medications in two coded envelopes for each patient. One envelope containing lornoxicam 8mg (L8), 16 mg (L16) or placebo to be given half an hour before induction of anesthesia and another envelope with fentanyl 100 µg (F) or placebo to be given with induction i.e. each patient received either IV (F), (L8) or (L16).The medications were administered by a different anesthetist, who was not involved in the study. Anesthesia was induced with propofol 2 mg/kg IV followed by cisatracurium 0.15 mg/kg IV to facilitate orotracheal intubation. After tracheal intubation, the patients were ventilated to normocapnia with sevoflurane (2-3% end tidal) in 50% oxygen in air. All patients received IV 1 gm of paracetamol after induction and were monitored with ECG, MAP, SpO2 and EtCO2. Supplementary fentanyl 0.5 µg/kg was given IV as required in all groups (if > 20% increases in MAP or HR than preinduction values in presence of adequate muscle relaxation). At the end of surgery, muscle relaxation was reversed and extubated. In the post-anaesthesia care unit (PACU), the time from extubation to spontaneous eye opening was compared between the groups. The patients were monitored with ECG, SpO2, MAP, respiratory rate (RR), VAS and sedation score (0 =awake, 1=mild sedation, 2=sleepy but arousable, and 3 = very sleepy) at 0.5,1, 2, 3 and 4 hours by an anaesthetist, who was not aware of the study drug used. Intramuscular (IM) injection of meperidine 1 mg/kg was administered as a rescue analgesic at VAS > 4. The total amount of meperidine required during first 4 hrs postoperative was recorded. The time of the study drugs injection was recorded after decoding their codes. The first need for rescue analgesic was recorded as the time from the administration of the study-drug and the administration of meperidine. The incidence of PONV or any adverse event was recorded. The PACU staff was not aware of the study drug given. The results were analyzed using SPSS version 16. Sample size was 35 patients for each group in order to detect a 20% change in HR and MAP. The α-error was assumed to be 0.05 and the type II error was set at 0.20. Numerical data were expressed as mean ± SD. The groups were compared with analysis of variances (ANOVA). The VAS pain scores were analyzed by Mann-Whitney U test. Categorical data were compared using the Chi square test. P value of 0.05 was used as the level of significance. Results 105 patients aged between 18 and 52 yr were enrolled in the study. There were no significant demographic differences between groups (Table 1). HR and MAP were significantly higher at 10 and 20 minutes after induction of anaesthesia in group L8 compared to groups F and L16 (P < 0.05) (Fig. 1,2). The number of patients with inadequate intra-operative analgesia was significantly higher in group L8 compared to groups F and L16 (Fig 3). In PACU, 40 minutes postoperatively, HR, MAP and VAS were significantly higher in groups F and L8 (Fig 4,5,6). The first analgesic requirement time was significantly longer in group L16 compared to groups F and L8 (Table 2). The mean sedation scores in PACU were insignificantly higher in groups F and L8 compared to group L16 (Table1). While the incidence of PONV was significantly higher in groups F and L8 (p<0.05) (Table 1). Table 1: Demographic characteristics, eye opening time, incidence of postoperative nausea and postoperative sedation score:
F
L8
L16
P
Age (year) - mean (range)
31 (18-52)
32 (18-51)
31 (20-49)
0.129
Sex F/M
Oct-25
Oct-25
Sep-26
0.695
Weight (Kg)
72.7±11.7
74.1±11.3
75.3±9.9
0.402
Height (cm)
166.2±14.7
169.4±11.9
161±19.5
0.482
ASA physical status I/II
23-Dec
22/13
25-Oct
0.312
Duration of surgery (min)
58.8±21.8
59.6±21.4
56.9±23.3
0.675
Time to eye opening (min)
7.2±3.1
6.4±1.2
3.7±1.6*
0.019*
Postoperative nausea
9/35
7/35
3/35*
0.002*
Postoperative sedation score (0 – 3)
1.7±0.6
1.9±1.1
1.4±0.6
0.357
Data are expressed as mean ± SD or number of patients* Significant difference (P < 0.05). NS: Non significant.- Time to eye opening is the time from extubation to spontaneous eye opening.Table 2: Perioperative analgesic requirements and time to first postoperative analgesic requirement (mean ± SD)
F
L8
L16
P
Intra-operative fentanyl supplementation (µg)
45.5 ± 13.2
67.8 ± 16.4*
43.1 ± 10.2
0.012*
Time of 1st postoperative rescue analgesic (min)
94.3 ± 33.4
101.6 ± 51.5
223.9 ± 62.3*
0.0002*
Postoperative meperidine rescue (mg)
76.3 ± 12.5
80.5 ± 11.7
39.9 ± 7.6*
0.001*
-Data are expressed as mean ± SD.* Significant difference (P < 0.05). NS: Non significant.-Time of 1st postoperative rescue analgesic is the time elapsed between the administration of the study drug and the administration of an analgesic postoperatively. Fig 1: Intra-operative changes in heart rate in groupsFig 2: Intra-operative changes in MAP in groupsFig 3: Number of patients requested perioperative analgesic supplementationFig 4: Changes in heart rate in PACUFig 5: Changes in MAP in PACU:Fig 6: Changes in VAS in PACUDiscussion: The use of an opioid, even a short acting one can be associated with adverse effects, which may not be acceptable for patients scheduled for day case surgery. For this reason, it was suggested to substitute an opioid with a non-opioid analgesic for postoperative pain control. The use of a NSAID is associated with adverse effects [1]. Lornoxicam has been successfully used in the prevention and treatment of postoperative pain. It has been shown to be as effective as morphine [4], meperidine [5] and tramadol [6]. To the best of our knowledge, this is the first study to compare the perioperative analgesic efficacy of lornoxicam to fentanyl in patients undergoing day case ENT surgery. We gave Lornoxicam half an hour before induction of anesthesia as the time taken to reach peak plasma concentration (Tmax) was determined to be 0.5 h [7]. During the operative procedure, HR and MAP were significantly higher in group L8 compared to group F and L16. While in PACU, patients in groups F and L8 had higher HR, MAP and VAS score in the early postoperative period compared to patients in group L16. This may be due to inadequate analgesic effect of L8 and the shorter plasma half life of fentanyl compared to L16. The analgesic efficacy of L16 might be attributable to inhibition of cyclo-oxygenase (COX1) and (COX2) activity [2], release of endogenous dynorphin and β-endorphin [5], decrease in peripheral and central prostaglandin production [8] as well as exertion of some of its analgesic activity via the central nervous system [9]. Lornoxicam has a more potent anti-inflammatory and analgesic effect than other oxicams as well as a shorter half life, which decreases the incidence of side effects of drugs with long plasma half life [10]. Arslan and colleagues reported decreased opioid need, PONV and postoperative pain scores when 16 mg of lornoxicam was administered after thyroidectomy [11]. While Xuerong and colleaguessuggested that the increase of postoperative morphine requirements induced by intra-operative administration of fentanyl could be prevented by ketamine or lornoxicam [12]. Rawal reported that NSAIDs are effective as the sole analgesic in a high proportion of cases of mild to moderate pain and it is more convenient to give these drugs by the IV route rather than by IM or rectal administration [13]. The analysis of pain intensity differences was complicated by the fact that many patients postoperatively were asleep at the time their pain assessments were due which may be attributed to effect of opioid and anesthetic medications used. To minimize any missing data we used time to the first dose rescue analgesia (based on changes in hemodynamic data) to evaluate pain intensity differences from baseline. L16 was well tolerated in this study, and was associated with a significantly lower incidence of adverse events than F and L8 which could be due to the opioid side effects in both groups. Norholt and colleaguessupported our results as they reported that, in terms of common acute adverse events, lornoxicam appeared to possess a higher benefit/risk ratio compared with morphine [4]. Zuurmond et al reported that, there is good evidence that avoidance of opioid virtually abolishes the PONV that preclude oral intake of fluids after surgery [14]. In our study, nausea developed in 25.7% of patients in group F, 20% in group L8 but only 8.6% in group L16 who received the least rescue opioid analgesia. Regarding bleeding abnormalities, Hodsman et al reported extensive bleeding required reoperation on two diclofenac group patients submitted to abdominoperitoneal resection of the rectum [15]. In our study no abnormal bleeding was reported by ENT surgeons in any of the study patients. In agreement with our results, Ilias et al[16], Trampitsch et al[17] and Karaman et al [18] used lornoxicam and they did not detect problems with surgical bleeding, bleeding time, blood transfusion requirement or postoperative bleeding. Stroissnig et al reported that overall, in healthy adult volunteers, oral doses of lornoxicam up to 70 mg have been well tolerated, and there have been no effects on vital signs, urine analysis parameters or clinical serum biochemistry [19]. In our study, none of the patients receiving study drugs experienced severe gastric discomfort, needed rescue antiemetic medication or required admission because of poor pain control. Previous studies used lornoxicam for reduction of postoperative opioid consumption but none of them had studied the intra-operative use of lornoxicam. So, we selected certain type of surgical procedures which might be suitable to use lornoxicam as a sole intra-operative analgesia. The adjunctive use of acetaminophen may have additive analgesic efficacy to lornoxicam because of its intrinsic opioid-sparing activity. Measurement of serum catecholamine would have been useful. These could be considered as a limitation for the present study. Conclusion: Intravenous 16 mg lornoxicam with the present study design was comparable to 100 µg fentanyl as intra-operative analgesia but more effective than fentanyl in preventing early postoperative pain in mild to moderate ENT surgical procedures. Intravenous lornoxicam 8 mg was not satisfactory as a sole intra-operative analgesia. The overall incidence of adverse effects of lornoxicam was lower than that of fentanyl.
According to The National Kidney Foundation of The United States of America 1 CKD is defined as (1) evidence of kidney damage based on abnormal urinalysis results (e.g., proteinuria, hematuria) or structural abnormalities observed on ultrasound images or (2) an absolute GFR of less than 60 mL/min for 3 or more months. Based on this definition there are five stages. See Table 1. Anemia affects 60% to 80% of patients with chronic kidney disease (CKD) and reduces their quality of life. Treatment options are blood transfusion, epoietin alfa and darbepoetin alfa 2 . Anemia of CKD is, in most patients, normocytic and normochromic and primarily caused by depressed production of erythropoietin (EPO), oxidative stress and inflammation, erythropoiesis inhibition and reduction in red blood cell survival 3,4,5 . The other cause of anemia is deficiency of iron. The dialysis patient is in a state of continuous iron loss from gastrointestinal bleeding, blood drawing, and/or, most important with hemodialysis (HD), the dialysis treatment itself. HD patients lose an average of 2 g of iron per year. Thus, iron deficiency will develop in virtually all dialysis patients receiving EPO unless supplemental iron therapy is given orally or intravenously. DRIVE study, a randomized trial study, adds direct evidence that administration of intravenous iron to patients with functional iron deficiency who were on supplemental EPO therapy results in increase in the hemoglobin level 6. The aim of this review is to assess that whether Erythropoietin (EPO) treatment is beneficial or harmful in the management of anemia associated with CKD. To address these issues, we have analyzed randomized controlled trials, observational studies and meta-analyses.
Table 1: Stages of CKD according to NKF.
CKD Stage
Kidney damage
GFR
Stage 1
No kidney damage
>90 mL/min
Stage 2
mild kidney damage
60-90 mL/min
Stage 3
moderate kidney damage
30-59 mL/min
Stage 4
severe kidney damage
15-29 mL/min
Stage 5
Endstage kidney damage
<15 mL/mi
Methods:
Search strategy: The search strategy was designed to capture the patient population, suffering from CKD on supplemental erythropoietin (EPO) therapy. Literature search (1989 to 2008) was carried out using MEDLINE, PubMed as well as other electronic databases and in online journals using the keywords "Kidney failure, chronic and "erythropoietin" for studies up to 1996, and "epoetin alfa" for subsequent years.
Selection of studies: All papers identified were English-language, full text papers. In addition, the reference lists of identified relevant articles were also searched. The search was not limited to any specific study design, and we searched for randomized controlled trials (RCTs), observational studies, systemic review and meta-analysis. Citations identified in the literature search were independently screened by author to select potentially relevant articles. The full articles from this list were retrieved and subsequently reviewed by author for inclusion in the systematic review. During selection preference was given to articles published within last five years. Articles were included if they met the following inclusion criteria 1) published in a peer reviewed journal; 2) written in English; 3) reported randomized controlled trials of EPO; 4) observational studies regarding EPO and quality of life; 5) Review articles and meta-analyses about EPO therapy in CKD patients.
Results:
470 citations were identified in search from PubMed, Medline and from other online journals. Of these 470 citations, 444 did not meet the selection criteria and were excluded, leaving 26. Out of 26 citations 11 were RCTs, 10 were observational studies and 5 were reviews and meta-analysis.
Five studies (Parfrey et al7, Foley et al8, Furuland et al9, Drüeke et al10, and Canadian Erythropoietin Study Group11) showed that correction of anemia result in improvement of quality of life, although the singh et al12 showed such improvement with partial correction of anemia, and no detectable difference in the quality of life was evident in Roger et al13 study. Five studies Parfrey et al7, Foley et al8 and Levin et al14 and McMahon et al15 and Roger et al13 showed that normalization of hemoglobin does not lead to regression of established concentric LV hypertrophy or LV dilation. It may, however, prevent the development of LV dilation. In McMahon et al15 study the only factor that seemed to predict normalization of LV mass in patients who had LV hypertrophy at study entry was a lower pulse pressure. One study Sikole et al16 correction of renal anemia can normalize heart morphology and improve heart function. Three studies Besarab et al17, Drüeke et al10 and Singh et al12 demonstrated increased cardiovascular events whereas two studies Drüeke et al10 and Singh et al12 also showed progression to dialysis in patients assigned to the highest hemoglobin targets (>13.0 g/dL), compared with <12 g/dL, trial design of three studies was same in respect that both arms were on EPO. In comparison to Drüeke et al10 and Singh et al12 studies, in Roger et al13 study the renal function was not adversely affected in the group randomized to the higher Hb. (Table 2).
Table 2: Randomized controlled trials (RCTs)
Study
Study design
Patients enrolled
Parameters observed
Outcomes
Parfrey et al7
RCT double blind
596
QoL, LVVI
No change LVVI. QoL improved.
Foley et al8
RCT open label
146
QoL, LVH, LVD
QoL improved, No change LVMI
Furuland et al9
RCT open label
416
QoL, Safety.
QoL improved.
Drüeke et al10
RCT open label
603
CVE, QoL, LVMI, Renal function
QoL improved, No change LVMI.
Canadian Erythropoietin Study Group11
RCT double blind
118
QoL .
QoL improved.
Singh et al12
1432
CVE, QoL, Renal function
QoL not improved.
Roger et al et al13
RCT open label
155
LVMI. Renal function, QoL
No change.
Levin et al14
RCT open label
172
LVMI.
No change.
McMahon et al15
RCT open label
120
Change in LVMI.
Prevention&↓ in LVMI.
Sikole et al16
RCT open label
38
Heart morphology & functions.
Heart function
Improved.
Besarab et al17
RCT open label
1233
Effects of normal HCT.
↑CVE
Both Phrommintikul et al18andGiovanni et al19 addressed the similar issues, to evaluate the benefits and harms of different hemoglobin (Hb) targets in CKD in their meta-analyses. They reached to similar conclusion, increase in the risk of all-cause mortality in anemic patients with CKD in whom a higher Hb target (in the normal physiological range) is aimed for with treatment with EPO. Such patients are also at an increased risk of arteriovenous access thrombosis and poorly controlled hypertension, which could contribute to the increased risk of mortality. Furthermore, there seems to be no beneficial effect on left ventricular mass in such patients. There were similarities and differences in inclusion criteria. Both used the trials targeting different Hb concentrations in patients with anemia caused by CKD, majority of trials analyzed were different except 4 trials which were same in both. The difference in inclusion criteria was that Giovanni et. al analyzed two groups of studies: The first group contained studies in which the intervention was to achieve different Hb targets compared (higher versus lower Hb targets), both arms were on EPO and trials included individuals with clinical cardiovascular disease. The second group compared EPO treatment with no EPO treatment. The results of these two groups of studies were analyzed separately. In Phrommintikul only one group of studies “EPO treatment with no EPO treatment” was analyzed. Meta-analysis by Phrommintikul et alincludes nine RCTs, which enrolled 5143 patients.
In Jones et al20 meta-analysis both randomized controlled trials and uncontrolled trial were analyzed, all studies were of the “pre/post” design, in that measurements of anemia, quality of life, hospitalizations, and transfusions were taken before and after initiation of EPO therapy. They drew these conclusions from 16 published studies of which 5 were randomized clinical trials. He found that treatment with EPO raised hemoglobin levels, reduced transfusion requirements and improved quality of life. For quality of life outcome in these meta-analysis please review Table 3.
Table: 3 Meta-analysis.
Meta-analysis
Question addressed
No of studies included.
Assessed quality of life (QoL).
What measures of quality of life used in these trials.
Were the major gains in QoL seen with EPO.
Phrommintikul et.al18
Target Hb and cardiovascular events in CKD.
9
No
_____
_____
Giovanni et al19
Evaluate the benefits and harms of different Hb targets in CKD.
19
Yes
KDQ
QoL
Improved
↑KDQ
Jones et al20
Effects of
EPO on clinical efficacy, QoL hospitalizations,
and transfusions.
16
Yes
KPS
KDQ
SIP
QoL improved
↑KDQ
↑ KPS
↓SIP
Discussion:
Erythropoietin (EPO) has become an essential part of the management of anemic patients with CKD. It is also used to treat the anemia associated with chemotherapy and other diseases, and it improves quality of life 21,22 . The introduction of EPO in 1989 significantly improved the clinical management of anemia of CKD. By 2005, 99% of incenter hemodialysis patients received EPO treatment for their anemia. EPO dosing has changed dramatically in the past decade and a half; between 1991 and 2005, the mean dose of EPO increased about 4-fold in dialysis patients. Today, EPO therapy is the largest single Medicare drug expenditure totaling $1.8 billion in 2004 (an increase of 17% from 2003) and EPO comprised 11% of all Medicare ESRD costs 23
EPO and left ventricular hypertrophy. Randomized vs. Observational studies. Anemia is a contributing factor in many of the symptoms associated with reduced kidney function. These include fatigue, depression, reduced exercise tolerance, dyspnea.Data from observational studies shows that severe anemia may results in cardiovascular consequences, such as left ventricular hypertrophy (LVH) and left ventricular systolic dysfunction 24. Left ventricular hypertrophy (LVH) is present in nearly 80% of dialysis patients and is associated with higher rates of cardiovascular events 25. It is also associated with an increased risk of morbidity and mortality principally due to cardiac disease and stroke 26,27. As a result, patients with anemia due to CKD are at increased risk of hospitalization, hospital length of stay, reduced quality of life and mortality 28. Uncontrolled studies suggested that partial correction of anemia with EPO therapy may result in prevention or regression of CHF 29 and LVH 30,31. Several randomized controlled trials showed that left ventricular hypertrophy was not further improved by a complete correction of anemia compared to only partial correction 7,13,14,15,17. Robert N Foley et al. randomly assigned 146 patients with either concentric LV hypertrophy or LV dilation to receive EPO to achieve hemoglobin levels of 10 or 13.5 g/dL. He concluded that normalization of hemoglobin does not lead to regression of established concentric LV hypertrophy or LV dilation. It may, however, prevent the development of LV dilation, and it leads to improved quality of life 8. Partial correction of severe anemia <8 or 9g/dl to mild anemia (10-11 g/dL) likely reduces mortality, but further treatment to higher Hb levels has not been shown to further reduce mortality, and has actually increased mortality. Controlled studies with quality of life (QOL) and left ventricular mass as end points support partial correction of hemoglobin in dialysis patients 11,13,16,32, The fact that anemic renal failure patients have more LVH than non-anemic renal failure patients does not prove that anemia causes LVH. Vaziri et al in a review mentioned that the real culprits are oxidative stress, inflammation and diminished biological capacity that simultaneously cause treatment-resistant anemia and adverse cardiovascular and other outcomes 33.
EPO and quality of life:Numerous randomized, controlled trials have demonstrated that EPO significantly raises hemoglobin levels, reduces transfusion requirements, and improves quality of life in anemic patients with chronic renal failure. Lefebvre et al conducted an analysis on data from a multicenter, open-label, prospective study of EPO for anemia in patients with CKD not on dialysis to evaluate the relationship between Hb level and quality of life (QOL). The results showed that the maximal incremental gain in QOL occurred when Hb reached 11 to 12 g/dL. This suggests that treating anemic patients with non-dialysis CKD until their Hb level reaches 12 g/dL will result in the greatest QOL improvement per Hb unit increase 34.
Randomized vs. Observational studies. Many randomized controlled trials suggest an association between higher hemoglobin level and improved quality of life, physical function, and exercise capacity 7,8,9,35 but the association with survival is less clear. Whereas observational studies have generally shown increased survival with higher hemoglobin level 36,37,38,39,40 randomized trials have not shown such benefits. The extent anemia of inflammation varies between patients with renal failure. It is this factor that likely explains the following paradox: in observational studies, higher hemoglobin associates with better survival in CKD, while in controlled trials, higher hemoglobin achieved by escalated EPO dosing decreases survival. In the observational studies, those with the higher Hb levels were likely those patients who had the least component of anemia of inflammation, and therefore less resistant to EPO supplementation; they survived better not because they had better hemoglobin, but because they had less burden of inflammatory disease. Anemia of chronic disease is a highly conserved response that is mediated by multiple mechanisms acting in concert to lower the hemoglobin in the face of inflammation, and should be presumed until proven otherwise to be adaptive for most patients who exhibit it. That this is so is supported by the observation that the correction of anemia confers lower survival not only in renal failure, but also in cancer patients and in patients in the critical care unit.
