A 75 year old woman with a history of prosthetic mitral valve replacement, atrial fibrillation & TIA on warfarin was scheduled for TURBT to be done under spinal anaesthetic. Warfarin was stopped one day prior to admission and heparin infusion commenced on admission, with target APTT 2.5 times the normal. Heparin was stopped 4 hours prior to the spinal anaesthetic, which was difficult due to ankylosing spondylitis and needed four attempts. However, after an atraumatic tap and good sensory motor block, surgery was commenced without incident. Post-operatively, the patient developed a lower respiratory tract infection for which co-amoxyclav was commenced. On the fourth day post-op, the patient developed sudden onset, right leg weakness and paraesthesia, with right lower limb power 3/5, decreased tone and absent reflexes, leading to the diagnosis of a spinal haematoma post spinal anaesthesia. However on further examination, she was also noted to be anaemic with a drop in haemoglobin to 6g/dl, with an INR of 3.4 and an acute renal impairment with a serum creatinine of 120. In addition, bruising in the right flank, abdominal pain and a right iliac fossa mass were also noted. An urgent MRI was booked, but as the patient was haemodynamically unstable, a CT scan was deemed more appropriate, which showed a retroperitoneal bleed into the right illio-psoas. This was confirmed with a spinal MRI done subsequently, which also ruled out any spinal haematoma. The patient was treated conservatively with 5units PCV and 3units FFP. Her clotting profile gradually normalised as did her renal function and her right sensory-motor deficit continues to improve.
Discussion:Retroperitoneal bleed The predilection for bleeding into the retroperitoneal space has not been fully explained but a unique weakness of the vascular and connective tissue has been suggested.2 It is also most commonly seen in association with patients on anticoagulation therapy or haemodialysis, or with bleeding abnormalities,3 and may represent one of the most serious and potentially lethal complications of anticoagulation therapy. The incidence of retroperitoneal haematoma has been reported at 0.6-6.6% of patients undergoing therapeutic anticoagulation.4, 5, 6 Warfarin, unfractionated and low-molecular weight heparin have all been implicated.7 The risk of bleeding during unfractionated heparin therapy has been estimated to be two- to five fold greater than that with warfarin.8 However, it is nonetheless important to note that the therapeutic index of warfarin is narrow 9 and anticoagulant control is easily deranged by drugs (such as antibiotics) and co-morbid factors such as renal or hepatic dysfunction. Frequent INR measurement is the best way to avoid haemorrhagic complications. Patients report lower abdominal or hip pain radiating to the groin or anterior thigh. Bleeding into the psoas muscle causes spasm and hip flexion and, as it extends, flank or thigh bruising may appear. Femoral nerve compression reduces quadriceps power and causes loss of knee jerk and paraesthesia in the area of cutaneous supply. CT scan is the investigation of choice10 but ultrasound is also sensitive and is more rapidly available. Delay in diagnosis is potentially fatal because severe haemorrhage can supervene. Locally the haematoma may cause ureteric obstruction and acute renal failure, or femoral nerve compression.11 (Both of which were seen in the case reported). Treatment options are surgery 12 and conservative management consisting of treating the anaemia associated with the bleed and correcting the coagulopathy.13 Options to treat the coagulopathy would mainly depend on how quickly correction is required, to what range and how long normal clotting indices would be safe in a patient on therapeutic or treatment anticoagulation. Fresh frozen plasma (FFP at a dose 15ml/kg) is given for rapid but short-lived correction with the usual risks of transfusion of blood products. Vitamin K (>2.5mg) is given for a slower but more prolonged correction (leaving patients with artificial valves at risk of thromboembolic events and valve failure). Over-anticoagulation due to warfarin can be reversed completely and immediately by infusion of a complex concentrate of factors 2, 7, 9 and 10.14Spinal haematoma The true incidence of spinal haematoma is unknown and due to its rarity it is very difficultto evaluate risk factors prospectively and any properly poweredstudy would require many thousands of patients to investigatethis. Therefore, data on the incidence of spinal haematoma followingneuraxial blockade are mainly based on audit studies and casereports. Tryba15 reported that the incidence of spinal haematoma afterepidural and spinal anaesthesia is 1 in 150,000 and 1 in 220,000, respectively. The insertion and removal of an epidural catheter appeared to be of far greater importance in the genesis of a spinal hematoma.16, 17 The incidence of spontaneous spinal haematomais rarer still and is estimated at 1 patient per 1,000,000 patientsper year. 18 Central neuraxial blockade has a low incidence of major complications, many of which resolve within 6 months. 19 The symptoms of an acute spinal hematoma include a sharp irradiating back pain of radicular character, and sensory and motor deficits which outlast the expected duration of the anaesthetic. Not all of these symptoms have to be present at the same time. The clinical suspicion can only be confirmed by means of an emergency CT-scan (with myelography) or magnetic resonance imaging.20 The only treatment of a compressing spinal hematoma is an emergency decompressive laminectomy with evacuation of the hematoma. Final neurologic outcome depends on21, 22 the speed with which the hematoma develops; the severity of the preoperative neurologic deficit; the size of the hematoma; and most importantly, the time span between hematoma formation and surgical decompression. Complete recovery of neurologic function is possible if surgery is performed within 8 hours of the onset of the paraplegia. Conclusion The aim of this report is in no way to undermine the importance of Alderman’s advice to suspect the spine as an area of bleeding in patients on anticoagulant therapy. The above case is a reminder to consider retroperitoneal bleeding as one of the differential diagnoses of spinal haematoma in an anticoagulated patient who develops sudden onset spinal pain, with or without neurological deficit post spinal anaesthetic. The presenting symptoms are similar and early management is equally important in terms of associated morbidity when management is delayed.
The genus pseudomonas are Gram-negative, aerobic, rod-shaped bacterium with unipolar motility,[1]contains more than 140 species, most of which are saprophytic. More than 25 species of pseudomonas are associated with humans [2]. Most pseudomonads known to cause disease in humans are associated with opportunistic infections. These include Ps. aeruginosa,Ps. fluorescens, Ps. putida, Ps. cepacia, Ps. stutzeri, Ps. maltophilia, and Ps. putrefaciens. Only two species, Ps. mallei and Ps. pseudomallei, produce specific human diseases: glanders and melioidosis. Ps. aeruginosa and Ps. maltophilia account for approximately 80 percent of pseudomonads recovered from clinical specimens [1,4].
Because of the frequency with which it is involved in human disease, Pseudomonas. aeruginosa has received the most attention. It is a ubiquitous free-living bacterium and is found in most moist environments. Although it seldom causes disease in healthy individuals, it is a major threat to hospitalised and immunocompromised patients, particularly those with serious underlying diseases such as cancer and burns [5]. The high mortality associated with these infections is due to a combination of weakened host defenses, bacterial resistance to antibiotics, and the production of extracellular bacterial enzymes and toxins [6].
Pseudomonas aeruginosa is a leading gram negative pathogen that causes nosocomial infections, accounting for 20% of pneumonia and 16% of urinary tract infections according to recent data from national nosocomial infection surveillance system [7]. According to the CDC, the overall incidence of Pseudomonas aeruginosa infections in U.S. hospitals averages about 0.4 percent (4 per 1000 discharges), and the bacterium is the fourth most commonly isolated nosocomial pathogen accounting for 10.1 percent of all hospital-acquired infections[9].
Resistance of this notorious bacterium to commonly used antimicrobial agents is becoming an increasing clinical problem and a recognised public health threat because there are limited number of antimicrobial agents including the antipseudomonal penicillins, cephalosporins, carbapenems, aminoglycosides and fluoroquinolones with reliable activity against it [11]. It has intrinsic resistance to many antimicrobial agents and only a few antimicrobial agents show potent antibacterial activity against this bacterium. The emergence of multidrug resistance (MDR) Pseudomonas aeruginosa has became a serious problem [12]. There are several mechanisms which may contribute to the antimicrobial resistance among Pseudomonas aeruginosa including the production of chromosomally encoded Amy C B-lactamases [13]. Hypermutable strains of Pseudomonas aeruginosa with defects in themethyl directed mismatch repair (MMR) system are also being frequently isolated from the lungs of cystic fibrosis (CF) patients [13].
MATERIALS AND METHODS:
Samples collection: For this study, a total of 1008 clinical isolates of Pseudomonas aeruginosa, were isolated from 2800 different clinical specimens including; urine (n= 905), ear swabs (n= 496), eye swabs (n=26), fluids (n= 31), pus swabs (n= 342), HVS (n= 157), and sputum (n= 843) received at the microbiology section of Burgor Anklesaria Hospital’s pathological laboratory between January 2008 and September 2008.
Primary isolation of test strains: For the primary isolation of test culture specimens were inoculated on routine culture media including CLED agar (Merck, Germany), EMB agar (Merck, Germany), MacConkey’s agar (Oxoid, UK), and Chocolate agar (Merck, Germany). Pigment production was interpreted on the basis of growth on Nutrient agar (Merck, Germany).
Control stain: ATCC Control strain of Pseudomonas aeruginosa(27853).
Spot tests: Selected colonies were further confirmed by spot tests including; Gram’s stain (Merck, Germany), Oxidase test (Oxoid, UK), Citrate utilisation test (Merck, Germany), and Urease tests (Merck, Germany) [1,4].
Sugar fermentation & IMVIC: Selected colonies were also subjected to Oxidative fermentation and IMVIC i.e. Indole, Methyl reductase test, Vogus prosekure test for confirmation of specie [1,4].
Antibacterial susceptibility testing: Antibacterial susceptibility testing of selected Pseudomonas aeruginosa species was done on Mueller Hinton agar (MHA) (Merck, Germany). To make bacterial suspensions, four to five colonies of pure growth from overnight cultures of test strains were transferred into a tube containing four to five millilitres of nutrient broth (Merck, Germany), and incubated at 37 °C to match the turbidity with McFarland’s index of 0.5 (usually 2-6 hours). Lawns of each bacterial suspension were made on MHA using sterile cotton swabs. Commercially available standard antibiotic discs of standardised concentrations (Oxoid, UK) (Amikacin, Ceftriaxone, Cefotaxime, Sulzone (Cefapeozone+Sulbactum), Meropenam, Ciprofloxacin, and Fosfomycin) were positioned at appropriate distances on the bacterial lawns and incubated at 37 °C for 24 hours. The growth inhibition zones were carefully measured with calipers and recorded according to the standard Kirby-Bauer disc diffusion method[2] and CLSI/NCCLS guidelines 2003 & 2007[8,9,13].
RESULTS:
This study was conducted on 2800 multiple type of clinical specimens received at Burgor Anklesaria Hospital’s pathological laboratory during January 2008 to September 2008. Out of these a total of 1008 clinical isolates were identified as Pseudomonas aeruginosa on the basis of gram’s stain and spot test reactions. Morphologically all of these isolates were gram negative, non sporing, capsulated, and motile short rods, produced typical grapes like odor of amino acetophenone and blue water soluble non fluorescent pigment pyocyanin.They were also positive for oxidase and citratase with variable ability to utilize urea agar. Of these1008 Ps. aeruginosa, 532 isolates were from male patients (504 adults and 28 children), and 476 isolates were from female patients (442 adults and 34 children) (Table 1).
Antibacterial susceptibility of seven selected antibiotics was determined against 1008 test strains of
Pseudomonas aeruginosa, using Kirby and Bauer disc diffusion method[2], against commercially available standardised antibiotic filter discs (Oxoid, UK). These strains were isolated from seven different categories of specimens including ear swabs, wound pus, urine, sputum, eye swab, fluids and high vaginal swab (HVS) (Table 2 & 3).
Another interesting observation was that a maximum number of test strains were isolated from urine i.e. 403 (40%). While, only 6 (0.6%) were isolated from eye swabs (Table 2). When susceptibility results were compared according to the age and sex, not a significant difference was observed (Table 3).
Out of a total of 504 isolates from male adults, 45 (9%) were resistant to Amikacin, 140 (28%) were resistant Ciprofloxacin, 185 (37%) were resistant to Cefotaxime, 174 (34%) were resistant to Ceftriaxone, 34 (7%) were resistant to Sulzone, 140 (28%) were resistant to Fosfornycin and 25 (6%) were resistant to Meropenam. Among 28 male children, the maximum resistance was observed to Ciprofloxacin (Table 3) out of 442 isolates from female adults 39 (9%) were resistant to Amikacin 84 (19%) were resistant to Ciprofloxacin, 78 (18%) were resistant to Cefotaxime, 151 (34%) were resistant to Ceftriaxone, 28 (6%) were resistant S ulzone (Cefapeozone+Sulbactum), 145 (33%) were resistant to Fosformycin and 11 (2%) were resistant to Meropenam. On the whole, the maximum resistance was observed from the male adults isolates against Cefotaxime (n=185, 37%) and in the case of isolates from the female adults to Ceftriaxone (n=151, 34%) .
Collectively, we can say that maximum resistance was observed when target cells were subjected to antimicrobial susceptibility testing against third generation Cephalosporins i.e. Ceftriaxone and Cefotaxime. The most effective antibiotic in the isolates from the male patients was Sulzone (Cefapeozone+Sulbactum) i.e. 465 (92%), while in the case of isolates from female patients it was Meropenam i.e. 414 (94%) (Table 3).
Table 1: Age and Gender wise distribution of clinical isolates of Pseudomonas aeruginosa
Total No. of samples N
2800 n (%)
Positive for Ps. aeruginosa
1008 (36%)
Male adult(>12 years)
504 (50%)
Male children (0-12 years)
28 (3 %)
Female adult (>12 years)
442 (44%)
Female children (0-12 years)
34 (3%)
Table 2: Resistance of Pseudomonas aeruginosa from different clinical specimens toantibiotics determined by Kirby-Bauer disc diffusion method
%=Percentage,n= Individual type of sample,N=Total number of sample,AK= Amikacin (R =>22 mm),CRO= Ceftriaxone (R=>21 mm),CTX=Cefotaxime (R=>22 mm),SCF= Sulzone (R= > 20 mm) (Cefapeozone+Sulbactum), MEM=Meropenam (R= >18 mm), CIP=Ciprofloxacin (R= > 21mm),FOS=Fosfomycin (R= > 18mm ),µgms= micro grams, S= sensitive
Table 3: Age and Gender wise sensitivity of Pseudomonas aeruginosa from different clinical specimens to antibiotics determined by Kirby-Bauer disc diffusion method
% =Percentage,n= Individual type of sample,N=Total number of sample,AK= Amikacin (R =>22 mm),CRO= Ceftriaxone (R=>21 mm),CTX=Cefotaxime (R=>22 mm),SCF= Sulzone (R= > 20 mm) (Cefapeozone+Sulbactum), MEM=Meropenam (R= >18 mm), CIP=Ciprofloxacin (R= > 21mm),FOS=Fosfomycin (R= > 18mm ),µgms= micro grams, S= sensitive
DISCUSSION:
Pseudomonasaeruginosa is a leading Gram-negative pathogen thatcauses nosocomial infections, accounting for 20% of pneumoniaand 16% of urinary tract infections according to recent datafrom the National Nosocomial Infections Surveillance System [1].
Optimisation of therapy against Pseudomonas aeruginosa starts with the initial empirical antibiotic choice. Surveillance data and hospital or unit antibiograms may inform this decision, although individualisation of the initial regimen on the basis of prior antibiotic use and prior isolation of resistant pathogens may be more important. Combinations of antibiotics are often required empirically, and "combination antibiograms" may need to be developed for this purpose. Preliminary data suggest that extending the time over which a dose of antipseudomonal beta-lactam antibiotics is infused may improve clinical outcomes; however, this idea remains to be confirmed in randomised trials. For example Moody et al in 1972 showed that some of the Pseudomonas speciesother than Pseudomonas. aeruginosa were resistant to a number of antibiotics.Among these were antibiotics that are in general use for P.aeruginosa infections. Such differences in antibiotic susceptibilities emphasise the necessity for careful speciation of this groupof microorganisms to assure proper epidemiological documentationof colonisation and infection, as well as to ensure therapywith an antimicrobial agent to which the organism is susceptiblein vitro. The role of direct susceptibility testing in aiding more rapid initiation of appropriate antibiotic therapy is also being studied. When identification and susceptibility testing is complete, the antibiotic regimen for infections due to Gram-negative pathogens can be "fine tuned." On some occasions, this fine tuning necessitates the introduction of "salvage" antibiotics, such as Colistin or Tigecycline; on others, it necessitates de-escalation and early termination of therapy. The lack of new antibiotic options against gram-negative pathogens underscores the need for optimisation of current therapies and prevention of the spread of these organisms.
In 2008 Javiya etal reported the highest number of Pseudomonas infections was found in urine, followed by pus and sputum. Pseudomonas species demonstrated marked resistance against monotherapy of penicillins, cephalosporins, fluoroquinolones, tetracyclines and macrolides. Only combination drugs like Ticarcillin + Clavulanic acid, Piperacillin + Tazobactum, Cefoperazone + Sulbactum, Cefotaxime + Sulbactum, Ceftriaxome + Sulbactum and monotherapy of Amikacin showed higher sensitivity to Pseudomonas infections; however, the maximum sensitivity was shown by the Carbapenems.
Our study was therefore carried out, using Kirby-Bauer method [2], to determine the antibiotic susceptibility patterns of Pseudomonas aeruginosa isolates from in-patients and out-patients attending the microbiology section of Burgor Anklesaria Hospital’s pathological laboratory between January 2008 and September 2008. The isolation rate of Pseudomonas aeruginosa in clinical specimens was found to be 36%, with the highest occurrence of 403 (40%) in urine samples followed by 258 (26%) occurrence in ear swabs. The susceptibility pattern showed that 85% were sensitive to Meropenam and 84% to Sulzone (Cefapeozone+Sulbactum). The isolates from the male patients showed almost equal resistance to all the antibiotics tested, as in case of isolates from the female patients, most especially Ceftriaxone and Cefotaxime. However, no consistent antibiotic susceptibility pattern could be established for this pathogenic bacterium based on sources.
Treatment of Pseudomonas aeruginosa is a challenge because resistance limits dramatically therapeutic options. In this review, we discuss data of in vitro susceptibility for the management of infections caused by Pseudomonas aeruginosa. Currently, published data from Pakistan are limited, and there are no such randomised clinical trials involving the treatment of infections caused by multidrug resistant Gram-negative rods. At present newer antimicrobial agents active against multidrug resistant bacteria like Pseudomonas aeruginosa are not available or under investigation.
CONCLUSION:
Antibiotic resistant organisms appear to be biologicallyfit and are capable of causing serious, life-threatening infectionsthat are difficult to manage because treatment options are limited.This increase in the prevalence of drug resistant pathogensis occurring at a time when the discovery and development ofnew anti-infective agents is slowing down dramatically.
The Pseudomonas aeruginosa species isolated from patients in the Microbiology section of Burgor Anklesaria Hospital’s pathological laboratory, Karachi, Pakistan were tested in vitro for antibacterial susceptibility of currently available and commonly prescribed drugs. Meropenam and Sulzone were the two antibiotics found to be the most susceptible against this pathogen. The emergence of multidrug resistant (MDR) Pseudomonas aeruginosa is a challenging clinical problem. This study investigated the pattern of antibiotic resistance to test antibiotics and helps us in determining the role of combination therapy in its management. The results of this study suggest that use of triple antimicrobial therapy (Meropenam, Sulzone and Amikacin) can be a useful alternative treatment for multidrug resistant (MDR) Pseudomonas aeruginosa infection in certain circumstances.
Chronic infections appear to be common features of various diseases, including neurodegenerative, psychiatric and neurobehavioral diseases, autoimmune diseases, fatiguing illnesses and other conditions.1-4 Neurodegenerative diseases, chronic degenerative diseases of the central nervous system (CNS) that cause dementia, are mainly diseases of the elderly. In contrast, neurobehavioral diseases are found mainly in younger patients and include autism spectrum disorders (ASD), such as autism, attention deficit disorder, Asperger’s syndrome and other disorders.5 For the most part, the causes of these neurological diseases remain largely unknown.2 Neurodegenerative diseases are characterized by molecular and genetic changes in nerve cells that result in nerve cell degeneration and ultimately nerve cell dysfunction and death, resulting in neurological signs and symptoms and dementia.2,3 On the other hand, neurobehavioral diseases are related to fetal brain development but are less well characterized at the cellular level and involve both genetic and environmental factors.6, 7 Even less well characterized at the cellular and genetic level are the psychiatric disorders, such as schizophrenia, paranoia, bipolar disorders, depression and obsessive-compulsive disorders.
Genetic linkages have been found in neurodegenerative and neurobehavioral diseases, but the genetic changes that occur and the changes in gene expression that have been found are complex and usually not directly related to simple genetic alterations.2, 6-8 In addition, it is thought that nutritional deficiencies, environmental toxins, heavy metals, chronic bacterial and viral infections, autoimmune immunological responses, vascular diseases, head trauma and accumulation of fluid in the brain, changes in neurotransmitter concentrations, among others, are involved in the pathogenesis of various neurodegenerative and neurobehavioral diseases.2, 3, 5-16 One of the biochemical changes found in essentially all neurological, neurodegenerative and neurobehavioral diseases is the over-expression of oxidative free radical compounds (oxidative stress) that cause lipid, protein and genetic structural changes.9-11 Such oxidative stress can be caused by a variety of environmental toxic insults, and when combined with genetic factors could result in pathogenic changes.14
Neurodegenerative diseases
Infectious agents are important factors in neurodegenerative and neurobehavioral diseases and may enter the brain within infected migratory macrophages. They may also gain access by transcytosis across the blood-brain-barrier or enter by intraneuronal transfer from peripheral nerves.15 Cell wall-deficient bacteria, such as species of Mycoplasma, Chlamydia (Chlamydophila), Borrelia and Brucella, among others, and various viruses are candidate brain infectious agents that may play important roles in neurodegenerative and neurobehavioral diseases.16-19 Such infections are systemic and can affect the immune system and essentially any organ system, resulting in a variety of systemic signs and symptoms.4, 15, 16, 19, 20
Amyotrophic lateral sclerosis
Amyotrophic lateral sclerosis (ALS) is an adult-onset, idiopathic, progressive neurodegenerative disease that affects both central and peripheral motor neurons.21 Patients show gradual progressive weakness and paralysis of muscles due to destruction of upper motor neurons in the motor cortex and lower motor neurons in the brain stem and spinal cord. This ultimately results in death, usually by respiratory failure.21, 22 The overall clinical picture of ALS can vary, depending on the location and progression of pathological changes.23
The role of chronic infections has attracted attention with the finding of enterovirus sequences in a majority of ALS spinal cord samples by polymerase chain reaction (PCR).24 However, others have failed to detect enterovirus sequences in spinal cord samples from patients with or without ALS.25-26 In spite of the mixed findings on enterovirus, infectious agents that penetrate the CNS could play a role in the aetiology of ALS. Evidence for transmission of an infectious agent or transfer of an ALS-like disease from man-to-man or man-to-animals has not been found.27
Using PCR methods systemic mycoplasmal infections have been found in a high percentage of ALS patients.28, 29 We found that 100% of Gulf War veterans from three nations diagnosed with ALS had systemic mycoplasmal infections.28 All but one patient had M. fermentans, and one veteran from Australia had a systemic M. genitalium infection. In nonmilitary ALS patients systemic mycoplasmal infections of various species were found in approximately 80% of cases.28 Of the mycoplasma-positive civilian patients who were further tested for various species of Mycoplasma, most were positive for M. fermentans (59%), but other Mycoplasma species, such as M. hominis (31%) and M. pneumoniae infections (9%) were also present. Some of the ALS patients had multiple infections; however, multiple mycoplasmal infections were not found in the military patients with ALS.28 In another study 50% of ALS patients showed evidence of systemic Mycoplasma species by PCR analysis.29
ALS patients who live in certain areas often have infections of Borrelia burgdorferi, the principal aetiological agent in Lyme disease. For example, ALS patients who live in a Lyme-prevalent area were examined for B. burgdorferi infections, and over one-half were found to be seropositive for Borrelia compared to 10% of matched controls.30 In addition, some patients diagnosed with ALS were subsequently diagnosed with neuroborreliosis.31 Spirochetal forms have been observed in the brain tissue of ALS patients and in patients with other neurodegenerative diseases.32 In general, however, the incidence of Lyme infections in ALS patients is probably much lower. In one recent study on 414 ALS patients only about 6% showed serological evidence of Borrelia infections.33 Some Lyme Disease patients may progress to ALS, but this is probably only possible in patients who have the genetic susceptibility genes for ALS as well as other environmental toxic exposures.34, 35
Additional chronic infections have been found in ALS patients, including human herpes virus-6 (HHV-6), Chlamydia pneumoniae andother infections.36, 37 There is also a suggestion that retroviruses might be involved in ALS and other motorneuron diseases.38 McCormick et al.39 looked for reverse transcriptase activity in serum and cerebrospinal fluid of ALS and non-ALS patients and found reverse transcriptase activity in one-half of ALS serum samples tested but in only 7% of controls. Interestingly, only 4% of ALS cerebrospinal fluid samples contained reverse transcriptase activity.39
Although the exact cause of ALS remains to be determined, there are several hypotheses on its pathogenesis: (1) accumulation of glutamate causing excitotoxicity; (2) autoimmune reactions against motor neurons; (3) deficiency of nerve growth factor; (4) dysfunction of superoxide dismutase due to mutations; and (5) chronic infection(s).24, 27-40 None of these hypotheses have been ruled out or are exclusive, and ALS may have a complex pathogenesis involving multiple factors. 28, 36
It is tempting to propose that infections play an important role in the pathogenesis or progression of ALS.28, 40 Infections could be cofactors in ALS pathogenesis, or they could simply be opportunistic, causing morbidity in ALS patients. For example, infections could cause the respiratory and rheumatic symptoms and other problems that are often found in ALS patients. Since the patients with multiple infections were usually those with more rapidly progressive disease,28 infections likely promote disease progression. Indeed, when Corcia et al.41 examined the cause of death in 100 ALS patients, the main causes were broncho-pneumonia and pneumonia. Finally, there are a number of patients who have ALS-like signs and symptoms but fall short of diagnostic criteria. Although a careful study has not been attempted on these patients, there is an indication that they have the same infections as those found in patients with a full diagnosis of ALS (personal communication). Thus ALS-like diseases may represent a less progressive state, in that they may lack additional changes or exposures necessary for full ALS.
Multiple sclerosis
Multiple sclerosis (MS) is the most common demyelinating neurological disease. It can occur in young or older people and is a cyclic (relapsing-remitting) or progressive disease that continues progressing without remitting.42 Inflammation and the presence of autoimmune antibodies against myelin and other nerve cell antigens are thought to cause the myelin sheath to break down, resulting in decrease or loss of electrical impulses along the nerve fibers.42, 43 In the progressive subset of MS neurological damage occurs additionally by the deposition of plaques on the nerve cells to the point where nerve cell death occurs. In addition, breakdown of the blood-brain barrier in MS is associated with local inflammation caused by glial cells.42, 43 The clinical manifestations of demyelinization, plaque damage and blood-brain barrier disruptions cause variable symptoms, but they usually include impaired vision, alterations in motor, sensory and coordination systems and cognitive dysfunction.43
There is strong evidence for a genetic component in MS.44, 45 Although it has been established that there is a genetic susceptibility component to MS, epidemiological and twin studies suggest that MS is an acquired, rather than an inherited, disease.46
MS has been linked to chronic infection(s).46, 47 For example, patients show immunological and cytokine elevations consistent with chronic infections.48-50 An infectious cause for MS has been under examination for some time, and patients have been tested for various viral and bacterial infections. 44, 45,47, 48, 51 One of the most common findings in MS patients is the presence of C. pneumoniae antibodies and DNAin their cerebrospinal fluid.51-53 By examining relapsing-remitting and progressive MS patients for the presence of C. pneumoniae in cerebrospinal fluid by culture, PCR and immunoglobulin reactivity Sriram et al.52 were able to identify C. pneumoniae in 64% of MS cerebrospinal fluid versus 11% of patients with other neurological diseases. They also found high rates (97% positive) of PCR-positive MOMP gene in MS- patients versus 18% in other neurological diseases, and this correlated with 86% of MS patients being serology-positive patients by ELISA and Western blot analysis.52 Examination of MS patients for oligoclonal antibodies against C. pneumoniae revealed that 82% of MS patients were positive, whereas none of the control non-MS neurological patients had antibodies that were absorbed by C. pneumoniae elemental body antigens.53 Similarly, Contini et al.54 found that the DNA and RNA transcript levels in mononuclear cells and cerebrospinal fluid of 64.2% of MS patients but in only 3 controls.
Using immunohistochemistry Sriram et al.55 later examined formalin-fixed brain tissue from MS and non-MS neurological disease controls and found that in a subset of MS patients (35%) chlamydial antigens were localized to ependymal surfaces and periventricular regions. Staining was not found in brain tissue samples from other neurological diseases. Frozen tissues were available in some of these MS cases, and PCR amplification of C. pneumoniae genes was accomplished in 63% of brain tissue samples from MS patients but none in frozen brain tissues from other neurological diseases. In addition, using immuno-gold-labeled staining and electron microscopy they examined cerebrospinal fluid sediment for chlamydial antigens and found that the electron dense bodies resembling bacterial structures correlated with PCR-positive results in 91% of MS cases.55 They also used different nested PCR methods to examine additional C. pneumoniae gene sequences in the cerebrospinal fluid of 72 MS patients and linked these results to MS-associated lesions seen by MRI.56
MRI was used by Grimaldi et al.57 to link the presence of C. pneumoniae infection with abnormal MRI results and found linkage in 21% of MS patients. These turned out to be MS patients with more progressive disease.58 In addition, higher rates of C. pneumoniae transcription were found by Dong-Si et al.58 in the cerebrospinal fluid of 84 MS patients. The data above and other studies strongly support the presence of C. pneumoniae in the brains of MS patients,59-61 at least in the more progressed subset of MS patients.
Other research groups have also found evidence for C. pneumoniae in MS patients but at lower incidence. Fainardi et al.62 used ELISA techniques and found that high-affinity antibodies against C. pneumoniae were present in the cerebrospinal fluid of 17% of MS cases compared to 2% of patients with non-inflammatory neurological disorders. They found that the majority of the progressive forms of MS were positive compared to patients with remitting-relapsing MS. The presence of C. pneumoniae antibodies was also found in other inflammatory neurological disorders; thus it was not found to be specific for MS.62
In contrast to the studies above, other researchers have not found the presence of C. pneumoniaeor other bacteriain the brains of MS patients.63-65 For example, Hammerschlag et al.66 used nested PCR and culture to examine frozen brain samples from MS patients but could not find any evidence for C. pneumoniae. However, in one study C. pneumoniae was found at similar incidence in MS and other neurological diseases, but only MS patients had C. pneumoniae in their cerebrospinal fluid.64 Swanborg et al.67 reviewed the evidence linking C. pneumoniae infection with MS and concluded that it is equivocal, and they also speculated that specific genetic changes may be necessary to fulfill the role of such infections in the aetiology of MS.
Another possible reason for the equivocal evidence linking MS with infections, such as C. pneumoniae, is that multiple co-infections could be involved rather than one specific infection. In addition to C. pneumoniae found in most studies, MS patients could also have Mycoplasma species, B. burgdorferi and other bacterial infections as well as viral infections.68 When multiple infections are considered, it is likely that >90% of MS patients have obligate intracellular bacterial infections caused by Chlamydia (Chlamydophila), Mycoplasma, Borrelia or other intracellular bacterial infections. These infections were found only singly and at very low incidence in age-matched subjects.68 In spite of these findings, others did not find evidence of Mycoplasma species in MS brain tissue, cerebrospinal fluid or peripheral blood.69
Viruses have also been found in MS. For example, HHV-6 has been found at higher frequencies in MS patients, but this virus has also been found at lower incidence in control samples.70 Using PCR Sanders et al.70 examined postmortem brain tissue and controls for the presence of various neurotrophic viruses. They found that 57% of MS cases and 43% of non-MS neurological disease controls were positive for HHV-6, whereas 37% and 28%, respectively, were positive for herpes simplex virus (HSV-1 and -2) and 43% and 32%, respectively, were positive for varicella zoster virus. However, these differences did not achieve statistical significance, and the authors concluded “an etiologic association to the MS disease process [is] uncertain.” They also found that 32% of the MS active plaques and 17% of the inactive plaque areas were positive for HHV-6.70 Using sequence difference analysis and PCR Challoner et al.71 searched for pathogens in MS brain specimens. They found that >70% of the MS specimens were positive for infection-associated sequences. They also used immunocytochemistry and found staining around MS plaques more frequently than around white matter. Nuclear staining of oligodendrocytes was also seen in MS samples but not in controls.71 Using immunofluorescent and PCR methods HHV-6 DNA has also been found in peripheral leukocytes in the systemic circulation of MS patients.72, 73 However, using PCR methods, others did not found herpes viruses in the peripheral blood or CSF of MS patients.74, 75 Evidence that prior infection with EBV could be related to the development of MS was proposed; however, EBV infects more than 90% of humans without evidence of health problems and 99% of MS patients.76 The difference in MS patients could be the presence of multiple infections, including EBV. Recently Willis et al.77 used multiple molecular techniques to examine MS tissue but failed to find EBV in any MS tissues but could find EBV in CNS lymphomas.
Current reviews and the information above points to an infectious process in MS.47, 48, 75, 76, 78-80 Although a few studies did not come to this conclusion,74, 75 most studies have found infections in MS patients. It is interesting that it is the progressive rather than relapsing-remitting forms of MS which have been associated with chronic infections; therefore, infections might be more important in MS progression than in its inception. Various infections may also nonspecifically stimulate the immune system.47, 48 Infections may also invade immune cells and alter immune cell function in a way that promotes inflammation and autoimmune activity.78 If infections like C. pneumoniae and Mycoplasma species are important in MS, then antibiotics effective against these infections should improve clinical status. Although preliminary, that is in fact what has been seen, but not in all patients.81 As in other neurodegenerative diseases, multiple factors appear to be involved in the pathogenesis of MS.
Alzheimer’s disease
Alzheimer’s Disease (AD) is a family of brain disorders usually found in elderly patients and is the most common cause of dementia. AD is characterized by slow, progressive loss of brain function, notable lapses in memory, disorientation, confusion, mood swings, changes in personality, language problems, such as difficulty in finding the right words for everyday objects, loss of behavioral inhibitions and motivation and paranoia. The course of AD varies widely, and the duration of illness can range from a few years to over 20 years. During this period the parts of the brain that control memory and thinking are among the first affected, followed by other brain changes that ultimately result in brain cell death.82
AD is characterized by distinct neuropathological changes in brain tissues and cells. Among the most notable are the appearance of plaques and tangles of neurofibrils within brain nerve cells that affect synapses and nerve-nerve cell communication. These structural alterations involve the deposition of altered amyloid proteins.83, 84 Although the cause of AD is not known, the formation of the amyloid plaques and neurofibrillary tangles may be due to genetic defects and resulting changes in the structure of beta amyloid proteins. This in turn may be caused by chemicals or other toxic events, inflammatory responses, excess oxidative stress and increases in reactive oxygen species, loss of nerve trophic factors and reductions in nerve cell transmission.83-87
Recently AD brain infections have become important.88-90 For example, one pathogen that has attracted considerable attention is C. pneumoniae.91, 92 As mentioned above, this intracellular bacterium has a tropism for neural tissue, and it has been found at high incidence in the brains of AD patients by PCR and immunohistochemistry.92C. pneumoniae has also been found in nerve cells in close proximity to neurofibrillary tangles.92, 93 Similarly to Mycoplasma species, C. pneumoniae can invade endothelial cells and promote the transmigration of monocytes through human brain endothelial cells into the brain parenchyma.94C. pneumoniae has been found in the brains of most AD patients,91 and it has been cultured from AD brain tissue.95 Injection of C. pneumoniae into mice stimulates beta amyloid plaque formation.96 Although the data are compelling, some investigators have not found C. pneumoniae infections in AD.97, 98
AD patients also have other bacterial infections, such as B. burgdorferi.99 Using serology, culture, Western blot and immunofluorenscence methods this Lyme Disease infection has been examined in AD.100, 101 Not all researchers, however, have found evidence of B. burgdorferi in AD patients.102, 103 The presence of intracellular infections like B. burgdorferi in AD patients has been proposed to be a primary event in the formation of AD beta amyloid plaques. This is thought to occur by the formation of “congophilic cores” that attract beta amyloid materials.104 Multiple reports indicate that AD nerve cells are often positive for B. burgdorferi, indicating that this intracellular bacteria could be important in the pathogenesis of AD.99, 100, 104, 105
The hypothesis in AD that intracellular microorganisms could provide “cores” for the attraction of beta amyloid materials is appealing, but other factors, including the induction of reactive oxygen species, lipid peroxidation and the breakdown of the lysosomal membranes releasing lysosomal hydrolases, are also thought to be important in beta amyloid deposition.105 That infections may be important in AD pathogenesis is attractive; however, some negative reports have not confirmed the presence of infections like B. burgdorferi in AD patients.99-101 This suggests that the infection theory, although compelling, remains controversial.102, 105
Herpes virus infections have also been found in AD,especially HSV-1.106, 107 Previously it was determined that HSV-1 but not a related neurotrophic virus (varicella zoster virus) is present more often in AD brains, and this could be linked to AD patients who have the risk factor ApoE e4 allele.108, 109 HSV-1 is thought to be involved in the abnormal aggregation of beta amyloid fragments within the AD brain by reducing the amount of full-length beta amyloid precursor protein and increasing the amounts of their fragments.110 HSV-1 infection of glial and neuronal cells results in a dramatic increase in the intracellular levels of beta amyloid forms, whereas the levels of native beta amyloid precursor protein are decreased.111 This is similar to what has been found in mice infected with HSV-1, indicating that HSV-1 is probably involved directly in the development of senile-associated plaques. Another herpes virus, HHV-6, has also been found in AD patients, but it is thought that this virus is not directly involved in AD pathogenesis. HHV-6 may exacerbate the effects of HSV-1 in AD ApoE e4 carriers.112
Other infections have been found in AD patients, for example, C. pneumoniae, Helicobacter pylori amongst others.113 It has been proposed that such infections may act as a trigger or co-factor in AD.114 Although experimental evidence that pathogens can elicit the neuropathological changes and cognitive deficits that characterize AD is lacking, this approach may yield interesting and important results. These authors also stressed that systemic infections must be considered as potential contributors to the pathogenesis of AD.114
Parkinson’s disease
Parkinson’s disease (PD) is characterized by akinesia, muscular rigidity and resting tremor.103 In addition, autonomic dysfunction, olfactory disturbances, depression, sensory and sleep disturbances and frequently dementia characterize this disease.115 The pathology of PD indicates a progressive loss of the dopamine neurons of the substantia nigra together with the presence of Lewy bodies and alpha-synuclein. More extensive brain degeneration also occurs, from the medulla oblongata to the cerebral cortex.116, 117
Age-related inclusion bodies and protein aggregations or defects in their degradation characteristically occur in PD, but their role in PD pathogenesis remains unclear.117, 118 Some evidence suggests a relationship between PD and specific genetic changes, such as changes in the genes affecting mitochondria, protein degradation, organelle trafficking and vesicular fusion, and in proteins involved in oxidative stress or antioxidant function.102 Inflammation has also been associated with PD pathology.119
The pathogenesis of PD has been proposed to be due to multiple genetic and neurotoxic events that produce oxidative damage and cell death. In the case of PD the relevant targets of toxic events are neuromelanin-containing dopaminergic neurons of the substantia nigra.118, 120 A case-control study indicated that multiple environmental factors and genetic background were statistically related risk factors for PD.121 Prominent among these were long-term toxic exposures and trauma early in life.122 For example,early life exposure to brain injury, chemicals and/or infections may initiate a cyclic inflammatory process involving oxidative damage, excitotoxicity, mitochondrial dysfunction and altered proteolysis that later in life results in substantia nigra neuron death.123, 124
A role for chronic infections in PD pathogenesis has been proposed.123, 124 One infection found in PD that has aroused considerable interest is the presence of chronic gastrointestinal Helicobacter pylori.125 Indeed, treatment of this infection offers relief to late stage cachexia in PD patients receiving L-dopa.126Helicobacter pylori-infected PD patients showed reduced L-dopa absorption and increased clinical disability,127 whereas treatment of this infection increased L-dopa absorption and decreased clinical disability.128H.pylori may not be directly involved in the pathogenesis of PD, but its systemic presence could affect the progression and treatment of PD, probably by stimulating inflammation and autoimmunity.128
Chronic infections in PD have been linked to inflammation and autoimmune responses.129-131 Experimental models of PD have been developed using neurological viral or bacterial infections to initiate the pathogenic process.132, 133 Spirochetes have also been found in Lewy bodies of PD patients.30 Other infections, such as viral encephalitis,134 AIDS-associated opportunistic infections of the basal ganglia,135 coronavirus,136 among other infections,68, 137, 138 have been found in PD and could be important in stimulating inflammation and autoimmune responses. It has been stressed that additional research will be necessary to establish whether a causal link exists between PD and chronic infections.139
Neurobehavioral diseases
Autism spectrum disorders
ASD, such as autism, Asperger’s syndrome, etc., are neurobehavioral diseases of primarily the young where patients generally suffer from an inability to communicate properly, form relationships with others and respond appropriately to their environment. Such patients do not all share the same signs and symptoms but tend to share certain social, communication, motor and sensory problems that affect their behavior in predictable ways. These patients often display repetitive actions and develop troublesome fixations with specific objects, and they are often painfully sensitive to certain sounds, tastes and smells.140, 141
ASD cases are likely to be caused by multiple factors, including genetic defects, heavy metal, chemical and biological exposures, among other important events, which are probably different in each patient. ASD patients appear to have similarities in genetic defects and environmental exposures that are important in patient morbidity or in illness progression.5-8, 140-142
Chronic infections appear to be an important element in the development of ASD.6, 16, 143, 144 In ASD patients more than 50 different bacterial, viral and fungal infections have been found,6 some apparently more important than others in causing symptoms. It has been known for some time that ASD patients have a number of nonspecific chronic signs and symptoms, such as fatigue, headaches, gastrointestinal, vision problems, occasional intermittent low-grade fevers and other signs and symptoms that are generally excluded in the diagnosis of ASD but are consistent with the presence of infections.143 Indeed, increased titres to various viruses as well as bacterial and fungal infections have been commonly seen in ASD patients.6, 16, 19, 143-145 Not withstanding these reports, epidemiological evidence for an association of childhood infections in the first two years of life and ASD has been mixed.146
Environmental exposures to chemicals and heavy metals also appear to be important in the development of ASD.140, 141, 147, 148 The relationship between ASD and heavy metals may involve the role of multiple vaccines in ASD pathogenesis.130, 141 ASD patients often show their first signs and symptoms after multiple childhood immunizations, and the sharp increase in Autism rates occurred only after the multiple MMR vaccine came into widespread use.141 In some states in the U.S. children receive as many as 33 vaccines before they can enroll in school.140 Such vaccines can contain mercury and other toxic preservatives, and some may also contain contaminating bacteria, as found in veterinary vaccines.149
There are very few studies that have followed the transmission of infections and subsequent autism. Previously we found that veterans of the Gulf War with chronic fatiguing illnesses (Gulf War illnesses, GWI) exhibited multiple nonspecific signs and symptoms similar to chronic fatigue syndrome/myalgic encephalomyopathy (CFS/ME).150, 151 After returning to the home with GWI, their children subsequently became symptomatic, and these children were often diagnosed with ASD.152, 153 Symptomatic children (mostly diagnosed with ASD) were infected with the same Mycoplasma species, M. fermentans, that was found in the veterans and their symptomatic family members, and this was not seen in aged-matched control subjects or in military families without GWI. In the GWI families some non-symptomatic family members did have mycoplasmal infections (~10%), but this was not significantly different from the incidence of mycoplasmal infections in healthy control subjects.152, 153
Subsequently ASD patients who were not in military families were examined for systemic mycoplasmal infections.153 The majority (~54%) were positive for mycoplasmal infections. However, in contrast to the children of GWI patients who for the most part had only M. fermentans, the civilian children tested positive for a variety of Mycoplasma species. We also tested a few siblings without apparent signs and symptoms, and for the most part few had these infections.153 In another study we examined the blood of ASD patients from Central and Southern California and found that a large subset (>58%) of patients showed evidence of Mycoplasma infections compared to age-matched control subjects (Odds Ratio=13.8, p<0.001).19 ASD patients were also examined for C. pneumoniae (8.3% positive, Odds Ratio=5.6, p<0.01) and HHV-6 (29.2% positive, Odds Ratio=4.5, p<0.01). The results indicated that a large subset of ASD patients display evidence of bacterial and/or viral infections (Odds Ratio=16.5, p<0.001).19
ASD patients have been examined for B. burgdorferi infections.154 Various studies revealed that 22-30% of ASD patients (N=76) have Borrelia infections.6, 154 The incidence of Borrelia infections in ASD patients may be related to Lyme disease distribution, with some Lyme-intense areas having high prevalence, and other areas having a low prevalence. Other infections, such as Lyme-associated Bartonella, Babesia, Ehrlichia and non-Lyme-associated CMV, Plasmodium species, Toxoplasma species and Treponema species may also be associated with ASD.6
Final comments to part 1
When neurological symptoms are present, infections of the CNS must be considered. Brain infections can stimulate glial responses, and the presence of viral and bacterial infections in nerve cells, can stimulate autoimmune responses against nerve cell antigens as well as the infections within them.155 For example, in MS some 20 different bacterial and viral infections have been found, but the link between these infections and the pathogenesis of MS is still being debated.16,47, 75 One or even a few types of infections cannot be causally linked to MS, and the reason for this is that there may be too many possibilities. No one infection or a group of infections needs to be the trigger in MS to be important in the pathogenesis of MS. In time combinations of certain infections may eventually be identified at least in a subset of MS patients, and this will allow the development of new therapeutic approaches for many MS patients that are not recognized today.
One problem that is rarely discussed is the apparent disparity between the laboratory results from different laboratories. Often different laboratories cannot agree on types of infections found in various chronic diseases.47 There are a number of reasons for this, including differences in the source of materials, qualities of reagents and techniques used.16 Some procedures, such as PCR, have specific challenges that must be overcome in the handling of specimens, their stability, presence of interfering substances, contamination, sensitivity and specificity of the tests and interpretation of the results. Variability in results from different laboratories will remain a problem unless research groups work closely together to solve these problems. One example of how this has been overcome is a multi-centre research study on the presence of C. pneumoniae in the cerebrospinal fluid of clinically defined, mono-symptomatic MS patients.156Sriram et al.156 conducted this diagnostic trial with good concordance of results between different laboratories. Cooperative studies such as this should eventually alleviate discrepancies in the types of infections found by different research groups.
This review continues in Part 2 with psychiatric diseases, autoimmune diseases, fatiguing illnesses, and other infectious diseases with neurological aspects and an overall discussion of the topic. 157
The herniation of a gravid uterus through an incisional hernia site is a rare occurrence. Incisional hernia is a frequent complication of abdominal wall closure and the management of pregnancy with a large incisional hernia with gravid uterus in its sac is challenging. The following is a case report of gravid uterus through an incisional hernia of a midline incision. Case Report Mrs LB, 35 years, Parity 2, period of amenorrhea of 34 weeks 3 days, married for 12 years was admitted to the hospital from the outpatient department due to the ulceration of abdominal skin as a result of herniation of gravid uterus through the midline longitudinal incision of a previous caesarean section . She was a booked case of our hospital and had been receivingantenatal care since 20 weeks of gestation. At 20 weeks there was no herniation of the uterus through the incision line. In her subsequent visits she came with the uterus protruding through the incisional hernia. She was referred to the General Surgeon who recommended elective Caesarean section with repair of hernia. Her past obstetric history revealed that she had her first emergency caesarean section eight years before because of a breech presentation and a second caesarean section, due to thepremature rupture of membranes at term. Both the babies were living & well. On both occasions she was operated on through infra umbilical midline vertical incision. There was no history of caesarean section wound infection during the post operative period in the previous two pregnancies. On examination, she was moderately built and adequately nourished. There was mild pallor. Her pulse rate was 88 beats per minute and her blood pressure was 126/86 mm Hg. Heart and chest were normal. Abdominal examination revealed distention of the abdomen in thecentral area. The uterus was felt just underneath the skin with acomplete lack of anterior abdominal wall. (Figure I) Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair.
Bronchogenic cysts are lesions of congenital origin derived from the primitive foregut. They form due to ectopic budding of the foregut during the first trimester. Epithelial cells of the developing trachea and lung are pinched off and grow separately from the airways. Bronchogenic cysts are most commonly mediastinal, unilocular and contain clear fluid. Clinically, most cysts are symptomatic and occur in infancy or early childhood. Respiratory distress is the most common presentation in paediatric patients, manifested by recurring episodes of cough, stridor, and wheezing. Patient Description: A 13-year-old female presented with a two month history of right-sided back pain and five days of intermittent fever. The pain was worse on inspiration and made sleeping difficult. She denied wheezing, chest pain, or cough. She continued daily participation in competitive sports. Previous trials of antibiotics and an inhaled bronchodilator for presumed exercise-induced asthma were unsuccessful. Chest x-ray (CXR) showed a large cyst (10x10x8 cm3) in the posterior right lung. (Image 1). Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2) Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4) Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid. Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung. Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
Bronchogenic cyst should be included in the differential diagnosis of a child with cough, dyspnoea, and fever. Although rare, we stress the importance of keeping mycobacterial infection in mind in cases of an infected cyst. Acid-fast culture should be done on sputum and cyst contents. Due to the frequency of negative cultures, stains should also be performed on resected cyst specimens. Antibiotic therapy should be considered and administered based on the extent of infection. All symptomatic or enlarging cysts warrant surgical excision. Prophylactic removal of asymptomatic cysts is recommended due to higher rates of perioperative complications once cysts become symptomatic.10 We raise the question of whether earlier CXR is indicated to rule out bronchogenic cyst, particularly when patients do not improve after trials of watchful waiting, antibiotics, and bronchodilators for other possible respiratory diagnoses.
Introduction:The aim of the NHS Modernisation Agency’s Hospital at night project is to “Redefine how medical cover is provided in hospitals during the out of hours period.”(1) The project “requires a move from cover requirements defined by professional demarcation and grade, to cover defined by competency in order to release significant amounts of medical staff time and support the compliance with WTD (Working Time Directive) while enhancing clinical practice and training.”(1) Chairman of the BMA’s Junior Doctors Committee and also medical advisor to the Hospital at Night Project undertook a survey of junior doctors’ activity in the evening, night, and weekends. They noted that the evenings were very busy and the nights quieter, that general physicians work harder at night than those in other specialties or orthopaedic surgeons. In summary their survey showed that a huge amount of doctors’ time was wasted on tasks which did not require their level of skills. Such tasks included phlebotomy, searching for notes, and x-rays.(1) An evaluation report into the implementation and impact of the hospital at night pilot project, August 2005, identified key elements to minimize medical workload at night. These included working within a multidisciplinary, competency-based team, with extended skills ward staff to minimize reliance on the night team, reduce duplication, take away inappropriate tasks, bleep-filtering and better use of new technologies such as digital imaging and e-prescribing (2). Our aim was to assess the experience of a typical junior orthopaedic doctor’s experience during his on-call to assess their perspective of the implementation of hospital at nightand to establish whether the recommendations of the evaluation report were being implemented. Methods: A prospective review was conducted of the night duties of all junior doctors working or cross-covering trauma and orthopaedics across Frenchay and Southmead hospital sites of the North Bristol NHS Trust between December 2007 and January 2008.A questionnaire included nature of activity and level of experience, closed questions relating to the hand-over experience. Details of calls received and the nature of tasks undertaken during on-call period with times. Data were then stored and analysed using excel-office 2002. Results:Total of 51 questionnaires were completed by the junior orthopaedic doctors during their respective on-call duties. A total of 109 calls were received or tasks requested. The average time spent during hand-over was 14.1 minutes (range 5-20 minutes). Discussion: Our data indicates busiest times occurred between 21:00 – 23:00 (Fig 1) Figure 1, illustrates a distribution of the peak work-load period which occurred between 9pm-11pm and 1am-3am. This finding contradicts previous surveys done prior to the implementation of the hospital at night where it was noted that the nights were quieter and sub-specialist such as orthopaedic surgeons were not working as hard as general medics (1). Figure 2, shows the overall experience of the hand-over as judged by the orthopaedic juniors. There was an eighty-five percent (43/51) attendance by the on-call orthopaedic juniors of which seventy-two percent (32/44) thought that it was a useful experience Figure 3 illustrates a distribution of the calls received. As illustrated, 37/109 calls were viewed as inappropriate The majority of the orthopaedic juniors surveyed framed hospital-at-night hand-over was useful but thirty-four percent (37/109) of the calls they received were viewed as inappropriate (Fig 2,3). The most frequent of the inappropriate ward calls were ‘requests to rewrite drug-charts’ (Fig 4,5). Figure 4 describes the frequencies of these calls. As illustrated the most frequently inappropriate ward-call was to ‘rewrite drug-charts’. There were twenty-three (23/37) inappropriate ward-calls Figure 5 shows the reasons given by the on-call doctors for the inappropriate tasks. The most frequently given reason was that ‘the request should have been done during the day’. The second most frequently given reason for inappropriate calls was the fact that ‘it was a duplicated request’ Our survey also highlighted that the most frequently given reason for inappropriate tasks was firstly that the request should have been done during the day and secondly that it was a duplicated request. These findings seem to defeat the key purpose of the hospital-at-night project for an orthopaedic SHO on-call. Conclusion: Hospital at night cannot function in isolation. There are fewer doctors available then normally and the system has to use their time effectively. 30% of inappropriate calls to wards were to rewrite drug charts and to prescribe warfarin. This should have been identified and performed by the day staff. 10% of calls were to review X-rays. Much of the inappropriate activity could be pre-empted if both day and night staff attended the handover and the tasks outstanding from the day identified. The doctor on the night could then perform an hourly ward round completing these tasks without interrupting at the beginning of the night.
Introduction Dysmenorrhoea and other premenstrual symptoms are common among women of reproductive age and lead to suffering and impact on home, school, and work performance. Earlier studies have focused on the prevalence and risk factors of dysmenorrhoea 1, 2, 3. Surveys in Pakistan have found the prevalence of premenstrual symptoms varying from 53% to 67% in college girls 4, 5, 6. About 57% of students in one study reported that dysmenorrhoea affected their work5. Although these surveys document the prevalence and severity of symptoms they do not correlate it with the impact of specific symptoms on daily activities or with healthcare seeking behaviour. A population-based survey of 2262 women from Goa, India, revealed a linear association between pain severity and treatment seeking and time off from work 3. However the impact of specific symptoms of premenstrual syndrome on treatment seeking and rest was not reported. Aims Primary objective: The authors carried out a cross-sectional study to explore the impact of dysmenorrhoea and other premenstrual symptoms among women of reproductive age.Secondary objective: The authors intended to find out the predictors of healthcare-seeking behaviour including self-treatment for premenstrual symptoms. Methodology A cross-sectional survey study design was chosen. A 13-item questionnaire was administered to women, aged 16 to 50, who were not pregnant and had no known gynaecological, medical, musculoskeletal or neurological diagnosis. Participants were recruited from multiple sites using convenience sampling within urban areas of Islamabad and Rawalpindi in Pakistan. Trained interviewers (physicians, medical students, nursing staff, and high school students) filled out questionnaires interviewing female students at a medical college, a nursing college, and at city schools; as well as housekeeping staff and patients’ attendants at a tertiary care teaching hospital in Islamabad. A proportion of women completed the questionnaire themselves. Ethical approval was obtained from the Shifa International Hospital Ethics committee. No personally identifiable data such as the respondents’ names were recorded. ResultsStudy population characteristics A total of 1236 women from multiple locations within Islamabad and Rawalpindi, Pakistan, participated in the survey. Most of the women were in the younger age groups: 402 women (33%) were 16–20 years old and 622 (50%) were 21–35 years old. Fewer women were in the older age groups: 147 women (12%) were 36–45 years old and 63 (5%) were more than 45 years old. About 55% were unmarried and 61% had no children. The distribution of educational achievement was weighted towards the more educated: 16% were able to read a religious book (basic literacy); 49% had some school education (up to 12th grade); and 34% had professional level education. About 27% of the respondents were homemakers (among women with professional level education, 10% reported staying at home). Age at menarche was less than 12 years old for 16%; between 12 and 14 years for 62%; and more than 14 years old for 23% of the respondents. Severity of dysmenorrhoea and its correlation with premenstrual symptoms On the 10-point visual pain scale, 465 women (38%, 95% CI 35–41) reported mild dysmenorrhoea severity from 0 to 3; 517 women (42%, 95% CI 39–45) reported moderate severity from 4 to 7; and 248 women (20%, 95% CI 18–23) reported severe pain rated from 8 to 10. The linear regression coefficient between dysmenorrhoea severity score and the number of days unable to work in a month was 0.59 (standard error: 0.031). Table 1: Prevalence of premenstrual symptoms and their contribution to pain severity and days lost from work
Women reporting symptoms, n (%, 95% CI) a
Contribution to pain score b
Contribution to days out of work c
Low back pain
879 (72, 69–74)
0.39 *
0.05
Depressed mood
484 (40, 37–43)
0.17 *
-0.05
Headache
268 (22, 20–24)
0.25 *
0.22 *
Swelling
218 (18, 16–20)
0.03
0.12
Nausea
218 (18, 16–20)
0.17 *
0.01
* Statistically significant values (P < 0.005)a Respondents were allowed to select more than one option. Total respondents: 1236.b Linear regression coefficients for a 10-point visual pain score categorized into three levels.c Linear regression coefficients for self-reported days unable to work in a month. Table 1 shows the prevalence of primary symptoms of preceding menstruation and their contribution to a 10-point visual pain scale and to self-reported days unable to work in a month. Low back pain and headache contributed most to the pain score while headache and swelling correlated with days out of work. Impact of dysmenorrhoea Among the working women (366 professionals and housekeeping staff) 49% (95% CI 44–54) reported one or more days out of work in a month due to pain. Similarly, among the 452 students surveyed, 53% (95% CI 48–58) reported dysmenorrhoea affecting school performance (Table 2).
Table 2: Impact of premenstrual symptoms and dysmenorrhoea on household, school and work performance
All respondents, n (%)
Students, n (%)
Maids and housekeeping staff, n (%)
Self-employed, n (%)
Professionals, n (%)
Affected domain
Household chores
441 (37)
124 (28)
59 (40)
31 (52)
75 (35)
Household income
129 (11)
24 (5.3)
33 (22)
12 (20)
18 (8.5)
Performance in school
313 (25)
239 (53)
N/A
N/A
N/A
Social obligations
395 (33)
130 (29)
58 (39)
31 (52)
85 (40)
Unable to work for one or more days in a month
643 (53)
282 (63)
75 (51)
38 (63)
103 (50)
Percentages do not add up to 100% as respondents were allowed to select more than one affected domain.Values for 50% or more respondents acknowledging an impact in a domain are given in bold.
Treatment taken for dysmenorrhoea relief
Table 3 outlines the remedies sought for the relief of dysmenorrhoea symptoms and the reported effectiveness of each type of remedy. All treatments except homeopathic were felt to be effective. Logistic regression analysis showed that the use of any treatment type was related to low back pain (odds ratio 2.2, 95% confidence interval 1.6–2.9), pain severity (OR 2.0, 95% CI 1.6–2.5), headache (OR 1.7, 95% CI 1.2–2.4), depressed mood (OR 1.7, 95% CI 1.3–2.2), increasing education (OR 1.1, 95% CI 1.0–1.2) and not being unmarried (OR 0.52, 95% CI 0.34–0.79).
Table 3: Remedies sought for dysmenorrhoea relief and their patient-reported effectiveness
Women reporting use of treatment, n (%, 95% CI)a
Odds ratio for self-reported effectiveness, (95% CI)b
Conventional medicine
496 (56, 53–59)
13 (8.7 to 21)
Household remedies
285 (32, 29–35)
6.5 (4.1 to 11)
Herbal
90 (10, 8–12)
4.1 (2.2 to 7.7)
Homeopathic
125 (14, 12–17)
1.5 (0.89 to 2.6)
a Respondents were allowed to select more than one option. Total respondents: 1236. b Unconditional logistic regression (converged, 6 iterations, 878 cases included, using Epi Info 3.4.3). All odds ratios with P < 0.005, except homeopathic, P = 0.12.[CI, confidence interval]
Conventional medicine was sought by women with higher pain scores (OR 2.2, 95% CI 1.8–2.8) and greater years of education (OR 1.2, 95% CI 1.1–1.3); other factors such as age and specific symptoms were not statistically related. Women with a greater number of days unable to work were more likely to use herbal treatment (OR 1.4, 95% CI 1.1–1.9) while household remedies like hot water bottles and warm drinks were more commonly taken by women with headache (OR 1.66, 95% CI 1.2–2.4), depressed mood (OR 1.6, 95% CI 1.2–2.3) and lesser years of education (OR 0.88, 95% CI 0.78–0.99). Discussion This paper is the first, to the best of our knowledge, to show an association between specific premenstrual symptoms and dysmenorrhoea severity and healthcare-seeking behaviour. We found that certain symptoms, namely low back pain and headache, contributed more to the perceived severity than other complaints. This finding may be of importance to clinicians treating women with menstrual complaints especially when the treatment is symptom-oriented. In women working outside their homes clinicians may wish to target headache and swelling as these symptoms correlated with days unable to work. Prevalence of premenstrual symptoms in the present study was higher than a Japanese survey7 that reported back pain in 6.9% of women and headache in 11% of women (compared with our results of 72% and 22% respectively). This difference may be due to cultural differences in perception and reporting of symptoms, overall better health, and being strong and hardworking. It may simply be the perception difference in underdeveloped or developed country i.e. lack of resources, poor diet, and poor health. Menstrual symptoms caused a heavy impact on social, school, and work responsibilities in women, a finding we share with previous studies. A cross-sectional survey from India found that 17% of adolescent girls reported missing school classes due to dysmenorrhoea while 60% reported disruption of their daily activities8. In an Australian study, 53% of high school girls reported that dysmenorrhoea limited daily routines and 37% stated that it affected schoolwork9. A study from New York found 46% of students missing one or more days of school due to dysmenorrhoea10. Corresponding figures from the present study were: 62% students reported missing at least one day of school and 53% reported an impact on school performance. The authors would like to reiterate the need for screening for and treating menstrual symptoms because of the impact on daily activities and the potential to reduce avoidable suffering. Women seek a variety of sources for relief of menstrual symptoms. A survey of 2411 high school girls in Malaysia showed that 11% sought medical care although the majority (80%) obtained advice from their mothers regarding premenstrual symptoms11. A study of adolescent girls in Haryana, India, found that 5.3% consulted a physician for menstrual symptoms and 22% self-treated with over-the-counter medicines12. 52% reported self-treatment and 7.7% used complementary medicines in a Japanese study13. In the present study, although conventional medicine was felt to be most effective, it was used by only half of the women. This indicates poor access or awareness of available effective treatments. Even household and herbal remedies were infrequently used possibly due to their limited effectiveness. As menstruation and its associated symptoms are often thought to be a ‘normal’ part of women’s lives these issues may remain untreated in the community. Women who were more educated tended to seek more effective treatments, as did those who had more severe symptoms. Clinicians and public health professionals need to proactively reach women from less privileged background to reduce suffering from menstrual symptoms. Educational campaigns to improve awareness of safe and effective conventional medicine, such as non-steroidal anti-inflammatory drugs, could reach women not aware of these options. These public health campaigns may be addressed toward high-school girls, homemakers, and professionally employed women through separate targeted channels. The present study was limited by non-random (convenience) sampling yielding a study sample skewed towards more educated women. This may be due to sampling in urban areas only. The questionnaire was designed using closed-ended questions, to reduce subjectivity in data recording, limiting exploration of unanticipated variables. Psychosocial issues, such as socio-economic disadvantage and mental health, play an important role in the perception and reporting of menstrual symptoms3 but these factors were not explored in this study. Further research in this area should focus on awareness, access to care, and quality of life outcomes with different treatment options. ConclusionLow back pain and headache contribute the most to severity of dysmenorrhoea while headache and body swelling (fluid retention) were predictive of days unable to work. Conventional medicine is commonly used by more educated women, as well as those with more severe symptoms, and was perceived to be effective more often than other treatment modalities. Effective treatments for the relief of menstrual symptoms remain underutilized causing avoidable suffering.
IntroductionHospital inpatient falls have remained the subject of extensive research and intervention over the past 55 years1. Despite risk factor identification, multiple prediction system developments and harm reducing technologies, the issue of falls remains. The incidence of falls varies between 2.2 and 14 per 1000 patient days 2,3 and increases with age 4. In the UK’s National Health Service, 32% of adverse incident reports are due to falls 2 . In 2007 it reported 200,000 inpatient falls to the National Patient Safety Association 5. Whilst most patients (96%) came to no harm or minor harm, they estimated that over 500 hip fractures and 26 deaths resulted from these falls.Inpatient falls lead to greater morbidity and mortality than equivalent fractures in the community, 6 and they significantly increase the length of stay in hospital7. Apart from physical harm, there are also psychological consequences for patients such as anxiety, loss of confidence, and fear of falling 4. The risk of falls leads to a conundrum in rehabilitative care. Ideally, patients’ mobility, autonomy and dignity must be encouraged and respected - yet slips, trips and falls must be pre-empted often with varying degrees of intrusion and even restraint. In order to selectively target individual patients who would benefit from closer attention, many risk stratification tools have been developed to predict potential fallers. They were developed on a background of over 400 independent risk factors identified with falls 8. The most prominent in the UK are STRATIFY (St Thomas's risk assessment tool in falling elderlyinpatients) and Downton with the recent addition of the Wandering Behaviour Assessment 8. STRATIFY 4 was designed to be used once per week and assesses 5 factors –falls history, patient agitation, visual impairment that limits daily function, frequent toileting, and a transfer or mobility score of 3 or 4 . Each factor scores 1 point and a score greater than 2 was found to have a 92% sensitivity and 68% specificity for a fall in the following week. In the Wandering Behaviour study the STRATIFY criteria results were not reproduced and were found to have only an 82% sensitivity and 34% specificity in their study population 8. Downton 9 also has 5 categories of assessment; falls history, medication subtypes, audio-visual-sensory deficits, mental state (using the Mini Mental State Score <24) and stability of gait. Each category scores 1 point and a score of greater than 3 is considered significant. In the Wandering Behaviour study, when applying the Downton criteria they only found an 82% sensitivity and 36% specificity 8. The Wandering Behaviour assessment looks for the presence of the following :checking, pottering, aimless walking, walking with inappropriate purpose, walking with appropriate purpose but inappropriate frequency, excessive activity, night-time walking, attempts to leave the hospital and being brought back to hospital. The presence of any one of these was found to have a sensitivity of 43% but specificity of 91% 8. Thus, both STRATIFY and Downton are limited by the multi-disciplinary assessments required, so that even when implemented, it is difficult to repeat them on a daily or weekly basis. The Wandering Score is easily repeatable on a daily basis, but lacks the sensitivity of STRATIFY and Downton 8. The aim of this study is to investigate whether changes in a patient’s physiology can be predictive of falls risk, and if so, can they become a useful tool for calculating risk? The reason why we have chosen to investigate this is that many of the commonly encountered risk factors can potentially be reflected in the patient’s routine observations 10. For example, fever could indicate infection and delirium. Hypotension could result from anti-hypertensives, sedatives, or dehydration. Hypertensive states could result from stroke, stress response to infection, or even be a surrogate marker of cardiovascular disease predisposing to arrhythmias. Blood pressure variation could also be predictive since dynamic orthostatic challenges such as lying and standing blood pressure measurements are known to predict falls 10. Thus, by measuring fluctuations in the observations we hypothesised that it may be possible to make an accurate short term prediction of falls riskMethodsSubjectsWe obtained consent for this retrospective study from the hospital’s ethics committee. We based this study in the Acute Medical Unit of our hospital, as it has the largest case mix of patients recently admitted and is therefore most likely to have the largest physiological instability. We aimed to detect a mean difference of 10% in the physiological variability prior to falling with 80% power, p-value < 0.05, and a common standard deviation of 5 %. Our power calculation indicated that we needed to study 12 patients. We identified all the falls in the calendar year of 2008 by examining the records of all the incident report forms submitted by the ward. A total of 33 incident reports related to falls were logged. Two reports related to staff slips and trips and were excluded, and a third incident report failed to adequately identify either the patient’s name, date of birth or hospital number and so had to be excluded. One of the 30 patients fell twice, and this was treated as its own incident as with the STRATIFY paper. The incident report forms were also used to identify the time, nature, and outcome of the fall. Of all the case notes related to the 30 falls requested from medical records, only 13 were available for detailed review. MeasurementsHeart rate (HR), Blood Pressure (BP), Temperature and Respiratory Rates were all recorded and analysed. The PAR (Patient at Risk) Score as calculated by the nursing staff was included too. PAR Scores are validated mechanisms of identifying sick patients who may go on to develop deterioration to the point of requiring Intensive Care. Scores of >3 are associated with a high risk of deteriorating health and are calculated using the routine nursing observations set. Oxygen saturations were not included in this study, as even small deviations tend to be rapidly corrected by staff with oxygen and therefore were not thought to be a useful marker. Recordings of blood pressure and heart rate were all done with ward based equipment. It is impossible to know which machines were used on individual patients as the equipment has varied, both over the course of time, and between multiple wards. However, because the subjects were their own controls, we are confident that the same machine and cuff were used for taking all the 12 hour recordings as each individual machine is allocated to a given bay. Blood pressures were obtained using semi-automatic Dynamap equipment, therefore the readings are in effect calculated from the Mean Arterial Pressure (MAP). We elected to study the systolic readings only, as this represents the maximum perfusion pressure to the brain and carotid sinus. Two of the thirteen patients were known to have undergone orthostatic challenges as part of their admission work up and these were included. Other parameters recorded included the time of the fall, number of medications on the drug chart, whether the fall was observed and any injuries sustained. ControlsWe had two sets of controls. The first set was used to compare the age and gender profile of the fallers to those of the general adult admissions. We had to do this because the official hospital statistics included obstetric and paediatric admissions and comparison would have been inaccurate. We therefore took 4 random days’ of acute adult medical admissions (i.e. over the age of 18) in order to compile an age and gender profile of patients admitted with a ratio of 4:1 (n=110). In order to compare the variability in physiological parameters between fallers and non fallers we generated a second set of controls matched for age (± 5 years) and gender in a ratio of 4 to 1 from a random week’s cohort of patients in February 2009 (for practical purposes). For each matched control, recordings were made at the equivalent length of stay and the controls were not known to have previously fallen. The patients were taken from across the hospital’s medical wards (not Intensive Care or Surgical) with their diagnosis blinded from the investigators. We were able to match 47 of the 52 controls that we were aiming for. Only BP and HR data were recorded in the controls, as we already established that temperature and respiratory rate were not sensitive markers from our faller data. StatisticsOur 13 patients allowed us to reach sufficient statistical power of 80%. Physiological parameters were tested within groups using the Students t-test (paired, two tailed) and when comparing to controls using the Students t-test (unpaired, two tailed). The null hypothesis were rejected when p<0.05. Variability in heart rate, temperature, respiratory rate and PAR (Patient At Risk Score) were calculated using the mean, range and standard deviation between maximum and minimum values. Blood pressure variability was measured by using the maximum and minimum systolic pressure and calculating the mean, range and standard deviation. We have chosen to primarily measure variability by the range as it is a simple calculation that can be done by anyone on a ward. It doesn’t require a calculator nor any detailed knowledge of mathematics. It is therefore an effective and repeatable measure which could be easily implemented as part of a scoring system. Data processing and Statistical Analyses was done in MS Excel 2002 and SPSS v.14. ResultsThe mean age of fallers was 79 years old (SD 16, n=30) and of the acute medical admission controls 67 years old (SD 20, n=110) with p=0.003. The gender distribution of males to females was 63% to 37% respectively for fallers (n=30), but 38% to 62% in general medical take controls (Fishers exact test p<0.001). 54% of fallers (n=13) were admitted from their own home with 31% from Residential Homes and 15% from Nursing Homes. 54% were known to have a preceding falls history (n=13). The timings of the falls showed that 60% of falls occurred between 08.00 and 20.00 (n=30). 77% of falls occurred within 48 hours of admission (n=13). The circumstances of the falls were consistent with the NPSA statistics with 20% falling out of bed, 17% from chair, 17% from commode / toilet, 20% when walking, 3% in the bath and 23% not documented. The significance of the falls as measured by the incident report forms (n=26, in 4 cases not recorded) was 70% under the level of 6 (i.e. low level and did not require further investigation), 13% were over the level of 6 (i.e. were serious and required further investigation) and 17% were unrecorded. Most of the injuries (n=30) were none or minor – 47%, 10% had a head injury and 43% were not recorded. 95% of the falls were not observed. 31% of the patients (n=13) were taking fewer than 4 medications, 38% were taking between 4 and 7 medications and 32% were taking over 8 medications. Comparing the demographic characteristics of our fallers to the age and gender matched controls; average age was 79 for both fallers and controls (p=0.94) and the gender distribution was 7 females : 6 males in the fallers, and 27 females: 21 males in the controls (Fisher’s Exact Test p=1.0). The overall PAR score (n=13) was not sufficiently sensitive to predict falls risk – 77% had no change in their PAR score, 8% had a 1 point change and 15% had a 2 point change ( Table 1). Temperature variation (n=13) was minimal with 69% having less than 1 degree Celsius change and 31% having change of 1 to 1.5 degrees Celsius . Recorded respiratory rate variation was also minor (n=13) with 85% having a maximum change of up to 4 breaths per minute. Table 1. Physiological Parameter Data * denotes p<0.05
Fallers N = 13Mean ± SDRange (x-x)
Controls N = 47Mean ± SDRange (x-x)
PAR Score
1.2 ± 0.6(1 – 3)
PAR Score Variability
0.4 ± 0.6(0 – 2)
Temperature (Celsius)
37.1 ± 0.5(36.4 - 38.1)
Temperature Variability (Celsius)
0.6 ± 0.5(0 – 1.3)
Respiratory Rate (Breaths/Minute)
18.5 ± 1.9(16 – 22)
Respiratory Rate Variability (Breaths/Minute)
1.1 ± 1.5(0 – 4)
Highest Heart Rate (Beats/Minute)
86 ± 13(70 - 110)
86 ± 14(60 -112)
Lowest Heart Rate(Beats/Minute)
71 ± 16(50 -101)
79 ± 14(55 – 110)
*Heart Rate Variability (Beats/Minute)
15 ± 10(0 – 39)
7 ± 7(0 – 27)
Highest Systolic BP (mmHg)
142 ± 22(102 – 180)
140 ± 24(99 – 218)
Lowest Systolic BP(mmHg)
116 ± 19(71 – 150)
129 ± 24(86 – 199)
*Systolic Variability (mmHg)
26 ± 12(2 – 40)
11 ± 7(0 – 26)
In fallers (n=13), the mean highest heart rate was 86 bpm (SD=13) and the mean lowest heart rate was 71 bpm (SD=16). The range was 15 bpm (SD=9.6) with p<0.001. In controls (n=47) the mean highest heart rate was 86 bpm (SD=14) and the mean lowest heart rate was 79 bpm (SD=14). The range was 7 bpm (SD=7) with p<0.001. The significance test when comparing the highest average heart rate between fallers and controls shows p=0.98 showing that they were well matched. The significance test for comparing the variation of the heart rate between fallers and controls is p<0.001. In fallers (n=13), the mean highest systolic BP was 142 mmHg (SD=22) and the mean lowest systolic BP was 116 mmHg (SD=19). The average variation was 26 mmHg (SD=12) with p<0.001. In controls (n=47) the mean highest systolic BP was 140 mmHg (SD=24) and the mean lowest systolic BP was129 mmHg (SD=24). The average variation was 11 mmHg (SD=6.5) with p<0.001. The significance test when comparing the highest average systolic BP between fallers and controls shows p=0.77 showing that they were well matched. The significance test for comparing the variation of the systolic BP between fallers and controls is p<0.001. Charts 1 and 2 show the spread of measurements in the cardiovascular parameters between fallers and controls.
Chart 1. Comparison of the heart rate variation between Fallers and Controls
Chart 2. Comparison of the systolic blood pressure variation between Fallers and Controls
DiscussionThe average age of the fallers was significantly greater than the average age of those admitted to the hospital in general. This is unsurprising considering both mechanical deterioration of the musculoskeletal system with advancing age and the accumulation of disease processes. It is noteworthy that despite making up the smaller percentage of admissions to the hospital, men made up the greater proportion of fallers. Other much larger studies show considerable variability in their gender proportions 11,12, therefore this finding is unlikely to be truly significant. Apart from age and gender, polypharmacy was also a feature of our fallers. This is consistent with other studies 13,14,15. Additionally, our data was consistent with the overall NPSA statistics in terms of the significance and circumstances of the falls 5. The main and novel finding of our study was that fallers were significantly more likely to display a larger range in their cardiovascular observations than the standard hospital population. Whilst it is generally expected that subjects undergoing any routine measurement of heart rate and blood pressure will have a variation in measurements of about 10% over the course of 12 hours 16,17, we found that our fallers had a variation in their heart rate and blood pressure of approximately 20%. This is similar to the dips experienced by the normal population over the course of the night and during orthostatic challenge. This was despite the fact that the baseline measurements of highest value were virtually the same for both populations. Furthermore, almost all the values recorded were within normal limits – and would not normally require specific remedial action to be taken. This could also explain why this risk factor has not previously been identified in other studies. Our study indicates that it is the cardiovascular lability rather than the cardiovascular measurements per se, which acts as an acute predictor of falls. In fact, the sensitivity for falls prediction with either a range of HR values > 15 beats per minute or range of BP systolic values >25 mmHg was 77%. We would therefore expect that when such patients mobilize, the superadded orthostatic challenge would be too great for cardiac output to be suitably matched and so patients are at greater risk of falling. In terms of the 12 hour prospective risk of falling this could certainly explain why a patient with known risk factors will fall during a given nursing shift. Indeed it may also explain why a patient may fall during a hospital admission when patients were, for example, already parkinsonian and arthritic and yet had not previously fallen. Interestingly, neither temperature, respiratory rate, nor PAR Score showed any significant lability in the lead up to the falls. This was surprising as we would have expected them to be predictive of other well known risk factors. The lack of fluctuation in temperature and respiratory rate could provide further evidence that the key short term factor responsible for falls is cardiovascular lability. More detailed analysis showed that it was more likely that these measurements were insufficiently sensitive. Only four of the fallers were admitted with infections, and those subjects showed some temperature fluctuations. However, only 2 had temperatures above 37.5 degrees Celsius, which is consistent with the blunted fever response that is well known to occur in 50% of the elderly population 19,20 (and most fallers were elderly). The lack of value in respiratory rate recordings probably reflects the lack of due care and attention paid to this, the only manually measured parameter. It has long been recognized that respiratory rate recordings tend to be inaccurate 21 . The highly limited range of measurements recorded (16-22 breaths per minute) amongst all the fallers, despite some patients having severe pneumonia, further supports this finding. Finally, the PAR score tended to be quite static. This was a result of its constituent parameters not being sensitive (temperature, respiratory rate) and the fact that most of the heart rate and blood pressure recordings were within normal limits. LimitationsDespite the fact that this study was well powered and statistically significant, ultimately it is quite limited in numbers with just 13 patients. It was disappointing that we were not able to obtain case-notes or the appropriate file in the other 17. We are also presenting calculated data from the MAP measurements, without knowing the exact algorithms being used. For this reason, we analysed the given systolic pressures as further data manipulation would have increased inaccuracies. Our data is taken from relatively acute admissions and as such may not necessarily be applicable to long stay patients, where cardiovascular lability may not play an important role.Furthermore, controls were not matched for diagnosis or for the number of medications taken. This could lead to criticism that the comparison was poor, though the baseline measurements for the two were remarkably consistent. One of our aims was to see if variability could be used to accurately model general falls risk. We therefore thought it would be more useful to study the hospital’s general physiology, in all its varying degrees of illness. ConclusionsThis study shows the value of looking closely at patients’ observations and that even ‘normal’ values have to be interpreted in context . The data supports the finding that the risk of falling at a given point in time relates not only to predisposing factors, but also to their current cardiovascular status. We therefore suggest that a one-off falls risk assessment is no longer appropriate, but should be continuously reviewed on a shift-by-shift basis by nursing staff. This has significant ramifications for modernizing current risk stratification tools so that they are able take this into account.
Barrett’s Oesophagus (BO) describes a histological abnormality of the lower oesophagus widely accepted to be associated with gastro-oesophageal reflux disease (GORD). The nature of this disease has been a subject of debate since its description by Tileston in 1906 as peptic ulceration of the oesophagus. Barrett himself initially theorised that the abnormal oesophagus was in fact stomach that had been pulled into the chest by a congenitally short oesophagus (1). This idea was ultimately challenged as the area in question lacked a peritoneal covering, contained submucosal glands and muscularis propria characteristic of the oesophagus (2). In 1976, Paull et al described a distinctive type of intestinal metaplasia the investigators called "specialised columnar epithelium”. Specialised intestinal metaplasia is now widely accepted to be the hallmark of BO with its presence predisposing to dysplasia and cancer regardless of its location within the oesophagus (3).
Barrett’s Oesophagus, its identification and treatment continues to be an area of debate and interest. Although not sinister in itself, it is a known precursor to malignant disease and strongly associated with GORD. Barrett’s oesophagus is the most frequent predisposing risk factor for the progression to adenocarcinoma in the oesophagus. Sufferers have a 40 fold increased risk when compared to the general population (4).
The progression of GORD to BO appears to be related to exposure of oesophageal tissue to the acidic contents of the stomach. It is therefore seen in hiatus hernia, lower oesophageal dysfunction, delayed oesophageal acid clearance and duodenogastric reflux. Furthermore, it is the duration and not frequency of exposure to acidity that dictates erosive damage to the oesophagus. Levels of acidity also contribute. The damage to cells incurred leads to inflammatory infiltration and cell necrosis with replacement of oesophageal epithelium by metaplastic columnar cells.
Assessing severity of BO relies partly on endoscopic visualisation techniques and length of oesophagus involved. Long segment Barrett’s oesophagus (LSBO) indicated a >3cm segment of involvement with short segment disease involving <3cm. LSBO carries a higher risk of progression to adenocarcinoma. Its development is associated with long term symptoms, severe combined patterns of reflux (both erect and supine) on 24 hour pH monitoring and reduced lower oesophageal sphincter pressures. Patients are less sensitive to direct acid exposure than those with short segment disease. The latter group also tend to have shorter duration of symptoms, normal sphincter pressures and only upright reflux on 24 hour pH monitoring (3).
The Prague C and M criteria is a recently developed classification system utilising the circumferential and maximal extent of oesophageal columnar tissue to assess disease severity endoscopically (5). Its accuracy is yet to be assessed clinically, however, it is believed to largely improve the overall assessment of Barrett’s (6). The further classification of disease severity is based on the degree of dysplasia, with high grade dysplasia carrying a higher risk of progression to malignancy.
Barrett’s oesophagus is predominantly seen in the age group 55-65, with males being affected twice as frequently as females. The disease is more prevalent in the white population. Obesity, smoking and alcohol intake being further risk factors. H.pylori may be protective against Barrett’s oesophagus with two mechanisms postulated. Namely, the induction of atrophic gastritis, which results in decreased acid production and the production of neutralising ammonia independent of gastric atrophy (7). The duration of symptoms of GORD but not necessarily symptom severity is also associated with increased risk of progression to BO. The exact pathogenesis is not clearly understood and is believed to be a culmination of both hereditary and environmental factors. For example, some studies report a greater incidence of BO amongst first degree relatives in comparison to their unrelated counterparts (8). Other reports associate environmental factors such as a high body mass index, with an increasing risk of GORD and progression to BO (9). Underlying mechanisms include the proposition that central obesity predisposes to hiatus hernia formation (10) and subsequent gastric acid reflux. However further research is required to unlock the key processes that lead to the formation of BO; as these pathways may hold novel therapeutic targets.
Prevalence of BO is difficult to ascertain due to the lack of population based studies. Studies from the United States involving patients aged over 40 years undergoing gastroscopy reported a prevalence of 6.8% in all patients (11). A Swedish study involving 1000 volunteers is the only available true population based study and found a prevalence of 1.6% (12).
Endoscopic surveillance
The most appropriate method for both diagnosis and surveillance of Barrett’s Oesophagus is endoscopy. Its sensitivity is higher than other comparative techniques, such as barium based studies or CT/MRI. Endoscopic screening programmes can be beneficial in both highlighting patients with BO from those with chronic GORD, as well as monitoring patients with established disease who are at risk of progressing to adenocarcinoma of the oesophagus. The American College of Gastroenterologists identify older patients with chronic GORD symptoms as the most likely to benefit from endoscopic surveillance techniques. Studies have also shown that five year survival rates are generally greater for patients who have had their adenocarcinoma identified by surveillance in comparison to those who have not (13). Importance also lies in the method of surveillance, for example shorter endoscopic interval analysis for surveillance in low grade dysplasia, are associated with higher rates of detection of adeonacarcinoma (14).
Although screening for Barrett’s oesophagus relies largely on established endoscopic techniques, it remains an area of contention for several reasons. These include low prevalence and the invasiveness of endoscopy, as well as a lack of an easily identifiable demographic group. Alternative methods include the use of capsule endoscopy which offers increased acceptability of screening, is less invasive and carries an increased uptake rate in comparison (15). However a study involving 96 patients demonstrated only 67% sensitivity and 84% specificity for identifying the condition using this technique (16). A recent meta-analysis of nine studies comprising 618 patients offers the most up to date evaluation of this technique. The pooled sensitivity and specificity for diagnosing BO using this method was found to be 77% and 86% respectively. Studies using OGD as reference demonstrated sensitivity 78% and specificity 90%. With intestinal metaplasia as the reference standard, sensitivity 78% and specificity 73% was discovered although the latter figure was particularly affected by one study with very low values for this (17). Capsule endoscopy offers benefits in patient tolerance and morbidity as well as cost as the capsule can be swallowed in an office, potentially under nursing supervision. Despite this latter point, cost-benefit analysis of this technique have proved equivocal. There are also several drawbacks. Views achieved are no longer under operator control and anatomical landmarks are more difficult and potentially impossible to identify. Oesophageal transition time has been demonstrated to be as short as 1 second and biopsy is not possible regardless of this. This greatly limits the use of capsule endoscopy in BO surveillance which relies on biopsy. Ultimately, the use of capsule endoscopy in diagnosis or screening of BO is unsupported at this current time and is an area for future research.
Other methods include small calibre trans-nasal endoscopy, which involves inserting a small-calibre endoscope through the nose and oesophageal sphincter to visualise the oespophagus, stomach and duodenum. It has the advantage of not requiring any sedation only topical anesthesia, having a lower complication rate, requiring less nursing staff and being more cost effective in comparison to its more frequently performed counterpart. Capsule endoscopy, as described earlier, also has the advantage of lacking sedation, being less invasive and yielding lower complication rates. Other alternatives include narrow band imaging, which involves scanning large areas of mucosa for possible neoplasia and autoflourescence imaging in which dysplastic lesions are visualised by differences in colour. The usefulness of visualisation techniques including high-resolution magnification endoscopy and tissue staining with agents such as methylene blue or indigo carmine are still an area of debate. These techniques have been evaluated when used in combination and alone. Pit patterns identified using acetic acid chemoendoscopy were described in 2001 by Guelrud et al (18) and Sharma et al described differing mucosal patterns in BO (19). Numerous other agents and classification systems have been described. Currently the use of these techniques for diagnostic purposes has not been shown to offer superior results than the current gold standard of four quadrant biopsies. Comparison of biopsies taken with methylene blue directed biopsy versus conventional biopsy showed no significant benefit (20). The ability to identify areas of BO (particularly high-grade dysplasia) are not in question. However, low grade dysplasia may be missed and operator experience and skill must be greatly superior to utilise the benefits of these techniques. Staining techniques offer the additional complications and additional expense of carrying out the procedure. Methylene blue has been shown to induce cellular DNA damage in vitro via the generation of singlet oxygen when photoexcited by light (21) thereby potentially being carcinogenic in itself. Evidence to support non-biopsy detection of BO is currently not sufficient to replace the current gold standard but is another area of current and future research.
The low prevalence of BO in the general population makes screening, with upper GI endoscopy, less viable on both a financial and logistic level. The general consensus is those individuals who suffer from chronic GORD are most susceptible to BO and would therefore benefit the most from upper GI endoscopy (22). However the factors involved in the progression of BO to dysplasia and subsequent adenocarcinoma remain unclear, and hence the value of endoscopic surveillance remains a point of discussion.
Treatment options
The treatment options for BO must also be taken into consideration when addressing surveillance and burden of the disease. The treatment options can broadly be divided into three groups, which include conservative management with surveillance endoscopy, endoscopic therapy and surgical oesophagectomy. The pathways of treatment are governed by patient-specific factors as well as the degree of oesophageal dysplasia. Surveillance endoscopy forms an integral part of the management of BO, and this is largely due to studies which have demonstrated a greater five year survival and an earlier stage of detection of oesophageal carcinomas detected by surveillance endoscopy (13, 23). Current recommendations target individuals at high risk of BO, for example those with chronic GORD symptoms. If no dysplasia is found on biopsies from two endoscopies, surveillance intervals of 3 years are recommended. However, patients with low-grade dysplasia on biopsy should have an immediate repeat endocopy to confirm the diagnosis, and then yearly surveillance endoscopies until no dysplasia is observed. The management of patients with high-grade dysplasia is contentious and varies between centres. Recommendations include a repeat endoscopy to evaluate for cancerous progression, with some centres instituting regular three month surveillance with biopsies every 1-2cm of effected mucosa (6). Other centres, depending on the multi-focal extent of dysplasia recommend surgical intervention with oesophagectomy or endoscopic therapy; which includes mucosal resection, photodynamic therapy, argon plasma coagulation and endoscopic ablative techniques.
Surgery
Oesophagectomy is normally reserved for the management of high grade dysplasia with the potential for malignant transformation. The percentage of high grade dysplasia which progress to adenocarcinoma vary throughout the literature from 5% to 59% up to seven years from initial diagnosis (7). Although oesophagectomy provides potential for complete resolution, it also carries increased number of adverse effects which include strictures, infections and anastomotic leaks. Mortality rates may also exceed 18% in centres which perform smaller amounts of the procedure on average every year (24) in comparison to high volume centres where the mortality rates can be lower than 5% (25); making the procedure very operator-dependent. As a result less invasive therapeutic modalities are preferred in the management of lower grade oesophageal dysplasia.
Endoscopic Therapy
Endoscopic treatment of Barrett’s oesophagus is currently an area of great interest. Endoscopic resection alone, or in combination with other treatments, have been investigated thoroughly in the past; however studies including large populations based and long term standardised protocol are lacking. The interpretation of these results is therefore very difficult.
Endoscopic mucosal resection (EMR) for high grade dysplasia in BO was first reported in 2000 (26). The procedure involved initial identification of macroscopically visible or chemoendoscopically identifiable Barrett’s lesions. If the lesion showed no evidence of penetration into deeper tissue or metastasis, confirmed by ultrasound guidance, it would be open to resection (27). Ideal lesions include those easily identifiable by macroscopic techniques, limited in size and restricted to the mucosa. However, almost all reports realised the risk of incomplete treatment with recurrence of disease. Some authors advocated the use of circumferential endoscopic resection in order to minimise this risk (28). Endoscopic ultrasound has also been used, prior to treatment, to optimise therapy and has a degree of use in staging of oesophageal cancers (29). Post EMR data showed a low rate of complications with high rate of complete eradication of Barrett’s tissue in the short term. Larghi et al (30) investigated the long-term follow-up of patients undergoing EMR and complete Barrett’s eradication (CBE-EMR). This study involved 24 patients over a 3 year period. Histological eradication of Barrett’s oesophagus was achieved in 87.5% of patients. 3 patients suffered strictures which were endoscopically resolved. Other studies have shown similarly successful eradication with similar complications of bleeding and stricture formation (31, 32). Comparison with previous studies also demonstrated the need for long follow-up to identify potential disease recurrence. In order to minimise stricture formation, a maximum cirmcumference of 50% could be resected during each therapy. A median of 2 sessions was required for complete eradication. 13 patients also received argon plasma photocoagulation in order to ablate isolated islands of a few centimetres of BO. These studies highlight the use of mucosal resection either alone or in conjunction with other treatment modalities, such as argon plasma coagulation, in the treatment of BO. Other options are discussed below.
Argon Plasma Coagulation
This procedure involves the use of a high voltage current to ionise a jet of argon gas and treat the effected tissue. It is also used to treat bleeding lesions endoscopically hence the term coagulation. This procedure has been suggested to be of use in the treatment of BO (33, 34) and several studies have evaluated its efficacy (35-37). Conclusions have been mixed with some studies showing high rates of Barrett’s recurrence and others also suggesting poor rates of initial lesion ablation (37). Generally, rates of complete reversal of BO range in the region of 61-70% (38-42). Other studies have shown more successful results with complete ablation in 87-100% of patients (43-46). A later study evaluated these results as well as performing a further long-term follow-up of 66 patients with high-grade dysplasia undergoing APC with anti-reflux treatment. Histologically confirmed Barrett’s oesophagus was found in 12.1% of patients during further endoscopic surveillance. Patients were treated with anti-reflux therapy (both medical and surgical) and one repeat session of APC. No intraepithelial neoplasia or oesophageal adenocarcinoma was detected during the entire follow-up period of 51 months median (range 9-85) (35).
The available evidence in relation to APC still remains slightly difficult to interpret. Even the larger trials do not involve extensive samples of patients. Furthermore there is a variance between studies with regard to patient selection and exclusion criteria, anti-reflux strategies and the procedure itself. Other pitfalls include the difficulty in assessing the precise depth of the lesion and whether the penetration during treatment was successful enough to ablate the entire lesion. There is also no histological confirmation to help correct insufficient ablation and for this reason some studies have reported an increased risk of progression to cancer and metastasis if invasion past the muscularis occurs (47). Low rates of recurrence seem to be related to the use of higher power settings for ablation, up to 90W as demonstrated by Madisch et al (35). This group also demonstrated the potential role for high dose proton pump inhibitor therapy using a total of 120mg daily in three divided doses to suppress acid for the duration of treatment. Surgical anti-reflux procedures were also found to be associated with reduced recurrence rates. As mentioned above, this procedure may in itself provide a form of treatment for BO and further progression.
Although rare, complications of APC can be severe. Oesophageal perforation has been reported with 2 patient deaths as a consequence (40, 42). Mild oesophageal strictures amenable to endoscopic dilatation have been widely reported. Pleural effusions and bleeding ulcers have also been reported. Despite this, APC can be useful as an adjunct and also effective in the treatment of distinct groups of Barrett’s sufferers with amenable lesions.
Photodynamic therapy
Photodynamic therapy (PDT) involves the systemic administration of a photosensitising drug, followed by irradiation with a controlled light source via an endoscope. The light, in the presence of oxygen, activates the photosensitiser causing photochemically induced tissue destruction (48). Although technically this sounds a difficult procedure, in practice it is actually one of the simplest to perform. However, as with surgical oesophagectomy, it is operator dependent with complication rates increasing within the community in comparison to specialist centres.
The component parts of the photosensitisation process have also evolved with time.
Several photosensitisers have undergone trial with varying results. Trials with Hematoporphyrin derivative as the photosensitising agent showed high rates of stenosis as well as prolonged sensitivity of the skin to light (49). More recently, 5-aminolevulinic acid (5-ALA) has shown promise with good therapeutic results and reduced side-effects in the short term (50-51). 5-ALA also has a reduced period of cutaneous photosensitivity of around one week, in comparison to previous photosensitisers such as sodium porfimer, in which patients would need to take precautions for thirty to ninety days (27). Several studies have demonstrated the effectiveness of photodynamic therapy in BO. The first randomised clinical trial looked at 485 patients with BO and high grade dysplasia (HGD) (52). 208 patients were accepted into the to-treat population, and received photodynamic therapy and omeprazole (PDT+OM); whilst 202 patients formed the control group and received omeprazole alone (OM). The study demonstrated a significant difference with 77% of the PDT+OM group, compared with 39% of the OM group, receiving complete ablation of HGD. The progression from HGD to adenocarcinoma was also significantly lower in the PDT+OM group (13% vs 28%). This study highlighted the effectiveness of photodynamic therapy in conjunction with medical antacid therapy, in ablating high grade dysplasia and reducing the incidence of oesophageal adenocarinoma.
Pitfalls of PDT include the suggestion that lesions greater than 2mm in depth cannot be effectively removed (53), although the photosensitising agent used can influence this. For example, some studies have shown sodium porfimer to have an increased treatment depth of 3-4mm in comparison to other agents (54-55). However limited depth of penetration overall can compromise the ability of PDT to effectively treat high-grade dysplasia. Other common complications post PDT include stricture formation with some studies reporting rates as high as 30% overall and 50% in patients undergoing more than one procedure (56). Although high, long term complications related to this are not reported and most cases are relieved with endoscopic dilatation. Similarly other endoscopic techniques, photodynamic therapy may be inadequate at eliminating dysplastic tissue that is not visible on endoscopy. The issue of buried glands is an area of great interest due to the implication that a treated patient with macroscopically normal tissue may have dysplastic or even malignant tissue beneath. This highlights the importance of regular follow-up endoscopies with a thorough biopsy protocol. An additional complication with photodynamic therapy is the lack of histological samples post therapy, which might be used to assess the completeness of resection as in EMR.
Despite its limitations, photodynamic therapy has been proven an effective treatment for BO in numerous trials and case reports. Future directions include steps to improve photosensitiser agents, dosimetry, and light parameters which should help minimise the associated complication rate.
Radiofrequency Ablation
Radiofrequency ablation is one of the newer endoscopic treatment modalities to show promise in preventing the progression of Barrett’s oesophagus and eliminating the lesion completely. The technique utilises a balloon, 3cm long and consisting of a 60 electrode rings spaced narrowly together every 500micrometres in a bipolar fashion (HALO360 system, Barrx Co, Sunnyvale, CA, USA). A sizing balloon is used to ascertain the circumference of the area to be treated before the ablation balloon is introduced. The system then delivers radiofrequency energy to the tissue circumferentially for 300milliseconds. A dose of 12J/cm2 has been shown to be effective in achieving depth penetration accurately above the muscularis mucosae thus limiting the complications involved with damaging deeper tissues (57). The close spacing of electrodes allows uniform penetration of the entire treated circumference and thus this technique can be used circumferentially with reports of stricture formation being minimal (58). This ability to control the depth of ablative penetration means that many other adverse side effects seen with alternative endoscopic techniques are greatly reduced. These include lower rates of chest pain, odynophagia, perforation and pneumothorax in comparison with laser and thermal ablation techniques.
One recent paper reviewed the progress of 142 patients with endoscopically identifiable Barrett’s oesophagus and high-grade dysplasia managed at 16 separate academic and community centres. These patients underwent a total of 229 radiofrequency ablations and were followed up with repeat endoscopy and systematic biopsy for a median length of 12 months. The only adverse event of note was a stricture noticed on endoscopy in an asymptomatic patient. At follow-up, biopsy specimens were negative for high-grade dysplasia in 90% of patients. 80% of patients had no dysplasia on biopsy and 54% of patients were negative for intestinal metaplasia (59). These results are very encouraging, particularly as high-grade dysplasia carries the greatest risk of malignant progression.
Other benefits include minimal post-procedure discomfort with patients able to go home within hours of the procedure. Regarding the issue of buried glands, a study following 102 patients post circumferential ablation showed no evidence of buried glands in 4306 biopsy samples taken over a year follow-up (60). This once again highlights the advantages of RFA in comparison to other endoscopic techniques.
Conclusion
The surveillance and treatment of Barrett’s Oesphagus remains an area of interest and controversy. This is heightened by the inability to discriminate those patients with BO which are most likely to progress to high grade dysplasia and then to adenocarcinoma of the oesophagus. This places greater emphasis on the endoscopic surveillance programme to identify this potentially pre-malignant state at an early stage. Future advances, particularly in endoscopic techniques, will help to increase efficacy of treatment and minimise complication rates. Further developments include progress in identification of genetic biomarkers which may help elucidate those patients at greatest risk. The management of Barrrett’s Oesophagus is becoming increasingly more important, particularly with the rise in incidence of oesophageal carcinomas in the Western world. The issues to address therefore include the identification and screening of at-risk groups and the further management from diagnosis of BO. Patients with chronic GORD symptoms are most in need of screening. Currently this should include the gold-standard four quadrant biopsy technique. This may include techniques to enhance visualisation as described above. In the authors opinion, non-biopsy screening does not carry enough evidence to support its use in replacement of biopsy as of yet. Medical treatment with PPI (if necessary in high-dose) as well as surgical treatment of GORD are essential considerations in the prevention and treatment of BO. Their use in combination with endoscopic therapy has proven benefits as outlined. Of the endoscopic therapies, the lack of complications combined with excellent post-procedure rates of disease elimination seen with RFA are most encouraging. Oesophagectomy should be reserved for those patients with disease not amenable to conservative or endoscopic therapy. Continual research is required to help us gain more understanding into the pathogenesis of this condition, enabling us to effectively target and manage BO appropriately.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the heart, lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In the previous two editions of pictorial essay, we have discussed the normal and abnormal positions of tracheal tube, nasogastric tube and central venous catheters on chest radiographs. In this edition, we shall look into permanent pacemakers and oesophageal Doppler probe on chest radiographs. PERMANENT PACEMAKERS A permanent pacemaker (artificial pacemaker) is a small battery powered medical device that is placed subcutaneously in the chest or abdomen to help control abnormal heart rhythms. They are inserted for different types of conduction problems (eg: sinus node disease, atrio-ventricular block, tachyarrhythmia etc). Permanent cardiac pacemakers consist of two parts:1. Pulse generator (power unit) – usually felt like a “bar of soap” beneath the skin and2. Pacing electrode leads The pulse generator consists of an energy source (battery) and all electrical circuits necessary for pacing and sensory function. The electrode is the exposed metal tip in contact with the myocardium. The electrode is connected to the pulse generator via an insulated wire (lead). Details regarding classification and functioning of a pacemaker is beyond the scope of this article and can be found in any standard cardiology text book. We shall now discuss what to look for in a chest radiograph in a patient with permanent cardiac pacemaker. Chest radiograph is one of the important diagnostic tools used in the evaluation of a patient with a pacemaker. However, it is not complete by itself and in addition to reviewing chest radiographs, it is important to take a detailed history from the patient, do a thorough examination of the patient, review all necessary case notes and analyse the ECG. If required, a cardiology opinion should be sought. Important points to note on a chest radiograph are: Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3. Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835). Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values. Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
First of all, check whether you are looking at the correct chest radiograph (not another patient’s chest radiograph)Identify the pulse generatorIdentify whether it is a single chamber, dual chamber or biventricular pacemaker. This can be done by counting the number and tracing the pacing leads to the cardiac chamber it is implantedCheck that the pacing leads are not dislodgedCheck that the pacemaker leads are intact and not brokenFinally, look for any abnormal shadowing behind the pacemaker as these can be easily missed1
CONCLUSION Valuable information can thus be obtained on reviewing chest radiographs. Our aim is to provide a quick overview on what to look for in pacemakers and oesophageal Doppler probe on chest radiographs. It is by no means an exhaustive description. This article is for the benefit of medical students, junior doctors in training, nurses and paramedical teams who would be involved in the care of critically ill patients. Self Assessment Multiple Choice questions (only one option is correct):1. The wires of permanent pacemakers are usually inserted viaA. Femoral veinB. Basilic veinC. Subclavian veinD. Subclavian artery 2. A chest radiograph is not useful in one of the followingA. To detect intact pacemaker wiresB. To indicate whether a pacemaker is working optimallyC. To detect whether pacemaker wires are dislodgedD. To identify a single chamber or dual chamber pacemaker Answers:1. C2. B
Day-case surgery is of great value to patients and the health service. It has rapidly expanded as a cost-effective and resource-conserving surgical intervention. However, the ability to deliver a safe and cost-effective general anesthetic with minimal side effects and rapid recovery is demanded in a day-case surgery unit. Pain and emesis are the two major complaints after day case surgery. Opioids are the agents of choice for severe pain. However, this class of analgesics is associated with dose-dependent adverse effects such as PONV, sedation, respiratory depression, resulting in delayed discharge or prolonged hospital stay. Non-opioid analgesics, e.g. acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs), are often used alone or as adjuncts to opioids because of fewer adverse effects compared to opioids alone. However, NSAIDs also have side effects [1]. Lornoxicam is a new NSAID that belongs chemically to oxicams, a chemical class including piroxicam and tenoxicam. Lornoxicam is a potent inhibitor of cyclo-oxygenase and the only oxicam with a 15 times shorter half-life than piroxicam and tenoxicam [2]. In addition, lornoxicam can be given by I.V. route. Lornoxicam has a better safety profile than diclofinac and naproxen with regards to renal and hepatic function tests. In addition to better GIT tolerability compared to selective COX2 inhibitors; it is completely metabolized to inactive metabolites [2,3]. Lornoxicam has been successfully used in prevention and treatment of postoperative pain. However, evaluation of the perioperative analgesic efficacy of lornoxicam in day-case surgery has not yet been studied. This randomized, double blinded study was designed to compare the quality of perioperative analgesia as well as side effects of IV lornoxicam versus fentanyl in patients scheduled for minor to moderate day-case ENT surgical procedures. Materials and Methods: Male or female patients (aged 18-60 yr) were eligible for inclusion in the study. After obtaining the approval of the Hospital Research & Ethical Committee and patient’s informed consent, patients were randomized into three groups of ASA class I and II, scheduled to undergo minor to moderate day-case ENT surgical procedures e.g. tonsillectomy, excision of ENT lesion (e.g. vocal cord nodules and cysts), polypectomy and endoscopic sinus operations were enrolled in this randomized, double blinded study between May and December 2008. Exclusion criteria were patients with body mass index (BMI) > 30%, drug or alcohol abuse, and known allergy to NSAIDs, paracetamol or any contraindications for opioid use. The protocol was similar for all patients. Prior to surgery, patients were educated in the use of the 10 – point visual analog scale (VAS) for pain assessment (0 = no pain to 10 = maximum pain). No premedication was given. In the holding area, an IV cannula was inserted and an IV infusion of Lactated Ringer’s was started. HR, MAP and SpO2 were recorded before induction (baseline value). Since fentanyl is a clear fluid while lornoxicam is yellow, the pharmacist prepared, covered and coded the medications in two coded envelopes for each patient. One envelope containing lornoxicam 8mg (L8), 16 mg (L16) or placebo to be given half an hour before induction of anesthesia and another envelope with fentanyl 100 µg (F) or placebo to be given with induction i.e. each patient received either IV (F), (L8) or (L16).The medications were administered by a different anesthetist, who was not involved in the study. Anesthesia was induced with propofol 2 mg/kg IV followed by cisatracurium 0.15 mg/kg IV to facilitate orotracheal intubation. After tracheal intubation, the patients were ventilated to normocapnia with sevoflurane (2-3% end tidal) in 50% oxygen in air. All patients received IV 1 gm of paracetamol after induction and were monitored with ECG, MAP, SpO2 and EtCO2. Supplementary fentanyl 0.5 µg/kg was given IV as required in all groups (if > 20% increases in MAP or HR than preinduction values in presence of adequate muscle relaxation). At the end of surgery, muscle relaxation was reversed and extubated. In the post-anaesthesia care unit (PACU), the time from extubation to spontaneous eye opening was compared between the groups. The patients were monitored with ECG, SpO2, MAP, respiratory rate (RR), VAS and sedation score (0 =awake, 1=mild sedation, 2=sleepy but arousable, and 3 = very sleepy) at 0.5,1, 2, 3 and 4 hours by an anaesthetist, who was not aware of the study drug used. Intramuscular (IM) injection of meperidine 1 mg/kg was administered as a rescue analgesic at VAS > 4. The total amount of meperidine required during first 4 hrs postoperative was recorded. The time of the study drugs injection was recorded after decoding their codes. The first need for rescue analgesic was recorded as the time from the administration of the study-drug and the administration of meperidine. The incidence of PONV or any adverse event was recorded. The PACU staff was not aware of the study drug given. The results were analyzed using SPSS version 16. Sample size was 35 patients for each group in order to detect a 20% change in HR and MAP. The α-error was assumed to be 0.05 and the type II error was set at 0.20. Numerical data were expressed as mean ± SD. The groups were compared with analysis of variances (ANOVA). The VAS pain scores were analyzed by Mann-Whitney U test. Categorical data were compared using the Chi square test. P value of 0.05 was used as the level of significance. Results 105 patients aged between 18 and 52 yr were enrolled in the study. There were no significant demographic differences between groups (Table 1). HR and MAP were significantly higher at 10 and 20 minutes after induction of anaesthesia in group L8 compared to groups F and L16 (P < 0.05) (Fig. 1,2). The number of patients with inadequate intra-operative analgesia was significantly higher in group L8 compared to groups F and L16 (Fig 3). In PACU, 40 minutes postoperatively, HR, MAP and VAS were significantly higher in groups F and L8 (Fig 4,5,6). The first analgesic requirement time was significantly longer in group L16 compared to groups F and L8 (Table 2). The mean sedation scores in PACU were insignificantly higher in groups F and L8 compared to group L16 (Table1). While the incidence of PONV was significantly higher in groups F and L8 (p<0.05) (Table 1). Table 1: Demographic characteristics, eye opening time, incidence of postoperative nausea and postoperative sedation score:
F
L8
L16
P
Age (year) - mean (range)
31 (18-52)
32 (18-51)
31 (20-49)
0.129
Sex F/M
Oct-25
Oct-25
Sep-26
0.695
Weight (Kg)
72.7±11.7
74.1±11.3
75.3±9.9
0.402
Height (cm)
166.2±14.7
169.4±11.9
161±19.5
0.482
ASA physical status I/II
23-Dec
22/13
25-Oct
0.312
Duration of surgery (min)
58.8±21.8
59.6±21.4
56.9±23.3
0.675
Time to eye opening (min)
7.2±3.1
6.4±1.2
3.7±1.6*
0.019*
Postoperative nausea
9/35
7/35
3/35*
0.002*
Postoperative sedation score (0 – 3)
1.7±0.6
1.9±1.1
1.4±0.6
0.357
Data are expressed as mean ± SD or number of patients* Significant difference (P < 0.05). NS: Non significant.- Time to eye opening is the time from extubation to spontaneous eye opening.Table 2: Perioperative analgesic requirements and time to first postoperative analgesic requirement (mean ± SD)
F
L8
L16
P
Intra-operative fentanyl supplementation (µg)
45.5 ± 13.2
67.8 ± 16.4*
43.1 ± 10.2
0.012*
Time of 1st postoperative rescue analgesic (min)
94.3 ± 33.4
101.6 ± 51.5
223.9 ± 62.3*
0.0002*
Postoperative meperidine rescue (mg)
76.3 ± 12.5
80.5 ± 11.7
39.9 ± 7.6*
0.001*
-Data are expressed as mean ± SD.* Significant difference (P < 0.05). NS: Non significant.-Time of 1st postoperative rescue analgesic is the time elapsed between the administration of the study drug and the administration of an analgesic postoperatively. Fig 1: Intra-operative changes in heart rate in groupsFig 2: Intra-operative changes in MAP in groupsFig 3: Number of patients requested perioperative analgesic supplementationFig 4: Changes in heart rate in PACUFig 5: Changes in MAP in PACU:Fig 6: Changes in VAS in PACUDiscussion: The use of an opioid, even a short acting one can be associated with adverse effects, which may not be acceptable for patients scheduled for day case surgery. For this reason, it was suggested to substitute an opioid with a non-opioid analgesic for postoperative pain control. The use of a NSAID is associated with adverse effects [1]. Lornoxicam has been successfully used in the prevention and treatment of postoperative pain. It has been shown to be as effective as morphine [4], meperidine [5] and tramadol [6]. To the best of our knowledge, this is the first study to compare the perioperative analgesic efficacy of lornoxicam to fentanyl in patients undergoing day case ENT surgery. We gave Lornoxicam half an hour before induction of anesthesia as the time taken to reach peak plasma concentration (Tmax) was determined to be 0.5 h [7]. During the operative procedure, HR and MAP were significantly higher in group L8 compared to group F and L16. While in PACU, patients in groups F and L8 had higher HR, MAP and VAS score in the early postoperative period compared to patients in group L16. This may be due to inadequate analgesic effect of L8 and the shorter plasma half life of fentanyl compared to L16. The analgesic efficacy of L16 might be attributable to inhibition of cyclo-oxygenase (COX1) and (COX2) activity [2], release of endogenous dynorphin and β-endorphin [5], decrease in peripheral and central prostaglandin production [8] as well as exertion of some of its analgesic activity via the central nervous system [9]. Lornoxicam has a more potent anti-inflammatory and analgesic effect than other oxicams as well as a shorter half life, which decreases the incidence of side effects of drugs with long plasma half life [10]. Arslan and colleagues reported decreased opioid need, PONV and postoperative pain scores when 16 mg of lornoxicam was administered after thyroidectomy [11]. While Xuerong and colleaguessuggested that the increase of postoperative morphine requirements induced by intra-operative administration of fentanyl could be prevented by ketamine or lornoxicam [12]. Rawal reported that NSAIDs are effective as the sole analgesic in a high proportion of cases of mild to moderate pain and it is more convenient to give these drugs by the IV route rather than by IM or rectal administration [13]. The analysis of pain intensity differences was complicated by the fact that many patients postoperatively were asleep at the time their pain assessments were due which may be attributed to effect of opioid and anesthetic medications used. To minimize any missing data we used time to the first dose rescue analgesia (based on changes in hemodynamic data) to evaluate pain intensity differences from baseline. L16 was well tolerated in this study, and was associated with a significantly lower incidence of adverse events than F and L8 which could be due to the opioid side effects in both groups. Norholt and colleaguessupported our results as they reported that, in terms of common acute adverse events, lornoxicam appeared to possess a higher benefit/risk ratio compared with morphine [4]. Zuurmond et al reported that, there is good evidence that avoidance of opioid virtually abolishes the PONV that preclude oral intake of fluids after surgery [14]. In our study, nausea developed in 25.7% of patients in group F, 20% in group L8 but only 8.6% in group L16 who received the least rescue opioid analgesia. Regarding bleeding abnormalities, Hodsman et al reported extensive bleeding required reoperation on two diclofenac group patients submitted to abdominoperitoneal resection of the rectum [15]. In our study no abnormal bleeding was reported by ENT surgeons in any of the study patients. In agreement with our results, Ilias et al[16], Trampitsch et al[17] and Karaman et al [18] used lornoxicam and they did not detect problems with surgical bleeding, bleeding time, blood transfusion requirement or postoperative bleeding. Stroissnig et al reported that overall, in healthy adult volunteers, oral doses of lornoxicam up to 70 mg have been well tolerated, and there have been no effects on vital signs, urine analysis parameters or clinical serum biochemistry [19]. In our study, none of the patients receiving study drugs experienced severe gastric discomfort, needed rescue antiemetic medication or required admission because of poor pain control. Previous studies used lornoxicam for reduction of postoperative opioid consumption but none of them had studied the intra-operative use of lornoxicam. So, we selected certain type of surgical procedures which might be suitable to use lornoxicam as a sole intra-operative analgesia. The adjunctive use of acetaminophen may have additive analgesic efficacy to lornoxicam because of its intrinsic opioid-sparing activity. Measurement of serum catecholamine would have been useful. These could be considered as a limitation for the present study. Conclusion: Intravenous 16 mg lornoxicam with the present study design was comparable to 100 µg fentanyl as intra-operative analgesia but more effective than fentanyl in preventing early postoperative pain in mild to moderate ENT surgical procedures. Intravenous lornoxicam 8 mg was not satisfactory as a sole intra-operative analgesia. The overall incidence of adverse effects of lornoxicam was lower than that of fentanyl.
The Foundation Programme1,2,3 is a 2-year, ubiquitous, vocational curriculum undertaken by newly qualified doctors wishing to proceed onto speciality training in the United Kingdom (UK). Since 2006, Foundation Year Trainees in the UK have been required to complete one clinical audit during their two year programme. We review the practice of audit and doctors’ attitudes to the difficulty in performing audits at a National Health Service (NHS) hospital trust comprising three hospital sites in the South East of England. The Foundation Programme demands that Foundation Year Trainees are able to consider the relevance of clinical audit and describe the audit cycle with regard to developing patient care, clinical governance and risk management. They are expected to undertake a clinical audit and recognize how it relates to the improving clinical standards and addressing clinical governance1. Clinical audit can be defined as the processof reviewing the delivery of care to identify deficiencies sothat they may be remedied4. Whilst it was initially used in assessing medicalpractice against local standards, audit ‘has evolved conceptuallyas a mechanism through which evidence-based guidelines can beintroduced into routine clinical practice’5. Apart from fulfilling the requirements of the syllabus, reasons for audit include professional education and the opportunity to improve patient care6. Barriers to audit might include: disagreement amongst professionals as to what constitutes a good audit5;organisational impediments; and a lack of resouces6. This study therefore sets out to investigate the level of audit activity in a hospital trust in South East England amongst all Foundation Year Trainees. Importantly it will also assess doctors’ attitudes and views towards the audit process and perceived or actual barriers to their completion. METHOD Questionnaires were sent to all Foundation Year 1 (F1s = 63 in total) and Foundation Year 2 (F2s = 56 in total) Trainees in the trust (119 doctors). The study group involved trainees in the Foundation Programme from 31st July 2007 to 30th July 2008. Doctors who had been transferred out of the trust were not included in the study. There were no doctors who had transferred into the trust and were in the Foundation Programme. A study representative at each of the 3 hospital sites was tasked to distribute the questionnaires. Trainees were asked to complete the questionnaires in an informal setting and to return them directly to the site representative. The study environment was variable, and questionnaires were distributed and completed on the wards or at group teaching sessions. Participants were given the choice of completing and submitting their form immediately, or submitting it at a later date. Data collection was commenced 11 months after the trainees had commenced employment in the trust and concluded after 2 weeks. This was invoked as many trainees were clearing annual-leave requirements towards the end of their hospital posting, and the consensus that very few audits would be officially completed at that stage of training in the summer. Questions were drawn from previous studies to the barriers to audit in our Trust. In the first section of the questionnaire, participants were asked about: “the number of all audits attempted or applied for”; “the number of new audits attempted or applied for”; “the number of audits completed and presented so far”; and “the number of audits started but never completed”. The second part of the questionnaire assessed subjective opinions on barriers to completing audits. Participants were asked to rate the following 5 statements on a comparative scale of 1-5 (1 being “strongly disagree” and 5 being “strongly agree”): “The audit department is helpful in approving audits”; “senior staff are helpful in involving me in audits”; “I can complete audits within official working hours”; “most audit opportunities are in my area of interest”; “most audit opportunities are of clinical value”. Results were collated and tabulated and presented at local meetings where feedback was received. RESULTS Ninety-two out of a possible 119 (77.3%) Foundation Year Trainees completed the questionnaire (57/63 - F1s, 35/56 - F2s). There were 106 total attempts at audit for the F1 trainees and 65 total attempts for the F2s. Most trainees had attempted 1 or 2 audits in their respective year (42 F1s at 73.7% and 23 F2s at 65.7%). 5 F1s (8.8%) and 3 F2s (8.6%) had neither attempted nor applied for any audits. Ten F1s (17.5%) and 9 F2s (25.7%) had attempted more than 2 audits (Table 1). Table 1: Number of audits attempted by trainees
Number of all audits applied for or attempted
F1s
F2s
Number
Percentage (%)
Number
Percentage (%)
0
5
8.8
3
8.6
1
21
36.8
17
48.6
2
21
36.8
6
17.1
3
3
5.3
3
8.6
4
2
3.5
5
14.3
5
4
7.0
0
0
6
1
1.8
0
0
7
0
0
1
2.8
Total
57
100
35
100
The results for the total number of completed audits (i.e. an audit that included data collection, analysis and formal presentation to the respective department) are summarized in Table 2. For F1s, 32 out of a total 106 attempted audits were completed (30.2%), this percentage rising for F2s (38/65; 58.5%). Thirty-three (57.9%) F1s and 10 F2s (28.6%) failed to complete any audit, with a number able to complete one audit presentation in the year: 18 F1s (31.6%) and 16 F2s (45.7%). Table 2: Number of audits completed by trainees
Number of completed audits
F1s
F2s
Number
Percentage (%)
Number
Percentage (%)
0
33
57. 9
10
28.6
1
18
31.6
16
45.7
2
5
8.8
6
17.1
3
0
0
2
5.7
4
1
1.7
1
2.9
Total
57
100
35
100
With respect to new and original audits attempted by trainees, this was achieved by 66.7% of F1s and 74.3% of F2s (Table 3). There was no formal data on the number of audit loops being closed. Table 3: Number of new audits designed by trainees
Number of new audits attempted or applied for
F1s
F2
Number
Percentage (%)
Number
Percentage (%)
0
19
33.3
9
25.7
1
25
43.9
19
54.3
2
9
15.8
3
8.6
3
1
1.75
2
5.7
4
1
1.75
2
5.7
5
2
3.5
0
0
Total
57
100
35
100
With regard to barriers to completion of audits (Table 4), results were notably equivocal for “helpfulness of the audit department and senior staff” (both averaging 3.1 on the comparative scale of 1-5), and “the clinical value of the audits available” (mean score 3.2). The mean score for “completing audits within official hours” was 2.1 with a similar trend observed in “the audits available in an area of interest” (mean score 2.6). Table 4: Trainees’ experiences with audit
Statement
Score¶
Total responses
1
2
3
4
5
Audit department is helpful
Percentage %
9.1
12.5
44.3
22.7
11.4
100
Numbers
8
11
39
20
10
88
Mean score
0.1
0.3
1.3
0.9
0.6
3.1
Senior staff are helpful
Percentage %
15.4
20.9
23.1
22.0
18.7
100
Numbers
14
19
21
20
17
91
Mean score
0.2
0.4
0.7
0.9
0.9
3.1
Audit completed in working hours
Percentage %
46.2
22.0
16.5
8.8
6.6
100
Numbers
42
20
15
8
6
91
Mean score
0.5
0.4
0.5
0.4
0.3
2.1
Audits in the area of interest
Percentage %
18.7
30.8
25.3
17.6
7.7
100
Numbers
17
28
23
16
7
91
Mean score
0.2
0.6
0.8
0.7
0.4
2.7
Audits have clinical value
Percentage %
7.7
18.7
30.8
34.1
8.8
100
Numbers
7
17
28
31
8
91
Mean score
0.1
0.4
0.9
1.4
0.4
3.2
¶Key: 1= strongly disagree; 2=disagree; 3 = equivocal; 4 = agree; 5 = strongly agreeNB: Some forms were incomplete, and therefore responses may not add up to 92. CONCLUSIONS Although audit is well established to be beneficial in improving clinical practice7, this study suggests that trainees under-perform against the curriculum of the Foundation Programme. Historically, the level of audit activity amongst doctors has been low; for example, McCarthy (1997) demonstrated that whilst doctors see the conceptual value of audit, approximately one-third only had presented their data at a pertinent audit meeting8. These results have been replicated in numerous other studies9,10,11. We believe that this data-set is the first available for junior trainees who have undertaken the Foundation Programme curriculum, with a good response rate of 77.3%, and incorporates the contractual pressures invoked by a European Working Time Directive (EWTD)-compliant Rota12,13. While the results show that the majority of respondents (>90%) had attempted an audit, most significantly the majority of audits that were started were not completed. A large percentage of F1s (57.9%) and F2s (28.6%) failed to complete an audit at all. Similar numbers have been reported, even among senior pediatric trainees at registrar level, where one study demonstrated that whilst audit activity was above 90%, only 16% had completed the audit cycle14. One possible explanation is that many trainees appear to have a sub-optimal comprehension about audit and its process. Our consensus was that some trainees attempted audits that were too large or unmanageable, or even of insufficient quality, in striving to achieve a peer publication from their work. When realized that the publication value is poor, or that the audit design is flawed, many trainees lose interest and fail to complete. Another concept highlighted by this study is confusion over the definition of a “completed audit”. For consideration of completion of an audit, a trainee has to demonstrate both the ability to collect the data and present it to among his peers in a formal meeting. This generally amounts to completion of 5 out of the 6 stages of the audit loop15. Surgical morbidity and mortality presentations had been considered audit by some trainees, as they were termed by the trust as a “surgical audit”. However, the overall clinical consensus is that they are not audit but formative educational meetings because no systemic local or national standards were employed for comparison. This poor understanding of audit has been well described previously16. Potential barriers to the completion of audit include some of the issues raised in this study. In this sample, doctors were equivocal about whether the barrier was the audit department or lack of senior support. This reflected the variability of experience as well as the lack of teaching of the purpose and methods of audit in the undergraduate curriculum. They were also equivocal about the clinical value of audits they had completed. By comparison, a study in Leeds showed that less than half of the 232 respondents were aware of subsequent change in clinical practice and 27% felt it was “a waste of time”7. However this study did not focus on the junior doctor in the beginnings of their postgraduate training. Trainees felt that an additional barrier to audit completion included difficulty in completing audits within their working hours. All Foundation Year Trainees in the trust were working to a EWTD-compliant Rota during the year, where trainees did not exceed 48 hours a week of on-site hospital clinical duties. Trainees also found it difficult to undertake audits in their area of clinical interest. Although part of the reason is circumstantial - the Foundation Year Programme mandates that trainees rotate around various core specialties - this may also reflect a lack of understanding of what the audit cycle actually incorporates, and how it is not formal research in itself15. Approval of audit studies was also thought to be problematic because such meetings only took place monthly with a pre-determined agenda, and consequently, this meant that approval might take several months to obtain for trainees who would actually be based in the trust for no more than 12 months in 3 different specialty departments. There were a number of limitations of the study, one being the small sample size. Secondly, in asking trainees to rate each of the six statements from 1 to 5, trainees who did not complete audits tended to score 3 (neither agree or disagree), and as the results above show, they represented a considerable proportion. A larger sample size and a semantic differential scale (rating responses between 1 and 7) might have been more discerning. The fact that some trainees may have included “audits” which on reflection did not meet the criteria for inclusion was not only interesting but may also have distorted results. Finally, audits that involved joint effort among trainees, but were presented only by one of them in the absence of the others were still regarded by some trainees to be “completed and presented” by all of them. This study has highlighted a number of issues which need to be addressed for clinical audits to be successfully completed during the Foundation Programme. The authors believe that poor completion rates are most probably the result of poor understanding of audit. Potential solutions include teaching medical students concepts of audit; giving structured teaching early in the Foundation Programme; instituting regular audit meetings; incorporating audit as part of contracted working hours; defining audit more clearly among trainees and clinical staff and encouraging more cooperation and integrative liaison with the audit department to process audit proposals quickly and efficiently. Additionally, doctors’ contractual pay-bandings should reflect any out-of-hours work undertaken on audits that improve clinical governance for their Trusts. However, in spite of all these considerations, we speculate that because trainees are only in each post for no more than 4 months during their foundation years, and with the restriction of working hours, the expectation of foundation year trainees to have undertaken and properly understood an audit cycle, implemented change and closed the audit loop is unrealistic. It would be more helpful to the trusts and trainees for audits to be part of the specialty training programme onwards, where trainees stay in a department for a longer time even as they move from one team to another. Further studies might consider in detail the difficulties in each step of the audit cycle15 and explore: Foundation Trainees’ use of the audit department; guidance from senior members of staff; and perceived benefits in clinical practice. Ultimately, audits must implement change17 and all truly successful clinical audits should aid in some way to achieving our fundamental goal in medicine; that being the best clinical practice and best quality of care.
Implantation of prosthetic mesh in repair of different hernias has gained a global acceptance and popularity. It is thought to be a potent safeguard against recurrence of hernias 1, 2.The use of prosthetic mesh in different types of hernias has brought a phenomenal change in the out look of hernia patients all over the world 3. Today, an ever increasing number of hernias are repaired by implanting prosthetic meshes either by conventional open method or by laparoscopic approach 4. Beside its well known advantages and global acceptance in every day hernia surgery, a number of complications are thought to be associated with the use of mesh in different types of hernias 5-15. We present our experience of mesh related complications in different open hernia repairs and their management in this study.MARERIALS AND METHODSIt’s a descriptive observational study over 5 years during which a total number of 1008 patients with different types of hernias were repaired electively in a teaching hospital as well as in private hospitals by the same surgical team. Of these, 638 (63.29 %) hernias were repaired by implanting prolene mesh of different sizes depending on the size of the defect. A drain was left in place in selected cases .The patients were followed up to a period of three years after discharge from the hospital. The follow up visits were scheduled at 1 month, 6 months, and then yearly. Of the total patients , 432(67.71%) were followed up to three years while 159 (26%) patients were lost in the follow up from day of discharge from the hospital. Another 47 patients attended follow up up to 2 years only and then disappeared. Sixteen of these patients continued to complain about chronic pain and foreign body sensation up to two years and then they did not return while 4 of these patients developed recurrent hernia in one year time but they were lost in follow up. The data of every patient is recorded on a proforma and their follow up records are maintained. The variables studied included immediate, early and late post-operative complications in addition to the demographic details. The statistical analysis of the data is done on SPSS version 12.RESULTSThe mean age of the patients is 41 years with a range of 73 years and a STD of 19.089. There is a male dominance (N=531, 83%) over females (N=107, 17 %). The commonest type of hernia in this series is inguinal hernia (n=518, 81%) followed by Para-umbilical hernia (n=83, 13 %). Distribution of different varieties of hernias among male and female study population is shown inTable-I. Table-1. Frequency of hernias and distribution among males and females
Type of hernia
Total
Inguinal
Para- umbilical
Incisional
Epigastric
Male
518
4
3
6
531
Female
0
79
26
2
107
Total
518
83
29
8
638
Of the total number, 34 (5 %) hernias were recurrent hernias including 21 inguinal hernias, 11 Para-umbilical hernias and 2 Incisional hernias. The patients were operated after preliminary investigations and medical fitness. All the patients were operated by open conventional technique regardless of the type of hernia. Total duration of operation is shown in Figure -I with maximum patients (467, 73%) operated with in 60 minutes. Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation
Type of hernia
Complications during same hospitalization
Total
Wound infection
Reaction
Mechanical failure
Seroma
Pain
Mesh infection
Hematoma
Inguinal
14
3
4
7
1
1
3
518
paraumbilical
5
1
2
3
0
3
3
83
Incisional
0
0
0
1
0
2
1
29
Epigastric
0
0
0
0
0
1
0
8
Total
19
4
6
11
1
7
7
638
Wound infection has an alarmingly high incidence in our series (n=19, 3 %). Most of these infections are superficial and effectively controlled by intensive antibiotic therapy so that the failure of repair is saved and mesh rejection prevented effectively. Four of recurrences occurred during 2 years follow up but patient discontinued follow up afterwards. Remaining 07 recurrences occurred between 24 to 36 weeks. The complications observed during the follow up period of up to three years in different hernias are shown in Table-III.Table-III Type of hernia * Late Complications after discharge Cross tabulation
Complications after discharge
Total
Type of hernia
Pain
Recurrence of hernia
Thickening of spermatic cord
Testicular atrophy
Inguinal
10
4
7
2
518
paraumbilical
2
7
2
0
83
Incisional
2
0
0
0
29
Epigastric
1
0
0
0
8
Total
15
11
9
2
638
A remarkably low incidence of wound infection in para-umbilical and incisional hernia is attributable to the placement of suction drain which prevents hematoma formation and secondary infection. Seven (2%) recurrences occurred in para-umbilical hernias where suction drain did not work. Mesh infection with massive reaction , although, treated conservatively in 5 patients with vigorous antibiotic therapy led to the formation of a weaker scar which later on gave way and recurrence of hernia occurred. Follow up was not 100% and about 26% patients were lost in the follow up. Majority of the patients (n=457, 90 %) were discharged within 4 days while patients who were complicated had a longer stay up to 15 days (P <0.001). Late complications were mostly chronic pain and foreign body sensations with 2 cases of unilateral testicular atrophy. DISCUSSION A number of non-infectious and infectious complications are attributed to the use of mesh in the repair of most of the hernias5, 13, 16. The type of mesh as well as their composition seems to affect complications following their use and specific materials are related to specific complications. We present 638 patients of different types of hernias repaired by implanting polypropylene mesh of varying sizes depending upon the size of defect. Prolene meshes are monofilaments, non-absorbable, inert, sterile and porous synthetic materials commonly used for this purpose. The use of mesh in hernia repair has brought a phenomenal change in the overall outcome of hernia repair especially in terms of recurrence of hernia 17. We experienced wound infection as the commonest complication in our series (n=19, 3%) and this was more so in the inguinal hernias. Most of the wound infections are superficial and very easy to control on conservative measures. On the contrary deep seated mesh infections are always dreaded complications and if not treated vigorously can lead to total failure and rejection of prosthetic mesh. A number of similar studies have reported an increased infection rate in mesh hernia repair testifying our results 18-28. Grant AM 29, however claims no difference in the incidence of infection between mesh and non-mesh repair of groin hernias. A severe local reaction occurred in 4 (0.62%) patients which resolved in few days without any consequences. Seroma and hematoma occurred in 11(2 %) and 7(1.09%) patients respectively. Only 3 seromas and one hematoma needed evacuation. We report a recurrence of 11(2 %) hernias of which 4 are inguinal and 7 are para-umbilical hernias. All of the recurrent para-umbilical hernias had severe reaction and wound infection in the post-operative period which was effectively controlled by vigorous antibiotic therapy and local wound care. There is probably a weaker scar after resolution of the infective process which resulted in recurrence. A significantly low recurrence rate in inguinal hernias in our study (0.77%) is consistent with the results of other similar reports 30-32. Chronic pain and a foreign body sensation poses a real problem and though it occurred in only two cases but a similar study by Bay-Nielsen M 33 claims 22.9% study population having chronic pain and more so in the adult males. CONCLUSION Although mesh repair is an efficient method of hernia repair, a number of complications may be associated and can lead to failure. An aggressive antibiotic therapy and wound care may control even massive infections.