Jones et al. in their very thorough meta-analysis 20 indeed found that treatment with EPO raised hemoglobin levels, reduced transfusion requirements and improved quality of life. Studies have demonstrated that morbidity and mortality rates are lower when hematocrit values are within the Disease Outcomes Quality Initiative (DOQI) target range (33 to 36%) 40. Ernesto Paoletti et alin their review of observational and randomized studies concluded from the results of observational studies that normalization of Hb in renal patients seems to be associated with further improvement in quality of life and physical activity but with no significant differences in mortality rate, hospitalization rate, and the extent of LVH regression, but the results of randomized trials show that achieving near-normal Hb did not reduce the risk for death from all causes or the risk for cardiac death. The latter risk actually increased slightly, in the group of dialysis patients with normalized Hb concentration 41. For CKD stage 3 and 4 patients, no improvement seen in CHOIR, but improvements reported in CREATE. There may be reporting bias in CREATE as it was an open label study, and the low target arm had to develop worsening anemia prior to initiating EPO therapy 10,12
EPO and Cardiovascular Events:Anemia is a common complication of chronic kidney disease. Determination of the appropriate target hematocrit level for patients undergoing hemodialysis continues to be a controversial area 40. The National Kidney Foundation Dialysis Outcomes Quality Initiative (K/DOQI) states when a decision to use EPO is made, some Hgb value in the range of 11 to 12, but no higher than 13 should generally be chosen. 42. The European Best Practice Guidelines (EBPGs) recommend that most patients with CKD achieve a target hemoglobin (Hb) 11 g/dl to reduce the risk of adverse outcomes 43.Randomized vs. Observational studies. Observational studies have shown a strong association between severity of anemia and risk of morbidity and mortality from cardiovascular disease and other causes in CKD patients 36,37,38,39,40. These findings have been interpreted as evidence for the causal role of anemia in the pathogenesis of adverse outcomes in these patients. On the hand, randomized clinical trials of anemia management revealed either no effect or increased morbidity and mortality in patients assigned to normal hemoglobin Hb targets 10,12,17. Meta- analyses of randomized clinical trials have shown a significant increase in cardiovascular and all-cause mortality and arteriovenous access thrombosis among patients assigned to the higher than those randomized to the lower Hb targets 18,19. Meta-analysis of Phrommintikul shows a significantly higher risk of all-cause mortality (targeting a Hb level higher than 12 g/dL results in a 17% increased risk of death compared with target hemoglobin levels less than 12 g/dL), arteriovenous access thrombosis and higher risk of poorly controlled blood pressure in the higher Hb target group than in the lower target Hb. The incidence of myocardial infarction was much the same in the two groups 18. Meta-analysis of Giovanni F.M et al shows that on the basis of available randomized, controlled trials, Hb targets of <12.0 g/dL are associated with a lower risk of death in the population with cardiovascular disease and CKD compared with Hb targets of >13.0 g/dL. For every 30 patients treated to an Hb target of <12.0 g/dL compared with an Hb target of >13.0 g/dL, approximately one death is avoided 19. Two large randomized controlled trials; CREATE [38] and CHOIR [39] demonstrated increased cardiovascular events and progression to dialysis in patients assigned to the highest hemoglobin targets (>13.0 g/dL), compared with <12 g/dL. US Food and Drug Administration (FDA) warned that use of erythropoiesis-stimulating agents (ESAs) increases mortality and morbidity risk. The warning follows publication of studies suggesting that correction of anemia in patients with CKD did not reduce the risk of cardiovascular events and that reaching a target Hb level of >13 g/dL, compared with a target level of 11.3 g/dL, was associated with increased risk of cardiovascular events. FDA said recent studies had found increased risk of death, blood clots, strokes, and myocardial infarctions in patients with chronic renal disease who received ESAs at higher-than-recommended doses that maintained their hemoglobin levels at more than 12 g/dL 44.
EPO and kidney:EPO has been found to interact with its receptor in a large variety of non-haematopoietic tissues, which result into cytoprotective cellular responses, like mitogenesis, angiogenesis, inhibition of apoptosis and promotion of vascular repair through mobilization of endothelial progenitor cells from the bone marrow. In experimental ischaemic and toxic acute renal failure administration of EPO, promotes renoprotection. Preliminary experimental and clinical evidence also indicates that EPO may be renoprotective in chronic kidney disease22 .EPO is used widely to treat anemia in patients with CKD, but the benefits of EPO use in patients with acute renal failure (ARF) are unclear. In vitro and animal studies suggest that EPO may promote renal recovery and decrease mortality in ARF 45. Partial amelioration of anemia with low doses of EPO was reported to slow the rate of progression to ESRD in a group of CKD patients 46. These cellular protection from EPO observed in animal models has not been confirmed in humans, and has been specifically addressed and disproven in large randomized trial. The CREATE study found as a secondary endpoint that early treatment with EPO increased the likelihood of starting dialysis. CHOIR found no reduction in the rate of progression of CKD in patients given more EPO (the higher target arm) compared to the lower target arm 10,12.
EPO for other Indications:In recent years, studies in animals and humans have focused on the use of EPO for other indications. It has been found to play a role in both cardioprotection and neuroprotection. It has effects on the immune system, and can cause regression in hematologic diseases such as multiple myeloma. It may also improve the response of solid tumors to chemotherapy and radiation therapy 21. Again the cellular protection from EPO observed in animal models has not been confirmed in humans.
EPO and Seizures:Seizures are reported to be a complication of EPO in the product information. However, in a meta-analysis conducted by Giovanni et alshowed that treating with EPO may be protective against seizures Lower Hb targets of <95 g/L in individuals who are not treated with EPO are associated with a significantly increased risk of seizures compared with treatment with EPO and Hb values of >100 g/L 19.
EPO and Hypertension:Administration of ESA may be associated with exacerbation of
hypertension in about 5% of patients. Robert N. Foley et alin his analysis of observational and randomized studies found that most of the trials that have been reported to date have shown that higher hemoglobin targets lead to higher BP levels and/or greater requirements for antihypertensive therapy, he drew this conclusion from nine randomized trials 47. The mechanism of ESA induced hypertension is thought to be related to stimulation of the vascular endothelium by ESA resulting in increased circulating levels of endothelin. Furthermore the increase in hemoglobin associated with ESA therapy may increase blood viscosity resulting in vasospasm. As such routine monitoring of blood pressure is essential in patients treated with ESA 48. Meta-analysis of Phrommintikul et al showed a significantly higher risk of poorly controlled blood pressure in the higher haemoglobin target group than in the lower target hemoglobin 18 . Giovanni et almeta-analysis showed lower Hb levels of <95 g/L with no EPO treatment are associated with a reduced risk of patients who present with hypertensive episodes. In absolute terms, the risk of developing hypertensive episodes is 16% lower with Hb values <95 g/L compared with Hb >100 g/L. For every seven patients treated to obtain an Hb >100 g/L, one patient will require additional antihypertensive medication 19
EPO and Access:Normalizing hemoglobin has been associated with a higher incidence of vascular access clotting 40. Randomized, prospective, open-label trial study of Besarab et al, showed a significantly higher risk of access thrombosis with the higher Hb targe17. Meta-analysis of Phrommintikul et alshowed a significantly higher arteriovenous access thrombosis in the higher Hb target group than in the lower target Hb 18.
EPO and Pure Red Cell Aplasia (PRCA):Although rare, administration of ESA may result in formation of anti-erythropoietin antibodies, thereby leading to pure red cell aplasia and erythropoietin resistance 49 In patients in whom ESA doses have been maximized without effect and no other causes can be identified, serum anti-erythropoietin levels and bone marrow biopsy should be performed. If confirmed, erythropoietin administration should be ceased and the patient treated with periodic blood transfusions.
Conclusion: Achieving hemoglobin control over time is a major challenge because of the various physiological factors that influence the response in individual patients and the potential risk for increased mortality, particularly for patients with co morbidities 50. The association data led to several hypotheses about what anemia was causing e.g. LVH, fatigue, and increased mortality. These hypotheses have been tested in RCT's and in most cases anemia is associated with but does not cause the outcome, such as LVH or mortality. Fatigue is improved somewhat by anemia treatment with EPO, and transfusion frequency is reduced, though the cost is high. In the case of EPO balance is critical. Too little treatment and patients with chronic kidney disease are subjected to a lifetime of exhaustion and blood transfusions. Too much and they could be threatened with an increased risk of death. The overall quality of life is improved when anemia is treated with EPO, but aiming for a target value of 13.5 g of hemoglobin per deciliter provided no additional quality-of-life benefit 12.
Key Points:
Anemia is associated with bad outcomes; Anemia is nearly universal in advanced renal disease. In these patients, anemia is associated with increased cardiovascular morbidity and mortality, reduced quality of life, and accelerated renal disease progression, though those associations do not necessarily establish causation.
Treatment of anemia reduces transfusion requirements and improves quality of life in anemic patients with CKD.
Mortality increases with treatment to higher targets; Recent studies have found an increased risk of death, blood clots, strokes, and myocardial infarctions in patients with chronic renal disease who received ESAs at doses that maintained their hemoglobin levels at more than 12g/dL, leading the Food and Drug Administration to apply a 'black box' warning to the product monographs of licensed ESAs.
Recent studies support partial correction, not normalization of hemoglobin.
The Foundation Programme1,2,3 is a 2-year, ubiquitous, vocational curriculum undertaken by newly qualified doctors wishing to proceed onto speciality training in the United Kingdom (UK). Since 2006, Foundation Year Trainees in the UK have been required to complete one clinical audit during their two year programme. We review the practice of audit and doctors’ attitudes to the difficulty in performing audits at a National Health Service (NHS) hospital trust comprising three hospital sites in the South East of England. The Foundation Programme demands that Foundation Year Trainees are able to consider the relevance of clinical audit and describe the audit cycle with regard to developing patient care, clinical governance and risk management. They are expected to undertake a clinical audit and recognize how it relates to the improving clinical standards and addressing clinical governance1. Clinical audit can be defined as the processof reviewing the delivery of care to identify deficiencies sothat they may be remedied4. Whilst it was initially used in assessing medicalpractice against local standards, audit ‘has evolved conceptuallyas a mechanism through which evidence-based guidelines can beintroduced into routine clinical practice’5. Apart from fulfilling the requirements of the syllabus, reasons for audit include professional education and the opportunity to improve patient care6. Barriers to audit might include: disagreement amongst professionals as to what constitutes a good audit5;organisational impediments; and a lack of resouces6. This study therefore sets out to investigate the level of audit activity in a hospital trust in South East England amongst all Foundation Year Trainees. Importantly it will also assess doctors’ attitudes and views towards the audit process and perceived or actual barriers to their completion. METHOD Questionnaires were sent to all Foundation Year 1 (F1s = 63 in total) and Foundation Year 2 (F2s = 56 in total) Trainees in the trust (119 doctors). The study group involved trainees in the Foundation Programme from 31st July 2007 to 30th July 2008. Doctors who had been transferred out of the trust were not included in the study. There were no doctors who had transferred into the trust and were in the Foundation Programme. A study representative at each of the 3 hospital sites was tasked to distribute the questionnaires. Trainees were asked to complete the questionnaires in an informal setting and to return them directly to the site representative. The study environment was variable, and questionnaires were distributed and completed on the wards or at group teaching sessions. Participants were given the choice of completing and submitting their form immediately, or submitting it at a later date. Data collection was commenced 11 months after the trainees had commenced employment in the trust and concluded after 2 weeks. This was invoked as many trainees were clearing annual-leave requirements towards the end of their hospital posting, and the consensus that very few audits would be officially completed at that stage of training in the summer. Questions were drawn from previous studies to the barriers to audit in our Trust. In the first section of the questionnaire, participants were asked about: “the number of all audits attempted or applied for”; “the number of new audits attempted or applied for”; “the number of audits completed and presented so far”; and “the number of audits started but never completed”. The second part of the questionnaire assessed subjective opinions on barriers to completing audits. Participants were asked to rate the following 5 statements on a comparative scale of 1-5 (1 being “strongly disagree” and 5 being “strongly agree”): “The audit department is helpful in approving audits”; “senior staff are helpful in involving me in audits”; “I can complete audits within official working hours”; “most audit opportunities are in my area of interest”; “most audit opportunities are of clinical value”. Results were collated and tabulated and presented at local meetings where feedback was received. RESULTS Ninety-two out of a possible 119 (77.3%) Foundation Year Trainees completed the questionnaire (57/63 - F1s, 35/56 - F2s). There were 106 total attempts at audit for the F1 trainees and 65 total attempts for the F2s. Most trainees had attempted 1 or 2 audits in their respective year (42 F1s at 73.7% and 23 F2s at 65.7%). 5 F1s (8.8%) and 3 F2s (8.6%) had neither attempted nor applied for any audits. Ten F1s (17.5%) and 9 F2s (25.7%) had attempted more than 2 audits (Table 1). Table 1: Number of audits attempted by trainees
Number of all audits applied for or attempted
F1s
F2s
Number
Percentage (%)
Number
Percentage (%)
0
5
8.8
3
8.6
1
21
36.8
17
48.6
2
21
36.8
6
17.1
3
3
5.3
3
8.6
4
2
3.5
5
14.3
5
4
7.0
0
0
6
1
1.8
0
0
7
0
0
1
2.8
Total
57
100
35
100
The results for the total number of completed audits (i.e. an audit that included data collection, analysis and formal presentation to the respective department) are summarized in Table 2. For F1s, 32 out of a total 106 attempted audits were completed (30.2%), this percentage rising for F2s (38/65; 58.5%). Thirty-three (57.9%) F1s and 10 F2s (28.6%) failed to complete any audit, with a number able to complete one audit presentation in the year: 18 F1s (31.6%) and 16 F2s (45.7%). Table 2: Number of audits completed by trainees
Number of completed audits
F1s
F2s
Number
Percentage (%)
Number
Percentage (%)
0
33
57. 9
10
28.6
1
18
31.6
16
45.7
2
5
8.8
6
17.1
3
0
0
2
5.7
4
1
1.7
1
2.9
Total
57
100
35
100
With respect to new and original audits attempted by trainees, this was achieved by 66.7% of F1s and 74.3% of F2s (Table 3). There was no formal data on the number of audit loops being closed. Table 3: Number of new audits designed by trainees
Number of new audits attempted or applied for
F1s
F2
Number
Percentage (%)
Number
Percentage (%)
0
19
33.3
9
25.7
1
25
43.9
19
54.3
2
9
15.8
3
8.6
3
1
1.75
2
5.7
4
1
1.75
2
5.7
5
2
3.5
0
0
Total
57
100
35
100
With regard to barriers to completion of audits (Table 4), results were notably equivocal for “helpfulness of the audit department and senior staff” (both averaging 3.1 on the comparative scale of 1-5), and “the clinical value of the audits available” (mean score 3.2). The mean score for “completing audits within official hours” was 2.1 with a similar trend observed in “the audits available in an area of interest” (mean score 2.6). Table 4: Trainees’ experiences with audit
Statement
Score¶
Total responses
1
2
3
4
5
Audit department is helpful
Percentage %
9.1
12.5
44.3
22.7
11.4
100
Numbers
8
11
39
20
10
88
Mean score
0.1
0.3
1.3
0.9
0.6
3.1
Senior staff are helpful
Percentage %
15.4
20.9
23.1
22.0
18.7
100
Numbers
14
19
21
20
17
91
Mean score
0.2
0.4
0.7
0.9
0.9
3.1
Audit completed in working hours
Percentage %
46.2
22.0
16.5
8.8
6.6
100
Numbers
42
20
15
8
6
91
Mean score
0.5
0.4
0.5
0.4
0.3
2.1
Audits in the area of interest
Percentage %
18.7
30.8
25.3
17.6
7.7
100
Numbers
17
28
23
16
7
91
Mean score
0.2
0.6
0.8
0.7
0.4
2.7
Audits have clinical value
Percentage %
7.7
18.7
30.8
34.1
8.8
100
Numbers
7
17
28
31
8
91
Mean score
0.1
0.4
0.9
1.4
0.4
3.2
¶Key: 1= strongly disagree; 2=disagree; 3 = equivocal; 4 = agree; 5 = strongly agreeNB: Some forms were incomplete, and therefore responses may not add up to 92. CONCLUSIONS Although audit is well established to be beneficial in improving clinical practice7, this study suggests that trainees under-perform against the curriculum of the Foundation Programme. Historically, the level of audit activity amongst doctors has been low; for example, McCarthy (1997) demonstrated that whilst doctors see the conceptual value of audit, approximately one-third only had presented their data at a pertinent audit meeting8. These results have been replicated in numerous other studies9,10,11. We believe that this data-set is the first available for junior trainees who have undertaken the Foundation Programme curriculum, with a good response rate of 77.3%, and incorporates the contractual pressures invoked by a European Working Time Directive (EWTD)-compliant Rota12,13. While the results show that the majority of respondents (>90%) had attempted an audit, most significantly the majority of audits that were started were not completed. A large percentage of F1s (57.9%) and F2s (28.6%) failed to complete an audit at all. Similar numbers have been reported, even among senior pediatric trainees at registrar level, where one study demonstrated that whilst audit activity was above 90%, only 16% had completed the audit cycle14. One possible explanation is that many trainees appear to have a sub-optimal comprehension about audit and its process. Our consensus was that some trainees attempted audits that were too large or unmanageable, or even of insufficient quality, in striving to achieve a peer publication from their work. When realized that the publication value is poor, or that the audit design is flawed, many trainees lose interest and fail to complete. Another concept highlighted by this study is confusion over the definition of a “completed audit”. For consideration of completion of an audit, a trainee has to demonstrate both the ability to collect the data and present it to among his peers in a formal meeting. This generally amounts to completion of 5 out of the 6 stages of the audit loop15. Surgical morbidity and mortality presentations had been considered audit by some trainees, as they were termed by the trust as a “surgical audit”. However, the overall clinical consensus is that they are not audit but formative educational meetings because no systemic local or national standards were employed for comparison. This poor understanding of audit has been well described previously16. Potential barriers to the completion of audit include some of the issues raised in this study. In this sample, doctors were equivocal about whether the barrier was the audit department or lack of senior support. This reflected the variability of experience as well as the lack of teaching of the purpose and methods of audit in the undergraduate curriculum. They were also equivocal about the clinical value of audits they had completed. By comparison, a study in Leeds showed that less than half of the 232 respondents were aware of subsequent change in clinical practice and 27% felt it was “a waste of time”7. However this study did not focus on the junior doctor in the beginnings of their postgraduate training. Trainees felt that an additional barrier to audit completion included difficulty in completing audits within their working hours. All Foundation Year Trainees in the trust were working to a EWTD-compliant Rota during the year, where trainees did not exceed 48 hours a week of on-site hospital clinical duties. Trainees also found it difficult to undertake audits in their area of clinical interest. Although part of the reason is circumstantial - the Foundation Year Programme mandates that trainees rotate around various core specialties - this may also reflect a lack of understanding of what the audit cycle actually incorporates, and how it is not formal research in itself15. Approval of audit studies was also thought to be problematic because such meetings only took place monthly with a pre-determined agenda, and consequently, this meant that approval might take several months to obtain for trainees who would actually be based in the trust for no more than 12 months in 3 different specialty departments. There were a number of limitations of the study, one being the small sample size. Secondly, in asking trainees to rate each of the six statements from 1 to 5, trainees who did not complete audits tended to score 3 (neither agree or disagree), and as the results above show, they represented a considerable proportion. A larger sample size and a semantic differential scale (rating responses between 1 and 7) might have been more discerning. The fact that some trainees may have included “audits” which on reflection did not meet the criteria for inclusion was not only interesting but may also have distorted results. Finally, audits that involved joint effort among trainees, but were presented only by one of them in the absence of the others were still regarded by some trainees to be “completed and presented” by all of them. This study has highlighted a number of issues which need to be addressed for clinical audits to be successfully completed during the Foundation Programme. The authors believe that poor completion rates are most probably the result of poor understanding of audit. Potential solutions include teaching medical students concepts of audit; giving structured teaching early in the Foundation Programme; instituting regular audit meetings; incorporating audit as part of contracted working hours; defining audit more clearly among trainees and clinical staff and encouraging more cooperation and integrative liaison with the audit department to process audit proposals quickly and efficiently. Additionally, doctors’ contractual pay-bandings should reflect any out-of-hours work undertaken on audits that improve clinical governance for their Trusts. However, in spite of all these considerations, we speculate that because trainees are only in each post for no more than 4 months during their foundation years, and with the restriction of working hours, the expectation of foundation year trainees to have undertaken and properly understood an audit cycle, implemented change and closed the audit loop is unrealistic. It would be more helpful to the trusts and trainees for audits to be part of the specialty training programme onwards, where trainees stay in a department for a longer time even as they move from one team to another. Further studies might consider in detail the difficulties in each step of the audit cycle15 and explore: Foundation Trainees’ use of the audit department; guidance from senior members of staff; and perceived benefits in clinical practice. Ultimately, audits must implement change17 and all truly successful clinical audits should aid in some way to achieving our fundamental goal in medicine; that being the best clinical practice and best quality of care.
Implantation of prosthetic mesh in repair of different hernias has gained a global acceptance and popularity. It is thought to be a potent safeguard against recurrence of hernias 1, 2.The use of prosthetic mesh in different types of hernias has brought a phenomenal change in the out look of hernia patients all over the world 3. Today, an ever increasing number of hernias are repaired by implanting prosthetic meshes either by conventional open method or by laparoscopic approach 4. Beside its well known advantages and global acceptance in every day hernia surgery, a number of complications are thought to be associated with the use of mesh in different types of hernias 5-15. We present our experience of mesh related complications in different open hernia repairs and their management in this study.MARERIALS AND METHODSIt’s a descriptive observational study over 5 years during which a total number of 1008 patients with different types of hernias were repaired electively in a teaching hospital as well as in private hospitals by the same surgical team. Of these, 638 (63.29 %) hernias were repaired by implanting prolene mesh of different sizes depending on the size of the defect. A drain was left in place in selected cases .The patients were followed up to a period of three years after discharge from the hospital. The follow up visits were scheduled at 1 month, 6 months, and then yearly. Of the total patients , 432(67.71%) were followed up to three years while 159 (26%) patients were lost in the follow up from day of discharge from the hospital. Another 47 patients attended follow up up to 2 years only and then disappeared. Sixteen of these patients continued to complain about chronic pain and foreign body sensation up to two years and then they did not return while 4 of these patients developed recurrent hernia in one year time but they were lost in follow up. The data of every patient is recorded on a proforma and their follow up records are maintained. The variables studied included immediate, early and late post-operative complications in addition to the demographic details. The statistical analysis of the data is done on SPSS version 12.RESULTSThe mean age of the patients is 41 years with a range of 73 years and a STD of 19.089. There is a male dominance (N=531, 83%) over females (N=107, 17 %). The commonest type of hernia in this series is inguinal hernia (n=518, 81%) followed by Para-umbilical hernia (n=83, 13 %). Distribution of different varieties of hernias among male and female study population is shown inTable-I. Table-1. Frequency of hernias and distribution among males and females
Type of hernia
Total
Inguinal
Para- umbilical
Incisional
Epigastric
Male
518
4
3
6
531
Female
0
79
26
2
107
Total
518
83
29
8
638
Of the total number, 34 (5 %) hernias were recurrent hernias including 21 inguinal hernias, 11 Para-umbilical hernias and 2 Incisional hernias. The patients were operated after preliminary investigations and medical fitness. All the patients were operated by open conventional technique regardless of the type of hernia. Total duration of operation is shown in Figure -I with maximum patients (467, 73%) operated with in 60 minutes. Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation
Type of hernia
Complications during same hospitalization
Total
Wound infection
Reaction
Mechanical failure
Seroma
Pain
Mesh infection
Hematoma
Inguinal
14
3
4
7
1
1
3
518
paraumbilical
5
1
2
3
0
3
3
83
Incisional
0
0
0
1
0
2
1
29
Epigastric
0
0
0
0
0
1
0
8
Total
19
4
6
11
1
7
7
638
Wound infection has an alarmingly high incidence in our series (n=19, 3 %). Most of these infections are superficial and effectively controlled by intensive antibiotic therapy so that the failure of repair is saved and mesh rejection prevented effectively. Four of recurrences occurred during 2 years follow up but patient discontinued follow up afterwards. Remaining 07 recurrences occurred between 24 to 36 weeks. The complications observed during the follow up period of up to three years in different hernias are shown in Table-III.Table-III Type of hernia * Late Complications after discharge Cross tabulation
Complications after discharge
Total
Type of hernia
Pain
Recurrence of hernia
Thickening of spermatic cord
Testicular atrophy
Inguinal
10
4
7
2
518
paraumbilical
2
7
2
0
83
Incisional
2
0
0
0
29
Epigastric
1
0
0
0
8
Total
15
11
9
2
638
A remarkably low incidence of wound infection in para-umbilical and incisional hernia is attributable to the placement of suction drain which prevents hematoma formation and secondary infection. Seven (2%) recurrences occurred in para-umbilical hernias where suction drain did not work. Mesh infection with massive reaction , although, treated conservatively in 5 patients with vigorous antibiotic therapy led to the formation of a weaker scar which later on gave way and recurrence of hernia occurred. Follow up was not 100% and about 26% patients were lost in the follow up. Majority of the patients (n=457, 90 %) were discharged within 4 days while patients who were complicated had a longer stay up to 15 days (P <0.001). Late complications were mostly chronic pain and foreign body sensations with 2 cases of unilateral testicular atrophy. DISCUSSION A number of non-infectious and infectious complications are attributed to the use of mesh in the repair of most of the hernias5, 13, 16. The type of mesh as well as their composition seems to affect complications following their use and specific materials are related to specific complications. We present 638 patients of different types of hernias repaired by implanting polypropylene mesh of varying sizes depending upon the size of defect. Prolene meshes are monofilaments, non-absorbable, inert, sterile and porous synthetic materials commonly used for this purpose. The use of mesh in hernia repair has brought a phenomenal change in the overall outcome of hernia repair especially in terms of recurrence of hernia 17. We experienced wound infection as the commonest complication in our series (n=19, 3%) and this was more so in the inguinal hernias. Most of the wound infections are superficial and very easy to control on conservative measures. On the contrary deep seated mesh infections are always dreaded complications and if not treated vigorously can lead to total failure and rejection of prosthetic mesh. A number of similar studies have reported an increased infection rate in mesh hernia repair testifying our results 18-28. Grant AM 29, however claims no difference in the incidence of infection between mesh and non-mesh repair of groin hernias. A severe local reaction occurred in 4 (0.62%) patients which resolved in few days without any consequences. Seroma and hematoma occurred in 11(2 %) and 7(1.09%) patients respectively. Only 3 seromas and one hematoma needed evacuation. We report a recurrence of 11(2 %) hernias of which 4 are inguinal and 7 are para-umbilical hernias. All of the recurrent para-umbilical hernias had severe reaction and wound infection in the post-operative period which was effectively controlled by vigorous antibiotic therapy and local wound care. There is probably a weaker scar after resolution of the infective process which resulted in recurrence. A significantly low recurrence rate in inguinal hernias in our study (0.77%) is consistent with the results of other similar reports 30-32. Chronic pain and a foreign body sensation poses a real problem and though it occurred in only two cases but a similar study by Bay-Nielsen M 33 claims 22.9% study population having chronic pain and more so in the adult males. CONCLUSION Although mesh repair is an efficient method of hernia repair, a number of complications may be associated and can lead to failure. An aggressive antibiotic therapy and wound care may control even massive infections.
Good Medical Practice describes the professional behaviour expected of doctors and advocates that it should be taught as well as assessed. GMC’s Good Medical Practice specifies the standards of team working, communication skills, accessibility and trustworthiness in relation to professional behaviour1. Ramsden2 stated that: “the students will learn what they think they will be assessed on, not what is in the curriculum, or even on what has been 'covered in class'.” Hence, if the intended learning objectives are to improve professional behaviour and team working in a trainee doctor, then a tool that assesses these characteristics along with providing suggestions for improvement is critical. Multisource Feedback (MSF) is a formative assessment tool that was designed to assess professional behaviour and attitudes, with the aim of continually improving an individual’s team working. Team Assessment of Behaviour (TAB) is an assessment tool for MSF (Appendix 1), and is one of the 2 assessment tools used to assess professional behaviour of foundation doctors in training in the UK, the other being the Mini-Peer Assessment Tool (mini-PAT)3. Our aims for this article were to evaluate whether the format of TAB allowed the MSF process to occur as originally intended, along with looking at possible barriers that may have to be overcome to make it an effective tool. A literature review was carried to appraise the present evidence regarding TAB as an assessment tool and only studies which had relevance to MSF/TAB were included in the study. As TAB is a relatively new tool, there were very few papers’ exploring this is depth which was a major limitation. Hence in the barriers section, we have discussed the possible obstacles to the whole MSF process rather than just TAB. Background The concept of MSF was originally developed by industrial organisations and has been used in postgraduate medicine in USA for assessment of professional behaviour since the 1990’s4,5. Ramsey6 suggested that it is feasible to obtain assessments from professional associates of practicing physicians in areas such as clinical skills, humanistic qualities, and communication skills. TAB was developed by educationalists and senior doctors at the West Midlands deanery7,8,and has undergone extensive field testing among 171 trainees, with analysis of received feedback from 1378 assessments across four different hospitals in the West Midlands. It is currently being used in the West Midlands Deanery for the multisource feedback of foundation programme trainees. Process of TAB The primary aim of TAB as an assessment tool is to identify trainees whose professional behaviour does not meet GMC requirements for good medical practice, so that appropriate action may be taken and also to compliment those trainees who receive good reports. For TAB, up to 10-15 multi-disciplinary colleagues of a doctor assess his/her workplace behaviour. It assesses four domains of professional behaviour: professional relationship with patients, verbal communications, team-working and accessibility. It is the initiative of the trainee to distribute at least 15 TAB forms to peers of their own choice and a minimum of 10 completed forms are required to be returned. The raters should include at least three other doctors including a consultant supervisor and at least five allied healthcare professionals. It’s the responsibility of the educational supervisor to collate and summarise these forms, identifying perceived weaknesses, offering them feedback and directed learning objectives to address any issues. Critique of TAB:1. Validity and reliability of TAB:Validity is a demonstration that a particular instrument can in fact measure what it purports to measure9. TAB portrays face as well as content validity as it assesses areas identified by the GMC1 for good professional behaviour. It is shown to be capable of identifying problem behaviour in trainees, which was the primary aim of the tool7. This tool appears to have good construct validity as it is testing trainee’s behaviour in real life situations. It is difficult to define the predictive validity of any tool, more so in a formative assessment tool. The developers of TAB have not tested for concurrent validity. The concurrent validity for TAB could have been tested by using another MSF tool in addition to TAB for some participants during the field-testing for reliability and validity of the tool. A reliable instrument for a piece of research will yield similar data from similar respondents over a period of time9. Whitehouse7 demonstrated in the pilot study that TAB had intra-observer reliability and inter-observer variability. For inter-observer variability, the Royal College of Psychiatrists compiled a map of assessment programmes against good medical practice domains and considered it appropriate for assessing four domains: good clinical care, working with colleagues, probity, and health11. 2. RatersRamsey et al5 concluded that, with MSF, 10-11 responses per physician were necessary to achieve a generalisablity coefficient of 0.70. Wood et al11 concluded that eight raters were sufficient for a representative score in their study on Obstetrics & Gynaecology trainees in the UK. Obviously more raters would lead to better coefficient and more generalisable results. TAB presently advocates at least ten raters to achieve reliable results.3. Feasibility TAB has four domains and a three point rating scale which are relatively easy to understand and complete. There is no training required for raters and usually takes less than five minutes per assessment per assessor. The paper-based system demanded considerable administrative resources, and therefore a web-based TAB assessment form was successfully piloted in the West Midlands8.4. Trainer & trainee’s evaluation of the processThe evaluation of TAB as an assessment tool was done by Whitehouse et al8 as a part of their field assessment of TAB. The assessors and trainers found the process practical, valuable and fair. 76% of the trainees who responded to the questionnaire felt that it was a useful addition to the assessment of the SHO’s. The educational supervisors had mixed views, with 77% of them finding out nothing new about the trainees. 5. Scoring systemInstead of a Likert scale, the TAB employs broad boxes which offer the rater a choice of giving specific feedback under each domain. This is more helpful to a summariser/assessor than mini-PAT, where a scoring scale is not substantiated by relevant feedback. This assessment tool does not assess clinical performance and one could argue that there could have been more than four domains in order to include other areas of performance, such as clinical skills. However having just four domains can reduce the impact of the halo effect. The halo effect12 can be defined as a rater making an overall judgement of the trainee and scoring the whole form accordingly rather than considering each domain separately. This could be a potential advantage of TAB over mini-PAT where there is no opportunity to provide specific feedback in individual domains, but rather utilises an overall action plan, which may lead to concentrating single element deficiencies while masking other shortcomings. 6. Patient OutcomesThe MSF process in itself doesn’t bear direct consequences on patients’ management, but can help the doctor improve his professionalism, which is critical element of good medical practice1. An improvement in a doctor’s behaviour secondary to the appraisal-feedback process can indirectly improve and contribute to patient management and satisfaction. Potential barriers: 1.Choice of rater:The trainee has the choice of raters, except for the supervising consultant, who must be involved in the process. This is a potential area of difficulty, as the trainee might pick individuals who are more sympathetic to their cause, or who cannot comment much on their interpersonal behaviour, thus leading to skewed results. Kuzmits13 showed that both rater and those being rated needed to be trained to make the rating and feedback process more effective, but this is not felt necessary for TAB. There is also a potential conflict between being a trainer and assessor, and this conflict might lead to clouding of judgement14, which can be addressed by having different assessors and trainers, but considering the service pressures in the NHS, this may not always be possible. 2. Feedback:The value of the MSF process can be limited by the quality of feedback provided to the trainee at the end of the process and depends on the relationship of the trainee and the supervisor15. Evidence shows that non-specific feedback does little to change performance16. Whitehouse8 concluded in their initial study that TAB was able to produce descriptive feedback that was more specific and helpful than existing MSF tools. Assessors completing TAB may not give specific comments or feedback although they are instructed to give some details especially if they chose the rating of “some concern” or “major concern”. Bret and Atwater17 have shown that negative feedback can discourage individuals, and they can even react in anger. Feedback about performance must be descriptive and specific if it is to be helpful to trainees18. Hence it is the responsibility of the supervisor to give feedback which is relevant and helpful, along with creating an action plan with the trainee to address any perceived deficiencies. It must also be stressed that good performers need to be complimented, and encouraged to continue to do so. 3. Training the raters and the supervisor:The raters also need to be educated in the process otherwise they may not give reliable views about the trainee13,19. From the rater’s point of view, it would be beneficial if they were to give specific comment, in order that more relevant feedback can be provided. Most importantly, the educational supervisors who provide the feedback to the trainee can make a difference in constructing agreed learning objectives, and not demoralise the trainee with negative feedback. Kaplan20 also noted that negative feedback can demotivate individuals. Giving face to face negative feedback can be a daunting task and supervisors, if not trained in giving negative feedback may dislike doing it, and so not give properly constructed feedback. The provision of training, however, has time as well as cost implications. Conclusions TAB continues to be part of the national foundation programme curriculum and, used correctly, can serve its purposes both as a screening tool and also for the trainees to use the feedback provided to improve their interpersonal behaviour when needed. Evaluation and quality assurance of this assessment tool should be an ongoing process. More field work in relation to assessment of behaviour in relation to TAB is needed. Patient feedback could be included in TAB which can make it a more reliable tool for assessing a doctor’s behaviour.Further qualitative studies to explore the views and experiences of trainees can help to understand the barriers and attempt to improve the usefulness of the process for the trainees. There are several potential barriers which can subvert the process of MSF by using TAB, and these need to be addressed to make the assessment process more effective and efficient. KEY POINTS
MSF is designed to assess professional behaviour and attitudes
TAB along with Mini-PAT and other tools map MSF principles
The supervisor assumes a key role in giving constructive feedback without demotivating the trainee
Relevant training while giving feedback is critical to the success of MSF
Patient’s involvement in the MSF process could make it more robust.
Leg ulcers are defined as discontinuity of the epidermis and dermis in the lower limb of more than 6 weeks duration 1, 2. They are a common presentation in the elderly population and are associated with a negative impact on the quality of life of patients and they also cause a substantial burden on the health budget 3. Pathogenesis of leg ulceration is heterogeneous 4. Prevention strategies, early identification and proper management are paramount in improving quality of life of patients and reducing costs on an already strained health budget. In this article we review the prevalence of leg ulcers in the elderly people, its common causes and management.