Good Medical Practice describes the professional behaviour expected of doctors and advocates that it should be taught as well as assessed. GMC’s Good Medical Practice specifies the standards of team working, communication skills, accessibility and trustworthiness in relation to professional behaviour1. Ramsden2 stated that: “the students will learn what they think they will be assessed on, not what is in the curriculum, or even on what has been 'covered in class'.” Hence, if the intended learning objectives are to improve professional behaviour and team working in a trainee doctor, then a tool that assesses these characteristics along with providing suggestions for improvement is critical. Multisource Feedback (MSF) is a formative assessment tool that was designed to assess professional behaviour and attitudes, with the aim of continually improving an individual’s team working. Team Assessment of Behaviour (TAB) is an assessment tool for MSF (Appendix 1), and is one of the 2 assessment tools used to assess professional behaviour of foundation doctors in training in the UK, the other being the Mini-Peer Assessment Tool (mini-PAT)3. Our aims for this article were to evaluate whether the format of TAB allowed the MSF process to occur as originally intended, along with looking at possible barriers that may have to be overcome to make it an effective tool. A literature review was carried to appraise the present evidence regarding TAB as an assessment tool and only studies which had relevance to MSF/TAB were included in the study. As TAB is a relatively new tool, there were very few papers’ exploring this is depth which was a major limitation. Hence in the barriers section, we have discussed the possible obstacles to the whole MSF process rather than just TAB. Background The concept of MSF was originally developed by industrial organisations and has been used in postgraduate medicine in USA for assessment of professional behaviour since the 1990’s4,5. Ramsey6 suggested that it is feasible to obtain assessments from professional associates of practicing physicians in areas such as clinical skills, humanistic qualities, and communication skills. TAB was developed by educationalists and senior doctors at the West Midlands deanery7,8,and has undergone extensive field testing among 171 trainees, with analysis of received feedback from 1378 assessments across four different hospitals in the West Midlands. It is currently being used in the West Midlands Deanery for the multisource feedback of foundation programme trainees. Process of TAB The primary aim of TAB as an assessment tool is to identify trainees whose professional behaviour does not meet GMC requirements for good medical practice, so that appropriate action may be taken and also to compliment those trainees who receive good reports. For TAB, up to 10-15 multi-disciplinary colleagues of a doctor assess his/her workplace behaviour. It assesses four domains of professional behaviour: professional relationship with patients, verbal communications, team-working and accessibility. It is the initiative of the trainee to distribute at least 15 TAB forms to peers of their own choice and a minimum of 10 completed forms are required to be returned. The raters should include at least three other doctors including a consultant supervisor and at least five allied healthcare professionals. It’s the responsibility of the educational supervisor to collate and summarise these forms, identifying perceived weaknesses, offering them feedback and directed learning objectives to address any issues. Critique of TAB:1. Validity and reliability of TAB:Validity is a demonstration that a particular instrument can in fact measure what it purports to measure9. TAB portrays face as well as content validity as it assesses areas identified by the GMC1 for good professional behaviour. It is shown to be capable of identifying problem behaviour in trainees, which was the primary aim of the tool7. This tool appears to have good construct validity as it is testing trainee’s behaviour in real life situations. It is difficult to define the predictive validity of any tool, more so in a formative assessment tool. The developers of TAB have not tested for concurrent validity. The concurrent validity for TAB could have been tested by using another MSF tool in addition to TAB for some participants during the field-testing for reliability and validity of the tool. A reliable instrument for a piece of research will yield similar data from similar respondents over a period of time9. Whitehouse7 demonstrated in the pilot study that TAB had intra-observer reliability and inter-observer variability. For inter-observer variability, the Royal College of Psychiatrists compiled a map of assessment programmes against good medical practice domains and considered it appropriate for assessing four domains: good clinical care, working with colleagues, probity, and health11. 2. RatersRamsey et al5 concluded that, with MSF, 10-11 responses per physician were necessary to achieve a generalisablity coefficient of 0.70. Wood et al11 concluded that eight raters were sufficient for a representative score in their study on Obstetrics & Gynaecology trainees in the UK. Obviously more raters would lead to better coefficient and more generalisable results. TAB presently advocates at least ten raters to achieve reliable results.3. Feasibility TAB has four domains and a three point rating scale which are relatively easy to understand and complete. There is no training required for raters and usually takes less than five minutes per assessment per assessor. The paper-based system demanded considerable administrative resources, and therefore a web-based TAB assessment form was successfully piloted in the West Midlands8.4. Trainer & trainee’s evaluation of the processThe evaluation of TAB as an assessment tool was done by Whitehouse et al8 as a part of their field assessment of TAB. The assessors and trainers found the process practical, valuable and fair. 76% of the trainees who responded to the questionnaire felt that it was a useful addition to the assessment of the SHO’s. The educational supervisors had mixed views, with 77% of them finding out nothing new about the trainees. 5. Scoring systemInstead of a Likert scale, the TAB employs broad boxes which offer the rater a choice of giving specific feedback under each domain. This is more helpful to a summariser/assessor than mini-PAT, where a scoring scale is not substantiated by relevant feedback. This assessment tool does not assess clinical performance and one could argue that there could have been more than four domains in order to include other areas of performance, such as clinical skills. However having just four domains can reduce the impact of the halo effect. The halo effect12 can be defined as a rater making an overall judgement of the trainee and scoring the whole form accordingly rather than considering each domain separately. This could be a potential advantage of TAB over mini-PAT where there is no opportunity to provide specific feedback in individual domains, but rather utilises an overall action plan, which may lead to concentrating single element deficiencies while masking other shortcomings. 6. Patient OutcomesThe MSF process in itself doesn’t bear direct consequences on patients’ management, but can help the doctor improve his professionalism, which is critical element of good medical practice1. An improvement in a doctor’s behaviour secondary to the appraisal-feedback process can indirectly improve and contribute to patient management and satisfaction. Potential barriers: 1.Choice of rater:The trainee has the choice of raters, except for the supervising consultant, who must be involved in the process. This is a potential area of difficulty, as the trainee might pick individuals who are more sympathetic to their cause, or who cannot comment much on their interpersonal behaviour, thus leading to skewed results. Kuzmits13 showed that both rater and those being rated needed to be trained to make the rating and feedback process more effective, but this is not felt necessary for TAB. There is also a potential conflict between being a trainer and assessor, and this conflict might lead to clouding of judgement14, which can be addressed by having different assessors and trainers, but considering the service pressures in the NHS, this may not always be possible. 2. Feedback:The value of the MSF process can be limited by the quality of feedback provided to the trainee at the end of the process and depends on the relationship of the trainee and the supervisor15. Evidence shows that non-specific feedback does little to change performance16. Whitehouse8 concluded in their initial study that TAB was able to produce descriptive feedback that was more specific and helpful than existing MSF tools. Assessors completing TAB may not give specific comments or feedback although they are instructed to give some details especially if they chose the rating of “some concern” or “major concern”. Bret and Atwater17 have shown that negative feedback can discourage individuals, and they can even react in anger. Feedback about performance must be descriptive and specific if it is to be helpful to trainees18. Hence it is the responsibility of the supervisor to give feedback which is relevant and helpful, along with creating an action plan with the trainee to address any perceived deficiencies. It must also be stressed that good performers need to be complimented, and encouraged to continue to do so. 3. Training the raters and the supervisor:The raters also need to be educated in the process otherwise they may not give reliable views about the trainee13,19. From the rater’s point of view, it would be beneficial if they were to give specific comment, in order that more relevant feedback can be provided. Most importantly, the educational supervisors who provide the feedback to the trainee can make a difference in constructing agreed learning objectives, and not demoralise the trainee with negative feedback. Kaplan20 also noted that negative feedback can demotivate individuals. Giving face to face negative feedback can be a daunting task and supervisors, if not trained in giving negative feedback may dislike doing it, and so not give properly constructed feedback. The provision of training, however, has time as well as cost implications. Conclusions TAB continues to be part of the national foundation programme curriculum and, used correctly, can serve its purposes both as a screening tool and also for the trainees to use the feedback provided to improve their interpersonal behaviour when needed. Evaluation and quality assurance of this assessment tool should be an ongoing process. More field work in relation to assessment of behaviour in relation to TAB is needed. Patient feedback could be included in TAB which can make it a more reliable tool for assessing a doctor’s behaviour.Further qualitative studies to explore the views and experiences of trainees can help to understand the barriers and attempt to improve the usefulness of the process for the trainees. There are several potential barriers which can subvert the process of MSF by using TAB, and these need to be addressed to make the assessment process more effective and efficient. KEY POINTS
MSF is designed to assess professional behaviour and attitudes
TAB along with Mini-PAT and other tools map MSF principles
The supervisor assumes a key role in giving constructive feedback without demotivating the trainee
Relevant training while giving feedback is critical to the success of MSF
Patient’s involvement in the MSF process could make it more robust.
Leg ulcers are defined as discontinuity of the epidermis and dermis in the lower limb of more than 6 weeks duration 1, 2. They are a common presentation in the elderly population and are associated with a negative impact on the quality of life of patients and they also cause a substantial burden on the health budget 3. Pathogenesis of leg ulceration is heterogeneous 4. Prevention strategies, early identification and proper management are paramount in improving quality of life of patients and reducing costs on an already strained health budget. In this article we review the prevalence of leg ulcers in the elderly people, its common causes and management.
Prevalence The estimated prevalence of leg ulcers in the UK is between 1.5 and 3 per 1,000 population 3.A studies by Moffat et al 2004 showed a prevalence of 0.45 per 1000 which is less than the previously reported figures 5. In the same study leg ulceration was found to be more common in females than males 5. In a systematic review of prevalence studies for leg ulcer, the authors also reported an increase in prevalence of leg ulcers with age and in women 6.The overall prevalence of ulcers is not affected by social class although ulcers tend to take longer to heal in lower socio economic classes 7.Quality of life Several studies have shown that patients with leg ulcers have a poor quality of life compared to age matched controls 8, 9.A systematic review of studies measuring quality of life of patients with leg ulcers showed a negative impact on several domains of quality of life 8. In most of the studies pain was shown to be the major complaint among leg ulcer patients compared to controls, with males experiencing greater pain intensity than female patients. 10, 11 Restricted mobility and sleep disturbance due to pain was also reported in other studies.12 Leg ulcer patients often complain of itchiness, odour and leg swelling 8. In one study, unpleasant odour was reported as causing social embarrassment leading to higher anxiety and depression scores as well as altered body image 12.Reduced mobility due to leg ulceration can restrict working capacity in younger patients13.A negative emotional impact on life with symptoms such as anger, depression, and social isolation was reported by 68% of patients in another study looking at impact of leg ulcers on quality of life 14. Aetiology Several factors contribute to the development of leg ulcers. However majority of ulcers are due to venous insufficiency which accounts for about 80-85% of all cases. 15, 16. Frequency of venous ulcers increases with age as a result of several factors such as immobility and venous disease15. Other risk factors for venous ulceration include obesity, previous deep vein thrombosis, thrombophlebitis, previous fracture, and varicose veins 17.Venous ulcers(also referred to as varicose or stasis ulcer)are commonly found between the malleoli and lower calf and are associated with a shallow base covered with granulation tissue and fibrinoid material, and have irregular margins 16,17. The mechanism of venous ulceration involves initial damage to valves as a result of thrombosis or valve incompetence in varicose veins leading to pooling of blood in lower limbs. Extravasation of red blood cells then follows which causes a local inflammatory reaction and collagen deposition. This impairs the healing process eventually resulting in tissue breakdown and hence ulceration16. Venous ulcers are also associated with symptoms such as oedema, eczema.Arterial ulcers form the second largest group of leg ulcers and account for about 20% of leg ulcers. Atherosclerosis and diabetes are the commonest causes of this group of ulcers. Thrombotic episodes secondary to vasculitis, thromboangitis, and sickle cell disease can also result in arterial ulcers17.Arterial insufficiency causes hypoxia, ischaemia, tissue necrosis and consequently ulceration 18.Arterial ulcers are usually found below the ankle especially on the toes. The ulcers are characteristically small, have steep edges and a dry base. Risk factors for arterial ulcers include conditions that predispose to peripheral vascular disease such as smoking, diabetes, hypertension, hyperlipidaemia and obesity 17. It is worth mentioning that diabetes causes foot ulcers via two mechanisms: ischemia and neuropathy. Neuropathic ulcers are usually found on the plantar surface of metatarsal heads or on the toes. They are a consequence of poor glycaemic control19. The risk of malignancy in chronic leg ulcers is generally believed to be small, but a study by Yang et al 1997 showed a rate of 4.4% in chronic leg ulcers. The diagnosis should be considered in patients with non healing ulcers despite optimum management 20. Chronic inflammatory conditions such as rheumatoid arthritis, inflammatory bowel diseases are also associated with leg ulceration. Rare causes of leg ulceration such as ill fitting shoes have also been reported in literature. In a study looking at complications of ill fitting footwear among 65 elderly patients, foot ulceration was reported by 15% of the patients 21. Although small, this study showed that simple measures such as appropriate foot wear may be useful in preventing foot ulcers. Table 1: summarises causes of ulcers and main characteristics of leg ulcers 16, 17
Aetiology of ulcer
Characteristics
Venous
Between malleoli and lower calf, shallow, irregular margins, granulation base. Oedema, eczema
Arterial
Painful, below ankle distal, especially toes, small, dry baseIntermittent claudication
Vasculitis
Associated with Rheumatoid arthritis, Polyarhritis Nodosa(PAN)
Malignancy
Basal cell , squamaous cell carcinoma, melanoma
Neuropathic
Common in diabetes, wet, deep, sharp borders on pressure points
Management Like all medical conditions, management of leg ulcer should include a detailed history of the onset of the problem (as well as past medical history), examination of the legs and skin, investigations and modalities of treatments. The underlying causes need to be identified as this has crucial implications for management. A medical history suggestive of venous and arterial ulcers have been mentioned above but other factors to consider while assessing leg ulcer are: general health status, cigarette smoking, nutrition, limitation to self care, pedal pulses, Ankle Brachial Pressure Index (ABPI), oedema, limb size and shape, sensation and pain (Table 2). Table 2: Assessment of lower limb ulcers
Patient
History of ulcer developmentPast and current medical problemsGeneral health statusNutritionSocial, occupationMobility problemsLimitation to self careObesityDepression
Skin changes
VenousArterialMalignantAuto immune
Vascular assessment
Pedal pulsesAnkle Brachial Pressure Index
Limb factors
OedemaCircumferencesLymphoedemaOrthopaedic problemsSensation and pain
Examination of the legs and skin identifies markers of underlying pathology. Venous disease may present with some or all of the following: brawny skin, haemosiderin staining, lipodermatosclerosis, atrophie blanche (patchy areas of ischemia),and stasis eczema, while the skin of patients with arterial disease is often shiny, hairless, pale and cool; with thickened nails and changes in foot structure. The absence of venous or arterial signs and symptoms raises the possibility of less common causes of ulceration like: Sun damaged skin, Bowen disease or a history of previous skin cancer treatment is an alert to a malignant lesion. Site & Appearance: Most venous ulcer occur in the “gaiter” area of the leg (i.e. area extending from just above the ankle to below the knee and tends to occur on both lateral and medial aspect of the leg), they are usually superficial with poorly defined margins. The base of the wound is usually red granulation tissue with moderate to high levels of exudates. Arterial ulcers can occur anywhere on the lower leg and may appear in the gaiter region, especially with coexisting venous disease. Many arterial/ischaemic ulcers occur over bony prominences and have a history of pressure related cause. They are often deeper with a punched out appearance and may involve structures such as muscles, tendon and bone in the base. They have sloughy, devitalized tissue in the wound base and low levels of wound exudates. Ulcers occurring in atypical site with an atypical appearance require further investigation to determine the cause. Ulcers with a violaceous (purple) border, inflammation, and extreme pain, may be related to vasculitis problem or underlying connective tissue disorder. Size: Dimensions of the ulcer should be taken at first presentation and fortnightly thereafter and recorded in the notes. This is important as it gives an objective assessment of the effectiveness of the current treatment plan, and modify as necessary22.There are a range of techniques available such as digital photography, ruler based vertical, horizontal and depth measurements and circumferential tracings of wound margins using acetate sheets over cling film .The system chosen needs to reflect consistency, accuracy, and reduced operator error, and also provide visual feedback to the patient. Pain: The level of pain associated with ulcer must be assessed on presentation and at each visit thereafter using a standardized pain scale (0-10). Pain may suggest infection or arterial disease, so careful assessment is required.Surrounding skin area should be observed for the presence of eczema, hyperkeratosis skin, maceration, cellulitis, signs of irritation and scratching which are signs and symptoms associated with underlying venous disease.Assessment should also include palpation of peripheral pulses, regular blood pressure measurement, weight (with reference to a Body Mass Index chart) as well as routine urinalysis (to screen for diabetes). Vascular Assessment: This is mainly carried out by the use of Doppler ultrasound to measure the Ankle Brachial Pressure Index (ABPI).This is mandatory and must be repeated every 3 months. All patients with a non healing wound on the leg of greater than 4-6weeks should have a vascular assessment to eliminate any underlying ischaemic disease22.The result of ABPI are used to determine the likelihood of arterial insufficiency and can be used to guide the management plan, especially in relation to healing potential, referral for vascular assessment and use of appropriate compression bandages. 23 The normal range for ABPI is 0.8-1.2. An ABPI of less than 0.5 or greater than 1.2 needs vascular opinion.Treating the ulcer Many dressing materials are available for the treatment of leg ulcers and there is no adequate evidence from clinical trials to recommend one dressing type over another, but we have to bear in mind few criteria in choosing a particular dressing. The dressing should be low adherent, cost effective and must also be comfortable as well as acceptable for the service user. The choice of product should be determined by the level of exudate. Products which commonly cause skin sensitivity such as those containing lanolin and topical antibiotics should not be used on any service user22. The use of white soft paraffin has been identified as a potential fire hazard risk, hence a water based emollient should be considered as an alternative to a paraffin emollients e.g aqueous cream. Please note water based emollients are not as effective in providing sustained emollient therapy as an ointment and also contain preservatives, which are known potential irritants. Other modalities of treatments of leg ulcers are described below. Compression Therapy The mainstay of treatment of any venous component to ulceration is the application of sustained, graduated compression at therapeutic level 24 .Graduated compression increases venous flow, decreases valvular reflux while walking and increases the effectiveness of the calf muscle pump resulting in a “thinning leg”. The most effective level of compression to overcome venous hypertension has been determined to be around 40mmHg at the ankle 25. Correct application of bandages is essential to avoid pressure ulceration over the bony high points and along the anterior border of the tibia. It is acknowledged that the application of compression bandaging is a specialized skill traditionally undertaken by nurses. The combination of compression bandages used to achieve compression of 40mmHg at the ankle will depend on ankle circumference, according to Laplace’s law, which states that the sub bandage pressure is inversely proportional to the circumference of the limb. A modified compression regimen is necessary when pain is present. This may be achieved by providing periods of relief until pain is controlled or removing the bandage at night when the leg is elevated. Patients with mixed arterial and venous disease may only tolerate up to 20mmHg compression to treat oedema. Bandage choices include short stretch, long stretch, multilayer systems and stockings. A Cochrane Review of compression regimens identified increased healing rates with compression compared to no compression26 . A high compression bandages were better than moderate compression bandages, and that multi-layered bandages were better than single layered bandages. Comparisons between various high compression bandages systems, e.g. 4 layer and short stretch bandages, were unable to find any difference in effectiveness. For venous ulcer with ABPI > 0.8, use 4 layer bandages as per ankle circumference below (Table 3) Ulcers with ABPI between 0.6-0.8: Reduced compression is achieved by omitting the outer cohesive bandage (e.g. Coban) Table 3: Multilayered bandage regime in relation to ankle circumference.
ANKLE CIRCUMFERENCE
BANDAGE REGIME
Up to 18cm
2 or more wool padding1 light stretch bandage(Elastocrepe)1 light elastic bandage 3a(K-plus)1 cohesive bandage 3b(Coban)
Once the ulcer site is well healed, continue with the compression bandages for at least 4 weeks and then maintain compression at a slightly lower level indefinitely as tolerated. It must be replaced annually. Other factors to consider and deal with include: Infection This requires regular cleansing, more frequent changes of dressing (especially if exudates levels are high), topical antimicrobial dressings or systemic antibiotics. Pain Ranging from simple analgesia to potent opioid (depending on severity of pain), non steroidal anti inflammatory drugs may be beneficial. For neuropathic pain, amitriptyline can be started which can be replaced by gabapentin if no improvement. The dose can be titrated upwards. Pressure: Requires pressure relief for the ulcer to heal especially over bony prominences. Larval Therapy Larval therapy has been used for debridement of wounds for many years.27 Debridement is an essential component of wound care as the presence of devitalized tissue can impede the healing process. While the exact mechanism of larval therapy remains unknown, it encompasses three processes: debridement, disinfection and promotion of healing. The beneficial effects of larval therapy were first observed during the Napoleonic war by Larrey, who noted that soldiers whose wounds had become infested with maggots had an improved prognosis 27. During the First World War, Baer documented the successful treatment of leg ulcers and osteomyelitis using larval therapy, and paved the way for further use of it by doctors of that time. However, the development of antibiotics and improvements in surgical techniques reduced larval therapy to a “treatment of last resort”, reserved for the most intractable wounds 28. The emergence of antibiotic- resistant strains of bacteria such as methicillin resistant staphylococcus aureus (MRSA) and the curiosity of researchers has prompted a resurgence of interest in larval therapy. Larval therapy has been employed effectively to treat a wide spectrum of wounds including venous and arterial leg ulcers29.Some of the benefits of larval therapy include: reduction in wound pain and odour, and promoting healing process with relatively few side effects30 .Larval therapy is also reported as being cost-effective in comparison with conventional wound dressings. The use of larval therapy often resulted in quicker healing, and a subsequent reduction of nursing time and materials30. A further advantage of larval therapy is that, as larvae are typically applied for 3 days, wounds are disturbed less frequently than conventional dressings that require changing every 1-2days.In addition to this, a further advantage is that treatment can usually be carried out in outpatient and community settings. A study at an outpatient wound clinic on chronic wounds, of varying aetiologies reported that using larval therapy resulted in a 62% decrease in need of amputation 31. Larvae offer the benefit of eliminating bacteria from the wound through ingestion and subsequent degradation within their intestinal tract. They also act to reduce bacterial activity through the production of inhibitory secretions. The most commonly mentioned disadvantage of larval therapy is the negative perception with which it is regarded by both patients and practitioners because of the unpleasant appearance. The use of “Biobags”, which completely enclose the larvae within a polyvinyl alcohol membrane, has become a popular method of improving the application of this treatment, as larvae are able to feed freely through the open cell polymer. Pain has occasionally been reported by patients, the cause may be the sharp mouth hooks and spicules with which larvae anchor themselves onto tissue. A case history has suggested larval therapy to be contraindicated with fistulae, exposed wounds connecting to vital organs32 because bloodstream infections have been reported with some larvae33.Alteration of the disinfection process appeared to eliminate this problem, and with no further cases of sepsis occurring during the subsequent 12 months The risk of cross-infection by escaped larvae may be greatly reduced through careful dressing. Vacuum Assisted Closure therapy Vacuum Assisted Closure (VAC) therapy involves the application of controlled negative pressure to wounds 34. Negative pressure, as a method of management for difficult to heal wounds, was initially explored in 1970, with the first wound drainage system being introduced in 1989. The use of negative pressure to heal wounds, however, is more commonly associated with the work of Argenta and Morykwas in 1997.35 VAC therapy was designed with the aim of improving healing, decreasing morbidity, and decreasing the cost and length of hospital stay in patients with chronic, non healing wounds. VAC therapy promotes healing in several ways. Firstly, the foam dressing, in combination with adhesive tape, creates an occlusive dressing. This alone prevents dessication and increases the rate at which epithelial tissue is developed, therefore aiding healing times. Occlusive dressing prevents an increase in infection. Secondly, the suction effect and the mechanical forces generated at the interface of the foam work to decrease interstitial fluid accumulation, control wound exudates, stimulate granulation tissue formation, reverse tissue expansion, decrease bacterial colonisation and increase blood flow and dermal perfusion. In summary, VAC therapy aids wound healing by: Maintaining a moist environment Increasing local blood flow Removing wound exudates Promoting granulation tissue formation Reducing infection Exerting mechanical pressuresVAC therapy is suitable for the following wound types/processes 36 Acute (trauma, burns) Chronic (pressure sores, leg ulcers, diabetic ulcers) Surgical (skin grafts, flap surgery, wound bed preparation) Salvage (wound dehiscence, wound infection, post operative sternum infections) Contraindications to the use of vacuum therapy include: wounds with untreated osteomyelitis, grossly infected wounds, when necrotic tissue is present or when there is unspecified disorder of the blood. VAC therapy should also not be used in wounds with malignancy .Dressings should not be placed over any exposed vessels or organs and VAC therapy should be used with caution in patients with active bleeding, difficult wound haemostasis and in patients taking anticoagulants. Skin grafting Skin grafting is the transplanting of skin, and, occasionally, other underlying tissues to another location of the body. It is the only means of reconstructing a defect in the skin, regardless of the cause of the defect 37. Generally, skin grafting is used when, in the opinion of the reconstructive surgeon, other methods of reconstruction such as primary closure, secondary intention healing, or local skin flap are inappropriate, are unavailable or would produce a suboptimal result. Skingraft are divided into 2 major categories: full thickness skin graft (FTSGs) and split thickness skin graft ( STSGs).STSGs may be subdivided into thin (0.008-0.012mm),medium(0.012-0.018mm) and thick (0.018-0.030mm)grafts 37. STSGs are the one used in covering chronic unhealing cutaneous ulcer. Split skin grafting is technically demanding and requires hospital admission25. The discharge from the surface of venous ulcers tends to dislodge continuous sheets of split skin, leaving a choice between mesh and pinch skin grafting. Pinch skin grafting provides epithelial islands, from which epithelial growth may spread outwards as well as inwards from the ulcer margin. Pinch skin grafting has been done by district nurses in the community and has been found to be cost effective accelerating healing when used with multilayer compression bandaging.25 Some contraindications to the use of skin graft generally include: vascular tissues such as exposed bone or cartilage (as this will lead to graft necrosis), uncontrolled bleeding of the recipient because of haematoma and/or seroma formation under the graft compromises graft survival. Venous Surgery Superficial venous surgery has been shown to improve ulcer healing in patients with only superficial venous incompetence38. In patients with no deep reflux on duplex imaging, superficial venous surgery has been shown to reduce long term ulcer recurrence25 . Indications for superficial venous surgery are:
Patient fit for surgery
Sufficient mobility to activate calf muscle pump
Prepared to attend hospital for investigation and surgery
Obesity controlled (BMI <30)
Superficial venous incompetence
There are few other modalities of treatment of leg ulcers currently in use, although no strong evidence has been found to show they really improve healing. Intermittent Pneumatic Compression Intermittent pneumatic compression (IPC) is a mechanical method of delivering compression to swollen limbs that can be used to treat venous leg ulcers and limb swelling due to lymphoedema.It uses an air pump to inflate and deflate an airtight bag wrapped around the leg.39 However, review of trials found conflicting evidence about whether it is better than compression bandages. It may increase healing compared with no compression but it is unclear whether it improves healing when added to treatment with bandages. Electromagnetic Therapy Electromagnetic therapy involves the use of electromagnetic, microwave, or infrared energy to diagnose or treat an illness by detecting and correcting imbalances in the body's energy fields. Electronic devices that emit some form of low-voltage electrical current or radio frequency are often involved. It has been used in the treatment of chronic diseases like venous leg ulcers. Cochrane wound group conducted trials on several occasions comparing electromagnetic therapy with other treatments and up till now, there is no reliable evidence of benefit of electromagnetic therapy in the healing of venous leg ulcers.40 Further research is still needed.Oral Zinc Supplement Leg ulcers may take long time to heal despite good wound care. This may be due to poor nutrition which reduces the ability of the body to repair itself. Minerals such as zinc are necessary for good healing and so it has been thought that taking zinc sulphate tablets might aid healing of ulcers especially if patients were found to have low baseline Zinc level. Few trials were found where zinc was used to treat leg ulcers but all were too small to pick up on any benefit, if such a benefit exists. In addition, the quality of those trials was mediocre. On the basis of the evidence available so far, it appears that taking zinc tablets does not improve leg ulcer healing, however more good quality trials are needed.41Laser Therapy Low level laser therapy (LLLT) refers to the use of red beam or near infrared laser with a wavelength between 600and 1000nm power from 5-500 milliwatts.It is also referred to as cold laser therapy, low power laser therapy (LPLT), low intensity laser and low energy laser therapy. The exact effect of its mechanism is unknown; however, hypotheses have included improved cellular repair and stimulation of the immune, lymphatic and vascular system. Several randomised controlled trials involving patients with venous ulcers failed to demonstrate any significant benefits of LLLT when compared to standard treatment methods or placebos.42Hyperbaric Oxygen Therapy Oxygen is one of the most versatile and powerful agents available to the modern medical practitioner. The therapeutic use of oxygen under pressure is known as hyperbaric oxygen therapy (HBO2) and has been used to assist wound healing for almost 40 years. HBO2 has several specific biological actions which can enhance wound healing processes .These include: Hyper-oxygenation of tissue, vasoconstriction, down regulation of inflammatory cytokines, up-regulation of growth factors, antibacterial effects, potentiation of antibiotics, and leukocyte effects.43 Systemic oxygen can be administered via 2 basic chambers: Type A( multiplace) and Type B(monoplace). Both types can be used for routine wound care, treatment of most dive injuries, and treatment of patients who are ventilated or in critical care.HBO2 is a relatively safe non-invasive therapy. Side effects include middle ear and pulmonary barotraumas and myopia. Contraindications include poor cardiac output and severe obstructive pulmonary disease. Conclusion In this article, we have been able to show that leg ulcers are a common presentation in the elderly population and have negative impact on the quality of life of affected patients. It has been found to be more common in females. Most leg ulcers (about 80-85%) are caused by venous insufficiency, followed by arterial ulcers. A comprehensive assessment of the patient, skin, vascular status, limb and ulcer is required to determine aetiology and to formulate an appropriate management plan as described above. Several researches are still going on other modalities of treatment of leg ulcers. However, all patients should be provided with both verbal and written information to help them understand their condition and treatments they receive, as this will enable them to better understand their conditions, and will support concordance between patients and staff.
Spasticity is a common symptom seen as a consequence of an injury to the brain (stroke, trauma, hypoxia, infection, cerebral palsy and post surgery), spinal cord injury or multiple sclerosis. It is a complex problem, which can cause profound disability alone or in combination with other features of upper motor neuron syndromes (figure 1). The word “spasticity” is derived from the Greek word “spasticus”, which means “To pull or To Tug”. Spasticity is defined1 as “Disordered sensori-motor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles”. Simply stated, spasticity is stiffness of muscles that occurs after injury to the spinal cord or brain. Awareness of the implications and associated symptoms can minimise development of long term secondary complications (table 1). The impact of spasticity can be devastating. If not managed early and appropriately it may result in progressive disability, resulting in secondary complications such as contractures and pressure sores. This significant impact has ensured that spasticity management is a prominent feature in the national management guidelines for long term neurological conditions, promoting coordination of care between primary, secondary and social care providers. Symptoms Spasticity can range from mild muscle stiffness to severe, painful and uncontrollable muscle spasms. It is associated with both positive and negative components of upper motor neuron syndromes. Positive components include muscle overactivity, flexor and extensor spasm, hyperreflexia, athetosis, spastic dystonia, clonus, and an extensor plantar response. Common negative symptoms comprise weakness/ paralysis, early hypotonia, fatigue and loss of dexterity. Spasticity can be distinguished from rigidity by its dependence on the speed of muscle stretch and characteristic distribution in antigravity muscle groups. Spasticity does not always cause harm and can occasionally assist in the rehabilitation process by enabling a patient to stand when their limb weakness would not otherwise allow it Table 1 Clinical and functional problems associated with severe Spasticity
Physical
Emotional / social
·Non- specific pain·Discomfort·Painful muscle spasm·Difficulties with activities of daily living. e.g. washing, dressing, eating, toileting, maintaining hygiene, sexual activity·Problems with posture and mobility·Physical deformity and longterm contracture·Pressure ulcers
·Emotional e.g. low mood, distorted self image, impaired motivation·Impact on fulfilment of life roles as a partner or a parent·Sleep disturbance – due to pain and discomfort·Vocational- impact on employment or education·Social isolation – due to restricted mobility
Figure 1 Vicious cycle of spasticity Assessment of spasticityBefore any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale
4 Rigid extremity 3 Loss of full joint movement, difficult movement, considerable tone2 Full joint/ limb movement, but more increase in tone, limb still easily moved.1+ Slight increase in tone, catch and resistance through out range of movement1 Slight increase in tone, catch or minimal resistance at end of range of movement0 no increase in tone
It is also important to remember that not every “tight” muscle is spastic. The clinically detectable increase in muscle tone may be due to spasticity, rigidity or a fixed muscle contracture.Management The key to successful spasticity management is education of the patient and carers with both verbal and written information. This allows them to understand, appreciate and be fully involved in the management plan. All patients with spasticity should be followed up by a coordinated multidisciplinary team, which allows more timely intervention and close monitor of the progress. Liaison between health and social services in both primary and secondary care is essential in long term management. This helps to deliver a more consistent approach to the individual over time (figure 2). Table 3 Aims of spasticity management.
1.Improve function- mobility , dexterity2.Symptom relief-· Ease pain- muscle shortening, tendon pain, postural effects· Decrease spasms· Orthotic wearing3. Postural- Body image4. Decrease carer burden- Care and hygiene, positioning, dressing5. Optimise service responses- to avoid unnecessary treatments, facilitate other therapy, delay/prevent surgery
The first step in the management of spasticity is to identify the key aims and realistic goals of therapy. Understanding the underlying pathology and possible prognosis is helpful in planning these goals (table 3). Other key points to consider are: · Identification and management of any trigger or aggravating factors-Initial assessment should exclude any co morbidity that may worsen spasticity such as pressure sores, chronic pain, infection (commonly urinary tract infection), constipation or in-growing toe nails.· Instigation of an effective and realistic physical programme including attention to posture and positioning Figure 2 Approach to spasticity assessmentComprehensive assessment of spasticityRecognition of underlying provocative factorsImpact on the individualMeasurement of spasticityPotential goals- individualised and person focussed Initial approachEducation to patient/ and their family /carersMultidisciplinary team assessmentIdentification of clear treatment goalsEstablish mechanism for monitoring and review Management Manage triggering factorsBalance between positioning and movementPosture and seatingPhysical therapy and active exercise programmeSplinting and use of orthoticsPharmacotherapy A) Physical modalities· Stretching- this intervention has the benefit of being benign and non-invasive. Maintaining muscle length through passive or active exerciseand stretching regimens including standing or splinting canbe key to managing spasticity both in the short and the longterm.· Cooling of muscles- this inhibits mono synaptic stretch reflex and lowers the receptor’s sensitivity, different techniques such as quick icing and evaporating spray like ethyl chloride are occasionally used.· Heat-heat may increase the elasticity of the muscles. Techniques used include ultrasound, fluidotherapy, paraffin, superficial heat and whirlpools. These techniques should be combined with stretching and exercise.· Orthosis/equipment/ aids – an orthosis or splint is an external device designed to apply, distribute or remove forces to or from the body in a controlled manner to control body motions and /or alter the shape of body tissues. E.g. ankle foot orthosis, insoles, ankle supports, wrist/ hand/ elbow splints, knee splints, spinal brace, hip brace, neck collar. Some equipment can also aid positioning e.g. T roles, wedges, cushions and foot straps.These are usually used in combination with other modalities like botox therapy. Attention to posture and positioning, whichmay include the provision and regular review of seating systems,is paramount in managing severe spasticity· Massage– althoughvarious techniques are in use there is no evidence to support this· Dynamic physiotherapy technique- many schools of physiotherapy claim that particular technique has antispastic and functional benefits, particularly for the more mobile person. E.g. Bobath technique, proprioceptive neuromuscular facilitation, Brunnstrom technique. B) Electrical therapy· Functional Electrical stimulation –Thisis an adjunct to physiotherapythat can be of benefit to selected individuals who are predominantlyaffected by upper motor neuron pathologies resulting in a foot drop. Randomised controlled trial by Burridge et al in patients following stroke found that the use of functional electrical stimulation in combination with physiotherapy was statistically superior to physiotherapy alone3· Transcutaneous electrical nerve stimulation – this has been found to reduce spasticitythrough its nociceptive action and reduction of pain.C) PharmacologicalMedicationshould always be used as adjunct to good general management and education. Identification of treatment goals will help optimise drug therapy not only in terms of choice of agent, but also in timing and dose. Aims of medication should be to improve function or relieve troublesome symptoms rather than to simply reduce the degree of spasticity. Table 4 Useful things to remember to optimise medication effects
1. Clear written/verbal information for patients about effects/adverse symptoms of drugs 2. Clear treatment goals3. Detailed drug history- Review of other medication and potential drug interaction4. Appropriate form of drug e.g. liquid preparation if swallowing difficulties5. Regular review of efficacy and side effects6. Aids to help administer drugs e.g. dossette box, timer to remind7. “Start low and go slow” to avoid deleterious effects on function or unwanted side effects8. Combination of drugs to obtain synergistic action
Table 5 Different methods of delivery of medication
·Enteral – orally or via PEG e.g. baclofen, benzodiazepins, dantrolene, clonidine, tizanidine, gabapentin·Transdermal system e.g. catapress TTS·Intrathecal e.g. baclofen pump (other drugs used alone or in combination intrathecally include clonidine, morphine, fentanyl, midazolam, lidocaine)·Intra muscular/ focal injection e.g. botulinum toxin·Nerve blocks e.g. Phenol, Ethanol
The oral agentsAlthough different categories of drugs are available, those most commonly used to treat spasticity are baclofen,tizanidine, benzodiazepines, dantrolene, and gabapentin4, 5, 6. Different agents act through different mechanisms (table 6 and 7) for e.g. GABA-like (baclofen, benzodiazepine), central alpha 2 agonists (tizanidine, clonidine) and peripheral anti-spastics (dantrolene). Antispastic drugs act in the CNS either by suppression of excitation (glutamate), enhancement of inhibition (GABA, glycine) or a combination of the two. Table 6 Mechanism of action of commonly used oral antispasticity medication
Drugs acting on
Drugs
GABA- ergic system
baclofen, benzodiazepines, piracetam, progabide
Ion flux
dantrolene sodium, lamotrigine, riluzole
Monoamines
tizanidine, clonidine, thymoxamine, beta blockers, and cyproheptadine
Excitatory amino acids
orphenadrine citrate, cannabinoids, inhibitory neuromediators and other miscellaneous agents.
Baclofen remains the most commonly used anti-spastic agent. The preferential indication is spasticity caused by spinal cord disease especially in multiple sclerosis. Many studies including the pilot study by Scheinberg et al 7 demonstrated that oral baclofen has an effect beyond placebo in improving goal-oriented tasks (such as transfers), in children with spastic quadriplegic cerebral palsy. In open-label studies of oral baclofen, the drug improved spasticity in 70-87 per cent of patients; additionally improvement in spasms was reported in 75-96 per cent of patients. In double-blind, crossover, placebo-controlled trials, baclofen was reported to be effective, producing statistically significant improvements in spasticity8.The main adverse effects of oral baclofen include sedation or somnolence, excessive weakness, vertigo and psychological disturbances. The incidence of adverse effects is reported to range from 10 to 75 per cent. The majority of adverse effects are not severe; most are dose related, transient and/or reversible. The main risks of oral baclofen administration are related to withdrawal; seizures, psychic symptoms and hyperthermia. These symptoms improve after the reintroduction of baclofen, usually without sequelae. When not related to withdrawal, these symptoms mainly present in patients with brain damage and in the elderly. The limited data on baclofen toxicity in patients with renal disease suggest that administration of the drug in these persons may carry an unnecessarily high risk. Tizanidine is an efficient and well tolerated antispastic. It is predominantlyan alpha 2 agonist and thus decreases presynaptic activity of theexcitatory interneurones. There is a large body of evidence for the effective use of tizanidine monotherapy in the management of spasticity 15. Tizanidine is the antispasticity drug that has been most widely compared with oral baclofen. Studies have generally found the two drugs to have equivalent efficacy, although tizanidine has better tolerability; in particular weakness was reported to occur less frequently with tizanidine than with baclofen.Dantrolene has a peripheral mechanism of action and acts primarily on muscle through inhibitingcalcium release from the sarcoplasmic reticulum. It decreasesthe excitation–coupling reaction involved in muscle contraction and can be prescribed in the different forms of spasticity. The efficacy of benzodiazepines (diazepam, tetrazepam, clonazepam) is comparable with baclofen. Although there is no evidence to suggest any difference in effectiveness between them, diazepam and dantrolene are associated with more side effects than baclofen and tizanidine. There are other compounds with anti-spastic properties (gabapentine, cyproheptadine, piracetam). Their advantage is
Table 7
Drug
Dosage
Doses per day
Mechanism of action
Common side effects
Initial dosage
Maximum dosage
Baclofen
5mg x3
90mg
4
GABA ergic
Seizure, Sedation, Dizziness, GI disturbances, psychosis, Muscle weakness
rather limited when used alone. Generally, they are administrated in combination with usual anti-spastic drugs. A few short term trials have trialed gabapentin with good results 19 .Pregabalin may be of value as a systemic agent in the treatment of spasticity, although properly controlled studies with clearly defined outcome measures are required to confirm this finding 22. The Sativex Spasticity in MS Study Group23 concluded that oromucosal whole plant cannabis-based medicine (CBM) containing delta-9 tetrahydrocannabinol (THC) and cannabidiol (CBD) may represent a useful new agent for treatment of the symptomatic relief of spasticity in MS. Intrathecal pump· Baclofen- If oral drug treatment is inadequate in controlling lower limb spasticity or is not tolerated, intrathecal delivery of baclofen should be considered. This has been found to be a cost-effective strategy when compared to conventional medical management alone by Bensmail et al 20 .The benefits of continuous intrathecal baclofen infusion have been demonstrated in more than 80 percent and over 65 percent of patients report an improvement in tone and spasms respectively. The main risks of intrathecal baclofen infusion are symptoms related to overdose or withdrawal. These are mostly related to catheter disruption, failure to refill the pump reservoir or failure of the pump's power source. Abrupt disruption of intrathecal baclofen can be a serious scenario with continuous spasms, tremors, temperature elevation, seizure and death having been reported.· Phenol- As phenol is a destructive agent which indiscriminately damagesmotor and sensory nerves, it is reserved for those individualswho do not have any functional movement in the legs, who havelost bladder and bowel function and who have impaired leg sensation. Intrathecal phenol can be an effective treatmentwhich, though it requires expert administration, does not havethe long term maintenance or cost issues that are associated with intrathecalbaclofen treatment. The effect of a single injection often lastsmany months and can be repeated if necessary 24. D) Nerve blockPeripheral nerve blockade/ Regional blocks/ Neurolytic blockade25 are another therapeutic possibility in the treatment of spasticity. This can be done with the help of fluoroscopy or nerve stimulation. Chemical neurolysis by phenol/ alcohol is irreversible and can be used at several sites. Blocks are applied most often to 4 peripheral sites: the pectoral nerve loop, median, obturator, and tibial nerves. The main indication is debilitating or painful spasticity. Peripheral blocks with local anaesthetics are used as tests to mimic the effects of motor blocks and determine their potential adverse effects. Peripheral neurolytic blocks are easy to perform, effective, and inexpensive30.E) Botulinum toxin injectionBotulinum toxin is the most widely used treatment for focal spasticity27,28,29. The effect of the toxin is to inhibit the release of acetylcholine at the neuromuscular junction. The clinical effect of injecting botulinum toxin is reversible due to nerve sprouting and muscle reinnervation, leading to functional recovery of the muscle in a few months. It is essential that botulinum toxin injections are given in conjunction with physiotherapy in order to obtain the maximum benefit. The toxin is injected directly into the targeted muscle and an effect can be noticed from as early as 2-3 days with a maximum effect seen by about 3 weeks, lasting at least 3 months. As it is not a permanent treatment it may have to be repeated after a few months.Many randomisedcontrolled trials show that botulinum toxin is effectivein reducing muscle tone in various conditions 28, 29. Brashear and colleaguesdemonstrated a reduction in spasticity in the wrist andfingers of patients following stroke with the use of botulinum toxin, together with an improvementin their disability assessment scale29.E) Surgical techniqueMost surgical procedures are irreversible. This means that realistic goal setting between the health care provider, family and patient is critical. Neurosurgical techniques have been proven useful in conditions like cerebral palsy 32, 33.· Neurosurgical techniques- Anterior and posterior rhizotomy, peripheral neurotomy 31, Drezotomy, percutaneous radiofrequency rhizotomy, spinal cord and deep cerebellar stimulation of the superior cerebellar peduncle 32, functional neurosurgery 33· Orthopaedic procedures- directly act on muscles and tendons e.g. lengthening operation, tenotomy, neurectomies, and transfer of tendons.
Key Points to remember1.Spasticity management is more effective in multidisciplinary settings2.Early multidisciplinary approach and goal setting is crucial3.Education and clear communication between patients, carers and health care providers is essential4.Early intervention and optimal therapy prevents long term complications.5.Focal spasticity responds well to botulinum toxin injection, while generalised spasticity needs oral/ intrathecal medications
Healthcare organisations are a fertile breeding ground for interpersonal conflict and the development of dysfunctional relationships. The supervisory relationship between trainer and trainee is a particular area of concern for junior doctors. Aside from a problem trainee, such conflict can arise from a difficult supervisor, poor communication, personality clashes and power inequalities. This article will come from a trainee’s perspective in emphasising how these factors relate to the difficult supervisor. Recommendations are made for organisations and individuals on how the causes and consequences of this problem can be addressed .
The nature of working relationships
“Like a successful personal relationship, both sides must be able to acknowledge their goals, the obstacles they perceive in achieving their goals, and must be willing to compromise …” 1
Working relationships, like personal relationships, are embedded in a complex and diverse world with people of different personalities, backgrounds, motives and desires. Getting on with our fellow humans is a fundamental part of living and a challenge in our working lives. Garelick and Fagin (2004) have explored this area and have identified what facilitates a good working relationship (figure 1):
Figure 1: Factors that encourage good working relationships 2
Clarity about the organisation’s tasks and objectives
Clarity about the authority structure, with clear lines of accountability
The presence of a common goal or objectives
The opportunity to participate and contribute
The ability to trust and compromise
The possibility of setting aside inessential differences
Respect for alternative viewpoints
Protection of the weakest member of the team
Good leadership
A balance between individual aspirations and corporate needs
Sharing similar life experiences or cultural background
Dysfunctional Working Relationships
“Differences of perspectives … lead to interpersonal conflict that spirals into dysfunctional relationships” 3
Interpersonal conflict is a “dynamic process that occurs between interdependent parties as they experience negative emotional reactions to perceived disagreement and interference with the attainment of their goals” 4. Interpersonal work conflict can impact in terms of satisfaction, well-being, work disability, and mental health outcomes such as psychiatric morbidity, depression, fatigue and psychological distress 4. Factors that can play a role in conflict include perceived disagreements about tasks, ambiguities in role definition, or if the responsibilities are unclear 4.
One of the central issues inherent in workplace disputes is irrational behaviour on the part of one (or both) of the employees when the facts get confused with their highly charged feelings 5. In an attempt to avoid conflict the other individual may be uncomfortable about raising the issue, feel intimidated by someone with greater authority or power, or suspect a personal agenda, but does not want to sound argumentative. This can result in an emotionally charged situation with layer upon layer of faulty assumptions building up to a proverbial house of cards and the development of entrenched beliefs 3. Therefore what started as a misunderstanding can lead to a dysfunctional relationship3, which can result in multiple problems impacting on the organisation and the individuals involved. Specific consequences include complaints of bullying and racism against the trainer, labelling of the trainee as a doctor in difficulty, or the trainer developing a reputation as a “difficult supervisor”.
Causes of trainer-trainee conflict in medicine
In the field of medicine, particularly given the hierarchical structure of the profession, the potential for conflict is accentuated. Trainees tend to rotate around jobs, and educational supervisors, every 6-12 months. Trainees and trainers are expected to adapt to working with each other with differences in personality, styles of working, and expectations. It is therefore inevitable that difficulties will develop.The fundamental causes of the conflict between trainer and trainee in healthcare are:
1. The problem trainee
The problem junior doctor is a well-established area of concern 6. This type of doctor may be inflexible, clinically incompetent, arrogant, have poor time keeping or organisational skills, refuse to do what is asked, exhibit poor communication skills, lack enthusiasm, lack educational objectives, or have a difficult personality. Despite the “doctor in difficulty” being regarded as a “problem trainee” the dysfunctional relationship between trainer and trainee in medicine is usually a product of both parties.
2. The difficult supervisor
The most important factor in determining trainee satisfaction has been shown to be the quality of supervision provided by the consultant trainer 7. However the difficult supervisor, often a consultant, is an issue that is underreported. The problem consultant comes in various guises shown in figure 2:
Figure 2: The problem consultant 2
Authoritarian and bullying
Controlling
Indecisive and disorganised
Burnt-out
A consultant who is never there
A consultant biding time to retirement
The flirtatious consultant
Poor teacher and communicator
Generally a problem consultant would have, over the years, established a reputation as a difficult person to work with, usually confirmed by their peers and trainees. Unfortunately this aspect of their personality is ignored when they complain about a new trainee. Therefore the consultant is never identified as a difficult supervisor. Knowledge of what constitutes a bad supervisor should be accompanied by what is a good supervisor. In the field of psychology the notion of a good supervisor applies to any supervisory relationship (figure 3).
Figure 3: Good supervisor 8
Straddling the potentially conflicting roles of mentor and evaluator
Providing impartial and thorough evaluation within contexts that respect supervisee’s integrity
Having expertise
Being trustworthy
Modelling respect of differences in values, expectations and experiences
Tolerant of mistakes and facilitating trainees progress
Providing direct and clear feedback to trainees
Open to feedback about their own style of working
3. Communication problems
A supervisor should possess good communication skills in the form of: active listening, demonstrating understanding, using open questions, building areas of agreement and being open. As a good communicator the supervisor should refrain from stating unreasonable expectations, views, or opinions. They should avoid offering incentives / warning of consequences or revealing feelings. In the workplace, in times of pressure, dysfunctional communication is instrumental in trainer-trainee conflict.
These communication problems are prominent in the area of feedback 9. Feedback is a key role of the supervisor 10. Feedback should be honest, relevant, objective, specific, timely, and planned 9. It should be based on accurate information rather than hearsay and focused on behaviour and performance rather than personality and attitude. It should be constructive, conducted in private, descriptive rather than evaluative, and designed to avoid personalising and blaming 9. Feedback should not be given on things the trainee cannot change e.g. personality.
Should the trainee feel offended by feedback at any point then it may be that the supervisor has a hidden agenda or is a bully. A delay in feedback impedes efficient working so the giving and receiving of feedback should also be a balanced ongoing process in order to boost morale and motivation, leading to greater effectiveness and job satisfaction 9. If the supervisor has a good relationship with the trainee then constant feedback should be given about his/her performance: the final report should never be a surprise 11.
4. Personality clashes
Conflict may also reveal itself in personality differences between trainee and trainer. Personality characteristics of the latter that can significantly affect an otherwise healthy relationship include a trainer who is preoccupied with details, order, organisation and schedule. Such trainers may be seen as perfectionist, pedantic, rigid and stubborn, and often insist that others submit to their way of doing things, according to their own self-proclaimed high standards.
Personality clashes may arise from poor communication or underlying factors including racism, sexism, religion, or jealousy and envy interfering with the relationship on both sides 12. The crucial question to ask is whether the trainer-trainee conflict is a result of a difficult trainee, or whether it arises when a trainee does not fit the supervisor’s scheme of things.11
5. Power differential
The trainer/supervisor also has an evaluative function in relation to the trainee and therefore the potential for abuse and trainee vulnerability in respect of the supervisor, is clear 8. The dependence of trainees on trainers for references creates a “potential power imbalance and in some cases may lead to intentional or unintentional harm to the trainee” 13. This harm may be identified in the trainer’s assessment of the trainee when completing the end-of-post evaluation. The trainer taking a proactive approach in writing complaints and sending emails to sabotage a trainees’ career may also demonstrate abuse of power.
Equally an overpowering consultant may, consciously or unconsciously, take advantage of the situation by going on a fault-finding mission. This can become part of a self-fulfilling prophecy. If the trainee is perceived to be poorly performing the supervisor may feel under more pressure and become hostile towards the trainee, without addressing the main problem 12. The result is that the supervisor engages in “continuous criticism and academic humiliation” 12 which causes the trainee to feel more useless and helpless. This can lead to the trainee becoming a scapegoat in an already dysfunctional team12.
Another consequence of the power imbalance is that it causes a state of confusion for trainees who want things to change but will often tolerate the problem and endure it to avoid jeopardising their career prospects. The trainee may feel powerless and fearful about addressing the current problem and choose to be silent on the matter, rather than risk an unpleasant situation 12. Unfortunately such passive behaviour may result in the problem escalating and the trainer may, unconsciously and unwittingly, bully the trainee 8.
How to deal with trainer-trainee conflict?
“Conflicts are really a house of cards ... you can bring them down by getting to the bottom and getting to the facts” 3 .
Dealing with trainer-trainee conflict involves good emotional intelligence, self-awareness (being self aware and taking an honest look at oneself), self-regulation (ability to control emotions), empathy (ability to identify and understand the wants, needs and viewpoints of others), being well-motivated, and having good social skills 14. In other words, successful conflict resolution relies on first understanding ourselves, being aware of our personality, our prejudices, why we like some people and not others, and recognising that certain things will annoy us and not others 11.
From a trainee’s perspective conflict with the supervisor should be addressed at an early stage to prevent escalation of the problem 12. This should include self-appraisal, thinking about the root of the problem in a factual and non-personal way, and informal discussion with a discreet colleague to gain another perspective. Trainees should find out how their predecessor got on in the post. Finally, problems should be freely discussed with the supervisor. However, there may be supervisors with whom it is difficult to have a discussion; therefore the trainee must involve others to deal with the issues which escalate or remain unresolved. If the supervisor is considered the source of the problems there are steps to take to ensure the power of the supervisor is not misused against trainees (figure 4):
Figure 4: Steps to deal with a difficult supervisor 13
College / speciality tutors and clinical tutors / programme directors have an obligation to act as the trainee’s advocate
Where tutors and programme directors fail to act appropriately, a direct approach by the trainee to the local postgraduate dean or relevant college may be indicated
The local trainees’ committee, trade union, and its officers / representatives may also be helpful in acting as the trainee’s advocate in appropriate circumstances
Deanery contact monitoring and training programmes’ approval visits, involving the College and conducted on behalf of the Postgraduate Medical Education and Training Board, also afford opportunity to raise concerns about supervisors
If trainees consider their health affected by the stress of working with a difficult supervisor they should seek help from their occupational health department or postgraduate dean, who may offer confidential services and helpful advice for the assessment of mental health problems affecting doctors
Trainees may be reluctant to take the steps described in figure 4. The power differential between trainer and trainee, as well as acting as an antecedent to the conflict, is a perpetuating factor that ensures nothing is done about it. The difficult supervisor may be underreported for the same reasons seen with workplace bullying, namely, fear of making matters worse, belief that nothing will be done, concerns regarding confidentiality, fear of victimisation, and concerns about being labelled as a troublemaker 15. Ultimately it is the fear of the consequences that deters trainees from speaking out, though it is worth remembering that Franklin D Roosevelt stated in his first inaugural speech, “the only thing we have to fear is fear itself”.
What can healthcare organisations do about supervisory conflict?
Organisations must be proactive in identifying and dealing with problems between trainers and trainees, who in turn ought to be aware of their responsibilities. Organisations may be tempted to sweep problems under the carpet but there are recommendations on how they can address the causes of trainer-trainee conflict (figure 5):
Figure 5: Steps for organisations to tackle the causes of trainer-trainee conflict
Cause
Solution
Problem trainee
Training of supervisors in not only how to identify the problem junior, but how to constructively manage the problem at the outset. Adopting a positive, non-judgemental and non-confrontational approach, and having a problem-solving mindset are essential
Difficult supervisor
Training of supervisors regarding their roles as a educational and clinical supervisor
Training of supervisors in sensitive areas of diversity and equality, and self-reflection, with the support of college tutors and programme directors
360 degree feedback carried out frequently and acted upon promptly during the supervisor’s appraisal
Communication Problems
Communication skills training
Constructive feedback training
Personality Clashes
Training of supervisor and trainee in conflict resolution since there may be personality differences between the two, rather then an individual doctor in difficulty.
Power differential
Power imbalance of feedback can be countered if feedback from each trainee becomes part of appraisal and revalidation for consultants
Colleges should collect anonymous feedback about educational and clinical supervisors from trainees and review their future role as supervisor
Complaints of bullying and racism should be dealt with promptly and effectively by the organisation.
Paice (2002) describes an excellent mentor as someone who “will always inspire, teach by example, and excite admiration and emulation” 16. Mentoring can be beneficial in facilitating the development of the trainee but “faculty mentoring should be avoided’’ 17. In other words mentoring of doctors should not be carried out by the trainee’s educational supervisor or line manager, nor should they be involved in their assessment or appraisal, to avoid blurring the distinction between the roles 17. A good mentor should :
Motivate
Empower and encourage
Nurture self-confidence
Teach by example
Offer wise counsel
Raise the performance bar
However, the authors argue that these are the qualities that should be part of being a good supervisor 17.
Conclusion
“Differences in power and status, and dependence on references, places juniors in invidious positions when they experience problems in their relationships with trainers” 2
The relationship between trainer and trainee should reflect the same warmth and nurturing as in a parent-child relationship. There is a parallel with both types of relationship in that there is an imbalance of power that interacts with poor communication and personality conflicts. In medicine although the problem junior doctor is frequently highlighted it must be remembered that the trainer-trainee conflict may reflect a difficult supervisor. The supervisor needs to achieve a healthy relationship that is sensitive to the needs of the trainee, void of any of their preconceived beliefs and prejudices, and act as a role model in making a good doctor and achieving their full potential 16. Interpersonal conflict can nevertheless develop and escalate to the extent that the trainee may suffer in silence. Healthcare organisations can be more proactive in penetrating the causes of the dysfunctional working relationship. Trainees should be fearless in turning to existing support in face of a difficult supervisor.
KEY POINTS:
Professional working relationships are a major challenge in healthcare
Interpersonal conflicts can lead to a dysfunctional working relationship
Issues include problem trainees, poor communication, and personality clashes
Power inequalities and the difficult supervisor need to be addressed
Trainer-trainee conflict can be resolved with steps taken by the individual
Organisations must address the causes of dysfunctional working relationships
Trainees need to overcome their own fears when tackling conflict
Schwannoma (neurilemmoma) is a peripheral nerve sheath tumour and commonly occurs on the head, neck and trunk. Giant schwannoma is rarely located in the retroperitoneum and the pelvis but rarer in the mesorectum. The majority of symptoms caused by the tumour are due to its mass effect. Surgical resection is enough to treat the tumour. Schwannoma is usually a benign tumour. Its malignant transformation is usually very rare. We report a 36 year old male patient with a giant mesorectal schwannoma who presented with vague symptoms.
Case Report
A 36 year old male patient presented with a lower abdominal mass since 2 months, urgency of defecation since 6 months and erectile dysfunction for more than 3 years. There was no history of urinary disturbances. General physical examination did not reveal any abnormality. Abdominal examination showed a non tender, firm, fixed mass with well defined borders over the suprapubic region which was extending into the pelvis. No organomegaly was detected. On rectal examination a hard, immobile mass was felt 5 cm away from the anal verge and lying anterior to the rectum.
His urine analysis, routine hematological investigations and renal function test were within normal limits. Total bilirubin was raised to 24.9 µmol/l (3.42-20.52 µmol/l), direct bilirubin was also elevated 8.2 µmol/l (0-6.8 µmol/l) while all other results were within normal range. The patient was positively screened for Hepatitis B and Syphilis. CT scan (figure 1) of abdomen revealed a large soft tissue mass measuring 10x11 cm in the pelvis. It was a well defined mass without any infiltration to the following structures: sigmoid, rectum, prostate gland, the bladder and the sacral bone.
Figure 1 shows a large soft tissue mass measuring 10x11 cm which compresses the rectum.
FNAC of the mass which was taken 3 cm from the anal verge showed isolated fibrotic tumor.
The patient was advised for HIFU therapy (high intensity focused ultrasound) in view of eventual surgery. In HIFU therapy, the ultrasound beams are focused on the diseased tissue and due to the significant energy deposition at the focus, temperature within the tissue rises to 65° to 85°C, destroying the diseased tissue by coagulation necrosis and hence facilitating the dissection of the mass during surgery. After HIFU therapy, the patient no longer complained of urgency of defecation. But there was no significant change in the size of the mass after a rectal examination.
Hence, explorative laparotomy was carried out. The abdomen was opened through the lower midline incision. A huge mesorectal mass of 15x11x8 cm (figure 2), was identified on the right side of the rectum and behind the prostate gland extending upwards, without any posterior infiltration into the sacral bone. Complete excision of the mass was achieved by blunt dissection and the mass was sent for histopathological examination. The operation was uneventful.
Figure 2 shows the complete excision of a well encapsulated mass of 15x11x8 cm. The external surface of the mass was gray-white and smooth.
Figure 3: Histology showing typical pallisading arrangement of spindle cells (Antoni-A/Verocay Body) and less cellular myxoid areas (Antoni-B)
Discussion
Schwannoma (Neurilemmoma) is a benign neoplasm arising from the myelinated nerve sheaths. Malignant schwannoma despite their name, never arise from malignant degeneration of schwannomas. Instead they occur from transformation of a plexiform neurofibromatosis. This fact provides the basis for their association with neurofibromatosis1.
Schwannomas are frequently present in patients aged 20 to 50 years with a male predominance. They comprise 5% of all benign soft tissue tumors and have a predilection for the head and neck2, 3, 4 and flexor surfaces of the upper and lower extremities5. Pelvic schwannoma is rare and accounts for less than 1% of all benign schwannomas6. The rarity of this tumor and the lack of clinical manifestations make a pre-surgical diagnosis very difficult.
These tumors slowly increase in size before becoming symptomatic. Clinical signs or symptoms manifest themselves only by the compression or infiltration of adjacent organs. Therefore, detection is often accidental.
Schwannoma typically appears as a solitary, well encapsulated, firm and smooth-surfaced round mass. In large tumors (>8-10 cm), a degenerative pattern (cystic areas, calcifications, interstitial fibrosis, and hyalinization) is commonly found that identifies the “ancient” variant7. Histologically, typical schwannomas are composed of inter mixed Antoni A components (cellular and arranged in short bundles or interlacing fascicles) and Antoni B areas (less cellular and organized with more myxoid components).Schwannomas show uniform and intense staining for S 100 protein8.
Malignant transformation is very rare and controversial9. Malignant schwannomas are large in size and highly aggressive tumours. They are painful, and may cause many different symptoms depending on the location and size. They infiltrate into the adjacent structures and metastasize to distant sites. Histologically, the nuclear palisading may be a striking feature. There will be perineural and intraneural spread of tumour, lesional proliferation, or herniation into the lumina of the vessels10.
A combination of clinical, pathological and immuno-histochemial studies help to make the diagnosis.
However preoperative diagnosis of schwannomas is not easy owing to the difficulty in finding imaging features (with Ultrasonography, CT, or MRI) that enable the discrimination of schwannomas from other soft tissue tumors (fibrosarcoma or liposarcoma) and benign forms from malignant ones11. Schwannomas can frequently be misdiagnosed as psoas abscesses, pancreatic cysts, neoplasms, adnexal masses, adrenal, kidney or hepatic tumors, as reported in the literature12, 13, 14. Yet, radiological imaging is helpful in therapeutic planning, as it gives information about the tumor’s size, location, and possible invasion of other structures. Fine-needle aspiration biopsy may theoretically be useful if Schwann cells are found in the sample, but the tissue specimen collected for diagnosis is often inadequate and may be misleading because of cellular pleomorphism in degenerated areas which might be interpreted as consistent with malignancy15.
Hughes MJ et al11, in their largest radiological series of abdominal or pelvic schwannomas, showed that a smooth well defined border, ovoid or spherical shape and location in the pre sacral region or lower retro peritoneum at the pelvic brim, are frequent findings in primary abdominal or pelvic schwannomas ; 11 of 13 cases showed all these features. Evidence of degeneration was common, with 8 schwannomas showing cystic change and 3 showing areas of calcification. The cystic schwannomas tended to be larger, with a mean diameter of 10.5cm.
It is difficult to make an accurate pre operative diagnosis. The treatment depends solely on surgery. Malignant schwannomas are insensitive to chemotherapy and radiation, resulting in poor prognosis16.
Conclusion
Schwannoma is a benign encapsulating neoplasm with an overall low incidence, occurring mostly in the head, neck and trunk regions. Giant schwannoma is rarely located in the retroperitoneum, the pelvis and rarer in the mesorectum.
Schwannomas pose a difficult diagnostic challenge. Radiological findings are often non-specific. Ultrasonography can differentiate between solid and cystic tumours. CT can be helpful in determining the size, location, local involvement and distant spread. MRI provides similarly useful information as CT, but yields better visualization of the tumour. FNAC is not often helpful because the tissue architectural information required is not obtainable from cytological specimen. The only gold standard diagnostic investigation is histology of either biopsy or excised specimen.
Surgical excision has remained the mainstay of treatment. Although benign, large and incompletely excised lesions are capable of recurrence, malignant change is exceedingly rare.
Inadvertent carotid arterial puncture complication is reported to have an incidence of 2% - 8% 1, 2 and usually results in localised haematoma formation.
Case presentation
We present a case of a 72 year old man with acute on chronic renal failure referred for intensive care (ITU) management. History revealed dehydration and anuria for 3 days. His blood pressure was 80/40, sinus tachycardia around 130/min with cold clammy peripheries. Blood investigations revealed urea 23mmol, creatinine 800mmol, and potassium-7.7, with ECG changes of hyperkalemia. We attempted a right internal jugular (IJV) venous cannulation using landmark technique and inserted an Arrow-Howes central venous catheter with blue flexi tip, 8.5FR, 5 lumen, and 16cm length. The technique was difficult due to low blood pressure, and patient’s inability to lie flat. The ultrasound machine was unavailable at that moment.Soon after the catheter was introduced using seldinger technique, a swelling was noticed from the site of IJV cannulation .the blood sample analysis revealed arterial blood. The catheter was removed and pressure applied for 45 minutes. Thereafter, a left femoral vein catheter was inserted for central venous access and right femoral vascath –VYGON, DUALYSE Expert, 2 lumen catheter set, 12 fr, 20cm was inserted uneventfully.1 hour later the bleeding from the right carotid puncture site was examined and was found to have ceased. The patient was put on the continuous veno- venous haemofiltration (CVVHF), which clotted after 15minutes.Heparin was used as an anticoagulant for the filter. This was repeated thrice with same result. Three hours later, a haematoma was noticed in area of IJV puncture, which was gradually increasing in size. The haematoma spread to the neck and chest after which the patient complained of discomfort with breathing difficulty. In view of increasing airway compromise the patient was transferred to theatre for elective intubation and surgical intervention. Ultrasonongraphy by radiology consultant showed a large haematoma, but unable to see the damage in the vessel and a CT neck, thorax angiography was suggested. CT angiogram revealed a leak in the bifurcation of the carotid artery. Surgical access was difficult in view of the large persistent leak. Ultrasound probe was used to make the incision superficial to the leak. A small leak was identified in the artery, which was sutured uneventfully. He was then continued on CVVHF with no further complications Discussion Complications include arterial puncture, pneumothorax, neck or mediastinal haematoma and hemothorax3, 4. The haematoma may enlarge rapidly if the patient is coagulopathic, or if a large puncture wound is produced by the introduction of the sheath itself into the carotid artery. Airway obstruction 5, 6, pseudo aneurysm 7, 8, arterio-venous fistula formation 9 and retrograde aortic dissection 10 have all been reported as a consequence of carotid puncture. In the presence of occlusive (atheromatous) carotid disease, inadvertent puncture may carry the risk of precipitating a cerebrovascular accident 11. NICE guidelines 2002 recommended use of ultrasound for central venous cannulation12. The Royal College of Radiology (RCOR) recommends practical training in vascular ultrasound should involve at least two ultrasound lists per week over less than three months up to 6 months. Meta-analysis including 18 Randomised Controlled Trials by NICE concluded that ultrasonongraphic (USG) venous catheterisation was more effective than landmark technique for all outcomes 13 Royal College Of Anaesthetists feels guidance is fair and sensible but landmark technique is still acceptable alternative whether 2D available or not. Conclusion Complications following central venous cannulation are reduced if the procedure is USG guided and therefore must be used whenever possible. But landmark technique is still an acceptable alternative.
We describe a case of a 32 year old primigravida with type III Klippel-Feil Syndrome for an elective Caesarean section. A preanaesthetic assessment at 32nd week of pregnancy revealed a history of mild asthma for which the patient was on regular salbutamol inhaler. She had no history of cardiovascular or respiratory insufficiency. There was no significant family history. Anaesthetic history included a repair of encephalomyelocele immediately after birth and a squint correction surgery at the age of 6 years under general anaesthesia which was uneventful.
Examination revealed a woman of small stature, 137 cm in height and weighing 52 kg. Airway examination revealed Mallampati III with a normal mouth opening, a reduced thyromental distance (3 cm) and inability to flex or extend the neck (Figure 1). She had thoraco-lumbar kyphoscoliosis and examination of the respiratory and cardiovascular system was unremarkable. Electrocardiogram was within normal limits as were haemoglobin, urea and electrolyte estimation. Radiography revealed fusion of atlanto-axial joint (flexion and extension views, Figure 2 ) and also fusion of lumbar vertebrae with associated scoliosis (Figure 3Cobb’s angle 25 degree) and Cobb’s angle 25 degree Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.
Chest radiographs are one of the most common radiological procedures performed in medical practice. The chest radiograph should ideally include views of the heart, lungs, trachea, mediastinum, bones of the chest and upper part of the abdomen. Chest radiographs are normally taken in the posterior-anterior (PA) view with the patient in upright / standing position but for patients admitted in the intensive care unit (ICU) or other emergency situations, this is not possible and so they are taken in the supine (anterior-posterior views) or semi-erect position.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In this article, we aim to discuss and compare the normal and abnormal positions of central venous catheter (CVC) on chest radiographs.
Indications for Central Venous Catheter (Internal Jugular Vein Cannulation)
There are many indications for central venous cannulation 1. These include:
Central venous pressure (CVP) monitoring
Pulmonary artery catheterisation and monitoring
Transvenous cardiac pacing
Administration of drugs (vasoactive drugs, chemotherapy etc)
Aspiration of air emboli
Administration of fluids (in case of difficult peripheral venous access)
Confirming the position of the central venous catheter tip:
For accurate CVP measurement, the tip of the central venous catheter (CVC) should lie within the superior vein cava (SVC), above its junction with the right atrium and parallel to the vessel walls 1. After insertion of a CVC, the position of the catheter tip must be confirmed radiologically, as catheter tips located within the heart can cause cardiac perforation and tamponade 1. Hence, optimum positioning of the CVC tip is required to prevent complications.
If the CVC tip is situated high up (above the pericardial reflection), this can cause vessel wall erosion and if they are very low (in the right atrium), they can cause arrhythmias, placement in the coronary sinus and damage to the tricuspid valve 2.
The carina is a useful radiological landmark for CVC tip position. In this edition of pictorial essay, we aim to discuss the optimum position of both the right and left sided IJV cannula on chest radiographs.
Fig: 1 (CR-1819) shows the normal position of a right sided IJV catheter. The tip of the right sided IJV cannula should ideally lie just above the level of the carina 2. This is the junction of the left and right innominate veins with the superior vena cava (SVC).
Fig: 2 (CR-1829): The optimum position of the left sided IJV cannula is at or just below the level of the carina 2. This radiograph shows the comparison between the right and left sided IJV cannula in the same patient.
The right sided IJV cannula is too low (below the level of the carina) and is probably in the right atrium while the tip of the left sided IJV cannula is optimally placed.
Fig: 3 (CR-1832): In this radiograph, the right sided IJV cannula is too high in the neck. This will not give an accurate CVP measurement. Besides, there is also a risk that the CVC might get dislodged and lead to extravasation of administered fluids and drugs.
Seldinger technique for CVC insertions:
The CVC’s are usually inserted using the Seldinger technique. The IJV can be located by using anatomical landmarks or under direct vision with the help of an ultrasound machine. In the Seldinger technique, after puncture of the IJV, a thin J-shaped guide wire is introduced through the puncture needle. The needle is then slowly withdrawn leaving the J-shaped guide wire in place. A dilator is then introduced over the guide wire to dilate the skin and the subcutaneous tissue. Next, the dilator is removed and the CVC is introduced over the guide wire. Finally, it is important that the guide wire is removed and the CVC is secured.
Fig: 4 (CR-1831). This chest radiograph shows an unusual complication where the guide wire has been left accidentally in situ on the right side. (Note the presence of the J-shaped guide wire on the right side of the neck). This can result in serious complications if the guide wire migrates distally.
Conclusion:
In this article, we have highlighted the optimum placement of central venous catheters on chest radiographs. It is imperative that after every CVC insertion (via the IJV or subclavian vein), the position of the tip be confirmed radiologically and if any re-positioning is required, it must be done. The above discussion is true for even CVC’s inserted through the subclavian veins.
Self Assessment MCQ:
The tip of the right sided IJV cannula should be located a. below the level of the carina b. at the level of the clavicle c. just above the level of the carina d. in the right atrium
Answer: c
ACKNOWLEDGEMENTS We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs. COMPETING INTERESTS None Declared AUTHOR DETAILS DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Bedford Hospital NHS Trust, UK DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Bedford Hospital, Bedford, UK Email: drkrishnanmr@gmail.com
References
Mark JB, Slaughter TF and Gerald Reves J. Cardiovascular monitoring. In: Miller RD ed. Anesthesia. 5th edition. Churchill Livingstone; 1144-51.
Stonelake PA and Bodenham AR. The carina as a radiological landmark for central venous catheter tip position. British Journal of Anaesthesia 2006; 96: 335-340
The incidence of caesarean section is rising1 and there is evidence that women who have a caesarean section may be at increased risk of complications in a subsequent pregnancy2. Compared with vaginal delivery in the first pregnancy, caesarean section has been found to be associated with significantly increased rates of: uterine rupture in labour;3 placenta previa and placental abruption;4 placenta previa leading to peri-partum hysterectomy;5 stillbirth;6 and perinatal death7. Sometimes some unusual complication develops with which, we are not familiar. Here an uncommon complication following caesarean section in a post caesarean pregnancy has been reported.
Case report
A 25 years old lady P 1+4 presented at the emergency department of NRS Medical College & Hospital, Kolkata as an unbooked sixth gravida with the complaint of leaking per vagina for last 4 hours and the period of amenorrhoea was 38weeks. Her past obstetric history revealed that she had caesarean section 4 years earlier (indication of caesarean section was not known to the patient) and 4 successive M.T.Ps, the last being done 1 year back. The baby was alive. The couple wanted ligation operation.
On examination, she was mildly anaemic. Pulse was 88/min and BP was 126/80 mm Hg. She was free of any medical or surgical complications like morbid obesity, COPD and umbilical hernia. Per abdominal finding revealed a term size uterus with cephalic presentation and average liquor. FHS was 144/min and regular. Her previous caesarean section scar was low transverse and there was no scar tenderness.
Per speculum examination showed dribbling of clear liquor. Vaginal examination revealed cervix was 1.5 cm dilated, tubular, station was high up (-3) and membranes were absent.
An emergency L.S.C.S. was performed under spinal anesthesia. The skin incision was Pfannenstiel with excision of the previous scar. On opening the abdomen, uterus was found to be adherent with anterior abdominal wall from which uterus was separated for delivery of the baby (a living male baby of 2.75 Kg) and bilateral tubectomy operation. Bladder was also pulled high up which was dissected and pushed down before opening the uterus. Parietal peritoneum was not closed and rectus sheath was repaired with no 1 chromic catgut. Duration of operation was one hour which was longer than usual operation time of 35 minutes.
First two post operative days were uneventful. On the 3rd day there was a small amount of serosanguinous discharge from the umbilicus. The caesarean section wound, which was located much below the umbilicus, was healthy. Methylene blue dye was introduced into the bladder to rule out any communication with umbilicus, through which no dye came out. On 4th post operative day a mass was seen protruding through the umbilicus and on gentle prodding it seemed to be omentum like structure (Fig-I) A provisional diagnosis of omental hernia through umbilicus was made.
Figure I showing omentum like structure protruding through umbilicus
Figure II showing omental tag held during herniorrhaphy operation
On the 5th post operative day, she underwent herniorrhaphy operation under general anesthesia. A tag of omentum was seen to herniate through anterior rectus sheath and skin (Fig-II). The protruding tag of omentum (sent for histopathological examination and confirmed) was excised and a double breasting of rectus sheath was done, keeping a drain which was removed after 48 hours. Her subsequent recovery was uneventful. She came for check up after 6 weeks, when no abnormality was detected.
Discussion
A review of literature has failed to demonstrate the type of complication mentioned above . Intra operative complication like dense intra abdominal adhesion resulting in injury to the bladder and the bowel is not uncommon8. Probably this case report presents an unusual complication for the first time. Probable explanation is that during too much dissection of anterior rectus sheath (to get access to the fallopian tubes) which was firmly adherent with uterus, there was inadvertent injury to the anterior rectus sheath and skin through which omentum had protruded.
COMPETING INTERESTS None Declared AUTHOR DETAILS CHANDANA DAS, MBBS, MD , Associate Professor ,Gynaecology & Obstetrics , NRS Medical College. SNEHAMAY CHAUDHURI, MBBS, MD, DNB , Assistant Professor, Gynaecology & Obstetrics, NRS Medical College. CORRESPONDENCE: DR SNEHAMAY CHAUDHURI, Sopan Kutir , Flat No 1G, 53 B Dr S C Banerjee Road , Kolkata -700010, West Bengal, India Email: snehamay_chaudhuri_dr@yahoo.com
References
Arjun G Caesarean section: evaluation, guidelines and recommendations Indian Journal of Medical Ethics available at www.ijme.in/163co117.html accessed on 29/09/2008
Taylor MK, Simpson JM, Roberts CL,Olive EC, Handerson- Smart D J Risk of complications in a second pregnancy following caesarean section in the first pregnancy: a population-based study MJA 2005; 183 (10): 515-519
Gregory KD, Korst LM, Cane P, et al. Vaginal birth after cesarean and uterine rupture rates in California. Obstet Gynecol 1999; 94: 985-989.
Lydon-Rochelle M, Holt VL, Easterling TR, Martin D. First-birth cesarean and placental abruption or previa at second birth. Obstet Gynecol 2001; 97: 765-769.
Crane JM, Van den Hof MC, Dodds L, et al. Maternal complications with placenta previa. Am J Perinatol 2000; 17: 101-105.
Smith GCS, Pell JP, Dobbie R. Caesarean section and risk of unexplained stillbirth in subsequent pregnancy. Lancet 2003; 362: 1779-1784.
Smith GCS, Pell JP, Cameron AD, Dobbie R. Risk of perinatal death associated with labour after previous cesarean delivery in uncomplicated term pregnancies. JAMA 2002; 287: 2684-2690
Sobande A, Eskander M. Multiple Repeat Caesarean Sections: Complications and Outcomes. J Obstet Gynaecol Can 2006;28(3):193–197
An 82 year old lady, who had suffered multiple strokes in the past and was currently on long term percutaneous endoscopic gastrostomy( PEG) feeding, was admitted as an emergency from a nursing home with a two week history of productive cough and fever. She had been on PEG feeding since her first stroke six years previously. The first PEG tube (placed in 2001) subsequently fell out of position, and a second tube (15 French Frecka PEG tube) was inserted in 2003.
On admission, she was pyrexial, dehydrated, and hypoxic on room air. Chest examination revealed bilateral crackles and neurological examination revealed expressive dysphasia, and spastic weakness in both lower limbs. Abdominal examination revealed an inflamed PEG site with purulent discharge. Blood tests revealed raised inflammatory markers with neutrophilia (WBC 20 x 109 /L with a neutrophil count of 12 x 109/L) and a raised C-reactive protein at 193 mg/L.
She was managed with intravenous fluids and antimicrobial therapy (tazocin and metronidazole) for possible aspiration pneumonia. Vancomycin was subsequently commenced as methicillin resistant staphylococcus aureus (MRSA) was isolated from the PEG site. As she remained stable, PEG feeding was recommenced.
A week following her admission she became unwell with an episode of vomiting and choking following PEG feeding. This was associated with difficulty in infusing feeds and medications through the PEG tube. Multiple flushes through the tube were unsuccessful. The tube was found to be persistently blocked and lacked free mobility within the tract.
Urgent upper gastro intestinal endoscopy revealed a buried bumper as the cause of blockage of the PEG tube. This necessitated insertion of a new PEG tube (9 French Frecka) for enteral feeding. The old PEG tube was removed surgically under local anaesthesia in due course. As the removal of the buried bumper was found to be very difficult endoscopically, and surgical intervention was deemed to be inadvisable in view of co morbidities, the bumper was left in situ. Feeding was recommenced through a new tube. In view of persistent discharge through the PEG site, abdominal ultrasound examination was performed, revealing a possible gastro-cutaneous fistula. No local collection was seen around the PEG wound.
As the patient remained clinically stable, she was discharged home with necessary instructions to her carers for regular flushing of the PEG tube with water, before and after each feed, to prevent further blockages.
Fig 1: Buried bumper (stomach-lower body)
Fig 2: New peg and buried bumper
Discussion
PEG is primarily used for long term (longer than 6 weeks) enteral alimentation for patients with impaired swallowing (e.g. from stroke, degenerative neurological disease, head injury, and oropharyngeal malignancy). However numerous complications have been reported since its introduction in 1980.
Buried bumper syndrome (BBS) is an uncommon but well documented complication of PEG insertion, first described in 1988 1. It is usually a late complication occurring up to 3 years post PEG insertion and reported to occur in 0.3-2.4 % of patients2.
The internal bumper of the PEG tube should normally sit snugly against the anterior gastric wall, and this is confirmed endoscopically at the time of initial placement. BBS develops when there is migration of the internal bumper/flange through or into the anterior abdominal wall. This probably occurs as a result of excessive tension between the internal and external bumpers, from over-tightening of the external flange, leading to gastric wall erosion. During migration it becomes lodged along the gastrostomy tube tract between the gastric and abdominal walls. Once epithelialisation occurs the bumper gets covered with gastric mucosa3.
The diagnosis of BBS should be suspected if localised abdominal pain, peri-tubal leakage or inability to infuse feed occurs. Initial measures to deal with a blocked tube include flushing with warmed water, and occasionally passage of a flexible wire through the lumen, in order to unblock any obstruction. Tube obstruction is usually related to the administration of protein-enriched formulae or medications, especially if the tube size is 9 French. Fungal colonisation may also lead to tube blockage, requiring specific solutions for flushing the tube4. Tube exchange should only be considered if the gastrocutaneous tract is mature (6 weeks or longer after placement of the tube).
Endoscopy is confirmatory in cases of BBS. The internal bumper is not seen, and the site of the PEG is indicated by an elevated area of submucosa with a central depression. Failure to recognise BBS can result in gastric perforation and gastrointestinal haemorrhage or intra abdominal sepsis, peritonitis and even death5.
Ideally, the buried bumper should be removed even if the patient is asymptomatic, to avoid potential complications from continued tube migration until it is completely impacted in the abdominal wall. The literature describes various methods of dealing with this complication. Endoscopic ultrasound of the gastric wall with a catheter US probe can facilitate the localisation of the bumper and also provides information regarding feasibility of surgical or endoscopic removal of PEG tube6.
Regular and optimal PEG care has been vital in identifying and prevention of this complication. During daily cleaning of the external PEG site, the PEG should be pushed in approximately 1 cm and rotated prior to repositioning of the external bumper. The length of the tube outside the abdominal wall should be examined at regular intervals so that migration can be recognised5.
This report reinforces the fact that physicians should be aware of this recognised risk of PEG feeding and prompt referral for endoscopy is necessary to avoid serious consequences including gastro-intestinal bleeding, peritonitis and death. Similarly specific instructions should be given to carers for prevention of BBS.
COMPETING INTERESTS None Declared AUTHOR DETAILS VIJAY JOSHI, Trust registrar in integrated medicine, Chase Farm Hospital, Enfield, UK ASHIS BANERJEE, Consultant in emergency medicine, Chase Farm Hospital, Enfield, UK CORRESPONDENCE: MR ASHIS BANERJEE, Consultant/honorary senior lecturer in emergency medicine, Chase Farm Hospital, The Ridgeway, Enfield EN2 8JL United Kingdom E-mail: libra19542003@yahoo.co.uk
References
Shallman RW, Norfleet RG, Hardache JM. Percutaneous endoscopic gastrostomy feeding tube migration and impaction in the abdominal wall. Gastrointest Endosc 1988; 34: 367–68.
Venu RP, Brown RD. Pastika BJ Erickson LW. The buried bumper syndrome: a simple management approach in two patients. Gastrointest Endosc 2002; 56: 582–84.
Anagnostopoulos GK, Kostopoulos P, Arvanitidis DM. Buried Bumper Syndrome with a fatal outcome, presenting early as gastrointestinal bleeding after percutaneous endoscopic gastrostomy placement. J Postgrad Med 2003; 49:325–27
Iber, FL, Lusak, A, Patel, M Importance of fungus colonization in failure of silicone rubber percutaneous gastrostomy tubes (PEGs) Dig Dis Sci, 1996, 41: 226-231
Braden B, Brandstaetter M, Caspary WF, Seifert H. Buried bumper syndrome: treatment guided by catheter probe US. Gastrointest Endosc 2003;57:747-51
Ma MM, Semalacher EA, Fedorak RN, Llor EA, Duerksen DR et al The buried gastrostomy bumper syndrome: prevention and endoscopic approaches to removal. Gastrointest Endosc 1995 ; 41:505-8
The acquired immunodeficiency syndrome (AIDS) was first recognized among homosexual men in the United States in 19811,2. While initially limited, infection with the human immunodeficiency virus (HIV) has immensely increased over the past two decades to become the biggest epidemic of the twentieth century. However, we have witnessed dramatic improvement in prevention of disease progression and long-term survival in the era of Highly Active Anti Retroviral Therapy (HAART).
Apart from biological factors associated with the virus and host which play a role in the transmission and progression of HIV infection, several demographic and social variables have been studied and described in different studies worldwide. Understanding the variety of non-biological factors and behavioral patterns which can affect care and prognosis of HIV patients gives us the opportunity to design non-pharmacological interventions and where possible, to facilitate better care for our HIV positive population.
BACKGROUND:
J.E. Wood clinic of Pennsylvania Hospital in Philadelphia is a teaching outpatient care facility where Internal Medicine residents of Pennsylvania Hospital acquire their ambulatory care experience under supervision of teaching attendings. We have once a week clinic sessions dedicated to the care and follow-up of HIV/AIDS patients under close supervision of Infectious Disease specialists. Our patients have diverse socio-economic, educational and stages of HIV infection.
OBJECTIVE:
We aimed at finding out basic understanding of HIV infection, degree of awareness regarding the ongoing treatment and reasons behind irregular follow-up visits of our HIV patients who attend J.E. Wood outpatient clinic of Pennsylvania Hospital, Philadelphia for treatment of HIV/AIDS.
PARTICIPANTS AND METHODS:
In order to collect relevant information from our patients, a two paged, anonymous, study questionnaire was given to all patients who attended the clinic during January 2007 to December 2007. The questionnaire looked into three different areas of patient related factors which can influence the disease outcome: demographic and social information (Age, Sex, level of education), patients’ knowledge about their HIV disease (source of the infection, duration of HAART, individual recent CD4 count, names of current medications, duration of therapy, medication side-effects) and their behavior (sexual precautions, reasons for medication and follow-up non-compliance). Out of the 75 patients who were given the questionnaire, 7 questionnaires were rejected from the study because of the information received was incomplete, illegible or not related to the questions. 68 completed questionnaires were evaluated and comparative data was tallied using Microsoft excel sheet. We also reviewed relevant literature in pubmed to understand our findings in the light of previous studies related to demographic, socio-economic and psychological aspects of HIV treatment.
RESULTS:
We analyzed the information which was obtained from 68 patients by means of the questionnaire. Our patients consisted of 35 male, 33 female (Table 1). We had a wide range of patients regarding distribution of their age as shown in Table 2 below. Significant numbers of our patients (36%) were diagnosed with HIV for >10 years ago and more than 60% had the diagnosis at least for 5 years (Table 3)
Table 1: Socio-demographic characteristics of patients (n=68)
Variables
Percentage
Gender
Male
51.5%
Female
48.5%
Education
<High school
34%
High school graduate
50%
>High school
16%
Table 2: Age distribution of patients (n=68)
Age group
Percentage
Upto 30 years
19%
31 to 40 years
22%
41 to 50 years
37%
51 to 60 years
18%
61 years and above
4%
Table 3: Duration of diagnosis (in years)
Duration of
diagnosis (years)
Percentage of
total patients (n=68)
Unknown
3%
< 5
36%
>5 to 10
25%
>10
36%
Half of our patients (n= 68) completed high school education or equivalent. About 34% quit education before attaining high school diploma. Roughly, 10% of our patients went to college for further education and 6% acquired some vocational training after high school.
We tried to establish the level of our patients’ participation in their treatment by gathering information through the questionnaire whether they could recall the names of their HIV medicines and the last CD4 count. We found that 74% of our patients, who are on HIV medicines, could recall the names of their medicines but only about 45% of our patients remembered their last CD4 count. Our patients who had completed high school education or equivalent were 2.5 times more likely to remember the names of their HIV medications(95 % confidence interval CI=1.42 to 4.98) and 1.75 times more likely to remember their last CD4 count(95 % confidence interval CI=1.12 to 4.38).
We asked our patients whether they knew that HIV medications need to be taken life long and we also enquired about their knowledge about their safe sexual practices. Only 48% patients of our study group knew that HIV medicines are for life. About 50% of all our patients mentioned that they ensure use of condom during sexual activity and another 40% claimed they practice sexual abstinence. Women patients in our practice were 2.0 times more likely to practice use protective measures during sexual activity (95 % confidence interval CI=1.22 to 4.67).
In our study, only 32 patients (47%) attempted to answer the question where we asked about reason behind not turning up for their follow up appointments as scheduled. Eight patients could not specify a cause, 7 mentioned transport related problems and 2 had insurance issues. Five patients thought their appointments were too often whereas 3 just forget to keep the appointment. Although we did not specifically ask questions on psychological state of our patients, 7 out of the 32 patients mentioned significant psychological problems in their daily life as the reason for non-adherence to medication or follow-up appointments. The responses included responses like “still dealing with the diagnosis mentally”, “feel lack of energy in life”, “life seems to have too many problems”, “been drinking heavy lately” etc.
DISCUSSION:
Interestingly, our small patient cohort roughly reflects the sex ratio of HIV patients globally in 2007 as published by World Health Organization (WHO). In our study the ratio was Male : Female = 51.5% : 48.5% and in the WHO worldwide survey it was 50% : 50%; At the end of 2007, estimated total global HIV positive adults = 33 million (30million – 36 million) 3.
Rates of progression of HIV disease appear to be similar by sex and race category if adjusted for the quality of care 4, 5. Multiple studies on chronic disease management showed that patients’ level of education and health literacy has direct influence on the treatment compliance. Moreover, limited health literacy is thought to be a strong contributing factor to racial disparities in health care. A study was published in 2007 which examined the mediating effect of limited health literacy on the relationship between race and HIV-medication adherence. For the study, a total of 204 patients infected with HIV were recruited and structured in-person interviews were conducted to obtain information. In an adjusted analysis that excluded literacy, African Americans were 2.40 times more likely to be non-adherent to their HIV-medication regimen than whites (95% confidence interval [CI]=1.14-5.08). When literacy was included in the final model, the effect estimates of race diminished from 25% to insignificant level. Therefore, health care providers need to consider the potential utility of responding to literacy and communication barriers in health care as part of interventions to reduce racial disparities 6. In our study, we found that patients who had completed high school education or equivalent were more conscientious regarding their HIV care as demonstrated by the fact that they were more likely to remember their last CD4 count and current HIV medications.
Multiple studies have demonstrated that increasing age at the time of HIV infection is associated with more rapid progression to AIDS in the absence of antiretroviral therapy. In one series, for example, the median time from seroconversion to AIDS without therapy was 15 years for patients aged 16 to 24 years at seroconversion, compared to 6 years for those 35 years or older at seroconversion 7. In our study, it is notable that 36% of patients were diagnosed with HIV >10 years ago and more than 60% had the diagnosis at least for 5 years. The reason behind the high survival rate is clearly attributable to HAART. Fifty-four patients out of the 68 are currently on HAART and 25 of them are on it for more than last 5 years.
Patients' knowledge of their HIV condition and its treatment has been recognized as a factor that influences adherence to antiretroviral therapy. Patients’ knowledge & perception of the disease and participation in the treatment can be improved through targeted educational programs and support groups. One study done in Nigeria found that individuals living with HIV/AIDS who belonged to a support group and had availed themselves of relevant literature were more knowledgeable and positive about their illness than those who did not belong to support groups. The study concluded that HIV/AIDS support group membership is an important component of psycho-social care in HIV/AIDS patients 8. Another study done in France showed that an educational intervention improves adherence to antiretroviral regimens and health status and suggests that it should be initiated early in therapy 9. Communicating with patients about adherence issues is important issue, although this may not have an immediate impact on patients' behaviors. Health care professionals should play a pro-active role in this regard. The use of multi-disciplinary adherence teams to ensure that each HIV-positive patient receives the optimal amount of information and support for adherence is a practical approach. Health literacy should be provided in the context of different ethnicity, culturally sensitivity and individual needs associated with HIV, like any other chronic diseases. Epidemiological researches have shown that injection drug abusers and younger patients tend to have worse compliance, as well as subjects with depression and lack of self-perceived social support 10. Therefore, special care should be taken by health care providers to ensure treatment compliance and health literacy in these patients. In our J.E. Wood clinic, we have dedicated psychologist and social worker to for care of our HIV patients.
Psychological impact associated with treatment of any chronic illness is often neglected in clinical practice but indeed carries a huge significance in terms of long-term treatment compliance and outcome. We identified 7 of our patients who clearly expressed psychological issues related to their HIV infection and it was evident enough that those psychological problems were adversely affecting their treatment compliance. Formal and regular counseling sessions should be arranged for HIV/AIDS patients to promptly identify and manage any psychological or psychiatric disturbance that HIV patients might suffer from. We know that presence of a preexisting psychiatric disorder can increase the risk of HIV acquisition and can also complicate HIV treatment. Moreover, HIV infection can produce a number of psychiatric conditions and exacerbate many others; there is an intense co-morbidity and linkage between HIV and various types of psychiatric conditions. Personality disorders are more prevalent among HIV-infected (19 to 36 percent) and HIV at-risk (15 to 20 percent) individuals 11, 12 than the general population (10 percent). Antisocial personality disorder (ASPD) is the most common personality disorder among HIV infected individuals, and has been shown to significantly increase risk of HIV infection 13. Successful treatment can be achieved with even the most difficult patients by applying a comprehensive diagnostic formulation that includes psychiatric disease syndromes such as major depression, personality vulnerabilities, behavioral disorders such as addiction, and problems of life experiences such as trauma. With regards to anti-retroviral treatment of HIV positive or AIDS patients, nearly perfect compliance seems to be indispensable to obtain the maximum benefit from HAART. There is a clear relation between high adherence levels and virologic success. We reviewed relevant published literatures to understand the adverse effects and possible interventions of psychological problems in HIV patients. A prospective, randomized, two-arm controlled study was published in 2000 which included 116 patients starting their first-or second-line HAART who were randomized to receive psychoeducative intervention to implement adherence (experimental group [EG]) or a usual medical follow-up (control group [CG]). The study showed that specific and maintained psychoeducative interventions based on excellence on clinical practice are useful to keep high levels of adherence and therefore, high levels of viral suppression 14.
CONCLUSION:
Human Immunodeficiency Virus infection is one of the most serious disease entities in our modern time. We have witnessed dramatic improvement of long-term survival rate of HIV positive patients due to use of HAART in clinical practice. By identifying the demographic, socio-economic, behavioral and psychological variables which significantly influence patients’ adherence to treatment and understanding of the disease process, we can further improve treatment compliance and the long term prognosis of our HIV patients. These factors may not have very significant role individually, but collectively can dictate the course of success of HAART treatment in patients. Increasing awareness of these factors by practitioners caring for HIV-infected persons, recognizing and potentially treating some of them, should indirectly improve the effectiveness of antiretroviral therapy.
COMPETING INTERESTS None Declared AUTHOR DETAILS SUBHASISH BOSE, M.B.B.S., M.R.C.P, PGY1 in Internal Medicine, Pennsylvania Hospital, Philadelphia, USA. AJAY VARANASI, M.B.B.S.; PGY3 in Internal Medicine, Pennsylvania Hospital, Philadelphia, USA. GYI MO, M.B.B.S., M.P.H.; Director of J.E. Wood clinic, Pennsylvania Hospital, Philadelphia, USA. CORRESPONDENCE: DR SUBHASISH BOSE, Apartment 601, 269 South Ninth Street, Philadelphia, PA-19107, USA. Email: kumub@yahoo.com
Kaposi's sarcoma and Pneumocystis pneumonia among homosexual men--New York City and California. MMWR Morb Mortal Wkly Rep 1981; 30:305.
Status of the global HIV epidemic. http://data.unaids.org/pub/GlobalReport/2008/jc1510_2008_global_report_pp29_62_en.pdf. Accessed January 31, 2009.
Collaborative Group on AIDS Incubation and HIV Survival including the CASCADE EU Concerted Action. Time from HIV-1 seroconversion to AIDS and death before widespread use of highly-active antiretroviral therapy: a collaborative re-analysis. Lancet. 2000 Apr 1; 355(9210):1131-7.
Altisent, C, Montoro, JB, Ruiz, I, Lorenzo, JI. Long-term survivors and progression of human immunodeficiency virus infection. N Engl J Med 1996; 334:1065.
Osborn CY, Paasche-Orlow MK, Davis TC, Wolf MS. Health literacy: an overlooked factor in understanding HIV health disparities. Am J Prev Med. 2007 Nov; 33(5):374-8.
Mariotto, AB, Mariotti, S, Pezzotti, P, et al. Estimation of the acquired immunodeficiency syndrome incubation period in intravenous drug users. Am J Epidemiol 1992; 135():428.
Olley BO. The role of support group and duration of infection in HIV/AIDS patients' knowledge and attitudes to their illness. Afr J Med Med Sci. 2007 Mar; 36(1):11-6.
Goujard C, Bernard N, Sohier N, Peyramond D, Lançon F, Chwalow J, Arnould B, Delfraissy JF. Impact of a patient education program on adherence to HIV medication: a randomized clinical trial. J Acquir Immune Defic Syndr. 2003 Oct 1; 34(2):191-4.
Gordillo V, del Amo J, Soriano V, González-Lahoz J. Sociodemographic and psychological variables influencing adherence to antiretroviral therapy. AIDS. 1999 Sep 10; 13(13):1763-9.
Sher, KJ, Trull, TJ. Substance use disorder and personality disorder. Curr Psychiatry Rep 2002; 4:25.
Jacobsberg, L, Frances, A, Perry, S. Axis II diagnoses among volunteers for HIV testing and counseling. Am J Psychiatry. 1995; 152:1222.
Perkins, DO, Davidson, EJ, Leserman, J, et al. Personality disorder in patients infected with HIV: a controlled study with implications for clinical care. Am J Psychiatry. 1993; 150:309.
Tuldrà A, Fumaz CR, Ferrer MJ, Bayés R, Arnó A, Balagué M, Bonjoch A, Jou A, Negredo E, Paredes R, Ruiz L, Romeu J, Sirera G, Tural C, Burger D, Clotet B. Prospective randomized two-Arm controlled study to determine the efficacy of a specific intervention to improve long-term adherence to highly active antiretroviral therapy. J Acquired Immune Deficiency Syndrome. 2000; 25(3):221-8.
The significance of disturbed subjective sleep quality in the general population is important because of high prevalence rates (of up to 30%)1 and the association with decreased quality of life.2 Poor sleep affects cognitive and physical functioning, and insomnia is associated with a greater risk of falls and accidents,3 higher rates of absenteeism4 and increased health care utilization.4
Insomnia is commonly encountered in primary and secondary care settings, and can be symptomatic of many medical, neurological, substance abuse or primary sleep disorders.
Epidemiological and clinic-based studies consistently demonstrate high rates of psychiatric comorbidity.5,6 Sleep disturbance is an important clinical construct in psychiatry. It represents formal diagnostic criterion in mental illnesses such as affective and anxiety disorders.7,8
Insomnia is broadly defined as the subjective experience of poor or unrefreshing sleep, with some objective evidence of reduced time asleep or delayed sleep-onset. The subjective nature of such complaints remains key, because sleeping is a private event, and there is often no informant history. Furthermore, it is the perceptual aspects of sleep that influence patients’ help-seeking behaviour, such as consultation requests, demands for night sedation, and medication and substance use. It is noteworthy that despite the wide-ranging implications and subjectively distressing nature of this phenomenon, it remains arguably one of the least satisfying symptoms to treat. Seeking a better understanding of the extent and nature of patients’ sleep perception can help optimise appropriate therapeutic strategies.
This is the first study assessing the subjective sleep quality of a sample of psychiatric disordered in-patients in a UK psychiatric hospital setting, using the Pittsburgh Sleep Quality Index (PSQI).9 This study is framed in the context of increasing the awareness of the significance of patients’ complaints of insomnia and addressing the wider psychosocial issues that this raises.
Method
Design: This was a cross-sectional survey of the self-reported quality of sleep in a population of psychiatric in-patients on the acute adult wards of a London psychiatric hospital.
Participants and Procedure:Participants consisted of psychiatric in-patients (ages 18-65) on all five of the acute adult open psychiatric wards of the Highgate Mental Health Centre, London, currently admitted for the assessment or treatment of mental illness. Financial compensation was not provided for any subject.
Subjects were approached on the ward by a member of nursing staff and asked if they were interested in participating in a study about sleep. The researcher was then introduced to explain further details with the aid of the participant information sheet. After a minimum of 24 hours, patients were approached again by the researcher and asked if they were willing to participate. Recruitment of subjects took place if the patient was agreeable to take part and did not meet any of the exclusion criteria (listed below). A scheduled time and date was made with participants in order to obtain written informed consent and to administer the questionnaire. Questionnaire data was collected from each subject by the researcher in a private interview room located on the patient’s psychiatric ward. Demographic and clinical data required from the patient’s medical notes was recorded on the day of sampling. Exclusion criteria were: the presence of severely disturbed behaviour, or having received rapid tranquilisation for such behaviour on the day of sampling; a significant impairment in physical condition (e.g. infection, trauma); a history of a sleep disorder (e.g. obstructive sleep apnoea); the presence of organic illness including dementia; and lack of capacity to give informed consent.
Quality of Sleep:Subjects' quality of sleep was assessed by the administration of the Pittsburgh Sleep Quality Index (PSQI).9 This is one of the most widely used questionnaires employing standardised measures to assess subjective sleep quality in clinical and research settings. It assesses sleep quality and disturbances over a 1-month time interval. 19 individual items are used to generate 7 component scores (with a range of possible subscale scores from 0 to 3): 1) overall subjective sleep quality; 2) sleep latency; 3) sleep duration; 4) habitual sleep efficiency; 5) sleep disturbances 6) use of hypnotic or sedative medication; 7) daytime dysfunction. Higher scores indicate greater sleep disturbances. The sum of the component scores yields a global score (ranging from 0 to 21), which was used as the primary outcome measure in this study. A global PSQI score cut off score of 5 discriminates between good and bad sleepers and the PSQI gives acceptable measures of internal homogeneity, consistency (test-retest reliability) and validity.9,10
Other Variables:Demographic and clinical data recorded concurrently from participant's medical notes included: sex (male/female); age (years); ethnicity (Asian/Black/Mixed//Other); body mass index (BMI) (calculated as the ratio between weight [kilograms] and squared height [metres]); primary psychiatric diagnosis (based on ICD-10 criteria); duration of psychiatric illness (years); past medical history; number of currently prescribed medications; length of admission to date (days); current admission status (informal/detained under Section 2 of the Mental Health Act (MHA) (1983) (this is for a maximum period of 28 days for further assessment)/detained under Section 3 MHA (1983) (this is for a maximum period of 6 months for psychiatric treatment). A further category (detained under another type of section) was dropped as this did not apply to any of the subjects.
Ethics Committee Approval:Ethical and research governance authorisations were granted from Camden and Islington Community Local Research Ethics Committee, and from the North Central London Research Consortium, respectively.
Statistical Analysis:The aim was to compare clinical, demographic and PSQI data between the poor sleepers and good sleepers. The prevalence (%) of poor sleep was determined by the proportion of subjects with global PSQI score of 5 or more. Statistical analyses were predominantly performed using the software package Stata, version 9.2.
Results
Sample Characteristics
77 patients were initially identified as potentially eligible subjects. Of these, 31 (40%) were excluded due to: the presence of disturbed behaviour (n=1); inability to give informed consent (n=9); unwillingness to participate (n=19); absence from ward (either on leave or absent without leave) (n=2).
This left a total of 46 patients who were enrolled in to the study. Subject characteristics are given in Table 1. Table 1: Demographic and clinical characteristics of study subjects
Sex, n (%)
Male
24 (52)
Female
22 (48)
Ethnicity, n (%)
Asian
1 (2)
Black
9 (20)
Mixed
1 (2)
Other
1 (2)
White
34 (74)
Current Admission Status, n (%)
Detained under Section 3 MHA
22 (48)
Detained under Section 2 MHA
5 (11)
Informal
19 (41)
Age, years: mean (s.d.)
38 (11.1)
Range
18-62
Body Mass Index, kg/m²: mean (s.d.)
25.99 (4.96)
Range
17.9-41.5
Duration of mental illness, years: mean (s.d.)
10.51 (7.93)
Range
0.17-30
Length of admission, days: mean (s.d.)
42.43 (63.21)
Range
2-366
Prescribed regular medications, mean (s.d.)
1.83 (1.05)
Range
0-5
Medical comorbidities, mean (s.d.)
0.59 (0.98)
Range
0-3
s.d.: standard deviation
As defined by ICD-10 criteria, the most common subdivisions of patients’ psychiatric diagnoses in descending order were: paranoid schizophrenia, F20.0, (n=16); emotionally unstable personality disorder, F60.3, (n=6); depressive disorder, F32, (n=6); bipolar affective disorder, F31 (n=5). Other subdivisions of subjects’ diagnoses included: organic mood disorder, F06.3 (n=1); organic personality disorder, F07, (n=1); residual and late onset psychotic disorder due to alcohol use, F10.7, (n=1); persistent delusional disorder, F22, (n=1); acute and transient psychotic disorder, F23, (n=1); unspecified non-organic psychosis, F29, (n=1); post traumatic stress disorder, F43.1, (n=1). One patient was undergoing psychiatric evaluation and therefore had no formal diagnosis.
Medications prescribed regularly were: antipsychotics (for 40% of the total sample of patients), mood stabilizers (16%), antidepressants (14%) and benzodiazepines (7%). In terms of regular night time sedation, two patients out of a total of 46 were prescribed zopiclone and diazepam respectively. Zopiclone was prescribed on an “as required” basis for 15 patients (33% of the total sample).
Overall sleep quality evaluated by the PSQI revealed a mean score of 9.74 (standard deviation= 5.11). Poor sleep quality (defined as a global PSQI score of 5 or more) was present in 36 out of the total of 46 subjects (78% of the sample).
Comparison between good and poor sleepers
Comparison of numerical measurements between the two sleep groups is presented in Table 2. For the normally distributed variables the figures reported for each group are the mean (standard deviation) and the p-value from the t-test. For the non-normally distributed variables the figures reported are the median (inter-quartile range) and the p-value from the Mann-Whitney test.
Table 2: Comparison of demographic and clinical data between good and poor sleepers.
(*) Median (Inter-quartile range) reported. Analysis performed using Mann-Whitney test
The results indicate that there was no strong evidence of a statistically significant difference between good and poor sleepers for any of the variables examined. However, there was a possible difference for duration of admission, although this result was only of borderline statistical significance (p=0.06). The results indicate a median duration of admission of 44 days for good sleepers and 15 days for poor sleepers.
The difference between sleep groups for the categorical variables was examined using Fisher’s exact test. Results, presented in Table 3, show the number (and percentage) of subjects falling into each category, with the p-value indicating the significance of the results.
Table 3: Comparison of categorical data between good and poor sleepers
Variable
Group
Good sleepers
(total PSQI <5)
N (%)
Poor sleepers
(total PSQI ≥5)
N (%)
P-value
Sex
Female
3 (30%)
19 (53%)
0.29
Male
7 (70%)
17 (47%)
Admission status
Section 3
9 (90%)
18 (50%)
0.01
Section 2
0 (0%)
5 (14%)
Informal
1 (10%)
13 (36%)
Physical
comorbidities
None
7 (70%)
24 (67%)
1.00
1+
3 (30%)
12 (33%)
There was a significant difference between sleep groups with regard to their admission status. Almost all (90%) of the good sleepers were detained under Section 3 MHA (1983), whilst this applied to only half of those in the poor sleepers group. Being detained under Section 2 MHA and informal admission were more commonly found amongst those categorised as poor sleepers.
There was no significant difference between groups in terms of sex or the presence of physical comorbidities.
The final set of analyses compared the differences between groups for the PSQI measures, and the results are summarised in Table 4. The figures reported are the mean (standard deviation) score for each group. For the individual components the Mann-Whitney test was used to compare between groups, and the p-values from this analysis are reported. For the PSQI total score, the unequal variance t-test was used to compare between groups.
Table 4: Comparison of PSQI measures between the good and poor sleepers
Good sleepers
(total PSQI <5)
Mean (SD)
Poor sleepers
(total PSQI ≥5)
Mean (SD)
P-value
PSQI C1 score (quality) (*)
0.2 (0.84)
1.6 (0.9)
<0.001
PSQI C2 score (latency) (*)
0.9 (1.0)
1.8 (1.0)
0.02
PSQI C3 score (duration) (*)
0.1 (0.3)
1.7 (1.3)
0.002
PSQI C4 score (efficiency) (*)
0.1 (0.3)
1.7 (1.3)
0.001
PSQI C5 score (disturbances) (*)
0.7 (0.5)
1.4 (0.6)
0.003
PSQI C6 score (sedatives) (*)
0.4 (1.0)
1.5 (1.4)
0.04
PSQI C7 score (daytime dysfunction) (*)
0.7 (0.9)
2.1 (0.8)
0.004
PSQI total
3.1 (1.3)
11.6 (4.1)
<0.001
(*) Analysis performed using Mann-Whitney test
There was a statistically significant difference between good and poor sleepers for all PSQI components and for the PSQI total. The PSQI component values and PSQI total scores for poor sleepers were significantly higher than for good sleepers.
A profile of the mean PSQI individual component scores between the two groups (good sleepers versus poor sleepers) is displayed in Figure 1.
Figure 1: Mean component PSQI scores of good and bad sleepers Profiles of the PSQI represent group differences of individual component scores. Mann-Whitney test, *p<0.05).
Subjective Patient Comments
The PSQI also comprises an open ended question, providing subjects with the opportunity to cite “other” (subjective) reasons for difficult sleep. The most common response was anxiety (n=8). Other examples included: medication alterations (n=3); environmental noise (n=2); “thinking excessively” (n=1); “a desire to be creative” (n=1); hard mattress (n=1); “food eaten” (n=1); “sedentary lifestyle” (n=1); alcohol (n=1); hunger (n=1); asthma (n=1); symptoms of the menopause (n=1); and “voices”(n=1).
Discussion
Main Results
This is the first study to examine the subjective quality of sleep among a population of psychiatric in-patients in the UK. The prevalence of poor sleep, as defined by a cut off PSQI score of 5 or more, was present in 78% of the patients sampled. Patients detained under Section 3 MHA (1983) were more likely to report sleeping well when compared to informal patients or those detained under section 2 MHA (1983). There was some evidence of good subjective sleep quality being related to a longer duration of admission, but this requires further investigation.
There were no significant differences between good and poor sleepers for any of the other demographic and clinical variables studied, including age, body mass index, duration of psychiatric illness, number of prescribed medications, sex, and physical comorbidities.
Individual PSQI component scores and global scores were significantly lower for good sleepers compared to poor sleepers. This would be expected given that higher scores indicate more severe sleep complaints, and this supports the consistency of the PSQI as a research instrument.
Factors Affecting Sleep
In-patients’ disturbed sleep may be caused by a variety of exogenous factors such as unfamiliar surroundings, environmental noise, bright lighting and staff interactions or monitoring. Physical and psychological factors, such as the side-effects of medication and substance use, may also have a detrimental effect on sleep quality. In the added presence of a psychiatric disorder, each of these factors may act synergistically on the relationship between mental illness and sleep. Despite substantial research supporting the robust associations between insomnia and comorbid conditions, specific mechanisms linking sleep, medical and psychiatric factors have not been well established.
Sleep complaints may represent early symptoms and risk factors for new episodes of mental illness rather than simply representing phenomena secondary to experience of mental illness. For example, longitudinal studies have found insomnia to be a substantial risk factor for the development of a depressive disorder5,11,12 and the risk for developing new anxiety disorders and alcohol abuse is also greater for insomniacs.6
Stepanski & Rybarczyk13 present research arguing against the more traditional conceptualisation of insomnia as simply a consequence of another disorder. They propose the need for a revised model to understand insomnia that is comorbid with medical and/or psychiatric illness. Abnormalities of the hypothalamic-pituitary-adrenal (HPA) axis may represent the underlying pathophysiological process in many chronic insomnia patients.14 This may signify a common risk factor for insomnia and depression, thus predisposing the individual to a vulnerability to both conditions.15
In this study, detained patients (under Section 3 MHA (1983)) were significantly more likely to be classified as good sleepers. A suggestion for this finding could be that these patients may be less resisting of remaining and sleeping on the ward due to the involuntary nature of their admission. Alternatively these patients may represent the group with the most severe mental illnesses and with the least insight, and therefore less able to accurately recall their (poor) sleeping habits over the previous month.
There was also a potential association between longer admission status and better sleep quality. Explanations for this observation might include: patients’ acceptance over time of their admission and the consequent conditioning to, and familiarisation with, the ward environment; achievement of stability in mental state over time; or the adaptation of the perception of sleep quality to the sleep disturbances that accompany mental illness.
Limitations
This study is based on cross-sectional data and the relationship between the course of mental illness and sleep perception cannot be determined. In order to verify the direction of causality, it is necessary to demonstrate longitudinally that improvement in symptom severity is accompanied by an increase in subjective sleep quality.
This study was not designed to look at the prevalence of poor sleep across the different classes of psychiatric illnesses and dual diagnoses were not considered. It did not measure psychopathology or self-reported psychological distress. Possible confounding factors were not taken in to account, such as concurrent use of caffeine, alcohol, nicotine, illicit substances, hypnotics or other medications known to affect sleep.
The PSQI measures sleep quality averaged over the previous month. In cases where patients had only very recently been admitted to hospital, measurements would have been unlikely to accurately reflect the perspective of an in-patient’s experience. The mean length of admission for this population however was longer than one month (42 days).
These results were drawn from a small sample, with a fairly high proportion of excluded patients (40%). This may explain why this study did not identify factors previously found to more frequently affect sleep adversely such as female gender, the elderly and those with chronic medical conditions.16 In addition the population sample has little ethnic diversity which limits the generalisability of the results.
Implications
This study found that the prevalence of poor sleep quality was more common than previously reported in the general population17 and more comparable to the higher rates reported in similar patient populations. Two previous studies investigating subjective sleep quality using the PSQI, found prevalence rates of poor sleepers to be 45.5%18, and 91.22%19 among a population of schizophrenia patients and psychiatric in-patients respectively.
Complaints of poor sleep are important for diagnostic purposes and also raise the need to address the adequacy of therapeutic strategies, given the consequent adverse impact on patients’ mental state, physical health, daytime function and quality of life.
Improving Sleep
Hypnotics such as benzodiazepines and benzodiazepine receptor agonists can be efficacious for the treatment of insomnia.20,21 However the clinical benefits must be weighed against well known adverse effects, such as daytime sedation, agitation, memory impairment, confusion and ataxia. This, together with the recommendation that hypnotics should only be used for short periods of time because of the risk of drug tolerance and dependence,22 highlights the need for suitable non-pharmacological alternatives.
Recent reviews support the notion of the effectiveness of Cognitive Behavioural Therapy for insomnia in the treatment of people with psychiatric or medical conditions.13,23 Modified, lower cost education initiatives to promote good sleep could be employed by utilising the skills of the mental health professionals caring for patients on the ward, supplemented by the provision of clear written material.
Environmental variables to consider include adherence to regular ward routines including bedtime and awakening times, attention to ward layout and design (including the provision individual bedrooms), lighting, ambient noise, temperature, and the provision of comfortable mattresses and appropriate bed linen. Medication scheduling times, regular medication reviews, and avoidance of non-prescribed substances such as caffeine, alcohol and illicit substances are also important. Physical health problems, pain and psychological distress should be optimally managed. Moderate intensity exercise programs have also been found to bring about significant improvements in self-rated sleep quality.24 Finally, increased staff awareness and sensitivity to the sleep problems on the ward, supplemented with objective recording of such disturbances, would be informative in gaining a further understanding of patients’ insomnia experiences.
Future Directions for Research
The PSQI is simple and inexpensive to perform. Results could be followed longitudinally in order to examine the course of sleep problems throughout an episode of acute mental illness, or to examine the effects of specific therapeutic interventions for sleep disorders. Sleep diaries have been shown to provide reliable estimates of subjective sleep parameters25 and could be used as an adjunct to the PSQI. Ideally, concomitant objective measures such as polysomnography or wrist actigraphy (which detects physical motion), as well as cognitive and behavioural measures could be used to provide additional data.
This study represents the first attempt to examine the degree of self-reported poor sleep quality in a UK-based population of psychiatric in-patients and results suggest unsatisfactory sleep is a common finding. Large prospective longitudinal studies of sleep quality with control for confounding factors are needed to confirm the high prevalence rates in psychiatric in-patients. Studies comparing psychiatric patients with healthy controls, and also with insomniacs without psychiatric comorbidity, would further clarify the role of psychopathology in sleep disturbance.
ACKNOWLEDGEMENTS With thanks to Mr Paul Bassett, Statistical Consultant COMPETING INTERESTS None Declared AUTHOR DETAILS LUCINDA DONALDSON, BSc, MB BS, MRCPsych, Specialty Registrar, Barnet, Enfield and Haringey Mental Health Trust, United Kingdom PRAVEEN KUMAR CHINTAPANTI, MB BS, DPM, MRCPsych, Consultant Psychiatrist, Camden and Islington NHS Foundation Trust, United Kingdom CORRESPONDENCE: LUCINDA DONALDSON, Specialty Registrar, South West Complex Mental Health Team, 7th Floor Premier House, 112 Station Road, Edgware, Middlesex HA8 7BJ, United Kingdom Email: lucindadonaldson@yahoo.co.uk
References
1. Ancoli-Israel S, Roth T. Characteristics of insomnia in the United States: results of the 1991 National Sleep Foundation Survey. I. Sleep 1999;22 Suppl 2:S347-53.
2. Leger D, Scheuermaier K, Philip P, et al. SF-36: Evaluation of quality of life in severe and mild insomniacs compared with good sleepers. Psychosom Med 2001;63:49-55.
3. Roth T. Prevalence, associated risks, and treatment patterns of insomnia. J Clin Psychiatry 2005;66 suppl 9:10-13.
4. Leger D, Guilleminault C, Bader G, et al. Medical and socio-professional impact of insomnia. Sleep 2002;25(6):625-629.
5. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA 1989;262:1479-84.
6. McCall WV. A psychiatric perspective on insomnia. J Clin Psychiatry 2001;62 Suppl 10:27-32.
7. World Health Organisation. The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research. Geneva: World Health Organisation, 1993.
8. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th edn) (DSM-IV). Washington, DC: American Psychiatric Association, 1994.
9. Buysse DJ, Reynolds CF 3rd, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193-213.
10. Doi Y, Minowa M, Uchiyama M, et al. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res 2000;97:165-172.
11. Breslau N, Roth T, Rosenthal L, et al. Sleep disturbance and psychiatric disorders: a longitudinal epidemiological study of young adults. Biol Psychiatry 1996;39:411-418.
12. Chang PP, Ford DE, Mead LA, et al. Insomnia in young men and subsequent depression. The Johns Hopkins Precursors Study. Am J Epidemiol 1997;146:105-114.
13. Stepanski EJ, Rybarczyk B. Emerging research on the treatment and etiology of secondary of cormorbid insomnia. Sleep Med Rev 2006;10:7-18.
14. Richardson GS, Roth T. Future directions in the management of insomnia. J Clin Psychiatry 2001;62 suppl 10:39-45.
15. Roth T, Roehrs T. Insomnia: Epidemiology, Characteristics, and Consequences. Clin Cornerstone 2003;5(3):5-15.
16. Morin CM, Hauri PJ, Espie CA, et al. Nonpharmacologic treatment of chronic insomnia: an American Academy of Sleep Medicine review. Sleep 1999;22:1134-56.
17. Doi Y, Minowa M, Uchiyama M, et al. Subjective sleep quality and sleep problems in the general Japanese adult population. Psychiatry Clin Neurosci 2001; 55(3): 213-215.
18. Ritsner M, Kurs R, Ponizovosky A, et al. Perceived quality of life in schizophrenia: Relationships to sleep quality. Qual Life Res 2004;13:783-791.
19. Prieto-Rincón D, Echeto-Inciarte S, Faneite-Hernández P, et al. [Quality of sleep in hospitalized psychiatric patients]. Invest Clin 2006;47:5-16.
20. Nowell PM, Mazumdar S, Buysse DJ, et al. Benzopdidazepines and zolpidem for chronic insomnia: a meta-analysis of treatment efficacy. JAMA 1997;278:2170-7.
21. Holbrook AM, Crowther R, Lotter A, et al. Meta-analysis of benzopdiazepine use in the treatment of insomnia. CMAJ, 2000; 162: 225-233.
22. National Institute for Health and Clinical Excellence. Guidance on the use of zaleplon, zolpidem and zopiclone for the short-term management of insomnia. London: NICE, 2004. (Technology Appraisal 77.) Available from: URL: http://www.nice.org.uk/TA077guidance
23. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25:559-92.
24. King AC, Oman RF, Brassington GS, Bliwise DL, Haskell WL. Moderate-Intensity Exercise and Self-rated Quality of Sleep in Older Adults. A Randomized Controlled Trial. JAMA 1997;277:32-37.
25. Coates TJ, Killen JD, George J, et al. Estimating sleep parameters: A multitrait-multimethod analysis. J Consult Clin Psychol 1982;50:345-52.
Hepatitis B is one of the world’s major health problems 1. By recent estimates, worldwide more than 2 billion people have been infected with hepatitis B virus (HBV) globally and more than 350 million have chronic (long term) liver infections2. The infection is supposed to be causally related to 1 to 2 million deaths per year worldwide 3. Hepatitis B is a blood borne infection that is transmitted 1) by an infected mother to the newborn, 2) by contact with infected blood through unsafe injection, transfusion, open wounds, and sharing toothbrush or razors, and 3) by unprotected sex. Approximately 90% of newborns infected with HBV develop chronic infection, whereas 30-50% of children under age 5 years, 10% of adolescents aged 15 years, and 2-5% of older individuals develop chronic infection 4,5.
In Pakistan, it is Hepatitis (B & C) not Human immuno deficiency virus (HIV) that is the most common serious viral infection. Number of hepatitis B carriers in Pakistan is estimated at around seven million4 that is about 5% of the world wide 350 million carriers of hepatitis B 5. Unlike HIV, there was no large-scale national awareness campaign to educate the public and healthcare professionals in Pakistan about these infections before 2006, but now a comprehensive national strategy that will lead to the elimination and control of hepatitis B is becoming a top public health priority in Pakistan after inclusion of HBV immunization in government’s expanded Program for Immunization (EPI). The World Health Organization (WHO) Assembly endorsed the recommendation of its Global Advisory Group that all countries should implement a hepatitis B immunization program6. The threat of HBV to the health of the nation is frequently under-recognized by epidemiologists, policy makers and the public because unlike the influenza virus, it is often not the acute infection that makes people sick, but the consequences of chronic HBV infection that occurs after 20-30 years. Fortunately, hepatitis B is a vaccine preventable disease, global eradication is therefore possible if everyone worldwide receives the HBV vaccine before they become infected. Despite advances in antiviral therapy, only a minority of patients with chronic hepatitis B will have a sustained response. Thus, primary prevention by vaccination to increase herd immunity remains the main thrust in the control of HBV infection.
The development of hepatitis B vaccine is considered to be one of the major achievements of modern medicine. Three different classes of hepatitis B vaccine are available based upon how they are derived (from plasma, yeast, or mammalian cells).The first generation HBV vaccine was prepared by concentrating and purifying plasma from Hepatitis B surface antigen (HbsAg) carriers to produce 22 nm sub viral particles, which contain HBsAg alone. Derivation from plasma has left lingering concerns regarding the potential to transmit blood-borne infections, although this vaccine has excellent efficacy and safety7. Yeast-derived recombinant HBV vaccines were first introduced in the mid 1980s. They are produced by cloning of the HBV-S gene in yeast cells. These vaccines contain non-glycosylated HBV small S protein as the envelope antigen which must be released from the yeast during the manufacturing process 8. These vaccines do not contain antigens of the pre-S regions. The third class of HBV vaccine is the mammalian cell-derived recombinant vaccine. Three vaccines of this class have been developed. In addition to the S antigen, one of these contain antigen from the pre-S2 region while the other two contain antigens from both the pre-S1 and pre-S2 regions 9
The efficacy of universal immunization has been shown in different countries, with striking reductions of the prevalence of HBV carriage in children, most importantly; the HBV vaccine can be considered the first successful anti-cancer vaccine, as 20 years of mass vaccination has clearly reduced the incidence of hepatocellular carcinoma in children, at least in Taiwan 10. Currently available hepatitis B vaccine in Pakistan’s market are genetically engineered DNA recombinant vaccines and the recommended series of three intramuscular doses of hepatitis B vaccines induces a protective antibody response (anti-HBs > =10 milli-international units {mIU/ml}) in > 90% of healthy adults and in >95% of infants, children and adolescents 7, 11.
A vaccine consists of many parts, only one of which is the antigen by which it is known. Other components of the presentation may include, for instance, an adjuvant, a preservative or other ingredient. There may be components not stated on the information sheet that are classified as proprietary and therefore the manufacturers are not obliged to declare them. Thus, the effect the vaccine has, on an individual may be influenced in various ways by each and all of these components. Preservatives are just one of a number of additives to vaccines that are carefully regulated and which come under special scrutiny from time to time 12. Several case reports raised concerns that hepatitis B (HB) immunization might be linked to new cases or reactivation of multiple sclerosis, could shift the immune system toward an auto-immune direction, or may cause central nervous system (CNS) demyelinating diseases etc 13, 14, 15, 16. The present study sought to compare the safety of four hepatitis B vaccine regimens available in Pakistan’s market, in apparently healthy young females, and to determine the sero-response (i.e. reactogenicity and immunogenicity) to these vaccine in the same group of volunteers.
MATERIALS AND METHODS: Study Duration: Jan 2003 to Jan 2006 Study Design: Prevention, Open Label, Dose Comparison, Parallel Assignment, Safety/Efficacy Study. Subject: A total of 243 apparently young healthy female students of two Universities of the city were included in this study. Informed Consent: Prior to immunization, all volunteers were requested to give written informed consent to participate in this study. The volunteers were also advised that they are free to withdraw from the study at any time without any obligation to disclose her reason (s) for so doing. Criteria For Inclusion In The Study: All volunteers after submitting their signed consents were subjected to selection criteria on the basis of health checkups by a medical doctor to record the various factors including: a) Age: 18 – 30 years, b) History of Jaundice, blood transfusion, exposure to syringe, surgical and dental, c) Weight: > 45 Kg, d) Body Temperature: 96 – 98°F, e) Hemoglobin: > 10 g/ dl, f) Blood Pressure: Systolic 100 – 180 mm of Hg, Diastolic: 60 – 100 mm of Hg, g) Pulse rate: > 65/min.
After qualifying for inclusion in this study, volunteers were asked to give 10 cc of blood sample for different hematological (CP i.e. complete blood picture and Hb% i.e. hemoglobin percentage by Sysmex blood analyzer & ESR i.e. erythrocyte sedimentation rate by Westergreen method ), and Biochemical analysis (Direct Bilirubin, Indirect Bilirubin, ALT, AST and, Alkaline phosphatase by MicroLab- Merck chemistry analyzer), this data was used to keep the record of health status of participants and its comparison with adverse effects if appeared. Screening for HBs antigen, anti HBs antibodies and HBc IgM antibodies by Immunochromatography (ICT, Australia and Abbott, USA) and confirmation by enzyme linked immunosorbent assay (IMX ELISA - Abbott, USA) was also done before first dose of immunization. Test Vaccines: Fourrecombinant yeast derived HB vaccine were used as test regimens i.e. Euvax-B (LG Chemicals Ltd., Korea), Heptis-B (Boryang, Korea), Amvax-B (Amson, Pakistan) and Engerix-B (GS & K, Belgium). To avoid complications related to multi dose vials, it was strictly followed that the vaccination dose for each subject should be company packed, individually in a sealed container and, formulated for intra muscular injection. The dosage vial should contain same amount i.e. 20 μgm/ ml of HBs Ag absorbed on to approximately 0.5 μgm / ml adjuvant (aluminum hydroxide) and 100 μgm / ml preservative (Thiomersal/ Thimerosol) in a final volume of 1.1 ml (1 dose/ vial). Storage temperature should maintain as 2ºC to 8ºC to ensure integrity. Participants were injected with the vaccine of their own choice. Information broachers of the four vaccines were distributed among participants to help them make a choice. Out of total 729 doses administered to 243 individuals during this study, 195 were of Engerix-B, 420 were Heptis-B, 75 were Amvax-B, and 39 doses were of Euvax-B. Categories for Determining Severity of an Adverse Effect:
Local Symptoms: Soreness, indurations, swelling and redness.
General Symptoms: Fever, headache and dizziness.
Mild: Adverse events easily tolerated
Moderate: Adverse event of sufficient discomfort to interfere with daily activity or requiring simple treatment (e.g. Paracetamol, Generic name: Paracip).
Severe: Adverse event incapacitating and preventing usual activity or which may be life threatening, requiring hospitalization or completed treatment.
The course of an adverse event was described as:
Spontaneous recovery without discontinuation of vaccination
Recovery after discontinuation of vaccination
Continuation of recovery after symptomatic treatment
Eight samples of Peripheral blood (2-3 ml) were taken from all vaccinees before administration of each dose, and at different intervals after completion of immunization as per schedule given below; the sera were collected and stored at - 20°C.
Table 1: Visits Were Scheduled As Follows:
Vaccination number & sample collection
1.
First sample Before 1st dose of Vaccine (Jan, 2003)
2.