Prevalence The estimated prevalence of leg ulcers in the UK is between 1.5 and 3 per 1,000 population 3.A studies by Moffat et al 2004 showed a prevalence of 0.45 per 1000 which is less than the previously reported figures 5. In the same study leg ulceration was found to be more common in females than males 5. In a systematic review of prevalence studies for leg ulcer, the authors also reported an increase in prevalence of leg ulcers with age and in women 6.The overall prevalence of ulcers is not affected by social class although ulcers tend to take longer to heal in lower socio economic classes 7.Quality of life Several studies have shown that patients with leg ulcers have a poor quality of life compared to age matched controls 8, 9.A systematic review of studies measuring quality of life of patients with leg ulcers showed a negative impact on several domains of quality of life 8. In most of the studies pain was shown to be the major complaint among leg ulcer patients compared to controls, with males experiencing greater pain intensity than female patients. 10, 11 Restricted mobility and sleep disturbance due to pain was also reported in other studies.12 Leg ulcer patients often complain of itchiness, odour and leg swelling 8. In one study, unpleasant odour was reported as causing social embarrassment leading to higher anxiety and depression scores as well as altered body image 12.Reduced mobility due to leg ulceration can restrict working capacity in younger patients13.A negative emotional impact on life with symptoms such as anger, depression, and social isolation was reported by 68% of patients in another study looking at impact of leg ulcers on quality of life 14. Aetiology Several factors contribute to the development of leg ulcers. However majority of ulcers are due to venous insufficiency which accounts for about 80-85% of all cases. 15, 16. Frequency of venous ulcers increases with age as a result of several factors such as immobility and venous disease15. Other risk factors for venous ulceration include obesity, previous deep vein thrombosis, thrombophlebitis, previous fracture, and varicose veins 17.Venous ulcers(also referred to as varicose or stasis ulcer)are commonly found between the malleoli and lower calf and are associated with a shallow base covered with granulation tissue and fibrinoid material, and have irregular margins 16,17. The mechanism of venous ulceration involves initial damage to valves as a result of thrombosis or valve incompetence in varicose veins leading to pooling of blood in lower limbs. Extravasation of red blood cells then follows which causes a local inflammatory reaction and collagen deposition. This impairs the healing process eventually resulting in tissue breakdown and hence ulceration16. Venous ulcers are also associated with symptoms such as oedema, eczema.Arterial ulcers form the second largest group of leg ulcers and account for about 20% of leg ulcers. Atherosclerosis and diabetes are the commonest causes of this group of ulcers. Thrombotic episodes secondary to vasculitis, thromboangitis, and sickle cell disease can also result in arterial ulcers17.Arterial insufficiency causes hypoxia, ischaemia, tissue necrosis and consequently ulceration 18.Arterial ulcers are usually found below the ankle especially on the toes. The ulcers are characteristically small, have steep edges and a dry base. Risk factors for arterial ulcers include conditions that predispose to peripheral vascular disease such as smoking, diabetes, hypertension, hyperlipidaemia and obesity 17. It is worth mentioning that diabetes causes foot ulcers via two mechanisms: ischemia and neuropathy. Neuropathic ulcers are usually found on the plantar surface of metatarsal heads or on the toes. They are a consequence of poor glycaemic control19. The risk of malignancy in chronic leg ulcers is generally believed to be small, but a study by Yang et al 1997 showed a rate of 4.4% in chronic leg ulcers. The diagnosis should be considered in patients with non healing ulcers despite optimum management 20. Chronic inflammatory conditions such as rheumatoid arthritis, inflammatory bowel diseases are also associated with leg ulceration. Rare causes of leg ulceration such as ill fitting shoes have also been reported in literature. In a study looking at complications of ill fitting footwear among 65 elderly patients, foot ulceration was reported by 15% of the patients 21. Although small, this study showed that simple measures such as appropriate foot wear may be useful in preventing foot ulcers. Table 1: summarises causes of ulcers and main characteristics of leg ulcers 16, 17
Aetiology of ulcer
Characteristics
Venous
Between malleoli and lower calf, shallow, irregular margins, granulation base. Oedema, eczema
Arterial
Painful, below ankle distal, especially toes, small, dry baseIntermittent claudication
Vasculitis
Associated with Rheumatoid arthritis, Polyarhritis Nodosa(PAN)
Malignancy
Basal cell , squamaous cell carcinoma, melanoma
Neuropathic
Common in diabetes, wet, deep, sharp borders on pressure points
Management Like all medical conditions, management of leg ulcer should include a detailed history of the onset of the problem (as well as past medical history), examination of the legs and skin, investigations and modalities of treatments. The underlying causes need to be identified as this has crucial implications for management. A medical history suggestive of venous and arterial ulcers have been mentioned above but other factors to consider while assessing leg ulcer are: general health status, cigarette smoking, nutrition, limitation to self care, pedal pulses, Ankle Brachial Pressure Index (ABPI), oedema, limb size and shape, sensation and pain (Table 2). Table 2: Assessment of lower limb ulcers
Patient
History of ulcer developmentPast and current medical problemsGeneral health statusNutritionSocial, occupationMobility problemsLimitation to self careObesityDepression
Skin changes
VenousArterialMalignantAuto immune
Vascular assessment
Pedal pulsesAnkle Brachial Pressure Index
Limb factors
OedemaCircumferencesLymphoedemaOrthopaedic problemsSensation and pain
Examination of the legs and skin identifies markers of underlying pathology. Venous disease may present with some or all of the following: brawny skin, haemosiderin staining, lipodermatosclerosis, atrophie blanche (patchy areas of ischemia),and stasis eczema, while the skin of patients with arterial disease is often shiny, hairless, pale and cool; with thickened nails and changes in foot structure. The absence of venous or arterial signs and symptoms raises the possibility of less common causes of ulceration like: Sun damaged skin, Bowen disease or a history of previous skin cancer treatment is an alert to a malignant lesion. Site & Appearance: Most venous ulcer occur in the “gaiter” area of the leg (i.e. area extending from just above the ankle to below the knee and tends to occur on both lateral and medial aspect of the leg), they are usually superficial with poorly defined margins. The base of the wound is usually red granulation tissue with moderate to high levels of exudates. Arterial ulcers can occur anywhere on the lower leg and may appear in the gaiter region, especially with coexisting venous disease. Many arterial/ischaemic ulcers occur over bony prominences and have a history of pressure related cause. They are often deeper with a punched out appearance and may involve structures such as muscles, tendon and bone in the base. They have sloughy, devitalized tissue in the wound base and low levels of wound exudates. Ulcers occurring in atypical site with an atypical appearance require further investigation to determine the cause. Ulcers with a violaceous (purple) border, inflammation, and extreme pain, may be related to vasculitis problem or underlying connective tissue disorder. Size: Dimensions of the ulcer should be taken at first presentation and fortnightly thereafter and recorded in the notes. This is important as it gives an objective assessment of the effectiveness of the current treatment plan, and modify as necessary22.There are a range of techniques available such as digital photography, ruler based vertical, horizontal and depth measurements and circumferential tracings of wound margins using acetate sheets over cling film .The system chosen needs to reflect consistency, accuracy, and reduced operator error, and also provide visual feedback to the patient. Pain: The level of pain associated with ulcer must be assessed on presentation and at each visit thereafter using a standardized pain scale (0-10). Pain may suggest infection or arterial disease, so careful assessment is required.Surrounding skin area should be observed for the presence of eczema, hyperkeratosis skin, maceration, cellulitis, signs of irritation and scratching which are signs and symptoms associated with underlying venous disease.Assessment should also include palpation of peripheral pulses, regular blood pressure measurement, weight (with reference to a Body Mass Index chart) as well as routine urinalysis (to screen for diabetes). Vascular Assessment: This is mainly carried out by the use of Doppler ultrasound to measure the Ankle Brachial Pressure Index (ABPI).This is mandatory and must be repeated every 3 months. All patients with a non healing wound on the leg of greater than 4-6weeks should have a vascular assessment to eliminate any underlying ischaemic disease22.The result of ABPI are used to determine the likelihood of arterial insufficiency and can be used to guide the management plan, especially in relation to healing potential, referral for vascular assessment and use of appropriate compression bandages. 23 The normal range for ABPI is 0.8-1.2. An ABPI of less than 0.5 or greater than 1.2 needs vascular opinion.Treating the ulcer Many dressing materials are available for the treatment of leg ulcers and there is no adequate evidence from clinical trials to recommend one dressing type over another, but we have to bear in mind few criteria in choosing a particular dressing. The dressing should be low adherent, cost effective and must also be comfortable as well as acceptable for the service user. The choice of product should be determined by the level of exudate. Products which commonly cause skin sensitivity such as those containing lanolin and topical antibiotics should not be used on any service user22. The use of white soft paraffin has been identified as a potential fire hazard risk, hence a water based emollient should be considered as an alternative to a paraffin emollients e.g aqueous cream. Please note water based emollients are not as effective in providing sustained emollient therapy as an ointment and also contain preservatives, which are known potential irritants. Other modalities of treatments of leg ulcers are described below. Compression Therapy The mainstay of treatment of any venous component to ulceration is the application of sustained, graduated compression at therapeutic level 24 .Graduated compression increases venous flow, decreases valvular reflux while walking and increases the effectiveness of the calf muscle pump resulting in a “thinning leg”. The most effective level of compression to overcome venous hypertension has been determined to be around 40mmHg at the ankle 25. Correct application of bandages is essential to avoid pressure ulceration over the bony high points and along the anterior border of the tibia. It is acknowledged that the application of compression bandaging is a specialized skill traditionally undertaken by nurses. The combination of compression bandages used to achieve compression of 40mmHg at the ankle will depend on ankle circumference, according to Laplace’s law, which states that the sub bandage pressure is inversely proportional to the circumference of the limb. A modified compression regimen is necessary when pain is present. This may be achieved by providing periods of relief until pain is controlled or removing the bandage at night when the leg is elevated. Patients with mixed arterial and venous disease may only tolerate up to 20mmHg compression to treat oedema. Bandage choices include short stretch, long stretch, multilayer systems and stockings. A Cochrane Review of compression regimens identified increased healing rates with compression compared to no compression26 . A high compression bandages were better than moderate compression bandages, and that multi-layered bandages were better than single layered bandages. Comparisons between various high compression bandages systems, e.g. 4 layer and short stretch bandages, were unable to find any difference in effectiveness. For venous ulcer with ABPI > 0.8, use 4 layer bandages as per ankle circumference below (Table 3) Ulcers with ABPI between 0.6-0.8: Reduced compression is achieved by omitting the outer cohesive bandage (e.g. Coban) Table 3: Multilayered bandage regime in relation to ankle circumference.
ANKLE CIRCUMFERENCE
BANDAGE REGIME
Up to 18cm
2 or more wool padding1 light stretch bandage(Elastocrepe)1 light elastic bandage 3a(K-plus)1 cohesive bandage 3b(Coban)
Once the ulcer site is well healed, continue with the compression bandages for at least 4 weeks and then maintain compression at a slightly lower level indefinitely as tolerated. It must be replaced annually. Other factors to consider and deal with include: Infection This requires regular cleansing, more frequent changes of dressing (especially if exudates levels are high), topical antimicrobial dressings or systemic antibiotics. Pain Ranging from simple analgesia to potent opioid (depending on severity of pain), non steroidal anti inflammatory drugs may be beneficial. For neuropathic pain, amitriptyline can be started which can be replaced by gabapentin if no improvement. The dose can be titrated upwards. Pressure: Requires pressure relief for the ulcer to heal especially over bony prominences. Larval Therapy Larval therapy has been used for debridement of wounds for many years.27 Debridement is an essential component of wound care as the presence of devitalized tissue can impede the healing process. While the exact mechanism of larval therapy remains unknown, it encompasses three processes: debridement, disinfection and promotion of healing. The beneficial effects of larval therapy were first observed during the Napoleonic war by Larrey, who noted that soldiers whose wounds had become infested with maggots had an improved prognosis 27. During the First World War, Baer documented the successful treatment of leg ulcers and osteomyelitis using larval therapy, and paved the way for further use of it by doctors of that time. However, the development of antibiotics and improvements in surgical techniques reduced larval therapy to a “treatment of last resort”, reserved for the most intractable wounds 28. The emergence of antibiotic- resistant strains of bacteria such as methicillin resistant staphylococcus aureus (MRSA) and the curiosity of researchers has prompted a resurgence of interest in larval therapy. Larval therapy has been employed effectively to treat a wide spectrum of wounds including venous and arterial leg ulcers29.Some of the benefits of larval therapy include: reduction in wound pain and odour, and promoting healing process with relatively few side effects30 .Larval therapy is also reported as being cost-effective in comparison with conventional wound dressings. The use of larval therapy often resulted in quicker healing, and a subsequent reduction of nursing time and materials30. A further advantage of larval therapy is that, as larvae are typically applied for 3 days, wounds are disturbed less frequently than conventional dressings that require changing every 1-2days.In addition to this, a further advantage is that treatment can usually be carried out in outpatient and community settings. A study at an outpatient wound clinic on chronic wounds, of varying aetiologies reported that using larval therapy resulted in a 62% decrease in need of amputation 31. Larvae offer the benefit of eliminating bacteria from the wound through ingestion and subsequent degradation within their intestinal tract. They also act to reduce bacterial activity through the production of inhibitory secretions. The most commonly mentioned disadvantage of larval therapy is the negative perception with which it is regarded by both patients and practitioners because of the unpleasant appearance. The use of “Biobags”, which completely enclose the larvae within a polyvinyl alcohol membrane, has become a popular method of improving the application of this treatment, as larvae are able to feed freely through the open cell polymer. Pain has occasionally been reported by patients, the cause may be the sharp mouth hooks and spicules with which larvae anchor themselves onto tissue. A case history has suggested larval therapy to be contraindicated with fistulae, exposed wounds connecting to vital organs32 because bloodstream infections have been reported with some larvae33.Alteration of the disinfection process appeared to eliminate this problem, and with no further cases of sepsis occurring during the subsequent 12 months The risk of cross-infection by escaped larvae may be greatly reduced through careful dressing. Vacuum Assisted Closure therapy Vacuum Assisted Closure (VAC) therapy involves the application of controlled negative pressure to wounds 34. Negative pressure, as a method of management for difficult to heal wounds, was initially explored in 1970, with the first wound drainage system being introduced in 1989. The use of negative pressure to heal wounds, however, is more commonly associated with the work of Argenta and Morykwas in 1997.35 VAC therapy was designed with the aim of improving healing, decreasing morbidity, and decreasing the cost and length of hospital stay in patients with chronic, non healing wounds. VAC therapy promotes healing in several ways. Firstly, the foam dressing, in combination with adhesive tape, creates an occlusive dressing. This alone prevents dessication and increases the rate at which epithelial tissue is developed, therefore aiding healing times. Occlusive dressing prevents an increase in infection. Secondly, the suction effect and the mechanical forces generated at the interface of the foam work to decrease interstitial fluid accumulation, control wound exudates, stimulate granulation tissue formation, reverse tissue expansion, decrease bacterial colonisation and increase blood flow and dermal perfusion. In summary, VAC therapy aids wound healing by: Maintaining a moist environment Increasing local blood flow Removing wound exudates Promoting granulation tissue formation Reducing infection Exerting mechanical pressuresVAC therapy is suitable for the following wound types/processes 36 Acute (trauma, burns) Chronic (pressure sores, leg ulcers, diabetic ulcers) Surgical (skin grafts, flap surgery, wound bed preparation) Salvage (wound dehiscence, wound infection, post operative sternum infections) Contraindications to the use of vacuum therapy include: wounds with untreated osteomyelitis, grossly infected wounds, when necrotic tissue is present or when there is unspecified disorder of the blood. VAC therapy should also not be used in wounds with malignancy .Dressings should not be placed over any exposed vessels or organs and VAC therapy should be used with caution in patients with active bleeding, difficult wound haemostasis and in patients taking anticoagulants. Skin grafting Skin grafting is the transplanting of skin, and, occasionally, other underlying tissues to another location of the body. It is the only means of reconstructing a defect in the skin, regardless of the cause of the defect 37. Generally, skin grafting is used when, in the opinion of the reconstructive surgeon, other methods of reconstruction such as primary closure, secondary intention healing, or local skin flap are inappropriate, are unavailable or would produce a suboptimal result. Skingraft are divided into 2 major categories: full thickness skin graft (FTSGs) and split thickness skin graft ( STSGs).STSGs may be subdivided into thin (0.008-0.012mm),medium(0.012-0.018mm) and thick (0.018-0.030mm)grafts 37. STSGs are the one used in covering chronic unhealing cutaneous ulcer. Split skin grafting is technically demanding and requires hospital admission25. The discharge from the surface of venous ulcers tends to dislodge continuous sheets of split skin, leaving a choice between mesh and pinch skin grafting. Pinch skin grafting provides epithelial islands, from which epithelial growth may spread outwards as well as inwards from the ulcer margin. Pinch skin grafting has been done by district nurses in the community and has been found to be cost effective accelerating healing when used with multilayer compression bandaging.25 Some contraindications to the use of skin graft generally include: vascular tissues such as exposed bone or cartilage (as this will lead to graft necrosis), uncontrolled bleeding of the recipient because of haematoma and/or seroma formation under the graft compromises graft survival. Venous Surgery Superficial venous surgery has been shown to improve ulcer healing in patients with only superficial venous incompetence38. In patients with no deep reflux on duplex imaging, superficial venous surgery has been shown to reduce long term ulcer recurrence25 . Indications for superficial venous surgery are:
Patient fit for surgery
Sufficient mobility to activate calf muscle pump
Prepared to attend hospital for investigation and surgery
Obesity controlled (BMI <30)
Superficial venous incompetence
There are few other modalities of treatment of leg ulcers currently in use, although no strong evidence has been found to show they really improve healing. Intermittent Pneumatic Compression Intermittent pneumatic compression (IPC) is a mechanical method of delivering compression to swollen limbs that can be used to treat venous leg ulcers and limb swelling due to lymphoedema.It uses an air pump to inflate and deflate an airtight bag wrapped around the leg.39 However, review of trials found conflicting evidence about whether it is better than compression bandages. It may increase healing compared with no compression but it is unclear whether it improves healing when added to treatment with bandages. Electromagnetic Therapy Electromagnetic therapy involves the use of electromagnetic, microwave, or infrared energy to diagnose or treat an illness by detecting and correcting imbalances in the body's energy fields. Electronic devices that emit some form of low-voltage electrical current or radio frequency are often involved. It has been used in the treatment of chronic diseases like venous leg ulcers. Cochrane wound group conducted trials on several occasions comparing electromagnetic therapy with other treatments and up till now, there is no reliable evidence of benefit of electromagnetic therapy in the healing of venous leg ulcers.40 Further research is still needed.Oral Zinc Supplement Leg ulcers may take long time to heal despite good wound care. This may be due to poor nutrition which reduces the ability of the body to repair itself. Minerals such as zinc are necessary for good healing and so it has been thought that taking zinc sulphate tablets might aid healing of ulcers especially if patients were found to have low baseline Zinc level. Few trials were found where zinc was used to treat leg ulcers but all were too small to pick up on any benefit, if such a benefit exists. In addition, the quality of those trials was mediocre. On the basis of the evidence available so far, it appears that taking zinc tablets does not improve leg ulcer healing, however more good quality trials are needed.41Laser Therapy Low level laser therapy (LLLT) refers to the use of red beam or near infrared laser with a wavelength between 600and 1000nm power from 5-500 milliwatts.It is also referred to as cold laser therapy, low power laser therapy (LPLT), low intensity laser and low energy laser therapy. The exact effect of its mechanism is unknown; however, hypotheses have included improved cellular repair and stimulation of the immune, lymphatic and vascular system. Several randomised controlled trials involving patients with venous ulcers failed to demonstrate any significant benefits of LLLT when compared to standard treatment methods or placebos.42Hyperbaric Oxygen Therapy Oxygen is one of the most versatile and powerful agents available to the modern medical practitioner. The therapeutic use of oxygen under pressure is known as hyperbaric oxygen therapy (HBO2) and has been used to assist wound healing for almost 40 years. HBO2 has several specific biological actions which can enhance wound healing processes .These include: Hyper-oxygenation of tissue, vasoconstriction, down regulation of inflammatory cytokines, up-regulation of growth factors, antibacterial effects, potentiation of antibiotics, and leukocyte effects.43 Systemic oxygen can be administered via 2 basic chambers: Type A( multiplace) and Type B(monoplace). Both types can be used for routine wound care, treatment of most dive injuries, and treatment of patients who are ventilated or in critical care.HBO2 is a relatively safe non-invasive therapy. Side effects include middle ear and pulmonary barotraumas and myopia. Contraindications include poor cardiac output and severe obstructive pulmonary disease. Conclusion In this article, we have been able to show that leg ulcers are a common presentation in the elderly population and have negative impact on the quality of life of affected patients. It has been found to be more common in females. Most leg ulcers (about 80-85%) are caused by venous insufficiency, followed by arterial ulcers. A comprehensive assessment of the patient, skin, vascular status, limb and ulcer is required to determine aetiology and to formulate an appropriate management plan as described above. Several researches are still going on other modalities of treatment of leg ulcers. However, all patients should be provided with both verbal and written information to help them understand their condition and treatments they receive, as this will enable them to better understand their conditions, and will support concordance between patients and staff.
Emergency contraception (E.C) is also known as post-coital pill (PCC) or ‘the morning after pill’. It is the provision of preventing the establishment of a pregnancy following either an unprotected sexual intercourse or a potential contraceptive failure (1). Patients presenting to a general practitioner asking for emergency contraception should be seen and treated the same day. All the reception staff working in a surgery should be trained and patient requesting a PCC over the phone should be fitted in the surgery the same day.Teenage pregnancy is a public health priority (2) and government targets have been set to half the rate of conceptions in people under the age of 18 years in England by 2010 (3).Most people begin to consider sexual activity in adolescence(4).This is a period of psychological maturation.The UK has a higher teenage birth rate in Western Europe (5).About 90,000 teenagers in England become pregnant, resulting in 56,000 live births. Of these 2,200 are to girls aged 14 or under and 7,700 are to under 16 years age.There is a need to improve the provision of emergency contraception (6), but access to the service with in 72 hours can be difficult for young girls who may be worried about the confidentiality (2).
WHEN NEEDED
Emergency contraception is needed either because of split or slipped durex or a potential contraceptive failure e.g. late starter of the contraceptive pill on top of usual seven day break, forgetting to take the pill because of excessive alcohol intake or not taking precautions if vomiting/diarrhoea or antibiotic usage. Missing more than one pill in the first week of the pack could be another reason.Young women for whom sexual intercourse is often unpremeditated and therefore unprotected represents one of the most important groups requiring emergency contraception (7).
HISTORY
Before issuing a prescription, an accurate history to assess the risk of a pregnancy and whether an emergency contraception is needed must be taken (2).There may be a significant age difference between the patient and the partner or there could be an issue of abuse. General practitioner must have an access to local and national child protection guidelines. An accurate history of last menstrual period, usual cycle, date and time of last unprotected sexual intercourse and whether she has had other episodes of UPSI during that cycle should be recorded. History of current medication—enzyme inducing drugs e.g.antiepileptics, St John’s wort which could reduce the efficacy of E.C. should be taken.The only absolute contraindications are pregnancy or a history of serious allergy to any ingredient of the medication.Acute intermittent porphyria, severe liver disease, venous thromboembolism on anticoagulants, breast cancer is some of the relative contraindications.
EXAMINATION
Physical examination should include measurement of height, weight, and blood pressure. A routine urine check for protein & sugar should be done. Advice and help regarding smoking, alcohol and drugs should be given if needed. A pelvic examination is only necessary if an infection is suspected or if the IUCD method is used.
TREATMENT
Two methods are available in the UK-
1) Hormonal method. This contains 1.5 mg of Levonorgestrel (LNS) and is given as a single dose as soon as possible after an UPSI. This is available on the prescription as Levonelle 1500 or as purchase by women over sixteen at pharmacies as Levonelle One Step, both by Schering Health UK. Only those pharmacists who have undertaken training and signed Patient Group Direction (PGD) can dispense the pill.
The sooner it is taken, the greater the efficacy
0 - 24 hours 95% efficacy
25 – 48 hours 85% efficacy
49 -- 72 hours 58% efficacy
It is licensed to be prescribed with in 72 hours of UPSI, although it is known to have some efficacy for up to 120 hours but effectiveness decreases the longer the delay. It acts by interrupting the follicular development and ovulation. There is no effect on implantation. Side effects with E.C are rare. Nausea is reported in 15% of cases and vomiting in 1-2 % cases. If vomiting occurs with in two hours of taking the pill, the patient should return for a repeat dose of Levonelle 1500(1).Irregularity of cycle is another side effect.50% of women reported bleeding a few days earlier or later than expected and 16% had bleeding unrelated to menses within the next seven days (8). Cramps, headaches, dizziness and breast tenderness could be some other side effects. Because this is a progestogen, the oestrogen related cardiovascular risks are not a concern.
2) Copper containing IUCD (not Mirena). This is more effective and prevents nearly 100 % of pregnancies. It has both pre and post ovulation effects .The toxicity of copper prevents fertilisation. If inserted later in the cycle, it causes an inflammatory reaction in the endometrium; preventing implantation (9).It can be inserted with in five days (120 hours) after UPSI. If intercourse has occurred more than five days previously, an IUCD can still be inserted up to five days after the earliest likely calculated ovulation. Before inserting the coil a pelvic examination and swabs should be taken to exclude sexually transmitted diseases. If patient is at a risk, treatment with 1 Gm, Azithromycin should be given. Absolute contraindications to the coil insertion are few and same as to the routine use of coil. This is a better option if patient is taking enzyme inducing drugs such as antiepileptic or St John’s wort.
FOLLOW UP
All patients should be followed up in three or four week time after prescribing a PCC or the coil insertion.
No emergency contraception is 100% effective. Pregnancy should be excluded by doing a pregnancy test if period is late by one week or more. If patient is pregnant various options regarding termination/continuation/adoption should be discussed.Regular methods of contraception should be discussed and advice should be given regarding safe sex. If indicated screening for STD should be done. A general practitioner can do a lot to reduce the burden of STI. Chlamydia screening in England varies from area to area. One can visit www.chlamydiascreening.nhs.uk to find out what is happening in one’s practice area. NICE and the national Collaborating Centre for women and children’s health have produced a guideline recommending that Long Acting Reversible Contraception (LARC) should be offered to all women as part of their contraceptive choices after emergency contraception.