Second sample Before 2nd dose of Vaccine (Feb, 2003)
3.
Third sample Before3rd dose of Vaccine (June, 2003)
4.
Fourth sample After 6 months of 3rd dose (Dec, 2003)
5.
Fifth sample After 15 months of 3rd dose (Sep, 2004)
6.
Sixth sample After 19 months of 3rd dose (Jan, 2005)
7.
Seventh sample After 22 months of 3rd dose (May, 2005)
8.
Eighth sample After 30 months of 3rd dose (Jan, 2006)
Antibody Estimation and Statistics:
Anti-HBs were detected by ELISA using IMX- Abbott and quantitated using appropriate dilution of a positive sample with a known concentration of anti-HBs expressed as IU/L, provided by the manufacturer. The assay determined IgG type of anti- HBs antibody and the protective level of antibody was considered >10 IU/L. P values of less than 0.05 were considered significant. On the whole Hepatitis B antibodies titer was determined in participants using five standards i.e. <10 IU/ml, Between 10 – 100IU/ml, Between 100 – 1000 IU/ml, >1000 IU/ml, and no response or no antibody titer for the period of 36 months starting Jan’2003 till Jan’ 2006.
RESULTS:
Percentage of Geometric mean titer (GMT) of antibodiesbelow 10 IU/ml was in between 0.0% to 0.22% in case of Engerix-B, 0.0% to 0.20% in case of Euvax B, 0.0% to 0.30% in case of Amvax-B and 0.0% to 0.25% in case of Heptis-B. Percentage of GMT of antibodies between 10 – 100 IU/ml was in between 0.0% to 10% in case of Engerix-B, 0.0% to 9% in case of Euvax B, 0.0% to 8.9% in case of Amvax-B and 0.0% to 9.3% in case of Heptis-B. Percentage of GMT of antibodies between 100 – 1000 IU/ml was in between 0.0% to 35% in case of Engerix-B, 0.0% to 30.1% in case of Euvax B, 0.0% to 39.3% in case of Amvax-B and 0.0% to 40% in case of Heptis-B. While, Percentage of GMT of antibodies above 1000 IU/ml was in between 0.0% to 23% in case of Engerix-B, 0.0% to 25% in case of Euvax B, 0.0% to 26% in case of Amvax-B and 0.0% to 23.7% in case of Heptis-B. When Percentage of GMT of negative response was calculated we found that on the whole Engerix-B showed no response after 6 months of 3rd dose in 0.9% recipients leading towards no response in 31.78% of recipients after 30 months of 3rd dose. Euvax-B showed no response after 6 months of 3rd dose in 7.9% recipients leading towards no response in 35.68% of recipients after 30 months of 3rd dose. Amvax-B showed no response after 6 months of 3rd dose in 11.6% recipients leading towards no response in 25.5% of recipients after 30 months of 3rd dose. While, Heptis-B showed no response after 6 months of 3rd dose in 9.88% recipients leading towards no response in 26.75% of recipients after 30 months of 3rd dose. Period after 6 months of 3rd dose and before 15th month of 3rd dose was the period when highest Percentage of GMT of anti- HBs was observed .
Local and generalized adverse effects observed during and after the immunization of volunteers were recorded separately for each vaccine (Table 2, 3, 4 & 5).
Table 2 Incidence of Local and/or Generalized Symptoms on Vaccination With Engerix-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
N
%
n
%
n
%
1
65
19
29
5
8
10
15
38
58
2
65
11
17
3
5
7
11
29
45
3
65
8
12
0
0
0
0
18
28
Total
195
38
19
8
4
17
9
85
44
Table 3 Incidence of Local and/or Generalized Symptoms on Vaccination With Euvax-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
13
4
31
2
15
3
23
8
62
2
13
2
15
1
0
2
15
6
46
3
13
2
15
0
0
0
0
0
0
Total
39
8
21
3
8
5
13
14
36
Table 4 Incidence of Local and/or Generalized Symptoms on Vaccination With Heptis-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
140
53
38
10
7
34
24
95
68
2
140
25
18
25
18
27
19
70
50
3
140
22
16
7
5
32
23
84
60
Total
420
100
24
42
10
93
22
249
59
Table 5 Incidence of Local and/or Generalized Symptoms on Vaccination With Amvax-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
25
13
52
8
32
3
56
23
92
2
25
2
8
6
24
4
16
9
36
3
25
14
56
3
12
25
100
12
48
Total
75
29
39
17
27
32
43
44
59
As Shown in Table 6 that one month after the first dose, 180/243 subjects (74.45%) had seroprotection with respect to anti-HBs. One month after the second dose, 189/243 subjects (77.92%) showed seroprotection, four months after second dose, at month 6, 224/243 subjects (92.43%) were seroprotective. After 15 months of 3rd dose 231/243 subjects (95.27%) showed maximum seroprotection level in the immunized women. Later on seroprotection level was determined after 19, 22 and 30 months of 3rd dose. 170/243 subjects (70.08%) subjects were seroprotected even after 30 months of 3rd dose without having any booster dose.
Table 6: Over All Seroprotection Levels and Geometric Mean Titers (GMT) of Anti- HBs Antibodies
Timing
N
S+
% of S+
GMT
Range of Anti HBs Titer
PRE
Before Vaccination (Jan, 03)
243
0
0
0
0
M1
Before 2nd dose (Feb, 03)
243
180
74.45
16
0-50
M2
Before 3rd dose (June, 03)
243
189
77.92
143
1-700
M3
After 6 months of 3rd dose(Dec, 03)
243
224
92.43
18500
45-50000
M4
After 15 months of 3rd dose(Sep, 04)
243
231
95.27
23000
40-50000
M5
After 19 months of 3rd dose(Jan, 05)
243
222
91.57
12100
39-33000
M6
After 22 months of 3rd dose(May, 05)
243
195
80.53
1875
5-17000
M7
After 30 months of 3rd dose(Jan, 06)
243
170
70.08
690
1-1500
Comparative results of serum protection analysis of 04 candidate vaccines determined after 15 months of third dose without giving any booster dose, were found effective in healthy young female volunteers, demonstrating induction of very good immunogenicity. No significant differences were observed in seroprotection level of test vaccines (Table7). Overall serum protection rate achieved in case of Engerix-B was 95.9%, in case of Euvax-B, it was 95.2%, in case of Heptis-B was 95.0% , and in case of Amvax-B it was 95.1%. Calculated P values for all four test vaccines were lesser than 0.05 indicating significance of the used vaccines.
Table 7: Comparative Serum Protection analysis of 04 different Hepatitis-B Vaccines(n= 243; mean age= 21.5+3.7 Years)
As yet no such immunogenicity trials have been conducted in Pakistan or risk factors indigenous to the region assessed for any of the vaccine being utilized at the population level for such long period. Our study, is one of the longest study, conducted between Jan’2003 and Jan’ 2006, which includes total 243 healthy women subjects of child bearing age group. In this study we have demonstrated that there is no significant difference in reactogenicity and serum protection level among all four candidate vaccines we tested here, excellent immunogenicity of vaccines in volunteers recommends their usage for immunization purpose among different communities without having any doubts related to reactogenicity and side effects.
Recombinant hepatitis B vaccines have long been used for protection in the serum of and three doses have been shown to produce Anti HBs in the serum of approximately 95% of people who have not encountered the virus. The antibody response declines with increasing age. Patientsolder than 30 years have an increased risk of no response toHBV vaccine, as compared with younger persons 17. Thus, immunizationduring childhood or adolescence offers the greatest potentialfor protection 17 and provides lifelong immunity. Ninety percent of healthy adults and 95 percent of infants, children, and adolescents have protective serum anti-HBs antibody concentrations after the vaccine series has been completed 18.
Two kinds of recombinant vaccine are used for active immunization against hepatitis B; one of them contains the PreS1 and PreS2 antigenic domains while the other kind contains S and PreS polypeptide. No important differences between the effectiveness of these two types of vaccine have been detected 19. In a series of studies it has been demonstrated that 90-99% of healthy neonates, children, adolescents and adults develop protective levels of anti-HBs antibody following a standard vaccination course with hepatitis B vaccine 20, 21, 22, 23, 24, 25.
Efficacy of vaccines in the field have been measured long after the vaccine have been introduced at large scale population levels and only selected countries have record keeping such as the Centers for Disease Control in USA and the National Health Services in UK. Most developing countries do not have infra structure to support these activities and therefore the efficacy and risk indigenous to the population remains unknown.
Procurement and delivery of high-quality vaccine has national and international public health and ‘public good’ implications far beyond the scope of most products. People immunized with vaccines of inadequate quality can become ill and die from the disease that the vaccine should have prevented. Even more lives are placed at risk if vaccination coverage declines as a result of reduced public confidence in immunization programs. If we look at the outcome of immunization programs in different countries then we will have a good idea that how mass vaccination helped in reduction of disease burden?26
Importance of dose size, number of doses and dose response is another important issue related to immunization programs. Published studies regarding the dose-response relationship in terms of immunogenicity and sero-protection are highly varied. Chiaramonte et al 27reported that the sero-protection reached a level of 99.6% within one month after primary immunisation with the recombinant hepatitis B vaccine. The findings of Assateerawatt et al28 and Just et al 29 also were the same. Baldy JLS et al carried out a comparative study with three recombinant hepatitis B vaccines, one Brazilian (Butang, Instituto Butantan) and two Korean vaccines (Euvax-B, LG Life Sciences Ltd. and Hepavax-Gene, Green cross Vaccine Corp.), administered intramuscularly to students aged 17to19 years in three doses (corresponding to half the amount of antigen routinely used for adult vaccination) at intervals of one month between the first and second dose, and of four months between the second and third dose. The GMT of anti-HBs induced by the Euvax-Band Engerix-B vaccines were higher than those obtained with the Butangvaccine (p < 0.05); this difference was not significant when comparing the other vaccines two-by-two. No spontaneous adverse effects attributable to the application of any dose of the three vaccines were reported 30.
Vaccine efficacy is defined as the reduction in the incidence of a disease among people who have received a vaccine compared to the incidence in unvaccinated people. The efficacy of a vaccine is measured in clinical trials by giving one group of people a vaccine and comparing the incidence of disease in that group to another group of people who do not receive the vaccine. In our study overall efficacy of the vaccines used was satisfactory, without producing sever adverse effects, also there is no report of incidence of disease till now, in those who were vaccinated during this study(Table 2, 3, 4, 5).
Maximum protection level in terms of immunogenicity was observed in Euvax-B, which showed GMAT of 35.68% in test population. Engerix-B showed GMAT of 31.78%, Heptis-B showed GMAT of 26.75% and, Amvax-B showed GMAT of 25.5% after 30 months of 3rd dose of immunization While highest serum protection level was achieved in case of Engerix -B i.e. 95.9%. On the whole, r-hepatitis B vaccines showed high immunogenicity and good safety profile in the test population.
The inclusion of Hepatitis B in the list of compulsory and Extended Program for Immunization (EPI) in Pakistan since 2005 will result in mass vaccination of pediatric population. However, a big chunk of the adult population, especially healthcare workers, also needs to be immunized against Hepatitis B infection. We believe that all of the above mentioned HB vaccines, which are easily available in Pakistan’s market can be used for these mass vaccination programs without having any doubts related to Reactogenecity and Immunogenicity.
CONCLUSION:
In conclusion, this prospective study reinforces that the four different recombinant hepatitis B vaccines licensed in Pakistan have a good tolerability and are highly immunogenic among young women. It is also recommended that government should ensure the serosurvey of HBsAg and vaccine coverage at country level in order to reduce the disease burden on country’s economy.
ACKNOWLEDGEMENTS We are thankful to the administration of Jinnah University for Women, Karachi-Pakistan, administration of University of Karachi, Karachi-Pakistan, and team of Volunteer students from Microbiology Department, JUW for their cooperation during vaccination camps and manufacturers of test vaccines for giving consents to include their vaccines in this study. COMPETING INTERESTS None Declared AUTHOR DETAILS SHAZIA TABASSUM HAKIM, Ph.D., Virology and Tissue Culture Lab, Jinnah University for Women and I.I.D.R.Lab., University of Karachi, Pakistan SAYYADA GHUFRANA NADEEM, Virology and Tissue Culture Lab, Jinnah University for Women and I.I.D.R.Lab., University of Karachi, Pakistan SHAHANA UROOJ KAZMI, I.I.D.R.Lab., University of Karachi, Pakistan CORRESPONDENCE: SHAZIA TABASSUM HAKIM, Associate Professor & Chairperson, Department of Microbiology, Jinnah University for Women, Nazimabad, Karachi-74600, Pakistan Email: Shaz2971@yahoo.com
References
1.Kane MA, and Clements J. Hepatitis B. D. T. Jamison, W. H. Mosley, A. R. Meashan, and J. Bobadilla , editors. Disease control priorities in developing countries. New York: Oxford University Press N.Y; 1993:321–330.
2.World Health Organization, Revised fact sheet, August 2008.
3.Park K. Textbook of prevention and social medicine, 15th edition, Jabalpur, India: Banarsidas Bhanot Publishers;1997:159
4.Wasim J, Nadim J, Yakoob K , Muhammad I, Tirmizi SFA, et al. Hepatitis B and C: prevalence and risk factors associated with seropositivity among children in Karachi, Pakistan. BMC Infectious Disease. 2006;6:101
5.Zaman AS. 2003. Daily Dawn Internet Edition. 23 January.
6.WHO, 45th World Health Assembly, expanded programme on immunization and vaccine quality—progress report by the Director General, A45/8. World Health Organization, Geneva, Switzerland. 1992.
7.Szmuness W, Stevens CE et al. Hepatitis B vaccine: demonstration of efficacy in a controlled clinical trial in a high-risk population in the United States. N Engl J Med. 1980; 9;303(15):833-41.
8.Stephenne J. Development and production aspects of a recombinant yeast-derived hepatitis B vaccine. Vaccine. 1990;8 Suppl:S69-73; discussion S79-80.
9.Young MD, Schneider DL et al. Adult hepatitis B vaccination using a novel triple antigen recombinant vaccine. Hepatology. 2001;34(2):372-6.
10.Kao JH, Chen DS. Global control of Hepatitis B infection. Lancet Infect Dis. 2002;2(7):395-403.
11. Zajac BA, West DJ, McAleer WJ, Scolnick E M. Overview of clinical studies with hepatitis B vaccine made by recombinant DNA. J. Inf. 1986; Suppl A0:39–45.
12.Clements CJ. Vaccine preservatives: what is the big deal?. Indian J Med Res. 2006;124:5–8.
13.Duclos P. Safety of immunisation and adverse events following vaccination against hepatitis B. Expert Opin Drug Saf. 2003;2:225-31.
14.Hall A, Kane M, Roure C, Meheus A. Multiple sclerosis and hepatitis B vaccine? Vaccine. 1999;17:2473-2475.
15.DeStefano F, Verstraeten T, Jackson LA et al. Vaccinations and risk of central nervous system demyelinating diseases in adults. Arch Neurol. 2003;60:504-509.
16.Ascherio A, Zhang SM, Hernán MA et al. Hepatitis B vaccination and the risk of multiple sclerosis. N Engl J Med. 2001;344:327-332.
17.Fisman DN, Agrawal D, Leder K. The effect of age on immunologic response to recombinant hepatitis B vaccine: a meta-analysis. Clin Infect Dis. 2002;35:1368-1375.
18.Mast E, Mahoney F, Kane M, Margolis H. Hepatitis B vaccine. Plotkin SA, Orenstein WA, editors. Vaccines. Philadelphia: Saunders. 2004:299-337.
19.Bertino JS Jr, Tirrell P, Greenberg RN et al. A comparative trial of standard or high-dose S subunit recombinant hepatitis B vaccine versus a vaccine containing S subunit, pre-S1, and pre-S2 particles for revaccination of healthy adult nonresponders. J Infect Dis. 1997;175:678-681.
20.Zannolli R, Morgese G. Hepatitis B vaccine: current issues. Ann Pharmacother. 1997;31(9):1059-1067.
21.West DJ, Calandra GB. Vaccine induced immunologic memory for hepatitis B surface antigen: implications for policy on booster vaccination. Vaccine. 1996;14(11):1019-1027.
22.Jafarzadeh A, Shokri F. The antibody response to HBs antigen is regulated by coordinated Th1 and Th2 cytokine production in healthy neonates. Clin Exp Immunol. 2003;131(3):451-456.
23.Shokri F, Jafarzadeh A. High seroprotection rate induced by low doses of a recombinant hepatitis B vaccine in healthy Iranian neonates. Vaccine. 2001;19(31):4544-4548.
24.Jafarzadeh A, Kardar GA, Khoshnoodi J, Shokri F. Downregulation of IL-12 production in healthy nonresponder neonates to recombinant hepatitis B vaccine. Iran Biomed J. 2004;8:41-45.
25.Jafarzadeh A, Shokrgozar MA, Khoshnoodi J, Shokri F. Unresponsiveness to recombinant hepatitis B vaccine in healthy Iranian neonates: association with HLA antigens. Irn J Med Sci. 2002;27:51-55.
26.Proceedings of Who’s third expert working group meeting on hepatitis B. Tokyo, Japan 6-7 March 2007.
27.Chiaramonte M, Majori S, Ngatchu T et al. Two different dosages of yeast derived recombinant hepatitis B vaccines: A comparison of immunogenicity. Vaccine. 1996;14:135-7.
28.Assateerawatt A, Tanphaichitr VS, Suvatte V, Yodthong S. Immunogenicity and efficacy of a recombinant DNA hepatitis B vaccine, Gen Hevac B Pasteur in high risk neonates, school children and healthy adults. Asian Pac J Allergy Immunol. 1993;11:85-91.
29.Just M, Berger R, Just V. Reactogenicity and immunogenicity of a recombinant hepatitis B vaccine compared with a plasma derived vaccine in young adults. Postgrad Med J. 1987;63 (Suppl 2):121-3.
30.Baldy JLS, Lima GZ, Morimoto HK et al. Immunogenicity of three recombinant hepatitis B vaccines administered to students in three doses containing half the antigen amount routinely used for adult vaccination. Rev Inst Med Trop S Paulo. 2004;46(2):103-7.
Laparoscopic fundoplication (LF) has been emerging as the procedure of choice for selected patients with symptomatic and problematic reflux disease since the first described case by Dallemagne in 1991 (1). This was followed by a rapid expansion into routine clinical practice shortly afterwards. With increased acceptance and availability of laparoscopy as a safe surgical modality there has been a huge increase in the number of patients undergoing LF. This has probably been due to increased willingness of patients and referring doctors to consider the less invasive procedure, rather than the older ‘open’ surgical treatment, with its more rapid recovery, smaller incisions and earlier return to work and to normal daily activities.
Patient referral patterns have also changed over the last decade with the main indication for consideration of LF being patient choice, a general unwillingness to take long term medication as well as ineffective or intolerance of medications and relapse of symptoms (5-6). Several advantages of LF have been described by recent data including shorter hospital stay, less requirement for analgesia, and sooner return to work (7-9). These have to be offset against procedure specific complications including gastro-oesophageal perforation, pneumothorax, dysphagia, and bleeding (2-4). However, the other main downside to LF is the learning curve during which there are an increased number of complications. Previous reports have suggested the learning curve to be around 20 for an individual surgeon and 50 for an institution (10-12).
In a recent meeting of the Upper GI group at the Royal College of Surgeons there was discussion concerning the incidence and management of dysphagia following laparoscopic fundoplication (13 Bill Owen Day RCS (Eng) 2004). There is a paucity of data available in this regard with a general paucity of negative or unequivocal results in the literature equating to a selection bias towards only positive data and positive reporting of good results.
Therefore the aim of the present study was to look critically at the learning curve and, with respect to operative complications, with specific regard to the incidence and management of dysphagia in a personal series of patients who underwent a laparoscopic fundoplication in a District General Hospital in the United Kingdom.
Patients and Methods
From December 1997 to February 2004, 75 patients who underwent laparoscopic fundoplication under the care of a single consultant surgeon in a district general hospital were included in this study. It became routine practice for LF to be performed by one dedicated surgical team (JMT) who kept a complete prospective list of procedures. This series was complete and the hand written records of all the procedures were used to identify patients undergoing operations for LF with or without reduction and repair of Para-oesophageal hernia during the study period. These records were cross-checked with the theatre logbook, hospital computer system as well as with the surgeon’s own record. This ensured full inclusion in the analysis of patients.
The groups were not randomised and ‘all comers’ where included in the study. However, Group 1 consisted of the first 20 LF whereas Group 2 included LF (numbers 21-75). Informed consent was obtained in writing prior to surgery. At least a single dose of prophylactic antibiotics (of either a third generation cephalosporin or co-amoxiclav) was administered at induction; all patients received standard thromboprophylaxis (subcutaneous clexane, TEDS, intermittent pneumatic calf compression).
Patients underwent a laparoscopic fundoplication as briefly described below. The patient was placed in the lithotomy position with reversed Trendelberg tilt; a pneumoperitoneum was created and 4 ports inserted. The liver was elevated using a ‘Nathanson’ liver retractor placed through a 5 mm epigastric incision. Initially the right and left limbs of the right crus are dissected alongside the pancreaticogastric and phrenogastric ligaments. A window is created behind the distal oesophagus. A Penrose drain is passed through the gap. The short gastric vessels are divided using a harmonic scalpel (Ethicon, USA), if required. The crural limbs are approximated using 2, 2-0 ethibond sutures to leave a hiatus 1 cm wider than the oesophagus. A laparoscopic babcock is placed behind the oesophagus and the gastric fundus is brought left to right behind the oesophagus and bought round to meet with the remaining portion of the fundus anteriorly. Two (or rarely three) sutures of 2-0 ethibond were used for the fundoplication. The upper suture included a bite of the anterior hiatal margin to anchor the wrap. Of note, the important feature of the procedure is the creation of a ‘floppy’ tension free fundoplication. This is hugely aided by good mobilisation of the gastric fundus with its associated ligaments and if required, division of the short gastric vessels. Notably, one must carefully create a window behind the oesophagus and an overlap of no longer than 3 cms length and one must stay high up on the fundus in order to avoid the creation of a ‘2’ compartment stomach syndrome’.
Post-operatively all patients were treated in an identical manner. As soon as tolerated after the operations the patients were allowed the consumption of water; diet and analgesia were made available as soon after surgery as required by individual patients. Complications were noted as they occurred during the follow-up period. Both general and specific complications were documented for at least 6 months. Furthermore, patient demographics, details of operations, all complications and follow-up data were kept. Follow up for the purpose of this audit involved completion of a proforma at a minimum post operative period of one year and a maximum of eight years.
All patients where regularly reviewed daily on the ward whilst they were in-patients and in the outpatients at 4-6 week intervals or sooner should the need arise by the surgical team. Thereafter they were given a “see on request” appointment. Data on patient and procedure related morbidity and acceptability was also collected.
At the time of the study contact was made via the telephone and a questionnaire was completed. A telephone survey asking the patient four questions,
Where they happy with the operation
Would they reccomend the procedure to a friend
Had there symptoms resolved
If they had had post op dysphagia had it resolved
The data was reviewed and analysed in conjunction with our department of medical statistics. Analysis was performed using the Mann-U test. Multivariate analysis of the means was performed using the Kruskal-Wallis Test.
Results
Overall the 75 patients who underwent laparoscopic fundoplication consisted of 44 males (59%) and 31 females (41%). The mean age was 47.0 years (range 22-80 years). Group 1, which consisted of the first 20 LF cases included 11 male and 9 females. The mean age was 53.25 years (range 32-80). Group 2, which consisted of the LF cases numbering 21-75 included 33 male and 22 females. The mean age was 44.8 years (range 22-78). Both groups were well matched across the above parameters with no statistical differences (Table A). Only 4 patients were obese (5%), smoker (n=10, 14%), 7 patients suffering with Hypertension (10%) and one with diabetes mellitus (2%) and were equivalently represented in both groups (data not shown).
Presenting features are shown in Table B. Notably, the commonest presenting complaints included regurgitation of acid/ food in 79% (n=59), heartburn in 73% (n=55) and pain and discomfort 53% (n=35). Other complaints included dysphagia 21% (n=16), cough/wheeze 19% (n=14) and excess salivation 18% (n=13).
Table A: Patient Demographics
Group 1
Group 2
P value
Numbers
20
55
NS
Male: Female
9: 11
22: 33
NS
Age range (mean) yrs
32-80 (53)
22-78 (45)
NS
Operating time (median) mins
120-240 (190)
75-195 (144)
<0.05
Sliding/No sliding
11
44
NS
Type II/Type III hiatus hernia
9
11
NS
Table B: Presenting Features
No. of cases
Regurgitation (acid/food)
59 (79%)
Heartburn
55 (73%)
Dysphagia
16 (21%)
Cough/wheeze
14 (19%)
Excess Salivation
13 (17%)
Nausea
10 (14%)
Epigastric pain
6 (8%)
TOTAL
173 (100%)
Patients underwent pre-operative evaluation with Upper GI endoscopy 88% (n=66), pH manometry 47% (n=35) and barium swallow 32% (n=24). Previous to this procedure all patients (100%) were on or had been during some part of their illness on therapeutic doses of proton pump inhibitors.
There was a significant difference between the operating times in the two groups. Thus in Group 1 the average operating time was 190 minutes (range120-240 minutes) whereas in Group 2 the average operating time was 144 minutes (range 75-195 minutes, P <0.05).
Table C: Post Op Mild and Moderate Complications<
Cases (n=75)
Dysphagia
40
Regurgitation
7
Nausea
4
Diarrhoea
3
Heartburn
5
Excess Salivation
2
Portsite discomfort
6
Gas Bloat
4
Total
71
One of the major aims of the study was to record post-operative complications. Table C shows all mild and moderate complications which resolved completely with conservative management. Of note Table F shows that dysphagia occurred in up to 40 of our patients. Table F shows the distribution of dysphagia in both groups. In group A (n=20) the are 15 patients who complained with dysphagia (75%) of which 5 settled spontaneously and 10 required further investigation with OGD +/- dilation. in group B (n=55), 25 patients suffered with dysphagia all of which settled with conservative management. Our initial policy was to perform an OGD and dilate prophylactically; however, this was abandoned halfway through the study. It was found that the dysphagia settled in all patients with conservative management. Furthermore, other mild/moderate complications, of note included regurgitation of stomach contents (7/75) and port-site discomfort (6/75), all of which also resolved spontaneously
Table D: Major Complications Groups 1 & 2
Group 1
Group 2
P value
PE
1 (5%)
0
NS
Pneumonia
1 (5%)
1 (2%)
NS
Oesophageal Perforation
1 (5%)
1 (2%)
NS
Stomach perforation
0
1 (2%)
NS
Pneumothorax
0
1 (2%)
NS
Major desaturation
0
1 (2%)
NS
TOTAL
3 (15%)
5 (9%)
NS
Table E: Conversion to Open Surgery
Group 1(n=20)
Group 2(n=55)
P Value
Desaturation
0
1 (2%)
NS
Perforation viscus
1 (5%)
1 (2%)
NS
Pneumothorax
0
1 (2%)
NS
Technical (Obese/previous surgery)
2 (10%)
2 (4%)
NS
TOTAL
3 (15%)
5 (9%)
NS
Major complications are shown in Table D. Of note there are three conversions to ‘Open’ surgery in Group 1 and five in Group 2 (Table E). In detail, four cases (two in each group) were converted early because of poor or very difficult access. They included difficulty in reducing the stomach and omentum from the mediastinum into the abdomen, unable to reach the hiatus despite placing the ports as high as possible, dense adhesions between the liver and stomach and G-O junction thereby leaving no access to the hiatus and simply impossible access to the upper stomach. Further, oesophageal perforation which was caused by intra-operative insertion of a nasogastric bougie (Group 1), this was repaired laparoscopically with no sequelae. Other reasons for conversions included perforation of the greater curve of the stomach due to the fact that there was thickened fatty tissue around the greater curve of the stomach and spleen which produced a perforation while dissecting the stomach free. Also in Group 2 there was one pneumothorax and in another patient there was marked desaturation on creation of the pneumoperitoneum and in both cases it was deemed safer to open the patient.
Table F: Dysphagia Group
Group 1(n=20)
Group 2 (n=55)
P value
Dysphagia
15
25
NS
Resolved Spontaneously
5
25
<0.05
Investigated (swallow and OGD)
10
0
<0.05
Relaparotomy occurred in three patients; one developed severe pain and clinical shock at 24 hours and it was found on laparotomy to have a perforated oesophagus, the second patient we found disruption of the wrap (requiring re-operation and refashioning the wrap) and a final patient developed small bowel obstruction.
Finally a telephone survey at the conclusion of the study managed to contact 70/75 patients. It was found that overall 68/70 patients were satisfied with their procedure and would recommend the procedure to a relative or friend.
Discussion
Gastro-oesophageal reflux disease (GORD) is the commonest disorder of the Upper GI tract affecting approximately between 10-40% of most western populations and with rising incidence (11). In Australia it has shown to consume around 10% of the national expenditure on prescription drugs. Fortunately the majority of patients settle with simple measures including weight loss and reductions in smoking, caffeine and chocolate consumptions. Furthermore, better timing of meals as well as increasing the number of pillows and raising the head end of the bed can lead to improved symptoms. The advent of H2- receptor antagonist (H2RA) and later proton pump inhibitors (PPIs) has led to symptom control in the majority of patients. However, patients on maximum therapy who remain symptomatic or who develop complications (i.e. haemorrhage, oesophagitis, strictures) or those who refuse long term medication are deemed candidates for surgical intervention.
LF has emerged as the procedure of choice for GORD. The present study, which is a personal single surgeon series, shows that laparoscopic fundoplication is a safe and effective procedure with low rates of long-term complications. Importantly, post operatively these patients may develop dysphagia which settles with conservative measures in the vast majority of cases (13).
There is no doubt that for LF a ‘learning curve’ exists but there is debate about the actual numbers. Most studies suggest that it is around 20 for an individual and around 50 for a department (12), thus in the present study we compared our first 20 (classically thought to be within the learning curve) with the next 55 in order to assess major complications, conversions to open procedure. We found that in Group 1 there were 3 major complications (15%) whereas in the next 55 cases there were five (9%). Indeed only one major complication in Group 1 and two in Group 2 could be considered as technical, they were oesophageal and gastric perforations the rest being post operative pneumonia, PE and major desaturation. There were no deaths in either group. This was in keeping with previously published series (14-16).
Previously published data and our own observations revealed that there were significant post operative rates of dysphagia. In the present series dysphagia was the single commonest complication experienced by 53% of patients (n=40). Initially these were investigated with barium swallow and OGD and treated aggressively with early dilation (Group 1) however this strategy was abandoned after it was found that the vast majority of our patients resolved their dysphagia with conservative treatment. From thereon we adopted a very conservative approach reassuring the patient and keeping within close contact until the dysphagia resolved. We reserved dilatation for only highly resistant dysphagia or patients who where non-compliant with conservative treatment. We found that clear explanations pre-operatively, regular reassurance and assessment was generally all that was required. In Group 2 (21-75) none of the patients required dilation for dysphagia. It is almost universal that patients undergoing LF will have a degree of dysphagia. However what is now accepted and reflected from the experience from the present study is that dysphagia after LF should only cause concern if severe, presenting with severe pain, uncontrolled retching and vomiting requiring immediate surgical revision (17). Most commonly this is due to over-tightening of the hiatus or with poor mobilisation and a 360 degree wrap. This may be related to the learning curve, being more common in the earlier cases in a personal series. In our series 53% of patients (n=40) experienced dysphagia. This is comparable to previous reported data (2,16). Notably, Fontaumard et al reported a dysphagia rate of 78% (40/51). The reason for this post operative dysphagia has been thought to be related to the type of procedure. In our series all patients underwent a Nissen type of repair however evidence is now emerging that the incidence of dysphagia and gas related complications are reduced following anterior partial fundoplication (19,20). This is shown from the data of two recent randomised controlled studies. Baigrie et al (18) in a double-blind, randomized study compared laparoscopic Nissen total fundoplication and anterior partial fundoplication. There were no differences in mean heartburn scores between groups but dysphagia scores for both liquids and solids were lower after anterior fundoplication. Also Ludemann et al (19) compared total fundoplication for gastro-oesophageal reflux disease with an anterior 180 degrees partial fundoplication. Both achieved effective reflux control but the partial wrap was associated with fewer side-effects in the short term than total fundoplication. After 5 years, dysphagia, measured by a visual analogue score for solid food and a composite dysphagia score, was worse at 5 years after total fundoplication.
Our study confirms what has previously been shown with the learning curve for LF and its acceptability. It has also clearly highlighted that post operative dysphagia is common and affects a significant number of patients post operatively. However in our study we found that this was best managed conservatively and the almost all resolved spontaneously. There is no evidence to support early intervention unless the symptoms are very severe and occur very soon after surgery, when the patient should be taken back to theatre for another look. The specific causes of the dysphagia are not known but it is postulated that it is due to increased pressure as the upper part of the wrap augments the pressure of the lower oesophageal sphincter causing it to become over competent. Over time this mechanism relaxes leading to an improvement in dysphagia with simple conservative therapy. Furthermore, there was a hugely positive satisfaction score on a simple telephone survey suggesting symptom control from this procedure.
COMPETING INTERESTS None Declared AUTHOR DETAILS A A RIAZ, FRCS(I) FRCS(Eng) FRCS(Gen) PhD, Hunterian Professor RCS(Eng) and Senior Visiting Clinical Fellow, University of Hertfordshire, UK CORRESPONDENCE: A A RIAZ, Consultant Upper GI, Laparoscopic and General Surgeon, West Hertfordshire Hospitals NHS Trust, Waverley Road Hertfordshire, AL3 5PN, UK Email: mrariaz@hotmail.com
Watson DI, Johnson AG, Reed MWR, Stoddard CJ. Laparoscopic Fundoplication for gastroesophageal reflux. Ann R Coll Surg Engl 1994:76; 264-68.
Schauer PR, Meyers WC, Eubanks S et al. Mechanisms of avoidance of esophageal perforation during laparoscopic Nissens fundopliaction. Ann Surg 1996; 223:43-52.
Reid DB, Winning T, Bell G. Pneumothorax during laparoscopic dissection of the diaphragmatic hiatus. Br J Surg 1993;80:670
Perdikis G, Hinder RA. Lund J. Laparoscopic Nissens Fundoplication: where do we stand? Surg Laparosc Endosc 1997; 7; 17-21.
Laine S, Rantala A, Gullichsen R, Ovaska J. Laparoscopic vs. conventional Nissens Fundoplication. Surg Endosc 1997; 11:441-44.
Zacharoulis D, O'Boyle CJ, Sedman PC, Brough WA, Royston CM. Laparoscopic fundoplication: a 10-year learning curve. Surg Endosc. 2006; 20(11):1662-70.
Martin RC 2nd, Kehdy FJ, Allen JW. Formal training in advanced surgical technologies enhances the surgical residency. Am J Surg. 2005 Aug; 190(2):244-8.
Hwang H, Turner LJ, Blair NP. Examining the learning curve of laparoscopic fundoplications at an urban community hospital. Am J Surg. 2005 ;189(5):522-6;
7th Bill Owen Oesophago-Gastric Symposium 'Meet-the-Experts' The Royal College of Surgeons of England, London March 2005.
Watson DI, Baigrie RJ, and Jamieson GG. A learning curve for laparoscopic fundoplication. Definable, avoidable, or a waste of time? Ann Surg. 1996 August; 224(2): 198–203.
Champault GG, Barrat C, Rozon RC, Rizk N, Catheline JM. The effect of the learning curve on the outcome of laparoscopic treatment for gastroesophageal reflux. Surg Laparosc Endosc Percutan Tech. 1999 Dec; 9(6):375-81.
Cuschieri A, Hunter J, Wolfe B, Swanstrom LL, Hutson W. Multicenter prospective evaluation of laparoscopic antireflux surgery. Preliminary report. Surg Endosc. 1993; 7(6):505-10.
Jones NJ, Soper DB. Laparoscopic Nissens Fundoplication. Surg Rounds 1994:17;573-81
The Civil Rights Act 1964 remains of the greatest achievements in United States (US) history. It had implications internationally, making racial discrimination illegal, but its effectiveness in the employment domain remains contestable 2. The worldwide existence of workplace racism has attracted controversy and this is drawn out by psychiatry’s attempt to understand the nature of the problem 3. Discrimination at work, based on a person’s race, comes in different guises and can have negative consequences on both individuals and organisations 1. Despite legislation to protect individuals substantial progress needs to be made to eradicate the problem.
What is racism?
The concepts of “race”, “ethnicity” and “racism” are explained in figure 1.
Figure 1: Definition of race, ethnicity and racism 4, 5
Race
The group a person belongs to as a result of a mix of physical features, ancestry, and geographical origins, as identified by others or, increasingly, as self-identified. The importance of social factors in the creation and perpetuation of racial categories has led to a broadening of the concept to include social and political heritage, making its usage similar to ethnicity. Race and ethnicity are increasingly used synonymously.
Ethnicity
The group you belong to as a result of a mix of cultural factors that include language, diet, religion, ancestry, and race.
Racism
A belief that some races or ethnic groups are superior to others, used to devise and justify actions that create inequality between racial groups.
Racism is a social process associated with “overt and covert forceful establishment and maintenance of power by one social group over another” 3.
Racism can be seen as a misuse of power and, even today, power relations are signified by subtle cultural rules that perpetuate racial inequality 6.
What are the origins of racism?
That some races are superior to others has origins from the 19th century 5. The history of racism has stimulated considerable debate in understanding racism.
Racism may have origins in experiences derived from, what is known in analytical psychology as, the collective and personal unconscious. The personal unconscious arises from the lifetime experiences of the individual. This is distinct from the “collective unconscious” which psychiatrist Carl Jung described to represent a form of the unconscious common to mankind as a whole and originating in the inherited structure of the brain 7. This contains inherited primitive cultural and racial elements. Both the personal and collective unconscious, made from our individual and ancestral experiences respectively, may account for the manifestation of racism in society today.
In recent times the experience of overt racial bigotry and prejudice is seldom seen 8. Nevertheless discrimination against members of a social group may persist because it is so deeply entrenched within society, by the personal and collective unconscious, that it becomes the automatic response even when no conscious intent is present 9. “Everyday discrimination” is the discreet, pervasive discriminatory acts experienced by stigmatised groups on a daily basis 10, and highlights the modern perspective that racism is subtle.
The subtlety of racism
“Like a virus that has mutated, racism has evolved into a new form that is difficult to recognise and harder to combat” 8
As blatant forms of racism become extinguished, particularly in the current climate of political correctness, unconscious racial biases in subtle forms, known as ambivalent or modern racism 10, are appearing. This has been referred to as aversive racism occurring in people who possess strong egalitarian values, and who believe they are not prejudiced, but have negative racial feelings and beliefs that they are unaware of 8. These feelings and beliefs are rooted in the normal psychological processes of social categorisation, satisfaction of basic needs for power and control, and socio-cultural influences 8. The ambivalence involving positive and negative feelings creates a psychological tension that leads to an inconsistent pattern in their behaviour 8.
The cumulative effects of unpredictable and seemingly trivial behaviour such as avoidance of ethnic minorities, closed and unfriendly verbal and non verbal communication, and failure to provide assistance, is more damaging 10. Apparently harmless interactions, including racist assumptions and questioning about where somebody is from, also convey messages about marginality and not belonging 11. This subtle racism may contribute to the racism perceived by minority groups in higher status professions and organisations.
Does racism exist in healthcare organisations?
“American Medical Association apologizes for racism in medicine” (10th July 2008) 12.
This admission by the American Medical Association, of racial discriminatory practices against African-American physicians, reflects the recognition of racism in other western countries.
In the United Kingdom (UK) racism has been revealed in public institutions such as the metropolitan police 13 and widely reported in the nursing profession 14,15 within the National Health Service (NHS). Trevor Phillips, chairman of the Equality and Human Rights Commission, referred to the “snowy peaks of the NHS” 16 with a large number of ethnic minorities at the base. Less than 10% of senior managers and 1% of chief executives are from ethnic minority background 17. There is a “glass ceiling” 18 preventing promotion and black and minority ethnic (BME) managers feel they have to work twice as hard and have twice as many qualifications to succeed 19.
Since 2000, after a survey commissioned by Department of Health (DOH) reported that half of front-line NHS BME staff had been victims of racial harassment in the previous 12 months 20, reports of racism in healthcare have increased. In 2001 a Kings Fund report, “Racism in Medicine” 21, generated powerful debate after finding that bullying and discrimination were a daily fact of life for black and Asian doctors. Then in 2003 a British Medical Association (BMA) survey revealed that in ethnic minority doctors, who form nearly one third of the NHS workforce 22, more than 80 per cent believed that their ethnicity had a negative effect on their career advancement 23. In 2004 the Royal College of Psychiatrists accepted that racism existed in the NHS and in their own institution 24.
How does racism manifest itself in medicine?
“Discrimination can appear to be hidden when it is institutionalised, although it is not usually hidden from the person who is subjected to it” 3
Institutional racism is “the collective failure of an organisation to provide an appropriate and professional service to people because of their colour, culture and ethnic origin” 13. Health disparities among patients have been widely linked to racially biased discriminatory health practices 25, 26, 27 but how do structures, processes, and values within an organisation discriminate against those working in the medical profession?
There is considerable evidence to indicate that discriminatory practices against doctors evolved from medical school. For instance racial discrimination has operated at the time when students applied to study medicine 19, 28, through short-listing based on whether applications had Asian or English names 29, 30, and with downgrading of non-English names by computer 31. Discrimination has also been reported during medical school in the US and Canada 11. UK ethnic minority medical students also perform poorly in examinations compared to white students 32, 33 although the lack of evidence of explicit discrimination may suggest the involvement of more subtle communication styles and cultural differences 33.
If the problems at medical school are accountable by racial organisational processes it is not surprising that discriminatory practices persist after qualification (figure 2)
Figure 2: How BME doctors may experience racism 17, 19, 34, 35, 36
Bullying and harassment
More likely to experience bullying and harassment.
Recruitment and career advancement
More likely to be over-represented in junior grades. Reduced promotion and career advancement also seen in relation to academic careers. Underrepresented in senior leadership positions.
Disciplinary hearings
Over-represented at disciplinary hearings with nearly a third of complaints coming form other health professionals.
Disciplinary action and dismissals
Six times more likely to be disciplined e.g. in 2006 two thirds of the 54 doctors struck off in UK had trained outside UK.
Reward systems
Disadvantaged in the allocation of discretionary grants and NHS distinction awards.
What are the consequences of racism in healthcare?
“Racial discrimination damages both those discriminated against and those doing the discriminating” 37
The cost of workplace racism is that it acts as a chronic and acute stressor on the individual with a range of consequences (figure 3):
Figure 3: Consequences of racism on an individual 1, 10, 38, 39
Psychological
Poor well-being. Loss of confidence. Humiliation. Low morale. Gives a sense of thwarted aspirations.
Physiological
Increase blood pressure. Physical illness.
Behavioural
Bad work performance. Require time off work.
“Racial fatigue” characterises the potential emotional and psychological sequelae of feeling isolated in a work environment in which race regularly influences behaviour but is consistently ignored and nobody wants to discuss it (“racial silence”) 40. Racism may be underreported for the same reasons seen with workplace bullying: fear of making matters worse, belief that nothing will be done, concerns regarding confidentiality, fear of victimisation, and concern about being labelled as a troublemaker 41. In addition the individual may fear being regarded as having a “chip on one’s shoulder”.
Organisations may also suffer with disharmony at work, high sickness levels, and resignation 1. In medicine this results in the “double loss” of a speciality losing highly motivated people and gaining those where enthusiasm may be low 19. In addition victims of racial discrimination in healthcare may pursue legal action. In 2003 a surgeon won over £600,000 42 after being denied entry to the specialist registrar. Another surgeon successfully sued the BMA for more than £800,000 for racial discrimination after it failed to support his own claim against the DOH 43. In another case a UK trust paid £2.5m, including legal costs, for wrongful dismissal of a consultant obstetrician who was investigating discrimination 44.
What can be done if you are experiencing racism at work?
In the UK there is protection by legislation. It is unlawful to discriminate against anyone on racial grounds. The Race Relation Act 1976 defined three types of discrimination (direct, indirect, and victimisation) 1, 45,. Following this was the setting up of the Commission for Racial Equality (CRE) in the UK to tackle racism and promote racial equality 45. The Race Relations Act 1976 has now been superseded by the Race Relations (amendment) Act 2000 46 that requires public bodies to eliminate discrimination, promote equal opportunities, and ensure good race relations. However legal processes are stressful and there are some steps you can take before pursuing this route (figure 4).
Figure 4: Steps to take if you are a victim of racial discrimination 1
Talk to colleagues and friends who may have suffered a similar problem because it helps to share a problem and trying to cope on your own can be particularly stressful.
Keep a diary of events of who said what, when, circumstances and any witnesses – this will give a vital record of the nature of the racism.
Find out whether your employer has specific rules about racism at work or a grievance procedure you can use to raise a problem.
If you are in a union contact them to assist you with talking to management or approaching the perpetrator.
In the UK the Commission for Racial Equality is a national body that can help victims of racial discrimination.
Your local Citizens Advice Bureau or Law Centre may be able to help.
You may want to talk to a private law firm that specialises in discrimination issues.
Recommendations and Conclusion
“The law may be just but its implementation is another matter” 47
Despite legislation and procedures, to address racism at work, healthcare organisations are slow in introducing and supporting the policies for race equality 18. Suits come to legal action, not for a lack of policy, but because of not being enforced 48. Practice is not synonymous with policy 19. Reinforcement of policies depends on the degree to which upper management understands discrimination and harassment 48. Although implementation of policies could be successful in combating overt racism this is not so for the covert form.
The covert form of racism, as in institutional racism where organisational processes are “unwittingly” enacted 13, suggests that racism is inevitable. Even people with strong motivations to avoid it are subject to automatic cognitive activation of stereotypes, which can unconsciously influence behaviour, making diversity training courses and non-discrimination policies relatively ineffective 10. Attending to, and encouraging the reporting of, the “softer” aspects of racism may be the key to establishing a true “positively diverse climate” 10. New forms of racism require new approaches (Figure 5):
Figure 5: The STEEP model to approaching subtle racism in organisations 8
Structured Support
Visibly supported by senior management.
Training and Education
Educate people about subtle bias and training to recognise it.
Experience
Frequent and constructive interracial contact to decrease bias, enhance group cohesion, and increase productivity.
Personal Commitment
Individuals must be committed to recognise and combat subtle racism.
The most important part of the solution is education. Teaching on racism should be incorporated into the undergraduate and postgraduate curriculum 19. However of greater significance is recognising our own personal prejudices, at an early stage, so that prejudices we all harbour are challenged within ourselves.
“The hardest attitude to change is the one you don’t know you have” 8
KEY POINTS – RACISM:
Is associated with power and superiority
Has evolved from an overt to a covert form
Is commonplace in healthcare organizations
Is manifested at each stage of a doctors career
Has implications for individuals and organizations
Can be partly dealt with through policies and legislation
Requires a new approach to eradicate the problem
Useful UK online resources
http://www.oneworkplace.co.uk - “One Workplace Equal Rights” aims to tackle racism and promote equal opportunities in the workplace.
http://homepage.ntlworld.com/rajen/RacialEquality - Race Equality Ltd provides phone advice about racism in the medical establishment.
http://www.bidaonline.org.uk - The British International Doctors Association protects and promotes the interests of Ethnic Minority Doctors and Dentists working in the UK.
http://www.equalityhumanrights.com - A new commission working to eliminate discrimination, reduce inequality, protect human rights and build good relations.
COMPETING INTERESTS None Declared AUTHOR DETAILS MINAL MISTRY, BSc, BM, MRCPsych, MSc, Hampshire Partnership NHS Trust, United Kingdom JAVED LATOO, MBBS, DPM, MRCPsych, North East London NHS Foundation Trust, United Kingdom CORRESPONDENCE: Dr MINAL MISTRY, Hampshire Partnership NHS Trust, Melbury Lodge, Winchester, United Kingdom Email: minalmistry@yahoo.co.uk
References
1. TUC. Racism at work - a crime in anyone’s language. Available from: http://www.tuc.org.uk/tuc/rights_racism.cfm
2. Stainback K, Robinson CL, and Tomaskovic-Devey D. Race and workplace integration: a politically mediated process? Am Behav Sci. 2005; 48(9): 1200-1228.
3. Moore LJ. Psychiatric contributions to understanding racism. Transcult Psychiatry. 2000; 37(2): 147-182.
4. Bhopal R. Racism in medicine. Br Med J. 2001; 322: 1503-1504.
5. Bhopal R. Spectre of racism in health and health care: lessons from history and the United States. Br Med J. 1998; 316: 1970-1973.
6. Baker LD. Racism in professional settings: forms of address as clues to power relations. J Appl Behav Sci. 1995; 31(2): 186-201.
7. Encyclopaedia Britannica. Collective unconscious. Available from: http://www.britannica.com/EBchecked/topic/125572/collective-unconscious
8. Dovidio J. The subtlety of racism. Train Dev J. 1993; 47(4): 50-57.
9. Craig-Henderson KM. The automaticity of stereotyping and discrimination. PsycCritiques. 2006; 51(40): abstract.
10. Deitch EA, Barsky A, Butz RM, Chan S, Brief AP and Bradley JC. Subtle yet significant: the existence and impact of everyday racial discrimination in the workplace. Hum Relat. 2003; 56(11): 1299-1324.
11. Beagan BL. ‘Is this worth getting into a big fuss over?’ Everyday racism in medical school. Med Educ. 2003; 37: 852-860.
12. Aluko Y. American Medical Association apologizes for racism in medicine. J Natl Med Assoc. 2008; 100(10): 1246-1247.
13. Macpherson W. The Stephen Lawrence inquiry report. London: Stationary office, 1999.
14. Beishon S, Virdee S and Hagell A. Nursing in a multi-ethnic NHS. London: Policy studies Institute, 1995.
15. Staines R. Is racism a problem in nursing? Nurs Times. 2006; 102(10): 12-13.
16. Duffin C and Parish C. Freedom from racism. Nurs Stand. 2005: 20(4): 22-23.
17. White C. Trusts are making slow progress in promoting race equality, says Healthcare Commission. Br Med J. 2009; 338: b1357.
18. Sheikh A. What’s to be done about racism in medicine? J R Soc Med. 2001; 94(10): 499-500.
19. Coombes R. Mountains to climb. Health Serv J. 2004; 114(5925): 39-46.
20. Chand K. Letter: NHS racism is swept under the carpet. GP. 2004: 33-34.
21. Coker N (ed). Racism in medicine: an agenda for change. London: Kings Fund, 2001.
22. Esmail A. The prejudices of good people. Br Med J. 1994; 328: 1448-1449.
23. Cooke L, Halford S and Leonard P. Racism in the medical profession: the experience of UK graduates, 2006. Available from: http://www.bma.org.uk/employmentandcontracts/equality_diversity/ethnicity/racism.jsp
24. Mamode N. Is the BMA a 21st century organisation? Br Med J. 2004; 329: 161-163.
25. Dennis GC. Racism in medicine: planning for the future. J Natl Med Assoc. 2001; 93(3) Suppl: 1S-5S.
26. Clark PA. Prejudice and the medical profession; a five year update. J Law Med Ethics. 2009: 118-133.
27. Johnstone M-J. Nurses must take a stand against racism in health care. Inter Council Nurses. 2006; 53: 159-160.
28. Mcmanus IC. Factors affecting likelihood of applicants being offered a place in medical schools in the United Kingdom in 1996 and 1997: retrospective study. Br Med J. 1998; 317: 1111-1117.
29. Esmail A and Everington S. Racial Discrimination against doctors from ethnic minorities. Br Med J. 1993; 306: 691-692.
30. Esmail A and Everington S. Letters: Asian doctors are still being discriminated against. Br Med J. 1997; 314: 1619.
31. Lowry S and Macpherson G. A blot on the profession. Br Med J. 1988; 296: 657-658.
32. McManus IC, Richards P, Winder BC and Sproston KA. Final examination performance of medical students from ethnic minorities. Med Educ. 1996; 30(3): 195-200.
33. Wass V, Roberts C, Hoogenboom R, Jones R and Van der Vleuten C. Effect of ethnicity on performance in a final objective structured clinical examination: qualitative and quantitative study. Br Med J. 2003; 326: 800-803.
34. Fox S and Stallworth LE. Racial/ethnic bullying: exploring links between bullying and racism in the US workplace. J Vocat Beh. 2005; 66(3): 438-456.
35. Carr PL, Palepu A, Szalacha L, Caswell C and Inui T. ‘Flying below the radar’: a qualitative study of minority experience and management of discrimination in academic medicine. Med Educ. 2007; 41: 601-609.
36. Pitcher G. NHS human resources staff accused of ignoring racism and bullying of Asian doctors. Available from: http://www.personneltoday.com/articles/2007/08/20/41980/nhs-human-resources-staff-accused-of-ignoring-racism-and-bullying-of-asian-doctors.html
37. Smith R. Deception in research, and racial discrimination in medicine. Br Med J. 1993; 306: 668-669.
38. Forman TA. The social psychological costs of racial segmentation in the workplace: a study of African Americans’ well-being. J Health Soc Beh. 2003; 44(3): 332-352.
39. McKenzie K. Racism and health. Br Med J. 2003 ;326: 65-66.
40. Nunez-Smith M, Curry LA, Bigby JA, Berg D, Krumholz HM and Bradley EH. Impact of race on the professional lives of physicians of African descent. Ann Intern Med. 2007; 146: 45-51.
41. Mistry M and Latoo J (2009). Bullying: a growing workplace menace. Available from: http://www.bjmp.org/content/bjmp-march-2009-volume-2-number-1
42. Newman M. Who’s representing doctors on racism? Hospital Doctor. 11th Oct 2005: p. 9
43. Saleem A. How racism blocked this doctor’s career. Hospital Doctor. 18th Mar 2004: p. 26-27.
44. Symon A. institutional racism and discrimination: are they endemic in the NHS? Br J Midwifery. 2006; 14(6): 366.
45. Dimond Bridgit. Race relations and the law. Br J Midwifery. 2002; 10(9): 580-583.
46. Race relations (amendment) act 2000: New laws for a successful multi-racial Britain. Available from: http://www.homeoffice.gov.uk/documents/cons-2001-race-relations/
47. Dhruev N. Institutional racism: not just skin-deep: how systems sustain racism. Nurs Times. 2002; 98(23): 26-27.
48. Root M P P. The consequences of racial and ethnic origins harassment in the workplace: conceptualisation and assessment. In Barrett K H and George W H (ed). Race, culture, psychology and law. 2005: p. 125.
Ventilator Associated Pneumonia (VAP) is defined as pneumonia occurring in a patient within 48 hours or more after intubation with an endotracheal tube or tracheostomy tube and which was not present before1, 2. Early onset VAP occurs within 48 hours and late onset VAP beyond 48 hours of tracheal intubation.
Incidence
Between 5-15% of hospital in-patients develop infection during admission to ICU3. Patients are 5-10 times more likely to acquire nosocomial infections than patients in the wards4and approximately 86% of hospital associated pneumonia is linked with mechanical ventilation5.
Approximately 10-28% of critical care patients develop VAP6. VAP is also the most common and fatal infection of ICU7,8 and in the United States it affects 9-27% of intubated patients and doubles the risk of mortality as compared with similar patients without VAP9-13.
VAP may account for up to 60% of all Healthcare-Associated Infections14. VAP increases length of ICU stay by 28%16 and each incidence of VAP is estimated to generate an increased cost of £6000- £2200015.
Diagnosis
Despite the high incidence, diagnosis remains challenging because many conditions common to ICU patients like ARDS, sepsis, cardiac failure and lung atelectasis have similar clinical signs. More than 50% of patients diagnosed with VAP do not have the disease whereas upto one-third are not diagnosed17, 18. Unfortunately there is no clearly accepted gold standard for diagnosis of VAP19.
Centres for disease control and prevention (CDC) national healthcare safety network definition for VAP
Radiology signs (2 or more serial chest x-rays with at least one of the following)
New or progressive and persistent infiltrate
Consolidation
Cavitation
Clinical signs
At least one of the following
Fever (temperature > 38 deg C with no other recognised cause)
Leucocytosis > 12000WCC/uL or leucopenia (<4000 WCC /uL)
For adults 70 years or older, altered mental status with no other recognisable cause
and at least 2 of the following
New onset of purulent sputum, or change in character of sputum, or increased respiratory secretions, or increased suctioning requirements
New-onset or worsening cough, or dyspnoea or tachypnoea
Rales or bronchial breath sounds
Worsening gas exchange (eg. O2 desaturations [PaO2/FiO2 ≤ 240], increased O2 requirements, or increased ventilation demand)
Microbiological criteria (optional)
At least one of the following:
Positive growth in blood culture not related to another source of infection
Positive growth in culture of pleural fluid
Positive quantitative culture from bronchoalveolar lavage (≥104 colony forming units/ml) or protected specimen brushing (≥103colony forming units/ml)
5% or more of cells with intracellular bacteria on direct microscopic examination of Gram-stained bronchoalveolar lavage fluid
Histopathological evidence of pneumonia
Histological landmark of VAP is multifocal disease favouring dependant lung segments, often at different stages of development and severity with cultures growing heterogenous microbial flora.20,21
Risk Factors
Mechanical ventilation with Endotracheal intubation including Tracheostomy
Prolonged mechanical ventilation
Advanced age
Pre-existing sinusitis and lung disease
Micro or macroaspiration of oropharyngeal or gastric contents
Malnuitrition and immunosuppression
Obesity
Chronic lung disease
Several factors affect the aetiology of VAP
Time of onset of hospitalisation
Stress induced flora change
Antibiotic induced flora change
Exposure to contamination with nosocomial pathogens
Patient interventions
Pathogenesis:
VAP that occurs within 48 hours after tracheal intubation is usually termed as early onset often resulting from aspiration, which complicates intubation process22. VAP occurring after this period is late onset. Early onset VAP is often due to antibiotic sensitive bacteria (eg oxacillin-sensitive Staphylococcus aureus, Hemophilious influenza and Streptococcus pneumoniae), whereas late onset VAP is frequently caused by antibiotic resistant pathogens (eg.oxacillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa, acinetobacter species and enterobacter species) 23,24,25
The pathogenesis of VAP usually requires that two important processes take place:
Bacterial colonisation of the aero-digestive tract
Aspiration of contaminated secretions into the lower airway26.
Therefore, the strategies to prevent VAP usually focus on reducing the burden of bacterial colonisation in the aero-digestive tract, decreasing the incidence of aspiration or both.
The presence of invasive medical devices is an important contributor to the pathogenesis and development of VAP27. Many patients have nasogastric tubes that predispose them to gastric reflux and increase the potential for aspiration. Endotracheal tubes facilitate bacterial colonisation of the tracheo-bronchial tree and lower airway aspiration of contaminated secretions through mucosal injury, pooling of contaminated secretions above the endotracheal tube cuff and elimination of the cough reflex26. The ventilator circuit and the respiratory-therapy equipment may also contribute to the pathogenesis of VAP if they become contaminated with bacteria, which usually originate in the patient’s secretions26, 28.
Prevention:
The National Institute of Clinical Excellence (NICE) in collaboration with National Patient Safety Agency (NPSA) is examining four technical patient safety solutions for the prevention of VAP and in the process of publishing guidelines. The latest technical patient safety solutions for VAP was published in August 2008 which says
1. Body position-mechanically ventilated and intubated patients should be positioned with their upper body elevated for as long as possible. This may be inappropriate in some patients. eg. spinal injuries. 2. Oral antiseptics e.g. 2% chlorhexidine should be included as part of oral hygiene regimen for all patients who are intubated and ventilated. There is insufficient evidence to recommend any particular antibiotic regimen. 3. Use of kinetic beds - a lack of robust evidence meant the Committee was unable to make recommendations for action on the use of kinetic beds. 4. Care bundles - although the evidence supported the use of elements of care bundles; there was insufficient evidence to recommend a care bundle of any specific design.
The Department of Health published the following ‘High impact intervention’ for ventilated patients in June 2007
Elevation of the head of bed to 35-40 degrees
Sedation holding
Deep Vein Thrombosis prophylaxis
Gastric ulcer prophylaxis
Appropriate humidification of inspired gas
Appropriate tubing management
Suctioning of respiratory secretions (including use of gloves and decontaminating hands before and after the procedure)
Routine oral hygiene as per local policy
In addition the following also may contribute to the prevention of VAP
Prolonged nasal intubation (more than 48hrs) should be avoided because of the association between nosocomial sinusitis and ventilator-associated pneumonia29.
Several investigations have suggested that secretions that pool above the inflated endotracheal tube cuffs may be a source of aspirated material and thus VAP. Endotracheal tubes with separate dorsal lumen above the cuff to suction pooled secretions from the subglottic space are now available. The pressure of the endotracheal tube cuff should be adequate to prevent the leakage of colonised subglottic secretions into the lower airway26,30.
Antibiotic Administration:
Previous administration of antibiotics is an important risk factor for VAP because of the presence of antibiotic-resistant bacteria31. In an attempt to reverse the trend towards increasing rates of antimicrobial resistance among hospital acquired infections, more effective strategies for using antibiotics have been advocated that restrict antibiotic use or offer guidelines for their use 32, 33. Eliminating or reducing the unnecessary use of antibiotics should be the primary goal in reducing antibiotic-resistant nosocomial infections32.
The routine use of prolonged courses of empirical therapy i.e. therapy not supported by results of clinical cultures should be avoided to minimise the subsequent development of antibiotic-resistant infections.
The use of aerosolised antibiotics for the prevention of VAP has been abandoned because of its lack of efficacy and subsequent emergence of antibiotic-resistant infections28.
Similarly the routine use of selective digestive tract decontamination has not gained acceptance in the UK and USA because of its lack of demonstrated effect on mortality, emergence of antibiotic resistant infections and additional toxicity. NICE is currently in consultation for selective decontamination of digestive tract guidelines. The technical patient safety solutions for VAP in adults were published in August 2008.
The Committee examined evidence, which suggested that selective decontamination of the digestive tract (SDD) using topical antibiotics may reduce the incidence of VAP and that SDD regimes that include systemic antibiotics may also reduce mortality. However, Specialist Advisers stated that UK intensive care specialists had particular concerns about the risk of infection with Clostridium difficile and the induction and/or selection of resistant, including multiresistant, microorganisms as a result of SDD. Therefore the Committee recommended further research into SDD in a UK setting.
Use of broad-spectrum antibiotics is also not recommended for the prevention of VAP because of increasing antibiotic resistance among subsequent hospital acquired infections. Targeted antibiotic therapy with appropriate dose of appropriate antibiotic is the sensible thing to do.
Vaccines:
Various vaccination programmes in adults and children have reduced the incidence of pneumonia caused by specific pathogens including H.influenzae type B, Streptococcus Pneumoniae and Influenza virus 34, 35.Vaccinations against these may prevent some hospital acquired infections. Pneumococcal and influenza vaccination must be considered before hospital discharge or included in the discharge planning for all patients at increased risk for subsequent respiratory infections including VAP.
Newer Developments:
There have been new advances in equipment and techniques to help prevention of VAP
Endotracheal and tracheostomy tubes with an extra subglottic port to clear pooled secretions above the endotracheal and tracheostomy tube cuff.
Continuous suctioning of the subglottic secretions.
Endotracheal tubes with specially designed cuffs that do not allow pooled secretions above the cuff to trickle down causing micro-aspiration and ultimately leading to VAP. eg. Endotracheal tubes with microthin polyurethane cuff.
Specially designed closed Tracheal Suctioning Systems (TSS) as compared to open tracheal suctioning systems. However a meta analysis of randomised controlled trial showed that closed suctioning system is not associated with a lower incidence of VAP or mortality as compared to open suctioning36
ACKNOWLEDGEMENTS We thank Dr. S. Parida (Consultant Microbiologist) for her valuable contribution in helping us write this manuscript. COMPETING INTERESTS None Declared AUTHOR DETAILS HARSHAL WAGH, Registrar in Anaesthesia, St Albans City Hospital, United Kingdom DEVARAJA ACHARYA, Consultant in Anaesthesia and Critical Care, St Albans City Hospital, United Kingdom CORRESPONDENCE: DR HARSHAL WAGH, Registrar, Dept of Anaesthesia, Level I, St Julians Ward, St Albans City Hospital, St Albans, UK, AL3 5PN Email: drhdw@hotmail.com
References
Prevention of ventilator-associated pneumonia: consultation NICE, Sept 2007
Eggimann P, Pittet D. Infection control in the ICU. Chest 2001; 120: 2059-93
Weber DJ, Raasch R, Rutala WA. Nosocomial infections in the ICU: the growing importance of antibiotic-resistant pathogens. Chest 1999; 115: 34S-41S
Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in medical intensive care units in the United States. National Nosocomial infections Surveillance System.Crtic Care Med.1999 May; 27950: 887-92
The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee 1995.
Legras A, Malvy D, Quinioux AI, et al. Nosocomial Infections: prospective survey of incidence in five French intensive care units. Intensive Care Med.1998; 24: 1040-1046.
Urli T, Perone G, Acquarolo A, Zappa S, Antonini B, Ciani A. Surveillance of infections acquired in intensive care: usefulness in clinical practise. J Hosp Infect. 2002; 52: 130-135
Heyland DK, Cook DJ, Griffith L, keenan SP, Brun-Buisson C; Canadian Critical Trials Group. The attributable morbidity and mortality of ventilator-associated pneumonia. Am J Respir Crit Care Med. 1999; 159:1249-1256
Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gilbert C. Nosocomial pneumonia and mortality among patients in intensive care units. JAMA 1996; 275:866-869.
Rello J, Quintana E, Ausina V, et al. Incidence, etiology and outcome of nosocomial pneumonia in mechanically ventilated patients. Chest, 1991; 100:439-444.
Jiménez P, Torres A, Rodriguez-roisin R, et.al. Incidence and etiology of pneumonia acquired during mechanical ventilation. Crit care Med.1998; 17:882-885.
Safdar N, Dezfulian C, Collard HR, Saint S. Clinical and economic consequences of ventilator-associated pneumonia; a systemic review.Crit Care Med.2005; 33:2184-2193
CDC. Guidelines for preventing Health -Care -Associated Pneumonia, 2003. Recommendation of the CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR 2004; 53(No.RR-3)
Nosocomial pneumonia: incidence, morbidity and mortality in the intubated-ventilated patient. Pittett 1994
Nosocomial viral ventilator-associated pneumonia in the intensive care unit: a prospective cohort study. Pfr Vincent 2005
Petersen IS, Aru A, SkØdt V, et al. Evaluation of pneumonia diagnosis in intensive care patients. Scand J infect Dis.1999; 31:299-303
Fagon JY, Chastre J, Hance AJ, Domart Y, Trouillet JL, Gilbert C. Evaluation of clinical judgement in the identification and treatment of nosocomial pneumonia in ventilated patients.Chest.1993; 103:547-553
American Thoracic Society; Infectious diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med.2005; 171:388-416.
Rouby JJ, Martin De Lassale E, Poete P, et al. Nosocomial bronchopneumonia in the critically ill: histologic and bacteriologic aspects. Am Rev Respir Dis.1992; 146:1059-1066.
Fabregas N, Torres A, El-Ebiary M, et al. Histopathologic and microbiologic aspects of ventilator-associated pneumonia. Anaesthesiology.1996; 84:760-761
Pingleton SK, Fagon JY, Leeper KV Jr. Patient selection for clinical investigation of ventilator-associated pneumonia: criteria for evaluating diagnostic techniques. Chest 1990; 97:170-81.
Niederman MS,Craven DE, Fein AM, Schultz DE. Pneumonia in the critically ill hospitalised patient. Chest 1990; 97:170-81.
Kollef MH, Silver P,Murphy DM, Trovillion E. The effect of late-onset ventilator-associated pneumonia in determining patient mortality. Chest 1995; 108:1655-62.
Rello J, ausina V, Ricart M, Castella J, Prats G. Impact of previous antimicrobial therapy on the therapy on the etiology and outcome of ventilator-associated pneumonia. Chest 1993; 104:1230-5.
Craven DE, Steger KA. Epidemiology of nosocomial pneumonia: new perspectives on an old disease. Chest 1995; 108: Suppl: 1S-16S.
Kollef M. Current concepts - the prevention of VAP. NEJM 340; 8:627-634.
Tablan OC, Anderson LJ, Arden NH, Breiman RF, Butler JC, Mcneil MM. Guideline for prevention of nosocomial pneumonia: The Hospital Infection Control Practices Advisory Committee, Centres For Disease Control And Prevention.Infect Control Hosp Epidemiol 1998; 19:304
Rouby JJ, Laurent P, Gosnach M et al. Risk factors and clinical relevance of nosocomial maxillary sinusitis in the critically ill. Am J Respir Crit Care Med 1994; 150: 776-83
Valles J, Artigas A, Rello J et al. Continuous aspiration of subglottic secretions in preventing ventilator associated pneumonia. Ann Intern Med 1995; 122:179-86.
Crouch Brewer S, Wuderink RG, Jones CB, Leeper KV Jr. Ventilator-associated pneumonia due to Pseudomonas aeruginosa. Chest 1996; 109:1019-29
Goldman DA, Weinstein RA, Wenzel RP, et al. Strategies to prevent and control the emergence and spread of antimicrobial-resistant microorganisms in hospitals: a challenge to hospital leadership. JAMA 1996; 275:234-40.
Evans RS, Pestotnik SL, Classen DC, et al. A computer-assisted management programme for antibiotics and other anti-infective agents. N Engl J Med 1998; 338:232-8.
Herceg A.The decline of Haemophilus influenza type b disease in Australia.Commun Dis Intell 1997; 21:173-6.
Gross PA, Hermogenes AW, Sacks HS, Lau J, Levandowski RA. The efficacy of influenza vaccine in elderly persons: a meta analysis and review of literature. Ann Intern Med 1995; 123:518-27.
I I Siempos, K Z Vardakas, M E Falagas. Br J Anaesth 2008; 100(3): 299-306.
Technical patient safety solutions for Ventilator-associated pneumonia in adults. NICE August 2008
Photographic Documentation Of Open Fractures: A Survey Of Current Practice And Proposed Recommendations. R Ahmad, SKM Annamalai ,SMY Ahmed, SA Joseph And M Bould
The ‘Lost’ Mirena: What Investigations Are Required ? An Intraperitoneal Levonorgestrel-Releasing Intrauterine System Following Uterine Perforation: Case Report Shambhu S And Pappas M
An Unusual Presentation Of Left Ventricular Free Wall Rupture Following A Silent Myocardial Infarction Andrew Peter Vanezis, Rehan Quadery, Mohammad Wasil And Mohammed Azher
Mal-Distribution Of Medical Manpower Resultant Decay Of The Indian Medical Education System: Existing Problems And Possible Solutions Vallyamma P, Deshpande SR And Gayathree L
Chest radiographs are one of the most common radiological procedures performed in medical practice. The chest radiograph should ideally include views of the heart, lungs, trachea, mediastinum, bones of the chest and upper part of the abdomen. Chest radiographs are normally taken in the posterior-anterior (PA) view with the patient in upright / standing position but for patients admitted in the intensive care unit (ICU) or other emergency situations, this is not possible and so they are taken in the supine (anterior-posterior views) or semi-erect position.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In this article, we aim to discuss and compare the normal and abnormal positions of both the endotracheal tube (ETT) and nasogastric tube (NG) on chest radiographs.
Endotracheal tube (ETT):
Endotracheal tubes are used to secure the patients airway. Modern ETTs have a radio-opaque line running along their length which enables us to determine their position on chest radiographs 1.
Clinical methods 2 that can be used to determine the appropriate position of the ETT include:
Symmetrical rise and fall of the chest wall with each breath (on inspection and palpation of the chest).
Auscultation of the lung fields
Use of capnography
However, clinical methods cannot confirm how high or low the ETT is situated in the trachea. This can be confirmed by chest radiography. Optimum position of the ETT is required to ensure ventilation of both lungs.
A correctly positioned ETT lies in the mid trachea and its tip is approximately 5-7 cm above the carina 3 as seen in Fig: 1 (CR-1827).
In Fig: 2 (CR-1820), the tip of the ETT is low lying and is at the origin of the right main bronchus. Further migration of the ETT will result in right sided endobronchial intubation and collapse of the left lung. This will result in decreased oxygen saturation values (SpO2) on a pulse oximeter and low arterial partial pressure of oxygen (PaO2) on analysis of an arterial blood gas specimen.
Nasogastric tube (NG):
Nasogastric tube (NG) or orogastric tube (OG) is inserted for providing enteral nutrition, administration of drugs or for gastric drainage. NG feeding is a common practice in all age groups. There is a risk that the NG feeding tube can be misplaced into the lungs during insertion or may move out of the stomach at a later stage.
In the past, various methods 4 have been used to determine the position of NG feeding tubes.
These included:
Auscultation of air insufflated through the feeding tube - whoosh test
Testing acidity/alkalinity of the aspirate using blue litmus paper
Interpreting absence of respiratory distress as an indicator of correct positioning
Monitoring bubbling at the end of the NG tube
Observing the appearance of the feeding tube aspirate
The National Patient Safety Agency (NPSA) have issued a patient safety alert and have recommended that the above methods are not reliable and therefore should not be used to detect the position of NG tubes.
The NPSA recommend 5:
Measuring the pH of the aspirate using pH indicator strips/paper
Use of radiography
The most accurate method for confirming the correct position of a NG feeding tube is radiography 5.
The pH of the gastric aspirate can be affected by ongoing enteral feeding and medications viz: antacids, H2 antagonists and proton pump inhibitors. In these cases, measuring the pH of the aspirate may not be useful and so use of radiography is recommended. The NPSA have issued guidance on how to confirm the position of nasogastric feeding tubes.
Fig: 3 (CR-1822) indicates the normal position of the NG tip below the diaphragm in the upper part of the stomach (fundus).
Fig: 4 (CR-1826) shows the abnormal position of the NG tube situated in the right lower lobe bronchus. If NG feeds are commenced, this will result in lung injury.
Conclusion
We have highlighted the optimum position of both the ETT and NG tube on chest radiographs. Optimum positioning is required not only for safety reasons to avoid complications but also for optimum monitoring and treatment of patients. This series of chest radiographs will benefit not only medical students and doctors from all specialties but also nurses, physiotherapists and paramedical teams who will be involved in the care of critically ill patients.
Self Assessment
MCQ 1:
On a chest radiograph, the tip of the ETT:
a. should lie very close to carina
b. should lie 5-7 cm above the carina
c. should lie 5-7 mm above the carina
d. The ETT cannot be visualised on a chest radiograph
MCQ 2:
Which one of the following tests is the most accurate method to determine the correct position of NG feeding tubes?
a. testing the aspirate from the NG tube using a blue litmus paper
b. whoosh test
c. measuring the pH using pH indicator strips/paper
d. radiography
Answers for MCQs:
MCQ 1: b
MCQ 2: d
ACKNOWLEDGEMENTS
We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Bedford Hospital NHS Trust, UK
DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK
CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Bedford Hospital, Bedford, UK
Email: drkrishnanmr@gmail.com
References
Tracheal and tracheostomy tubes and airways. In: Al-Shaikh B and Stacey S eds. Essentials of anaesthetic equipment. 2nd edition. Churchill Livingstone, 2002: 56-67.
Hutton P. Airway management II: assessment, control and problems. In: Hutton P, Cooper GM, James III FM and Butterworth J eds. Fundamental Principles and Practice of Anaesthesia. Martin Dunitz Ltd, 2002; 79.
Goodman LR. The postoperative and critically ill patient. In: Grainger RG and Allison DJ eds. Diagnostic Radiology. 2nd edition. Churchill Livingstone, 1992; 368.
Reducing the harm caused by misplaced nasogastric feeding tubes. Patient safety alert National Patient Safety Agency (NPSA)
How to confirm the correct position of nasogastric feeding tubes in infants, children and adults National Patient Safety Agency (NPSA), Interim advice for healthcare staff, February 2005.
CAMBRIDGE CONFERENCE ON BREAST CANCER IMAGING March 23-24, 2009 Contact: Hampton Medical Conferences, Secretariat Tel: 011-44-20-8979-8300 Fax: 011-44-20-8979-6700 Email: hmc@hamptonmedical.com Website: www.cambridgeconferencebci.ukevents.org Radiology/Imaging, United Kingdom / Cambridge
2009 ANNUAL MEETING OF THE BRITISH SOCIETY OF GASTROENTEROLOGY March 23-26, 2009 Contact: British Society of Gastroenterology Tel: 011-44-207-387-3534 Fax: 011-44-207-487-3734 Email: bsg@mailbox.ulcc.ac.uk Website: www.bsg.org.uk/meet_calendar/calendar.htm Gastroenterology United Kingdom / Glasgow
BASIC PRACTICAL SKILLS IN OBSTETRICS & GYNAECOLOGY March 23-25, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Obstetrics/Gynecology United Kingdom / London
OESOPHAGO-GASTRIC CANCER SURGERY March 23-25, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6328 Email: general@rcseg.ac.uk Website: www.rcseng.ac.uk Oncology / Surgery United Kingdom / London
SPECIALTY SKILLS IN BREAST DISEASE MANAGEMENT (ADVANCED) March 23-26, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: breast@rcseng.ac.uk Website: www.rcseng.ac.uk Plastic Surgery / Surgery United Kingdom / London
CHILD HEALTH PROMOTION & SURVEILLANCE March 23-25, 2009 Contact: Symposium Office, Imperial College of London Tel: 011-44-20-7594-2150 Fax: 011-44-20-7594-2155 Email: sympreg@imperial.ac.uk Website: www.prossl.com/symposiassl/events.asp Pediatrics United Kingdom / London
2009 EUROPEAN ASSOCIATION FOR THE STUDY OF DIABETES (EASD) ROBERT TURNER CLINICAL RESEARCH COURSE March 23-27, 2009 Contact: EASD Secretariat Tel: 011-49-211-758-4690 Fax: 011-49-211-758-46929 Email: secretariat@easd.org Website: www.easd.org Endocrinology United Kingdom / Oxford
ROYAL COLLEGE OF PHYSICIANS - RESPIRATORY FAILURE March 24, 2009 Contact: Royal College of Physicians Tel: 011-44-20-7935-1174 Email: conferences@rcplondon.ac.uk Website: www.rcplondon.ac.uk/event Respirology, United Kingdom / London
5TH ANNUAL BRITISH COSMETIC DERMATOLOGY GROUP COURSE March 26-27, 2009 Contact: Rebecca Bennett Email: Rebecca_L_Bennett@btopenworld.com Website: www.bad.org.uk Dermatology United Kingdom / London
IDENTIFYING T CELL SUBSET PHENOTYPE AND FUNCTION IN PARASITE INFECTIONS. March 27, 2009 Contact: EuroSciCon Email: enquiries@euroscicon.com Website: www.euroscicon.com Infectious Disease / Other Specialties United Kingdom / Welwyn Garden City United Kingdom / London
ANNUAL SCIENTIFIC MEETING OF BRITISH SOCIETY FOR INVESTIGATIVE DERMATOLOGY (BSID March 30-April 01, 2009 Contact: Dr. Graham Ogg, BSID Chairman Tel: 011-44-1865-222-334 Fax: 011-44-1865-222-502 Email: graham.ogg@ndm.ox.ac.uk Website: www.bsid.org.uk Dermatology United Kingdom / Cirencester
164TH MEETING OF THE SOCIETY FOR GENERAL MICROBIOLOGY March 30-April 03, 2009 Contact: Josiane Dunn, Meetings Administrator Tel: 011-44-118-988-1805 Fax: 011-44-118-988-5656 Email: meetings@sgm.ac.uk Website: www.sgm.ac.uk/meetings Hematology / Infectious Disease / Other Specialties United Kingdom / Harrogate
2009 ANNUAL MEETING OF THE BRITISH PAIN SOCIETY March 31-April 03, 2009 . Contact: The British Pain Society Tel: 011-44-207-269-7840 Fax: 011-44-207-831-0859 Email: info@britishpainsociety.org Website: www.britishpainsociety.org Pain Management United Kingdom / London
9TH LONDON INTERNATIONAL EATING DISORDERS CONFERENCE March 31-April 02, 2009 Contact: MA Healthcare Events Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Website: www.mahealthcareevents.co.uk Family Medicine / General Medicine / Pediatrics / Psychiatry United Kingdom / London
ROYAL COLLEGE OF PHYSICIANS - ACUTE MEDICINE April 01, 2009 Contact: Royal College of Physicians Tel: 011-44-20-7935-1174 Email: conferences@rcplondon.ac.uk Website: www.rcplondon.ac.uk/event General Medicine / Internal Medicine United Kingdom / London
UROLOGICAL ANATOMY FOR SURGERY April 03, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: urology@rcseng.ac.uk Website: www.rcseng.ac.uk Surgery / Urology United Kingdom / London
UK RADIATION ONCOLOGY CONFERENCE (UKRO) April 06-08, 2009 Contact: UKRO Secretariat Tel: 011-44-1904-610-821 Fax: 011-44-1904-612-279 Email: ukro@ipem.ac.ukWebsite: www.ukro.org.uk Oncology / Radiology/Imaging United Kingdom / Cardiff
OTOLARYNGOLOGY FOR GENERAL PRACTITIONERS April 07, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6336 Email: ent@rcseng.ac.uk Website: www.rcsengac.uk General Medicine United Kingdom / London
EUROPEAN PSYCHIATRIC ASSOCIATION SECTION OF NEUROIMAGING 5TH ANNUAL MEETING: GENES, BRAIN, BEHAVIOUR April 09-10, 2009 Contact: Institute of Psychiatry, King's College London Tel: 011-44-20-7836-5454 Email: epaneuroimaging2009@iop.kcl.ac.uk Website: www.iop.kcl.ac.uk Psychiatry United Kingdom / Edinburgh
BASIC PRACTICAL SKILLS IN OBSTETRICS & GYNAECOLOGY April 15-17, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Obstetrics/Gynecology United Kingdom / London
PROMPT (PRACTICAL OBSTETRICS MULTI-PROFESSIONAL TRAINING) COURSE: TRAINING THE TRAINERS April 16, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Obstetrics/Gynecology United Kingdom / London
DRAWING FOR SURGEONS April 16-17, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6337 Email: drawingforsurgeons@rcseng.ac.uk Website: www.rcseng.ac.uk Surgery United Kingdom / London
PROMPT (PRACTICAL OBSTETRICS MULTI-PROFESSIONAL TRAINING) COURSE: TRAINING THE TRAINERS April 17, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Obstetrics/Gynecology United Kingdom / London
2009 ANNUAL MEETING OF THE RENAL ASSOCIATION April 20-24, 2009 Contact: The British Pain Society Tel: 011-44-207-269-7840 Fax: 011-44-207-831-0859 Email: info@britishpainsociety.org Website: www.britishpainsociety.org Nephrology United Kingdom / Liverpool
3RD NATIONAL CONFERENCE: TREATING SCHIZOPHRENIA April 27-28, 2009 Contact: MA Healthcare Events Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Website: www.mahealthcareevents.co.uk Psychiatry United Kingdom / London
RHEUMATOLOGY 2009 April 28-May 01, 2009 Contact: Louis Bellintani, Education and Events Officer Tel: 011-44-20-7842-0913 Fax: 011-44-20-7842-0914 Email: conferences@rheumatology.org.uk Website: www.bsrconference.org.uk Rheumatology United Kingdom / Glasgow
OPERATIVE SKILLS IN NEUROSURGERY April 28-30, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6336 Email: neurosurgery@rcseng.ac.uk Website: www.rcseng.ac.uk Neurology / Surgery United Kingdom / London
2009 PATIENT SAFETY CONGRESS April 30-May 01, 2009 Contact: Customer Service Team Tel: 011-44-207-554-5800 Email: psc2009@emap.com Website: www.patientsafetycongress.co.uk Other Specialties United Kingdom / Birmingham
ROYAL COLLEGE OF PHYSICIANS - DEVICE THERAPY FOR HEART FAILURE April 30, 2009 Contact: Royal College of Physicians Tel: 011-44-20-7935-1174 Email: conferences@rcplondon.ac.uk Website: www.rcplondon.ac.uk/event Cardiology United Kingdom / London
RISK MANAGEMENT AND MEDICO-LEGAL ISSUES IN WOMEN'S HEALTH May 06-07, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Legal/Ethics / Obstetrics/Gynecology United Kingdom / London
SPECIALTY SKILLS IN ONCOPLASTIC & BREAST RECONSTRUCTION SURGERY (ST 5-7) May 06-07, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6332 Email: breast@rcseng.ac.uk Website: www.rcseng.ac.uk Plastic Surgery / Surgery United Kingdom / London
ROYAL COLLEGE OF PHYSICIANS - NEUROLOGY ON ACUTE TAKE May 07, 2009 Contact: Royal College of Physicians Tel: 011-44-20-7935-1174 Email: conferences@rcplondon.ac.uk Website: www.rcplondon.ac.uk/event Neurology United Kingdom / London
THEORETICAL ATSM COURSE IN LAPAROSCOPY SURGERY May 08, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Obstetrics/Gynecology United Kingdom / London
URODYNAMICS ATSM COURSE May 11-12, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772- 6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetingsObstetrics/Gynecology / Urology United Kingdom / London
EMERGENCY SKILLS IN MAXILLOFACIAL SURGERY May 11-12, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: maxfac@rcseng.ac.uk Website: www.rcseng.ac.uk Emergency Medicine / Surgery United Kingdom / London
OPERATIVE SKILLS IN EAR, NOSE & THROAT SURGERY May 13-14, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6336 Email: ent@rcseng.ac.uk Website: www.rcseng.ac.uk Otolaryngology / Surgery United Kingdom / London
GP REFRESHER COURSE May 13-15, 2009 Contact: Symposium Office, Imperial College London Tel: 011-44-20-7594-2150 Fax: 011-44-20-7594-2155 Email: sympreg@imperial.ac.uk Website: www.prossl.com/symposiassl/events.asp Family Medicine / General Medicine United Kingdom / London
BIOLOGICAL & PHARMACOLOGICAL ASPECTS OF PERINATAL PSYCHIATRY May 14, 2009 Contact: Institute of Psychiatry, King's College London Tel: 011-44-20-7836-5454 Email: available through website Website: www.iop.kcl.ac.uk Psychiatry United Kingdom / London
ROYAL COLLEGE OF PHYSICIANS - ACUTE AND GENERAL MEDICINE FOR THE PHYSICIAN May 20-21, 2009 Contact: Royal College of Physicians Tel: 011-44-20-7935-1174 Email: conferences@rcplondon.ac.uk Website: www.rcplondon.ac.uk/event General Medicine United Kingdom / Birmingham
OBSTETRIC ANAESTHESIA 2009 May 20-22, 2009 . Contact: Meeting Secretariat Tel: 011-44-2-087-411-311 Fax: 011-44-2-087-410-611 Website: www.oaa-anaes.ac.uk Anesthesiology / Obstetrics/Gynecology United Kingdom / Jersey
FORENSIC GYNAECOLOGY May 21-22, 2009 Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Legal/Ethics / Obstetrics/Gynecology United Kingdom / London
INFECTIOUS DISEASES: ADULT ISSUES IN THE OUTPATIENT AND INPATIENT SETTING LONDON TO IRELAND CRUISE May 24-29, 2009 Contact: MCE Conferences Tel: 888-533-9031 Fax: 858-777-5588 Email: info@mceconferences.com Website: www.mceconferences.com Family Medicine / Internal Medicine United Kingdom / London
BASIC PRACTICAL SKILLS IN OBSTETRICS & GYNAECOLOGY May 26-28, 2009 Contact: Conference Office, Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings Obstetrics/Gynecology United Kingdom / London
ENDOSCOPIC SUTURING TECHNIQUES May 27-28, 2009 Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6337 Email: MIS@rcseng.ac.uk Website: www.rcseng.ac.uk Surgery United Kingdom / London
CURRENT ISSUES IN SEXUAL HEALTH May 28-29, 2009 Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk Infectious Disease United Kingdom / London
PROGRESS IN STEM CELL BIOLOGY May 29, 2009 . Contact: EuroSciCon Email: enquiries@euroscicon.com Website: www.euroscicon.com Biochemistry / Hematology United Kingdom / Welwyn Garden City
For generations the mind has been mystifying physicians all around the world. It is the powerhouse behind everything we do, and everything that we are therefore there is no wonder that reams of time, research, money and effort has been poured into this1.
The Association of British Neurologist, through various publications in the last 10years, has stated that there are too few neurologist consultants, and that provisions need to be made to ensure that there is comprehensive care to patients in hospitals2. In light of this there has been a recent drive into increasing the number of clinical consultant posts in local hospitals. This drive has lead to more innovative measures being implemented in this field, including new research on pharmaceuticals as well as introduction of new technologies.
A general misconception of the field of Neurology by medical students is that it is too complicated3. However, I found my experience to be one of the most organised, patient orientated, enjoyable experiences I have encountered on a ward setting. The teaching sessions that accompanied the firm brought all of the previous years of knowledge together like a solved jigsaw puzzle linking the neuroanatomy with the pathophysiology of an illness and the role and impact pharmaceuticals have4. With everything falling into place and having a better understanding, it gave me more confidence to explore further into this field.
Having previously only had brief exposure to Neurology, to be in a committed arena focused on this speciality was a daunting experience. Opposed to other specialities, where history taking is the millstone to your diagnosis, management and follow-up care, there is a much bigger onus on clinical skills and interpreting findings. The obvious signs of loss of sensory or motor functions are evident, but more subtle focal lesions are sometimes harder to pick up, this is when drawing on your clinical knowledge and application is required. This remains one of the evident advantages to Neurology, compared to other disciplines - that it remains clinically orientated. There is only so much that could be galvanised from a case history. As medical students we had ample exposure to the ward, and were able to approach patients and hone in on our clinical skills. As our basic knowledge had been laid down, through teaching sessions and also clinical case studies, we had the theory behind many of the clinical assessments, but lacked confidence and appropriate patients to assess. This changed as we integrated ourselves with the close-knit multidisciplinary team and the patients. There seemed to be buoyancy in mood, as we became more proficient undertaking assessments, for instance a cranial nerve examination that once took 10minutes to carry out was halved, without feeling like we had missed anything vital out.
More so, it was an eye-opener to experience, (even for a brief period), the sub-specialities that Neurology caters for, an aspect that I particular enjoyed was neuropsychiatry. Essentially the brain is an intricate piece of machinery, as with all things in life, sometimes this goes awry. For me to observe from a clinicians point of view and come to the same conclusion as my peers, gave me a sense of pride, knowing that I was moving in the right direction in my medical career, and that all that pent up knowledge was at last being implemented on a practical level. Unlike other fields, for the most part we were left to our own devices we were not spoon fed. This was refreshing, although a little overwhelming at first. We were responsible to find, clerk, assess and present patients to our team-members. The feedback we received was invaluable; it illustrated the extent of our competency and also left you with a sense of achievement knowing that you are capable and apt.
For those that are looking for a speciality once they have started their medical career, Neurology is an exciting and innovative place to be at right now. With an aging population worldwide, more effort, resources and money is being spent on degenerative illnesses such as Alzheimers disease and Parkinsons disease.5
Although to some extent current treatments offer benefits to sufferers, there is hope that new pioneering forms of treatment will be developed to manage patients. Additionally this gives students and qualified peers alike a great opportunity to conduct research and audits and get the opportunity to be published. Neurology still remains a minefield of the unknown, and it seems to be constantly on a quest to better itself and find new measures and treatments to bring to the patients.
With its new advancements in the pipeline, Neurology seems to have a bright future. However, there is the obvious downside to being in a speciality of this nature. You will come into contact with a large number of patients with untreatable disorders. It needs someone with a strong constitution to see someone that has a poor prognosis and an almost certain decrease in quality of life. For some, there will be an obvious deterioration before your eyes, others may have already suffered severe neurological deficits that ethical questions on the continuation of the life may arise. These are tough decisions to make, and needs someone with conviction and strong-will to stand by their decision.
Overall Neurology is what you make it, as is every profession. What stands out with Neurology is the exposure you get to patients. For students this is a valuable and undoubtedly crucial time in their medical training to perfect skills that will be called on in the future. Where else would we find another welcoming and encouraging place to learn the tools of our future trade, that allows freedom to learn, exposure to patients, a myriad of different diagnosis, and most importantly a practical use of your knowledge and clinical skills?
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
MATHAVI UTHAYANAN and MASHUD SOUROYER, 4th Year Medical Students reading at the Barts and London School of Medicine and Dentistry
Indian medical education system has seen rapid growth in the last two decades. From a miniscule number, private medical colleges have grown to account for more than half of the 270 medical colleges in 2008 and consequently, India has the highest number of medical educators in the world. This unregulated unequal growth brings two issues to focus: the failing quality of medical education and implementing effective solutions to address an artificial faulty shortage due to doctor mal-distribution. The menace posed by the growing merchandisation of medical education has to be warded off and efforts should be made to ensure maintenance of standards and check the unplanned growth of substandard medical colleges and substandard education norms in universities or their constituent medical colleges. There is a strong case for a review of the entire system of medical education and examinations in the country. Some solutions like increasing retirement ages of MD faculty to 70 years, sharing of faculty, increasing MD seats, allowing clinical MDs to teach paraclinical and preclinical subjects or temporary merger of specialities have been proposed to address the faculty shortage instead of relying on inadequately qualified MSc non-medical faculty.
Keywords: Qualified Medical teacher, India, medical colleges, faculty shortage, Medical Council of India (MCI).Abbreviations DCI=Dental Council of India. MSc=Master of Science
Establishing a medical college is not similar to establishing a science or Arts College and apart from a huge capital requires a huge number of qualified, competent, MCI compliant manpower to produce quality doctors.1,4,7 Having established a Medical College, maintaining the standards of education to world acceptable levels with a vision to serve poor Indian masses has been a concern of the Indian planning committees. Also, the good name a college attains is due to the accomplishments of its faculty and alumni. In that regard, proper emphasis on the quality of medical education ,inspite of the recent rapid proliferation of private medical colleges, has rightly been the working domain of Medical Councils all over the country and has consumed energies of Medical Council of India over the last forty years. 1, 4, 7,10,12
The Medical Council of India (MCI), the regulatory and advisory body on medical education, approves medical curricula and permits medical school existence and allows for recognition of medical degrees issued by various universities. The accreditation process for medical schools focuses largely on the infrastructure and human resources required and little on the process and quality of education or outcomes.15 The implementation of the recommendations of MCI regarding recognition or de-recognition of a medical college is governed by the Ministry of Health and Family Welfare, whilst individual universities also have variable sets of regulations for their affiliated medical schools. As a result, there is no uniformity in the standard of medical education across the country. At the time of independence there were just 19 medical schools with an output of 1200 doctors.10 In 1965, there were 86 medical colleges in India with only a few private colleges7 The college total increased to 112 by 1980(at a rate of 30%), to 143 in next decade (rate of growth of 28%) and since 1990 over past 18 years the number has increased to 271, an increase of ~90% compared with the figure in 1990.7 Today, there are 271 medical colleges out of which about 31,000 medical graduates pass out every year and private sector medical colleges have grown to account for more than half of all medical education institutions in India 13
Evidently, medical education system seems to have had an unregulated growth over the last two decades. It has been pointed out that even the prestigious colleges window dress faculty lists or put up names of non-existing academic members in their staff list. 5 Most medical college permissions were gifts given out as largesse or patronage to political heavyweights from health ministry.1,14 Very few have had adequate space, laboratories or hospitals as per MCI norms. They were and remain ill- equipped and inadequately staffed.10 This unregulated rapid growth in enrolment of medical students and poorly implemented regulations relating to admissions, faculty strength and infrastructure in medical colleges adversely impacts quality of training in Indias medical institutions.
Many reputed physicians and surgeons, professors, directors and deans working in new private medical colleges fabricate and falsify records like even birth records and lie to the MCI and the courts in order to get their medical college of questionable standards approved or recognized. Illegal money is involved in the business of getting new private medical colleges approved or recognized by the MCI and the health ministry. The decay of medical colleges reflects the general trend in this country .4,5 Corruption and bribery have made permanent inroads into medical education since past few decades in health universities or entrance examinations. Even clerks in the universities leak question papers and manipulate marks. 1 Perhaps the worst kind of gross unethical practice in academic medicine happens around the time of inspection by the Medical Council of India (MCI) post 1998-2000, in new private medical colleges. In emergency-like frenzied two day shows, busloads of patients are mobilized to fill up empty wards, carloads of doctors are paraded before the inspectors, and even instruments are hired or shifted between colleges, during the period of MCI inspections.4
Privatization in general has been known to increase the gap between rich and poor, amounting to encouraging survival of the richest which cannot be a acceptable goal of any civil society.8 And, the policy of excessive privatization of medical care delivery system has undermined health services and further limited the access of the underprivileged.3,8
Privately, many managements agree that it is very difficult to get faculty and that it is even more difficult to retain them in the wake of continuous offers or lure from newly established medical colleges. Certain medical college locations in smaller cities or semi-urban areas do not have facilities, ambience, or charm of big cities hence attracting teachers or other qualified staff to such medical colleges has been difficult, and various inducements have been applied. Such colleges have been surviving council inspections by window dressing or luring faculty with money. In certain new colleges which are literally brick fresh, bereft of hostel or quarters or other amenities the teachers delay even more to move or settle down themselves. At times doubts are established whether an impossible set of conditions and heavy financial burden is imposed on Medical college managements, by the MCI just to make management fail MCI inspections, but at the same time, some stringent MCI regulations have helped faculty of Medical colleges by ensuring job availability.
Doubling of medical colleges over last 15 years has improved the number of medical practitioners in India, but will the mere increased numbers mean a higher quality health care delivery system is debatable. Most management fail to fulfill the excellent set of norms stipulated by Medical Council of India. It is worthwhile, in national interest to note that, we have been loosing medically qualified post graduates to Western countries since till recently Medical College teaching jobs were low paid and did not give that richness or respect attained by private practitioners. After the Karnataka Government & Pondicherry scales new implementation in 2007, with a heavy Non Practicing allowance teaching profession has gained respectability vis--vis elite in society like software engineers. Similar uniform pay scale implementation is need of the hour, all over the country to prevent medical teacher mass migrations.
Nearly 27000 teachers are required as per Ananthakrishnans calculations 7 to fill the faculty positions in 270 medical colleges purely for the purpose of teaching MBBS.He ignores the existence of ~300 Diplomate National Board hospitals across India and requirement of faculty for DNB courses. He also ignores MCI recognized institutions exist in other countries like China, Nepal, Malaysia, Netherlands and have been training MBBS doctors of Indian origin. All these institutions have been drawing medical teachers to satisfy MCI or DNB stipulations for accreditation. Hence we have to account loosing faculty to such Institutions. Also his manpower calculations are only for colleges purely teaching MBBS and ignore multiple course Colleges like KMC Mangalore, Manipal which harbor 90 MSc students per year per department and ignores existence of PhD students which evidently will require more teachers. He also ignores the net strain on the same faculty who are simultaneously teaching BPT, MPT, etc in allied institutions. A great academic strain on medical college teachers ,exists,which has never been accounted by MCI nor by Dr Ananthakrishnan.So, on the whole, it means that a great qualified medical teacher shortage exists in India. Either it is due to the excessive number of courses imposed on the same faculty or maybe it is inefficient use of existing qualified medical teachers for non teaching purposes.
Contrary to the opinion of Health ministry, eminent educationists Sood & Adkoli point out that the doctor: population ratio has already exceeded that required by the country and there is mal-distribution of their services. They feel that the menace posed by the growing merchandisation of medical education has to be warded off and efforts should be made to ensure maintenance of standards and check the unplanned growth of substandard medical colleges and substandard education norms in universities or their constituent medical colleges. This mal-distribution of medical manpower is the centered on biased political will and seat purchasing power in the community. With the correction of medical manpower maldisditribution medical standards will harmonize throughout India.11,12
Indeed, given the sharp increase in the number of medical colleges and the doubling of enrolment capacity after1980s it is difficult to imagine that enough trained full-time faculty exist to adequately staff the newly created colleges or DNB Hospitals and maintain reasonable teacher-student ratios.9 Dr Ananthakrishnan proposes to allow MSc from Non Medical Universities to teach Medicine. 7 It will be gross medical impropriety to allow such injustice to be allowed by Medical council of India which is supposed to uphold medical education standards across India. What glory does it give Indian medical education system to have a bunch of unqualified non medical doctor MSc teachers seeking to run coaching medical classes a la science tuition centers we fail to see. What is the necessity to increase number of medical college, or medical college seats, in inadequacy of appropriate medical teachers? Is it possible to permit inadequately trained staff to run these colleges, and will the output reflect quality abroad? Emphasis here is not on excellent university results, these MSc teachers, produce by mere mugging up of unconnected facts or figures or excellent power point teaching but what MBBS educated teachers can produce by moulding young doctor student minds by bringing in relevant clinical experience.
Some Solutions
Today, India has the highest number of medical colleges in the world and consequently the highest number of medical teachers. Yet, shortage of medical faculty and lack of medically oriented teaching by appropriately trained MD faculty have tarnished Indian medical glory. The unprecedented institutional growth has created a national quality challenge for medical education and has resulted in varying standards across medical graduates. There is a national need for well-trained faculty who will help improve programs to produce quality graduates. 5,14 Annual student intake is said to be a critical factor in assessing the requirement for teachers as per Ananthakrishnan,7 and should dictate the employment. A punitive MCI, DNB Board and vigilant state medical councils can act synergistically to decrease medical student intake in Medical Institutions where teachers are not ready to go or do not exist. MCI and DNB Board also need to do more for its medical teachers- give them more respect, recognition, arrange for their pensions, gratuity, relieving orders or get involved in pay scale recommendations as no entity exists till date to safeguard medical teacher interests. Measures are required to ensure private medical colleges proper regulation by the medical council. Further, Indian Health ministry has been known to interfere in the functioning of MCI, DCI and DNB Boards, override MCI, DCI and supreme courts decisions and this is undesirable.12,14,15
Increasing the retirement age of MD teachers up to 70 years will harness hard earned medical experience of senior professors to guide preparation of efficient faculty and will reemploy retired teachers . This will also lead to discipline enforcement, more projects, PhDs and papers of relevance. Else, MCI can think of sharing of medical faculty among medical colleges, or dental colleges, and ensure less burdened teaching schedules. Implementing integrated medical education system-will help, as has been experimented in -KMC Manipal, Sri Ramachandra Medical College. Present paramedical system is a confused network of PhDs who have not enriched Medical education system, a proof of which can be the absence of a single Nobel laureate or international repute medical scientist or of the glory of IISc departments, in 270 odd medical colleges across India, even Manipal, or AIIMS in spite of having the system for 50 years. Merging of homogenous specialities like merging of biochemistry with physiology or pathology, microbiology with pathology, or creation of a discipline of laboratory medicine merging pathology, microbiology and biochemistry has been suggested in yahoo groups like mdbiochemists. Merging of homogenous specialities decreases the requirement of professors in biochemistry and microbiology by providing MCI norm requirements of professors from pathology. Also merging of Anatomy with Surgery will be worthwhile and achieve similar objective of providing deficient staff from Surgery department, who happen to be plenty. It is said to bring about some integrated medical education also. This cure is supposed to provide a broad based intermingling for net objective of efficient medical teaching by qualified professors, peers in interrelated departments. We would further extend their argument in suggesting that the proposed speciality merger need not be complete and final but a temporary arrangement for next 20 years.
Acute shortage of medical teachers needs to be filled. Appropriate solution exists within medical education system itself and help can come from recruitment of medical brethren from clinical sciences to fulfill non clinical department norms, as has been happening successfully ,silently ,without MCI approval ,in Tamilnadu and Andhra pradesh government medical colleges. A whole lot of MD or MS or DNB doctors are ready to serve as Medical teachers, but colleges have never used their teachership as MCI does not permit this. Many such part-time consultants who are practicing in community could deliver excellent teaching assignments and help tide over the so called artificial medical teaching crisis.MCIs generosity to allow MDs of homogenous specialties to teach in Pre or Para clinical sciences for a honoraria, rewards system will effectively ,in a short time solve inadequate improper medical staffing problems forever. Number of seats available in various post-graduate medical courses is approximately 11,005 annually which is one third of MBBS graduates coming out every year. Nearly a third of these seats are diplomas and a diplomate cannot be considered for even a junior lecturer post like an MSc graduate, but will be considered for post of Tutor, the lowest cadre of medical teachership. Thus all DCP (Diploma in Clinical Pathology) and DFM (Diploma in Forensic Medicine) loose out Lecturership to their MD colleagues. Increasing the number of MD seats in Para clinical and preclinical sciences and replacing existing Diploma seats with corresponding MD seats is a just approach and should be the right approach for MCI to follow, since in contrast to before 1960s,in present days no postgraduate seat goes vacant-it means there are no shortage of MD aspirants as wrongly assumed by Dr Ananthakrishnan7 .MCI also has to think of giving Junior lecturership posts to MBBS graduates who have been serving as tutors for more than 3 years in any department .
Continuing medical education
Thus there is a strong case for a review of the entire system of medical education and examinations in India. The American style of giving credits for demonstrable good performance throughout the years can be introduced. It will, of course, be necessary to ensure objective evidence of such assessment and performance.1,8 The Indian Health ministry has realized that efficient medically qualified teachers are in the best position to mould young physician minds hence, Indian National Knowledge Commission (NKC-2008) proposes raising average standards and creating centers of medical excellence, revised medical accreditation; methods of attracting and retaining talented medical faculty members and devising measures to ignite, promote and sustain the research tradition in medical colleges and teaching hospitals.
Medical teacher incentivisation8, i.e increments, promotions, paid study leaves will also attract good teachers to stable institutions. In order to recruit good and gifted medical teachers, it is necessary to provide them with regular attractive salaries, amenities and retirement benefits which are realistic and at least on par with the earnings of those in practice.2 Emigration of high quality physicians who could potentially serve as medical teachers in local Medical colleges may lead to further declines in the quality of medical graduates produced. To address regional inequities for medical training and related availability of doctors, firstly, it may be useful to set up adequately staffed medical research and training institutions in economically backward areas. Secondly, the government could subsidize the medical education of individuals living in backward areas, perhaps by combining such a subsidy with a bond to serve in the backward areas for a limited number of years. Implementing this bond system will be in the control of the health ministry.
For existing medical teachers, high standards of teaching are to be maintained and improved upon with constant seminars and workshops. Teaching aids, computers, medical CDs, DVDs, medical e-books, Internet facilities and availability of the latest journals and literature on the subject should be provided in every medical college or diploma national board certified hospital.2At the post graduate level, it is the duty of the senior teacher to train the young doctor so that he learns to perform according to accepted international standards.2 As a long- term policy, no new medical colleges must be permitted in prosperous states, unless they demonstrate an MCI compliant infrastructure and facilities better than those in existing institutions. A revitalized Medical Council of India must be the only agency permitted to recognize such colleges and health ministry need not have any role.1 Since advent of the MCI it has been noted that Indian health ministry can not only ignore a negative rating by Medical Council of India, but also openly defy the Supreme Court.12
India needs also a MCI controlled and Supreme Court monitored screening system of students admitted to medical colleges under the discretionary management quota so that merit remains the paramount criterion. This requires common entrance examinations to assess student performance across colleges, publicly accessible information on admission standards practiced by colleges, including transparent nondiscriminatory ranking by performance, and enforcement of sanctions on colleges violating norms. A useful first step is the government policy of maintaining a accessible list of recognized colleges, but obviously much more needs to be done to implement ways to increase the supply of MD teaching personnel .Indian policy makers need to think proactively about developing a cadre of doctors focused more on medical education and research. Lastly, the Indian Medical Association, Association of Medical Biochemists of India, All India MD/MS Doctors Association, and other national medical and dental professional bodies must play a greater role to foster true medical and dental education and prevent governmental and political interference.1,12,14
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR P VALLYAMMA MD, Professor & Head of Biochemistry, Periyaram Medical College, Kerala, India
DR SRINIVAS R DESHPANDE MD, Associate Professor in Biochemistry, Melmarvathur Adiparashakti Institute of Medical Sciences, Tamilnadu, India.
DR GAYATHREE L, MD, Assistant Professor in Microbiology, Hassan Institute of Medical Sciences, Hassan, Karnataka, India
CORRESPONDENCE: Dr P Vallyamma MD, Professor & Head of Biochemistry, Periyaram Medical College, Periyaram, Kannur Dt, Kerala, India
Email: aimdda@yahoo.com
References
Madhok P.Medical tuitions .Issues in Medical Ethics 1997; 5: 23
Chinoy R. F: Medical ethics: relationships between doctors.Ind J Med Ethics
Qadeer I: The real crisis in medical education. Ind J Med Ethics
Chattopadhyay S: Black money in white coats: whither medical ethics? Ind J Med Ethics ;Jan-Mar 2008(1)
Bansal P, Supe A. Training of medical teachers in India: Need for change. Indian J Med Sci [serial online] 2007 [cited 2008 Oct 1]; 61:478-84. Available from: http://www.indianjmedsci.org/text.asp?2007/61/8/478/32930
Nair KR :Medical college teachers and some ethical issues in Kerala .Ind J Med Ethics
Ananthakrishnan N: Acute shortage of teachers in medical colleges: Existing problems and possible solutions.NMJI Jan/Feb 2007: Vol 20, No 1:1-8.
Aggarwal A. Strengthening the health care system in India: Is privatization the only answer? Editorial. Indian J Community Med: April 2008; Vol 33; Isuue 2; 69-70.
Dutta R. Rash of medical colleges spawns corruption and mediocrity. Express Healthcare Management, August 2002
Richards T. Impressions of Medicine in India; Medical education in India-in poor health. British Medical Journal Volume 290; 13 April 1985;1132-34.
Sood R & Adkoli BV. Medical Education in India Problems and Prospects. Journal of Indian Academy of Clinical Medicine Vol. 1, No. 3; October-December 2000; 210-12.
Mahapatra D .Ramadoss nod to medical college despite SC no-Times of India National edition;29 Sep 2008, 0054 hrs IST, TNN.
India to recognize foreign medical degrees :an article published in India Chronicle a monthly e-newsletter Issue No 002;March 2008 http://indianembassy.ru
Rajeev D & Mahapatra D Did Ramadoss flout dental council norms?-Times of India National edition;30 Sep 2008, 0449 hrs IST, TNN
Sood R. Medical education in India ;Medical Teacher, Volume 30, Issue 6 2008 , pages 585 - 591
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) is a rare clinical syndrome, commonly seen in elderly patients who present with dorsal pitting edema of the hands and has a dramatic response to steroids, suggesting a benign nature. Sometimes it is associated with other rheumatologic conditions and potential underlying malignancy should be ruled out, especially when there is a poor response to steroids.
Elderly patients presenting with musculoskeletal symptoms such as painful, swollen or stiff jointsare challenging to physicians. The common conditions encountered are osteoarthritis, crystal arthropathies, spondyloarthropathies and rarely seropositive arthritis. RS3PE highlights a different inflammatory disease involving the tenosynovium of the tendons of the hands with a characteristic presentation. This case details such a presentation and aims to raise awareness amongst general physicians.
Case report:
An 83 year old man, with a history of chronic leg ulcers and poor mobility presented following a fall at home. On admission he also complained of a six to eight week history of bilateral hand swelling. This was of sudden onset, initially on the right hand and gradually progressed until the time of admission when it became prominent over the dorsum of both hands. Both hands were initially tender, but painfree at rest, and restricted in movement due to the swelling. Lately he had also noticed mild inactivity stiffness in his knees and shoulders, He had no previous musculoskeletal history, no skin rash or trauma to his hands.
Inspection of his hands revealed bilateral, symmetrical swelling, involving all the fingers and more pronounced on the dorsum. On palpation there was pitting oedema over the dorsum without signs of synovitis or joint deformity.(Figure 1 and 2).
On movement, finger flexion and opposition were limited, with reduced grip strength.
There was no girdle muscle weakness or pain. There was pitting oedema of both feet, with compression bandaging to the upper calf. This was chronic, and was likely to be secondary to peripheral vascular insufficiency.
Fig 1:Swollen hands
Fig 2: Dorsal pitting edema
Blood tests during this admission showed normocytic anaemia with low vitamin B12 levels but normal ferritin. Erythrocyte sedimentation rate (ESR) was raised at 100mm/hour and initial C-reactive protein (CRP) at 55 mg/l. Anti nuclear antibody (ANA) and rheumatoid factor were negative. X-rays of the hands revealed mild osteoarthrosis without any evidence of bony erosions. Computerised tomography (CT) of the chest and abdomen did not show any evidence of malignancy.
In view of the clinical presentation and seronegativity, a diagnosis of peritendinous rheumatoid arthritis was considered. He was commenced on low dose oral steroids following initial parenteral corticosteroid. Subsequent to the initiation of steroids, there was dramatic resolution of the swelling of the hands, within a week (Figure 3),
Fig 3: Response to steroids
Case discussion
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome was first described by McCarty et al in 1985 1 . It is also termed as peritendinous rheumatoid arthritis in Europe.
It predominantly affects elderly males and although not exceptionally rare, there is no clear documentation of the incidence of this condition (2).
The syndrome is a subset of symmetrical polyarthritis characterised by
Bilateral pitting oedema of both hands
Sudden onset of polyarthritis (A few cases report patients being able to state the time to the hour at which this occurred.1)
Age >50 years
Absence of rheumatoid factor (seronegativity).
Other features include symmetrical distal synovitis and tenosynovitis affecting the synovial sheaths of the flexor and extensor tendons of the hands and/or feet without evidence of joint erosions 2. It responds dramatically to corticosteroids with long term remission after withdrawal, suggesting a benign prognosis.
Although generally thought to be a characteristic benign syndrome with good outcomes, several studies have been published linking RS3PE to various rheumatic disorders such as spondyloathropathies, psoriasis (HLA associations), polymyalgia rheumatica, and temporal arteritis. 3 It may also be a paraneoplastic manifestation of haematological or solid malignancies 4 (eg. prostate, rectal, gastric and ovarian tumors) linked to the synthesis of interleukin, IL-6. Review of these cases suggested that RS3PE associated with neoplasia was associated with a poor response to steroid treatment. 4
Although MRI scanning offers the best imaging technique to diagnose the condition.,RS3PE is a clinical diagnosis. Scans typically demonstrate the tenosynovitis of the extensor tendons believed to cause the oedema which characterises the syndrome.3 MRIscans are valuable to exclude other bony pathologies like osteomyelitis.. An alternative imaging technique for identification of extensor tenosynovitis is ultrasonography. 5
Treatment generally involves steroids, but in some cases the patient may respond to NSAIDs or gold therapy
Learning points:
RS3PE should be considered as a diagnosis when a patient presents with bilateral symmetrical pitting oedema of the hands and or feet, and is found to be seronegative.
Patients are generally very responsive to corticosteroids.
A high index of suspicion is needed to search for underlying malignancy especially in the absence of associated rheumatic disorders and poor response to corticosteroid therapy.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. VIJAY JOSHI MD, Registrar, Internal Medicine, Chase Farm Hospital, UK
DR ANNA GREEN MBBS, FY1 Doctor, Chase Farm Hospital, UK
DR. JANE GRIFFIN FRCP, Consultant Rheumatologist, Chase Farm Hospital, UK
CORRESPONDENCE: DR. VIJAY JOSHI, Chase Farm Hospital, Enfield, UK
Mehmet Sayarlioglu Remitting Seronegative Symmetrical Synovitis with Pitting Edema (RS3PE) Syndrome and Malignancy. Eur J Gen Med 2004; 1(2): 3-5.
Oliveri I, Salvarani C,Cantini F. Remitting distal extremity swelling with pitting edema: a distinct syndrome or a clinical feature of different inflammatory rheumatic diseases.J.Rheumatol 1997;24:249-52
Sibilia J, Friess S, Schaeverbeke T et al. Remitting seronegative symmetrical synovitis with pitting edema (RS3PE): a form of paraneoplastic polyarthritis? J Rheumatol 1999;26:115-20
Agarwal et al . Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome: ultrasonography as a diagnostic tool. Clinical Rheumatology. Volume 25, Number 5/October 2005
Left ventricular free wall rupture is a serious complication of myocardial infarction (MI) with a mortality rate without intervention close to 100%. Its presentation is classically late following an MI but in some cases can present within 24 hours. There can be sudden overt clinical symptoms or it can present insidiously and therefore there must be a high index of suspicion. This report highlights the case of a gentleman with no prior history of ischaemic heart disease that presented with non-specific symptoms. A diagnosis of left ventricular (LV) free wall rupture near the atrial appendage, post MI was made and he was managed successfully.
Clinical Presentation
We present the case of a 75 year old gentleman who collapsed suddenly whilst riding his bicycle. According to an eye-witness he was unresponsive & confused for a few minutes after the episode. Paramedics attended and brought him to the Accident and Emergency department at a local hospital and he was subsequently transferred to the Admissions Unit. Initially he was confused with no recollection of the collapse however his confusion abated after a short period of time.
He was normally fit and well, his only past medical history of note being chronic neck pain requiring simple analgesia and mild asthma requiring when necessary salbutamol inhalers. He was however a life-long smoker with a minimal alcohol intake.
On arrival to the hospital, the patient was conscious, oriented, afebrile and not in any pain. His Glasgow Coma Scale (GCS) was 15/15, pulse was 92/min, regular but weak and the right radial and femoral pulses were absent. His systolic blood pressure was 55mmHg in the right arm and 105mmHg in the left arm. The only other positive finding on examination was muffled heart sounds. Bloods were taken and results are shown in Table 1 with normal ranges given for reference (results within normal limits are not shown).
Random Blood Glucose
16 mmol/l
<11.1 mmol/l
Troponin I (12 hour)
6.16 ng/ml
<0.04 ng/ml
WBC
14.0 x109/l
4-11 x109/l
CRP
179 mg/l
<10 mg/l
Hb
10.9 g/dl
13-18 g/dl (men)
Table 1. Blood results with normal ranges in italics.
In view of the high blood glucose and history of collapse, the patient was aggressively treated with insulin and intravenous fluids. However after receiving 2 litres of intravenous fluids, there was no haemodynamic response. An arterial blood gas on air was performed and the results are shown in Table 2 with normal ranges given for reference.
pH
7.40
(7.35-7.45))
pCO2
3.0 Kpa
(4.7-6.0 Kpa)
pO2
14.8 Kpa
(10.8-12.5 Kpa)
HCO3
13.6 mmol/l
(22-28 mmol/l)
Table 2. Arterial Blood Gas with normal ranges in italics.
A Chest X-ray was performed and showed nothing unusual. However an ECG demonstrated ST depression in the inferior leads & T- wave inversion with a Q wave in aVL (see figure 1). Differential diagnosis at this stage was therefore aortic dissection, carotid dissection and left ventricular wall rupture (post myocardial infarction).
A subsequent CT scan showed no aortic dissection, but probable haemopericardium together with an occluded right common iliac artery (see figure 2). Trans-thoracic echocardiogram confirmed haemopericardium with no suggestion of tamponade (see figure 3) and in addition demonstrated some mild LV diastolic dysfunction. CT scan of the brain and the carotids showed no evidence of carotid dissection but did indicate significant stenosis of the right subclavian artery. The diagnosis of left ventricular free wall rupture was made at this juncture. It was noted that the variability in blood pressure between both arms and between upper limbs and lower limbs was exacerbated by coincidental stenosis in the right common iliac and right subclavian arteries which possibly delayed diagnosis.
Subsequent coronary angiogram showed a blocked intermediate coronary artery (a branch of the left main coronary artery), 2 stenosed areas in the left anterior descending coronary artery (LAD) and a 50% occlusion of the right coronary artery (RCA). Later a trans-oesophageal echocardiogram (TOE) demonstrated separation of the ventricular free wall between the LAD artery and the left atrial appendage, high up in the heart a very unusual position indeed. The diagnosis of Left Ventricular Free Wall Rupture following a Silent Myocardial Infarction was therefore confirmed. The patient was transferred to a nearby cardiac surgery centre and an emergency patch repair of the ventricular free wall rupture was performed.
Figure 1. ECG demonstrating ST depression in II, III and aVL & T-wave inversion with a Q wave in aVL.
The patient had a prolonged recovery, spending 2 weeks on the Cardiac ICU and then subsequently developed hospital acquired pneumonia and remained an inpatient on a general medical ward for a further 4 weeks where he made slow progress. He later spent 4 weeks in a rehabilitation centre before finally returning home.
Figure 2. Thoracic CT with obvious haemopericardium.
Figure 3. Transthoracic echo with evidence of pericardial fluid.
Discussion
First described by William Harvey in 1647, left ventricular (LV) free wall rupture is a dramatic complication of myocardial infarction where there is a rupture of infarcted LV free wall tissue. The rupture is commonly insidious with bleeding into the pericardial sac and subsequent cardiac tamponade. It is hard to assess as clinical and autopsy results vary considerably. It contributes to nearly 15% of deaths due to acute MI1, with the average age of those affected being 69 years. It is third only to cardiogenic shock and arrhythmias as the leading cause of death following a myocardial infarction.2 Hutchins et al reviewed 153 post mortem results with gross and histological evidence of acute myocardial infarction and reported that 30.7% of patients in this group who had died from sudden death had a cardiac rupture.3 It is more common in females and classically occurs 3 to 6 days post MI, however in some studies, up to 50% of cases have been reported less than 24 hours post MI.4There is a history of previous MI in 25% cases but often LV free wall rupture can be the first presentation of ischaemic heart disease.5 Around 50% of the cases of LV free wall rupture are due to anterior MIs with LAD involvement.6There is a new murmur in 25% cases and echocardiography may often demonstrate a pericardial effusion. The prior use of NSAIDS and corticosteroids and a presentation which may mimic major artery dissection often delays thrombolytic therapy.
Unfortunately the current mortality rate in the UK is around 90%. Of note the incidence of LV free wall rupture post MI has increased since the more widespread availability of coronary care units and it is thought that this is because more people are now surviving the first few days post MI.7
The pathophysiological process involves thinning of the myocardial wall with the intensity of necrosis occurring at the terminal end of the vessel (watershed area) where there is often poor collateral flow. The shearing effect of myocardial contraction against a stiffened necrotic area causes rupture. The most common rupture location is on the anterior or lateral wall of the left ventricle.8 A midventricular position along the apex to base axis is most common. It can present either with sudden death or can present sub acutely e.g. with nausea, hypertension or pericardial type chest discomfort or pain. The gentleman discussed in this report collapsed with no preceding symptoms and as mentioned the location of his rupture was in a very unusual place, high up near the atrial appendage.
Transoesophageal echo (TOE) is diagnostic for this condition and is the gold standard.9 However it is found to have only a 70% sensitivity rate for LV free wall rupture10 and therefore some centres advocate the use of cardiac MRI when available.11 Initial management is haemodynamic stabilization and this is often followed by blood transfusion, pericardiocentesis12, inotropic support and the use of an intra-aortic balloon pump but ultimately prompt surgical repair is required.
Various surgical techniques have been applied including suturing of the infarcted ventricle but modern surgical repair involves the application of a Teflon felt patch over the ruptured area with a synthetic biocompatible glue (e.g. cyanoacrylate) as an adhesive to keep the patch attached to the epicardium.13,14 Crucially it can be performed without the use of cardiopulmonary bypass in most of cases. The current overall operative mortality for surgical intervention is reported to be around 24-35%15.
Ultimately survival depends on early recognition of the condition, prompt investigations & diagnosis and urgent surgical treatment. Unfortunately at the present time the condition is usually diagnosed at post-mortem.
Conclusion
The patients presentation i.e. collapse with no proceeding symptoms coupled with the fact that he was suffering a silent MI with no prior indications of ischaemic heart disease e.g. angina, shortness of breath etc and the rapid subsequent development of left ventricular free wall rupture in such an high position made this quite an unusual case. Stenosis in the right common iliac and subclavian arteries did delay diagnosis slightly, as aortic and carotid dissection had yet to be ruled out but ultimately this patient survived probably because of early diagnosis despite these obstacles and subsequent prompt treatment.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
ANDREW PETER VANEZIS MBChB BSc, FY2 Doctor, Barts and The London NHS Trust, UK.
REHAN QUADERY MBBS, ST3 Medicine, Bedford Hospital NHS Trust, UK
MOHAMMAD WASIL PhD, Assistant Director of Research & Development, Bedford Hospital NHS Trust, UK
MOHAMMED AZHER FCCP FRCP, Consultant Chest Physician, Bedford Hospital NHS Trust, UK
CORRESPONDENCE: REHAN QUADERY, Bedford Hospital NHS Trust, UK
Pohjola-Sintonen S, Muller JE, Stone PH, Willich SN, Antman EM, Davis VG, Parker CB, Braunwald E. Ventricular septal and free wall rupture complicating acute myocardial infarction: experience in the Multicenter Investigation of Limitation of Infarct Size. Am Heart J. 1989;117:809818
Hutchins, Kenneth D, Skurnick, Joan, Lavenhar, Marvin, Natarajan, Geetha A. Cardiac Rupture in Acute Myocardial Infarction: A Reassessment. American Journal of Forensic Medicine & Pathology. 23(1):78-82, March 2002.
Becker AE, Anderson RH. Cardiac pathology. An integrated text and colour atlas. London: Gower Medical Publishing; 1983.
Shirani J, Berezowski K, Roberts WC. Out-of-hospital sudden death from left ventricular free wall rupture during acute myocardial infarction as the first and only manifestation of atherosclerotic coronary artery disease. Am J Cardiol 1994 Jan; 73(1): 88-92
Slater J, Brown RJ, Antonelli TA, et al. Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction:A report from the SHOCK trial registry. J Am Coll Cardiology. 2000;36:1117-1122
Reddy SG, Roberts WC. Frequency of rupture of the left ventricular free wall or ventricular septum among necropsy cases of fatal acute myocardial infarction since introduction of coronary care units. Am J Cardiol 1989;63:90611
David, TE. Surgery for post infarction rupture of the free wall of the ventricle. In: David TE. , editor. Mechanical Complications of Myocardial Infarction. Austin, R.G. Landes Company; 1993. p. 142.
Cheitlin, MD et al. ACC/AHA/ASE 2003 Guideline update for the clinical application of echocardiography. J Am Coll Cardiol. 2003;42:95470
Lopez-Sendon J, Gonzalez A, Lopez de Sa E, Coma-Canella I, Roldan I, Dominguez F, et al. Diagnosis of subacute ventricular wall rupture after acute myocardial infarction: sensitivity and specificity of clinical, hemodynamic and echocardiographic criteria. J Am Coll Cardiol 1992;19: 114553.
Rajiv Agarwal, Pedro Diaz-Ortiz, Ravinder Reddy, Veronica Lenge, R. David Fish, David A. Ott, John Connelly, and Scott D. Flamm. Asymptomatic Incomplete Left Ventricular Apical Rupture Diagnosed by Cardiac Magnetic Resonance Imaging. Tex Heart Inst J. 2006; 33(1): 9395
Rolf Svedjeholma, Erik Hkansonb, Mrten Lindstrmc and Per Hjort. Case report - Cardiac general. Post-infarct left ventricular free wall rupture and ventricular septal defect managed by pericardial aspiration during transport to referral hospital. Interactive Cardiovascular and Thoracic Surgery. 2003; 2:193-195
Padro JM, Mesa JM, Silvestre J, Larrea JL, Caralps JM, Cerron F, Aris A. Subacute cardiac rupture: repair with a sutureless technique. Ann Thorac Surg. 1993;55:2023
Alejandro Aris. Surgical repair of left ventricular free wall rupture. Multimedia Manual of Cardiothoracics. 2004. doi:10.1510/mmcts.2004.
Malek G, Massas MD, Alexander SG. Surgical Repair of Mechanical Complications of Myocardial Infarction. World J Surg. 2004;28:847-856
The Mirena intrauterine system (IUS) has been licensed as a contraceptive in the UK since May 1995. Recent National Statistics suggest the Mirena IUS is used by only 1% of women aged 1649 years who are currently using contraception.1 The Mirena IUS now also has a licence for the management of idiopathic menorrhagia2 and may therefore be used by women who do not require contraception. Uterine perforation is a serious, albeit rare, potential complication of intrauterine device or system use. Women may be informed that uterine perforation occurs in fewer than 1 in 1000 of either copper intrauterine device (IUD) or IUS insertions.3,4 Rate of perforation reported with the Mirena IUS in a large observational cohort study was 0.9 per 1000 insertions.5 In this case report, an intraperitoneal Mirena IUS was detected nearly 4 years after its insertion and perforation of the uterus was diagnosed, despite vaginal hysterectomy and admissions to hospital. This case report demonstrates clearly that whenever there is suspicion from ultrasound scan report of an empty uterus that the IUS has fallen out, and in the persistence of symptoms, we should consider performing an abdominal X-Ray which is an easy, cheap method, to identify the IUS outside the uterus.
Case report
A 33-year-old woman, para 2, with a long standing history of menorrhagia, dysmenorrhoea and tiredness was referred by her GP to the hospital (2002). At the time she was treated for anaemia and felt tiredness. Also she was suffering from dysmenorrhoea; her periods had been regular although in the previous few months she was bleeding PV continuously. Her periods had become heavy after sterilisation (1996). She was anaemic. Cervical cytology had always been normal. In the past she had undergone a laparoscopy for pelvic pain for suspected endometriosis (1997), an appendicectomy (1997) and she was diagnosed with duodenal ulcer (1996). For management of her menorrhagia, she opted for Microwave Endometrial Ablation which was done in August 2002. After that she had an ultrasound scan for erratic bleeding which showed irregular endometrium. The patient was booked for hysteroscopy under general anaesthesia. The procedure was attempted in September 2003 and was abandoned due to difficulties passing the hysteroscope through the endocervical canal. The hysteroscopy was repeated in January 2004 and few intrauterine adhesions were reported. A Mirena IUS was inserted under the same general anaesthetic.
A month later she was admitted to the hospital with right upper quadrant pain and a problematic bleeding pattern. Ultrasound at this stage showed a normal size uterus but the Mirena IUS was not obviously in situ. It was assumed the Mirena IUS had fallen out and the patient was booked for vaginal hysterectomy, which was performed in September 2005.
In January 2007 was admitted to the hospital with right upper quadrant pain again and all investigations including chest X-ray, abdominal ultrasound scan and blood tests were normal. She had an upper GI endoscopy which showed a gastric ulcer (Cardia).
Fig.1 Abdominal X-Ray with the Mirena IUS (arrowed).
She was admitted again 1 year later with pelvic pain. An abdominal X-ray showed the lost IUS (fig. 1) and the CT scan showed the IUS to lie anteriorly under the rectus muscles and adjacent to the dome of the bladder. In April 2008 the IUS was retrieved laparoscopically. The omentum was adherent to anterior abdominal wall and the Mirena IUS was found in the omentum, (Fig.2). This was felt to be unlikely to be the cause of the pain. The IUS was removed easily from the abdominal cavity laparoscopically. The right tube and ovary were adherent to right pelvic side and they were freed up. The procedure was uneventful and the patient was discharged the same day and symptom free since.
Discussion
Uterine perforation is a serious, albeit rare, potential complication of Intrauterine contraceptive use. For informed consent, women should be informed that uterine perforation occurs in fewer than 1 in 1000 intrauterine LNG-IUS insertions4 Fig. 2 Mirena IUS (circled) within the omentum.
The rate of perforation reported with the LNG-IUS in a large observational cohort study was 0.9 per 1000 insertions.5 Current guidelines recommend that advice regarding the management of problems arising with the LNG-IUS use4 is similar to that for IUD use3. The problems are suspected perforation, lost threads, abnormal bleeding, pregnancy, presence of actinomyces-like organisms, pelvic infection, and postmenopausal removal.
The Royal College of Obstetricians & Gynaecologists recommends6 that women who present with persistent menorrhagia, despite LNG-IUS use, should be advised to return for further assessment of the uterine cavity (biopsy or ultrasound scan) to exclude pathology.
If menorrhagia persists despite medical treatments, women should be re-examined.6 An assessment of the uterine cavity should be performed using ultrasound scan. An endometrial biopsy should be considered in all women with persistent menorrhagia. When indicated, a hysteroscopy allows the assessment of the uterine cavity and biopsy under local anaesthesia.6 The WHO Selected Practice Recommendations for Contraceptive Use (WHOSPR) 7does not specifically refer to the Mirena IUS. Follow-up 36 weeks following IUD insertion is recommended and the Clinical Effectiveness Unit (CEU) advises similar follow-up for women using the Mirena-IUS.
In this case report, the detection of the Mirena IUS inside the peritoneal cavity was noted nearly 4 years after the insertion and the perforation of the uterus. The patient had several admissions to the hospital under the care of gynaecologists or gastroentero-logists always complaining for upper or lower abdominal pain. She even had a vaginal hysterectomy. Had she undergone an abdominal hysterectomy, the Mirena IUS may have been noted at that time.