CONCLUSION
There is an increased awareness of emergency contraception although the confusion exists particularly among those aged 16-20 years regarding the time limit for its effectiveness. Every GP practice should have a practitioner with an interest in family planning and sexual health or a family planning trained nurse.
Spasticity is a common symptom seen as a consequence of an injury to the brain (stroke, trauma, hypoxia, infection, cerebral palsy and post surgery), spinal cord injury or multiple sclerosis. It is a complex problem, which can cause profound disability alone or in combination with other features of upper motor neuron syndromes (figure 1). The word “spasticity” is derived from the Greek word “spasticus”, which means “To pull or To Tug”. Spasticity is defined1 as “Disordered sensori-motor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles”. Simply stated, spasticity is stiffness of muscles that occurs after injury to the spinal cord or brain. Awareness of the implications and associated symptoms can minimise development of long term secondary complications (table 1). The impact of spasticity can be devastating. If not managed early and appropriately it may result in progressive disability, resulting in secondary complications such as contractures and pressure sores. This significant impact has ensured that spasticity management is a prominent feature in the national management guidelines for long term neurological conditions, promoting coordination of care between primary, secondary and social care providers. Symptoms Spasticity can range from mild muscle stiffness to severe, painful and uncontrollable muscle spasms. It is associated with both positive and negative components of upper motor neuron syndromes. Positive components include muscle overactivity, flexor and extensor spasm, hyperreflexia, athetosis, spastic dystonia, clonus, and an extensor plantar response. Common negative symptoms comprise weakness/ paralysis, early hypotonia, fatigue and loss of dexterity. Spasticity can be distinguished from rigidity by its dependence on the speed of muscle stretch and characteristic distribution in antigravity muscle groups. Spasticity does not always cause harm and can occasionally assist in the rehabilitation process by enabling a patient to stand when their limb weakness would not otherwise allow it Table 1 Clinical and functional problems associated with severe Spasticity
Physical
Emotional / social
·Non- specific pain·Discomfort·Painful muscle spasm·Difficulties with activities of daily living. e.g. washing, dressing, eating, toileting, maintaining hygiene, sexual activity·Problems with posture and mobility·Physical deformity and longterm contracture·Pressure ulcers
·Emotional e.g. low mood, distorted self image, impaired motivation·Impact on fulfilment of life roles as a partner or a parent·Sleep disturbance – due to pain and discomfort·Vocational- impact on employment or education·Social isolation – due to restricted mobility
Figure 1 Vicious cycle of spasticity Assessment of spasticityBefore any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale
4 Rigid extremity 3 Loss of full joint movement, difficult movement, considerable tone2 Full joint/ limb movement, but more increase in tone, limb still easily moved.1+ Slight increase in tone, catch and resistance through out range of movement1 Slight increase in tone, catch or minimal resistance at end of range of movement0 no increase in tone
It is also important to remember that not every “tight” muscle is spastic. The clinically detectable increase in muscle tone may be due to spasticity, rigidity or a fixed muscle contracture.Management The key to successful spasticity management is education of the patient and carers with both verbal and written information. This allows them to understand, appreciate and be fully involved in the management plan. All patients with spasticity should be followed up by a coordinated multidisciplinary team, which allows more timely intervention and close monitor of the progress. Liaison between health and social services in both primary and secondary care is essential in long term management. This helps to deliver a more consistent approach to the individual over time (figure 2). Table 3 Aims of spasticity management.
1.Improve function- mobility , dexterity2.Symptom relief-· Ease pain- muscle shortening, tendon pain, postural effects· Decrease spasms· Orthotic wearing3. Postural- Body image4. Decrease carer burden- Care and hygiene, positioning, dressing5. Optimise service responses- to avoid unnecessary treatments, facilitate other therapy, delay/prevent surgery
The first step in the management of spasticity is to identify the key aims and realistic goals of therapy. Understanding the underlying pathology and possible prognosis is helpful in planning these goals (table 3). Other key points to consider are: · Identification and management of any trigger or aggravating factors-Initial assessment should exclude any co morbidity that may worsen spasticity such as pressure sores, chronic pain, infection (commonly urinary tract infection), constipation or in-growing toe nails.· Instigation of an effective and realistic physical programme including attention to posture and positioning Figure 2 Approach to spasticity assessmentComprehensive assessment of spasticityRecognition of underlying provocative factorsImpact on the individualMeasurement of spasticityPotential goals- individualised and person focussed Initial approachEducation to patient/ and their family /carersMultidisciplinary team assessmentIdentification of clear treatment goalsEstablish mechanism for monitoring and review Management Manage triggering factorsBalance between positioning and movementPosture and seatingPhysical therapy and active exercise programmeSplinting and use of orthoticsPharmacotherapy A) Physical modalities· Stretching- this intervention has the benefit of being benign and non-invasive. Maintaining muscle length through passive or active exerciseand stretching regimens including standing or splinting canbe key to managing spasticity both in the short and the longterm.· Cooling of muscles- this inhibits mono synaptic stretch reflex and lowers the receptor’s sensitivity, different techniques such as quick icing and evaporating spray like ethyl chloride are occasionally used.· Heat-heat may increase the elasticity of the muscles. Techniques used include ultrasound, fluidotherapy, paraffin, superficial heat and whirlpools. These techniques should be combined with stretching and exercise.· Orthosis/equipment/ aids – an orthosis or splint is an external device designed to apply, distribute or remove forces to or from the body in a controlled manner to control body motions and /or alter the shape of body tissues. E.g. ankle foot orthosis, insoles, ankle supports, wrist/ hand/ elbow splints, knee splints, spinal brace, hip brace, neck collar. Some equipment can also aid positioning e.g. T roles, wedges, cushions and foot straps.These are usually used in combination with other modalities like botox therapy. Attention to posture and positioning, whichmay include the provision and regular review of seating systems,is paramount in managing severe spasticity· Massage– althoughvarious techniques are in use there is no evidence to support this· Dynamic physiotherapy technique- many schools of physiotherapy claim that particular technique has antispastic and functional benefits, particularly for the more mobile person. E.g. Bobath technique, proprioceptive neuromuscular facilitation, Brunnstrom technique. B) Electrical therapy· Functional Electrical stimulation –Thisis an adjunct to physiotherapythat can be of benefit to selected individuals who are predominantlyaffected by upper motor neuron pathologies resulting in a foot drop. Randomised controlled trial by Burridge et al in patients following stroke found that the use of functional electrical stimulation in combination with physiotherapy was statistically superior to physiotherapy alone3· Transcutaneous electrical nerve stimulation – this has been found to reduce spasticitythrough its nociceptive action and reduction of pain.C) PharmacologicalMedicationshould always be used as adjunct to good general management and education. Identification of treatment goals will help optimise drug therapy not only in terms of choice of agent, but also in timing and dose. Aims of medication should be to improve function or relieve troublesome symptoms rather than to simply reduce the degree of spasticity. Table 4 Useful things to remember to optimise medication effects
1. Clear written/verbal information for patients about effects/adverse symptoms of drugs 2. Clear treatment goals3. Detailed drug history- Review of other medication and potential drug interaction4. Appropriate form of drug e.g. liquid preparation if swallowing difficulties5. Regular review of efficacy and side effects6. Aids to help administer drugs e.g. dossette box, timer to remind7. “Start low and go slow” to avoid deleterious effects on function or unwanted side effects8. Combination of drugs to obtain synergistic action
Table 5 Different methods of delivery of medication
·Enteral – orally or via PEG e.g. baclofen, benzodiazepins, dantrolene, clonidine, tizanidine, gabapentin·Transdermal system e.g. catapress TTS·Intrathecal e.g. baclofen pump (other drugs used alone or in combination intrathecally include clonidine, morphine, fentanyl, midazolam, lidocaine)·Intra muscular/ focal injection e.g. botulinum toxin·Nerve blocks e.g. Phenol, Ethanol
The oral agentsAlthough different categories of drugs are available, those most commonly used to treat spasticity are baclofen,tizanidine, benzodiazepines, dantrolene, and gabapentin4, 5, 6. Different agents act through different mechanisms (table 6 and 7) for e.g. GABA-like (baclofen, benzodiazepine), central alpha 2 agonists (tizanidine, clonidine) and peripheral anti-spastics (dantrolene). Antispastic drugs act in the CNS either by suppression of excitation (glutamate), enhancement of inhibition (GABA, glycine) or a combination of the two. Table 6 Mechanism of action of commonly used oral antispasticity medication
Drugs acting on
Drugs
GABA- ergic system
baclofen, benzodiazepines, piracetam, progabide
Ion flux
dantrolene sodium, lamotrigine, riluzole
Monoamines
tizanidine, clonidine, thymoxamine, beta blockers, and cyproheptadine
Excitatory amino acids
orphenadrine citrate, cannabinoids, inhibitory neuromediators and other miscellaneous agents.
Baclofen remains the most commonly used anti-spastic agent. The preferential indication is spasticity caused by spinal cord disease especially in multiple sclerosis. Many studies including the pilot study by Scheinberg et al 7 demonstrated that oral baclofen has an effect beyond placebo in improving goal-oriented tasks (such as transfers), in children with spastic quadriplegic cerebral palsy. In open-label studies of oral baclofen, the drug improved spasticity in 70-87 per cent of patients; additionally improvement in spasms was reported in 75-96 per cent of patients. In double-blind, crossover, placebo-controlled trials, baclofen was reported to be effective, producing statistically significant improvements in spasticity8.The main adverse effects of oral baclofen include sedation or somnolence, excessive weakness, vertigo and psychological disturbances. The incidence of adverse effects is reported to range from 10 to 75 per cent. The majority of adverse effects are not severe; most are dose related, transient and/or reversible. The main risks of oral baclofen administration are related to withdrawal; seizures, psychic symptoms and hyperthermia. These symptoms improve after the reintroduction of baclofen, usually without sequelae. When not related to withdrawal, these symptoms mainly present in patients with brain damage and in the elderly. The limited data on baclofen toxicity in patients with renal disease suggest that administration of the drug in these persons may carry an unnecessarily high risk. Tizanidine is an efficient and well tolerated antispastic. It is predominantlyan alpha 2 agonist and thus decreases presynaptic activity of theexcitatory interneurones. There is a large body of evidence for the effective use of tizanidine monotherapy in the management of spasticity 15. Tizanidine is the antispasticity drug that has been most widely compared with oral baclofen. Studies have generally found the two drugs to have equivalent efficacy, although tizanidine has better tolerability; in particular weakness was reported to occur less frequently with tizanidine than with baclofen.Dantrolene has a peripheral mechanism of action and acts primarily on muscle through inhibitingcalcium release from the sarcoplasmic reticulum. It decreasesthe excitation–coupling reaction involved in muscle contraction and can be prescribed in the different forms of spasticity. The efficacy of benzodiazepines (diazepam, tetrazepam, clonazepam) is comparable with baclofen. Although there is no evidence to suggest any difference in effectiveness between them, diazepam and dantrolene are associated with more side effects than baclofen and tizanidine. There are other compounds with anti-spastic properties (gabapentine, cyproheptadine, piracetam). Their advantage is
Table 7
Drug
Dosage
Doses per day
Mechanism of action
Common side effects
Initial dosage
Maximum dosage
Baclofen
5mg x3
90mg
4
GABA ergic
Seizure, Sedation, Dizziness, GI disturbances, psychosis, Muscle weakness
rather limited when used alone. Generally, they are administrated in combination with usual anti-spastic drugs. A few short term trials have trialed gabapentin with good results 19 .Pregabalin may be of value as a systemic agent in the treatment of spasticity, although properly controlled studies with clearly defined outcome measures are required to confirm this finding 22. The Sativex Spasticity in MS Study Group23 concluded that oromucosal whole plant cannabis-based medicine (CBM) containing delta-9 tetrahydrocannabinol (THC) and cannabidiol (CBD) may represent a useful new agent for treatment of the symptomatic relief of spasticity in MS. Intrathecal pump· Baclofen- If oral drug treatment is inadequate in controlling lower limb spasticity or is not tolerated, intrathecal delivery of baclofen should be considered. This has been found to be a cost-effective strategy when compared to conventional medical management alone by Bensmail et al 20 .The benefits of continuous intrathecal baclofen infusion have been demonstrated in more than 80 percent and over 65 percent of patients report an improvement in tone and spasms respectively. The main risks of intrathecal baclofen infusion are symptoms related to overdose or withdrawal. These are mostly related to catheter disruption, failure to refill the pump reservoir or failure of the pump's power source. Abrupt disruption of intrathecal baclofen can be a serious scenario with continuous spasms, tremors, temperature elevation, seizure and death having been reported.· Phenol- As phenol is a destructive agent which indiscriminately damagesmotor and sensory nerves, it is reserved for those individualswho do not have any functional movement in the legs, who havelost bladder and bowel function and who have impaired leg sensation. Intrathecal phenol can be an effective treatmentwhich, though it requires expert administration, does not havethe long term maintenance or cost issues that are associated with intrathecalbaclofen treatment. The effect of a single injection often lastsmany months and can be repeated if necessary 24. D) Nerve blockPeripheral nerve blockade/ Regional blocks/ Neurolytic blockade25 are another therapeutic possibility in the treatment of spasticity. This can be done with the help of fluoroscopy or nerve stimulation. Chemical neurolysis by phenol/ alcohol is irreversible and can be used at several sites. Blocks are applied most often to 4 peripheral sites: the pectoral nerve loop, median, obturator, and tibial nerves. The main indication is debilitating or painful spasticity. Peripheral blocks with local anaesthetics are used as tests to mimic the effects of motor blocks and determine their potential adverse effects. Peripheral neurolytic blocks are easy to perform, effective, and inexpensive30.E) Botulinum toxin injectionBotulinum toxin is the most widely used treatment for focal spasticity27,28,29. The effect of the toxin is to inhibit the release of acetylcholine at the neuromuscular junction. The clinical effect of injecting botulinum toxin is reversible due to nerve sprouting and muscle reinnervation, leading to functional recovery of the muscle in a few months. It is essential that botulinum toxin injections are given in conjunction with physiotherapy in order to obtain the maximum benefit. The toxin is injected directly into the targeted muscle and an effect can be noticed from as early as 2-3 days with a maximum effect seen by about 3 weeks, lasting at least 3 months. As it is not a permanent treatment it may have to be repeated after a few months.Many randomisedcontrolled trials show that botulinum toxin is effectivein reducing muscle tone in various conditions 28, 29. Brashear and colleaguesdemonstrated a reduction in spasticity in the wrist andfingers of patients following stroke with the use of botulinum toxin, together with an improvementin their disability assessment scale29.E) Surgical techniqueMost surgical procedures are irreversible. This means that realistic goal setting between the health care provider, family and patient is critical. Neurosurgical techniques have been proven useful in conditions like cerebral palsy 32, 33.· Neurosurgical techniques- Anterior and posterior rhizotomy, peripheral neurotomy 31, Drezotomy, percutaneous radiofrequency rhizotomy, spinal cord and deep cerebellar stimulation of the superior cerebellar peduncle 32, functional neurosurgery 33· Orthopaedic procedures- directly act on muscles and tendons e.g. lengthening operation, tenotomy, neurectomies, and transfer of tendons.
Key Points to remember1.Spasticity management is more effective in multidisciplinary settings2.Early multidisciplinary approach and goal setting is crucial3.Education and clear communication between patients, carers and health care providers is essential4.Early intervention and optimal therapy prevents long term complications.5.Focal spasticity responds well to botulinum toxin injection, while generalised spasticity needs oral/ intrathecal medications
The huge disease burden and vast health inequalities and given that one in six person in the world is an Indian on the one hand, and the country’s recent economic rise and its intellectual capital in-country and also overseas on the other hand, has created the Indian conundrum for global health challenges. India is now both: the problem – as it contributes to the challenges, and the solution – if it can mobilise its resources. This short paper will expand on the theme and especially explore how the Indian Diaspora in the UK can help to ensure good health and affordable health care to the needy.
The problem: Global health challenges
The World Health Organisation (WHO) has established the ten facts on the global disease burden (Table) (1) and its 2008 report: Primary Care: Now More than Ever (2) has identified the five global challenges in ensuring health care (Box).
TABLE : FACTS ON THE GLOBAL BURDEN OF DISEASE (Source: www.who.int)
1. Around 10 million children under the age of one year die each year
2. Cardiovascular diseases are the leading cause of death worldwide
3. HIV/AIDS is the leading cause of adult deaths in Africa
4. Population ageing is contributing to rise in cancer and heart disease
5. Lung cancer is most common cause of deaths from cancer in the world
6. Complications of pregnancy account for 15% of deaths in women of reproductive age worldwide
7. Mental disorders such as depression are among the leading causes of disability worldwide
8. Hearing loss, vision problems and mental disorders are the most common causes of disability worldwide
9. Road traffic injuries are projected to rise from the ninth leading cause of death worldwide in 2004 to fifth in 2030
10. Under-nutrition is the underlying cause of death for at least 30% of children under five years of age
BOX: FIVE COMMON SHORTCOMINGS OF HEALTH-CARE DELIVERY (Source: WHO Report 2008)
1. Inverse care. People with the most means – whose needs for health care are often less – consume the most care, whereas those with the least means and greatest health problems consume the least. Public spending on health services most often benefits the rich more than the poor in high- and low income countries alike.
2. Impoverishing care. Wherever people lack social protection and payment for care is largely out-of-pocket at the point of service, they can be confronted with catastrophic expenses.Over 100 million people annually fall into poverty because they have to pay for health care.
3. Fragmented and fragmenting care. The excessive specialization of health-care providers and the narrow focus of many disease control programmes discourage a holistic approach to the individuals and the families they deal with and do not appreciate the need for continuity in care. Health services for poor and marginalized groups are often highly fragmented and severely under-resourced, while development aid often adds to the fragmentation.
4. Unsafe care. Poor system design that is unable to ensure safety and hygiene standards leads to high rates of hospital-acquired infections, along with medication errors and other avoidable adverse effects that are an underestimated cause of death and ill-health.
5. Misdirected care. Resource allocation clusters around curative services at great cost, neglecting the potential of primary prevention and health promotion to prevent up to 70% of the disease burden. At the same time, the health sector lacks the expertise to mitigate the adverse effects on health from other sectors and make the most of what these other sectors can contribute to health.
As would be expected the situation in India confirms these facts and challenges. There is a lot of health information for India in the public domain (1,3) although the nature and detail could be improved. Like in many other developing countries the life expectancy has increased and although improved health has led to further economic welfare in India, the country is currently experiencing the triple whammy of the disease burden due to communicable (CD) and non-communicable (NCD) diseases and injuries. Communicable diseases account for about 38% of the disease burden – not only are the ‘traditional’ CDs like malaria rife, the country has seen a big increase in new infections like HIV/AIDS. NCDs including diabetes, heart disease and cancers account for 53% percent of all deaths in the age group 30-59 years in 2005. It is projected that by 2015, 59% of the total deaths in India would be due to NCDs. With 47% of men and 15% of women being regular consumers, tobacco remains the single biggest preventable risk factor. Whilst the developed world is seeing a reduction in deaths due to road traffic accidents, these injuries are projects to rise by nearly 150% in SE Asia region including India. This health picture is compounded by the lower human development, largely due to poverty – a situation that has not been addressed despite recent economic successes, as bemoaned by Amartya Sen (4):
“Yet even a hundred Bangalores and Hyderabads will not on their own solve India’s tenacious poverty and deep seated inequality. The very poor in India get a small- and basically indirect- share of the cake that information technology and related developments generate. The removal of poverty, particularly of existing poverty, calls for more participatory growth on a wide basis, which is not easy to achieve across the barriers of illiteracy, ill-health, uncompleted land reforms and other sources of severe societal inequality. The process of economic advancement cannot be divorced from the cultivation and enhancement of social opportunities over a broad front. “
India’s health sector is diverse and includes not just modern medicine but also a range of traditional systems like Homeopathy, Ayurveda and Unani. The overall governmental expenditure on health has been rather low (0.9% of GDP, whilst the total expenditure is about 5%), with 75% of it being borne by patients and, over 90% of the latter being out of pocket due to a lack of organized insurance. Being sick has meant being bankrupt for a substantial number of rural poor Indians. There is a burgeoning private sector that is driving the specialist end of the provision, with rather poor and often outdated primary care services. The cost of health care keeps going up with little or no assurance that services are appropriate or safe, and the regulatory mechanisms are few. The bottom line in India is that good health happens by chance and good quality health care is a privilege and not a right.
The solution: Add value to planned developments in India
Although it may not seem like it, there is a comprehensive plan to develop national health policy and address some of the fundamental challenges, the following are some of the highlights stated by the Government (1,5):
1. “Commitment of the Government to increase public health share to at least 2% of GDP
2. Efforts to develop regulatory frameworks and options for alternative financing mechanisms including insurance
3. National Rural Health Mission and Reproductive & Child Health Programme. Integrated Management of Newborn and Childhood Illnesses (IMNCI) pre-service and home-based newborn care activities initiated. Multi-skilling of health providers for Emergency Medical Obstetric Care. Introduction of Accredited Social Health Activists (ASHAs). Increased attention to women’s health in national Schemes
4.Increased commitment to health system strengthening, use of capacities in other sectors, and effective partnerships. Enhanced nursing profile and increasing nursing autonomy in practice.