This case report clearly demonstrates that following an ultrasound report showing an empty uterus in a symptomatic patient, an abdominal X-ray should be performed to identify whether or not the IUS is inside the peritoneal cavity. Also, we need to be aware of the peritoneal adhesion potential of Mirena IUS it is expected to be low. In another case report8, an intraperitoneal Mirena IUS resulted in plasma levonorgestrel levels 10 times higher (4.7 nmol/l) than the plasma level of levonorgestrel observed with Mirena IUS placed in utero. This high plasma LNG level suppresses ovulation. Therefore, aside from the adhesion potential, a misplaced Mirena IUS should be removed when pregnancy is desired9, 10.
The authors conclude that judicious use of the abdominal X-ray can lead to the early detection of a migrated IUS and expedite early removal.
A thorough literature search of the Medline, Embase and Cochrane databases did not reveal case reports similar to this and also did not report any formal guidance as to the use of the Mirena IUS device following endometrial microwave ablation, but we did find an article regarding insertion of Mirena IUS, after endometrial resection.11
Endometrial resection is a surgical method to manage menorrhagia. Intrauterine scarring may occur following treatment, but it is not known if the risk of uterine perforation is increased.
The Clinical Effectiveness Unit (CEU) responded12 recently that the British National Formulary (BNF)13 suggested that intrauterine devices (IUDs) should be used with caution in severely scarred uteri.
The United Kingdom Medical Eligibility Criteria for Contraceptive Use (UKMEC)14 recommends that if women have a distorted uterine cavity (any congenital or acquired uterine abnormality distorting the uterine cavity in a manner that is incompatible with IUD insertion), then the IUD or the levonorgestrel-releasing intrauterine system (LNG-IUS) should not be used (UKMEC 4).
A narrative review paper on treatment after hysteroscopic surgery suggests that an acceptable post-operative method of contraception after endometrial ablation is the LNG-IUS, as it protects the endometrium and there is a high amenorrhoea rate.15 However, following successful endometrial ablation the uterine cavity is usually severely narrowed making insertion of IUS (or IUD) impossible and it would not normally be considered as an appropriate method in these circumstances. Significant bleeding would suggest failure of the procedure, and if IUS or IUD was to be considered it should only be done with hysteroscopic assistance by an experienced gynaecologist.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
SHAMBHU S MBChB Senior House Officer, Department of Obstetrics and Gynaecology, Hull Royal Infirmary, UK
PAPPAS M MBChB Specialist Registrar, Department of Obstetrics and Gynaecology, Hull Royal Infirmary, UK
CORRESPONDENCE: DR SHAMBHU S, Senior House Officer in Obstetrics and Gynaecology, Hull Royal Infirmary, Hull, UK
Email: siddesh@doctors.org.uk
References
Dawe F, Meltzer H. Contraception and Sexual Health, 2002. London, UK: Office for National Statistics, 2003; 149 http://www.statistics.gov.uk.
Faculty of Family Planning and Reproductive Health Care (FFPRHC). FFPRHC Guidance (January 2004). The copper intrauterine device as long-term contraception. J Fam Plann Reprod Health Care 2004; 30(1): 2942.
Faculty of Family Planning and Reproductive Health Care (FFPRHC). FFPRHC Guidance (January 2004). The levonorgestrel-releasing intrauterine system (LNG-IUS) in contraception and reproductive health. Journal of Family Planning and Reproductive Health Care 2004; 30(2): 99109
Zhou L, Harrison-Woolrych M, Coulter DM. Use of the New Zealand Intensive Medicines Monitoring Programme to study the levonorgestrel-releasing intrauterine device (Mirena). Pharmacoepidemiol Drug Saf 2003; 12: 371377
Royal College of Obstetricians and Gynaecologists (RCOG). The Management of Menorrhagia in Secondary Care. National Evidence- Based Clinical Guidelines. London, UK: RCOG, 1999.
World Health Organization (WHO). Selected Practice Recommendations for Contraceptive Use. Geneva, Switzerland: WHO, 2002.
Management of a perforated levonorgestrel - medicated intrauterine device: pharmacokinetic study: Case report Ronit Haimov-Kochman et al, Human Reproduction Vol.18, No.6 pp. 12311233, 2003.
Adoni, A. and Ben Chetrit, A. (1991) The management of intrauterine devices following uterine perforation. Contraception, 43, 7781.
Andersson, K., Ryde-Blomqvist, E., Lindell, K., Odlind, V. and Milsom, I. (1998) Perforations with intrauterine devices. Report from a Swedish survey. Contraception, 57, 251255.
MEMBERS ENQUIRY RESPONSE Enquiry Reference: 2268, Sent: 2nd April 2008 . Faculty of Family Planning and Reproductive Health Care. Clinical Effectiveness Unit
British National Formulary. BNF 54. 2007.
Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit. UK Medical Eligibility Criteria for Contraceptive Use. http://www.ffprhc.org.uk/admin/uploads/UKMEC200506.pdf. 2006.
Romer, T., Schmidt, T., and Foth, D. Pre- and postoperative hormonal treatment in patients with hysteroscopic surgery. Contributions to Gynecology and Obstetrics 20, 1-12. 2000.
BACKGROUND : The present study was designed to measure changes in markers of antioxidant capacity (measured individually and total) following acute ischemic stroke.
METHODS : The study included 135 subjects. 62 were controls and 73 were ischemic stroke patients diagnosed clinically and by CT scan of the brain. The cases were divided into two groups, The ischemic stroke patients with large vessel / cortical, subcortical infarcts (Group. I) and small vessel / lacunar infarcts (Group. II) based on CT scan of the brain. Serum vitamin E, vitamin C, superoxide dismutase, uric acid and total antioxidant capacity were estimated in all the subjects.
RESULTS : Group I and Group II ischemic stroke cases had significantly lower levels of vitamin E, vitamin C and superoxide dismutase and significantly higher levels of uric acid compared to controls. The group I ischemic stroke cases had significantly lower levels of vitamin E, vitamin C, and superoxide dismutase and significantly higher levels of uric acid than group II ischemic stroke cases. Total antioxidant capacity strongly correlated with serum uric acid in cases
CONCLUSION: The present study suggests that estimation of vitamin E, vitamin C, SOD, uric acid and total antioxidant capacity may be used as an indirect evidence of oxidative stress induced neuronal damage in acute ischemic stroke which may be useful for monitoring and optimizing antioxidant therapy.
KEY WORDS: Stroke, oxidative stress, SOD, vitamin C, vitamin E. Total antioxidant capacity.
Several studies provide evidence of an association between ischemic stroke and oxidative stress. Increased free radical formation together with a reduced antioxidant defense causes oxidative stress, that may play an important role in the pathogenesis of stroke associated neuronal injury. Several studies demonstrate increased oxidative damage to neuronal cells during cerebral ischemia and reperfusion. Antioxidant activity is known to reflect the altered redox balance of affected fluids, tissues or organs in acute ischemic stroke patients. Therefore antioxidant concentrations or measures of their activity have been used to estimate the amount of oxidative stress 1. No single component of serum antioxidant complex could fully reflect the protective efficiency of blood, probably because of interactions that occur in vivo among different antioxidant compounds. Total antioxidant capacity considers the cumulative effect of all antioxidants present in blood and body fluids 2. The aim of this study was therefore to measure changes in markers of antioxidant capacity (measured individually and total) following acute ischemic stroke.
Materials and methods:
This study was conducted at Bapuji Hospital and Chigateri General Hospital, Davangere (Both Hospitals attached to J.J.M. Medical College, Davangere, karnataka), by including 62 healthy controls (of which 34 were men and 28 were women aged between 36 and 73 years) and 73 cases clinically diagnosed
as acute ischemic stroke patients of less than 48 hrs duration after the onset of symptoms) and confirmed by computerized tomography of the brain (of which 41 were men and 32 were women aged between 36 and 73 years). The cases were divided into two groups, The ischemic stroke patients with large vessel / cortical, subcortical infarcts (Group. I) and small vessel/lacunar infarcts (Group. II) based on CT scan of the brain. The stroke patients due to cerebral hemorrhage, malignancy, sepsis, severe medical or psychiatric illness, language disorders, swallowing difficulties, cognitive impairment, gout, renal failure and patients who were taking antioxidant vitamins were excluded from the study. The study was conducted after informed consent was obtained from them and the study has been approved by the ethical committee of the institution.
Under aseptic precautions about 6 ml of a non-fasting venous blood sample was collected from cases within 24 h following stroke onset and from healthy controls. Blood was collected in appropriate tubes and centrifuged at 3000 g for 15 min to separate plasma from red blood cells. The supernatant was stored at 40 C until analysis was carried out.
Serum vitamin E was estimated by Baker and Frank method 3, Vitamin C by 2, 4 DNPH method 4, SOD by Marklund and Marklund method 5, and uric acid by Henry Caraway method 6 and total antioxidant capacity (TAC) by FRAP assay method 2 in both the controls and cases. All the chemicals used were of highest analytical grade available in India.
TABLE I. Comparison of Serum Vitamin E, Vitamin C, SOD, Uric Acid and Total Antioxidant Capacity (Mean SD)
Vit. E mg/L
Vit. C mg/dl
SOD units/ml
Uric acid mg/dl
TAC (mol/l)
Controls (n = 62)
11.04 0.97
1.16 0.13
9.01 1.03
4.66 0.47
1079.7 197.9
Cases (n = 73)
7.22 0.81
0.52 0.16
4.35 0.70
6.56 0.73
1043.4 140.7
Comparison
p < 0.05
p < 0.05
p < 0.05
p < 0.05
p > 0.05
TABLE II. Comparison of Serum Vitamin E, Vitamin C, SOD, Uric Acid and Total Antioxidant Capacity (Mean SD) between Group I and Group II Cases.
Vit. E mg/L
Vit. C mg/dl
SOD units/ml
Uric acid mg/dl
TAC (mol/l)
Cases Group. I (n = 56)
6.93 0.67
0.45 0.08
4.14 0.61
6.78 0.62
1048.9 140.3
Cases Group. II (n = 15)
8.24 0.17
0.80 0.10
5.12 0.49
5.73 0.55
1038.1 142.9
Comparison (one way ANOVA and student t test)
p < 0.05
p < 0.05
p < 0.05
p < 0.05
p > 0.05
Statistical analysis :
Statistical analysis was performed with one way ANOVA test, student t test and Pearsons correlation coefficient using SPSS version 16.0. A value of p < 0.05 was taken to indicate statistical significance.
Results:
It was observed that the serum levels of Vitamin E, Vitamin C, TAC and SOD were significantly lower in ischemic stroke cases than those of controls and serum uric acid levels were significantly higher in ischemic stroke cases table I . Further it was observed that the group I ischemic stroke cases had significantly lower levels of serum Vitamin E, Vitamin C and SOD than group II ischemic stroke cases and significantly higher serum levels of uric acid in group I cases than group II ischemic stroke cases table II . Significant negative correlations were observed between vitamin C, vitamin E, SOD and TAC and significant positive correlation was observed between uric acid and TAC among cases table III.
TABLE III. Correlations of Vitamin E, Vitamin C, SOD, Uric Acid with Total Antioxidant Capacity in cases.
Vitamin C and TAC
Vitamin E and TAC
SOD and TAC
Uric acid and TAC
R value
-0.24
-0.1
-0.19
0.16
p value
< 0.05
< 0.05
< 0.05
< 0.05
Discussion:
In this study, there were reduced concentrations of vitamin E, vitamin C, SOD and TAC and increased concentrations of uric acid in stroke patients compared with controls. FRAP assay is presented as a novel method of assessing total antioxidant capacity 2 which is believed to be a useful measure of the ability of antioxidant present in the fluids to protect against oxidative damage to membranes and other cellular components..
Vitamin E, a potent chain breaking lipid soluble antioxidant, reacts with lipid peroxyl radicals eventually terminating the peroxidation chain reaction and thereby reducing oxidative damage. Some studies have shown reduced serum vitamin E levels in stroke patients and this may be due to high lesion volume resulting in production of more number of free radicals from a large ischemic injury. It is also shown that reduced vitamin E levels resulted in poor clinical outcome in stroke patients 7,8. In the present study serum vitamin E levels were significantly decreased in ischemic stroke cases (significantly decreased in large vessel infarcts than in small vessel infarcts) when compared to controls.
Vitamin C represents the major water-soluble antioxidant in the human body. Many studies show that reduced vitamin C levels are associated with increased risk of both ischemic and hemorrhagic strokes 9. In our present study the serum vitamin C levels were decreased significantly in ischemic stroke cases (decreased significantly in large vessel infarcts than in small vessel infarcts) compared to controls. It may be due to the exhaustion of this antioxidant in the neutralization of free radicals which are formed in excess during ischemia and reperfusion 10,11.
SOD is an endogenous antioxidant that catalyses the dismutation of the superoxide anion radical. SOD plays an important role in the defense against free radical damage in reperfusion injury and helps in reducing the infarct size during ischemia and reperfusion 12,13. In the present study the serum SOD levels were decreased significantly in ischemic stroke cases decreased in large vessel infarcts than in small vessel infarcts) compared to controls.
Uric acid, most abundant endogenous aqueous antioxidant in humans, may protect against oxidative modification of endothelial enzymes and preserves the ability of endothelium to mediate vascular dilatation during oxidative stress 14. Several studies have shown that increased oxidative stress is associated with high circulating uric acid levels due to elevation of xanthine oxidase in stroke induced brain damage 15,16. In this study, there was a significant increase in the serum levels of uric acid in ischemic stroke cases (increased significantly in large vessel infarcts than in small vessel infarcts) than in controls. Serum TAC strongly correlated with serum uric acid. Under multivariate analysis, serum uric acid explained most of the variance in TAC during the study period.
This study suggests that estimation of serum vitamin E, vitamin C, SOD, uric acid and total antioxidant capacity may be used as an indirect evidence of oxidative stress induced neuronal damage in ischemic stroke.
The limitations of our study are as follows: We have not estimated any markers of lipid peroxidation such as malondialdehyde which along with antioxidant levels would better explain oxidative stress. Antioxidant levels were measured only once, but prospective serial estimations would better predict the antioxidant status with prognosis of stroke. This study was conducted on a small group of stroke patients. Larger clinical studies in this area are needed to establish the relationships between antioxidant capacity and oxidative damage following ischemia and reperfusion in man, and to form the basis of appropriate antioxidant intervention strategies to minimize long-term brain injury following cerebral ischemia.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. SRIKRISHNA R, M.D., Assistant Professor, Department of Biochemistry, JJM Medical college, Davangere, India
DR. SURESH D R, M.D., Assistant Professor, Sri Siddhartha Medical College, Sri Siddhartha Academy of Higher Education (SSAHE), Tumkur, India
CORRESPONDENCE: DR. SURESH D R, 3/1, Seethappa layout, 5th Block, Doddabommasandra, Vidyaranyapura.P.O, Bangalore, Karnataka, INDIA- 560097.
Email: drsuri77@gmail.com
References
Leinonen JS, Ahonen JP, Lonnrot K, Jehkonen M, Dastidar P,Molnar G. Low plasma antioxidant activity is associated with high lesion volume and neurological impairment in stroke (2000). Stroke 31(9), 33-39.
Benzie FF, Strain JJ. The ferric reducing ability of plasma (FRAP) as a measure of antioxidant power: the FRAP assay (1996). Analytical Biochem 239, 7076.
Baker H, Frank O (1969). Clinical vitaminology. Academic Press. New York, pp169173.
Omage ST (1979). Ascorbic acid analysis II. Determination after derivatization with 2, 4, - Dinitrophenylhydrazine, Methods in Enzymology, 62, 7-8.
Nandi A, Chatterjee IB (1988). Assay of superoxide dismutase activity in animal tissues. J Biosci, 13 (3), 305-315.
Price CP, James DR (1988). Analytical reviews in clinical biochemistry: the measurement of urate. Ann Clin Biochem, 25 (5), 484-498.
Cherubini A, Ruggiero C, Polidori MC, Mecocci P. Potential markers of oxidative stress in stroke. Free Radical Biology and Medicine (2005), 39 (7), 841-852.
Tornwall ME, Virtamo J, Korhonen PA, Virtanen MJ, Albanes D, Huttunen JK (2004). Postintervention effect of alpha tocopherol and beta carotene on different strokes. A 6 year follow-up of the alpha tocopherol, beta carotene cancer prevention study. Stroke, 35(8), 1908-1913.
Yokoyama T, Date C, Kokubo Y, Yoshiike N, Matsumura Y, Tanaka H (2000). Serum vitamin C concentration was inversely associated with subsequent 20 year incidence of stroke in a Japanese Rural Community. Stroke, 31(10), 2287-2294.
Kurl S, Tuomainen TP, Laukkanen JA, Nyyssonen K, Lakka T, Sivenius J, Salonen JT (2002). Plasma vitamin C modifies the association between hypertension and risk of stroke. Stroke, 33(6), 1568-1573.
Kim GW, Kondo T, Noshita N, Chan PH (2002). Manganese superoxide dismutase deficiency exacerbates cerebral infarction after focal cerebral ischemia / reperfusion in mice. Stroke, 33(3), 809-815.
Zimmermann C, Winnefeld K, Streck S, Roskos M, Haberl RL (2004). Antioxidant Status in Acute Stroke Patients and Patients at Stroke Risk. Eur Neurol, 51(3), 157-161.
Weir CJ, Muir SW, Walters MR, Lees KR (2003). Serum urate as an independent predictor of poor outcome and future vascular events after acute stroke. Stroke, 34 (8), 1951-1957.
Hariklia VD, Apostolos IA, Haralambos IK (2008). The Role of Uric Acid in Stroke: The Issue Remains Unresolved. Neurologist, 14(4), 238-242.
Hozawa A, Folsom AR, Ibrahim H, Nieto JF, Rosamond WD, Shahar E (2006). Serum uric acid and risk of ischemic stroke : the ARIC study. Atherosclerosis, 187(2), 401-407.
The primary objective of this survey was to check the availability and use of cameras in documentation of open fractures in emergency departments in England, Wales and Scotland. We also checked the use of mobile phone cameras in emergency departments without cameras. A telephone questionnaire posed questions to the first on-call orthopaedic doctor aboutthe availability of a functional camera in the emergency department. Altogether, 102 doctors replied in 115 hospitals that were surveyed. Only 63 emergency departments had a camera available for photography of open fractures, in which 53 orthopaedic doctors would always take photographs of an open fracture. In 7 emergency departments a mobile phone camera was used for documentation of open fractures, as a camera was not available.
Subsequently, recommendations for wound documentation using a mobile phone camera have been proposed as it is easily accessible and portable with good picture quality that can be transmitted to offsite senior colleagues for advice. This would prevent wound infection and also act as an adjunct to a narrative description of the wound.
Open fractures are quite common and account for a considerable number of admissions to the emergency department with a frequency of approximately 23 per 100000 patients per year1. Infections of open musculoskeletal injuries, especially open fractures, continue to pose a challenge to the Orthopaedic and Trauma surgeons. To reduce the risk of nosocomial infections these wounds need to be instantly photographed before the application of a sterile dressing which has to be left undisturbed until the surgical intervention in the theatre2.
The British Orthopaedic Association and British Association of Plastic surgeons recommend that a Polaroid photograph of every open fracture should be taken, this recommendation is not followed due to non availability of the equipment in some institutions1. This leads to unnecessary disturbance of the wound dressing, distress to the patient and nosocomial infection.
The objective of this study was to look at the availability and use of cameras in compound fractures in Hospitals across England, Wales and Scotland by using a telephone questionnaire.
Methods
We randomly selected 115 NHS hospitals with A&E departments from all the regions of the England, Wales and Scotland using the www.specialistinfo.com website and selected every third hospital on the list. The survey was conduction by the means of a telephone questionnaire (Table 1); the questions were answered by the first on call Orthopaedic doctor. 89% (102/115) first on-call doctors answered the questionnaire.
TABLE 1 Telephonic questionnaire
1. Do you have access to a camera in the A&E?
2. If yes, is the camera available 24/7?
3. Have you found a functional camera available every time you have wanted to use it?
4. Do you always take a picture of an open fracture?
5. Do you think that a picture is a useful tool in the assessment of a wound?
6. If a camera is not available in the A&E do you use your mobile phone camera?
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
The questionnaire was meant to investigate if the doctor had access to a functional camera that was available round the clock in the Emergency department. It also questioned whether the doctor on call would always take a picture of an open fracture. They were also asked whether they thought that the picture was helpful in assessment of the wounds. Finally the respondents were asked whether they used a mobile phone camera in case of non availability of a camera in the emergency department.
Results
Of the 102 first on call Orthopaedic doctors questioned, 38% (39/102) stated that they were unable to photograph an open fracture due to non availability of a camera in the emergency department. A functional camera was not available in both trauma centers and small hospitals. Of the 61% (63/102) who had a camera available 22% (14/63) did not have 24 hour access to the camera. 33% (21/63) who have a Polaroid camera available have found occasions when they needed a camera but it was not functional. (Figure 2)
Figure 1
Figure 2 Availability of cameras in A&E.
84% (53/63) who had a camera available said that they always photographed an open fracture. (Figure 3) 28% (11/39) doctors who did not have a camera in the emergency department would use a mobile phone camera to photograph an open fracture (Fig 1). 4 doctors used it even though they had a Polaroid camera in the Accident and Emergency department (A&E) as they found a mobile phone camera easy to use and readily accessible.
All the doctors who responded to the questionnaire thought that a camera was a valuable tool in the documentation of an open fracture.
Discussion
The objective of this study was to look at the availability and use of cameras in compound fractures in hospitals across England, Wales and Scotland.
Figure 3 Percentage of doctors photographing open fractures in A&E.
We found that 38% of hospitals did not have access to a camera at all, in a further 15% there wasnt 24 hour access and another 21% had a camera that was not functional when needed at some time in the Emergency department. Thus 74% of hospitals did not have a functional camera available in the emergency department at all times. Therefore the photographic documentation of an open fracture as recommended by the British Orthopaedic association and the British association of Plastic Surgeons working party could not be implemented2. 13% (8/63) respondents who had a camera in the Emergency department did not routinely photograph an open fracture. A similar study done in London and south-east UK hospitals found that 10% hospitals did not have a camera to photograph an open fracture and another 19% did not have it available 24 hours1.
The potential reasons for failure of photographic wound documentation could be difficulty to obtain funding for purchase of a camera, lack of secure storage space and unfamiliarity of the junior doctors with the guidelines of photographic wound documentation
Open wounds of the musculoskeletal system are usually contaminated at presentation with pathogenic organisms3. In the A&E the wound should be assessed and dressed until the formal debridement in the theatre. The ideal practice is to photograph the wound before application of the sterile dressing. These photographs are a vital tool as they act as an adjunct to a narrative description allowing the wound to be accurately described to colleagues. This avoids unnecessary disturbance of the sterile dressing over the wound which has a risk of nosocomial infection2.
The problem of non availability of Polaroid cameras in the emergency department can be overcome by using mobile phone cameras. We faced the same problem of non availability of a camera in our A & E department and we started using our camera phones for photographing open fractures. The authors found that images on mobile phone cameras allowed a useful presentation in the morning trauma meetings. The incidence of re- examining of the wound by the senior surgeons also dropped significantly. Mobile phones can be used in A & E as the maximum distance at which any phone causes interference is only two meters4.
We found the mobile phone camera a valuable alternative as it is easy to use and has excellent portability with an image quality that is sufficient for interpretation. In our study it is already being used by many doctors in different hospitals. With the advancement in technology the mobile phones have become more user friendly with the power to process medical images5. The advantage over a Polaroid picture is that these images can be transferred to another mobile phone or sent as an e-mail attachment for assessment by the offsite registrars and consultants for immediate advice. This is even more useful in hospitals with hospital at night where second on call doctors are usually nonresident. It has been shown that it takes only 3-4 minutes from image taking to remote reception6. The Integrated Service Digital Network (IDSN) used for image transfer in some hospitals is expensive and mobile camera phones are a suitable inexpensive substitute.
We recommend supplying a mobile phone camera to the on call doctor. Unlike Polaroid cameras they dont need a constant supply of batteries and expensive film and the risk of theft is negligible as they are smaller, lighter with excellent portability. The picture can be magnified and is easier to store than traditional cameras. Images must be stored in a manner that prevents tampering and preserves confidentiality. This could be done by deleting the images after they have been assessed, hard copies produced and kept in the case notes as done with pictures taken with a Polaroid camera or storing them by using specific software packages that do not allow image manipulation7 .
There have been two studies assessing the accuracy of the use of mobile phone cameras in diagnosing intracranial pathologies and interpretation of emergency Ear Nose and Throat (ENT) radiological investigations. 5, 8 They have also been used to take pictures of injured digits and then transmitted to camera phones of plastic surgeons for assessment 6. Tsai et al. in their study on teleconsultation by using the mobile camera phone showed that the camera phone is valuable for remote management of the extremity wound9 .Lam TK et al. showed that low cost and the ease of use make the mobile camera phones easily incorporated into clinical practice10.
Conclusion
A functional camera was not available at all the times for photographic documentation of open fractures in the majority of the hospitals. We also feel that mobile phone cameras may be used as a powerful graphic adjunct to a verbal clinical presentation to other health professionals located on or off site.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
MR R AHMAD, MBBS, MRCS, MR S K M ANNAMALAI, MBBS, MRCS, Registrars in T & O, Weston General Hospital, UK
MR SMY AHMED, Registrar T & O, Great Western Hospital, Swindon, UK
MR SA JOSEPH MBBS MRCS, Registrar T & , Wolverhampton General Hospital, UK
MR M BOULD FRCS, Consultant Orthopaedic Surgeon, Weston General Hospital, UK
CORRESPONDENCE: MR. SKM ANNAMALAI, Registrar, T & O, House 18, Staff Residence, Weston General Hospital, Weston Super Mare, BS23 4TQ
Email: suresh.annamalai@nhs.net
References
1. Solan MC, Calder JD, Gibbons CE, Ricketts DM. Photographic wound documentation after open fracture. Injury 2001; 32: 33-35.
2. The management of Open Tibial Fractures. British Orthopaedic Association and British association of Plastic Working Party, London, 1997.
3. Akinyoola AL, Ako-Nai AK, Dosumu O, Aboderin AO, Kassim OO. Microbial isolates in early swabs of open musculoskeletal injuries. Niger Postgrad Med J 2006; 13: 176-81.
4. Tri JL, Hayes DL, Smith TT, Severson RP. Cellular phone interference with external cardiopulmonary monitoring devices. Mayo Clin Proc 2001; 76: 11-5.
5. Eze N, Lo S, Bray D, Toma AG. The use of camera mobile phone to assess emergency ENT radiological investigations. Clin Otolaryngol 2005; 30: 230-3.
6. Hsieh CH, Tsai HH, Yin JW, Chen CY, Yang JC, Jeng SF. Teleconsultation with the mobile camera-phone in digital soft-tissue injury: a feasibility study. Plast Reconstr Surg 2004; 114:1776-82.
7. Bhangoo P, Maconochie IK, Batrick N, Henry E. Clinicians taking pictures a survey of current practice in emergency departments and proposed recommendations of best practice. Emerg Med J 2005; 22: 761-5.
8. Yamada M, Watarai H, Andou T, Sakai N. Emergency image transfer system through a mobile telephone in Japan: technical note. Neurosurgery 2003; 52: 986-8.
9. Tsai HH, Pong YP, Liang CC, Lin PY, Hsieh CH. Teleconsultation by using the mobile camera phone for remote management of the extremity wound: a pilot study. Ann Plast Surg 2004; 53:584-7.
10. Lam TK, Preketes A, Gates R.Mobile phone photo messaging assisted communication in the assessment of hand trauma. Lam TK, Preketes A, Gates R. ANZ J Surg 2004; 74:598-60
Propofol is an IV anesthetic that is often used as an adjuvant during monitored anesthesia care, the addition of ketamine to propofol may counteract the cardiorespiratory depression seen with propofol used alone. Ketofol (ketamine/propofol combination) was used for procedural sedation and analgesia. However, evaluation of the effectiveness of different concentrations of Ketofol in procedural operation regarding changes in haemodynamics, emergence phenomena, recovery time, the doses, and adverse effects was not yet studied, so this randomized, double blinded study was designed to compare the quality of analgesia and side effects of intravenous different concentrations of ketofol in hundred children of both sex undergoing procedural operation, e.g. esophgoscopy, rectoscopy, bone marrow aspiration and liver biopsy participated in this randomized, double-blinded study. Patients received an infusion of a solution containing either combination of propofol: ketamine (1:1) (Group I) or propofol: ketamine (4:1) (Group II). Subsequent infusion rates to a predetermined sedation level using Ramsay Sedation Scale. Heart rate, noninvasive arterial blood pressure (NIBP), oxygen saturation (SpO2), end tidal carbon dioxide (Etco2) and incidence of any side effects were recorded. There were no significant hemodynamic changes in both groups after induction. However, there was an increase in postoperative nausea , psychomimetic side effects, and delay in discharge times with the largest ketamine dosage (Group I). We concluded that the adjunctive use of smaller dose of ketamine in ketofol combination minimizes the psychomimetic side effects and shorten the time to discharge.
Procedural operations, are procedures outside the operating room, which developed from a facilitation of diagnostic and therapeutic procedures into an independent subspecialty. Procedural sedation and analgesia is a minimally depressed level of consciousness that retains the patient's ability to maintain a patent airway independently and continuously(1).
Propofol is a short-acting intravenous sedative agent used for the induction and maintenance of general anesthesia for adults and children, sedation for intubated, mechanically ventilated adults in Intensive Care Units (ICU), and in procedures such as colonoscopy. It provides no analgesia(2). Ketamine is classified as an NMDA receptor antagonist and has also been found to bind to opioid receptors and sigma receptors. It induces a state referred to as "dissociative anesthesia"(3).
Ketofol (ketamine/propofol combination) was used for procedural sedation and analgesia. Ketamine and propofol are physically compatible for 1 hr at 23oC with no increase in particle content at Y site injection (4). Ketamine and propofol administered in combination have offered effective sedation for spinal anesthesia and for gynecologic, ophthalmologic, and cardiovascular procedures in all age groups. The opposing hemodynamic and respiratory effects of each drug may enhance the utility of this drug combination, increasing both safety and efficacy and allowing reduction in the dose of propofol required to achieve sedation.
However, evaluation of the effectiveness of different concentrations of Ketofol in procedural operation regarding changes in hemodynamic, emergence phenomena, recovery time, the doses, and adverse effects was not yet studied, so this randomized, double blinded study was designed to compare the quality of analgesia and side effects of intravenous different concentrations of ketofol in children scheduled for procedural operations.
Methods:
A hundred patients, American Society of Anesthesia (ASA) class I or II scheduled for procedural operation, ages 3 to 12 years were enrolled in this study. After obtaining approval from the local research ethics committee, all patients and their parents were informed about the procedure and the anesthetic technique and an informed written consent was obtained from each. Patients with clinically significant cardiovascular, respiratory, hepatic diseases or epileptic patients, longer procedures more than one hour and sensitivity to the drugs were excluded from the study.
Patients were randomized into two equal groups each of 50 patients going for procedural operation, e.g. esophgoscopy, rectoscopy, bone marrow aspiration and liver biopsy. Pre procedural visit was done to evaluate if that patient fulfils the criteria of study and for fasting instruction. In the preoperative waiting area, an IV catheter was placed after applying emla cream. Baseline measurements included Non Invasive Blood Pressure (NIBP), heart rate, respiratory rate, and pain faces scale which is recommended for children aged 3 years and older (Fig1)(5). The level of sedation was determined by Ramsay Sedation Scale(6). A separate observer who was blind to the drug combination being used assessed the depth of sedation of such patients.
*Ramsay Sedation Scale(6)
Patient is anxious and agitated or restless, or both
Patient is co-operative, oriented, and tranquil
Patient responds to commands only
Patient exhibits brisk response to light glabellar tap or loud auditory stimulus
Patient exhibits a sluggish response to light glabellar tap or loud auditory stimulus
Patient exhibits no response
Fig 1: Pain Faces Scale.
A propofol/ketamine admixture was prepared by an assistant who was not involved in the clinical management of the study patients. According to a prestudy randomization schedule of study group assignment, a ketofol (1:1): propofol 14.285 mg, ketamine 14.285 mg/ml by mixing 10 ml propofol 2% (20 mg/ml) with 4 ml ketamine (50 mg/ml) in group I, while in group II ketofol (4:1): propofol 18.1818 mg , ketamine 4.5454 mg/ml by mixing 10 ml propofol 2% (20 mg/ml) with 1 ml ketamine (50 mg/ml).
Both bolus and maintenance doses were given using syringe pump (B/Braun). Set up for delivery of Ketofol in both groups as an initial bolus of 600 g/kg IV (calculated as dose of propofol in these infusions for simplicity), followed by an initial maintenance infusion at 100 g/kg/min by anesthetist who was blinded to the identity of study infusion.The level of sedation was assessed at 1- 3 minutes intervals, and the initial infusion rate was adjusted (in 25 g/kg/min increments) to achieve Ramsay Sedation Scale of 5 before starting the procedure.
During the procedure, patients were kept on oxygen nasal prongs with a CO2 sampling port. All patients were monitored with NIBP, electrocardiography (ECG), Pulse oximetry(SpO2), heart rate (HR), and end tidal carbondioxide( EtCO2). The measurement started before commencement of the intravenous (IV) line and continued five minutes after induction. The patients were also assessed for apnoea, which was defined as the loss of respiratory efforts for more than 20 seconds or fall of SpO2 below 95%. Complaints of pain/discomfort were treated by an incremental increase in the study drug infusion rate.
The study drug infusion was discontinued at the end of the surgical procedure, and the total drug requirements were noted. After the completion of the procedure, patients were transferred to recovery room when an Aldrete score(7) 9-10 was confirmed, and kept there till ready for discharge. The recovery room nurses were blinded to the study medication received by the patients. The incidence of any episode of postoperative nausea and vomiting (PONV) or any other side effects (e.g. hallucinations, agitation or pain) was noted. The patients vital signs were assessed at 5-min intervals. Patients were considered "ready for discharge" when they had stable vital signs, oriented, able to ambulate unassisted, had no intractable nausea or vomiting, and had minimal pain. Discharge times were determined from the time the study drug infusion was discontinued. Outpatients were given written discharge instructions regarding post-procedure precautions and a telephone number to use in case of emergency.
Descriptive variables were analyzed using Students t-test and X2 test as appropriate using SPSS software statistical computer package version 15. Differences between the groups in mean blood pressure (BP),heart rate( HR), end-tidalCO2, oxygen saturation and ketofol requirements were compared using analysis of variance with repeated measures. A P value < 0.05 was considered to be statistically significant. Values are expressed as meanSD.
Results:
There were no significant differences among patients in both groups regarding number of patients, age, sex, weight, ASA physical status, and duration of ketofol infusion (table 1). There was 2 patients excluded in group I; one had a history of epilepsy and the other was acute lymphocytic leukemia on corticosteroids, while in group II only one patient was excluded due to history of epilepsy (Table 1).
Sedation scores were similar in both groups. The average ketofol initial dose in group I was 600 g /kg followed by an average infusion rate of 116 24 g/kg/min, while in group II the average ketofol initial dose was 600 g/Kg followed by an average infusion rate of 132 36 g/kg/min with a significant difference between groups (P <0.05).
There was a minimal decrease in mean arterial blood pressure (MAP) from baseline in both groups following the initial dose of ketofol. Significant hypotension was noted in 2 patients in group I (4%) and in 3 patients in group II (6%) which was corrected by a bolus of Ringers solution 10 ml/kg IV. The diffrence between the groups was statistically insignificant . All the patients had increase in pulse rate compared to the baseline. The change was least in group II (p <0.05), but no patient had severe tachycardia requiring treatment in both groups.
There was increase in Etco2 in both groups after induction with statistically insignificant difference between groups. Patients in both groups had decrease in arterial oxygen saturation (SpO2) after induction. Five patients (10%) in group I and three patients (6%) in group II had apnea and hypoxia after induction (SpO2 <95%). Excessive salivation was noted in 15 patients (31%) in group I but only two patients (4%) in group II. Eight patients (16%) in group I and two patients (4%) in group II experienced airway obstruction or apnea which required airway support. These changes were statistically significant between both groups.
Table 1. Demographic Characteristics, Intraoperative Management, and Recovery Times of Patients in the Study Groups
Group 1
Group 2
Number
50
50
Age (yr)
6.6 3.6
7 3.1
Weight (kg)
21 8
23 7.5
ASA physical status
(III)
(III)
Duration of infusion (min)
25.312.4
23.8 14.8
Average propofol concentration (mg/ml)
14.3
18.18
Average ketamine concentration (mg/ml)
14.3
4.54
ketofol bolus dose (g /kg)
600
600
Average Ketofol infusion rate (g/kg/min)
116 24
132 36*
Time to ambulation (min)
15.4 9.5
8.2 6.7*
Ready for discharge (min)
26.511.3
15.3 8.4*
Time to actual discharge (min)
38.813.5
28.2 8.9*
-Data are mean SD, median (range).
-Group I propofol/ketamine (1:1), Group II = propofol/ketamine (4:1)
-ASA = American Society of Anesthesiologists.
-Average bolus dose were calculated as dose of propofol in infusion. Average infusion rates were calculated as total drug (propofol) divided by weight and case duration.
* Significant difference (P < 0.05) versus group I.
Two patients in group II (4%) and one patient in group I (2%) had pain and discomfort during the procedure which was overcome by incremental boluses of infusions. In group I, one patient (2%) complained of postoperative nausea, four patients (8%) experienced bad dreams and hallucinations and five patients (10%) complained of agitations with no psychomimetic changes in group II
The time to ambulation in group I and II patients was 15.4 9.5 and 8.2 6.7 minutes respectively, while readiness to discharge was 26.5 11.3 in group I and 15.3 8.4 minutes in group II. The time to actual discharge was 38.8 13.5 minutes in group I and 28.2 8.9 minutes in group II. These changes in recovery timings were statistically significant.
Discussion:
The goals of procedural sedation are to provide an adequate level of sedation while minimizing pain and anxiety, maximizing amnesia, minimizing the potential for adverse drug-related events, controlling behavior, and maintaining a stable cardiovascular and respiratory status. A number of studies have demonstrated that the combination of ketamine and Propofol (ketofol) for sedation is safe and effective. The combination of the two agents appears to reduce side effects of each medication used alone, and allows for a rapid recovery time(1).
We compared the safety and efficacy of different concentrations of ketofol in procedural operations in children. The rate of ketofol infusion in group II was higher than in group I due to due to incremental doses of ketofol given to get the desired depth of sedation and abort pain sensation which was due to less ketamine content in such infusion compared to group I. Propofol in the recommended dose of 2-2.5 mg/kg almost always causes fall in blood pressure and the extent of fall depends upon the dose and adjuvant drugs used. Because we used an initial infusion dose of only 600 g/kg, the fall in MAP was mild (6%) and similar in both groups. The induction doses of propofol are reduced considerably by combination with small doses of ketamine. Ketamine had the additional advantage of better hemodynamic stability. Our results are consistent with Furuya et al and Hui et al who suggested that the minimal change observed in arterial pressure may be dose related and also because sympathomimetic actions of ketamine were effective in counter-acting the hemodynamic depression of propofol. There was a trend for pulse rate to increase after the induction in all the groups, but there was no occurrence of profound tachycardia in any group(8,9).
Akin et al published a trial of 60 patients between one month and 13 years of age undergoing cardiac catheterization who received sedation with propofol or propofol plus ketamine (3:1). They found a significant (decrease in MAP in 11 patients in the propofol monotherapy group and three patients in the ketofol group. They concluded that the addition of low-dose ketamine to propofol preserved MAP without prolonging recovery or increasing the incidence of adverse events(10). While, Goh et al published a 90 patients having a laryngeal mask airway (LMA) placed received propofol with either ketamine (5:1), fentanyl (1 g /kg), or placebo normal saline. They found the ketofol group had a significantly higher systolic blood pressure than the other two groups. They concluded that ketofol provided equivalent LMA insertion conditions while maximizing hemodynamics and minimizing apnea(11).
End-tidal CO2 increased slightly after induction in both groups. In agreement with our results, Mildh et al and Persson et al who reported that ketamine-induced sympathoadrenal activation may account for improved ventilation, also arousal secondary to the subjective side effects of ketamine (e.g., perceptual changes and anxiety) may also contribute (12,13). Also our results have confirmed the previous reports of Frey et al and Badrinath et al (14,15), suggesting that the combination of a small-dose ketamine with propofol improves ventilation during sedation.
We expect that the apnea and desaturation recorded in group I (10%) was due to the excessive salivation complicated the higher dose of ketamine in this group which led to impaired breathing and required airway support in 16% of such patients. While apnea and desaturation which happened in group II could be due to the higher infusion rate of propofol in ketofol combination.
Willman and Andolfatto published a study of 114 patients requiring procedural sedation and analgesia mainly for orthopedic procedures were given a 1:1 mixture of propofol and ketamine. Transient hypoxia occurred in 2.6% of patients, out of them one patient required bag valve mask ventilation. Three patients had an emergence reaction, one of whom received midazolam. No patient had vomiting or aspiration. Procedural success rate in this study without the use of adjunctive medications was 96.5%. Median time until recovery was 15 minutes (range 5 to 45 minutes) (16). Furthermore, Akin et al compared propofol to propofol plus ketamine (3:1) in 60 patients between one and 13 years of age undergoing auditory brainstem response testing. There were no cases of desaturation in the ketofol group, but in the propofol group 4/30 experienced desaturation and 6/30 had apnea. The authors concluded that the addition of low dose ketamine to propofol reduced the risk of respiratory depression and the need for repeat medication administration(17).
The incidence of clinically significant psychotomimetic effects was noted in the large-dose ketamine group (group I). This could be a dose-dependent interaction of the excitatory anesthetic ketamine with a pure central nervous system depressant, such as propofol (18,19). There were no post procedural psychotomimetic symptoms recorded in group II. In addition, the patients mood was significantly better in the recovery room and cognitive function recovered more rapidly in such group than those given higher dose of ketamine. Nagata et al and Mortero et al are coinciding with our results as they suggested that ketamine in sedative doses is associated with electroencephalographic activation. Furthermore, small-dose ketamine increases thalamic sensory output and arousal. Sedative effects of propofol may be partially antagonized by the arousal effects of ketamine(20,21). While Akin et al in a trial of 40 adult patients undergoing endometrial biopsy, reported that the combination of propofol (1 mg/kg) plus fentanyl (1 g/kg) was compared to the combination of propofol plus ketamine (2:1). Time to recovery was similar; however time to discharge was longer in the ketofol group secondary to the increased presence of adverse events including nausea, vertigo, and visual disturbances. These authors concluded that although both regimens seem safe, ketofol (2:1) had more adverse events leading to a longer time until discharge and had a lower overall patient satisfaction(22).
Badrinath et al, published One hundred female outpatients undergoing breast biopsy procedures under local anesthesia received an infusion of a solution containing propofol in combination with different doses of ketamine . The sedative infusion rate was varied to maintain a deep level of sedation and normal respiratory and hemodynamic functions. They reported that combination of propofol and ketamine (5:1) provides effective sedation/analgesia during monitored anesthesia care(15). Our results suggest that our combination propofol and ketamine (4:1) was more suitable in procedural operations as Badrinath et al used their preferred combination (5:1) only in monitored anesthesia care and they supplement their sedation with local anesthesia infiltration.
In conclusion, propofol combined with ketamine (4:1) infusion for procedural operations contributed adequate sedation and analgesia without hemodynamic and respiratory depression or psychotomimetic side effects and appears to be a safe and useful technique for procedural operations in the ambulatory setting.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
MOHAMED DAABISS, MEDHAT ELSHERBINY, RASHED ALOTIBI, Department of Anesthesia, Riyadh Armed forces Hospital, Kingdom of Saudi Arabia.
CORRESPONDENCE: DR MOHAMED DAABIS, P.O.Box 7897 - D186, Riyadh 11159, Saudi Arabia
Email: madaabiss@yahoo.com
References
Aouad MT, Moussa AR, Dagher CM. Addition of ketamine to propofol for initiation of procedural anesthesia in children reduces propofol consumption and preserves hemodynamic stability. Acta Anaesthesiol Scand; 2008, 52 (4) : 561-5.
Miner JR, Burton JH. Clinical practice advisory. Emergency department procedural sedation with propofol. Ann Emerg Med. 2007;50(2):182-7
Harrison N, Simmonds M. "Quantitative studies on some antagonists of N-methyl D-aspartate in slices of rat cerebral cortex". Br J Pharmacol 1985; 84 (2): 38191.
Trissl LA, Gilbert DL, and Martinez JF: compatibility of propofol injectable emulsion with selected drugs during simulated Y-site administration, Am J Health-Syst Pharm 1997;54:1287-92
Wong DL, Hockenberry-Eaton M, Wilson D, Windelstein ML, Schwartz P. Wong's Essentials of Pediatric Nursing, 6th Edition.St. Louis: 2001; page 1301.
Griffiths RD, Jones C. Recovery from intensive care. British Medical Journal 1999; 319: 427 9.
Furuya A, Matsukawa T, Czaki M, Nishiyama T, Kume M, Kumazawa T. Intravenous ketamine attenuates arterial pressurechanges during induction of anesthesia with propofol. Eur JAnesthesiol 2001; 18: 88-92.
Hui TW, Short TG, Hong W, Suen T, Gin T, Plummer J. Additive interactions between propofol and ketaminewhen used for anesthesia induction in female patients.Anesthesiology 1995; 82: 641-48.
Akin A, Esmaoglu A, Guler G, et al. Propofol and propofol-ketamine in
Goh PK, Chiu CL, Wang CY, et al. Randomized double-blind comparison of ketamine-propofol, fentanyl-propofol and propofol saline on haemodynamics and laryngeal mask airway insertion conditions. Anaesth Intensive Care. 2005; 33:223-8.
Mildh L, Taittonen M, Leino K, KirvelO. The effect of low-dose ketamine on fentanyl-induced respiratory depression. Anaesthesia 1998; 53: 96570.
Persson J, Scheinin H, Hellstrm G, et al. Ketamine antagonizes alfentanil-induced hypo-ventilation in healthy male volunteers. Acta Anaesthesiol Scand 1999; 43: 74452
Frey K, Sukhani R, Pawlowski J, et al. Propofol versus propofol-ketamine sedation for retrobulbar nerve block: comparison of sedation quality, intraocular pressure changes, and recovery profiles. Anesth Analg 1999;89:31721.
Badrinath S, Avramov MN, Shadrick M, et al. The use of a ketamine-propofol combination during monitored anesthesia care. Anesth Analg 2000; 90: 85862
Willman EV, Andolfatto G. A prospective evaluation of ketofol (ketamine/propofol combination for procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2007; 49:23-30.
Akin A, Esmaoglu A, Tosun Z, et al. Comparison of propofol with propofol-ketamine combination in pediatric patients undergoing auditory brainstem response testing. Int J Pediatr Otorhinolaryngol. 2005; 69:1541-1545.
Mori K, Kawamata M, Mitani H, et al. A neurophysiologic study of ketamine anesthesia in the cat. Anesthesiology 1971;35:37383.
Tomoda K, Shingu K, Osawa M, et al. Comparison of CNS effects of propofol and thiopentone in cats. Br J Anaesth 1993;71:3837.
Nagata A, Nakao S, Miyamoto E, et al. Propofol inhibits ketamine-induced expression in the rat posterior cingulate cortex. Anesth Analg1998;87:141620.
Mortero RF, Clark LD, Tolan MM, et al. The Effects of Small-Dose Ketamine on Propofol Sedation: Respiration, Postoperative Mood, Perception, Cognition, and Pain. Anesth Analg 2001;92:1465-9
Akin A, Guler G, Esmaoglu A, et al. A comparison of fentanyl-propofol with a ketamine-propofol combination for sedation during endometrial biopsy. J Clin Anesth. 2005; 17:187-90.
Bullying in the workplace is emerging as a problem over the past decade. Despite the tendency for incidents of bullying to be underreported 2 it is widespread in all sectors of the workforce including healthcare in the United Kingdom (UK) 3. The culture of bullying in medicine contributes to this pattern of bullying behaviour that can adversely affect any aspect of working life from an employees health 4 to the reputation of the organisation 5. Therefore immediate changes are required to increase the recognition of this problem and take further steps to a solution.
Bullying and harassment
There are different ways to understand the terms bullying and harassment but considerable overlap exists with similar patterns of behaviour (figure 1).
Figure 1: Examples of bullying and harassment 6
Spreading malicious rumours, or insulting someone by word or behaviour (particularly on the grounds of age, race, sex, disability, sexual orientation and religion or belief)
Copying memos that are critical about someone to others who do not need to know
Ridiculing or demeaning someone picking on them or setting them up to fail
Exclusion or victimization
Unfair treatment
Overbearing supervision or other misuse of power or position
Unwelcome sexual advances touching, standing too close, the display of offensive materials, asking for sexual favours, making decisions on the basis of sexual advances being accepted or rejected
Making threats or comments about job security without foundation
Deliberately undermining a competent worker by overloading and constant criticism
Preventing individuals progressing by intentionally blocking promotion or training opportunities.
The essential difference between bullying and harassment is that the latter is usually a single incident that relates to ones social identity and is therefore viewed as discriminatory in nature e.g. racial or sexual harassment. In legal terms harassment refers to a course of conduct directed at a specific person, which causes substantial emotional distress, and can be identified by equality laws in the relevant country.
On the other hand workplace bullying is generally not covered by specific legislation. The exception to this is found in such as Sweden and Norway 7. Indeed it is in Scandinavia where extensive research into bullying in the workplace originated 7.
Bullying
Bullying in the workplace is known internationally by terms such as mobbing, workplace harassment, employee abuse, mistreatment at work, and petty tyranny 8. There is no generally accepted definition of workplace bullying but it is summed up well by the following:
Persistent, offensive, abusive, intimidating or insulting behaviour, abuse of power or unfair penal sanctions which makes the recipient feel upset, threatened, humiliated or vulnerable, which undermines their self-confidence and which may cause them to suffer stress 9.
It is important to distinguish between bullying, which is always undermining and destructive, and constructive supervision that is developmental and supportive 8. The three essential elements of bullying are that it has a negative impact on the victim, it is persistent and, crucially, bullying is subjective 10. If a person feels bullied then he/she is being bullied 11. This last point may be controversial because it is dependent on the bullied persons views and not based on objective evidence. Nevertheless workplace bullying exists as a problem. According to the Chartered Institute of Personnel and Development (CIPD) there has been a shift of perception in organisations from denying it happens to accepting that bullying is a problem 3.
How common is bullying?
The Silent Epidemic 7
Workplace bullying affects up to 50 per cent of the UK workforce at some time in their working lives and has an annual prevalence nearly 40 per cent 7. One in 10 callers to the UK National Bullying Advice Helpline are health care professionals 3. A questionnaire survey 12 revealed that 38% of staff in a community healthcare trust were subject to workplace bullying in the previous year and that 42% had witnessed bullying of others. The British Medical Association (BMA) has acknowledged that bullying rates are higher in healthcare organisations and stated that 1 in 7 National Health Service (NHS) staff reported being bullied by other staff 13.
The scale of the problem has been widely highlighted as a problem in the nursing profession 10 with increased rates of bullying reported in Black and Minority Ethnic (BME) groups 14. In doctors bullying may occur in the clinical, educational 8 and research environment 15. One survey of doctors in the UK revealed that 37% of junior doctors had been bullied and 84% had experienced at least one bullying behaviour in the preceding year16. Higher rates have been reported in non-European Union (non-EU) doctors practicing in westernised countries 17 who are also less likely to take action against bullying 18.
Despite the growth of literature in this area the problem of workplace bullying is obscured by underreporting which has numerous causes (figure 2).
Figure 2: Reasons for underreporting of bullying 2
Fear it will make matters worse
The belief that nothing would be done about it
Concerns about confidentiality
Fear of possible victimisation
Concerns of being labelled a troublemaker
May be seen as an admission of failure
A degree of learned tolerance that may imply that the behaviour is acceptable
The greatest fear is that of reprisals from the employer, associates of the bully, and powerful professionals, who may close ranks and compromise the career of the whistle blower 1.
Why do people bully in medicine?
The antecedents to bullying have undergone considerable debate in the psychology literature. Bullies may be attracted to the caring professions to take advantage of the vulnerability embedded in them in relation to clients and employees 1. However in most cases the bullying in medicine is likely to be unintentional and could be shaped by the power inequality in relationships (e.g. consultant Vs junior doctor) in the field.
Moreover the traditional hierarchy within medicine and the teaching by intimidation and humiliation may foster a culture of bullying 18. Studies in the United States 19 and UK 13 have suggested that bullying commences with medical student and that this sets up a transgenerational legacy 7 as the behaviours of bullying are passed down. The BMA urges for a stop to the cycle of bullying and argue further that the target ethos in the health service with the survival of the fittest culture adds to bullying 13.
How do you know if you are being bullied?
If you are being bullied early warning signs may be present. These include the perception that your working relationship is different, that you are being persistently got at, that your work is being unfairly criticised, or you begin to question whether these mistakes you are supposed to have made really are your fault 20. In addition to feelings of being undermined, or humiliated, bullying may also be associated with symptoms (figure 3).
Figure 3: Symptoms of bullying 20
Physical
Emotional
Sleeplessness
Acute anxiety
Nausea
Feeling isolated
Migraine/severe headaches
Loss of confidence/self-esteem
Palpitations
Depression
Skin complaints
Panic attacks
Sweating/shaking
Anger
Stomach problems
Mood swings
Backache
Lack of motivation
Loss of appetite
Suicidal thoughts
Lethargy
Why does bullying matter?
It is clear from the physical and psychological effects that bullying affects people in their personal health. Workplace bullying can also contribute to problems of staff retention and economy. Estimates suggest that in the UK bullying cost employers 80milion lost working days and up to 2-30 billion in lost revenue each year 7. It costs the NHS more than 325 million a year and accounts for around 50 per cent of stress-related workplace illnesses 5.
Other effects of bullying at work include poor morale, poor employee relations, loss of respect for managers or supervisors, poor performance, lost productivity, absences, resignations, damage to organisations reputation and potential costs in tribunal and other court cases 6. Ultimately if the culture of bullying results in demoralized staff working, in a caring profession, it is the patients who will suffer.
What is currently being done about it?
In the UK the BMA has called for zero tolerance on bullying 13 and have provided a report on bullying and harassment in the workplace 21. Most NHS trusts disseminate anti-bullying policies, in connection with Dignity at Work, but the effective implementation of these policies has been questioned with the criticism that it is only for show 18. The information on guidance and policy, in relation to workplace bullying, is not widely publicised and the question is whether bullying is being systematically played down?
Recommendations
Although organisations such as the health service have taken steps to deal with bullying it is clear that problems persist. Heenan 5 states that an all-singing all-dancing policy is worthless without a culture that believes in and supports it and recommends steps employers need to consider (figure 4).
Figure 4: Key steps recommended for employers 5
Look at the culture of the organisation where and how might the risk of harassment arise?
Foster an environment where staff feel able readily to raise any concerns, before they become problems.
To support this, have a clear and well publicised policy to tackle harassment issues.
Back this up with training (including how to handle grievances) and set good examples through role models.
Deal with harassment wherever and however it arises, to demonstrate that it is unacceptable and will not be tolerated.
Provide independent employee assistance, including confidential counselling and other support for employees to enable to challenge unreasonable behaviour which, left unchecked, could lead to harassment.
Figure 5: What to do if you are being bullied 2
Steps to take
Options for support
Approach, or write to, the bully and ask them to stop
Speak to a friend, colleague, supervisor or manager
Ask line manager, supervisor, human resource representative or trade union official to speak to the bully.
Ask employer for support from a specially trained staff member
Keep a record of any incidents and informal action taken
Speak to general practitioner especially if your health is affected
Consider a formal complaint in writing to their line manager or human resources representative
Seek counselling which has been provided by the NHS to its entire staff since 2000
Have a colleague accompany you to any formal investigation meetings
Contact bullying and harassment hotlines
Formal investigation may recommend a disciplinary hearing
Employer may refer you to an external agency for more support
Alternative management action may be considered e.g. facilitated discussion or redeployment
Mediation may be on offer to encourage and help reach an informal outcome
Awareness of bullying needs to be raised and the problem dealt with at an organisational and individual level. The authors suggest that bullying should be incorporated into teaching programmes and induction of junior doctors. Heenan 5 recommends training for managers and supervisors so that they have the confidence to deal with a situation, and deal with it at an early stage, rather then allowing the problem to accumulate and end up in the courts. Therefore it is in the healthcare trusts interests to take these steps to monitor and manage this problem.
In addition employees in healthcare need to be better informed of what steps to take if they find themselves as victims of a bully at work. NHS employers provide options available to deal with bullying and provide support for it (figure 5).
Conclusion
The late Tim Field, founder of the National Workplace Bullying Helpline, warns that everyone is at risk of becoming a target of bullying 1. However the bully in healthcare organisations may not often realise what they are doing, so do both parties require help? There are conflicting views for the solution to bullying in the workplace regarding whether educational 22 or punitive 17 measures are appropriate. This will continue to be a matter of debate. Whichever approach is adopted, identification and increased awareness of bullying is the first step to the solution.
Bullying is an old problem that keeps re-emerging without a clear solution 3
KEY POINTS
Bullying is subjective if you feel bullied then you are bullied
Bullying is more prevalent then we think because of underreporting
Causes of bullying are complex and may be embedded in the culture of the organization
Being bullied is associated with emotional and physical symptoms
Bullying has implications at a personal, social, and organisational level
Implementation of policies by health care trusts need to be improved
Organisations need to be more proactive in raising awareness of this growing menace and demonstrate that it is unacceptable
JAVED LATOO, MBBS, DPM, MRCPsych, North East London NHS Foundation Trust, United Kingdom
CORRESPONDENCE: Dr MINAL MISTRY, Hampshire Partnership NHS Trust, Melbury Lodge, Winchester, United Kingdom
Email: minalmistry@yahoo.co.uk
References
1. Field T, Becker K, Mackenzie GM, and Crossan L. Bullying in medicine. BMJ. 2002; 324: 786.
2. NHS Employers. Bullying and harassment staff guidance. 2007. Available from: http://www.nhsemployers.org/HealthyWorkPlaces/BullyingAndHarassment/Pages/Staffguidance.aspx
3. Al-Daraji WI. An old problem that keeps re-emerging without a clear solution. Medico-Legal Update. 2008; 8(2), 24-30.
4. Kivimki M, Elovaino M and Vahtera J. Workplace bullying and sickness absence in hospital staff. Occup Environ Med. 2000; 57: 656-660.
5. Heenan R. How to beat the workplace bully. Health Service Journal. 12th February 2009: 25-27.
6. ACAS advice leaflet. Bullying and harassment at work: guidance for employees. 2008.
7. McAvoy B and Murtagh J. Workplace bullying the silent epidemic. BMJ. 2003; 326: 776-777.
8. Hicks B. Time to stop bullying and intimidation. Hosp Med. 2000; 61 (6): 428-431.
9. Lyons R, Tivey H, and Ball C. Bullying at work: how to tackle it. A guide for MSF representatives and members. London: MSF. 1995.
10. Quine L. Workplace bullying in nurses. J Health Psych. 2001; 6: 73-84.
11. Macpherson W. Stephen Lawrence inquiry: report of an enquiry by Sir William Macpherson of Cluny. London: Stationary Office. 1999.
12. Quine L. Workplace bullying in NHS community trust: staff questionnaire survey. BMJ.1999; 318: 228-232.
13. BMA Newswire article. BMA calls for zero tolerance on bullying and harassment in the Workplace. 19 May 2006.
14. Giga S, Hoel H, and Lewis D. A review of Black and Minority Ethnic (BME) employee experiences of workplace bullying. University of Bradford, (Research commissioned by the Dignity at Work Partnership). May 2008.
15. Stebbing J, Mandalia S, Portsmouth S, Leonard P, Crane J, Bower M, Earl H and Quine L. A questionnaire survey of stress and bullying in doctors undertaking research. Postgrad Med J. 2004; 80: 93-96.
16. Quine L. Workplace bullying in junior doctors: questionnaire survey. BMJ. 2002; 324: 878-879.
17. Cheema S, Ahmad K, Giri SK, Kaliaperumal VK, Naqvi SA. Bullying of junior doctors prevails in Irish health system: a bitter reality. Ir Med J. 2009; 98(9):274-5.
18. Hoosen A and Callaghan R. A survey of workplace bullying of psychiatric trainees. Psych Bull. 2004. 28: 225-227.
19. Frank E, Carrera JS, Stratton T, Bickel J, and Nora LM. Experiences of belittlement and harassment and their correlates among medical students in the United States: longitudinal survey. BMJ. 2006; 333:682
20. Andrea Adams Trust. Factsheet on workplace bullying. 1997. Available online from: http://www.andreaadamstrust.org/live/factsheet.html
21. BMA report. Bullying and harassment of doctors at work in the workplace, 17 May 2006. Available online from: http://www.bma.org.uk/employmentandcontracts/morale_motivation/bullying2006.jsp
22. Paice E, Aitken M, Houghton A, and Firth-Cozens J. Bullying among doctors in training: cross sectional questionnaire survey. BMJ. 2004. 329: 658-659.
Society of Hospital Medicine (SHM) defines 'Hospitalists' as physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital medicine.
The term "hospitalist"1was first introduced in 1996 by Robert M. Wachter and L Goldman to describe physicians who devote much of their professional time and focus to the care of hospitalized patients. In the most prevalent American model of hospitalist care, several doctors practice together as a group and work full-time caring for inpatients. Most of the (80%) of practicing hospitalists are board certified or eligible in internal medicine, and some (5%) have completed subspecialty fellowships. Although hospitalists first emerged in the care of adult inpatients, the field has grown rapidly in pediatrics, now accounting for nearly 10% of U.S. hospitalists2. Hospitalists typically provide 24/7 inpatient coverage and thus are more readily available to a patient than a doctor who spends much of the day outside the hospital in an office or clinic setting.
Over the past decade, the United States has undergone a remarkable evolution in the way it delivers inpatient medical care. In the mid-1990s, much of American health care was dominated by a managed care paradigm, which gave incentives to control health care inflation3. Hospitalist model was uniquely well versed in evidence based practice and systems improvement. Their focus on providing clinically appropriate care, improving efficiency, reduce length of inpatient stay and helping to make the hospital system work better, without compromising patient satisfaction & outcome was big boon for its growth. Hospitalist field has now become the fastest growing specialty in the history of American medicine, approximately today close to 15,000 hospitalists practice in America, and the field is likely to grow to about 30,000 making it a larger specialty than cardiology4.
Hospitalist Program, St Joseph's Hospital/Marshfield Clinic
In keeping pace with nation wide trend, St. Joseph's Hospital (SJH) Marshfield Clinic, Marshfield was developed in 2000 by the General Internal Medicine Department at the request of clinic leadership. Hospitalst Program was formally launched in October 2001. SJH was pioneer and leader during the time in the Midwest. Dr Qasim Raza & Dr Mark Schwartz were instrumental in establishing a full fledged hospitalist program that has grown tremendously over the years. Dr Bill Yanke, then Chairman of Internal Medicine made into a full subdivision in October 2005 under the leadership of Dr Qasim Raza as Medical Director and Dr Mark Schwartz as Associate Program Director. Today there are 24 full-time hospitalists providing 24/7 hours inpatient medical services, including consultative services to all sub-specialists at Marshfield Center. Their job also includes surgical co-management of all orthopedic patients admitted to St. Josephs hospital.
Hospitalists typically work in shift system, and on any given day we have about 7 day time non-teaching, 2-3 academic teaching, 1 back-up, 2 evening and 1 night time hospitalist covering all medical inpatient services. St. Joseph's Hospital/Marshfield has always been able to recruit the top graduating residents from Internal Medicine Residency/Med-Peds Programs across United States as we believe this is the first step towards success of our program. Many of our hospitalists are actively involved in academic research & teaching and hold Clinical Assistant Professor rank with School of Medicine & Public Health, University of Wisconsin, Madison.
Andy Weir, Director Quality & Strategic Analysis, St. Joseph's hospital (SJH), Ministry Health places our program among the top 15 in the State of Wisconsin. SJH continues to have a lower Length of Stay (LOS) for the top 25 DRG (Diagnosis Related Group) that usually makes typical hospitalist patients. In FY 2007 we still held a 0.16 LOS advantage compared to other 14 hospitals that round up the top 15 hospitals of Wisconsin. This literally means thousands of dollars saved for the patients in todays world of skyrocketing health care costs. This was achieved without significant compromise on quality of care or patient satisfaction. We have far few readmits when compared to our peers in other hospitals of the state. This was only achieved with hard work and dedication of our hospitalist team under the able leadership of Dr Roderick Koehler, Chairman of Internal Medicine Department and full support of Marshfield Clinic Board of Directors.
Marshfield Clinic physicians work in four other hospitalist programs besides St Joseph's Hospital/Marshfield Center. Marshfield Clinic Euclaire, Minocqua & Wausau Centers have 4 full time hospitalists each. Marshfield Clinic Lake View Medical Center; Rice Lake has one full time hospitalist. This makes Marshfield Clinic almost the largest employer of Hospitalists (total of 37 today) in Wisconsin.
The Future : Hospitalists are here to stay
Proponents say Hospitalists fill a growing gap in continuity of patient care. Typically Physicians spend more time today in treating patients in their offices than at hospitals. Hospitals are traditionally getting sicker patients than ever before, and no primary are physicians are willing to take care of unassigned patients (patients with no primary care provider privileged to work in their hospital). Hospitalists are easily available 24 hours daily to take are of these acutely ill patients. Primary care physicians and sub-specialists are happy in that they can spend more time in their practices. There is no competition as Hospitalists have no out-patient practice and their patients return back for follow-up appointments. Its a win-win situation for patients and physicians. Medicare and more insurance companies have now tagged reimbursement with quality of care provided to patients. Research has proven that in-house physicians are good for hospitals goal to achieve these targets5.
Table 1 Potential roles for hospitalists. ( Swiss Med Wkly 2006; 136:591-596 )
Clinical
Inpatient Wards
Intensive Care Unit
Medicine Consultation Services
Palliative Care Services
Post-discharge Clinic Services
Pre-operative Clinic Services
Non-teaching services (in Teaching Hospitals)
Skilled Nursing Facilities
Educational
Residency Program Directorship
Student Clerkship Directorship
Curriculum Development and Leadership
Operational
Emergency Department Triage Officers
Bed Flow Coordination
Discharge Planning Coordination
Transfer Center Coordination
Quality & Safety
Patient Safety Officer
Director of Quality (Compliance)
Quality Improvement Officer
Other
Clinical Information Technology Implementation
Hospital Leadership Positions
Dr Robert Watcher in his landmark article in JAMA concluded that implementation of Hospitalist programs was associated significant reductions in resource use, usually measured as hospital costs (average decrease , 13.4%) or average LOS (average, 16.6%). All research till date has empirically proven that hospitalists improve in-patient efficiency without harmful effects on quality or patient satisfaction6.
Hospitalists come from diverse training backgrounds and hence SHM has started implementing a process to start early training programs for hospitalists, including residency track and fellowship programs. Current educational deficits include training in communication skills, end-of-life care, quality improvement and patient safety, medical economics, follow-up of acute post-op surgical patients. Hospitalists are slowly expanding into other roles beyond the traditional role of medical consultant Table 1.
Hospital Medicine : New Specialty
Specialists in medicine are traditionally defined by organ disease, example Cardiology; Gastroenterology, Nephrology, Radiology, Oncology, General Surgery etc. The hospitalist, on the other hand is a site defined generalist specialist similar to ER physicians. They care for acutely ill patients with wide array of organ derangements and ages in a given specific location7. Hospitalist co-ordinate and integrate patient care within the health delivery system and reduce the distance between office and hospital with their round of clock availability. Hospitalists already have their own Clinical Textbook8 and SHM is the fastest growing medical society in United States and soon plan to get credentials from ABME (American Board of Medical Specialties) to start an accredited fellowship program in Hospital Medicine.
Critical Issues Facing Hospitalists today
There is significant variation in hospitalists training level, and in the way hospitalists groups are managed. Starting a Hospitalist core curriculum in Residency Training program is the key step towards this goal. Marshfield Clinic Internal Medicine Residents already do Hospitalist Service elective rotation for one month during their post-graduate training period at SJH. Funding of hospitalist programs remains a challenge for hospital administrators. Stagnant Medicare reimbursement, rise in uninsured patients, more acutely ill patients are increasing costs, while their ability to support these costs from hospital budgets is decreasing. There is increasing diversity of hospitalists clinical and non-clinical duties, burn out myth due to ever increasing work-loads, rise in demand for hospitalists (1 available for 10 jobs!), perceived shortage may potentially compromising the efficiency and advantages of hospitalists9. Division between out-patient and inpatient practices continues to widen, hence it is vital to maintain connections between referring and primary care physicians. All of these may in-turn negatively impact hospiltalist and patient satisfaction10.
Respondents (patients and allied health care providers) have overwhelming positive impressions of hospitalist movement. In one survey over 76% believed that they improve Emergency Room efficiency, and 66% felt hospitalists lower costs. Interestingly majority 69% would prefer hospitalists have additional certification or training. In 2007 at least 59% and probably closer to 2/3 of California Hospitals have hospitalists. I believe its true for Wisconsin as well. Quality improvement, keeping patients satisfaction (health care customer), challenging all the above critical issues discussed will be the key to success of this hospitalist program at St. Josephs Hospital/Marshfield Clinic in future.
The impact of this revolution in Inpatient care is just beginning to be felt, and history will tell us if this is the best thing that has happened to medicine this decade. Nevertheless, hospital care will likely remain a highly pluralistic system in which organization of care is determined by efforts to improve the value of care in context to local demands and needs11. I am sure everybody will agree that, method of care chosen should always be the one that promotes the best clinical outcomes and highest patient satisfaction at lowest costs. With these goals hospitalists will definitely have increasingly visible role in many institutions across the country in near future.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
MOHAMMED MOIZUDDIN MD, Clinical Assistant Professor of Medicine, School of Medicine & Public Health, University of Wisconsin, Madison. Hospitalist, St. Josephs Hospital/Marshfield Clinic, Marshfield, USA
QASIM RAJA, MD, Director, Hospitalist Division, Department of Internal Medicine, Marshfield Clinic, Marshfield, USA
QURETUL QURESH, MD, Deccan College of Medical Sciences, India
CORRESPONDENCE: MOHAMMED MOIZUDDIN, MD, Department of Internal Medicine, Hospitalist office 3J3, Marshfield Clinic, 1000 North Oak Avenue, Marshfield, USA, WI 54449
Email: moizuddin.mohammed@marshfieldclinic.org
References
1. Watcher RM, Goldman L. The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996; 335:514-7.
2. Bellet PS and Watcher RM. The hospitalist movement and its implications for care of hospitalized children. Pediatrics 1999; 103:47377
3. Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington DC: National Academy Press, 2001.
4. Niraj L Sehgal, RM Watcher The emerging role of "hospitalists" in the American health care system. Swiss Med Wkly 2006; 136:591-596
5. Hospitals & Health Network; June 2006, Vol. 80 Issue 6, p56-60, 3p
Treatment of low back pain remains a dilemma. In the USA more than 300 thousand back surgeries are performed each year. For about 10% to 39% patients, pain may continue or even get worse after back surgeries1. This condition is called failed back surgery syndrome. In the USA, about 80,000 new cases of failed back surgery syndrome are accumulated each year2. Pathological changes such as recurrent disc herniation, arachnoiditis, scar tissue formation, poor surgical indication, misdiagnosis, and surgical technique failure can all contribute to the failure of surgery. Pain after back surgery is difficult to treat. Many patients have to live with pain for the rest of their lives with severe disability.
Over the last several decades, our understanding of the causes of low back pain has been challenged. With a sensitivity up to 95%3, MRI has been used a gold standard for the diagnosis of spine disease such as lumbar disc herniation. With the MRI evidence of a disc herniation and nerve root compression, patients are more easily convinced surgery is their best and only option. However, the reliability of MRI as the evidence for surgical decision has been questioned. An early study found that in a group of asymptomatic volunteers at age of 60 years or older, about 57% had abnormal MRI findings including disc herniation and spinal stenosis4. Follow up studies have yielded similar results. Now it is widely accepted that degenerative disc disease, such as disc herniation is a common finding in asymptomatic adults. Even though at the age of 60 years or older, 57% or more may have abnormal MRI findings in the lumbar spine, however, only less than 20% of this group of people have chronic low back pain. A recent study also suggested a lack of correlation between imaging findings of spine degenerative change and back pain5. Simply, degenerative change in the lumbar spine, such as a herniated disc, is not necessary painful.
The results of these studies have changed our belief in the relationship between lumbar disc herniation and back pain. It is believed that back and leg pain in the presence of acute disc herniation is not merely the result of a pinched nerve root, rather it is more related to the inflammation of the nerve roots and nerve endings around the herniated disc or it may be the combined results of chemical inflammation and mechanical compression6. A herniated disc is not a sole indication for back surgery and up to 70% to 95% of patients may be pain free after 12 months without major intervention7. The primary goal of treatment of lumbar radicular pain should be the suppression of inflammation, relieving the pain and restoring function rather than removal of the herniated disc. Before one chooses an open back surgery the following options should be considered:
Diagnosis: Low back pain can be related to a herniated disc, nerve root irritation, annular tear, facet joint arthritis, muscle spasm, injuries to the ligament, sacroiliac joint arthritis and referred pain from visceral organs. An MRI finding of a herniated disc, no matter how large, is not enough to justify surgery. A thorough history and physical examination is tantamount to judge whether the herniated disc is the real source for the ongoing pain.
Medications: Non-steroid anti-inflammatory medications should be offered as the first line medication to patients with mild back pain. Early administration of oral steroid medication in patients with acute sciatica may lead to slightly more rapid improvement in pain, mental well-being, and disability scores8. Anti-depressants, especially tricyclic antidepressants, are often used to treat patients with chronic back pain.
Physical therapy, massage therapy and chiropractic management have been widely used for treatment of back pain and lumbar radicular pain, even though the value of these treatment modalities have yet to be proven.
Spine injections: Multiple double blind, clinical controlled studies have confirmed the clinical efficacy of lumbar epidural steroid injection (LESI) in relieving the acute radicular pain due to herniated nucleus pulposus, speeding the rate of recovery and return to function9. The pain relieving effect of LESI may last up to three months. Inflammatory mediators, such as phospholipase A2, have been implicated in lumbar radiculopathy and disc herniation and have been the focus of recent research. Lumbar epidural steroid injections can decrease pain by suppressing the function of inflammatory mediators. As long as the patient is pain free and is without any neurological deficits, a herniated disc should not be a clinical concern. Even though LESI alone may not decrease the necessity of back surgery, it will be intriguing to investigate whether a combination of LESI and other treatment such as physical therapy and life style modification will decrease the need for surgery.
Minimally invasive surgery: Minimally invasive surgery offers another alternative in the treatment of back pain. These treatments include chymopapaine, percutaneous nucleotome, automated percutaneous lumbar discectomy, laser discectomy, neucleoplasty and disc deKompressor. The advantage of the minimally invasive techniques is that it leaves no or minimal scar after the surgery. Among the minimal invasive techniques, laser discectomy has a reported success rate of 80% to 90%10. Neucleoplasty and disc deKompressor have been recently introduced with early non-controlled studies showing success rates up to 78%11. These procedures are still not widely accepted and more studies are needed to confirm their clinical efficacy.
Life style modification: Low back pain can often be the result of improper lifestyle choices. Smoking can increase the risk of low back pain12. Obesity can worsen back pain and contribute to disk degeneration13. Heavy lifting, sport related injuries and motor vehicle accidents can cause back pain. Education to patients with low back pain is critical to help them recover from back pain and prevent future back pain. Smoking cessation and weight control should be strongly recommended to back pain patients. Proper exercise techniques should be taught. Patients, especially those with spinal stenosis often have difficulty walking due to neurological claudication. Treadmills and long distance walking exercise may exacerbate back pain. Some studies suggested therapeutic aquatic exercise is potentially beneficial to patients suffering from chronic low back pain14.
Conclusion: Lumbar spine surgery can potentially provide quick pain relief and functional recovery. There are many downsides to surgery however that would include post laminectomy surgery syndrome and a lack of proven long term benefit. Because of these risks one should be very careful in determining surgical candidacy. A preliminary study15 has provided the evidence that the rate of back surgery can potentially be decreased through appropriate education and application of evidence-based medicine for patients, general practitioners and spine surgeons. Conservative treatment with the combination of medications, physical therapy, spinal injections and life style modification should be tried before surgery is considered.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
YILI ZHOU, MD, PH.D, Comprehensive Pain Management of North Florida, USA
STEPHEN IRWIN, MD, Comprehensive Pain Management of North Florida, USA
CORRESPONDENCE: YILI ZHOU, MD, PH.D, Medical Director, Comprehensive Pain Management of North Florida, Gainesville, USA, FL32608
Email: Yilizhoumd@yahoo.com
References:
Graz B, Wietlisbach V, Porchet F, et al. Prognosis or "curabo effect?": physician prediction and patient outcome of surgery for low back pain and sciatica. Spine 2005 June 15;30(12):1448-52.
Ragab A, Deshazo RD. Management of back pain in patients with previous back surgery. Am J Med 2008 April;121(4):272-8.
Mullin WJ, Heithoff KB, Gilbert TJ, Jr., et al. Magnetic resonance evaluation of recurrent disc herniation: is gadolinium necessary? Spine 2000 June 15;25(12):1493-9.
Boden SD, Davis DO, Dina TS, et al. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 1990 March;72(3):403-8.
Kalichman L, Kim DH, Li L, Guermazi A, et al. Spondylolysis and spondylolisthesis: prevalence and association with low back pain in the adult community-based population. Spine 2009 January 15;34(2):199-205.
Roberts S, Butler RC. Inflammatory mediators as potential therapeutic targets in the spine. Curr Drug Targets Inflamm Allergy 2005 April;4(2):257-66.
Legrand E, Bouvard B, Audran M, et al. Sciatica from disk herniation: Medical treatment or surgery? Joint Bone Spine 2007 December;74(6):530-5.
Holve RL, Barkan H. Oral steroids in initial treatment of acute sciatica. J Am Board Fam Med 2008 September;21(5):469-74.
Sethee J, Rathmell JP. Epidural steroid injections are useful for the treatment of low back pain and radicular symptoms: pro. Curr Pain Headache Rep 2009 February;13(1):31-4.
Goupille P, Mulleman D, Mammou S, et al. Percutaneous laser disc decompression for the treatment of lumbar disc herniation: a review. Semin Arthritis Rheum 2007 August;37(1):20-30.
Al-Zain F, Lemcke J, Killeen T, et al. Minimally invasive spinal surgery using nucleoplasty: a 1-year follow-up study. Acta Neurochir (Wien ) 2008 December;150(12):1257-62.
Mikkonen P, Leino-Arjas P, Remes J, et al. Is smoking a risk factor for low back pain in adolescents? A prospective cohort study. Spine 2008 March 1;33(5):527-32.
Hangai M, Kaneoka K, Kuno S, et al. Factors associated with lumbar intervertebral disc degeneration in the elderly. Spine J 2008 September;8(5):732-40.
Waller B, Lambeck J, Daly D. Therapeutic aquatic exercise in the treatment of low back pain: a systematic review. Clin Rehabil 2009 January;23(1):3-14.
Goldberg HI, Deyo RA, Taylor VM, et al. Can evidence change the rate of back surgery? A randomized trial of community-based education. Eff Clin Pract 2001 May;4(3):95-104.
Psychiatry is an unattractive profession. A bold statement to be made by medical students who have committed four years to this vocation, with an additional lifetime to follow. However, if facts and figures are to be believed medical students are turning their backs on this once valued and highly sought after profession and are chasing the glamour of emergency room medicine, serialised by popular television programmes. Within the UK approximately 4% of newly-qualified doctors specify Psychiatry as their first preference1, a remarkable low number, considering vast numbers qualify every August.
Maybe approaches like The Student Psychotherapy Scheme (SPS), implemented some 43years ago at University College London is needed. Whereby, medical students were given the opportunity to experience the doctor-patient relationship in a psychiatric setting. This led to a higher proportion of students choosing Psychiatry as a speciality, compared to a control group that were not given the opportunity.
The influence of a student psychotherapy scheme – a10-year retrospective study (2004)2
163 medical students undertook the SPS scheme, of which 77 replied to the questionnaire. Of these, 11, (14.3%), had become Psychiatrists, who had not thought about doing Psychiatry before entering the scheme. In the control group of 152, of which 128 responded, only two, (1.6%), had become Psychiatrists, who had not thought about this speciality at the same stage.
So why did the SPS have such an impact improving recruitment rates amongst medical students? From my point of view, it seems to be simply due to exposure. Exposure to the unknown and familiarisation of a speciality that is not regularly given the time and efforts during our medical training at University.
Our time in Psychiatry was punctuated by apprehension and a sense of intrigue. The hesitancy was rooted in preconceived notions that we were being sent to a sanatorium, whereby we would be battling to shake off patients that had latched on to my trouser legs in a bittersweet attempt to escape everyday - thankfully that never came into fruition. However, what did occur was far more surprising. We could see ourself pursuing a career in this speciality in the not so distant future. With acute medical emergencies, there seems to be an emphasis placed on ‘patching’ patients up and sending them home in an attempt to meet targets and tick all the boxes. With Psychiatry you play the ‘waiting game’, it requires patience, the efficacy of treatments rely on regular and lasting compliance, and the majority of benefits are seen in the long-term rather in an acute setting. Maybe the high rate of morbidity in psychiatric illnesses we see in our ageing population is dissuading potential Psychiatrists. Whatever the reason, there is a risk that this speciality will be understaffed in the future, creating a vacuum of care for those that really need it, especially when they do not have the mental faculties to be aware of their own needs.
The problem with Medicine as opposed to other careers is the wide range of specialities and sub-specialities that are available to students once they have finished the formal University training. There are the baseline individual specialities, such as Surgery, Medicine or General Practice – all of which have sub-specialities, intensifying their focus on particular area of clinical care available to patients. Perhaps that is why, in most cases, students allow their path to be dictated by their interests rather then the greater good of Medicine as a whole. As stated, there is a current crisis in Psychiatry, with only a 4% recruitment of newly qualified doctors. The 5-year undergraduate medical degree only allows a small window of exposure to Psychiatry and this is not enough to be able to explore the speciality and come to a conclusion, which would affect the students for the rest of their lives. Perhaps the short period of exposure continues to exacerbate the problem that most medical students view Psychiatry as a separate entity to Medicine, completely devoid of concrete management, unable to implement true and tested methods that would guarantee a cure.
There are 12 different sub-specialities in psychiatry3, of which we were exposed to General Adult and Old Age Psychiatry, from our time there we were able to experience the full spectrum of presentation, from the difficulties of dealing with mentally unstable patients, to the satisfaction of seeing slowed and gradual progress in someone’s mental wellbeing. What Psychiatry offers, that some fields tend to lack is rapport, created by extended patient contact and treating them as a whole rather then a specified issue. It dawned on me that even general practitioners do not have the luxury of getting to know their patients as well as Psychiatrists and that appealed to me a great deal, as I believe in the holistic approach to management. However, Psychiatry is still viewed as being disconnected from the rest of Medicine, perhaps due to the different history taking techniques, the lack of focus on the practical skills of medicine, the ‘trial and error’ method of therapy, whereby if one drug does not work another is given. Instead the focus lies on communication skills and other psychosocial aspects and this I find dissuades many of my colleagues, as there is nothing tangible for them to get to grips with and apply their knowledge to. In hindsight, Psychiatrists are not wholly responsible for just the mental health of a patient, but it does fall within their remit to identify, and manage co-morbidities they may have as well. A sound knowledge of all aspects of Medicine is required, and maybe the fact that ‘mind and body’ needs treating discourages future Psychiatrists.
Overall, there have been many times when we have been surprised at our own interest in Psychiatry. It is comforting to know that it is a welcoming speciality, unlike many other competitive specialities where there is intense pressure and any sense of enjoyment or achievement may be diminished. There are also immense opportunities open for research, even at this level as a medical student. Undoubtedly compared to other fields, Psychiatry offers a balance between work and personal life. Our only regret is that we did not have the opportunity to experience everything that Psychiatry has to offer, and make a more informative and well balanced decision on where my future lies within Medicine. Perhaps we will take the initiative to explore this field in my own time. One thing is for certain, Psychiatry is a dynamic field with many opportunities, and should not be disregarded for the flashing blue lights of emergency medicine.
COMPETEING INTERESTS
None Declared
AUTHOR DETAILS
MASHUD SOUROYER, 4th Year Medical Student, Bart’s and London School of Medicine and Dentistry, United Kingdom
MATHAVI UTHAYANAN, 4th Year Medical Student, Bart’s and London School of Medicine and Dentistry, United Kingdom
[1] The Royal College of Psychiatrists: Tackling the recruitment crisis in psychiatry Student Psychotherapy Scheme encourages medical students to choose psychiatry as a career [online]. 2004. Available URL: http://www.rcpsych.ac.uk/pressparliament/pressreleasearchive/pr550.aspx [Accessed 02/12/2008]
[4] Michael Gelder, Richard Mayou and John Geddes. Psychiatry: Third edition. Oxford University Press, 2005.
[5] Psychiatric Bulletin: What impact do undergraduate experiences have upon recruitment into psychiatry? [online]. 2007. Available URL:http://pb.rcpsych.org/cgi/content/full/31/2/70 [Accessed 02/12/2008]




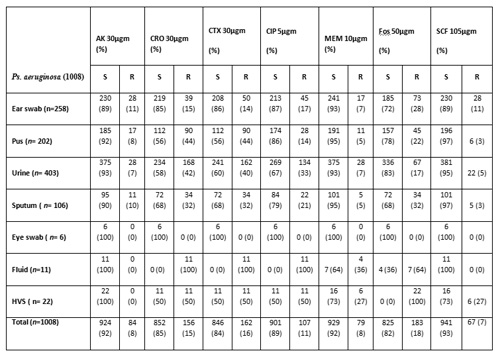
 Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair.
Figure 1- Photograph showing gravid uterus lying in the incisional hernia sac The overlying skin was necrosed with evidence of ulceration and the presence of engorged veins. The fetus was lying in the herniated gravid uterus outside the abdominal cavity. Routine investigations were within normal limits. Ultrasound examination showed the uterus herniated in the incisional hernia of the anterior abdominal wall with the live fetus in cephalic presentation without any gross congenital malformation. The placenta was located in the upper uterine segment. She was kept in the hospital for bed rest with abdominal support. Emollients & antiseptic skin ointment were applied over the skin of the anterior abdominal wall. An elective caesarean section was planned for 37 weeks but she went into labour at 36 weeks. The abdomen was opened by elliptical incision. The uterus was visualized just beneath the skin and there was no evidence of the rectus sheath in the vicinity of the incision. A uterineincision was made over the previous caesarean scar and the baby was delivered with APGAR 7/10 at 1 minute and 9/10 at 5 minutes. The uterus was repaired in layers and a bilateral tubal ligation was done. Herniorraphy was performed in double buttress fashion. She was given a course of antibiotics. Her post operative period was uneventful and she went home with a healthy baby weighing 2.25 Kg. During her follow up visits she was found to be problem free. Discussion The remote complication of a caesarean section could be an incisional hernia due to defective abdominal wound healing and herniation of gravid uterus through the abdominal wall. This is a rare complication.1 The complications that have been reported in literature in association with this complication include strangulation, abortion, pre-term labour, accidental haemorrhage, intrauterine fetal death and rupture of the lower uterine segment.2 Excessive stretching of the skin may cause ulceration of the skin as in this present case due to friction between the hernia sac and other parts of the patient’s body. Caesarean section should be performed and herniorrhaphy can be performed during the caesarean section as in the present case.1 Herniorrhaphy can be performed during pregnancy if there is evidence of morbid incarceration or the skin is necrosed.3 However, herniorrhaphy can be postponed until delivery, as the enlarged uterus may interfere with healing of the repair. Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2)
Image 1: Initial chest x-ray revealing bronchogenic cyst in the posterior right middle lobe (10x10x8 cm3) Computerized tomography (CT) scan showed a large cystic lesion arising entirely within the right lower lobe and extending the width of the hemithorax. (Image 2) 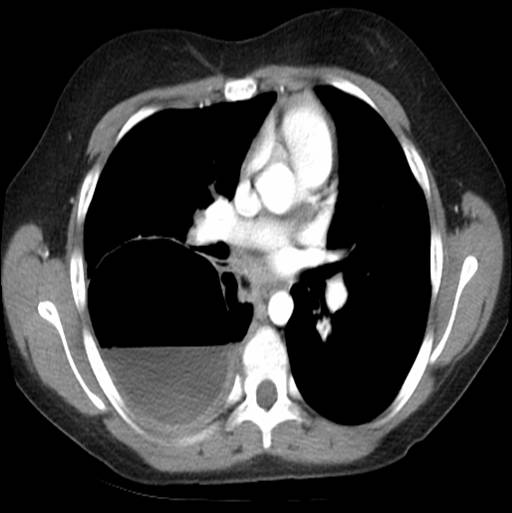 Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4)
Image 2: Chest CT shows bronchogenic cyst extending the entire width of the right hemithorax and approximately 50% full of fluid. There was an air-fluid level occupying ~50% of the cavity. She was diagnosed with a multilocular bronchogenic cyst. She was briefly hospitalized and discharged on azithromycin with plans to resect the cyst in one month. Severe cough, fever, and chills prompted readmission after 3 weeks of antibiotic therapy. CXR and CT showed cyst enlargement (16x9x11 cm3) with over 95% fluid. (Images 3 and 4)  Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid.
Image 3: Substantial bronchogenic cyst (16x9x11 cm3), over 95% full of fluid.  Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung.
Image 4: Lateral chest x-ray revealed opacification along superior margin of cyst. She was started on ampicillin/sulbactam. Percutaneous drain placement yielded a large volume of turbid fluid. Aerobe, anaerobe and fungal studies of the fluid were negative. Resection was postponed due to significant inflammation surrounding the cyst cavity. She was discharged on a seven day course of amoxicillin/clavulanate. Following six weeks of cyst drainage, a thoracoscopic right lower lobectomy was performed. Extensive inflammation and induration made dissection of the lower lobe and pulmonary vessels challenging. Fibrinoid adhesions extended to the pleural surface. Operative time was 418 minutes. Surgical pathology showed diffuse necrotizing granulomatous inflammation with acid-fast bacilli and multiple nodules up to 3.3 cm in diameter. Ninety-five percent of the pleural surface had nodular involvement. (Image 5) Areas of non-indurated lung also showed small nodules with a miliary appearance. Inflammation was present at the bronchovascular margins, hilar nodes, and distal lung.  Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
Image 5: Gross specimen of right lower lobe: Approximately half of the lobe was indurated and 95% of surfaces showed nodular involvement. Sectioning through indurated region revealed diffuse nodules up to 3.3 cm. Nonindurated lung showed small nodules with miliary appearance. The patient had no history of tuberculosis exposure, foreign travel or immunodeficiency. There was no family history of tuberculosis or respiratory disease. Based on the acid-fast bacilli identified on pathology stain, fluid drained from her chest tube was sent for acid-fast bacilli culture and smear. Mycobacterium was not isolated. It was determined that the source of the atypical mycobacterial infection was likely colonizing mycobacteria from her oropharynx that became entrapped in the cyst. A six-week course of clarithromycin, rifampin, and ethambutol was prescribed to treat any remaining organisms. At two-month follow-up, she had minimal pulmonary symptoms and inflammatory markers were improved. Erythrocyte sedimentation rate (normal: 0-15) and C-reactive protein level (normal: 0-10) decreased from 88 and 173 during her hospitalization, to 10 and 3.6, respectively. At four-month follow-up, she had resumed competitive sports and had no evidence of ongoing infection. Discussion: This case highlights a unique presentation of infected bronchogenic cyst after substantial cyst growth. Unusual aspects include the late onset of symptoms, multilocular intraparenchymal cyst appearance, turbid drainage, extensive nodularity, necrotizing granulomatous inflammation, and atypical Mycobacterium infection. Although comorbid infection is not uncommon, causative organisms are typically Haemophilus influenzae1,2 and Streptococcus pneumoniae.3 Cases of Streptococcus pyogenes,4 Escherichia coli,5and Salmonella enteritidis6have been reported. However, only four cases of bronchogenic cyst with Mycobacterium infection have been documented.7,8,9 Three of the Mycobacterium-infected cases are adult patients. Lin et. al reported a 39-year-old female with bronchogenic cyst complicated by Mycobacterium avium infection.7 The organism was identified by genetic sequencing of biopsied lung tissue. Sputum acid-fast stain and mycobacterial cultures were negative. Liman et al. reported two adult cases: a 20 year-old male with Mycobacterium identified in a right lower lobe specimen but with negative sputum culture, and a 32 year-old female with Mycobacterium isolated in a sputum culture but a negative microscopic exam and cyst fluid culture.8 The only documented paediatric case, a 9 year-old female with a 6 cm right lower lobe bronchogenic cyst, was reported by Houser et al.9 She underwent lobectomy; Kinyoun stain of the cyst specimen showed Mycobacterium. Sputum culture and acid-fast bacilli stain were negative. Tuberculin skin test was positive. Comorbid infection with Mycobacterium tuberculosis was suggested, but they were unable to isolate an organism. Treatment consisted of four months of rifampin and two years of isoniazid with pyridoxine. This is the first documented paediatric case of bronchogenic cyst infected with atypical Mycobacterium. Her presentation is noteworthy, given the substantially greater size of the cyst (16x9x11 cm), extensive pathologic findings, and success with a different antibiotic regimen.
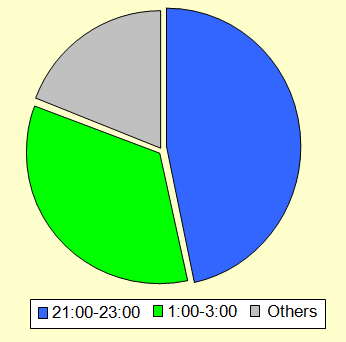 Figure 1, illustrates a distribution of the peak work-load period which occurred between 9pm-11pm and 1am-3am. This finding contradicts previous surveys done prior to the implementation of the hospital at night where it was noted that the nights were quieter and sub-specialist such as orthopaedic surgeons were not working as hard as general medics (1).
Figure 1, illustrates a distribution of the peak work-load period which occurred between 9pm-11pm and 1am-3am. This finding contradicts previous surveys done prior to the implementation of the hospital at night where it was noted that the nights were quieter and sub-specialist such as orthopaedic surgeons were not working as hard as general medics (1). 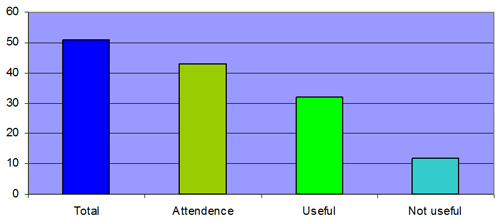 Figure 2, shows the overall experience of the hand-over as judged by the orthopaedic juniors. There was an eighty-five percent (43/51) attendance by the on-call orthopaedic juniors of which seventy-two percent (32/44) thought that it was a useful experience
Figure 2, shows the overall experience of the hand-over as judged by the orthopaedic juniors. There was an eighty-five percent (43/51) attendance by the on-call orthopaedic juniors of which seventy-two percent (32/44) thought that it was a useful experience 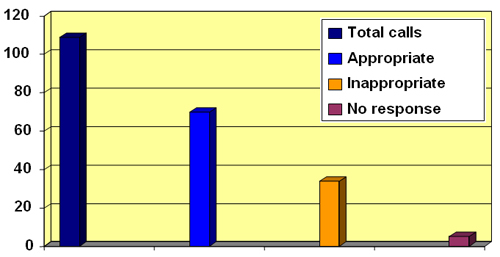 Figure 3 illustrates a distribution of the calls received. As illustrated, 37/109 calls were viewed as inappropriate The majority of the orthopaedic juniors surveyed framed hospital-at-night hand-over was useful but thirty-four percent (37/109) of the calls they received were viewed as inappropriate (Fig 2,3). The most frequent of the inappropriate ward calls were ‘requests to rewrite drug-charts’ (Fig 4,5).
Figure 3 illustrates a distribution of the calls received. As illustrated, 37/109 calls were viewed as inappropriate The majority of the orthopaedic juniors surveyed framed hospital-at-night hand-over was useful but thirty-four percent (37/109) of the calls they received were viewed as inappropriate (Fig 2,3). The most frequent of the inappropriate ward calls were ‘requests to rewrite drug-charts’ (Fig 4,5). 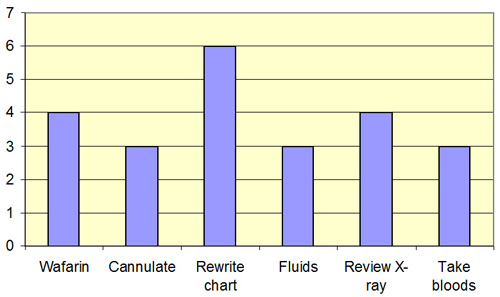 Figure 4 describes the frequencies of these calls. As illustrated the most frequently inappropriate ward-call was to ‘rewrite drug-charts’. There were twenty-three (23/37) inappropriate ward-calls
Figure 4 describes the frequencies of these calls. As illustrated the most frequently inappropriate ward-call was to ‘rewrite drug-charts’. There were twenty-three (23/37) inappropriate ward-calls 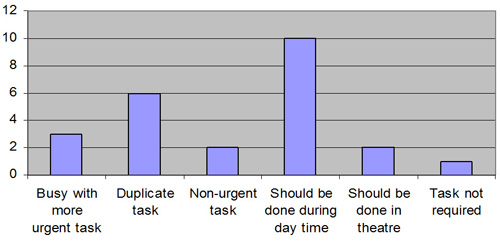 Figure 5 shows the reasons given by the on-call doctors for the inappropriate tasks. The most frequently given reason was that ‘the request should have been done during the day’. The second most frequently given reason for inappropriate calls was the fact that ‘it was a duplicated request’ Our survey also highlighted that the most frequently given reason for inappropriate tasks was firstly that the request should have been done during the day and secondly that it was a duplicated request. These findings seem to defeat the key purpose of the hospital-at-night project for an orthopaedic SHO on-call. Conclusion: Hospital at night cannot function in isolation. There are fewer doctors available then normally and the system has to use their time effectively. 30% of inappropriate calls to wards were to rewrite drug charts and to prescribe warfarin. This should have been identified and performed by the day staff. 10% of calls were to review X-rays. Much of the inappropriate activity could be pre-empted if both day and night staff attended the handover and the tasks outstanding from the day identified. The doctor on the night could then perform an hourly ward round completing these tasks without interrupting at the beginning of the night.
Figure 5 shows the reasons given by the on-call doctors for the inappropriate tasks. The most frequently given reason was that ‘the request should have been done during the day’. The second most frequently given reason for inappropriate calls was the fact that ‘it was a duplicated request’ Our survey also highlighted that the most frequently given reason for inappropriate tasks was firstly that the request should have been done during the day and secondly that it was a duplicated request. These findings seem to defeat the key purpose of the hospital-at-night project for an orthopaedic SHO on-call. Conclusion: Hospital at night cannot function in isolation. There are fewer doctors available then normally and the system has to use their time effectively. 30% of inappropriate calls to wards were to rewrite drug charts and to prescribe warfarin. This should have been identified and performed by the day staff. 10% of calls were to review X-rays. Much of the inappropriate activity could be pre-empted if both day and night staff attended the handover and the tasks outstanding from the day identified. The doctor on the night could then perform an hourly ward round completing these tasks without interrupting at the beginning of the night.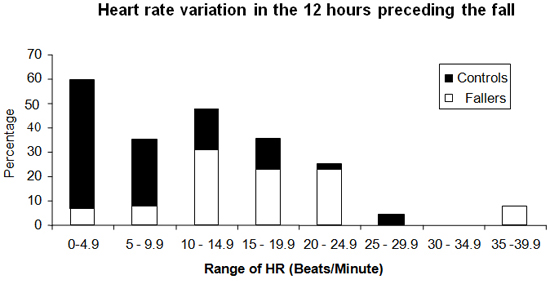
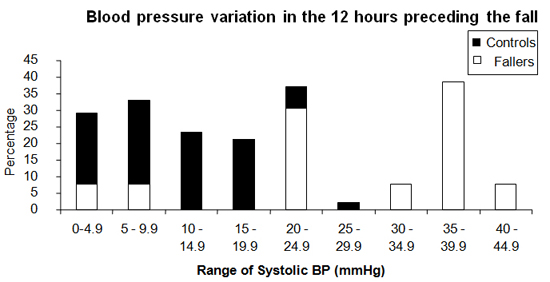
 Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3.
Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3.  Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835).
Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835).  Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values.
Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values. 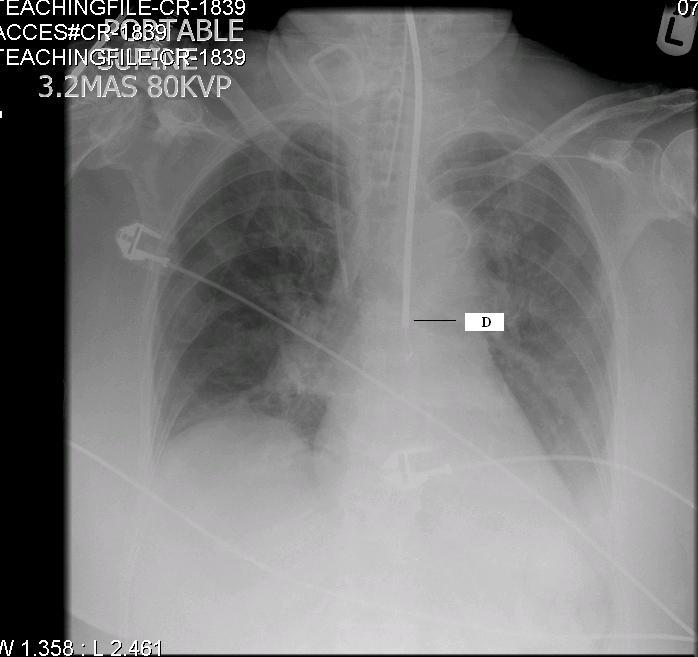 Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6]. 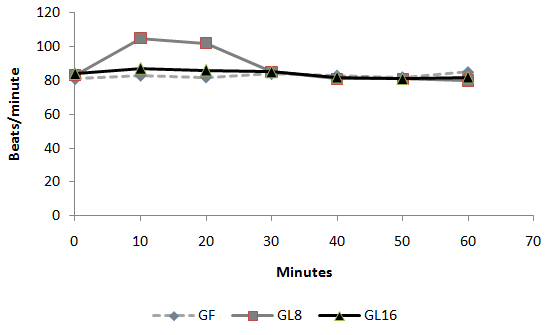 Fig 1: Intra-operative changes in heart rate in groups
Fig 1: Intra-operative changes in heart rate in groups 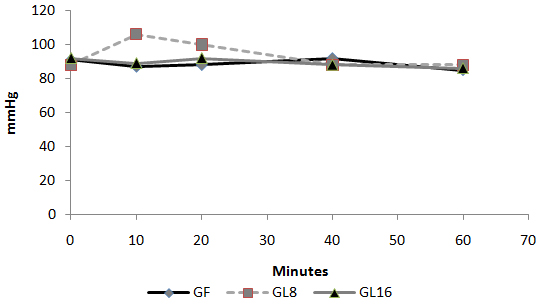 Fig 2: Intra-operative changes in MAP in groups
Fig 2: Intra-operative changes in MAP in groups 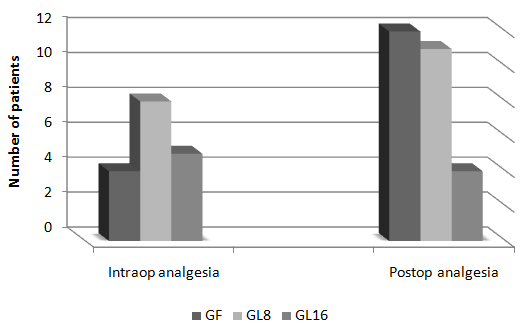 Fig 3: Number of patients requested perioperative analgesic supplementation
Fig 3: Number of patients requested perioperative analgesic supplementation 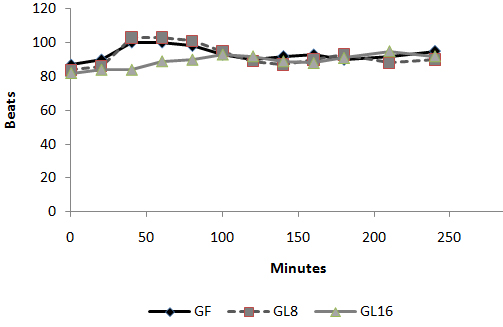 Fig 4: Changes in heart rate in PACU
Fig 4: Changes in heart rate in PACU 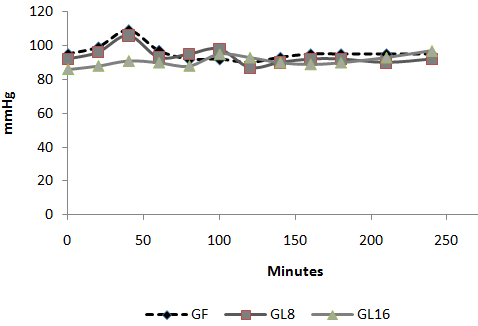 Fig 5: Changes in MAP in PACU:
Fig 5: Changes in MAP in PACU: 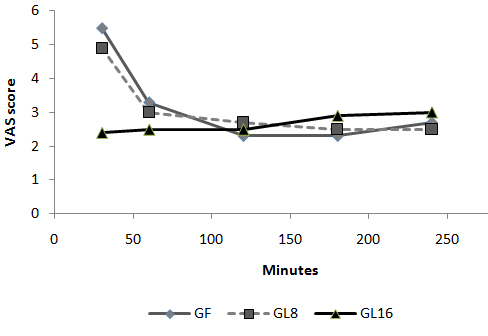 Fig 6: Changes in VAS in PACU Discussion: The use of an opioid, even a short acting one can be associated with adverse effects, which may not be acceptable for patients scheduled for day case surgery. For this reason, it was suggested to substitute an opioid with a non-opioid analgesic for postoperative pain control. The use of a NSAID is associated with adverse effects [1]. Lornoxicam has been successfully used in the prevention and treatment of postoperative pain. It has been shown to be as effective as morphine [4], meperidine [5] and tramadol [6]. To the best of our knowledge, this is the first study to compare the perioperative analgesic efficacy of lornoxicam to fentanyl in patients undergoing day case ENT surgery. We gave Lornoxicam half an hour before induction of anesthesia as the time taken to reach peak plasma concentration (Tmax) was determined to be 0.5 h [7]. During the operative procedure, HR and MAP were significantly higher in group L8 compared to group F and L16. While in PACU, patients in groups F and L8 had higher HR, MAP and VAS score in the early postoperative period compared to patients in group L16. This may be due to inadequate analgesic effect of L8 and the shorter plasma half life of fentanyl compared to L16. The analgesic efficacy of L16 might be attributable to inhibition of cyclo-oxygenase (COX1) and (COX2) activity [2], release of endogenous dynorphin and β-endorphin [5], decrease in peripheral and central prostaglandin production [8] as well as exertion of some of its analgesic activity via the central nervous system [9]. Lornoxicam has a more potent anti-inflammatory and analgesic effect than other oxicams as well as a shorter half life, which decreases the incidence of side effects of drugs with long plasma half life [10]. Arslan and colleagues reported decreased opioid need, PONV and postoperative pain scores when 16 mg of lornoxicam was administered after thyroidectomy [11]. While Xuerong and colleaguessuggested that the increase of postoperative morphine requirements induced by intra-operative administration of fentanyl could be prevented by ketamine or lornoxicam [12]. Rawal reported that NSAIDs are effective as the sole analgesic in a high proportion of cases of mild to moderate pain and it is more convenient to give these drugs by the IV route rather than by IM or rectal administration [13]. The analysis of pain intensity differences was complicated by the fact that many patients postoperatively were asleep at the time their pain assessments were due which may be attributed to effect of opioid and anesthetic medications used. To minimize any missing data we used time to the first dose rescue analgesia (based on changes in hemodynamic data) to evaluate pain intensity differences from baseline. L16 was well tolerated in this study, and was associated with a significantly lower incidence of adverse events than F and L8 which could be due to the opioid side effects in both groups. Norholt and colleaguessupported our results as they reported that, in terms of common acute adverse events, lornoxicam appeared to possess a higher benefit/risk ratio compared with morphine [4]. Zuurmond et al reported that, there is good evidence that avoidance of opioid virtually abolishes the PONV that preclude oral intake of fluids after surgery [14]. In our study, nausea developed in 25.7% of patients in group F, 20% in group L8 but only 8.6% in group L16 who received the least rescue opioid analgesia. Regarding bleeding abnormalities, Hodsman et al reported extensive bleeding required reoperation on two diclofenac group patients submitted to abdominoperitoneal resection of the rectum [15]. In our study no abnormal bleeding was reported by ENT surgeons in any of the study patients. In agreement with our results, Ilias et al[16], Trampitsch et al[17] and Karaman et al [18] used lornoxicam and they did not detect problems with surgical bleeding, bleeding time, blood transfusion requirement or postoperative bleeding. Stroissnig et al reported that overall, in healthy adult volunteers, oral doses of lornoxicam up to 70 mg have been well tolerated, and there have been no effects on vital signs, urine analysis parameters or clinical serum biochemistry [19]. In our study, none of the patients receiving study drugs experienced severe gastric discomfort, needed rescue antiemetic medication or required admission because of poor pain control. Previous studies used lornoxicam for reduction of postoperative opioid consumption but none of them had studied the intra-operative use of lornoxicam. So, we selected certain type of surgical procedures which might be suitable to use lornoxicam as a sole intra-operative analgesia. The adjunctive use of acetaminophen may have additive analgesic efficacy to lornoxicam because of its intrinsic opioid-sparing activity. Measurement of serum catecholamine would have been useful. These could be considered as a limitation for the present study. Conclusion: Intravenous 16 mg lornoxicam with the present study design was comparable to 100 µg fentanyl as intra-operative analgesia but more effective than fentanyl in preventing early postoperative pain in mild to moderate ENT surgical procedures. Intravenous lornoxicam 8 mg was not satisfactory as a sole intra-operative analgesia. The overall incidence of adverse effects of lornoxicam was lower than that of fentanyl.
Fig 6: Changes in VAS in PACU Discussion: The use of an opioid, even a short acting one can be associated with adverse effects, which may not be acceptable for patients scheduled for day case surgery. For this reason, it was suggested to substitute an opioid with a non-opioid analgesic for postoperative pain control. The use of a NSAID is associated with adverse effects [1]. Lornoxicam has been successfully used in the prevention and treatment of postoperative pain. It has been shown to be as effective as morphine [4], meperidine [5] and tramadol [6]. To the best of our knowledge, this is the first study to compare the perioperative analgesic efficacy of lornoxicam to fentanyl in patients undergoing day case ENT surgery. We gave Lornoxicam half an hour before induction of anesthesia as the time taken to reach peak plasma concentration (Tmax) was determined to be 0.5 h [7]. During the operative procedure, HR and MAP were significantly higher in group L8 compared to group F and L16. While in PACU, patients in groups F and L8 had higher HR, MAP and VAS score in the early postoperative period compared to patients in group L16. This may be due to inadequate analgesic effect of L8 and the shorter plasma half life of fentanyl compared to L16. The analgesic efficacy of L16 might be attributable to inhibition of cyclo-oxygenase (COX1) and (COX2) activity [2], release of endogenous dynorphin and β-endorphin [5], decrease in peripheral and central prostaglandin production [8] as well as exertion of some of its analgesic activity via the central nervous system [9]. Lornoxicam has a more potent anti-inflammatory and analgesic effect than other oxicams as well as a shorter half life, which decreases the incidence of side effects of drugs with long plasma half life [10]. Arslan and colleagues reported decreased opioid need, PONV and postoperative pain scores when 16 mg of lornoxicam was administered after thyroidectomy [11]. While Xuerong and colleaguessuggested that the increase of postoperative morphine requirements induced by intra-operative administration of fentanyl could be prevented by ketamine or lornoxicam [12]. Rawal reported that NSAIDs are effective as the sole analgesic in a high proportion of cases of mild to moderate pain and it is more convenient to give these drugs by the IV route rather than by IM or rectal administration [13]. The analysis of pain intensity differences was complicated by the fact that many patients postoperatively were asleep at the time their pain assessments were due which may be attributed to effect of opioid and anesthetic medications used. To minimize any missing data we used time to the first dose rescue analgesia (based on changes in hemodynamic data) to evaluate pain intensity differences from baseline. L16 was well tolerated in this study, and was associated with a significantly lower incidence of adverse events than F and L8 which could be due to the opioid side effects in both groups. Norholt and colleaguessupported our results as they reported that, in terms of common acute adverse events, lornoxicam appeared to possess a higher benefit/risk ratio compared with morphine [4]. Zuurmond et al reported that, there is good evidence that avoidance of opioid virtually abolishes the PONV that preclude oral intake of fluids after surgery [14]. In our study, nausea developed in 25.7% of patients in group F, 20% in group L8 but only 8.6% in group L16 who received the least rescue opioid analgesia. Regarding bleeding abnormalities, Hodsman et al reported extensive bleeding required reoperation on two diclofenac group patients submitted to abdominoperitoneal resection of the rectum [15]. In our study no abnormal bleeding was reported by ENT surgeons in any of the study patients. In agreement with our results, Ilias et al[16], Trampitsch et al[17] and Karaman et al [18] used lornoxicam and they did not detect problems with surgical bleeding, bleeding time, blood transfusion requirement or postoperative bleeding. Stroissnig et al reported that overall, in healthy adult volunteers, oral doses of lornoxicam up to 70 mg have been well tolerated, and there have been no effects on vital signs, urine analysis parameters or clinical serum biochemistry [19]. In our study, none of the patients receiving study drugs experienced severe gastric discomfort, needed rescue antiemetic medication or required admission because of poor pain control. Previous studies used lornoxicam for reduction of postoperative opioid consumption but none of them had studied the intra-operative use of lornoxicam. So, we selected certain type of surgical procedures which might be suitable to use lornoxicam as a sole intra-operative analgesia. The adjunctive use of acetaminophen may have additive analgesic efficacy to lornoxicam because of its intrinsic opioid-sparing activity. Measurement of serum catecholamine would have been useful. These could be considered as a limitation for the present study. Conclusion: Intravenous 16 mg lornoxicam with the present study design was comparable to 100 µg fentanyl as intra-operative analgesia but more effective than fentanyl in preventing early postoperative pain in mild to moderate ENT surgical procedures. Intravenous lornoxicam 8 mg was not satisfactory as a sole intra-operative analgesia. The overall incidence of adverse effects of lornoxicam was lower than that of fentanyl.
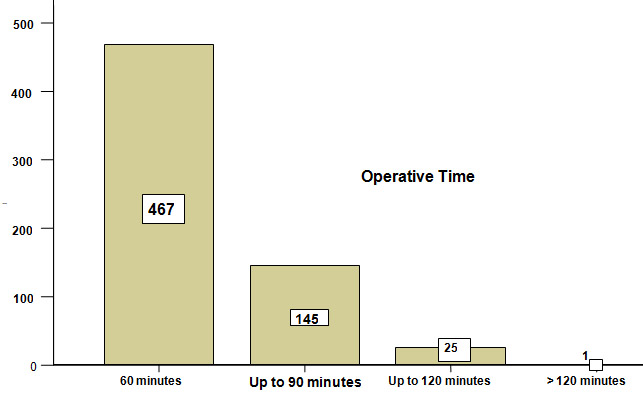 Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation
Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation  Assessment of spasticity Before any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale
Assessment of spasticity Before any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale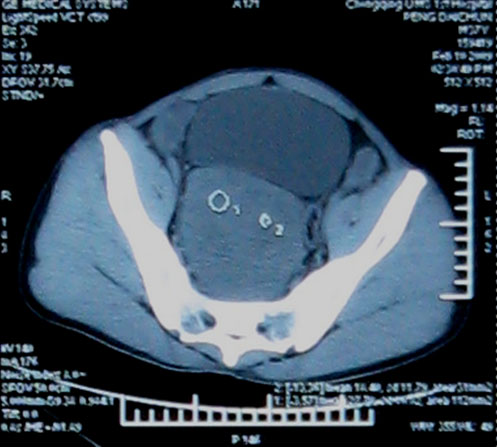
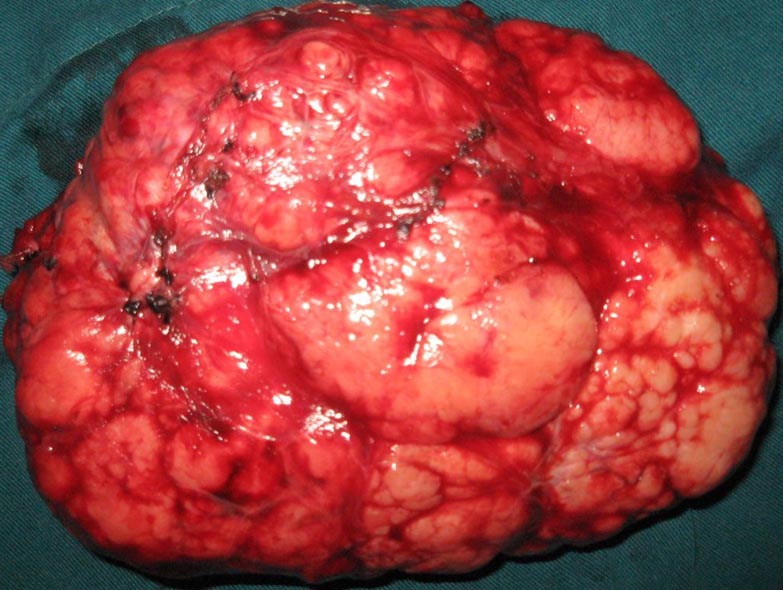
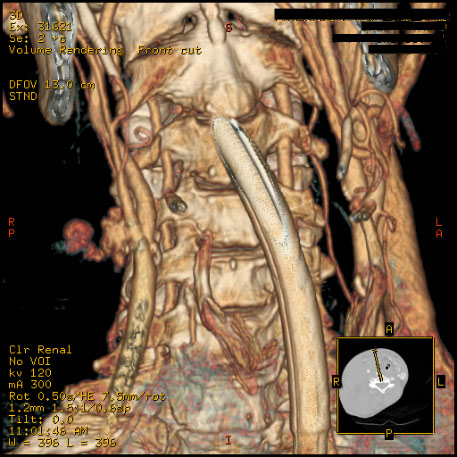
 Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements
Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements  Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae
Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae  Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.
Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.
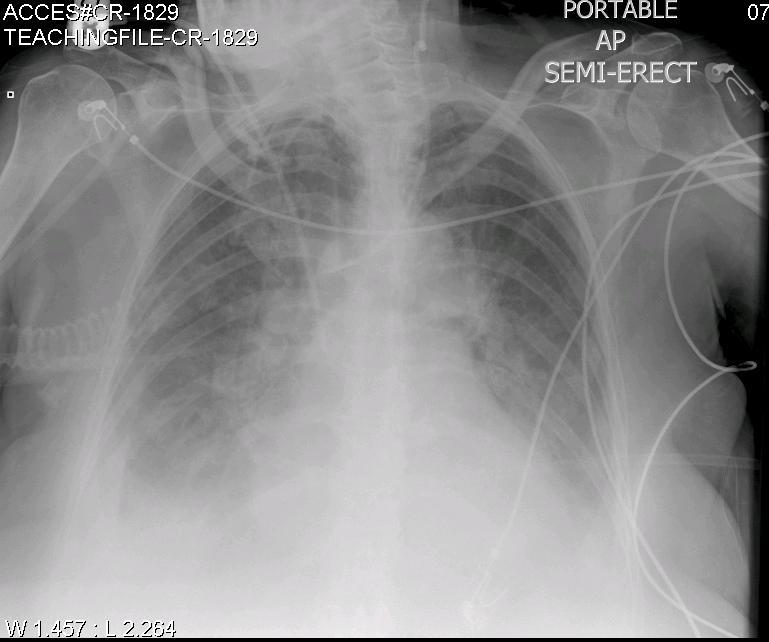
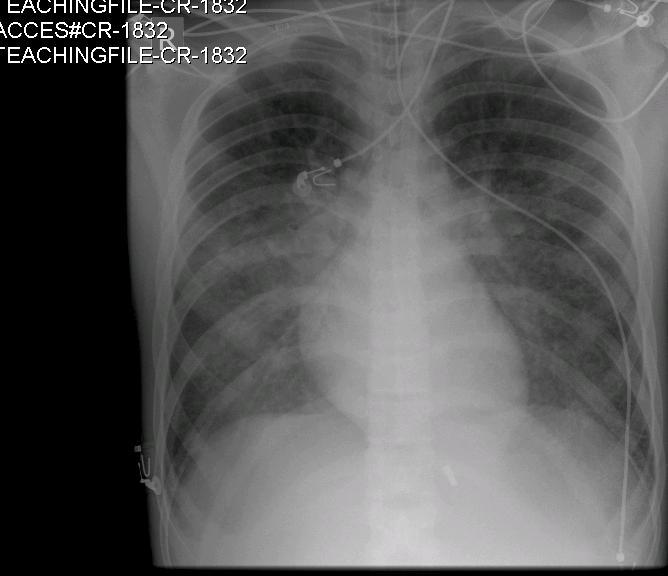
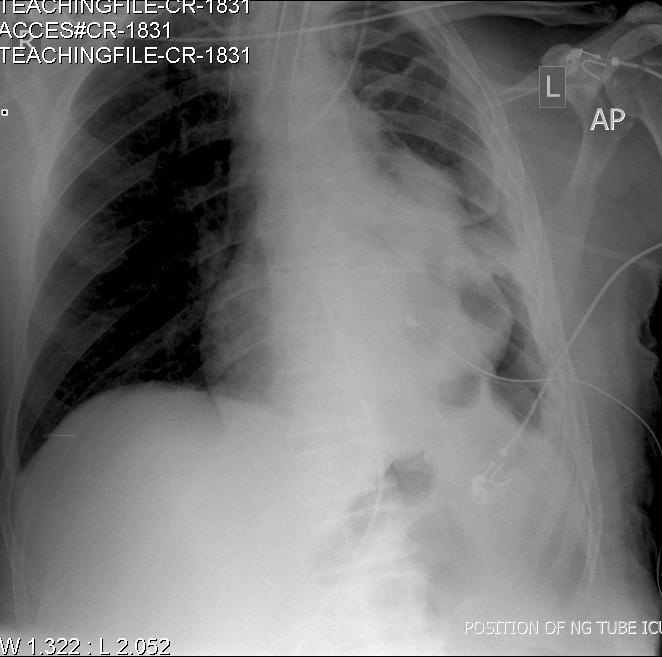



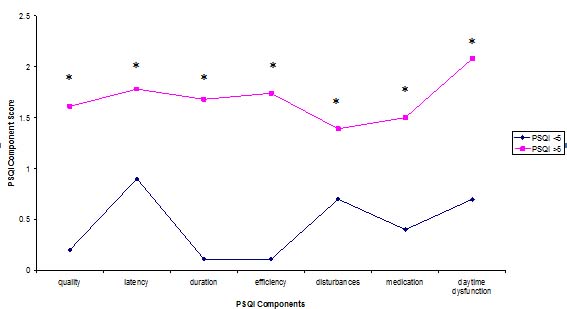
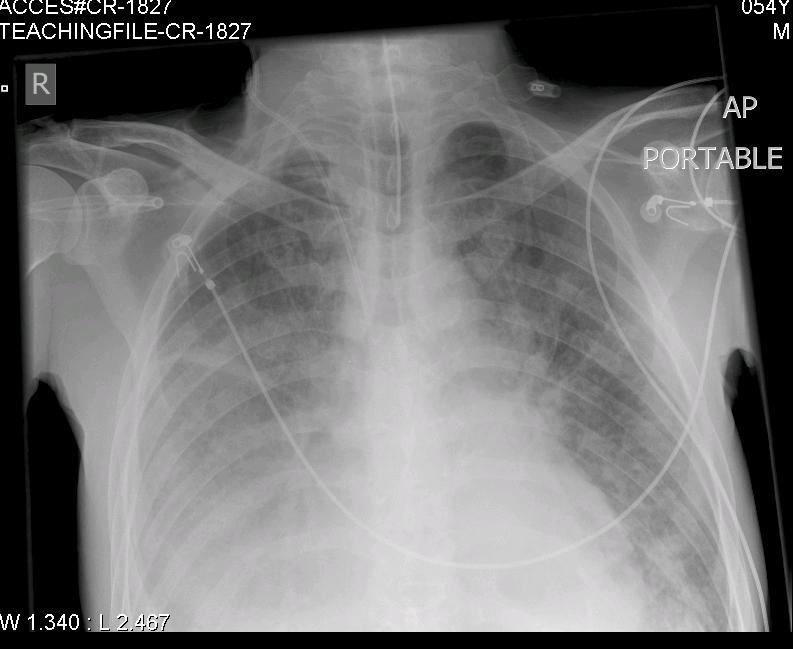

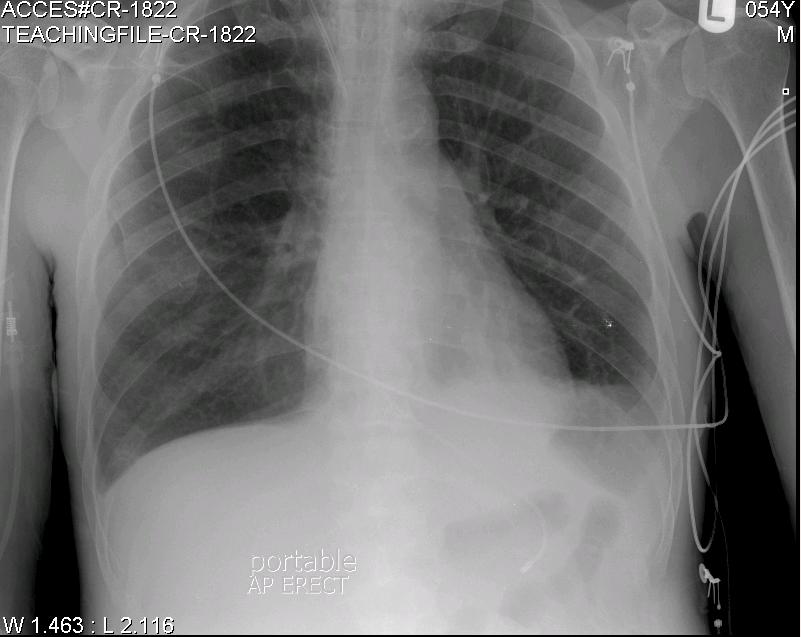
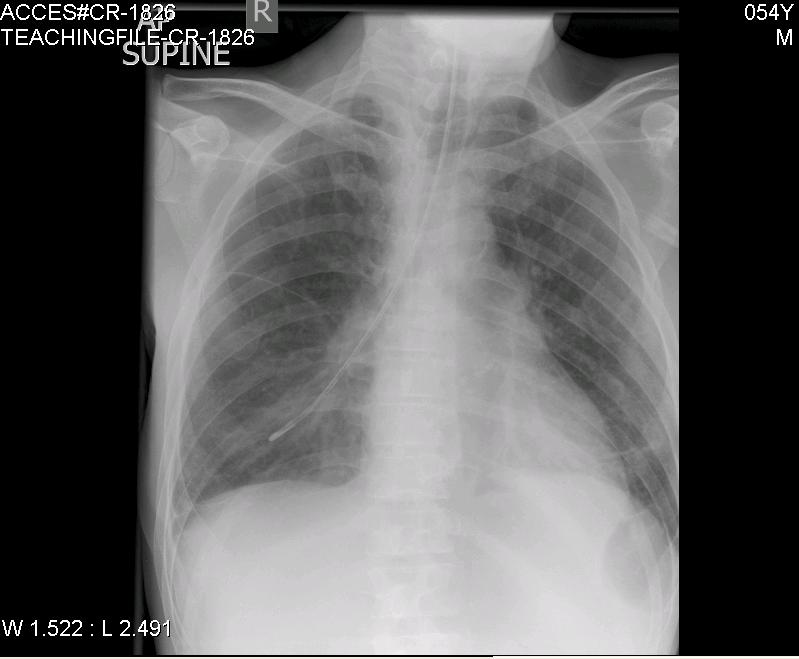



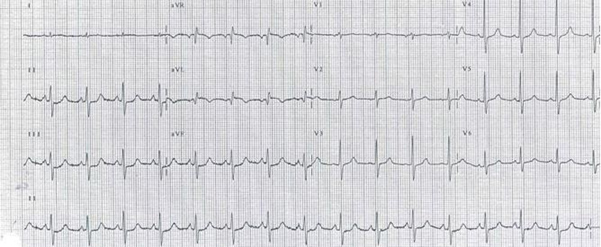

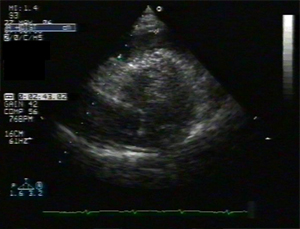

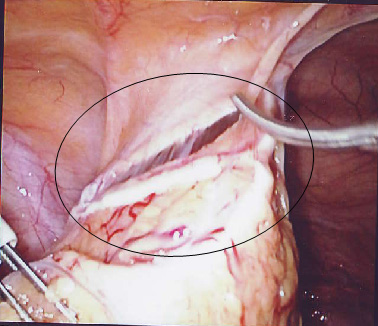

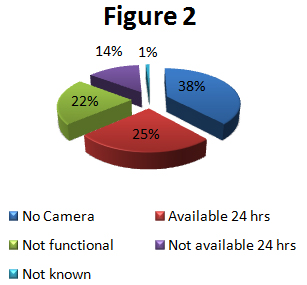
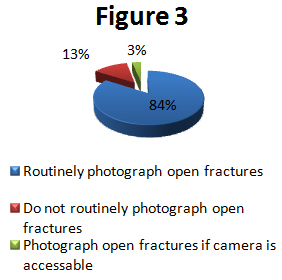
BJMP September 2009 Volume 2 Number 3
BJMP September 2009 Volume 2 Number 3
Full Issue Booklet (All articles)
PDF
Full issue Booklet
Editorial
Global Health Challenges: The Indian Conundrum
Rajan Madhok
Full Text
PDF
Review Articles
The Mental Capacity Act 2005: What it does and some thoughts on its impact on practice
Diane Brown
Full Text
PDF
Erythropoietin Friend or Foe in Chronic Kidney Disease Anemia: An Analysis of Randomized Controlled Trials, Observational Studies and Meta-analyses.
Amir Hayat
Full Text
PDF
Leg Ulcers in Older People: A Review of Management
Adeyemi Adeyi, Sharon Muzerengi, and Indrajit Gupta
Full Text
PDF
Approach to spasticity in General practice
Ganesh Bavikatte and Tarek Gaber
Full Text
PDF
Team Assessment Behaviour (TAB) as an assessment tool: A critical evaluation.
Milind Pant, Prabhu N Nesargikar and Daniel M Cocker
Full Text
PDF
Research Articles
Open Mesh Repair Of Different Hernia. Is The Technique Free Of Complications?
Arshad M Malik, Asad Khan, K Altaf Hussain Talpur and Abdul Aziz Laghari
Full Text
PDF
UK Junior Doctors’ Experience of Clinical Audit in the Foundation Programme
Andrew Cai, John Greenall And Dau Col Dau Ding
Full Text
PDF
Analgesia in day-case ENT surgery: The efficacy of lornoxicam
Mohamed Daabiss, Medhat Al-Sherbiny, Rashed Al-Otaibi and Rima Al-Nimar
Full Text
PDF
Case Reports
A case report of a Giant Schwannoma of the Mesorectum
Gopall Jayprakash , Cheng Yong and Wang Yanqing
Full Text
PDF
Anaesthetic management of a patient with Klippel-Feil syndrome for elective Caesarean section
M K Kada Venkata, Jameel Ahmed Khan, Muhammad Tayyab Qureshi, Asif Qureshi, Imtiaz Kar
Full Text
PDF
A case of accidental carotid artery cannulation in a patient for Hemofilter: complication and management
Sanil Nair , Harshal Wagh , Kavita Mordani and Salim Bhuiyan
Full Text
PDF
View Point
The dysfunctional relationship between trainer and trainee: mother of all problems
Minal Mistry and Javed Latoo
Full Text
PDF
Clinical Practice
Emergency Contraception
Anita Sharma
Full Text
PDF
Medicine in Pictures
Pictorial essay III: Permanent pacemakers and Oesophageal Doppler probe
Krishnan Melarkode and M Y Latoo
Full Text
PDF
Miscellaneous
Upcoming Medical Conferences & Meetings
Full Text
PDF
Corrections in Previous Issues
Full Text
PDF