5.Public health education, job descriptions and career paths under review; expanding efforts for multi-disciplinary and multi-sectoral approaches; establishment of the Public Health Foundation.
6.Ongoing capacity building to deal with international agreements and strengthening of the World Trade Organization (WTO) cell in the Union Ministry of Health.
7.Increased commitment and investments, and significant progress in the control and/or elimination of communicable diseases like yaws, leprosy, tuberculosis and several vaccine preventable diseases.”
Overall, there is action at all levels: national, state, institutional and individual and across the range of necessary issues: policy, regulation, resourcing, provision and capacity building by both, public and private sectors. The two key questions for the Indian Diaspora, however, are:
Can we help accelerate these developments?
How can we ensure that these become sustainable?
There is no denying that many individuals from the UK have been, and continue to be, involved in various efforts back in India; be it fundraising, community development, school education or direct clinical provision. In addition, there are various organisations like BIDA, IMA and BAPIO who have potentially the infrastructure albeit their focus has largely been on activities within the UK. The UK Government has recognised its responsibility in supporting international efforts as part of the recent Health is Global Strategy (6), and this provides another timely opportunity. From both, philanthropic and business angles, it makes sense to create a robust Indo: UK collaboration around health and education given common heritage and needs and opportunities on both sides. In addition to working on discrete areas like patient safety (7) or public health capacity building (8) an important first step would be to create a mechanism for regular dialogue in order to identify and progress priority projects of mutual interest.
Conclusions
India has come a long way since its independence and given its size and complexity continues to have ongoing challenges (9, 10,11). It is essential to recognise that health is not a consumptive sector, but by creating healthy people, free from illnesses, can be a productive sector. The basic message of this paper is that being a physician in India in the 21st century is both, a privilege – given the ancient history and traditions and recent economic successes, and a responsibility- given that despite being the world’s largest democracy and an economic superpower there are vast health inequalities and lack of safe, affordable basic health care to a large proportion of the citizens in India.
At the time of writing this paper, there is intense debate about the NHS in the American press triggered by President Obama’s attempts to reform US health care. No doubt whilst things could be better in the NHS, there is still a lot that the world, both developed and developing nations, can learn from the NHS (12, 13) . Indeed best practices, regardless of whether they come from US, UK or anywhere else could, and should, be adapted to support ongoing efforts in India.
Introduction.
This legislation is based on rules established by case law about how to work with people who lack capacity (either on a temporary or permanent basis).
The Act provides a definition of capacity, a functional test for capacity (see Box 1) and a checklist for Best Interest decision making which are under pinned by five key principles (See box 2). The Act is supported by a Code of Practice.
The Act, which applies to all adults aged 16 years or over (with some exceptions), provides a clear definition of incapacity, and for deciding if a person lacks capacity in respect of a particular matter.
“A person lacks capacity in relation to a decision or proposed intervention if, at the material time, he is unable to make a decision for himself in relation to the matter or proposed intervention because of an impairment of, or a disturbance in the functioning of the mind or brain. It does not matter whether the impairment or disturbance is permanent or temporary.” (S2 (1) and (2) MCA 2005.
Box 1. Testing Capacity
The responsibility for testing capacity rests with the person who wishes to make a decision on behalf of someone who lacks capacity.
The functional test of capacity:
Does the person have an impairment or disturbance in the functioning of his mind or brain?
Does the impairment or disturbance make the person unable to
A person is unable to take a decision for himself/herself if he/she is unable to:
Understand the information relevant to that decision;
Retain that information long enough to reach a decision;
Use or weigh that information as part of the process of making the decision; or
Communicate his decision (whether by talking, using sign language, visual aids or any other means).
Box 2. Principles (based on section 1 MCA 2005)
Best interests always.
Less restrictive care provision option.
Encourage individual to make own decisions.
Eccentric decisions are OK.
Presume capacity always.
It is important to note that the decision is always ‘time specific’ and ‘issue specific’. It is also a test applied both to people with temporary or fluctuating capacity (such as people experiencing mental ill-health) and those whose decision making ability is permanently impaired (such as people with a learning disability)
The Act starts from the presumption that those we work with do have capacity, and requires staff to involve them as much as possible in their own treatment and care including when there is evidence that they lack capacity in a particular matter.
The Act also introduces a statutory right to advocacy for those lacking capacity and “unbefriended” through the Independent Mental Capacity Advocacy Service (IMCA), Lasting Powers of Attorney for health and welfare and property and finance and two new criminal offences, i.e. “the wilful neglect or ill treatment of a person lacking capacity” (S 44 MCA 2005.)
The MCA will also apply when someone is detained under the Mental Health Act 1983. For example if the person lacks capacity to consent to treatment for a physical health issue rather than treatment related to mental disorder.
The Act has introduced safeguards for medical practitioners when working with advanced decisions made by people in advance for how they wish to be treated when or if they lose capacity in the future.
Best Interests Check List.
The best interests checklist represents the issues that decision makers must consider when decisions or interventions are made on behalf of someone who lacks capacity, if the decisions (and the decision maker) are to be protected by the MCA
The checklist items include that the decision maker:-
· Must not make their judgement based merely on the person’s age, appearance, condition (or diagnosis);
· Must take into account whether the person is likely to regain capacity with regard to the decision in hand, and whether the decision can wait;
· Must as far as reasonably practicable, ‘permit and encourage’ the person to communicate, including by acting to improve his or her ability to communicate (for example, by using an advocate);
· Must not, where the decision relates to life sustaining treatment, be motivated by a desire to bring about the relevant person’s death;
· Must so far as is possible consider the person’s past wishes and any preferences (particularly when written down) stated by him or her when they had capacity;
· Must take account of the beliefs and values that would have been likely to influence the person’s decision had they had capacity;
· Must, if practical and appropriate, consult anyone previously named by the patient as someone who should be consulted, any carers, anyone who has a relevant lasting power of attorney – a ‘donee’ (remembering that there are two kinds of LPA – (i) personal welfare, and (ii) property and affairs), and any appointed court deputy about their views concerning what would be in the person’s best interests. Protection from liability offered by Section 5 of the Mental Capacity Act
The MCA provides legal protection for people who need to intervene in the lives of people who lack capacity so that they are able to make a decision on that person’s behalf, or provide the care the person needs, as long as they have a reasonable belief that the person lacks capacity to make the particular decision and they are working in the person’s best interests.
Generally, however, protection is available as long as:-
· Reasonable steps have been taken to gain permission from the person concerned;
· The decision maker is reasonably sure the person lacks the capacity to make a particular decision;
· The decision maker is working in their best interests, and before making the intervention you have considered whether there is a “less restrictive’ option than the one proposed, and only ruled it out because it is less effective than the one you are now taking;
· Restraint if needed, is a proportionate response to the risk of harm if no action is taken;
· The action doesn’t amount to a deprivation of liberty, or conflict with an advance decision made by the person, their LPA or a Deputy;
· The decision maker is spending money to buy goods or pay for services that are in the person’s best interests and appropriate authority has been sought.
In a medical context, this could be helpful on a day-to-day basis, or to deal with an emergency situation where the Mental Health Act does not apply as illustrated in the example, taken form the Code of Practice, in box 3 below.
Box 3.
Example:You are called for advice by a local GP. She is with a patient in her home and the ambulance service is in attendance. The patient is dehydrated, and has a suspected UTI (urinary tract infection). The patient has become angry and belligerent at the idea that she needs admission to hospital and is refusing to go. She says that the doctor is in league with her neighbours and they intend to defraud her of her savings the moment she is out of the house. The ambulance staff refuse to intervene because they say it would contravene the woman’s human rights. The GP is considering asking for a Mental Health Act assessment. She says that, because of the advanced age and presentation of the patient, it is too risky to leave her at home. She confirms that she feels the woman lacks the capacity to take the decision about whether or not hospital admission is necessary because of the acute confusional state brought on by the dehydration and UTI.
You are able to advise the GP and the ambulance staff that, in this situation, the Mental Health Act may not be needed as their intervention would be covered by the Mental Capacity Act. The ambulance staff will be covered by sections 5 and 6 of the MCA, as long as their use of force in taking the woman to A&E is proportionate to the risks that staying at home poses to her. They need to be convinced themselves (as the professionals undertaking the act) that the actions would be in her ‘best interests’. The ambulance staff return to talk to the woman, and coax her to sit on their ‘lifting chair’. They are then able to wrap her securely in a blanket, with straps around her, so that they are able to carry her safely to the waiting ambulance despite her vocal protests.
Limitations to Section 5 by Section 6 Mental Capacity Act 2005.
It is important to recognise that section 5 of the Act does not offer practitioners total freedom from liability in providing care or treatment.
· Life-changing events: decisions about life-changing events, such as changes in residence and serious medical treatment will only be covered under Section 5 if the decision makers firstly consult all appropriate parties, and secondly consider whether there is a less restrictive way in which the care needed can be given. If there are no families or friends that professionals can consult in these specific circumstances, or if the decision maker deems the family member or friends “inappropriate", an Independent Mental Capacity Advocate (IMCA) must be instructed to support and represent the person whilst their best interests are being determined.
· The use of force, and depriving people of their Liberty: doctors and other professionals will continue to be protected by the law where, in an urgent situation, it is necessary to restrain or restrict a person who lacks capacity in order to protect them from harm. The force used must be proportionate to the risks involved. However, this protection has a ‘time limit’. Where restraint is needed on an ongoing basis (and restraint can mean the use of medication, or making a decision or making it known to a patient that they would be prevented from leaving) professionals involved won’t necessarily be protected by the MCA – this is where the Deprivation of Liberty Safeguards become important. Safeguards for patients: making decisions in advance Advance decisions to refuse medical treatment
People can now make advanced decisions to refuse treatment, provided that the decisions were made when the person had the capacity to make them.
To make a valid advance decision, a person must:
· Be 18 years or older
· Have capacity to make the specific decision
· Make a decision that is applicable (i.e. specific to the care and treatment they want to refuse and the circumstances in which it will be refused )
The decision doesn’t need to be in writing, unless it relates to life sustaining treatment – in which case it must be in writing, and witnessed.
An advanced decision becomes valid and applicable when all of the conditions described within it are present.
If Doctors are not informed about the existence of an advanced decision then they are expected to treat someone with that person’s bet interests in mind.
Lasting Powers of Attorney and Deputies from the Court of Protection
The MCA allows people to make arrangements for others to make decisions on their behalf when or if they lack capacity.
Lasting Powers of Attorney (LPAs) – The Act allows a person to appoint an attorney to act on their behalf if they should lose capacity in the future. The Act also allows people to empower an attorney to make health and welfare decisions, as well as financial & property decisions (a LPA for finance and property can be used whilst a person still has capacity, if the donee gives specific instruction). Before it can be used a LPA must be registered with the Office of the Public Guardian (see below).
Court appointed deputies – The Act provides for a system of court appointed deputies to replace the previous system of receivership in the “old” Court of Protection. Deputies will be able to be appointed to take decisions on welfare, healthcare and financial matters as authorised by the new Court of Protection (see below) but will not be able to refuse consent to life-sustaining treatment. They will only be appointed if the Court cannot make a one-off decision to resolve the issues.
A Court of Protection – The new Court has jurisdiction relating to the whole Act. It has its own procedures and nominated judges. It is able to make declarations, decisions and orders affecting people who lack capacity and make decisions for (or appoint deputies to make decisions on behalf of) people lacking capacity. It deals with decisions concerning both property and affairs, as well as health and welfare decisions.
A new Public Guardian – The Public Guardian has several duties under the Act and will be supported in carrying these out by an Office of the Public Guardian (OPG). The Public Guardian and his staff will be the registering authority for LPAs and deputies. They will supervise deputies appointed by the Court and provide information to help the Court make decisions. The OPG runs threes registers for Lasting Powers of Attorney, Enduring Powers of Attorney and Deputies; this information is available to members of the public. The OPG will also work together with other agencies, such as the police and social services, to respond to any concerns raised about the way in which an attorney or deputy is operating.
Independent Mental Capacity Advocate (IMCA) – An IMCA is someone instructed to support a person who lacks capacity but has no one to speak for him or her, such as family or friends , or if family or friends are present but considered “inappropriate” to assist in the process. IMCAs must be involved where decisions are being made about serious medical treatment or a change in the person’s accommodation where it is provided, or arranged, by the National Health Service or a local authority, and may be involved in abuse cases. The IMCA makes representations about the person’s wishes, feelings, beliefs and values, at the same time as bringing to the attention of the decision-maker all factors that are relevant to the decision. The IMCA can challenge the decision-maker on behalf of the person lacking capacity if necessary; challenges can be made via the Court of Protection or Judicial Review process. However, it is still up to the decision maker to consider what they believe is in the person’s best interests.
Key Concepts for doctors:
Lack of capacity in one area can’t be assumed to mean lack of capacity in another – and patients should be as involved as possible in all decisions made about their treatment.
Where it is proposed that a person move permanently into residential or nursing care, or serious medical treatment is proposed for someone who lacks capacity, the person’s relatives must be consulted about what they believe the person’s views about this would be, and whether the move or treatment would be in their best interest. If there are no relatives, an IMCA must be consulted.
The MCA s5 protects staff from liability as long as they have a reasonable belief that a person lacks capacity, and any force used in an urgent situation is proportionate to the risks that would fall to that person if they were not restrained. Where care needs to be provided in such a restricted way that it amounts to a ‘derivation of liberty’, this needs to be authorised. From April 09, the Deprivation of Liberty Safeguards may provide the authority needed to detain someone that is unable to consent to care or treatment being provided in a registered care home or hospital setting. (The Deprivation of Liberty Safeguards are the Government’s response to the European Court of Human Rights’ requirement that the so called “Bournewood Gap” be dealt with in British Law.)
Where staff become aware that a patient has made an advance decision refusing a particular treatment, that refusal has the same force as if the patient where making it contemporaneously, i.e. the medical treatment could not be given unless the doctor concerned was happy either that the patient did not have capacity when the decision was made, or that they did not intend the decision to have effect in the current circumstances.
Conclusion.
Anecdotally, medical practitioners appear to have been slow to make use of the powers and safeguards provided by the MCA. Relatively small numbers of referrals have been made to the IMCA services nationally to support those people that lack capacity and are “unbefriended” in the decision making processes around serious medical treatment. Only 671 eligible referrals were received by IMCA services in England and Wales in 2007/2008. (First Annual Report of the IMCA Service, July 2008). Could it be that an assumption is being made that the IMCA service may be seen more of a hindrance than a help, rather than a safeguard for the patient, in providing care and treatment?
The Act requires professionals to “presume capacity” rather than incapacity, for most professionals this is a challenge that we often fail to meet. It is easier to work with a presumption of incapacity and to act in that person’s best interest rather than take the time to “evidence” their capacity in relation to a variety of decisions that may need to be made.
The Act’s two new criminal offences have resulted in a small number of prosecutions to date. These prosecutions have tended to be brought against staff providing care in care homes or domiciliary settings rather than in hospital or other medial settings. Does this mean that staff working in hospitals or medical settings provide better care?
Healthcare organisations are a fertile breeding ground for interpersonal conflict and the development of dysfunctional relationships. The supervisory relationship between trainer and trainee is a particular area of concern for junior doctors. Aside from a problem trainee, such conflict can arise from a difficult supervisor, poor communication, personality clashes and power inequalities. This article will come from a trainee’s perspective in emphasising how these factors relate to the difficult supervisor. Recommendations are made for organisations and individuals on how the causes and consequences of this problem can be addressed .
The nature of working relationships
“Like a successful personal relationship, both sides must be able to acknowledge their goals, the obstacles they perceive in achieving their goals, and must be willing to compromise …” 1
Working relationships, like personal relationships, are embedded in a complex and diverse world with people of different personalities, backgrounds, motives and desires. Getting on with our fellow humans is a fundamental part of living and a challenge in our working lives. Garelick and Fagin (2004) have explored this area and have identified what facilitates a good working relationship (figure 1):
Figure 1: Factors that encourage good working relationships 2
Clarity about the organisation’s tasks and objectives
Clarity about the authority structure, with clear lines of accountability
The presence of a common goal or objectives
The opportunity to participate and contribute
The ability to trust and compromise
The possibility of setting aside inessential differences
Respect for alternative viewpoints
Protection of the weakest member of the team
Good leadership
A balance between individual aspirations and corporate needs
Sharing similar life experiences or cultural background
Dysfunctional Working Relationships
“Differences of perspectives … lead to interpersonal conflict that spirals into dysfunctional relationships” 3
Interpersonal conflict is a “dynamic process that occurs between interdependent parties as they experience negative emotional reactions to perceived disagreement and interference with the attainment of their goals” 4. Interpersonal work conflict can impact in terms of satisfaction, well-being, work disability, and mental health outcomes such as psychiatric morbidity, depression, fatigue and psychological distress 4. Factors that can play a role in conflict include perceived disagreements about tasks, ambiguities in role definition, or if the responsibilities are unclear 4.
One of the central issues inherent in workplace disputes is irrational behaviour on the part of one (or both) of the employees when the facts get confused with their highly charged feelings 5. In an attempt to avoid conflict the other individual may be uncomfortable about raising the issue, feel intimidated by someone with greater authority or power, or suspect a personal agenda, but does not want to sound argumentative. This can result in an emotionally charged situation with layer upon layer of faulty assumptions building up to a proverbial house of cards and the development of entrenched beliefs 3. Therefore what started as a misunderstanding can lead to a dysfunctional relationship3, which can result in multiple problems impacting on the organisation and the individuals involved. Specific consequences include complaints of bullying and racism against the trainer, labelling of the trainee as a doctor in difficulty, or the trainer developing a reputation as a “difficult supervisor”.
Causes of trainer-trainee conflict in medicine
In the field of medicine, particularly given the hierarchical structure of the profession, the potential for conflict is accentuated. Trainees tend to rotate around jobs, and educational supervisors, every 6-12 months. Trainees and trainers are expected to adapt to working with each other with differences in personality, styles of working, and expectations. It is therefore inevitable that difficulties will develop.The fundamental causes of the conflict between trainer and trainee in healthcare are:
1. The problem trainee
The problem junior doctor is a well-established area of concern 6. This type of doctor may be inflexible, clinically incompetent, arrogant, have poor time keeping or organisational skills, refuse to do what is asked, exhibit poor communication skills, lack enthusiasm, lack educational objectives, or have a difficult personality. Despite the “doctor in difficulty” being regarded as a “problem trainee” the dysfunctional relationship between trainer and trainee in medicine is usually a product of both parties.
2. The difficult supervisor
The most important factor in determining trainee satisfaction has been shown to be the quality of supervision provided by the consultant trainer 7. However the difficult supervisor, often a consultant, is an issue that is underreported. The problem consultant comes in various guises shown in figure 2:
Figure 2: The problem consultant 2
Authoritarian and bullying
Controlling
Indecisive and disorganised
Burnt-out
A consultant who is never there
A consultant biding time to retirement
The flirtatious consultant
Poor teacher and communicator
Generally a problem consultant would have, over the years, established a reputation as a difficult person to work with, usually confirmed by their peers and trainees. Unfortunately this aspect of their personality is ignored when they complain about a new trainee. Therefore the consultant is never identified as a difficult supervisor. Knowledge of what constitutes a bad supervisor should be accompanied by what is a good supervisor. In the field of psychology the notion of a good supervisor applies to any supervisory relationship (figure 3).
Figure 3: Good supervisor 8
Straddling the potentially conflicting roles of mentor and evaluator
Providing impartial and thorough evaluation within contexts that respect supervisee’s integrity
Having expertise
Being trustworthy
Modelling respect of differences in values, expectations and experiences
Tolerant of mistakes and facilitating trainees progress
Providing direct and clear feedback to trainees
Open to feedback about their own style of working
3. Communication problems
A supervisor should possess good communication skills in the form of: active listening, demonstrating understanding, using open questions, building areas of agreement and being open. As a good communicator the supervisor should refrain from stating unreasonable expectations, views, or opinions. They should avoid offering incentives / warning of consequences or revealing feelings. In the workplace, in times of pressure, dysfunctional communication is instrumental in trainer-trainee conflict.
These communication problems are prominent in the area of feedback 9. Feedback is a key role of the supervisor 10. Feedback should be honest, relevant, objective, specific, timely, and planned 9. It should be based on accurate information rather than hearsay and focused on behaviour and performance rather than personality and attitude. It should be constructive, conducted in private, descriptive rather than evaluative, and designed to avoid personalising and blaming 9. Feedback should not be given on things the trainee cannot change e.g. personality.
Should the trainee feel offended by feedback at any point then it may be that the supervisor has a hidden agenda or is a bully. A delay in feedback impedes efficient working so the giving and receiving of feedback should also be a balanced ongoing process in order to boost morale and motivation, leading to greater effectiveness and job satisfaction 9. If the supervisor has a good relationship with the trainee then constant feedback should be given about his/her performance: the final report should never be a surprise 11.
4. Personality clashes
Conflict may also reveal itself in personality differences between trainee and trainer. Personality characteristics of the latter that can significantly affect an otherwise healthy relationship include a trainer who is preoccupied with details, order, organisation and schedule. Such trainers may be seen as perfectionist, pedantic, rigid and stubborn, and often insist that others submit to their way of doing things, according to their own self-proclaimed high standards.
Personality clashes may arise from poor communication or underlying factors including racism, sexism, religion, or jealousy and envy interfering with the relationship on both sides 12. The crucial question to ask is whether the trainer-trainee conflict is a result of a difficult trainee, or whether it arises when a trainee does not fit the supervisor’s scheme of things.11
5. Power differential
The trainer/supervisor also has an evaluative function in relation to the trainee and therefore the potential for abuse and trainee vulnerability in respect of the supervisor, is clear 8. The dependence of trainees on trainers for references creates a “potential power imbalance and in some cases may lead to intentional or unintentional harm to the trainee” 13. This harm may be identified in the trainer’s assessment of the trainee when completing the end-of-post evaluation. The trainer taking a proactive approach in writing complaints and sending emails to sabotage a trainees’ career may also demonstrate abuse of power.
Equally an overpowering consultant may, consciously or unconsciously, take advantage of the situation by going on a fault-finding mission. This can become part of a self-fulfilling prophecy. If the trainee is perceived to be poorly performing the supervisor may feel under more pressure and become hostile towards the trainee, without addressing the main problem 12. The result is that the supervisor engages in “continuous criticism and academic humiliation” 12 which causes the trainee to feel more useless and helpless. This can lead to the trainee becoming a scapegoat in an already dysfunctional team12.
Another consequence of the power imbalance is that it causes a state of confusion for trainees who want things to change but will often tolerate the problem and endure it to avoid jeopardising their career prospects. The trainee may feel powerless and fearful about addressing the current problem and choose to be silent on the matter, rather than risk an unpleasant situation 12. Unfortunately such passive behaviour may result in the problem escalating and the trainer may, unconsciously and unwittingly, bully the trainee 8.
How to deal with trainer-trainee conflict?
“Conflicts are really a house of cards ... you can bring them down by getting to the bottom and getting to the facts” 3 .
Dealing with trainer-trainee conflict involves good emotional intelligence, self-awareness (being self aware and taking an honest look at oneself), self-regulation (ability to control emotions), empathy (ability to identify and understand the wants, needs and viewpoints of others), being well-motivated, and having good social skills 14. In other words, successful conflict resolution relies on first understanding ourselves, being aware of our personality, our prejudices, why we like some people and not others, and recognising that certain things will annoy us and not others 11.
From a trainee’s perspective conflict with the supervisor should be addressed at an early stage to prevent escalation of the problem 12. This should include self-appraisal, thinking about the root of the problem in a factual and non-personal way, and informal discussion with a discreet colleague to gain another perspective. Trainees should find out how their predecessor got on in the post. Finally, problems should be freely discussed with the supervisor. However, there may be supervisors with whom it is difficult to have a discussion; therefore the trainee must involve others to deal with the issues which escalate or remain unresolved. If the supervisor is considered the source of the problems there are steps to take to ensure the power of the supervisor is not misused against trainees (figure 4):
Figure 4: Steps to deal with a difficult supervisor 13
College / speciality tutors and clinical tutors / programme directors have an obligation to act as the trainee’s advocate
Where tutors and programme directors fail to act appropriately, a direct approach by the trainee to the local postgraduate dean or relevant college may be indicated
The local trainees’ committee, trade union, and its officers / representatives may also be helpful in acting as the trainee’s advocate in appropriate circumstances
Deanery contact monitoring and training programmes’ approval visits, involving the College and conducted on behalf of the Postgraduate Medical Education and Training Board, also afford opportunity to raise concerns about supervisors
If trainees consider their health affected by the stress of working with a difficult supervisor they should seek help from their occupational health department or postgraduate dean, who may offer confidential services and helpful advice for the assessment of mental health problems affecting doctors
Trainees may be reluctant to take the steps described in figure 4. The power differential between trainer and trainee, as well as acting as an antecedent to the conflict, is a perpetuating factor that ensures nothing is done about it. The difficult supervisor may be underreported for the same reasons seen with workplace bullying, namely, fear of making matters worse, belief that nothing will be done, concerns regarding confidentiality, fear of victimisation, and concerns about being labelled as a troublemaker 15. Ultimately it is the fear of the consequences that deters trainees from speaking out, though it is worth remembering that Franklin D Roosevelt stated in his first inaugural speech, “the only thing we have to fear is fear itself”.
What can healthcare organisations do about supervisory conflict?
Organisations must be proactive in identifying and dealing with problems between trainers and trainees, who in turn ought to be aware of their responsibilities. Organisations may be tempted to sweep problems under the carpet but there are recommendations on how they can address the causes of trainer-trainee conflict (figure 5):
Figure 5: Steps for organisations to tackle the causes of trainer-trainee conflict
Cause
Solution
Problem trainee
Training of supervisors in not only how to identify the problem junior, but how to constructively manage the problem at the outset. Adopting a positive, non-judgemental and non-confrontational approach, and having a problem-solving mindset are essential
Difficult supervisor
Training of supervisors regarding their roles as a educational and clinical supervisor
Training of supervisors in sensitive areas of diversity and equality, and self-reflection, with the support of college tutors and programme directors
360 degree feedback carried out frequently and acted upon promptly during the supervisor’s appraisal
Communication Problems
Communication skills training
Constructive feedback training
Personality Clashes
Training of supervisor and trainee in conflict resolution since there may be personality differences between the two, rather then an individual doctor in difficulty.
Power differential
Power imbalance of feedback can be countered if feedback from each trainee becomes part of appraisal and revalidation for consultants
Colleges should collect anonymous feedback about educational and clinical supervisors from trainees and review their future role as supervisor
Complaints of bullying and racism should be dealt with promptly and effectively by the organisation.
Paice (2002) describes an excellent mentor as someone who “will always inspire, teach by example, and excite admiration and emulation” 16. Mentoring can be beneficial in facilitating the development of the trainee but “faculty mentoring should be avoided’’ 17. In other words mentoring of doctors should not be carried out by the trainee’s educational supervisor or line manager, nor should they be involved in their assessment or appraisal, to avoid blurring the distinction between the roles 17. A good mentor should :
Motivate
Empower and encourage
Nurture self-confidence
Teach by example
Offer wise counsel
Raise the performance bar
However, the authors argue that these are the qualities that should be part of being a good supervisor 17.
Conclusion
“Differences in power and status, and dependence on references, places juniors in invidious positions when they experience problems in their relationships with trainers” 2
The relationship between trainer and trainee should reflect the same warmth and nurturing as in a parent-child relationship. There is a parallel with both types of relationship in that there is an imbalance of power that interacts with poor communication and personality conflicts. In medicine although the problem junior doctor is frequently highlighted it must be remembered that the trainer-trainee conflict may reflect a difficult supervisor. The supervisor needs to achieve a healthy relationship that is sensitive to the needs of the trainee, void of any of their preconceived beliefs and prejudices, and act as a role model in making a good doctor and achieving their full potential 16. Interpersonal conflict can nevertheless develop and escalate to the extent that the trainee may suffer in silence. Healthcare organisations can be more proactive in penetrating the causes of the dysfunctional working relationship. Trainees should be fearless in turning to existing support in face of a difficult supervisor.
KEY POINTS:
Professional working relationships are a major challenge in healthcare
Interpersonal conflicts can lead to a dysfunctional working relationship
Issues include problem trainees, poor communication, and personality clashes
Power inequalities and the difficult supervisor need to be addressed
Trainer-trainee conflict can be resolved with steps taken by the individual
Organisations must address the causes of dysfunctional working relationships
Trainees need to overcome their own fears when tackling conflict
Schwannoma (neurilemmoma) is a peripheral nerve sheath tumour and commonly occurs on the head, neck and trunk. Giant schwannoma is rarely located in the retroperitoneum and the pelvis but rarer in the mesorectum. The majority of symptoms caused by the tumour are due to its mass effect. Surgical resection is enough to treat the tumour. Schwannoma is usually a benign tumour. Its malignant transformation is usually very rare. We report a 36 year old male patient with a giant mesorectal schwannoma who presented with vague symptoms.
Case Report
A 36 year old male patient presented with a lower abdominal mass since 2 months, urgency of defecation since 6 months and erectile dysfunction for more than 3 years. There was no history of urinary disturbances. General physical examination did not reveal any abnormality. Abdominal examination showed a non tender, firm, fixed mass with well defined borders over the suprapubic region which was extending into the pelvis. No organomegaly was detected. On rectal examination a hard, immobile mass was felt 5 cm away from the anal verge and lying anterior to the rectum.
His urine analysis, routine hematological investigations and renal function test were within normal limits. Total bilirubin was raised to 24.9 µmol/l (3.42-20.52 µmol/l), direct bilirubin was also elevated 8.2 µmol/l (0-6.8 µmol/l) while all other results were within normal range. The patient was positively screened for Hepatitis B and Syphilis. CT scan (figure 1) of abdomen revealed a large soft tissue mass measuring 10x11 cm in the pelvis. It was a well defined mass without any infiltration to the following structures: sigmoid, rectum, prostate gland, the bladder and the sacral bone.
Figure 1 shows a large soft tissue mass measuring 10x11 cm which compresses the rectum.
FNAC of the mass which was taken 3 cm from the anal verge showed isolated fibrotic tumor.
The patient was advised for HIFU therapy (high intensity focused ultrasound) in view of eventual surgery. In HIFU therapy, the ultrasound beams are focused on the diseased tissue and due to the significant energy deposition at the focus, temperature within the tissue rises to 65° to 85°C, destroying the diseased tissue by coagulation necrosis and hence facilitating the dissection of the mass during surgery. After HIFU therapy, the patient no longer complained of urgency of defecation. But there was no significant change in the size of the mass after a rectal examination.
Hence, explorative laparotomy was carried out. The abdomen was opened through the lower midline incision. A huge mesorectal mass of 15x11x8 cm (figure 2), was identified on the right side of the rectum and behind the prostate gland extending upwards, without any posterior infiltration into the sacral bone. Complete excision of the mass was achieved by blunt dissection and the mass was sent for histopathological examination. The operation was uneventful.
Figure 2 shows the complete excision of a well encapsulated mass of 15x11x8 cm. The external surface of the mass was gray-white and smooth.
Figure 3: Histology showing typical pallisading arrangement of spindle cells (Antoni-A/Verocay Body) and less cellular myxoid areas (Antoni-B)
Discussion
Schwannoma (Neurilemmoma) is a benign neoplasm arising from the myelinated nerve sheaths. Malignant schwannoma despite their name, never arise from malignant degeneration of schwannomas. Instead they occur from transformation of a plexiform neurofibromatosis. This fact provides the basis for their association with neurofibromatosis1.
Schwannomas are frequently present in patients aged 20 to 50 years with a male predominance. They comprise 5% of all benign soft tissue tumors and have a predilection for the head and neck2, 3, 4 and flexor surfaces of the upper and lower extremities5. Pelvic schwannoma is rare and accounts for less than 1% of all benign schwannomas6. The rarity of this tumor and the lack of clinical manifestations make a pre-surgical diagnosis very difficult.
These tumors slowly increase in size before becoming symptomatic. Clinical signs or symptoms manifest themselves only by the compression or infiltration of adjacent organs. Therefore, detection is often accidental.
Schwannoma typically appears as a solitary, well encapsulated, firm and smooth-surfaced round mass. In large tumors (>8-10 cm), a degenerative pattern (cystic areas, calcifications, interstitial fibrosis, and hyalinization) is commonly found that identifies the “ancient” variant7. Histologically, typical schwannomas are composed of inter mixed Antoni A components (cellular and arranged in short bundles or interlacing fascicles) and Antoni B areas (less cellular and organized with more myxoid components).Schwannomas show uniform and intense staining for S 100 protein8.
Malignant transformation is very rare and controversial9. Malignant schwannomas are large in size and highly aggressive tumours. They are painful, and may cause many different symptoms depending on the location and size. They infiltrate into the adjacent structures and metastasize to distant sites. Histologically, the nuclear palisading may be a striking feature. There will be perineural and intraneural spread of tumour, lesional proliferation, or herniation into the lumina of the vessels10.
A combination of clinical, pathological and immuno-histochemial studies help to make the diagnosis.
However preoperative diagnosis of schwannomas is not easy owing to the difficulty in finding imaging features (with Ultrasonography, CT, or MRI) that enable the discrimination of schwannomas from other soft tissue tumors (fibrosarcoma or liposarcoma) and benign forms from malignant ones11. Schwannomas can frequently be misdiagnosed as psoas abscesses, pancreatic cysts, neoplasms, adnexal masses, adrenal, kidney or hepatic tumors, as reported in the literature12, 13, 14. Yet, radiological imaging is helpful in therapeutic planning, as it gives information about the tumor’s size, location, and possible invasion of other structures. Fine-needle aspiration biopsy may theoretically be useful if Schwann cells are found in the sample, but the tissue specimen collected for diagnosis is often inadequate and may be misleading because of cellular pleomorphism in degenerated areas which might be interpreted as consistent with malignancy15.
Hughes MJ et al11, in their largest radiological series of abdominal or pelvic schwannomas, showed that a smooth well defined border, ovoid or spherical shape and location in the pre sacral region or lower retro peritoneum at the pelvic brim, are frequent findings in primary abdominal or pelvic schwannomas ; 11 of 13 cases showed all these features. Evidence of degeneration was common, with 8 schwannomas showing cystic change and 3 showing areas of calcification. The cystic schwannomas tended to be larger, with a mean diameter of 10.5cm.
It is difficult to make an accurate pre operative diagnosis. The treatment depends solely on surgery. Malignant schwannomas are insensitive to chemotherapy and radiation, resulting in poor prognosis16.
Conclusion
Schwannoma is a benign encapsulating neoplasm with an overall low incidence, occurring mostly in the head, neck and trunk regions. Giant schwannoma is rarely located in the retroperitoneum, the pelvis and rarer in the mesorectum.
Schwannomas pose a difficult diagnostic challenge. Radiological findings are often non-specific. Ultrasonography can differentiate between solid and cystic tumours. CT can be helpful in determining the size, location, local involvement and distant spread. MRI provides similarly useful information as CT, but yields better visualization of the tumour. FNAC is not often helpful because the tissue architectural information required is not obtainable from cytological specimen. The only gold standard diagnostic investigation is histology of either biopsy or excised specimen.
Surgical excision has remained the mainstay of treatment. Although benign, large and incompletely excised lesions are capable of recurrence, malignant change is exceedingly rare.
Inadvertent carotid arterial puncture complication is reported to have an incidence of 2% - 8% 1, 2 and usually results in localised haematoma formation.
Case presentation
We present a case of a 72 year old man with acute on chronic renal failure referred for intensive care (ITU) management. History revealed dehydration and anuria for 3 days. His blood pressure was 80/40, sinus tachycardia around 130/min with cold clammy peripheries. Blood investigations revealed urea 23mmol, creatinine 800mmol, and potassium-7.7, with ECG changes of hyperkalemia. We attempted a right internal jugular (IJV) venous cannulation using landmark technique and inserted an Arrow-Howes central venous catheter with blue flexi tip, 8.5FR, 5 lumen, and 16cm length. The technique was difficult due to low blood pressure, and patient’s inability to lie flat. The ultrasound machine was unavailable at that moment.Soon after the catheter was introduced using seldinger technique, a swelling was noticed from the site of IJV cannulation .the blood sample analysis revealed arterial blood. The catheter was removed and pressure applied for 45 minutes. Thereafter, a left femoral vein catheter was inserted for central venous access and right femoral vascath –VYGON, DUALYSE Expert, 2 lumen catheter set, 12 fr, 20cm was inserted uneventfully.1 hour later the bleeding from the right carotid puncture site was examined and was found to have ceased. The patient was put on the continuous veno- venous haemofiltration (CVVHF), which clotted after 15minutes.Heparin was used as an anticoagulant for the filter. This was repeated thrice with same result. Three hours later, a haematoma was noticed in area of IJV puncture, which was gradually increasing in size. The haematoma spread to the neck and chest after which the patient complained of discomfort with breathing difficulty. In view of increasing airway compromise the patient was transferred to theatre for elective intubation and surgical intervention. Ultrasonongraphy by radiology consultant showed a large haematoma, but unable to see the damage in the vessel and a CT neck, thorax angiography was suggested. CT angiogram revealed a leak in the bifurcation of the carotid artery. Surgical access was difficult in view of the large persistent leak. Ultrasound probe was used to make the incision superficial to the leak. A small leak was identified in the artery, which was sutured uneventfully. He was then continued on CVVHF with no further complications Discussion Complications include arterial puncture, pneumothorax, neck or mediastinal haematoma and hemothorax3, 4. The haematoma may enlarge rapidly if the patient is coagulopathic, or if a large puncture wound is produced by the introduction of the sheath itself into the carotid artery. Airway obstruction 5, 6, pseudo aneurysm 7, 8, arterio-venous fistula formation 9 and retrograde aortic dissection 10 have all been reported as a consequence of carotid puncture. In the presence of occlusive (atheromatous) carotid disease, inadvertent puncture may carry the risk of precipitating a cerebrovascular accident 11. NICE guidelines 2002 recommended use of ultrasound for central venous cannulation12. The Royal College of Radiology (RCOR) recommends practical training in vascular ultrasound should involve at least two ultrasound lists per week over less than three months up to 6 months. Meta-analysis including 18 Randomised Controlled Trials by NICE concluded that ultrasonongraphic (USG) venous catheterisation was more effective than landmark technique for all outcomes 13 Royal College Of Anaesthetists feels guidance is fair and sensible but landmark technique is still acceptable alternative whether 2D available or not. Conclusion Complications following central venous cannulation are reduced if the procedure is USG guided and therefore must be used whenever possible. But landmark technique is still an acceptable alternative.
We describe a case of a 32 year old primigravida with type III Klippel-Feil Syndrome for an elective Caesarean section. A preanaesthetic assessment at 32nd week of pregnancy revealed a history of mild asthma for which the patient was on regular salbutamol inhaler. She had no history of cardiovascular or respiratory insufficiency. There was no significant family history. Anaesthetic history included a repair of encephalomyelocele immediately after birth and a squint correction surgery at the age of 6 years under general anaesthesia which was uneventful.
Examination revealed a woman of small stature, 137 cm in height and weighing 52 kg. Airway examination revealed Mallampati III with a normal mouth opening, a reduced thyromental distance (3 cm) and inability to flex or extend the neck (Figure 1). She had thoraco-lumbar kyphoscoliosis and examination of the respiratory and cardiovascular system was unremarkable. Electrocardiogram was within normal limits as were haemoglobin, urea and electrolyte estimation. Radiography revealed fusion of atlanto-axial joint (flexion and extension views, Figure 2 ) and also fusion of lumbar vertebrae with associated scoliosis (Figure 3Cobb’s angle 25 degree) and Cobb’s angle 25 degree Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.




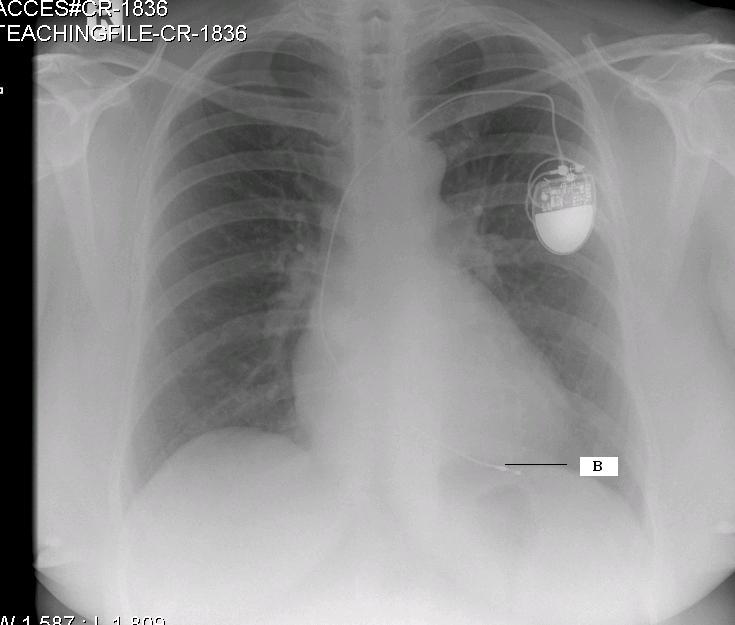 Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3.
Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3. 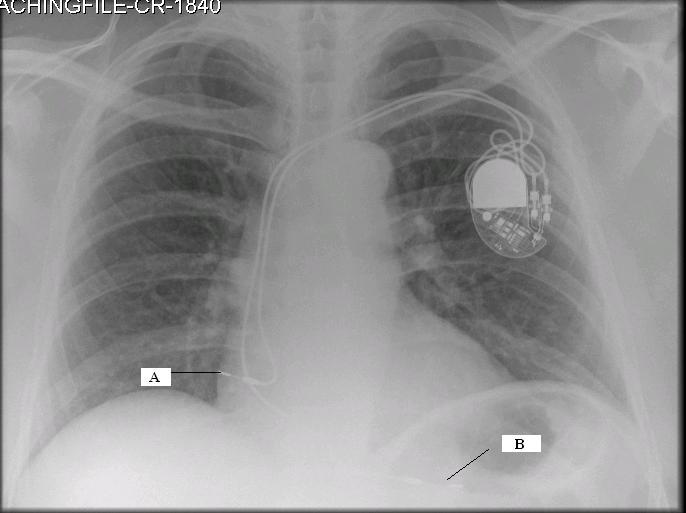 Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835).
Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835). 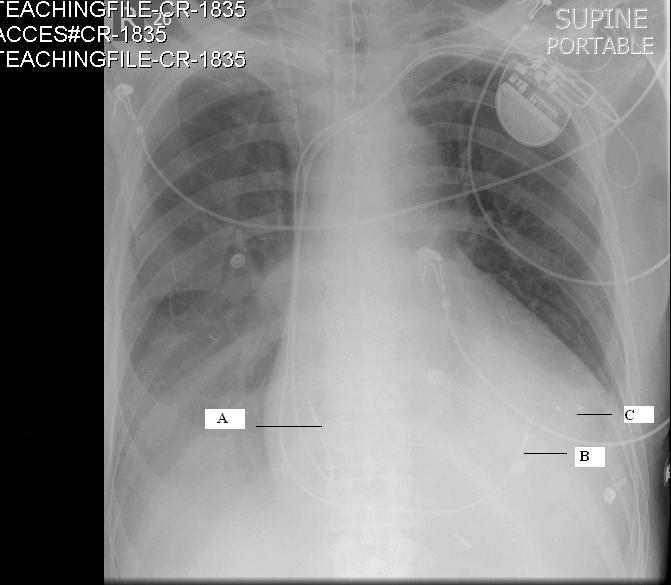 Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values.
Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values. 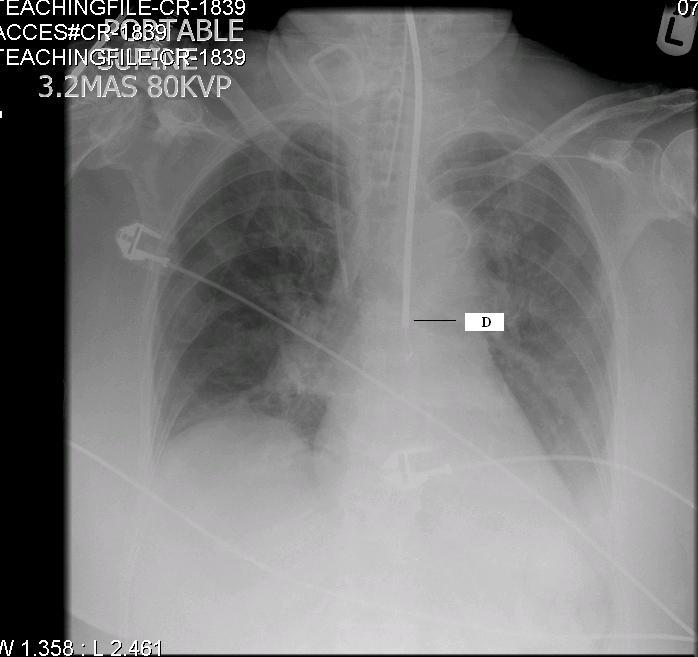 Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6]. 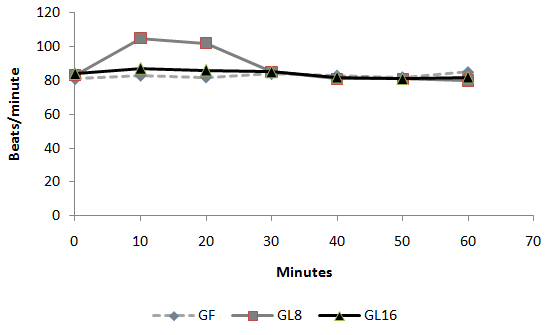 Fig 1: Intra-operative changes in heart rate in groups
Fig 1: Intra-operative changes in heart rate in groups 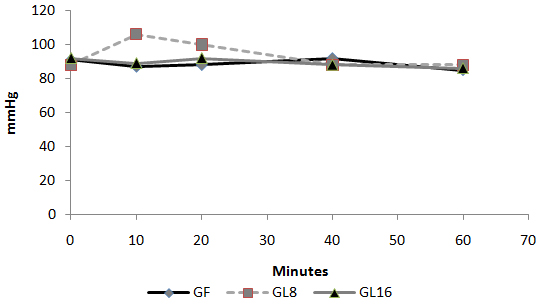 Fig 2: Intra-operative changes in MAP in groups
Fig 2: Intra-operative changes in MAP in groups 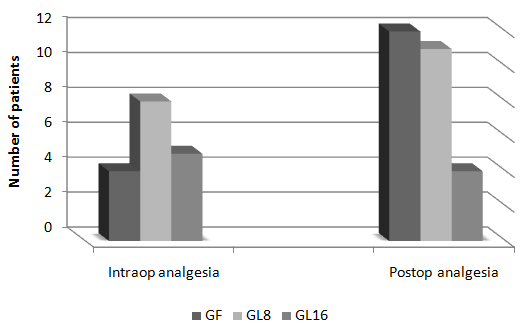 Fig 3: Number of patients requested perioperative analgesic supplementation
Fig 3: Number of patients requested perioperative analgesic supplementation 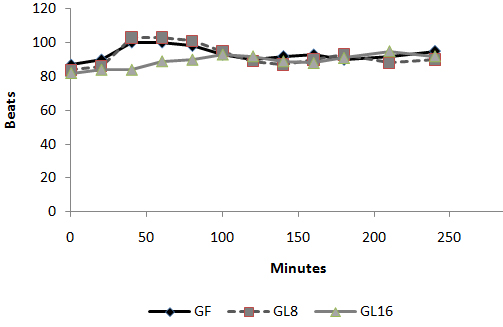 Fig 4: Changes in heart rate in PACU
Fig 4: Changes in heart rate in PACU 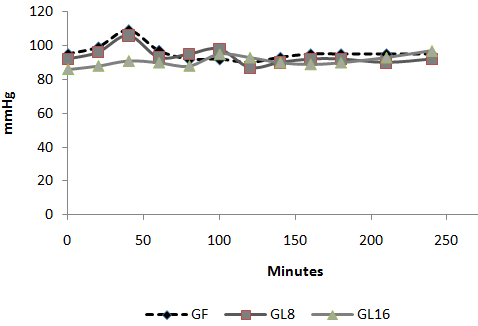 Fig 5: Changes in MAP in PACU:
Fig 5: Changes in MAP in PACU: 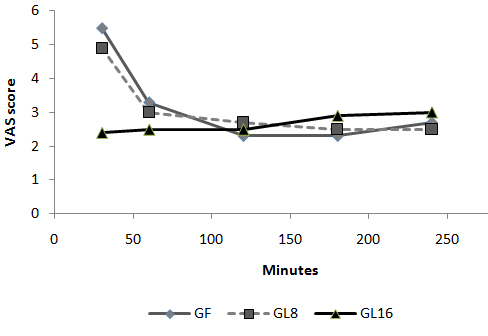 Fig 6: Changes in VAS in PACU Discussion: The use of an opioid, even a short acting one can be associated with adverse effects, which may not be acceptable for patients scheduled for day case surgery. For this reason, it was suggested to substitute an opioid with a non-opioid analgesic for postoperative pain control. The use of a NSAID is associated with adverse effects [1]. Lornoxicam has been successfully used in the prevention and treatment of postoperative pain. It has been shown to be as effective as morphine [4], meperidine [5] and tramadol [6]. To the best of our knowledge, this is the first study to compare the perioperative analgesic efficacy of lornoxicam to fentanyl in patients undergoing day case ENT surgery. We gave Lornoxicam half an hour before induction of anesthesia as the time taken to reach peak plasma concentration (Tmax) was determined to be 0.5 h [7]. During the operative procedure, HR and MAP were significantly higher in group L8 compared to group F and L16. While in PACU, patients in groups F and L8 had higher HR, MAP and VAS score in the early postoperative period compared to patients in group L16. This may be due to inadequate analgesic effect of L8 and the shorter plasma half life of fentanyl compared to L16. The analgesic efficacy of L16 might be attributable to inhibition of cyclo-oxygenase (COX1) and (COX2) activity [2], release of endogenous dynorphin and β-endorphin [5], decrease in peripheral and central prostaglandin production [8] as well as exertion of some of its analgesic activity via the central nervous system [9]. Lornoxicam has a more potent anti-inflammatory and analgesic effect than other oxicams as well as a shorter half life, which decreases the incidence of side effects of drugs with long plasma half life [10]. Arslan and colleagues reported decreased opioid need, PONV and postoperative pain scores when 16 mg of lornoxicam was administered after thyroidectomy [11]. While Xuerong and colleaguessuggested that the increase of postoperative morphine requirements induced by intra-operative administration of fentanyl could be prevented by ketamine or lornoxicam [12]. Rawal reported that NSAIDs are effective as the sole analgesic in a high proportion of cases of mild to moderate pain and it is more convenient to give these drugs by the IV route rather than by IM or rectal administration [13]. The analysis of pain intensity differences was complicated by the fact that many patients postoperatively were asleep at the time their pain assessments were due which may be attributed to effect of opioid and anesthetic medications used. To minimize any missing data we used time to the first dose rescue analgesia (based on changes in hemodynamic data) to evaluate pain intensity differences from baseline. L16 was well tolerated in this study, and was associated with a significantly lower incidence of adverse events than F and L8 which could be due to the opioid side effects in both groups. Norholt and colleaguessupported our results as they reported that, in terms of common acute adverse events, lornoxicam appeared to possess a higher benefit/risk ratio compared with morphine [4]. Zuurmond et al reported that, there is good evidence that avoidance of opioid virtually abolishes the PONV that preclude oral intake of fluids after surgery [14]. In our study, nausea developed in 25.7% of patients in group F, 20% in group L8 but only 8.6% in group L16 who received the least rescue opioid analgesia. Regarding bleeding abnormalities, Hodsman et al reported extensive bleeding required reoperation on two diclofenac group patients submitted to abdominoperitoneal resection of the rectum [15]. In our study no abnormal bleeding was reported by ENT surgeons in any of the study patients. In agreement with our results, Ilias et al[16], Trampitsch et al[17] and Karaman et al [18] used lornoxicam and they did not detect problems with surgical bleeding, bleeding time, blood transfusion requirement or postoperative bleeding. Stroissnig et al reported that overall, in healthy adult volunteers, oral doses of lornoxicam up to 70 mg have been well tolerated, and there have been no effects on vital signs, urine analysis parameters or clinical serum biochemistry [19]. In our study, none of the patients receiving study drugs experienced severe gastric discomfort, needed rescue antiemetic medication or required admission because of poor pain control. Previous studies used lornoxicam for reduction of postoperative opioid consumption but none of them had studied the intra-operative use of lornoxicam. So, we selected certain type of surgical procedures which might be suitable to use lornoxicam as a sole intra-operative analgesia. The adjunctive use of acetaminophen may have additive analgesic efficacy to lornoxicam because of its intrinsic opioid-sparing activity. Measurement of serum catecholamine would have been useful. These could be considered as a limitation for the present study. Conclusion: Intravenous 16 mg lornoxicam with the present study design was comparable to 100 µg fentanyl as intra-operative analgesia but more effective than fentanyl in preventing early postoperative pain in mild to moderate ENT surgical procedures. Intravenous lornoxicam 8 mg was not satisfactory as a sole intra-operative analgesia. The overall incidence of adverse effects of lornoxicam was lower than that of fentanyl.
Fig 6: Changes in VAS in PACU Discussion: The use of an opioid, even a short acting one can be associated with adverse effects, which may not be acceptable for patients scheduled for day case surgery. For this reason, it was suggested to substitute an opioid with a non-opioid analgesic for postoperative pain control. The use of a NSAID is associated with adverse effects [1]. Lornoxicam has been successfully used in the prevention and treatment of postoperative pain. It has been shown to be as effective as morphine [4], meperidine [5] and tramadol [6]. To the best of our knowledge, this is the first study to compare the perioperative analgesic efficacy of lornoxicam to fentanyl in patients undergoing day case ENT surgery. We gave Lornoxicam half an hour before induction of anesthesia as the time taken to reach peak plasma concentration (Tmax) was determined to be 0.5 h [7]. During the operative procedure, HR and MAP were significantly higher in group L8 compared to group F and L16. While in PACU, patients in groups F and L8 had higher HR, MAP and VAS score in the early postoperative period compared to patients in group L16. This may be due to inadequate analgesic effect of L8 and the shorter plasma half life of fentanyl compared to L16. The analgesic efficacy of L16 might be attributable to inhibition of cyclo-oxygenase (COX1) and (COX2) activity [2], release of endogenous dynorphin and β-endorphin [5], decrease in peripheral and central prostaglandin production [8] as well as exertion of some of its analgesic activity via the central nervous system [9]. Lornoxicam has a more potent anti-inflammatory and analgesic effect than other oxicams as well as a shorter half life, which decreases the incidence of side effects of drugs with long plasma half life [10]. Arslan and colleagues reported decreased opioid need, PONV and postoperative pain scores when 16 mg of lornoxicam was administered after thyroidectomy [11]. While Xuerong and colleaguessuggested that the increase of postoperative morphine requirements induced by intra-operative administration of fentanyl could be prevented by ketamine or lornoxicam [12]. Rawal reported that NSAIDs are effective as the sole analgesic in a high proportion of cases of mild to moderate pain and it is more convenient to give these drugs by the IV route rather than by IM or rectal administration [13]. The analysis of pain intensity differences was complicated by the fact that many patients postoperatively were asleep at the time their pain assessments were due which may be attributed to effect of opioid and anesthetic medications used. To minimize any missing data we used time to the first dose rescue analgesia (based on changes in hemodynamic data) to evaluate pain intensity differences from baseline. L16 was well tolerated in this study, and was associated with a significantly lower incidence of adverse events than F and L8 which could be due to the opioid side effects in both groups. Norholt and colleaguessupported our results as they reported that, in terms of common acute adverse events, lornoxicam appeared to possess a higher benefit/risk ratio compared with morphine [4]. Zuurmond et al reported that, there is good evidence that avoidance of opioid virtually abolishes the PONV that preclude oral intake of fluids after surgery [14]. In our study, nausea developed in 25.7% of patients in group F, 20% in group L8 but only 8.6% in group L16 who received the least rescue opioid analgesia. Regarding bleeding abnormalities, Hodsman et al reported extensive bleeding required reoperation on two diclofenac group patients submitted to abdominoperitoneal resection of the rectum [15]. In our study no abnormal bleeding was reported by ENT surgeons in any of the study patients. In agreement with our results, Ilias et al[16], Trampitsch et al[17] and Karaman et al [18] used lornoxicam and they did not detect problems with surgical bleeding, bleeding time, blood transfusion requirement or postoperative bleeding. Stroissnig et al reported that overall, in healthy adult volunteers, oral doses of lornoxicam up to 70 mg have been well tolerated, and there have been no effects on vital signs, urine analysis parameters or clinical serum biochemistry [19]. In our study, none of the patients receiving study drugs experienced severe gastric discomfort, needed rescue antiemetic medication or required admission because of poor pain control. Previous studies used lornoxicam for reduction of postoperative opioid consumption but none of them had studied the intra-operative use of lornoxicam. So, we selected certain type of surgical procedures which might be suitable to use lornoxicam as a sole intra-operative analgesia. The adjunctive use of acetaminophen may have additive analgesic efficacy to lornoxicam because of its intrinsic opioid-sparing activity. Measurement of serum catecholamine would have been useful. These could be considered as a limitation for the present study. Conclusion: Intravenous 16 mg lornoxicam with the present study design was comparable to 100 µg fentanyl as intra-operative analgesia but more effective than fentanyl in preventing early postoperative pain in mild to moderate ENT surgical procedures. Intravenous lornoxicam 8 mg was not satisfactory as a sole intra-operative analgesia. The overall incidence of adverse effects of lornoxicam was lower than that of fentanyl.
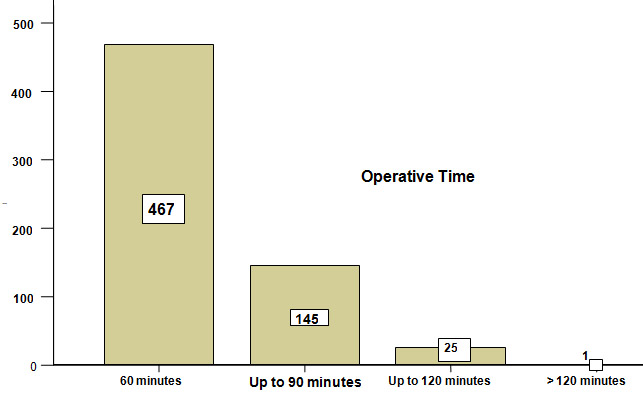 Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation
Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation  Assessment of spasticity Before any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale
Assessment of spasticity Before any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale
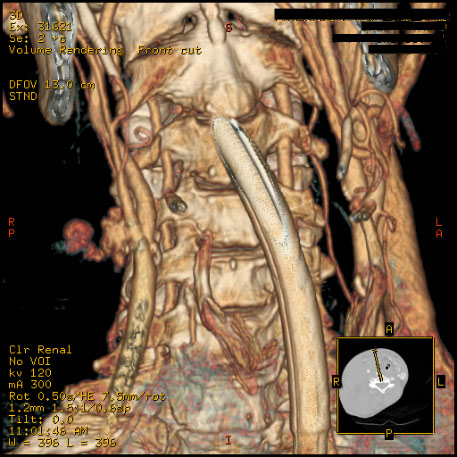
 Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements
Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements 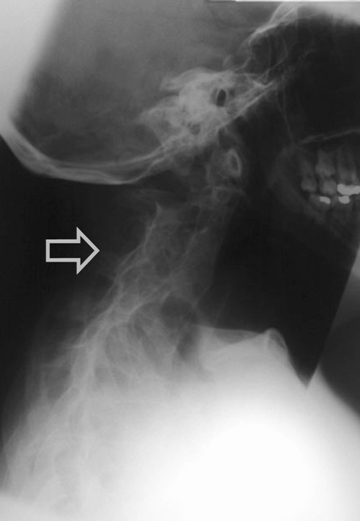 Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae
Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae 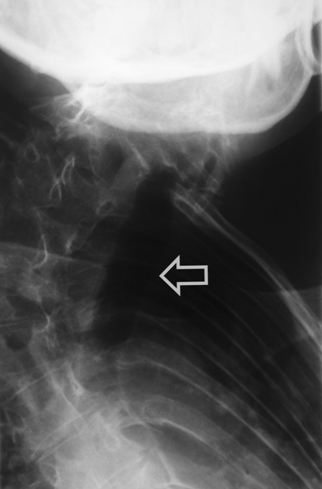 Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.
Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.
BJMP September 2009 Volume 2 Number 3
BJMP September 2009 Volume 2 Number 3
Full Issue Booklet (All articles)
PDF
Full issue Booklet
Editorial
Global Health Challenges: The Indian Conundrum
Rajan Madhok
Full Text
PDF
Review Articles
The Mental Capacity Act 2005: What it does and some thoughts on its impact on practice
Diane Brown
Full Text
PDF
Erythropoietin Friend or Foe in Chronic Kidney Disease Anemia: An Analysis of Randomized Controlled Trials, Observational Studies and Meta-analyses.
Amir Hayat
Full Text
PDF
Leg Ulcers in Older People: A Review of Management
Adeyemi Adeyi, Sharon Muzerengi, and Indrajit Gupta
Full Text
PDF
Approach to spasticity in General practice
Ganesh Bavikatte and Tarek Gaber
Full Text
PDF
Team Assessment Behaviour (TAB) as an assessment tool: A critical evaluation.
Milind Pant, Prabhu N Nesargikar and Daniel M Cocker
Full Text
PDF
Research Articles
Open Mesh Repair Of Different Hernia. Is The Technique Free Of Complications?
Arshad M Malik, Asad Khan, K Altaf Hussain Talpur and Abdul Aziz Laghari
Full Text
PDF
UK Junior Doctors’ Experience of Clinical Audit in the Foundation Programme
Andrew Cai, John Greenall And Dau Col Dau Ding
Full Text
PDF
Analgesia in day-case ENT surgery: The efficacy of lornoxicam
Mohamed Daabiss, Medhat Al-Sherbiny, Rashed Al-Otaibi and Rima Al-Nimar
Full Text
PDF
Case Reports
A case report of a Giant Schwannoma of the Mesorectum
Gopall Jayprakash , Cheng Yong and Wang Yanqing
Full Text
PDF
Anaesthetic management of a patient with Klippel-Feil syndrome for elective Caesarean section
M K Kada Venkata, Jameel Ahmed Khan, Muhammad Tayyab Qureshi, Asif Qureshi, Imtiaz Kar
Full Text
PDF
A case of accidental carotid artery cannulation in a patient for Hemofilter: complication and management
Sanil Nair , Harshal Wagh , Kavita Mordani and Salim Bhuiyan
Full Text
PDF
View Point
The dysfunctional relationship between trainer and trainee: mother of all problems
Minal Mistry and Javed Latoo
Full Text
PDF
Clinical Practice
Emergency Contraception
Anita Sharma
Full Text
PDF
Medicine in Pictures
Pictorial essay III: Permanent pacemakers and Oesophageal Doppler probe
Krishnan Melarkode and M Y Latoo
Full Text
PDF
Miscellaneous
Upcoming Medical Conferences & Meetings
Full Text
PDF
Corrections in Previous Issues
Full Text
PDF